welcome advisor live: july 27, 2017 - premier,...
TRANSCRIPT

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.
WelcomeAdvisor Live: July 27, 2017Our Presentation:Outpatient Prospective Payment System and Physician Fee Schedule CY 2018 Proposed RulesWill Begin Shortly
Listen to Today’s Audio: 888.225.2850
Download today’s slides at www.premierinc.com/events

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.
Advisor LiveOutpatient Prospective Payment System and Physician Fee Schedule CY 2018 Proposed Rules
July 27, 2017
@PremierHA#AdvisorLiveDownload today’s slides at www.premierinc.com/events

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.3
Logistics
AUDIODial in to our operator assisted call, 888.225.2850
QUESTIONSUse the “Questions and Answers”
RECORDINGThis webinar is being recorded. View it later today on the event post at premierinc.com/events.
NOTESDownload today’s slides from the event post at premierinc.com/events

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.4
Faculty
Danielle Lloyd, M.P.H. VP, policy and advocacy Deputy director, D.C. office, Premier, Inc.
Aisha Pittman, M.P.H. Senior director, quality policy and analysis,Premier, Inc.
Kellie Webb, M.B.A. Director, payment policy and analysis,Premier, Inc.
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.5
Agenda
§ Outpatient Prospective Payment System (OPPS)– Payment – 340B Program – Packaged Items and Services– Inpatient Only Procedures– Outpatient Quality Reporting– ASC Quality Reporting– ASC Payment Updates
§ Medicare Physician Fee Schedule (MPFS)– Telehealth Services– Site Neutral Payment– Appropriate Use for Diagnostic Imaging– PQRS/Value Modifier Updates– Medicare Shared Savings Program
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.6
Outpatient Prospective Payment System (OPPS)

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.7
OPPS Proposed Rule: Summary
§ OPPS Proposed Rule published in the July 20, 2017 Federal Register.
§ Market basket of 2.90%; update of 1.75%; average payment increase of ≈1.9 – 2.0%
§ Reduces payment for Part B Drugs acquired under the 340B program by almost 30%.
§ Conditionally packages payment for low-cost drug administration services, except for Medicare Part B vaccine administration services.
§ Removes total knee arthroplasty (TKA) from the inpatient only list in CY 2018.
§ Removes 2 measures for CY 2018 reporting/2020 payment.§ Delays Outpatient and Ambulatory Surgery CAHPS.§ Comment due by September 11, 2017
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.8
How To Submit a Comment
CMS OPPS Proposed Rule – Comments due 60 days from the date of display (September 11,
2017)1. Go to proposed rule2. Click “Submit a Formal Comment”, the green button on the right-
hand side of the page below the title.OR1. Go to http://www.regulations.gov2. Type “CMS-1678-P” into the search box3. Find “Medicare Program: Hospital Outpatient Prospective
Payment and Ambulatory Surgical Center Payment Systems and Quality Reporting Programs ” (should be first selection)
4. Click on “Comment Now”, the blue button to the right of the title.

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.9
Requests for Information
• Requests for public comment on solutions to better achieve transparency, flexibility, program simplification and innovation in the Medicare payment programs for outpatient and physician fee schedule services.
• Requests for public comment on payment policy options for addressing differentials between inpatient and outpatient payment for the same services.
• Requests for public comment on how the current scope of and restrictions on physician-owned hospitals affects healthcare delivery and its impact on Medicare beneficiaries.
• Invites the public to submit ideas for regulatory, sub-regulatory, policy, practice and procedural changes to achieve these goals.

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.10
OPPS Proposed Rule: Update Factors
§ Proposed Hospital Update and Estimated Change in Expenditures:−Update:
Market basket 2.90%Multifactor Productivity -0.40 percentage pointsACA Factor -0.75 percentage pointsTotal 1.75%
−Change in Expenditures:Update 1.75%Pass-Through Adjustment +0.20 percent*Outliers (’17→’18, 1.04% to 1%) -0.04 percentTotal ≈1.9 – 2.0 percent
§ Average payment increase may be higher or lower for an individual hospital:−Proposed rule estimates are slightly lower for major teaching hospitals
(1.7%) and higher for proprietary hospitals (2.3%). −Changes from the average are accounted for by differential impact of APC
recalibration and wage index.
* CMS advised that proposed rule incorrectly states this adjustment is 0.22 percent. The correct figure is 0.20 percent.

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.11
OPPS Proposed Rule: CF and Change in Spending
§ Conversion Factor (CF):−2017 CF = $75.001−Pass-Through x 1.0020*−Wage Index x 0.9999−Cancer Hospital x 1.0003−Update Factor x 1.0175−2018 CF = $76.483
§ Quality Data:−Reporting Hospital CF = $76.483.−Non-reporting Hospital CF = $74.953
§ CMS estimates:−Volume neutral spending ↑ 1.9% (including Cancer, Children’s and
Community Mental Health Centers) and $897 million for all facilities.− Including changes in enrollment, utilization, case-mix, CMS says spending
will ↑ $5.7 billion.
* CMS has indicated that pass-through adjustment in the rule is incorrect and should be 1.0020, not 1.0022.

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.12
OPPS Proposed Rule: Wage Index
§ Wage Index – Generally, prior policies continued without change in 2018.– Adopts the proposed fiscal year IPPS post-classified wage index as the
OPPS calendar year wage index for adjusting the OPPS standard payment amounts for labor market differences.
– Retains OPPS labor-related share of 60%.– Continues Frontier State wage index floor of 1.00.– Continues to allow non-IPPS hospitals paid under the OPPS to qualify for
the out-migration wage adjustment if in a “Section 505” out-migration county.
– Imputed Floor: proposes to let the imputed floor for all-urban states (NJ, DE, RI) expire at the end of 2017

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.13
OPPS Proposed Rule: Special Case Hospitals
§ Rural Adjustment– Proposes to continue a budget neutral 7.1% payment increase for rural Sole
Community Hospital (including Essential Access Community Hospital) services, excluding separately payable drugs and biologicals, devices paid under the pass-through payment policy, and items paid at charges reduced to costs.
§ Cancer Hospitals– Continue to provide additional payments to 11 cancer hospitals sufficient to
bring each hospital’s payment-to-cost ratio (PCR) up to the level of the PCR for all other hospitals–less 1.0 percentage point per the 21st Century Cures Act. (CMS makes an aggregate payment at cost report settlement rather than a claims-based adjustment).
– 1.0003 OPPS budget neutrality conversion factor adjustment for the cancer hospital adjustment.
– Proposed rule target PCR of 0.89 rather than 0.90 (including the 1.0% reduction for the 21st Century Cures Act) to determine the CY 2018 cancer hospital payment adjustment to be paid at cost report settlement, using the latest available cost data. Estimated adjustment range from 8.8% to 76.9%.

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.14
OPPS Proposed Rule: Outliers
§ Outliers – No Methodological Changes for 2018:– The OPPS makes outlier payments on a service-by-service basis when the
cost of a service exceeds the outlier threshold. – The proposed rule continues to set aside 1.0 percent of the estimated
aggregate total payments under the OPPS for outlier payments– To qualify for outlier payments in 2018, a service or procedure cost must
exceed 1.75 times the APC payment amount and also exceed the APC payment rate plus a $4,325 fixed-dollar threshold (compared to $3,825 in 2017).
– Payment equals 50 percent of the amount by which the cost of furnishing the service exceeds 1.75 times the APC payment amount when both thresholds are met.
– Allocates 0.0027% of the 1% outlier pool to Community Mental Health Centers for partial hospitalization program outlier payments.
– The inflation adjustment factors for cost-to-charge ratios and charges are the same as were used for the FY 2018 IPPS proposed rule.
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.15
OPPS Proposed Rule: CMS’ 340B Proposal
• Effective January 1, 2018, CMS proposes Medicare payments for all separately-payable Part B drugs purchased under the 340B program dispensed to hospital outpatients would be the average sales price (ASP) minus 22.5 percent.
• Proposal does not include:• “Pass Through” drugs• Vaccines• Drugs identified with a to-be-established modifier indicating that
the drug was not purchased at the 340B price• Proposal is a hybrid of previous recommendations made by
MedPAC and HHS-OIG.

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.16
OPPS Proposed Rule: Implications of 340B Proposal
• CMS estimates that the proposed payment reduction will result in $900 million in savings in Medicare payment for Part B outpatient hospital drugs.
• Would be implemented budget neutral by increasing payment for all other services paid under OPPS
• CMS estimates the redistribution in payments would result in an increase in other payments under OPPS by approximately 1.4 percent
• CMS solicits comments on other uses for the savings:• Increase payments for specific services paid under the OPPS;• Increase payments generally under Part B for services not paid
under the OPPS• Whether and how the offsetting increase could be targeted to
hospitals that treat a large share of indigent or uninsured patients.• Whether redistributing savings would result in unnecessary
increases in the volume of OPPS services.

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.17
OPPS Proposed Rule: Packaged Items & Services
• CY 2015 OPPS final rule began conditionally packaging services assigned to APCs with a geometric mean cost of $100 or less prior to packaging. Drug administration was not included.
• Conditionally packages payment for low-cost drug administration services starting CY 2018, except for Medicare Part B vaccine administration services. Requests comment on whether to package other drug administration services.
• Solicits comments on the impact of existing packaging policies under the OPPS, including those related to drugs that function as a supply in a diagnostic test or procedure, or in a surgical procedure.

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.18
OPPS Proposed Rule: Packaged Skin Substitutes
• Payment for skin substitutes is packaged into the payment for the associated primary procedure and based on whether they are assigned to either a “high cost group” or a “low cost group.”
• For CY 2018, CMS proposes to continue assigning skin substitutes with a geometric mean unit cost (MUC) or a per day cost (PDC) that exceeds either the MUC threshold or the PDC threshold to the high cost group.
• CMS proposes that skin substitutes not exceeding either the CY 2018 MUC or PDC threshold for CY 2018 but were assigned to the high cost group in CY 2017 will be assigned to the high cost group for CY 2018. This is a new policy proposal.

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.19
OPPS Proposed Rule: Inpatient Only List
• Proposes to continue to use the same methodology to decide whether to remove a procedure from the inpatient-only list.
• Total Knee Arthroplasty: Propose to remove total knee arthroplasty (TKA) from the inpatient only list in CY 2018, allowing these procedures to be performed in hospital outpatient departments.
• If finalized, Recovery Audit Contractors will be prohibited from conducting patient status reviews for two years on TKA procedures performed in the inpatient setting.
• Notes that removing TKA from inpatient only list allows Medicare to pay when performed outpatient but does not require TKA to be performed outpatient if not appropriate for the patient.
• Comments requested on whether total hip arthroplasty (THA) should be removed from the inpatient only list.
• The rule does not add TKA to the ambulatory surgical center (ASC) covered procedure list, though it solicits comments on whether TKA and THA meet the criteria to be included as an ASC covered procedure.
• Removes CPT code 55866 (laparoscopy, surgical prostatectomy, retropubic radical, including nerve sparing, includes robotic assistance, when performed) from the inpatient only list for CY 2018
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.20
OPPS Proposed Rule: Other Proposed Policies
• CMS proposes to reinstate the non-enforcement of direct supervision requirements for outpatient therapeutic services or critical access hospitals (CAHs) and small rural hospitals having 100 or fewer beds for CYs 2018 and 2019. The enforcement moratorium is designed to give affected hospitals more time to comply with the requirements.
• CMS does not propose but requests comments on potential modifications to the laboratory date of service policy to allow labs to bill Medicare directly for molecular pathology tests and/or advanced diagnostic laboratory tests excluded from the OPPS packaging policy ordered less than two weeks following the date of a patient's discharge from the hospital. Proposed rule indicates that CMS may finalize policy for 2018 even though not proposed.
• Proposes phased in reduction in payments for x-rays taken using CRT as required by statute during CYs 2018 through 2022 by 7 percent, and for services furnished during CY 2023 or a subsequent year by 10 percent. A new modifier would be reported on claims to identify those HCPCS codes that describe X-rays taken using CRT beginning January 1, 2018.
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.21
Hospital Outpatient Quality Reporting ProgramData Collection Summary
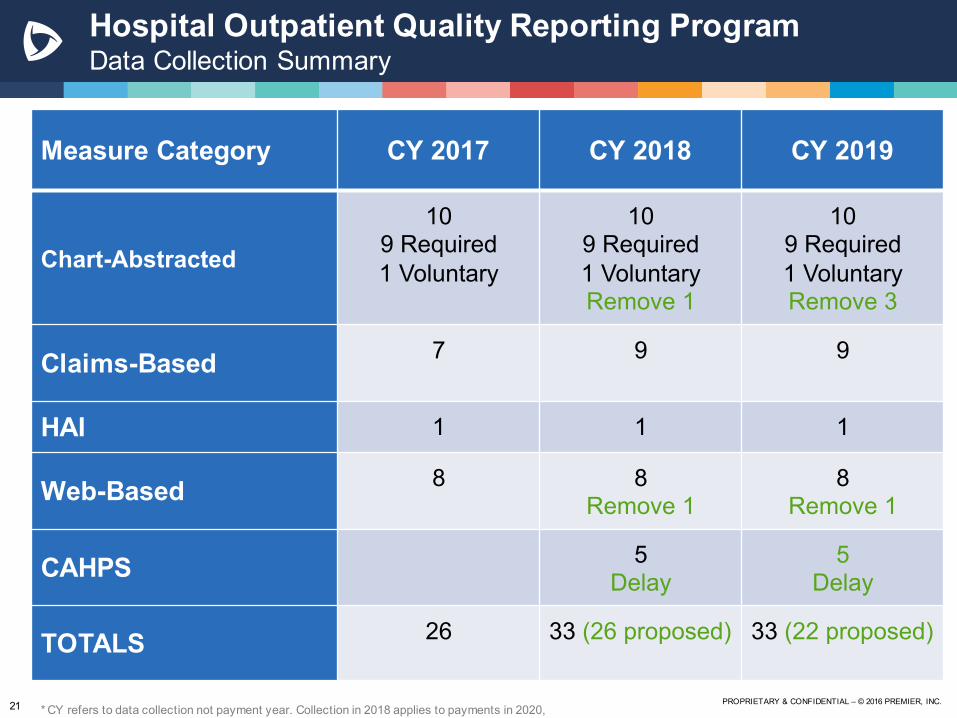
Measure Category CY 2017 CY 2018 CY 2019
Chart-Abstracted
109 Required1 Voluntary
109 Required1 VoluntaryRemove 1
109 Required1 VoluntaryRemove 3
Claims-Based 7 9 9
HAI 1 1 1
Web-Based 8 8Remove 1
8Remove 1
CAHPS 5Delay
5Delay
TOTALS 26 33 (26 proposed) 33 (22 proposed)
* CY refers to data collection not payment year. Collection in 2018 applies to payments in 2020,
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.22
OQR: Proposed Changes
• Remove 2 measures for CY 2018 reporting/2020 payment• OP-21: Median Time to Pain Management for Long Bone Fracture• OP-26: Hospital Outpatient Volume Data on Selected Outpatient Surgical
Procedures• Remove 4 measures for CY 2019 reporting/2021 payment
• OP-1: Median Time to Fibrinolysis • OP-4: Aspirin at Arrival• OP-20: Door to Diagnostic Evaluation by a Qualified Medical Professional• OP-25: Safe Surgery Checklist
• Delay OAS CAHPS• Future Measure Topics
• OP-2: Fibrinolytic Therapy Received Within 30 Minutes of Emergency Department Arrival as an eCQM
• Accounting for Social Risk Factors• Public Display
• Include OP-18c Median Time from ED Arrival to ED Departure for Discharged ED strata for psychiatric/mental health patients

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.23
Proposed CY 2018 Ambulatory Surgical Center Payment Updates
§ Payment increase = 1.9% for ASC reporting quality data, 0.1% for other ASCs
§ Consumer price index = 2.3%
§ Productivity adjustment = -0.4%
§ Net Update = 1.9%
§ Wage Index Budget Neutrality = 1.0004
§ Conversion factor of $45.876 ($44.976 for ASCs that do not submit quality data).
§ Estimated increase in aggregate ASC payments of $155 million over CY 2017.

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.24
ASCQR: Proposed Changes
• Remove 3 measures for CY 2017 reporting/2019 payment• ASC-5: Prophylactic Intravenous (IV) Antibiotic Timing • ASC-6: Safe Surgery Checklist Use• ASC-7: ASC Facility Volume Data on Selected Procedures
• Delay OAS CAHPS• New measure for CY 2019 reporting/2021 payment
• ASC-16: Toxic Anterior Segment Syndrome (TASS) measure• Two new measures for CY 2020 reporting/2022 payment
• ASC-17: Hospital Visits after Orthopedic ASC Procedures • ASC-18: Hospital Visits after Urology ASC Procedures
• Future Considerations• Ambulatory Breast Procedure Surgical Site Infection outcome
measure (NQF #3015)• Accounting for social risk factors

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.25
Medicare Physician Fee Schedule (MPFS)

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.26
MPFS Proposed Rule
§ Released July 13, published on July 21, Federal Register
§ Conversion Factor $35.9903 (2017 CF $35.8887)– Update Factor is 0.50 percent– Budget Neutrality Adjustment is -0.03 percent– Misvalued Codes Target Recapture Amount is -0.19 percent
§ Anesthesia CF is $22.0353 (2016 CF $ 22.0454)
§ Specialty-specific impact on allowed charges– Greatest Positive Impact: Clinical social workers (+3 percent), clinical
psychologists (+2)– Greatest Negative Impact: Diagnostic testing facilities (-6 percent),
allergy/immunology (-3)– -2 percent: cardiac surgery, cardiology, independent lab, oral/maxillofacial
surgery, otolaryngology, pathology and vascular surgery
§ Comments due September 11, 2017
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.27
PFS: Medicare Telehealth Services
• Add 3 codes that are similar to services currently on telehealth services list
• G0296: Counseling visit to discuss the need for lung cancer screening using low dose computed tomography (LDCT)
• 90839 and 90840: Psychotherapy for crisis; first 60 min• Add 4 add-on codes
• 90875: Interactive complexity• 96160 and 96161: Administration of patient-focused health risk
assessment instrument and Administration of caregiver-focused health risk assessment instrument
• G0506: Comprehensive assessment or/and care planning for patients requiring chronic care management services
• No longer require GT modifier on claims since telehealth POS code is required
• Seek comment on separate payment for codes that describe remote patient monitoring (99091) and codes for extensive use of communications technology (99090)
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.28
PFS: Outpatient Provider-Based Departments -Background
§ Section 603 of the Bipartisan Budget Act of 2015, enacted on November 2, 2015, imposed new payment rules for certain off-campus outpatient provider-based departments (PBDs).
§ Beginning January 1, 2017, non-excepted items and services furnished by non-excepted off-campus PBDs will no longer be paid under the OPPS; they will be paid under another Medicare Part B payment system not specified by the law.
§ The law does not apply to on-campus PBDs (main provider).
§ The law provides exceptions for:– PBDs within 250 yards of a remote location (straight line measurement from
any point of the inpatient hospital at the remote location).– PBDs billing prior to November 2, 2015.– Services furnished in a dedicated emergency department (ED). CMS
clarified in rulemaking that exception will apply all services in a dedicated ED, not just ED visits.
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.29
PFS: Outpatient Provider-Based Departments
• CY 2017 OPPS Final Rule– CMS issued Interim Final Rule with Comment (IFC) to make payment to
hospitals at a special Medicare Physician Fee Schedule (MPFS) rate for the non-excepted off-campus PBDs at 50% of OPPS rates for 2017, the PFS Relativity Adjuster
– Billed on an institutional claim with new claim line modifier “PN”– OPPS payment policies (e.g. C-APCs, OPPS packaging) will apply– Partial Hospitalization will be paid at CMHC rate.– Services paid under other fee schedules (MPFS, Clinical Laboratory Fee
Schedule and Ambulance Fee Schedule) will continue to be paid the same as currently without a reduction.
– Separately payable drugs and biologicals will be paid at ASP + 6%.– OPPS geographic adjustor (wage index) and OPPS supervision rules will
apply• CY 2018 MPFS Proposed Rule
– Adjust the PFS Relativity Adjuster to 25% of the OPPS rates– Seek comment on setting adjuster to 40%

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.30
PFS: Public Comment Solicitations
• Evaluation and Management Guidelines• Reducing burden and unnecessary documentation, relying on
electronic health technology• Extending practitioner autonomy to determine volume of E/M
services• Revision design that does not purposefully or inadvertently
provide inappropriate performance or payment advantages to subsets of physicians
• Care Management Services• Expansion beyond office visits• Reducing burden by harmonizing CMS requirements and CPT
guidance• Addressing health disparities and disabled patients
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.31
PFS: RHC/FQHC Care Management
• Proposing to create general care management codes and psychiatric collaborative care model codes for RHCs/FQHCs
• Codes and payment policies for these services finalized in CY 2017 MPFS don’t apply to RHCs and FQHCs
• General care management codes• CPT code 99490 – 20 minutes or more of CCM services• CPT code 99487 – at least 60 minutes of complex CCM services• HCPCS code G0507 – 20 minutes or more of BHI services• Same requirements as for CCM services; code can be billed
once per month per beneficiary• Psychiatric Collaborative Care Model
• G0502 – 70 minutes or more of initial psychiatric CoCM services and
• G0503 – 60 minutes or more of subsequent psychiatric CoCM services

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.32
PFS: Public Comment Solicitations
• Clinical Laboratory Fee Schedule• Beginning January 1, 2018 CLFS payment based on weighted
median of private payor rates; based on information collected during CMS data collection period
• Seek feedback on the CMS data reporting system• Biosimilars
• CY 2016 final rule indicated that the payment amount for a biosimilar biological product is based on the average sales price (ASP) of all National Drug Codes (NDCs) assigned to the biosimilar biological products included within the same billing and payment code
• Comments sought on:• New or updated information on the current biosimilar payment policy• Data on how individual HCPCS codes could impact the biosimilar
market• Other policies to foster competition and increase access
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.33
PFS: Appropriate Use Criteria (AUC) for Advanced Diagnostic Imaging
§ PAMA directed CMS to establish a program to promote the use of AUC for advanced diagnostic imaging services
§ CY 2016 rulemaking activities:– Advanced diagnostic imaging includes MRI, CT, PET, nuclear
medicine and other services identified by stakeholders– Provider led entities(PLE to develop AUC –identified 11 qualified
PLEs)
§ CY 2017 rulemaking activities:– Requirements and processes for specification of qualified clinical
decision support mechanisms(CDSMs) – The initial list of priority clinical areas: Coronary artery disease,
suspected pulmonary emboli, headache, hip pain, low back pain, shoulder pain, cancer of the lung, cervical or neck pain without change
– Exceptions to required consultation with AUCs

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.34
PFS: AUC for Diagnostic Imaging: CY 2018 Proposals
• Consultation with AUC beginning January 1, 2019; voluntary reporting beginning July 2018
• Ordering professional must consult with AUC through qualified CDSM• Furnishing professional must report the following on claims:
• CDSM consulted by ordering professional• If/not service adheres to AUC or if AUC exist for the service• NPI of ordering professional
• Codes to implement reporting requirements• HCPCS level 3 codes
• Modifiers to describe adherence to AUC, exceptions• G-code for every CDSM and generic code for new CDSMs
• Other considerations• QPP rule proposed to include AUC consultation as an improvement
activity; seek comment on development of quality measure• Align hardship exemption with those who are granted exception for
MIPS-ACI

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.35
PQRS/Value Modifier Updates
• PQRS: CY 2018 payment/ 2016 performance• Reduce required measures from 9 measures/3 NQF domains to 6
measures in any domain• Eliminate outcome or high priority measure requirement• Eliminate cross-cutting measure requirement• Eliminate CAHPS requirement for groups of 100 or more• Do not report VM cost and quality tiers
• Value Modifier: CY 2018 payment/ 2016 performance• If a successful PQRS reporter, held harmless from VM downward
adjustment• Reduce automatic downward adjustment for non reporters
• Groups with 10+: From -4% to -2%• Solo and groups up to 9: From -2% to -1%
• Reduce the maximum upward adjustment• Groups with 10+: From 4.0x to 2.0x• Solo and groups up to 9: From 2.0x to 1.0x

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.36
PFS: Medicare Shared Savings Program
• Reducing Application Burden• SNF 3-day waiver: remove narrative description describing financial relationships,
remove requirement to demonstrate affiliated SNFs have 3-star rating• Remove several aspects from the initial application and note that ACOs must
furnish upon CMS request• Compliance with ACO Participant TIN Exclusivity
• If CMS finds that during a benchmark or performance year, an ACO participant bills for services used in assignment under more than once ACO, CMS will not consider any services billed through that TIN during the relevant performance year when assigning beneficiaries for the applicable benchmark or performance year
• Provider remains on participant list but ACO must reconcile prior to recertification of ACO participant list
• Beneficiary Identifiable Payment Made under a Demonstration, Pilot or Time-Limited Program
• Benchmarks for agreements prior to 2018: all individually beneficiary identifiable payments, including interim payments, made under a demonstration, pilot, or time limited program are included
• Benchmarks for agreements 2018 and beyond/ 2018 performance year for agreement periods beginning 2015-2018: only final individually beneficiary identifiable payments made under a demonstration, pilot or time limited program would be included

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.37
PFS: Medicare Shared Savings Program
• Beneficiary Assignment Changes• RHC/FQHC assignment
• Eliminate need to attest to physicians who provide direct patient primary care in the ACO participant FQHC or RHC
• Treat services reported on FQHC or RHC claims as primary care services in the beneficiary assignment methodology for ACOs
• Primary care services definition• Add 3 chronic care management services: 99487, 99489 and G0506• Add 4 behavioral health integration services: G0502, G0503, G0504 and
G0507
• Quality Measures• Allow CMS to redesignate measures as pay for reporting when
substantive changes occur under the QPP• Validation Process
• Change audit threshold from 90% match rate to 80% match rate• Quality score adjustment if match rate is not reached: 1 percent for each
percentage point away from match rate

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.38
PFS: Patient Relationship Codes
• Required by MACRA, CMS sought comments through two RFIs
• Require reporting through modifiers beginning January 1, 2018
• Modifier will not be a condition of payment during an initial voluntary period
• Voluntary period was not specified
Number Proposed HCPCS Modifier Patient Relationship Categories
1x X1 Continuous/Broad Services
2x X2 Continuous/Focused Services
3x X3 Episodic/Broad Services
4x X4 Episodic/Focused Services
5x X5Only as Ordered by Another Clinician

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.39
Important Links
OPPS:Premier Detailed SummaryProposed Rule CMS Press Release CMS Fact Sheet
MPFS:Premier Detailed Summary Proposed RuleCMS Press Release CMS Fact Sheet

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.
Danielle Lloyd, M.P.H. VP, policy and advocacy Deputy director, D.C. office, [email protected]
Aisha Pittman, M.P.H. Senior director, quality policy and [email protected]
Kellie Webb, M.B.A. Director, payment policy and [email protected]

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.41
Transforming Healthcare TOGETHER

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.42
APPENDIX

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.43
OPPS: Overview of the 340B Program
• Congress created the 340B program in 1992 to help uninsured indigent patients gain better access to prescription drugs.
• The program is intended to reduce outpatient drug costs for certain types of health care facilities serving large numbers of uninsured indigent patients.
• The law requires pharmaceutical manufacturers to give statutorily specific discounts for drugs dispensed to outpatients of qualifying entities
• Administered by Health Resources and Services Administration (HRSA)
• Dramatically expanded due to ACA (583 participating hospitals in 2005 to 2,140 in 2014) (Some of the growth since 2010 has been in critical access hospitals that are paid differently than other hospitals for outpatient drugs.)

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.44
340B Program “Covered Entity” Eligibility
• Federal health care grant recipients• Certain disproportionate share hospitals (DSH), children’s
hospitals, cancer hospitals, critical access hospitals, sole community hospitals and rural referral centers
• All 340B-eligible hospitals except critical access hospitals must have a Medicare DSH adjustment percentage either greater than 11.75 percent (for DSH hospitals, Children’s hospitals and cancer hospitals) or greater than or equal to 8 percent (for rural referral centers and sole community hospitals).
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.45
OPPS: 340B Ceiling Price
• Maximum price a drug manufacturer can charge a covered entity for a drug
• The 340B ceiling price is statutorily defined as the Average Manufacturer Price (AMP) reduced by the rebate percentage, Unit Rebate Amount (URA)
• The URA is the greater of 23.1% of the Average Manufacturer Price (AMP) per unit or the difference between the AMP and the best price per unit and adjusted by the Consumer Price Index- Urban (CPI-U) based on launch data and current quarter AMP.

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.46
OQR: OAS CAHPS Measures
§ Composite Survey-Based Measures– The proportion of “top box” (yes or yes definitely) responses for
each question are averaged– OP-37a: OAS CAHPS—About Facilities and Staff– OP-37b: OAS CAHPS—Communication About Procedure– OP-37c: OAS CAHPS—Preparation for Discharge and Recovery
§ Global Survey-Based Measures– The proportion of “high-value” (9-10 or definitely yes) responses– OP-37d: OAS CAHPS—Overall Rating of Facility– OP-37e: OAS CAHPS—Recommendation of Facility
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.47
AUC: Implementation
§ Definition of CDSM: interactive, electronic tool that communicates AUC information and assists the clinician in making the most appropriate diagnostic decision– Can be free-standing or incorporated into EHR
§ Requirements for CDSM are not prescriptive about specific IT standards and functions on functionality– Applications from publication of final rule until March 1, 2017
(in later years, deadline is January 1 of each year)
§ Exceptions – Exception for “emergency medical condition” and Part A payment– EHR Incentive Program hardship– CMS discusses MAC granting hardship exemptions or establishing another
process for self-attestation of significant hardship for anesthesiology, radiology and pathology
PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.48
AUC: ImplementationCDSM Qualifications and Requirements
1. Make available specified applicable AUC and its related supporting documentation.
2. Identify the appropriate use criterion consulted if the CDSM makes available more than one criterion relevant to a consultation for a patient’s specific clinical scenario.
3. Make available, at a minimum, specified applicable AUC that reasonably address common and important clinical scenarios within all finalized priority clinical areas.
4. Be able to incorporate specified applicable AUC from more than one qualified PLE.
5. Determine, for each consultation, the extent to which the applicable imaging service is consistent with specified applicable AUC.
6. Generate and provide a certification or documentation at the time of order that documents:– Which qualified CDSM was consulted;– The name and national provider identifier (NPI) of the ordering professional that consulted the CDSM;– Whether the service ordered adhered to or did not adhere to specified applicable AUC; or whether the specified applicable AUC consulted was not
applicable to the service ordered; and– Include a unique consultation identifier generated by the CDSM.
7. Modifications to AUC within the CDSM must comply with the following requirements:– Make available updated AUC content within 12 months from the date the qualified PLE updates AUC;– Have a protocol in place to expeditiously remove AUC determined by the qualified PLE to be potentially dangerous to patients and/or harmful if followed; and
– Make available for consultation within 12 months of a priority clinical area being finalized by CMS specified applicable AUC that reasonably address common and important clinical scenarios within any new priority clinical areas.
8. Meet privacy and security standards under applicable provisions of law.
9. Provide to the ordering professional aggregate feedback regarding their consultations with specified applicable AUC in the form of an electronic report on at least an annual basis.
10. Maintain electronic storage of clinical, administrative, and demographic information of each unique consultation for a minimum of 6 years.
11. Comply with modification(s) to any requirements made through rulemaking within 12 months of the effective date of the modification.
12. Notify ordering professionals upon de-qualification.

PROPRIETARY & CONFIDENTIAL – © 2016 PREMIER, INC.49
PFS: VM Current and Proposed Quality Tiering
Groups 10+
Cost/Quality Low Quality Average Quality High QualityVM Payment Adjustment
Current Proposed Current Proposed Current Proposed
Low Cost +0.0% +0.0% +2.0x* +1.0x* +4.0x* +2.0x*
Average Cost -2.0% +0.0% +0.0% +0.0% +2.0x* +1.0x*
High Cost -4.0% +0.0% -2.0% +0.0% +0.0% +0.0%
Solo and Groups 2-9
Cost/Quality Low Quality Average Quality High QualityVM Payment Adjustment
Current Proposed Current Proposed Current Proposed
Low Cost +0.0% +0.0% +1.0x* +1.0x* +2.0x* +2.0x*
Average Cost -1.0% +0.0% +0.0% +0.0% +1.0x* +1.0x*
High Cost -2.0% +0.0% -1.0% +0.0% +0.0% +0.0%
Non-physician Groups or Solo PractitionersCost/Quality Low Quality Average Quality High Quality
VM Payment Adjustment Current Proposed Current Proposed
Current Proposed
Low Cost +0.0% +0.0% +1.0x* +1.0x* +2.0x* +2.0x*Average Cost +0.0% +0.0% +0.0% +0.0% +1.0x* +1.0x*
High Cost +0.0% +0.0% +0.0% +0.0% +0.0% +0.0%