wellbeing rural australia -...
TRANSCRIPT

Aboriginal and Torres Strait Islander readers are advised that this newsletter may contain images of people who have died.
Magazine of the National Rural Health Alliance Number 53 August 2015
Food insecurity in Australia
Critical success factors for the Primary Health Networks
Health reform - sense and nonsense!
13th National Rural Health Conference
GOODHEALTH
ANDWELLBEINGIN
RURALANDREMOTEAUSTRALIA

PHOTO: Julie STarkey Walking from the past into the present 2015 friends photo competition Winner

IN THIS ISSUE:
16 38
5 Editorial:Whose‘healthsystem’needsreform?
8 Primary Health Networks: criticalsuccessfactors
10 ProvidingCPDinmoreremoteareas:lessonsfromRHCE2
11 TheNDISinruralandremoteareas12 Healthreform—
Senseandnonsense!14 TheHealthDept’sFlexibleFunds16 StayingStrong
telehealthprogramtoexpand18 AustralianIndigenous
health services at NZruralhealthconference
20 Changestothepersonale-health record system
21 Elevenstepstobetterruralhealth24 ConferenceAwardwinners25 Beingwell–
artsandhealth@13NRHC28 TheNationalRuralWomen’s
CoalitionattheConference30 ReflectingontheConference31 FriendsoftheAlliance
attheConference31 Andthewinnersare…32 It’snolongerjustadreamto
flywiththeFlyingDoctor34 Overcomingaccessand
equityproblemsinruralprimarycareservices
36 Gettingtotheheartoftheproblem38 Don’tforgetyourmouthguard!40 20yearsofservicetotheprimary
healthcarecommunity41 Become a Friend42 FoodinsecurityinAustralia43 JimmyLittleFoundationseeks
supportforhealthyfoodprogram44 Studiestoinformservices
foradultswithautism45Websitededicatedtostroke
recoveryandsupport47 Onaverage,localactionisbest48 SupportingpregnantAboriginal
womentoquitsmoking50 Thecurrentchallengeof
ruralandregionaldata52 Summerresearch
scholarshipscheme54 Letter to the Editor:
OncologymassagetherapytraininginTamworth
54 2015FriendsPoetryCompetitionwinner:InmemoryofPhillipHughesbyAliStewart
52
5Partyline August 2015
Whose ‘health system’ needs reform?
O neoftenhearsreferencesto‘Australia’shealthsystem’.Cleverpeoplesaywedon’thaveahealthsystem.Becausethey’refragmented,includingby
jurisdictions,wehaveatleasteight.
Howevermanythereareandwhattheylooklikedependsentirelyonwho’slookingatthem.Thehealthsystem-anditsstatusorquality-isintheeyeofthebeholder.ConsidertheviewpointsofconsumersasdistinctfromthatoftheHealthServiceManagerintheirareaandtheDirectorGeneralofHealthintheirState.Apatient-centredsystemisonethatworksfortheconsumers;buthowhardisitfortheothertwotoreconstructtheirperceptionsofthesystemtomakeitpatient-centred?
THe CoNsuMeRs’ HeAlTH sysTeM
DanandMargaretWard#liveonapropertyincentralQueenslandwiththeirtwochildrenCharlie,seven,andRuth,three.AroundthekitchentabletheWardsdon’tdiscussthestateofthelocalorQueenslandhealthsystem.Whattheydodiscussisthestormwhichpassedthembyyesterday,thestateofthefeedontheproperty,andCharlie’sreportsofthebustriptoandfromschool.
WhenthekidsareinbedMargaretdoessometimesthinkaboutissuesrelatingtothehealthofherfamily.Theyhaven’tbeentothedoctorsinceCharliebrokeaboneinhisankleabout18monthsago.Shehasheardonthegrapevinethatthedoctorintownwithwhomshehasagoodrelationshiphasretiredorleft(hedeliveredRuthie).Ifthat’sthecase,what’sthenewdoctorlike?SheandDanaretryingforathirdchildandshe’sworriedaboutwhereshewillbeabletogivebirthandwhowilllookafterher.
WhenDan’sonhisbikemusteringorwhenhe’sfencingheoccasionallywonderswhatwouldhappenifhehadaseriousaccidentoraheartattack.HeknowsoftimeswhenpeoplelikehimhavehademergencyevacuationfromtheirpropertytoRockyorBrisbane,buthehasnoideawhatisentailed:whohiswifewouldcall,howmuchitwouldcostorwhowouldpay,whowouldcheckthestockifhewasinhospital.
EDITORIAL
THe HeAlTH seRviCe MANAgeR’s HeAlTH sysTeM
Anne#hasbeenHealthServiceManagerfornearly10yearsandhasworkedatthehospitalfor25.InthattimeshehasseennearlyadozendifferentiterationsofStateHealth,withlargeandsmalladminareascomingandgoing,andboundarieschanging.
Itwasquiteablowwhen,threeyearsago,thehospitalmaternityservicesunithadtoclose.RockhamptonblamedBrisbane,andBrisbaneblamedCanberra.AllAnneknewwasthatthefacilitywasofficiallyclosedandthattherewasnobudgetitemfordeliveriesorperinatalcare.Asaresult,thelong-servinglocalGPhadcalleditadayandretiredtotheSunshineCoast.HispracticehadbeenboughtbyanewGPwhosesurgeryopensjustfourdaysaweek.
Therewasnoconsultationaboutthematernityunit-presumablybecauseBrisbaneandtheMinisterdidn’twantabattlewiththelocalcommunity.EvenifBrisbanehadn’tpulledtheplugitwouldhavebeendifficulttocontinue:theyhadfoundithardtogetstaff-notjustmidwivesbutobstetriciansandanaesthetists.
Annehadspentyears trying toanswerquestions frompeoplewhowerewellknowntoher.“Whycan’twehaveanappendixoutherelikeweusedto?”“Whydoesmychildhave tobe sent away tohisbrokenarmset?” “Surely there’ssomeoneherewhocandoX-Rays?”
Anneiscontinuallyunderbudgetpressure,withlocumexpensesbitingdeeply.Thereisnobudgetforemergencytransport,despitethefactthatanumberoftripswillbeessential
People in town don’t understandwhymost acute patients are shipped out -especiallychildren,becauseof theguidelinesandprotocolsaround this.AndAnnehashadtocometogripswith‘bedclosures’and‘swingbeds’.
Makenomistake:Anne’shealthsystemishardwork.
…EDITORIAL
6 Partyline August 2015
THe DiReCToR-geNeRAl’s HeAlTH sysTeM
Clare# is Director General of Queensland Health. She wakes on MondaypreparingfortheweekaheadwithaplannedmeetingwithCommonwealthanddecisionsabouttheallocationoftheStatehealthbudgettogetthebestoutcomeforQueenslanders.Whereshouldtheprioritiesgo?
Clare opens the newspaper. The headline is Women’s group demands homebirthing options for Brisbane women.Hmmm:theMinisterandIaregoingtohavetorespondtothis.ButI’mworriedtherearesomewomeninruralandremoteQueenslandwhohavenochoiceatall,notonlynohomebirthingoptions:theyhavetotravelweeksbeforethedeliverytogivebirthawayfromfamilyandhometomakesurethey’resafe-pitythat’snotonthefrontpage.
ThinkingaboutStatehealthpriorities:arewegoing toputmore intoelectivesurgery?OurwaitingtimesareprettygoodbutthemediaandMinisterfindthisoneverypopular.ButAboriginalhealthcontinuestobeourbiggesthealthchallenge.HowdoIconvincethegovernmenttoputmostoftheirgrowthintopreventivehealthprogramsinpartnershipwiththeAboriginalcommunity?
We’reseeingtheCommonwealthfolksonWednesday.HowcanweworkmorecloselywiththemtogathertheevidenceforidentifyinggapsandprioritiesinthehealthsystembetweenhospitalsandGPs?MaybeourfutureinvestmentshouldbetoimprovebothhospitalandGPservicestothebush.Wehavetelehealthalreadysupportingspecialistservices,whynotGPs?Notetoself:asktheCommonwealthagaintosharetheirMedicareandPBSdatasowecanplantogether.Seemsanobrainerbutstillhasn’thappened.
NowwheredidIputthatbuspass?
# not real names
7Partyline August 2015

8 Partyline August 2015
Primary health netWorks: critical success factors
I n April 2015 the CommonwealthHealth Minister announced the
establishmentof31newPrimaryHealthNetworks(PHNs)thatwill“reshapethedeliveryofprimaryhealthcareacrossthenation.”PHNsaretobefocussedon improving frontline services andensuring better integration betweenprimaryandacutecareservices.TheAustralianGovernmentsetPHNssixkeyprioritiesfortargetedwork:mentalhealth, Aboriginal and Torres StraitIslander health, population health,health workforce, eHealth and agedcare.
With a mandate to improve theefficiency,effectivenessandoutcomesoflocalhealthsystems,PHNshavethepotentialtomakeasignificantpositivedifference in health outcomes for allAustralians.
Lessonslearntfrompreviousnationalprimary care models in Australiahighlightwhat isneededforPHNstocreate true public value. For PHNsto be successful they will need toachieveanddemonstratemeaningfuland measurable outcomes. As DrFrank Jones has said, “PHNs mustbe held accountable to their localcommunities,workingincollaborationwith other regional stakeholders,to improve patient and communityhealthoutcomes”.TheMedicareLocalreview recommended that “toenablePHNstoperformeffectively,reportingrequirements and processes needtobeprunedandstreamlined,withamajorfocusonmeasurableoutcomes”.Theclearidentificationofprioritiesandachievablekeyperformanceindicatorswillbecritical.
ResouRces:
To deliver on their stated objectivesthePHNswillneedtherightresources,including good people, expertise,fundingandgovernmentsupport.Theoperating context of each PHN willdiffer depending on factors such aslocationandgeography,demography,socio-economic distribution, thespecific needs of identified groups,populationhealthfactorsandchangesovertime.
ThefundingforeachPHNmustreflectthecostsofaddressingtheseneeds,not just the number of people in agiven location.Thewidely held viewof key stakeholders in the sector,as evidenced through consultationsconductedbytheAustralianHealthcareand Hospitals Association and thePublicHealthAssociationofAustralia,is that “resourcing of PHNs will beproblematiciffundingisprovidedonapopulationbasis,ratherthanaccordingtoneed.”
Relationships: The success of PHNswill rest, to asignificant extent, on their ability toengage and collaborate with others.“Thekeytoprogressingandenhancingoutcomes through PHNs will be anability to work collaboratively, andin genuine partnership with otherlikeminded organisations and keystakeholders, todeliverbetterhealthoutcomes”, Dwayne Crombie hassaid. Particularly important will be
effectiveengagementwithIndigenouscommunitiesandstakeholders.
Reputation:In thewords of theMedicare LocalsReview, PHNs must create andcommunicate an engaging narrativethat “clearly articulates the valuepropositionforpatients,GPs,primaryhealthcareprovidersandthebroadercommunity”.
leveRs:PHNsrequirestructuralandresourcingleverstoensuretheyhaveacredibleplaceatthenegotiationtablewiththeirhealth sector peers. GovernmentsmustacttoprovideamandateacrossthesystemforPHNstoexecutetheirresponsibilities throughanalignmentof relevant legislation and structures- thusensuring that theyareable toplaytheirroleineffectingsystemlevelchange.
PHNscanlearnfromtheexperiencesof Divisions of General PracticesandMedicareLocalstobuildonpastsuccesses and avoid repeating pastmistakes.
Krister partelAustralian Healthcare and Hospitals Association
9Partyline August 2015

10 Partyline August 2015
Providing cPd in more remote areas: lessons from rhce2
F orthepastfiveyearstheNationalRural Health Alliance has been
managing Stream 2 of the RuralHealthContinuingEducationprogram(knownasRHCE2)for theAustralianGovernment. Under the program,grants have been provided on acompetitivebasistoenablegroupsandindividualsworkinginruralandremoteareastoaccessand,wherenecessary,develop some of the continuingprofessional development that is soimportantforhealthprofessionals.
Competition for the grants hasbeen intense. The 119 successfulapplications over six rounds havetended to be those characterised byinter-professional learning, by theirprovision of clear evidence of theneedfortrainingandoftheprospectsfor sustainability of the programdeveloped, and by being located inmoreremoteareas.
The Department of Health hasindicatedthatfundingforCPDthroughRHCE2willcease,withresponsibilityfor theworknowfallingtothePHNs.A small proportion of the remainingRHCE2fundsistobeusedtohelpthetransitionfromthenationalprogram.
TheAllianceisthereforeworkingwithregional and national organisationson a knowledge transfer activity: toorganise and distribute knowledgeand ensure its availability for future
users.Anadhocworkinggrouphasbeenestablished in each jurisdictiontoadviseonthecontent,locationandtimingofasmallnumberofroundtables.
The key agencies involved are thejurisdictions’ Departments of Health;the PHN(s) covering rural areas;the local health or hospital districts;the University Departments of RuralHealth, Rural Clinical Schools andRural Workforce Agencies; othersthat have been involved with theprovisionofCPDinruralareas;thosewho received a RHCE2 grant; andorganisations representing varioushealthprofessions,includingAboriginalHealthWorkers,nursesandmidwives,allied health professionals, anddoctors.
Theactivity inall statesneeds tobecompletedbytheendofOctober2015.MeetingshavealreadybeenscheduledforGeraldton,Broome,Perth,AdelaideandSydneyandthoseforotherstatesare currently being organised. It isplanned to videoconference someoftheirkeysessionstootherregionalandruralcentres.
Anyone interested in the provisionof CPD to rural health professionalscan keep in touch with thescheduled activities by contactingWendy Downs, RHCE2 Manager, on02-61623374,freecall1800987440 or email [email protected]
Wendy Downs National Rural Health Alliance
2

11Partyline August 2015
the ndis in rural and remote areas
T he National Disability InsuranceScheme(NDIS)hasbeenheralded
as a once-in-a-generation reformthatwill change theway disability issupportedinthiscountry.
Theroll-outoftheSchemeisunderwayin various parts of Australia. Thereare trialsites inTasmania forpeopleagedbetween15and24,andinSouthAustralia for children under 13. It isoperating for people under 65 in theAustralianCapitalTerritory,theBarwonregionofVictoria,theBarklyregionoftheNorthernTerritory, thePerthHillsarea in Western Australia and theHunterregioninNewSouthWales.
The trial in the Barkly region almostcertainly provides the Scheme withthe greatest challenges, due to thescatteredpopulation,largedistances,and workforce and infrastructuredeficits.
The National Disability InsuranceAgency (NDIA) – the organisationresponsibleforimplementingtheNDIS– recognises that in some regionsit will be necessary to expand andstrengthen the market for disabilityservices.Thenotionofstrengtheningmarkets in many rural and remoteareasiscontentious,withsomepeoplequestioning its feasibility. They havechallengedtheNDIAonhowitwillbepossible to increase significantly thenumber of services in more remoteareas–forexampleforpersonalcare,respite care or specialised transportservices –when past efforts have sooftenfailed.
TheNationalRuralHealthAlliance isworkinginclosecollaborationwiththeNDIA to try to resolve this issueandothers that are critical to the success oftheNDISinruralandremoteareas.WhiletheNRHArecognisesthemanychallenges, it is keen to doanythingit can to ensure that people in ruraland remoteAustraliawho livewithadisabilityhavethebestpossiblecare,areengagedasmuchaspossiblewiththe local economy and community,andbythesemeanscanoptimisetheirlifestyleandchoices.
anne-marie Boxall National Rural Health Alliance

12 Partyline August 2015
W henever governments change,there is a risk that some
positiveandeffectivepolicieswill bediscontinued.
Thishappensonbothsidesofpoliticsand can occur for various reasons,such as political dogma, budgetaryconstraints,andalliancestomarginalelectorates.
OneofthechallengesforRuralDoctorsAssociation ofAustralia (RDAA) hasbeentoensurethatgoodpoliciesaremaintained.
Ithasbeenencouragingthat,despitethe recent change of government inQueensland, both the state’s LaborPartyandLiberal-NationalPartyhaveexpressed support for Queensland’ssuccessfulRuralGeneralistProgram,andthereintroductionofruralmaternityservicesthere.
WhiletherehavebeensomewelcomeannouncementsintheFederalsphere,otherpolicydecisionshavebeenmadewithnoregardforevidenceandinsteadappeartohavebeenbasedonshort-termbudgetaryimperatives.
The loss of the highly successfulPrevocational General PracticePlacements Program (PGPPP), animportantlinkinthechainofrecruitmentofyoungruraldoctors,isoneexample.
The Federal Government alsoappears tobedisregardingevidenceshowingthebenefitsofprimarycare,by continuing the freeze on MBSindexation and targeting generalpractice/primarycareforfundingcuts.
health reform — sense and nonsense!
Dennis Pashen
PHOTO: rDaa

13Partyline August 2015
When high quality primary care canbe provided efficiently via generalpractice,itmakesnosensetoreduceits attraction to new recruits norforcepatientsintothesecondaryandtertiaryhealthcaresectors.Onedayinhospitalforapatientcoststhenationconsiderablymore than any numberof visits to theGP— visits that canprevent the complications in chronicdisease that then lead to high costinterventionsinhospital.
Nor will overloading emergencydepartments with general practicepatientsassistthefiscalprudencethattheGovernmentistryingtoachieve.
WhiletheGovernmenthasbeenmakingsome savings in thePharmaceuticalBenefits Scheme, further substantialsavings could be made throughimplementingatenderingprocessformedications(asinNewZealand).
The $18.7 billion to be provided tothe pharmacy sector under the 6thCommunity PharmacyAgreement (a$3 billion increase on the previousagreement)seemstobeatoddswiththe Government’s desire to makehealth budget savings — includingthroughacutofat least$500millionfrom the Department of Health’sFlexible Funds program,which paysfornumeroushighly-effectiveruralandremotehealthinitiatives.
The medical profession must shareresponsibilityforleadinghealthreformin our sector. What can generalpractitioners do to make our sectormore responsive,moreeffectiveandabletodeliverbetterhealthoutcomesforpatients?
Firstly,theycanimprovecommunicationwith patients and colleagues and
explainmore clearly the nature of aGP’smanagementofpatientcare.
Criticism is leveled at those generalpractices which base their businessmodelonpatientthroughput,referringthe difficult cases and managementto other sectors (such as hospitaloutpatientandemergencydepartmentsettings) rather than deliveringongoing,highqualitycarewherethatispossibleandappropriate.
To absolve oneself of responsibilityfor apatient’s care in suchaway isneitherprofessionalnorappropriate.Itisalsodisrespectfulofourprofessionalcolleagues and our patients, whodeservebetter.
TheAustralianGovernmenthasmadesomewelcomeprogressinrecognisingandrewardingqualitygeneralpractice.
It has taken the profession’s adviceand returned the administration ofafter-hoursincentivepaymentstothePracticeIncentivesProgram.
It has also restructured theGeneralPractice Rural Incentives Program(GPRIP)toprovideincentivestomoredoctors towork in rural, remoteanddifficultpracticesettings,byadoptingthe Modified Monash Model (MMM)classificationsystem.
Thesedecisionsareawelcomestartandgiveushopethatgoodpolicyandgoodsensewillprevail.
You can email Dennis Pashen [email protected].
Dennis pashenPresident, Rural Doctors Association of Australia
FRIEND
CONTRIBUTED BY A

14 Partyline August 2015
S enate Estimates Committeehearingswith theDepartmentof
Health inearlyJuneconfirmedsomeof the details of the Government’splanned savings from the Portfolio’sFlexibleFunds.
Inthe2014Budget,cutsof$197mwereforeshadowedover threeyears.Thatamountistocomefrom‘theindexationpause’(presumablyasavingoftwopercentayear).
Thisyear’sBudget(May2015)addedanother$596moverfouryearstothatsavingstarget.Thisisa2.8percentperannumreductionwhich,compoundedoverfouryears,“comestoaboutsevenpercentoverall”.
FuNDs FoR FRoNTliNe seRviCes
The 14 Funds affected providesupport forawidevarietyof frontlineservices, including many directingcare to people in rural and remoteAustralia.TheseincludethoseworkingtoClose theGap inhealthoutcomesforIndigenousAustralians,responsestocommunicablediseases,deliveringsubstanceusetreatmentservices,andvariousruralhealthscholarships.
The National Rural Health Allianceis part of a coalition of peaknon-governmentorganisationsfromthehealthandcommunitysectorscallingon the Government for informationabout how specific decisions onsavingswithintheFundswillbemade.More information is expected soonfromtheDepartmentofHealth.
Two areas of particular concern arealcoholandotherdrugservices,andservicesmade available through thePHNs. The National Ice Taskforcehas recognised that the use ofmethamphetamines is particularlyserious in rural and regionalcommunities.Thatmustbeacaseforadditionalsupportforprogramsinthatareaofneed.
As for the PHNs, a great deal isexpected of them. It would be asetback ifastreamof resources thateveryoneinthesectoragreesshouldflowthroughthemwastobereduced.
suPPoRT FoR PeAk oRgANisATioNs
One of the affected Flexible Fundsprovides support for peak bodies inthesector.Thismeansthat instating
flexible adj. pron. /fleksəb(ə)l/ 1. able to make changes or deal with a situation that is changing 2. able to bend or move easily

15Partyline August 2015
flexible adj. pron. /fleksəb(ə)l/ 1. able to make changes or deal with a situation that is changing 2. able to bend or move easily
their views about funding changesthose bodies may be perceived ashaving a conflict of interest, but thisshouldnot inhibit them indoing theirjob.Apart from anything else, thesepeakbodieshavethecapacityandtheresponsibilitytotrytoensurethatthedifferent perceptions of the nation’shealth system come together in theinterestofpatients,taxpayersandthenational interest (see theEditorial inthisissue,p.5).
Industry or professional bodiesprovide consumers and clinicianswith a collective voice, and keepgovernments, policymakers and thepublic informed about issues in aparticulararea(eg.ruralandremoteinthe caseof theNRHA)or in relationto a particular health condition (egcancer,mentalhealth).
The Government recognises theimportant role of national peak andadvisory bodies in the health sectorandhasjustintroducedanewHealthPeakandAdvisoryBodiesProgramme.Informationonhowtoapplyforfundingunder theprogramme isavailableonthe Department of Health’s TendersandGrantswebsite.
Applicationsforfundingcloseat2pm(Canberra time) on Wednesday 26August2015
national Rural health alliance
“As for the PHNs, a great deal is expected of them. It would be a setback if a stream of resources that everyone in the sector agrees should flow through them was to be reduced.”

16 Partyline August 2015
staying strong telehealth Program to exPand
F ollowing the success of itsStaying Strong telehealth pilot
project, community care providerintegratedliving hasbegun to rollouttelehealth services to 13 regions infourstates.
The $2.1 million Staying Strongtrial project, originally funded underthe NBN Enabled Telehealth PilotsProgram,addressedchronicdiseasemanagement in rural and remotecommunities. It trialled in-homeand hub-based monitoring of vitalsigns for olderAboriginal andTorresStrait Islander people (seePartyline #50, p20 for a report on the pilot). The pilot project helped to deliver anewmodelofcarethroughtelehealthmonitoring of vital health signs for136olderAboriginalandTorresStrait
IslandersinfourNBN-enabledsitesinNewSouthWalesandQueensland -Armidale,CoffsHarbour,ToowoombaandGoodna.
The service was delivered bothin-homeand through telehealthhubsat local Aboriginal medical centreswhichprovidea safeandwelcomingenvironment for older Indigenouscommunity members to learn aboutandusethetelehealthservice.
Theprojectmonitoredparticipantswithvaryingconditions,includinghighbloodpressure, type 2 diabetes and highbloodcholesterol,withintegratedliving registered nurses working withparticipants and theirGP to developindividualhealthandmonitoringplans.
UsingtheTunstallmyclinictelehealthsolution—including a touchscreen
PHOTO: inTegraTeDliving

17Partyline August 2015
tablet, Integrated Care Platform(ICP) monitoring software, andvital sign peripherals—participantsself-monitoredtheirvitalsigns.
HealthdataweretransmittedtotheICPtriagemanager patientmanagement
systemwhichprioritised readings forclinicaltriage.Ifareadingwasoutsidethemonitoringplanrange,ICPtriagemanager raised an alert, allowing anurse to coordinate the appropriateresponse, in consultation with theparticipant and their GP or healthservice.
The pilot project found that evenparticipantswithchronicandcomplexhealth conditions were both willingandabletomanagethesimultaneousmonitoringoftheirmultipleconditionsthrough theuseof telehealth.Ninetyeightpercentofparticipantsreportedthey had enjoyed being part of theproject.
The cost for remote telehealthmonitoring for five days a weekwas $137.52 per participant. This issignificantly less than the estimated$347.82 it would usually cost fora registered nurse to travel to aparticipant’shomeforface-to-facevitalhealthsignmonitoring.
integratedlivingCEOCatherineDaleysaid, “the pilot has shown telehealth
can be useful in reducing the costburdenofhealthcare.”
“More importantly, Staying Strongfacil itated the development ofstrong and effective partnershipswith Aboriginal organisations and
communities, which was vital notonly to the successful attainment ofthe project objectives, but also forenhancingopportunitiestocontinuetosupportolderAboriginalpeople.”
Tunstall’s Corporate DevelopmentManager Lisa Capamagian said thesuccessofthetrialprovidesevidencethattelehealthshouldbeconsideredinnewmodelsofcarethatwillleadtothemainstreamingoftelehealthforaged,communityandsocialcare.
“integratedlivinghasnowbeenabletorolloutmainstreamtelehealthnursingservices on a bigger scale, covering13regionsacrossNewSouthWales,Queensland,theACTandTasmania,”MsCapamagiansaid.
ThefullStayingStrongprojectreportisavailableat integratedliving.org.au/article/staying-strong-pilot-project-reports-2505.html.
Kirsty JacksonTunstall Healthcare
“…even participants with chronic and complex health conditions were both willing and able to manage the simultaneous monitoring of their multiple conditions through the use of telehealth.”
FRIENDCONTRIBUTED BY A

18 Partyline August 2015
australian indigenous health services at nZ rural health conference
I am the Senior WorkforceDevelopment Officer for the
Queensland Aboriginal and TorresStraitIslanderHealthCouncil.InMarch2015, thanks to the National RuralHealthAlliance, Iwasable to attendandparticipate in theClose to Home NationalRuralHealthConferenceheldinRotorua,NewZealand.
ThiswasmyfirsttriptoNewZealand.Ienjoyedeveryaspectoftheconference.TheopeningceremonybyMaorielderswasahighlightandagreatstarttoanexcellent meeting. The respect thattraditionalpeoplehadtowardsvisitorsattendingtheconferencewasamazingandthismadeusfeelveryspecialandwelcomed.
The conference was well structuredand flowed between various themesandconsideredgroupsfromallareas
of New Zealand, including ruralcommunities.Thisallowedmetogaininsight into the hard work and greatinitiatives that are being conductedthroughout the country. There weremany health and social similaritiesbetween the Indigenous populationsofNewZealandandAustraliaandalsomanyworkforcesimilarities, includingthe unfortunate workforce shortagesthat occur particularly in rural andremoteareas.
Iparticipatedinoneoftheconferencepanel sessions which discussedvarioushealthsystemissues,includingequitable and accessible healthcare, partnerships and workforce. Ihad a chance to discuss AustralianIndigenoushealthsystemsandpolicy,includingGovernmentcommitments.

19Partyline August 2015
Both New Zealand and AustraliahavespecificgovernmentIndigenouspopulation health services andprograms butAustralia also has theAboriginal Community ControlledHealthServiceSector (ACCHS).TheACCHSsectorsupportsvarioushealthpolicyprogramsand inparticular theAustralianGovernment’scommitmentto closing the life expectancygap between Indigenous andnon-Indigenouspopulations.
There are over 150 AboriginalCommunityControlledHealthServicesin Australia. They are based onself-determination and principles ofholistic culturally appropriate serviceprovision.Theyaredirectedbyboardsof key community representatives,and are supported by the NationalAboriginal Community Controlled
Health Organisation (NACCHO) inCanberra and by Aboriginal HealthCouncilsineverystateandterritory.
Closing The Gap is a commitmentby the Australian government andall major political parties to takeaction to address the gap in lifeexpectancy between Indigenous andnon-Indigenous populations throughthe formal signing of the statementof intent and supported by specifichealthfundingthroughtheCouncilofAustralianGovernments.Whileitisstillearlydays,thepolicyhasledtosomeimprovementsineducationandhealthoutcomes. Importantly it has createdcapacity towork inpartnershipswithIndigenous health organisations andcommunities.
Annually Aboriginal CommunityControlled Health services provideprimary health care to 310,000Indigenouspeopleandareaccreditedwiththreequartersofthehealthgainsmade towards the Closing the Gaptargets.
christopher eldridgeQueensland Aboriginal and Torres Strait Islander Health Council (QAIHC)
Chris Eldridge
PHOTO: CHriS elDriDge

20 Partyline August 2015
changes to the Personal e-health record system
P lans have been underway inAustralia for many years for an
electronic record that would providea summary of an individual’s healthhistoryand that canbeaccessedbyboththeindividualhim/herselfandthehealth professionals who come intocontactwiththem.
Such a system has the potential toimprove informationsharingbetweenhealth professionals involved in aperson’scare.Oneoftheresultswouldbe the more efficient use of healthresourcesandbetterhealthoutcomesthrough improved care coordination,especiallyinruralandremoteareas.
From2012until2015thesystemwasanopt-inarrangementwiththename‘Personally Controlled ElectronicHealth Record’ (PCEHR). TheAustralianGovernmenthasannouncedamajornewcommitmenttotheidea,withre-badging,asignificantchangeinitsoperation,andrevisedmanagement.
The Government will invest $485.1million over the next four years inwhatisnowtobeknownasMy Health Record - to better reflect the linkbetween individuals and healthcareproviders.Aftersometrials,thesystemmaywellbecomeanopt-outmodelinwhich individuals will be registeredautomatically for an eHealth recordunlesstheyexplicitlychooseotherwise.
TheNRHAhasproposed thata ruralor regional area be chosen as oneof the trial sites. The benefits of aneHealth record system are likely to be of particular value in rural and
remote health, where professionalsworkinresourcelimitedenvironmentsandoftenincollaborativeteams.It isthereforesensibleforthesystemtobetrialledwithpeopleoutside themajorcities.
The trials will be supported throughlocalised information campaigns;training for GPs, pharmacies andaged care services; and revisedGPincentives. The outcomes from thetrialswill inform future strategies forincreasing participation in the My Health Recordsystem.
The National Electronic HealthTransition Authority (NEHTA) isto be replaced with the AustralianCommission for eHealth (ACeH), asingleauthoritythatwillbeaccountablefor the governance of all eHealthactivities.Theaimof theACeH is tosimplify governance arrangementsandimprovestakeholderengagement.Itwill be governed by a skills-basedBoardandbeadvisedbyanewACeHJurisdictionalCommittee.
It is to be hoped that there will besubstantial rural/remote healthexpertiseon theACeHBoardand itsadvisory committees. This will helpensure that ‘the rural voice’ is heardloudandclearaseHealthprogramsatlastbecomesignificantastheymoveintothefuture.
Damien hickmanNational Rural Health Alliance

Lesley Fitzpatrick presenting the Priority Recommendations at the 13NRHC
PHOTO: glenn CamPbell
ElEvEn stEps to bEttEr rural hEalth
The 37 member bodies in theNational Rural Health Alliance
have considered the pr ior i tyrecommendations from the 13thNationalRuralHealthConference.Thishas resulted in11highprioritypolicyproposals on which theAlliance willseekaction.
TheAlliancenowseeksresponsesto,and action on, these proposals fromany entity that can progress them –governments or NGOs, consumersorclinicians, localornationalbodies.Weencourageotherorganisationsthatshare our determination to improvehealthandhealthservicesinruralandremoteareas,tosupporttheproposalsanddoanythingtheycantoadvancethem.(Refer to the Alliance websiteforthecompleteversionoftheelevenproposals.)
Despitegoodintentionsandprogressin some functional areas, the nation
has failed toensuregoodhealthandwellbeing for many of its Aboriginaland Torres Strait Islander peoples.Achieving health equality requiresconsideration of more than healthserviceplanninganddelivery; it alsorequiresworkonthesocialandculturaldeterminantsofhealthandwellbeingthatfalloutsidethehealthsector.
Existing health and health-relatedprograms and initiatives that canprove their effectiveness, and whichare led andmanaged by Indigenouspeople themselves, should receivesustainable and ongoing support. Inaddition,theAllianceseeksbipartisanpolitical commitment to resource theImplementationPlanwhichsitsunderthe National Aboriginal and TorresStraitIslanderHealthPlan.
Someof theapproaches to improvedIndigenoushealth–andsomuchmorebesides - will be facilitated when all
21Partyline August 2015

22 Partyline August 2015
communitiesinremoteandruralareashavefast,reliableandaffordabledigitalaccess.Itwillbeaboonforbusiness,schooling, professional training andrecreationalpurposes-aswellasforhealthservicessuchastelehealthandtelecare.
TheAlliancecallsontheDepartmentof Health to undertake a review oftelehealth/telecareinitiativestoidentifyways of extending and improvingservices delivered through suchmediums; and to provide ongoingresourcing for the development andapplication of telehealth/telecareprogramsinruralandremoteareas.
MuchisexpectedofthenewPrimaryHealth Networks (see the article onpage 8 of this issue). The Allianceproposes the establishment of across-portfolioWorkingGrouptoassistruralPHNsinfindingwaysofworkingcollaborativelyacrossprogramareasindisability,agedcare,acuteandprimarycare,preventivehealth,educationandIndigenousaffairs.
ItisshamefultherearemanypeopleinAustraliawhodonothaveconsistentaccess to sufficient, affordable andnutritious food. In some cases thisisrelatedto incomebut thematter iscompounded by physical isolation.TheAlliancecallsforaSenateInquirytoexplorehowthisentirelyavoidablesituationcanbeovercome.
For theNationalDisability InsuranceScheme(NDIS)tobeeffectiveinrural
andremoteareas, thereneeds tobea substantial increase in the supplyofserviceprovidersavailableinthoseareas.TheAlliance is pleased to beworking closely with the NationalDisability InsuranceAgency on ruralandremoteaspectsofthescheme.Ofparticularimportancearethemeansbywhichthemarketforcareprofessionalsinmoreremoteareasisstrengthened,andthewayinwhichexistingworkers- both formal and informal - areintegratedwiththeNDIS.
The Alliance intends to call on theCommonwealth Government todevelopanewNationalRuralHealthWorkforce Strategy. It would identifywaysofaddressinglongstandingruralhealthworkforcechallenges,includingrecruitment, retention and return,access to continuing professionaldevelopment(seethearticleonpage10),andeffectivemethodsofidentifyingstudentsandgraduatesmostsuitedtoworkinginruralandremoteareas,thetraining of health servicemanagers,and developing the Aboriginal andTorresStraitIslanderhealthworkforce.
Although the burden of disease isgenerally higher in rural and remoteareas,expenditureonhealthcaretendstobelower,includingbecausepeopleinthoseareasoftenhavelimitedaccesstoservices fundedbyMedicare.TheAlliance calls on theCommonwealthGovernmenttoexaminetheextenttowhichpeopleinruralandremoteareasaremissingoutonhealthfunding,and
…ElEvEn stEps to bEttEr rural hEalth

themeansbywhichthegapinratesofserviceaccesscanbenarrowed.
In view of the rising prevalence ofchildren with chronic illness andlearningdifficultieswhose conditionsrequire early identification andmanagement, the Alliance is callingforanational,standardisedscreeningprogramforboth three-yearoldsandforschool-readiness.
Ninety-four per cent of vision loss inAboriginalcommunitiesispreventableor treatable. Governments shouldjointly fund an integrated strategytoClose theGap forVision. Itwouldinclude increased funding for visitingoptometryandophthalmologyservicesin areas of need, and a subsidisedspectacleschemeforruralandremoteareasandAboriginalandTorresStraitIslandercommunities.
As part of its commitment to itsinternational region,Australia shouldprovidesufficient,appropriatefundingand technical support to strengthenhealth systems in the region in theface of hazards such as naturaldisasters, compromised safety andsecurity of food and water, and thewidespread anticipated detrimentaleffects of climate change. Australiashouldalsoworkwithotherstodevelopa multinational plan to prevent andeliminate the infectious diseases ofgreatest burden regionally, includingmalaria,TBandleprosy.
Giventhehighburdenofmentalillness(includingsuicide)inruralandremoteareasandtheshortageofspecialisedmentalhealthworkersinthoseareas,theAlliancecallsontheCommonwealth
Government to injectmore flexibilityinto funding streams and servicemodels for rural and remote mentalhealth,enablinglocalisedsolutionsforlocalneedsandcontexts.
Action on these eleven fronts willcontribute substantially to betterhealthandwellbeingforthepeopleofruralandremoteAustraliaandprovidethemwithbetteraccesstohighquality,affordable,safeandwell-coordinatedhealthcare.
Gordon GregoryNational Rural Health Alliance
23Partyline August 2015
pRincipal sponsoR
THANK YOU from the 13NRHC
chieF paRtneR

24 Partyline August 2015
ConfErEnCE award winnErsunsung hero awards 2015
TheUnsungHeroAwards recognisethe work of special individuals whomake significant contributions to thehealth and wellbeing of Indigenous,remote,orsmallruralcommunities.
2015 Des Murray scholarhips
DesMurrayScholarshipsareawardedeverysecondyeartoenableayoungpersonfromamoreremoteareawhois committed to improving thehealthstatus of people in his/her region toattendtheConference.
PHOTOS: glenn CamPbell
2015 Des Murray Scholarship recipients, Erin Morrison of Kangaroo Island SA and
Russell Lamb of Woomargama NSW.
Unsung Hero Award winners Francis Hayes (l) and Ruby Stanley (r) of Katherine NT, with
Pauline Glover, Chair of Friends of the Alliance.
25Partyline August 2015
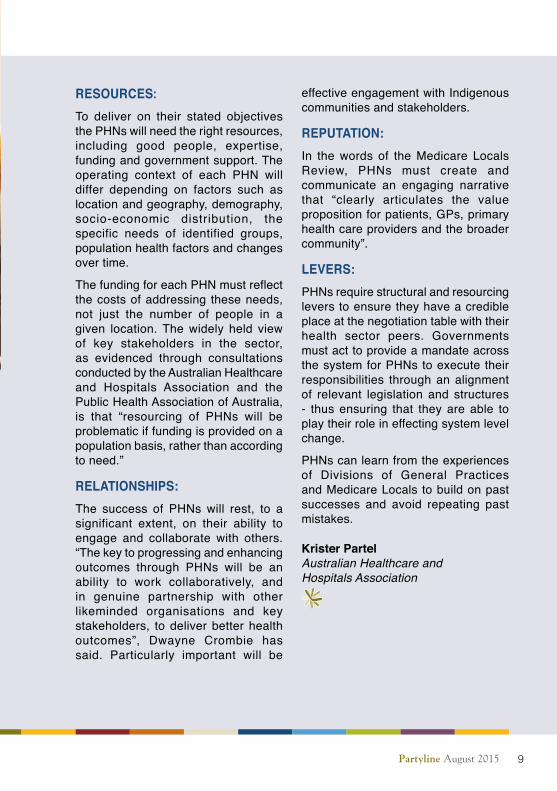
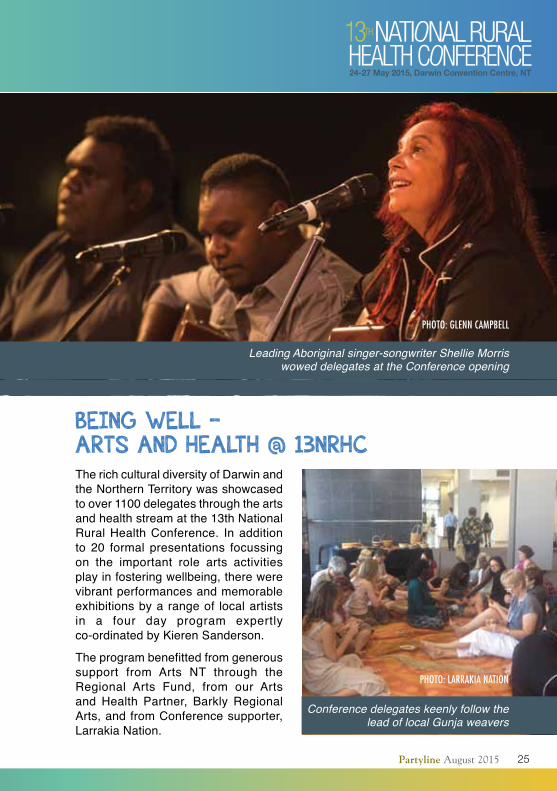
bEing wEll – arts and hEalth @ 13nrhC TherichculturaldiversityofDarwinandtheNorthernTerritorywasshowcasedtoover1100delegatesthroughtheartsandhealthstreamatthe13thNationalRuralHealthConference. Inadditionto 20 formal presentations focussingon the important role arts activitiesplayinfosteringwellbeing,therewerevibrantperformancesandmemorableexhibitionsbyarangeof localartistsin a four day program expertlyco-ordinatedbyKierenSanderson.
Theprogrambenefittedfromgeneroussupport from Arts NT through theRegional Arts Fund, from our Artsand Health Partner, Barkly RegionalArts,andfromConferencesupporter,LarrakiaNation.
PHOTO: larrakia naTiOn
PHOTO: glenn CamPbell
Leading Aboriginal singer-songwriter Shellie Morris wowed delegates at the Conference opening
Conference delegates keenly follow the lead of local Gunja weavers

26 Partyline August 2015
PHOTOS: glenn CamPbell
26 Partyline August 2015
bEing wEll – arts and hEalth @ 13nrhC
27Partyline August 2015
PHOTO: nrHa
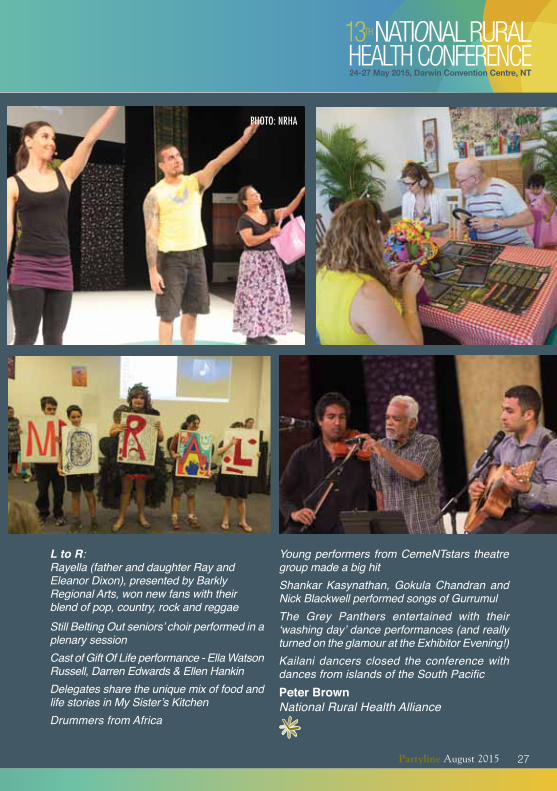
The Grey Panthers entertained with their ‘washing day’ dance performances (and really turned on the glamour at the Exhibitor Evening!)
Drummers from Africa
L to R: Rayella (father and daughter Ray and Eleanor Dixon), presented by Barkly Regional Arts, won new fans with their blend of pop, country, rock and reggaeStill Belting Out seniors’ choir performed in a plenary session
Shankar Kasynathan, Gokula Chandran and Nick Blackwell performed songs of Gurrumul
Cast of Gift Of Life performance - Ella Watson Russell, Darren Edwards & Ellen HankinDelegates share the unique mix of food and life stories in My Sister’s Kitchen
Kailani dancers closed the conference with dances from islands of the South Pacific
Young performers from CemeNTstars theatre group made a big hit
peter BrownNational Rural Health Alliance
27Partyline August 2015
28 Partyline August 2015
thE national rural womEn’s Coalition at thE national rural hEalth ConfErEnCE In2014, theNationalRuralWomen’sCoalition (NRWC) and the economicSecurity4Women (eS4W) alliancefacilitated roundtable discussionswith a range of rural and remotestakeholders and policy-makers toexaminehowwomenoftenshoulderadisproportionateburdenoftheeffectsofnaturaldisasters.
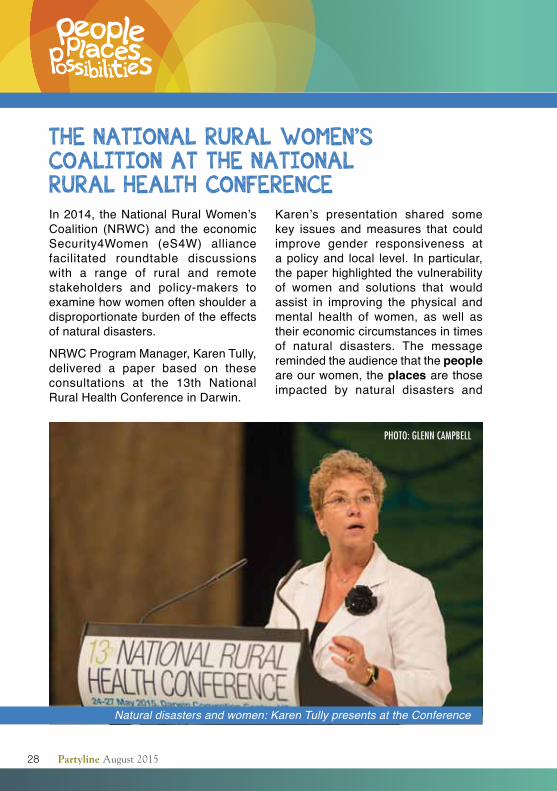
NRWCProgramManager,KarenTully,delivered a paper based on theseconsultations at the 13th NationalRuralHealthConferenceinDarwin.
Karen’s presentation shared somekey issues andmeasures that couldimprove gender responsiveness atapolicyand local level. Inparticular,thepaperhighlightedthevulnerabilityof women and solutions that wouldassist in improving the physical andmental health of women, as well astheireconomiccircumstancesintimesof natural disasters. The messageremindedtheaudiencethatthe people areourwomen,theplaces are those impacted by natural disasters and
PHOTO: glenn CamPbell
Natural disasters and women: Karen Tully presents at the Conference

the possibilities for addressing thegenderedimpactsofnaturaldisastersonwomenarenumerous.
TheNRWC congratulates theNRHAConference Committee on such awell-organised conference and forgivingourorganisationtheopportunityto share its research with a wider audience.
health anD Wellness RounDtaBleInMarch 2015, theNRWChosted aHealth and Wellness Roundtable inAdelaide to bring together a diversegroup of informed rural women fromallpartsofAustraliatoexaminewhatsupportcanbeprovided to ruralandremotewomenwhoexperiencefamilyviolence.The21womenrepresentedmember organisations of NRWC,includingChairofFriendsoftheNRHA,PaulineGlover.
The NRWC recognises that onein three Australian women haveexperiencedphysicalviolence.Almostone in five have experienced sexualviolence. It is time for that tochangefor all women, including those wholiverurallyandremotely.Womenwereaskedtosharetheirexperiencesandmakerecommendationson:• howtosupportthewellbeingofruralandremotewomenwhoexperiencefamilyviolence;
• theroleofprimarycareinsupportingwomen experiencing familyviolence;
• the barriers faced by rural andremotewomeninaccessingfamilyviolencesupport;
• the impact on rural and remotewomen when access to familyviolencesupport isnotaccessible;and
• howtheseimpactsandbarrierscanbeaddressed.
Itwasagreedthatthereisaneedfornationally consistent legislation andlegal and judicial system support,including a national police databaseforprotectionorders.
Rural, remote and regional womenwant to seeall levels of governmenthavingownershipofThe national plan to reduce violence against women and their children 2010-2022 and to beaccountablefordeliveryoftheplan.
The full report is on the NRWCwebsitewww.nrwc.com.au/projects/Roundtable.aspx
pat hamilton and irene MillsNational Rural Women’s Coalition
29Partyline August 2015
FRIENDCONTRIBUTED BY A

30 Partyline August 2015
rEflECting on thE 13th national rural hEalth ConfErEnCEThe 13th National Rural HealthConference in Darwin was certainlyoneofitsbestandtheNationalRuralHealthAllianceshouldbeproudofthisstand-out event on the rural healthcalendar.This event is not just another ruralconference as it carries with it acollective voice in the form of therecommendations andCommunique.Itprovidesaplacetolearnandshareexperience and enables delegatesto reflectonandcelebrate themanyachievementsacrossalldisciplines.Ourbusy rolesoftenafford little timefor reflection yet it is so important,particularlyasaunitedgroup.Itworkswelltoinvigoratethediscussionwhichat times suffers somepolicy fatigue:
perhaps a symptom of countlessreviewsinthepursuitofrealreform.Forme,fairnessandequitybecamearecurringthemethroughoutthefivedayevent.The drive and commitment oftheruralhealthsectoralwaysfeaturesstrongly here. It is a sector strivingtoward ensuring rural and remoteAustraliansreceivequalityhealthcareandonewhichisworkinghardtogethertoensurethatruralpatients’needsareprioritisedinpolicy.Congratulationstoallinvolved.
ayman shenoudaRoyal Australian College of General Practitioners National Rural Faculty
The RACGP National Rural Faculty team at the 13th National Rural Health Conference
raCgP naTiOnal rural FaCulTy

31Partyline August 2015
and thE winnErs arE…Sixty five organisations exhibited atthe13thConference inDarwin.Wearelookingforwardtoseeingthemagainatthe 14th Conference in 2017. CoralieCross,CredentialedDiabetesEducatorfromHealthyLiving inDarwin,won theExhibitionincentivecompetition.Ourthankstodelegateswhocompletedthe conference evaluation survey. Wehad a terrific response rate and theviewsreceivedwillhelp inourplanningofthe14thConference.ThewinneroftheEvaluationsurveycompetitionwasTraceyHeeps, Exercise ProgramCoordinator,TimboonandDistrictHealthcareService,PortCampbell,Victoria.The Conference Proceedings canbe found at www.ruralhealth.org.au/13nrhc.TheonlineProceedingsalsocontainabstracts,speakerbiographies,powerpoints,photosandfullpapers.WelookforwardtoseeingyouatthenextConference in 2017. In themeantime,keepintouch!Josie Dunham, National Rural Health Alliance
at thE ConfErEnCE The Friends advisory committee enjoyedabreakfastmeetingtoconcludemembers’ terms on the Committee.GordonGregory,CEOoftheAlliance,thankedmembers for their input andacknowledgedPaulineGlover,whohassteppeddownaftertwotermsasChairoftheCommittee.The Friendly networking session was anopportunity forFriends to networkwithothersworkingand living in ruralandremoteareasofAustralia.The Friends photo and poetry competitions celebratelifeinremoteand rural Australia. The entriescapturedsomeofthemagicoflifethere,and remindedusof thecreativityandresilience of the people of rural andremote areas.Thewinners, as votedbyConferencedelegates,were:
photographic competition1st Walking from the past into the present,byJulieStarkey,Wilmington,SA 2nd Billabong dreaming, by LindsayCupper,Mildura,VIC
poetry competition1st In memory of Phillip Hughes, byAli Stewart, Moonee Beach, NSW 2nd Suffer the country, by PatrickDaley,Curtin,ACT
Kellie sydlarczukNational Rural Health Alliance Coralie Cross accepts her prize as
winner of the Conference Exhibition incentive competition
PHOTO: glenn CamPbell
32 Partyline August 2015
it’s no longEr just a drEam to fly with thE flying doCtorEarlier this yearAnne-Marie Rojahnworked hands-on with the RFDS’Charlevi l le team while doingresearch for her Masters thesis.Born in Switzerland, growing up inNorway,andinrecentyearsstudyingmedicine inSwitzerland,Anne-Mariewill shortly be a trained doctor andiskeen to return toAustralia toworkfor the Royal Flying Doctor Service.Shewas interviewed recently by theRFDSonheradventures,studiesandaspirations.
RFDS: You originally heard of the Royal Flying Doctor Service through the Flying Doctors TV show many years ago. What was it about the show that caught your interest?
The Flying Doctors TV show airedinEurope in the90s.Mypassion foraviationwas theoriginal reason thatthe Flying Doctorscaughtmyattention.I was inspired by the way the show
portrayedtheRFDSandthepeopleoftheAustralian outback in a down-to-earthandlikeableway.Ireaduponthemedicineaftereachepisodeandlearntalotfromtheshow.TheRFDSbeingtotallydifferent frommyeveryday lifemadetheprogramsoenchanting.
RFDS: You came to Cairns to find out about the Flying Doctors. Describe that first trip to outback Australia and your experience with the RFDS.
My first encounter with the outbackwascaptivating.TheTVshowgavemeaninsightintoanaeromedicalserviceandIwascurioustofindoutabouttherealthing.
I visited theCairns andAliceSpringsbases and saw what a truly uniqueorganisation the RFDS is, howpassionatelythestaffgoabouttheirworkandtheimpacttheservicehasonpeoplewholiveandworkinremoteareas.Thisopenedupawholenewworld.
Ann-Marie Rojahn with the RFDS at Birdsville
PHOTOS: rOyal Flying DOCTOr ServiCe

33Partyline August 2015
RFDS: You described your recent trip to Australia as a 6th year Swiss medical student as “the best six weeks of my life”. Can you give us some insight into what you did over those six weeks?
Having already worked with RFDSinCharlevilleback in2013Ireturnedtodoresearch formyMasters thesisearly this year and worked full timeaspartofmyelectiveyear,attendedclinics,inter-hospitaltransfers,primaryresponsesandtookpartinemergencymedicinesimulations.Thegreatthingaboutworkingwith theRFDS is thatit gives you a unique opportunity togainexperienceinsubjectsnotwidelycovered in medical school such asremote practice and telemedicine. Itwasanincrediblybeneficialexperience,aswellasahugecontrasttoworkinginacityhospital.
RFDS: What did your thesis cover?
Mythesisdescribestheevolutionanduse of telemedicine by theRFDS inbringingpatientcaretopeopleinruraland remoteAustralia. Selected casestudiesfocusontelecommunicationinprimaryhealthcare,emergenciesandretrievals.Thisprojectenabledmetostudy and identify all aspects of theserviceandtomeetandworkwiththemostopenhearted,amazingpeopleallovertheoutback.
RFDS: Has this inspired you further about working in outback Australia?
Absolutely.I’dreallyliketoworkfortheRFDSoneday.TheyarethebestgroupofpeopleI’veworkedwith---ever!
RFDS: We look forward to staying in touch as you complete your medical exams at the end of this year, and then take the necessary steps to be accredited for your medical training and to be licensed in Australia.
Anne-Marie:IhopetobebackwiththeRFDSreallysoon.Imissthework,thestaffandpatients,thisbeautifulcountryand the sound of the Flying Doctoraircraft.
lana MitchellRoyal Flying Doctor Service
The RFDS was Chief Partner at the 13th National Rural Health Conference
Ann-Marie Rojahn
33Partyline August 2015
FRIENDCONTRIBUTED BY A

34 Partyline August 2015
ovErComing aCCEss and Equity problEms in primary CarE sErviCEs in rural and rEmotE australia
In 2010 the Centre of ResearchExcellence in Rural and RemotePrimary Health Care (CRERRPHC)wasestablishedundertheleadershipof Professor John Humphreys. Itspurpose was to undertake researchtobetterunderstandkeyaccessandequityissuesrelatingtotheprovisionof appropriate, effective and highqualityprimarycareservices in ruralandremotecommunitiesofAustralia.
TheworkoftheCentrehasadvancedour understanding of key issues,including:howtomeasurethecomplexconcept of access; the importanceofdifferent rural and remote contexts indevelopingfit-for-purposeprimarycareservice models; what is required toensureappropriatesustainableprimarycareservices;thenatureofabasketof‘core’primarycareservices ruralandremote residents should be able toexpect to access andhoweffectivelydifferent models deliver these coreservices;whatfactorsaffectanddriveprimarycareworkforce retention;andthe critical importance of communityparticipationandengagement.
PHOTO: millie Clery
Several policy lessons and optionshavebeenderivedfromtheresearch.
First,researchersneedaccesstothedata that governments and serviceproviderscollect.
Communityparticipation(especiallyforIndigenouscommunities)isessentialatallstagesoftheresearch:communitymembers are the arbiters of what isneededandwhatworks.
Measures of access need to takegreater account of health needs,patients’abilitiestoaccesscare,andtheavailabilityofappropriateprimarycareservices.
Defining and benchmarking ‘core’primarycareservices isessential formonitoring services and evaluatingnational policiesdesigned toprovideeffectiveandequitablehealthservicesandimprovedhealthoutcomes.
Thereisaneedtoidentifyandprovideeffective and sustainable primarycare service models that are fit-for-purpose for small rural and remotecommunities.Thisisbestachievedby

policymakersandfundersworkinginverycloseassociationwithlocalhealthprovidersandconsumers.
Evidence from detailed case studiesindicatesthatinvestmentinappropriateprimarycareservicesresultsinimprovedaccess to and utilisation of services,betterhealth literacy,andsignificantlyimprovedpopulationhealthoutcomesinruralandremotecommunities.
Researchcapacitybuildingprogramsshouldbetailoredtomeetthecontext,interests and needs of rural healthstakeholders.
The Australian Primary HealthCareResearch Inst i tute (APHCRI)is supported by the AustralianGovernment’sDepartmentofHealth’sPrimary Health Care Research,Evaluat ion and Development(PHCRED)Strategy.ThroughCentresof Research Excellence (CREs) andother mechanisms, APHCRI fundsresearchbasedonnational prioritiesthatinformspoliticians,policymakers,healthcareprovidersandconsumersabouthowprimaryhealthcarecanbeimprovedthroughpolicyandpractice.
lesley RussellAustralian Primary Health Care Research Institute, Australian National University
APHCRI was sponsor of the Sharing Shed Lounge at the 13th National Rural Health Conference
35Partyline August 2015
THANK YOU from the 13NRHC
arts and health sponsor
arts and health partner
conference sponsors
conference supporters
sharing shed lounge sponsor
conference Dinner sponsor

36 Partyline August 2015
getting to the heart of the Problem
O ne in four people living inrural areas is suffering from
cardiovascular disease (CVD)compared with one in five inmetropolitanareas.InAustralia,lowersocioeconomicgroups,AboriginalandTorresStraitIslanderpeopleandthoselivinginremoteareashavethehighestrate of hospitalisation and deathresulting fromCVD. IfCVD rates forthoselivinginruralareaswereidenticalto that of theirmetropolitan cousins,350,000feweradultswouldhaveCVD.
This higher rate of CVD is in partattributable to a higher prevalenceof associated lifestyle risk factors.People in ruralareasaremore likelyto smoke, be overweight and livesedentary lifestyles. There are anumber of reasons why this is thecase.Inruralareas,affordablehealthyfoodishardertocomebyandtherearefewersportingclubs,public transportoptions andenvironments conduciveto walking and cycling. There aregenerallylowerlevelsofhealthliteracy(meaning less capacity to obtain,process,andunderstandbasichealth
information and services needed tomake appropriate health decisions)and lower incomes (meaning lesscapacity to afford a visit to a healthprofessionalorfillaprescription).
TherearefewerGPsandalliedhealthprofessionals (such as dieticians,diabetes educators, physiotherapistsandspeechpathologists)who,alongwith nurses, play an important rolein the prevention, rehabilitation andongoingmanagementofCVD.Peopleinruralareasalsoencounterbarrierstoparticipatingincardiacrehabilitationprograms (such as the distance andtravelcoststoattendsuchprograms)-whichare important inreducing themorbidityandmortalityassociatedwithcardiovasculardisease,andreducingtheriskofrecurrentcardiacevents.
However,thegoodnewsisthatCVDislargelypreventable.So,whatcanyoudo?
Seeyourlocalhealthprofessionalforahearthealthcheck.Getyourbloodpressureandcholesterolcheckedandhaveachataboutyourrisk factors–

37Partyline August 2015
you can do this as part of a routinecheckup.Encourageyourfriendsandfamilytodothesame.VisittheNationalHealth Service Directory websiteto find a health service near you - www.nhsd.com.au
EducateyourselfabouthowtominimiseyourriskofacquiringCVDandmakechangeswherenecessary.Thereisamass of information, guidelines andsmartphone apps available online tohelpyou,whetherthatmeansquittingsmoking, getting physically active ormakinghealthierfoodchoices.Visitthehealthdirectwebsiteforalistofthese-www.healthdirect.gov.au
Work with your community to makepositivechanges.Rural communitiesarerenownedfortheirconnectednessandaresettingup initiativessuchaswalking groups and shared gardensfor growing fruit and vegetables. Inanother example, the Alliance has
been in contact with a group whodescribethemselvesas‘FatFarmers’,whohavecometogethertoloseweightandgethealthy.
Bothgovernmentandnon-governmentorganisationsoffera rangeofgrantsand funding opportunities to supportcommunity cardiovascular healthprograms. These may help with thepurchaseofsportinginfrastructureandequipment toencourageparticipationinphysicalactivityandsports,andinhealthpromotionactivitiesandhealthylifestyle programs (such as smokingcessationprograms).
Check out theAlliance’s Fact Sheeton Cardiovascular Disease at www.ruralhealth.org.au/factsheets
Dane MorlingNational Rural Health Alliance
Cardiovascular disease (CVD) describes all diseases and
conditions that affect the heart and blood vessels, including
heart attack, coronary heart disease, stroke and heart failure.
CVD is the leading cause of death and disability in Australia and
the world. It is estimated that one in six (3.72 million) Australians
have CVD and it kills one Australian every 12 minutes[1].
The good news is that heart disease is largely preventable.
There is no single cause of heart disease, but there are
risk factors that increase the chance of developing it. A
combination of risk factors contribute to the overall likelihood
of having a heart attack or stroke in the next five years - this
is known as the ‘absolute cardiovascular disease (CVD) risk’.
The more risk factors a person has, the higher their chance
of having a heart attack or stroke. Over 90 per cent of adult
Australians have at least one risk factor for CVD and 25 per
cent have three or more risk factors[1].
Some risk factors cannot be controlled, such as age, ethnic
background and family history of heart disease. Other
factors, however, are changeable. These include smoking,
high blood cholesterol, high blood pressure, diabetes,
physical inactivity, overweight, depression, social isolation
and lack of quality support. However, changing these risk
factors is not as simple as improving knowledge and skills.
It also requires access to affordable services and supportive
environments. This includes the availability of green space
and good walking/cycle paths to be physically active; access
to good quality affordable food for healthy eating; and access
to public transport to connect people to quality health
services, community networks and supports.
The disproportionate burden of CVD
in rural and remote Australia
Improvements in the treatment and experience of CVD
in recent years have not been equally distributed across
the population. The burden of CVD is felt more by lower
socioeconomic groups, Aboriginal and Torres Strait Islander
people, people from diverse cultural backgrounds, and
those living in rural and remote communities.
Australians living in rural and remote Australia experience
more CVD risk factors, higher rates of CVD-related
hospitalisation and are more likely to die of CVD than those
in metropolitan areas. The further a person lives from a
metropolitan centre, the greater their risk of hospitalisation
and death from cardiovascular disease[2].
If Australians living in rural and remote areas had the same
death rates as urban Australians, there would have been
3,632 fewer deaths due to coronary heart disease (16.5 per
cent fewer) in rural areas in 2009-2011[3].
The disproportionate burden of CVD experienced by
Aboriginal and Torres Strait Islander Peoples is further
exacerbated for those living in remote communities.
Aboriginal and Torres Strait Islander Peoples living in remote
Australia are twice as likely to report having heart and
...good health and wellbeing in rural and remote Australia
CARDIOVASCULAR DISEASE IN RURAL AUSTRALIA
One in four people living in regional and rural
areas is suffering from cardiovascular disease
compared with one in five metropolitan areas.
The further a person lives from a major city,
the higher their chance of being hospitalised
or dying from cardiovascular disease. These
differences are largely preventable. They stem
from unequal access to the conditions and
opportunities needed for good heart health.
FACT SHEET - MAY 2015
This Fact Sheet was produced in collaboration with the Heart Foundation. More information about the Heart Foundation can be found at http://www.heartfoundation.org.au
Source: AIHW Cardiovascular disease, diabetes and chronic kidney disease - Australian facts: Mortality
Cardiovascular disease death rates, by remoteness
and sex, 2009-2011[4]
MalesFemales
Deaths per 100,000 population
MAJOR CITIES INNER REGIONAL OUTER REGIONAL REMOTE AND VERY REMOTE
The Alliance’s Cardiovascular Disease Fact Sheet

38 Partyline August 2015
don’t forget your mouthguard!
A ustralians love their sport andbeingphysicallyactive.According
totheAustralianBureauofStatistics,over 60 per cent of Australians,wherevertheylive,participateinsport.
Inthisyear’sDentalHealthWeek(3-9August)Australianswhoplaysportorwork outwere encouraged to talk totheirdentist -as theiractionson thefieldorat thegymcouldbeaffectingtheiroralhealth.
The Australian Dental Association(ADA) asked all active Australianswhichofthesevensportingsinstheywerecommitting.
THe seveN siNs ARe:
Dental professionals have beenconcerned for some time aboutincreasing rates of dental problemsduetoparticularhabitsaroundplayingsportandbeingphysicallyactive.
Chair of the ADA’s Oral HealthCommittee,DrPeterAlldritt,saidthatmanyAustraliansareunawareof thedental health risks associated withplayingsportorotherphysicalactivity.“Youdon’thavetobeaneliteathletetobeatriskofmouthinjuryordentalerosionanddecay,”hesaid.
Each year thousands of adults andchildrenaretreatedfordentalinjuries
Sin 1:ALustforTaste- Areyouincreasingyourriskofdecay?
Sin 2:FuellingtheGreed- Areyoubeingpersuadedbymarketing?
Sin 3:TheWrathofTrauma- Wouldyouknowhowtodealwithdentaltrauma?
Sin 4:SupplementingVanity- Whatareyoureallytaking?
Sin 5:SportsGluttony- Howmanyacidattacksareyouhaving?
Sin 6:PerformanceEnvy- Isdehydrationgettingthebestofyou?
Sin 7:Slothfulavoidance- Whenwasyourlastcheckup?

that could have been preventedor minimised by simply wearing amouthguard.
DrAlldrittcontinued,“Whileawarenessofthebenefitsofwearingamouthguardisincreasing,especiallyinschoolsandatjuniorsportsclublevel,thereisstillaneed forgreateruptakeacross thecommunity”.
Schoolsandcommunitysportsclubsplay an important role in promotinggoodoralhealthonthesportingfield.
In conjunction with Sports MedicineAustralia (SMA ) the ADA hasdeveloped a Mouthguard Policy forsports clubs and schools to adopt.Theyareencouragedto implementastrict‘NoMouthguard,NoPlay’policy.
Schools and clubs in rural, regionaland remote areas of Australia candownload the policy from the ADA(www.ada.org.au) and SMA (www.sma.org.au)websites.
Tooth decay is the most prevalenthealth problem in Australia. Theconsumption of sugar-sweetenedbeveragessuchassportsdrinksandintra-workoutdrinksisespeciallyhighamongyoungadultsandadolescents,andisamajorcauseoftoothdecay.
DrAlldrittcontinued,“Sportsandintra-workoutdrinkscancauseirreversibledamagetoteeth—specifically,thehigh
acidity levels in these drinks erodetoothenamel,theglossyouterlayeroftheteeth”.
MostAustralianswhoareactivedonotneedtohaveheavilymarketedproductssuch as sports drinks, supplements,carbohydrate gels, and energy bars.These products are usually high insugarsandacidwhichcancausetoothdecayanderosion.
When it comes to keeping hydrated,tapwaterisjustasgoodand,inmostareas,hastheaddedbenefitoffluoridewhichwillhelpprotectyourteeth.
Being active is a great way ofmaintainingandimprovingyouroverallhealth,but it is important it doesnotcome at the expense of your oralhealth. The Dental Health Weekwebsite (www.dentalhealthweek.com.au) has a range of materialsto assist coaches, trainers, parents,teachers and health professionalstoeducate theirplayersabout reducingtheriskofpoororalhealth.
Bryan nguyenAustralian Dental Association
“You don’t have to be an elite athlete to be at risk of mouth injury or dental erosion and decay,”
39Partyline August 2015
40 Partyline August 2015
20 years of service to the Primary health care community
I nAugust 2015, thePrimaryHealthCare Research and Information
Service(PHCRIS)celebrates20yearsofservice.PHCRISworkswithpolicymakers,practitioners,researchersandconsumer advocates and generates,manages and shares research,information and knowledge aboutprimaryhealthcare.Thepurposeistoacceleratetheimpactofresearchandevidenceonhealthpolicyandpractice.
PHCRIS hosts the annual PHCResearchConference,themostrecentofwhichwasinJuly.Theconferenceis for those wishing to present
research findings, discuss researchmethodology and policy issues,and build and maintain networksbetween researchers, practitioners,policymakersand representativesofconsumerorganisations.
For more information go to www.phcris.org.au/
24th National Conference on Incontinencein association with the UroGynaecological Society of Australasia
Crown Conference Centre, Melbourne
25-28 November 2015
The latest in continence research and practice continence.org.au/national-conference
Registration OPENEarly bird closes
2 October

41Partyline August 2015
become a Friend
Now’s the time to join Friends oftheAlliance.Or, if youarealreadyamember, to re-join for the 2015-16financialyear.
Friends welcomesbothindividualandorganisationalmembers.Youcanjoinonline at www.ruralhealth.org.au/friends
FriendshelpstostrengthentheNationalRural Health Alliance’s advocacyaboutthehealthdivideexperiencedbyAustralia’scountrypeople.
It’s a network of people andorganisations that supports ourobjectives and provides theAlliancewith useful additional grassrootsconnections for its work in the
constantlychangingruralandremotehealthlandscape.Weneedregularandcurrentfeedbackfromyou.
As a Friendyouwillhaveopportunityto:• connect with other like-mindedcountrypeople;
• haveyourvoiceheardonthehealthneedsofyourcommunity;and
• sharepositivesolutions.
Help keep theAlliancewell-informedandstrong.Thankyou.
Kellie sydlarczukNational Rural Health Alliance
24th National Conference on Incontinencein association with the UroGynaecological Society of Australasia
Crown Conference Centre, Melbourne
25-28 November 2015
The latest in continence research and practice continence.org.au/national-conference
Registration OPENEarly bird closes
2 October

42 Partyline August 2015
food insecurity in australia
T his statement is included in theAustralianGovernment’sNational
Food Plan.Itisveryhardtodisagreewith.HowevertherealityisthatsomepeopleinAustraliadonotalwayshaveaccesstoenoughfood:theyexperiencewhatisknownasfoodinsecurity.
People in rural and remote areasand Indigenous people are moresusceptible than others to foodinsecurity.Thelatestnationalnutritionsurvey (conducted in 1995) foundthataboutaquarterofall Indigenouspeople experience food insecurity.Othergroupsthatareparticularlyproneinclude the unemployed, low-incomeearners, single parent households,refugees and people who misusealcoholandtobacco.
Price is one of the major factorscontributing to food insecurity.Surveyshaverepeatedlyshownthat,comparedwithmajor cities, the cost
of a collection of basic or essentialfoods is significantly higher in veryremoteareas, inpartbecauseof thehighfreightandstoragecosts.ArecentsurveyinWesternAustraliafoundthattheaveragecostoffruit,forexample,was32percenthigherinremoteareasofthestatethanitwasinmajorcities.The average cost of dairy productswas 40 per cent more. The surveyalsofoundthatthequalityofimportantfoodstuffs was much poorer in veryremoteareas.
In thepast,governmentshavemadesomeattempts to tackle the issueoffoodinsecurityinremoteAustralia.In2009, the House of RepresentativesAboriginal andTorres Strait IslanderAffairsCommitteeheldaninquiryintocommunitystoresinremoteAboriginalandTorresStraitIslandercommunities.LaterthatyeartheCouncilofAustralianGovernments (COAG) agreed on a
PHOTOS:Jimmy liTTle FOunDaTiOn
“In a country as wealthy as Australia, no one should be going hungry.”

NationalStrategyforFoodSecurityinRemote IndigenousCommunities.AspartofthisStrategy,COAGagreedtodevelop:• a national standards and qualityimprovement scheme for storesandtakeawaysthatserviceremoteIndigenouscommunities;
• a healthy eating action plan forremote Indigenous communities;and,
• aworkforceactionplantoimprovefoodsecurityinremoteIndigenouscommunities.
The efforts of past governments,however, have not been enough toaddress the problem.A 2014 reportfrom the Australian National AuditOfficeontheimpactofCOAG’s2009National Strategy for Food Securityfoundthatmanyoftheplannedactionshadnotbeencarriedoutand that its
impactontheproblemhadbeenlimited.Andtheproblemof food insecurity isnot restricted tocommunitystores inIndigenouscommunities.
Many people with an understandingand/or direct experience of life inmore remote communities continueto be concerned about the issue.Such concerns prompted delegatesat the 13th National Rural HealthConference to call on the Senate toestablishaninquiryintotheissue.TheAlliancewilladditsweighttothepushfor further government action on achallengewhichcanbeovercomeandwhich currently makes a significantcontribution to the poorer health ofpeopleinruralandremoteareas.
anne-marie BoxallNational Rural Health Alliance
Jimmy little foundation seeks suPPort for healthy food Program
The Jimmy Little Foundation hasbeen unsuccessful in gaining anyGovernment funding to continue theThumbs up! Healthy tucker for a long life program. Thumbs up! travelsto rural and remote communitiesaroundAustralia, usingmusic, videoand new media to education youngIndigenous Australians about thebenefitsofhealthyfoodandexerciseinthepreventionofchronicillness.Theprogramhasbeenrunningsuccessfullyforthelastsixyears.
Donationstosupportthecontinuationof Thumbs up! can be made tothe Jimmy Little Foundation via www.jlf.org.au
43Partyline August 2015

44 Partyline August 2015
landmark studies to inform services for adults With autism
T heCooperativeResearchCentrefor Living withAutism Spectrum
Disorders (AutismCRC)hasmadeasignificant investment in producingevidence-based, practical outcomesto assist adults on the spectrumacross Australia, including in ruraland regional areas. Never before inAustralia has there been a nationalresearch program dedicated toimprovingopportunitiesforpeopleonthe spectrum to participate in highereducation and employment, and toidentifyingbestpracticeinphysicalandmentalhealthmanagement.
To understand better the mentaland physical health, employment,community participation and overallwellbeing of adults on the spectrum,the Autism CRC has launched twolandmark longitudinal studies. Theresults of these studieswill be usedto inform services, guide policy anddeveloppracticaltoolstoassistadults
withautismtofindameaningfulplaceinsociety.
Thetransitionfromschooltoadultlifeforpeopleon thespectrumand theirfamilies is one of the most difficultperiods to traverse. Services arefragmented and poorly coordinated,andtheneedsofyoungadultsarenotwellunderstood.
Thefirststudyinvestigatesthetransitionfrom school into employment, furthertrainingorhighereducation.Thestudyaims to understand the process oftransitioning from school to adult lifeforAustralianstudentsdiagnosedwithautismandtheirfamilies.Weareinvitingyoungpeoplewithanautismspectrumconditionwhoareintheirfinalyearofschool,orfirstyearpostschool(aged15-25)andtheirparentsorguardians,toparticipateinthissurvey.
The second study is looking forparticipantswhoare25yearsorolderand their parents or care givers. Thesurveywilllookatmanyaspectsoflifeincludingmental and physical health,employment and other everydayoccupations,emotions,coping,memory,friendshipsandhealthserviceutilisation.
Onlyonepercentofall research intoautismhaspreviouslybeenfocusedonpost-schooloutcomesbutwith2,500to3,000school leavers inAustraliawithautism,itisanareawherethereismuchtolearnandmuchthatcanbedone.Inaddition,therehasneverbeensuchamulti-faceted, collaborative researcheffortfocusedonimprovingthephysicaland mental wellbeing of adults with

autism.Developinguseful health andwellbeing supports and protocolswillgive clear guidance to people withautism, their families and the healthprofessionalswhoassistthem.
Thesurveyscanbecompletedonlineorpaper-basedversionsareavailable.ThisensuresthatAutismCRCreceivesinformation from participants acrossAustralia, including rural and remoteareas. All communications can becarriedoutoveremailiftheparticipantpreferstonottalkonthephone.IfyouwouldlikefurtherinformationoneitherofthesestudiespleasevisittheAutismCRCwebsite:
www.autismcrc.com.au/school-leavers
www.autismcrc.com.au/adult-study
tess cosgroveAutism CRC
Website dedicated to stroke recovery and suPPort
The enableme online rehabilitationtool,setupbytheStrokeFoundationin partnershipwith the BUPAHealthFoundation, has been createdspecifically for theAustralian strokecommunity to give survivors, theirfamiliesandcarerschoiceandcontrolovertheirrecoveryjourney.
The website delivers personalisedinformation and tools to effectivelyenablesurvivorstocontinuerecoverymanyyearsaftertheirstroke.Itwillbeofvaluetopeopleinremoteandruralareasaswellasthemajorcities.
To find out more or to become partof the enableme community visit: www.enableme.org.au
45Partyline August 2015
Improving the management of remote health professionals who have
experienced a traumatic event
CRANAplus Bush support services together with the Centre for Remote Health are currently conducting a study aimed at improving the management of remote health professionals who have experienced a traumatic event.
The study will enable the development of best practice guidelines, education workshops, and materials.
iNviTATioN FoR ReMoTe HeAlTH prOfeSSIONAlS To Be iNTeRvieweDThe first part of the study is to gather information about what may have helped or what may have hindered you, as a remote health professional, in your recovery.
iNviTATioN FoR ReMoTe HeAlTH mANAgerS To Be iNTeRvieweDWe would also like to interview managers of remote health professionals about your experiences of managing staff who have experienced a traumatic event to identify factors such as support/constraints/resources that have influenced your management of the individual and the event.
we are also seeking feedback from health professionals and managers about what strategies you feel would improve the management of health professionals who have experienced a traumatic event.
The interviews will be conducted by a person experienced in trauma, but who is not part of the research team. All interviews will be confidential and only de-identified information will be published.
Research study
if you are willing to be interviewed for this study, please contact Sue lenthall email: [email protected] phone: 08 89514707
47Partyline August 2015
on average, local action is best
A greatdealofsignificancehasbeenattached to the Department ofHealth’sdecisiontoadopt theModifiedMonash Model as the remotenessclassificationsystemusedindistributingincentivesforruralgeneralpractice.
CertainlyitwillbegoodtoberidofsomeoftheanomaliesinherentintheASGC-RAsystem.ButitisusefultorecognisethattheadoptionoftheMMMisashiftfromoneveryblunttooltoanother.Thetimehas surely come for consideration ofsmarterwaysofusingdata inorder toincreasetheirvalueinthemanagementofhealthpoliciesandprograms.
Reporting on health status for broadgeographicareas suchasRAand theMMMleadstoanunderstandingoftheaverage conditions in large, disparateareas.Itistruethat,onaverage,health,incomes,education,serviceprovisionetcinOuterregionalareasareworsethaninMajorcities.ButweknowthatsomeareasinOuterRegionalAustraliaprovideverygoodlivingconditionsandhealth.
Given the capacity thatMPs have foreffective advocacy for change (or nochange)inpoliciesandprograms,it’sapitythathealthdataarenotmoreoftenreleasedbyelectorate.
Rather than basing analysis of healthissues on the averages in five RA orsevenMMMareas,therecouldbemorefocus on smaller areas, such as localauthorities,toidentifypocketsofparticularneed.Thiswouldenablefine-tuningandtargetingofspecificprograms toareaswiththegreatestneed.
CombiningthesetwoapproacheswouldseetheuseofRAorMMMlevelreportingto identify general issues, and smallerareaanalysestoidentifyandunderstandlocalneedsandpopulationgroupswithparticularproblems.
Iftheburdenofchronicconditionssuchasdiabetesorischaemicheartdiseaseishigherthanacceptable,itwilllikelybebecauseof thecharacteristicsofplaceand person.A detailed examination ofissuesonthegroundcanreliablyinformappropriateaction to transformaplaceanditscitizens’health.
Asocialdeterminantsapproachtohealthimprovementcouldworkinthisfashion.Ifaparticularlocalareahasacombinationofpoorenvironmentalconditions,limitedeconomic assets, and poor access topublicservices,anditspeoplehavelowlevelsofcompletededucationandhighlevelsofpersonalriskfactors, theyarelikelytobeinpoorhealth.
Clearevidenceabouttheseissuescouldbecomethetriggerforalocally-led,State-and Federally-supported project over5-10yearstotransformthelocality.Theprojectmightinclude:• analyses of the strengths,weaknesses,opportunitiesandthreatsinthecommunity;
• aplantostrengthenitseconomicbase;• a plan to enhance opportunities foryoungpeople;and
• programstoincreasephysicalactivity,help people quit smoking, improvediet,reducedrugandalcoholintake,and to strengthen social interactionandpositivecommunitysentiment.
Withsupportforsuchanapproachfromallthreelevelsofgovernment,localdatacanbethefirstpartofaprocessthroughwhichrelativelyimpoverishedareasandtheir citizens can be empowered. Onaverage,suchanapproachsurelymakesgoodsense?
andrew phillipsNational Rural Health Alliance

48 Partyline August 2015
neW online Portal to suPPort Pregnant aboriginal Women to quit smoking
T he Austra l ian IndigenousHealthInfoNet has joined forces
withCurtinUniversity, theAboriginalMaternityServicesSupportUnit,KingEdwardMemorialHospitalforWomen,andHealthwaytoproduceanewonlineportal for supporting the preventionof tobacco smokingamongpregnantAboriginalwomeninWesternAustralia.
Recentstudiesshowtobaccosmokingamong Aboriginal pregnant womenin WA is nearly four times higherthan for non-Indigenous womenand is responsible for higher risks ofhealth complications for women andtheir babies. The health risks due to
maternalsmoking includemiscarriage;ectopic pregnancy; preterm delivery;low birthweight; sudden infant deathsyndrome;andhigherriskofdeformityfor thebaby.The impactonAboriginalwomenandtheirbabiescanhavelongreachingnegativeconsequencesforlife.
Inruralandremotecommunities, thenormalisation of smoking has beeningrained for generations and thissmoking culture adversely affectsthehealthofAboriginalpeople-boththosewhosmokeandthosewhoareexposedtosecondhandsmoke.Thereis a variety of programs availablewhich address smoking prevention
Trish O’Hara and Jaime Read (HealthInfoNet), Roanna Lobo (Curtin University), Neil Drew (HealthInfoNet), Denese Griffin and Alexa Wilkins (AMSSU)
PHOTO: auSTralian inDigenOuS HealTHinfonet

49Partyline August 2015
and cessation in general, but it wasidentified that more is required tosupport the prevention of smokingamongpregnantAboriginalwomen.
Consequently, an online portal hasbeen created to provide improvedaccess to resources, information,training,andayarningplace(anonlineforum to encourage collaborationamong health workers). The portalis hosted on the well-establishedAustralian Indigenous HealthInfoNet web resource, making it readilyavailable for health professionalsworkinganywhereacrosstheState,inanysettingwithaccesstotheinternet.
Criticalselectionofcontentfortheportalensuresthattheinformationavailabletosupporthealthworkersandtobaccoprevention workers utilises themostculturallyappropriateandbestpracticemethods and strategies available forworkwithpregnantAboriginalwomen.Informationselectedforinclusionhasbeen carefully vetted in consultationwith a Project Reference Groupcomprisingmaternalandchildhealthandtobaccopreventionprofessionals,and through community and healthworkers’ feedback via a Statewidepre-evaluationsurvey.
Theportalallowshealthprofessionalsto access relevant resources quicklyand easily when planning smokingcessation interventions.Thisensuresthe best chance of success ofsupporting a pregnant woman whosmokes in her efforts to quit; beingpregnantshemaybemoremotivatedtomakepositivechangesthatimpactonherownhealthandthatofherbaby.
Whether smok ing cessat ionintervention takes place duringantenatalvisitsata localhospital,orduring visits by health professionalsin remote communities, the onlineinformationcollatedthroughtheportalwill be themost up-to-dateavailableforhealthprofessionalsinanysetting,anywhereacrossAustralia.
Ultimately,theportalwillcreateasolidknowledge base about Aboriginalmaternal smoking and establish thesiteasthe‘go-to’placeforinformation,resources, trainingopportunities andsupport for health professionalswhoworkwithpregnantAboriginalwomenandtheirfamilies,advancingAboriginalmaternalandchildhealthoutcomes.
Visit the Preventing Aboriginal maternal smoking Western Australia portal and theAustralian IndigenousHealthInfoNetwebresourceat:
www.healthinfonet.ecu.edu.au/population-groups/preventing-aboriginal-maternal-smoking
www.healthinfonet.ecu.edu.au/
Trish O’HaraAustralianIndigenous HealthInfoNet
“Recent studies show tobacco smoking among Aboriginal pregnant women in WA is nearly four times higher than for non-Indigenous women”
FRIENDCONTRIBUTED BY A
50 Partyline August 2015
rePurPose, reuse, and recycle: the current challenge of rural and regional data
C hronic illhealthhasemergedasthesinglemost importanthealth
issue inAustralia,particularly inruraland regional areas. In those areascommunitiestendtobeolderandmoresocioeconomically disadvantaged;havehigherproportionsofAboriginaland Torres Strait Islander people;have reducedaccess tohealth care;and typically have poorer healthbehaviours.However,foracommunitytotackletheseissueseffectively,thereis a need for more current, higherquality,andlocally-specificdata.
To understand chronic ill-health inour local region, the Hume healthregionofnortheastVictoria,areviewof peer-reviewed and grey literaturewas undertaken to identify researchpublications,governmentreportsandlocaldatathatexaminedtheextentandimpactofchronichealthconditions.
Despite being within 300 kilometresof Melbourne, the Northeast regionofVictoriaexperiencespoorerhealth,higher prevalence of many chronicconditionsandhighermortality ratesthanthestateaverage.
The review identified key chronicconditions in the region, includingdiabetes, chronic obstruct ivepulmonarydisease(COPD),ischaemicheartdisease,chronickidneydiseaseand lung cancer. The top threeavoidablecausesofdeathintheHumeregionasawholewereischaemicheartdisease, strokeand lungcancer;butwithinspecificlocalgovernmentareasthere were significant differences,for instance in relation to the extentof mortality from suicide, colorectalcancer,roadtrafficinjuryandCOPD.
Similarly, the top three reasons forhospitaladmissionsacrossthestateas
51Partyline August 2015
awholewerediabetescomplications,dental conditionsandpyelonephritis,whereas people across the Humeregionweremorelikelytobeadmittedtohospitalwithdiabetescomplications,irondeficiencyanaemiaandCOPD.
Thereviewalsohighlightedthatwhilechronicdiseasesarewellresearched,there was little evidence or datasystematically reporting on chronicillnessinspecificruralregions.
Additionally, rural-specific strategiesto manage these conditions and theinfluenceofruralsettingsandworkforceon chronic illness management wererarelydiscussed.Furthermore,therewasusuallyagapofuptotenyearsbetweendata collection and its use to informhealthpolicyandserviceplanning.
Most population studies of chronicillness involve largeurbancohortsoraggregated rural and remote healthdata. For example, data relating toa local government area is oftenaggregated to ensure adequatenumbers for statistical analysis, butkey local intricaciescanbelostuponaggregation.Specific informationcanbedifficulttocapture,andlocalhealthservicesmaythereforenotbeabletodeterminetheir‘unmetdemand’.
Soitremainsthecasethatup-to-date,local,ruraldataisofteninshortsupply.Good quality, local, contemporaryevidenceisessentialinhealthserviceplanning;yet,thisinformationanddataremain difficult to obtain, superficialand can be outdated. This meansthatoutdateddatacontinuestoinformcurrenthealthpolicyandhealthserviceplanning.
Chronicillhealthpresentsasignificantburden in remote, rural and regionalareas and is likely to continue tobe an increasingly important issueinto the future, as the populationages. Groups of people within ruralcommunities shoulder a greaterproportion of the burden, includingolderpeople, Indigenouspeopleandsocioeconomically disadvantagedgroups. Improvements in screeningrates,earlydetectionand reductionsin mortality for certain conditionshave often had less impact in ruralcommunities than in metropolitanareas.
Daniel terry, Kristen Glenister and lisa BourkeDepartment of Rural Health, The University of Melbourne

52 Partyline August 2015
summer scholarshiP scheme gives students a taste for country life, Work and research
Rural health research that informspractice,servicedeliveryandimprovedhealth outcomes has been a priorityfortheUniversityofSouthAustralia’sDepartmentofRuralHealth, (UDRH)since its inception. To ensure thiscontinues, students from health orhuman services disciplines have, fora numberof years, beenoffered theopportunity toundertake researchorproject work with UDRH academicsduring the summer vacation. Thescheme also seeks to encouragestudents to consider a rural careerfollowinggraduation.
Scholarships are offered on acompetitive basis. Students live andworkinWhyallaforatleastfourweeksfrom late November and/or frommid-January of the following year.TravelandaccommodationcostsaremetbytheUniversityandastipendof$375perweekisprovided.
Over the years projects have beenoffered in areas including chronicdisease self-management, mentalhealth, cardiovascular health, malehealth, health promotion, bonedensitometry and work health andsafety,tonamejustafew.
In 2014/15 projects included:developing a framework for trackinggraduate students; a review ofcomputerised therapy supports forpeople with cardiovascular disease;sourcingmaterials for amale healthpromotion event; developing healthpromotion materials for older men;
helping to develop a work, healthand safety management system fora localmen’s shed; several projectsin association with the local suicideprevention network; and producinga video to accompany a communityengagementprojectgrantapplication.
Students practised basic researchskillsincludingdatabasesearchingandretrieval,literaturereview,formulatingaresearchquestion,conductingneedsanalysis, designing surveys, grantwriting, quantitative data analysis,writing forpublication– including theopportunitytowriteahealthpromotionarticle for online publication by thelocalnewspaper–andreportwriting.Studentswereofferedmasterclassesin using bibliographic software,Microsoft Word, critical literatureappraisalandprogramevaluation–allskills that will serve studentswell inthefutureregardlessofwhether theypursueresearchcareers.
some reflections from this cohort were:
“The programwas both a rewardingand empower ing exper ienceand I appreciated the mixture oftheory and opportunity to applytheory in a practical setting.” Psychology student
“Theexperiencehasdefinitelyalteredmy understanding of research, andprovidedaninterestinhigherdegrees.” Nursing student

53Partyline August 2015
“The experience has opened upmycapacityforconnectionsandaffordedinput forpracticalskills thatcanonlybenefitmyacademicskillsinmydegree.” Laboratory Medicine student
“The scholarship program hasafforded me the ability to developtimemanagementskills,professionalnetworking, and have an insightfulopportunity to interact directlywith the Whyalla community.” Medical Sciences student
“My project enabled me to developconfidence in tasks such as callingmembersofthecommunity,organisingmytimeandmulti-tasking…theweeklyjournal club … developed my skillsin critically evaluating the qualityand content of research articlesand exposed me to articles I hadpreviously not encountered, bothin style and topic. This will proveinvaluable for my future studies…” Medical sciences student
“Thestipendwasmerelytheicingonthecake,asthelearningexperienceswhichwegottopractiseinourdegreewastherealprizewewalkedawaywith.” Social work student
Itisclearthatstudentsviewpositivelythesummerscholarshipsexperience.Theopportunitytoworkonrealprojectsin close communities under thesupervisionofexperiencedcliniciansand researchersprovidesa richnessofexperiencenotofferedthroughthetraditionalclinicalplacement.Wehopetohostmorestudentsinthefutureandthatasaconsequencesomeofthesestudentsconsiderruralhealthcareersor undertake research that improveshealthoutcomesforruralcommunities.
Gary Misan and Bronwyn ellisDepartment of Rural Health, University of South Australia
(L-R) Dr Martin Jones, Chris Ghan, Caralyn Hale, Fiona Norris, Ju Sung Han, Reem Hasaneen, Mitch Wilson, Dr Gary Misan (Absent: Bronwyn Ellis)
univerSiTy OF SOuTH auSTralia
in memory of PhilliP hughesAshewalkedtowardstheHeaven’sgates,hestoodthereallalone Andturnedhisfacebacktotheworld,andthecountryhe’dcalledhome Hesawthetear-stainedfacesthatspannedAustraliawide ForthelittleblokefromMacksville,whotragicallyhaddied. HespuntofaceSaintPeter,withhiscapandbatinhand. Heasked“Pleasedon’tletmyfriendsandfamilysuffer, Justhelpthemifyoucan”. SaintPeterembracedthesaddenedmanandheldhimstrongandtrue “They’llneverbealonemyson,they’llforeverstillhaveyou.” “Althoughyouhadtoleavethem,andthatworldyoudiddepart, Apieceofyouforeverremainsineachoftheirsadhearts”. AsHugheshadturnedtoenterHeaventhroughthestunningGoldenGate Avoiceyelledfromtheshadows“Comeoverherenowmate”. Bradmanstoodtheregrinningwithabatandballinhand. HeputhisarmaroundPhil’sshoulderandsaid“You’reuptobatyoungman”.
Winner of the 2015 Friends poetry competition,asvotedbydelegatestothe13thNationalRuralHealthConference
letter to the editor: oncology massage theraPy training in tamWorthAsanupdatetothestoryononcologymassage therapy training (Partyline #52, p53) I’m happy to report thatTamworth’s North West CancerCentre (NWCC) in NSW is about toget a brand new crop of oncologymassage therapists thanks to localcharity, Serendipity. In March thisyear,we spoke to the coordinator atNWCCandwereintroducedtoalocalmassage therapist, Sophie O’Neil(TamworthRemedialMassage),whoset about spreading the word aboutthe training. She quickly gatheredenough interest for us to set a dateandthenSerendipityagreedtocoverourcosts.Thisallowedlocaltherapiststoattend theOncologyMassageLtd
training program in July for 50 percentof theusual coursecosts -andwithoutneedingtotravel.Thetraineeswillcompletetheirqualificationlaterintheyear,withtheknowledgethattheywillbegettingplentyofreferralsfromtheregionalcancercentreandsupportgroupsinthearea.
Oncology Massage Ltd is a not forprofit training organisation. [email protected] for more information abouttraininginyourarea.
Kylie ochsenbeinOncology Massage Therapy Ltd
by ali stewart
54 Partyline August 2015
FRIENDCONTRIBUTED BY A
55Partyline August 2015
oPPortunities to advertise in Partyline
Partyline istheplacetobetopromoteyourproductorservicestopeopleandorganisationswhocareabouthealth‘inthebush’.
PartylineisthepremierpublicationoftheNationalRuralHealthAlliance.Issuedthreetimesayear, itholdsauniqueplaceasthenationalmagazineforgoodhealthandwellbeinginruralandremoteAustralia.Withpolicypieces,personalstories,reviews,poemsandpictures,themagazineisacomprehensiveroundupofthelatestinformationforthosewithaninterestinruralandremotehealth.
Partyline has:• over13,000hardcopysubscribers,andisfreelyavailableonline;• anationalreadershipthatspansrural,remoteandmetropolitanAustralia;and• an influential readership that includesCommonwealthandStateMinisters,MembersofParliamentandleadersinthecorporateandnot-for-profitsectors.
Forthetechnicalspecificationsandadvertisingratespleaseseewww.ruralhealth.org.au/publications/partyline/contributor-guidelines or contact theEditor,SusanMagnay(email:[email protected],orphone0262854660)
Issuesponsorshipoptionsarealsoavailable.TodiscusshowwecanhelpyoubecomePartylinesponsorcontacttheEditor,SusanMagnay.
cover photo: Arthur Mostead
eDiToRiAl DeTAils:PartylineistheMagazineoftheNationalRuralHealthAlliance,thepeakbodyworkingtoimprovehealthandwellbeinginruralandremoteAustralia.TheEditorialGroupforthisPartylinewasSusanMagnay(Editor),JennyFreemanandStephenKingston(GraphicDesign),theFriendsAdvisoryCommitteeandstaffoftheNRHA.
Articles,letterstotheeditor,photographs,poetryandanyothercontributionsarealwayswelcome.Pleaseemail these to: [email protected]:SusanMagnay,Editor,Partyline,POBox280,DeakinWest,ACT2600;Phone(02)62854660;Fax(02)62854670.
The opinions expressed inPartyline are those of contributors and not necessarily of theNationalRural HealthAlliance or its individualMember Bodies.TheAustralianGovernmentDepartment ofHealthprovidestheAlliancewithcoreoperationalsupport. Partylineisdistributedfree.Tosubscribe,email your contact details to [email protected] Partyline is also available online at www.ruralhealth.org.au
ISSN1442-0848

Key areas of focus include:• placingchildrenandtheirfamiliesatthecentreofcare
• enhancingthepatientjourneyfromprimarytotertiarycare–andbackagain
• improvingaccesstotherightcare,intherightplace,attherighttime
• buildingthecapacityofthelocalhealthworkforceteamtocareforchildren
• improvinghealthcareoutcomesforAboriginalandTorresStraitIslanderchildren
• caringforkidswithchronicand/orcomplexhealthneeds
• providingemergencycare
• mentalhealthcare
• careofruralandremotechildrenwithtraumaticinjury
Children’s Healthcare Australasia (CHA) and the National Rural Health Alliance (NRHA) are joining forces to host a conference on quality health care for children and young people
living in rural, regional and remote communities across Australia.
www.countrykids.org.au