week 10 peds/gero
TRANSCRIPT

Peds/GeroWeek 10

Neonatal and Pediatric Emergencies

Pregnancy• If pregnancy is suspected or
imminent:• ALS• Support ABCsCommon Complications
Ectopic Pregnancy: Occurs when a fertilized ovum is implanted outside of the endometrial lining of the uterine wall. ● As the ovum begins to develop into an embryo and eventually into a fetus, it will stretch the
fallopian tube, which can result in rupture and massive hemorrhage.● Prompt transport is a high priority.
Preeclampsia & Eclampsia: ● A BP greater than 140/90 mm/Hg is considered abnormal for the pregnant patient. If the
patient is found to have elevated blood pressure, protein in the urine, edema and is beyond 20 weeks of gestation, she is diagnosed with preeclampsia.
● Eclampsia is a severe complication of preeclampsia. HTN results in a seizure. Eclampsia is defined as resulting seizure occurring during pregnancy when there is no other known cause
Pregnancy• If pregnancy is suspected or
imminent:• ALS• Support ABCsCommon Complications
Placenta Abruptio:● Premature separation of the implanted placenta from the uterine wall● Causes hemorrhage on inside● Painful vaginal bleeding, but not always present● Uterine contractions
Placenta Previa: ● Placenta overlaps and implants on the cervix, covering the cervical opening● Bleeding but little pain.● Blood leaking from placenta itself.

Vital Signs
- 15 to 30 second visual assessment
- Appearance- Check level of consciousness, interactiveness, and muscle tone- TICLS (tickles): tone, interactiveness, consolability, look or gaze, speech or cry
- Work of Breathing- Signs include tachypnea, abnormal airway sounds (grunting or wheezing), and
retractions of the intercostal muscles or sternum
- Circulation to the Skin- Pallor of the skin and mucous membranes, mottling, and cyanosis may be
indicative of poor perfusion, compensated shock, anemia, or hypoxia
Pediatric Assessment Triangle
- May be caused by foreign objects or infections such as pneumonia, croup, epiglottitis, bronchiolitis, or bacterial tracheitis
- Croup is a viral infection below the level of the vocal cords
- Epiglottitis is a soft tissue infection above the level of the vocal cords- Look for congestion, fever, drooling, and cold symptoms- Lung sounds will resemble a barking seal
- Bronchiolitis is a viral infection that affects newborns and toddlers- Look for signs of dehydration, shortness of breath, and fever
Airway Obstruction
- Asthma attacks may be caused by upper respiratory infection, exercise, exposure to cold air, emotional states, and passive exposure to smoke
- Treatment- Have the patient to sit in a comfortable position- Administer oxygen if needed- Help the patient take their MDI (after you DICCE it)
- Status Asthmaticus- Prolonged asthma attack that is unrelieved- Transport ASAP
- Pediatric patients will stop breathing if they get tired
Asthma
- May be caused by or related to a cold, sore throat, accidental ingestion, direct lung injury, near drowning, or disease related to immunodeficiency
- Signs and symptoms include rapid breathing, grunting, or wheezing- May also be nasal flaring, tachypnea, crackles, hypothermia, fever, unilateral
diminished breath sounds, or accessory muscle use
- Treatment is primarily supportive, monitoring ABC’s
Pneumonia
● Create a safe environment○ Get on the child’s level! Crouch!○ If a child has separation anxiety, let the parent hold them○ Let the child play with your pen light or other materials to help distract them
● Be aware of their stage of life○ Teething → might have eaten something poisonous○ Infant to Preschool Age Children → rapid trauma from toe to head○ School Age Children (6-12) → can assist in the medical history portion
● Do painful procedures at the end
Patient Assessment
● Sliding Scale for Vitals○ Younger means lower BP, higher respirations and pulse○ Sustained labor breathing may lead to…
■ Respiratory failure → hypoxia → bradycardia → cardiac arrest■ Cyanosis is a late sign
● How to Take Vitals○ Respirations
■ Count for 30 seconds if older than 3■ Count rise and fall of the abdomen if younger than 3■ Note effort of breathing
○ Pulse■ Take brachial pulse on infants
Patient Assessment

- Normal vital signs are different for pediatric patients!
- Do CPR on prepubescent children who have a pulse under 60
- Compression to Ventilation Ratio- 1 rescuer → 30:2- 2 rescuers → 15:2
- Rescue Breathing- 1 breath every 3-5 sec
- For an unwitnessed event, if alone, perform two rounds of CPR before calling ALS
CPR

Geriatric Emergencies

Special Considerations of Geriatric Patient● They are likely to have more than one chronic illness.● Chronic health problems can make assessment for acute problems challenging. Signs and
symptoms of chronic illnesses can overlap with acute illness.● Aging can affect a person’s response to illness and injury.● Pain may be diminished or absent.● Social and emotional factors may have a greater influence on health.● The patient may fear losing autonomy and may have financial concerns about the cost of care.● Communication Techniques
1. Always identify yourself2. Speak at eye level3. Locate hearing aids, eye glasses, and dentures4. Speak slowly and distinctly5. Use the patient’s surname6. Be patient7. Preserve dignity8. Explain what you will do before you do it
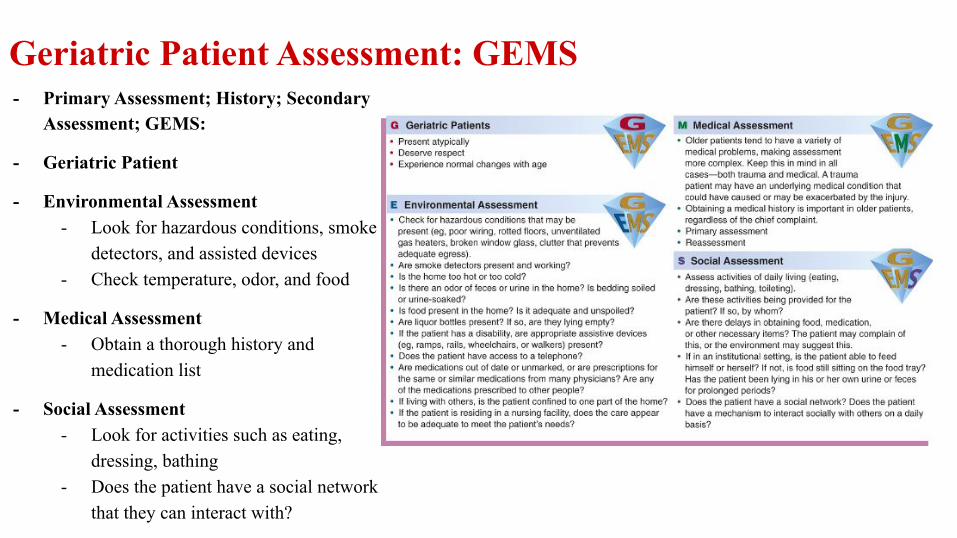
- Primary Assessment; History; Secondary Assessment; GEMS:
- Geriatric Patient
- Environmental Assessment- Look for hazardous conditions, smoke
detectors, and assisted devices- Check temperature, odor, and food
- Medical Assessment- Obtain a thorough history and
medication list
- Social Assessment- Look for activities such as eating,
dressing, bathing- Does the patient have a social network
that they can interact with?
Geriatric Patient Assessment: GEMS

Special Considerations: Treating older patients1. Expect Age-Related Differences
○ Age-related decline in the function of our organs alters our body’s response to illness and injury○ After the age of 30, our organ systems lose 1% of function per year, meaning the body is less able to compensate for shock. ○ With depleted calcium levels, our bones can break easier and simple burns, lacerations and abrasions can cause greater harm since our skin dermis thins
by 20% and perfusion of blood to the extremities decreases. ○ Brain tissue shrinks, a void is created in our cranial vault so head injuries are more lethal and can take days to develop.
2. Pay extra attention to medications○ geriatric patients may forget to take their meds or take the wrong dose. Therefore, along with asking patients about medications, it is also important to
locate the prescription bottles, perform a pill count (if indicated) and bring the medications to the ER with the patient.
3. Look Beyond the Chief Complaint○ Since elderly patients often have multiple medical problems and co-morbidities, don’t stop your detective work at what they believe is their chief
complaint. This complaint may, or may not, be their most life-threatening condition and it is up to you to form your own informed, provider impression.
○ Increase our index of suspicion with elderly patients. Vague and non-specific complaints and traumatic injuries with a low-energy mechanism of injury can have life-altering effects on an older patient.
4. Look for Signs of Elder Abuse and/or Neglect○ If the patient is living alone, they can easily feel isolated, depressed or suicidal at the loss of loved ones, their decreasing health or financial situation. If
you expect elder abuse or depression, it is important to notify proper authorities
5. Identify Communication Barriers and Address Them○ Since senses such as sight and hearing can be dulled in an elderly patient, communication can be difficult
○ Many geriatric patients fear a loss of independence and being moved into a nursing home so they may not want to go to the hospital. However, it is
important to explain your assessment findings, treatment plan and why it is in their best interest that they see a doctor.
○ Once you’ve stabilized the patient and taken care of the medical side of things, don’t be afraid to engage your elderly patient on a personal level. In many
cultures around the world, elderly people are revered for their life experience and wisdom. Don’t be afraid to ask about their life. Suddenly, the person
sitting on the gurney next to you is no longer simply a patient, but a person who’s likely lived an amazing life and will be eager to share it with you.
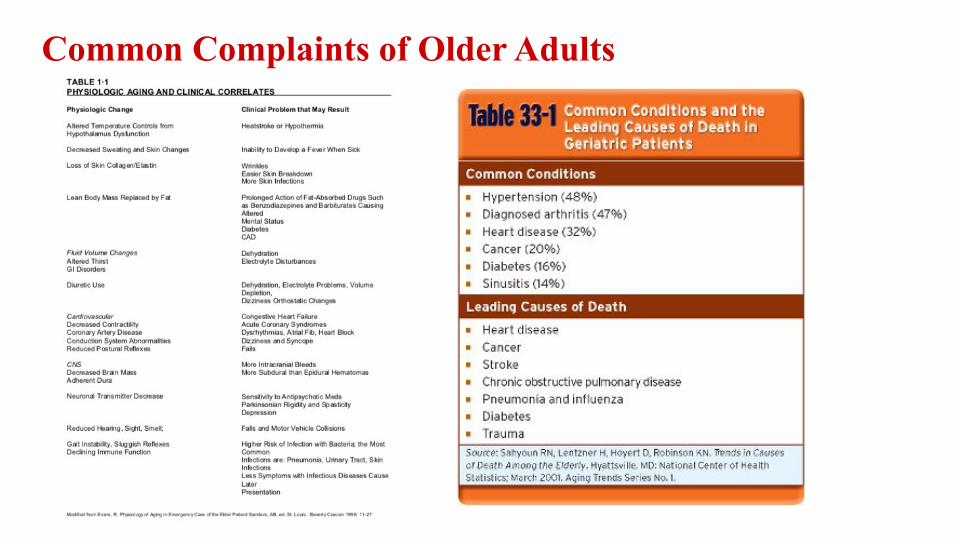
Common Complaints of Older Adults
- Primary Assessment- Airway and Breathing
- Loss of mechanisms that protect the upper airway cause a decreased ability to clear secretions
- Air and breathing issues should be treated with O2 as soon as possible
- Circulation- Poor perfusion is a serious issue in older adults- Vascular changes and circulatory compromise might make it
difficult to feel a pulse - Transport Decision
- Any complaints that compromise the ABCs should result in prompt transportation
Assessment

Secondary Assessment● Vital signs
○ Heart rate should be in the normal adult range but may be compromised by medications such as beta-blockers (lower BP &
○ Circulatory compromise might make it difficult to feel a radial pulse; consider other pulse points
○ Cap Refill is not a good assessment○ Blood pressure tends to be higher
● Typical Interventions Include○ Positioning○ Oxygenation○ Administration of glucose○ Psychological support
■ May need to assist with nitroglycerin, aspirin, or inhalers

Physiological Changes in the Body due to Aging- The decrease in the functional capacity of various organ systems is normal but
can affect the way in which a patient responds to illness- Normal changes should not be mistaken for sign of illness
- Depression is not part of normal aging- Falls may result from
- Fainting - Cardiac rhythm disturbance- Medication interaction- Consider that the fall may have been caused by a medical condition
- Geriatric patient has higher likelihood of decompensating after trauma, so repeat the primary assessment

- Pneumonia- Risk factors include if institutionalized, immunological compromise, chronic
and terminal conditions, history of COPD or cancer, and history of inhaled toxins
- Patient presents with cyanosis, dry skin, possible fever, tachycardia or hypotension, diminished breath sounds, possible feber
- Pulmonary Embolism- Blockage of an artery by a venous clot- Risk factors include recent surgery, obesity, and a sedentary lifestyle
- Patient will generally complain of symptoms of chest pain and present with tachycardia, cough, syncope, anxiety, shoulder back or chest pain
- Treatment- Suction blood from the airway- Provide oxygen and ventilate if needed- Prepare to use advanced airways
Respiratory System
- Dementia- Slow onset of progressive disorientation, shortened attention span, and loss of
cognitive function
- Assessment: Short and long-term memory loss, decreased attention span, be unable to perform daily routines, decreased ability to communicate, appears confused or angry, have impaired judgement, be unable to vocalize pain
- Delirium- Sudden change in mental status, consciousness, or cognitive processes- Marked by inability to focus, think logically, and maintain attention
- In the history, look out for intoxication or withdrawal from alcohol, withdrawal from sedatives, certain medical conditions
- Determine the patient’s baseline LOC!
- Reassess A&O and GCS
Nervous System

● When responding to a call with an elderly patient who has symptoms of confusion or altered mental status,
you may assume that their symptoms are part of the normal aging process or a result of dementia. However,
we can never assume that altered mental status is a patient's baseline as these symptoms could very likely
be caused by some other life-threatening condition.
● Sepsis is a common condition in the elderly that cannot be overlooked.
○ When an elderly patient has altered mental status, look for signs of infection, such as red or swollen
surgery wounds, foul odors, or history of taking antibiotics.
○ Other symptoms such as hypotension, hot skin, or fever can also be indicators that the patient is septic
○ Hyperglycemia is another condition that can lead to altered mental status in the elderly. Even if they do
not have a history of diabetes, the aging process can lead to a pancreatic failure as well as insulin
resistance, which may result in a patient having high glucose levels. This is another reason to do a
thorough assessment of all elderly patients with altered mental status and never assume their condition
is caused by aging or dementia.
--
Altered Mental Status in Elderly

- Syncope- Possible causes include arrhythmias or heart attacks, medication interactions,
changes in blood pressure or volume, seizures, or strokes
- Nerve Disorders- Motor → muscle weakness, cramps, spasms, loss of balance or coordination- Sensory → tingling, numbness, itching, pain, sensitivity to touch- Autonomic → changes in blood pressure and heart rate, constipation, bladder
and sexual dysfunction
Nervous System

- Heart Attack- Classic signs of heart attack are often not present in geriatric patients
- Shortness of breath, not due to exertion- Nausea, sudden weakness, or sweating- Syncope, confusion, altered mental status- Pale, cyanotic mottled skin, decreased breath sounds, increased peripheral
edema- Main complaint in elderly females is fatigue (not pain)
- Stroke- Risk factors include smoking, obesity, sedentary lifestyle, high cholesterol,
hypertension, cardiac disease, and atrial fibrillation
- Common Medications- Nitroglycerin, aspirin, cardizem, amlodipine, propranolol, atenolol
Circulatory System

- Acid Reflux- G-tube, GI bleed (coffee-ground emesis/hematemesis)
- Arrhythmias- Pulsemaker
- COPD- Chronic O2 use or respiratory therapy
- Diabetes- Diabetic emergency
- Kidney Failure- Dialysis cath or port
- Ulcers- Bed sores can become infected if left untreated
Underlying Conditions and Complications
- Need proof or verification of DNR from family members- Must have a doctor’s signature and license number- Tattoos, tags, and word of mouth are not valid
- Find what treatment is limited and provide supportive care
- If something is unclear, objection, change of mind- Begin resuscitation IMMEDIATELY
Advanced Directives

- Physical- Assault, neglect, diet, poor home maintenance, poor personal hygiene- Note injuries that can’t be explained by the patient’s lifestyle or condition- Progressed ulcers can often develop from untreated bed sores
- Psychological- Neglect, threats, shame, treating as an infant, deprivation of sensory stimuli
- Financial- Theft of valuables, embezzlement
- Victims may feel shame for having raised the abuser or be afraid of retaliation
Elder Abuse

Ageism● What is Ageism:
○ Ageism is widespread and an insidious practice which has harmful effects on the health of older adults. Ageism is everywhere, yet it is the most socially “normalized” of any prejudice, and is not widely countered – like racism or sexism.
- Why is Ageism Bad- These attitudes lead to the marginalisation of older people within our communities and have negative impacts on their
health and well-being- Over time, research shows, exposure to ageism is associated with higher cortisol levels, which can harm cognitive ability
and increase inflammation, leading to overall poorer health
● Stereotypes○ Stereotypes of aging include assumptions and generalizations about how people at or over a certain age should behave,
and what they are likely to experience, without regard for individual differences or unique circumstances ○ Stereotypes of aging in contemporary culture, particularly North America, are primarily negative, depicting later life as a
time of ill health, loneliness, dependency, and poor physical and mental functioning○ Make every attempt to avoid ageism
■ Not all older people have dementia■ Not all older people are hard of hearing■ Not all older people are sedentary or immobile
● Age-friendly practices○ Treat all older adults individually, with dignity and compassion○ Every person should have a sense of independence, autonomy , and self○ Be considerate to any body changes associated with aging
