what?, why?, and how? to refer imran jawaid. introduction what?, why? and how? to refer
TRANSCRIPT

What?, Why?, and How? to refer
Imran Jawaid
INTRODUCTIONWhat?, Why? and How? To refer

The day job..OPTOMETRISTS OPHTHALMOLOGISTS
Asymptomatic Symptomatic
No ocular pathology Ocular pathology
Screening / disease detection Treatment / disease management
Detect abnormality Diagnosis and investigation
Spectacles and contact lenses No refractive correction
Retail pressures (ATV, CR etc.) No retail pressures
9-5pm 24 hours
Career progression not based on ability to detect/manage ocular abnormality
Career progression based on ability to manage ocular abnormality

CHANGING TIMESWhat? Why? and How ?to refer

“Call to action” – The future...
• Improve IT links between community optical practices and the rest of the NHS and primary care
as well as improved systems in hospitals
• Address capacity issues in hospital eye clinics to save patients from unnecessary blindness and vision impairment
• Maximise the use of the skills in the eye care pathway by ensuring that patients are treated in the appropriate place by the appropriate professional at the appropriate time, whether in the community or in the hospital
• Procure community schemes at greater scale to reduce procurement and commissioning costs and direct more resource to clinical care.
• Improve communication and relationships between the multiple professions through better commissioning to achieve a more integrated eye care pathway and better patient care
ARE WE READY FOR THE CHANGE?What?, Why?, and How to refer
Bridging the gap
• Improve knowledge base• Improve feedback to referring optometrists• Increased exposure to ocular abnormality• Improve understanding of disease
management• Improve understanding of new treatments
and diagnostic equipment

Common problems
• Raised IOP• Flashes and floaters• Retinal haemorrhages• Red eye

Elevated IOPs
22T29 HistoryAsymptomatic?Angle closure sxs? (acute/intermittent)Photophobia?Visual change?Previous Trauma?Medications? (Steroid/Topiramate)Ocular treatments (Laser/Buckle)Ocular History (Ischaemic retina)

Pressure..
• History – Symptomatic vs Asymptomatic
• Anterior Segment signs– Red eye– KS, KPs and corneal pathology– AC activity and depth– Iris atrophy / TIDs / NVI– Significant cataract


Pressure..
• Gonioscopy• www.gonioscopy.org
• Redmond-Smith Index• Van Herrick
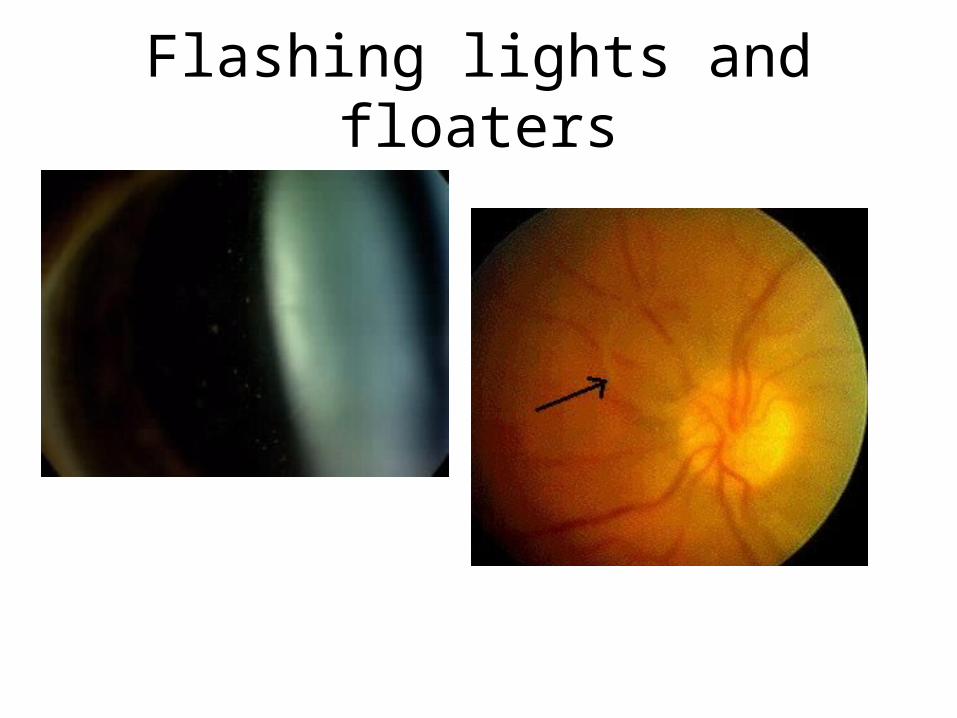
Flashing lights and floaters

Flashing lights and floaters...
4. Sudden blind spot in your side vision
Flashing lights and floaters...
• History– Myopia– Family history– Visual field defect– Fellow eye status
• Age – 6% under 50, 53% over 50, 67% over 65

Examination
• IOP• AC activity• Vitreous – tobacco dust?, RBC?, vitritis?• Fundus
– Weiss ring– Vitreous or pre-retinal hge– Peripheral retina
• Tear/break +/- SRF• Peripheral degeneration - Lattice
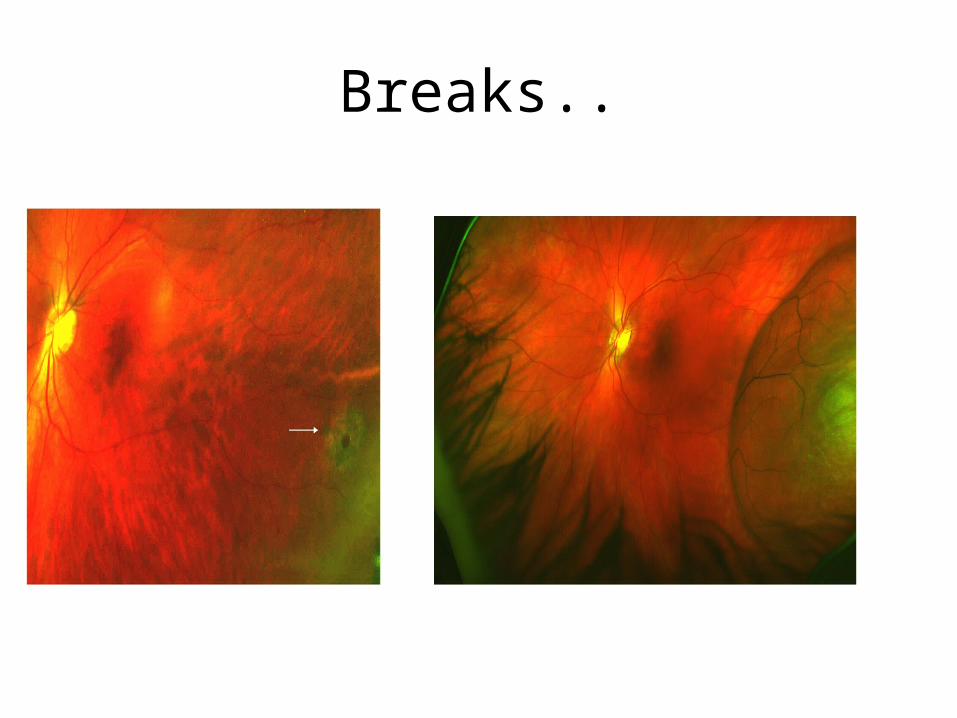
Breaks..

Retinal Haemorrhage
• Anatomy– Inner 2/3 - CRA – Outer 1/3 - Choroidal circulation– CRA divides into superior and inferior branches which
each divide into nasal and temporal branches– Functionally these are end-arteries– Central foveal avascular zone contains outer retinal layers
only. Blood supply to this area is derived from the underlying choroidal circulation.
– Post arteriole retinal capillaries - NFL – Pre-venular capillaries - INL
Pre-retinal haemorrhage...
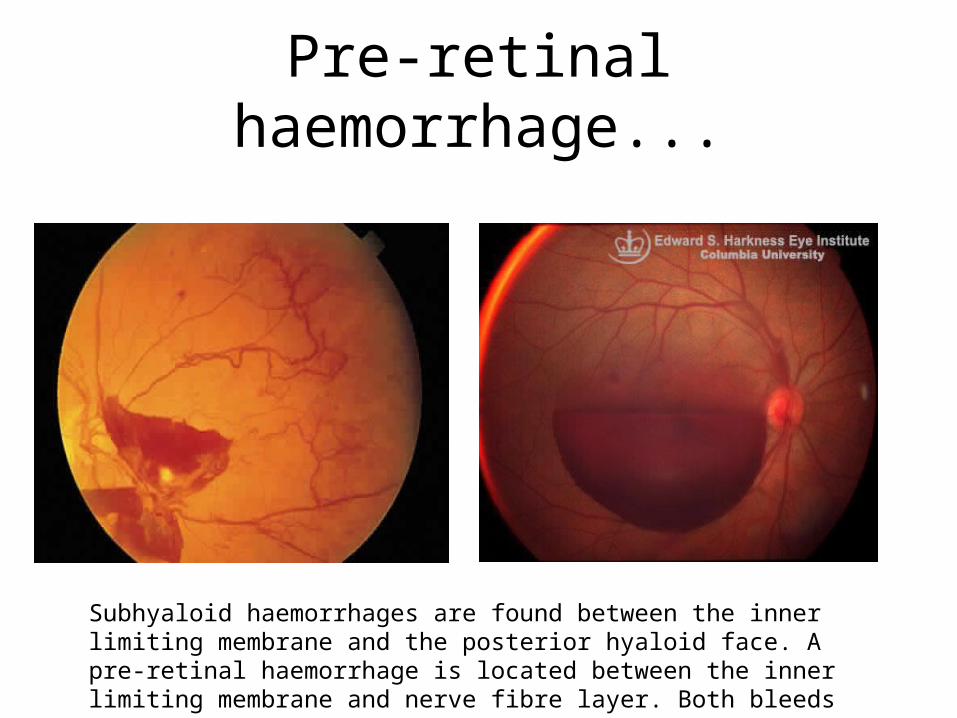
Subhyaloid haemorrhages are found between the inner limiting membrane and the posterior hyaloid face. A pre-retinal haemorrhage is located between the inner limiting membrane and nerve fibre layer. Both bleeds mask the underlying vessels

Flame haemorrhage
Hypertensive retinopathy, vein occlusion, AION, disc swelling amongst othersRecording blood pressure is essential Marker for the site of future nerve fibre and corresponding visual field lossLocation should be accurately documented and further investigations performed
Pale centred linear haemorrhage
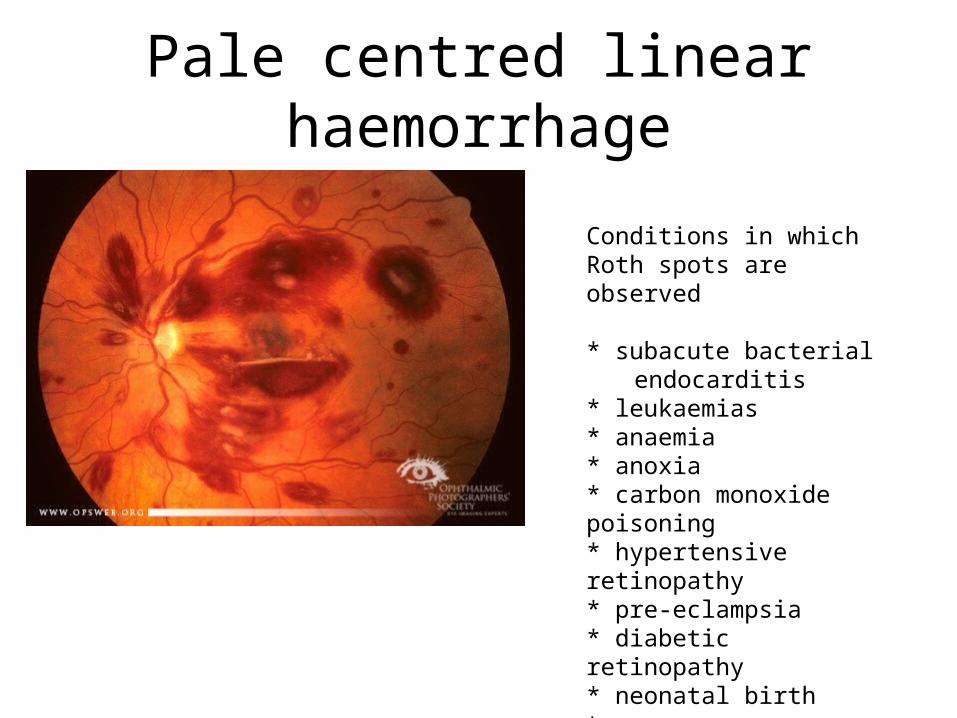
Conditions in which Roth spots are observed * subacute bacterial endocarditis* leukaemias* anaemia* anoxia* carbon monoxide poisoning* hypertensive retinopathy* pre-eclampsia* diabetic retinopathy* neonatal birth trauma* shaken baby syndrome
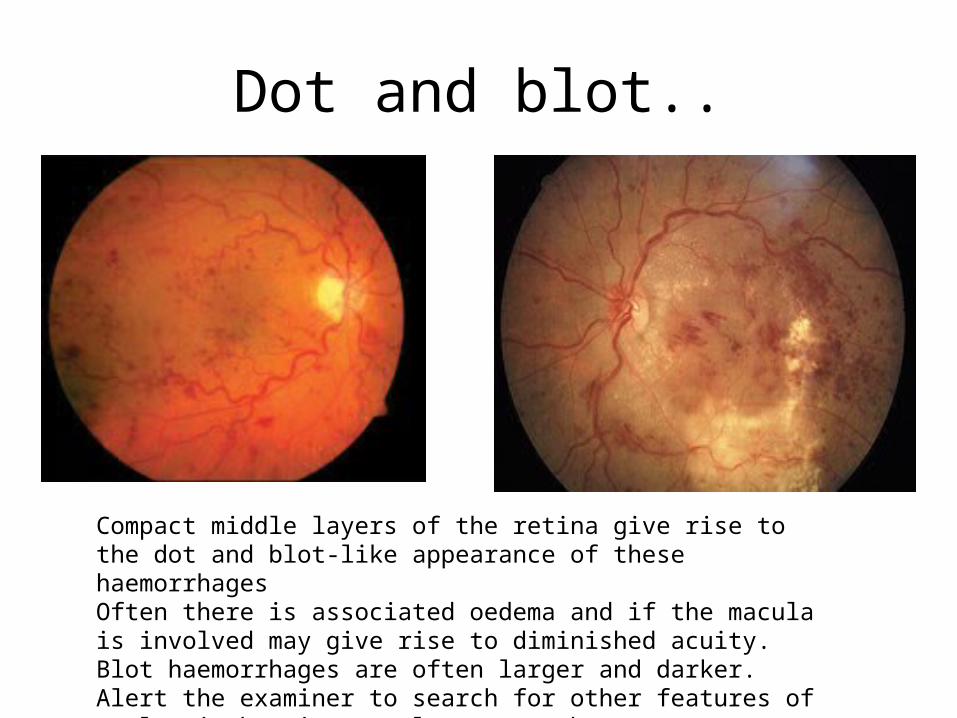
Dot and blot..
Compact middle layers of the retina give rise to the dot and blot-like appearance of these haemorrhagesOften there is associated oedema and if the macula is involved may give rise to diminished acuity. Blot haemorrhages are often larger and darker.Alert the examiner to search for other features of ocular ischaemia –namely venous changes, cotton wool spots and neovascularisation.

Sub-retinal Haemorrhage
Between neuro-sensory retina and RPE. They are dark in colour and the retinal vasculature is clearly visible aboveBleed can be large in area and variable in shape Sub-RPE bleeds, (between RPE and Bruch’s membrane of the choroid), have a more confined arrangement as there are tight junctions between RPE cells Commonest cause is choroidal neovascularisationOther causes include trauma, tumours and retinal angiomas

Red eye
• History– Pain
• FB sensation/ache/ deep pain
– Photophobia– V/A– Lacrimation / discharge– Associated symptoms
• Nausea and vomiting/ frontal headache
– C/L wear

Examination
• Pattern of redness– Diffuse and superficial– Diffuse and deep– Circum-corneal– Sectoral
• Reduced vision• Pupils• NaFl

Subconjunctival haemorrhage
ManagementBP Reassure
PainPhotophobiaV/ADischargeAssoc. Sxs.C/L wear

PainPhotophobiaV/ADischargeAssoc. Sxs.C/L wear
Conjunctivitis- bacterial/viral
ManagementStrict hygieneCool compressLubricants +/- CPL

PainPhotophobiaV/ADischargeAssoc. Sxs.C/L wear
Herpetic Keratitis
ManagementReferStart oc. Aciclovir 5 x daily if confidentDO NOT GIVE STEROIDS

Contact lens-related keratitis
ManagementStop C/L wearHourly g. levofloxacinREFER
PainPhotophobiaV/ADischargeAssoc. Sxs.C/L wear

PainPhotophobiaV/ADischargeAssoc. Sxs.C/L wear
Episcleritis
Scleritis

PainPhotophobiaV/ADischargeAssoc. Sxs.C/L wear
Acute anterior uveitis
ManagementRefer to eye casualty same or next day

How to refer• S Situation: • Identify yourself the site/unit you are calling from • Identify the patient by name and the reason for your report • Describe your concern
• B Background: • Give the patient's reason for attendance• Explain significant medical/ocular history
• A Assessment: • Clinical impressions, concerns
R Recommendation: • Explain what you need - be specific about request and time frame • Make suggestions • Clarify expectations

THANK YOUQUESTIONS?
What?, why? and how to refer