volumetric laser endomicroscopy for barrett’s … · volumetric laser endomicroscopy for...
TRANSCRIPT

J Gastrointestin Liver Dis, September 2017 Vol. 26 No 3: 291-297
1) Division of Gastroenterology and Hepatology, Department of Internal Medicine, Albert Einstein Medical Center, Philadelphia, PA;2) Department of Internal Medicine, Albert Einstein Medical Center, Philadelphia, PA;3) Department of Pathology, Baylor College of Medicine, Houston, Texas;4) Division of Gastroenterology, Hepatology and Nutrition, University of Texas Health Science Center at Houston, Houston, Texas, USA
Address for correspondence: Shashideep Singhal, MDDivision of Gastroenterology, Hepatology and Nutrition, University of Texas Health Science Center at Houston, 6431 Fannin, MSB 4.234, Houston, Texas, USA 77030 [email protected]
Received: 20.05.2017 Accepted: 12.07.2017
Volumetric Laser Endomicroscopy for Barrett’s Esophagus – Looking at the Fine Print
Deepanshu Jain1, Sanna Fatima2, Shilpa Jain3, Shashideep Singhal4
INTRODUCTION
Barrett’s esophagus (BE) is a premalignant condition characterized by intestinal metaplasia that replaces the normal squamous epithelium. Barrett’s esophagus develops in association with chronic gastroesophageal reflux disease (GERD). Chronic GERD and BE are considered major risk factors for the development of esophageal adenocarcinoma (EAC) [1, 2]. The true prevalence of BE is difficult to assess as most patients are asymptomatic and it is only detected on endoscopic evaluation. The incidence of EAC
REVIEW
ABSTRACT
Barrett’s esophagus (BE) is a premalignant condition. The incidence of adenocarcinoma in BE has been reported to be between 0.1-3%. Dysplasia in BE is patchy and extensive biopsy sampling is labor intensive, low yield and does not eliminate the sampling error completely. Volumetric laser endomicroscopy (VLE) is expected to enable endoscopists to do targeted biopsy of dysplastic/cancerous lesions (not visible on white light endoscopy) among patients with BE. We reviewed 7 studies with a total of 62 subjects who had undergone VLE. Of 34 patients with available data, VLE correlated with histology in 17 subjects (50%). It missed the underlying diagnosis in one subject (2.9%). VLE led to inadvertent biopsy in 16 patients (47.1%), and led or would have led to upstaging of disease in 11 subjects (32.4%). In the entire cohort, the sensitivity, specificity, positive predictive value and negative predictive value (NPV) of VLE for diagnosis of dysplasia, buried Barrett’s or intramucosal carcinoma was 92.3%, 23.8%, 42.9% and 83.3%, respectively. High sensitivity and NPV can potentially help space out the surveillance intervals. Low specificity does lead to a high number of biopsies, which are likely less than non targeted biopsies. Volumetric laser endomicroscopy is a safe and sensitive test to identify mucosal lesions in patients with BE which are invisible under standard white light endoscopy. Key words: Volumetric laser endomicroscopy – Barrett’s esophagus – esophageal adenocarcinoma.
Abbreviations: BE: Barrett’s Esophagus; BB: Buried Barrett’s; EAC: Esophageal adenocarcinoma; EDS: Evans Dysplasia Score; EMR: Endoscopic Mucosal Resection; GERD: Gastro-esophageal reflux disease; HGD: High grade dysplasia; IMC: Intra-mucosal adenocarcinoma; LGD: Low grade dysplasia; NBI: Narrow Band Imaging; OCT-SI: Optical Coherence Tomography Scoring Index; RFA: Radiofrequency ablation; SGS: Sub-squamous glandular structures; VLE: Volumetric Laser Endomicroscopy; WLE: White Light Endoscopy.
Available from: http://www.jgld.ro/wp/archive/y2017/n3/a14/DOI: http://dx.doi.org/10.15403/jgld.2014.1121.263.jai
in BE has been reported to be between 0.1-3% [3-6]. In recent decades, the incidence of EAC has been increasing despite current screening guidelines [7, 8]. The primary strategy to prevent death from EAC has been to perform endoscopy in high-risk patients with GERD to detect BE and in patients with BE to perform surveillance endoscopies at regular interval to detect neoplasia [9]. The current gold standard for surveillance in patients with BE is random 4-quadrant biopsy every 1-2 cm. If any irregularities such as nodules are noted, then endoscopic mucosal resection (EMR) is performed [10]. Dysplasia in BE is patchy in extent and severity and can be missed because of sampling error [11-14]. Extensive biopsy sampling is labor intensive, low yield and does not eliminate the sampling error completely. In addition, when dysplasia is detected, foci of invasive cancer may be missed [15-17].
Several advanced techniques have been proposed to enhance the identification of dysplastic areas in BE [18]. Advanced endoscopic imaging enables targeted biopsies and improves accuracy of endoscopic surveillance and may

292 Jain et al
J Gastrointestin Liver Dis, September 2017 Vol. 26 No 3: 291-297
complement traditional white light endoscopy (WLE) [19, 20]. Volumetric laser endomicroscopy (VLE) is one such technique. It utilizes optical scattering of near-infrared light to generate cross-sectional images of the esophageal mucosa based on differences in tissue composition. Volumetric laser endomicroscopy has an axial resolution of 7 µm, a transverse resolution of about 30 µm, and can reach an imaging depth of up to 2 to 3 mm [21-23].
The studies describing the use of VLE in surveillance of BE have been reviewed.
METHODS
An extensive literature review was done through January 2017 using Pubmed, Google Scholar and Medline. The included studies were identified using keywords – volumetric laser endomicroscopy, Barrett’s esophagus, esophageal adenocarcinoma. The references of pertinent studies were manually searched to identify additional relevant studies. Human only articles were selected.
RESULTS
We identified 7 studies [23-29] that were relevant to our review. The total number of patients in all of the studies was 62. We included one single center prospective study by Leggett et al. that was conducted in the United States [23]. Three case series, one each by Swager et al. (The Netherlands) [24], Trindade et al. (USA) [25], Benjamin et al. (USA) [26] and three case reports from the USA one each by Leggett et al. [27], Atkinson et al. [28] and Trindade et al. [29] were also included in the review. Results from each study have been summarized in Table I.
Equipment and techniquesThe NvisionVLETM system was used in all studies [23-
29]. Volumetric laser endomicroscopy is a second-generation optical coherence tomography. The NvisionVLETM imaging system consists of a console, monitor and a balloon based optical probe. The optical probe is designed to fit through the therapeutic endoscope’s instrument channel. The probe is centered by a 20-25 mm balloon that is 6 cm in length. The console generates near-infrared light (bandwidth range 1250-1350 nm), has a display with user interface and data acquisition monitor. The probe allows the balloon to be centered in the middle of the esophageal lumen for in vivo imaging. Long segment imaging can be obtained with an axial resolution of 7 µm, a transverse resolution of about 30 µm, and can reach an imaging depth of up to 2 to 3 mm. A total of 1200 images can be obtained in 96 secs [23-26].
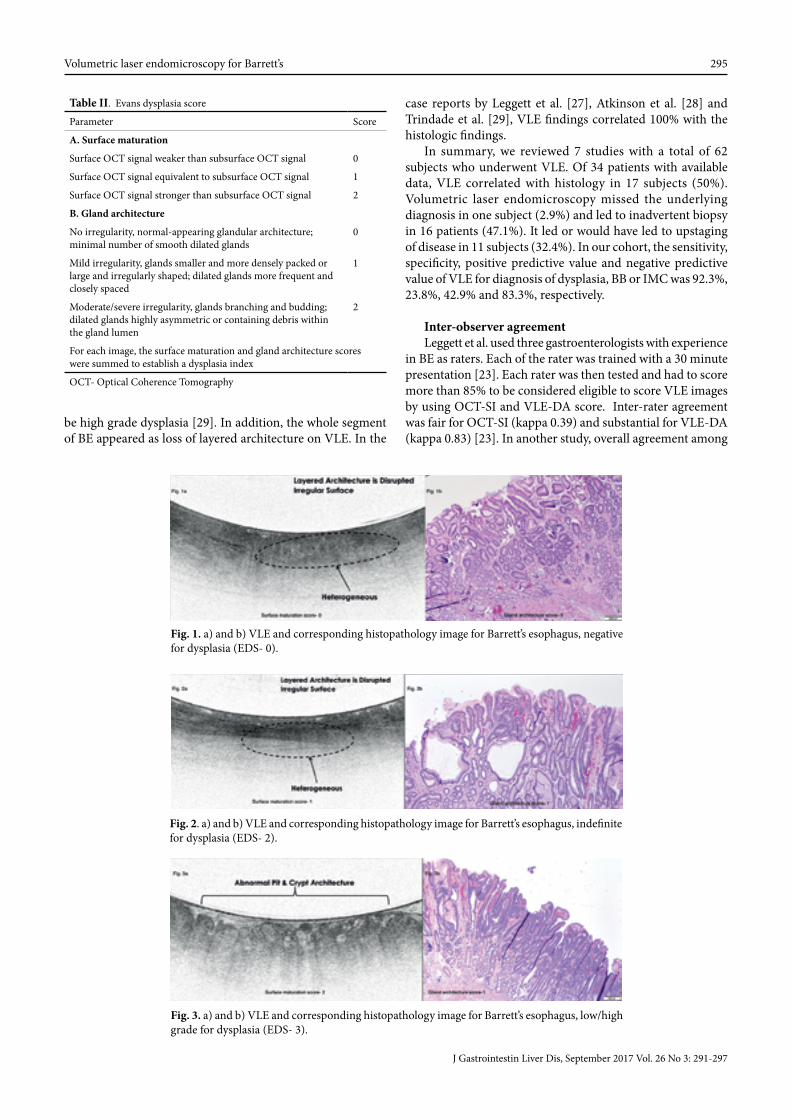
Normal esophageal mucosa on VLE imaging is characterized by a layered horizontal architecture without glands in the epithelium while intestinal metaplasia shows loss of layered architecture and absence of surface pits, crypts or glands in the epithelium. Glandular architecture and surface maturation (determined by signal intensity) are the two main features that determine presence of dysplasia. Evans et al. came up with a scoring method to aid in determining the severity of dysplasia (Table II) [30]. Figures 1- 5 represent corresponding
VLE and histopathology images for different Evans dysplasia scores (EDS).
Leggett et al. performed VLE on 50 ex-vivo EMR specimens obtained from 27 patients with BE not previously treated with radiofrequency ablation (RFA) [23]. The authors devised a new algorithm named VLE-DA for detection of dysplasia in the background of BE. VLE-DA used degree of effacement of the mucosal layer and the number of atypical glandular structures as salient characteristics associated with dysplasia in BE. If complete effacement of mucosal architecture was seen and the surface intensity was greater than sub-surface or if partial effacement was seen with >5 atypical glands, then dysplasia was suspected. Homogeneous scattering was suggestive of a high-grade dysplasia or intramucosal adenocarcinoma. The VLE-DA showed a sensitivity of 86% (95%CI, 69-95), a specificity of 88% (95%CI, 60-99) and diagnostic accuracy of 87% for the detection of BE [23]. The authors also compared the VLE-DA to Optical Coherence Tomography-Scoring Index (OCT-SI or EDS) previously proposed by Evans et al. [22, 23]. OCT-SI (=> 3) in the study by Leggett et al. had a sensitivity of 70% (95% CI, 52-84) and specificity of 60% (95% CI, 36-79) for the detection of BE [23]. The sensitivity and specificity of VLE was shown to vary with the cut-off threshold for OCT-SI [23]. At a lower threshold of OCT-SI (=>2) the sensitivity of VLE for BE was higher (93%) but the specificity much lower (18%). Similarly, at a higher threshold of OCT-SI (=>4), the sensitivity (93%) was higher but the specificity much lower (14%) [23].
Indications and contraindicationsThere were 33 cases of BE, 4 cases of low-grade dysplasia
(LGD), 13 cases of high-grade dysplasia (HGD) and 12 cases of intramucosal adenocarcinoma (IMC) [23-29]. The indication for endoscopy was surveillance for IMC or dysplasia among patients with BE or for surveillance of buried Barrett’s (BB) among post ablation subjects, except two cases where the indication was therapeutic for LGD and IMC [26]. In 7 cases, no previous treatment was performed [25, 26]. Twenty-eight patients had no information available about prior treatment [23, 29], while the rest of patients had received either RFA, EMR or dilation of esophageal stricture [24-27].
Volumetric laser endomicroscopy is contraindicated in patients with esophageal varices and in patients with diseases that prevent full distension of VLE catheter balloon such as esophageal mass, strictures and eosinophilic esophagitis [26]. In addition, inability to undergo endoscopic resection (such as due to bleeding diathesis) also precludes VLE [24].
DISCUSSION
In the case series reported by Swagger et al., WLE and narrow band imaging (NBI) were performed on all patients (N = 17) post RFA [24]. Volumetric laser endomicroscopy in 13/17 patients showed sub-squamous glandular structures (SGS) that were delineated by cautery marks and reconfirmed by VLE that prompted targeted endoscopic resection [24]. Histopathology in these cases showed only one case of BB while the rest of the 12 cases showed normal histological features of dilated submucosal glands and blood vessels. In the rest (4/17) of the patients, VLE was reported as normal.

Volumetric laser endomicroscopy for Barrett’s 293
J Gastrointestin Liver Dis, September 2017 Vol. 26 No 3: 291-297
Table I. Descriptive summary of individual studies
Author/ Year/ Location
Study type
No of subjects
Previous diagnosis
Previous treatment
Current indication
White light endoscopy (WLE)
Narrow Band Imaging (NBI)
Volumetric Laser Endo-microscopy (VLE)
Biopsy type
Histo-pathology
Legget et al. [23] 2016 USA
Single center prospective study
27 Barrett‘s esophagus
NA Surveillance Not performed
Not performed
NA EMR 1. Non-dysplastic Barrett‘s - 10 pts 2. LGD - 6 pts 3.HGD -24 pts 4. IMC - 10 pts
Swager et al. [24] 2015 Netherlands
Case Series 17 1. Early adeno-carcinoma -8 pts 2. HGD - 9 pts
1. Endoscopic resection and RFA - 14 pts 2. RFA mono-therapy- 3 pts
Surveillance No suspicious regions identified
No suspicious regions identified
1.SGS in 13 pts 2. 4 pts with normal VLE
1. Targeted endoscopic resection in patients with sub SGS2. Random biopsy in 4 patients with normal VLE
1. 1 patient had BB 2. Most patients with SGS on VLE had normal histology
Trindade et al. [25] 2016 USA
Case series 1 1. Barrett‘s esophagus 2. Stricture
Dilation of stricture
Surveillance 1. Barrett‘s esophagus 2. stricture
No suspicious regions identified
1. ISM 2. LLA 3. Irregular surface
Targeted HGD
1 Barrett‘s esophagus
None Surveillance Barrett‘s esophagus
No suspicious regions identified
1. LLA 2. ISM
Targeted LGD
1 Barrett‘s esophagus
None Surveillance Barrett‘s esophagus
No suspicious regions identified
1. LLA 2. ISM 3. AG
Targeted LGD
1 Barrett‘s esophagus
None Surveillance Barrett‘s esophagus
No suspicious regions identified
1. LLA 2. AG
Targeted LGD
1 1. Barrett‘s esophagus 2. LGD
None Surveillance Barrett‘s esophagus
No suspicious regions identified
AG Targeted HGD
1 1. Barrett‘s esophagus 2. Random biopsies showed IMC
None Surveillance Barrett‘s esophagus
No suspicious regions identified
1.LLA 2. AG 3. HO
Targeted IMC
Benjamin et al. [26] 2016 USA
Case Series 1 IMC None Therapeutic Performed but NA
NA HO suggestive of IMC
1. Targeted 2. Guided EMR
IMC
1 LGD RFA Surveillance Performed but NA
NA Glands in the epithelium suggesting BB
Random No metaplasia
1 LGD RFA Surveillance Performed but NA
NA Glands in the epithelium suggesting BB
Random No metaplasia
1 HGD RFA Surveillance Performed but NA
NA Normal Random No metaplasia
1 HGD 1. RFA 2. EMR 3. PDT
Surveillance Performed but NA
NA Glands in the epithelium suggesting BB
Random No metaplasia
1 LGD None Therapeutic Performed but NA
NA Dysplasia None Not applicable
1 HGD RFA Surveillance Performed but NA
NA Normal Random No metaplasia
1 IMC 1. RFA 2. EMR
Surveillance Performed but NA
NA Normal Targeted IMC

294 Jain et al
J Gastrointestin Liver Dis, September 2017 Vol. 26 No 3: 291-297
Table I (continued)
Author/ Year/ Location
Study type
No of subjects
Previous diagnosis
Previous treatment
Current indication
White light endoscopy (WLE)
Narrow Band Imaging (NBI)
Volumetric Laser Endo-microscopy (VLE)
Biopsy type
Histo-pathology
1 HGD RFA Surveillance Performed but NA
NA Glands in the epithelium suggesting BB
Random No metaplasia
Legget et al. [27] 2016 USA
Case Report
1 IMC EMR and RFA
Surveillance No suspicious regions identified
Not performed
1. Increased signal intensity 2. Numerous atypical appearing glands and dilated ducts
Mapping Moderate to poorly differentiated IMC invading into the lamina propria and muscularis mucosa
Atkinson et al. [28] 2016 USA
Case report
1 Barrett‘s esophagus
NA Surveillance No suspicious regions identified
No suspicious regions identified
2 regions with-1. Lack of regular striations in architecture 2. Jagged shaped ducts suggestive of glandular atypia 3. Hetero-geneous signal intensity consistent with irregular nuclei
Targeted 1. HGD with focal IMC 2. HGD with papillary IMC
Trindade et al. [29] 2015 USA
Case Report
1 Long segment Barrett‘s esophagus
NA NA 7 cm segment of flat salmon-colored mucosa
No suspicious regions identified
1. LLA in the entire Barrett‘s esophagus segment 2. Focal area of atypical mucosal glands
Targeted HGD
AG: atypical glands; BB: Buried Barrett’s; EAC: Esophageal adenocarcinoma; EDS: Evans Dysplasia Score; EMR: Endoscopic Mucosal Resection; HGD: High grade dysplasia; HO: homogeneous scattering; IMC: Intra-mucosal adenocarcinoma; ISM: inverted surface maturation; LGD: Low grade dysplasia; LLA: Loss of layered architecture; NA: date not available; RFA: Radiofrequency ablation; PDT: photodynamic therapy; pts: patients; RFA: radiofrequency ablation.
The vast majority of SGS found in this study did not correspond to BB. The authors cited low prevalence of BB in their study population and meticulous treatment of BE as the reason for this discrepancy. Overall, in this study, the correlation between VLE and histology was accurate only in 29.4% (5/17) of the cases [24]. Trindade et al. report a case series of 6 patients with long segment BE who underwent WLE, NBI followed by VLE within 6 months [25]. In 5 out of 6 patients VLE was performed for surveillance which resulted in upstaging of their disease to dysplastic BE that prompted ablative therapies. The 6th patient had IMC that was re-confirmed using VLE, which showed homogeneous scattering and washout suggestive of cancer. Overall, in this study, the correlation between VLE and histology was accurate in 100% (6/6) of the cases [25]. Benjamin et al. reported 9 cases (BE with dysplasia - 7/9; IMC - 2/9) [26]: 6 out of 7 patients with dysplastic BE had post ablation follow-up and 1/7 had no prior treatment. In 4/6 cases, VLE showed BB but the targeted biopsy failed to show any metaplasia; in 1/6 cases, VLE showed IMC which was consistent with biopsy; in 1/6 cases, VLE was normal, consistent with biopsy. One patient with known IMC who had not been previously treated underwent targeted biopsy and guided EMR. Volumetric laser endomicroscopy findings and histopathology were consistent for IMC in this patient.
However, another patient with IMC who had undergone RFA previously was found to have normal VLE while histopathology showed IMC. Further details for the discrepancy have not been provided in the study. Overall, in this study, the correlation between VLE and histology was accurate only in 37.5% (3/8) of the cases [26]. Leggett et al. reported a case of IMC which was treated by RFA and EMR [27]. The patient surveillance biopsies (one year post treatment) showed recurrence of sub-squamous IMC for which repeat EMR was performed. Volumetric laser endomicroscopy on ex-vivo specimen showed increased signal intensity with atypical glands and dilated ducts under the squamous epithelium. Histopathology confirmed moderate to poorly differentiated IMC [27]. Atkinson et al. described a case of BE in which VLE identified two areas of IMC that appeared normal on high magnification NBI [28]. The features of IMC on VLE were jagged shaped ducts suggestive of glandular atypia and heterogeneous signal intensity consistent with irregular nuclei. This prompted EMR and histopathology showed two areas of HGD with focal IMC and HGD with papillary IMC [28].
Trindade et al. report a case of long segment BE. High definition WLE showed a 7cm segment of salmon colored mucosa, NBI was normal and VLE showed a focal area of atypical mucosal glands that was confirmed on histology to
Volumetric laser endomicroscopy for Barrett’s 295
J Gastrointestin Liver Dis, September 2017 Vol. 26 No 3: 291-297
be high grade dysplasia [29]. In addition, the whole segment of BE appeared as loss of layered architecture on VLE. In the
case reports by Leggett et al. [27], Atkinson et al. [28] and Trindade et al. [29], VLE findings correlated 100% with the histologic findings.
In summary, we reviewed 7 studies with a total of 62 subjects who underwent VLE. Of 34 patients with available data, VLE correlated with histology in 17 subjects (50%). Volumetric laser endomicroscopy missed the underlying diagnosis in one subject (2.9%) and led to inadvertent biopsy in 16 patients (47.1%). It led or would have led to upstaging of disease in 11 subjects (32.4%). In our cohort, the sensitivity, specificity, positive predictive value and negative predictive value of VLE for diagnosis of dysplasia, BB or IMC was 92.3%, 23.8%, 42.9% and 83.3%, respectively.
Inter-observer agreementLeggett et al. used three gastroenterologists with experience
in BE as raters. Each of the rater was trained with a 30 minute presentation [23]. Each rater was then tested and had to score more than 85% to be considered eligible to score VLE images by using OCT-SI and VLE-DA score. Inter-rater agreement was fair for OCT-SI (kappa 0.39) and substantial for VLE-DA (kappa 0.83) [23]. In another study, overall agreement among
Table II. Evans dysplasia score
Parameter Score
A. Surface maturation
Surface OCT signal weaker than subsurface OCT signal 0
Surface OCT signal equivalent to subsurface OCT signal 1
Surface OCT signal stronger than subsurface OCT signal 2
B. Gland architecture
No irregularity, normal-appearing glandular architecture; minimal number of smooth dilated glands
0
Mild irregularity, glands smaller and more densely packed or large and irregularly shaped; dilated glands more frequent and closely spaced
1
Moderate/severe irregularity, glands branching and budding; dilated glands highly asymmetric or containing debris within the gland lumen
2
For each image, the surface maturation and gland architecture scores were summed to establish a dysplasia index
OCT- Optical Coherence Tomography
Fig. 1. a) and b) VLE and corresponding histopathology image for Barrett’s esophagus, negative for dysplasia (EDS- 0).
Fig. 2. a) and b) VLE and corresponding histopathology image for Barrett’s esophagus, indefinite for dysplasia (EDS- 2).
Fig. 3. a) and b) VLE and corresponding histopathology image for Barrett’s esophagus, low/high grade for dysplasia (EDS- 3).

296 Jain et al
J Gastrointestin Liver Dis, September 2017 Vol. 26 No 3: 291-297
8 high volume users from different academic centers in the United States was almost perfect (kappa 0.81, CI 0.79- 0.83) [31]. The study further categorized the results based on the diagnosis. For esophageal squamous (kappa 0.95) and gastric cardia (kappa 0.86) the agreement was almost perfect. For non-neoplastic BE and neoplastic BE, the agreement was strong (kappa 0.66 and 0.79, respectively) [31].
ComplicationsNo complications were noted in any of the studies.
CONCLUSION
Our cohort size being low restricts our ability to draw strong conclusions. High sensitivity (92.3%) and NPV (83.3%) do give gastroenterologists more confidence during follow-up with observation alone or making treatment decisions. It also help to reduce patient anxiety. Low specificity (23.8%) does lead to a high number of biopsies, which are likely less than non targeted biopsies. Refinement of diagnostic criteria on VLE imaging of patients with BE for diagnosis of BB, dysplasia and IMC may help to improve the above discussed pitfalls.
Conflicts of interest: None of the authors has any conflicts of interest.
Funding: No grant or funding source was involved in writing up the review article.
Authors’ contribution: D.J. contributed to literature review, data collection, interpretation of data and drafting of the manuscript. S.F. contributed in acquisition of data and drafting of the manuscript. S.J. contributed to literature review, histopathology images and revision of the manuscript. S.S. contributed to literature review and critical revision of the manuscript for important intellectual content.
REFERENCES
1. Rastogi A, Puli S, El-Serag HB, Bansal A, Wani S, Sharma P. Incidence of esophageal adenocarcinoma in patients with Barrett’s esophagus and high-grade dysplasia: a meta-analysis. Gastrointest Endosc 2008;67:394–398. doi:10.1016/j.gie.2007.07.019
2. Sharma P, Falk GW, Weston AP, Reker D, Johnston M, Sampliner RE. Dysplasia and cancer in a large multicenter cohort of patients with Barrett’s esophagus. Clin Gastroenterol Hepatol 2006;4:566–572. doi:10.1016/j.cgh.2006.03.001
3. Shakhatreh MH, Duan Z, Kramer J, et al. The incidence of esophageal adenocarcinoma in a national veterans cohort with Barrett’s esophagus. Am J Gastroenterol 2014;109:1862-1868. doi:10.1038/ajg.2014.324
4. Desai TK, Krishnan K, Samala N, et al. The incidence of oesophageal adenocarcinoma in non-dysplastic Barrett’s oesophagus: a meta-analysis. Gut 2012;61:970-976. doi:10.1136/gutjnl-2011-300730
5. Bhat S, Coleman HG, Yousef F, et al. Risk of malignant progression in Barrett’s esophagus patients: results from a large population-based study. J Natl Cancer Inst 2011;103:1049-1057. doi:10.1093/jnci/djr203
6. Hvid-Jensen F, Pedersen L, Drewes AM, Sorensen HT, Funch-Jensen P. Incidence of adenocarcinoma among patients with Barrett’s esophagus. N Engl J Med 2011;365:1375-1383. doi:10.1056/NEJMoa1103042
7. Pohl H, Sirovich B, Welch HG. Esophageal adenocarcinoma incidence: are we reaching the peak? Cancer Epidemiol Biomarkers Prev 2010;19:1468-1470. doi:10.1158/1055-9965.EPI-10-0012
8. Thrift AP, Whiteman DC. The incidence of esophageal adenocarcinoma continues to rise: analysis of period and birth cohort effects on recent trends. Ann Oncol 2012;23:3155-3162. doi:10.1093/annonc/mds181
9. Spechler SJ. Barrett esophagus and risk of esophageal cancer: a clinical review. JAMA 2013;310:627-636. doi:10.1001/jama.2013.226450
10. Shaheen NJ, Falk GW, Iyer PG, Gerson LB; American College of Gastroenterology. ACG Clinical Guideline: Diagnosis and Management
Fig. 4. a) and b) VLE and corresponding histopathology image for Barrett’s esophagus with intramucosal carcinoma (EDS- 3).
Fig. 5. a) and b) VLE and corresponding histopathology image for Barrett’s esophagus with adenocarcinoma (EDS- 2).

Volumetric laser endomicroscopy for Barrett’s 297
J Gastrointestin Liver Dis, September 2017 Vol. 26 No 3: 291-297
of Barrett’s Esophagus. Am J Gastroenterol 2016; 111:30-50. doi:10.1038/ajg.2015.322
11. Reid BJ, Weinstein WM, Lewin KJ, et al. Endoscopic biopsy can detect high-grade dysplasia or early adenocarcinoma in Barrett’s esophagus without grossly recognizable neoplastic lesions. Gastroenterology 1988;94:81-90. doi:10.1016/0016-5085(88)90613-0
12. Cameron AJ, Carpenter HA. Barrett’s esophagus, high-grade dysplasia, and early adenocarcinoma: a pathological study. Am J Gastroenterol 1997;92:586-591.
13. Konda VJ, Ross AS, Ferguson MK, et al. Is the risk of concomitant invasive esophageal cancer in high-grade dysplasia in Barrett’s esophagus overestimated? Clin Gastroenterol Hepatol 2008; 6:159-164. doi:10.1016/j.cgh.2007.09.013
14. Nasr JY, Schoen RE. Prevalence of adenocarcinoma at esophagectomy for Barrett’s esophagus with high grade dysplasia. J Gastrointest Oncol 2011; 2:34-38. doi:10.3978/j.issn.2078-6891.2010.027
15. Levine DS, Haggitt RC, Blount PL, Rabinovitch PS, Rusch VW, Reid BJ. An endoscopic biopsy protocol can differentiate high-grade dysplasia from early adenocarcinoma in Barrett’s esophagus. Gastroenterology 1993;105:40-50. doi:10.1016/0016-5085(93)90008-Z
16. Falk GW, Rice TW, Goldblum JR, Richter JE. Jumbo biopsy forceps protocol still misses unsuspected cancer in Barrett’s esophagus with high-grade dysplasia. Gastrointest Endosc 1999;49:170-176. doi:10.1016/S0016-5107(99)70482-7
17. Abela JE, Going JJ, Mackenzie JF, McKernan M, O’Mahoney S, Stuart RC. Systematic four-quadrant biopsy detects Barrett’s dysplasia in more patients than nonsystematic biopsy. Am J Gastroenterol 2008; 103:850-855. doi:10.1111/j.1572-0241.2007.01746.x
18. Boerwinkel DF, Swager AF, Curvers WL, Bergman JJ. The clinical consequences of advanced imaging techniques in Barrett’s esophagus. Gastroenterology 2014;146:622-629. doi:10.1053/j.gastro.2014.01.007
19. Sharma P. Clinical practice. Barrett’s esophagus. N Engl J Med 2009;361:2548-2456. doi:10.1056/NEJMcp0902173
20. Qumseya BJ, Wang H, Badie N, et al. Advanced imaging technologies increase detection of dysplasia and neoplasia in patients with Barrett’s esophagus: a meta-analysis and systematic review. Clin Gastroenterol Hepatol 2013;11:1562-1570.e1-2. doi:10.1016/j.cgh.2013.06.017
21. Sauk J, Coron E, Kava L, et al. Interobserver agreement for the detection of Barrett’s esophagus with optical frequency domain imaging. Dig Dis Sci 2013;58:2261-2265. doi:10.1007/s10620-013-2625-x
22. Evans JA, Poneros JM, Bouma BE, et al. Optical coherence tomography to identify intramucosal carcinoma and high-grade dysplasia in Barrett’s esophagus. Clin Gastroenterol Hepatol 2006;4:38-43. doi:10.1016/S1542-3565(05)00746-9
23. Leggett CL, Gorospe EC, Chan DK, et al. Comparative diagnostic performance of volumetric laser endomicroscopy and confocal laser endomicroscopy in the detection of dysplasia associated with Barrett’s esophagus. Gastrointest Endosc 2016;83:880-888.e2. doi:10.1016/j.gie.2015.08.050
24. Swager AF, Boerwinkel DF, de Bruin DM, et al. Detection of buried Barrett’s glands after radiofrequency ablation with volumetric laser endomicroscopy. Gastrointest Endosc 2016;83:80–88. doi:10.1016/j.gie.2015.05.028
25. Trindade AJ, George BJ, Berkowitz J, Sejpal DV, McKinley MJ. Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment Barrett’s esophagus. Endosc Int Open 2016;4:E318–E322. doi:10.1055/s-0042-101409
26. Benjamin T, Shakya S, Thota PN. Feasibility of volumetric laser endomicroscopy in Barrett’s esophagus with dysplasia and in post-ablation surveillance. J Gastrointestin Liver Dis 2016;25:407-408. doi:10.15403/jgld.2014.1121.253.brt
27. Leggett C, Gorospe E, Owens VL, Anderson M, Lutzke L, Wang KX. Volumetric laser endomicroscopy detects subsquamous Barrett’s adenocarcinoma. Am J Gastroenterol 2014;109:298–299. doi:10.1038/ajg.2013.422
28. Atkinson C, Singh S, Fisichella PM. Volumetric laser endomicroscopy in the detection of neoplastic lesions of the esophagus. Dig Liver Dis 2016;48:692. doi:10.1016/j.dld.2016.02.013
29. Trindade AJ, Vamadevan AS, Sejpal DV. Finding a needle in a haystack: use of volumetric laser endomicroscopy in targeting focal dysplasia in long-segment Barrett’s esophagus. Gastrointest Endosc 2015;82:756. doi:10.1016/j.gie.2015.03.1984
30. Evans JA, Poneros JM, Bouma BE, et al. Optical coherence tomography to identify intramucosal carcinoma and high-grade dysplasia in Barrett’s esophagus. Clin Gastroenterol Hepatol 2006;4:38-43. doi:10.1016/S1542-3565(05)00746-9
31. Trindade AJ, Inamdar S, Smith MS, et al. Volumetric laser endomicroscopy in Barrett’s esophagus: interobserver agreement for interpretation of Barrett’s esophagus and associated neoplasia among high-frequency users. Gastrointest Endosc 2017;86:133-139. doi:10.1016/j.gie.2016.11.026