wernicke's encephalopathy in a young girl suffering from acute
TRANSCRIPT

574 Letters to Editor
Published by: Tehran University of Medical Sciences (http://ijp.tums.ac.ir)
Wernicke's Encephalopathy in a Young Girl
Suffering from Acute Myeloblastic Leukemia
Askar Ghorbani1, MD; Farzad Fatehi*1, MD;Akbar Soltanzadeh1, MD; Amirali Hamidieh2, MD
and Zahra Vahabi1, MD
1. Iranian Center of Neurological Research, TehranUniversity of Medical Sciences, Tehran, Iran2. Hematology-Oncology and Stem Cell TransplantationResearch Center, Shariati Hospital, Tehran University ofMedical Sciences, Tehran, IranReceived: Jun 02, 2011; Accepted: Apr 01, 2012
Wernicke's encephalopathy (WE) is a potentiallyfatal, neuropsychiatric syndrome and absolutelya neurological emergency caused mostcommonly by thiamine deficiency[1]. It isrecognized by the constellation of symptomsincluding ataxia, confusional state, and diplopia.The disorder is still significantly missed, leadingto death or to the chronic form of theencephalopathy recognized as Korsakoff'ssyndrome[2]. Herein, we describe the disease in agirl who suffered from acute myeloblasticleukemia (AML).A 12-year-old female, known case of AML M4was consulted due to mild confusion, diplopia,and ataxia. Her disease had started 6 monthsprior to admission. She had received bonemarrow transplantation from her brother 40days before. On neurological examination, shewas mildly confused with right sixth nerve palsyand truncal ataxia; also, she demonstrated gaitataxia and impaired finger to nose testprominently on the right side. For the betterevaluation, brain MRI was recommended. On T2weighted axial brain MRI (Fig. 1, parts A and B),hyperintense lesions in middle cerebellarpeduncles, and similar intensities in the tectumand tegmentum of midbrain on the left side weredetected; furthermore, on brain T1 weightedMRI with contrast (Fig. 1, part C), severelyintense enhancement in mammillary bodies wasseen; on the other hand, diffusion weight brainMRI revealed hyperintense lesions in the medialportions of thalami (Fig. 1, part D).According to the clinical findings inconjunction with imaging studies, the diagnosis
of WE was made and thiamin was started. In thenext day visit, ocular palsy had resolvedcompletely.We believe that malnutrition stemming frompersistent loss of appetite as a result of thechemotherapeutic agents or the leukemia itselfmay have provoked thiamin deficiency and hadcaused WE.The clinical settings in which WE takes placeis growing; conspicuously, in conditions likealcohol consumption, prolonged feeding throughparenteral routes, hyperemesis gravidarum,AIDS, anorexia nervosa, thyrotoxicosis,malabsorption states, dialysis, malignancy, andgastroplasty with postoperative vomiting[3].Previously, few authors have described theassociation of acute lymphoblastic leukemia(ALL) and Wernicke's encephalopathy[4-9];likewise, on the subject of AML, the reports arescarce, too[10,11]. Baek et al[10], described a case ofacute WE arising following allogeneic peripheralblood stem cell transplantation accompanyingwith prolonged administration of totalparenteral nutrition. Also, Pitella et al[11]reported a 30-year-old female suffering from WEassociated with promyelocytic leukemia whichwas detected at autopsy.In WE, characteristic radiologic findings onbrain MRI consist of symmetric signal changes inthe thalami, mamillary bodies, tectal plate, andperiaqueductal area[12]. Atypical MRI findingscomprise symmetric alterations of thecerebellum, vermis of cerebellum, cranial nervenuclei, red nuclei, dentate nuclei, caudate nuclei,splenium, and cerebral cortex[12].In conclusion, the possible occurrence ofWernicke’s encephalopathy should be regardedin young patients encountering confusion orother neurological deficits who are sufferingfrom malignancies especially when concurrentchemotherapy is administrated. It is significantthat clinical suspicion is of utmost importance inthe diagnosis and treatment of WE since delayeddiagnosis may potentially cause devastatingresults.Key words: Wernicke’s Encephalopathy; KorsakoffSyndrome; Transplantation; Acute MyeloblasticLeukemia
* Corresponding Author; Address: Shariati Hospital and IranianCenter of Neurological Research, Tehran University of MedicalSciences, Tehran, IranE-mail: [email protected]
Iran J Pediatr, Vol 22 (No 4); Dec 2012 575
Published by: Tehran University of Medical Sciences (http://ijp.tums.ac.ir)
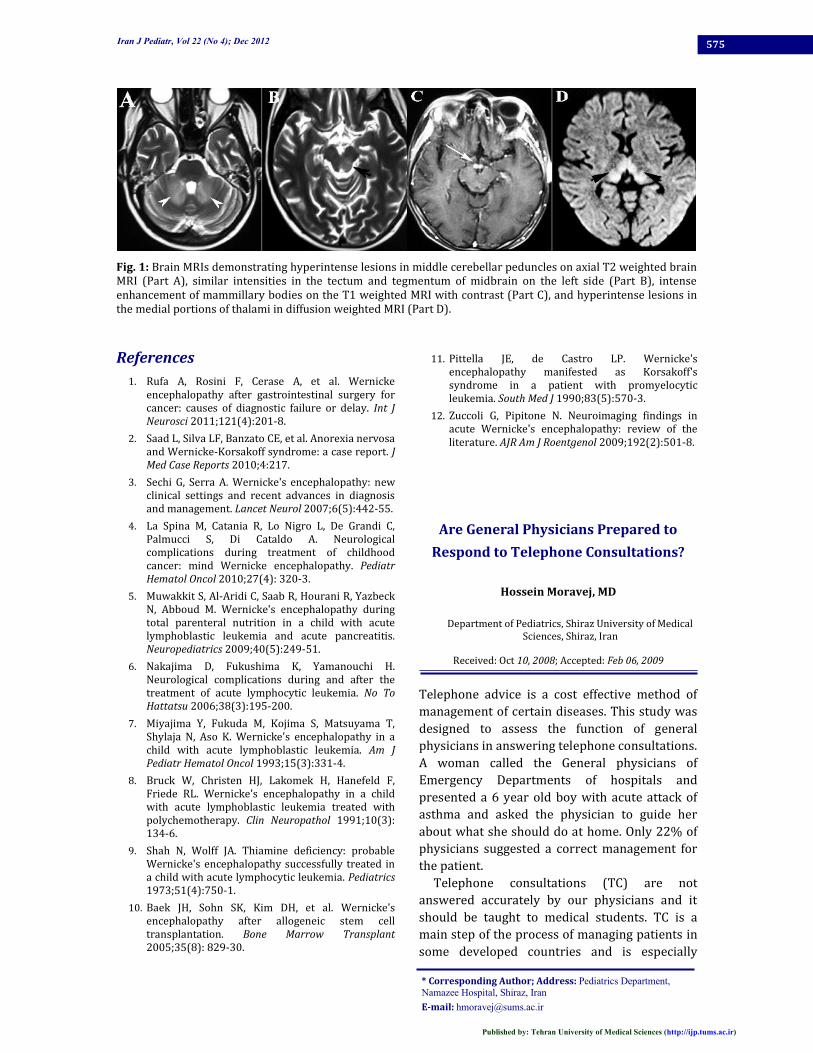
Fig. 1: Brain MRIs demonstrating hyperintense lesions in middle cerebellar peduncles on axial T2 weighted brainMRI (Part A), similar intensities in the tectum and tegmentum of midbrain on the left side (Part B), intenseenhancement of mammillary bodies on the T1 weighted MRI with contrast (Part C), and hyperintense lesions inthe medial portions of thalami in diffusion weighted MRI (Part D).References1. Rufa A, Rosini F, Cerase A, et al. Wernickeencephalopathy after gastrointestinal surgery forcancer: causes of diagnostic failure or delay. Int J
Neurosci 2011;121(4):201-8.2. Saad L, Silva LF, Banzato CE, et al. Anorexia nervosaand Wernicke-Korsakoff syndrome: a case report. JMed Case Reports 2010;4:217.3. Sechi G, Serra A. Wernicke's encephalopathy: newclinical settings and recent advances in diagnosisand management. Lancet Neurol 2007;6(5):442-55.4. La Spina M, Catania R, Lo Nigro L, De Grandi C,Palmucci S, Di Cataldo A. Neurologicalcomplications during treatment of childhoodcancer: mind Wernicke encephalopathy. PediatrHematol Oncol 2010;27(4): 320-3.5. Muwakkit S, Al-Aridi C, Saab R, Hourani R, YazbeckN, Abboud M. Wernicke's encephalopathy duringtotal parenteral nutrition in a child with acutelymphoblastic leukemia and acute pancreatitis.Neuropediatrics 2009;40(5):249-51.6. Nakajima D, Fukushima K, Yamanouchi H.Neurological complications during and after thetreatment of acute lymphocytic leukemia. No ToHattatsu 2006;38(3):195-200.7. Miyajima Y, Fukuda M, Kojima S, Matsuyama T,Shylaja N, Aso K. Wernicke's encephalopathy in achild with acute lymphoblastic leukemia. Am JPediatr Hematol Oncol 1993;15(3):331-4.8. Bruck W, Christen HJ, Lakomek H, Hanefeld F,Friede RL. Wernicke's encephalopathy in a childwith acute lymphoblastic leukemia treated withpolychemotherapy. Clin Neuropathol 1991;10(3):134-6.9. Shah N, Wolff JA. Thiamine deficiency: probableWernicke's encephalopathy successfully treated ina child with acute lymphocytic leukemia. Pediatrics1973;51(4):750-1.10. Baek JH, Sohn SK, Kim DH, et al. Wernicke'sencephalopathy after allogeneic stem celltransplantation. Bone Marrow Transplant2005;35(8): 829-30.
11. Pittella JE, de Castro LP. Wernicke'sencephalopathy manifested as Korsakoff'ssyndrome in a patient with promyelocyticleukemia. South Med J 1990;83(5):570-3.12. Zuccoli G, Pipitone N. Neuroimaging findings inacute Wernicke's encephalopathy: review of theliterature. AJR Am J Roentgenol 2009;192(2):501-8.
Are General Physicians Prepared to
Respond to Telephone Consultations?
Hossein Moravej, MD
Department of Pediatrics, Shiraz University of MedicalSciences, Shiraz, IranReceived: Oct 10, 2008; Accepted: Feb 06, 2009Telephone advice is a cost effective method ofmanagement of certain diseases. This study wasdesigned to assess the function of generalphysicians in answering telephone consultations.A woman called the General physicians ofEmergency Departments of hospitals andpresented a 6 year old boy with acute attack ofasthma and asked the physician to guide herabout what she should do at home. Only 22% ofphysicians suggested a correct management forthe patient.Telephone consultations (TC) are notanswered accurately by our physicians and itshould be taught to medical students. TC is amain step of the process of managing patients insome developed countries and is especially* Corresponding Author; Address: Pediatrics Department,Namazee Hospital, Shiraz, IranE-mail: [email protected]