what is wrong with emr? james j. cimino, m.d., columbia university jonathan m. teich, m.d., ph.d.,...
Post on 19-Dec-2015
217 views
TRANSCRIPT

What is Wrong with EMR?
James J. Cimino , M.D., Columbia University
Jonathan M. Teich , M.D., Ph.D., Partners Healthcare System
Vimla L. Patel , Ph.D., DSc. McGill University
Jiajie Zhang , (Organizer), Ph.D., UT Houston

What is an ideal EMR?

•Complete•Accurate•Timely
Paper-based Records
Good Features
Bad Features
Electronic Medium
Good Features
Bad Features
•Data
•Alerts
•Reminders
•Decision support
•Medical knowledge
•Communications
•Other aids
•At all points of care
•For all healthcare professionals
•At all times
X
X
Dramatically improve the quality of healthcare
This Is The Ideal EMR!

Status of Current EMR
many non-trivial problems
wide acceptance
X
Four Perspectives
• System functions (Cimino)
• Clinical (Teich)
• Cognitive (Patel)
• Human-Computer Interaction (Zhang)

System Functions PerspectiveJames Cimino
• Two Models of EMRs
• Old Vision
• New Vision
Two Models of the EMR
• Financial system add-on
• Repository

Financial System Add-On
Patient
Admission Admission Admission
PrimaryDiagnosis
OtherDiagnoses
Diagnosis/S Diagnosis/S Diagnosis/P
Allergies
Penicillin
Drug Admin
Aspirin
Reaction
Allergy
GlucoseGlucose Glucose

Repository
Diagnosis DiagnosisDrug Admin:
AspirinAllergy: AspirinGlucoseAllergy:
PenicillinGlucose
AllergiesAdmission
Glucose
Patient

Old Vision
• Medical record as history
• Terminology as codes

Problems with the Old Vision
• Cognitive overload
• Poor coordination of caregivers
• Computer unable to help with plan

New Vision
• Medical record as Daytimer®
• Terminology as knowledge base

Medical Record as Daytimer®
• Future is more important than past
• Goals are stated
• Alternatives are anticipated
• Status can be determined
• Computer can help with planning and timing

Terminology as Knowledge Base
• Coded data become symbols
• Care plans can be codified
• Computer can share tasks in the care process

Promises of the New Vision
• Initial status is determined
• Problems and tasks codified
• Daily notes are updates to status
• Progress can be charted
• Milestones can be anticipated
• Patient’s distance from desired state can be determined
• Expert systems can help with state transitions

Workflow, scenarios of care, and the EMR
Jonathan Teich, MD, PhD
November 9, 1999
A little disclaimer

What are the Winners?
• Results review– No work required
• E-mail– Immediate benefit
• Important or requested alerts– No work, high importance– Non-judgmental, valuable immediate benefit
• Order sets

What are the Losers?
• Supplying reasons for orders
• Multiple click sequences
• Prednisone tapers without support
EMR’s run into acceptance problems because…
• They’re not oriented to the scenario• Immediate effort > Immediate benefit• They’re slow• “Perfect is the enemy of good”• They over-use technology• They have an activation energy• They follow data categories, not clinical scenarios

Scenarios – ambulatory
• Coming into the office
• New patient precis
• Familiar patient review
• End-of-visit
• Phone call
Scenarios – inpatient
• Rounds• Results review• Orders
– Entry and processing– Prioritize tasks among several patients [ED
display]
• Daily notes• Signing out

Scenarios – community/patient
• Ask a question
• Request a service
• Convey information
• Do it all without phone tag

The ‘bang per buck’ approach
• Computerize if:– Immediate Workflow benefit + cost benefit +
(future usefulness x lifetime) > Extra work + Extra time
– WI + CS + (FU X L) > WE + TE
• Example: inpatient notes• Example: ambulatory documentation• Add no-input benefits

Property: Workflow
• The one-click rule
• Common things quickly, uncommon things possible
• Associated information
Property: Data re-use
• Med list -> prescription -> refill
• Meds, allergies -> conflict checking
• Problem list, dx -> pathway, flu shot reminder
• Structured docu -> later default [aging]

Other issues
• Shortcuts, templates, and pre-fills• Parsimoniousness – problem list
– Simple– Usable
• Avoiding aggravation– Appropiate alerting modes– Avoiding over-alerting
• Inclusive approach – data capabilities

Ambulatory documentation
• Modes– Dictation– Hand-entry– Structured entry– Structured dictation– Voice recognition– Partial structure
• Cost it out

Post-high-tech: people, paper, and free text
• Sign-out sheets
• Structured documentation
• Mix structured and free entry

“Make something better and nothing worse”

Studies of the provider’s day
• Tang – time spent in activities
• Awoniyi
• Lee – what is liked vs. what is used
• What problems can be helped by information tools?
What’s Wrong With The EMR:A Cognitive Perspective
Vimla L. Patel, PhD, DSc, FRSC
Cognitive Studies in MedicineCentre for Medical Education
McGill University Montreal, Canada
EMR and Paper-Based Records
• Cognitive artifacts
• Embody processes
• Promote use of heuristics
But, as I will show:
• They support different cognitive processes– Paper: Focus is on exploration and discovery– EMR: Focus is on problem solving

1. Chief Complaint 10 282. Past Medical History 13 133. Life Style 33 194. Psychological Profile 10 115. Family History 7 146. History of Present Illness 55 277. Review of Systems 52 258. Physical Examination 60 559. Diagnosis 14 910. Investigation 29 1711. Treatment 21 24
Total Entries 304 252
Category of Information Hand-WrittenPatient Record
ElectronicPatient Record
Information in EMR and Hand-Written Records
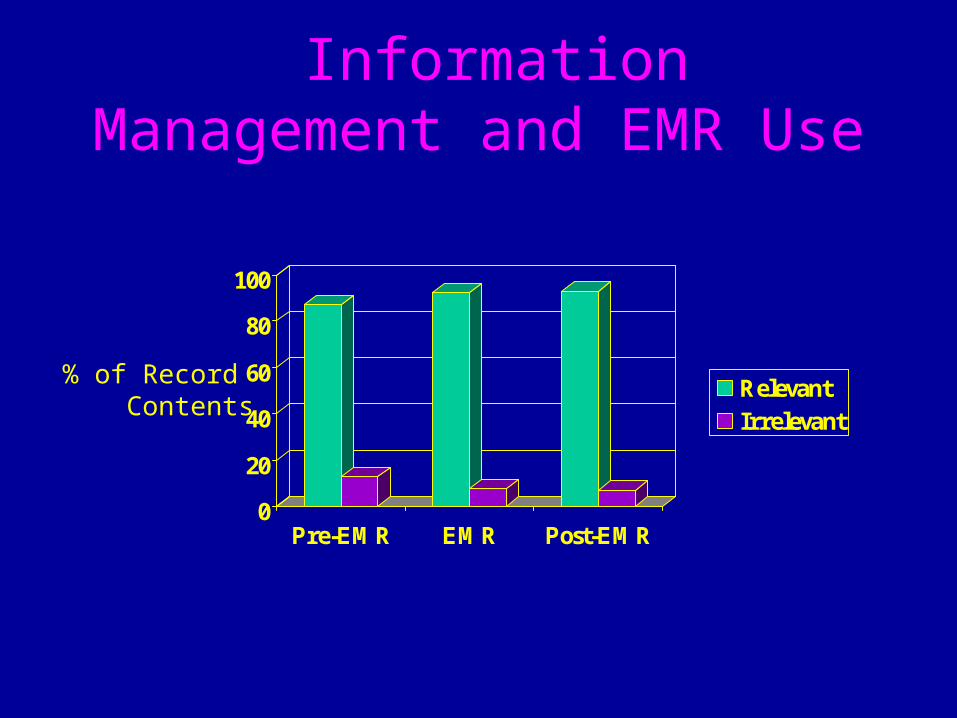
Information Management and EMR Use
0
20
40
60
80
100
Pre-EMR EMR Post-EMR
RelevantIrrelevant
% of Record Contents
First section from paper-based record
(Pre-CPR) 74 year old woman, whose diagnosis was made in February, as she complained of polyuria/nocturia and fatigue for a few years. She was told her sugar was very high and she was sent to Dr. K., who started her on Diabeta 5 mg/d and sent her to Dr. S. in ophthalmology who reported normal retina. She lost weight, her polyuria improved, her bladder urgency got better, and her glucose values improved dramatically. She does no monitoring at home. She had to be hospitalized for an ankle fracture after falling on ice, for 3 months. At follow-up, Dr. K. seemed pleased with the results.
First Section from Electronic Medical Record (EMR)
CHIEF COMPLAINT: Type II diabetes mellitus
PERSONAL HISTORYSURGICAL: cholecystectomy: Age 60 years old
MEDICAL: hypothyroidism: asymptomatic since 25 years
LIFE STYLEMEDICATION
DIABETA (Tab 2.5 MG)Sig: 1 tab(s) Oral before breakfast
SYNTHROID (Tab 0.125 MG)Sig: 1 tab(s) Oral before breakfast
HABITS: smoking: 0 alcohol: 0
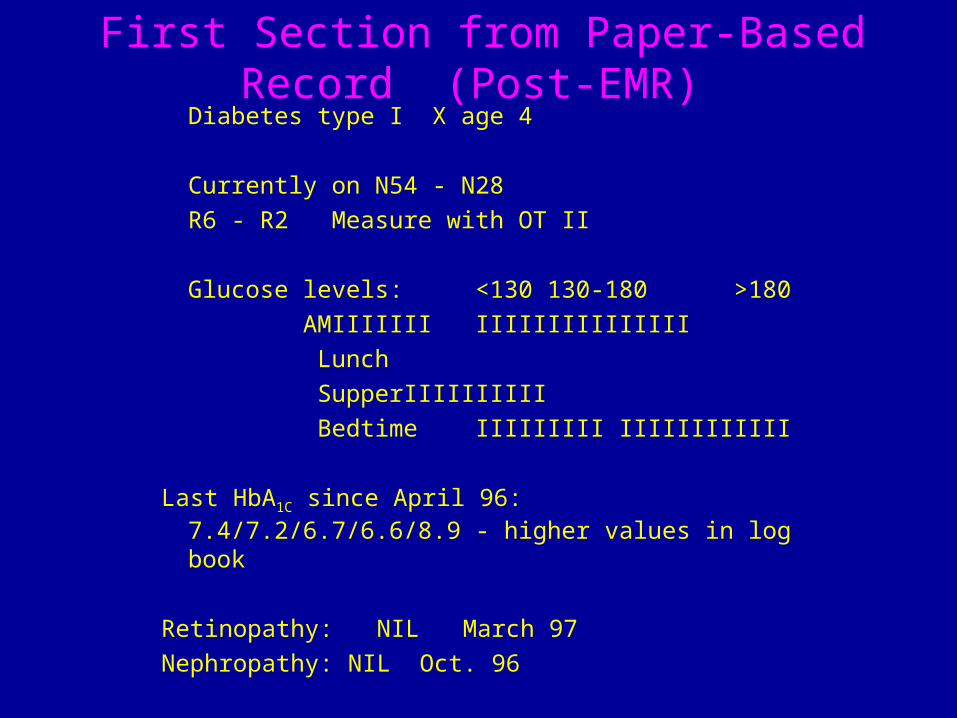
First Section from Paper-Based Record (Post-EMR)
Diabetes type I X age 4
Currently on N54 - N28
R6 - R2 Measure with OT II
Glucose levels: <130 130-180 >180
AM IIIIIII IIIIIIIIIIIIIII
Lunch
Supper IIIIIIIIII
Bedtime IIIIIIIIIIIIIIIIIIIII
Last HbA1C since April 96: 7.4/7.2/6.7/6.6/8.9 - higher values in log book
Retinopathy: NIL March 97
Nephropathy: NIL Oct. 96

Categories Accessed by Intermediate
1. Chief Complaint 1 12. Past Medical History 2 33. Life Style 3 64. Psychosocial Profile 6 35. Family History 7 66. History of Present Illness 8 87. Review of Systems 9 38. Physical Examination 10 49. Diagnosis 11 810. Investigations 911. Treatment 11
92
11
Sections of EMR Accessed by Intermediate and Expert Users for Two
Typical CasesCategory of Information(in order on CPR screen)
Categories Accessed by Expert
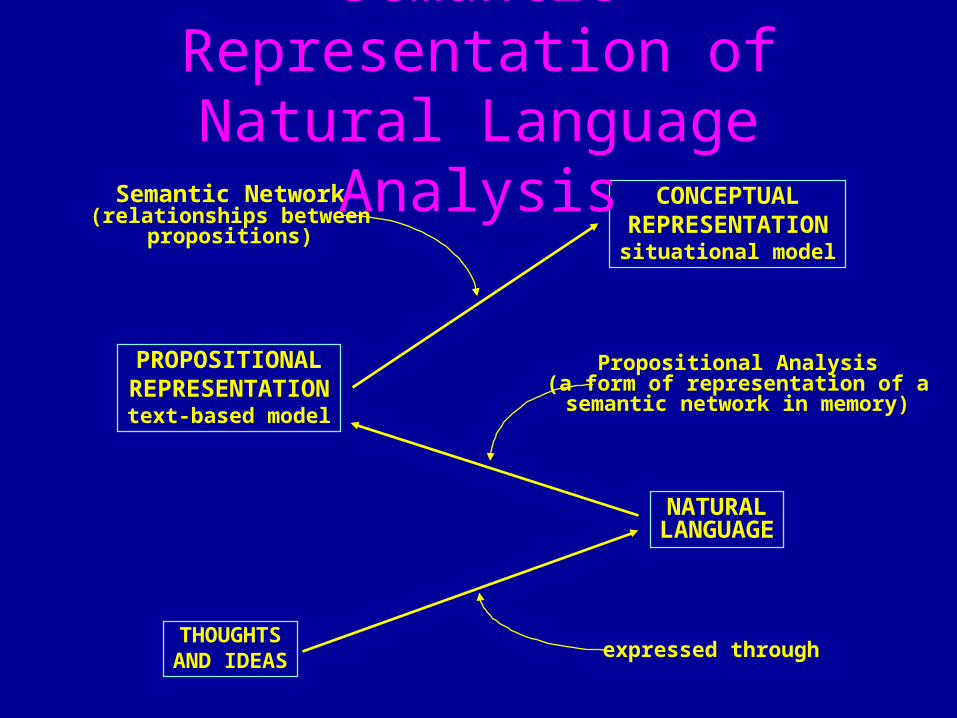
THOUGHTSAND IDEAS
PROPOSITIONALREPRESENTATION
text-based model
Propositional Analysis(a form of representation of asemantic network in memory)
NATURALLANGUAGE
expressed through
Semantic Network(relationships between
propositions)
CONCEPTUALREPRESENTATION
situational model
Semantic Representation of Natural Language Analysis

Types of Propositions• Single propositions
• A single idea– “She lost weight”
• Embedded propositions• Contain one or more single propositions
– “She lost weight relative to her premorbid baseline”
• Linking propositions• Connect different portions of the text
– “She lost weight and control of her blood sugar improved”

Propositional Analysis: Pre-EMR
74 year old woman who was diagnosed in February, as she complained of polyuria/nocturia and fatigue for a few years. She was told her sugar was very high...
1.1 Woman ATT:Old, DEG:74;
1.2 Diagnose PAT:1.1, TEM:February;
1.3 Complain THM:Polyuria/Nocturia
1.4 Complain THM:Fatigue
1.5 AND: [1.3],[1.4],TEM:Years, ASPCT:CONT,DEG:Few;
1.6 COND: [1.3. 1.4, 1.5], [1.2]1.7 Tell PAT:She, ATT:(that), THM:1.8;1.8 Sugar PAT:Her, DEG:High, MOD:QUAL:Very;

Propositional Analysis: EMR
1.1 Complaint PAT: ____, CAT: C hief, THM: 1.3;
1.2 Refer AGT: D., ATT: Dr.; PAT: ____
1.3 ____ ATT: Diabetes Mellitus, CAT: type II;
1.4 History ATT: Personal, THM: Surgery;
1.5 Surgery THM: Cholecystectomy;
1.6 (Patient) ATT: Age, DEG: 60;
1.7 Remove OBJ: Stone, LOC: Kidney, PRT: Left side;
Chief complaint: Referred by Dr. D. Type II diabetes mellitusPersonal history: Surgical: cholecystectomy; Age 60 years oldRemoval of kidney stone on left side
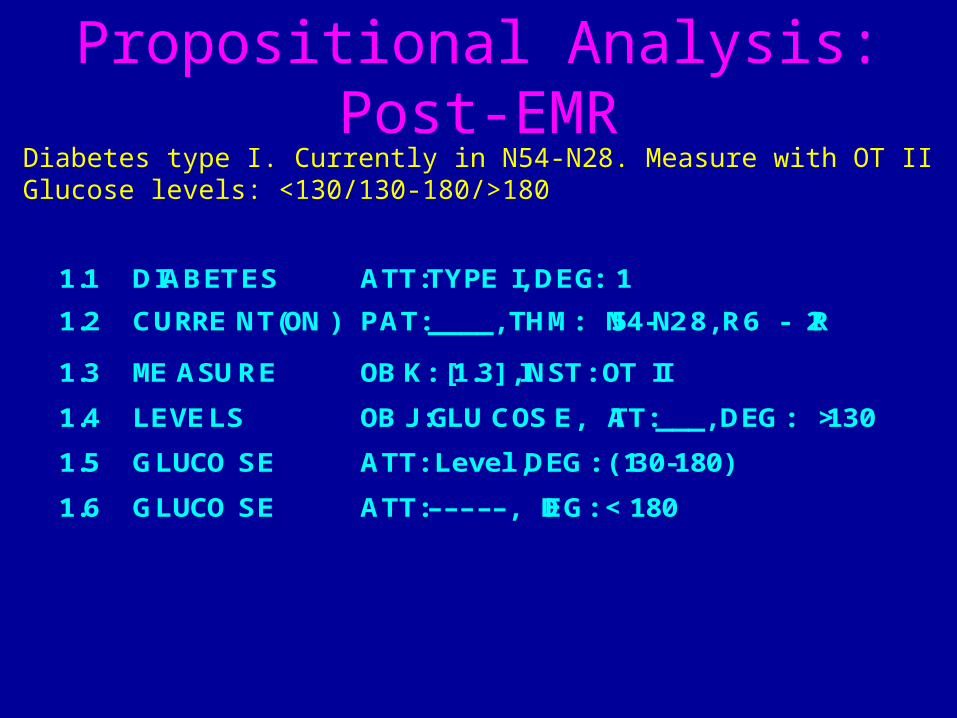
Propositional Analysis: Post-EMR
1.1 DIABETES ATT:TYPE I, DEG: 1
1.2 CURRENT(ON) PAT:____, THM: N54-N28, R6 - R2
1.3 MEASURE OBK: [1.3], INST: OT II
1.4 LEVELS OBJ:GLUCOSE, ATT:___, DEG: > 130
1.5 GLUCOSE ATT: Level, DEG: (130-180)
1.6 GLUCOSE ATT:–––––, DEG: < 180
Diabetes type I. Currently in N54-N28. Measure with OT IIGlucose levels: <130/130-180/>180
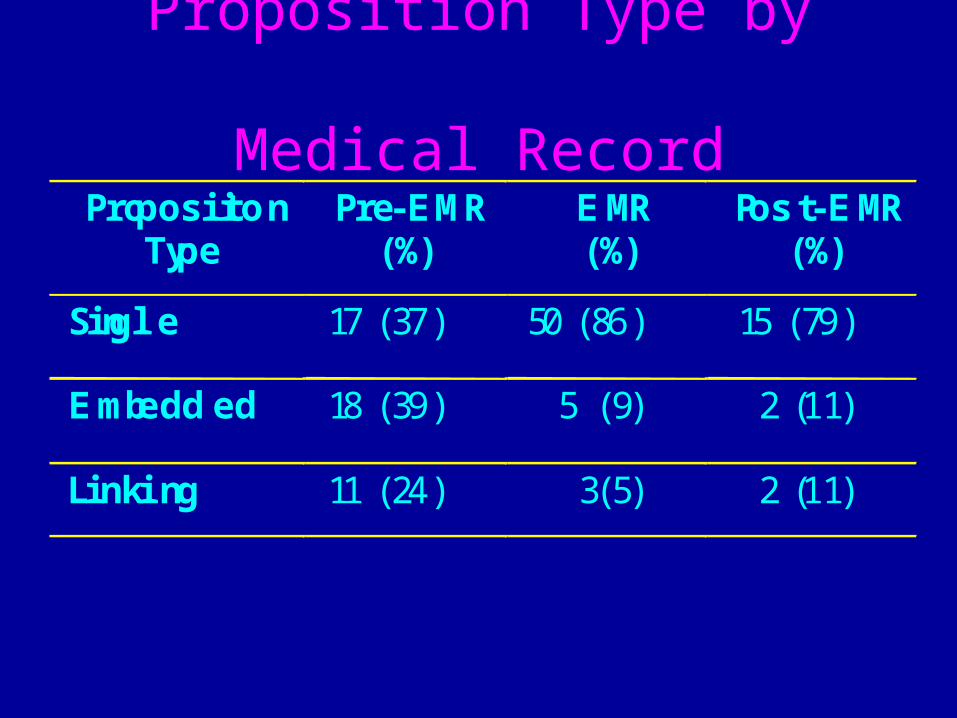
Proposition Type by Medical Record
Propos itio nType
Singl e
Embedd ed
Linking
Pre-EMR(%)
17 (37)
18 (39)
11 (24)
EMR(%)
50 (86)
5 (9)
3(5)
Pos t-EMR(%)
15 (79)
2 (11)
2 (11)
Changes in Reasoning Patterns
– Paper Records• Data-driven reasoning
– Electronic Medical Record• Problem-directed reasoning
– Return to Paper Record after EMR• Problem-directed reasoning
– Residual effect of EMR on behavior (after EMR removed)

Multiple Hypotheses
Electronic Medical Record
HypothesesPatient Data
Diagnostic Reasoning
Patient Data
Paper Record
Return to Paper Record
Same as EMR!

Paper-Based Medical Records• Record before EMR:
• Coherent discourse structure
• Fewer inferences needed
• Temporal order of causal relationships explicit
• Data-driven reasoning
• Increases cognitive load
• Linking propositions constrain interpretation
• Return to paper-based record after EMR• Hypothesis-directed reasoning
• EMR structure maintained: No linking propositions
• Less Information: more inferences needed
Electronic Medical Record• Supports hypothesis-directed reasoning
• Provides flexible structure for data entry and review
• Provides direction and reminders
• Suffers from lack of linking propositions
– Interpretation relies on the users
• Despite time-stamping of events, lacks representation of temporal relationships in evolution of disease processes
– Area for research and implementation


Human-Computer Interaction (HCI) Perspective
Jiajie Zhang, Ph.D.
Department of Health Informatics
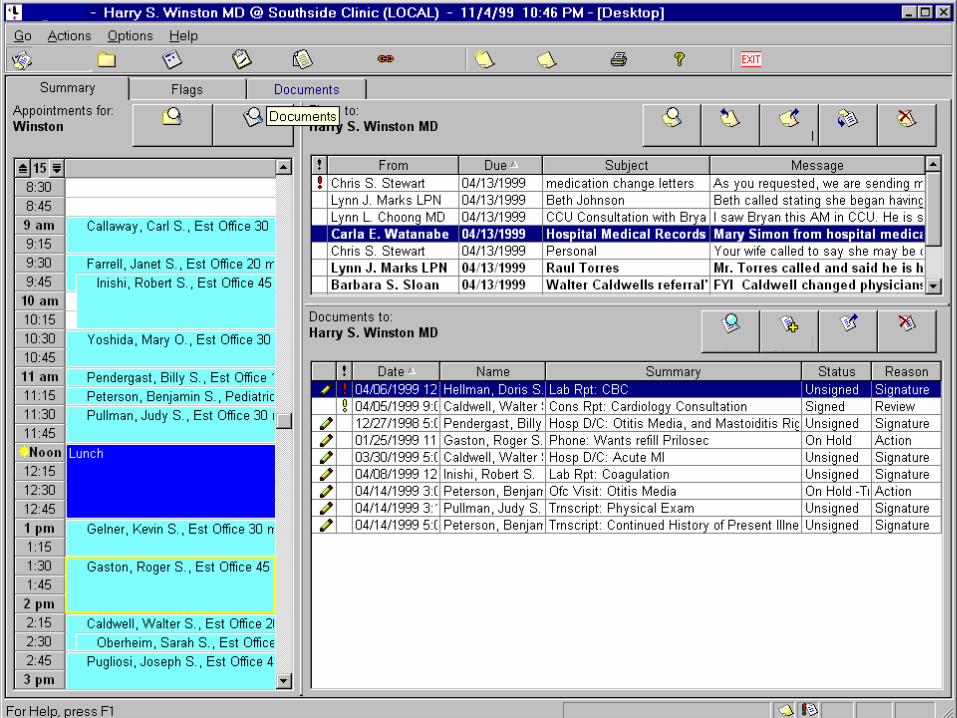
Usability Problems of Current EMR
Desired Features
• Easy to learn• Easy to use• Little or no memorization• Low mental workload• Error proof• Task-Interface match• User-Interface match• Subjectively pleasing
Current Status
• Difficult to learn• Difficult to use• Too much memorization• High mental workload• Error prone• Task-Interface mismatch• User-Interface mismatch• Not subjectively pleasing
Low Acceptance
of EMR

Cost vs. Benefit of Usability
• Phone: 0.15 seconds/digit $1,000,000/year • 757: 3 pilots 2 pilots• Pager: 3000 words 150 words
• Form: $100,000 total $536,023/year• Sign-on: $20,700 total $41,700 1st day • IBM: $1 investment $100 return
Nielsen (1993)
• EMR:

Is the Code Useful?
• 48% code is for user interface.
• Usability engineering ensures that the 48% code is usable.
Nielsen (1993)

Accidents due to Human Errors
0%
20%
40%
60%
80%
100%
Petrochemicalplants
Worldwide Jetcargo
US nuclearpower plants
Automobiles Air trafficcontrol
Human Error Others
(Van Cott, 1994)

Annual Death Rates in US
329 395914986
43649
120000
0
50000
100000
150000
commericalaviationdeaths
drowningdeaths
deaths fromfalls
motor vehicledeaths
deaths frommedical errors
Philadelphia Enquirer (9/12/99)
One jumbo jet crash every day
Direct Interaction Interface
• Direct interaction interfaces are transparent to users such that:– users can directly and completely engage in the primary
desired task.
– users do not have to interact with the interfaces that mediate the system.
• With direct interaction interfaces, – users are able to easily, accurately, and timely retrieve,
seek, gather, encode, transform, organize, and manipulate information to accomplish desired tasks.

System Activities
User Activities
Norman’s Action Theory
Gulf of
Execution
Gulf of
Evaluation
Physical Systems
DirectInteraction
Goal
Delete file
IntentionUse remove command
ActionSpecification
“remove ../../home/paper/talk_old.ver1”
ExecutionTyping command text, hit return
Evaluation Form sub-goal
Interpretation Nothing happened
Perceptionprompt symbol ($),
no feedback
Direct
Action Direct
PerceptionMove to trash can
Click, drag, drop
Physical actions
Goal achieved
File deleted
File disappeared

• From the system side– by direct interaction interfaces.
• From the user side – by extensive and long-term learning.
Bridging the Gulfs
X

Mapping between Task & Interface

InterfaceTaskUniverse
Atoms
Objects
Intention
Steps
Actions
Metaphor
Icons
Objects
Plan
Clicks
Actions
Shneiderman’s Object-Action Model

Universe
Atoms
Intention
Steps
TaskObjects
Actions
Metaphor
Icons
Plan
Clicks
InterfaceObjects
Actions
X
X
Task-Interface Mismatch
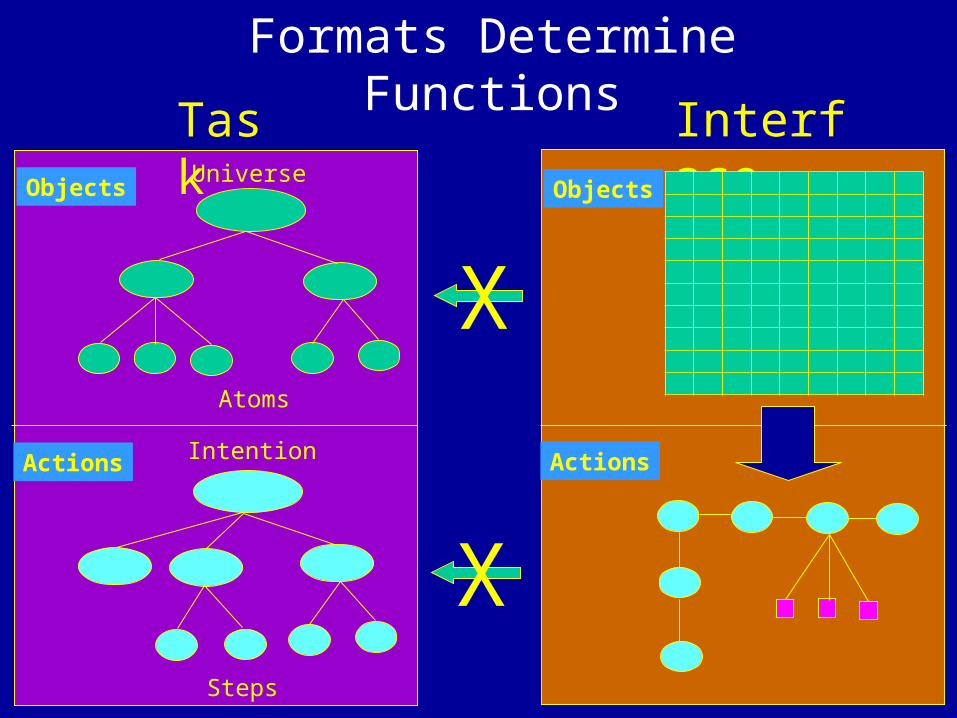
Universe
Atoms
Intention
Steps
TaskObjects
Actions
InterfaceObjects
Actions
X
X
Formats Determine Functions

Conclusion
• In order for EMR to perform the functions that it is promised to perform and to be universally accepted by healthcare professionals, user interface design principles should be systematically applied to the design of EMR at the earliest possible stage.

Usability Now!