week 3: hiv/aids in africa takashi yamano development problems in africa spring 2006
TRANSCRIPT
FASIDFASID
Week 3: HIV/AIDS in Africa
Takashi Yamano
Development Problems in Africa
Spring 2006

FASIDFASID
ContentsEconomics of Communicable
Diseases– Market Failures
HIV/AIDS in Africa– Infections and Prevalence– Preventions– Treatments– Vaccines

FASIDFASID
Economics of Communicable Diseases
Background on Communicable DiseasesEvery year, 1.1 million people, mostly children and
pregnant women, die of malaria (90% of them are in Africa)
Every year, 1.9 million people die of tuberculosis (98% in developing countries, many in Africa).
In 2003, 2.9 million people died of AIDS (total of over 20 million since 1981). About 38 million people are living with HIV.
Kremer (2000a) “Creating Markets for New Vaccines Part I”

FASIDFASID
Deaths from Diseases for which Vaccines are Needed
Diseases Deaths (millions)
%
AIDS 2.3 27.5
Tuberculosis 1.5 18.0
Malaria 1.1 13.3
Pneumococcus 1.1 13.2
Rotavirus 0.8 9.6
Shigella 0.6 7.2
E.Coli 0.5 6.0
Others - -
Total 8.3 100Kremer (2000b) “Creating Markets for New Vaccines Part II”

FASIDFASID
Failures in the Market of Vaccines
Under Consumption of Vaccines Individuals who take vaccines not only benefit
themselves, but also break the chain of disease transmission. They do not, however, such external benefits into account.
The chief beneficiaries of vaccines are often children. Individuals seem much more willing to pay for
treatment than prevention.
Kremer (2000b) “Creating Markets for New Vaccines Part I”

FASIDFASID
Monopoly Market
A
B
E
C
D
Monopoly Price (MP)
Manufacturing Cost (MC)
Monopoly Profit
Alternatively: The government pay A + B + C + D to the firm, taxing Group X just below MP and Group Y just over MC. >> everyone is better off !
Willingness to pay
Fraction of population vaccinated Group A
01
Group B
Kremer (2000b) “Creating Markets for New Vaccines Part I”

FASIDFASID
Social vs. Private Returns Private returns to curing the disease is based on the income saved by
taking drugs or vaccines.
But because infectious diseases spread among people, the social returns have to take into account the saved incomes of potential patients who would be infected by the disease from the particular patient.
Thus, Social Returns of a communicable disease is higher than the private returns. Negative Externality!
Implication: medical costs of communicable diseases should be subsidized. Earlier the interventions are, the lower the costs.
Kremer (2000b) “Creating Markets for New Vaccines Part I”

FASIDFASID
Understanding HIV and AIDS1981 Reported in The Morbidity and M
ortality Weekly Report, CDC1983 The HIV is identified by Luc Montagnier, fol
lowed by Robert Gallo (for details see And the Band Played On by
Randy Shilts or video)
2006 25 years after the first report about AIDS
HIV: Human Immunodeficiency Virus AIDS: Acquired Immunodeficiency Syndrome

FASIDFASID
How the virus Works: Infection• HIV attacks a particular set of sells in the human
immune system known as CD4 cells. CD4 cells • organize the body’s overall immune response, and• engulf foreign invaders and ensure that the body’s immune system
will recognize them.
• HIV enters CD4 cells and makes copies of themselves, destroying the CD4 cells.
• At infection, the immune system responses and the vital load is high, “the window period.” A person is highly infectious and can not be detected for HIV because of high levels of CD4 cells.
>> The more people there are in the early stage of infection, the greater the chance of effective transmission between people.

FASIDFASID
Barnett and Whiteside (2002) AIDS in the 21st century

FASIDFASID
Probability of HIV-1 infection per exposure
Infection per 1000 exposure
Female-to-Male, unprotected sex 0.33 – 1.0
Male-to-female, unprotected sex 1 – 2
Male-to-male, unprotected anal sex 5 – 30
Needle stick 3
Mother-to-child transmission 130 – 480
Exposure to contaminated blood products
900 – 1,000
World Bank (1997) Confronting AIDS

FASIDFASID
Epidemiology 101• An Epidemic is a rate of disease that reaches unexpectedly
high levels, affecting a large number of people in a relatively short time.
• A disease is considered as Endemic if it is continuously present in a population (e.g., malaria).
• A pandemic describes epidemics of world wide proportions (e.g., influenza in 1918 or HIV/AIDS).
• Incidence is the number of new infections which occur over a time period.
• Prevalence is the absolute number of infected people in a population.

FASIDFASID
Barnett and Whiteside (2002) AIDS in the 21st century

FASIDFASID
Prevalence: A Global Overview
Region Number of adults (15-49) living with HIV
(millions)
HIV prevalence rate among
adults (15-49)
Sub-Saharan Africa 23 7.5
East Asia 0.9 0.1
South & SE Asia 6.3 0.6
E. Europe & C. Asia 1.3 0.6
Western Europe 0.57 0.3
N. Africa & Middle East
0.46 0.2
North America 0.99 0.6
Caribbean 0.41 2.3
Latin America 1.6 0.6
Total 36 1.1Source: UNAIDS (2004) Report on the global AIDS Epidemic

FASIDFASID
Source: UNAIDS (2004) Report on the global AIDS Epidemic
HIV Prevalence: Urban vs. Rural

FASIDFASID
Source: UNAIDS (2004) Report on the global AIDS Epidemic
Changes in HIV: Men vs. Women

FASIDFASID
HIV Prevalence in Kenya

FASIDFASID
Why in Africa?– Largely unknown– Known or the conventional hypothesis
• It originated from Central Africa• More than 90% of adult HIV infection is due to
(hetero-) sexual transmission• Economic development and globalization helped:
the virus spreads because people spreads
Examples: Drivers, Migration workers, prostitutes• Poor health care systems exaggerated the epidemic• Sexually Transmitted Infections increase infections
per exposure

FASIDFASID
Source: UNAIDS (2004) Report on the global AIDS Epidemic

FASIDFASID
Source: UNAIDS (2004) Report on the global AIDS Epidemic
Life expectancy in selected countries

FASIDFASID Source: UNAIDS (2004) Report on the global AIDS Epidemic
Demographic Outlook in South Africa

FASIDFASID
Source: UNAIDS (2004) Report on the global AIDS Epidemic

FASIDFASID
PreventionTarget Groups• In low-prevalence settings: target key
population groups (e.g., sex workers and clients, injecting drug users, men who have sex with men)
• In high-prevalence settings: key groups and the total population
Prevention efforts should be accompanied with universal access to treatment, impact and vulnerability-reduction measures.

FASIDFASID
PreventionProjects• AIDS education and awareness• Behavior change programs• Condom promotion• Voluntary counsel and testing• Preventing and treating STIs• Prevent mother-to-child transmission• Harm reduction programs for drug users• Safe blood supply• Infection control in health care settings

FASIDFASID
PreventionABCs in HIV preventions• A means Abstinence: not engaging in sexual
intercourse or delaying sexual initiation.• B means Being Faithful: being faithful to one’s
partner or reducing the number of sexual partners.
• C means Condom use: condoms reduce the risk of HIV transmission.
FASIDFASID
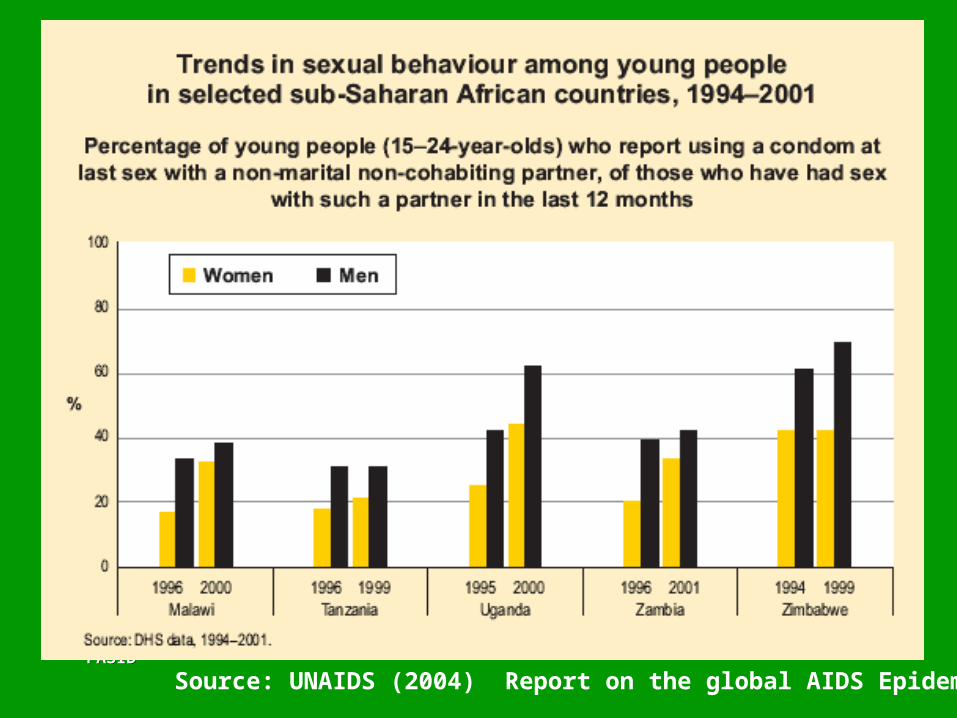
Source: UNAIDS (2004) Report on the global AIDS Epidemic
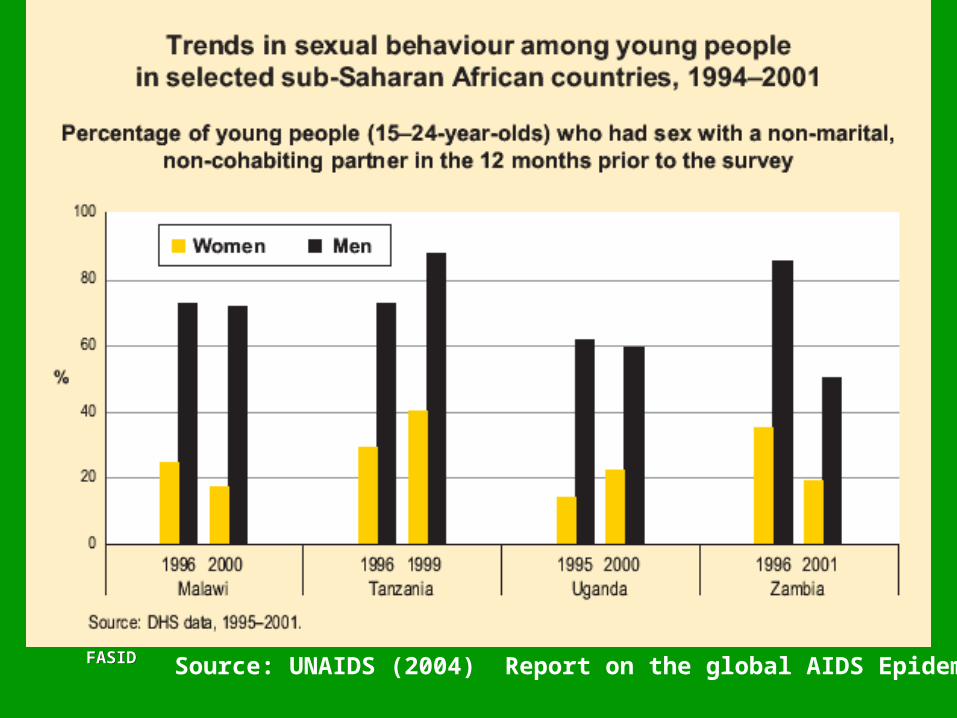
FASIDFASID Source: UNAIDS (2004) Report on the global AIDS Epidemic

FASIDFASID
The Success Story: UgandaThe national HIV prevalence rate declined from 15% in 199a t
o 5% in 2001Why?
– High-level political support– Behavior Change Communication (BCC) interventions r
eached the general population and key target groups– Early and significant mobilization of Ugandan religious l
eaders– A decrease in multiple sexual partnerships– Use of condoms
Source: Hogle, et al., USAID, 2002

FASIDFASID
Treatment• Five to six million people in low-and middle-income
countries need antiretroviral treatment immediately. But only 0.4 million (7%) in 2003 receive it (WHO).
• The price has come down from over $10,000 to $300 per person per year.
• The 3 by 5 Initiative: Treating 3 million people by 2005 (WHO)
– This initiative did not achieve the target (3 million) but helped the triple the number of people with access to drugs from 0.4 to 1.3 million people in just two years.

FASIDFASID Source: UNAIDS (2004) Report on the global AIDS Epidemic
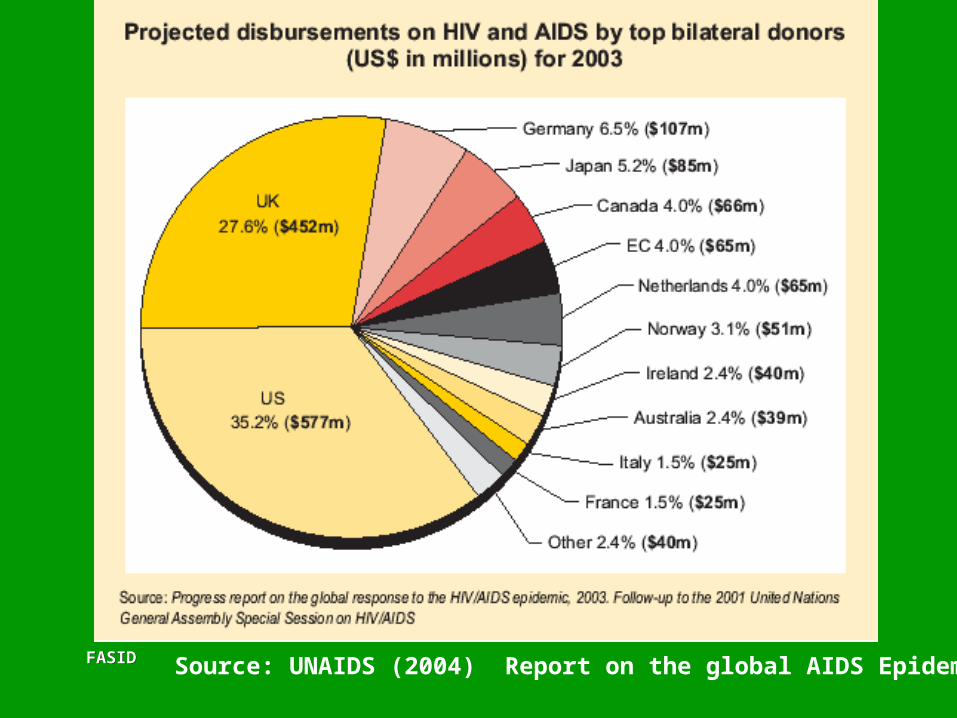
FASIDFASID Source: UNAIDS (2004) Report on the global AIDS Epidemic