what you need to know about diabetes and footcare€¦ · what you need to know about diabetes and...
TRANSCRIPT
1
What you need to know about diabetes and footcare.
Peter G. Guy B.Sc D.ChPrivate Practice Whitby and Peterborough, ONProfessor Podiatric Medicine Program, Michener InstituteAdvisory Board Paris Orthotics Ltd, Vancouver
CLHIA Claims Section Annual ConferenceMay 4 – May 7, 2010 Fairmont Queen ElizabethMontréal, Québec
Diabetes is a serious chronic disease that is a leading cause of lower limb amputations in Canada.
The private health insurance industry will have to navigate some difficult economic challenges.
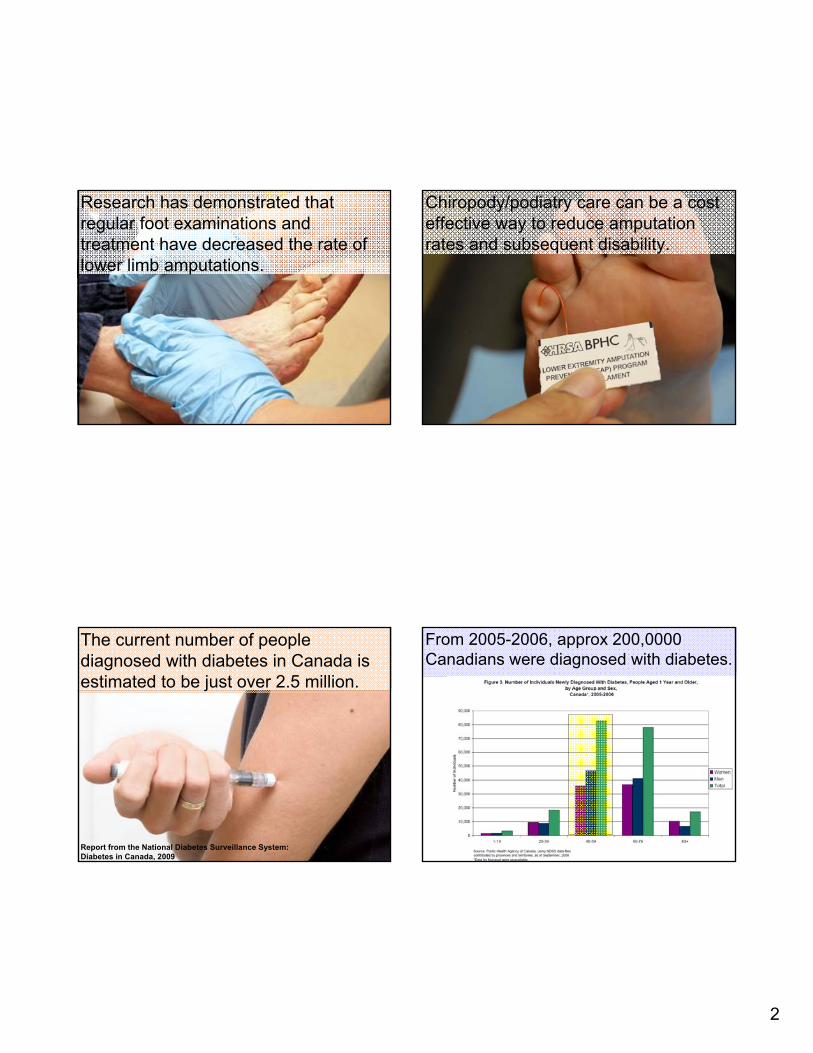
Over the next 10 -15 years the cases of diabetes are projected to reach epidemic levels in Canada.
2
Research has demonstrated that regular foot examinations and treatment have decreased the rate of lower limb amputations.
Chiropody/podiatry care can be a cost effective way to reduce amputation rates and subsequent disability.
The current number of people diagnosed with diabetes in Canada is estimated to be just over 2.5 million.
Report from the National Diabetes Surveillance System:Diabetes in Canada, 2009
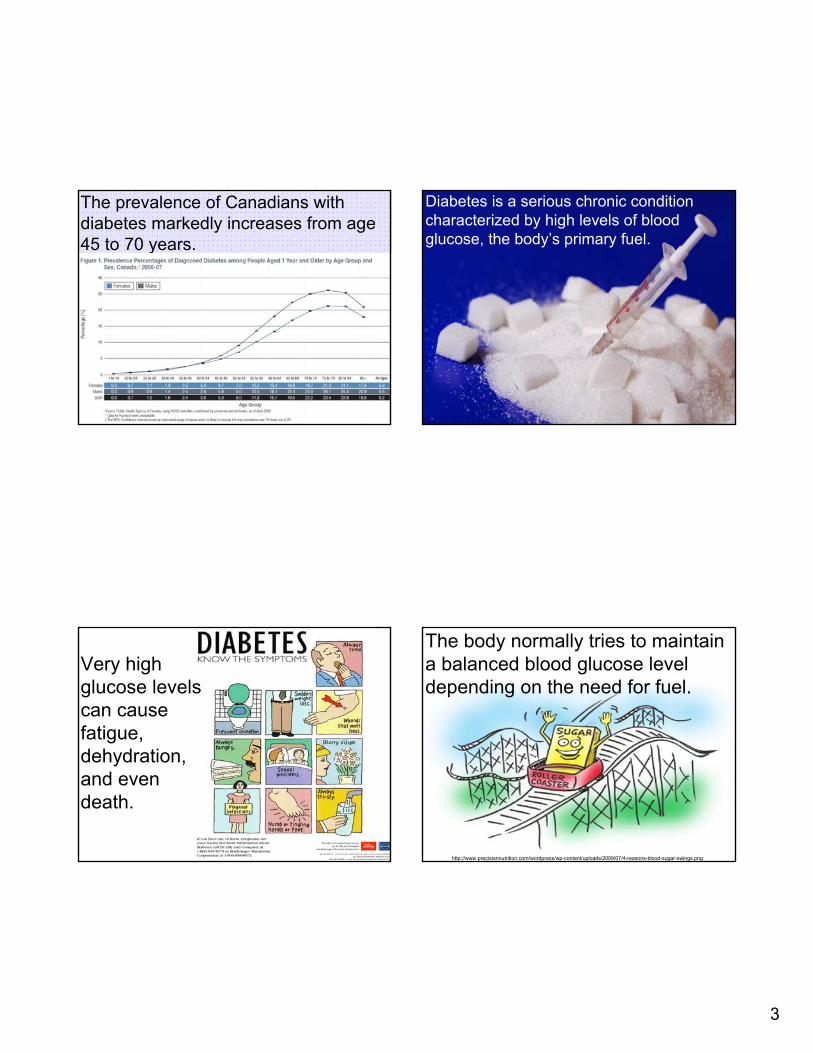
From 2005-2006, approx 200,0000 Canadians were diagnosed with diabetes.
3
The prevalence of Canadians with diabetes markedly increases from age 45 to 70 years.
Diabetes is a serious chronic conditioncharacterized by high levels of blood glucose, the body’s primary fuel.
Very high glucose levels can cause fatigue, dehydration, and even death.
The body normally tries to maintain a balanced blood glucose level depending on the need for fuel.
http://www.precisionnutrition.com/wordpress/wp-content/uploads/2009/07/4-reasons-blood-sugar-swings.png
4
The body reduces high blood sugar using insulin.
http://www.morefocused.com/images/imgRI-blood-sugar-levels.gif
Glucose is transferred from the blood stream into tissue cells through the action of insulin.
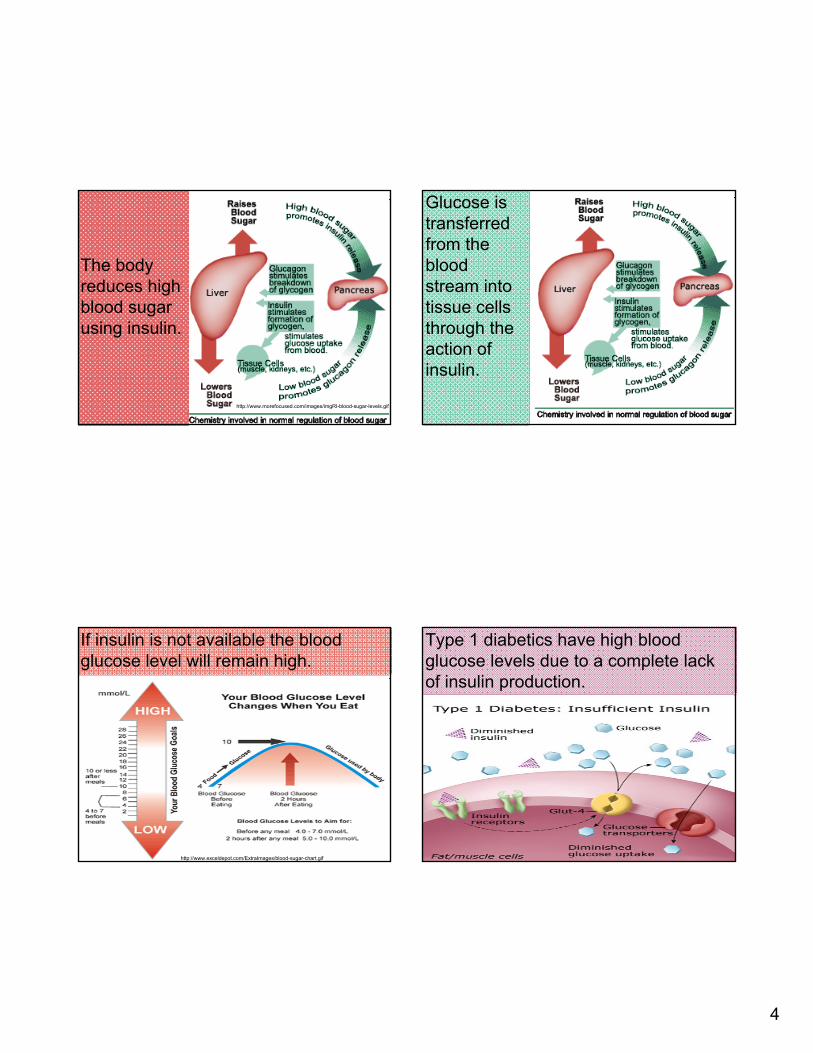
If insulin is not available the blood glucose level will remain high.
http://www.exceldepot.com/ExtraImages/blood-sugar-chart.gif
Type 1 diabetics have high blood glucose levels due to a complete lack of insulin production.
5
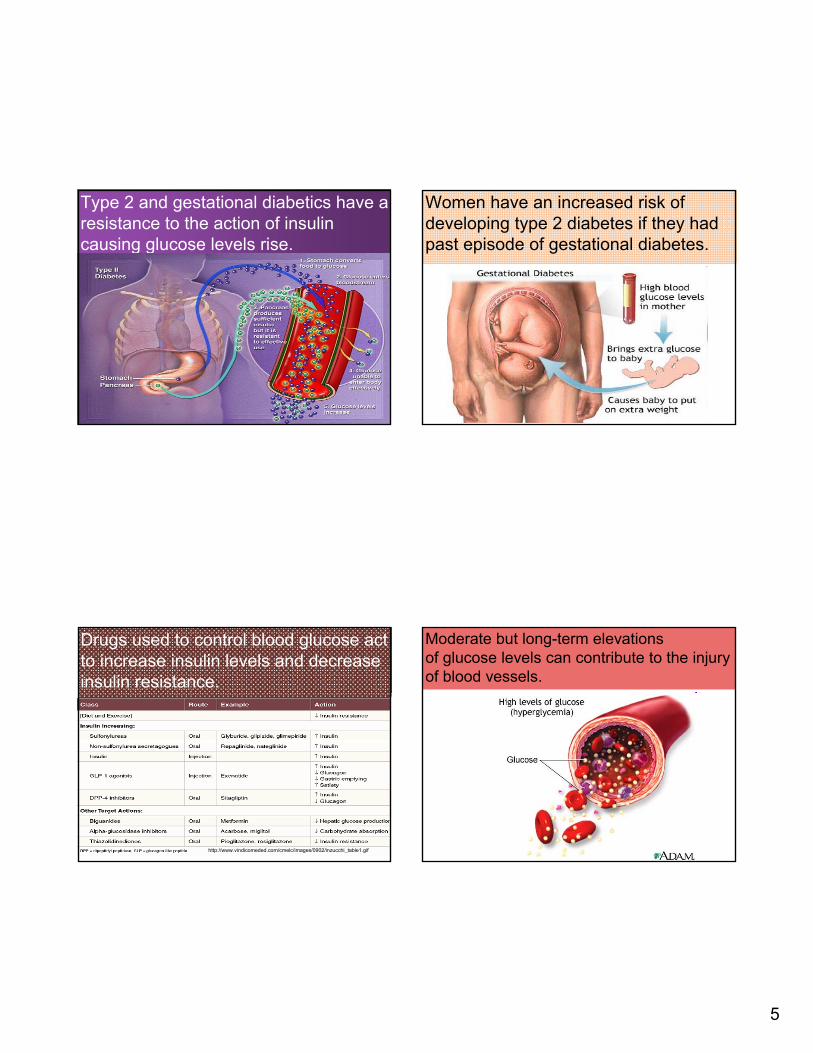
Type 2 and gestational diabetics have a resistance to the action of insulin causing glucose levels rise.
Women have an increased risk of developing type 2 diabetes if they had past episode of gestational diabetes.
Drugs used to control blood glucose act to increase insulin levels and decrease insulin resistance.
http://www.vindicomeded.com/cmelc/images/0902/inzucchi_table1.gif
Moderate but long-term elevationsof glucose levels can contribute to the injury of blood vessels.
6
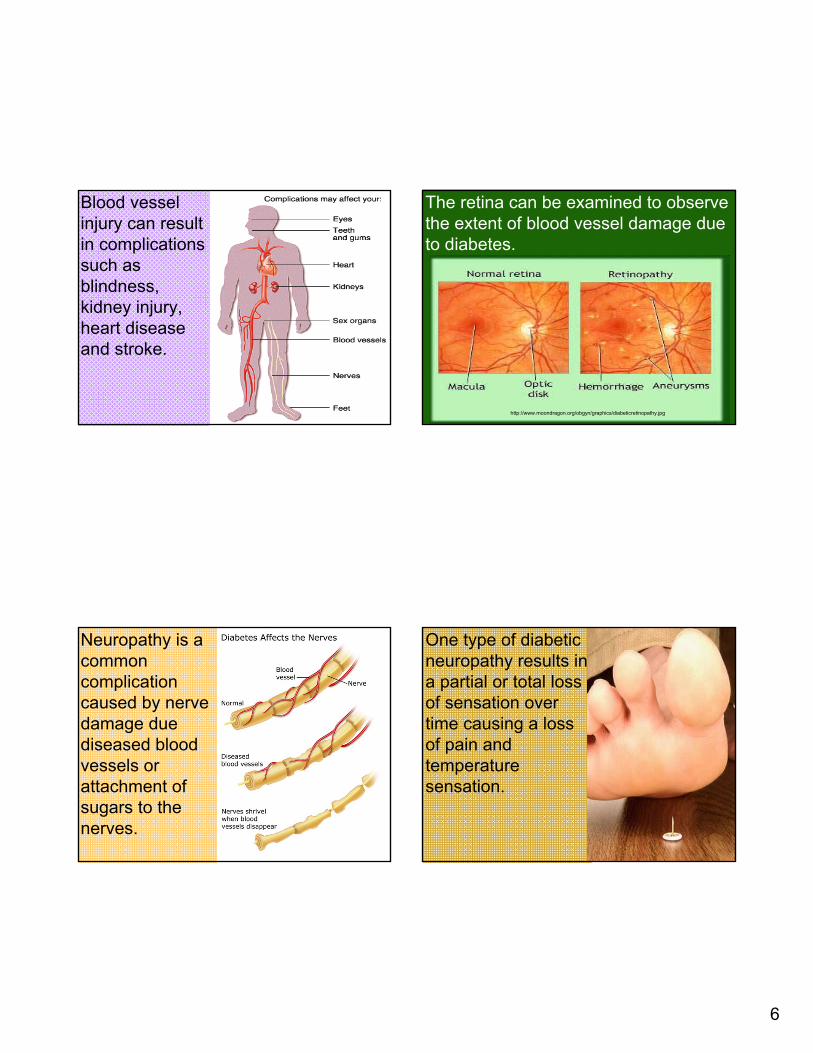
Blood vessel injury can result in complications such as blindness,kidney injury, heart disease and stroke.
The retina can be examined to observe the extent of blood vessel damage due to diabetes.
http://www.moondragon.org/obgyn/graphics/diabeticretinopathy.jpg
Neuropathy is a common complication caused by nerve damage due diseased blood vessels or attachment of sugars to the nerves.
One type of diabetic neuropathy results in a partial or total loss of sensation over time causing a loss of pain and temperature sensation.
7
In the lower extremity, a lack of sensation can lead to skin ulceration and possibly amputation due to infection.
The importance of controlling blood sugars
Two multicenter, randomized, 10 year, studies demonstrated that intensive glucose control delayed the appearance of diabetic complications.
Hemoglobin A1C is used as indicator of blood glucose control during the previous 3 months.
8
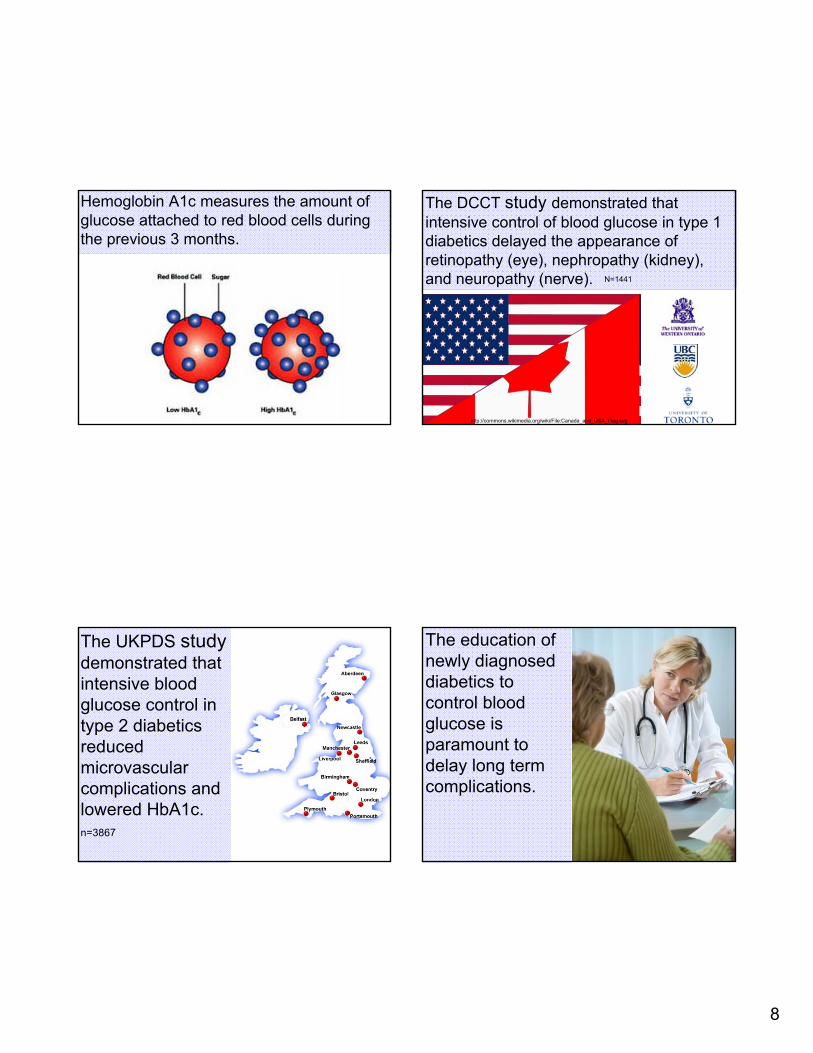
Hemoglobin A1c measures the amount of glucose attached to red blood cells during the previous 3 months.
The DCCT study demonstrated that intensive control of blood glucose in type 1 diabetics delayed the appearance of retinopathy (eye), nephropathy (kidney), and neuropathy (nerve). N=1441
http://commons.wikimedia.org/wiki/File:Canada_and_USA_Flag.svg
The UKPDS studydemonstrated that intensive blood glucose control in type 2 diabetics reduced microvascularcomplications and lowered HbA1c.n=3867
The education of newly diagnosed diabetics to control blood glucose is paramount to delay long term complications.
9
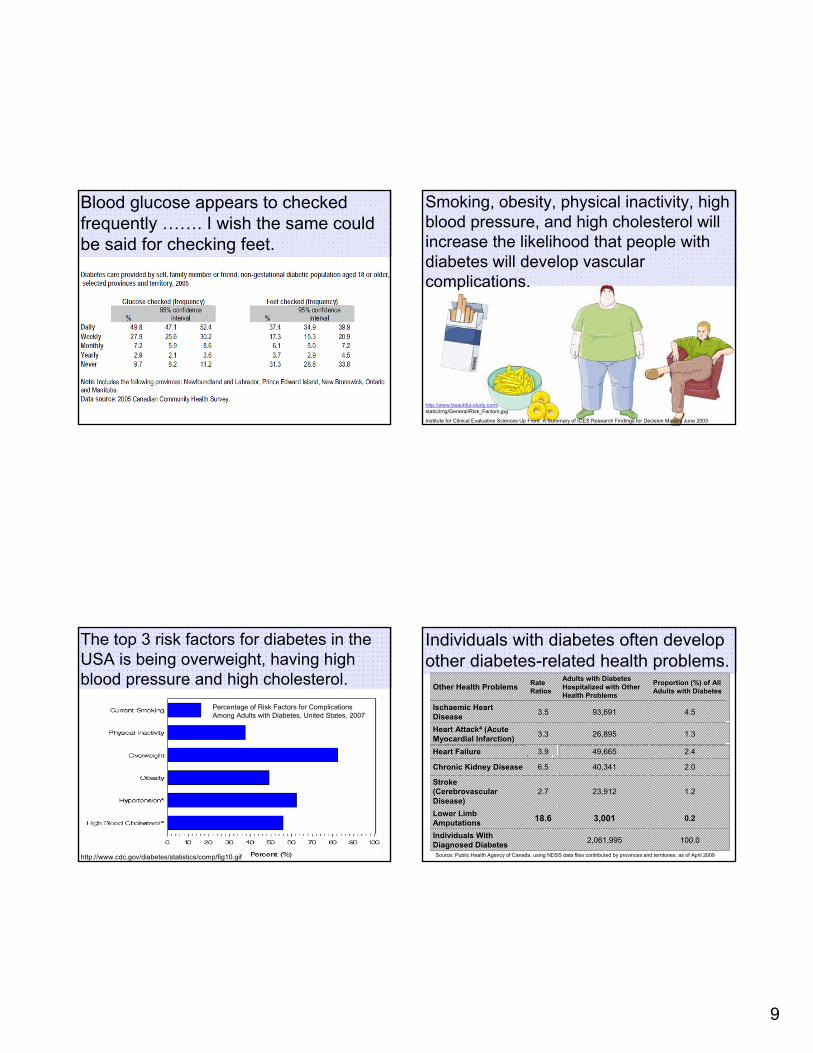
Blood glucose appears to checked frequently ……. I wish the same could be said for checking feet.
Smoking, obesity, physical inactivity, high blood pressure, and high cholesterol will increase the likelihood that people with diabetes will develop vascular complications.
http://www.beautiful-study.com/static/img/General/Risk_Factors.jpg
Institute for Clinical Evaluative Sciences Up Front A Summary of ICES Research Findings for Decision Makers June 2003
The top 3 risk factors for diabetes in the USA is being overweight, having high blood pressure and high cholesterol.
http://www.cdc.gov/diabetes/statistics/comp/fig10.gif
Percentage of Risk Factors for Complications Among Adults with Diabetes, United States, 2007
Individuals with diabetes often develop other diabetes-related health problems.
100.02,061,995Individuals With Diagnosed Diabetes
0.23,00118.6Lower Limb Amputations
1.223,9122.7Stroke (CerebrovascularDisease)
2.040,3416.5Chronic Kidney Disease
2.449,6653.9Heart Failure
1.326,8953.3Heart Attack4 (Acute Myocardial Infarction)
4.593,6913.5Ischaemic Heart Disease
Proportion (%) of All Adults with Diabetes
Adults with Diabetes Hospitalized with Other Health Problems
Rate RatiosOther Health Problems
Source: Public Health Agency of Canada, using NDSS data files contributed by provinces and territories, as of April 2009
10
In 2005, 63% of adults with diabetes (1.3 million) also had a diagnosis of hypertension which is 3 times more often than those without diabetes.
Your Community, Your Health: Findings from the Canadian Community Health Survey 3.1 (2005) Smoking and Diabetes Care: Results from the CCHS Cycle
Cardiovascular disease is the leading cause of death among persons with diabetes as compared to the general population.
Hux J E., Booth G L., Slaughter PM., Laupacis A., Diabetes in Ontario ,Diabetes and cardiac disease 5.124
Strategies have been developed to minimize all diabetic complications.
Unfortunately, with all the interventions diabetes is a major public health problem and economic burden due to the long term complications of uncontrolled diabetes.
http://blog.mlive.com/saginawnews_impact/2009/04/large_APS.Diabetes.jpg
11
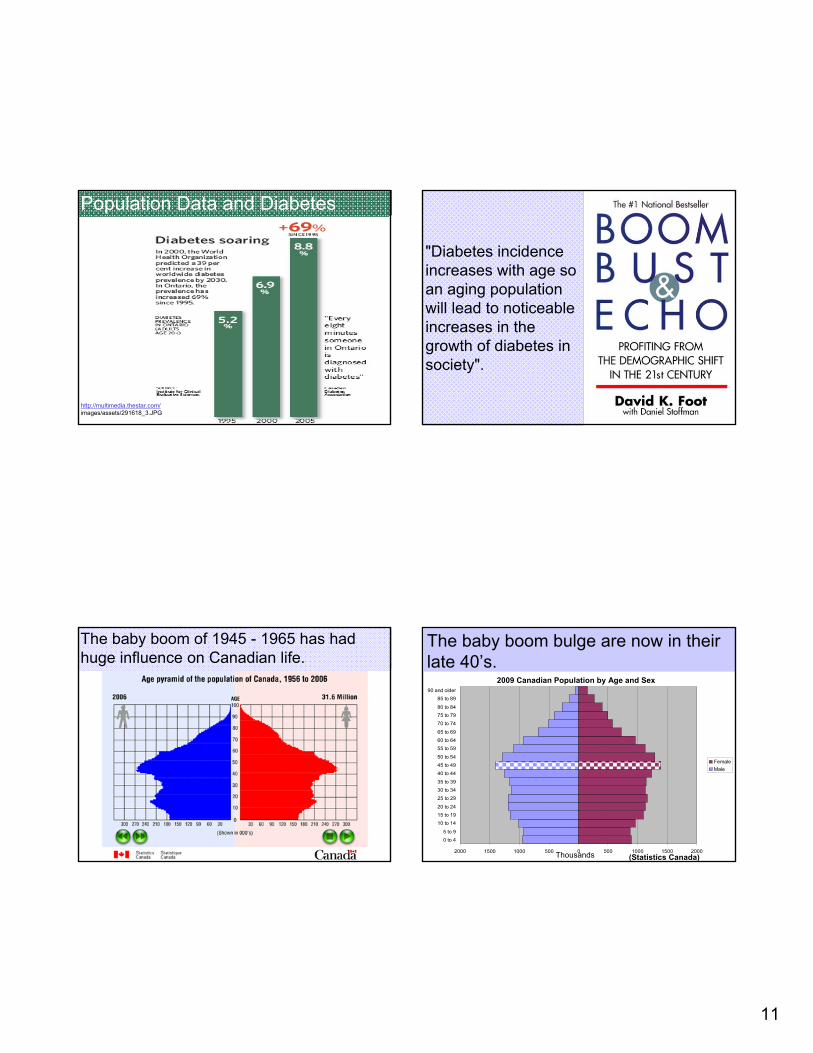
Population Data and Diabetes
http://multimedia.thestar.com/images/assets/291618_3.JPG
"Diabetes incidence increases with age so an aging population will lead to noticeable increases in the growth of diabetes in society".
The baby boom of 1945 - 1965 has had huge influence on Canadian life.
2000 1500 1000 500 0 500 1000 1500 2000
0 to 45 to 9
10 to 1415 to 1920 to 24
25 to 2930 to 3435 to 39
40 to 4445 to 4950 to 54
55 to 5960 to 6465 to 69
70 to 7475 to 7980 to 84
85 to 8990 and older
FemaleMale
The baby boom bulge are now in their late 40’s.
2009 Canadian Population by Age and Sex
Thousands (Statistics Canada)
12
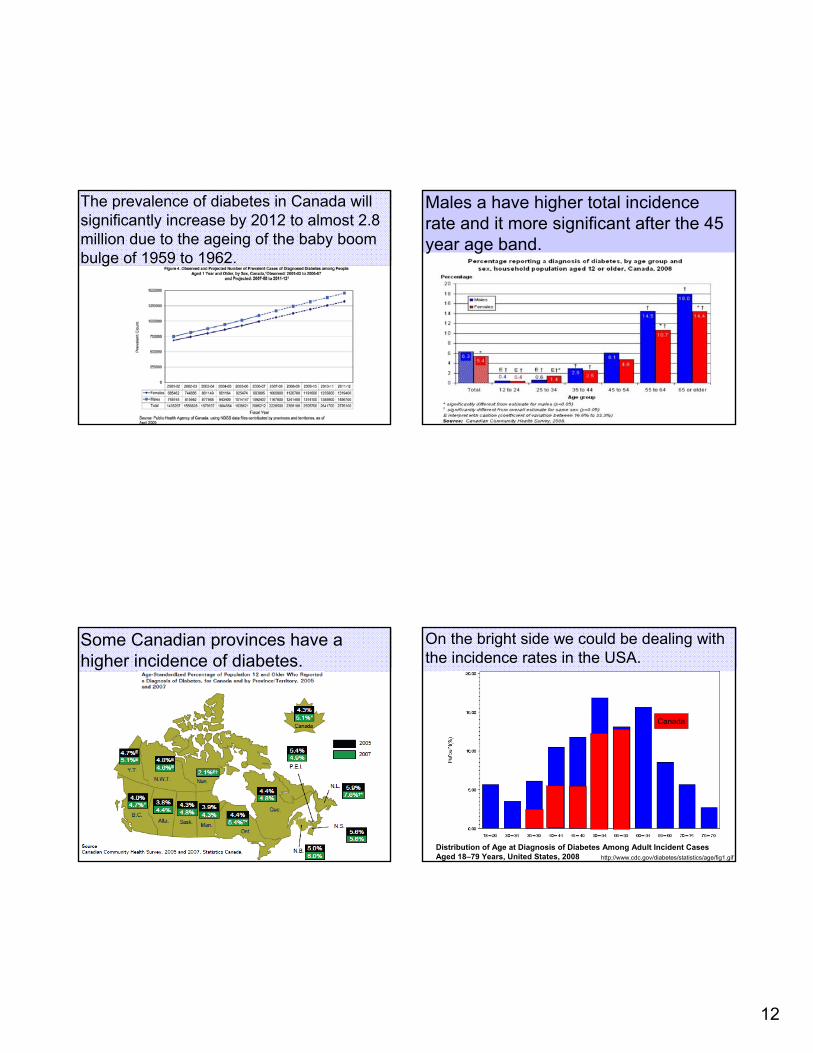
The prevalence of diabetes in Canada will significantly increase by 2012 to almost 2.8 million due to the ageing of the baby boom bulge of 1959 to 1962.
Males a have higher total incidence rate and it more significant after the 45 year age band.
Some Canadian provinces have a higher incidence of diabetes.
On the bright side we could be dealing with the incidence rates in the USA.
http://www.cdc.gov/diabetes/statistics/age/fig1.gifDistribution of Age at Diagnosis of Diabetes Among Adult Incident Cases Aged 18–79 Years, United States, 2008
Canada
13
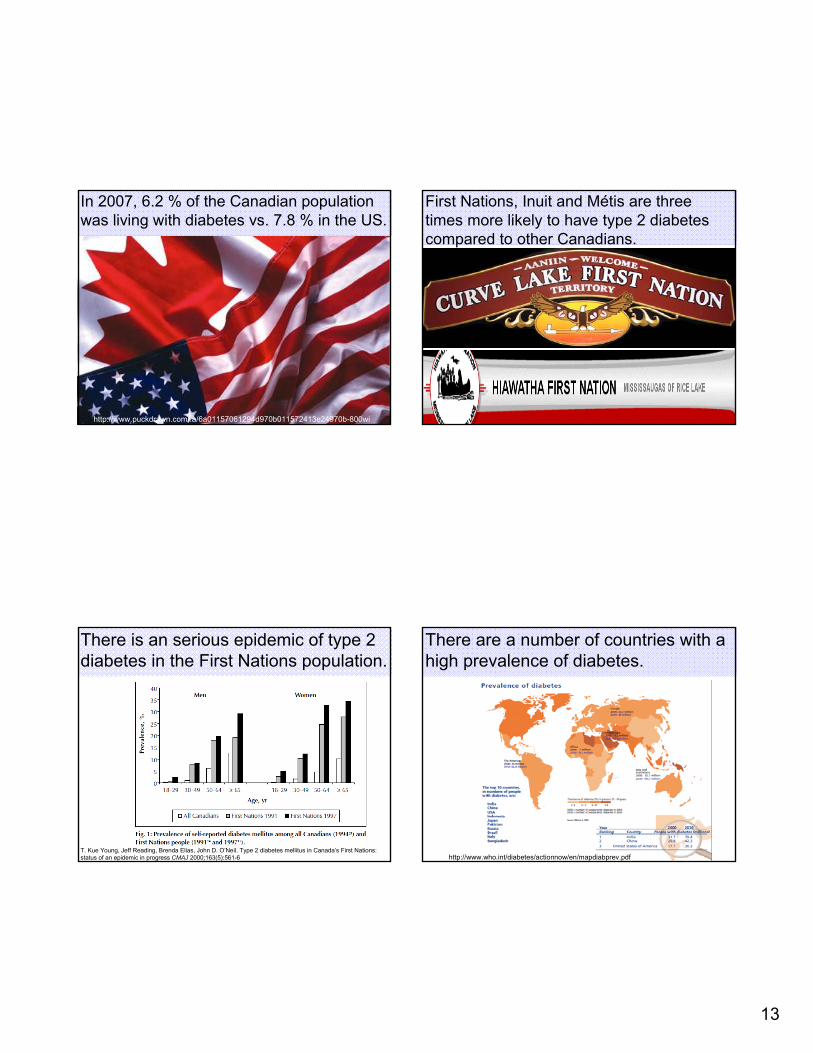
In 2007, 6.2 % of the Canadian population was living with diabetes vs. 7.8 % in the US.
http://www.puckdrawn.com/.a/6a01157061294d970b011572413e24970b-800wi
First Nations, Inuit and Metis are three times more likely to have type 2 diabetes compared to other Canadians.
´
There is an serious epidemic of type 2 diabetes in the First Nations population.
T. Kue Young, Jeff Reading, Brenda Elias, John D. O’Neil. Type 2 diabetes mellitus in Canada’s First Nations: status of an epidemic in progress CMAJ 2000;163(5):561-6
There are a number of countries with a high prevalence of diabetes.
http://www.who.int/diabetes/actionnow/en/mapdiabprev.pdf
14
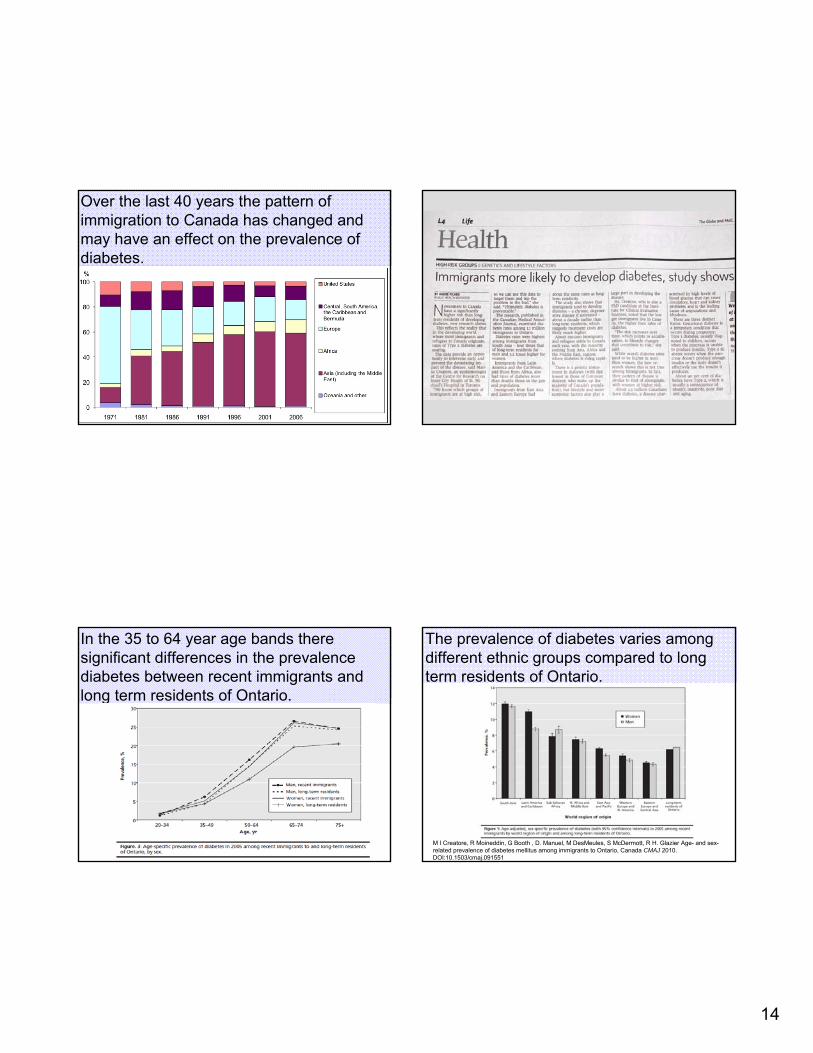
Over the last 40 years the pattern of immigration to Canada has changed and may have an effect on the prevalence of diabetes.
In the 35 to 64 year age bands there significant differences in the prevalence diabetes between recent immigrants and long term residents of Ontario.
The prevalence of diabetes varies among different ethnic groups compared to long term residents of Ontario.
M I Creatore, R Moineddin, G Booth , D. Manuel, M DesMeules, S McDermott, R H. Glazier Age- and sex-related prevalence of diabetes mellitus among immigrants to Ontario, Canada CMAJ 2010. DOI:10.1503/cmaj.091551
15
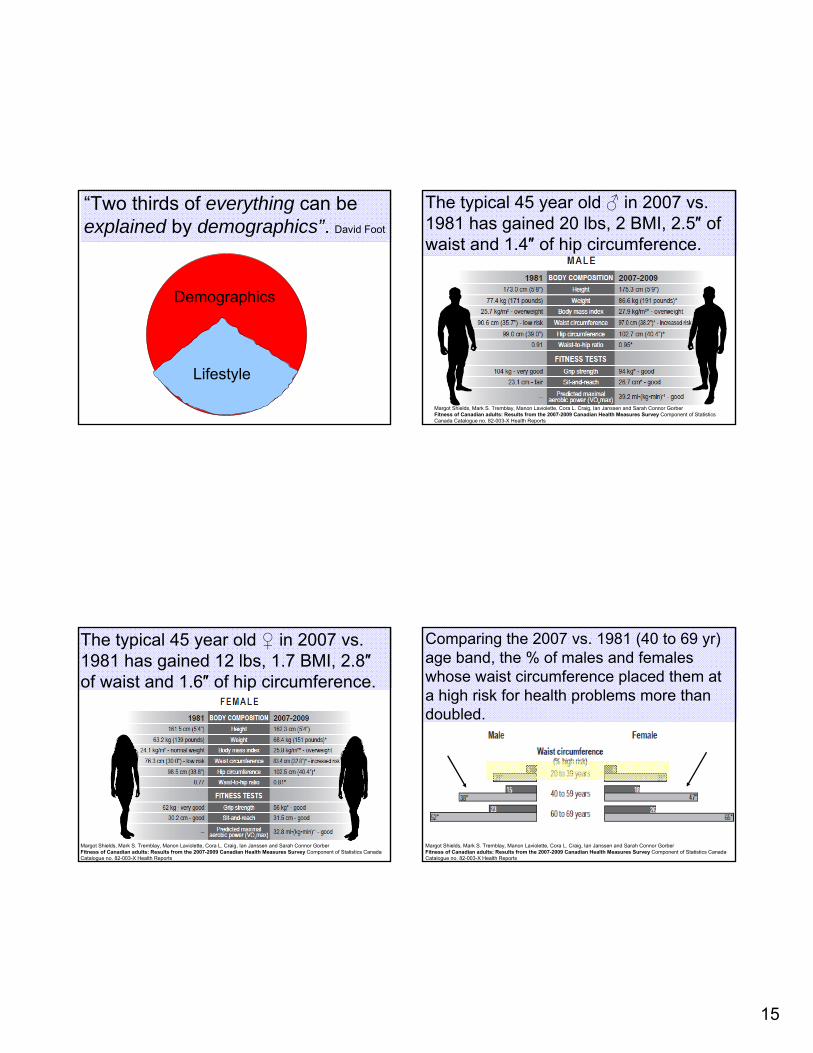
“Two thirds of everything can be explained by demographics”. David Foot
Lifestyle
Demographics
The typical 45 year old ♂ in 2007 vs. 1981 has gained 20 lbs, 2 BMI, 2.5″ of waist and 1.4″ of hip circumference.
Margot Shields, Mark S. Tremblay, Manon Laviolette, Cora L. Craig, Ian Janssen and Sarah Connor GorberFitness of Canadian adults: Results from the 2007-2009 Canadian Health Measures Survey Component of Statistics Canada Catalogue no. 82-003-X Health Reports
The typical 45 year old ♀ in 2007 vs. 1981 has gained 12 lbs, 1.7 BMI, 2.8″of waist and 1.6″ of hip circumference.
Margot Shields, Mark S. Tremblay, Manon Laviolette, Cora L. Craig, Ian Janssen and Sarah Connor GorberFitness of Canadian adults: Results from the 2007-2009 Canadian Health Measures Survey Component of Statistics Canada Catalogue no. 82-003-X Health Reports
Comparing the 2007 vs. 1981 (40 to 69 yr) age band, the % of males and females whose waist circumference placed them at a high risk for health problems more than doubled.
Margot Shields, Mark S. Tremblay, Manon Laviolette, Cora L. Craig, Ian Janssen and Sarah Connor GorberFitness of Canadian adults: Results from the 2007-2009 Canadian Health Measures Survey Component of Statistics Canada Catalogue no. 82-003-X Health Reports
16
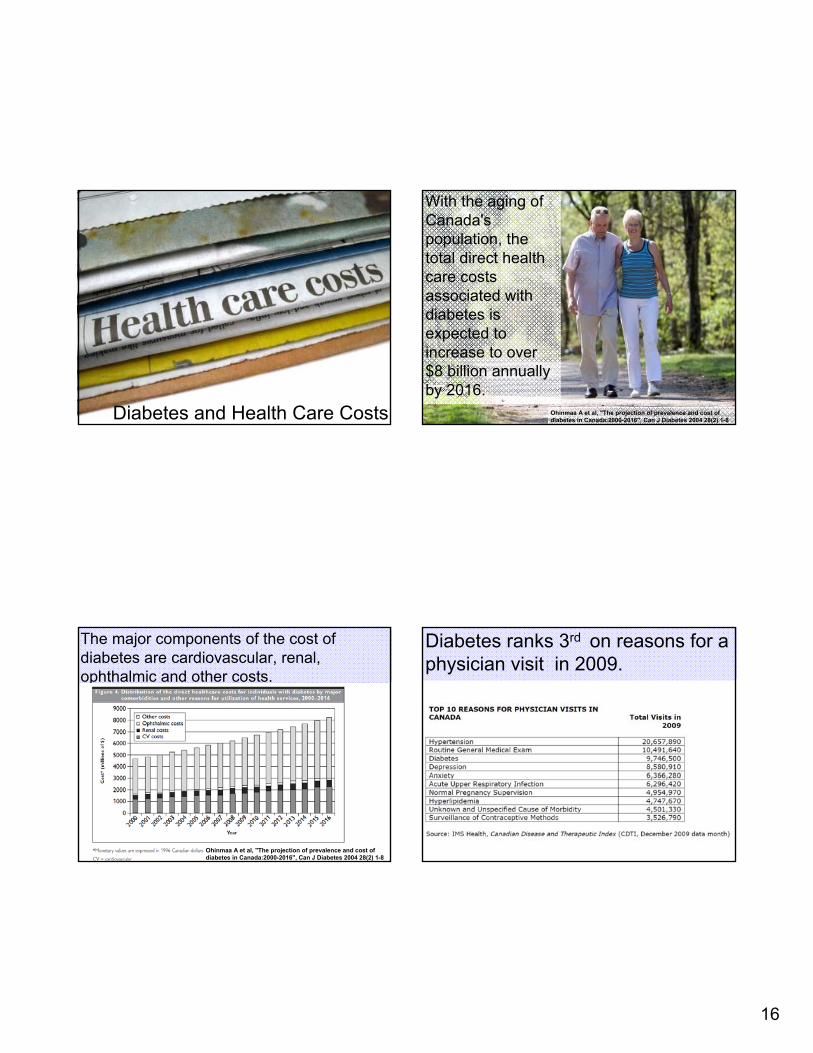
Diabetes and Health Care Costs
With the aging of Canada's population, the total direct health care costs associated with diabetes is expected to increase to over $8 billion annually by 2016.
Ohinmaa A et al, "The projection of prevalence and cost of diabetes in Canada:2000-2016", Can J Diabetes 2004 28(2) 1-8
The major components of the cost of diabetes are cardiovascular, renal, ophthalmic and other costs.
Ohinmaa A et al, "The projection of prevalence and cost of diabetes in Canada:2000-2016", Can J Diabetes 2004 28(2) 1-8
Diabetes ranks 3rd on reasons for a physician visit in 2009.
17
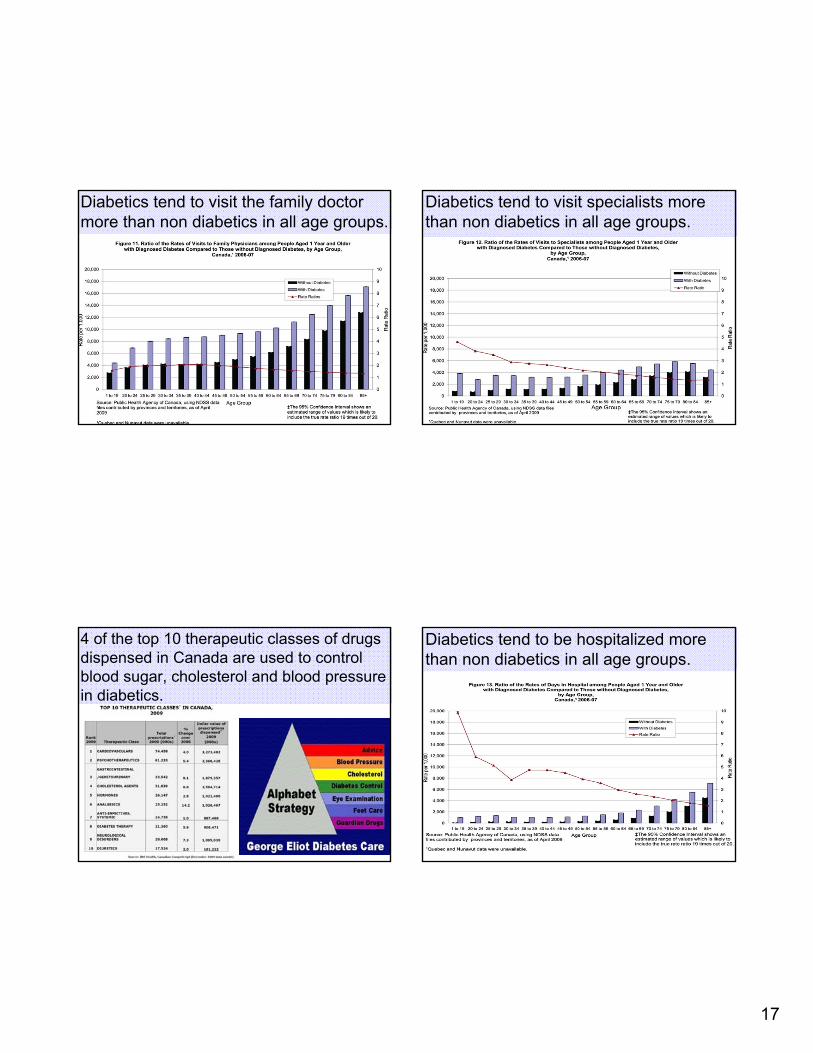
Diabetics tend to visit the family doctor more than non diabetics in all age groups.
Diabetics tend to visit specialists more than non diabetics in all age groups.
4 of the top 10 therapeutic classes of drugs dispensed in Canada are used to control blood sugar, cholesterol and blood pressure in diabetics.
Diabetics tend to be hospitalized more than non diabetics in all age groups.
18
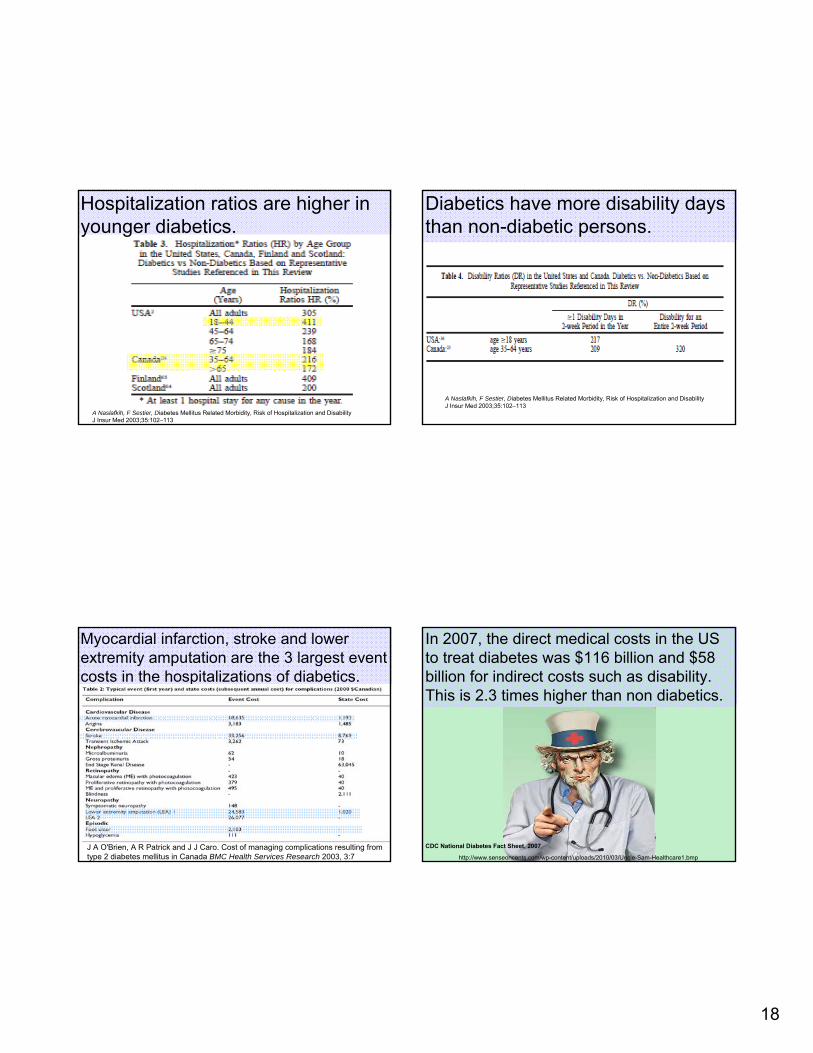
Hospitalization ratios are higher in younger diabetics.
A Naslafkih, F Sestier, Diabetes Mellitus Related Morbidity, Risk of Hospitalization and Disability J Insur Med 2003;35:102–113
Diabetics have more disability daysthan non-diabetic persons.
A Naslafkih, F Sestier, Diabetes Mellitus Related Morbidity, Risk of Hospitalization and Disability J Insur Med 2003;35:102–113
Myocardial infarction, stroke and lower extremity amputation are the 3 largest event costs in the hospitalizations of diabetics.
J A O'Brien, A R Patrick and J J Caro. Cost of managing complications resulting from type 2 diabetes mellitus in Canada BMC Health Services Research 2003, 3:7
In 2007, the direct medical costs in the US to treat diabetes was $116 billion and $58 billion for indirect costs such as disability. This is 2.3 times higher than non diabetics.
CDC National Diabetes Fact Sheet, 2007
http://www.senseoncents.com/wp-content/uploads/2010/03/Uncle-Sam-Healthcare1.bmp
19
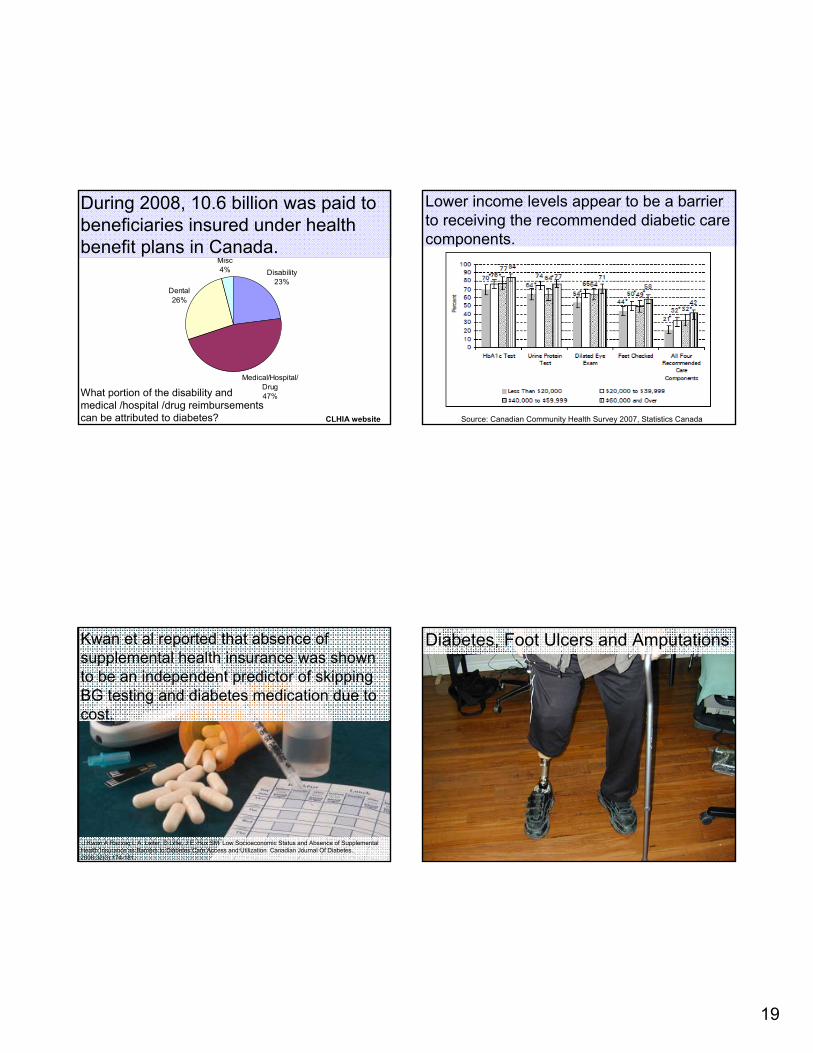
Disability23%
Dental26%
Misc4%
Medical/Hospital/Drug47%
During 2008, 10.6 billion was paid to beneficiaries insured under health benefit plans in Canada.
CLHIA website
What portion of the disability and medical /hospital /drug reimbursements can be attributed to diabetes?
Lower income levels appear to be a barrier to receiving the recommended diabetic care components.
Source: Canadian Community Health Survey 2007, Statistics Canada
Kwan et al reported that absence of supplemental health insurance was shown to be an independent predictor of skipping BG testing and diabetes medication due to cost.
J Kwan A Razzaq L A. Leiter, D Lillie, J E. Hux SM Low Socioeconomic Status and Absence of Supplemental Health Insurance as Barriers to Diabetes Care Access and Utilization Canadian Journal Of Diabetes. 2008;32(3):174-181.
Diabetes, Foot Ulcers and Amputations
20
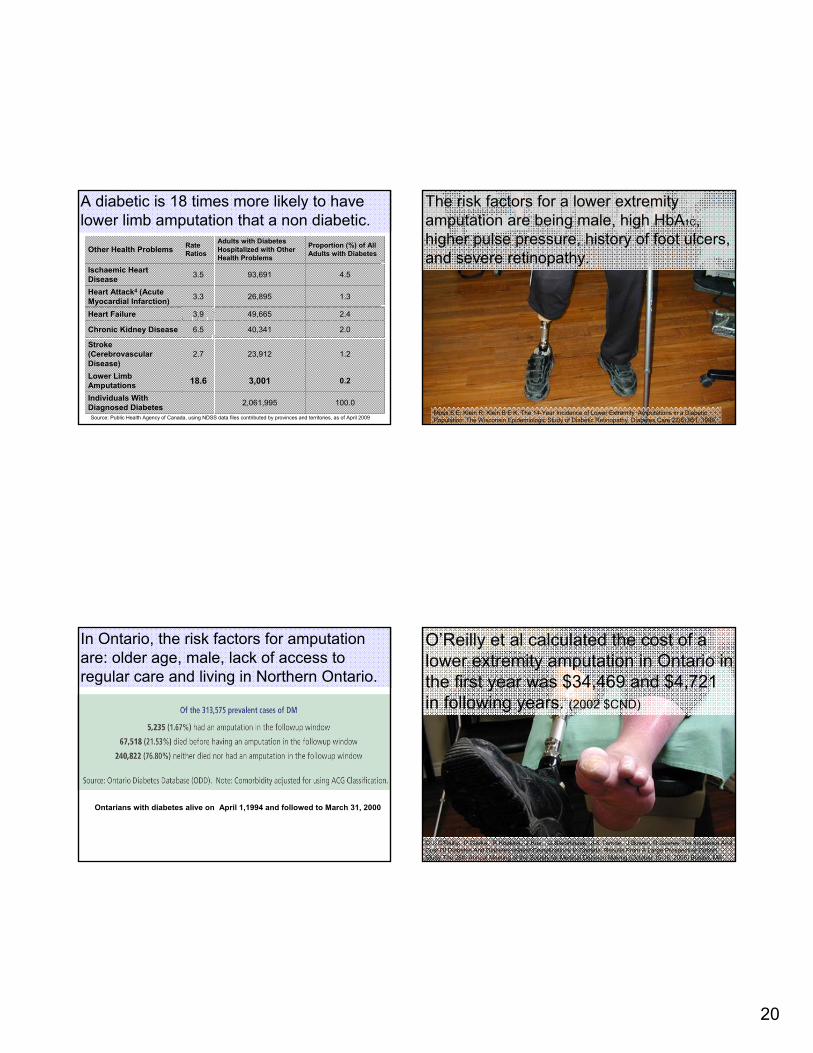
A diabetic is 18 times more likely to have lower limb amputation that a non diabetic.
100.02,061,995Individuals With Diagnosed Diabetes
0.23,00118.6Lower Limb Amputations
1.223,9122.7Stroke (CerebrovascularDisease)
2.040,3416.5Chronic Kidney Disease
2.449,6653.9Heart Failure
1.326,8953.3Heart Attack4 (Acute Myocardial Infarction)
4.593,6913.5Ischaemic Heart Disease
Proportion (%) of All Adults with Diabetes
Adults with Diabetes Hospitalized with Other Health Problems
Rate RatiosOther Health Problems
Source: Public Health Agency of Canada, using NDSS data files contributed by provinces and territories, as of April 2009
The risk factors for a lower extremity amputation are being male, high HbA1C, higher pulse pressure, history of foot ulcers, and severe retinopathy.
Moss S E, Klein R, Klein B E K, The 14-Year Incidence of Lower Extremity Amputations in a Diabetic Population: The Wisconsin Epidemiologic Study of Diabetic Retinopathy. Diabetes Care 22(6):951, 1999
In Ontario, the risk factors for amputation are: older age, male, lack of access to regular care and living in Northern Ontario.
Ontarians with diabetes alive on April 1,1994 and followed to March 31, 2000
O’Reilly et al calculated the cost of a lower extremity amputation in Ontario in the first year was $34,469 and $4,721 in following years. (2002 $CND)
D J. O'Reilly, P Clarke, R Hopkins, J Hux, , G Blackhouse, J-E Tarride, J Bowen, R Goeree The Incidence And Cost Of Diabetes And Diabetes-related Complications In Canada: Results From A Large Prospective Cohort Study The 28th Annual Meeting of the Society for Medical Decision Making (October 15-18, 2006) Boston, MA
21
A Ndip, L A. Lavery, J Lafontaine, M K. Rutter, A Vardhan, L Vileikyte, Andrew J.M. Boulton. High Levels of Foot Ulceration and Amputation Risk in a Multiracial Cohort of Diabetic Patients on Dialysis Therapy. Diabetes Care 33:878–880, 2010 http://www.dch.org.uk/img/renaldialysis.jpg
Diabetics receiving dialysis are at high risk of lower-limb complications such as neuropathy, peripheral vascular disease, history of foot ulcers or current foot ulcer.
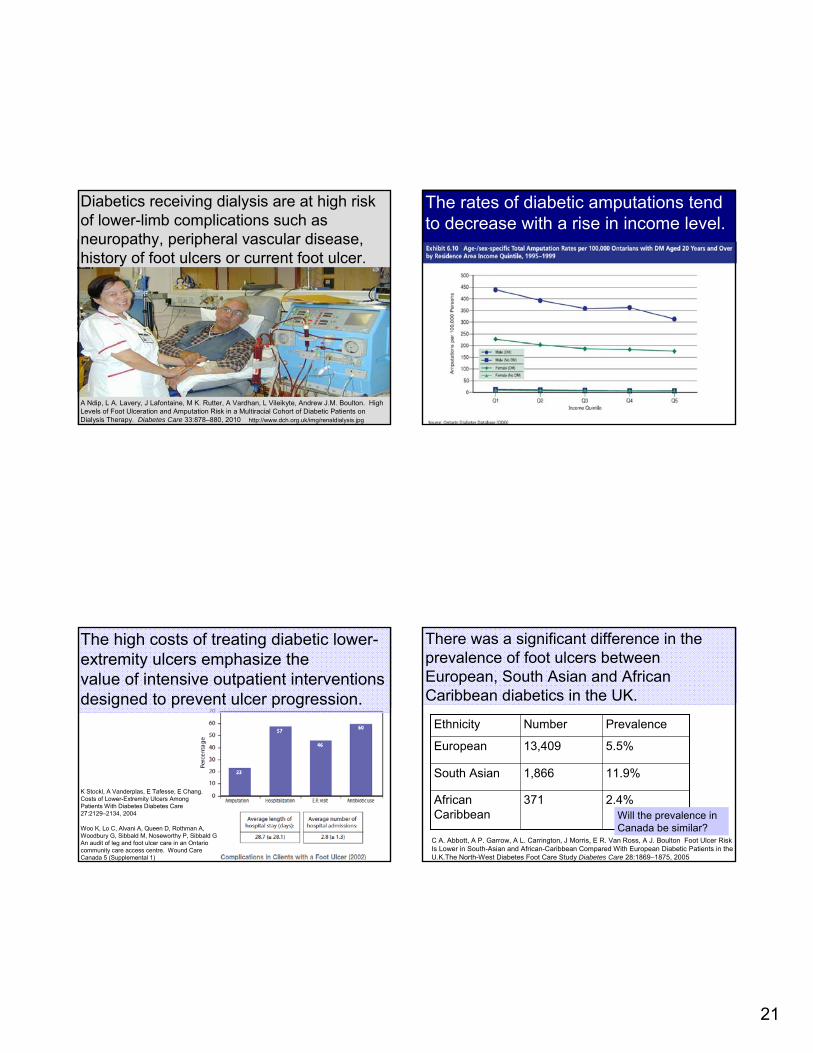
The rates of diabetic amputations tend to decrease with a rise in income level.
The high costs of treating diabetic lower-extremity ulcers emphasize thevalue of intensive outpatient interventions designed to prevent ulcer progression.
Woo K, Lo C, Alvani A, Queen D, Rothman A, Woodbury G, Sibbald M, Noseworthy P, Sibbald GAn audit of leg and foot ulcer care in an Ontario community care access centre. Wound Care Canada 5 (Supplemental 1)
K Stockl, A Vanderplas, E Tafesse, E Chang. Costs of Lower-Extremity Ulcers AmongPatients With Diabetes Diabetes Care 27:2129–2134, 2004
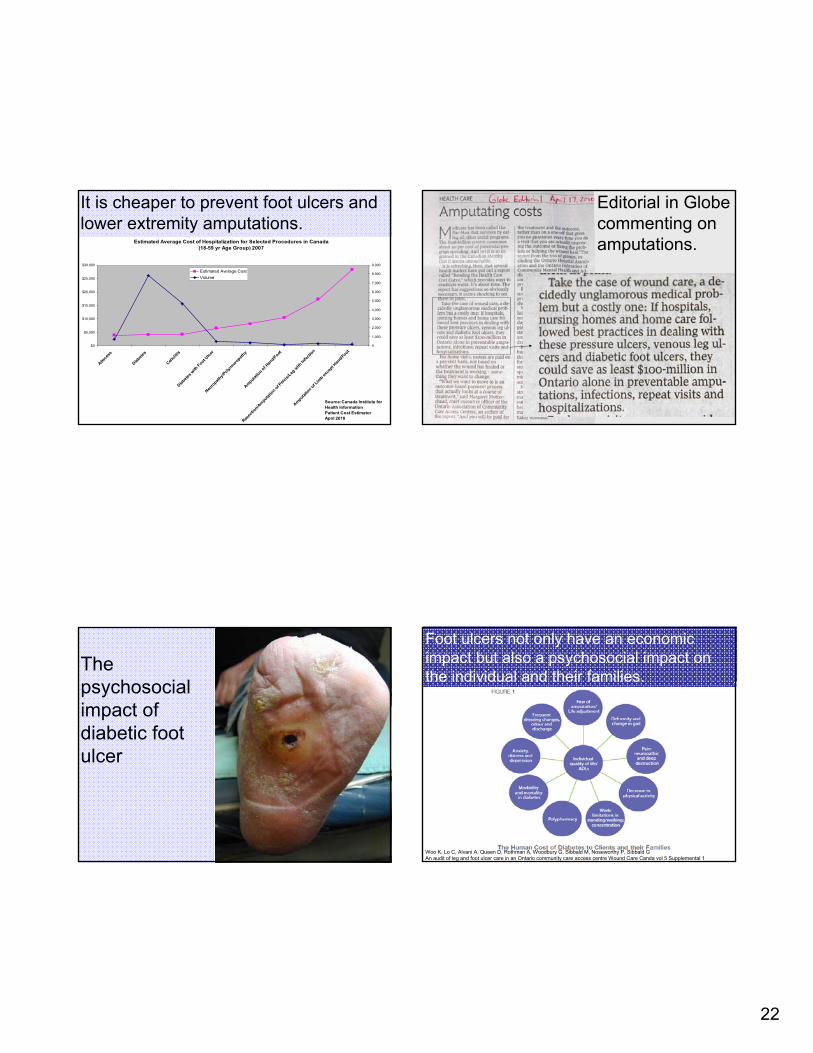
There was a significant difference in the prevalence of foot ulcers between European, South Asian and African Caribbean diabetics in the UK.
PrevalenceNumberEthnicity
2.4%371African Caribbean
11.9%1,866South Asian
5.5%13,409European
C A. Abbott, A P. Garrow, A L. Carrington, J Morris, E R. Van Ross, A J. Boulton Foot Ulcer Risk Is Lower in South-Asian and African-Caribbean Compared With European Diabetic Patients in the U.K.The North-West Diabetes Foot Care Study Diabetes Care 28:1869–1875, 2005
Will the prevalence in Canada be similar?
22
It is cheaper to prevent foot ulcers and lower extremity amputations.
Estimated Average Cost of Hospitalization for Selected Procedures in Canada (18-59 yr Age Group) 2007
$0
$5,000
$10,000
$15,000
$20,000
$25,000
$30,000
Absce
ss
Diabete
s
Celluliti
s
Diabete
s with
Foot Ulce
r
Neuro
pathy/P
olyneu
ropath
y
Amputatio
n of Han
d/Foot
Resec
tion/A
mputat
ion of Pelv
is/Leg
with
Infec
tion
Amputatio
n of Lim
b exce
pt Han
d/Foot
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
Estimated Average CostVolume
Source:Canada Institute for Health InformationPatient Cost EstimatorApril 2010
Editorial in Globe commenting on amputations.
The psychosocial impact of diabetic foot ulcer
Foot ulcers not only have an economic impact but also a psychosocial impact on the individual and their families.
Woo K, Lo C, Alvani A, Queen D, Rothman A, Woodbury G, Sibbald M, Noseworthy P, Sibbald GAn audit of leg and foot ulcer care in an Ontario community care access centre Wound Care Canda vol 5 Supplemental 1
23
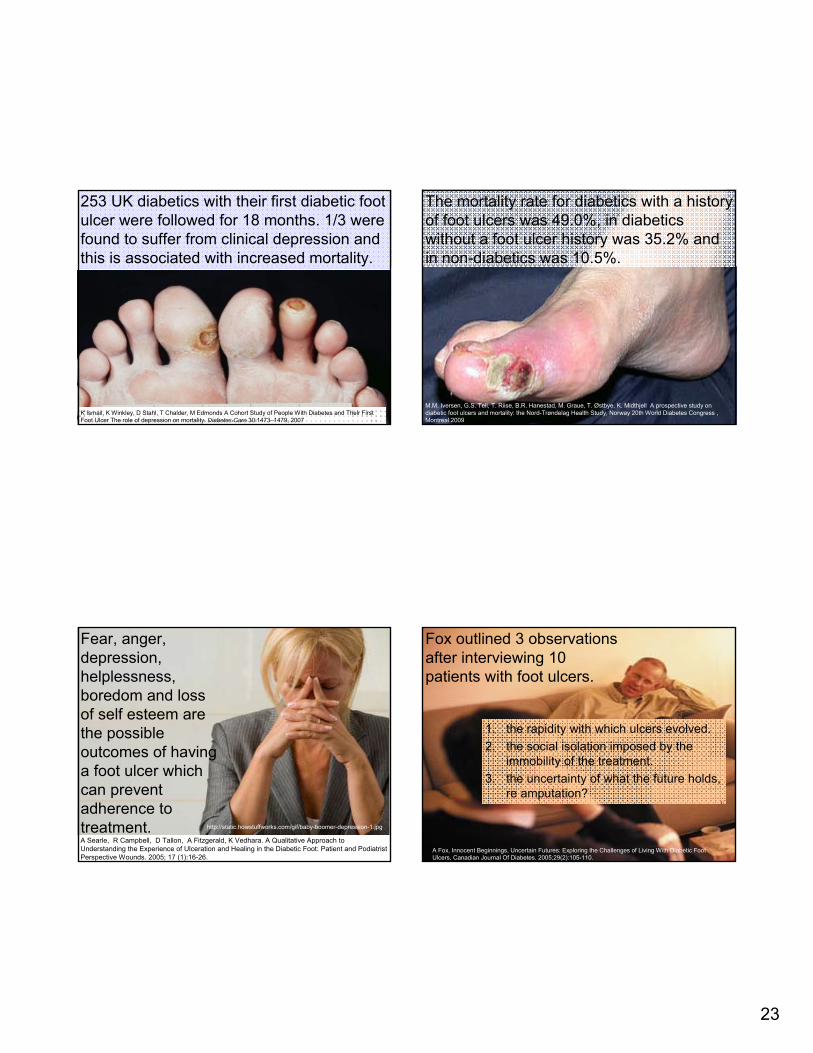
253 UK diabetics with their first diabetic foot ulcer were followed for 18 months. 1/3 were found to suffer from clinical depression and this is associated with increased mortality.
K Ismail, K Winkley, D Stahl, T Chalder, M Edmonds A Cohort Study of People With Diabetes and Their First Foot Ulcer The role of depression on mortality. Diabetes Care 30:1473–1479, 2007
The mortality rate for diabetics with a history of foot ulcers was 49.0%, in diabetics without a foot ulcer history was 35.2% and in non-diabetics was 10.5%.
M.M. Iversen, G.S. Tell, T. Riise, B.R. Hanestad, M. Graue, T. Østbye, K. Midthjell A prospective study on diabetic foot ulcers and mortality: the Nord-Trøndelag Health Study, Norway 20th World Diabetes Congress , Montreal.2009
Fear, anger, depression, helplessness, boredom and loss of self esteem are the possible outcomes of having a foot ulcer which can prevent adherence to treatment.A Searle, R Campbell, D Tallon, A Fitzgerald, K Vedhara. A Qualitative Approach to Understanding the Experience of Ulceration and Healing in the Diabetic Foot: Patient and Podiatrist Perspective Wounds. 2005; 17 (1):16-26.
http://static.howstuffworks.com/gif/baby-boomer-depression-1.jpg
Fox outlined 3 observations after interviewing 10 patients with foot ulcers.
1. the rapidity with which ulcers evolved.2. the social isolation imposed by the
immobility of the treatment.3. the uncertainty of what the future holds,
re amputation?
A Fox, Innocent Beginnings, Uncertain Futures: Exploring the Challenges of Living With Diabetic Foot Ulcers, Canadian Journal Of Diabetes. 2005;29(2):105-110.
24
For many participants, the “innocent” way the ulcer began made them feel foolish or negligent.
“What happened was, about 5 or 6 years ago, I did something really stupid. I peeled some skin off the bottom of my foot. I knew I was diabetic, that’s real stupid.… It went into complete sepsis, and, oh man, was I sick, but denial was the biggest problem with me.…You know, you think you can get away with cheating a bit with your food intake or your insulin or not taking your medications. You have to keep up on everything, watch your sugars, that’s all I can say.”
A Fox, Innocent Beginnings, Uncertain Futures: Exploring the Challenges of Living With Diabetic Foot Ulcers, Canadian Journal Of Diabetes. 2005;29(2):105-110.
A father of 3 boys described his disappointment at not being able to play sports with his sons.
“I used to play road hockey with the older kids, and go bike riding and swimming. There was a pond north of here and we used to go ice skating at night and light a bonfire. When the older kids come and we sit down and they say, ‘Remember the time we went ice skating?’ and the little one’s sitting there listening, I know in the back of his mind he’s thinking, ‘Well, why can’t we do that?’ ”
A Fox, Innocent Beginnings, Uncertain Futures: Exploring the Challenges of Living With Diabetic Foot Ulcers, Canadian Journal Of Diabetes. 2005;29(2):105-110.
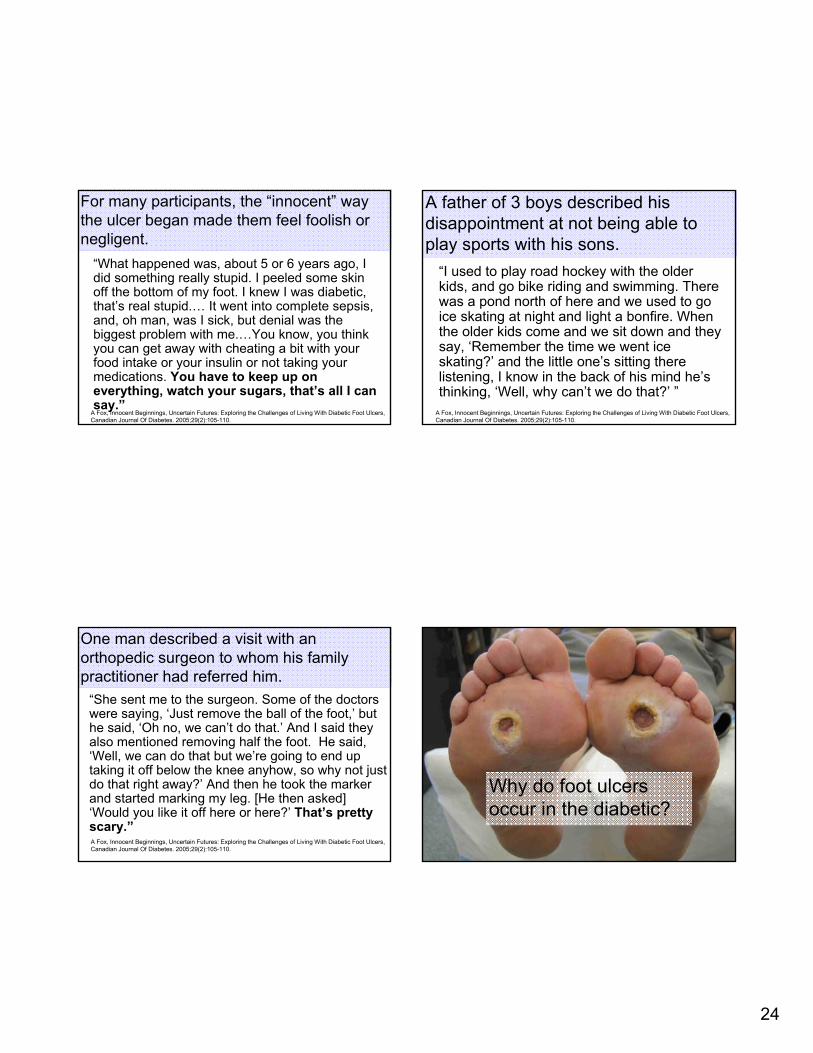
One man described a visit with an orthopedic surgeon to whom his family practitioner had referred him.
“She sent me to the surgeon. Some of the doctors were saying, ‘Just remove the ball of the foot,’ but he said, ‘Oh no, we can’t do that.’ And I said they also mentioned removing half the foot. He said, ‘Well, we can do that but we’re going to end up taking it off below the knee anyhow, so why not just do that right away?’ And then he took the marker and started marking my leg. [He then asked] ‘Would you like it off here or here?’ That’s pretty scary.”A Fox, Innocent Beginnings, Uncertain Futures: Exploring the Challenges of Living With Diabetic Foot Ulcers, Canadian Journal Of Diabetes. 2005;29(2):105-110.
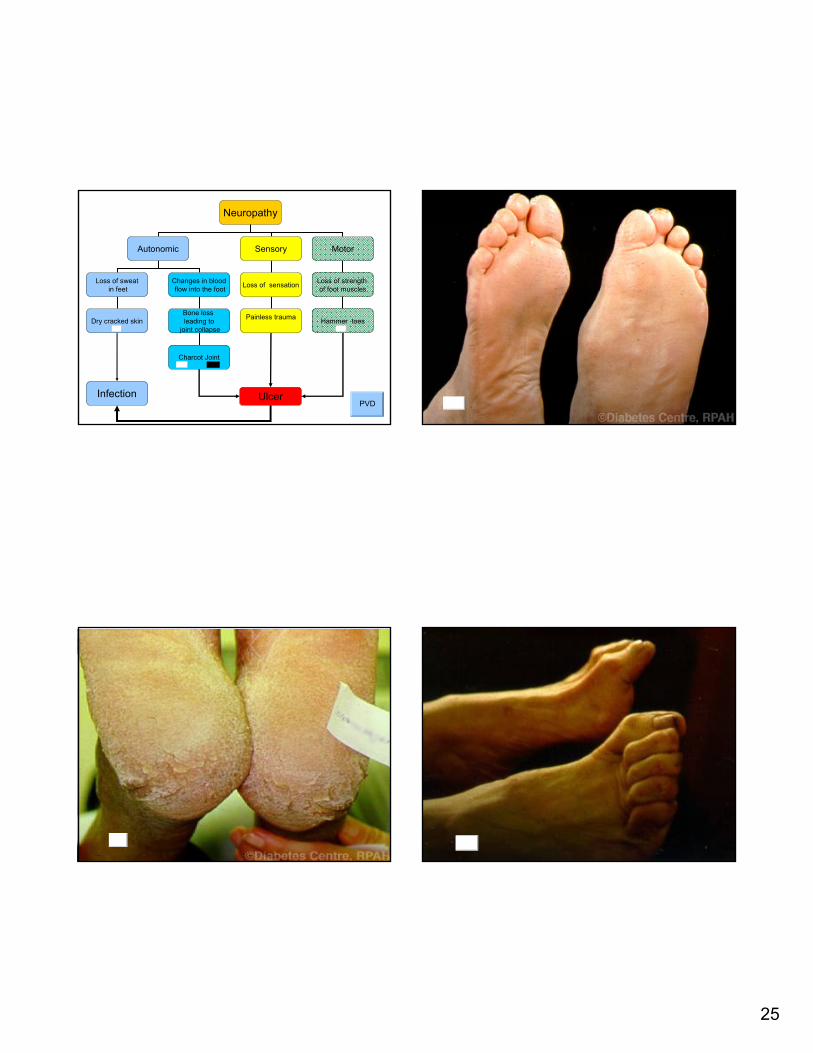
Why do foot ulcers occur in the diabetic?
25
Neuropathy
Autonomic Sensory Motor
Loss of sweatin feet
Changes in bloodflow into the foot Loss of sensation Loss of strength
of foot muscles
Hammer toesPainless traumaBone loss leading to
joint collapseDry cracked skin
Charcot Joint
UlcerInfectionPVD
26
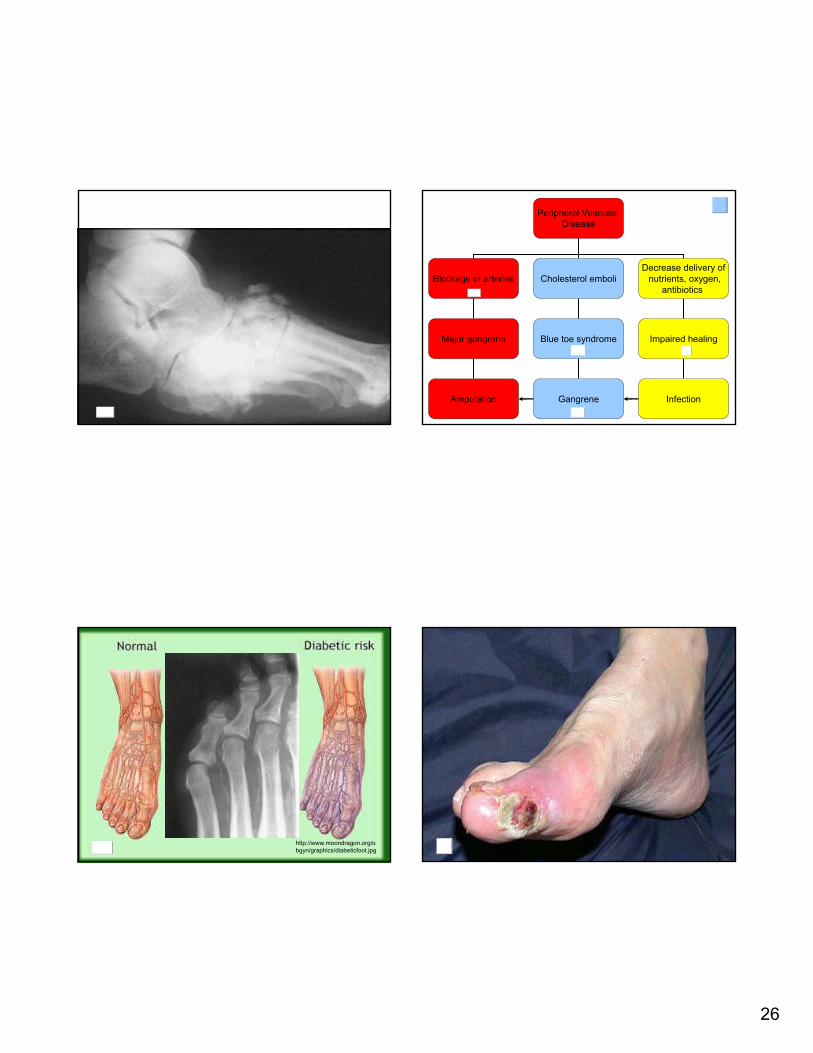
Peripheral Vascular Disease
Blockage of arteries Cholesterol emboliDecrease delivery of
nutrients, oxygen,antibiotics
Major gangrene Blue toe syndrome Impaired healing
Gangrene InfectionAmputation
http://www.moondragon.org/obgyn/graphics/diabeticfoot.jpg
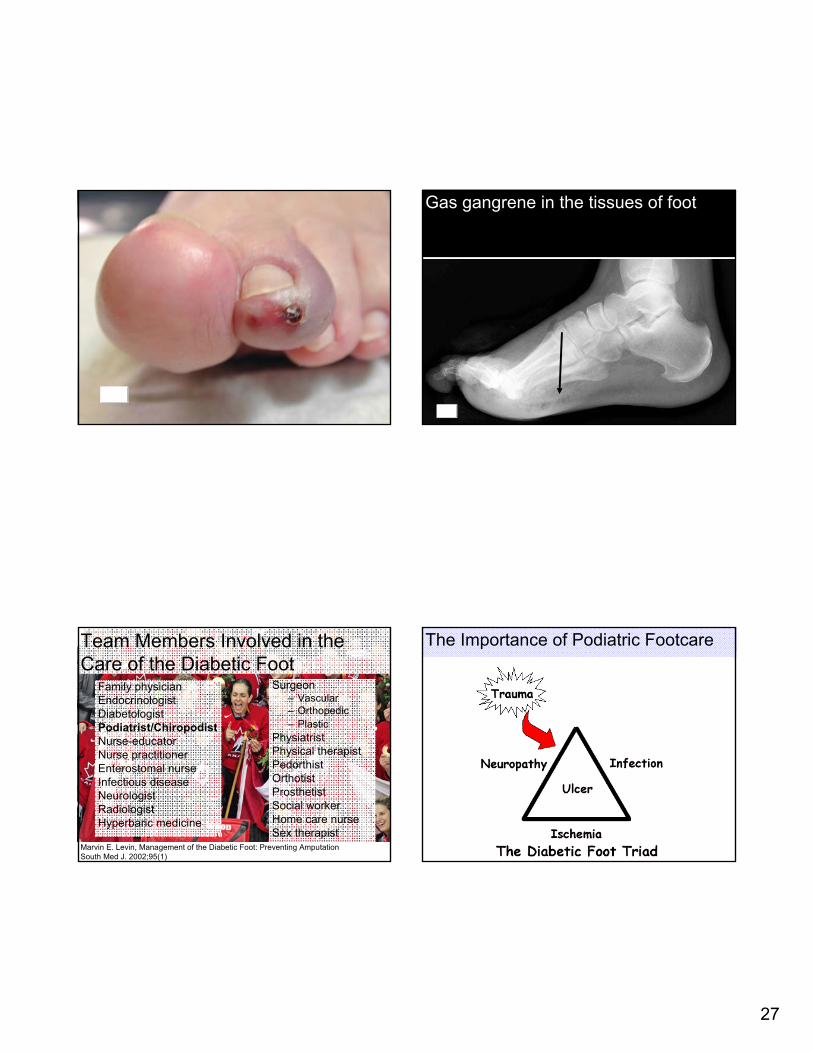
27
Gas gangrene in the tissues of foot
Team Members Involved in the Care of the Diabetic Foot
Family physician Endocrinologist DiabetologistPodiatrist/ChiropodistNurse-educator Nurse practitioner Enterostomal nurse Infectious diseaseNeurologist Radiologist Hyperbaric medicine
Surgeon – Vascular – Orthopedic – Plastic
Physiatrist Physical therapist PedorthistOrthotistProsthetistSocial worker Home care nurse Sex therapist
Marvin E. Levin, Management of the Diabetic Foot: Preventing AmputationSouth Med J. 2002;95(1)
The Importance of Podiatric Footcare
28
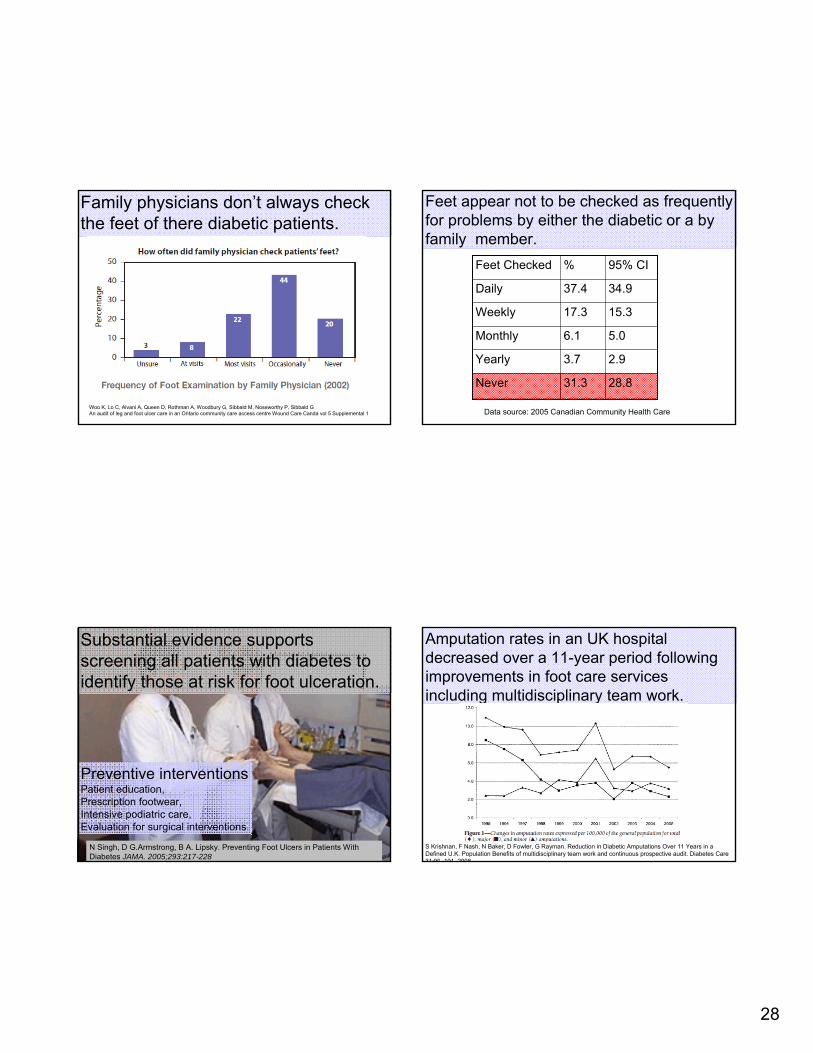
Family physicians don’t always check the feet of there diabetic patients.
Woo K, Lo C, Alvani A, Queen D, Rothman A, Woodbury G, Sibbald M, Noseworthy P, Sibbald GAn audit of leg and foot ulcer care in an Ontario community care access centre Wound Care Canda vol 5 Supplemental 1
Feet appear not to be checked as frequently for problems by either the diabetic or a by family member.
28.831.3Never
2.93.7Yearly
5.06.1Monthly
15.317.3Weekly
34.937.4Daily
95% CI%Feet Checked
Data source: 2005 Canadian Community Health Care
Substantial evidence supports screening all patients with diabetes to identify those at risk for foot ulceration.
N Singh, D G.Armstrong, B A. Lipsky. Preventing Foot Ulcers in Patients With Diabetes JAMA. 2005;293:217-228
Preventive interventionsPatient education, Prescription footwear,Intensive podiatric care, Evaluation for surgical interventions.
Amputation rates in an UK hospital decreased over a 11-year period following improvements in foot care services including multidisciplinary team work.
S Krishnan, F Nash, N Baker, D Fowler, G Rayman. Reduction in Diabetic Amputations Over 11 Years in a Defined U.K. Population Benefits of multidisciplinary team work and continuous prospective audit. Diabetes Care 31:99–101, 2008
29
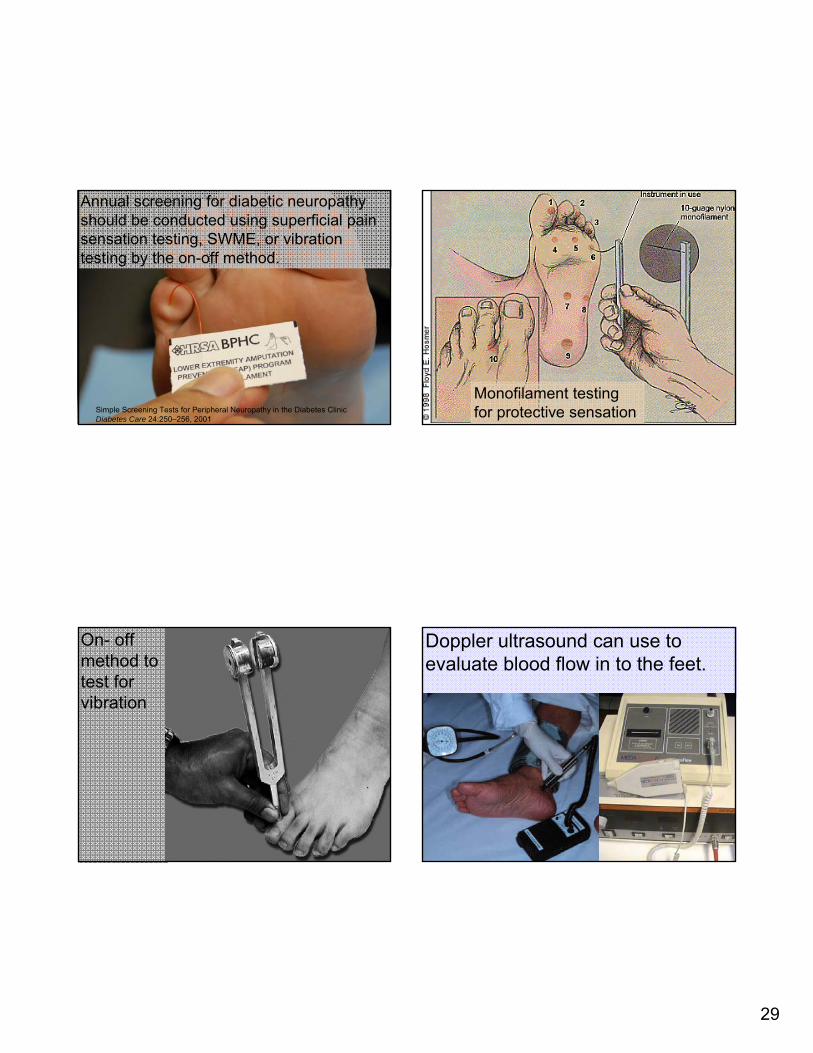
Annual screening for diabetic neuropathy should be conducted using superficial pain sensation testing, SWME, or vibration testing by the on-off method.
Simple Screening Tests for Peripheral Neuropathy in the Diabetes Clinic Diabetes Care 24:250–256, 2001
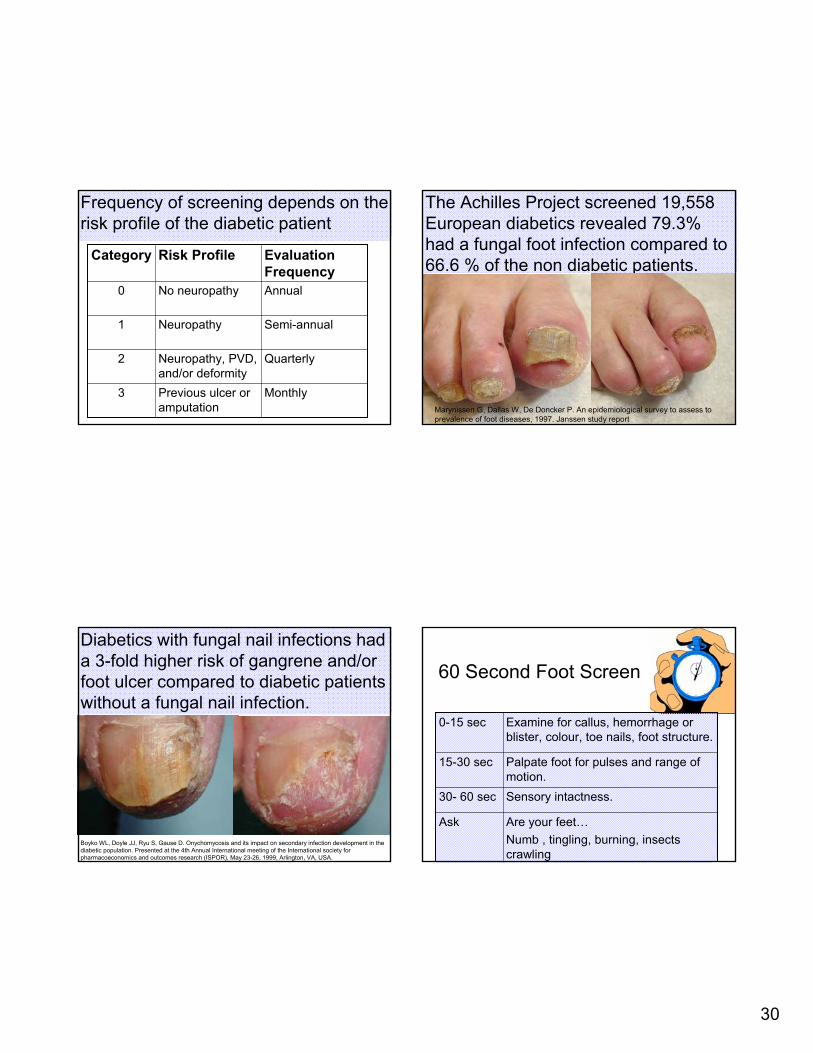
Monofilament testing for protective sensation
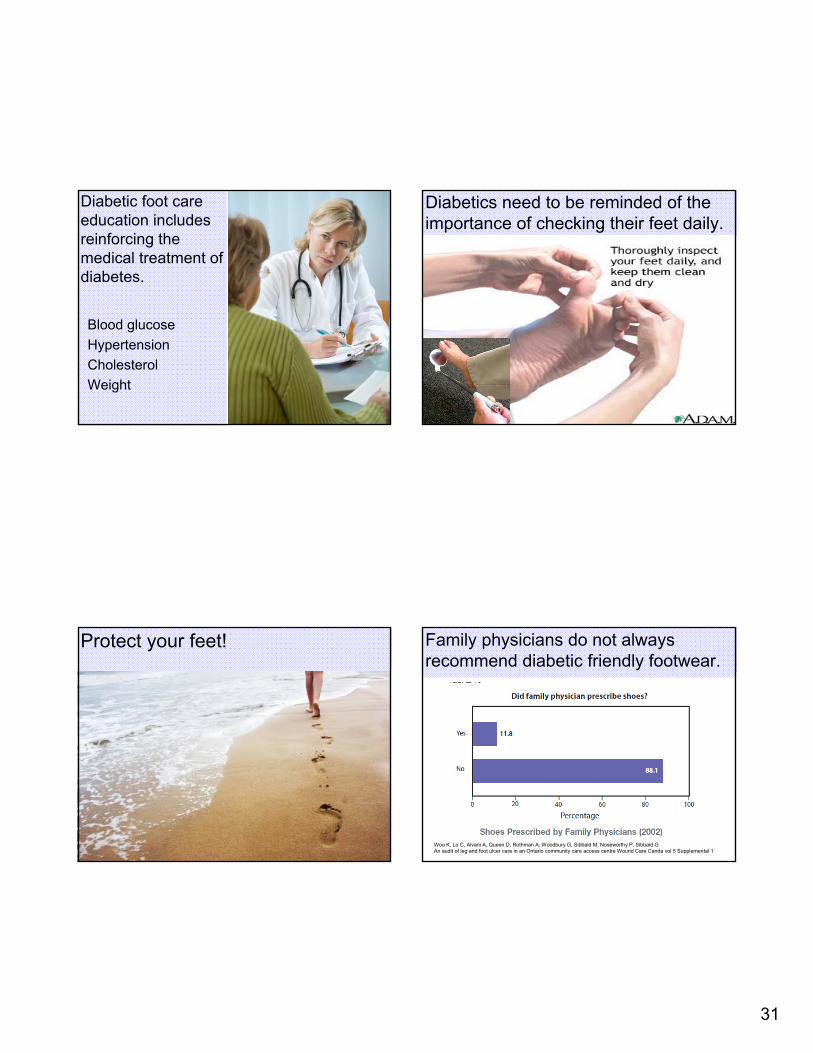
On- off method to test for vibration
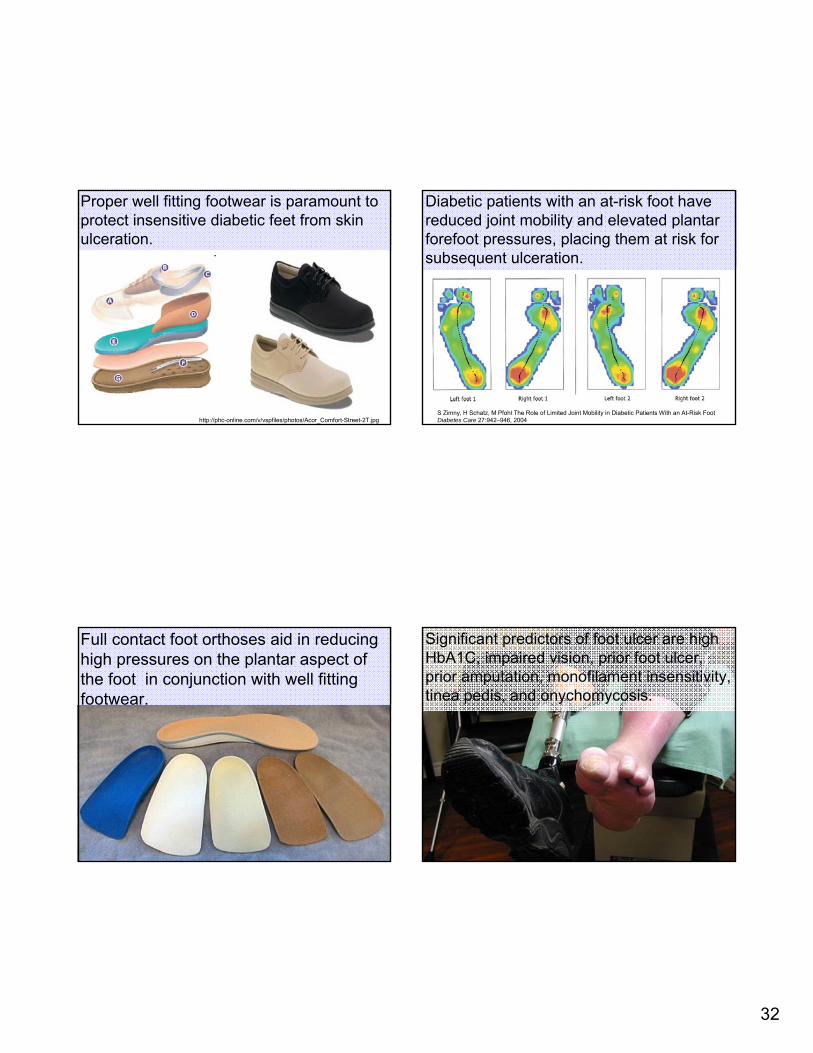
Doppler ultrasound can use to evaluate blood flow in to the feet.
30
Frequency of screening depends on the risk profile of the diabetic patient
MonthlyPrevious ulcer or amputation
3
QuarterlyNeuropathy, PVD, and/or deformity
2
Semi-annualNeuropathy1
AnnualNo neuropathy0
Evaluation Frequency
Risk ProfileCategory
The Achilles Project screened 19,558 European diabetics revealed 79.3% had a fungal foot infection compared to 66.6 % of the non diabetic patients.
Marynissen G, Dallas W, De Doncker P. An epidemiological survey to assess to prevalence of foot diseases, 1997. Janssen study report
Diabetics with fungal nail infections had a 3-fold higher risk of gangrene and/or foot ulcer compared to diabetic patients without a fungal nail infection.
Boyko WL, Doyle JJ, Ryu S, Gause D. Onychomycosis and its impact on secondary infection development in the diabetic population. Presented at the 4th Annual International meeting of the International society for pharmacoeconomics and outcomes research (ISPOR), May 23-26, 1999, Arlington, VA, USA.
60 Second Foot Screen
Are your feet…Numb , tingling, burning, insects crawling
Ask
Sensory intactness.30- 60 sec
Palpate foot for pulses and range of motion.
15-30 sec
Examine for callus, hemorrhage or blister, colour, toe nails, foot structure.
0-15 sec
31
Diabetic foot care education includes reinforcing the medical treatment of diabetes.
Blood glucoseHypertension CholesterolWeight
Diabetics need to be reminded of the importance of checking their feet daily.
Protect your feet! Family physicians do not always recommend diabetic friendly footwear.
Woo K, Lo C, Alvani A, Queen D, Rothman A, Woodbury G, Sibbald M, Noseworthy P, Sibbald GAn audit of leg and foot ulcer care in an Ontario community care access centre Wound Care Canda vol 5 Supplemental 1
32
Proper well fitting footwear is paramount to protect insensitive diabetic feet from skin ulceration.
http://phc-online.com/v/vspfiles/photos/Acor_Comfort-Street-2T.jpg
Diabetic patients with an at-risk foot have reduced joint mobility and elevated plantar forefoot pressures, placing them at risk for subsequent ulceration.
S Zimny, H Schatz, M Pfohl The Role of Limited Joint Mobility in Diabetic Patients With an At-Risk Foot Diabetes Care 27:942–946, 2004
Full contact foot orthoses aid in reducing high pressures on the plantar aspect of the foot in conjunction with well fitting footwear.
Significant predictors of foot ulcer are high HbA1C, impaired vision, prior foot ulcer, prior amputation, monofilament insensitivity, tinea pedis, and onychomycosis.
33
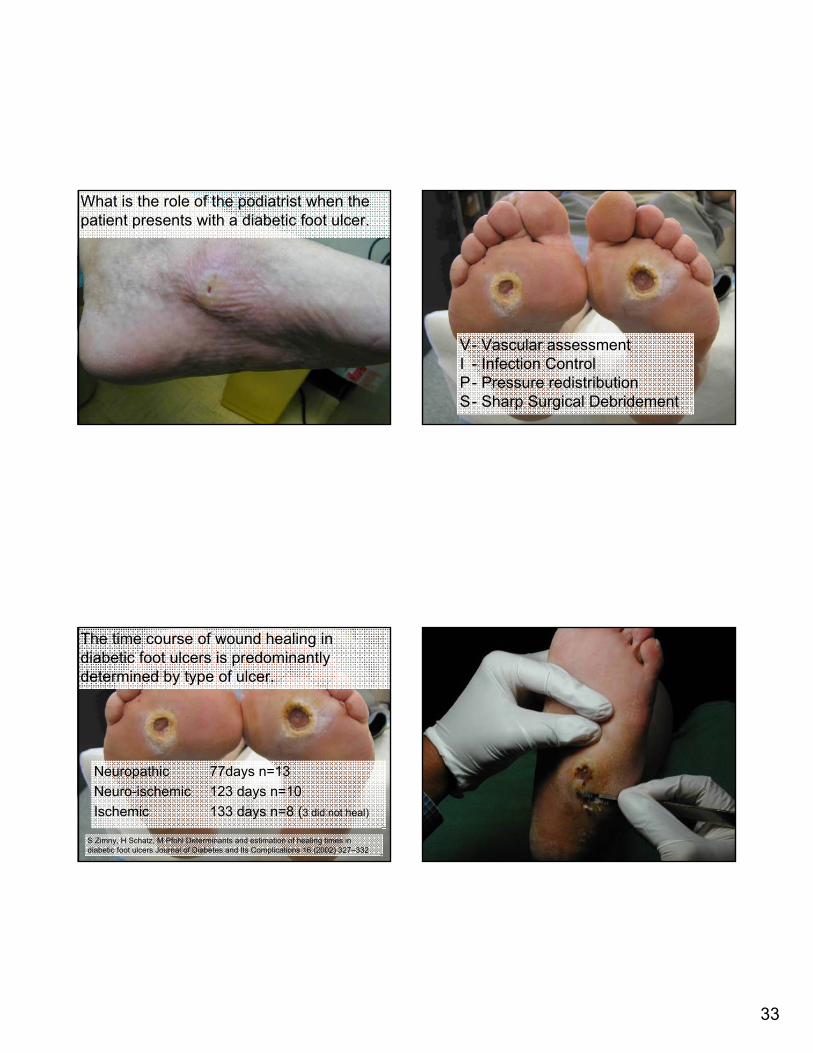
What is the role of the podiatrist when the patient presents with a diabetic foot ulcer.
V- Vascular assessmentI - Infection ControlP- Pressure redistributionS- Sharp Surgical Debridement
Neuropathic 77days n=13Neuro ischemic 123 days n=10Ischemic 133 days n=8 3 did not heal
Neuropathic 77days n=13Neuro-ischemic 123 days n=10Ischemic 133 days n=8 (3 did not heal)
The time course of wound healing in diabetic foot ulcers is predominantlydetermined by type of ulcer.
S Zimny, H Schatz, M Pfohl Determinants and estimation of healing times in diabetic foot ulcers Journal of Diabetes and Its Complications 16 (2002) 327–332

34
The total contact cast is the gold standard for pressure offloading of a plantar foot ulcer.
Journal of the American Podiatric Medical Association • Vol 92 • No 7 • July/August 2002 405
35
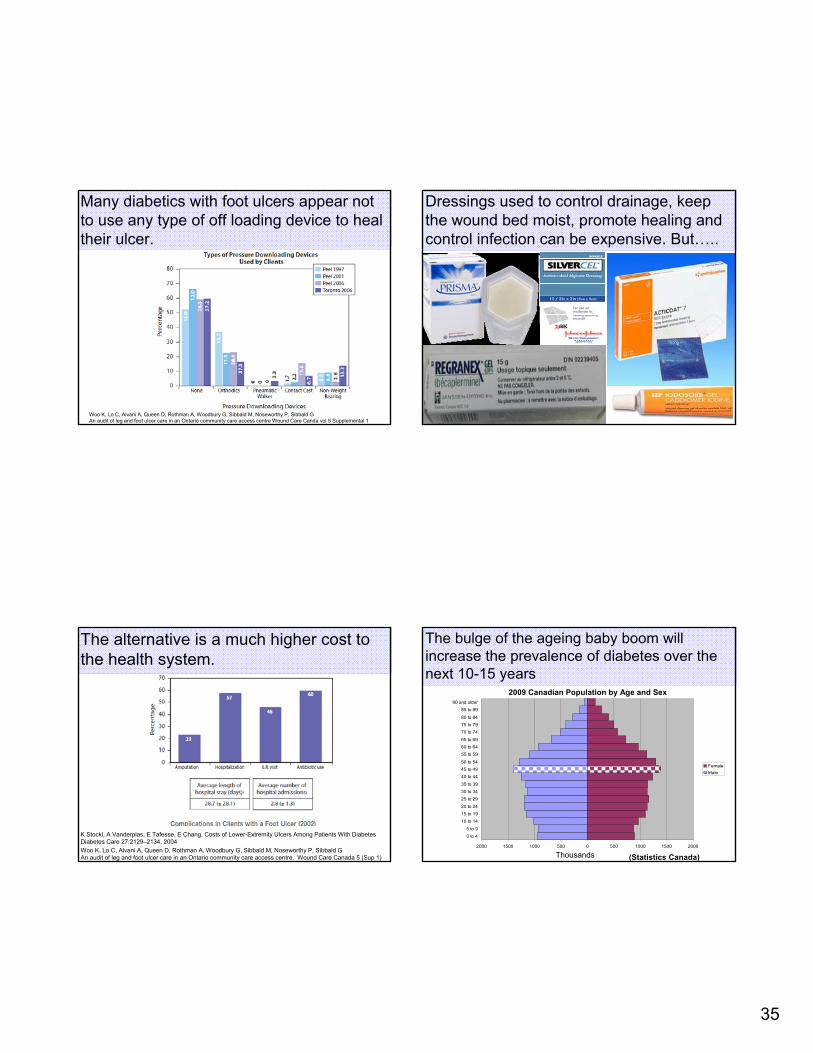
Many diabetics with foot ulcers appear not to use any type of off loading device to heal their ulcer.
Woo K, Lo C, Alvani A, Queen D, Rothman A, Woodbury G, Sibbald M, Noseworthy P, Sibbald GAn audit of leg and foot ulcer care in an Ontario community care access centre Wound Care Canda vol 5 Supplemental 1
Dressings used to control drainage, keep the wound bed moist, promote healing and control infection can be expensive. But…..
The alternative is a much higher cost to the health system.
Woo K, Lo C, Alvani A, Queen D, Rothman A, Woodbury G, Sibbald M, Noseworthy P, Sibbald GAn audit of leg and foot ulcer care in an Ontario community care access centre. Wound Care Canada 5 (Sup 1)
K Stockl, A Vanderplas, E Tafesse, E Chang. Costs of Lower-Extremity Ulcers Among Patients With Diabetes Diabetes Care 27:2129–2134, 2004
The bulge of the ageing baby boom will increase the prevalence of diabetes over the next 10-15 years
2000 1500 1000 500 0 500 1000 1500 2000
0 to 45 to 9
10 to 1415 to 1920 to 24
25 to 2930 to 3435 to 39
40 to 4445 to 4950 to 54
55 to 5960 to 6465 to 69
70 to 7475 to 7980 to 84
85 to 8990 and older
FemaleMale
2009 Canadian Population by Age and Sex
Thousands (Statistics Canada)
36
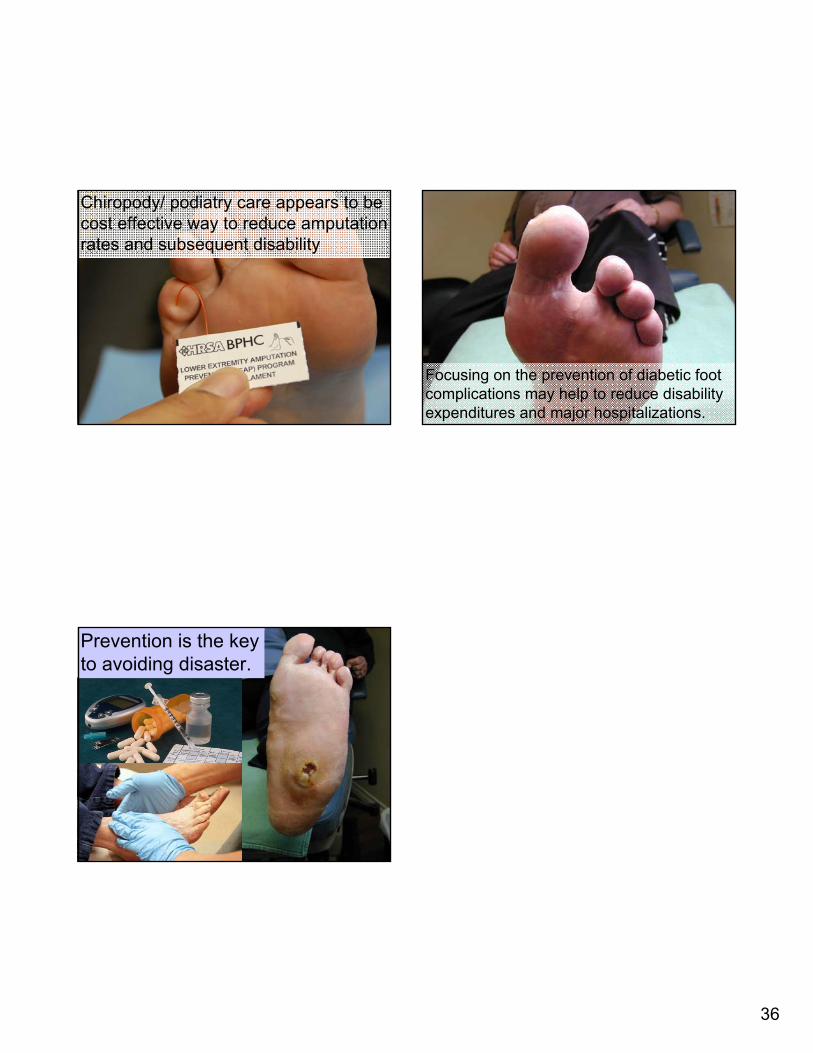
Chiropody/ podiatry care appears to be cost effective way to reduce amputation rates and subsequent disability
Focusing on the prevention of diabetic foot complications may help to reduce disability expenditures and major hospitalizations.
Prevention is the key to avoiding disaster.