west michigan renal symposium - nkfm
TRANSCRIPT

1
West Michigan
Renal Symposium: Managing CKD
NKF of Michigan Mission Statement:
Prevent kidney disease and improve the quality of life for those living with it.
Mary Cooley, RN, BSN, MS
AVP, Care Management and Operations

2
Priority Health
Michigan’s second largest health plan serving more than half a million
people.
Committed to improving the health and lives of our neighbors.
Offer health plans for every stage of life –from the young to the young
at heart
Feature a network of more than 95% of health care providers in
Michigan
3
Priority Health’s Core Purpose
To Improve the health and lives of the
Members we Serve.
Strategic Goal:
Attacking chronic disease to improve outcomes, lower
cost and improve members' quality of life

4
Change
The way
care
is delivered
Engage
Members
In their
health
Innovate
Products
and
distribution + +
Priority Health’s Value Proposition

5
The Triple Aim Population Health
Exceptional Experience
Better Care for Individuals
Lower Costs

0
5
10
15
20
25
0
1
2
3
4
5
6
7
8
1958 61 64 67 70 73 76 79 82 85 88 91 94 97 00 03 06 09
Nu
mb
er
wit
h D
iab
ete
s (
Millio
ns)
Perc
en
tag
e w
ith
Dia
bete
s
Year
Percentage with Diabetes
Number with Diabetes
Number and Percentage of U.S. Population with Diagnosed Diabetes,
1958–2010
CDC’s Division of Diabetes Translation. National Diabetes Surveillance System
available at http://www.cdc.gov/diabetes/statistics
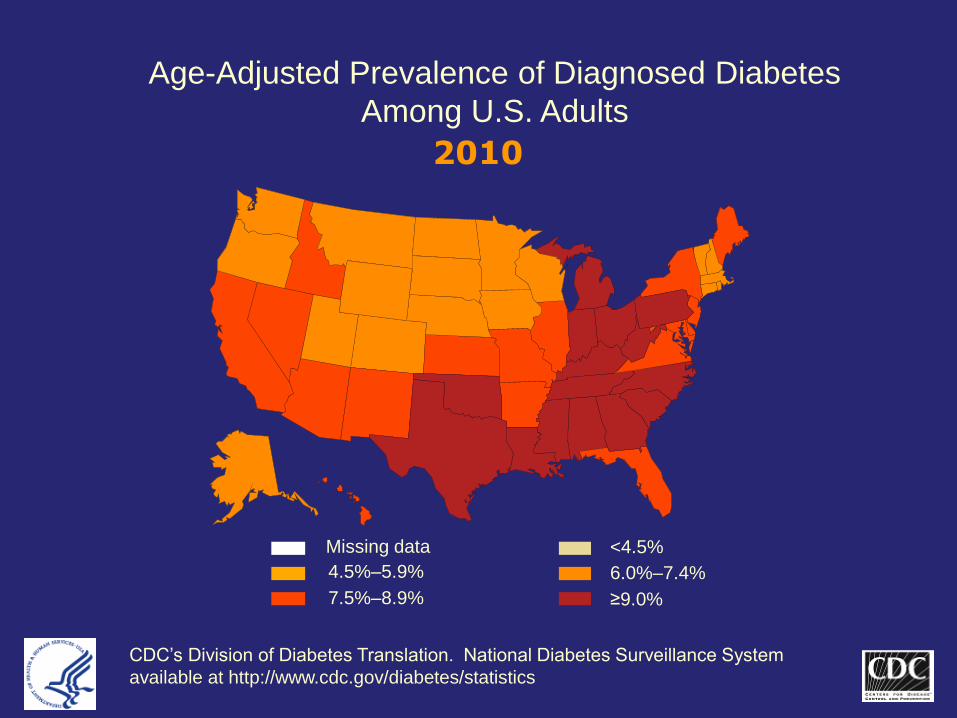
Age-Adjusted Prevalence of Diagnosed Diabetes
Among U.S. Adults
<4.5% Missing data
4.5%–5.9% 6.0%–7.4%
7.5%–8.9% ≥9.0%
CDC’s Division of Diabetes Translation. National Diabetes Surveillance System
available at http://www.cdc.gov/diabetes/statistics
2010

8
Although one out of three adults—about 78 million people—has hypertension, only 52.5% of adults have it controlled. With direct medical expenses estimated at $47.5 billion a year and $3.5 billion in lost productivity. This rate has not changed since 2007 with an expected rate of 37.2% by 2030.
Hypertension

9
One in three Americans is at risk for
kidney disease
10
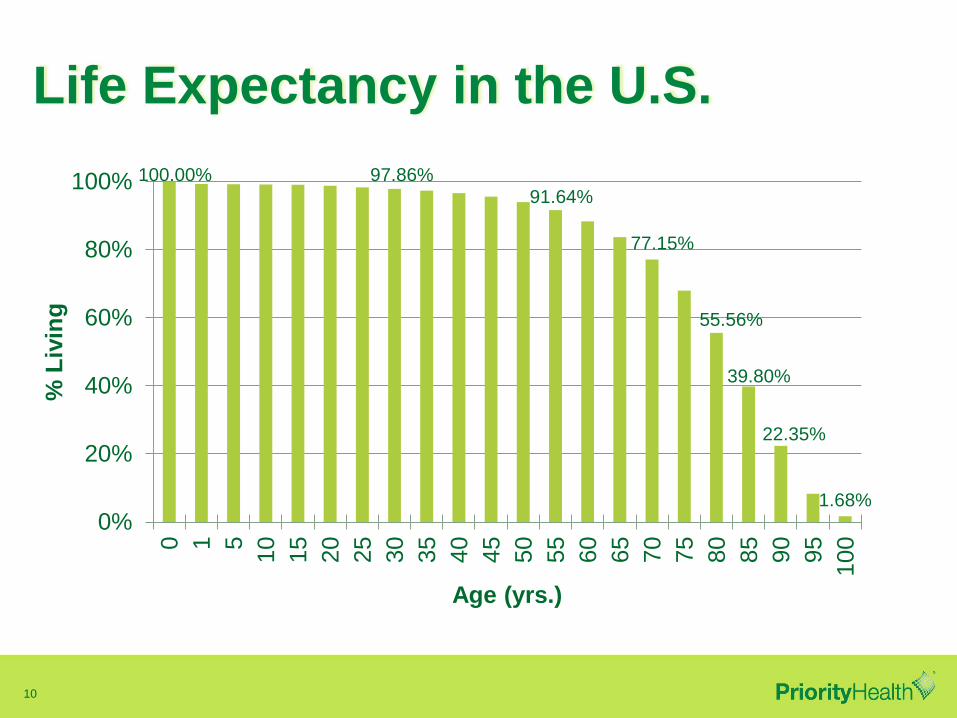
Life Expectancy in the U.S.
100.00% 97.86%
91.64%
77.15%
55.56%
39.80%
22.35%
1.68%
0%
20%
40%
60%
80%
100%0 1 5
10
15
20
25
30
35
40
45
50
55
60
65
70
75
80
85
90
95
100
% L
ivin
g
Age (yrs.)
11
Emerging Issues in Access to
Health Services*
Access to health care services in the United States is
regarded as unreliable; many people do not receive the
appropriate and timely care they need. The U.S. health
care system, which is already strained, will face an influx
of patients in 2014, when 32 million Americans will have
health insurance for the first time. All of these issues, and
others, make the measurement and development of new
strategies and models essential.
*CDC-HealthyPeople.Gov

12
Main Drivers of Total Cost of Care: Chronic Disease
•Accounts for 70% of deaths and ~75% of direct healthcare costs in
USA
•Nearly 1 of every 2 adult Americans has at least one chronic disease
•Prevalence of major contributing factors:
-adult obesity 36%
-diabetes 7-10%
-hypertension 31%
NHANES, CDC, 2011
Prevalence increases dramatically with age
# of Members Annual cost Cost/mbr
CKD w/out ESRD 2154 $3,175,776 $ 1,474.36
CKD with ESRD 504 $20,465,712 $ 40,606.57

13
Social Determinants of Health
Source: Authors’ analysis and adaption from the
University of Wisconsin Population Health Institute’s
County Health Rankings model (2010)
countyhealthrankings.org/about-project/background

14
Barriers to CKD Improvement:
Claims data alone is insufficient to identify mbr population with
CKD (only 32% of PH mbrs with stage 3 CKD had a renal dx).
Often patients do not know they have CKD!
CKD clinical practice guidelines are complex. PCP awareness,
time and capacity are limited. Simple, iterative intervention/solution
needed.
CKD care fragmented, Nephrologist often consulted too late, and
access/availability is inadequate.
Mortality and CV events strongly correlated with progression of
CKD
CKD complex, spans multiple chronic conditions – does not fit into
traditional disease management program structure.

15
Gaps in Care
In 2005, approximately 1.2% of Medicare's 31 million
beneficiaries who had ESRD generated 6.4% of Medicare's
total costs. One of the most important aspects of CKD
diagnosis and treatment is early detection and aggressive
management of underlying causes. However, care for CKD
patients is fragmented. Primary care physicians,
cardiovascular specialists, endocrinologists, dietitians, and
pharmacists may be engaged in the patient's care early but
the nephrologist may not be approached until late, if at all.

16
Why is this important and what are
our next steps?
17
The
The
Priority Health
Difference

18
Triple Aim Goals of CKD Workgroup
Progression of CKD reduced as a result of improvement in
evidence-based medicine accelerated by provider incentive
program:
•Improved screening/identification of members with CKD
•Improved provider adherence to CKD clinical practice guidelines
(care tailored to CKD stage)
•Improved management of key risk factors
BP <130/80
HbA1c < 7%
Persistence of Ace/Arb therapy, >75% MPR
•Care management for patients in Stage 3 and beyond
•Improvement in QOL/Functional status for members with CKD
•Reduction in cost/mbr with CKD as incidence of ESRD
19
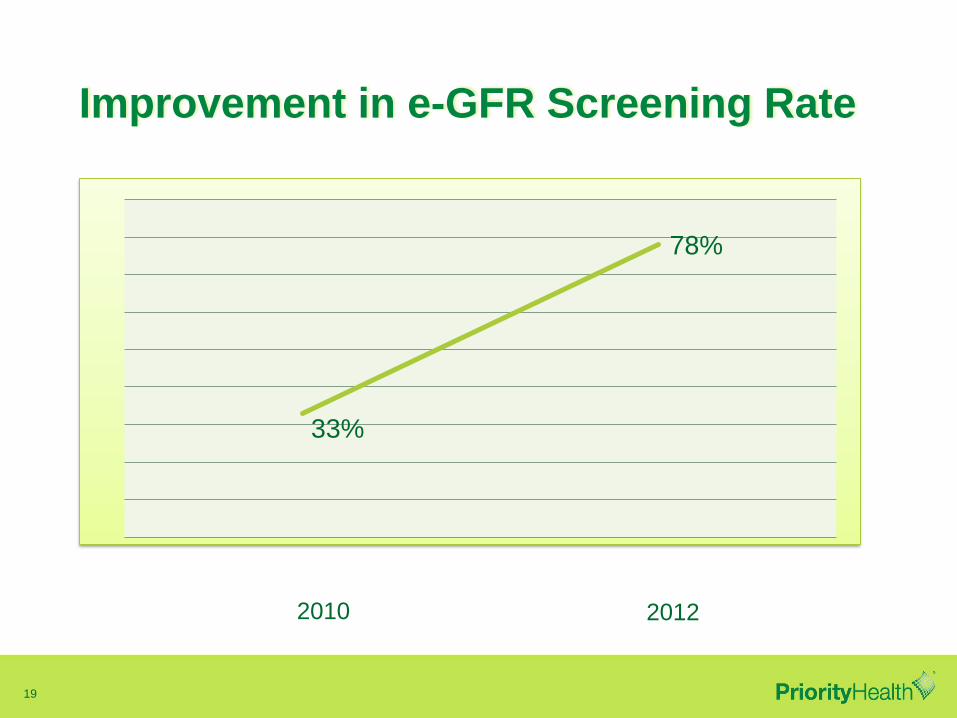
Improvement in e-GFR Screening Rate
33%
78%
2010 2012

20
Medical Cost Avoided - Diabetes
Potentially Avoidable Complications (PAC) – lower is better
High quality and better management reduces avoidable cost
0%
5%
10%
15%
20%
25%
30%
35%
Diabetes
PH PAC Cost Percent
MI Avg PAC Cost Percent
US Avg PAC Cost Percent
US Minimum
PAC
Percent
of Costs

21
Diabetes ACE/ARB

22
Diabetes
60%
65%
70%
75%
80%
85%
90%
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Priority Health Average 90th percentile Benchmark Plan
A1c testing and outcome
LDL testing and outcome
BP outcome
Eye exams
Nephropathy screening

23
Cardiovascular
40%
50%
60%
70%
80%
90%
100%
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Priority Health Average 90th percentile Benchmark Plan National Average
Hypertension BP control
Cholesterol testing and outcome, with CV disease
Beta Blocker after AMI
24
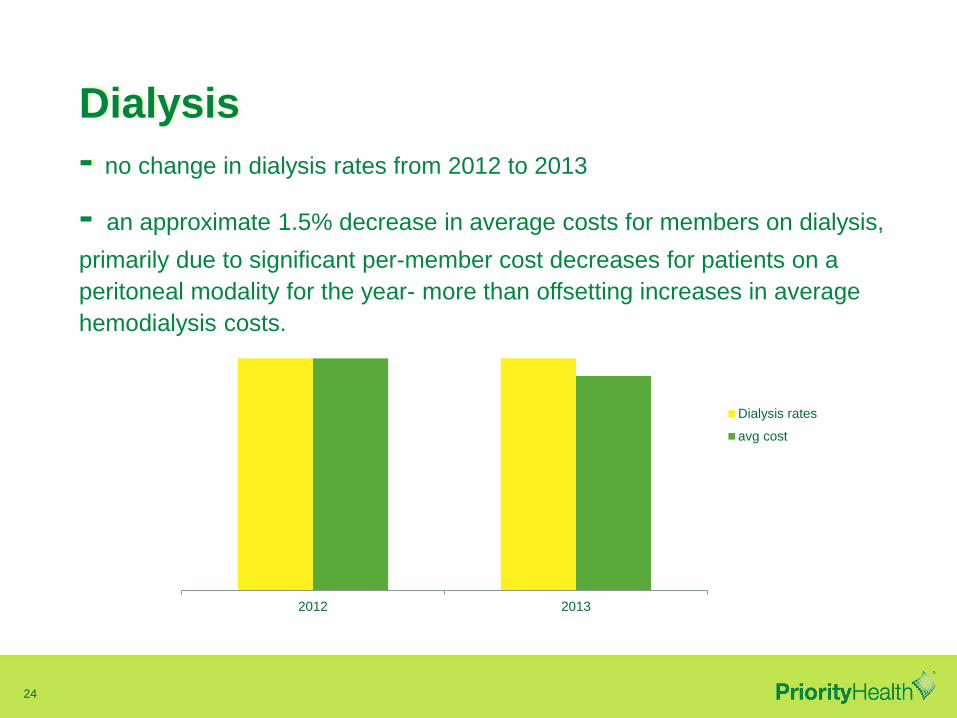
Dialysis
- no change in dialysis rates from 2012 to 2013
- an approximate 1.5% decrease in average costs for members on dialysis,
primarily due to significant per-member cost decreases for patients on a
peritoneal modality for the year- more than offsetting increases in average
hemodialysis costs.
2012 2013
Dialysis rates
avg cost

25
The Role of Care Management
Care Management Influences Patient Engagement:
More activated members have more positive and supportive
health care experiences.
• Successful navigation of the complex and confusing
health care system
• patients with chronic conditions get significant
support from their health care team
• patients experience fewer problems with access to needed
care

26
Population Segmentation Makes It Feasible to Measure and
Manage the Population Health Management Value Equation
How good is
our aim? Right members,
Right timing,
Right allocation
of effort
How well do
we connect? People, program
offerings, and
outreach that
inspire members
towards active
participation to
goal completion
How much
difference
does it
make? Effect of
intervention on
the intervened
How quickly do
we achieve
results? Progress rate,
time to successful
completion
$$$
Program Inputs (cost of
staff, other resources)
= ROI

27
Care Management is a pivotal component
of team based care
Team-based health care is the provision of health
services to individuals, families, and/or their
communities by at least two health providers who work
collaboratively with patients and their caregivers—to the
extent preferred by each patient—to accomplish shared
goals within and across settings to achieve coordinated,
high-quality care.

28
Additional Programmatic Interventions Via
Community Partnerships:
Diabetes prevention program, in partnership with the NKF of Michigan
•Building awareness of the importance of diabetes prevention.
•Free to our members!
•200 members enrolled
•A total of 1,904 pounds lost!
•An average activity level of 160 minutes/member/week!
The research and evaluation of studies on DPP reveal that for every 100
participants:
•15 cases of type 2 DM are prevented.
•162 missed work days are avoided.
•11 patients will not require lipid lowering rx.
•Avoid $91,400 in (avoidable) healthcare costs.
•Adds the equivalent of 20 years of perfect health!
29
Interventions
Partnership with Davita
•Individual Counseling
•Group Classes
•Kidney Smart Program
THRIVE (Personal Action Toward Health)

30
Interventions
Clinical Decision Support Tools
EMMI – Communication solutions that empower patients to take action
around a healthcare event or condition.
Patient Empowerment
EMMI has an entire suite of programs dedicated to educating people about
renal related conditions and circumstances.

31
Guiding Principles
• Patient Centered
• Integrated, holistic model
• Multidisciplinary approach to
patient care
• Partnership with providers
• Adherence to evidence based
standards of practice
• Engaged patient with input into
clinical decision support
• Promotes safe, timely care

32
Alone we can do so little; together we can do so much
-Helen Keller