welcome to the aml18 initiation version 1.2 july 2014
TRANSCRIPT

Welcome to the AML18 initiation
Version 1.2 July 2014

Welcome• Site will require the following personnel to attend
training before site is opened:– PI– Research nurse– Pharmacist
• Information should be cascaded down and on-site training documented in training log
• Training certificates will be emailed

Trial Background
• Phase III multi-centre trial• Replacement trial for intensive arm of AML16 • Building on findings from AML18 Pilot• > 60 years of age• Standard chemotherapy plus novel treatment• 5 treatment arms• Not all randomisation options may be
available, we’ll keep you informed!

Trial Design

Objectives• Does a fractionated schedule of two doses of Mylotarg
3mg/m2 improve upon the current standard of care for patients with good and intermediate risk cytogenetics?
• Does the addition of Ganetespib starting at course 2 improve outcomes?
• Does the addition of either a short or long (maintenance) course of AC220 improve outcomes?

• Is MRD status following course 1 of clinical value?
• Does intensification of treatment for MRD+ patients improve outcome ?
• To compare a total of two versus three courses of treatment in patients who are in CR or CRi and MRD -ve after induction course 1
• To assess the value of Reduced Intensity Allogeneic Stem Cell Transplantation as consolidation for patients with a matched sibling or matched unrelated donor
Continued
Endpoints
• Overall survival• Complete remission (CR + CRi) achievement
and reasons for failure (for induction questions)• Duration of remission, relapse rates and deaths
in first CR• Toxicity, both haematological and non-
haematological• Supportive care requirements (and other
aspects of health economics)

Randomisation optionsThere are four randomisations in the trial •one at entry to the trial (1 or 2 doses of Mylotarg)•two following course 1 when MRD status is known
– For no CR or MRD +ve patients (DA versus DAC versus FLAG-Ida)
– one is for all patients eligible to enter the small molecule (AC220 or ganetespib) randomisation
•A fourth randomisation follows course 2 for MRD-ve patients (2 vs 3 courses of chemotherapy)
•In special circumstances, contact HCTU
Eligibility – all patientsInclusion:• They have one of the forms of AML, or high risk MDS.• Over the age of 60, but patients under this age are eligible if they are not considered eligible for
the MRC AML17 trial.• They have given written informed consent.• Serum creatinine ≤ 1.5 × ULN (upper limit of normal) • Patients eligible for the Mylotarg randomisation must have ALT and AST ≤2.5 × ULN and
bilirubin ≤2.× ULN• In order to be eligible to receive cladrabine, serum creatinine must be within the local ULN to
enter that randomisation. Patients for whom this is not the case can be randomised between the remaining options.
• Adequate and medically accepted method of contraception throughout the study. These measures must be in place for at least 30 days after the last administration of ganetespib and 6 months after the last administration of Cladribine.
• ECOG Performance Status of 0-2
Exclusion:

Eligibility – all patientsExclusion:
• They have previously received cytotoxic chemotherapy for AML• [Hydroxycarbamide, or similar low-dose therapy, to control the white
count prior to initiation of intensive therapy, is not an exclusion]• They are in blast transformation of chronic myeloid leukaemia (CML)• They have a concurrent active malignancy excluding basal cell
carcinoma• They are pregnant or lactating• They have Acute Promyelocytic Leukaemia• Known infection with human immunodeficiency virus (HIV)• Patients with AST or ALT more than 2.5 times the local upper limit of
normal, or bilirubin more than twice upper limit of normal, are not eligible for the Mylotarg randomisations.

Cardiovascular System Exclusion Criteria– Small Molecule
Known serious cardiac illness or medical conditions, including but not limited to:•Clinically unstable cardiac disease, including unstable atrial fibrillation, symptomatic bradycardia, unstable congestive heart failure, active myocardial ischemia, or indwelling temporary pacemaker•Ventricular tachycardia or a supraventricular tachycardia that requires treatment with a Class Ia antiarrhythmic drug (e.g., quinidine, procainamide, disopyramide) or Class III antiarrhythmic drug (e.g., sotalol, amiodarone, dofetilide). Use of other antiarrhythmic drugs is permitted. •Use of medications that have been linked to the occurrence of torsades de pointes (see Appendix for the list of such medications) •Second- or third-degree atrioventricular (AV) block unless treated with a permanent pacemaker•Complete left bundle branch block (LBBB)•History of long QT Syndrome or a family member with this condition•QTc >470 ms (average of triplicate ECG recordings); a consistent method of QTc calculation must be used for each patient’s QTc measurements. QTcF (Fridericia’s formula) is preferred.•Serum potassium, magnesium, and calcium levels not outside the laboratory’s reference range

Current IMPs
• Gemtuzumab Ozogamicin (Mylotarg)• Cladribine• Quizartinib (AC220)• Ganetespib
Note:
Standard chemotherapy drugs are not IMPs

Treatments & schedules see section 9 in the protocol
Course 1 – All patients (Patients with known poor risk cytogenetics at diagnosis will receive DA only)
DA plus Mylotarg 1 schedule
•Daunorubicin 60mg/m2 daily by IV infusion on days 1, 3 and 5 (3 doses)
•Cytosine Arabinoside 100 mg/m2 12-hourly by i.v. push on days 1 – 10 inclusive (20 doses)
•Mylotarg (GO) 3mg/m2 on day 1 of DA chemotherapy
DA plus Mylotarg 2 schedule
•Daunorubicin 60mg/m2 daily by i.v. infusion on days 1, 3 and 5 (3 doses)
•Cytosine Arabinoside 100 mg/m2 12-hourly by i.v. push on days 1 – 10 inclusive (20 doses)
•Mylotarg (GO) 3mg/m2 (capped at a maximum of 5mg per dose for patients with BSA above 1.67 m2) on days 1 and 4 of DA chemotherapy

Treatments & schedulesMRD-ve Patients
Course 2 (2 vs 3 randomisation)
DA 3+8 •Daunorubicin 50 mg/m2 daily by i.v. infusion on days 1, 3 and 5 (3 doses)•Cytosine Arabinoside 100 mg/m2 12-hourly by i.v. push on days 1 – 8 inclusive (16 doses)
Course 3 (if applicable)
DA 2+5•Daunorubicin 50 mg/m2 daily by i.v. infusion on days 1 and 3 (2 doses)•Cytosine Arabinoside 100 mg/m2 12-hourly by i.v. push on days 1 – 5 inclusive (10 doses)

Treatments & schedules - MRD+ve/unknown Patients
FLAG-Ida or Mini FLAG-Ida Therapy
Course 2
For patients aged 60-69 years – FLAG-Ida
•Fludarabine 30 mg/m2 daily i.v. on days 2-6 inclusive (5 doses)
•Cytosine Arabinoside 1 g/m2 daily over 4 hours, starting 4 hours after Fludarabine on days 2-6 inclusive (5 doses). G-CSF [Lenograstim 263 mg (1 vial)] s.c. daily days 1-7 inclusive (7 doses).
•Idarubicin x 8mg/m2 i.v. daily on days 4, 5 and 6
For patients aged 70+ years - Mini FLAG-Ida
•Fludarabine 25 mg/m2 daily i.v. on days 2-5 inclusive (4 doses)
•Cytosine Arabinoside 1 g/m2 daily over 4 hours, starting 4 hours after Fludarabine on days 2-5 inclusive (4 doses)
•G-CSF [Lenograstim* 263mg (1 vial)] s.c. daily days 1-6 inclusive (6 doses).
•Idarubicin 5 mg/m2 i.v. daily on days 3, 4 and 5 (3 doses)

Treatments & schedules• Course 3 Mini FLAG-Ida (for all patients)• Fludarabine 25 mg/m2 daily i.v. on days 2-5 inclusive (4 doses)• Cytosine Arabinoside 1 g/m2 daily over 4 hours, starting 4 hours after
Fludarabine on days 2-5 inclusive (4 doses)• G-CSF [Lenograstim* 263mg (1 vial)] s.c. daily days 1-6 inclusive (6
doses).• Idarubicin 5 mg/m2 i.v. daily on days 3, 4 and 5 (3 doses)
G-CSF: Lenograstim is recommended in this regime but is not obligatory
Treatments & schedulesDAC Therapy
Course 2: DAC 3+8+5•Daunorubicin 50 mg/m2 daily by i.v. infusion on days 1, 3 and 5 (3 doses)•Cytosine Arabinoside 100 mg/m2 12-hourly by i.v. push on days 1 – 8 inclusive (16 doses)•Cladribine 5mg/m2 daily on days 1-5 inclusive by subcutaneous injection (capped at a maximum of 10mg per dose)
Course 3: DAC 2+5+5•Daunorubicin 50 mg/m2 daily by i.v. infusion on days 1 and 3 (2 doses)•Cytosine Arabinoside 100 mg/m2 12-hourly by i.v. push on days 1 – 5 inclusive (10 doses)•Cladribine 5mg/m2 daily on days 1-5 inclusive by subcutaneous injection (capped at a maximum of 10mg per dose)
Please note: Daily monitoring of creatinine is required during cladribine therapy

Treatments & schedulesDA Therapy
Course 2: DA 3+8 •Daunorubicin 50 mg/m2 daily by i.v. infusion on days 1, 3 and 5 (3 doses)•Cytosine Arabinoside 100 mg/m2 12-hourly by i.v. push on days 1 – 8 inclusive (16 doses)
Course 3: DA 2+5•Daunorubicin 50 mg/m2 daily by i.v. infusion on days 1 and 3 (2 doses)•Cytosine Arabinoside 100 mg/m2 12-hourly by i.v. push on days 1 – 5 inclusive (10 doses)

IMP Specifics IMylotarg
– Supplied as an amber glass vial containing
5mg of Mylotarg lyophilised powder
– Light-sensitive and must be protected from direct and indirect sunlight and unshielded fluorescent light
– Reconstitute as per pharmacy manual
– Diluted drug solution may be stored for up to 16 hours at room temperature
– Administered as a 2 hour intravenous infusion (DO NOT administer as an intravenous push or bolus).
– Mylotarg will be given at a dose of 3mg/m2 on day 1 of course 1 for patients in arm A (1 dose of Mylotarg) and at a dose of 3mg/m2 on days 1 and 4 of course 1 for patients in arm B (2 doses of Mylotarg).
IMP Specifics IICladribine
– Cladribine (Litak) is a 2mg/ml solution for injection
– Supplied in a type 1 glass vial with rubber stopper and flip off aluminium cap
– Each vial contains 10mg of cladribine in 5ml of solution
– Cladribine is supplied as a ready to use solution for injection
– Inject as a subcutaneous bolus injection without dilution

IMP Specifics IIIAC220
– AC220 is supplied in a tablet formation, each containing 20mg AC220
– Packaged in high density polyethylene bottles, containing 30 tablets, with child-resistant caps
– Patients will take 2 x 20mg AC220 tablets once a day on an empty stomach at least 1 hour before or 2 hours after a meal in the morning
– Take for 14 days after cycles 2 and 3 of chemotherapy
– Patients on maintenance AC220 will take AC220 for 28 days for 12 cycles
– AC220 must be discontinued 48 hours prior to the next course

IMP Specifics IVGanetespib
– Supplied as a 300mg/vial (25mg/mL) – Each vial contains 12ml of deliverable ganetespib– It is a clear, colourless-to-pale yellow solution,
essentially free of visible particles– Follow the protocol and pharmacy manual preparation
guideline– Please ensure patients are hydrated– Follow guidance in protocol for management
of diarrhoea

IMP Distribution
• All IMPs will be delivered by SMPU• Seeder stock of Mylotarg will be ordered by
HCTU following Green Light procedure• HCTU will replenish Mylotarg after site
randomisation• HCTU will order course 2 IMP (cladribine and
small molecule)• All subsequent course IMPs (cladribine and
small molecule) will need to be ordered by site.

IMP management
• Request procedure– Request forms provided in pharmacy file– Shipment of course 1 and 2 requested automatically by
HCTU, subsequent courses must be requested by site
• Accountability– Forms available in site file– Will be requested annually (approx.)
• Destruction– Must be authorised by Sponsor– Temperature deviations should be reported, along with
temp logs

Site file & essential documents
• Site files have been issued to all participating PIs
• Your file should contain ‘the usual’, including:– Copy of your signed agreement– Training log & initiation attendance certificates– Correspondence about clinical queries– Details of amendments
• Periodically, we’ll ask for confirmation that your site file is up to date

Online Randomisation• System ‘very similar’ to AML16 non-intensive and all other AML trials• Contact HCTU if in doubt

Data & Documentation
• CRFs similar to AML16 and LI-1 trials
• Documentation may be filled in online or sent to HCTU
• Data queries will be issued at regular intervals
• Please ensure that data is up to date
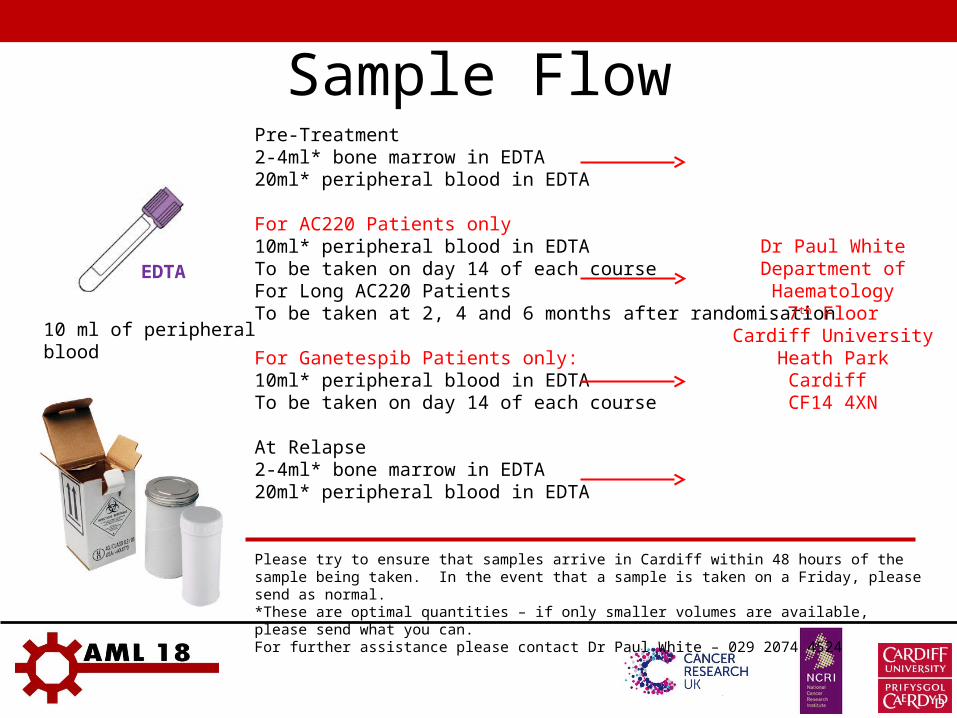
Sample Flow
10 ml of peripheral blood
EDTA
Pre-Treatment2-4ml* bone marrow in EDTA20ml* peripheral blood in EDTA
For AC220 Patients only10ml* peripheral blood in EDTATo be taken on day 14 of each courseFor Long AC220 PatientsTo be taken at 2, 4 and 6 months after randomisation
For Ganetespib Patients only:10ml* peripheral blood in EDTATo be taken on day 14 of each course
At Relapse2-4ml* bone marrow in EDTA20ml* peripheral blood in EDTA
Please try to ensure that samples arrive in Cardiff within 48 hours of the sample being taken. In the event that a sample is taken on a Friday, please send as normal. *These are optimal quantities – if only smaller volumes are available, please send what you can.For further assistance please contact Dr Paul White – 029 2074 4524
Dr Paul WhiteDepartment of Haematology
7th FloorCardiff University
Heath ParkCardiff
CF14 4XN

Enhanced Monitoring
• Enhanced monitoring will be required for every patient
receiving DA + GO x 2, DAC, AC220, Ganetespib
• Monitoring will last for 4 weeks in courses 1 and 2
• Via telephone or e-mail
Quality of Life assessment
• Key endpoint (see protocol section 2.2)• You will be provided with hard copies of QoL
questionnaires and FREEPOST envelopes• Reminder (at randomisation) for baseline QoL• Baseline QoL must be completed before
treatment commences• Auto-reminders at 3, 6 and 12 months
– Important to inform HCTU of patient death

PRE-DOSE
ECGx3
Site Review
In the event that a concomitant medication is introduced that is
known to cause QTc prolongation follow this path from Day 1 of commencing the concomitant
medication.
ECGx3
IF: Abnormality of concern e.g. value of QTcF increases
to >500ms
Site Review
ECGx3
Site Review
+ 2 HOURS + 4 HOURS
IF: value of QTcF remains >500ms = DLT= DLT
ECGx3
Site Review
Within 3 HOURS
ECGx3
DAILY
until QTc <500ms
N.B. It is not expected that 40mg AC220 will result in QTc problems but please see section
9.6.6 of protocol should any issues arise.
ECGx3
Within 2 HOURS
Cardiac Monitoring – AC220 To be completed at Day 1, Day 7 and Day 14 for cycles 2 – 4 (no small molecule in cycle 1)
Please note: ECG machines are not provided in this trial

PRE-DOSE
ECGx3
Site Review
In the event that a concomitant medication is introduced that is
known to cause QTc prolongation follow this path from Day 1 of commencing the concomitant
medication.
ECGx3
IF: Abnormality of concern e.g. value
of QTcF increases to >500ms
Site Review
+ 2 HOURS
IF: value of QTcF remains >500ms = DLT= DLT
ECGx3
Site Review
Within 3 HOURS
ECGx3
DAILY
until QTc <500msN.B. If you suspect an abnormality of concern contact HCTU
See section 9.6.6 of protocol for details.
ECGx3
within 2 HOURS
Cardiac Monitoring – AC220 Long To be completed at Day 1, Day 8, Day 15, Day 21 for cycle 1 of AC220
maintenance. Pre-dose on Day 1 only for subsequent cycles.

PRE-DOSE
ECGx3
Site Review
IF: Abnormality of concern e.g. value of QTcF increases
to >470ms
IF: value of QTcF remains >470ms = = infusion should be infusion should be
delayed until <470msdelayed until <470ms
N.B. If you suspect an abnormality of concern contact HCTU
See page 66 of protocol for details.
ECGx3
Cardiac Monitoring - Ganetespib To be completed pre-dose on Day 1 for cycles 2 - 4
Patients with reported Grade 4 QTc prolongation (QTc >500 ms or >60 ms change from baseline and torsades de pointes or polymorphic ventricular tachycardia or signs/symptoms of serious arrhythmia) or repeated Grade 3 or higher QTc prolongation must discontinue treatment with ganetespib.
QTc should be <470ms prior to each dose or delayed till it falls to
<470ms

SAE Reporting
What to include in report within 24 hours:•Patient identifiers (Trial No, DoB, Initials, Sex) *•Associated Drugs and treatment dates *•Category of event (hospitalisation/death/life threatening etc.) *•SAE start date *•Details of event *•Causality assessment for each individual associated drug *•Details of person reporting•PI signature*once these details are available the reporting clock has started
What NOT to report (see section 16.2):
• Pre-existing toxicities (only development of these toxicities requires reporting)
• Neutropenic fever and its consequences (unless >42 days post chemo)
• Death due or associated with persistent or progressive disease (although this should still be recorded, see Section 16.5)
•Unrelated SAEs 28 days or more after last dose of treatment

SAE Form
Site must complete these sections

Current Approved Documents• Protocol V3.1 May 2014
• PIS1 V2.1 April 2014
• PIS2 V1.2 April 2014
• PIS3 V2.2 April 2014
• PIS4 V3.0 May 2014
• PIS5 V2.0 July 2013
• GP Letter Course 1 V1.1 July 2013
• GP Letter Course 2 Residual Disease V2.2 April 2014
• GP Letter Course 2 CR-MRD Neg V2.0 July 2013
• GP Letter Course 3 CR-MRD Neg V2.0 July 2013

Contact detailsFor randomisations, data entry, IMP and all other queries
relating to AML18:Trial Management
&
Pharmacovigilance
Helen Clark (Tues – Fri)
029 2074 8976
Sarah Burns (Mon – Wed)
029 2184 7942
Data Manager Nuria Marquez Almunia
029 2074 6413
Trials Office Drug ordering: 029 2074 6413
Other (data): 029 2074 6413
Email: [email protected]
Return address for QoL FREEPOST Dept Haematology, 6th Floor A-B link, School of Medicine, Cardiff University, Heath Park,
Cardiff, CF14 4XN

For site activation ‘Green Light Process’
What we need from you
•Fully signed Site Agreement•Centre Registration Form •R&D approval letter
– Provide a copy to HCTU
•Initiation of key personnel

Site Activation Cont
What you’ll receive from us•Log in details for the randomisation system and website (we can’t do this without your centre registration form)•An email stating that you are now open to recruitment•Order your seeder supply of Mylotarg

Thank you for all your hard work and good luck with your recruitment
Any questions?