welcome to our booklet on
TRANSCRIPT

2
We want to talk to you about care for older people – now and in the future. Partners in this care are:
• NHS Ayrshire & Arran
• East, North and South Ayrshire Councils
• The independent sector - including care homes and care at home services
• Voluntary and community groups – which are also known as the Third sector
These agencies have contributed to this booklet. It explains how and why services may need to change over the coming years; and to ask your opinion about what services you would like to see, or possibly use, in the future.
Contents
Page 3 Why do health and social care services for older people need to change?
Page 4 Our vision
Page 5 How can we do this?
Page 6 How do we get the balance right?
Page 7 Where do we begin?
Page 9 Illustration showing how services could be provided
Page 10 Examples of how we provide services and our vision for services in the future
Page 17 Tell us what you think
Page 19 Get in touch
All our publications are available in other formats
Welcome to our booklet on Reshaping care for older people in Ayrshire and Arran.

3
Why do health and social care services for older people need to change?
Something to celebrate – people are living longer. This is because our living standards are getting better and care and support has improved.
We have created this booklet to give you information about services and ask your opinion about what you would like to see in the future.
As part of Reshaping care for older people, we have already started to increase the level of support and services available to people in the community – this will help older people stay in their own homes for longer, rather than being admitted to hospital or a care home.
Scotland’s changing population of older people
Population in 2008 Population in 2018 Population in 2028
Over 65s 856,000 1,047,000 (up 22 per cent) 1,288,000 (up 50 per cent)
Over 85s 100,000 141,000 (up 41 per cent) 208,000 (up 108 per cent)
In Ayrshire and Arran the number of those aged 85 plus between 2012 and 2022 is expected to rise from 8,637 to 12,343 (30 per cent increase).
Help us develop our plan for the next ten years …
Older people are incredibly important in our society. They contribute in lots of different ways and it is important to recognise the contribution older people make.
We know that people aged between 65 and 84 often need little care or support from organisations. Indeed, the charity Age Scotland reports that people aged 50 and over provide more than 40 per cent of all volunteering in Scotland.

4
Importantly, more than 320,000 of people aged 50 and over provide unpaid care to someone. This is an invaluable contribution to society. However, those aged 85 and over tend to need more care and support from organisations such as health, social care, independent and voluntary sector.
We also know that younger generations are making poorer lifestyle choices, such as drinking too much, eating unhealthily and not being active enough. This means that when the younger generation gets older they are more likely to have long-term health conditions caused by
unhealthy life choices – meaning they will be more dependent on services. However, it is never too late and never too early to change lifestyles.
This is why we need to start planning now, so our services will be able to cope in the future – when increasing numbers of older people may have more health problems and may need more support from health and social care.
What happens now What could happen in the futureReactive care which is provided when you become sick or have a crisis in your health
Proactive care which will help people stay healthy and plan for health conditions
Majority of care provided in hospitals
Community based care in people’s own homes, if possible, as well as acute and community hospitals, and other local facilities
Disjointed care Integrated, continuous careCare is provided to patients and carers Patients and carers fully involved in their careCarers undervalued Carers supported as partnersNot enough use of self-care People are encouraged and helped to self-care Low tech High techCare provided for each episode of illness Team-based which anticipates future needs
Geared towards acute conditions which need hospital treatment
Geared towards long-term conditions
“We want to stay in our homes for as long as possible.” That’s the message older people, locally and nationally, have been giving health and social care services for some time.
We understand this message and are taking steps to ensure the wishes of older people are respected and met.
Our vision: Older people in Ayrshire and Arran enjoy full and positive lives within their own communities

5
So how can we do this?
Through:
Local communities
We need to change the way we view ageing and older people and consider where responsibility for care and support lies. To achieve this, local communities must:
• respect and include older people
• take responsibility for their welfare and well- being
• welcome the skills and experiences that older people can contribute
• contain strong support networks offering a variety of activities and opportunities for older people
And services for older people
We need to look at all services and how they are provided. Some services may need to change and less effective services may need to stop so we can introduce better ways of working together.
Services should:
• be developed with older people
• take into account the views of carers, family, friends and social networks
• meet their needs and aspirations
• be on time, and co-ordinated
• anticipate future needs
• work in partnership with older people
But we need to remember that we have one pot of money to provide services. In the future we want to spend less on providing hospital-based services and use more of it to provide support and services in local communities.
Community wellbeing(Level 1)
Intensive support(Level 4)
Hospital care(Level 5)
Staying independent(Level 2)
Rehabilitation and
enablement (Level 3)
Balance of care
and resources
We use 15 per cent of our resources here
We use 17 per cent of our resources here
We use three per cent of our resources here
We use 20 per cent of our resources here
We use 45 per cent of our resources here

6
So how do we get the balance right?
By working together we want our future services to be:
Person-centred and focused on outcomes, so care and support is provided and arranged to suit the needs of each individual person, their carers and family. It would also take into account each individual’s choices about what care they want and how they want to receive it. Older people will be encouraged to be a partner in their own care - we will provide rehabilitation and enablement services to support and encourage older people to regain the confidence to do the things they used to do. For example, information on how to avoid falls or installing Telecare equipment, such as community alarms.
Proactive. We want to work together to make sure that people receive services when they need them rather than waiting until their situation becomes so serious that they end up being admitted to hospital or residential care.
Joined-up. If partners are able to share information with each other then problems can often be detected more quickly. Early warning of a possible health problem could mean that the person receives care more quickly and avoid an emergency admission to hospital.
Services which are flexible, responsive and always looking forward.
Our services should be able to change to suit a person’s needs. We are increasingly providing community-based services seven-days-a-week rather than keeping office hours of 9am to 5pm Monday to Friday.
We also want to encourage the use of technology such as telehealth and telecare to monitor conditions like Chronic Obstructive Pulmonary Disease, dementia and diabetes.
We also want to enable and empower communities to provide ways for older people to receive care and support through promoting volunteering and to ensure that older people are not isolated in their homes.
Accessible. We want to put as many services and supports as possible in local communities. Information about all services should be readily available for people so they can make informed decisions about the care they want, how they can prevent ill-health, and ways in which they can self-manage any long-term conditions.
Supportive of individuals and families and encourage their resilience. We recognise the huge contribution that family members, carers and volunteers have in providing care and support for older people. We want to support families to have both a role and a responsibility in the care of their older relative.

7
So where do we begin?
The next three years are going to be vital if we are to achieve our vision for older people’s services.
We have already started making changes. We have introduced ‘Hubs’ in some areas of Ayrshire, where health and social care professionals work side-by-side to provide a range of services. They work together to care for the person at home for as long as possible to reduce the need for the person to be admitted to hospital.
Each area of Ayrshire is different so we have developed draft plans for the work which needs to happen over the next three years in East, North and South Ayrshire to achieve the ten year vision. For more information on the ten year vision and three-year plans please contact us using one of the methods at the end of this booklet.
All of the partners involved in this work will need to work together. Workforce planning and development will be extremely important so we need to start planning now to make sure we have the right people, trained in the right skills, and working in the right locations, to be able to support the vision.
Unpaid carers contribute to health and social care and we want to work with carers as equal partners in the planning and delivery of care and support.
We are fully committed to ensuring that unpaid carers are assisted in their role and that the services they provide are recognised and fully supported.
How could services change?
Preventing ill-health and anticipating care needs
• Shifting the balance of care. If more people with high-level needs can be cared for at home, fewer will need to go into long-stay hospitals or care homes;
• Promoting awareness of the main causes of falls and training a wide range of people to recognise and help those who are at risk of falls;
• Community groups recognised and supported, through funding and training, to help older people stay active and healthy and to offer a place to share positive health advice and information;
• Independent sector staff in care homes and home carers are able to access more training and support from clinicians such as nutritionists and occupational therapists;
• Services located together, easy for people to get to and well-publicised;
• Resources for local communities to allow them to support their older residents;
• Dementia Action Plans to target resources for people with dementia across Ayrshire; and
• Voluntary organisations play a significant role in organising resources in local communities.

8
Keeping people independent
• More older people receiving support from community-based services such as ‘enablement’ - which means encouraging people who have been ill or injured to have confidence to do things for themselves and remain independent and community nursing and community- based therapy teams;
• Support for carers’ groups, training and good quality respite in recognition of and support for family and friends who care for a loved one;
• Making the best use of telehealth and telecare to support people in their homes; and
• More services provided out-of-hours and at weekends to support care at home.
Effective care at times of change
• Making it easier to get equipment when it is needed;
• Home care services with a focus on enablement; and
• Organisations working together so that care is co-ordinated in the best way possible.
Care homes
• Changing the way care home places are used, aiming to reduce the number of long stay care home places and increasing the number of places used for respite and rehabilitation. This could offer an alternative to hospital admission, and a place to go for rehabilitation after leaving hospital, if people need more support but are not in need of medical care; and
• Clinicians available to support staff and residents in care homes.
Hospitals
• More comprehensive assessment services at the ‘front door’ of the hospital including possible safe alternatives to reduce the need for an ‘automatic admission’ to hospital for older people who attend A&E. This could include extra support and care provided in the home, or a brief spell in a care home; and
• Reducing the length of time a person has to stay in hospital, and speeding up their discharge when they no longer need medical care, by increasing support and services for them in local communities.
We need to know what you think about our vision for older people’s services. It is important that we recognise that this is not just about today’s older people. Everyone will be affected by these changes at some point in their lives so we need your views.
9
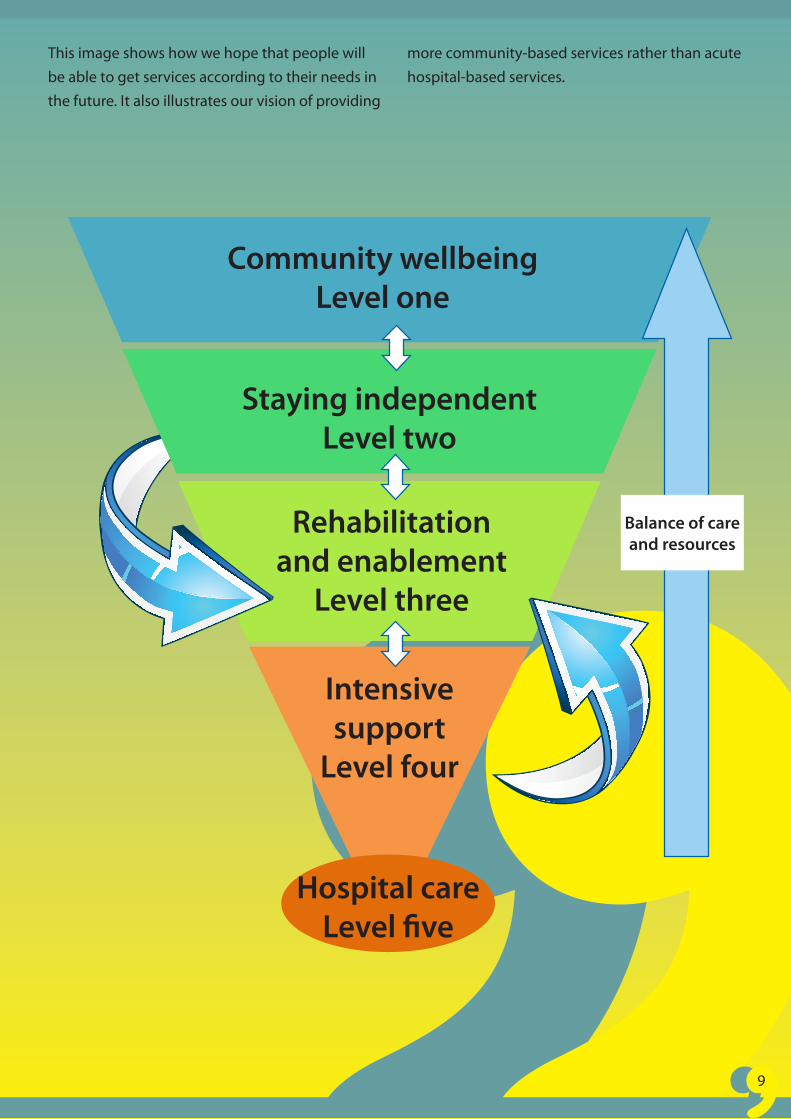
This image shows how we hope that people will be able to get services according to their needs in the future. It also illustrates our vision of providing
more community-based services rather than acute hospital-based services.
Community wellbeingLevel one
Rehabilitation and enablement
Level three
Intensive support
Level four
Hospital careLevel five
Balance of care and resources
Staying independentLevel two

The following pages feature examples of how we provide services today, alongside how we hope that services could be provided for older people in the future.
Billy is 64, has been retired for a year and has been bereaved. He is feeling isolated and beginning to experience symptoms of depression.
Billy goes to see his GP
Our vision
GP suggests getting involved in local activities and also prescribes anti-depressants for him. Billy goes along to a Men’s Health Walking Group.
Billy’s community pharmacist provides him with information and support on his anti-depressant under the New Medicines element of the Chronic Medication Service.
Through this he makes contact with a local older people’s lunch club which he volunteers to help in and this leads to him being involved in a small Community Transport scheme as a volunteer driver.
GP Surgery
Pharmacy
Billy goes to see his GP
What might happen now?
GP suggests getting involved in local activities and also prescribes anti-depressants for him.
GP would like to send him for some counselling but hasn’t got easy and quick access.
GP Surgery
10
Carers’ Centre
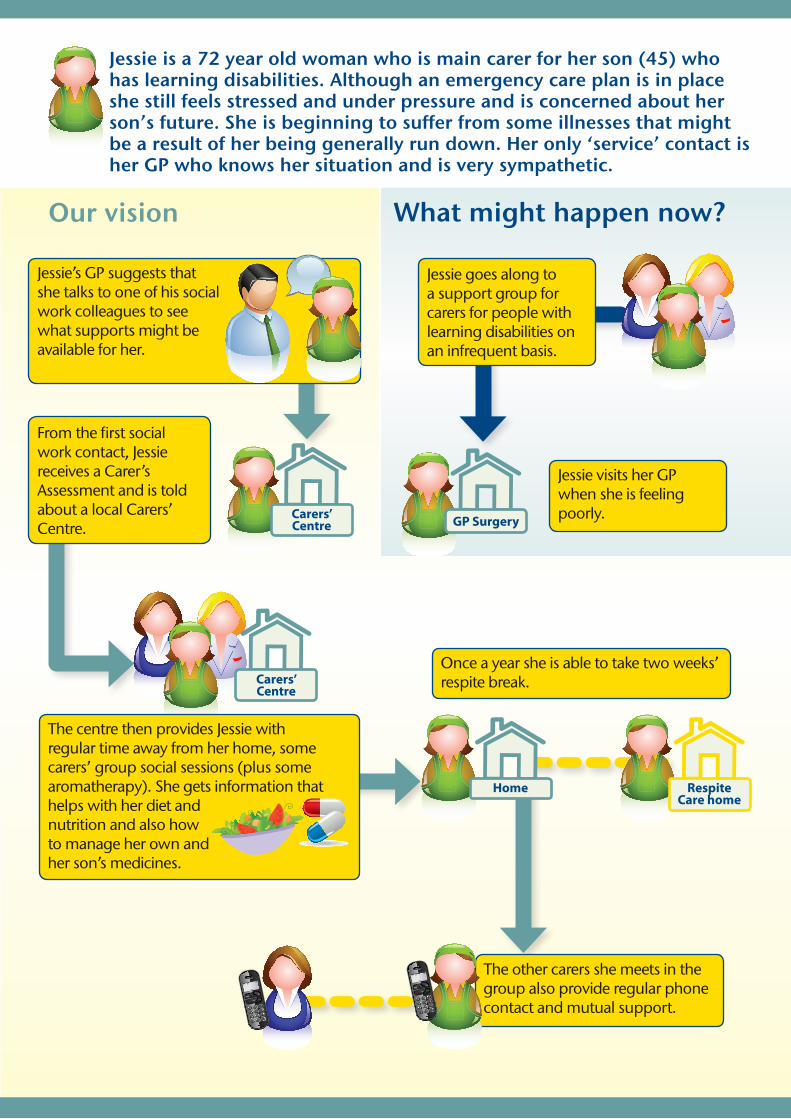
The centre then provides Jessie with regular time away from her home, some carers’ group social sessions (plus some aromatherapy). She gets information that helps with her diet and nutrition and also how to manage her own and her son’s medicines.
Jessie’s GP suggests that she talks to one of his social work colleagues to see what supports might be available for her.
From the first social work contact, Jessie receives a Carer’s Assessment and is told about a local Carers’ Centre.
The other carers she meets in the group also provide regular phone contact and mutual support.
Once a year she is able to take two weeks’ respite break.
Jessie is a 72 year old woman who is main carer for her son (45) who has learning disabilities. Although an emergency care plan is in place she still feels stressed and under pressure and is concerned about her son’s future. She is beginning to suffer from some illnesses that might be a result of her being generally run down. Her only ‘service’ contact is her GP who knows her situation and is very sympathetic.
What might happen now?Our vision
Carers’ Centre GP Surgery
Jessie goes along to a support group for carers for people with learning disabilities on an infrequent basis.
Jessie visits her GP when she is feeling poorly.
Home Respite Care home

Janet and John are referred to the local social care and health hub. This leads to a review of her medicines as some may be causing her to fall, and a worker carrying out a Falls screen in
their house.
Her medicines are changed as recommended by the clinical pharmacist.
This helps to build her confidence and John starts to worry less.
Some low level telecare equipment being installed, some advice on the home environment being given (about some of the carpeting and rugs) and a referral to the local Invigor8 Exercise Class which Janet starts attending.
John and Janet are in their late 70s and manage to live a full and active life. Janet has a fall which leads to an emergency hospital visit. This happens again during the night when she visits the lavatory and it is an hour before John hears her cry for help. John is getting a bit worried about leaving Janet on her own.
What might happen now?Our vision
Janet is admitted to hospital after another fall and after returning home lacks the confidence to leave the house.
Hospital
Home
Home GP Surgery
Invigor8 Exercise Class

Alice has her inhalers and medicines reviewed by her community pharmacist who works with a specialist nurse to help her manage her condition better.
She also receives Telecare equipment in her home which allows her to provide health monitoring information to her local hub, and, in particular, her local district nurse.
She is referred to an 8 week community pulmonary rehab course and also becomes involved in a local self-help group for people with COPD.
Because of all of these supports she becomes much more confident with her condition and feeling safer because her condition is being monitored. While she still needs a bit of clinical help from her community pharmacist,
district nurse and her GP, she has not needed to be admitted to hospital in an emergency situation for some time.
Alice is in her mid 70s and has suffered from Chronic Obstructive Pulmonary Disease (COPD) for a number of years. She lives alone and is a regular visitor to her GP and in the past year she has been admitted (by ambulance) to hospital when she has become very breathless.
What might happen now?Our vision
Alice continues to be admitted to hospital when she becomes breathless.Hospital
Pharmacy
HospitalHospital
Home
HomeHome GP Surgery
Home
13
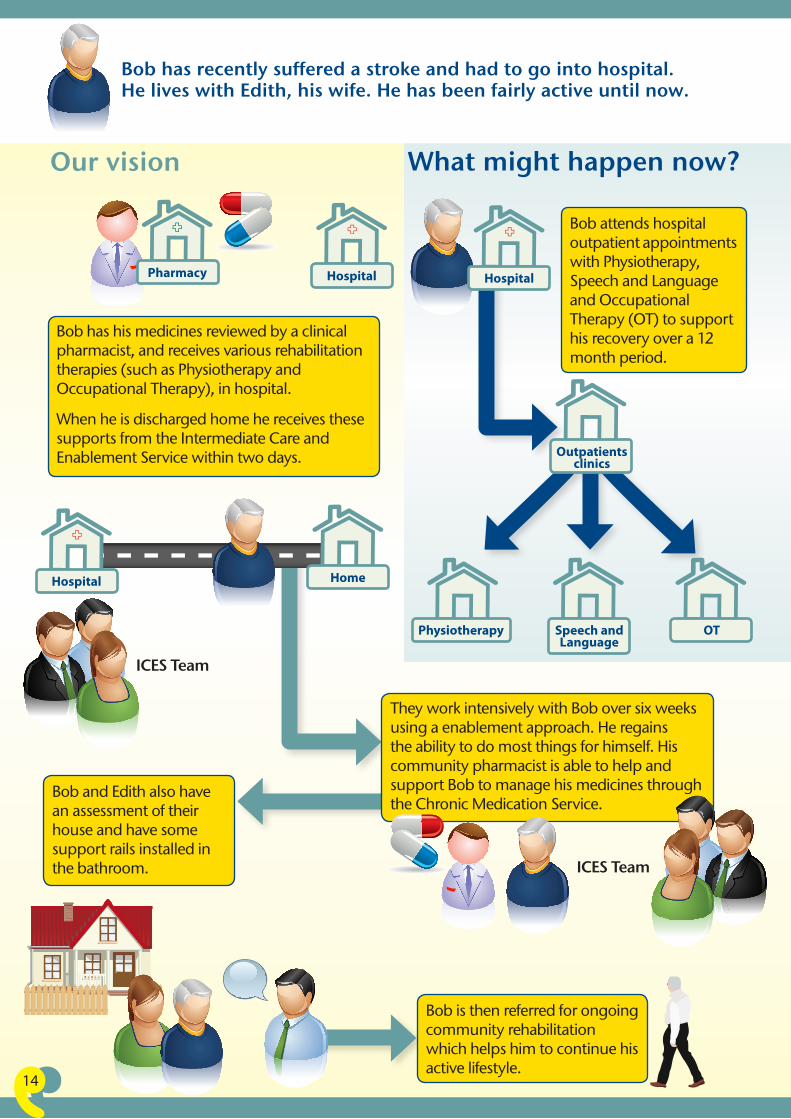
Bob has his medicines reviewed by a clinical pharmacist, and receives various rehabilitation therapies (such as Physiotherapy and Occupational Therapy), in hospital.
When he is discharged home he receives these supports from the Intermediate Care and Enablement Service within two days.
They work intensively with Bob over six weeks using a enablement approach. He regains the ability to do most things for himself. His community pharmacist is able to help and support Bob to manage his medicines through the Chronic Medication Service.
Bob and Edith also have an assessment of their house and have some support rails installed in the bathroom.
Bob has recently suffered a stroke and had to go into hospital. He lives with Edith, his wife. He has been fairly active until now.
What might happen now?Our vision
Bob attends hospital outpatient appointments with Physiotherapy, Speech and Language and Occupational Therapy (OT) to support his recovery over a 12 month period.
Hospital
Outpatients clinics
Speech and Language
Physiotherapy OT
Hospital
HomeHospital
Pharmacy
Bob is then referred for ongoing community rehabilitation which helps him to continue his active lifestyle.
ICES Team
ICES Team
14

Mary’s GP refers her to the Community Ward. The Community Ward doctor and nurse offer her more intensive support in her home. Mary’s community pharmacist has been helping Mary to use her medicines more effectively, and the clinical pharmacist working in her local hub has been providing expert input to the team looking after her.
The voluntary (Third) sector start offering an older person’s exercise class and lunch club in the sheltered housing complex and Mary’s confidence increases as she joins these groups and her health improves as she starts to take mild exercise.
Mary is 88 years old and is quite frail. She suffers from several long-term conditions including angina and diabetes. She lives in a sheltered housing complex which has disabled adaptations including a walk-in shower. She has some telecare equipment and in emergencies she can contact the alert service. She has been admitted to hospital three times in the past six months.
What might happen now?Our vision
Mary’s GP Practice monitors her hospital admissions using the SPARRA* register and she goes to the practice nurse for support.
GP Surgery
Community ward Pharmacy
Hospital
GP Surgery
VolunteersExercise
Lunch club
15
* Scottish Patients At Risk of Readmission and Admission
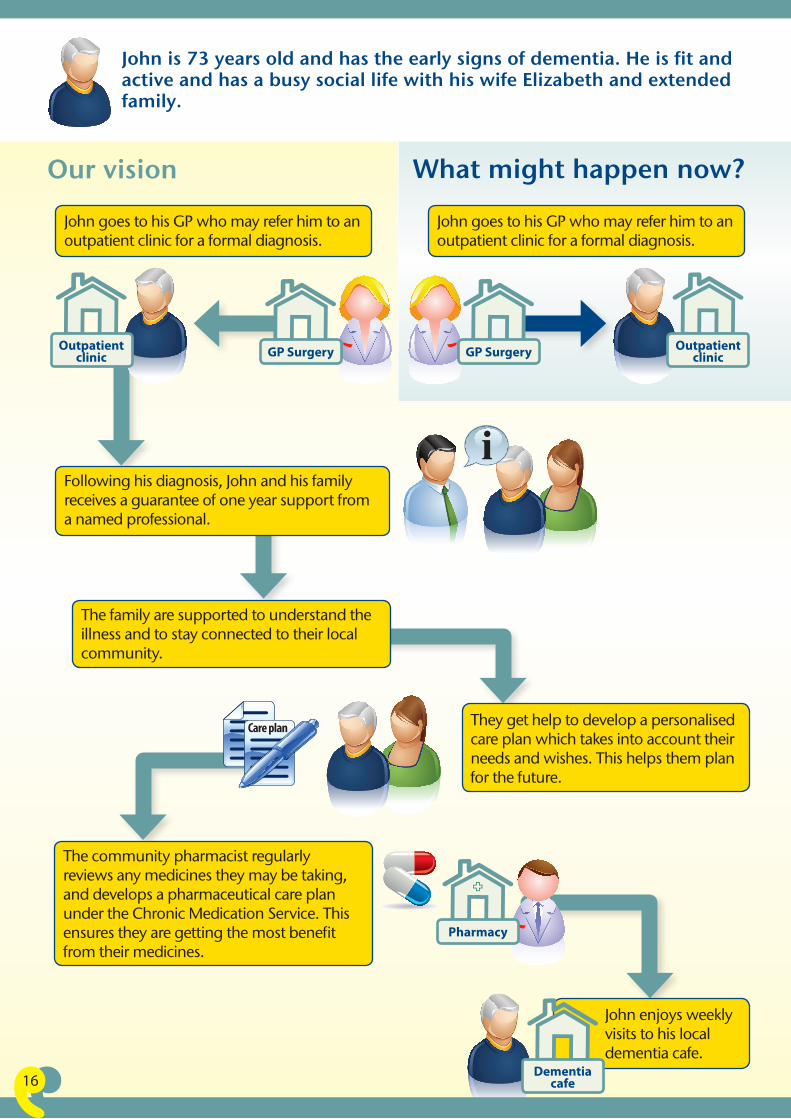
John is 73 years old and has the early signs of dementia. He is fit and active and has a busy social life with his wife Elizabeth and extended family.
Our vision
John goes to his GP who may refer him to an outpatient clinic for a formal diagnosis.
John goes to his GP who may refer him to an outpatient clinic for a formal diagnosis.
Following his diagnosis, John and his family receives a guarantee of one year support from a named professional.
They get help to develop a personalised care plan which takes into account their needs and wishes. This helps them plan for the future.
The community pharmacist regularly reviews any medicines they may be taking, and develops a pharmaceutical care plan under the Chronic Medication Service. This ensures they are getting the most benefit from their medicines.
GP SurgeryGP Surgery Outpatient clinic
Outpatient clinic
The family are supported to understand the illness and to stay connected to their local community.
John enjoys weekly visits to his local dementia cafe.
Care plan
Pharmacy
Dementia cafe
What might happen now?
16
17
Tell us what you think
The stories you’ve just read show our vision for the future. But we need you to help us get there. While we will continue to provide services for people as they get older we also need people to take more ownership of their own health and the choices they make. We all know that smoking is bad for our health and that by being overweight we are more likely to develop diabetes. But we can prevent ill-health by making positive health choices now. With more people living longer it will be more important than ever for people to
have taken responsibility for their own health in their youth to reduce their chances of developing avoidable medical conditions which would need intensive health and social care services later in life.
Our ten year vision for joint services for older people is that: Older people in Ayrshire and Arran enjoy full and positive lives within their own communities.
Please tell us what you think about our vision:
Q1. Do you support our ten year vision for joint services for older people?
Q2. Is there anything else you feel should be included which would help to prevent or anticipate future care needs?
Q3. Is there anything else you feel should be included which would help older people stay independent and self-manage their conditions?

18
Q4. Is there anything else you feel should be included which would enable older people or encourage confidence and independence?
Q5. Is there anything else you feel should be included which would provide effective care as an alternative to hospital admission?
Q6. Is there anything you think we should stop doing?
Q7. Can you suggest other ways in which people can be supported to enjoy full and positive lives within their own communities?

19
You can let us know what you think in lots of different ways:
Send a letter to:
FREEPOST RRRZ-TYRA-LGCT
Older People’s Services
Patient and Community Relations
Eglinton House, Ailsa Hospital
Dalmellington Road
Ayr KA6 6AB
Email: [email protected]
Telephone free: 0800 169 1441
You can also find out more information from the following websites:
www.nhsaaa.net
www.east-ayrshire.gov.uk
www.north-ayrshire.gov.uk
www.south-ayrshire.gov.uk
www.cvoea.co.uk
www.tsinorthayrshire.org.uk
www.voluntaryactionsouthayrshire.org.uk
www.scottishcare.org
You can also request a copy of the draft Ten year vision for joint services for older people, and the three-year plans for East, North and South Ayrshire, by contacting us using any of the methods above.
We need your comments by Friday 15 February 2013.
We hope you have found this booklet informative. If you want to find out more we also have a DVD featuring Eileen McCallum, star of River City, who explains more about the services on offer just now in East, North and South Ayrshire. Eileen talks to members of the public, service-users, clinicians and staff about what they think about older people’s services while taking part in lots of different activities such as ‘Musical Minds’ – where older people get together to enjoy an afternoon of singing well-known songs - and visiting a dementia café.

MIS12-357-GD