wavelength october volume 16 no. 2
TRANSCRIPT
Agility™ shines on clinical frontPAGE 4
25 years of Gamma Knife® surgery at UPMCPAGE 8
Brachytherapy for gynecological treatmentPAGE 16
The future of cancer carePAGE 21
Vol. 16 | No. 2 | October 2012
PIONEERING SIGNIFICANT INNOVATIONS IN CLINICAL SOLUTIONS FOR TREATING CANCER AND BRAIN DISORDERS
Elekta’s ground-breaking 4 new MLC sweeping the globe
Agility™ shines on clinical front 5 A quarter century of Leksell 8 Gamma Knife® excellence
DBS – stimulating 10 a more normal life
MEG – valuable insight 12 into brain connectivity
Looking to the future – what will 14 we see in the next 40 years?
MRI sharpens vision 16 of cervical tumors
MOSAIQ® – a patient-centered 18 workflow
New software developments 20 in planning and scanning
The future of cancer care 21 Elekta around the world 22 What makes 24 your center unique?
Vision without action
is a dream. Action without
vision is simply passing time.
Action with vision is making
a positive difference.
Professor Lars Leksell (1907–1986) Inventor of radiosurgery and founder of Elekta
Elekta has been a company for four decades, and the gem that symbolizes
this 40th anniversary is the ruby. Appropriately, Elekta launched its Rubicon™
technology this year, in which rubies tip the multileaf collimator leaves of Agility™.

Elekta’s ground-breaking 4 new MLC sweeping the globe
Agility™ shines on clinical front 5 A quarter century of Leksell 8 Gamma Knife® excellence
DBS – stimulating 10 a more normal life
MEG – valuable insight 12 into brain connectivity
Looking to the future – what will 14 we see in the next 40 years?
MRI sharpens vision 16 of cervical tumors
MOSAIQ® – a patient-centered 18 workflow
New software developments 20 in planning and scanning
The future of cancer care 21 Elekta around the world 22 What makes 24 your center unique?
3
Contents
Dear friends,It is with a profound sense of pride that my colleagues
at Elekta and I mark our 40th year as a company.
I credit our many clinical customers and collaborators
worldwide for turning the small research company,
started by Professor Lars Leksell in 1972, into a global
leader in cancer care management. On behalf of the
Elekta community, I extend our gratitude to all of
you for joining us on this journey.
Working together with our partners, we have given
life to incredible advancements in the management
of serious disease. Our technological progress has
made a real difference for patients, the sole focus of
our joint efforts.
In this issue of Wavelength, we reflect on our
past and look to the future.
Dr. L. Dade Lunsford, Professor of Neurological
Surgery at the University of Pittsburgh Medical Center,
reflects on his center’s remarkable 25 years of Gamma
Knife® radiosurgery. We report on the global spread
of our revolutionary Agility™ beam-shaping solution
– launched just six months ago – and on the fascinating
potential of deep brain stimulation. And several Elekta
customers reveal what they see in store for the next
four decades of radiation therapy and radiosurgery.
As we begin our next 40 years,
I wish you good reading!
Tomas Puusepp
President & CEO of Elekta AB
All letters, comments or suggestions for future articles, requests for reprints and permissions are welcome.
Contact Wavelength: Michelle Joiner, Director, Global PR and Brand Management Tel: +1-770-670-2447 (time zone: Eastern Standard) | Email: [email protected]
Regulatory status of products: This document presents Elekta’s product portfolio. Products and indications mentioned may not be approved for certain markets.Art. No. 1501416 © Elekta AB (publ). All mentioned trademarks and registered trademarks are the property of the Elekta Group. All rights reserved. No part of this document may be reproduced in any form without written permission from the copyright holder.
Vol. 16 | No. 2 | October 2012
Published by Elekta | www.elekta.com
4
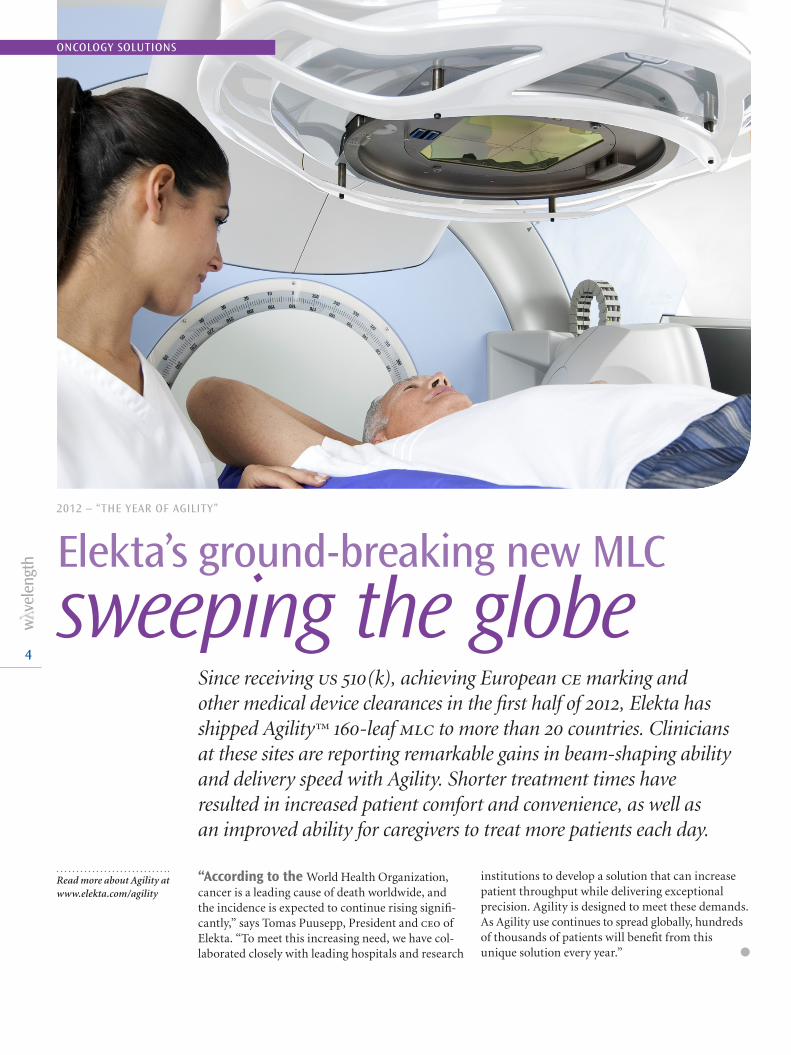
2012 – “THE YEAR OF AGILITY”
Elekta’s ground-breaking new MLC
sweeping the globeSince receiving us 510(k), achieving European ce marking and other medical device clearances in the first half of 2012, Elekta has shipped Agility™ 160-leaf mlc to more than 20 countries. Clinicians at these sites are reporting remarkable gains in beam-shaping ability and delivery speed with Agility. Shorter treatment times have resulted in increased patient comfort and convenience, as well as an improved ability for caregivers to treat more patients each day.
“According to the World Health Organization, cancer is a leading cause of death worldwide, and the incidence is expected to continue rising signifi-cantly,” says Tomas Puusepp, President and ceo of Elekta. “To meet this increasing need, we have col-laborated closely with leading hospitals and research
institutions to develop a solution that can increase patient throughput while delivering exceptional precision. Agility is designed to meet these demands. As Agility use continues to spread globally, hundreds of thousands of patients will benefit from this unique solution every year.” l
ONCOLOGY SOLUTIONS
Read more about Agility at www.elekta.com/agility

5
Agility shines on clinical front
St. James’s University Hospital – Leeds, U.K.
“We can schedule treatments to more patients per day.”l In April 2012, St. James’s became the first in the world to use Agility™ clinically, following up this success with the first combined Agility/vmat treat ment only weeks later. The combination of the two innovations reduced the time it takes to deliver the treatment from five minutes down to just two minutes. Elekta’s Monaco® treatment planning system also contributed to the patient’s treatment by enabling much lower doses to nearby critical structures than traditional plans the Leeds team had been producing.
“The combination of planning with Monaco, vmat and Agility means that treatment times are significantly reduced,” says John Lilley, physicist at St. James’s, part of The Leeds Teaching Hospitals nhs Trust. “For this patient, the vmat delivery was three minutes quicker than the regular conformal plan. This is very important because the immobilization mask the patient wears for treatment can be uncom-fortable and reduced treatment times mean less risk of patient movement. Quicker treatment times make a big difference for us as well, as it means we can schedule treatments to more patients per day.” l
The James Cook University Hospital – Middlesbrough, U.K.
“Treatment speed reduces the likelihood that the patient moves.”l Soon after St. James’s treated its first patients with Agility, The James Cook University Hospital became clinically operational with the new beam-shaping innovation. Three months later, physicians here achieved another benchmark – their first use of Agility to deliver radiation therapy employing Elekta’s Volumetric Modulated Arc Therapy (vmat). The ability to accelerate both beam shaping and beam delivery with Agility and vmat shaved 57 seconds off the beam delivery time of the first patient.
“This was our first experience with vmat and it went very well,” says Christopher Walker, phd, Head of Radiotherapy Physics at The James Cook University Hospital. “The treatment speed not only reduces the likelihood that the patient will move and that the internal organs will shift position, but it also contributes to faster patient throughput, which is key. With Agility/vmat we expect to be able to treat five patients per hour.” l
Agility – now shipped to over 20 countries

6
ONCOLOGY SOLUTIONS
SALK and Paracelsus Medical University – Salzburg, Austria
“Greater precision improves our ability to focus radiation to the tumor.”l As the first center to field-upgrade to Agility™, salk and Paracelsus Medical University treated its first patient using Agility on May 14, increas-ing its daily patient volume to 50 on its Agility-equipped Elekta Synergy® system after only a month. Based on their experiences, clinicians at the Salzburg clinic report that the Agility mlc’s new design provides them with more precise dose sculpting capabilities and remarkably lower non-therapeutic radiation dose delivered to the patient.
“Looking closely at several cases, we’ve calcu-lated a measureable improvement in dose shaping precision with the five millimeter leaves of Agility,” says Felix Sedlmayer, md, Professor and Chairman, Department of Radiotherapy and Radio-Oncology. “This greater precision improves our ability to focus radiation to the tumor, while strictly limiting exposure to surrounding critical structures, such as the rectum and bladder. We were astonished at the amount of healthy tissue dose reduction we could achieve. This capacity theoretically enables us to improve outcomes and reduce the potential for complications.” l
Riverina Cancer Care Centre – Wagga Wagga, NSW, Australia
“Interdigitation enables far fewer segments for complex plans.”l Transitioning from its two Siemens treatment machines to, eventually, two Elekta Synergy radiotherapy systems equipped with Agility 160-leaf multi-leaf collimator (mlc) – physicians at Riverina Cancer Care Centre, have been able to decrease beam delivery time by up to seven minutes for a variety of cancers. Riverina treated its first patients using its first Agility-equipped Synergy system on July 30, making the New South Wales facility first in the southern hemisphere to go clinical with the beam-shaping device.
“We have been very pleasantly surprised with the delivery speed of Agility, in addition to its beam-shaping accuracy,” says Damien Williams, Riverina Cancer Care Centre Managing Director. “Reducing beam delivery time for complex imrt treatments by up to seven minutes – from around 16 or 17 minutes with our previous system to 9 or 10 minutes with the Agility-equipped Synergy – is a very significant efficiency and clinical benefit. The interdigitation capabilities of Agility enable far fewer segments for complex plans. We also have observed a marked difference in the precision we can achieve.” l

7
Intelligent beam shapingAgility, compared to other multi-leaf collimators, is in class by itself – combining leaf speeds that are twice as fast as conventional beam-shaping devices.
The 160 leaves of Agility are 5 mm in width at isocenter and are capable of interdigitation to enable treatment of island fields and multiple targets in a single session.
Rubicon optical leaf positioning technology improves accuracy and increases the reliability and seamlessness of beam-shaping, and the exception-ally low leaf transmission of less than 0.5 percent enhances treatment delivery while reducing integral dose.
The integrated whole results in a sophisticated multi-functional beam-shaping solution.

8
Elekta interviewed Dr. L. Dade Lunsford, md, co-director of the upmc Center for Image-Guided Neurosurgery and Lars Leksell Professor and Distinguished Professor, Department of Neurological Surgery, University of Pittsburgh School of Medicine, recently about upmc’s experience with stereotactic radiosurgery.
What radiosurgery technology has UPMC used over the years?
‘‘At one time we had three Gamma Knife sys-tems, the original unit, a 4c and then Perfexion.
Today, we continue to use the Leksell Gamma Knife 4c and Leksell Gamma Knife® Perfexion™.
What are your thoughts about the growth of radiosurgery over the last 25 years?
‘‘Gamma Knife fits the paradigm of ‘disrup-tive innovation’. When it first arrived in the
United States after a six-year effort – culminat-ing in 1987 when we treated the first patient – Gamma Knife was totally unknown in terms of its role, potential and outcomes. However, after just 25 years, Gamma Knife, as opposed to many other technologies, has evolved, has continually been applied and is continuing to grow. While to some extent this form of radiosurgery may be con-sidered to be more esoteric because of its focus on the brain only, that is what Gamma Knife is designed for. Its growth in applications, patients treated and centers has been almost logarithmic.
Gamma Knife surgery for the treatment of metastatic disease continues to grow. To what do you attribute this trend?
‘‘ In the past, when a patient’s cancer spread to the brain, it was regarded as a very fatalistic event.
They would receive a very substandard treatment – whole brain radiation therapy [wbrt] – which
was all that was available. That started the clock; outcome data showed that the average patient lived only five or six months. So, both the oncologist and the patient essentially gave up, and most of these patients ended up dying of spread of the tumor to the brain. That’s not the case anymore. We replaced wbrt with radiosurgery one or more times if new disease shows up in the future. We can control the spread of cancer to the brain in more than 85-90 percent of patients. That pushes the oncologist to develop and use more effective tools to control the systemic disease, rather than throwing in the towel.
And there have been many successes over the last 25 years. Patients have presented with brain disease – essentially Stage 4 of their cancer – who respond to systemic treatment and Gamma Knife. They end up with no active disease at this time and are living normal lives.
EXPERT Q&A
A quarter century of Gamma Knife excellence at UPMC
The University of Pittsburgh Medical Center (upmc) marked its 25th year of Gamma Knife® surgery on August 14, 2012, and is on track to treating its 12,000th patient in that quarter century period by December 12, 2012 (12/12/12).
Dr. L. Dade Lunsford, md, co-director of the upmc Center for Image-Guided Neurosurgery
NEUROSCIENCE SOLUTIONS

9
Given this shift to radiosurgery, what is your opin-ion of the future of WBRT as a treatment option?
‘‘Gamma Knife is changing the treatment para-digm in metastatic cancer to the brain away from
reflexively using wbrt to only selectively using it in patients with miliary disease or carcinomatous men-ingitis. Since their survival has increased, there is a higher risk over many years that patients can develop that late problem related to cancer. If you initially held off on using wbrt, you can at least use it then.
The shift away from wbrt has already begun. We are seeing that more and more patients are being diagnosed early because they are getting an mri scan as part of staging. They receive stereo-tactic radio surgery early – when the tumors are smaller and there is a very high tumor control rate.
Gamma Knife surgery is increasingly used to treat multiple metastases in a single session. How do you see this trend evolving?
‘‘The number of mets is not the issue. Many insurance companies don’t understand this
either. The volume of the treated tumors is impor-tant. So, a patient with a single, large volume brain met may have more difficulties that a patient with 20 mets all of which are small. The issue is, if you treat all existing disease, then you simply have to wait and see whether anything shows up in the future – but Gamma Knife is effective in more than 90 percent of every treatable tumor. So, we gener-ally use Gamma Knife not by the total number of brain metastases but by the volume that is there. And, we don’t find that there is a significant change in benefit between one or four or ten or even 20 as long as you are treating everything that exists.
What is the future of Gamma Knife radiosurgery?
‘‘Radiosurgery has evolved in the United States and is
very much a team effort in which there is participation
from neurosurgeons, radia-tion oncologists, medical
physicists and nurses.
First UPMC Gamma Knife surgery patient marks 25-year milestone with gratitude
John Lynch, UPMC’s first Gamma Knife surgery patient – the first in North America and only the world’s fifth – has celebrated 27 birthdays since his surgery. On August 14, 1987, Lynch – then 25 years-old – received radio surgery to treat an AVM that every surgeon he spoke with had said was inoperable. Just 12 months later, the AVM had shrank and his symptoms – severe migraine headaches and seizures – began to disappear. Since then, every follow up appointment that the Pittsburgh resident has had has indicated that the AVM is gone for good.
“I had an MRI just six months ago and the AVM is still gone – I’m fine,” Lynch, now 52, reports. “I’m very grateful to have had the chance to have Gamma Knife surgery. Surgery wasn’t an option because the AVM was located too deeply inside my brain, and I was having some micro-hemorrhaging so it wasn’t looking good until I found Dr. Lunsford. I have a lot of gratitude.”
And, it is this team management that parallels how medical care in general has evolved in the United States. Rather than a ‘lone wolf’ doing everything, it is a team of people with expertise that is providing a high level of care to people with complex medical problems.
Gamma Knife is here to stay. I think it is going to continue to evolve, but it is being focused more on high volume needs. That is to say, if we look across the world, it is dealing with metastatic cancer that has spread to the brain. Gamma Knife clearly has revolutionized the management of patients when cancer spreads to the brain. l
‘‘The shift away from whole brain
radiation therapy has already begun.”

10
DEEP BRAIN STIMULATION THERAPY WITH LEKSELL STEREOTACTIC SYSTEM
DBS – stimulating a more normal life
NEUROSCIENCE SOLUTIONS
What began in 2006 as some slight trembling in her left knee and arm, evolved in six months to increasingly debilitating left leg stiffness that made her gait seem hardly like walking at all. Mrs. Christine Barker, now a 64-year-old retired school teacher from Crowthorne, Berkshire, u.k., was diagnosed with Parkinson’s disease*, her leg stiffness – dystonia – a symptom of the disorder.
“Instead of bending my foot properly, I was sort of putting my foot down flat and I was becom-ing increasingly aware that I couldn’t get my heel down on the ground properly,” she recounts. “The dystonia got much worse, and after about 18 months I was walking in a very bizarre man-ner, and walking any distance at all was completely exhausting. I ended up being in a wheelchair for most of the time if I was going out of the house.”
Medications (e.g., levodopa) made no impact at all, which prompted her neurologist in 2010 to refer her to the National Hospital for Neurology and Neurosurgery’s Unit of Functional Neurosurgery in London. There, she met Ludvic Zrinzo, md, phd, a neurosurgeon and specialist in Deep Brain Stimula-tion (dbs) therapy (see sidebar). Dr. Zrinzo told her that while Mrs. Barker’s case was unusual, he thought
there was a chance that dbs could help her.“It would be a leap of faith, really,” she remarks.
“They said dbs might have no effect, or it might provide a 10 percent improvement or 20 percent or 30 percent. They said that it was very difficult to tell because they couldn’t compare my situation with anyone else’s.”
A second chance
Mrs. Barker was scheduled for surgery on February 15, 2011. The Unit’s dbs experience spans a decade and over 300 patients – 40 implants from January to July 2012 alone – allowing Mrs. Barker to benefit from the refinement of the technique over the years. Shaving the patient’s entire head is now a thing of the past as scientific evidence doesn’t support the premise that it reduces infection. In addition,
Mrs. Christine Barker
*To learn more about the equipment used to perform DBS for the treatment of Parkinson’s disease, see page 11.

11
instead of conducting the procedure using micro-electrode recording (mer) under local anesthesia, the Unit ensures accurate anatomical placement of electrodes using post-implantation mri.1
“Our surgical protocol maximizes the use of imaging to minimize the number of brain passes and reduce the risk of hemorrhage and its poten-tially severe sequalae,” Dr. Zrinzo says. “Instead of relying on subjective intraoperative observations, we place increasing emphasis on mri. Among other things, this allows us to perform surgery under general anesthetic without having to totally with-draw pd medication – something many patients are grateful for. It also means that we have reduced the procedure time such that we regularly per-form two dbs procedures in one day. Moreover, we haven’t noticed any decline in efficacy.”
Mrs. Barker didn’t have to wait long before knowing her surgery had been successful.
“I could tell even a couple of days after the operation that my walking was slightly better,” she recalls. “To cut a long story short, the doctors gradually increased the simulation and my walking improved tremendously over the next several months.
“It has just been a very positive experience,” she continues. “If anyone would ever ask me if I recom-mend it, I would say: ‘Yes, go for it all the way.’ It has made a difference in my life – I have a future I can look forward to. Having dbs therapy was a life changing experience.” l
References1. Foltynie T, Zrinzo L, Martinez-Torres I, Tripoliti E, Petersen E, Holl E, Aviles-Olmos I, Jahanshahi M, Hariz M, Limousin P. MRI-guided STN DBS in Parkinson’s disease without microelectrode recording: effi-cacy and safety. J Neurol Neurosurg Psychiatry. 2011;82:358-363.
Ludvic Zrinzo, md, phd, at London’s National Hospital for Neurology and Neurosurgery
Leksell Stereotactic System® a key to DBS accuracyThe sophistication of the center-of-arc principle of Leksell Stereotactic System enables physicians at the Unit of Functional Neurosurgery to ensure an accurate trajectory to the brain target, in Christine Barker’s case, the globus pallidus internus (GPi).
“A trajectory that avoids the sulci and ventricle of the brain will also avoid the vessels enclosed within these structures and will greatly reduce the risk of bleeding,” Dr. Zrinzo explains. “Leksell Stereotactic System has a long heritage and there are many reasons that make it an excellent choice when performing precision stereotactic surgery. It is an MRI compatible frame and the fiducials are close to the head, minimiz-ing MRI distortion.”
He continues, “In addition, the principles are easy to understand and the surgeon can calculate target coordinates manually, removing blind reliance on software. Phantom experiments have shown that it performs favorably in comparison to other stereotactic frames in terms of accuracy. Importantly, Elekta is responsive and has produced custom made RF probes and taken our advice for product improvements, such as a counter scale on the x coordinate.”
What is DBS therapy?DBS is a surgical procedure in which an electrode** the thickness of an uncooked spaghetti noodle is implanted in the subthalamic nucleus (STN) or globus pallidus internus (Gpi), brain regions that are responsible for controlling movement.
To navigate to the pre-cise brain region accurately, the team at the Unit of
Functional Neurosurgery uses Leksell Stereotactic System (see above).
The electrode is con-nected to a pulse generator that is implanted subcutane-ously below the clavicle.
When the generator is activated, it transmits mild electrical pulses through the electrode to the brain. These electrical pulses modulate
the brain’s electrical signals to help control or stop abnormal movements.
Deep brain stimula-tion is both adjustable and reversible. Patients can use a remote control to modify the stimulation level neces-sary to afford the greatest symptom relief with the least amount of side effects.
**The electrode and associated equipment are manufactured by Medtronic, Inc. and are indicated for unilateral thalamic stimulation for the suppression of tremor in the upper extremity in patients who are diagnosed with essential tremor or Parkinsonian tremor not adequately controlled by medications and where the tremor constitutes a significant functional disability.

12
The progenitor of MEG was an induction-coil magnetometer with two million turns of copper wire wound around a ferrite core. In 1968, Dr. David Cohen used the device to perform the first successful recording of a magnetic field emanating from the living human brain.
“You couldn’t use it clinically – it was too weird and cumbersome,” recalls Dr. Cohen, then a physics professor at Chicago’s University of Illinois. “The coil was just proof of principle that the brain’s mag-netic field existed.”
Four years later as a researcher at mit, Dr. Cohen used a Superconducting Quantum Interference Device (squid) invented by James Zimmerman to attempt to refine the measurement of these fields.
“Once I had the squid, I could revisit this idea and try it again,” he says. “And this time it was glori-ous, because the noise was a thousand times less, and you could see the brain’s magnetic field just as easily as you could see the eeg. That is when the field took off, and when the word ‘meg’ really had meaning.”
Dr. Cohen published this success in Science in 19721, the magazine bestowing upon him the title of the “Father of meg.”
MEG finds its place
The evolution of meg since 1972 entailed the incor-poration of hundreds of squids, analogous to eeg with its numerous electrodes placed on the scalp.
“With many eeg electrodes, you can make a map of the whole head as a function of time – like a movie happening over the whole head,” Dr. Cohen explains. “The same applies to meg. If you just mea-sure the magnetic field as I did in the early 1970’s – at one place – it was, at most, interesting, but it doesn’t lead to any application. Once companies such as Neuromag began making whole head systems that enabled mapping the magnetic field over the entire head, then it really got fascinating.”
Whole head arrays enabled researchers to detect
the source of the magnetic fields in a way not possible before.
First, meg detected auditory evoked responses. Around 1990, clinical meg work began, involving the measurement of the interictal spikes of epilepsy.
“Sometimes the spikes in epileptic kids could not be seen on eeg, but could be seen on meg – that made a lot of neurologists sit up and take notice,” he remarks. “Now, meg could be used to help the surgeon decide if they need to oper-ate on epilepsy, where to go and where to cut.”
In research, meg is providing valuable insight into brain connectivity – how different parts of the brain communicate with each other – and is
NEUROSCIENCE SOLUTIONS
MAGNETOENCEPHALOGRAPHY
MEG – valuable insight into
brain connectivity
Dr. David Cohen
Dr. David Cohen, often referred to as “The Father of meg”, reflects on the technique he brought to life 40 years ago.
13
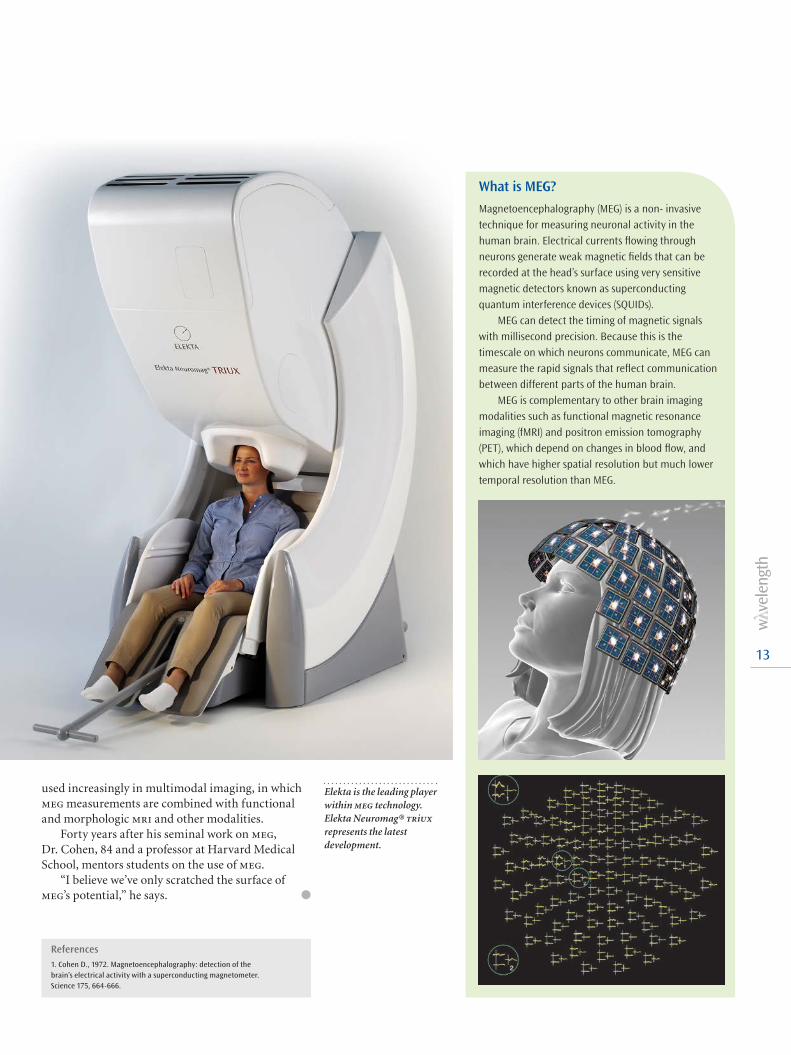
used increasingly in multimodal imaging, in which meg measurements are combined with functional and morphologic mri and other modalities.
Forty years after his seminal work on meg, Dr. Cohen, 84 and a professor at Harvard Medical School, mentors students on the use of meg.
“I believe we’ve only scratched the surface of meg’s potential,” he says. l
References1. Cohen D., 1972. Magnetoencephalography: detection of the brain’s electrical activity with a superconducting magnetometer. Science 175, 664-666.
What is MEG?
Magnetoencephalography (MEG) is a non- invasive technique for measuring neuronal activity in the human brain. Electrical currents flowing through neurons generate weak magnetic fields that can be recorded at the head’s surface using very sensitive magnetic detectors known as superconducting quantum interference devices (SQUIDs).
MEG can detect the timing of magnetic signals with millisecond precision. Because this is the timescale on which neurons communicate, MEG can measure the rapid signals that reflect communication between different parts of the human brain.
MEG is complementary to other brain imaging modalities such as functional magnetic resonance imaging (fMRI) and positron emission tomography (PET), which depend on changes in blood flow, and which have higher spatial resolution but much lower temporal resolution than MEG.
Elekta is the leading player within meg technology. Elekta Neuromag® triux represents the latest development.

14
What do you believe we will see in the next 40 years in radiation therapy or in radiosurgery?
We asked several Elekta customers to predict advances in their field over the next four decades.
‘‘Radiosurgery will be more and more widely used for functional neurological disorders in 40 years.
With refinement of imaging and neurophysiological techniques, non-invasive physiological confirmation of functional targets in the brain will be possible, which makes radiosurgery for functional disorders more feasible.”
Takaomi Taira, MD, PhD • Professor of Neurosurgery Tokyo Women’s Medical University • Tokyo, Japan
‘‘Radiation oncology will continue to maintain an important role in treating cancer beyond
2050. Robotic-assisted treatment, based on molecular imaging, cancer nanotechnology, and the genomic profile of every patient, will allow optimal individualized patient care, both in delivering radiation alone and in combining radiation with smart drugs. Radiation schedules will be strongly hypofractionated in the majority of cancer sites.”
Umberto Ricardi, MD, PhD • Full Professor Radiation Oncology University of Turin • Turin, Italy
‘‘Citius, altius, fortius: radiotherapy of the next decades will strongly act upon the Olympic maxim.
Faster treatments, higher doses, stronger effects. Continuous progress in adaptive dose conformation in all terms of on-time tracking a tumor’s position and its biology will intensify radiation response while dramatically reducing normal tissue exposure. Major solutions in cancer cure are to be expected from physics and hence, radiation oncology.”
Felix Sedlmayer, MD • Professor and Chairman Dept. of Radiotherapy and Radio-Oncology • SALK and Paracelsus Medical University • Salzburg, Austria
‘‘All treatments will be image guided to accurately target the radiation based on surface anatomy,
internal anatomy and molecular characteristics of the tumor with real time feedback.”
Ruth Heimann, MD, PhD • Professor, Radiation Oncology • Vermont Cancer Center • University of Vermont/Fletcher Allen Health Care, USA
‘‘ In the next 40 years I think we will be able to locate the genetic loci responsible for a few or
many of the cancer-causing genomes and will have developed radiation delivery systems with adequate verification tools to be able to knock out the malignant loci with preservation of the basic codes for normal tissue structures and functions. The EMR would have grown to record all these changes and reflect them in the clinical follow up and patient profiling.”
Tejinder Kataria, MD • Chairperson Radiation Oncology Medanta-the Medicity, Gurgaon, India
‘‘The next 40 years is sure to be our professions’ most exciting. As we gain greater under standing of
tumor and normal tissue biology, we will individualize radiation treatments and optimally combine radiation with molecular targeted treatments and immuno-therapy to increase cure rates.”
Thomas A. Buchholz, MD, FACR • Head, Division of Radiation Oncology The University of Texas M. D. Anderson Cancer Center, USA
‘‘Technological innovation will remain the primary driver of radiotherapy. Comparative effectiveness
research will prove the high value of radiotherapy hopefully leading to more funding for biological innovation, allowing us to do more with less dose. Population constraints we will be replaced by patient specific constraints. Patients with metastatic disease being treated for cure or prolongation of life, not just palliation, will ultimately be the most common patient in the radiotherapy clinic.”
Robert Timmerman, MD • Professor of Radiation Oncology and Neurosurgery • University of Texas Southwestern Medical Center, USA
‘‘With the ability to dose escalate while sparing normal tissue combined with better imaging
capabilities – including real-time imaging – radiosur-gery will become more widely adopted as a minimally invasive surgically ablative procedure. The new specialty of “Radiosurgeon” will treat both malignant and benign tumors, as well as perform functional treatments, to many different organ systems.”
Peter C. Gerszten, MD, MPH • Associate Professor, Neurological Surgery and Radiation Oncology • University of Pittsburgh Medical Center, USA
‘‘ Imaging will continue to push the frontiers in radiotherapy for the foreseeable future. Clinical
trials will be aimed at understanding the relationship between biological imaging metrics and treatment outcome that will lead to individualized prescriptions with targeted dose escalation. High precision targeted radiotherapy will be further aided by radiation activated cytotoxic agents, and treatment planning will be based on probabilistic dose distributions, which account for treatment uncertainties and radiation responsiveness.”
John Simpson, PhD • Director of Medical Physics Radiation Oncology Institute, Sydney, Australia
‘‘Radiotherapy will continue to be an important tool to fight disease locally with ever decreasing
side effects and it will help to unlock the full potential of systemic treatments such as immunotherapy.”
Frank Lohr, MD • Vice Chairman University Medical Center (UMC) Mannheim, Germany

15
‘‘Patients will have worldwide access to the same high quality of care, in which information and pro-
cess flow will be completely integrated from diagnosis, treatment, and long-term follow up, It also will involve complex algorithms for decision-making through the continuum of care and for resources utilization.”
Marie-Andrée Fortin, MD, FRCPC • Head of Radiation Oncology Centre intégré de cancérologie de Laval, Québec, Canada
‘‘Radiosurgery will continue to grow and become a main trend of treatment for most vascular
lesions, such as AVMs and DAVFs, deep-seated benign brain tumors, and certain functional disorders, such as trigeminal neuralgia.”
Prof. David Hung-Chi Pan, MD • Professor, Functional Neurosurgery • Taipei Veterans General Hospital, Taiwan
And from some of our Elekta experts:
‘‘Radiation Medicine will be one of if not the safest therapy for managing cancer beyond 2050.
Automation, instant feedback, and multi-modality imaging will help cure cancers in their early stages. Global aggregation of patient follow-up and treatment outcomes facilitated by the Oncology EMR will enable clinicians to find and deliver the best treatments to every cancer patient no matter where on the globe they live.”
Timothy J. Prosser, MBA • Director, Oncology Business Line Management, Elekta • Crawley, West Sussex UK
‘‘ In the next 40 years, I believe Radiosurgery technol-ogy will develop to the point where a therapeutic
radiation dose will be precisely and safely delivered in a single session, to fully control medium and even larger targets, anywhere in the body, regardless of target movement during imaging or treatment. And with this advancement, Radiosurgery will also expand clinically, to treat new indications and diseases that can be well localized with anatomic or functional imaging.”
Ray Rau • Vice President, Gamma Knife Sales, Elekta Latin America, Middle East, and Eastern Europe
‘‘Radiosurgery will become standard of care for treatment of brain metastases in combination
with drug therapies for a lifelong disease management and thus proliferate into every comprehensive cancer care facility. SRS in combination with sophisticated biological modifiers will open a new field of modulating neurological activity for functional indications.”
Per Nylund, MSc • Vice President, Product Management, Elekta Neuroscience Solutions
‘‘Radiotherapy will play an essential role in highly diversified and individualized multi-disciplinary
concepts. Strict boundaries between curative and pal-liative treatment will be lost, rendering many cancers a chronic disease due to integrated systemic and local treatments. Software solutions will actively assist in all decision-making processes and radiotherapy steps by combined analyses of clinical evidence and institutional outcome data.”
Prof. Dr. Matthias Guckenberger, MD • Vice Chairman, Dept. of Radiation Oncology • University Hospital Würzburg, Germany
‘‘ Stereotactic radiosurgery should see significant advances with the integration of sophisticated
neuro-imaging modalities to patient selection, targeting, dose planning, and post-treatment assessment.”
Jason Sheehan, MD, PhD, FACS • Alumni Professor, Department of Neurological Surgery • University of Virginia, USA
‘‘ Large cancer registries, established from EMR data transfers, will allow Radiation Oncology to become
transformed based on predictive analytics that establish best care models and directives that are personalized and evidence-based. Likewise, the process of delivering radiation therapy will become predictable and safer due to novel management processes.”
Louis Potters, MD, FACR, FASTRO • Prof & Chair, Dept of Radiation Medicine • North Shore - LIJ Health System, USA
‘‘Even with the huge expenditure on cancer drug research, in 40 years time, therapy with radiation
is still likely to be one of the most cost-effective and curative of cancer treatments. This will no doubt be supported by more accurate tumor cell localization, right down to microscopic levels, so that we can do away with the concept of CTV!”
Vivian Cosgrove, PhD • Head of Radiotherapy Physics St. James’s Institute of Oncology, Leeds, UK
‘‘Rooted in the 1950’s, the radiosurgical revolution is still ongoing and will continue to transform the
practice of neurosurgery in the coming decades for the greatest benefit of patients. Functional neurosurgery indications will continue to expand and we will come to a better understanding of the benefit of low non-necrotizing dose on the cerebral parenchyma. These two factors are expected to play major roles in the future development of radiosurgery.”
Prof. Jean Régis • Head of Functional Neurosurgery Timone Hospital, Marseilles, France
16
GYNECOLOGICAL TREATMENT
MRI sharpens vision of
cervical tumorsNational Cancer Centre Singapore clinicians harness magnetic resonance imaging (mri) to better tailor brachytherapy radiation dose to the tumor, sparing normal tissues
The ability of MRI to create exquisite images of the body’s soft tissues – and the tumors that arise amid them – is helping physicians at National Cancer Centre Singapore (nccs) to precisely shape brachytherapy doses to cervical tumors, while at the same time avoiding exposure to critical healthy organs and tissues. Since November 2011, nccs clinicians have used mri to characterize soft tissues, organs-at-risk and lesions before successive brachy-therapy treatments using the microSelectron® Digital remote afterloader and Oncentra® 3d Brachy Image Guided Treatment Planning system, both manufactured by Nucletron, an Elekta company. Nucletron is a pioneer in image-guided brachytherapy.
Brachytherapy is an advanced, highly targeted cancer treatment in which radiotherapeutic sources are placed in or near a tumor, giving a high radia-tion dose to the tumor while reducing the radia-tion exposure in the surrounding healthy tissues. nccs uses the microSelectron Digital high dose rate (hdr) brachytherapy, which introduces the radiation source for a certain time using a special applicator.
“After our first year using ct based planning for 3d brachytherapy, we felt confident enough to take the next step: mri guided adaptive brachytherapy,” says Richard Yeo, md, Senior Consultant Radiation Oncologist at nccs. “The ability to visualize the tumor on mri and plan the treatment ‘live’ is nothing short of amazing.”
Better images, better treatment
mri provides information about the tumor’s volume (3d) and how the volume and shape change between treatment sessions (4d). Performing an mri scan before each brachy session enables clinicians to adapt the dose to the unique anatomy of each patient, accounting for not only the position of organs-at-risk, but also tumor regression or move-ment, which may have occurred during preceding
external beam radiotherapy and/or chemotherapy and between brachy sessions themselves.
Conforming brachytherapy doses closely to the tumor’s shape and position is important in order to apply the highest possible dose to the tumor while limiting the dose to critical structures such as the bladder and rectum, thereby decreas-ing the likelihood of treatment side effects.
“The Oncentra Treatment Planning (otp) sys-tem is very user friendly, with its intuitive inter-face and flexible workflow for managing ct and mr images,” says Lawrence Ng, Consultant Physicist at
BRACHYTHERAPY SOLUTIONS

17
nccs. “The recently upgraded otp version 4.1 incor-porates a very useful 3d modeling library for accu-rate applicator placement during planning. This results in enhanced accuracy in source dwell posi-tion reconstruction and dose calculation which hopefully will translate into better treatment result.”
Various publications from leading hospitals around the world have shown that use of this advanced technology allows health care teams to treat even the most complex cervical cancers, expected to result in lower recurrence rates and higher survival. Intensive multi-center research is
ongoing with the aim to provide more data to confirm these treatment benefits over traditional methods. This will allow experts to address unmet medical needs for this common cancer. 1
World-class training
A group of nccs experts received training on mri guided adaptive therapy at the University Hospital of Vienna, a leading center pioneering the development of this technique for the treat-ment of cervical cancer. The advanced work done in medical centers in Austria, and across Europe will now gradually be adopted in a growing num-ber of hospitals in the Asia Pacific region.
“Building a network of regional expertise will help other Asian hospitals adopt this new technol-ogy and provide state-of-the-art treatments to their patients,” says Ulrich Krumme, Regional Director for Sales and Marketing Elekta Brachytherapy Far East. “This will be especially important, as technolo-gies that have been developed in Europe will need to be adapted to local infrastructures and patient demographics. The potential clinical benefit of 3d gynecological planning and treatment over the conventional 2d approach makes it attractive for us to help hospitals with the adoption.” l
To better fulfill the needs of customers in Southeast Asian markets, Elekta will launch a smaller version of its well-known applicator this autumn. The Fletcher CT/MR Applicator Set XS is designed to better meet the needs of women in countries such as China, India, Japan, and Malaysia who tend to be more slightly built.
The new applicator is a scaled-down version of the standard Fletcher Applicator Set. It has the same features and options, but in a smaller size. For example, the set’s adjustable intrauterine tube has a four-millimeter radius rather than the standard six millimeters.
“The introduction of this new brachytherapy solution is a great example of personalizing medical technology for a certain group of patients,” says Maurits Wolleswinkel, VP, Elekta Brachytherapy Solutions. “This is important not only regionally – because smaller female anatomies are found most commonly in Asian countries – but also clinically, because up to now there hasn’t been a good brachytherapy applicator for smaller patients regardless of where they live.”
According to the World Health Organization, cervical cancer is the second most common cancer in women worldwide, with about 500,000 new cases and 250,000 deaths each year.
Adapted brachytherapy applicator for Asian marketsThe new applicator will also enable an easier change process for customers who want to make the transition from 2D to 3D treatment planning. In developed countries, many customers have made the transition to 3D, but that requires computed tomography (CT) and magnetic resonance (MR) capabilities – the imaging modalities that generate 3D data sets. Since this applicator is CT- and MR-compatible, these customers will have the opportunity to upgrade over time.
The XS applicator is integrated in Oncentra® Brachy treatment planning. The software recognizes the applicator stored in an applicator library, which allows the clinical team to reconstruct the applicator with just a couple of mouse-clicks. Applicator Modeling in Oncentra Brachy offers better visibility, accuracy and reproducibility for physicians and physicists.
‘‘The ability to visualize the tumor
on MRI and plan the treatment ‘live’ is nothing short of amazing.”
References1. Radiotherapy and Oncology 94 (2010) 173–180, Int. J. Radiation Oncology Biol. Phys., Vol. 65, No. 2, pp. 624–630, 2006, Clinical Oncology 22 (2010) 602-604.
18
The resolve to put the patient’s needs first in every decision they made regarding the establish-ment of a new cancer center drove officials at Quebec’s Centre de Santé et de Services Sociaux de Laval (csssl) to unite both radiation oncology and medical oncology departments under mosaiq®.
The new facility, Centre Intégré de Cancérologie de Laval (cicl), officially opened on February 21, 2012. cicl is Quebec’s first center to implement mosaiq for both oncology departments.
“When we initiated the cicl project, our first objective was to define the cancer centre’s vision,” says Marie-Andrée Fortin, md, Chief Radiation Oncologist at csssl. “The goal was to facilitate cancer care deliv-ery around the patient’s needs. We concluded that to achieve that goal we needed to implement an ois.”
Dr. Fortin and her colleagues dedicated time to visit u.s. and u.k. medical centers that operated mosaiq and another vendor’s Oncology Information System (ois) to evaluate their respective strengths. According to Dr. Fortin, mosaiq offered more
flexibility to configure the ois according to cicl’s unique processes than did another vendor’s ois.
“It was important that the ois adapt to our pro-cesses instead of us adapting to the ois,” she says. “From our perspective, mosaiq would best meet that requirement, enabling us to create the workflow we wanted from referral to follow up. The overriding goal was to streamline and automate our processes. This is one of the reasons why the mosaiq iq Scripts™ functionality was so important to us.”
Throughout the mosaiq implementation pro-cess, Elekta worked closely with cicl staff to ensure a successful outcome.
“We had extremely high standards and worked hard to develop our processes and workflow,” Dr. Fortin remarks. “We had to get very creative to use all the mosaiq functionality we could to meet those standards. To that end, we had a great collaboration with Elekta and the ro and mo staffs to find ways to make it work. Elekta’s team was quite flexible in accommodating our needs.”
MOSAIQ IN CANADA
A patient-centered
workflowThanks to mosaiq®, a new Quebec center’s radiation oncology and medical oncology departments are paperless from day one.
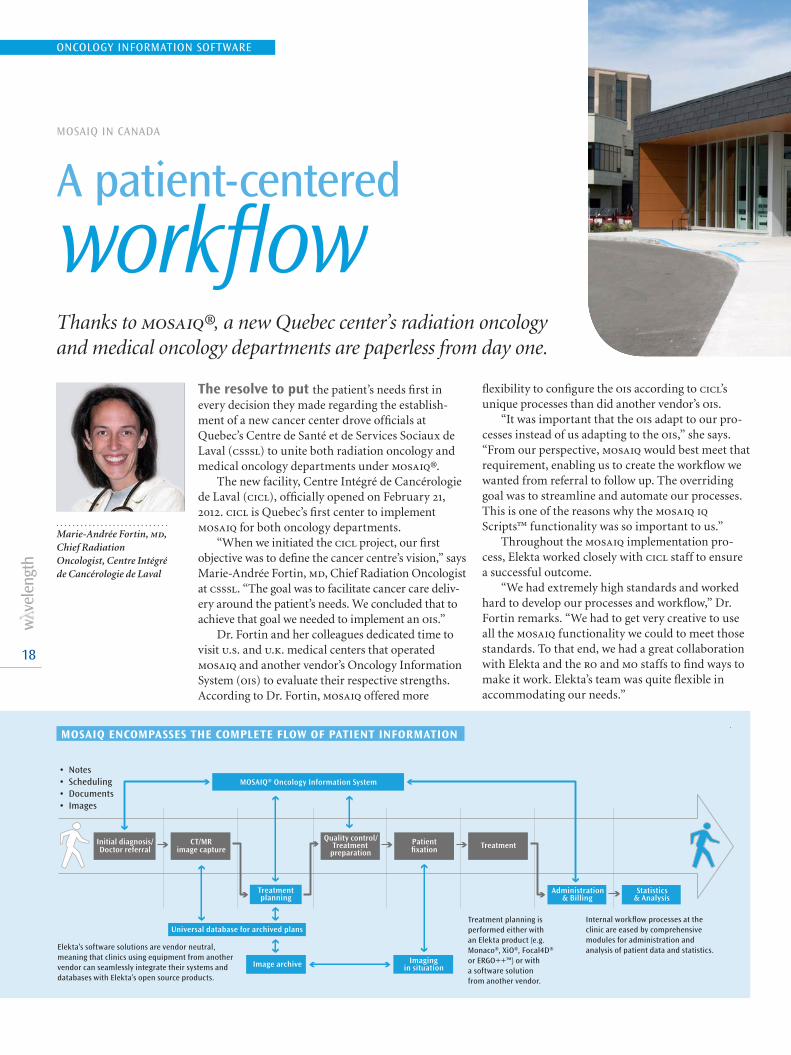
Initial diagnosis/Doctor referral
CT/MRimage capture
Quality control/Treatment
preparationPatientfixation
Imagingin situation
Treatment
MOSAIQ® Oncology Information System
Universal database for archived plans
Treatmentplanning
Administration& Billing
Statistics& Analysis
Image archive
• Notes• Scheduling• Documents• Images
Elekta’s software solutions are vendor neutral,meaning that clinics using equipment from anothervendor can seamlessly integrate their systems and databases with Elekta’s open source products.
Treatment planning is performed either with an Elekta product (e.g. Monaco®, XiO®, Focal4D®or ERGO++™) or witha software solution from another vendor.
Internal workflow processes at the clinic are eased by comprehensive modules for administration and analysis of patient data and statistics.
Marie-Andrée Fortin, md, Chief Radiation Oncologist, Centre Intégré de Cancérologie de Laval
MOSAIQ ENCOMPASSES THE COMPLETE FLOW OF PATIENT INFORMATION
ONCOLOGY INFORMATION SOFTWARE

19
Real-time data access
While both medical oncology departments at cicl were paperless with mosaiq from their first day, for cicl the most critical benefit is real-time data access. At cicl, access is even more convenient with an IT infrastructure that sites 200 mosaiq client worksta-tions throughout the facility.
“We want the workflow to be around the patient, not the physician or caregiver,” Dr. Fortin says. “With mosaiq workstations in multiple locations, I can log in anywhere to see the patient’s chart. It’s very efficient and it gives us mobility.”
Diverse data
mosaiq is compatible with virtually any treatment or planning system, giving cicl clinicians access to a wide variety of information. mosaiq has interfaces with cicl’s his, adt and lab results systems, all modalities in the imaging department, and the hospital’s pacs and emr systems and metriq® cancer registry.
Adhering to provincial standards that seek to ensure patients receive equitable and timely care, cicl has implemented a patient priority system inte-grated within mosaiq.
“Based on the seriousness of their case, patients can be prioritized to be seen and/or treated earlier, which avoids a simple ‘first-come-first-served’ policy that is not medically rational,” Dr. Fortin explains. “In addition, at cicl we can be even more precise and systematic in patient care through standardized care plans, which are integrated in mosaiq.”
Standardized care plans provide evidence-based guidelines for a given diagnosis, including recom-mended consultations, medical regimens, tests, rt planning and patient-specific quality control.
“Standardizing case management helps us pro-vide the same high quality to patients regardless of who they see – it’s not physician dependent,” Dr. Fortin says. “This reduces the chance of error. Also, the mosaiq iq Scripts functionality reinforces the
standardized care plan by specifying a sequence of tasks that have to be done by different care managers. Once each task is completed, it is automatically pushed to the next caregiver in the sequence, making the process quite efficient. It also helps us see where bottlenecks are and determine where you need to put more resources.”
The mosaiq implementation has brought pre-dictability and order to the workflow, adds cicl Chief of Physics Fadi Hobeila.
“The patient’s emr will have all the information necessary to plan for cases,” he says. “For example, if the emr shows the patient has a pacemaker and her first treatment is on May 15th, I know I have to be there and need to prepare my in vivo dosimetry tools.
“In this way, the ois helps the physics team be more an integrated part of the clinical team,” Hobeila continues. “We’re not just doing machine and patient qa, we’re always working in the patient record, and have ongoing, close contact with the dosimetrists, therapists and doctors, because all communication goes through the patient record.”
Patient-centered OIS
Communicating and accessing information in real time has streamlined cicl operations noticeably, mainly to the benefit of patients.
“Patient wait times are shorter,” she says. “They were used to waiting for chemotherapy. Now, because medication orders are done through mosaiq, the nurse can consult the emr anytime to see when the pharmacy has completed the preparation. They don’t have to call or walk to the pharmacy to check.”
In addition, since cicl’s first day, there also has been an absence of the clutter and physical transpor-tation of paper charts and documents in both radia-tion oncology and medical oncology departments. This has made these clinical environments more tranquil places, Dr. Fortin adds.
“I’ve had experience in paper-based depart-ments, with people bustling around carrying charts or hunting for misplaced charts,” she says. “This environment is so peaceful and much tidier without all that paper.” l
FACTS
Centre Intégré de Cancérologie de Laval (CICL): F Uses MOSAIQ (v.2.4) in the French Canadian LanguageF Operates two Elekta Infinity treatment systems.
Two additional Elekta Infinity systems will be up and running in 2013.F Has 30 infusion rooms, two CT systems, laboratory, and
patient information center.F In its first year, will treat approximately 1,000 patients with radiation therapy.F Gives approximately 10,000 chemotherapy treatments per year.
Cancer is the leading cause of death in Quebec (and Canada), surpassing cardiovascular disease. 1
1. Canadian Cancer Statistics 2010 (www.cancer.ca)
‘‘We had extremely high stan-
dards and worked hard to develop our processes and workflow.”

New software developments in
planning & scanning
20
SOFTWARE SOLUTIONS
Monaco 3.20The launch of the most recent release of Monaco® Treatment Planning System, version 3.20 offers customers improved vmat planning and delivery support, in addition to support for Elekta’s Agility™ 160 multileaf collimator. The release promises to create new workflow efficiencies through inte-grated plan approval and enhanced integration with mosaiq® Oncology Information System.
The new Segment Shape Optimization™ is driving better dose conformity, plan quality and delivery effi-ciency through its proprietary approach to smoothing and clustering segments, then optimizing beam weights and shapes. Powered by the renowned Monte Carlo algorithm, the results are plans that improve sparing of organs-at-risk and dose conformality.
In addition, the release’s new contouring tool, ez Sketch, and Room’s Eye View increase workflow efficiency. Support for Agility means that Monaco 3.20 users can achieve a new level of beam-shaping precision and delivery speed. l
Clarity with AutoscanClarity® soft tissue visualization system now provides an Autoscan option for automated ultra-sound scanning from outside of the treatment room, employing a motorized probe positioned at the patient’s perineum. The transperineal approach also benefits planning by providing a clear view of the prostate and surrounding critical areas. Clearly visualizing these critical structures could enable physicians to create plans with tighter margins around intended targets, thus avoiding exposure to uninvolved tissues.
Clarity with Autoscan provides a flexible alternative to traditional hand-held scanning and is the ideal platform on which to build future live (i.e., real time) imaging applications that will track the prostate and surrounding anatomy during treatment*. Live imaging has become increasingly important for physicians wanting to pursue reduced margin hypofractionated therapy. l
* Works in progress and not available for sale or distribution.

THE FUTURE OF CANCER TREATMENT
21
Everyone agrees that there will be radical changes in how to treat cancer in the next decade. This applies to everything from the devices used and locating and eliminating tumors, to the role of soft-ware and data. Obviously, no crystal ball can show us what lies ahead, but Elekta has a few experts willing to make an educated guess.
Kevin Brown, Global Vice President, Scientific Research, says he expects the value and effective ness of rt will continue to develop with better diagnos-tics and improved imaging.
“I believe improved targeting through image guidance will be the biggest breakthrough for rt,” Brown says. “Elekta is already a trailblazer with Clarity® soft tissue visualization, Elekta Synergy® with 3d and 4d image guidance, and our research program into using magnetic resonance imag-ing [mri] for image guidance. It’s inevitable that all rt devices will have integral image guidance.
“Better imaging means we will be able to treat much smaller fields with much higher doses. We’ll have functional imaging that will tell us which parts are already dead and which are still active or have metastatic potential.”
Brown says the real intellectual breakthrough in treating cancer, though, will be in software. This view is shared by Dr. John Christodouleas, Vice President of Clinical Affairs at Elekta, and Adjunct Assistant Professor of Radiation Oncology at the Hospital of the University of Pennsylvania.
“The biggest change in the next ten years will be a result of improvements in information technol-ogy,” Christodouleas says. “The widespread use of data registries – perhaps Elekta’s – will give us the potential to learn from literally everyone we treat.”
Today, every hospital in the usa is required to have a separate cancer-registry department, and Elekta’s Oncology Data Alliance (oda) helps them aggre-gate oncology data. Christodouleas believes that in the future there will be registries in every country, in every hospital. This, he says, will open oncology to the world of big data (data that exceeds the pro-cessing capacity of conventional database systems).
“Big data opens the door to substantially differ-ent kinds of analyses and enables running experi-ments within the data,” he says. “It will allow us to appreciate very small differences between treatments and procedures, and to identify small subgroups that may benefit more or less than the average person.”
Joel Goldwein, Senior Vice President, Medical Affairs, believes the future of oncology and cancer care will be the use of specifically targeted thera-pies, not just focusing on a particular lesion, but targeting particular cells and particular patients.
“We will have much more granular under-standing of the genetic basis of cancer and the genetic makeup of patients who are more likely at risk of recurrence after surgery or chemo-therapy. We will be able to select patients much more intelligently and irradiate them much more deliberately to a much more focused area.”
Goldwein says rt treatment will be more than just pointing and focusing a beam at a par-ticular tumor. “We’ll be able to point the beam at the right place, but then have something administered to the patient that will enhance the effects of the radiation on the cancer cells while protecting the normal cells,” he says.
All three agree that this is an exciting time for radiosurgery and radiotherapy, and that the future holds amazing and untold developments. l
Elekta’s Kevin Brown, Global VP, Scientific Research; Dr. John Christodouleas, VP, Clinical Affairs; and Joel Goldwein, Senior VP, Medical Affairs

Elekta around the world AMSTERDAM, THE NETHERLANDS
In 2011, Elekta acquired Nucletron BV. Headquartered in Veenendaal, The Netherlands, Nucletron is the undisputed global leader in brachytherapy, a very precise, highly effective and well-tolerated treatment option that is tailored to the needs of individual patients. By joining forces with Elekta, Nucletron became part of a world-leading provider of therapy for many types of cancers.
ATLANTA, GEORGIA, USA
September 22-25, 2013 the American Society for Radiation Oncology will hold its 55th Annual Meeting at the Georgia World Congress Center in Atlanta. Home of Elekta’s newly-relocated North America headquarters, the company’s first foreign subsidiary opened in the United States in 1983. Today, North America remains the single largest market for Elekta, as well as the world’s largest market for radiotherapy.
BEIJING, CHINA
In the last five years, Elekta has concentrated resources to support China’s initiatives to modernize and improve access to cancer care. This has resulted in a number of firsts and milestones, including Elekta BMEI shipping its 100th Elekta Compact™, the release of MOSAIQ® in the Chinese Language and installation of China’s first Leksell Gamma Knife® Perfexion™ and Elekta Axesse™ treatment systems.
DUBAI, UNITED ARAB EMIRATES
In recent years, Elekta has increased its focus and resources on the Middle East, establishing new offices or improving its distribution network, education and training, users meetings, clinical collaborations, equipment service infrastructure, spare parts management and regional offices. In October 2010, Elekta opened an office in Dubai, where all Elekta key technologies and functions are individually represented.
LONDON, ENGLAND
Acknowledging its contribution to the discovery and delivery of new technology, Elekta’s Crawley facility is known as “home of the world’s first digital linac.” Since the company’s 1997 acquisition of Philips’ radiotherapy division, the finest scientific talent has collaborated with clinicians to pioneer advancements such as the new Agility™ MLC – an innovation that precisely shapes radiation beams to tumor targets.
MONTREAL, CANADA
Following the 2010 acquisition of Canada-based Resonant Medical Inc., Montreal became home to Elekta’s Clarity® research and development team. Earlier this year, Elekta held its first European Clarity User Meeting, where users from Germany, Denmark, Ireland, Italy and France convened to learn more about the Clarity product roadmap and breakthrough studies that suit the clinical needs of the European market.
SINGAPORE
In March 2011, the inaugural meeting of Elekta’s trans-Asia consortium met in Singapore to focus on the study of nasopharyngeal carcinoma (NPC). The group reviewed their respective experiences in treating NPC and deliberated research topics. In September 2012, Gleneagles Hospital became the first in Singapore to begin radiotherapy treatments with the center’s new Agility™ 160-leaf multi-leaf collimator.
Elekta Instrument AB founded by Professor Lars Leksell
First foreign subsidiary established in the USA
First fully digital accelerator introduced
First commercial Leksell Gamma Knife® delivered
Leksell Gamma Knife® Society formed
Elekta AB listed on the Stockholm Stock Exchange
IMRT Consortium established
Stereotactic Body Frame®
22
Year 1972 1985 1990 1995

SAN FRANCISCO, CALIFORNIA, USA
Following the 2005 acquisition of California-based IMPAC Medical Systems Inc., Elekta became the world’s largest supplier of oncology software. In 2012, U.S. News & World Report issued its annual list of America’s best hospitals, including the top-ranked hospitals for cancer. Out of the top 50 cancer hospitals listed, more than half are users of Elekta’s MOSAIQ® Oncology Information System.
SÃO PAULO, BRAZIL
In recent years, Elekta has strengthened its presence in Latin America. To support the region’s growing cancer management requirements; Elekta relocated its office to São Paulo, as well as acquired Radon Ltda., the leading linear accelerator service company in Brazil. Through the acquisition, Elekta’s customer base increased 25 percent regionally. In 2012, the first TPS User Meeting took place in Salvador.
NUREMBERG, GERMANY
In July 2012, IBA opened its International Competence Center (ICC).The ICC provides high-level practical training to promote safer radiation therapy to healthcare professionals. The training courses will include topics such as efficient and effective Elekta linac and RTPS commissioning. The goal is to provide high-end dosimetry training on how to plan and safely use the latest techniques, such as Elekta VMAT.
ST. LOUIS, MISSOURI, USA
In 2008, Elekta acquired St. Louis-based CMS Inc., adding a suite of advanced RTP systems, a large and growing installed base and a well-established RTP infrastructure. Most recently, an updated version of Elekta’s Monaco® treatment planning system was launched, offering customers better VMAT and workflow, in addition to support for Elekta’s Agility™ MLC, and enhanced integration with MOSAIQ®.
STOCKHOLM, SWEDEN
Before Elekta became a company in 1972, Swedish neurosur-geon Prof. Lars Leksell invented Leksell Gamma Knife® and Gamma Knife® radiosurgery in 1968 for treating a variety of intracranial disorders. Since then, more than 600,000 patients have been treated, and this gold-standard technique has been validated by over 3,000 publications documenting the results. In 2012, the company marked its 40th year.
SYDNEY, AUSTRALIA
A well-established market for Elekta, an estimated 300 clinicians from 12 countries gathered in Sydney in 2012 for Elekta’s 16th International Gamma Knife Society Meeting. The continent’s first Leksell Gamma Knife® Perfexion™ was installed in 2010 and most recently, sites throughout Australasia – including clinics in New South Wales and Melbourne – have begun treating patients with Elekta’s Agility™ MLC.
TOKYO, JAPAN
Elekta and Toshiba Medical Systems Corporation opened a 420m2 radiation therapy training center in Nasu (about 150km north of Tokyo) on July 16, 2012. With full scale operation expected by April 2013, the facility provides customers from both companies access to a training environment that includes a fully-functional Elekta linear accelerator, including supporting imaging and software systems.
Digital linear accel-erator with integrated MLC (MLCi)
Philips Radiation Therapy Division, acquired
Leksell Gamma Knife® C with Automatic Positioning System™
iViewGT™ and Active Breathing Coordinator™
Manufacturing facility estab-lished in China
Elekta IntelliMax™
Medical Intelligence Medizin-technik GmbH acquired
IMPAC Medical Systems Inc acquired
Leksell Gamma Knife® Perfexion™
Elekta Axesse™
80% of BMEI in China acquired
Elekta Infinity™
Elekta Compact™
3D Line Research and Develop-ment Srl acquired
XiO® with Electron Montecarlo
FDA clearance for VMAT with Monaco®
Elekta Agility™
Radon Ltda acquired
PrecisePLAN®
Leksell Gamma Knife® 4 C
FDA clearance for VMAT
CMS Inc acquired
Elekta Synergy® for clinical use
Neuromag Oy acquired
Resonant Medical Inc acquired
Nucletron BV acquired
23
2000 2005 2010 2012
24
What makes your center unique?
We share the passion of our customers in advancing the frontiers of cancer care, and we enjoy news from clinics that are treating patients more effectively, precisely and efficiently with the help of Elekta technology. Here are a few stories from across the globe.
In April, the Prime Minister of India, Dr. Manmohan Singh, honored the Dr. Bhubaneswar Borooah Cancer Institute (bbci) by presiding over the inauguration of its Elekta Synergy® linear accel-erator. Established in 1973, bbci is among the leading cancer institutes in east India, and was recognized as a Regional Cancer Centre in 1980.
In the state of Assam – as it is across India – head-and-neck cancer and tobacco-related cancers (mainly lung cancer) comprise 15-20 percent of the total cancers. Among males, the top three cancer incidences are oral cavity, larynx and lung cancer, while in women, cervical and breast cancer are the most common. In metro areas, prostate and breast cancer incidences are rising. At any given time in India, about three million individuals have cancer, with approximately 960,000 new cases identified per year, and rising rapidly. A national task force estimates that two-thirds of those diagnosed with cancer will need radiation therapy.
Elekta and other healthcare providers have collab-orated with medical centers and clinics across India to address a shortage of radiation therapy equipment. bbci’s new Synergy system is fully equipped with the most advanced radiation therapy techniques in use today, including imrt, igrt, srs and sbrt. l
Prime Minister of India Inaugurates Elekta Linear Accelerator
‘‘In metro areas, prostate
and breast cancer incidences are rising.”
ELEKTA CUSTOMERS IN FOCUS

25
In June, Vejle Hospital, Region of Southern Denmark, and Elekta collaborated to host a sympo-sium on advanced treatment of breast cancer. Bringing together 117 participants from 18 countries, including more than a dozen European countries and participants from the us and Canada, the sym-posium focused on topics such as target delineation, 3d conformal, imrt and vmat planning, sparing of the heart using breath hold or gated techniques and patient positioning protocols.
Together, with Elekta, Vejle Hospital donated the registration fee for the symposium to the Danish Cancer Society, totaling nearly dkk 83,800 (usd 14,200). Closely aligned with Elekta’s mis-sion to improve, prolong and save lives, the Danish Cancer Society – the largest organization of its kind in Denmark – is very active in fighting cancer.
In his closing remarks, Martin Berg, msc, Head of Medical Physics at Vejle Hospital and symposium chair, said: “The meeting was a great success and hopefully laid the groundwork for a second such symposium.”
At Vejle Hospital, all left-sided breast cancer patients receiving radiotherapy after surgery are treated with Elekta Active Breathing Coordinator™, which assists patients in maintaining a deep-breath hold while irradiating the breast. This separates the
breast tissue from the heart, which helps irradiate more breast tissue while sparing the heart and its critical blood vessels at the same time.
The clinical focus at Vejle Hospital – apart from breast cancer treatments – includes lung cancer, prostate cancer and rectal and anal cancers. The department is currently developing an mri compatible shielded applicator for conformal hdr brachytherapy boosts given to rectal and anal cancer patients receiving intensity modulated external beam treatment. l
Danish Hospital Donates Proceeds from Breast Cancer Symposium to Local Cancer Society
‘‘The meeting was a great success and
hopefully laid the groundwork for a second such symposium.”

26
What makes your center unique?
Do you have some special treatment or compelling patient story from your center that you want to share? Tell us! Send us your story and we may feature your clinic in an upcoming issue of Wavelength. Write a brief description of your story, include photographs (high-resolution jpgs) and your name, clinic or hospital name and email address. Send it, marked “Unique Center”, to [email protected]. We look forward to hearing from you!
Tell us what’s happening where you are!
Among the largest public hospitals in Brazil, Barretos Cancer Hospital recently made a major commitment to the healthcare of the country’s citizens by acquiring a range of advanced Elekta cancer management solutions. The technology, including Elekta Synergy® Platform, Monaco® and XiO® treatment planning systems and Clarity® 3d ultrasound-assisted image guided radiation therapy (igrt) were delivered in August 2012.
“As a teaching hospital, it was important for us to broaden our range of cancer treatment systems beyond our existing equipment – to enable us to evaluate how Elekta’s solutions might improve the provision of healthcare,” says Rodrigo Gadia, md, Head of the Department of Radiotherapy. “In Brazil, this is critical, as access to advanced treatment technology is limited. In particular, we hope that use of Elekta Synergy Platform – once it is upgraded with igrt capabilities – may rep-resent a practical demonstration of a good cost-benefit ratio for the use of igrt in Brazil.”
Barretos will use its two Clarity systems – the first in Latin America – to provide image guidance for soft tissue targets. The center also intends to pursue clinical studies on the planning benefits of integrating 3d ultrasound with ct based planning. This work will help explore the local applicability of a relatively low-cost imaging modality that could be retrofitted on existing equipment in the region.
“Clarity will be another way to obtain fast, accu-rate soft tissue igrt that we can integrate with any of our linear accelerators, with the added benefit of non-invasiveness,” he says. l
Brazilian Hospital First in Latin America to Acquire Clarity Soft Tissue Visualization Software
‘‘Clarity will be another
way to obtain fast, accurate soft tissue IGRT that we can integrate with any of our linear accelerators.”
ELEKTA CUSTOMERS IN FOCUS

imagine
...twice the leaves at twice the speed
With Agility™, it’s reality.As the ultimate device for advancing modern radiotherapy, Elekta’s Agility MLC precisely sculpts radiation with 160 high-resolution leaves across a 40 cm x 40 cm field. Capable of managing the broadest spectrum of therapies, Agility also boasts ultra-fast leaf movements with extraordinarily low leakage to maximize the potential for advanced techniques such as SRS, SRT and VMAT.
Human care makes the future possible.More at elekta.com/imagine
4513
371
099
3 03
:12
Agility is not licensed for sale in all markets. Please contact your local Elekta representative for details.

Corporate Head Office:
Elekta AB (publ) Box 7593, SE-103 93 Stockholm, Sweden
Tel +46 8 587 254 00 Fax +46 8 587 255 00
Regional Sales, Marketing and Service:
North America
Tel +1 770 300 9725 Fax +1 770 448 6338
Europe, Latin America, Africa, Middle East & India
Tel +46 8 587 254 00 Fax +46 8 587 255 00
Asia Pacific
Tel +852 2891 2208 Fax +852 2575 7133
www.elekta.com
Human Care Makes the Future Possible