welcome to the jungle - wordpress.com · 2017-08-04 · welcome to the jungle! dr aileen oon, 2017...
TRANSCRIPT

Welcome to the
Jungle! Dr Aileen Oon, 2017
Microbiology Registrar
AA 55M presented with sores on left olecranon and umbilical
area
Umbilical sores present for 3 weeks
Left olecranon lesions for 1 week
Now erythematous tracking up medial arm
No recorded fevers but reported night sweats
Also had lower limb lesions which had healed spontaneously

PMHx Renal calculi
Laparotomy and appendectomy
Nil regular medications
SHx Non- smoker
Occasional EtOH
Ex-fire brigade
Travelled to Costa Rica for 3 weeks to visit son
Spent time in the jungle
Sustained cut to leg and wound took long time to heal

Costa Rica
O/E Lesion on left olecranon with surrounding erythema and
tracking erythema medial arm
2 periumbilical lesions with crusting
Given IV cefazolin and discharged on cephalexin

An astute ID physician gives
phone advice to ED… Biopsy of wound
Mycobacterial and fungal culture/PCR
Malaria thick and thin smear, ICT
Zika serology
Rickettsial serology
HIV serology
Results Rickettsial and Zika serology negative
Mycobacterial PCR on tissue negative
HIV serology negative
Swab MCS of lesions no growth

Leishmania PCR positive!
Likely L.braziliensis

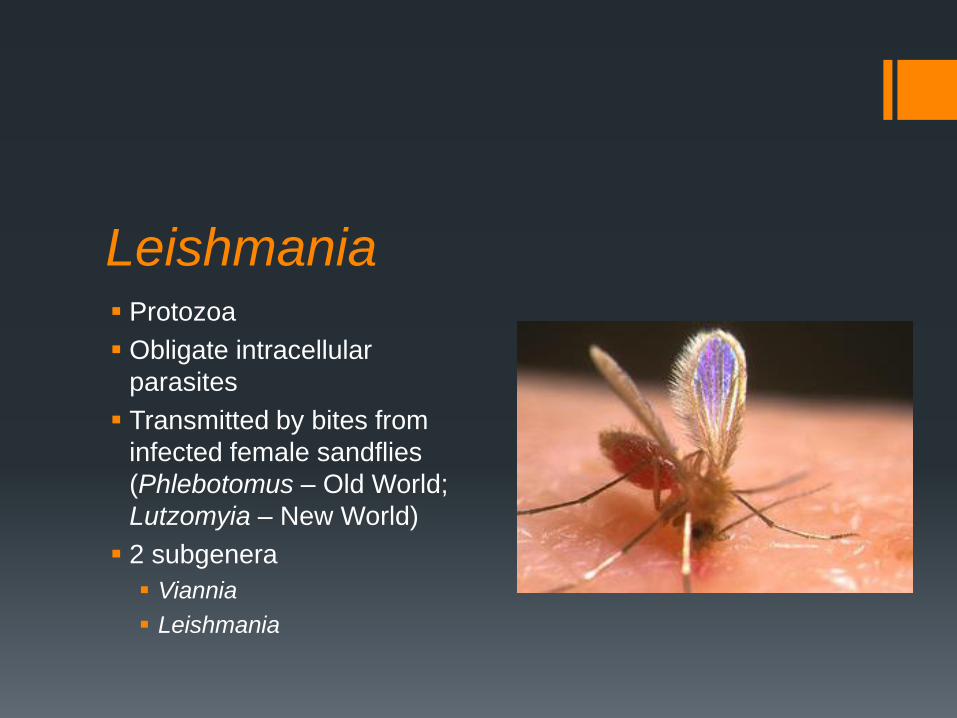
Leishmania Protozoa
Obligate intracellular
parasites
Transmitted by bites from
infected female sandflies
(Phlebotomus – Old World;
Lutzomyia – New World)
2 subgenera
Viannia
Leishmania


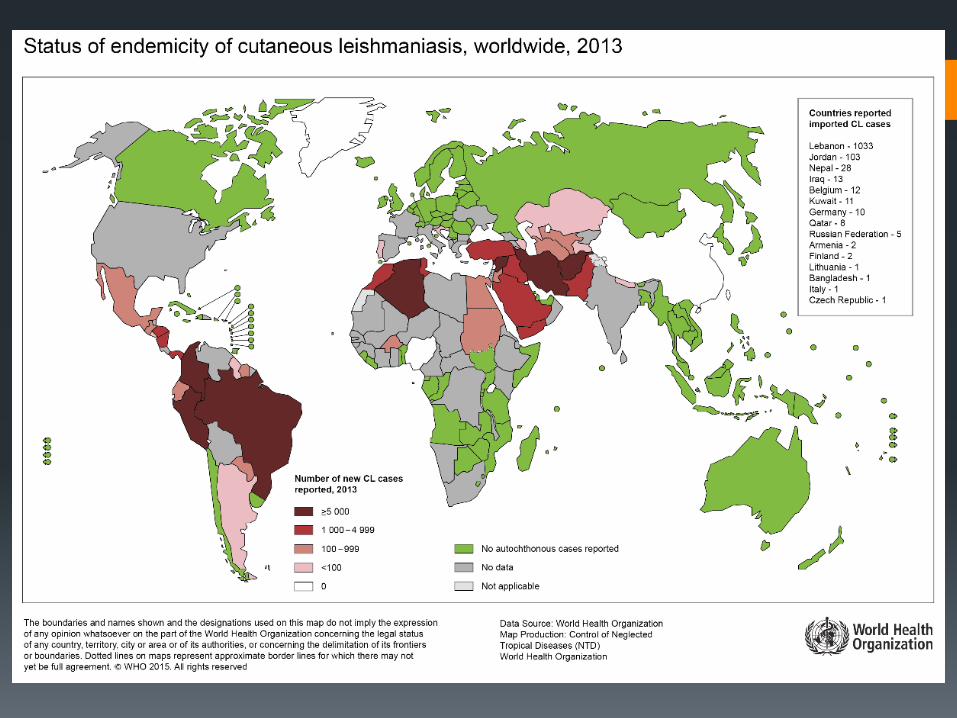
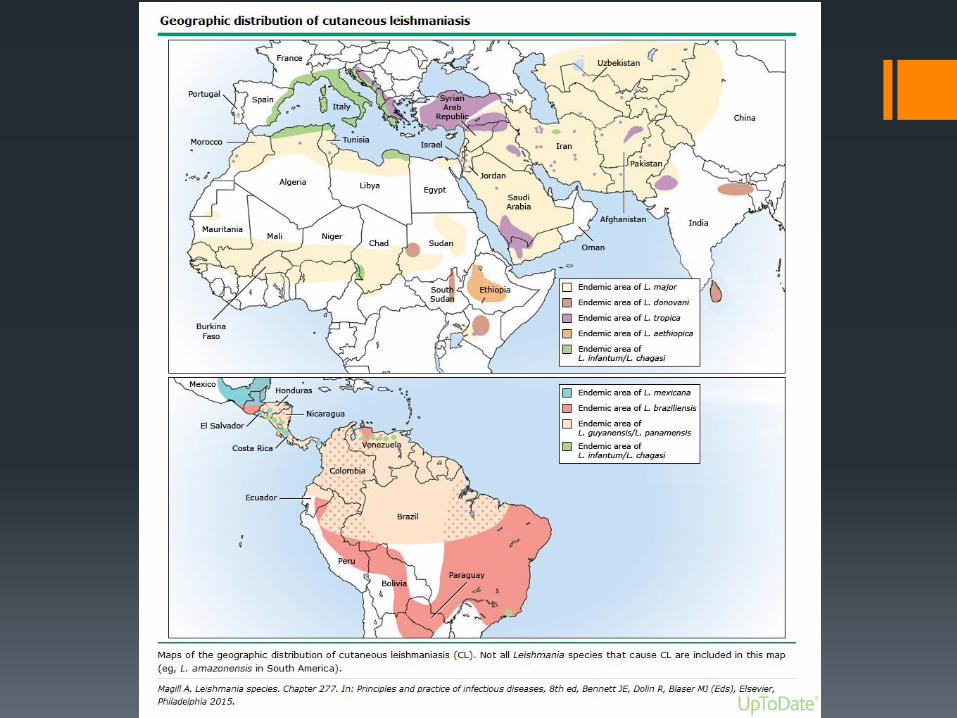
Old World vs New World Old world – “oriental sore”
Middle East, Mediterranean, Africa, India and Asia
L.major, L.tropica, L.donovani and L.infantum
New world
Widespread in Latin America
L.braziliensis, L.mexicana, L.panamensis

What’s in a name? Cutaneous, diffuse cutaneous, mucocutaneous or visceral
disease (kala azar)

In Australia No localised transmission
Cases in dogs imported from endemic countries (L. infantum)
Australian phlebotomine sandflies don’t bite humans
Zelonia australiensis affecting kangaroos
www.uts.edu.au

Cutaneous Leishmaniasis In New World vector usually Lutzomyia spp
Papule forms at initial bite site developing into papulonodule
which has central ulceration
Amastigote containing macrophages dominate in acute
infection
Granulomatous response
Lesions heal slowly
Recovery associated with high level of resistance to
reinfection with homologous spp

L.braziliensis regional
lymphadenopathy can precede
cutaneous lesions by 1-12wks
When skin ulcer develops the
lymphadenopathy and systemic
symptoms subside
Malekpour et al NEJM 2010

Diagnosis Can be made on clinical grounds in endemic countries
Definitive Dx
Detection of amastigotes in clinical specimens
Promastigotes in culture
Sampling of cutaneous lesions
Clean with 70% EtOH and debris removed
Scrape base of ulcer or edge of lesion
Submit tissue for histology
Giemsa stain



PCR PCR more sensitive cf direct microscopy, histology and
culture
Limited availability
No standardisation and lack of multicentered studies for
validation
Targets
rRNA ITS, 7SL RNA gene, HSP 70 gene, cytochrome b gene
Multiple targets needed due to gene polymorphism
Jara et al JCM 2013
Culture Collect tissue aseptically
Mince tissue prior to culture
Novy, MacNeal, Nicolle’s medium,
Schneider’s Drosophila medium
supplemented with 30% foetal
bovine serum
Incubate up to 4wks
Promastigotes can be detected on
wet mounts
Manual clinical micro 2015

Serology Only available for research or epidemiologic purposes
Not useful for diagnosis
Available at CDC
Treatment Simple cutaneous lesions heal spontaneously
Cryotherapy, heat, photodynamic therapy, surgical excision,
chemotherapy
Azoles, amphotericin B, miltefosine, pentavalent antimonials
Visceral leishmaniasis fatal if not treated
No human vaccine available

Pentavalent antimony
Intramuscular Sb overall cure rate
76%
20 day course
Young age, non immune persons
(e.g tourists), geographic location
correlate with Rx failure
Toxic and poorly tolerated

Miltefosine 50mg 3 times daily for 28 days
Exact mechanism of action
unknown
?interacts with phospholipids and
steroids in cell membrane
Inhibition of cytochrome c oxidase
FDA approved for 3 spp
L.braziliensis, L.panamensis,
L.guyanensis

Prevention Personal protective measure
Clothing
DEET based insect repellants
Vector control in endemic countries
Sandfly resistance to insecticides

Outcome AA was seen in the
outpatient ID clinic
No evidence of mucosal
involvement
Commenced on 28 day
course of oral
miltefosine
Cutaneous lesions
improving
Take home messages Suspect in pts with non healing wounds who have travelled
through endemic areas
Difficult to culture
Utility in PCR but not validated
Don’t get bitten by sandflies
Acknowledgements Dr John Burston (ID consultant)
QUESTIONS?