what helps when it hurts: children's views on pain relief
TRANSCRIPT
What helps when it hurts: children’s views onpain relief
L. S. Franck,*† A. Sheikh† and K. Oulton‡
*lnstitute of Child Health, University College London†University College London, and‡Great Ormond Street Hospital for Children NHS Trust, London, UK
Accepted for publication 8 October 2007
Keywordschildren’s views, healthbeliefs, pain
Correspondence:Linda S. Franck, PhD, RN,RGN, RSCN, FRCPCH,FAAN, Institute of ChildHealth & Great OrmondStreet Hospital forChildren NHS Trust, Level7, Old Building, GreatOrmond Street, LondonWC1N 3JH, UKE-mail:[email protected]
AbstractBackground Previous studies have focused on children’s views of sources of pain and only
secondarily explored their views on pain-relief strategies.
Methods An exploratory cross-sectional descriptive design and ‘draw and write’ technique were
used to investigate what children think helps them when they have pain.
Results The sample (n = 71) was comprised of 33% boys and 67% girls, with an age range of
4–16 years (mean � SD: 9.25 � 3.04). Four overarching themes were derived that were common to
both the texts and drawings: ‘People who help’, ‘What I do that helps’, ‘What other people do that
helps’ and ‘Things that help’. Children also described their emotional reactions to pain or pain relief.
Multiple themes were represented in most of the texts and drawings. There were few differences in
the themes present in the children’s texts and drawings based on developmental age and no
differences based on gender.
Conclusions Children across the three developmental age groups view themselves as active
agents in pain relief. Although less than half of the children described specific behaviours they had
taken, almost all children indicated their active role as the central figure in relation to use of objects
or the actions of others.
Introduction
The first investigations of children’s views about pain were con-
ducted in the 1970s and 1980s (Schultz 1971; Unruh et al. 1983;
Ross & Ross 1984; Gaffney & Dunne 1986; Hurley & Whelan
1988) showing that school-aged children understood the
concept of pain and could describe its causes and consequences,
and its sensory, cognitive and emotional characteristics. Two of
these studies had large school-based cohorts of 994 (Ross &
Ross 1984) and 680 (Gaffney & Dunne 1986) children, one of
which suggested that children’s understanding of the concept of
pain followed a developmental age trajectory consistent with
Piagetian stages (Gaffney & Dunne 1986) and the other did not
(Ross & Ross 1984). Some studies found a difference in the
descriptors used by boys and girls (Gaffney & Dunne 1986),
whereas others did not (Unruh et al. 1983; Ross & Ross 1984).
Later studies of healthy children’s understanding of and
responses to everyday and medical pain (Alex & Ritchie 1992;
Ely 1992; Harbeck & Peterson 1992; McGrath et al. 1997;
Kortesluoma & Nikkonen 2004) added support to the notion
that children’s concept of pain followed the stages of general
cognitive development and also revealed the importance of
influencing factors such as the child’s gender and type of pain.
In contrast to the body of research about how children per-
ceive pain, less is known about the views of children regarding
people, objects or actions that prevent or relieve pain. Previous
studies have focused primarily on children with post-operative
pain (Woodgate & Kristjanson 1995; Palermo & Lambert 1997;
Original Article doi:10.1111/j.1365-2214.2008.00812.x
© 2008 The AuthorsJournal compilation © 2008 Blackwell Publishing Ltd430
Child: care, health and development

Polkki et al. 2003) and suggest that children may attempt basic
cognitive or physical actions aimed at reducing pain or anxiety.
Ely (1992) found that ‘bandaids’ (plasters) and medicine fea-
tured prominently in school-aged children’s drawings about
pain. However, because of the nature of the research questions
and samples used in previous studies, the findings tended to
emphasize the role of health professionals or parents in chil-
dren’s pain relief. Thus, the broad question of what helps chil-
dren when they have pain has never been directly posed. Greater
understanding of children’s general views on what constitutes
pain-relieving strategies and the factors that influence these
views is essential to ensuring that interventions are develop-
mentally appropriate and generalizable. This report provides
the first in depth analysis of children’s views when asked directly
what helps when they have pain, and provides the basis for
further research on influencing factors and effectiveness of
interventions.
Methods
Design
We used a descriptive, mixed methods design to investigate
what children think helps them when they have pain. The ‘draw
and write’ technique (Bradding & Horstman 1999; Horstman &
Bradding 2002) was used to ascertain children’s views in a child-
friendly manner, with as little adult influence as possible.
Sample and setting
The sample was recruited from children visiting Great Ormond
Street Hospital NHS Trust during the study period as part of a
programme of events to highlight the Global Day against Chil-
dren’s Pain initiated by the IASP, 2005–2006 (http://www.iasp-
pain.org/GlobalDay-2005.htm). Inpatients and outpatients,
as well as siblings or friends of the patients, were all actively
encouraged to take part. Children were eligible to participate if
they were able to draw pictures or write about the topic.
Instruments
The ‘draw and write’ technique gives children the opportunity
to answer the research question themselves without any
prompting or interference from an interviewer. It is often a
better choice of instrument than structured interviews or ques-
tionnaires as it is not intimidating and does not presuppose the
children’s answers, increasing response validity. Internal validity
is also strengthened because there are two within-subject
sources of data, drawings and text. The task involves children
drawing pictures in response to a question or theme as well as
writing their thoughts about the topic. The ‘draw and write’
technique has been used extensively to elicit children’s views
of health and health services (Pridmore & Bendelow 1995;
Pridmore & Lansdown 1997; Bradding & Horstman 1999;
Horstman & Bradding 2002). Drawings have also been used to
explore children’s views about pain (Unruh et al. 1983; Liossi
2000; Stafstrom et al. 2002).
Procedures
Children visiting hospital during the study period were in-
vited to enter a competition. Announcements were displayed
throughout the wards, in the lobby and near the outpatients
department. Nurses and play specialists encouraged participa-
tion of all children regardless of health status.
The competition entry form was an A3 folded sheet with two
large boxes, one for drawing and one for writing. At the top of
each sheet was the incomplete phrase ‘When I hurt the things
that help me are . . . ’. Children were asked to complete the
sentence by drawing or writing something (Fig. 1). They were
asked to give their age and gender. No other personal or clinical
data were obtained. Children could submit their entries to a
member of staff, deposit them in collection boxes or post them.
Children received a box of coloured pencils with the entry form
and those who submitted entry forms were eligible for prize
drawings in one of two age groups, under 8 years and over
8 years of age.
We are trying to find out more about what helps children when they are hurt. Can you help us by drawing or writing about the things that help YOU when you are hurt. If you agree, we would like to display your picture or writing in the hospital or on the hospital website so that other children and adults can learn more about what helps children when they hurt.
Figure 1. ‘Draw and write’ template.
Children’s views on pain relief 431
© 2008 The AuthorsJournal compilation © 2008 Blackwell Publishing Ltd, Child: care, health and development, 34, 4, 430–438

A Research Ethics Committee reviewed the project outline
and determined that it was exempt from review because no
medical or personally identifying data were collected. Parents
and children gave written consent for the anonymized drawings
and text to be displayed.
Data analysis
Thematic content analysis (Boyatzis 1998) was used to derive
the major themes and subthemes represented in the children’s
drawing and writings separately. This methodology is a process
for systematically and objectively encoding qualitative data into
categorical data, extracting patterns, and describing or organiz-
ing observations. The units of analysis were the message char-
acteristics encoded within the texts and drawings. Data were
initially organized by one investigator (AS) using open coding,
without regard for relative importance. In this way, the breadth
of conceptual possibilities was appreciated. Conceptual catego-
ries that were salient across participants were created and vali-
dated by the second investigator (LF). Coding and conceptual
categories were defined precisely, and illustrated with verbatim
quotes to ensure completeness, inter-rater reliability and
validity.
Descriptive statistics were computed for the demographic
variables (age and gender) and for the major thematic catego-
ries. Non-parametric tests were used for all comparisons, and
P-values of less than 0.05 were considered significant.
Results
The sample (n = 71) was comprised of 33% boys and 67% girls,
with an age range of 4–16 years (mean � SD: 9.25 � 3.04).
According to Piagetian developmental stages (Meadows 2006),
24% of the children were preoperational (less than 7 years of
age), 49% of them were concrete operational (7–11 years of age)
and 27% were formal operational (12 years and older). Three
boys (aged 9, 9 and 6 years) provided drawings only. All other
children provided texts and drawings.
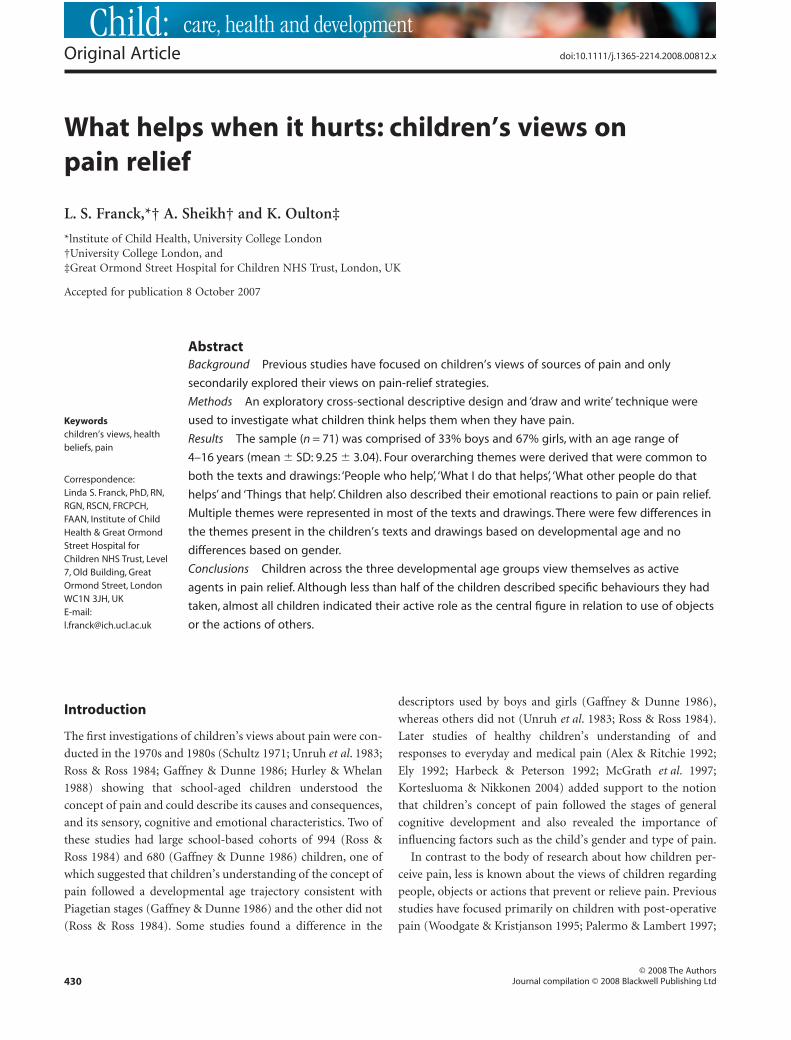
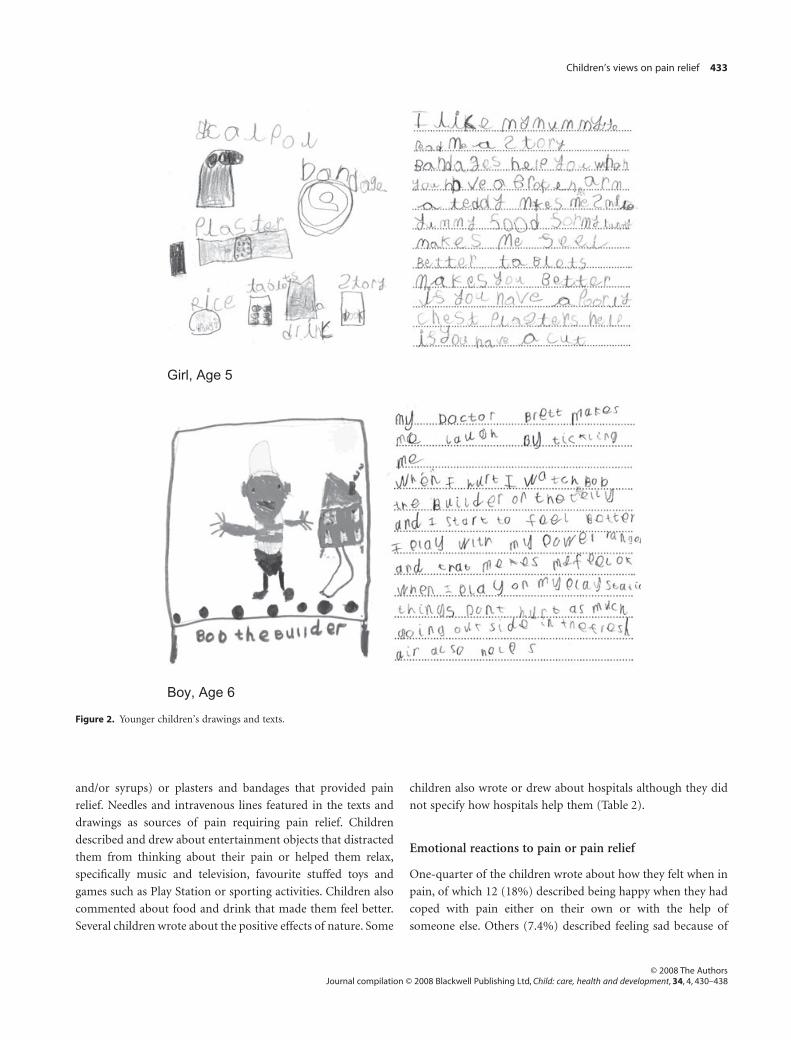
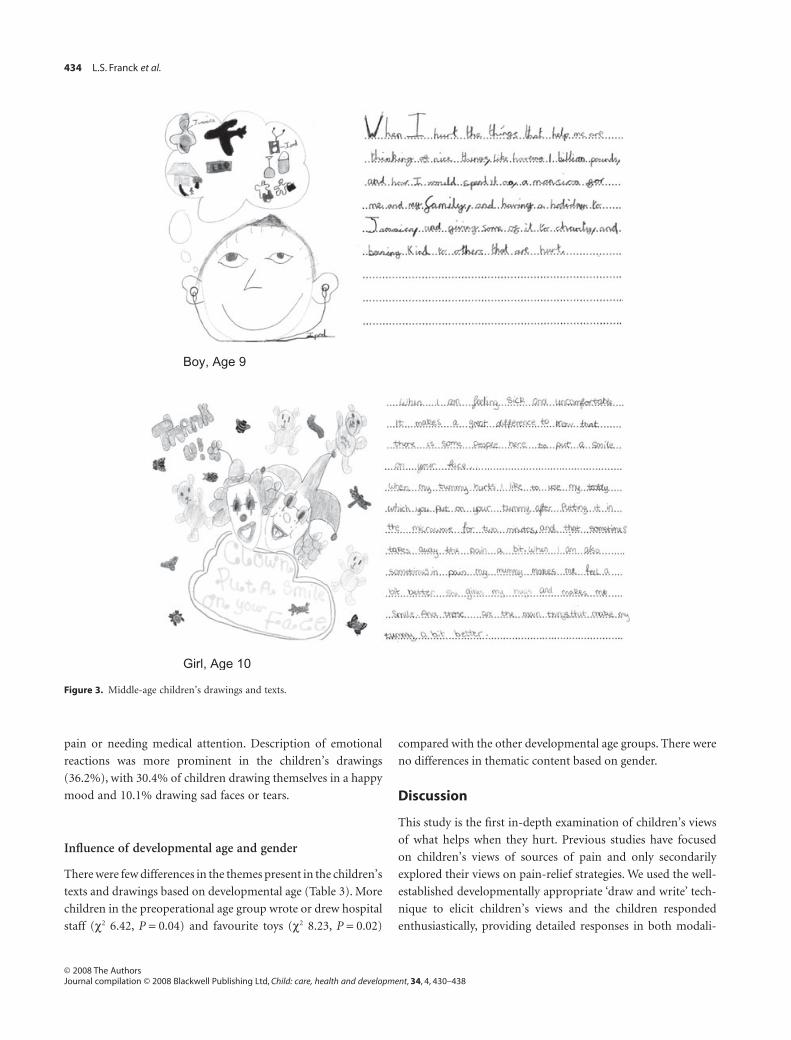
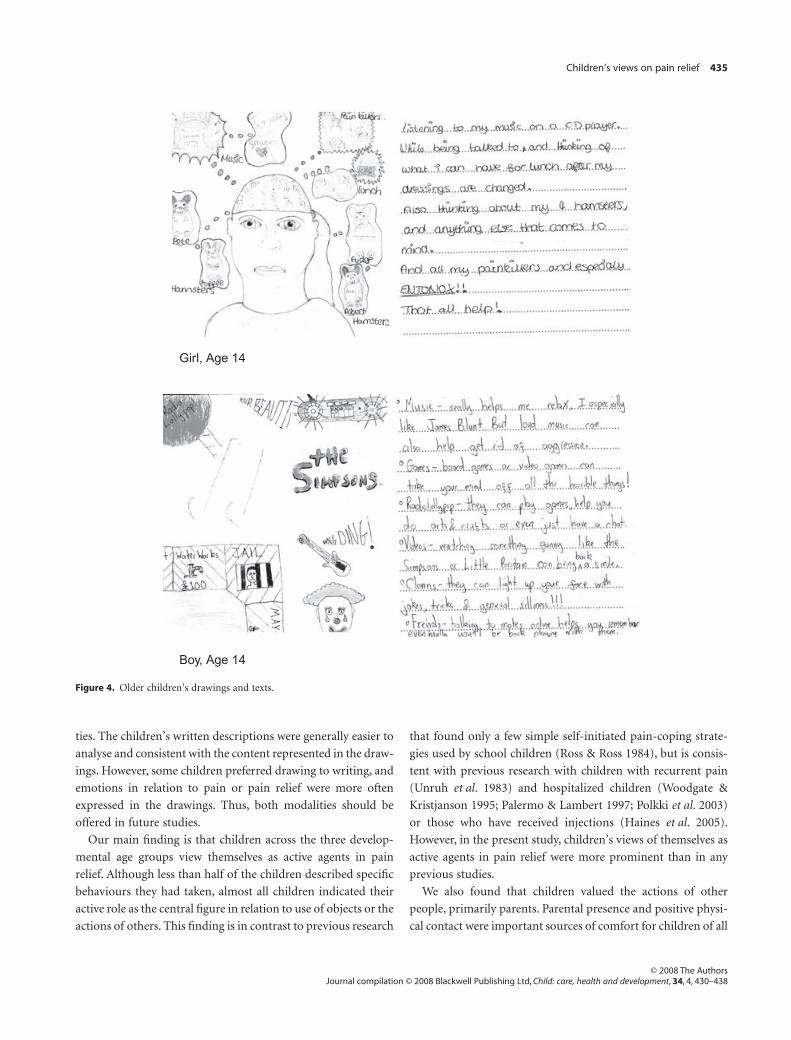
Four overarching themes were derived that were common
to both the texts and drawings: ‘People who help’, ‘What I do
that helps’, ‘What other people do that helps’ and ‘Things
that help’. Children also described their emotional reactions
to pain or pain relief. Multiple themes were represented in
most of the texts and drawings. Examples illustrating these
themes across the three developmental ages are shown in
Figs 2–4. More examples can be viewed on the Children’s First
for Health website, Kid, Creative Corner (http://www.
childrenfirstforhealth.org).
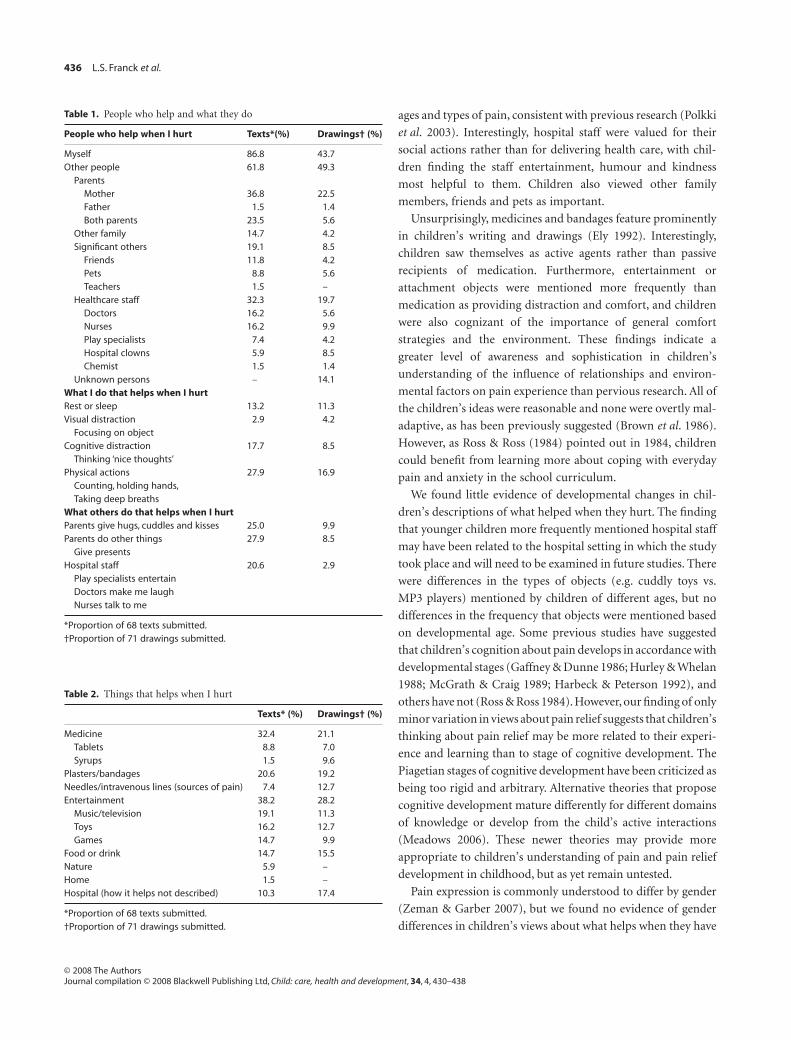
People who help when I hurt
Table 1 shows the percentages of children who wrote or drew
about people who helped them when they hurt. Almost all of
the children wrote about people (n = 64; 94.1%) who help to
make their pain better. Fewer children (n = 50; 70.4%) drew
pictures of people who helped them when they hurt. Most of the
children mentioned themselves as the central figure in dealing
with pain and about half as many children drew pictures of this.
Parents were the next most frequent person to appear in the
texts and drawings. More children identified their mother
or both parents as helping them. Other family members who
helped included siblings and grandparents and significant
others such as friends, pets and teachers. Hospital staff were
described, specifically doctors and nurses, play specialists, hos-
pital clowns and the chemist. In 10 cases, the persons drawn
were not identifiable from the drawings or from the accompa-
nying text.
What I do that helps when I hurt
Over half of the children (n = 43; 63.2%) wrote about behav-
iours or actions they initiated themselves to provide pain relief.
Slightly fewer children (n = 38; 53.5%) drew pictures of these
actions. The self-initiated strategies were varied and included
limiting activity by resting or sleeping, engaging in visual dis-
traction by concentrating on an object in front of them (e.g.
the fish on the cubicle curtain fabric), cognitive distraction by
thinking of ‘nice things’ or by physical actions such as counting
to 10, holding someone’s hand or taking deep breaths (Table 1).
Many of the children wrote about their active role in taking
medication or about how they decided when medication was
indicated. They notably did not use words or phrases indicating
a passive role (e.g. ‘mummy gave me’ or ‘I was given’).
What others do that helps when I hurt
Children described in writing (n = 39; 57.3%) or drew (n = 11;
15.5%) the actions of other people that helped them when they
hurt. The most common were hugs, cuddles and kisses from
parents and other actions by parents, such as giving gifts to
children. Fewer children wrote or drew about the actions of
hospital staff, and the actions described were predominantly
entertainment provided by play specialists or clowns, doctors
making children laugh and nurses talking to them (Table 1).
Things that help when I hurt
Many children described in their writing (n = 56; 82.3%) and
drawing (n = 54; 76.1%) objects such as medicine (tablets
432 L.S. Franck et al.
© 2008 The AuthorsJournal compilation © 2008 Blackwell Publishing Ltd, Child: care, health and development, 34, 4, 430–438
and/or syrups) or plasters and bandages that provided pain
relief. Needles and intravenous lines featured in the texts and
drawings as sources of pain requiring pain relief. Children
described and drew about entertainment objects that distracted
them from thinking about their pain or helped them relax,
specifically music and television, favourite stuffed toys and
games such as Play Station or sporting activities. Children also
commented about food and drink that made them feel better.
Several children wrote about the positive effects of nature. Some
children also wrote or drew about hospitals although they did
not specify how hospitals help them (Table 2).
Emotional reactions to pain or pain relief
One-quarter of the children wrote about how they felt when in
pain, of which 12 (18%) described being happy when they had
coped with pain either on their own or with the help of
someone else. Others (7.4%) described feeling sad because of
Girl, Age 5
Boy, Age 6
Figure 2. Younger children’s drawings and texts.
Children’s views on pain relief 433
© 2008 The AuthorsJournal compilation © 2008 Blackwell Publishing Ltd, Child: care, health and development, 34, 4, 430–438
pain or needing medical attention. Description of emotional
reactions was more prominent in the children’s drawings
(36.2%), with 30.4% of children drawing themselves in a happy
mood and 10.1% drawing sad faces or tears.
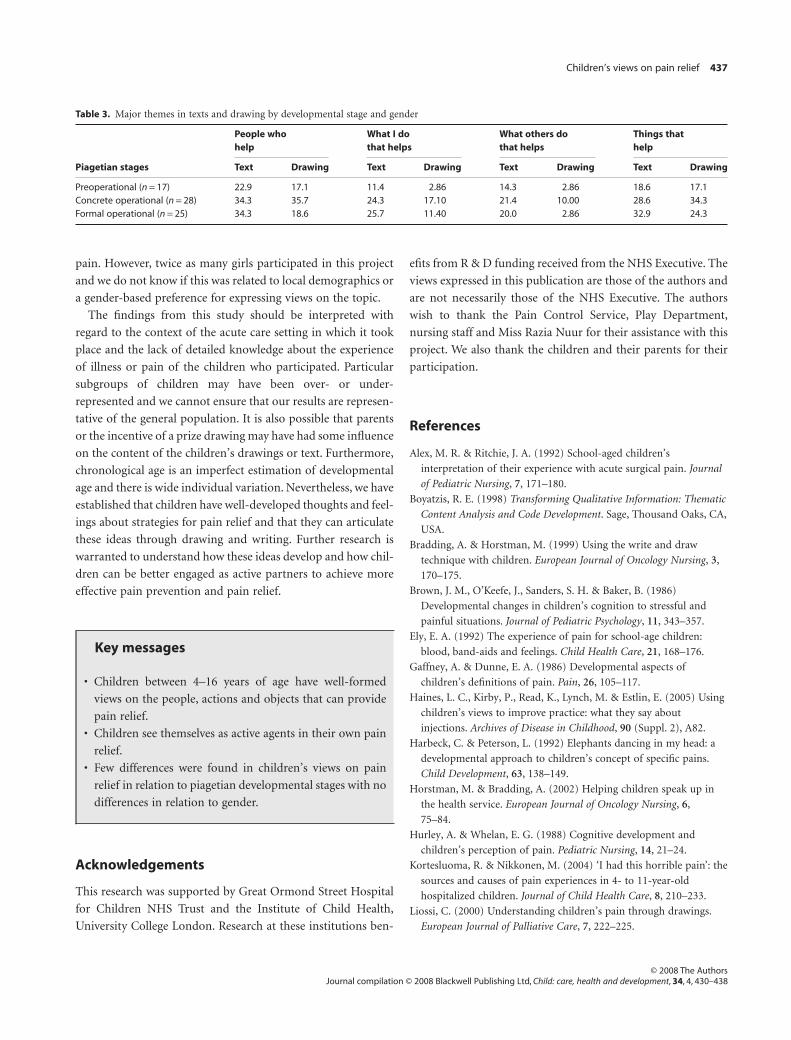
Influence of developmental age and gender
There were few differences in the themes present in the children’s
texts and drawings based on developmental age (Table 3). More
children in the preoperational age group wrote or drew hospital
staff (c2 6.42, P = 0.04) and favourite toys (c2 8.23, P = 0.02)
compared with the other developmental age groups. There were
no differences in thematic content based on gender.
Discussion
This study is the first in-depth examination of children’s views
of what helps when they hurt. Previous studies have focused
on children’s views of sources of pain and only secondarily
explored their views on pain-relief strategies. We used the well-
established developmentally appropriate ‘draw and write’ tech-
nique to elicit children’s views and the children responded
enthusiastically, providing detailed responses in both modali-
Boy, Age 9
Girl, Age 10
Figure 3. Middle-age children’s drawings and texts.
434 L.S. Franck et al.
© 2008 The AuthorsJournal compilation © 2008 Blackwell Publishing Ltd, Child: care, health and development, 34, 4, 430–438
ties. The children’s written descriptions were generally easier to
analyse and consistent with the content represented in the draw-
ings. However, some children preferred drawing to writing, and
emotions in relation to pain or pain relief were more often
expressed in the drawings. Thus, both modalities should be
offered in future studies.
Our main finding is that children across the three develop-
mental age groups view themselves as active agents in pain
relief. Although less than half of the children described specific
behaviours they had taken, almost all children indicated their
active role as the central figure in relation to use of objects or the
actions of others. This finding is in contrast to previous research
that found only a few simple self-initiated pain-coping strate-
gies used by school children (Ross & Ross 1984), but is consis-
tent with previous research with children with recurrent pain
(Unruh et al. 1983) and hospitalized children (Woodgate &
Kristjanson 1995; Palermo & Lambert 1997; Polkki et al. 2003)
or those who have received injections (Haines et al. 2005).
However, in the present study, children’s views of themselves as
active agents in pain relief were more prominent than in any
previous studies.
We also found that children valued the actions of other
people, primarily parents. Parental presence and positive physi-
cal contact were important sources of comfort for children of all
Girl, Age 14
Boy, Age 14
Figure 4. Older children’s drawings and texts.
Children’s views on pain relief 435
© 2008 The AuthorsJournal compilation © 2008 Blackwell Publishing Ltd, Child: care, health and development, 34, 4, 430–438
ages and types of pain, consistent with previous research (Polkki
et al. 2003). Interestingly, hospital staff were valued for their
social actions rather than for delivering health care, with chil-
dren finding the staff entertainment, humour and kindness
most helpful to them. Children also viewed other family
members, friends and pets as important.
Unsurprisingly, medicines and bandages feature prominently
in children’s writing and drawings (Ely 1992). Interestingly,
children saw themselves as active agents rather than passive
recipients of medication. Furthermore, entertainment or
attachment objects were mentioned more frequently than
medication as providing distraction and comfort, and children
were also cognizant of the importance of general comfort
strategies and the environment. These findings indicate a
greater level of awareness and sophistication in children’s
understanding of the influence of relationships and environ-
mental factors on pain experience than pervious research. All of
the children’s ideas were reasonable and none were overtly mal-
adaptive, as has been previously suggested (Brown et al. 1986).
However, as Ross & Ross (1984) pointed out in 1984, children
could benefit from learning more about coping with everyday
pain and anxiety in the school curriculum.
We found little evidence of developmental changes in chil-
dren’s descriptions of what helped when they hurt. The finding
that younger children more frequently mentioned hospital staff
may have been related to the hospital setting in which the study
took place and will need to be examined in future studies. There
were differences in the types of objects (e.g. cuddly toys vs.
MP3 players) mentioned by children of different ages, but no
differences in the frequency that objects were mentioned based
on developmental age. Some previous studies have suggested
that children’s cognition about pain develops in accordance with
developmental stages (Gaffney & Dunne 1986; Hurley & Whelan
1988; McGrath & Craig 1989; Harbeck & Peterson 1992), and
others have not (Ross & Ross 1984). However, our finding of only
minor variation in views about pain relief suggests that children’s
thinking about pain relief may be more related to their experi-
ence and learning than to stage of cognitive development. The
Piagetian stages of cognitive development have been criticized as
being too rigid and arbitrary. Alternative theories that propose
cognitive development mature differently for different domains
of knowledge or develop from the child’s active interactions
(Meadows 2006). These newer theories may provide more
appropriate to children’s understanding of pain and pain relief
development in childhood, but as yet remain untested.
Pain expression is commonly understood to differ by gender
(Zeman & Garber 2007), but we found no evidence of gender
differences in children’s views about what helps when they have
Table 1. People who help and what they do
People who help when I hurt Texts*(%) Drawings† (%)
Myself 86.8 43.7Other people 61.8 49.3
ParentsMother 36.8 22.5Father 1.5 1.4Both parents 23.5 5.6
Other family 14.7 4.2Significant others 19.1 8.5
Friends 11.8 4.2Pets 8.8 5.6Teachers 1.5 –
Healthcare staff 32.3 19.7Doctors 16.2 5.6Nurses 16.2 9.9Play specialists 7.4 4.2Hospital clowns 5.9 8.5Chemist 1.5 1.4
Unknown persons – 14.1What I do that helps when I hurtRest or sleep 13.2 11.3Visual distraction 2.9 4.2
Focusing on objectCognitive distraction 17.7 8.5
Thinking ‘nice thoughts’Physical actions 27.9 16.9
Counting, holding hands,Taking deep breaths
What others do that helps when I hurtParents give hugs, cuddles and kisses 25.0 9.9Parents do other things 27.9 8.5
Give presentsHospital staff 20.6 2.9
Play specialists entertainDoctors make me laughNurses talk to me
*Proportion of 68 texts submitted.†Proportion of 71 drawings submitted.
Table 2. Things that helps when I hurt
Texts* (%) Drawings† (%)
Medicine 32.4 21.1Tablets 8.8 7.0Syrups 1.5 9.6
Plasters/bandages 20.6 19.2Needles/intravenous lines (sources of pain) 7.4 12.7Entertainment 38.2 28.2
Music/television 19.1 11.3Toys 16.2 12.7Games 14.7 9.9
Food or drink 14.7 15.5Nature 5.9 –Home 1.5 –Hospital (how it helps not described) 10.3 17.4
*Proportion of 68 texts submitted.†Proportion of 71 drawings submitted.
436 L.S. Franck et al.
© 2008 The AuthorsJournal compilation © 2008 Blackwell Publishing Ltd, Child: care, health and development, 34, 4, 430–438
pain. However, twice as many girls participated in this project
and we do not know if this was related to local demographics or
a gender-based preference for expressing views on the topic.
The findings from this study should be interpreted with
regard to the context of the acute care setting in which it took
place and the lack of detailed knowledge about the experience
of illness or pain of the children who participated. Particular
subgroups of children may have been over- or under-
represented and we cannot ensure that our results are represen-
tative of the general population. It is also possible that parents
or the incentive of a prize drawing may have had some influence
on the content of the children’s drawings or text. Furthermore,
chronological age is an imperfect estimation of developmental
age and there is wide individual variation. Nevertheless, we have
established that children have well-developed thoughts and feel-
ings about strategies for pain relief and that they can articulate
these ideas through drawing and writing. Further research is
warranted to understand how these ideas develop and how chil-
dren can be better engaged as active partners to achieve more
effective pain prevention and pain relief.
Acknowledgements
This research was supported by Great Ormond Street Hospital
for Children NHS Trust and the Institute of Child Health,
University College London. Research at these institutions ben-
efits from R & D funding received from the NHS Executive. The
views expressed in this publication are those of the authors and
are not necessarily those of the NHS Executive. The authors
wish to thank the Pain Control Service, Play Department,
nursing staff and Miss Razia Nuur for their assistance with this
project. We also thank the children and their parents for their
participation.
References
Alex, M. R. & Ritchie, J. A. (1992) School-aged children’s
interpretation of their experience with acute surgical pain. Journal
of Pediatric Nursing, 7, 171–180.
Boyatzis, R. E. (1998) Transforming Qualitative Information: Thematic
Content Analysis and Code Development. Sage, Thousand Oaks, CA,
USA.
Bradding, A. & Horstman, M. (1999) Using the write and draw
technique with children. European Journal of Oncology Nursing, 3,
170–175.
Brown, J. M., O’Keefe, J., Sanders, S. H. & Baker, B. (1986)
Developmental changes in children’s cognition to stressful and
painful situations. Journal of Pediatric Psychology, 11, 343–357.
Ely, E. A. (1992) The experience of pain for school-age children:
blood, band-aids and feelings. Child Health Care, 21, 168–176.
Gaffney, A. & Dunne, E. A. (1986) Developmental aspects of
children’s definitions of pain. Pain, 26, 105–117.
Haines, L. C., Kirby, P., Read, K., Lynch, M. & Estlin, E. (2005) Using
children’s views to improve practice: what they say about
injections. Archives of Disease in Childhood, 90 (Suppl. 2), A82.
Harbeck, C. & Peterson, L. (1992) Elephants dancing in my head: a
developmental approach to children’s concept of specific pains.
Child Development, 63, 138–149.
Horstman, M. & Bradding, A. (2002) Helping children speak up in
the health service. European Journal of Oncology Nursing, 6,
75–84.
Hurley, A. & Whelan, E. G. (1988) Cognitive development and
children’s perception of pain. Pediatric Nursing, 14, 21–24.
Kortesluoma, R. & Nikkonen, M. (2004) ‘I had this horrible pain’: the
sources and causes of pain experiences in 4- to 11-year-old
hospitalized children. Journal of Child Health Care, 8, 210–233.
Liossi, C. (2000) Understanding children’s pain through drawings.
European Journal of Palliative Care, 7, 222–225.
Table 3. Major themes in texts and drawing by developmental stage and gender
Piagetian stages
People whohelp
What I dothat helps
What others dothat helps
Things thathelp
Text Drawing Text Drawing Text Drawing Text Drawing
Preoperational (n = 17) 22.9 17.1 11.4 2.86 14.3 2.86 18.6 17.1Concrete operational (n = 28) 34.3 35.7 24.3 17.10 21.4 10.00 28.6 34.3Formal operational (n = 25) 34.3 18.6 25.7 11.40 20.0 2.86 32.9 24.3
Key messages
• Children between 4–16 years of age have well-formed
views on the people, actions and objects that can provide
pain relief.
• Children see themselves as active agents in their own pain
relief.
• Few differences were found in children’s views on pain
relief in relation to piagetian developmental stages with no
differences in relation to gender.
Children’s views on pain relief 437
© 2008 The AuthorsJournal compilation © 2008 Blackwell Publishing Ltd, Child: care, health and development, 34, 4, 430–438

McGrath, P. J. & Craig, K. D. (1989) Developmental and
psychological aspects of pain in children. Pediatric Clinics of North
America, 36, 823–836.
McGrath, P. A., Speechley, K. N., Seifert, C. E. & Gorodzinsky, F. P.
(1997) A survey of children’s pain experience and know;
edge-phase 1. In: Proceedings of the 8th World Congress on Pain (eds
T. S. Jensen, J. A. Turner & Z. Weisenfiled-Hallin), pp. 903–916.
IASP Press, Seattle, WA, USA.
Meadows, S. (2006) The Child as Thinker: Development and
Acquisition of Cognition in Childhood, 2nd edn. Routledge, London,
UK.
Palermo, T. M. & Lambert, S. A. (1997) A descriptive study of
children’s beliefs concerning the use of analgesics in treating
postoperative pain. Children’s Health Care, 26, 47–59.
Polkki, T., Pietila, A. M. & Vehvilainen-Julkunen, K. (2003)
Hospitalized children’s descriptions of their experiences with
postsurgical pain relieving methods. International Journal of
Nursing Studies, 40, 44.
Pridmore, P. & Bendelow, G. (1995) Images of health: exploring
beliefs of children using the ‘draw-and-write’ technique. Health
Education Journal, 54, 473–488.
Pridmore, P. & Lansdown, R. (1997) Exploring children’s perceptions
of health: does drawing really break down barriers? Health
Education Journal, 56, 219–230.
Ross, D. M. & Ross, S. A. (1984) Childhood pain: the school-aged
child’s viewpoint. Pain, 20, 179–191.
Schultz, N. (1971) How children perceive pain. Nursing Outlook, 19,
670–673.
Stafstrom, C. E., Rostasy, K. & Minster, A. (2002) The usefulness of
children’s drawings in the diagnosis of headache. Pediatrics, 109,
460–472.
Unruh, A., McGrath, P. J., Cunningham, S. J. & Humphreys, P.
(1983) Children’s drawings of their pain. Pain, 17, 385–392.
Woodgate, R. & Kristjanson, L. J. (1995) Young children’s
behavioural responses to acute pain: strategies for getting better.
Journal of Advanced Nursing, 22, 243–249.
Zeman, J. & Garber, J. (2007) Display rules for anger, sadness and
pain: it depends on who is watching. Child Development, 67,
957–973.
438 L.S. Franck et al.
© 2008 The AuthorsJournal compilation © 2008 Blackwell Publishing Ltd, Child: care, health and development, 34, 4, 430–438