warrington clinical commissioning group … papers/archived board... · large conference room, the...
TRANSCRIPT
Warrington Clinical Commissioning Group
Meeting of the Governing Body
Agenda – 13th September 2017
WARRINGTON CLINICAL COMMISSIONING GROUP
MEETING OF THE GOVERNING BODY TO BE HELD ON WEDNESDAY 13th SEPTEMBER 2017 AT 1.30 P.M. LARGE CONFERENCE ROOM, THE GATEWAY, SANKEY STREET,
WARRINGTON
A G E N D A Agenda Item No
Timings (approx.)
044/17 1.30 The role of the Third Sector in supporting the Development and Delivery of Integrated Health and Social Care
Michael Sheppard CEO Warrington Community Living
Presentation
A 1.45 Apologies for Absence: Nick Atkin
All
B Declarations of Interest in Agenda Items
All
C 1.50 Minutes of Warrington Clinical Commissioning Group Governing Body Meeting held on Wednesday 12th July 2017 (to approve)
D Bunstone Enclosure
D Matters arising from the meeting
D Bunstone Enclosure
E 1.55 Chair's Remarks and Questions from the Floor
D Bunstone Verbal
F 2.00 Governing Body Member feedback from Federations
GP Federation Representatives
Verbal
F 2.10 Patient Representative Feedback
P Taylor Verbal
G 2.20 Clinical Chief Officer Report (to note and endorse)
A Davies Enclosure
Corporate Business & Governance:
045/17 2.30 Assurance Framework (to receive assurance)
R Knight Enclosure
046/17 2.40 Update Report on Emergency Preparedness, Resilience and Response (EPRR) (to approve)
R Knight Enclosure
047/17 2.50 Quality Report (to receive assurance)
J Wharton Enclosure
048/17 3.00 Financial Performance for the period ending 31st July 2017 (to note)
D Cooper
Enclosure
Warrington Clinical Commissioning Group
Meeting of the Governing Body
Agenda – 13th September 2017
049/17 3.10 Performance Report (to receive assurance)
P Broadhead Enclosure
050/17 3.20 Contract Report (to note)
P Broadhead Enclosure
051/17 3.30 Commissioning Intentions Refresh 2017/19 (for approval)
L Bennett Enclosure
052/17 3.40 Terms of Reference for Joint Committee of NHS Halton CCG; NHS Knowsley CCG; NHS St Helens CCG and NHS Warrington CCG (to approve)
A Davies Enclosure
053/17 3.50 Business Conduct & Conflict of Interest Policy (to ratify)
N Armstrong Enclosure
Items to Note:
054/17 4.00 Summaries of Governing Body Committees
Audit Committee Terms of Reference (to note and ratify)
Respective Chairs
Enclosure
055/17 4.05 Any Other Business
All
056/17 4.10 Questions from the Floor
All
057/17 4.15 Date and Time of Next Meeting: Wednesday 8th November 2017 at 2.00 p.m. Board Room, Arpley House, Birchwood
Warrington Clinical Commissioning Group Minutes of Governing Body Meeting 12 July 2017
1
Minutes of the Meeting of the Governing Body held on Wednesday 12th July 2017 at 2.00p.m.
Board Room, Arpley House, Birchwood
Present:
Nick Atkin (Chair) Lay Member
Dr Andrew Davies Clinical Chief Officer David Cooper Chief Finance Officer
Dr Laura Mount GP Governing Body Member – Teaching Practices Dr Ian Watson GP Governing Body Member – Phoenix Federation
Pat Taylor Patient Representative Dawn Chalmers Deputy Chief Nurse Representing John Wharton In Attendance:
Pam Broadhead Chief Performance Officer Nick Armstrong Chief Operating Officer
Sarah Leach Implementation Manager, Continuing Health Care Team
Tracy Flute Head of Public Health Intelligence, Public Health Team
Zoe Graham Senior Communications Officer Julie McCarthy Executive Assistant (Minutes)
There were 3 members of the public in attendance.
Agenda Item No
Action
A APOLOGIES FOR ABSENCE Dr Dan Bunstone, Mr John Wharton, Mr Gareth Hall, Dr Rashmi Jain, Dr Michihiro Tomonaga, Mrs Linda Bennett, Mr Simon Kenton
033/17 PRESENTATION – PERSONAL HEALTH BUDGETS Ms Sarah Leach, Implementation Manager from the Continuing Healthcare Team, delivered a presentation on Personal Health Budgets. Dr Ian Watson questioned the terminology with regard to the criteria for continuing healthcare for adults in the community; it was confirmed that the eligibility is for more complex care. Dr Laura Mount asked if the allocated funds are monitored under an NHS Contract. Mrs Pam Broadhead confirmed that work is being undertaken by Ms June Walsh and Ms Sarah Leach to ensure that the allocated funds are regulated under NHS Contracts as soon as possible. Action: Pam Broadhead will liaise with June Walsh and Sarah Leach to ensure that the contracts are in place. Dr Laura Mount questioned if patients who lack capacity, and their rights are governed by the Mental Health Capacity Act, have
Pam Broadhead
Agenda Item No: C
Warrington Clinical Commissioning Group Minutes of Governing Body Meeting 12 July 2017
2
representation for the decisions that are made on their behalf. Ms Sarah Leach confirmed that a set criteria has to be met, a ‘Best Interest’ Meeting will be held and the same process will apply for options of choice. Mrs Pat Taylor stated that the patients that she had spoken to, who already have personal health budgets, confirmed that they prefer this system; it was questioned if a patient decided that they would like to go back to an allocated system of care, would they have this option. Ms Sarah Leach confirmed that there hadn’t been any patients in Warrington who had decided yet to go back to the previous system; however this is an option. If the patient does not wish to handle the finance and funding of the care themselves; the CCG can arrange for funding to be invoiced. Mrs Pam Broadhead asked if an increase in the use of personal care budgets would have an impact on primary care. Sarah Leach confirmed that the budgets were having a positive effect, for example, one patient who had more support at home had reduced the requirement for acute care. The Chair thanked Sarah Leach for the Personal Health Budget information.
B DECLARATIONS OF INTEREST IN AGENDA ITEMS There were no declarations of interest in the agenda items aside to those already declared on the CCG Register of Interest.
C
MINUTES OF THE WARRINGTON CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING HELD ON WEDNESDAY 10TH MAY 2017
The minutes of the meeting held on 10 May 2017 were recorded as accurate record of the meeting with the exception of: Page 4 – Phoenix Federation Update Remove sentence: …. and that the training and development is in place to ensure that they are fully skilled up.
The minutes were approved as a true and accurate record of the meeting.
D
MATTERS ARISING FROM THE MEETING There were no matters arising.
E
CHAIR’S REMARKS AND QUESTIONS FROM THE FLOOR Mr Nick Atkin welcomed everyone to the meeting and advised that the public and Governing Body members can be assured that, in light of the Grenfell Tower fire tragedy, all local NHS Buildings have been checked and they meet fire regulations and don’t have similar cladding. NHS Warrington CCG extended its sympathy and condolences to all those
Warrington Clinical Commissioning Group Minutes of Governing Body Meeting 12 July 2017
3
affected by this tragedy. There were no questions from the floor.
F
GP GOVERNING BODY MEMBER FEEDBACK FROM FEDERATIONS Teaching Practices Federation Dr Mount presented the feedback from the last federation meeting which was held on 28 June 2017 where the following items were discussed:
The Four Seasons Medical Centre was welcomed as a new member and the Terms of Reference were updated accordingly to reflect this change.
The Procedures of Limited Clinical Priority. Diabetes – the work of the task force was recognised. Primary Care Development. PMS and the diagnostic bundle and any interface issues. Appointment letter issues are on-going – issues will be reported
to the Quality Committee. Warrington Health Plus – the vote results were 1 yes, 1 no and 1
undecided. Phoenix Federation Dr Watson advised that the Phoenix Federation had met on 29 June 2017, the following items were discussed:
Current ASC Stroke Services – the transfer of services to Whiston The Procedures of Limited Clinical Priority. There will be an event to discuss the Emotional Health and Well
Being of Children held in Penketh. Diabetes funding and targets. Primary Care Development Group Diagnostic Group Local Enhanced Service Template – it was confirmed that the
template had a deadline for completion to ensure that if amendments are required to be made, these can be done prior the submission of the template. Marie Ann Hunter has added some tips for completion onto the intranet. Action: Pam Broadhead will liaise with Marie Ann Hunter to ensure that the template completion is not onerous.
Healthy Warrington Local Commissioning Group Federation Dr Andrew Davies provided feedback on behalf of Dr Tomonaga from two recent meetings; the following items were discussed: 25 May 2017
Accountable Care Partnership Five year forward view and non-recurrent funding The Warrington Brand ECG Equipment
Pam Broadhead
Warrington Clinical Commissioning Group Minutes of Governing Body Meeting 12 July 2017
4
Changes to the Deep Vein Thrombosis Pathway Training Needs Assessment Primary Care and SPA – inconsistencies with regard to opening
hours has been fed back to the commissioners. IT issues – looking at 4G networks. Recovery of Special Losses – any liabilities.
29 June 2017
Data dry run – populated from scratch Warrington Health Plus and how this will flow into Accountable
Care Partnership – 4 voted yes. GPs have taken on a physio pilot to encourage core stability to
prevent falls.
Action: Update for next Governing Body Meeting the positive effects of the physio pilot and the prevention of falls. Warrington Alliance Dr Jain will present feedback from her last federation meeting at the next Governing Body Meeting.
The Governing Body Members NOTED the Federation Updates.
Dr Jain
G PATIENT REPRESENTATIVE FEEDBACK Mrs. Pat Taylor, Patient Representative presented her report which focussed on feedback from patients via activity undertaken, the main agenda items that were discussed at the CCG’s Health Forum, included:
The changes to stroke services; the rationale for the changes has been explained to patients and they accept that the changes were necessary.
There is concern that homeless people aren’t engaging with health services; Katie Horan is engaging with vulnerable people to try and improve this situation.
A THRIVE event for young people had been well attended. Diabetic patients will be encouraged to take up opportunities for
education. It had been encouraging that there had been an increase in men
attending health clinics as they are now based at the Halliwell Jones Stadium.
Action: Mr. Nick Atkin confirmed that he is the Chair of the Warrington Homeless Priority Action Group and he would liaise with Pat Taylor outside the meeting to see how improvements to the health of the homeless can be made.
Dr Andrew Davies confirmed that the engagement with regard to the changes to the stroke services had achieved positive results. Dr Laura Mount questioned if the service was being monitored. It was confirmed that patient experience is measured by a Sentinel Audit and the Stroke National Audit Programme (SSNAP) data has improved.
Nick Atkin
Warrington Clinical Commissioning Group Minutes of Governing Body Meeting 12 July 2017
5
Mrs. Pat Taylor confirmed that another engagement event would be beneficial. Mr. Nick Atkin highlighted that the engagement process to ensure that the public to understand the rationale for changes to patient services is very important. Mr. Nick Atkin thanked Mrs. Pat Taylor for her update.
The Governing Body NOTED the content of the Patient Representative Feedback.
H
CLINICAL CHIEF OFFICER’S REPORT
Dr Davies presented his report to provider members with an update on key issues not covered elsewhere in an individual report and information about the activities undertaken by the Clinical Chief Officer and his team since the last report. Dr Davies highlighted the following key areas from this month’s Clinical Chief Officer’s report:
The Purdah period had now finished and normal business has resumed.
Plans are in place to update the CCG statutory guidance on managing conflicts of interest and associated supporting documents.
There have been changes to the vaccination programmes enhanced service specifications contracts for 2017/18. The vaccines have traditionally been provided by public health but a small amount of funding has now been allocated for this.
The roll-out of NHS Wi-Fi to primary care has now moved into its second phase.
A meeting held on 5 July 2017 to discuss the Five Year Forward View had taken place; Andrew Gibson was announced as the new Chief Executive and Richard Barker provided a national view of Sustainability and Transformation Plans; with the focus being on Primary Care, Mental Health, Cancer and Urgent and Emergency Care.
Dr Davies reported that:
Sue Musson has taken up the position of Independent Chair of ‘Well Warrington’, the Borough’s Accountable Care Partnership Board, which aims to bring together resources for health and social care into one place; forging new partnerships and delivering more efficient value for money services.
Ingrid Fife has been confirmed as being the new Chair of the Alliance LDS Leadership Group.
Mr. Nick Atkin thanked Dr Davies for the update on the business of the Clinical Chief Officer.
The Governing Body NOTED the contents of the Clinical Chief Officer’s report.
034/17 QUALITY REPORT
Warrington Clinical Commissioning Group Minutes of Governing Body Meeting 12 July 2017
6
Dawn Chalmers presented this report to provide information about the quality of services commissioned by Warrington CCG, by identifying areas where performance falls below expected standards and to see scrutiny of the assurance provided by the Committee in relation to risks and concerns that may impact on quality. The following areas were highlighted:
There had been a never event on an individual at the hospital trust. This was the third event to have been reported; schemes have been implemented to improve the safety culture.
Concerns have been raised with regard to complex spinal surgery; this service has been suspended and discussions are taking place with the Walton Centre.
A letter had been received from the Clatterbridge Cancer Centre highlighting that there are workforce issues that have led to a shortage of oncologists. Clinics have been consolidated and the CCG has employed a nurse consultant. Improvements are required to be implemented by January 2018. Chemotherapy services have not been affected.
Mr. Nick Atkin questioned why the letter had been received at such short notice and why hadn’t the provider notified the commissioner. Dr Andrew Davies confirmed that a recent teleconference with Clatterbridge Cancer Centre NHS Trust and Warrington and Halton Hospital NHS Foundation Trust had now resolved some of the issues. Dawn Chalmers reported that the Governing Body and Public could be assures that Mr Ian Paterson, a consultant surgeon employed by the Heart of England NHS Foundation Trust, who had also operated in Spire’s Parkway and Little Aston Hospitals, had not worked at all the Warrington Spire Hospital.
The Governing Body NOTED and discussed the work being carried out with the providers to address concerns regarding areas of quality provision where the provider may be experiencing difficulties. The Governing Body NOTED the assurances from the acute provider’s mortality work and the establishment of the systems and processes to scrutinise and address mortality issues.
035/17 FINANCIAL PERFORMANCE FOR THE PERIOD ENDING 31ST MAY 2017
Warrington Clinical Commissioning Group Minutes of Governing Body Meeting 12 July 2017
7
Mr. Cooper presented this report and highlighted the following areas: The financial performance at the end of month 2 for the end of May is in line with the planned position. Within the month 2 reporting issued to NHS England, the net financial risk was reported as break even. At month 2, using the April performance detail, there is adverse variance across a number of acute providers. It was reported that the CCG has adopted a Quality, Innovation, Productivity and Prevention (QIPP) programme and the CCG is considering participating in a Mersey Internal Audit Agency (MIAA) programme for Quality, Innovation, Productivity and Prevention. The Governing Body members were keen for the CCG to participate in this MIAA review. Regular Collaborative Sustainability Meetings are taking place with the Trust to focus on the sustainability of finance and performance, recovery and to develop mitigating actions. Action: Feedback and Recovery Ideas will be an agenda item at the September Finance and Performance Committee. Mr. David Cooper confirmed that discussions with regard to recovery and sustainability are taking place on a regular basis. Dr Laura Mount questioned who the membership of the Collaborative Sustainability Meeting was; it was confirmed that Mrs Linda Bennett is the Chair, Mr David Cooper, Mrs Pam Broadhead and members of the Acute Hospital Management Team are invitees. Clinicians from the Trust are co-opted to attend the meetings. An invitation will be extended to GPs.
The Governing Body noted the financial position as at the end of May 2017 and acknowledged the financial risks identified in the report.
036/17 PERFORMANCE REPORT
Mrs. Broadhead presented this report to provide members with an update on NHS Warrington CCG’s delivery of key areas from the Improvement and Assessment Framework. Mrs Broadhead reported that she was delighted to inform the Governing Body that the All Party Parliamentary Group of Cancer made an award to the CCG on 5th July in recognition that NHS Warrington CCG is the second most improved CCG for one-year cancer survival rates. The Chair commented that this was indeed recognition and was something to be celebrated. Mrs Broadhead reminded the Board that this is a reflection of the hard work undertaken by commissioners, providers and primary care to ensure that the health of the patients in Warrington is excellent.
Warrington Clinical Commissioning Group Minutes of Governing Body Meeting 12 July 2017
8
Mrs Broadhead continued to inform the meeting that this month’s performance report is more of an informative report to reiterate to the governing body the requirements of the CCG with respect to the NHS constitution. The report details the summary position for 2016/17 and gives a first overview of the 2017/18 position. Mrs Broadhead reiterated that for those members of the governing body who can access the Aristotle system this information is available on that system. Mrs Broadhead informed the meeting that future performance reports to the governing body will, as previous, focus on areas where the CCG is in exception and that it will detail and explain the control processes in place to remedy to ensure that Warrington patients receive the rights and pledges as set out in the constitution. Dr Watson asked for an explanation as to the poorer than usual performance in April. Mrs Broadhead explained that a collaborative exercise of validation in areas such as cancer waits had caused part of this exception as well as failures in both the A&E waiting times and ambulance response times. Pam Broadhead confirmed that the Performance Team does respond to the monitoring to ensure that there is an improvement in performance. Action: Pam Broadhead to ensure that the Communications Team will communicate the cancer survival information to Patient Representatives.
The Chair confirmed that the meeting received the report and that it suitable assurance had been provided.
Pam Broadhead
The Governing Body noted the Performance Report.
037/17 GP FORWARD VIEW SUBMISSION
Marie Ann Hunter confirmed that the CCGs GP Forward View submission had been sent on 23 December 2016 and feedback from NHS England had been positive. Marie Ann Hunter explained that the CCG had allocated £0.322m to Primary Care over the next two years. The CCG will invest in the following schemes; Acute Signposting, Social Prescribing and Supporting Self Care. It was confirmed that funding has been allocated to a pool budget to provide training for clerical staff in GP surgeries; a positive response had been received to the Training Needs Analysis questionnaire and 6 bids to provide the training have been received so far. Marie Ann Hunter explained that five practices have received income from NHS England under the resilience programme; £20,000 has been allocated to Stretton Medical Centre; and £2,000 was allocated to Folly Lane Medical Centre, Westbrook Medical Centre, Chapelford Health Centre and Causeway Medical Centre. Marie Ann Hunter advised that the CCG is currently gathering base line data of the current work force across every practice in Warrington and this has been used to develop a primary care work force strategy.
Warrington Clinical Commissioning Group Minutes of Governing Body Meeting 12 July 2017
9
Dr Laura Mount recommended that international recruitment is included in the strategy, along with current schemes and extended access. Dr Laura Mount questioned if planning for the retirement of GPs had been taken into account as over the next two to three years there will be a reduction in the workforce due to retirement. Marie Ann Hunter confirmed that the retirement of both GPs and nurses had been taken into account. Mrs Tracy Flute highlighted that public health had taken into account population changes and strategic estates in the Joint Strategic Needs Assessment document. This document would aid the continual refresh of a revised local plan. Action: Mrs Tracy Flute will send the JSNA document to Marie Ann Hunter.
Tracy Flute
The Governing Body noted the contents of the CCGs submission to NHS England. The Governing Body noted the work to date. The Governing Body agreed the next steps for implementation of the GPFV.
038/17 PUBLIC HEALTH ANNUAL REPORT
Mrs Tracy Flute presented the Public Health Annual report to the Governing Body Members on behalf of Dr Muna Abdel Aziz. The members were advised that prevention is high on the agenda and it is ‘Everybody’s Business.’ Work will continue with all partners to improve the health of residents in Warrington. A range of interventions and national best practice has been deployed; with a focus being on:
People – Well Being Hub, centralised services, improve housing, holistic assessments
Place – Redevelopment, regeneration and housing provision Prosperity – equal opportunities, economic growth.
Mrs Tracy Flute advised that there will be system wide collaborative effort, the brand will be embedded into primary care and each practice will be encouraged to appoint a public health champion. It was reported that the Hub is a real opportunity for patients to benefit from referrals and the recommendations will be in the collaborative plan. It was confirmed that Partners will be asked to support the lifestyle survey at a Sub-Warrington level and the Governing Body Members were asked for their commitment.
Warrington Clinical Commissioning Group Minutes of Governing Body Meeting 12 July 2017
10
Mr Nick Atkin highlighted that the Public Health Annual Report is a useful document and acts as a reference point when decisions are made throughout the year. Dr Laura Mount asked Mrs Tracy Flute if she was asking for resources as well as support, and her response was no, that it was for support and not resource although that question will be raised at a later date to system partners. Dr Laura Mount confirmed that in her work at Folly Lane Medical Centre, the Well Being Hub and the Citizens Advise Bureau had helped to make lives more bearable. Dr Laura Mount questioned if the changes to funding would have a detrimental effect on the health education offered to children in schools. Tracy Flute replied that Public Health does not have any influence on how budgets in schools are spent, many schools are changing to academy status and the only service that is then funded by Public Health is school nursing provision. Dr Laura Mount asked if there is anything that the CCG could do. Action: Mrs Tracy Flute will liaise with Dr Muna Abdel Aziz with regard to any support that the CCG can provide to promote health education in schools.
Tracy Flute

Warrington Clinical Commissioning Group Minutes of Governing Body Meeting 12 July 2017
11
The Governing Body discussed the issues raised within the report and supported the recommendations to:
Maximise the opportunity to systematically embed prevention within Primary Care through the Warrington Brand, and support the aim to ensure every Practice has a primary care public health champion.
Commit as a pro-active partner to Warrington Wellbeing. There is real opportunity to ensure that pathways are developed to ensure that the appropriate patients are referred to Warrington Wellbeing. Getting this right will both benefit patients and reduce demand on General Practice. Close collaborative working and effective exchange of patient information between Primary Care and Warrington Wellbeing is fundamental to making this happen.
Support the work to embed prevention across all commissioned services and clinical pathways. Working in this way, rather than seeing prevention support as a separate strand, will maximise the opportunities to support all patients holistically and improve their wellbeing.
Commit to supporting and resourcing a repeat population lifestyle survey to update the information we have on prevalence of key population risk factors. This information is used by all partners to inform numerous strategies. Without updated intelligence we have no way of measuring the impact of our collective efforts. Support is needed to both fund the survey, and also ensure methods used are robust and comparable; this means facilitating appropriate access to an accurate sampling frame.
Capitalise on the planning process in order to ‘design in health’ and improve and develop the necessary infrastructure for health and wellbeing. Continued collaborative working is needed to ensure the NHS Strategic Estates Plan and council masterplan are aligned and focussed on improving wellbeing and addressing inequalities.
Commit to embracing the concept of commissioning for social value. As public sector commissioners there is much more we could all do through the procurement process to maximise the additional benefit that can be generated to support the social economy and influence local economic growth.
039/17
JSNA ANNUAL REPORT
Tracy Flute reported that the Joint Strategic Needs Assessment has been operational since 2008 and it was stream lined in 2015. It was confirmed that the over-arching indicators for prioritising a work programme are:
Unemployment Sexual Health Substance Misuse
Warrington Clinical Commissioning Group Minutes of Governing Body Meeting 12 July 2017
12
Emotional Well Being and Health of Children and Young People Vulnerable Adults and Older People
There will be a deep dive into:
Air pollution – deferred from 2016 work programme
Smoking
Cardiovascular Disease prevention
Domestic Abuse
Tracy Flute reported that there will be a refresh of the pharmaceutical needs assessment before 1 April 2017. Work driven by the Steering Group and Working Groups will use intelligence to identify gaps in services. Mr. Nicholas Armstrong confirmed that the CCG links in with the Joint Strategic Needs Assessment and are champions in key areas. Dr. Andrew Davies highlighted that the cancer targets had improved with the exception of breast cancer; Tracy Flute confirmed there will be focus on breast cancer to identify why this target is lagging. Dr. Andrew Davies confirmed that the Winter mortality data had improved; Tracy Flute confirmed that the data is generally good but she had been unable to identify a reason why there had been an anomaly in the previous year. Mr. Nick Atkin asked why the number of patients registered is higher than the Office for National Statistics data; it was confirmed that some patients from Vale Royal attend practices in Warrington; the town is the second lowest funded per capita and the data does not keep up with growth, it has a three year lag. Dr. Andrew Davies questioned if there were any plans to look at how Scandinavia supports its population. Tracy Flute confirmed that fuel poverty and energy efficiency is good in Warrington.
Action: Tracy Flute will liaise with Dr Ian Watson to provide a public health overview of the JSNA to the Phoenix Federation.
Tracey Flute
The Governing Body approved and supported the following three recommendations:
To continue to pro-actively engage in the JSNA programme. This is needed in both the annual prioritisation of chapters and in the scoping, direction and production of those chapters.
To support access to the necessary data and intelligence required to inform and develop the topic specific chapters, and the PNA.
To continue to support the dissemination of intelligence from the JSNA and ensure that findings and recommendations inform commissioning strategies and action plans.
Warrington Clinical Commissioning Group Minutes of Governing Body Meeting 12 July 2017
13
040/17 SUMMARIES OF GOVERNING BODY COMMITTEES
The Governing Body members reviewed the Committee Summaries.
The Governing Body noted the decisions made on their behalf and supported them.
041/17 ANY OTHER BUSINESS There was no other business raised at the meeting
042/17 QUESTIONS FROM THE FLOOR There were no questions from the floor.
043/17 Date and Time of Next Meeting Wednesday 13th September 2017 at 2.00 p.m. in the Board Room, Arpley House Signed …………………………………………….. Date ……………….

KEY:
Governing Body Meeting 12
th July 2017
Complete
Not Started
In Progress
Delayed
NHS WARRINGTON CCG GOVERNING BODY MEETING ACTION NOTES 12th July 2017
(Actions highlighted in red have been carried over from the previous meeting)
Present: Apologies
Dr Andrew Davies, Clinical Chief Officer Dr Michihiro Tomonaga, GP Governing Body Member
David Cooper, Chief Finance Officer Dr Dan Bunstone, Chair
Nick Atkin, Lay GB Member Gareth Hall, Lay GB Member
Dr Laura Mount, GP Governing Body Member Dr Rashmi Jain, GP Governing Body Member
Dr Ian Watson, GP Governing Body Member John Wharton, Chief Nurse & Quality Lead
Pat Taylor, Patient Representative Linda Bennett, Chief of Healthcare Commissioning
Dawn Chalmers, Deputy Chief Nurse
Action Ref
Agenda Item Action Lead Person Date Required
Status Action Recorded
004/17 033/17 12.7.17
Presentation – Personal Health
Budgets
Pam Broadhead will liaise with June Walsh and Sarah Leach to ensure that the contracts are in place.
P Broadhead 13.9.17
Action complete - June Walsh has reviewed all individual placements made by CCG teams including the CHC team and is now working with the relevant commissioners, where appropriate, to put NHS Standard Contracts in place. There is a risk on the risk register in relation to placements where an NHS Standard Contract is not in place

KEY:
Governing Body Meeting 12
th July 2017
Complete
Not Started
In Progress
Delayed
005/17 F GP GB
Federation Summaries
12.7.17
Pam Broadhead will liaise with Marie Ann Hunter to ensure that the template completion is not onerous.
P Broadhead 13.9.17 Action Complete - Pam Broadhead has liaised with Marie-Ann Hunter, with the performance team and the CSU. A number of meetings have been held including a “deep dive” meeting on 8th September and a revised return for practices issued. The CSU will now be part of the reporting process to make it less onerous but still in line with the contractual requirements.
006/17 F GP GB
Federation Summaries
12.7.17
Update for next Governing Body Meeting the positive effects of the physio pilot and the prevention of falls.
Ian Watson 13.9.17
007/17 G Patient
Representation Feedback 12.7.17
Mr. Nick Atkin confirmed that he is the Chair of the Warrington Homeless Priority Action Group and he would liaise with Pat Taylor outside the meeting to see how improvements to the health of the homeless can be made.
N Atkin 13.9.17 Action complete - Meeting scheduled with Pat. Will also raise with relevant contacts from Warrington Homelessness PAG.
KEY:
Governing Body Meeting 12
th July 2017
Complete
Not Started
In Progress
Delayed
008/17 035/17 Finance Report 12.7.17
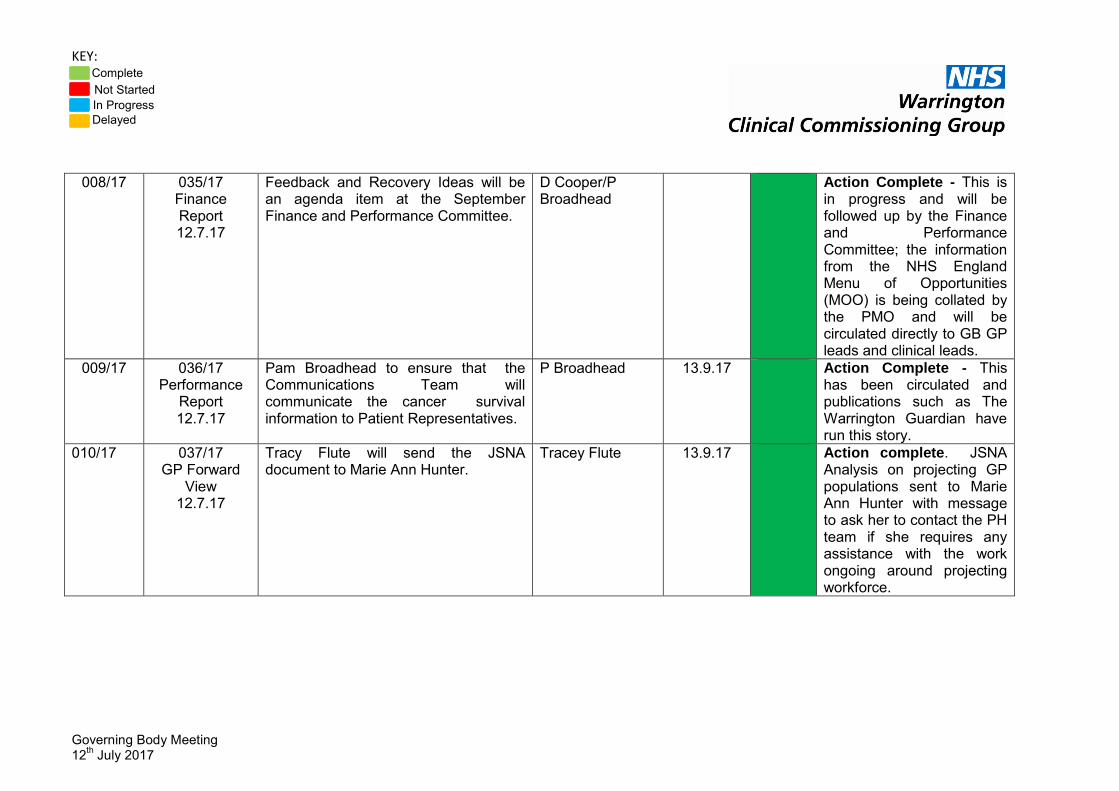
Feedback and Recovery Ideas will be an agenda item at the September Finance and Performance Committee.
D Cooper/P Broadhead
Action Complete - This is in progress and will be followed up by the Finance and Performance Committee; the information from the NHS England Menu of Opportunities (MOO) is being collated by the PMO and will be circulated directly to GB GP leads and clinical leads.
009/17 036/17 Performance
Report 12.7.17
Pam Broadhead to ensure that the Communications Team will communicate the cancer survival information to Patient Representatives.
P Broadhead 13.9.17 Action Complete - This has been circulated and publications such as The Warrington Guardian have run this story.
010/17 037/17 GP Forward
View 12.7.17
Tracy Flute will send the JSNA document to Marie Ann Hunter.
Tracey Flute 13.9.17 Action complete. JSNA Analysis on projecting GP populations sent to Marie Ann Hunter with message to ask her to contact the PH team if she requires any assistance with the work ongoing around projecting workforce.
KEY:
Governing Body Meeting 12
th July 2017
Complete
Not Started
In Progress
Delayed
011/17 038/17 Public Health Annual Report
12.7.17
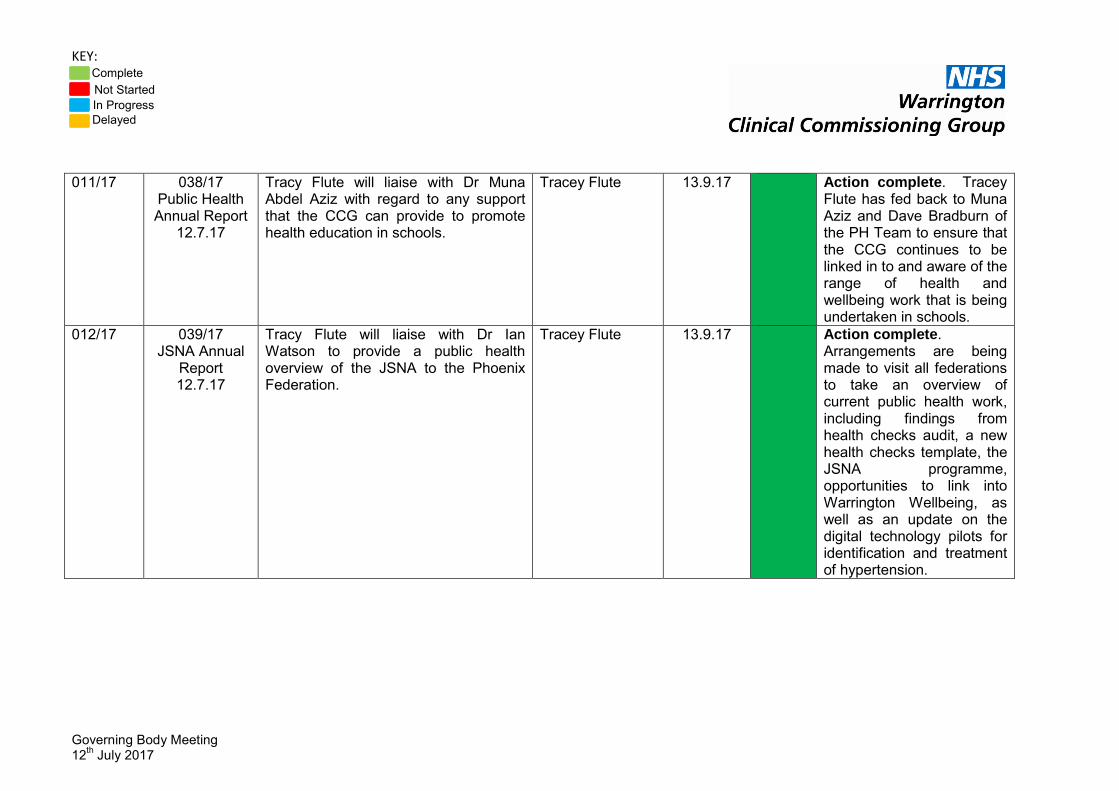
Tracy Flute will liaise with Dr Muna Abdel Aziz with regard to any support that the CCG can provide to promote health education in schools.
Tracey Flute 13.9.17 Action complete. Tracey Flute has fed back to Muna Aziz and Dave Bradburn of the PH Team to ensure that the CCG continues to be linked in to and aware of the range of health and wellbeing work that is being undertaken in schools.
012/17 039/17 JSNA Annual
Report 12.7.17
Tracy Flute will liaise with Dr Ian Watson to provide a public health overview of the JSNA to the Phoenix Federation.
Tracey Flute 13.9.17 Action complete. Arrangements are being made to visit all federations to take an overview of current public health work, including findings from health checks audit, a new health checks template, the JSNA programme, opportunities to link into Warrington Wellbeing, as well as an update on the digital technology pilots for identification and treatment of hypertension.
AGENDA ITEM NO: G
Patient Representation Feedback Warrington CCG Governing Body Meeting 13
th September 2017
GOVERNING BODY MEETING:
Governing Body Meeting
DATE OF MEETING:
13th September 2017
REPORT AUTHOR AND JOB TITLE:
Pat Taylor Governing Body Patient Representative Katie Horan Engagement Manager
REPORT TITLE:
Patient Representative Feedback
STRATEGIC OBJECTIVES:
Please tick which strategic objectives the paper relates to
NHS Constitution
* Improve quality of services
*
Sustained financial balance
Improve healthy life expectancy
Reduce inequalities
* Build an effective and motivated workforce
Sound governance arrangements
*
OUTCOME REQUIRED (tick)
Approval
Assurance
* Discussion
Information
*
EXECUTIVE SUMMARY
The report aims to provide the CCG Governing Body with feedback from patients via activity undertaken from the Patient Representative. The report highlights the main agenda items that were discussed at the CCG’s Health Forum, including outreach from the Health Forum to people with learning disabilities. The main discussions were:
Changes to Stroke services
RECOMMENDATIONS
To note the contents of the report and provide any relevant feedback to the Health Forum
The report aims to assure the Governing Body the voice of patient is integral to the CCG
AGENDA ITEM NO: G
Patient Representation Feedback Warrington CCG Governing Body Meeting 13
th September 2017
Outline any engagement – staff, clinical, stakeholder and patient / public
Feedback from Warrington CCG’s Health Forum
Are there any conflicts of interest which may be associated with this paper?
N/A
Does this paper address any existing risks which are included on the Assurance Framework or Risk Register?
N/A
Have the following areas been considered whilst producing this report?
Yes
N/A
Equality Impact Assessment (if yes, attach to paper)
*
Quality Impact Assessment (if yes, attach to paper)
*
Regulation, legal, governance and assurance implications (reference in the report if applicable)
*
Procurement process (reference in the report if applicable)
*
Document development
Has this document been presented to any other Committee or Forum? If yes, please list which meeting, date and outcome of presentation
The document has been discussed and agreed by the CCG Health Forum – a Sub Committee of the Quality Committee
AGENDA ITEM NO: G
Patient Representation Feedback Warrington CCG Governing Body Meeting 13
th September 2017
Strategic Objectives and Risks 2016/17
A1 Failure to understand the NHS Constitution in the local context
A2 Failure to impact on indirectly commissioned services with regard to the NHS Constitution
B1 Failure to establish quality monitoring
B2 Failure to identify and act upon early warnings of a failing by any commissioned provider
B3 Failure to performance manage to ensure continuous improvement
B4 Failure to impact on quality standards applied to indirectly commissioned services
B5 Failure to agree and measure outcomes
C1 Failure to develop a financial strategy
C2 Failure to implement the financial strategy
C3 Failure to ensure sound business practices are at the heart of running the CCG
C4 Failure to secure best value
D1 Failure to demonstrate improvement
E1 Failure to identify appropriate segmentation for the local population
F1 Failure to define the needs of the workforce
F2 Failure to promote the organisational culture that meets the needs of the workforce
F3 Failure to implement a system which monitors success
F4 Failure of delivery by outsourced critical business functions
G1 Failure to ensure that we are compliant with our statutory responsibilities
G2 Failure to demonstrate patient and public engagement
G3 Failure to demonstrate innovation or support research
AGENDA ITEM NO: G
Patient Representation Feedback Warrington CCG Governing Body Meeting 13
th September 2017
Feedback from CCG Health Forum Meetings
The meeting received and discussed the agenda items listed above. Health Forum members considered the contents of the papers / presentations and requested that the following points to be raised at Governing Body or with members of the CCG Support Team
Outline of Issue/Concern or Highlight
Main Presentation Changes to Stroke Services The Forum discussed the changes to Stroke services with staff from Warrington and Halton Hospitals and Whiston Hospital. The feedback will be included in the final engagement report. Stroke services has also been discussed as part of the Health Forum outreach with Warrington Speak Up (adults with learning disabilities) The main discussions were:
Support for the changes if patients are seen by the most appropriate, skilled Consultant
Concern regarding if a patient presented at A&E themselves and the time to identify stroke symptoms
Capacity concerns short and long term
To ensure that Whiston staff are aware of Lets Check for people with learning disabilities (a file containing the most relevant and up to date information)
Meeting Date: 31.07.17 7pm – 9pm
Key Agenda Items
Changes to Stroke Services
Representation/ Attendance
Governing Body Patient Representative Public Governor Bridgewater Bridgewater Causeway PPG WIRED Carers Representative Public Health Collaboration Lakeside PPG Public Governor NWAS Fearnhead PPG Holes Lane PPG Eric Moore PPG Stockton Health PPG Healthwatch Warrington Homestart Warrington Contact the Elderly St Roccos Papyrus

AGENDA ITEM NO: G
Patient Representation Feedback Warrington CCG Governing Body Meeting 13
th September 2017
Other Topics
The Forum wanted assurance that the CCG were involved in the Council’s Local Development Plan (plan for increased housing and employment land over the next 20 years.)
Bridgewater held their Big Conversation to hear what their patients thought about their services – this will be ongoing as part of a patient experience programme.
Meeting Date: 21.08.17
Key Agenda Items
Patient Representation Training
Representation/ Attendance
Governing Body Patient Representative Causeway PPG Fearnhead PPG Holes Lane PPG Eric Moore PPG Culcheth PPG Greenbank PPG CRI Pathways Vulnerable Communities Development Officer Healthwatch Warrington Deputy Chief Nurse for Quality Engagement Manager Business Administrator Communications Officer
Outline of training
The training focused on enabling interested patients to effectively become patient representatives within the CCG. A patient charter was drawn up and agreed on the day. The CCG is now being encouraged to identify opportunities for patient’s representatives to be included in meetings and committees. The Patient Charter is below: Patients Representatives will:
Take responsibility for their actions
Be accessible and communicate with each other and the CCG
Bring no personal agenda to the meetings
Commit to the role and be honest with their commitment
Be there to listen as well as to be heard The CCG will:
Continuously update the patient representatives on national, regional and local work and news
Ensure the Patient Representation Policy is flexible and adaptable to ensure the best outcomes for the CCG and the patient representatives.

AGENDA ITEM NO: H
Clinical Chief Officer Report Warrington CCG Governing Body Meeting 13
th September 2017
GOVERNING BODY MEETING:
CCG Governing Body
DATE OF MEETING:
13
th September 2017
REPORT AUTHOR AND JOB TITLE:
Dr Andrew Davies, Clinical Chief Officer
REPORT TITLE:
Clinical Chief Officer Report
STRATEGIC OBJECTIVES:
Please tick which strategic objectives the paper relates to
Improve quality of services
Sustained financial balance
Build an effective and motivated whole system workforce
Sound governance arrangements
Ensure integration and joint working arrangements
OUTCOME REQUIRED (tick)
Approval
Assurance
Discussion
Information
EXECUTIVE SUMMARY
To provide Warrington CCG Governing Body with
an update the on some of the key issues that have not been covered elsewhere in an individual report;
information of the activities undertaken by the Clinical Chief Officer and senior team since the last report; and
if appropriate, seek the approval of the Governing Body for actions to be taken
RECOMMENDATIONS
The Governing Body is asked to note the report.

AGENDA ITEM NO: H
Clinical Chief Officer Report Warrington CCG Governing Body Meeting 13
th September 2017
Outline any engagement – staff, clinical, stakeholder and patient / public
Not applicable
Are there any conflicts of interest which may be associated with this paper?
None
Does this paper address any existing risks which are included on the Assurance Framework or Risk Register?
N/A
Have the following areas been considered whilst producing this report?
Yes
N/A
Equality Impact Assessment (if yes, attach to paper)
Quality Impact Assessment (if yes, attach to paper)
Regulation, legal, governance and assurance implications (reference in the report if applicable)
Procurement process (reference in the report if applicable)
Document development
Has this document been presented to any other Committee or Forum? If yes, please list which meeting, date and outcome of presentation

AGENDA ITEM NO: H
Clinical Chief Officer Report Warrington CCG Governing Body Meeting 13
th September 2017
WARRINGTON CLINICAL COMMISSIONING GROUP CLINICAL CHIEF OFFICER REPORT
Purpose 1. The purpose of this report is to provide Members of the Governing Body with:
information on key issues that have not been covered elsewhere in an individual report;
information on the activities undertaken by the Clinical Chief Officer and senior team since the last report; and
if appropriate, ratify agreements made and seek the approval of the Governing Body for actions to be taken
Key national requirements for clinicians and managers across the NHS briefing document published
2. NHS England and partner healthcare organisations have produced a briefing
document that describes key national requirements aimed at improving the interface between GPs and secondary care providers. Clinicians and managers need to be aware of these requirements set out in the new NHS Standard Contract for 2017-19, which came into effect on 1 April 2017 and which will remain in place until 31 March 2019. NHS England and NHS Improvement have written to CCGs and NHS trusts urging them to take these requirements forward as a priority at a local level.
2016/17 CCG annual assessments and clinical priority area assessments 3. Following discussions at previous Governing Body and Audit Committee
meetings the CCG wrote to Paul Baumann, Chief Finance Officer of NHS England, on 31st March regarding the decision to assess the CCGs 16/17 financial performance against the outturn position before the release of the risk reserve.
4. NHS England wrote to the CCG on 13th July with the outcome of the CCG annual assessment for 2016/17. This provides each CCG with a headline assessment against the indicators in the CCG improvement and assessment framework (CCG IAF). The CCG IAF aligns key objectives and priorities as part of our aim to deliver the Five Year Forward View. The headline assessment has been confirmed by NHS England’s Commissioning Committee.
5. The final draft headline rating for 2016/17 for Warrington CCG is Requires Improvement.
6. Additional assessments have also been undertaken by three independent clinical panels for each of the priority areas set out in The Next Steps on the Five Year Forward View: cancer, mental health and dementia. The headline assessment for each of these areas is as follows;
AGENDA ITEM NO: H
Clinical Chief Officer Report Warrington CCG Governing Body Meeting 13
th September 2017
NHS WARRINGTON CCG
Clinical priority area Headline rating 2016/17
Cancer Requires improvement
Mental Health Good
Dementia Good
7. The CCG is particularly disappointed with the CCG IAF headline assessment made by NHS England and feel that it does not really reflect our overall performance and achievements during 2016/2017. A formal response has been sent to NHS England on this matter.
8. Specifically, as we raised concern earlier in the year regarding the change in year to the treatment of the additional 1% non-recurrent reserve and raised further concern that all CCG financial positions were to be assessed prior to the closing of the year-end financial accounts. The impact of this has resulted in the CCG moving from an assessment position which should have been ‘Good’ to ‘Requires Improvement’.
9. The CCG has written to local providers, MPs and Warrington Borough Council to explain the position. At the time of writing the CCG has received formal responses and support from North West Boroughs Healthcare and Bridgewater Healthcare.
10. The detail of the CCGs response to the 2016/17 assessment was reviewed and discussed at the Audit Committee on 23rd August with agreement that all possible actions had now been exhausted in relation to this matter.
Clinical streaming in accident and emergency departments 11. Good quality initial assessment at the front door of accident and emergency
(A&E) departments is integral to the delivery of high quality patient care. In order to support local planning and decision making around front door streaming, a set of principles for streaming have been developed. These principles and the Royal College of Emergency Medicine guidelines refer to clinical streaming at the front door of A&E, including to primary care services, as being an integrated function.
Immigration health surcharge; removal of assisted conception services
12. Amendments to the NHS (Charges to Overseas Visitors) Regulations 2015 were introduced into Parliament on 19 July 2017. As a result, from 21 August 2017, assisted conception services will no longer be included in the scope of services available for free for those who pay the immigration health surcharge. The CCG, as required by NHS England, has its website, to ensure potential users of these services are aware of the changes. Further information can be found in the Explanatory Memorandum for these regulations.
New Implementation guide and resource pack for dementia care published 13. A new Implementation guide and resource pack for dementia care has been
published on NHS England’s website. The guide sets out what good quality assessment, diagnosis and care looks like in relation to NICE and other formal guidance, as well as the views and expectations of people living with

AGENDA ITEM NO: H
Clinical Chief Officer Report Warrington CCG Governing Body Meeting 13
th September 2017
dementia and their carers. This is set within the framework set by the NHS Mandate and two clear requirements for improvement reinforced by NHS Operational Planning and Contracting Guidance 2017-19; to increase the number of people starting treatment within six weeks from referral; and to improve the quality of post-diagnostic treatment and support for people with dementia and their carers.
Falls and fracture prevention commissioning resource pack 14. Public Health England, NHS England and the National Falls Prevention
Coordination Group member organisations have published a resource pack to support falls and fracture prevention commissioning. The pack contains information on key interventions including cost and clinical effectiveness. It provides links to an extensive range of documents and tools including commissioning support, clinical guidance and quality standards, frailty, and research and policy documents. The pack also includes suites of indicators that can be chosen for local collection and a practical commissioner’s checklist.
Integrated Support and Assurance publication 15. The updated Integrated Support and Assurance Process (ISAP) guidance
has been published. ISAP is NHS England and NHS Improvement process for supporting commissioners and providers looking to procure and bid for complex contracts. It replaces the introductory document published in November 2016. All commissioners and providers looking to procure and bid for complex contracts should review this guidance and commissioners should engage with their regional NHS England teams as early as possible to establish whether the procurement or other arrangement would benefit from going through the ISAP.
Health Funding for CCGs as part of the Vulnerable Person Resettlement Programme 16. The Vulnerable Person Resettlement Programme reimburses health
commissioners for medical care for vulnerable persons resettled under the Programme for the first year after they arrive in the UK. The following funding is available for CCGs to claim; £2,600 per person to cover initial primary and some secondary care costs. The CCG simply needs to provide confirmation the individual has registered with a GP and any additional funding for any further secondary care needs identified in the first 12 months after arrival. These are considered on a case-by-case basis. For more detail, see the 2017/18 Health Funding Instructions for England.
Vacant Space Handback Scheme launched 17. From August 2017, a new scheme has launched to allow commissioners to
pass back vacant space to NHS Property Services (NHSPS). The Vacant Space Handback Scheme has been developed following extensive consultation with NHSPS customers, the Department of Health and NHS England. The scheme is available for applications from commissioners (CCGs, CSUs and NHS England), who can choose to pass on liability for eligible space creating savings and increasing estate efficiency. For further
AGENDA ITEM NO: H
Clinical Chief Officer Report Warrington CCG Governing Body Meeting 13
th September 2017
information please visit NHS Property Services’ website.
The Culture of Care Barometer is now available online
18. The Culture of Care Barometer (CCB) is now available online. The CCB is designed to help teams and organisations gauge the culture of care in an organisation. It is a quick and easy to complete questionnaire that creates the opportunity for staff to engage in discussions about the culture of the organisation, area or team. By encouraging reflection and stimulating conversation, the CCB helps to break down barriers and to highlight troubled areas. Visit NHS England’s website to find out more and use the tool.
Model service specification for wheelchair and posture services published
19. Recent data shows 25% of children wait more than 18 weeks for their wheelchair. Through CCGs’ improvement work (following the NHS Planning Guidance target of all children receiving their wheelchair within 18 weeks by quarter four 2018/19), it is hoped this figure will reduce. In collaboration with stakeholders, NHS England has developed a model service specification, describing its ambition for excellent wheelchair services. CCGs are encouraged to use this as a tool for reviewing and improving their services to support individuals, their families and carers to achieve greater independence and quality of life, through timely provision of the right wheelchair.
Better Care Fund planning requirements
20. The Better Care Fund (BCF) planning requirements and allocations are now available on the NHS England website. This underpins the 2017-2019 Integration and Better Care Fund Policy Framework published by the Department of Health and the Department of Communities and Local Government. NHS England’s Better Care team have acknowledged the problems caused by the delay in publication of the planning requirements and have made changes to the assurance process and timeline to mitigate further delays in BCF plans being signed off.
GP Resilience Programme guidance 2017/18 published
21. NHS England has published updated guidance on the 2017/18 allocations under the GP Resilience Programme, which will see a further £8 million go to GP practices to support them in becoming more sustainable and resilient, better placed to tackle the challenges they face now and in the future. Last year 2,100 GP practices received support for resilience work as part of the Vulnerable Practices Programme (VPP) (£10 million) and the GP Resilience Programme (GPRP) (£16 million).
NHS RightCare Pathway for Diabetes published
22. NHS RightCare, in partnership with Healthier You, has produced a clinically led pathway for diabetes. The pathway highlights the high-level overarching national case for change, best practice pathway for diabetes; and best practice case studies for elements of the pathway demonstrating what to change, how to change and the scale of improvement. This uses the evidence-base, clinical interventions, information on the risk conditions, and
AGENDA ITEM NO: H
Clinical Chief Officer Report Warrington CCG Governing Body Meeting 13
th September 2017
potential opportunities for improvement for use by local health economies when commissioning services. Local health economies may find it useful during the ‘What to Change’ phase of their RightCare work.
MEETINGS Meetings attended by the Clinical Chief Officer on behalf of the CCG 23. Since the last report in July, Dr Andrew Davies as Clinical Chief Officer for the
Clinical Commissioning Group has attended the following meetings:
20.7.17 Cheshire & Merseyside Accident & Emergency Event
26.7.17 Cheshire & Merseyside Urgent & Emergency Care Network STP Working Group
27.7.17 Commissioning Protected Learning Time Event
2.8.17 STP Working Group Meeting
9.8.17 Knowledge Brief Innovation Day – Become a Smarter Organisation
16.8.17 Meeting with Professor Steven Broomhead, Warrington Borough Council
16.8.17 STP Working Group Meeting
17.8.17 Cheshire & Merseyside Urgent and Emergency Care Network Programme Meeting
18.8.17 Accountable Officers Meeting
23.8.17 CCG Plan Refresh Meeting between Warrington CCG & Warrington Borough Council
29.8.17 Meeting with Councillor Patricia Wright
29.8.17 Meeting with Mel Pickup and Andrew Chadwick, Warrington & Halton Hospitals
30.8.17 Meeting with Sue Musson, Independent Chair of the Shadow ACO Board
1.9.17 TCP Strategic Board
5.9.17 Urgent & Emergency Care Network Meeting
6.9.17 Meeting with Alan Moore, Coroner for Cheshire
7.9.17 A&E Delivery Board – System Leadership Event
RECOMMENDATIONS 24. Members of the Governing Body are asked to:
a) Note the contents of this report
Dr Andrew Davies Clinical Chief Officer September 2017
AGENDA ITEM NO: 045/17
Assurance Framework Warrington CCG Governing Body Meeting 13
th September 2017
GOVERNING BODY MEETING:
Governing Body Meeting
DATE OF MEETING:
13
th September 2017
REPORT AUTHOR AND JOB TITLE:
Rebecca Knight Head of Assurance & Risk
REPORT TITLE:
Assurance Framework
STRATEGIC OBJECTIVES:
Please tick which strategic objectives the paper relates to
NHS Constitution
Improve quality of services
Sustained financial balance
Improve healthy life expectancy
Reduce inequalities
Build an effective and motivated workforce
Sound governance arrangements
OUTCOME REQUIRED (tick)
Approval
Assurance
Discussion
Information
EXECUTIVE SUMMARY
Assurance Framework was scrutinised by the Audit Committee on 23 August 2017
All actions are showing as complete against each risk for Quarter 1, with the exception for D1
An update on all completed actions is included for those completed in Quarter 1
There has been a small change to the risk description for A2
RECOMMENDATIONS
The Governing Body is asked to:
a. Receive assurance that there is a robust process in place to scrutinise the
management of all strategic risks.

AGENDA ITEM NO: 045/17
Assurance Framework Warrington CCG Governing Body Meeting 13
th September 2017
Outline any engagement – staff, clinical, stakeholder and patient / public
Not applicable
Are there any conflicts of interest which may be associated with this paper?
None known
Does this paper address any existing risks which are included on the Assurance Framework or Risk Register?
Not applicable
Have the following areas been considered whilst producing this report?
Yes
N/A
Equality Impact Assessment (if yes, attach to paper)
Quality Impact Assessment (if yes, attach to paper)
Regulation, legal, governance and assurance implications (reference in the report if applicable)
Procurement process (reference in the report if applicable)
Document development
Has this document been presented to any other Committee or Forum? If yes, please list which meeting, date and outcome of presentation
The Assurance Framework was presented to the Audit Committee on 23 August 2017
AGENDA ITEM NO: 045/17
Assurance Framework Warrington CCG Governing Body Meeting 13
th September 2017
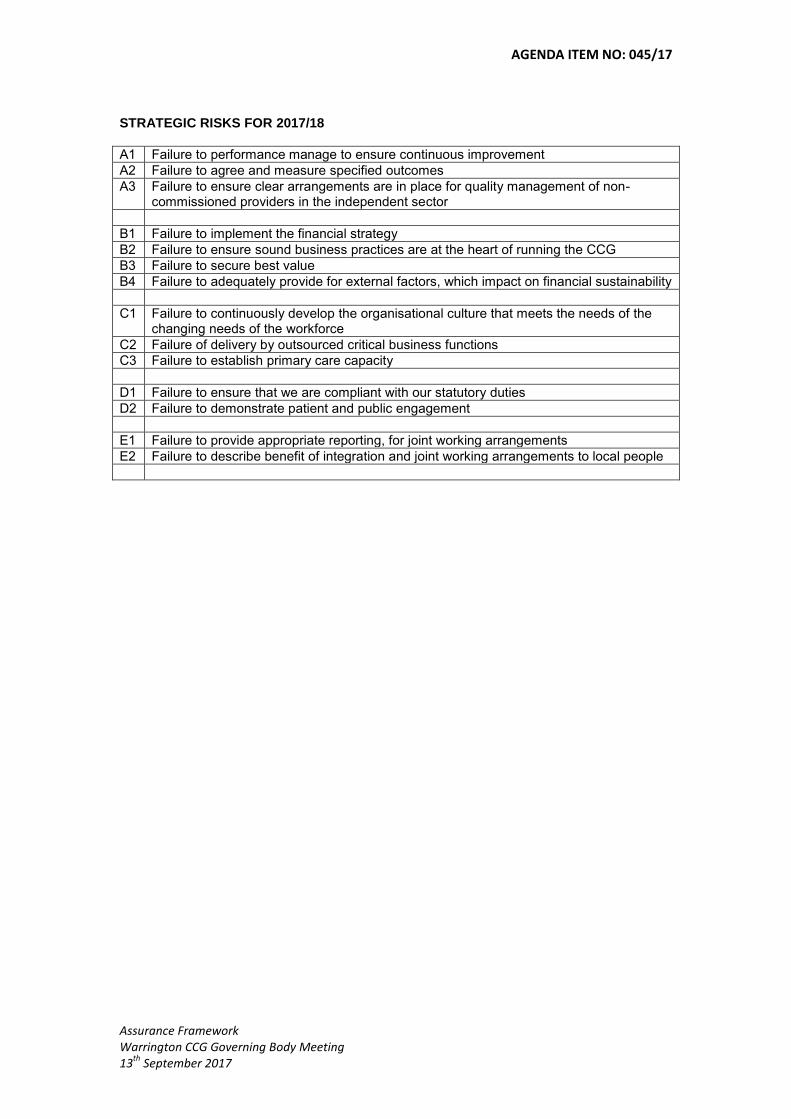
STRATEGIC RISKS FOR 2017/18
A1 Failure to performance manage to ensure continuous improvement
A2 Failure to agree and measure specified outcomes
A3 Failure to ensure clear arrangements are in place for quality management of non-commissioned providers in the independent sector
B1 Failure to implement the financial strategy
B2 Failure to ensure sound business practices are at the heart of running the CCG
B3 Failure to secure best value
B4 Failure to adequately provide for external factors, which impact on financial sustainability
C1 Failure to continuously develop the organisational culture that meets the needs of the changing needs of the workforce
C2 Failure of delivery by outsourced critical business functions
C3 Failure to establish primary care capacity
D1 Failure to ensure that we are compliant with our statutory duties
D2 Failure to demonstrate patient and public engagement
E1 Failure to provide appropriate reporting, for joint working arrangements
E2 Failure to describe benefit of integration and joint working arrangements to local people
AGENDA ITEM NO: 045/17
Assurance Framework Warrington CCG Governing Body Meeting 13
th September 2017
ASSURANCE FRAMEWORK
BACKGROUND
1. All NHS organisations are required to develop and maintain an Assurance Framework in accordance with the government regulations applied to the NHS. The Assurance Framework allows the Governing Body to consider the risks that may hamper the CCG from delivering its statutory duties and functions.
PURPOSE
2. The purpose of this report is to provide an overview of the proposed strategic risks, which may threaten the achievement of Warrington CCG’s strategic objectives. These will be used to populate the Assurance Framework.
KEY ITEMS TO NOTE 3. The Assurance Framework was presented to the Audit Committee on 23
August 2017, where discussion took place about the assurances provided with a particular focus on all of the risks related to finance (B1, B2, B3 and B4). Following the focus on financial risks, it was agreed that the risk rating for B4 should be reviewed.
4. The Assurance Framework has fourteen strategic risks identified in association with the achievement of its five strategic objectives.
5. Any areas shown in red in Appendix A, are those actions which have not been completed in quarter one or where changes have been made to scores or wording.
6. There is one risk showing slippage against actions due to be completed in
quarter one (D1). Further detail of this is shown below in the status update.
7. The following risk wording has been amended slightly:
Risk A2 – has had the word “specified” added to the description. This is now failure to agree and measure specified outcomes.
8. All risks have had their risk scoring reviewed for the uncontrolled, current
and target risk. Four risks have had their risk rating reduced (A2, B2, C1 and D2) in one of more of the ratings (uncontrolled, current or target) and one risk has had its target risk rating increased (D1).
9. The reduction in risk rating is due to the mitigation of the risks through the
existing control and assurances. The increase in target rating reflects the likelihood of failure which has changed from rare to unlikely.

AGENDA ITEM NO: 045/17
Assurance Framework Warrington CCG Governing Body Meeting 13
th September 2017
10. The key for management resource has now been included. Currently, all risks which have internal audits due as part of the assurance are showing as having focused management effort.
STATUS UPDATES FOR QUARTER ONE
11. The following actions have been completed for risks D1, D2 and E1: Chief Operating Officer
D1 – Internal audits for complaints and Freedom of Information have been completed and the outcomes have been submitted to the August Audit Committee. However, the internal audit for statutory duties which was due to be completed in quarter one is in draft form and not yet complete. This should now be completed in quarter 2;
E1 – a paper was presented to the Governing Body in May 2017 with regards to the Mid Mersey Alliance Joint Commissioning Committee.
Strategic Head of Communication and Engagement
D2 – The CCG Annual Report and Accounts 2016/17, Engagement Annual Report 2016/17 and Equality and Diversity Annual Report 2016/17 were all completed in quarter one.
RECOMMENDATIONS 12. The Governing Body is asked to:
a. Receive assurance that there is a robust process in place to scrutinise
the management of all strategic risks.
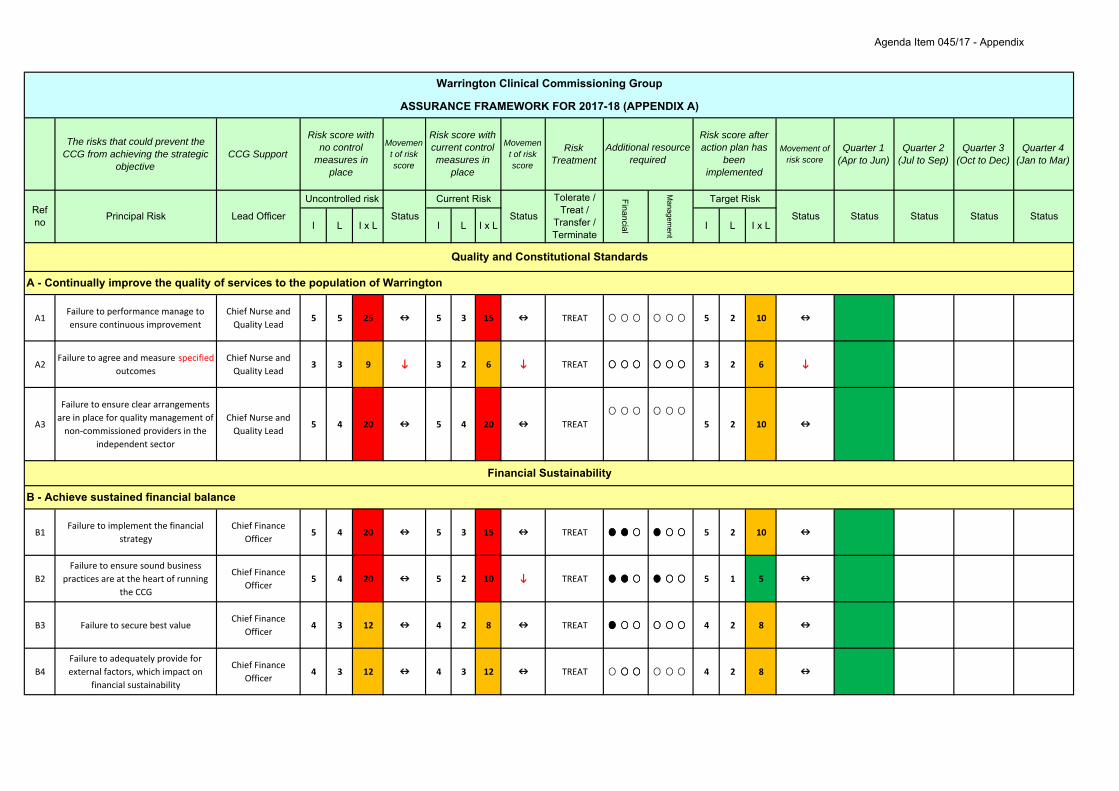
The risks that could prevent the CCG from achieving the strategic
objectiveCCG Support
Movement of risk score
Movement of risk score
Risk Treatment
Movement of risk score
Quarter 1 (Apr to Jun)
Quarter 2 (Jul to Sep)
Quarter 3 (Oct to Dec)
Quarter 4 (Jan to Mar)
I L I x L I L I x L I L I x L
A1Failure to performance manage to ensure continuous improvement
Chief Nurse and Quality Lead
5 5 25 5 3 15 TREAT 5 2 10
A2Failure to agree and measure specified
outcomesChief Nurse and Quality Lead
3 3 9 3 2 6 TREAT 3 2 6
A3
Failure to ensure clear arrangements are in place for quality management of non‐commissioned providers in the
independent sector
Chief Nurse and Quality Lead
5 4 20 5 4 20 TREAT 5 2 10
B1Failure to implement the financial
strategyChief Finance
Officer5 4 20 5 3 15 TREAT 5 2 10
B2Failure to ensure sound business
practices are at the heart of running the CCG
Chief Finance Officer
5 4 20 5 2 10 TREAT 5 1 5
B3 Failure to secure best valueChief Finance
Officer4 3 12 4 2 8 TREAT 4 2 8
B4Failure to adequately provide for external factors, which impact on
financial sustainability
Chief Finance Officer
4 3 12 4 3 12 TREAT 4 2 8
A - Continually improve the quality of services to the population of Warrington
Financial Sustainability
B - Achieve sustained financial balance
Quality and Constitutional Standards
Status
Tolerate / Treat /
Transfer / Terminate
Financial
Managem
ent
Target Risk
StatusRef no Principal Risk Lead Officer
Uncontrolled risk
Status
Current Risk
Status Status Status Status
Warrington Clinical Commissioning Group
ASSURANCE FRAMEWORK FOR 2017-18 (APPENDIX A)
Risk score with no control
measures in place
Risk score with current control measures in
place
Additional resource required
Risk score after action plan has
been implemented
Agenda Item 045/17 - Appendix

C1Failure to continuously develop the
organisational culture, that meets the changing needs of the workforce
Chief Operating Officer
4 4 16 4 2 8 TREAT 4 2 8
C2Failure of delivery, by outsourced
critical business functionsChief Operating
Officer4 4 16 4 2 8 TREAT 4 2 8
C3Failure to establish primary care
capacityChief of Healthcare Commissioning
3 4 12 3 3 9 TREAT 3 2 6
D1Failure to ensure that we are
compliant with our statutory dutiesChief Operating
Officer5 5 25 5 2 10 TREAT 5 2 10
D2Failure to demonstrate patient and
public engagement
Strategic Head of Communication &
Engagement4 4 16 4 2 8 TREAT 4 2 8
E1Failure to provide appropriate reporting, for joint working
arrangements
Chief Operating Officer
5 5 25 5 4 20 TREAT 5 2 10
E2Failure to describe benefit to local
people
Strategic Head of Communication &
Engagement4 5 20 4 3 12 TREAT 4 2 8
Key for quarterly status Key for financial status Key for management status
Not started Upto £10k required Focused management effort
Started but not complete Between £10k‐£90k required Workplan lead in place
Complete More than £90k required Requires additional management support
C - Build an effective and motivated whole system workforce
D - Ensure sound governance arrangements are in place
E - Ensure integration and joint working arrangements for the benefit of local people
Assurance Process
Agenda Item 045/17 - Appendix
AGENDA ITEM NO: 046/17
Update Report on Emergency Preparedness, Resilience and Response (EPRR) Warrington CCG Governing Body Meeting 13
th September 2017
GOVERNING BODY MEETING:
Governing Body Meeting
DATE OF MEETING:
13
th September 2017
REPORT AUTHOR AND JOB TITLE:
Rebecca Knight Head of Assurance & Risk
REPORT TITLE:
Update Report on Emergency Preparedness, Resilience and Response (EPRR)
STRATEGIC OBJECTIVES:
Please tick which strategic objectives the paper relates to
NHS Constitution
Improve quality of services
Sustained financial balance
Improve healthy life expectancy
Reduce inequalities
Build an effective and motivated workforce
Sound governance arrangements
OUTCOME REQUIRED (tick)
Approval
Assurance
Discussion
Information
EXECUTIVE SUMMARY
Annual Report for 2016-17 included for assurance and information
Substantial compliance with NHS England Core Standards with a focus of the development of an Health and Social Care Pandemic Influenza Plan
Deep dive for governance is also included, but is not included as part of the overall assurance statement
RECOMMENDATIONS
The Governing Body is asked to:
a. Approve the proposal that NHS Warrington CCG is substantially compliant
with EPRR core standards and is also therefore compliant with the Civil Contingencies Act 2004.
AGENDA ITEM NO: 046/17
Update Report on Emergency Preparedness, Resilience and Response (EPRR) Warrington CCG Governing Body Meeting 13
th September 2017
Outline any engagement – staff, clinical, stakeholder and patient / public
Not applicable
Are there any conflicts of interest which may be associated with this paper?
None known
Does this paper address any existing risks which are included on the Assurance Framework or Risk Register?
Not applicable
Have the following areas been considered whilst producing this report?
Yes
N/A
Equality Impact Assessment (if yes, attach to paper)
Quality Impact Assessment (if yes, attach to paper)
Regulation, legal, governance and assurance implications (reference in the report if applicable)
Procurement process (reference in the report if applicable)
Document development
Has this document been presented to any other Committee or Forum? If yes, please list which meeting, date and outcome of presentation
AGENDA ITEM NO: 046/17
Update Report on Emergency Preparedness, Resilience and Response (EPRR) Warrington CCG Governing Body Meeting 13
th September 2017
STRATEGIC RISKS FOR 2017/18
A1 Failure to performance manage to ensure continuous improvement
A2 Failure to agree and measure specified outcomes
A3 Failure to ensure clear arrangements are in place for quality management of non-commissioned providers in the independent sector
B1 Failure to implement the financial strategy
B2 Failure to ensure sound business practices are at the heart of running the CCG
B3 Failure to secure best value
B4 Failure to adequately provide for external factors, which impact on financial sustainability
C1 Failure to continuously develop the organisational culture that meets the needs of the changing needs of the workforce
C2 Failure of delivery by outsourced critical business functions
C3 Failure to establish primary care capacity
D1 Failure to ensure that we are compliant with our statutory duties
D2 Failure to demonstrate patient and public engagement
E1 Failure to provide appropriate reporting, for joint working arrangements
E2 Failure to describe benefit of integration and joint working arrangements to local people
Agenda Item No: 046/17
EMERGENCY PREPAREDNESS, RESILIENCE AND RESPONSE (EPRR) ASSURANCE REPORT 2017-18
Background 1. NHS Warrington CCG is classed as a Category 2 responder under the
Civil Contingencies Act 2004. Category 2 responders are considered to be “co-operating bodies” which are less likely to be involved in core planning work for emergency preparedness but may be heavily involved in the response to an emergency that affect their sector. Category 2 responders have a lesser set of duties – co-operating and sharing relevant information with other Category 1 and 2 responders.
2. NHS England Core Standards for EPRR are the minimum standards which
NHS organisations and providers of NHS funded care must meet. Assurance 3. In July 2017, NHS England issued a directive about the EPRR assurance
process for 2017-18. This letter can be found below: https://www.england.nhs.uk/wp-content/uploads/2014/05/Guidance-for-2017-18-EPRR-assurance-process.pdf
4. This report provides an update against the requirements laid out in the NHS England letter.
Assurance Outcome 5. NHS Warrington CCG is considered to be substantially compliant with the
EPRR core standards (see Appendix A for further detail). The resulting action plan relates to the ongoing development of an Health and Social Care Pandemic Influenza Plan.
Annual Report 6. The Annual Report for 2016-17 is also attached for information. This
provides some further detail about how the CCG complies with the Civil Contingencies Act 2004 and the EPRR Core Standards.
Recommendations 7. NHS Warrington CCG Governing Body is asked to:
a. Approve the proposal that NHS Warrington CCG is substantially
compliant with EPRR core standards and is also therefore compliant with the Civil Contingencies Act 2004.
Agenda Item No: 046/17
EMERGENCY PREPAREDNESS, RESILIENCE AND RESPONSE (EPRR) ANNUAL REPORT 2016/17
Purpose 1. The purpose of this report is to provide an overview of NHS Warrington
CCG role and responsibilities and its compliance with those, as stated in the Civil Contingencies Act (CCA) 2004 and the supporting guidance.
Background 2. NHS Warrington CCG is classed as a Category 2 responder under the
Civil Contingencies Act 2004. Category 2 responders are critical players in EPRR who are expected to work closely with partners. They are required to co-operate with and support other Category 1 and Category 2 responders. They are less likely to be involved in the heart of planning work, but will be heavily involved in incidents that affect their own sector Category 2 responders have a lesser set of duties – co-operating and sharing relevant information with other Category 1 and 2 responders. CCGs are also expected to provide support to NHS England in relation to the co-ordination of their health economy.
3. NHS England Core Standards for EPRR are the minimum standards which
NHS organisations and providers of NHS funded care must meet. Further guidance can be found relating to NHS England Core Standards for EPRR at:
4. http://www.england.nhs.uk/wp-content/uploads/2015/06/nhse-core-
standards-150506.pdf Roles and Responsibilities 5. The EPRR role and responsibilities of CCGs are to:
Ensure contracts with all commissioned provider organisations contain relevant EPRR elements, including business continuity;
Monitor compliance by each commissioned provider organisation with their contractual obligations in respect of EPRR and with applicable Core Standards;
Ensure robust escalation procedures are in place so that if a commissioned provider has an incident, the provider can inform the CCG 24/7;
Ensure effective processes are in place for the CCG to properly prepare for and rehearse incident response arrangements with local partners and providers;
Be represented at the Local Health Resilience Partnership (LHRP), either on their own or through a nominated lead CCG representative;
Agenda Item No: 046/17
Provide a route of escalation for the LHRP, in respect of commissioned provider EPRR preparedness;
Support NHS England in discharging its EPRR functions and duties locally, including supporting health economy tactical co-ordination during incidents; and
Fulfil the duties of a Category 2 responder under the CCA 2004 and the requirements in respect of emergencies within the NHS Act 2006.
Accountability 6. The Clinical Chief Officer is the Accountable Officer for emergency
preparedness in NHS Warrington CCG. The Head of Assurance & Risk has delegated responsibilities for ensuring that emergency preparedness requirements are met within the organisation.
Commissioning Support Unit (CSU) 7. NHS Warrington CCG has a Service Level Agreement in place with the
CSU (NWCSU) to provide support to the CCG for its emergency preparedness arrangements, specifically in relation to business continuity planning. These arrangements are delivered by Midlands and Lancashire CSU (MLCSU).
Local Health Resilience Partnership (LHRP) 8. The LHRP provides a strategic quarterly forum for local organisations to:
a. Facilitate health sector emergency preparedness and resilience; b. Provide support to NHS England, Public Health England and public
health colleagues to represent health sector emergency preparedness and resilience matters;
c. Provide support to NHS England, Public Health England and public health colleagues in assessing and assuring the ability of the health sector to respond to emergencies
9. The Head of Assurance & Risk represents Warrington CCG as a member
on the LHRP. In the event that the Head of Assurance & Risk cannot attend, the meeting has been attended by the Chief Operating Officer. 75% of the meetings were attended in 2016-17 which meets the requirements.
On-call arrangements 10. NHS Warrington CCG has an on-call rota in place which operates on a
24/7 basis. The rota is populated by managers at Band 8b and above. All managers have received familiarisation training and have appropriate documentation in place to support any required response.
11. One additional manager was added to the rota within the financial year
and received the necessary training.
Agenda Item No: 046/17
Training and exercises 12. The Head of Assurance & Risk attended a Cheshire & Merseyside
exercise in April 2016, to test the pandemic flu arrangements (known as Exercise Bluebird).
13. A post exercise report was produced following the exercise, which
identified some key learning across the region. These are being followed through by the Local Health Resilience Partnership and a Pandemic Flu Group for the area.
14. Issues which specifically impact on CCGs included the need to review and
update business continuity plans and the review of business continuity plans in care homes (see section on business continuity).
15. The requirement of all CCGs to provide support to NHS England in an
emergency led to the delivery of tactical training to all CCG on-call staff. This training was delivered by NHS England and was held at Police Headquarters in Winsford. All members of staff, with the exception of two managers, who operate on the on-call rota have attended the tactical training. The training incorporated the following:
a. Changes to NHS guidance; b. Roles of Providers; c. Role of CCGs; d. Role of NHS England; and e. Familiarisation of Police Headquarters.
Business Continuity arrangements 16. The main area of support commissioned from MLCSU is in relation to the
development of a Business Continuity Plan, including facilitation of the business impact analysis process, development of the plan, training of key staff and finally exercising of the final plan arrangements.
17. Key lead managers were identified to undertake business impact analysis
(BIA) in their areas of work. The completion of the BIA in each area was preceded by a business continuity session, facilitated by the MLCSU to raise awareness of what was required. All BIAs have been completed for all key areas and the updated Business Continuity Plan is being finalised to incorporate the updated information.
18. At the end of 2016/17, a review of all business continuity plans for those
homes with NHS funded patients has commenced. The local authority has the responsibility for reviewing business continuity plans for all care homes, where they hold the contract.
Agenda Item No: 046/17
Assurance 19. In 2016/7, all CCGs were required to ensure that its contracts with
commissioned providers contain relevant EPRR elements, including business continuity and that the compliance to these is monitored.
20. The NHS Standard Contract contains a section relating to EPRR which
outlines the requirements of providers.
21. All NHS providers and commissioners are required to provide assurance of compliance with core standards to NHS England. Warrington CCG was advised that the following organisations self-assessed themselves as follows:
a. Warrington and Halton Hospitals Foundation Trust (substantial
compliance); b. Bridgewater Community Healthcare Foundation Trust (substantial
compliance); and c. 5 Boroughs Partnership Foundation Trust (full compliance)
22. In addition, assurance must be provided to NHS England that the CCG is
compliant with core standards. A statement of compliance (substantial) was submitted to NHS England in September 2016, following submission and approval by the Governing Body.
23. In last year’s submission to NHS England, Warrington CCG declared that the Business Continuity Plan was undergoing review. All business impact analysis (BIA) templates have been completed and these are currently being reworked into the update of the Business Continuity Plan.
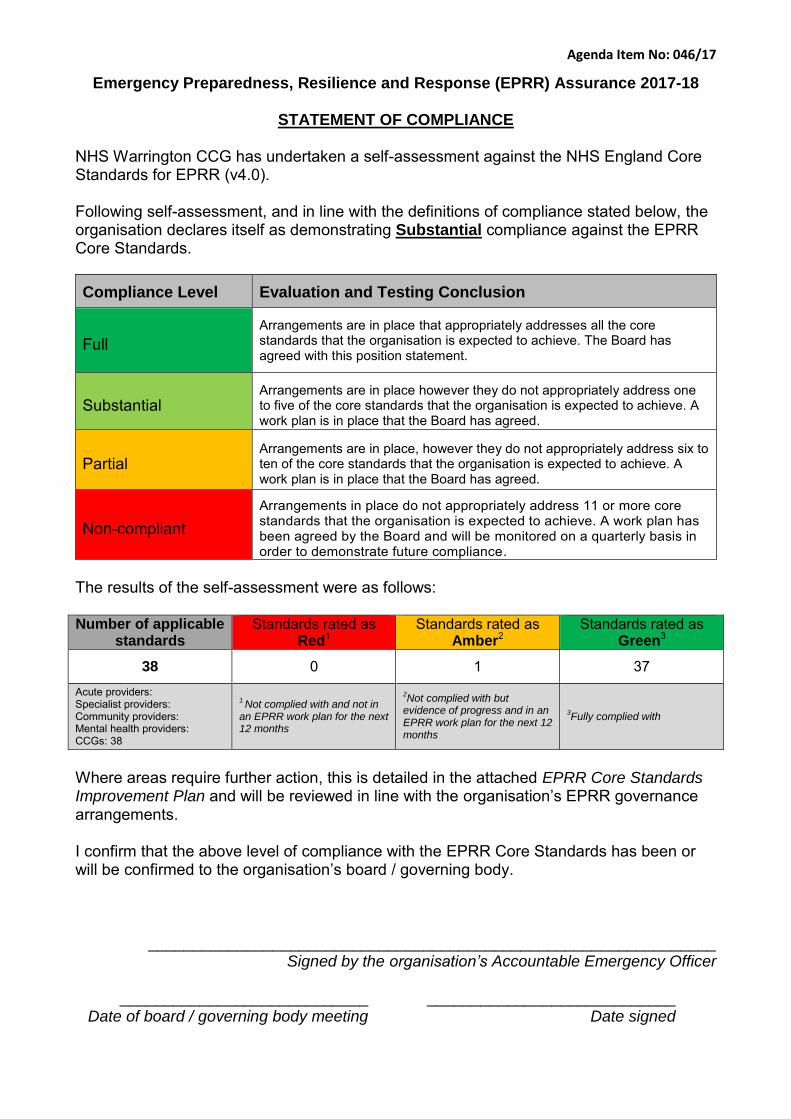
Agenda Item No: 046/17
Emergency Preparedness, Resilience and Response (EPRR) Assurance 2017-18
STATEMENT OF COMPLIANCE
NHS Warrington CCG has undertaken a self-assessment against the NHS England Core Standards for EPRR (v4.0). Following self-assessment, and in line with the definitions of compliance stated below, the organisation declares itself as demonstrating Substantial compliance against the EPRR Core Standards.
Compliance Level Evaluation and Testing Conclusion
Full
Arrangements are in place that appropriately addresses all the core standards that the organisation is expected to achieve. The Board has agreed with this position statement.
Substantial Arrangements are in place however they do not appropriately address one to five of the core standards that the organisation is expected to achieve. A work plan is in place that the Board has agreed.
Partial Arrangements are in place, however they do not appropriately address six to ten of the core standards that the organisation is expected to achieve. A work plan is in place that the Board has agreed.
Non-compliant
Arrangements in place do not appropriately address 11 or more core standards that the organisation is expected to achieve. A work plan has been agreed by the Board and will be monitored on a quarterly basis in order to demonstrate future compliance.
The results of the self-assessment were as follows: Number of applicable
standards Standards rated as
Red1 Standards rated as
Amber2 Standards rated as
Green3
38 0 1 37
Acute providers: Specialist providers: Community providers: Mental health providers: CCGs: 38
1 Not complied with and not in
an EPRR work plan for the next 12 months
2Not complied with but
evidence of progress and in an EPRR work plan for the next 12 months
3Fully complied with
Where areas require further action, this is detailed in the attached EPRR Core Standards Improvement Plan and will be reviewed in line with the organisation’s EPRR governance arrangements. I confirm that the above level of compliance with the EPRR Core Standards has been or will be confirmed to the organisation’s board / governing body.
________________________________________________________________ Signed by the organisation’s Accountable Emergency Officer
____________________________ ____________________________
Date of board / governing body meeting Date signed
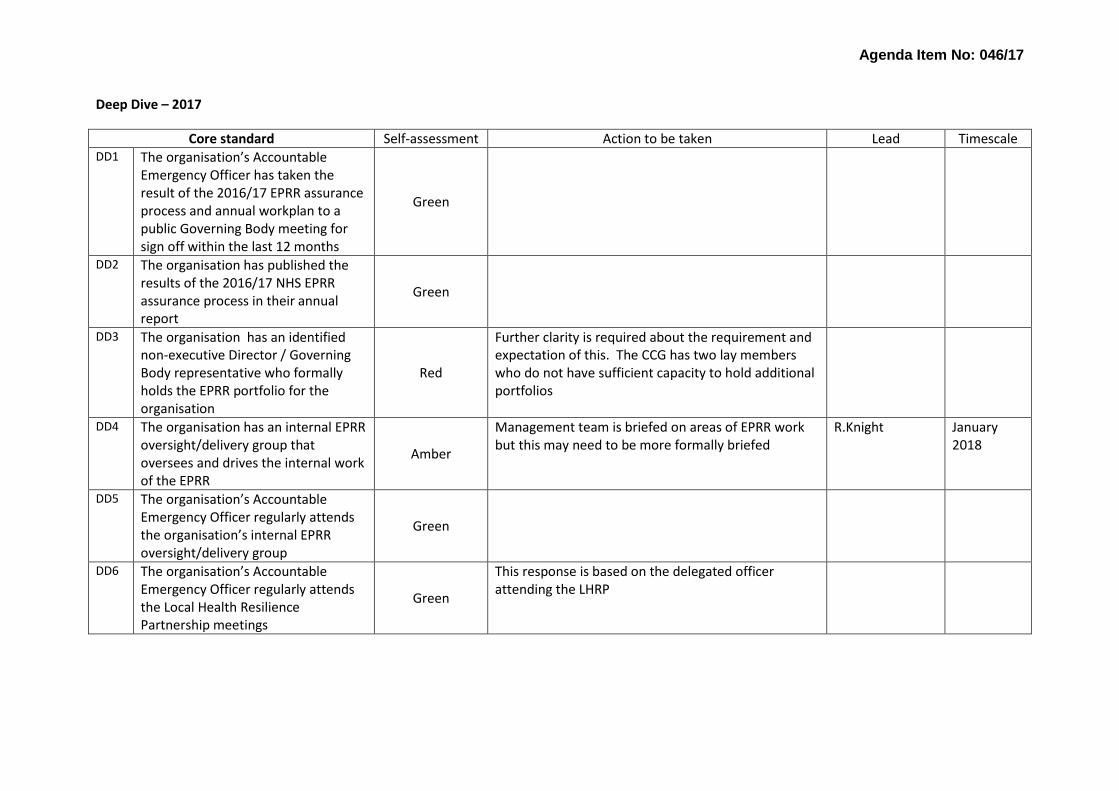
Agenda Item No: 046/17
Deep Dive – 2017
Core standard Self-assessment Action to be taken Lead Timescale DD1 The organisation’s Accountable
Emergency Officer has taken the result of the 2016/17 EPRR assurance process and annual workplan to a public Governing Body meeting for sign off within the last 12 months
Green
DD2 The organisation has published the results of the 2016/17 NHS EPRR assurance process in their annual report
Green
DD3 The organisation has an identified non-executive Director / Governing Body representative who formally holds the EPRR portfolio for the organisation
Red
Further clarity is required about the requirement and expectation of this. The CCG has two lay members who do not have sufficient capacity to hold additional portfolios
DD4 The organisation has an internal EPRR oversight/delivery group that oversees and drives the internal work of the EPRR
Amber
Management team is briefed on areas of EPRR work but this may need to be more formally briefed
R.Knight January 2018
DD5 The organisation’s Accountable Emergency Officer regularly attends the organisation’s internal EPRR oversight/delivery group
Green
DD6 The organisation’s Accountable Emergency Officer regularly attends the Local Health Resilience Partnership meetings
Green
This response is based on the delegated officer attending the LHRP
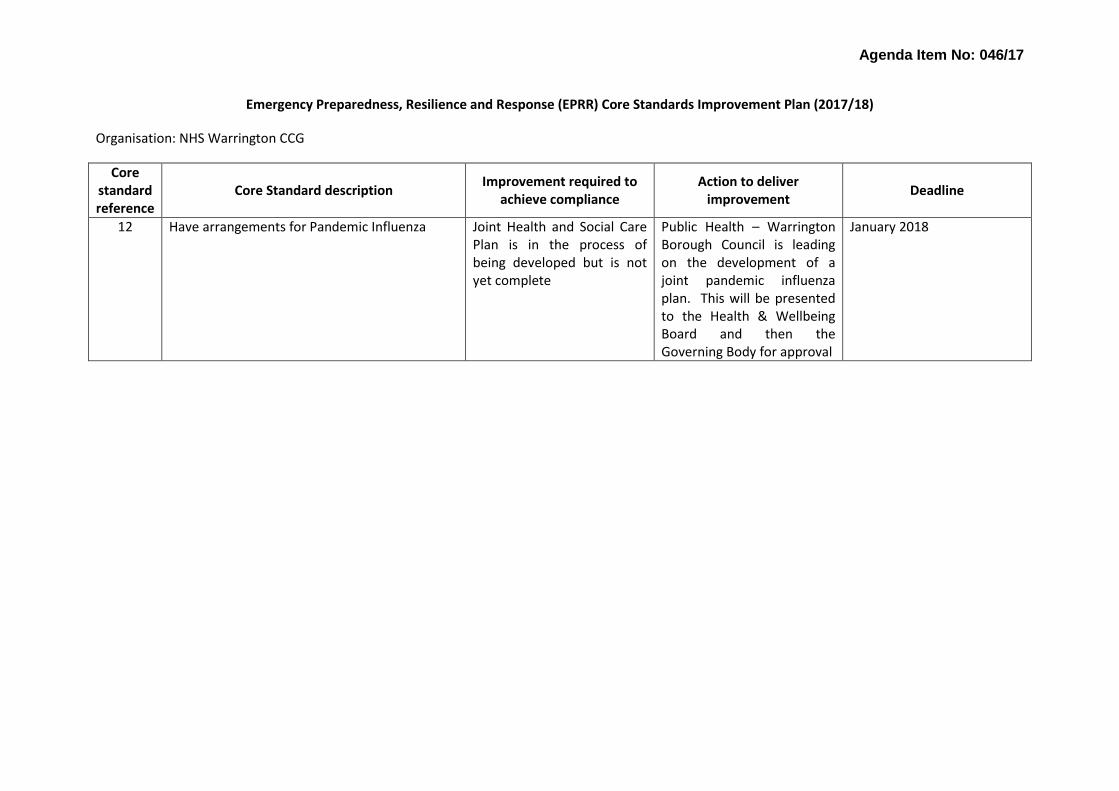
Agenda Item No: 046/17
Emergency Preparedness, Resilience and Response (EPRR) Core Standards Improvement Plan (2017/18)
Organisation: NHS Warrington CCG
Core standard reference
Core Standard description
Improvement required to achieve compliance
Action to deliver improvement
Deadline
12 Have arrangements for Pandemic Influenza Joint Health and Social Care Plan is in the process of being developed but is not yet complete
Public Health – Warrington Borough Council is leading on the development of a joint pandemic influenza plan. This will be presented to the Health & Wellbeing Board and then the Governing Body for approval
January 2018
AGENDA ITEM NO: 047/17
Quality Report Warrington CCG Governing Body Meeting 13
th September 2017
GOVERNING BODY MEETING:
Governing Body Meeting
DATE OF MEETING:
13
th September 2017
REPORT AUTHOR AND JOB TITLE:
John Wharton, Chief Nurse & Quality Lead Dawn Chalmers, Deputy Chief Nurse
REPORT TITLE:
Quality Report
STRATEGIC OBJECTIVES:
Please tick which strategic objectives the paper relates to
Improve quality of services
Sustained financial balance
Build an effective and motivated whole system workforce
Sound governance arrangements
Ensure integration and joint working arrangements
OUTCOME REQUIRED (tick)
Approval
Assurance
Discussion
Information
EXECUTIVE SUMMARY
To provide information to the Governing Body on the quality of services commissioned by NHS Warrington Clinical Commissioning Group by identifying areas where performance falls below expected standards.
To seek scrutiny of the assurance provided by the Quality Committee in relation to the risks and concerns managed by the committee that may impact on patient safety, experience and outcomes in this health economy.
RECOMMENDATIONS
Note and discuss the work being carried out with the providers to address concerns regarding areas of quality provision where the provider may be experiencing difficulties.
Note the assurances regarding NHS Health Education England report and the supporting work to ensure improved synergy between provider and commissioner to ensure potential workforce issues are addressed.
AGENDA ITEM NO: 047/17
Quality Report Warrington CCG Governing Body Meeting 13
th September 2017
Acknowledge the pro-active work being recognised at local and national level by the CHC team in ensuring that patients influence and receive the care from the people / organisations they wish to deliver it.
Outline any engagement – staff, clinical, stakeholder and patient / public
Not applicable
Are there any conflicts of interest which may be associated with this paper?
None identified
Does this paper address any existing risks which are included on the Assurance Framework or Risk Register?
Have the following areas been considered whilst producing this report?
Yes
N/A
Equality Impact Assessment (if yes, attach to paper)
Quality Impact Assessment (if yes, attach to paper)
Regulation, legal, governance and assurance implications (reference in the report if applicable)
Procurement process (reference in the report if applicable)
Document development
Has this document been presented to any other Committee or Forum? If yes, please list which meeting, date and outcome of presentation
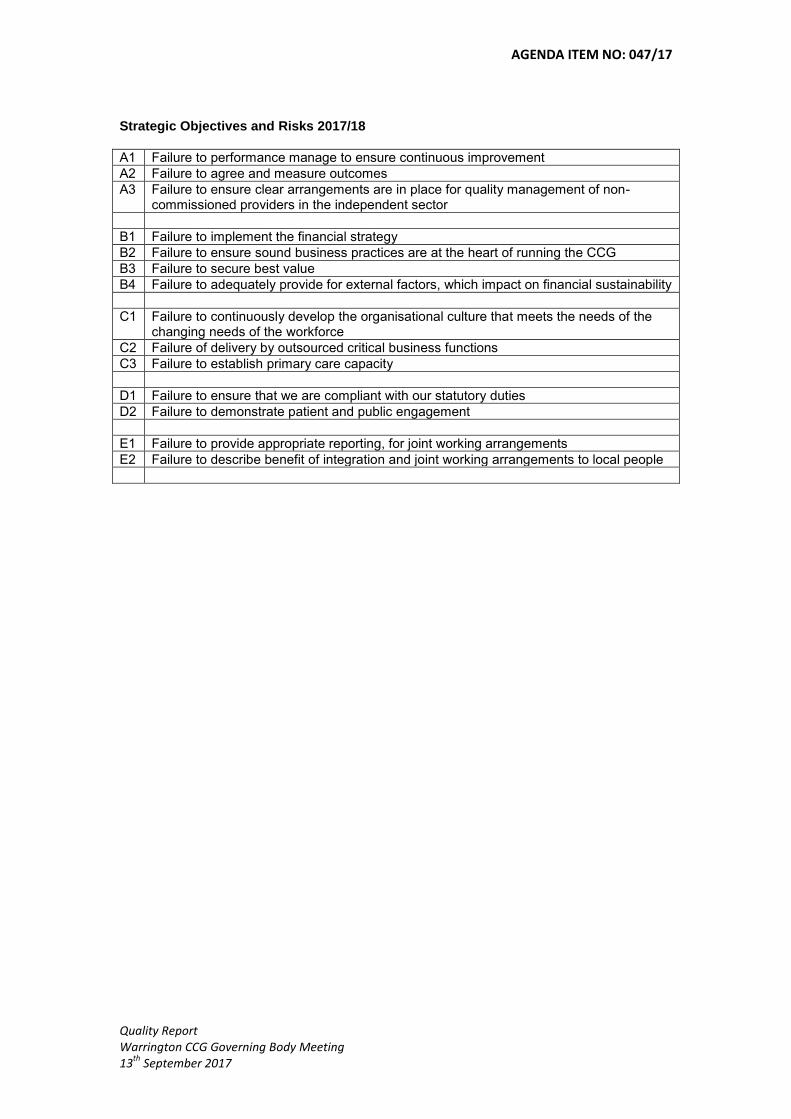
AGENDA ITEM NO: 047/17
Quality Report Warrington CCG Governing Body Meeting 13
th September 2017
Strategic Objectives and Risks 2017/18
A1 Failure to performance manage to ensure continuous improvement
A2 Failure to agree and measure outcomes
A3 Failure to ensure clear arrangements are in place for quality management of non-commissioned providers in the independent sector
B1 Failure to implement the financial strategy
B2 Failure to ensure sound business practices are at the heart of running the CCG
B3 Failure to secure best value
B4 Failure to adequately provide for external factors, which impact on financial sustainability
C1 Failure to continuously develop the organisational culture that meets the needs of the changing needs of the workforce
C2 Failure of delivery by outsourced critical business functions
C3 Failure to establish primary care capacity
D1 Failure to ensure that we are compliant with our statutory duties
D2 Failure to demonstrate patient and public engagement
E1 Failure to provide appropriate reporting, for joint working arrangements
E2 Failure to describe benefit of integration and joint working arrangements to local people
AGENDA ITEM NO: 047/17
Quality Report Warrington CCG Governing Body Meeting 13
th September 2017
WARRINGTON CLINICAL COMMISSIONING GROUP QUALITY REPORT SEPTEMBER 2017
PURPOSE
1. To provide information to the Governing Body on the quality of services commissioned by NHS Warrington Clinical Commissioning Group by identifying areas where performance falls below expected standards.
2. To seek scrutiny of the assurance provided by the Quality Committee in relation to the risks and concerns managed by the committee that may impact on patient safety, experience and outcomes in this health economy.
NEVER EVENTS
3. Spire Cheshire have informed the CCG that there has been a never event regarding a ‘wrong site’ procedure. This was quickly recognised by the organisation and no harm was caused to the patient.
4. The provider adhered to the agreed procedure for reporting to the commissioner and will be submitting a report which will be scrutinised by the Serious Untoward Incident (SUI) group in the coming weeks.
WARRINGTON & HALTON HOSPITAL NHS FOUNDATION TRUST
5. The Clinical Commissioning Group is still awaiting the Care Quality Commission report from the trust; it is anticipated that the trust will be providing detailed feedback at the next Clinical Quality Focus Group.
6. Health Education England have kept the trust on Enhanced Monitoring due to concerns regarding the experience and supervision of trainees working in acute medicine, and concerns have been raised regarding the student experience with the trust in anaesthetics
7. The report by NHS Health Education England offers assurances that following a focused visit earlier in the year small improvements have been made. The trust is looking at ways to increase the numbers of supervisors. This is also backed up by the submission of regular monitoring reports from the trust to Health Education England.
8. The report confirms that improvements have been made in cardiology but the trust will need to strengthen their work particularly around acute medicine and elderly care if their current monitoring status is to be improved upon.
9. The CCG will be working with both organisations to ensure that patient safety is not compromised and that students and trainees are supported appropriately.
AGENDA ITEM NO: 047/17
Quality Report Warrington CCG Governing Body Meeting 13
th September 2017
10. The CCG has not been informed of any issues which may have
impacted of patient care and safety following the recent industrial action by staff members covering the Operating Theatre Department.
BRIDGEWATER COMMUNITY HEALTH NHS FOUNATION TRUST
11. The Clinical Commissioning Group continues to have concerns regarding the organisations governance/risk management processes. Since the last Governing Body a number of serious incidents have been raised and not all have been reported via the correct mechanisms.
12. The Quality Team is working closely with the contracts team to manage both these and other commissioner concerns with respect to delivery of services.
13. The Quality Team will be undertaking an unannounced quality visit
during September to the trusts leg ulcer clinics in response to the outcome of the trusts clinical audit report on compliance against leg ulcer standards
CONTINUING HEALTH CARE ASSURANCE
14. NHS England undertook a CCG assurance deep dive review into NHS Continuing Healthcare in Warrington.
15. The review looked at three domains:- Assessment & Decision Making - lawful, high quality & timely Fast Track Care & Support Planning
16. NHS England has assessed the CCG as OUTSTANDING across all
three domains.
17. Please see Appendix 1 for further information
18. The work of the CHC team has also been acknowledged in NHS England’s recently published Annual Report (2016-17) with reference to the team’s significant work regarding personal health budgets (PHBs) for patients receiving end of life care.
19. Hospice staff identify suitable recipients for PHBs through the Fast Track funding process and have been trained to co-develop personalised support plans and identify health outcomes with patients.
20. Four months into the pilot, 17 people have received PHBs, which have
been used for a range of services to support health outcomes, such as

AGENDA ITEM NO: 047/17
Quality Report Warrington CCG Governing Body Meeting 13
th September 2017
pain management and mental health care. Traditionally, the home care and support package consists of four visits per day and three overnight stays. All recipients of PHBs in the pilot have opted for alternative care and support to this traditional offer, with a fully tailored package and plan put in place that includes services and support the individual may be accessing in the community.
21. Each of the PHBs has resulted in a more efficient use of resources. Work is now in progress to offer PHBs to people not accessing the hospice service, in order to secure equity of access and support across the locality.
PATIENT EXPERIENCE ENGLAND
22. It is nearly ten years since the publication of the Darzi Review, High Quality Care for All. Chapter 4 of that review, “Quality at the heart of everything we do” said, “If quality is to be at the heart of everything we do, it must be understood from the perspective of patients.” It went on to list the three cornerstones of high quality care as patient safety, patient experience and effectiveness of care.
23. A great deal of time and money is now spent on efforts to understand patient experience. Hundreds of organisations produce thousands of reports every year. It can be hard for health professionals and the general public to make sense of it all. This report provides an overview and set out to answer three basic questions:
How is patient experience evidence gathered and disseminated? What are we learning? Are we acting on the learning?
24. The report explains how patient experience evidence is gathered and
disseminated. It shows what has been learnt about patient experience in England over the last year. And importantly, it looks at whether health service providers are acting on the learning.
25. The report highlights positive experiences for cancer patients and an increase in confidence and trust in clinical staff from hospital inpatients.
26. However the report also flags "significant declines" in key areas of
person-centred care.
27. "Substantial concerns" remain about the quality of care some people using community mental health services receive. In maternity services, some women were left alone at a time that worried them during early labour, and of those who raised concerns, not all felt that their concerns were taken seriously.
AGENDA ITEM NO: 047/17
Quality Report Warrington CCG Governing Body Meeting 13
th September 2017
28. A copy of the full report can be found by following the link below https://www.patientlibrary.net/tempgen/162496.pdf
The Governing Body is asked to:
a) Note and discuss the work being carried out with the providers
to address concerns regarding areas of quality provision where the provider may be experiencing difficulties.
b) Note the assurances regarding NHS Health Education England report and the supporting work to ensure improved synergy between provider and commissioner to ensure potential workforce issues are addressed.
c) Acknowledge the pro-active work being recognised at local and
national level by the CHC team in ensuring that patients influence and receive the care from the people / organisations they wish to deliver it.
John Wharton Chief Nurse & Quality Lead Dawn Chalmers Deputy Chief Nurse & Quality Lead September 2017

Dear Chief Nurse CCG Assurance Deep Dive Review into NHS Continuing Healthcare – Warrington
Thank you for your recent participation in the NHS England deep dive review of NHS Continuing Healthcare as part of the assurance process for CCGs in 2017/18, which was presented by Johnathon Murray-Seddon and Louise Long.
We have now completed the process using the evidence submitted, the discussion at the deep dive meeting in addition we considered performance data for 15/16 and 16/17. As part of the Assurance process, NHS England need to understand and evaluate CCGs processes and governance for Continuing Healthcare. This falls out of the need to seek assurance that organisations are well led and review performance including NHS Continuing Healthcare (CHC). The NHS England Continuing Healthcare Operating Model states NHS England needs to be assured that arrangements are in place to meet the overall strategic challenges for NHS Continuing Healthcare in terms of:
• the delivery of the National Framework; • assessment processes that achieve a consistent approach to eligibility
throughout England; • decision making that is sound and legally complaint; and • high quality care being delivered to those found eligible for NHS Continuing
Healthcare. NHS England has assessed the CCG as OUTSTANDING across all three domains.
Continuing Healthcare Priorities for Assurance
Outcome
Assessment & Decision Making - lawful, high quality & timely
Assured Outstanding
Fast Track Assured Outstanding
Care & Support Planning Assured Outstanding
Cheshire & Merseyside Regatta Place
Brunswick Business Park Summers Road
Liverpool L3 4BL
14th July 2017
047/17 Quality Report - Appendix
This was a very good submission with evidence to support compliance against all standards, with good practise described. The discussion at the meeting highlighted the journey the CCG has been on, the model in place currently and future priorities. NHS England was impressed with the comprehensive picture provided of control and insight into managing CHC across Warrington CCG, both in terms of organisational responsibilities and in terms of system leadership.
We would like to thank Johnathon for his continued engagement with the Cheshire and Merseyside network and the contribution made to sharing good practise across and the team, for their professionalism when liaising with NHS England and requests for information.
Next Steps
We will be collating the findings from the Continuing Healthcare deep dives to report at regional and national level. As stated at meetings individual CCG performance will not be shared with wider stakeholders.
The outcome of this deep dive will feed into the overall CCG assurance process. Can I take this opportunity to thank you again for your positive engagement with this process and for your use of the CHAT tool which can be updated and used locally to demonstrate your compliance to the National Framework.
If you have any questions please do not hesitate in contacting me.
Yours sincerely,
Michelle Cox Continuing Health Care Manager – NHS England - North
Julie McGregor Regional Lead Continuing Healthcare – NHS England North
047/17 Quality Report - Appendix
Page 1 of 42
North Region Nursing Assurance Framework
Version 6
NHS England North Nursing Team "Everyone Deserves Great Care"
Agenda Item No: 047/17 - Appendix
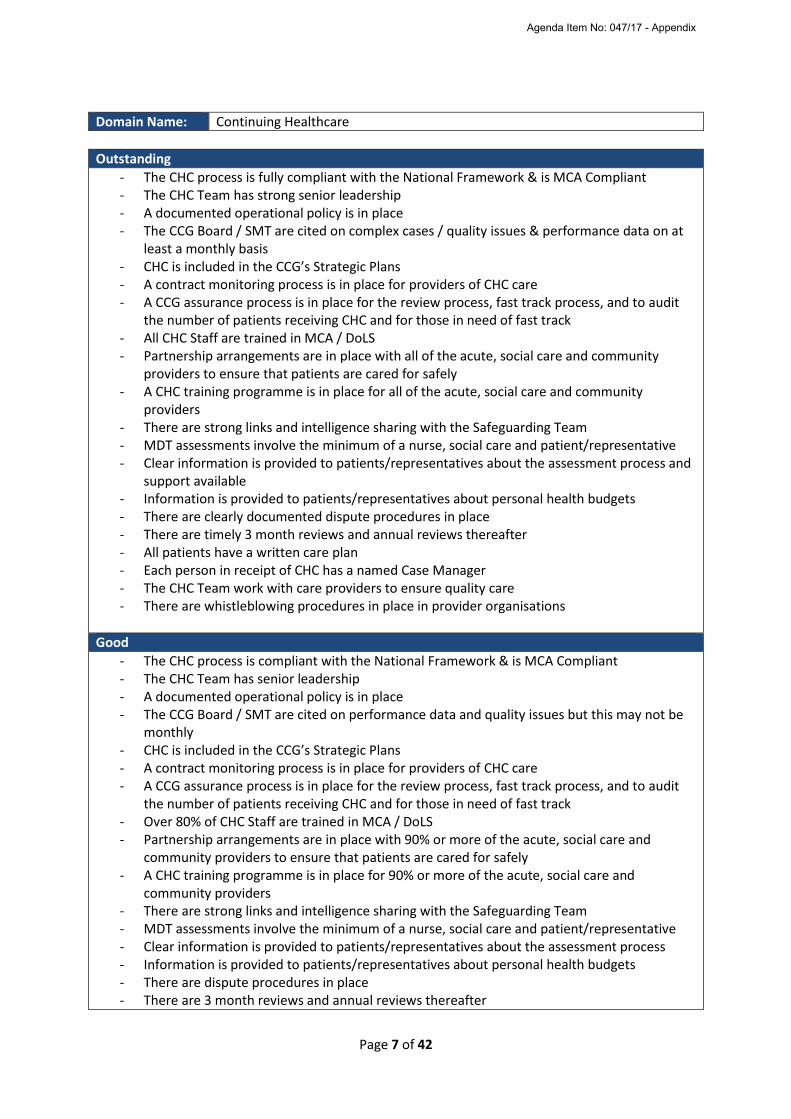
Page 7 of 42
Domain Name: Continuing Healthcare
Outstanding
- The CHC process is fully compliant with the National Framework & is MCA Compliant - The CHC Team has strong senior leadership - A documented operational policy is in place - The CCG Board / SMT are cited on complex cases / quality issues & performance data on at
least a monthly basis - CHC is included in the CCG’s Strategic Plans - A contract monitoring process is in place for providers of CHC care - A CCG assurance process is in place for the review process, fast track process, and to audit
the number of patients receiving CHC and for those in need of fast track - All CHC Staff are trained in MCA / DoLS - Partnership arrangements are in place with all of the acute, social care and community
providers to ensure that patients are cared for safely - A CHC training programme is in place for all of the acute, social care and community
providers - There are strong links and intelligence sharing with the Safeguarding Team - MDT assessments involve the minimum of a nurse, social care and patient/representative - Clear information is provided to patients/representatives about the assessment process and
support available - Information is provided to patients/representatives about personal health budgets - There are clearly documented dispute procedures in place - There are timely 3 month reviews and annual reviews thereafter - All patients have a written care plan - Each person in receipt of CHC has a named Case Manager - The CHC Team work with care providers to ensure quality care - There are whistleblowing procedures in place in provider organisations
Good
- The CHC process is compliant with the National Framework & is MCA Compliant - The CHC Team has senior leadership - A documented operational policy is in place - The CCG Board / SMT are cited on performance data and quality issues but this may not be
monthly - CHC is included in the CCG’s Strategic Plans - A contract monitoring process is in place for providers of CHC care - A CCG assurance process is in place for the review process, fast track process, and to audit
the number of patients receiving CHC and for those in need of fast track - Over 80% of CHC Staff are trained in MCA / DoLS - Partnership arrangements are in place with 90% or more of the acute, social care and
community providers to ensure that patients are cared for safely - A CHC training programme is in place for 90% or more of the acute, social care and
community providers - There are strong links and intelligence sharing with the Safeguarding Team - MDT assessments involve the minimum of a nurse, social care and patient/representative - Clear information is provided to patients/representatives about the assessment process - Information is provided to patients/representatives about personal health budgets - There are dispute procedures in place - There are 3 month reviews and annual reviews thereafter
Agenda Item No: 047/17 - Appendix
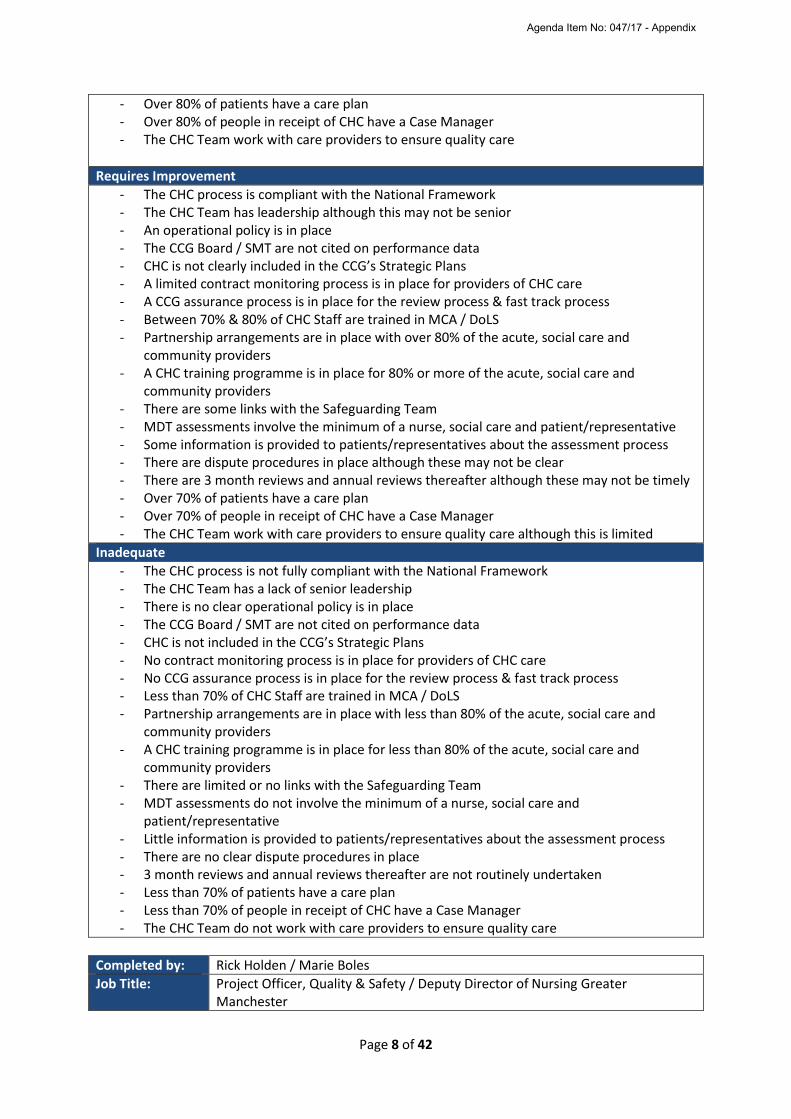
Page 8 of 42
- Over 80% of patients have a care plan - Over 80% of people in receipt of CHC have a Case Manager - The CHC Team work with care providers to ensure quality care
Requires Improvement
- The CHC process is compliant with the National Framework - The CHC Team has leadership although this may not be senior - An operational policy is in place - The CCG Board / SMT are not cited on performance data - CHC is not clearly included in the CCG’s Strategic Plans - A limited contract monitoring process is in place for providers of CHC care - A CCG assurance process is in place for the review process & fast track process - Between 70% & 80% of CHC Staff are trained in MCA / DoLS - Partnership arrangements are in place with over 80% of the acute, social care and
community providers - A CHC training programme is in place for 80% or more of the acute, social care and
community providers - There are some links with the Safeguarding Team - MDT assessments involve the minimum of a nurse, social care and patient/representative - Some information is provided to patients/representatives about the assessment process - There are dispute procedures in place although these may not be clear - There are 3 month reviews and annual reviews thereafter although these may not be timely - Over 70% of patients have a care plan - Over 70% of people in receipt of CHC have a Case Manager - The CHC Team work with care providers to ensure quality care although this is limited
Inadequate
- The CHC process is not fully compliant with the National Framework - The CHC Team has a lack of senior leadership - There is no clear operational policy is in place - The CCG Board / SMT are not cited on performance data - CHC is not included in the CCG’s Strategic Plans - No contract monitoring process is in place for providers of CHC care - No CCG assurance process is in place for the review process & fast track process - Less than 70% of CHC Staff are trained in MCA / DoLS - Partnership arrangements are in place with less than 80% of the acute, social care and
community providers - A CHC training programme is in place for less than 80% of the acute, social care and
community providers - There are limited or no links with the Safeguarding Team - MDT assessments do not involve the minimum of a nurse, social care and
patient/representative - Little information is provided to patients/representatives about the assessment process - There are no clear dispute procedures in place - 3 month reviews and annual reviews thereafter are not routinely undertaken - Less than 70% of patients have a care plan - Less than 70% of people in receipt of CHC have a Case Manager - The CHC Team do not work with care providers to ensure quality care
Completed by: Rick Holden / Marie Boles
Job Title: Project Officer, Quality & Safety / Deputy Director of Nursing Greater Manchester
Agenda Item No: 047/17 - Appendix
Agenda Item No: 048/17
Financial Performance for the period ending 31st
July 2017 NHS Warrington CCG Governing Body 13
th September 2017
COMMITTEE MEETING:
Governing Body Meeting
DATE OF MEETING:
13
th September 2017
REPORT AUTHOR AND JOB TITLE:
David Cooper, Chief Finance Officer
REPORT TITLE:
Financial Performance for the period ending 31
st July 2017
STRATEGIC OBJECTIVES:
Please tick which strategic objectives the paper relates to
Improve quality of services
Sustained financial balance
Build an effective and motivated whole system workforce
Sound governance arrangements
Ensure integration and joint working arrangements
OUTCOME REQUIRED (tick)
Approval
Assurance
Discussion
Information
EXECUTIVE SUMMARY
The financial position at the end of month 4 is reporting an adverse position to plan of £0.145m. Within this year to date position, the following are evident:
Contingency of £1.395m is fully utilised.
Activity Reserve of £0.465m (4/12ths of £1.395m budget) utilised.
Material financial risks (greater than £0.25m) identified during the planning stage, and evident to date, are in the following areas:
- Acute Sector – Historically this service segment has the most variable activity and
high cost performance issues. Growth assumptions have been included within the financial plan but a risk remains that activity, and particularly prices, exceed planned levels. QIPP schemes in place to address this include Ambulatory Emergency Care, Enhanced Care Home Support and Extended Primary Care Access. Further options to secure greater financial stability and a reduction in activity are being explored.
- Community Services impact on Acute Sector activity – The CCG is working with
Agenda Item No: 048/17
Financial Performance for the period ending 31st
July 2017 NHS Warrington CCG Governing Body 13
th September 2017
Bridgewater Community Healthcare Foundation Trust to ensure that services commissioned to reduce the level of activity in the Acute Sector are delivered in accordance with the service specification. For example Paediatric Phlebotomy, Extended Access and Single Point of Access (SPA).
- PbR Tariff Changes (HRG4+) – The CCG earmarked c£2.5m of resource to
accommodate the impact of HRG4+. However the allocation provided to the CCG only amounted to £0.520m, considerably less. The new tariff includes additional coding options to facilitate better data capture. However, the enhanced range of codes available is a risk of a higher cost to CCGs, for the same type and level of activity.
- Better Care Fund: Joint Funded Packages of Care – The increased caseload that
presented during both 2015/16 and 2016/17 financial years identifies a trend that expenditure is expected to grow in this area. Resources are planned at 2016/17 outturn levels plus growth. Commissioning schemes such as the Acquired Brain Injury (ABI) House project and package reviews should manage expenditure growth in this area.
- Prescribing – Horizon scanning has been factored into the planned budget but price
/ demand fluctuations could result in significant pressures. The CCG has a number of
QIPP schemes identified to reduce GP Prescribing costs, including 3rd Party Ordering
(Repeat prescriptions), Optimise Rx, etc.
RECOMMENDATIONS
The Governing Body is asked to:
Note the financial position at the end of July 2017;
Acknowledge financial pressures to date and utilisation of activity reserves and contingency to mitigate;
Acknowledge that the Finance & Performance Committee have instructed that a financial recovery plan be established, with progress monitored; and
Acknowledge the financial risks identified within the report.
Outline any engagement – staff, clinical, stakeholder and patient / public
Not applicable
Are there any conflicts of interest which may be associated with this paper?
None known
Does this paper address any existing risks which are included on the Assurance Framework or Risk Register?
This report provides assurance against risks B2, B3 and B4 from the Assurance Framework.
Have the following areas been considered whilst producing this report?
Yes
N/A
Equality Impact Assessment (if yes, attach to paper)
Agenda Item No: 048/17
Financial Performance for the period ending 31st
July 2017 NHS Warrington CCG Governing Body 13
th September 2017
Quality Impact Assessment (if yes, attach to paper)
Regulation, legal, governance and assurance implications (reference in the report if applicable)
Procurement process (reference in the report if applicable)
Document development
Has this document been presented to any other Committee or Forum? If yes, please list which meeting, date and outcome of presentation
Yes, the Finance & Performance Committee held on 23rd August 2017
Strategic Objectives and Risks 2017/18
A1 Failure to performance manage to ensure continuous improvement
A2 Failure to agree and measure outcomes
A3 Failure to ensure clear arrangements are in place for quality management of non-commissioned providers in the independent sector
B1 Failure to implement the financial strategy
B2 Failure to ensure sound business practices are at the heart of running the CCG
B3 Failure to secure best value
B4 Failure to adequately provide for external factors, which impact on financial sustainability
C1 Failure to continuously develop the organisational culture that meets the needs of the changing needs of the workforce
C2 Failure of delivery by outsourced critical business functions
C3 Failure to establish primary care capacity
D1 Failure to ensure that we are compliant with our statutory duties
D2 Failure to demonstrate patient and public engagement
E1 Failure to provide appropriate reporting, for joint working arrangements
E2 Failure to describe benefit of integration and joint working arrangements to local people
Agenda Item No: 048/17
Financial Performance for the period ending 31st
July 2017 NHS Warrington CCG Governing Body 13
th September 2017
Purpose
1. The purpose of this report is to update members of the NHS Warrington CCG Governing Body on the financial position of the CCG for the 2017/18 financial year.
NHS Warrington CCG Month 4 Financial Position (Detailed in Appendix 1)
2. The financial position at the end of month 4 is an adverse position to plan of £0.145m. Within this reported position, the Contingency resource (£1.395m) has been fully utilised and £0.465m of the Activity Reserve (4/12ths of £1.395m) has also been utilised. The national Risk Reserve (£1.370m), as part of NHS England Business Rules for 2017/18, remains uncommitted at month 4.
3. The level of efficiency savings required in 2017/18 to release the resources required to
support health economy transformation is £8.4m (as agreed during the budget setting
process).
4. Current performance, within the remainder of this report, is outlined in accordance with the
CCG 2017/18 financial planning templates.
Revenue Resource Limit 5. The CCG revenue resource limit has increased by £0.434m to £278.169m. The additional
resources are to support the following items:
+ £0.295m GP Access funding Quarter 1 for 2017/18; and + £0.139m PMS Premium Redistribution Quarter 1 for 2017/18.
6. These resource items are committed in 2017/18 financial year and are not discretionary to
improve the financial position.
Financial Risks and Mitigations
7. The financial risks identified are consistent with performance pressures evident in prior years,
with the most significant risk attributed to acute sector performance.
8. The net risk position for NHS Warrington CCG at month 4 is an in year deficit position of
£0.560m.
9. The underlying financial position reported to NHS England at month 4 has deteriorated further to £1.25m (0.45% of 2017/18 Resource Allocation).
10. The Finance & Performance Committee has instructed the CCG Support Team to establish
as financial recovery plan with progress monitored through the Committee in future periods.
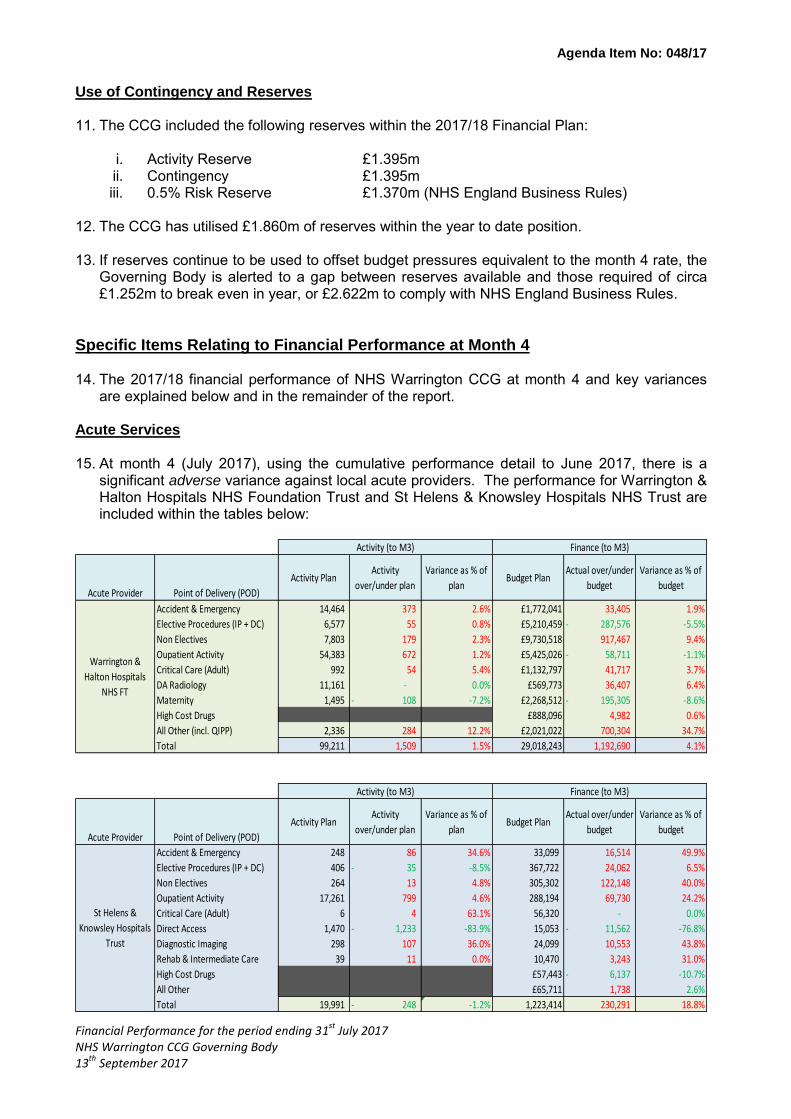
Agenda Item No: 048/17
Financial Performance for the period ending 31st
July 2017 NHS Warrington CCG Governing Body 13
th September 2017
Use of Contingency and Reserves 11. The CCG included the following reserves within the 2017/18 Financial Plan:
i. Activity Reserve £1.395m ii. Contingency £1.395m iii. 0.5% Risk Reserve £1.370m (NHS England Business Rules)
12. The CCG has utilised £1.860m of reserves within the year to date position. 13. If reserves continue to be used to offset budget pressures equivalent to the month 4 rate, the
Governing Body is alerted to a gap between reserves available and those required of circa £1.252m to break even in year, or £2.622m to comply with NHS England Business Rules.
Specific Items Relating to Financial Performance at Month 4 14. The 2017/18 financial performance of NHS Warrington CCG at month 4 and key variances
are explained below and in the remainder of the report. Acute Services 15. At month 4 (July 2017), using the cumulative performance detail to June 2017, there is a
significant adverse variance against local acute providers. The performance for Warrington & Halton Hospitals NHS Foundation Trust and St Helens & Knowsley Hospitals NHS Trust are included within the tables below:
Acute Provider Point of Delivery (POD)
Activity PlanActivity
over/under plan
Variance as % of
planBudget Plan
Actual over/under
budget
Variance as % of
budget
Accident & Emergency 14,464 373 2.6% £1,772,041 33,405 1.9%
Elective Procedures (IP + DC) 6,577 55 0.8% £5,210,459 287,576- -5.5%
Non Electives 7,803 179 2.3% £9,730,518 917,467 9.4%
Oupatient Activity 54,383 672 1.2% £5,425,026 58,711- -1.1%
Critical Care (Adult) 992 54 5.4% £1,132,797 41,717 3.7%
DA Radiology 11,161 - 0.0% £569,773 36,407 6.4%
Maternity 1,495 108- -7.2% £2,268,512 195,305- -8.6%
High Cost Drugs £888,096 4,982 0.6%
All Other (incl. QIPP) 2,336 284 12.2% £2,021,022 700,304 34.7%
Total 99,211 1,509 1.5% 29,018,243 1,192,690 4.1%
Acute Provider Point of Delivery (POD)
Activity PlanActivity
over/under plan
Variance as % of
planBudget Plan
Actual over/under
budget
Variance as % of
budget
Accident & Emergency 248 86 34.6% 33,099 16,514 49.9%
Elective Procedures (IP + DC) 406 35- -8.5% 367,722 24,062 6.5%
Non Electives 264 13 4.8% 305,302 122,148 40.0%
Oupatient Activity 17,261 799 4.6% 288,194 69,730 24.2%
Critical Care (Adult) 6 4 63.1% 56,320 - 0.0%
Direct Access 1,470 1,233- -83.9% 15,053 11,562- -76.8%
Diagnostic Imaging 298 107 36.0% 24,099 10,553 43.8%
Rehab & Intermediate Care 39 11 0.0% 10,470 3,243 31.0%
High Cost Drugs £57,443 6,137- -10.7%
All Other £65,711 1,738 2.6%
Total 19,991 248- -1.2% 1,223,414 230,291 18.8%
Activity (to M3) Finance (to M3)
St Helens &
Knowsley Hospitals
Trust
Activity (to M3) Finance (to M3)
Warrington &
Halton Hospitals
NHS FT
Agenda Item No: 048/17
Financial Performance for the period ending 31st
July 2017 NHS Warrington CCG Governing Body 13
th September 2017
Warrington & Halton Hospitals NHS Foundation Trust (£1.60m adverse variance) 16. Non Elective activity continues to be a key driver of overperformance at this Trust. A straight
line forecast for the year would result in an adverse variance for this contract of circa £3m.
17. QIPP schemes, included within the contract, are reported separately to the activity plan that they relate to. Therefore the expected annual activity savings for the following programmes are not included within the year to date performance.
Enhanced Care Home Support £0.276m
Ambulatory Emergency Care £0.385m
Extended Access in Primary Care £0.126m
18. The forecast outturn variance to plan for Non Elective activity would therefore be circa £3.8m based upon performance to date.
19. The CCG’s Management Team, using the process outlined in the Performance paper delivered to the Governing Body, reviewed the progress of the schemes to date and agreed the actions required to bring activity back in line with plan and to recover any slippage.
St Helens & Knowsley Hospitals NHS Trust (£0.281m adverse variance)
20. Activity costs across all points of delivery (POD) are delivering the year to date adverse position. In most PODs the cost variance exceeds the activity variance, particularly for Non Elective activity (£0.122m adverse at month 4), which suggests that the impact of HRG4+ on the contract is more significant than the contract plan accounted for.
21. On a straight line basis, the forecast outturn position for this contract is circa £1m adverse variance based upon the cumulative position at June 2017.
Mental Health (0.268m favourable variance) 22. The favourable variance reflected in month 4 position relates to investment resources,
established through the budget setting process, that have not been fully utilised to date.
23. Expenditure plans identified against this resource include:
Locked Rehabilitation Facility £0.40m
IAPT Waiting List investment £0.19m
Paediatric Eating Disorder Service £0.17m
Mental Health Crisis House £0.13m
ADHD Assessments (mop up) £0.10m Better Care Fund 24. The CCG has agreed a budget for the year, for the Integrated Commissioning purposes of the
Better Care Fund, amounting to £15.81m of a total £26.1m. The contribution is assigned to the following schemes:
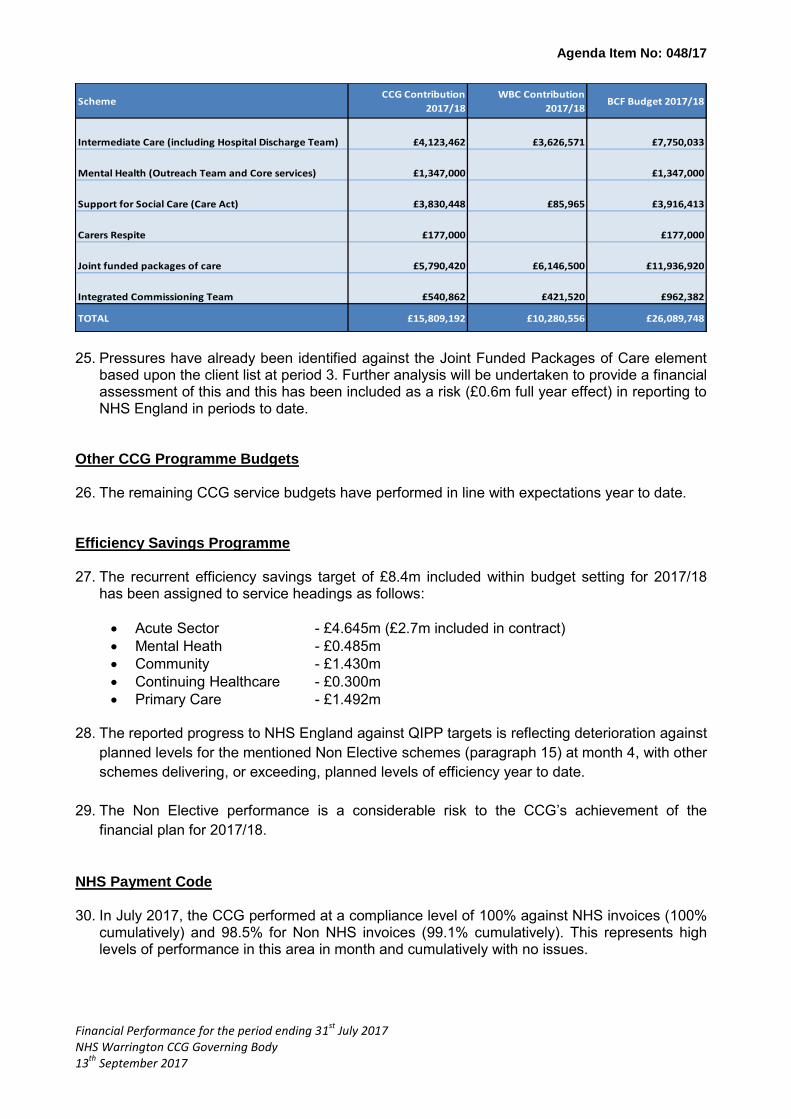
Agenda Item No: 048/17
Financial Performance for the period ending 31st
July 2017 NHS Warrington CCG Governing Body 13
th September 2017
25. Pressures have already been identified against the Joint Funded Packages of Care element
based upon the client list at period 3. Further analysis will be undertaken to provide a financial assessment of this and this has been included as a risk (£0.6m full year effect) in reporting to NHS England in periods to date.
Other CCG Programme Budgets 26. The remaining CCG service budgets have performed in line with expectations year to date. Efficiency Savings Programme 27. The recurrent efficiency savings target of £8.4m included within budget setting for 2017/18
has been assigned to service headings as follows:
Acute Sector - £4.645m (£2.7m included in contract)
Mental Heath - £0.485m
Community - £1.430m
Continuing Healthcare - £0.300m
Primary Care - £1.492m 28. The reported progress to NHS England against QIPP targets is reflecting deterioration against
planned levels for the mentioned Non Elective schemes (paragraph 15) at month 4, with other
schemes delivering, or exceeding, planned levels of efficiency year to date.
29. The Non Elective performance is a considerable risk to the CCG’s achievement of the
financial plan for 2017/18.
NHS Payment Code 30. In July 2017, the CCG performed at a compliance level of 100% against NHS invoices (100%
cumulatively) and 98.5% for Non NHS invoices (99.1% cumulatively). This represents high levels of performance in this area in month and cumulatively with no issues.
SchemeCCG Contribution
2017/18
WBC Contribution
2017/18BCF Budget 2017/18
Intermediate Care (including Hospital Discharge Team) £4,123,462 £3,626,571 £7,750,033
Mental Health (Outreach Team and Core services) £1,347,000 £1,347,000
Support for Social Care (Care Act) £3,830,448 £85,965 £3,916,413
Carers Respite £177,000 £177,000
Joint funded packages of care £5,790,420 £6,146,500 £11,936,920
Integrated Commissioning Team £540,862 £421,520 £962,382
TOTAL £15,809,192 £10,280,556 £26,089,748
Agenda Item No: 048/17
Financial Performance for the period ending 31st
July 2017 NHS Warrington CCG Governing Body 13
th September 2017
Further Information 31. Further details of the CCG’s financial performance to 31st July 2017 can be found in the
following Appendices:
Appendix 1 Financial Performance 2017/18
Recommendations 32. The Governing Body is asked to:
Note the financial position at the end of July 2017;
Acknowledge performance pressures and utilisation of activity reserves and contingency to mitigate;
The Finance & Performance Committee has instructed that a financial recovery plan be established with progress reported in future periods; and
Acknowledge the financial risks identified within the report.
David Cooper Chief Finance Officer September 2017

Agenda Item No: 048/17
2017/18 Financial Performance at Month 4
2017/18 Budget
LedgerYTD Budget YTD Actuals YTD Variance
£ £ £ £
2017-18 Allocations (CCG Resource Limit)Confirmed Allocation 275,568,000 93,092,052 93,092,052 0
Running Costs 4,601,000 1,490,548 1,490,548 0
Total Resource Limit 280,169,000 94,582,600 94,582,600 0
Secondary and Community Care Services
Acute services
Acute contracts -NHS (includes Ambulance services) 147,978,048 49,927,939 51,940,605 -2,012,667
Acute contracts - Other providers (non-nhs, incl. VS) 4,880,731 1,626,898 1,592,898 34,000
Acute - Exclusions / Cost per Case / Non Contracted Activity 2,998,055 999,340 970,265 29,075
Sub-total Acute services 155,856,834 52,554,177 54,503,768 -1,949,592
Mental Health Services
MH contracts - NHS 18,301,235 6,100,401 5,931,335 169,066
MH contracts - Other providers (non-nhs, incl. VS) 5,646,657 1,939,538 1,694,209 245,329
MH - Exclusions / cost per case / Non Contracted Activity 2,343,226 781,049 927,906 -146,857
Better Care Fund Services - Joint Funded MH 2,811,016 937,001 937,001 0
Better Care Fund Services - Mental Health 1,361,957 453,984 453,984 0
Sub-total MH services 30,464,091 10,211,973 9,944,435 267,538
Community Health Services
Community Contracts - NHS 19,832,123 6,675,358 6,810,144 -134,786
Community Contracts - Other providers (non-nhs, incl. VS) 1,566,178 522,040 537,991 -15,951
Better Care Fund Services - Community 4,799,569 1,599,856 1,599,856 0
Sub-total Community services 26,197,870 8,797,254 8,947,991 -150,737
Continuing Care Services
Continuing Care Services (All Care Groups) 9,476,160 3,158,632 3,203,268 -44,636
Free Nursing Care 4,923,105 1,640,995 1,537,923 103,072
Better Care Fund - Joint Funded Care Packages 2,461,029 820,334 820,334 0
Sub-total Continuing Care Services 16,860,294 5,619,961 5,561,525 58,436
Primary Care Services
Prescribing 32,202,507 10,734,129 10,605,473 128,656
Primary Care Investment 576,889 342,550 396,491 -53,941
Out of Hours 1,829,723 609,902 600,000 9,902
Other 2,822,082 940,573 759,461 181,112
Sub-total Primary Care Services 37,431,201 12,627,154 12,361,426 265,728
Other Programme Services
Better Care Fund - Social Care Services 3,867,358 1,289,117 1,289,117 0
Sub-total Other Programme Services 3,867,358 1,289,117 1,289,117 0
Corporate Costs (Running Costs)
Running Cost Corporate Services 4,601,000 1,490,548 1,433,495 57,053
Sub-total Corporate Running costs 4,601,000 1,490,548 1,433,495 57,053
Other Corporate Costs (Non-Running Costs)
Non Running Cost Corporate Services 1,653,173 551,024 637,528 -86,504
Better Care Fund - Additional support roles 145,179 48,392 48,392 0
Sub-total Corporate Non Running costs 1,798,352 599,416 685,920 -86,504
Transformation Investment
Non Recurrent Headroom 1,370,000 0 0 0
Contingency 1,395,000 1,395,000 0 1,395,000
Planned Surplus 31,000 -2,000 -145,077 143,077
Sub-total Transformation Investment 3,092,000 1,393,000 -145,077 1,538,077
Total Planned Expenditure 280,169,000 94,582,600 94,582,600 0
Appendix 1

AGENDA ITEM NO: 049 17
Performance Report focussing on the IAF and Clinical Priorities Year-End Assessment Warrington CCG Governing Body Meeting 13
th September 2017
GOVERNING BODY MEETING:
Governing Body Meeting
DATE OF MEETING:
13
th September 2017
REPORT AUTHOR AND JOB TITLE:
Pam Broadhead Chief Performance Officer
REPORT TITLE:
Performance Report
STRATEGIC OBJECTIVES:
Please tick which strategic objectives the paper relates to
Improve quality of services
Sustained financial balance
Build an effective and motivated whole system workforce
Sound governance arrangements
Ensure integration and joint working arrangements
OUTCOME REQUIRED (tick)
Approval
Assurance
Discussion
Information
EXECUTIVE SUMMARY
The year-end assessments for 2016/17 against the CCG Improvement and Assessment Framework (IAF) and three of the six Clinical Priority areas that sit within the framework have been published. The Clinical Priority Areas draw together the IAF indicators that relate to six vital clinical areas that within the Five Year Forward View and Planning Guidance are national ambitions for transformation. This report details the outcomes published and the actions undertaken and in plan by NHS Warrington CCG.
RECOMMENDATIONS
Report for information and assurance only
AGENDA ITEM NO: 049 17
Performance Report focussing on the IAF and Clinical Priorities Year-End Assessment Warrington CCG Governing Body Meeting 13
th September 2017
Outline any engagement – staff, clinical, stakeholder and patient / public
Not applicable
Are there any conflicts of interest which may be associated with this paper?
None known
Does this paper address any existing risks which are included on the Assurance Framework or Risk Register?
A1 - Failure to performance manage to ensure continuous improvement A2- Failure to agree and measure outcomes
Have the following areas been considered whilst producing this report?
Yes
N/A
Equality Impact Assessment (if yes, attach to paper)
Quality Impact Assessment (if yes, attach to paper)
Regulation, legal, governance and assurance implications (reference in the report if applicable)
Procurement process (reference in the report if applicable)
Document development
Has this document been presented to any other Committee or Forum? If yes, please list which meeting, date and outcome of presentation
Not applicable

AGENDA ITEM NO: 049 17
Performance Report focussing on the IAF and Clinical Priorities Year-End Assessment Warrington CCG Governing Body Meeting 13
th September 2017
Strategic Objectives and Risks 2017/18
A1 Failure to performance manage to ensure continuous improvement
A2 Failure to agree and measure outcomes
A3 Failure to ensure clear arrangements are in place for quality management of non-commissioned providers in the independent sector
B1 Failure to implement the financial strategy
B2 Failure to ensure sound business practices are at the heart of running the CCG
B3 Failure to secure best value
B4 Failure to adequately provide for external factors, which impact on financial sustainability
C1 Failure to continuously develop the organisational culture that meets the needs of the changing needs of the workforce
C2 Failure of delivery by outsourced critical business functions
C3 Failure to establish primary care capacity
D1 Failure to ensure that we are compliant with our statutory duties
D2 Failure to demonstrate patient and public engagement
E1 Failure to provide appropriate reporting, for joint working arrangements
E2 Failure to describe benefit of integration and joint working arrangements to local people
AGENDA ITEM NO: 049 17
Performance Report focussing on the IAF and Clinical Priorities Year-End Assessment Warrington CCG Governing Body Meeting 13
th September 2017
Introduction
1. 2016/17 saw NHS England introduce a new Improvement and
Assessment Framework for CCGs (CCG IAF). The new framework
aligned key objectives and priorities and formed the basis of the NHS
England assessment of CCGs. The 2016/17 year-end assessment
against the IAF and three of the six Clinical Priority areas (that sit within
the framework) have been published.
2. This report to the Governing Body outlines the areas in exception for
the IAF and provides members with detail on the indicators that sit
within the published Clinical Priorities. Appendix A shows the summary
of the IAF indicators and Appendix B is the Clinical Priority
Assessment.
2016/17 IAF Assessment
3. The published annual assessment under the NHS England CCG
Improvement and Assessment Framework for 2016/17 for NHS
Warrington CCG is one of “requires improvement”. This represents
maintenance of the assessment of the previous year. 25% of the
assessment is based on the financial outturn of the CCG (not covered
in this report) and 25% on the quality of leadership of the CCG
(assessed as green – the second highest rating). The remaining 50%
of the CCG assessment process is based on performance and
outcome measures.
4. CCGs are scored out of 2 and from that score categorised into one of
four groups; Outstanding, Good, Requires Improvement or Inadequate.
NHS Warrington CCG scored 0.87 (the threshold for an assessment of
“good” is a score of one).
IAF Indicators in the Lowest Quartile
5. Better Health – Diabetes – Attendance at Structured Education – the
assessment for 2016/17 is based on the results from the 2015/16
survey. (The 2016/17 survey has just been completed and all practices
in Warrington have submitted.) Governing Body is reminded that prior
to April 2016 the provider of the education service did not confirm
patient attendance with general practice and therefore this information
was not recorded in patient clinical records (the source of the Diabetes
Survey), resulting in the 0% achievement cited in the assessment.
Diabetes education within Warrington is currently being re-launched
AGENDA ITEM NO: 049 17
Performance Report focussing on the IAF and Clinical Priorities Year-End Assessment Warrington CCG Governing Body Meeting 13
th September 2017
following the successful bid for funding from the Diabetes Treatment
and Care Transformation monies.
6. Better Health – Falls – Emergency Admissions due to Falls in People
aged 65+ - in comparison with peer CCGs, Warrington has the second
highest rate of admissions attributed to falls in the 65+ cohort. This
measure was reviewed as part of the Quality, Innovation, Productivity
and Prevention (QIPP) monitoring process in August and remedial
actions were identified to improve the rate of admissions due to falls,
including:
Re-launch of the Falls Strategy to include specific actions and
responsible leads for delivery.
Governance and Terms of Reference of the Falls Strategy to be
formalised through Senior Management Team to ensure
appropriate reporting and accountability is defined.
Clinical Pharmacists review of poly-pharmacy patients internally
escalated to ensure this work is scheduled.
Review of care homes with “no-lift” policies and lifting equipment to
be trialled.
7. Better Health/Better Care – Inequality in Unplanned Admissions for
Urgent Care Sensitive Conditions and Emergency Admissions for
Urgent Care Sensitive Conditions (two linked indicators) – the
underlying number of admissions for conditions included within these
indicators has increased. These conditions have been reviewed
internally and the committee should note that the majority are within the
Ambulatory Emergency Care (AEC) category. Therefore an increase in
admissions for most of this cohort of patients is not unexpected as the
appropriate management of people on an AEC pathway is a zero
length of stay admission. The CCG has plans for the management of
frailty on attendance at hospital which should lead to more appropriate
management of some conditions within this category.
8. Well Led – Working Relationship Effectiveness – This indicator was
assessed using the CCG stakeholder 360⁰ survey. This survey was
sent to each of the key CCG stakeholder groups: upper tier/unitary
local authority, health and wellbeing board, Healthwatch and patient
groups, GP member practices, NHS providers, other CCGs and key
stakeholders. The score can vary from 0 to 100, with 100 being the
best possible score. The final score is an average from all respondents.
9. NHS Warrington CCG saw a slight deterioration in the results from the
stakeholder survey. The reduction in the 2016/17 results can be
attributed to a number of factors which include being a pro-active co-
AGENDA ITEM NO: 049 17
Performance Report focussing on the IAF and Clinical Priorities Year-End Assessment Warrington CCG Governing Body Meeting 13
th September 2017
ordinator for a wide range of NHS Standard Contracts. Actions taken
in respect to the deterioration in working relationships include; a new
process to support Federation Leads and enable a more effective
dialogue across the four federations regarding commissioning
business, the introduction of a new schedule Commissioning Protected
Learning Time (PLTs) supported by clinical leads and commissioners
and Primary Care Service Development Managers are now in post to
support the development of the Primary Care Clusters and the
Warrington Enhanced Service.
10. Better Care – Cancer Waiting Times – 62 day GP referral to treatment -
Performance against cancer waiting times standards has been
pressured for some time, particularly in respect of 62 days from GP
referral and 2 week waits for breast symptoms (where cancer is not
initially suspected).
11. Significant work has been undertaken by the support team with our
Providers and primary care in relation to cancer waiting time standards.
The performance for both of these indicators improved in June 2017
compared to the previous month and the CCG has been given an early
indication that, on a provider basis at Warrington & Halton Hospitals
NHS Foundation Trust, the July performance shows further
improvement.
12. An example result of the collaborative work between the CCG support
team and providers is at Warrington & Halton Hospitals NHS
Foundation Trust where significant changes to their processes related
to the tracking and escalation of pathways have been implemented.
The impact of these changes should be reflected in the July
performance.
13. Better Care – Experience and Choice of Maternity Services –
performance against these two indicators for 2016/17 has been
assessed against the survey from 2015. The next iteration of the
National Maternity Survey is underway with the results expected in late
2017. Until recently the available choices within maternity services
were not consistently, routinely explained to patients either verbally or
in writing. Therefore, supported by the CCG Communications and
Engagement team, a patient information leaflet detailing the Warrington
specific choice options for maternity care has been published and is
given out to all expectant mothers registered with NHS Warrington
CCG GPs.
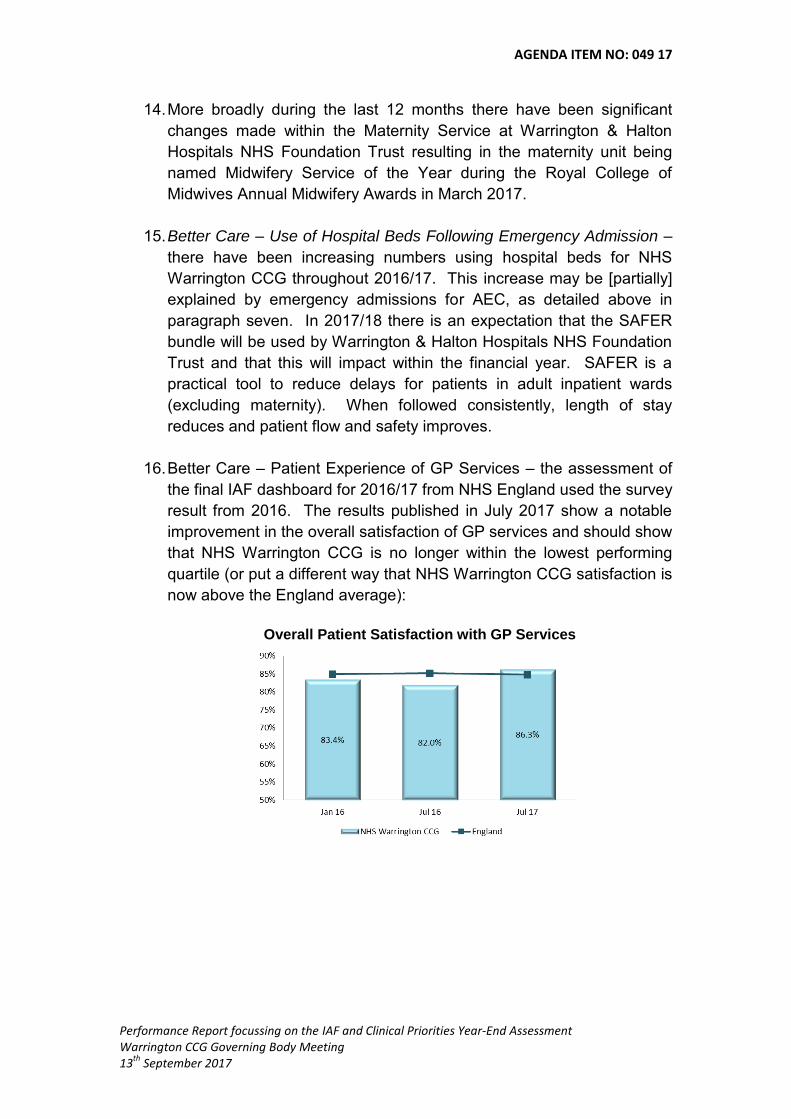
AGENDA ITEM NO: 049 17
Performance Report focussing on the IAF and Clinical Priorities Year-End Assessment Warrington CCG Governing Body Meeting 13
th September 2017
14. More broadly during the last 12 months there have been significant
changes made within the Maternity Service at Warrington & Halton
Hospitals NHS Foundation Trust resulting in the maternity unit being
named Midwifery Service of the Year during the Royal College of
Midwives Annual Midwifery Awards in March 2017.
15. Better Care – Use of Hospital Beds Following Emergency Admission –
there have been increasing numbers using hospital beds for NHS
Warrington CCG throughout 2016/17. This increase may be [partially]
explained by emergency admissions for AEC, as detailed above in
paragraph seven. In 2017/18 there is an expectation that the SAFER
bundle will be used by Warrington & Halton Hospitals NHS Foundation
Trust and that this will impact within the financial year. SAFER is a
practical tool to reduce delays for patients in adult inpatient wards
(excluding maternity). When followed consistently, length of stay
reduces and patient flow and safety improves.
16. Better Care – Patient Experience of GP Services – the assessment of
the final IAF dashboard for 2016/17 from NHS England used the survey
result from 2016. The results published in July 2017 show a notable
improvement in the overall satisfaction of GP services and should show
that NHS Warrington CCG is no longer within the lowest performing
quartile (or put a different way that NHS Warrington CCG satisfaction is
now above the England average):
Overall Patient Satisfaction with GP Services
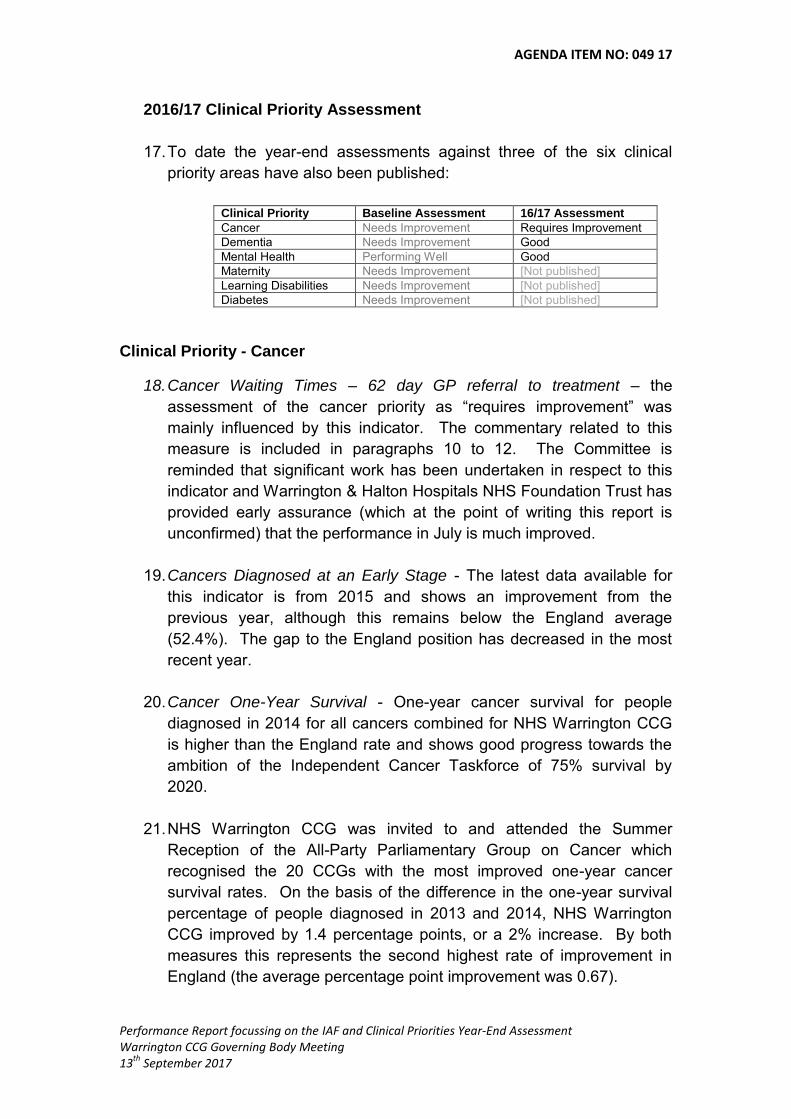
AGENDA ITEM NO: 049 17
Performance Report focussing on the IAF and Clinical Priorities Year-End Assessment Warrington CCG Governing Body Meeting 13
th September 2017
2016/17 Clinical Priority Assessment
17. To date the year-end assessments against three of the six clinical
priority areas have also been published:
Clinical Priority Baseline Assessment 16/17 Assessment
Cancer Needs Improvement Requires Improvement
Dementia Needs Improvement Good
Mental Health Performing Well Good
Maternity Needs Improvement [Not published]
Learning Disabilities Needs Improvement [Not published]
Diabetes Needs Improvement [Not published]
Clinical Priority - Cancer
18. Cancer Waiting Times – 62 day GP referral to treatment – the
assessment of the cancer priority as “requires improvement” was
mainly influenced by this indicator. The commentary related to this
measure is included in paragraphs 10 to 12. The Committee is
reminded that significant work has been undertaken in respect to this
indicator and Warrington & Halton Hospitals NHS Foundation Trust has
provided early assurance (which at the point of writing this report is
unconfirmed) that the performance in July is much improved.
19. Cancers Diagnosed at an Early Stage - The latest data available for
this indicator is from 2015 and shows an improvement from the
previous year, although this remains below the England average
(52.4%). The gap to the England position has decreased in the most
recent year.
20. Cancer One-Year Survival - One-year cancer survival for people
diagnosed in 2014 for all cancers combined for NHS Warrington CCG
is higher than the England rate and shows good progress towards the
ambition of the Independent Cancer Taskforce of 75% survival by
2020.
21. NHS Warrington CCG was invited to and attended the Summer
Reception of the All-Party Parliamentary Group on Cancer which
recognised the 20 CCGs with the most improved one-year cancer
survival rates. On the basis of the difference in the one-year survival
percentage of people diagnosed in 2013 and 2014, NHS Warrington
CCG improved by 1.4 percentage points, or a 2% increase. By both
measures this represents the second highest rate of improvement in
England (the average percentage point improvement was 0.67).

AGENDA ITEM NO: 049 17
Performance Report focussing on the IAF and Clinical Priorities Year-End Assessment Warrington CCG Governing Body Meeting 13
th September 2017
22. For both early diagnosis and one-year survival the activities to improve
performance are similar. Work is on-going in respect of reporting of
localised screening rates, cancer symptoms awareness-raising in
conjunction with the Local Authority/Public Health and supporting Be
Clear on Cancer campaigns. NHS Warrington CCG with Macmillan
Cancer Support is also in the second year of providing a 12 month
course for practice nurses to increase knowledge of cancer signs and
symptoms and to help them support people living with and beyond
cancer.
23. Cancer Patient Experience - The Independent Cancer Taskforce set an
ambition for continuous improvement in patient experience and has
given it the same priority as clinical outcomes. The 2016 Cancer
Patient Experience Survey has been published and NHS Warrington
CCG has been identified as having no significant change in any
indicator (either positive or negative) from the 2015 report but the
overall score for the CCG has declined slightly from the 2015 position.
Similarly the Warrington & Halton Hospitals NHS Foundation Trust
results show no significant change but the overall score is below than
the expected range.
24. Warrington & Halton Hospitals NHS Foundation Trust and NHS
Warrington CCG have instigated a series of workshops for Cancer
Nurse Specialists. The September workshop will be used, in part, to
identify the actions and responsible leads to improve patient
experience within cancer services.
Clinical Priority – Mental Health
25. The assessment of this priority in 2016/17 was “good”. There were five
indicators included within the assessment.
26. Improving Access to Psychological Therapies – Recovery Rate – the
national requirement is for at least 50% of people receiving therapies to
recover. NHS Warrington CCG achieved an average of 54% across
the year and 53% in the rolling quarter to January used in the
assessment.
27. This achievement has been established following the implementation of
a Recovery Protocol in December 2015. This increased recovery rates
to 50% almost immediately. The Recovery Protocol has continued to
be adapted to meet patient needs and requirements and is amended,
when required, to compliment new ways of working.
AGENDA ITEM NO: 049 17
Performance Report focussing on the IAF and Clinical Priorities Year-End Assessment Warrington CCG Governing Body Meeting 13
th September 2017
28. Early Intervention Psychosis (EIP) – Waiting Times – the national
requirement is for at least 50% of people referred experiencing first
episode psychosis or at ‘risk mental state’ to start treatment within two
weeks of referral. For the year to March 2017 this was achieved with
86% starting treatment within two weeks.
29. The EIP service seeks to continuously develop and implement
improved ways of working to ensure the achievement of the required
standard is maintained. All referrals to the service are reviewed on a
‘working’ daily basis and the provider manages capacity and demand
accordingly. The team assertively outreaches to those who cannot or
do not attend assessment appointments.
30. Mental Health Transformational Milestones – there are three indicators
within this section relating to Children and Young People (CYP), Out of
Area Placements and Crisis Care/Liaison. These were assessed
according to the information provided on a self-assessment submission
in April 2017. In the assessment all three indicators were significantly
above the minimum level required.
Clinical Priority – Dementia
31. The 2016/17 rating for dementia considered two indicators: dementia
diagnosis rates and care plan reviews. The overall assessment was
“good”.
32. Dementia Diagnosis Rate – the requirement is for at least 66.7% of the
estimated population with dementia have the diagnosis recorded on the
GP clinical system. The March 2017 rate used in the assessment was
70%.
33. Dementia Care Plan Reviews – this indicator requires that people with
dementia have a face-to-face review of their care plan as a proxy
measure for post-diagnosis support. The Local Enhanced Service
agreement encourages GP practices to review patients with dementia
and provide regular support alongside routine medical care. This
indicator was assessed in comparison to the 2014/15 baseline and saw
an increase the rate of care plans for NHS Warrington CCG completed
by one percentage point.
34. The assessment of the dementia priority area has improved in the
2016/17 review compared to the previous year. This demonstrates the
on-going work undertaken by Primary Care to improve the rate of

AGENDA ITEM NO: 049 17
Performance Report focussing on the IAF and Clinical Priorities Year-End Assessment Warrington CCG Governing Body Meeting 13
th September 2017
referrals to the Memory Clinic by increasing service capacity though
discharge of stable patients to their own GP.
35. Margi Butler, Head of Commissioning for Mental Health, Learning
Disability & Dementia acknowledged the work that colleagues across
primary and secondary care, statutory and independent sectors and
commissioners have undertaken to achieve these good results, which
will improve outcomes for patients and their carers. Warrington has
intelligent and meaningful local strategies for mental health and
dementia and these are supported by national strategy. The CCG
Clinical Leads have also supported successful delivery of these IAF
priorities.
Pam Broadhead Chief Performance Officer 5th September 2017

CCG Summary Dashboard
NHS Warrington CCG
Better Health Period CCG Peers England Trend Better Care Period CCG Peers England Trend
R 101a n/d Maternal smoking at delivery 16-17 Q3 7.9% 1/11 65/209 R 121a n/a High quality care - acute 16-17 Q4 63 2/11 28/209
R 102a n/d % 10-11 classified overweight /obese12/13 to 14/15 31.3% 3/11 73/209 R 121b n/a High quality care - primary care 16-17 Q4 65 6/11 99/209
R 103a n/d Patients who achieved NICE targets2015-16 40.6% 7/11 69/209 R 121c n/a High quality care - adult social care16-17 Q4 64 3/11 12/209
R 103b ✘ Attendance of structured education course2014 0.0% 11/11 207/209 R 122a n/d Cancers diagnosed at early stage2015 51.0% 7/11 133/209
R 104a ✘ Injuries from falls in people 65yrs +16-17 Q3 2,997 10/11 205/209 R 122b ✘ Cancer 62 days of referral to treatment16-17 Q4 76.4% 9/11 162/209
R 105a n/a Utilisation of the NHS e-referral 2017 03 63.8% 4/11 #DIV/0! R 122c n/d One-year survival from all cancers2014 71.3% 2/11 46/209
R 105b n/a Personal health budgets 16-17 Q4 50 2/11 23/209 122d n/d Cancer patient experience 2015 8.7 9/11 100/209
R 105c n/a % of deaths in hospital 16-17 Q2 49.7% 4/11 78/209 R 123a n/d IAPT recovery rate 2017 01 53.0% 6/11 56/209
105d n/d LTC feeling supported 2016 03 66.3% 6/11 58/209 R 123b ✔ EIP 2 week referral 2017 03 86.4% 2/11 39/209
R 106a n/d Inequality Chronic - ACS 16-17 Q3 1,063 6/11 147/209 R 123c n/a MH - CYP mental health 16-17 Q4 85% 3/11 74/209
R 106b ✘ Inequality - UCS 16-17 Q3 3,438 11/11 206/209 R 123d n/a MH - Crisis care and liaison 16-17 Q4 75.0% 5/11 86/209
R 107a ✘ AMR: appropriate prescribing 2017 02 1.12 4/11 122/209 R 123e n/a MH - OAP 16-17 Q4 100.0% 1/11 1/209
R 107b ✘ AMR: Broad spectrum prescribing2017 02 8.7% 7/11 102/209 R 124a ✘ LD - reliance on specialist IP care16-17 Q4 70 6/11 146/209
108a n/a Quality of life of carers 2016 03 0.81 3/11 71/209 124b n/d LD - annual health check 2015-16 36.4% 5/11 114/209
Sustainability Period CCG Peers England Trend R 125a n/d Neonatal mortality and stillbirths2015 5.4 2/11 48/209
R 141a n/a Financial plan 2016 Amber 5/11 88/209 125b n/a Experience of maternity services2015 75.2 11/11 188/209
R 141b n/a In-year financial performance 16-17 Q4 Red 7/11 88/209 125c n/a Choices in maternity services 2015 61.1 10/11 185/209
R 142a n/a Improvement area: Outcomes 16-17 Q3 50.0% 9/11 165/209 R 126a n/a Dementia diagnosis rate 2017 03 70.1% 5/11 83/209
R 142b n/a Improvement area: Expenditure 16-17 Q3 0.0% 11/11 204/209 126b n/d Dementia post diagnostic support2015-16 78.0% 9/11 134/209
R 143a n/a New models of care 16-17 Q4 N #VALUE! R 127a n/a Delivery of an integrated urgent care service2017 01 5 6/11 65/209
R 144a n/a Local digital roadmap in place 16-17 Q4 Y #VALUE! R 127b n/d Emergency admissions for UCS conditions16-17 Q3 3,334 9/11 189/209
R 144b n/a Digital interactions 16-17 Q4 73.5% 2/11 25/209 R 127c ✘ A&E admission, transfer, discharge within 4 hours2017 03 90.9% 6/11 90/209
R 145a n/a SEP in place 2016-17 Y #VALUE! #VALUE! R 127e n/d Delayed transfers of care per 100,000 population2017 03 8.3 5/11 46/209
Well Led Period CCG Peers England Trend R 127f ✘ Hospital bed use following emerg admission16-17 Q3 618.6 11/11 204/209
R 161a n/a STP 2016-17 Green 1/11 1/209 R 128a n/d Management of LTCs 16-17 Q3 949 4/11 130/209
R 162a n/a Probity and corporate governance16-17 Q4 Fully Compliant 1/11 1/209 R 128b n/d Patient experience of GP services2016 03 82.0% 11/11 171/209
R 163a n/a Staff engagement index 2016 3.74 8/11 156/209 R 128c n/a Primary care access 2017 03 60.7% 3/11 36/209
R 163b n/a Progress against WRES 2016 0.07 3/11 19/209 R 128d n/d Primary care workforce 2016 09 0.93 6/11 124/209
R 164a n/a Working relationship effectiveness16-17 62.50 9/11 168/209 R 129a ✔ 18 week RTT 2017 03 93.9% 4/11 30/209
R 165a n/a Quality of CCG leadership 16-17 Q4 Green 2/11 31/209 R 130a n/a 7 DS - achievement of standards2016-17 0.0% 1/11 #N/A
Key R 131a n/a People eligible for standard NHS CHC16-17 Q3 36.5 6/11 130/209
Worst quartile in England Best quartile in England
Interquartile range
Requires Improvement
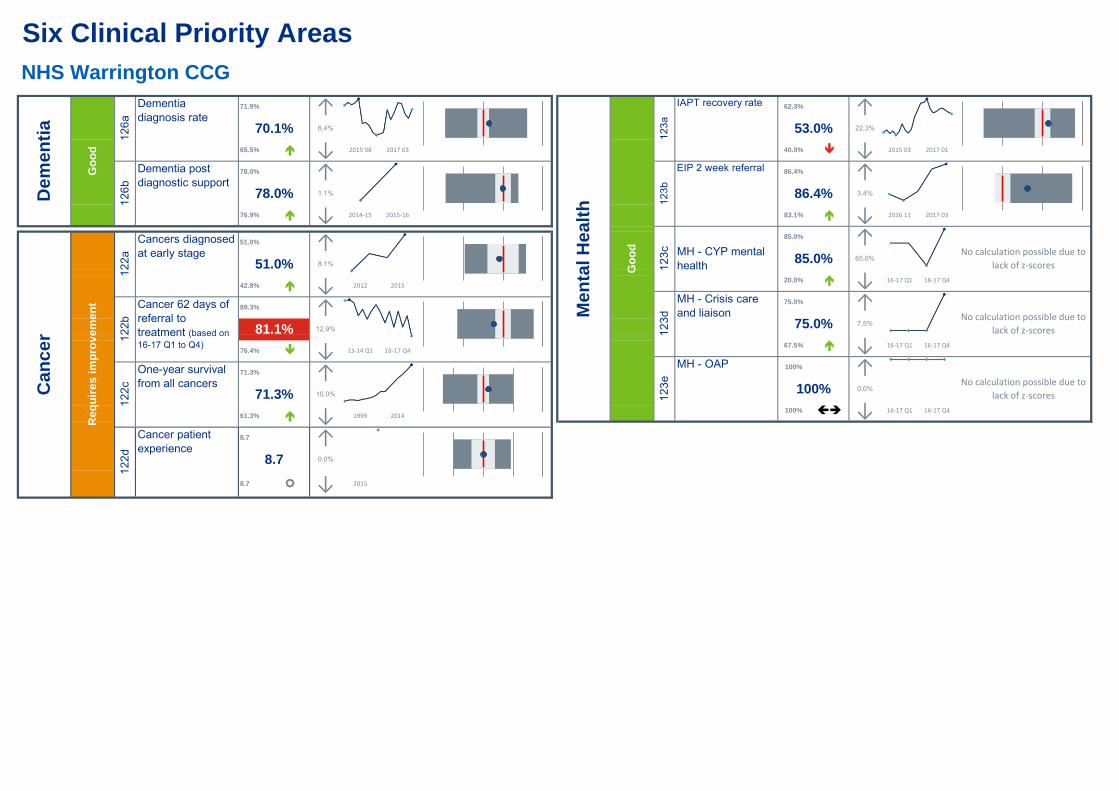
Six Clinical Priority Areas
NHS Warrington CCG
22.3%
3.4%
↑
16-17 Q1 16-17 Q4
No calculation possible due to
lack of z-scores
67.5%
100% 1
1
100%
100%
No calculation possible due to
lack of z-scores
No calculation possible due to
lack of z-scores
↑↓
65.0%
7.5%
↑
2015 03 2017 01
2016 11
1
81.1%
Me
nta
l H
ea
lth
12
3a
12
3b
83.1%
0.0%
↑↓
Go
od
1
85.0%
75.0%
↓
86.4% 1
↓
MH - OAP
↑↓
85.0%
20.0%
75.0%
Dementia post
diagnostic support
Cancers diagnosed
at early stage
Dementia
diagnosis rate70.1%
71.9% 1
65.5%
78.0% 1
78.0%
76.9%
2014-15 2015-16
12
3c
12
3d
12
3e
IAPT recovery rate 62.3% 1
53.0%
40.0%
86.4%
EIP 2 week referral
MH - CYP mental
health
MH - Crisis care
and liaison
2017 03
16-17 Q1 16-17 Q4
16-17 Q1 16-17 Q413-14 Q1 16-17 Q4
2012
1999 2014
2015
76.4%
89.3%
71.3% 1
71.3%
61.3%
51.0% 1
51.0%
42.8%
One-year survival
from all cancers
Cancer patient
experience
8.7
Cancer 62 days of
referral to
treatment (based on
16-17 Q1 to Q4)
2015 08 2017 03
Go
od
De
me
nti
a
12
6a
12
6b
12.9%
↓↑10.0%
↑
↓
12
2a
12
2b
12
2c
6.4%
↑1.1%
↓
Ca
nc
er
12
2d
↓ 2015 2015
Re
qu
ire
s i
mp
rov
em
en
t
8.7 1 ↑8.7 0.0%
↑
↓
↑
↓
8.1%
AGENDA ITEM NO: 050/17
Contract Update Warrington CCG Governing Body 13
th September 2017
GOVERNING BODY MEETING:
Governing Body Meeting
DATE OF MEETING:
13
th September 2017
REPORT AUTHOR AND JOB TITLE:
Pam Broadhead Chief Performance Officer
REPORT TITLE:
Contract Report
STRATEGIC OBJECTIVES:
Please tick which strategic objectives the paper relates to
Improve quality of services
Sustained financial balance
Build an effective and motivated whole system workforce
Sound governance arrangements
Ensure integration and joint working arrangements
OUTCOME REQUIRED (tick)
Approval
Assurance
Discussion
Information
EXECUTIVE SUMMARY
This contract report gives information to the Governing Body with respect to service delivery by the following providers
Bridgewater Community Healthcare NHS Foundation Trust
Care Homes
North West Boroughs Healthcare NHS Foundation Trust (formerly 5 Boroughs Healthcare NHS Foundation Trust
Mental Health Matters
Primary Care
Warrington & Halton Hospitals NHS Foundation Trust
WRAG
RECOMMENDATIONS
For information only

AGENDA ITEM NO: 050/17
Contract Update Warrington CCG Governing Body 13
th September 2017
Outline any engagement – staff, clinical, stakeholder and patient / public
Not applicable
Are there any conflicts of interest which may be associated with this paper?
None known
Does this paper address any existing risks which are included on the Assurance Framework or Risk Register?
A1 - Failure to performance manage to ensure continuous improvement A2- Failure to agree and measure outcomes
Have the following areas been considered whilst producing this report?
Yes
N/A
Equality Impact Assessment (if yes, attach to paper)
Quality Impact Assessment (if yes, attach to paper)
Regulation, legal, governance and assurance implications (reference in the report if applicable)
Procurement process (reference in the report if applicable)
Document development
Has this document been presented to any other Committee or Forum? If yes, please list which meeting, date and outcome of presentation
Not applicable
AGENDA ITEM NO: 050/17
Contract Update Warrington CCG Governing Body 13
th September 2017
Strategic Objectives and Risks 2017/18
A1 Failure to performance manage to ensure continuous improvement
A2 Failure to agree and measure outcomes
A3 Failure to ensure clear arrangements are in place for quality management of non-commissioned providers in the independent sector
B1 Failure to implement the financial strategy
B2 Failure to ensure sound business practices are at the heart of running the CCG
B3 Failure to secure best value
B4 Failure to adequately provide for external factors, which impact on financial sustainability
C1 Failure to continuously develop the organisational culture that meets the needs of the changing needs of the workforce
C2 Failure of delivery by outsourced critical business functions
C3 Failure to establish primary care capacity
D1 Failure to ensure that we are compliant with our statutory duties
D2 Failure to demonstrate patient and public engagement
E1 Failure to provide appropriate reporting, for joint working arrangements
E2 Failure to describe benefit of integration and joint working arrangements to local people
AGENDA ITEM NO: 050/17
Contract Update Warrington CCG Governing Body 13
th September 2017
Introduction
1. The Finance and Performance Committee held on 30th September 2017 requested a
report to be presented to Governing Body detailing the current headlines/key issues for a number of specific contracts held by NHS Warrington CCG.
2. This outline report is provided to Governing Body and gives an overview position. If
any additional information is required about any of the issues outlined below the table below gives the contact details of the relevant governing body lead and/or senior management lead. Alternatively there is a generic email address for the Contracts and Performance Team which is [email protected]
Contract GP Governing Body Lead/Senior Management Team Lead
Bridgewater Community Healthcare NHS Foundation Trust
Dr Michihiro Tomanaga
Care Homes Mr John Wharton
North West Boroughs Healthcare NHS Foundation Trust (formerly 5 Boroughs Healthcare NHS Foundation Trust
Dr Laura Mount
Mental Health Matters Pam Broadhead
Primary Care Linda Bennett
Warrington & Halton Hospitals NHS Foundation Trust
Dr Ian Watson
WRAG Nick Armstrong
Bridgewater Community Healthcare NHS Foundation Trust (Community Services
Provider)
Contract Value (excluding CQUIN) £19,389,000
Contract Value (including CQUIN) £19,874,000
Performance Notices o No current Performance Notices
Performance Notices Details / Other Items to Note:
3. A number of concerns have been raised by and to the CCG with respect to services provided by Bridgewater NHS Foundation Trust. To date business as usual contract management processes have been adopted to manage the issues however more recently this approach has not felt right. The CCG has therefore written to the Provider requesting formal action plans (which will be reviewed and discussed at the Contract Review Meeting on 14 September 2017) in relation to the following areas of concern:
Non-provision of commissioned slots/sessions within the Primary Care Out of Hours and Extended Access service
Unexpected temporary suspension/partial withdrawal of a number of services with little or no notice
Long waiting times in OCATS
Serious incident reporting processes
Cost Improvement Plans
Enhanced Care Home Support service
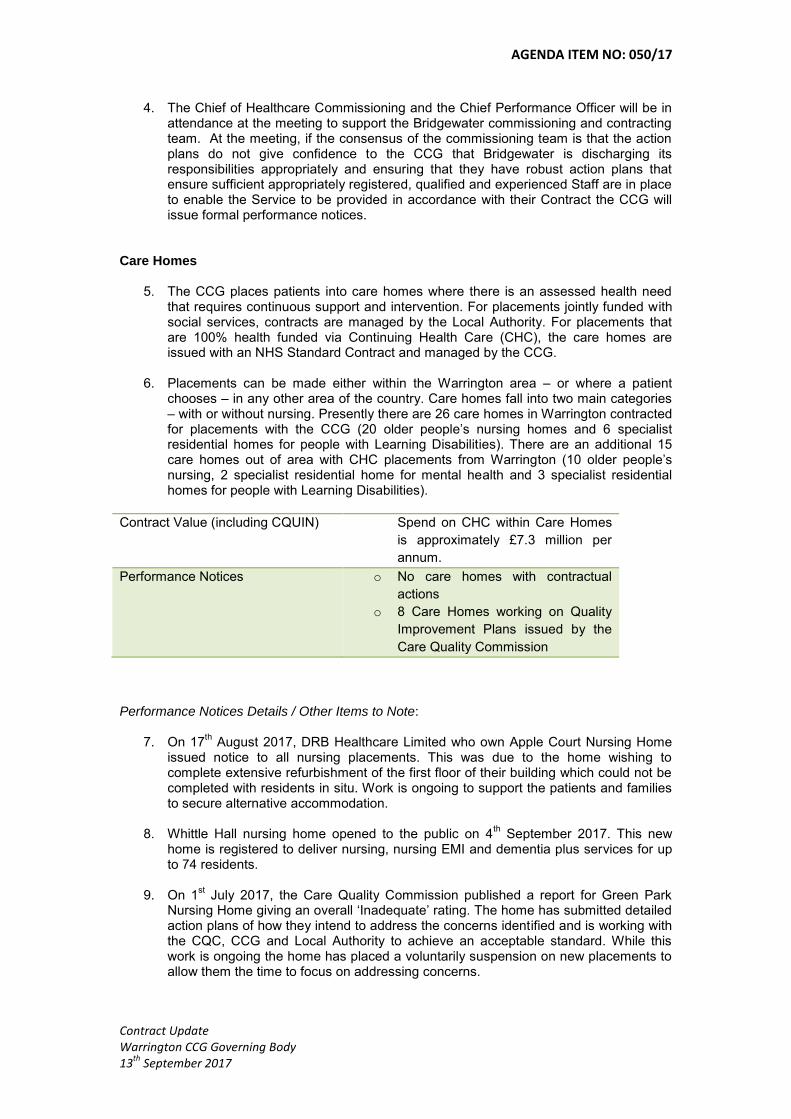
AGENDA ITEM NO: 050/17
Contract Update Warrington CCG Governing Body 13
th September 2017
4. The Chief of Healthcare Commissioning and the Chief Performance Officer will be in attendance at the meeting to support the Bridgewater commissioning and contracting team. At the meeting, if the consensus of the commissioning team is that the action plans do not give confidence to the CCG that Bridgewater is discharging its responsibilities appropriately and ensuring that they have robust action plans that ensure sufficient appropriately registered, qualified and experienced Staff are in place to enable the Service to be provided in accordance with their Contract the CCG will issue formal performance notices.
Care Homes
5. The CCG places patients into care homes where there is an assessed health need that requires continuous support and intervention. For placements jointly funded with social services, contracts are managed by the Local Authority. For placements that are 100% health funded via Continuing Health Care (CHC), the care homes are issued with an NHS Standard Contract and managed by the CCG.
6. Placements can be made either within the Warrington area – or where a patient
chooses – in any other area of the country. Care homes fall into two main categories – with or without nursing. Presently there are 26 care homes in Warrington contracted for placements with the CCG (20 older people’s nursing homes and 6 specialist residential homes for people with Learning Disabilities). There are an additional 15 care homes out of area with CHC placements from Warrington (10 older people’s nursing, 2 specialist residential home for mental health and 3 specialist residential homes for people with Learning Disabilities).
Contract Value (including CQUIN) Spend on CHC within Care Homes
is approximately £7.3 million per
annum.
Performance Notices o No care homes with contractual
actions
o 8 Care Homes working on Quality
Improvement Plans issued by the
Care Quality Commission
Performance Notices Details / Other Items to Note:
7. On 17th August 2017, DRB Healthcare Limited who own Apple Court Nursing Home
issued notice to all nursing placements. This was due to the home wishing to complete extensive refurbishment of the first floor of their building which could not be completed with residents in situ. Work is ongoing to support the patients and families to secure alternative accommodation.
8. Whittle Hall nursing home opened to the public on 4th September 2017. This new
home is registered to deliver nursing, nursing EMI and dementia plus services for up to 74 residents.
9. On 1st July 2017, the Care Quality Commission published a report for Green Park
Nursing Home giving an overall ‘Inadequate’ rating. The home has submitted detailed action plans of how they intend to address the concerns identified and is working with the CQC, CCG and Local Authority to achieve an acceptable standard. While this work is ongoing the home has placed a voluntarily suspension on new placements to allow them the time to focus on addressing concerns.
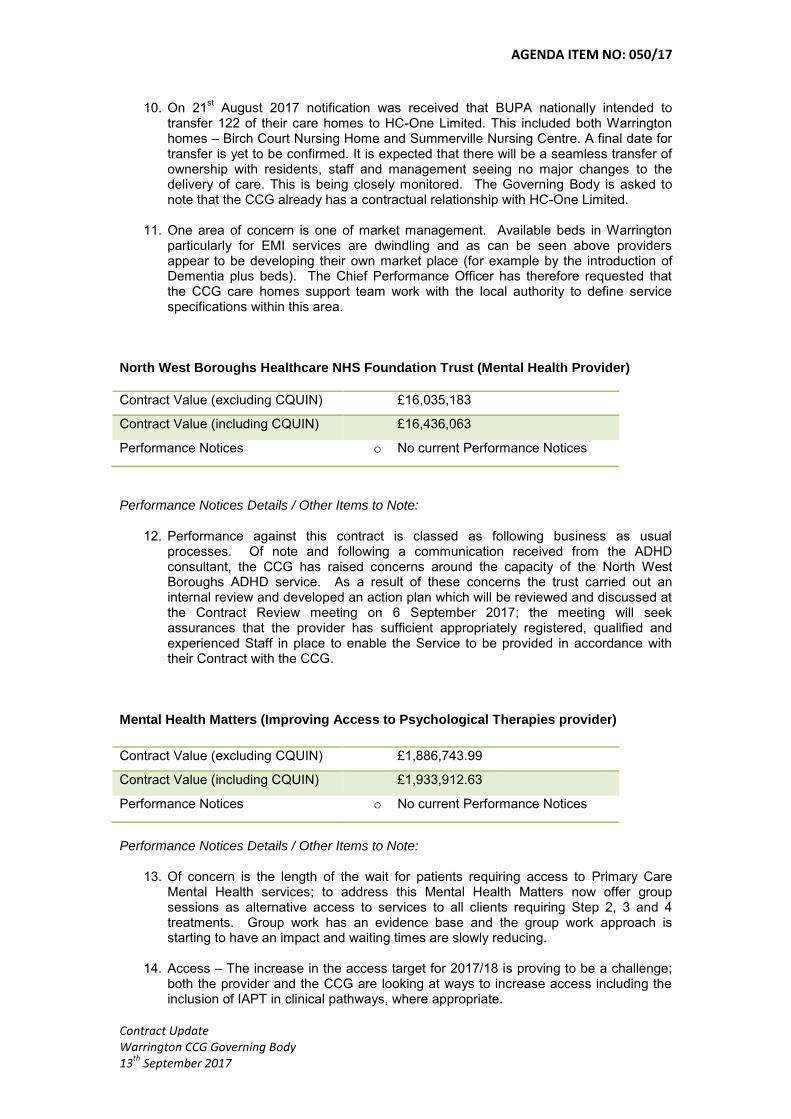
AGENDA ITEM NO: 050/17
Contract Update Warrington CCG Governing Body 13
th September 2017
10. On 21st August 2017 notification was received that BUPA nationally intended to
transfer 122 of their care homes to HC-One Limited. This included both Warrington homes – Birch Court Nursing Home and Summerville Nursing Centre. A final date for transfer is yet to be confirmed. It is expected that there will be a seamless transfer of ownership with residents, staff and management seeing no major changes to the delivery of care. This is being closely monitored. The Governing Body is asked to note that the CCG already has a contractual relationship with HC-One Limited.
11. One area of concern is one of market management. Available beds in Warrington particularly for EMI services are dwindling and as can be seen above providers appear to be developing their own market place (for example by the introduction of Dementia plus beds). The Chief Performance Officer has therefore requested that the CCG care homes support team work with the local authority to define service specifications within this area.
North West Boroughs Healthcare NHS Foundation Trust (Mental Health Provider)
Contract Value (excluding CQUIN) £16,035,183
Contract Value (including CQUIN) £16,436,063
Performance Notices o No current Performance Notices
Performance Notices Details / Other Items to Note:
12. Performance against this contract is classed as following business as usual processes. Of note and following a communication received from the ADHD consultant, the CCG has raised concerns around the capacity of the North West Boroughs ADHD service. As a result of these concerns the trust carried out an internal review and developed an action plan which will be reviewed and discussed at the Contract Review meeting on 6 September 2017; the meeting will seek assurances that the provider has sufficient appropriately registered, qualified and experienced Staff in place to enable the Service to be provided in accordance with their Contract with the CCG.
Mental Health Matters (Improving Access to Psychological Therapies provider)
Contract Value (excluding CQUIN) £1,886,743.99
Contract Value (including CQUIN) £1,933,912.63
Performance Notices o No current Performance Notices
Performance Notices Details / Other Items to Note:
13. Of concern is the length of the wait for patients requiring access to Primary Care Mental Health services; to address this Mental Health Matters now offer group sessions as alternative access to services to all clients requiring Step 2, 3 and 4 treatments. Group work has an evidence base and the group work approach is starting to have an impact and waiting times are slowly reducing.
14. Access – The increase in the access target for 2017/18 is proving to be a challenge; both the provider and the CCG are looking at ways to increase access including the inclusion of IAPT in clinical pathways, where appropriate.
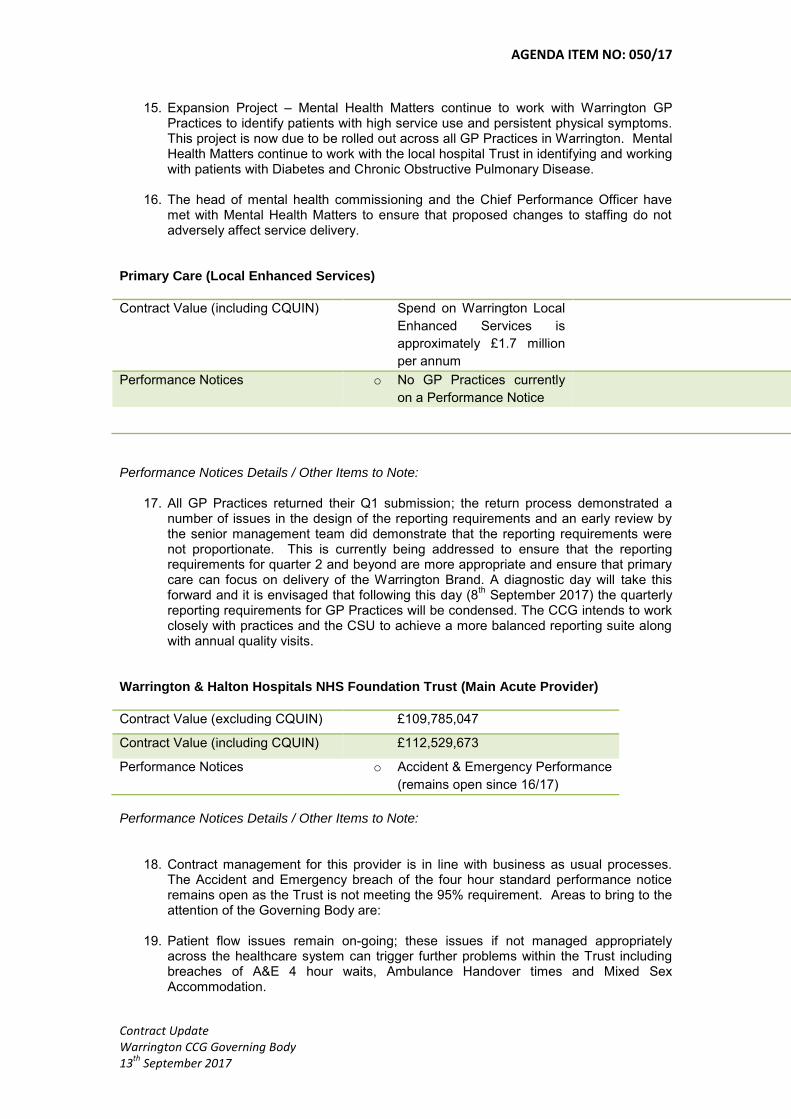
AGENDA ITEM NO: 050/17
Contract Update Warrington CCG Governing Body 13
th September 2017
15. Expansion Project – Mental Health Matters continue to work with Warrington GP Practices to identify patients with high service use and persistent physical symptoms. This project is now due to be rolled out across all GP Practices in Warrington. Mental Health Matters continue to work with the local hospital Trust in identifying and working with patients with Diabetes and Chronic Obstructive Pulmonary Disease.
16. The head of mental health commissioning and the Chief Performance Officer have met with Mental Health Matters to ensure that proposed changes to staffing do not adversely affect service delivery.
Primary Care (Local Enhanced Services)
Contract Value (including CQUIN) Spend on Warrington Local
Enhanced Services is
approximately £1.7 million
per annum
Performance Notices o No GP Practices currently
on a Performance Notice
Performance Notices Details / Other Items to Note:
17. All GP Practices returned their Q1 submission; the return process demonstrated a number of issues in the design of the reporting requirements and an early review by the senior management team did demonstrate that the reporting requirements were not proportionate. This is currently being addressed to ensure that the reporting requirements for quarter 2 and beyond are more appropriate and ensure that primary care can focus on delivery of the Warrington Brand. A diagnostic day will take this forward and it is envisaged that following this day (8
th September 2017) the quarterly
reporting requirements for GP Practices will be condensed. The CCG intends to work closely with practices and the CSU to achieve a more balanced reporting suite along with annual quality visits.
Warrington & Halton Hospitals NHS Foundation Trust (Main Acute Provider)
Contract Value (excluding CQUIN) £109,785,047
Contract Value (including CQUIN) £112,529,673
Performance Notices o Accident & Emergency Performance
(remains open since 16/17)
Performance Notices Details / Other Items to Note:
18. Contract management for this provider is in line with business as usual processes.
The Accident and Emergency breach of the four hour standard performance notice remains open as the Trust is not meeting the 95% requirement. Areas to bring to the attention of the Governing Body are:
19. Patient flow issues remain on-going; these issues if not managed appropriately across the healthcare system can trigger further problems within the Trust including breaches of A&E 4 hour waits, Ambulance Handover times and Mixed Sex Accommodation.
AGENDA ITEM NO: 050/17
Contract Update Warrington CCG Governing Body 13
th September 2017
20. The 2016/17 and 2017/19 NHS Standard Contracts introduced areas where Trusts and primary care are required to work together to ensure seamless patient care. These are more commonly known as Interface Issues. One area where the contract lead, Dr Ian Watson, supported by the quality lead and the clinical leads for urgent care is discharge summaries from secondary care to primary care. This has caused great concern [in previous years and] in particular when the Trust implemented the Lorenzo patient administration system. Through continuous development and collaborative working there has been an improvement in summaries received. The Trust as assured the CCG that it will not be sending any hand written summaries from September 2017 onwards.
21. The clinical quality focus group has a schedule of collaborative work for clinical
pathways. Most recently amended flowcharts with respect to the anaemia pathway for the management of anaemia and chronic anaemia is being finalised and will be circulated to GPs as soon as possible.
22. The CCG is awaiting formal sight of the Trust’s CQC report. The schedule session
for discussion on the report planned for 6th September 2017 was cancelled by the
Trust due to the final agreed report not being published. WRAG – Warrington Referral Assistance Gateway Specifically the Service Level Agreement with Manchester Integrated Care Gateway (MICG) provided by the Manchester CCGs for Referral Management Services
23. On 1st September the CCG received formal notice from the Manchester Health and
Care Commissioning that it was transferring the referral management services from the MICG to the Greater Manchester Shared Services hosted by Oldham CCG. The letter indicated that as part of the transfer process a review of service by the new provider was undertaken concluding that they were no longer in a position to provide services for NHS Warrington CCG (WRAG) and serving 4 months’ notice.
24. The Chief Operating Officer is therefore pursuing alternative solutions for the service
that will ensure a seamless transfer and have little or no effect on primary care. Pam Broadhead Chief Performance Officer 5
th September 2017

AGENDA ITEM NO: 051/17
Commissioning Plan Refresh 2017/19 Warrington CCG Governing Body Meeting 13 September 2017
GOVERNING BODY MEETING:
Governing Body Meeting
DATE OF MEETING:
13
th September 2017
REPORT AUTHOR AND JOB TITLE:
Linda Bennett Chief of Healthcare Commissioning
REPORT TITLE:
Commissioning Plan Refresh 2017/19
STRATEGIC OBJECTIVES:
Improve quality of services
√ Sustained financial balance
√
Build an effective and motivated whole system workforce
√ Sound governance arrangements
√
Ensure integration and joint working arrangements
√
OUTCOME REQUIRED (tick)
Approval
√ Assurance
Discussion
Information
EXECUTIVE SUMMARY
The Commissioning Plan Refresh 2017/19 reflects;
the requirements of the NHSE Operational Planning & Contracting Guidance 2017/19
the direction of travel detailed in the NHS Five Year Forward View (2014) and GP Forward View (2016) and the ambitions of the emerging Sustainability & Transformation Partnerships
locally identified priority areas including implementation of the CCG’s Primary Care Strategy intentions
the CCG’s current financial plan overview
the CCG’s intention for strategic commissioning and operational alignment with key partners while wider integration is considered and
reinforces the CCG’s focus on improving quality in its commissioned services
includes commitment to the continued development of local Accountable Care Partnership to deliver ‘new models of care’
meets the required constitutional standards
AGENDA ITEM NO: 051/17
Commissioning Plan Refresh 2017/19 Warrington CCG Governing Body Meeting 13 September 2017
RECOMMENDATIONS
The Governing Body is asked to;
Recognise the requirement for publication of a comprehensive ‘Commissioning Prospectus’ to meet the NHS England ‘Checkpoint’ schedule and facilitate development of the local Accountable Care Partnership
Approve the commissioning of work to produce the prospectus before the end of Quarter 3, 2017
Approve the ‘Commissioning Plan Refresh 2017/19’
Outline any engagement – staff, clinical, stakeholder and patient / public
-The draft document has been available on the CCG website for 3+ months - Clinical engagement via Commissioning PLT Draft to Health & Wellbeing Board 6.7.17 - Draft to WBC Commissioning Team joint plans review session 23.8.17 - WBC Health Scrutiny Committee 26.6.17 - Health Forum
Are there any conflicts of interest which may be associated with this paper?
None identified
Does this paper address any existing risks which are included on the Assurance Framework or Risk Register?
None identified
Have the following areas been considered whilst producing this report?
Yes
N/A
Equality Impact Assessment (if yes, attach to paper)
Undertaken by individual work streams
Quality Impact Assessment (if yes, attach to paper)
Undertaken by individual work streams
Regulation, legal, governance and assurance implications (reference in the report if applicable)
N/A
Procurement process (reference in the report if applicable)
N/A
Document development
Version 1.1 - 3.7.17 Version 1.2 – 20.7.17 Version 1.3 – 27.7.17 (Final)
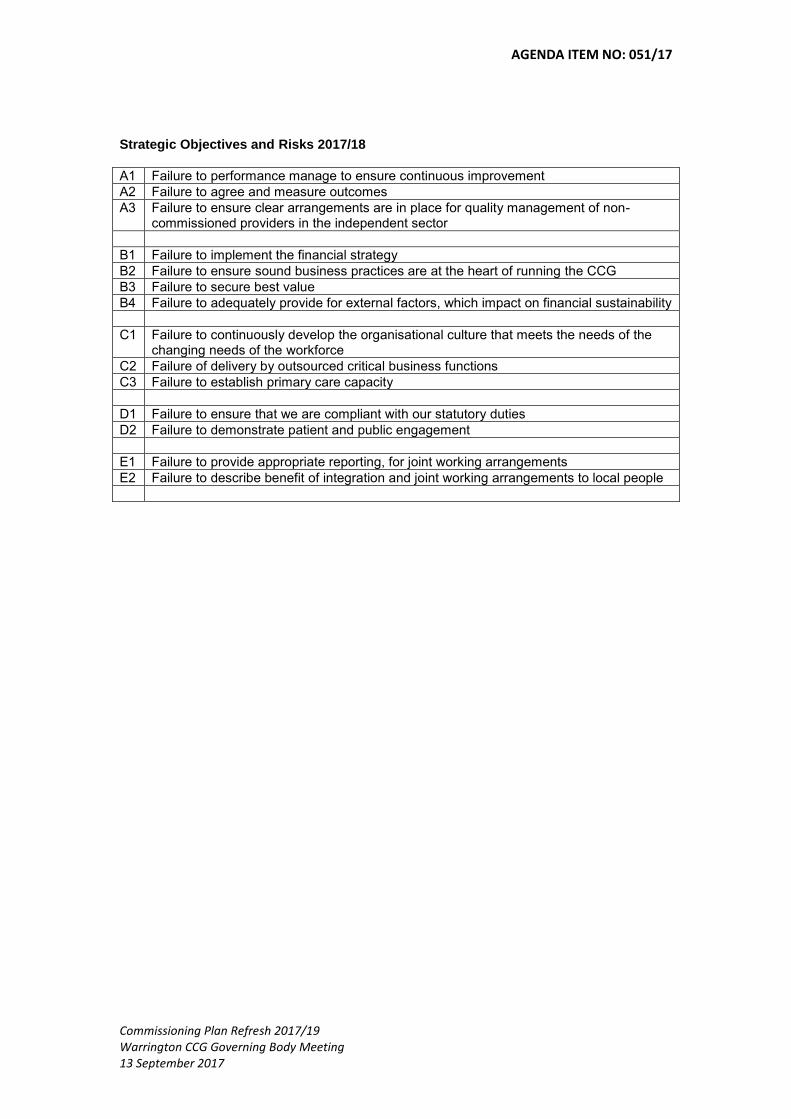
AGENDA ITEM NO: 051/17
Commissioning Plan Refresh 2017/19 Warrington CCG Governing Body Meeting 13 September 2017
Strategic Objectives and Risks 2017/18
A1 Failure to performance manage to ensure continuous improvement
A2 Failure to agree and measure outcomes
A3 Failure to ensure clear arrangements are in place for quality management of non-commissioned providers in the independent sector
B1 Failure to implement the financial strategy
B2 Failure to ensure sound business practices are at the heart of running the CCG
B3 Failure to secure best value
B4 Failure to adequately provide for external factors, which impact on financial sustainability
C1 Failure to continuously develop the organisational culture that meets the needs of the changing needs of the workforce
C2 Failure of delivery by outsourced critical business functions
C3 Failure to establish primary care capacity
D1 Failure to ensure that we are compliant with our statutory duties
D2 Failure to demonstrate patient and public engagement
E1 Failure to provide appropriate reporting, for joint working arrangements
E2 Failure to describe benefit of integration and joint working arrangements to local people

Commissioning Plan Refresh
2017/19
COMMISSIONING PLAN REFRESH
2017 – 2019
(DRAFT)
Agenda Item No 051/17
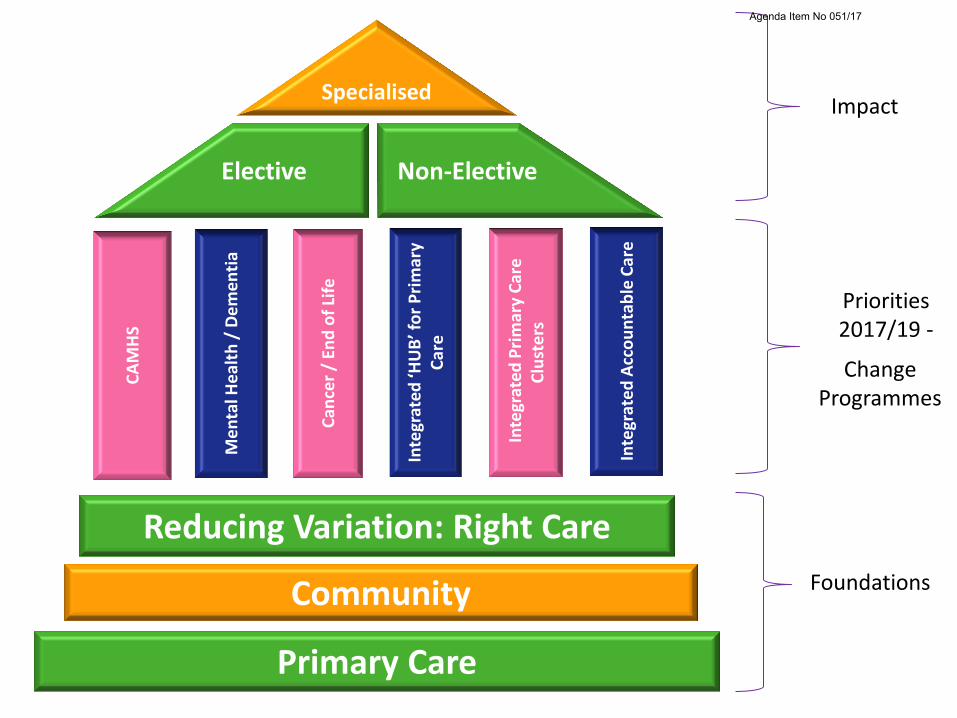
Impact
Change Programmes
Foundations
Primary Care
Community
Elective
Specialised
Non-Elective
Inte
grat
ed P
rim
ary
Car
e
Clu
ste
rs
Me
nta
l He
alth
/ D
em
en
tia
CA
MH
S
Can
cer
/ En
d o
f Li
fe
Inte
grat
ed ‘H
UB
’ fo
r P
rim
ary
Car
e
Inte
grat
ed A
cco
un
tab
le C
are
Reducing Variation: Right Care
Priorities 2017/19 -
Agenda Item No 051/17

• Review all commissioned services including access to community services, 24/7 crisis resolution and liaison
mental health services ensuring equity of access for vulnerable groups
• Continue to develop a workforce plan in partnership with CCGs in the Alliance Local Delivery System (LDS)
• Co-design new whole system service model/integrated pathways in line with the THRIVE model (new models of care)
• Further develop the joint agency approach between schools and CAMHS
• Work with NHS England to develop a joint LDS commissioning plan for provision of tier 4 beds
• Explore lead provider arrangement through a collaborative commissioning approach across the Alliance LDS
• Commission eating disorder services so that 95% of children and young people receive treatment within 4 weeks of referral for routine cases and one week for urgent cases
Impact: • Intervene early and build resilience by Improving access to achieve national
trajectories (reaching 35% by March 2020/21) • Virtual single point of access across providers including self referral access points • More effective clinical pathways (underpinned by Children and young people’s
Improving Access to Psychological Therapies (CYP IAPT), capacity and demand planning and improved patient flow (by 2018)
• Integrated pathways with Children’s services for managing and sharing risk • Achieve alignment of provision through integrated commissioning arrangements • Reduce substantially the use of specialist inpatient beds for children with an eating
disorder
Children and young people’s mental health (CAMHS)
Agenda Item No 051/17

• Commission additional and expanded specialist perinatal community mental health services to increase access to more women within Warrington
• Additional psychological therapies will be commissioned to deliver treatments to support people with physical and mental health problems
• The CCG will continue to commission Early Intervention Services to ensure that more than 50% of people experiencing a first episode of psychosis start treatment within 2 weeks of referral
• Working with partners, the CCG will contribute fully to the local ‘Multi-Agency Suicide Prevention Plan’ to reduce suicides
• Develop effective 24/7 crisis response and home treatment teams as alternatives to acute admissions • Continue to reduce non-specialist mental health Out of Area (OOA) placements with the aim of elimination
by 2020/21 • Additional screening and physical health interventions will be commissioned for people with Severe Mental
Illness (SMI) on GP registers
• Working with acute providers to meet the ‘core 24’ standard for mental health liaison • Work with partners to increase access to placement support for people with SMI • The CCG will maintain and improve our dementia diagnosis rate • Use the ‘Local Digital Roadmap’ to facilitate improvements in data quality, transparency
and increase digital maturity in mental health services • In line with recommendations in “Building the Right support” maintain the achieved
reduction in the acute inpatient bed base (50% prior to March 2019). • Ensure that the revised and reissued care policy treatment plans and guidance remain
updated in line with published guidance • Maintain the dynamic support database in place across the footprint
Mental Health, Learning Disability & Dementia
Agenda Item No 051/17
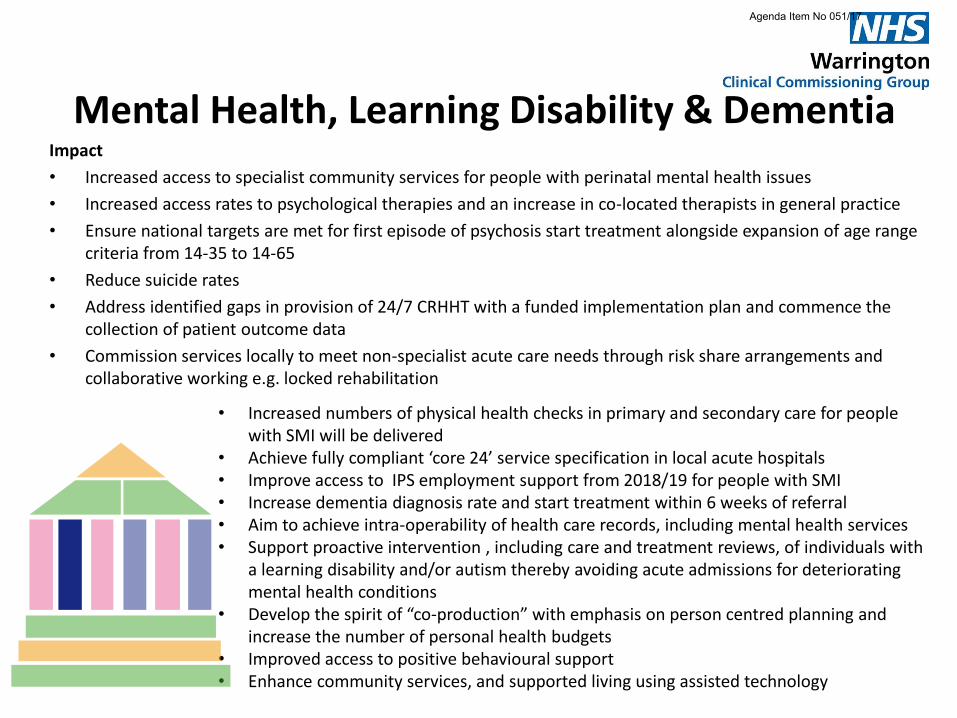
Mental Health, Learning Disability & Dementia Impact
• Increased access to specialist community services for people with perinatal mental health issues
• Increased access rates to psychological therapies and an increase in co-located therapists in general practice
• Ensure national targets are met for first episode of psychosis start treatment alongside expansion of age range criteria from 14-35 to 14-65
• Reduce suicide rates
• Address identified gaps in provision of 24/7 CRHHT with a funded implementation plan and commence the collection of patient outcome data
• Commission services locally to meet non-specialist acute care needs through risk share arrangements and collaborative working e.g. locked rehabilitation
• Increased numbers of physical health checks in primary and secondary care for people with SMI will be delivered
• Achieve fully compliant ‘core 24’ service specification in local acute hospitals • Improve access to IPS employment support from 2018/19 for people with SMI • Increase dementia diagnosis rate and start treatment within 6 weeks of referral • Aim to achieve intra-operability of health care records, including mental health services • Support proactive intervention , including care and treatment reviews, of individuals with
a learning disability and/or autism thereby avoiding acute admissions for deteriorating mental health conditions
• Develop the spirit of “co-production” with emphasis on person centred planning and increase the number of personal health budgets
• Improved access to positive behavioural support • Enhance community services, and supported living using assisted technology
Agenda Item No 051/17
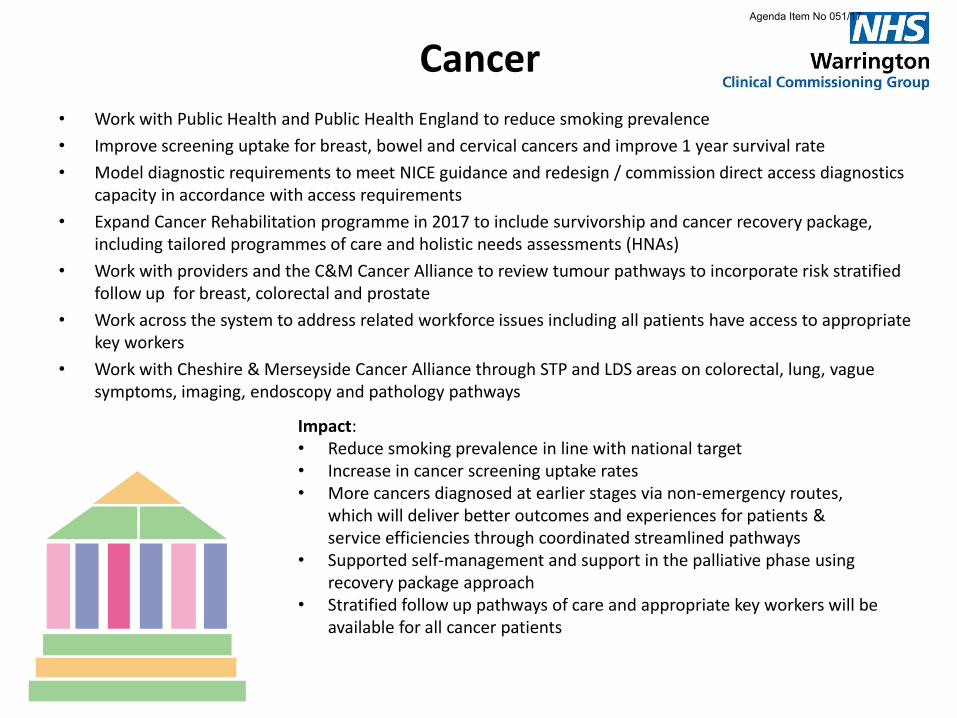
Cancer • Work with Public Health and Public Health England to reduce smoking prevalence
• Improve screening uptake for breast, bowel and cervical cancers and improve 1 year survival rate
• Model diagnostic requirements to meet NICE guidance and redesign / commission direct access diagnostics capacity in accordance with access requirements
• Expand Cancer Rehabilitation programme in 2017 to include survivorship and cancer recovery package, including tailored programmes of care and holistic needs assessments (HNAs)
• Work with providers and the C&M Cancer Alliance to review tumour pathways to incorporate risk stratified follow up for breast, colorectal and prostate
• Work across the system to address related workforce issues including all patients have access to appropriate key workers
• Work with Cheshire & Merseyside Cancer Alliance through STP and LDS areas on colorectal, lung, vague symptoms, imaging, endoscopy and pathology pathways
Impact: • Reduce smoking prevalence in line with national target • Increase in cancer screening uptake rates • More cancers diagnosed at earlier stages via non-emergency routes,
which will deliver better outcomes and experiences for patients & service efficiencies through coordinated streamlined pathways
• Supported self-management and support in the palliative phase using recovery package approach
• Stratified follow up pathways of care and appropriate key workers will be available for all cancer patients
Agenda Item No 051/17
End of life • Scope existing service provision working with providers and patients to co-design optimum pathways of care
for general and specialist palliative care and end of life care
• Working with providers ensure people approaching end of life are offered timely personalised support for all their needs, including access to rehabilitation support services to maximise their independence and social participation for as long as possible
• Working with providers embed consistent quality use of newly developed palliative and end of life care documentation, for example Individual Plan of Care, Community Ceiling of Care, Advanced Care Plans and unified Do Not Attempt Resuscitation
• Support commissioning of education programmes for health, social and third sector to improve skill mix and have competent staff that are empowered to deliver quality care for people approaching end of life and their families/carers.
• Support implementation of Electronic Palliative Co-ordinated Care Systems (EPaCCs) across all providers
• Working with providers to achieve the Ambitions for Palliative Care, a framework for quality care 2015-2020
Impact: • Each person is seen as an individual and asked what matters most to them • Each person gets fair access to good quality care • Each person has maximised comfort and wellbeing with care regularly reviewed by
competent staff, who always offer compassionate quality care • Care is coordinated for all addressing individual needs and care plan wishes, with
access 24/7 • Each community is prepared to help and through engagement prepared to have
conversations about death and dying • To reduce inappropriate admissions to hospital at end of life through coordinated care
for all
Agenda Item No 051/17
Integrated ‘HUB’ for Out of Hours Primary Care
• Implementation of integrated Primary Care Out of Hours Hub incorporating extended GP access, pharmacy, Single Point of Access (SPA) and GP Out Of Hours services
• Working with North West Ambulance Service (NWAS) developing a virtual clinical hub / Clinical Advice Service (CAS)
• Developing mechanisms for transition of care between core/hours and out of hours services • Developing booking and communication systems which are robust • Developing working relationships between services working in similar timeframes including Paediatric
Acute Response Team (PART), Children’s Community Respiratory Team (CCREST), Emergency dental services, for delivery of care in the appropriate sector
Impact: • Reduce presentations to A&E for people with a primary care need • Increase choice for people in terms of time and location of care • Reduce pressure on primary care during core hours through
provision of increased capacity
Agenda Item No 051/17
Integrated Primary Care Clusters Working collaboratively across Warrington to develop general practice at scale, delivering new care
models that will ensure system integration of providers who will take responsibility for delivering a range of primary, community, mental health and hospital services for our local population.
New care model will offer provision of care to a defined population of between 30,000 and 50,000.
Improve co-ordination of services and move care out of hospital where appropriate
Develop the primary care medical and non-medical workforce by having different staff groups to deliver care, e.g. Clinical Pharmacists, GP Assistants, Physician Associates and Mental Health Therapists
Using Primary Care Infrastructure Funding we will implement the priorities identified in the CCG Estates Strategy
Demonstrate increased patient satisfaction by improving access to services with a combined focus on personalised care to improve population health and wellbeing outcomes.
Impact: • Increase accessibility of Primary Care Services whilst reducing acute activity. • Reduce GP Practice workload by alignment of wider services around the
registered patient list, and working towards sustaining Primary Care • Fit for purpose Primary Care Estates and technology • Integrated workforce to focus on population needs and provide care closer to
home • Improve the wellbeing and quality of life for patients and for the primary care
workforce
Agenda Item No 051/17
Accountable Care Partnership (ACP): The Model
• Scope & Scale: Health and Social Care services provided in Warrington for Warrington people
• Model: A system of delivery which is arranged via both horizontal and vertical integration
• Development of a Commissioning Prospectus that describes the case for change,
essential success factors and parameters of the model • New model of care may require new business models e.g. contracts
Impact • Supports care pathways and activity for the services in scope
within existing resource • Address population health management • Supports patient choice for place of care • Enables delegated decision making with regards to primary
care and specialised services • Offers single regulatory approach NHSE and NHSI • Offers the ability to redeploy attributable staff and related
funding from NHSE and NHSI to support ACP • Facilitates access to the development programme for “fast
followers”
Agenda Item No 051/17

Accountable Care Partnership: The Model
Horizontal
• Integration between services which are related
• Brings increased resilience
• Increased capability
• Economies of scale
Horizontal integration
Primary
Care Community Mental Health
Social Care
Prevention Hubs Outpatient Medical
Mechanisms for horizontal integration Primary Care Home Clusters Integrated out of hospital services Contractual remedy NHS standard contract with link KPIs Proposed MCP contract model
Agenda Item No 051/17

Accountable Care Partnership: The Model
Vertical integration
Acute
•Surgical Pathways
•Chronic and Acute ACS
•AEC pathways
•Comprehensive Geriatric Assessment
Community
•Tier 2 surgical
•Chronic disease management
•Step Up Nursing
•Early supported discharge
Mental Health
•Liaison Psychiatry
•Personality disorder service
•Outreach
Social Care
•Respite
•Step up
•ESD
Primary Care
•Chronic disease management for ACS conditions
•AEC pathways initiation
•Medical cover for proactive care and ESD
Mechanisms for vertical integration • Mergers and
Acquisitions • Lead contractor with
options arrangements • PACS model contract
development to start soon
Vertical • Integration of
different service within a supply chain under one organisation
• Resolves the
hold up problem
• Allows
maximising efficiency along the value chain
Agenda Item No 051/17
Control Programmes
Diabetes
Enhanced Care Home
Support
Patient Flow
Initiatives
Vanguards: Women’s & Children’s
Neuro-Vanguard
Right Care Programmes
Diabetes
Enhanced Care Home support
Patient flow initiatives
Women’s & children’s Vanguard
Neuro-Vanguard
Agenda Item No 051/17

Diabetes Care • The CCG appointed dedicated clinical lead for Diabetes continues to work with primary care on the
development of pathways
• National Diabetes Audit for 2015/16 audit shows an increase in the number of patients on the diabetic register who have received the eight care processes but there is significant variation within the system
• A Tier 3 service for weight management has been commissioned
• The CCG has successfully secured funding for the 4 available bids from NHS England National Diabetes Transformation Fund (2017/18)
• Working with public health and the STP regarding a Phase 3 bid for the National Diabetes Prevention Programme (NDPP)
• Both National and local predictions confirm increased levels of obesity and type 2 diabetes in the population
Impact • Provide high quality, consistent care for people with diabetes • Reduce variation in the care received by people with diabetes • Reduce complications associated with diabetes • Improve confidence levels to self-manage care • Reduce number of people progressing to a diabetes diagnosis • Improve aspects of care demonstrated to be weaker within the system
Diabetes
Enhanced Care
Home support
Patient flow
initiatives
Women’s & children’s
Neuro-Vanguard
Neuro-
Vanguard
Agenda Item No 051/17
Enhanced Care Home Support Service (ECHSS) • Deliver a proactive model of care across all care homes through a multi-disciplinary approach consisting of
GPs, Nurses and Pharmacists, supported where possible through telehealth
• MDT meetings in each café home
• Enhances the care currently delivered by a residents registered GP, thus The outcome for residents being they will be looked after well for their remaining days in their own home without the need to be admitted into an acute setting which is not the place for them
• Develop clinical pathways to aid care home staff in managing their residents and to access the most appropriate route to manage residents’ conditions
• Provide direct access fro the homes to the ECHSS through a dedicated help-line for triage, treatment or onward referral
• Develop greater integration across different staff disciplines, other services and development of the MDT’s within each home
Impact • Creates capacity in general practice, • Supports the patient to live as well as can be during their last 12-
18 months of life through robust advanced care planning • To reduce avoidable attendance and admission to A&E by
provision of educated and empowered care home staff • Reduce length of stay through supported discharge process • Supports residents to achieve preferred place of death • Increases completion of comprehensive care plans
Diabetes
Enhanced Care
Home support
Patient flow
initiatives
Women’s & children’s
Neuro-Vanguard
Neuro-
Vanguard
Agenda Item No 051/17
Patient flow initiatives: An holistic approach to patient flow
• The community based Paediatric Acute Response Team (PART)
• Out of Hospital Services (step up and step down care)
• Ambulatory Emergency Care providing same day treatment for patients who would have otherwise been admitted for 1-3 days
• Acute Visiting Service reducing conveyance to hospital via ambulance reducing subsequent admission
• Clinical Advice Service reducing conveyance by ambulance and attendance for patients accessing 999/111 services by increasing the number of clinical conversations
• Crisis Care within the CAMHS local transformation plan intends to reduce unnecessary admissions and reduce length of stay
• RightCare commissioning for value
• Adopting new care models - Vanguards
Diabetes
Enhanced Care
Home support
Patient flow
initiatives
Women’s & children’s
Neuro-Vanguard
Agenda Item No 051/17
Patient flow initiatives: Ambulatory Emergency Care
Ambulatory Emergency Care (AEC) or ‘same day emergency care’ is a whole system approach that includes both primary and secondary care to ensure that, patients who are assessed as appropriate for AEC, are diagnosed and treated on the same day
• AEC Service went live in April 2016
• With support from the Ambulatory Emergency Care Network the service was embedded over the summer months
• Continue to refine the patient cohort to ensure only those patients who would otherwise have been admitted are seen and treated in the service
• Continue to work to refine and identify effective measures of success for the service
• Work towards a detailed and robust demand and capacity model for the next 3 years
• Continue to refine the financial value for the service delivering value for money and a sustainable future
Impact: • Reduced admissions for identified patient group • Improved quality of care offering same day treatment • Improved patient journey • A sustainable robust service offering high quality care and best
practice pathways
Diabetes
Enhanced Care
Home support
Patient flow
initiatives
Women’s & children’s
Neuro-Vanguard
Agenda Item No 051/17

Patient flow initiatives: Frailty
The challenge: To provide safe, compassionate care for Frail Older people using an integrated whole system pathway to ensure people live independently for longer.
• Develop and implement effective screening and assessment using recognised tools identifying demand
• Delivering an acute Frailty Unit ensures that where acute admission is unavoidable, patients are cared for by an MDT with a focus on short stay and safe discharge back to a community setting
• Working towards a seamless pathway across the health and social care system.
• The health and social care system is able to respond in a timely and targeted way to changes in demand targeting resources and utilising skills and expertise across traditional organisational boundaries
Impact: • Directing our most vulnerable patients to the most appropriate care
setting • Acute admissions for our frail and elderly population do not increase • Reduced LOS in an acute setting for patients • Improved outcomes for patients • Reduced risk of deconditioning whilst in an acute setting
Diabetes
Enhanced Care
Home support
Patient flow
initiatives
Women’s & children’s
Neuro-Vanguard
Agenda Item No 051/17

Patient flow initiatives: Primary Care Streaming
Upon entering the emergency department, patients will be streamed by an experienced clinician to the most appropriate service. One of these streams will be primary care.
• Deliver a re-design of the existing estate to accommodate new ways of working
• Develop a robust capacity and demand model ensuring the new space is fit for purpose and sustainable
• Work towards a refined value for this patient group ensuring effective use of resources
• Agree patient pathways from the point of arrival for this patient group
Impact:
• Reduced pressure within the main emergency department
• Improved performance against the 4 hour target
• More appropriate care
• Improved patients and staff experience
Diabetes
Enhanced Care
Home support
Patient flow
initiatives
Women’s & children’s
Neuro-Vanguard
Agenda Item No 051/17
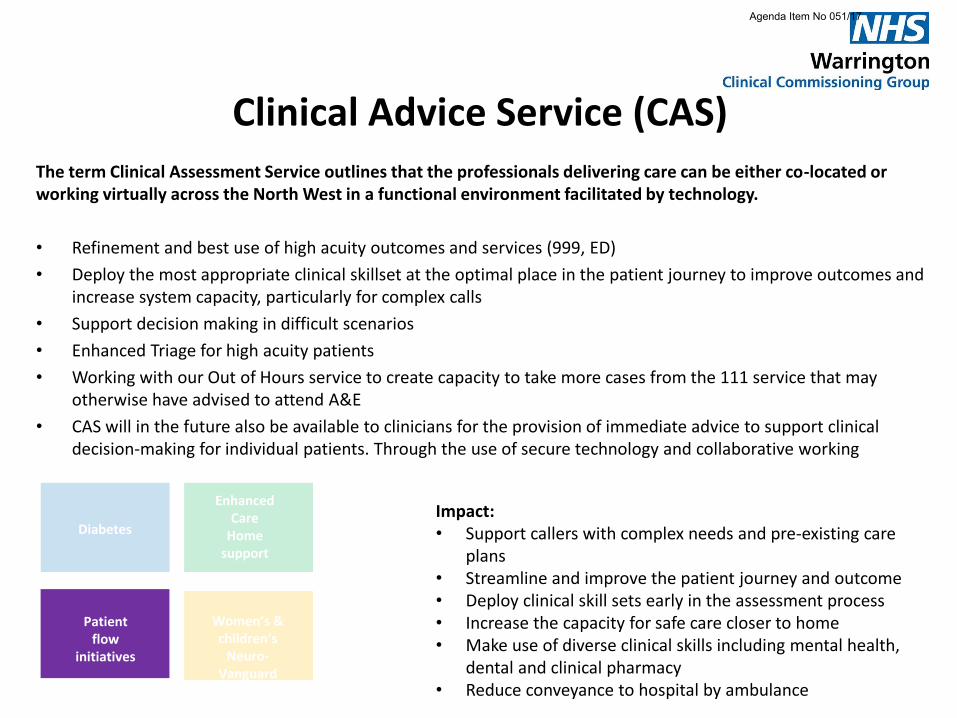
Clinical Advice Service (CAS) The term Clinical Assessment Service outlines that the professionals delivering care can be either co-located or working virtually across the North West in a functional environment facilitated by technology.
• Refinement and best use of high acuity outcomes and services (999, ED)
• Deploy the most appropriate clinical skillset at the optimal place in the patient journey to improve outcomes and increase system capacity, particularly for complex calls
• Support decision making in difficult scenarios
• Enhanced Triage for high acuity patients
• Working with our Out of Hours service to create capacity to take more cases from the 111 service that may otherwise have advised to attend A&E
• CAS will in the future also be available to clinicians for the provision of immediate advice to support clinical decision-making for individual patients. Through the use of secure technology and collaborative working
Impact: • Support callers with complex needs and pre-existing care
plans • Streamline and improve the patient journey and outcome • Deploy clinical skill sets early in the assessment process • Increase the capacity for safe care closer to home • Make use of diverse clinical skills including mental health,
dental and clinical pharmacy • Reduce conveyance to hospital by ambulance
Diabetes
Enhanced Care
Home support
Patient flow
initiatives
Women’s & children’s
Neuro-Vanguard
Agenda Item No 051/17
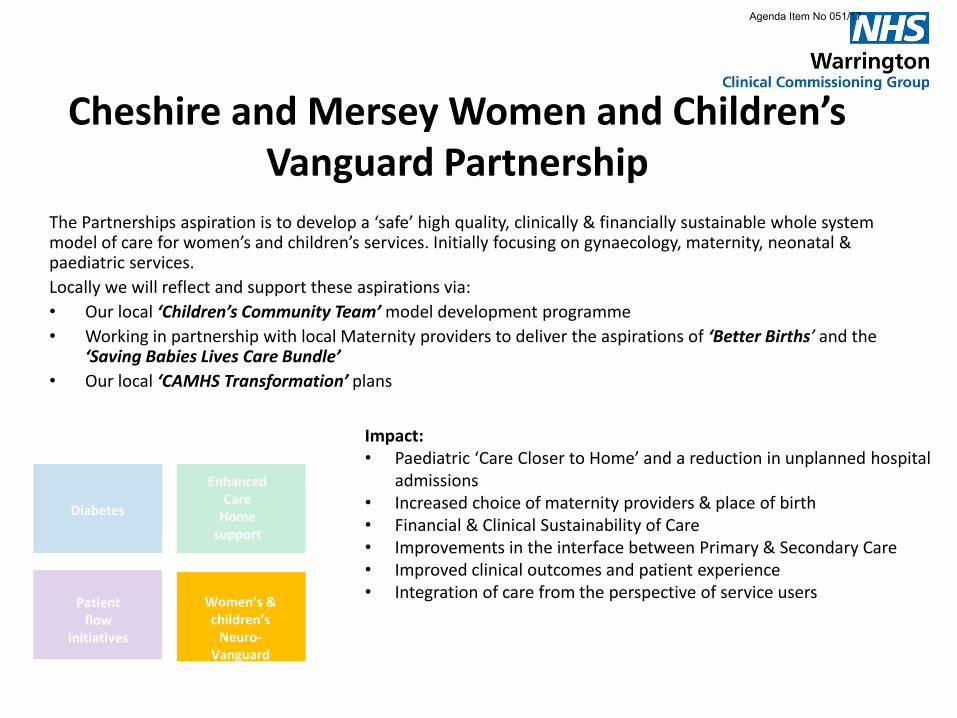
Cheshire and Mersey Women and Children’s Vanguard Partnership
The Partnerships aspiration is to develop a ‘safe’ high quality, clinically & financially sustainable whole system model of care for women’s and children’s services. Initially focusing on gynaecology, maternity, neonatal & paediatric services.
Locally we will reflect and support these aspirations via:
• Our local ‘Children’s Community Team’ model development programme
• Working in partnership with local Maternity providers to deliver the aspirations of ‘Better Births’ and the ‘Saving Babies Lives Care Bundle’
• Our local ‘CAMHS Transformation’ plans
Impact: • Paediatric ‘Care Closer to Home’ and a reduction in unplanned hospital
admissions • Increased choice of maternity providers & place of birth • Financial & Clinical Sustainability of Care • Improvements in the interface between Primary & Secondary Care • Improved clinical outcomes and patient experience • Integration of care from the perspective of service users
Diabetes
Enhanced Care
Home support
Patient flow
initiatives
Women’s & children’s
Neuro-Vanguard
Agenda Item No 051/17
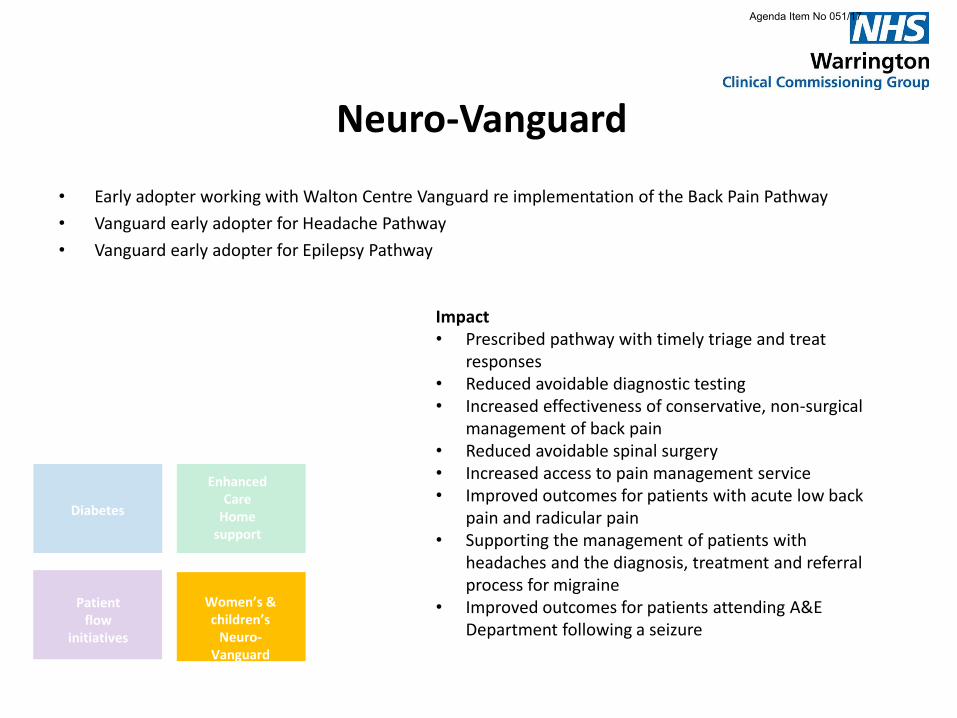
Neuro-Vanguard
• Early adopter working with Walton Centre Vanguard re implementation of the Back Pain Pathway
• Vanguard early adopter for Headache Pathway
• Vanguard early adopter for Epilepsy Pathway
Impact • Prescribed pathway with timely triage and treat
responses • Reduced avoidable diagnostic testing • Increased effectiveness of conservative, non-surgical
management of back pain • Reduced avoidable spinal surgery • Increased access to pain management service • Improved outcomes for patients with acute low back
pain and radicular pain • Supporting the management of patients with
headaches and the diagnosis, treatment and referral process for migraine
• Improved outcomes for patients attending A&E Department following a seizure
Diabetes
Enhanced Care
Home support
Patient flow
initiatives
Women’s & children’s
Neuro-Vanguard
Agenda Item No 051/17
Foundations Substantive work streams supporting the
CCGs overall strategy
Primary Care
Community
Reducing Variation: Right Care
Agenda Item No 051/17

RightCare: Gastro-Intestinal
• A review of gastro-intestinal services across Warrington, based on the NHS Right Care Pack, with a view to enhancing the care provided to the people of Warrington through appropriate care pathways with a focus on diagnostics, endoscopy, prescribing cholecystectomy and prevention of alcoholic liver disease
• Working with primary and secondary care, public health and medicines management to review and develop optimum pathways of care
• Work with Public Health to raise awareness if alcohol harm
Impact
• Improved protocols and pathways to support best practice diagnostic testing
• Reduction in less invasive diagnostic procedures supported through appropriate pathways / work up of patients
• Improved awareness / education campaigns in relation to consumption of alcohol
• Long term aim of reduction in alcoholic liver disease and other associated health issues
Agenda Item No 051/17
RightCare: Trauma & Orthopaedics
Using right care methodology to identify areas of focus where there is opportunity to improve Quality, value and outcomes for patients.
Use additional business intelligence for the focus areas to understand trends and opportunities for improvement
Agree key improvements for each focus area and implement in a phased approach
Maximise where possible the resources and experience of system partners aligning services where possible to ensure improvement patient experience
Impact: • Reduced variation against our comparator CCG areas • Improved Patient experience • Reduction in avoidable acute activity • Improved pathways and consistency in condition
management
Agenda Item No 051/17
RightCare: Neurology
• Early adopter working with Walton Centre Vanguard for implementation of the ‘Back Pain Pathway’
• Vanguard early adopter for Headache Pathway
• Vanguard early adopter for Epilepsy Pathway
Impact • Prescribed pathway with timely triage and treat responses • Reduced avoidable diagnostic testing • Increased effectiveness of conservative, non-surgical management
of back pain • Reduced avoidable spinal surgery • Increased access to pain management service • Improved outcomes for patients with acute low back pain and
radicular pain • Supporting the management of patients with headaches and the
diagnosis, treatment and referral process for migraine • Improved outcomes for patients attending A&E Department
following a seizure
Agenda Item No 051/17
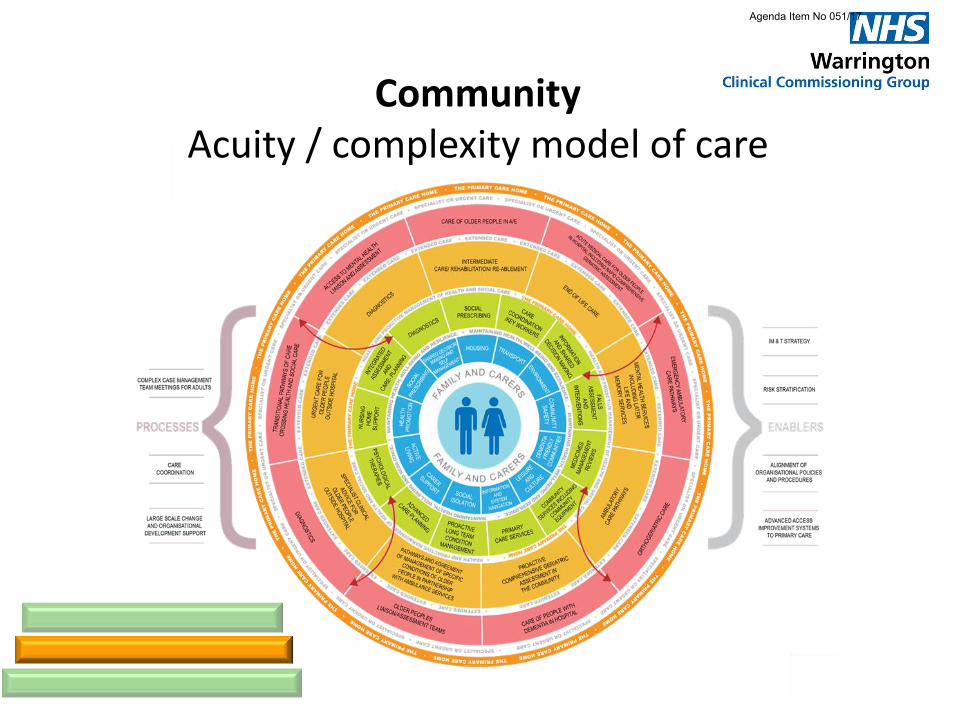
Community Acuity / complexity model of care
Agenda Item No 051/17
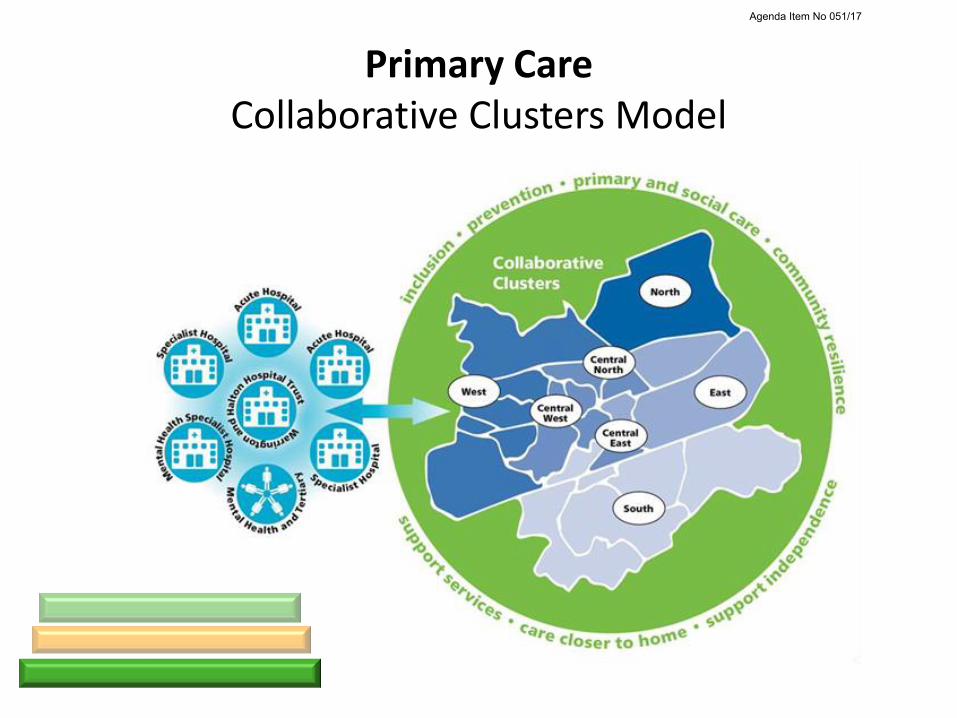
Primary Care Collaborative Clusters Model
Agenda Item No 051/17
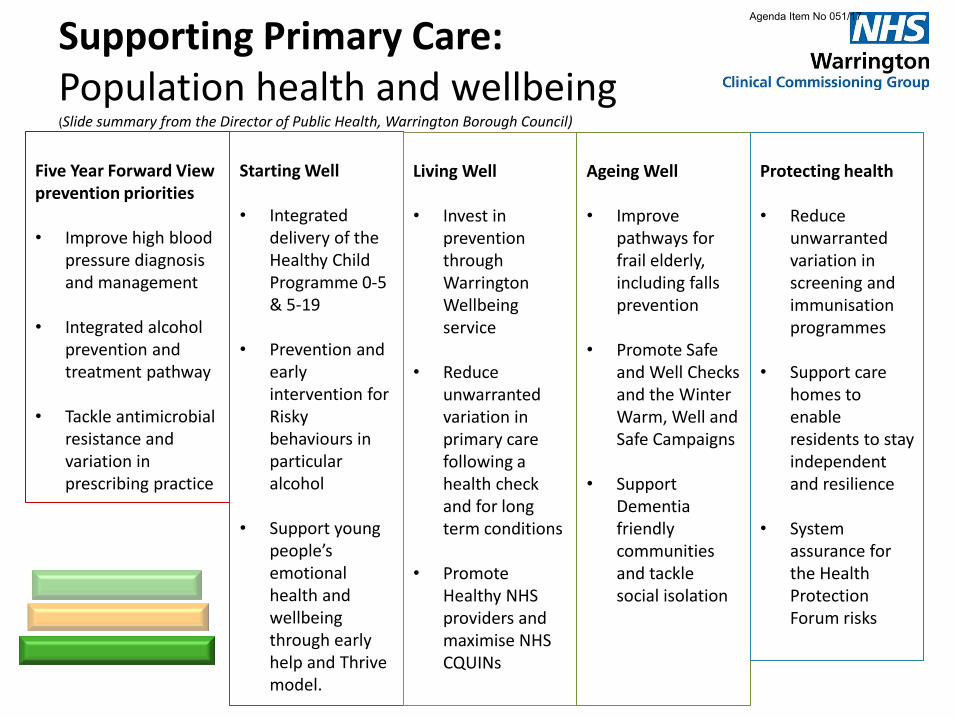
Supporting Primary Care: Population health and wellbeing (Slide summary from the Director of Public Health, Warrington Borough Council)
Five Year Forward View prevention priorities • Improve high blood
pressure diagnosis and management
• Integrated alcohol
prevention and treatment pathway
• Tackle antimicrobial
resistance and variation in prescribing practice
Starting Well • Integrated
delivery of the Healthy Child Programme 0-5 & 5-19
• Prevention and early intervention for Risky behaviours in particular alcohol
• Support young people’s emotional health and wellbeing through early help and Thrive model.
Living Well • Invest in
prevention through Warrington Wellbeing service
• Reduce
unwarranted variation in primary care following a health check and for long term conditions
• Promote Healthy NHS providers and maximise NHS CQUINs
Ageing Well • Improve
pathways for frail elderly, including falls prevention
• Promote Safe
and Well Checks and the Winter Warm, Well and Safe Campaigns
• Support Dementia friendly communities and tackle social isolation
Protecting health • Reduce
unwarranted variation in screening and immunisation programmes
• Support care
homes to enable residents to stay independent and resilience
• System
assurance for the Health Protection Forum risks
Agenda Item No 051/17
Commissioning Plan Refresh
2017/19
Key documents
Publications Gateway Reference: 05829 ‒ NHS Operational Planning and Contracting
Guidance (2017- 2019) ‒ Technical Guidance for NHS planning 2017/18 and
2018/19 (Publications Gateway Reference: 05829)
Agenda Item No 051/17
AGENDA ITEM NO: 052/17
Joint Committee Terms of Reference Warrington CCG Governing Body Meeting 13
th September 2017
GOVERNING BODY MEETING:
Governing Body Meeting
DATE OF MEETING:
13
th September 2017
REPORT AUTHOR AND JOB TITLE:
Dr Andrew Davies, Clinical Chief Officer
REPORT TITLE:
Terms of Reference for Joint Committee of NHS Halton CCG; NHS Knowsley CCG; NHS St Helens CCG and NHS Warrington CCG
STRATEGIC OBJECTIVES:
Please tick which strategic objectives the paper relates to
Improve quality of services
Sustained financial balance
Build an effective and motivated whole system workforce
Sound governance arrangements
√
Ensure integration and joint working arrangements
√
OUTCOME REQUIRED (tick)
Approval
√
Assurance
√
Discussion
Information
EXECUTIVE SUMMARY
The Five Year Forward View footprints were established in accordance with the NHS Shared Planning Guidance requirements 2015/16 which required every health and care system to come together to create their own ambitious local blueprint for accelerating implementation of the NHS Five Year Forward View. In Cheshire and Merseyside it was agreed that within the overall footprint there would be three Local Delivery Systems (LDS) - Alliance, Cheshire & Wirral, and North Mersey. The Alliance LDS includes the 4 CCGs of NHS Halton CCG, NHS Knowsley CCG, NHS St. Helens CCG and NHS Warrington CCG. The CCGs have agreed to establish and constitute a Joint Committee with these terms of reference to be known as the Alliance CCGs Joint Committee.
RECOMMENDATIONS
The Governing Body as asked to approve the amended Terms of Reference to establish a joint commissioning committee.
AGENDA ITEM NO: 052/17
Joint Committee Terms of Reference Warrington CCG Governing Body Meeting 13
th September 2017
Outline any engagement – staff, clinical, stakeholder and patient / public
Not Applicable
Are there any conflicts of interest which may be associated with this paper?
No Known Conflict of interests known.
Does this paper address any existing risks which are included on the Assurance Framework or Risk Register?
B2, B4, D1, E1
Have the following areas been considered whilst producing this report?
Yes
N/A
Equality Impact Assessment (if yes, attach to paper)
√
Quality Impact Assessment (if yes, attach to paper)
√
Regulation, legal, governance and assurance implications (reference in the report if applicable)
√
Procurement process (reference in the report if applicable)
√
Document development
Has this document been presented to any other Committee or Forum? If yes, please list which meeting, date and outcome of presentation
Version history is within terms of reference as developed by the working group delegated to undertake the work on 11
th May 2016 by the Governing Body. The latest
amendments are highlighted in yellow. The TOR working group involved the Clinical Chief Officer of each of the CCGs, governance leads, finance director and Chairs were available.
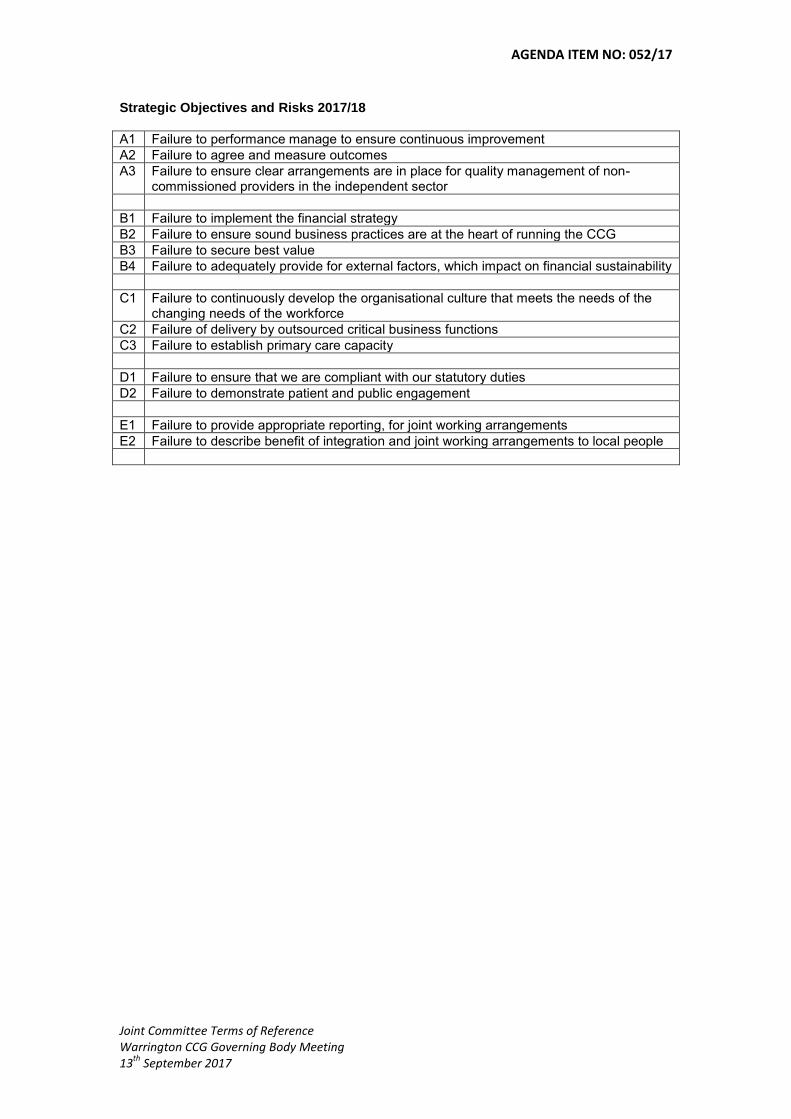
AGENDA ITEM NO: 052/17
Joint Committee Terms of Reference Warrington CCG Governing Body Meeting 13
th September 2017
Strategic Objectives and Risks 2017/18
A1 Failure to performance manage to ensure continuous improvement
A2 Failure to agree and measure outcomes
A3 Failure to ensure clear arrangements are in place for quality management of non-commissioned providers in the independent sector
B1 Failure to implement the financial strategy
B2 Failure to ensure sound business practices are at the heart of running the CCG
B3 Failure to secure best value
B4 Failure to adequately provide for external factors, which impact on financial sustainability
C1 Failure to continuously develop the organisational culture that meets the needs of the changing needs of the workforce
C2 Failure of delivery by outsourced critical business functions
C3 Failure to establish primary care capacity
D1 Failure to ensure that we are compliant with our statutory duties
D2 Failure to demonstrate patient and public engagement
E1 Failure to provide appropriate reporting, for joint working arrangements
E2 Failure to describe benefit of integration and joint working arrangements to local people
Agenda Item No: 052/17
Halton Clinical Commissioning Group Knowsley Clinical Commissioning Group St Helens Clinical Commissioning Group
Warrington Clinical Commissioning Group
Title Terms of Reference for Joint Committee of NHS Halton CCG; NHS Knowsley CCG; NHS St Helens CCG and MHS Warrington CCG
Authors Associate Director, Corporate Governance – NHS St Helens CCG Head of Governance NHS Knowsley CCG
Target Audience CCG Governing Bodies
Date of Issue
Description Terms of Reference to support establishment of Joint Committee, to be known as the Alliance Joint Committee (AJC).
Approved by
Document History
Date Version Author Notes
09/07/17 0.1 Angela Delea First draft for review by CCG Governance Leads
28/07/17 0.2 Angela Delea Draft for review by CEOs prior to approval by CCG Governing Bodies
10/08/17 0.3 Angela Delea Revisions from CCGs following CEO discussions, and guidance from NHSE re: joint committees.
01/09/17 0.4 Dianne Johnson Revisions following review and developments re NM JC and S&O Hospitals Trust
04/09/17 0.5 Angela Delea Reviews following telcon with CEOs

Agenda Item No: 052/17
Halton Clinical Commissioning Group Knowsley Clinical Commissioning Group St Helens Clinical Commissioning Group
Warrington Clinical Commissioning Group
1. Introduction
1.1 The NHS Act 2006 (as amended) (‘the NHS Act’), was amended through the introduction of a Legislative Reform Order (“LRO”) to allow CCGs to form joint committees. This means that two or more CCGs exercising commissioning functions jointly may for a joint committee as a result of the LRO amendment to s.14Z3 (CCGs working together) of the NHS Act. Joint committees are a statutory mechanism which gives CCGs an additional option for undertaking collective strategic decision making.
1.2 The Five Year Forward View footprints were established in accordance with the NHS Shared Planning Guidance requirements 2015/16 which required every health and care system to come together to create their own ambitious local blueprint for accelerating implementation of the NHS Five Year Forward View. In Cheshire and Merseyside it was agreed that within the overall footprint there would be three Local Delivery Systems (LDS) - Alliance, Cheshire & Wirral, and North Mersey.
1.3 The Alliance LDS includes the 4 CCGs of NHS Halton CCG, NHS Knowsley CCG, NHS St. Helens CCG and NHS Warrington CCG.
2. Establishment
2.1 The CCGs have agreed to establish and constitute a Joint Committee with these terms of reference to be known as the Alliance CCGs Joint Committee.
3. Role of the Committee
3.1 The overarching role of the Joint Committee is to take commissioning decisions for the footprint, that are appropriate and in accordance with delegated authority from each CCG Member. Decisions will support the aims and objectives of the Cheshire & Mersey STP, Cheshire & Mersey STP Plan whilst contributing to the sustainability of the local health and social care systems. The Joint Committee will at all times, act in accordance with all relevant laws and guidance applicable to the Parties.
4. Remit of the Joint Committee
4.1 The Joint Committee will be responsible for the delivery of a programme of transformation / service redesign across a defined range of services commissioned by its members. The defined services will be those relating to hospitals in respect of the outputs relating to the C&M STP Cross Cutting themes stated below:
Urgent and Emergency Care Hospital Services Women and Children’s Services

Agenda Item No: 052/17
Halton Clinical Commissioning Group Knowsley Clinical Commissioning Group St Helens Clinical Commissioning Group
Warrington Clinical Commissioning Group
4.2 Services provided at the following hospitals within the Alliance LDS footprint will be in scope of the Joint Committee:
St Helens & Knowsley Teaching Hospitals NHS Trust Warrington and Halton Hospitals NHS Foundation Trust
4.3 The Joint Committee will take into account other service providers as may be
relevant to the transformation / service redesign under consideration.
4.4 The Joint Committee will develop a draft work plan to reflect the agreed priorities from the Cheshire & Mersey STP and Alliance LDS Plan, where joint commissioning decisions are required. The draft work plan will be presented to the respective CCG Governing Bodies for approval, defining the conditions for progressing individual work streams in advance of the work commencing. The priorities within each of the work streams will align with that of the Cheshire & Mersey STP and will take account of any issues that need consideration as a consequence of service reconfiguration under the STP.
5. Functions of the Joint Committee
5.1 The Committee is a Joint Committee of NHS Halton CCG, NHS Knowsley CCG, NHS St. Helens CCG and NHS Warrington CCG, established through the powers conferred by section 14Z3 of the NHS Act 2006 (as amended). Its primary function is to make collective decisions on the review, planning and procurement of health services within its delegated remit.
5.2 In order to deliver its delegated functions the Joint Committee will:
Agree an annual work plan for approval by each Governing Body
Agree and oversee an effective risk management strategy to support decision-making in all areas of business related to the Joint Committee’s remit
Approve individual programme and project briefs, initiation documents and plans. This will include agreeing the parameters at the start of each programme of work, governance and financial arrangements for individual programmes.
Act as a decision-making body; authorising sub-groups to oversee and lead implementation of service changes
Approve future service reconfiguration, service models, specifications, and business cases up to the value as determined for the Governing Body by each constituent CCG’s Scheme of Reservation & Delegation
Ensure appropriate patient and public consultation and engagement and compliance with public sector equality duties as set out in the Equality Act 2010 for the purposes of implementation.
Ensure consultation with the Overview and Scrutiny Committees and Health and Wellbeing Boards (or equivalent) established by the relevant Local Authorities
Agree and oversee the communications and engagement framework relevant to areas of work of the Joint Committee.
Agenda Item No: 052/17
Halton Clinical Commissioning Group Knowsley Clinical Commissioning Group St Helens Clinical Commissioning Group
Warrington Clinical Commissioning Group
5.3 Whilst it is acknowledged that individual CCGs remain accountable for meeting their statutory duties, the Joint Committee will undertake its delegated functions in a manner which complies with the statutory duties of the CCGs as set out in the NHS Act 2006 and including:
Management of the conflicts of interest (section 14O)
Duty to promote the NHS Constitution (section 14P)
Duty to exercise its functions effectively, efficiently and economically (section 14Q)
Duty as to the improvement in quality of services (section14R)
Duties as to reducing inequalities (section 14T)
Duty to promote the involvement of patients (section 14U)
Duty as to patient choice (section 14V)
Duty as to promoting integration (section 14Z1)
Public involvement and consultation (section 14Z2)
5.4 In discharging its responsibilities the Joint Committee will provide assurance to each Governing Body through the submission of minutes from each meeting and an annual report to inform constituent members’ annual governance statements.
5.5 The Committee will conduct an annual effectiveness review which will be reported to each CCG’s Audit Committee.
6. Membership
6.1 The Committee will have two levels of membership, full members and associate members.
6.1.1 The full member organisations are:
NHS Halton CCG
NHS Knowsley CCG
NHS St Helens CCG
NHS Warrington CCG
Each full member organisation will nominate three Governing Body level representatives to sit on the Committee.
The Chairing of the Joint Committee will be managed on a 6 month rotation between the four CCG members;
Each CCG’s Chief Finance Officer (CFO) will either be a member or in attendance.
6.1.2 The associate member organisations are:
Halton Borough Council
Knowsley Council
St Helens Council

Agenda Item No: 052/17
Halton Clinical Commissioning Group Knowsley Clinical Commissioning Group St Helens Clinical Commissioning Group
Warrington Clinical Commissioning Group
Warrington Borough Council
One senior local authority officer representative from each of the local authorities will be invited to attend the Committee.
6.2 Decisions made by the Joint Committee will be binding on its member Clinical
Commissioning Groups.
6.3 Healthwatch will be invited to have one representative to be in attendance on behalf of the local Healthwatch Groups in the LDS Alliance.
6.4 Other organisations may be invited to send representatives to the meetings. In attendance members represent other functions / parties/ organisations or stakeholders who are involved in the programmes of work of the Joint Committee and will provide support and advise the members on any proposals.
Representatives from NHS England will be co-opted to attend as required.
7. Deputies
7.1 An individual may deputise for any Joint Committee Member representative as long as the deputy has delegated decision making authority to fully participate in the business of the Committee.
8. Decision-Making
8.1 The Parties agree that for matters relating to services, there are two different levels of decision making
8.1.1. Level 1: those decisions which are delegated by each party to the Joint Committee (“Joint Committee Decisions”); and
8.1.2 Level 2: those decisions that impact on some but not all member, a decision will be reached by the CCGs with direct in interest in the matter (“CCG(s) decisions”)
8.2 The aim of the Joint Committee is to achieve consensus in decision-making, therefore all Level 1 decisions will require unanimous agreement of all CCG members.
8.3 In the event that consensus cannot be reached the matter will be referred back to individual Governing Bodies and a joint Governing Body meeting (dependent on the number of CCGs involved in the decision) will be convened. If agreement cannot be reached the Joint Committee will be asked to amend the proposals in order to achieve consensus.

Agenda Item No: 052/17
Halton Clinical Commissioning Group Knowsley Clinical Commissioning Group St Helens Clinical Commissioning Group
Warrington Clinical Commissioning Group
9. Quoracy
9.1 The meeting will be considered quorate with two representatives of each CCG (including the Chair); one representative from each CCG must be an officer of the CCG.
10. Meetings
10.1 The Joint Committee shall meet at least six times per year; the Chair will have authority to call an extraordinary meeting with at least 2 days notice.
10.2 Meetings will be scheduled to ensure they do not conflict with respective CCG Governing Body meetings.
10.3 Meetings with other Joint Committees in the Cheshire & Merseyside STP will be arranged, as required. In the event that a sub group or working group is considered appropriate from such a meeting, both parties will need to agree the reporting arrangements.
10.4 Members of the public may also attend meetings of the Joint Committee. They may observe deliberations of the Committee but do not have the right to contribute to the debate. Items the Committee considers not to be in the public interest will be held in Part 2 of the meeting, which will not be held in public as per Schedule 1A, paragraph 8 of the NHS Act 2006.
11. Conflicts of Interest
11.1 The Committee shall hold and Register of Interests. This register shall record all relevant and material, person or business interest, and management action, and will be published on CCG websites.
11.2 Each member and attendee of the Committee shall be under a duty to declare any such interests. Any change to these interests should be notified to the Chair.
11.3 Where any Joint Committee member has an actual or potential conflict of interest in relation to any matter under consideration at any meeting, the Chair (in their discretion) shall decide, having regard to the nature of the potential or actual conflict of interest, whether or not that Joint Committee member may participate in the meeting (or part of meeting) in which the relevant matter is discussed. Where the Chair decides to exclude a Joint Committee member, the relevant party may send a deputy to take the place of that conflicted Joint Committee member in relation to that matter, as per section 7 above.
11.4 Should the Committee Chair have a conflict of interest, he/she will appoint a deputy chair, for the purpose of chairing that particular meeting.
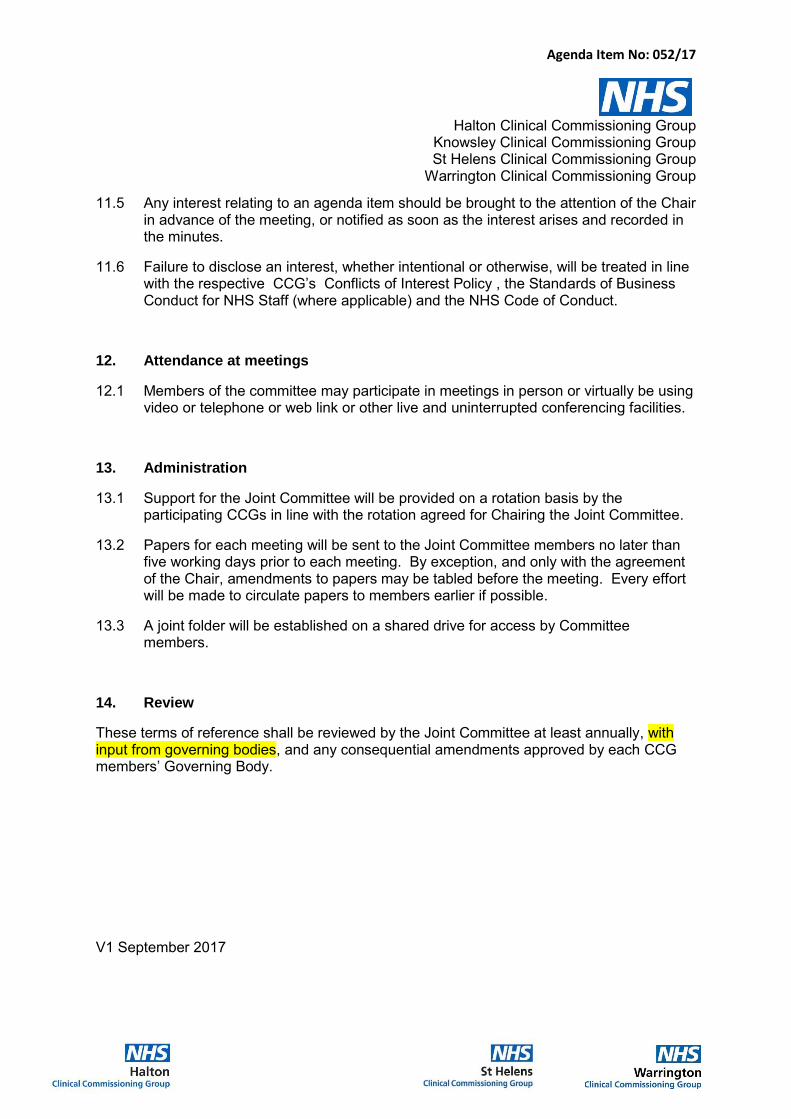
Agenda Item No: 052/17
Halton Clinical Commissioning Group Knowsley Clinical Commissioning Group St Helens Clinical Commissioning Group
Warrington Clinical Commissioning Group
11.5 Any interest relating to an agenda item should be brought to the attention of the Chair in advance of the meeting, or notified as soon as the interest arises and recorded in the minutes.
11.6 Failure to disclose an interest, whether intentional or otherwise, will be treated in line with the respective CCG’s Conflicts of Interest Policy , the Standards of Business Conduct for NHS Staff (where applicable) and the NHS Code of Conduct.
12. Attendance at meetings
12.1 Members of the committee may participate in meetings in person or virtually be using video or telephone or web link or other live and uninterrupted conferencing facilities.
13. Administration
13.1 Support for the Joint Committee will be provided on a rotation basis by the participating CCGs in line with the rotation agreed for Chairing the Joint Committee.
13.2 Papers for each meeting will be sent to the Joint Committee members no later than five working days prior to each meeting. By exception, and only with the agreement of the Chair, amendments to papers may be tabled before the meeting. Every effort will be made to circulate papers to members earlier if possible.
13.3 A joint folder will be established on a shared drive for access by Committee members.
14. Review
These terms of reference shall be reviewed by the Joint Committee at least annually, with input from governing bodies, and any consequential amendments approved by each CCG members’ Governing Body.
V1 September 2017
Agenda Item No: 053/17
Business Conduct & Conflict of Interest Policy Warrington CCG Governing Body Meeting 13
th September 2017
GOVERNING BODY MEETING:
CCG Governing Body
DATE OF MEETING:
13
th September 2017
REPORT AUTHOR AND JOB TITLE:
Nick Armstrong Chief Operating Officer
REPORT TITLE:
Business Conduct & Conflict of Interest Policy
STRATEGIC OBJECTIVES:
Please tick which strategic objectives the paper relates to
Improve quality of services
Sustained financial balance
Build an effective and motivated whole system workforce
Sound governance arrangements
Ensure integration and joint working arrangements
OUTCOME REQUIRED (tick)
Approval
Assurance
Discussion
Information
EXECUTIVE SUMMARY
To provide Warrington CCG Governing Body with
An update on the revised statutory guidance on managing conflicts of interest for CCGs
Request approval of minor changes to the CCGs Business Conduct & Conflict of Interest Policy to adhere to revised guidance
RECOMMENDATIONS
The Governing Body is asked to;
a) Note the revised statutory guidance on managing conflicts of interest for CCGs
b) Ratify the minor changes to the CCGs Business Conduct & Conflict of Interest Policy to adhere to revised guidance, as approved by Audit Committee
Agenda Item No: 053/17
Business Conduct & Conflict of Interest Policy Warrington CCG Governing Body Meeting 13
th September 2017
Outline any engagement – staff, clinical, stakeholder and patient / public
Not applicable
Are there any conflicts of interest which may be associated with this paper?
None
Does this paper address any existing risks which are included on the Assurance Framework or Risk Register?
Yes – B2 & D1
Have the following areas been considered whilst producing this report?
Yes
N/A
Equality Impact Assessment (if yes, attach to paper)
Quality Impact Assessment (if yes, attach to paper)
Regulation, legal, governance and assurance implications (reference in the report if applicable)
Procurement process (reference in the report if applicable)
Document development
Has this document been presented to any other Committee or Forum? If yes, please list which meeting, date and outcome of presentation
Yes – The revised policy was presented and approved for Governing Body ratification at the Audit Committee meeting on 23
rd August.

Agenda Item No: 053/17
Business Conduct & Conflict of Interest Policy Warrington CCG Governing Body Meeting 13
th September 2017
WARRINGTON CLINICAL COMMISSIONING GROUP
BUSINESS CONDUCT & CONFLICT OF INTEREST POLICY
Purpose 1. The purpose of this report is to provide Members of the Governing Body with:
An update on the revised statutory guidance on managing conflicts of interest for CCGs
Ratify of minor changes to the CCGs Business Conduct & Conflict of Interest Policy to adhere to revised guidance, as approved by Audit Committee
Revised statutory guidance on managing conflicts of interest for CCGs 2. On 16 June 2017 NHS England published updated CCG statutory guidance
on managing conflicts of interest and associated supporting documents. This is to ensure the CCG guidance is fully aligned with the recently published cross system conflicts of interest guidance - Managing conflicts of interest in the NHS: Guidance for staff and organisations.
Key changes to the guidance 3. The key changes from the 2016 version of the guidance include:
Registers of interest: the CCG guidance has been changed to require that CCGs have systems in place to satisfy themselves as a minimum on an annual basis that their registers of interest are accurate and up-to-date, and to require that only decision-making staff are included on the published register.
Gifts from suppliers or contractors: In line with the NHS-wide guidance, gifts of low value (up to £6), such as promotional items, can now be accepted.
Gifts from other sources: Also in line with the wider guidance, gifts of under £50 (rather than £10) can be accepted from non-suppliers and noncontractors, and do not need to be declared; and gifts with a value of over £50 can now be accepted on behalf of an organisation, but not in a personal capacity.
Hospitality - meals and refreshments: The thresholds have been amended to advise that hospitality under £25 does not need to be declared. Hospitality between £25 and £75 can be accepted, but must be declared, and hospitality over £75 should be refused unless senior approval is given.
New care models: a new annex has been included to provide further advice on identifying, declaring and managing conflicts of interest in the commissioning of new care models.

Agenda Item No: 053/17
Business Conduct & Conflict of Interest Policy Warrington CCG Governing Body Meeting 13
th September 2017
4. In addition supporting documents which include: 2-page summary guides for different professional groups; case studies on conflicts of interest management; and templates and toolkits to support with implementation of the guidance have been updated. All information can be viewed at https://www.england.nhs.uk/commissioning/pc-co-comms/coi/
Key changes to the Business Conduct & Conflict of Interest Policy 5. Warrington CCGs Business Conduct and Conflict of Interest Policy, available
on the CCG Website has been updated to include the changes listed above in order that it adheres to the new guidance.
6. Furthermore a paragraph has also been added to make it explicit to Chairs of meetings that if exclusions arising from a conflict of interest affect the quoracy of the meeting the Chair must postpone the agenda item until a quorum can be achieved without conflict. This requirement was an action arising from the MIAA review of the policy in 16/17.
7. Finally appendices B to K have been replaced with a weblink to ensure the most up to date documents are accessed from the NHS England website by users of the policy.
8. The updated policy was reviewed, discussed and approved for Governing Body ratification at Audit Committee on 23rd August. The Audit Committee also requires actions of the CCG management team in relation to implementation of the new policy which will be monitored through the Committee.
RECOMMENDATIONS 9. Members of the Governing Body are asked to:
a) Note the revised statutory guidance on managing conflicts of interest
for CCGs b) Ratify the minor changes to the CCGs Business Conduct & Conflict of Interest Policy to adhere to revised guidance, as approved by Audit Committee Nick Armstrong Chief Operating Officer September 2017
AGENDA ITEM NO: 054/17
Committee Summary Paper Warrington CCG Governing Body Meeting 13
th September 2017
GOVERNING BODY MEETING:
Governing Body Meeting
DATE OF MEETING:
13
th September 2017
REPORT AUTHOR AND JOB TITLE:
Nick Armstrong, Chief Operating Officer
REPORT TITLE:
Committee Summary Report
STRATEGIC OBJECTIVES:
Please tick which strategic objectives the paper relates to
Improve quality of services
Sustained financial balance
Build an effective and motivated whole system workforce
Sound governance arrangements
√
Ensure integration and joint working arrangements
OUTCOME REQUIRED (tick)
Approval
Assurance
Discussion
Information
√
EXECUTIVE SUMMARY
To provide Warrington CCG Governing Body with summaries of discussions and decisions of the Committees established by the Governing Body, or Joint Committees across the North West which have an influence on the CCG’s business.
RECOMMENDATIONS
The Governing Body are asked to:
Note the decisions made on their behalf and support them
Ratify the amended Terms of Reference of the Audit Committee as agreed at the Audit Committee meeting on the 23
rd August 2017
AGENDA ITEM NO: 054/17
Committee Summary Paper Warrington CCG Governing Body Meeting 13
th September 2017
Outline any engagement – staff, clinical, stakeholder and patient / public
Not applicable
Are there any conflicts of interest which may be associated with this paper?
Not applicable
Does this paper address any existing risks which are included on the Assurance Framework or Risk Register?
Not applicable
Have the following areas been considered whilst producing this report?
Yes
N/A
Equality Impact Assessment (if yes, attach to paper)
√
Quality Impact Assessment (if yes, attach to paper)
√
Regulation, legal, governance and assurance implications (reference in the report if applicable)
√
Procurement process (reference in the report if applicable)
√
Document development
Has this document been presented to any other Committee or Forum? If yes, please list which meeting, date and outcome of presentation

AGENDA ITEM NO: 054/17
Committee Summary Paper Warrington CCG Governing Body Meeting 13
th September 2017
Strategic Objectives and Risks 2017/18
A1 Failure to performance manage to ensure continuous improvement
A2 Failure to agree and measure outcomes
A3 Failure to ensure clear arrangements are in place for quality management of non-commissioned providers in the independent sector
B1 Failure to implement the financial strategy
B2 Failure to ensure sound business practices are at the heart of running the CCG
B3 Failure to secure best value
B4 Failure to adequately provide for external factors, which impact on financial sustainability
C1 Failure to continuously develop the organisational culture that meets the needs of the changing needs of the workforce
C2 Failure of delivery by outsourced critical business functions
C3 Failure to establish primary care capacity
D1 Failure to ensure that we are compliant with our statutory duties
D2 Failure to demonstrate patient and public engagement
E1 Failure to provide appropriate reporting, for joint working arrangements
E2 Failure to describe benefit of integration and joint working arrangements to local people
AGENDA ITEM NO: 054/17
Committee Summary Paper Warrington CCG Governing Body Meeting 13
th September 2017
Primary Care Co-Commissioning Committee – 13th July 2017
The Committee noted the Risk Report and agreed that the necessary
actions are in place to mitigate all risks and agreed any additional
assurance that may be required in relation to any risks. The
Committee discussed whether any further assurance is required in
relation to any risk where the timescales have been changed and the
reasons for the slippage. The Committee agreed that there were no
further risks identified as a result of papers presented to the Committee
which may need to be added to the risk register.
The Committee noted the contents of the Delegated Transition Plan
and agreed to this item being a standard agenda item at future
Committee Meetings.
The Committee received a joint primary care update from Warrington
CCG and NHS England and agreed to “full delegated commissioning”
being a standing agenda item for future committees
The Committee received the Financial Performance Report and noted
the financial position at 31st May 2017. Members approved the PMS
redistribution methodology for the brought forward resources.
The Committee noted and discussed the contents of the Primary Care
Workforce report.
The Committee received a presentation from NHS England around the
GP Forward View.
Quality Committee – 26th July 2017
The Committee noted the Risk Schedule and agreed that the
necessary actions are in place to mitigate all risks. The Committee
agreed any additional assurance that may be required in relation to a
specific risk and discussed whether any further assurance is required in
relation to any risks where the timescales have been changed and he
reasons for slippage.
The Committee noted and discussed the Quality Report and noted the
concerns and assurances provided.
The Committee considered the serious incident report and noted the
update on never events at the hospital and noted the themes and
trends identified through serious incidents at the hospital. The
Committee discussed the issues raised within the report regarding the
appropriateness of admission for frail and elderly people. The
committee noted the concerns raised with Bridgewater Community
Healthcare Foundation Trust and received assurance about the serious
incident management process.
The Committee approved the Warrington Joint Policy on Section 117
Aftercare for Children, Young People and Adults.
AGENDA ITEM NO: 054/17
Committee Summary Paper Warrington CCG Governing Body Meeting 13
th September 2017
The Committee noted the minutes from the Contract and Quality
Meetings.
Finance & Performance Committee – 26th July 2017
The Committee noted the Risk Report and agreed the necessary
actions are in place to mitigate all risks and agreed any additional
assurance that may be required in relation to a specific risk. The
Committee discussed whether any further assurance or support is
required in relation to any risk where the timescales have been
changed.
The Committee received the Finance Report and noted that there is a
robust process in place to monitor the QIPP process for the financial
year 2017/18. The Committee noted the financial position as at the
end of June 2017. The Committee acknowledged the financial
pressures to date and the utilisation of activity reserves to mitigate.
The Committee acknowledged the financial risks identified within the
report and discussed an additional areas that it requires the CCG
support team to implement to achieve additional efficiency savings.
The Committee received a report around the Better Care Fund and
ratified the proposals within the report.
Audit Committee – 23rd August 2017
The Committee reviewed the Audit Committee Terms of Reference and
agreed to a number of amendments before they are presented to the
next Governing Body Meeting.
The Committee received a report around the Business Conduct and
Conflict of Interest Policy and noted the revised statutory guidance on
managing conflicts of interest for CCGs. The Committee approved the
changes to the policy.
The Committee noted the Governance and External Assurance Report.
The Committee noted the Information Governance Report as
assurance of the CCG’s ongoing work in relation to Information
Governance and preparation for GDPR.
The Committee noted the Internal Audit Report from Mersey Internal
Audit Agency.
The Committee noted the Follow Up Report and members were
assured from the recommendations that have now been completed and
for the outstanding recommendations they will ensure that there is
sufficient Senior Management oversight to ensure these remaining
recommendations are implemented in a timely manner in order to
mitigate any potential risks to the organisation.

AGENDA ITEM NO: 054/17
Committee Summary Paper Warrington CCG Governing Body Meeting 13
th September 2017
The Committee noted the contents of the Audit Committee Self
Assessment report and the recommendations arising from the reviews.
The Committee noted the contents of the Insight Report.
The Committee noted the Annual Audit Letter and its contents and that
in line with reporting throughout the year.
The Committee received the Risk Assurance Framework and
discussed in detail Risk D1.
The Committee received an update from Risk Owners.
The Committee noted a tender waiver
Commissioning & Service Development Committee
The Committee received a clinical lead update from the Medicines
Management Clinical Lead and Mental Health Clinical Leads.
The Committee considered the agenda planning process for Protected
Learning Time Events.

Agenda Item No: 054/17 - Appendix
NHS Warrington Clinical Commissioning Group
Audit Committee
Terms of Reference
1. Introduction
The Audit Committee (the Committee) is established in accordance with Warrington Clinical Commissioning Group’s constitution. These terms of reference set out the membership, remit, responsibilities and reporting arrangements of the Committee.
2. Membership
The Committee shall be appointed by the Clinical Commissioning Group as set out in the Clinical Commissioning Group’s constitution and may include individuals who are not on the governing body. The Audit Committee comprises of the following members:
2 Lay Advisors
GP member of Clinical Commissioning Group
1 Other Clinical Member
All of the above members shall have a vote. The chair of the committee will normally be a non-clinical member of the governing body.
3. Role of the Chair
The Governing Body recognise the role of the Chair of the Audit Committee goes beyond chairing meetings and is key to achieving Committee effectiveness. The role is set out in detail in Appendix 1.
4. External Auditors
The Group has the power to appoint it’s External Auditors. The External Auditors for the Group will be appointed on behalf of the Clinical Commissioning Group by a joint external audit procurement panel covering the Cheshire area.
5. Attendance
The Committee may also extend invitations to other personnel with relevant skills, experience or expertise as necessary to deal with the business on the agenda. Such personnel will be in attendance and will have no voting rights. This will normally include:
Chief Finance Officer
Clinical Chief Officer
Chief Operating Officer
Agenda Item No: 054/17 - Appendix
Head of Finance
Head of Assurance & Risk
Internal Auditors
External Auditors
On a less frequent basis the following good practice will be followed:
At least once a year the committee should meet privately with the external and
internal auditors.
Representatives from NHS Counter Fraud Authority may be invited to attend
meetings and will normally attend at least one meeting each year.
Regardless of attendance, external audit, internal audit, local counter fraud and
security management (NHS Counter Fraud Authority) providers will have full and
unrestricted rights of access to the audit committee.
The Accountable Officer would normally be invited to attend and discuss, at least
annually with the committee, the process for assurance that supports the
statement on internal control. and when the committee considers the draft
internal audit plan and the annual accounts.
Any other members or employees may be invited to attend, particularly when the
committee is discussing areas of risk or operation that are the responsibility of
that members or employee.
The chair of the governing body may also be invited to attend one meeting each
year in order to form a view on, and understanding of, the committee’s
operations.
6. Secretary
The Committee will be supported by both the Chief Finance Officer and the Head of Assurance & Risk who will be responsible for supporting the Chair in the management of the Committee’s business and for drawing the Committee’s attention to best practice, national guidance and other relevant documents, as appropriate.
7. Quorum
A quorum shall be 2 members; including one Lay Member. The Lay Member should chair the committee.
8. Frequency and notice of meetings
Meetings shall be held not less than four times a year. The minutes of Committee meetings will be formally recorded and submitted to the Governing Body.
9. Remit and responsibilities of the Committee
The responsibility of the Committee covers all activities within the remit of the Governing Body.
Agenda Item No: 054/17 - Appendix
Its duties can be categorised as follows: Internal Control and Risk Management
The Committee shall review the establishment and maintenance of an effective system of integrated governance, internal control, and risk management that supports the achievement of the organisation’s objectives. In particular, the Committee will review the adequacy of:
All risk and control related disclosure statements, together with any accompanying
Head of Internal Audit statement, prior to endorsement by the Audit Committee.
All of the Group’s processes of corporate governance to enable the organisation to
implement best practice as set out in appropriate guidance.
The structures, process and responsibilities for identifying and managing key risks
facing the organization; including the Risk Assurance Framework.
The policies for ensuring that there is compliance with relevant regulatory, legal and
code of conduct requirements and other relevant guidance; and
The operational effectiveness of policies and procedures.
The CCG annual programme of Clinical audits, the outcome Clinical audits is
reported to the CCG quality committee.
Internal audit of effectiveness of organisational policies
Internal Controls ensuring that there is an effective system of integrated Governance
across the whole of the organisation that supports the achievements of the
organisation’s objectives.
Regularly monitor relevant Key Performance Indicator reports for example risk
management, incidents and near misses, information governance, complaints, FOIs
and statutory and mandatory training.
Internal Audit
Review, and recommend for approval, the internal audit programme (and any major
changes to the plan), consider the major findings of internal audit investigations (and
management’s response), and ensure co-ordination between Internal and External
Auditors.
Ensure that the Internal Audit function is adequately resourced, reflects a risk-based
approach to audit, and has appropriate standing within the organisation.
Consider the Chief Internal Auditor’s Opinion Statement and the Accountable
Officer’s Statement of Internal Control (SIC);
Agenda Item No: 054/17 - Appendix
Ensure there is an annual review of the CCGs Internal Audit provider; and
Receive regular reports from the Chief Internal Auditor.
Local Counter Fraud Service
To agree the annual Counter Fraud Plan and Annual Report as presented by the
CCGs Local Counter Fraud Specialist; and
The policies and procedures for all work related to fraud and corruption as set out by
the NHS Counter Fraud Authority
External Audit
Review, and recommend for approval, the external audit programme (and any major
changes to the plan), and approve any additional off plan work;
Review External Audit reports, including value for money reports and annual audit
letters, together with the management response;
Receive regular reports from the External Auditor; and
Ensure there is an annual review of the CCGs External Audit provider.
Financial Reporting
Review the annual financial statements on behalf of the Governing Body focusing
particularly on:
o Changes in, and compliance with, accounting policies and practices
o Major judgmental areas; and
o Significant adjustments resulting from the audit.
10. Assurance Framework
The Committee will monitor the development of a comprehensive Assurance Framework for the Group including:
Review of the Assurance Framework to ensure that there is an appropriate spread of
strategic objectives and that the main inherent/residual risks have been identified, as
well as any that are newly arising.
Assurance that the process of compiling the Framework meets good practice
guidelines, that directors and managers have been involved, and take responsibility
for their entries, and that there are no major omissions from the list of controls.

Agenda Item No: 054/17 - Appendix
Monitor the implementation of response plans.
Consider the “audit needs” of the organisation in terms of the sources of assurance,
both independent and from line management, and ensure that there is a plan for
these assurances to be received.
Review the results of assurances, and the implications that these have on the
achievement of Group objectives.
11. Relationship with the governing body
The Committee is authorised by the Governing Body to investigate any activity within its Terms of Reference. It is authorised to seek any information it requires from any member or employee who is directed to co-operate with any request made by the Committee.
12. Reporting to the governing body
The Committee will report its activity and actions taken to the next governing body meeting following a meeting of the Committee.
13. Policy and best practice
The Committee is authorised by the Governing Body to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary. This includes seeking the advice of specialists from within, and outside, the NHS as necessary, such as. advisors from related bodies.
14. Induction Arrangements
The Committee recognise the need to support members in understanding the role of the Audit Committee and their role on the Committee. The Internal Auditors will provide regular induction and refresher training as required. All members are expected to be aware of the NHS Audit Committee Handbook which will be provided to all new members of the Committee by the Secretary.
15. Conduct of the committee
The Committee will develop a work plan with specific objectives which will be reviewed regularly and formally on an annual basis.
Approved by: …………………………….. Issued date: ……………………………. Review date: .……………………………
Agenda Item No: 054/17 - Appendix
Appendix 1
THE ROLE OF THE CHAIR
The role of the Chair of the Audit Committee is key to achieving Committee effectiveness. The additional workload will be taken into account in the appointment of the Chair. Key activities beyond Committee meetings should include the following.
Agenda setting
Before each meeting the Chair and the Committee Secretary should meet to discuss and agree the business for the meeting. The Chair should take ownership of, and have final say in, the decisions about what business will be pursued at any particular meeting.
Communication
The Chair should ensure that after each meeting appropriate reports are prepared from the Audit Committee to the Governing Body and the Clinical Chief Officer. The Chair should ensure that the Audit Committee provides a suitable Annual Report to the Governing Body. The Chair should have bilateral meetings at least annually with the Accounting Officer, the Head of Internal Audit and the External Auditor, and with the Chair of the Board. In addition, the Chair should meet any people newly appointed to these positions as soon as practicable after their appointment. The Chair should also ensure that all Committee members have an appropriate programme of interface with the organisation and its activities to help them understand the organisation, its objectives, business needs and priorities.
Monitoring actions:
The Chair should ensure that there is an appropriate process between meetings for action points arising from Committee business to be appropriately pursued. The Chair should also ensure that members who have missed a meeting are appropriately briefed on the business conducted in their absence.
Appraisal:
The Chair should take the lead in ensuring that Committee members are provided with appropriate appraisal of their performance as a Committee member and that training needs are identified and addressed. The Chair should themselves seek appraisal of their performance from the Chair of the Governing Body.