volume 29, issue 6 march 2014 - university of florida
TRANSCRIPT

PharmaNote Volume 29 Issue 6 March 2014 1
ajordepressivedisorder(MDD)isacom-monandprevailingmentaldisorderthataffectsanindividual’soverallhealth,qualityoflifeandproductivity.Thean-
nualandlifetimeprevalenceofMDDinUnitedStatesis6.7%and16.5%oftheadultpopulation,respectively,and50%to80%willexperiencean-otherdepressiveepisode.1,2MDDalsocarriesasigni icanteconomicburdeninUnitedStates,con-tributing$83.1billioninhealthcareandproduc-tivitycostsin2000.3Theexactpathophysiologyisstillunknownbutlikelymulti-factorialandasso-ciatedwithdifferentneurotransmitterpathways.4
Longtermtreatmentwithantidepressantscanreducereoccurrenceupto70%.5However,upto40%ofaffectedindividualsdonotreceivetreatment.6ForindividualsreceivingtreatmentforMDDtherearemanyoptions.Pharmacologictreatmentoptionsincludeserotonin-norepinephrinereuptakeinhibitors(SNRIs),se-lectiveserotoninreuptakeinhibitors(SSRIs),ser-otoninmodulators,atypicalantidepressants,monoamineoxidaseinhibitorsandtricyclicanti-depressants.7Inspiteoftheavailableoptions,MDDcontinuestobedif iculttotreat.Majorob-staclesincludedelayedtherapeuticeffect,highnon-responserateduetoheterogeneoustreat-mentresponses,adverseeffects,andconsequent
lowcompliance.8Inresponsetothesetreatmentissuesandamultifactorialpathophysiology,new-erantidepressantstargetdifferentbutcomple-mentarytherapeuticmechanismofactions.
Vortioxetine(Brintellixa)isoneofthenewmulti-modalantidepressants.OnSeptember30,2013,theFDAapprovedvortioxetineformajordepressivedisorderinadults.Itwasjointlymar-ketedbyLundbeckandTakedaPharmaceuticalsIncorporated.Theobjectivesofthispaperaretoreviewthepharmacology,pharmacokinetics,per-tinentclinictrials,safetyanddosingofvortiox-etine.
P P
VortioxetineisaSSRIthatbindstothepre-
synapticserotoninreuptakesite,increasingthelevelofserotonin(5-HT)intheneuronalsynapse,aswellasselectivelybindingtoavarietyofotherserotoninreceptors.Itselectivelybindstoandactsasanantagonistto5-HT3,5-HT1D,and5-HT7receptors,partialagonistto5-HT1Breceptors,andagonistto5-HT1Areceptors(Table1).8Althougheachserotoninreceptorsubtypeisassociatedwithdifferentfunctions,theclinicaleffectsofthesereceptoractivitymodulationsinvortiox-etinearestillunknown(Table2).9,10Its5-HT1A
Volume 29, Issue 6 March 2014
®
Vortioxetine(Brintellix®):AReview
Qian Ya Lensa Zeng, PharmD Candidate
I T I :
V (B ®):AR
A ®( ):AR
M

C T
VortioxetinewasgrantedapprovalintheUnitedStatesbasedonsixshort-termtrialsandonemaintenancestudyinadultpatientswithDi-agnosticandStatisticalManualofMentalDisor-ders,FourthEdition,TextRevision(DSM-IV-TR)majordepressivedisorder.9,13,17-21Thesetrialswererandomized,multi-center,double-blinded,placebo-controlled, ixed-dosetrials.Approxi-matelyhalfofthesestudieswerepresentedasab-stractsattheAmericanPsychiatricAssociationannualmeetingandhavenotyetbeenpublishedorpeer-reviewed.Theexclusioncriteriavariedbetweenstudiesbutgenerallyexcludedpartici-pantswithahistoryofapsychiatric,neurologic,orsubstanceabusedisorderbesidesdepression,clinicallysigni icantmedicalcomorbidities,con-sideredatriskofsuicidalbehavior,
agonistactivitymaysupplementtheantidepres-santactivitysimilartotheproposedmechanismforbuspironeandvilazodone.9,11,12In-vivostud-iesfoundvortioxetinewasassociatedwithin-creasedlevelsotherneurotransmitters,suchasdopamine,norepinephrine,acetylcholineandhis-tamine,inadditiontoserotonin.13Vortioxetineiscurrentlybeinginvestigatedforitsanxiolyticandpotentialprocognitiveeffects,whichmaybeduetothereceptoractivitymodulations.
Inclinicaltrials,vortioxetinedisplayedalineardose-responserelationshipwithahalf-lifeof66hours.Therelativelylonghalf-lifeallowsoncedailydosingandmaypossiblyreducethereboundandwithdrawaleffectsfrommissingdosesorstoppingthedrug.Afteroraladministra-tion,peakplasmaconcentrationswereachievedin7to11hoursandvortioxetinedisplayed75%bioavailability.Sincefooddidnothaveanob-servedeffect,vortioxetinecanbetakenwithoutregardstofood.9
VortioxetineisprimarilymetabolizedbythecytochromeP450(CYP)pathwayintheliver.AlthoughvortioxetineisasubstrateformanyCYPenzymes,CYP2D6istheprimaryenzyme,whichmetabolizesvortioxetinetoapharmacologicallyinactivemetabolite.Thus,dosingadjustmentmaybenecessaryforpeopletakingstrongCYP2D6in-hibitorsorinducersconcomitantlywithvortiox-etine.9Noadjustmentisneededforrenalimpair-mentormildtomoderatehepaticimpairment.Nodoseadjustmentsareneededforagealthoughvortioxetinehasnotbeenstudiedinthepediatricpopulation.
Table1|ReceptorPro ilesfortheNewMulti‐ModalAntidepressantsComparedwithCom‐monlyUsedSSRIsandSNRIs8,23
Class Drug 5‐HT1A 5‐HT1B 5‐HT2C 5‐HT3 5‐HT7SERTinhibition
NETinhibition
DATinhibition
SSRI Citalopram +++
Fluoxetine ++ +++
SNRI Duloxetine +++ +++ +
Venlafaxine +++ ++
Vilazodone +++ +++
Vortioxetine +++ +++ +++ +++ +++
DAT:dopaminetransporter;NET:norepinephrinetransporter;SERT:serotonintransporter;+:weakaf inity;++:moder-ateaf inity;+++:strongaf inity.AdaptedfromRichelsonetal.8
Multi‐modal
Table 2 | Loca on and Clinically Relevant Func-on of Selected Serotonin Subtype Receptors10
Receptor Subtype
Loca on Func on
5-HT1A CNS Neuronal inhibi on, behavioral effects (sleep, feeding, thermoregula on, and anxiety)
CNS Presynap c inhibi on, behavioral effects
Vascular Pulmonary vasoconstric on
5-HT1D Unknown Unknown
5-HT3 GI tract Sensory and enteric nerves, emesis
5-HT7 CNS, blood vessels, GI tract
Unknown
5‐HT: serotonin; CNS: central nervous system; GI: Gastroin‐tes nal. Adapted from Mohammad‐Zadeh et al.10
5-HT1B
PharmaNote Volume 29 Issue 6 March 2014 2

mild-to-moderatedepressionortreatment-resistantdepression.ThemeanbaselineMADRSorHDRS-24scoreacrossallthesixshort-termtrialswasapproximately30,re lectingahighmoderatetoseveredepressionpatientpopula-tion.14,15Theprimaryendpointofallthestudieswaschangeintotalscoreofavalidateddepres-sionscalefrombaselinecomparedtoplacebo.AllthestudiesusedMontgomery-AsbergDepressionRatingScale(MADRS)excepttwostudiesusedHamiltonDepressionScale(HDRS-24).AlthoughHDRS-24hasbeenmorecommonlyusedinclini-caltrials,thereisahighcorrelationbetweenthetwoscales.16Forbothscales,ahigherscoreisas-sociatedwithincreasedseverity.
Fiveoftheshort-termclinicaltrialswereconductedinadultsbetweentheagesof18to75yearsdiagnosedwithMDD(Table3).17-21Thesetrialswereapproximately6to8weekslongandthreeofthe ivestudieswereconductedoutsideoftheUnitedStatesandmostlyinEurope.Collec-tively,theparticipantswererandomizedtooneofthetreatmentgroups(vortioxetine5mg,10mg,15mgor20mg)orplacebooncedaily.Partici-pantsassignedto15mgor20mgweretitratedfrom10mgwithin1week.AlvarezetalandBou-lengeretalusedvenlafaxineXR225mgdailyastheactivecontrolforassaysensitivitytovalidatetheir indings.16,17Itisunknownwhethertheoth-erthreetrialsusedanactivecontrolsincetheyhavenotbeenpublished.Ineachofthe ivetrials,atleastoneofthevortioxetinearmshadstatisti-callysigni icantchangesindepressionscorescomparedtoplacebo(Table3).Ofnote,thestatis-ticallysigni icantdifferencesindepressionscorefromplaceborangedfrom-4.1to-7.1inthenon-USstudiesand-2.8to-3.6intheUSstudies.Thecauseandsigni icanceofthenon-USstudiescon-sistentlyachievingahigherreductioninseverityscoreshavenotbeendetermined.Possiblerea-sonsaredifferencesincompliance,reportingre-sponses,anddifferencesinweightbetweenEuro-peanandAmericanpopulations.
Katonaetalconductedan8-week,multi-centertrialin453elderlypatientswithMDDwhorangedbetween64and88yearsoldinsevencountries,includingtheUnitedStates.Partici-pantswererandomlyassignedtovortioxetine5mg,placebo,orduloxetine60mg,whichwasthe
activecontrol.13Participantswereconsideredre-spondersiftheyhad50%orgreaterreductionintotalHDRS-24scoreatendpointcomparedtotheirbaselinescore.Signi icantlymorepartici-pantsinthevortioxetinegroupwereresponderscomparedtoplacebo(53.2%versus35.2%,P<0.05)(Table3).Nauseawasthesolesideeffectsigni icantlymoreprevalentinthetreatmentarmcomparedtoplacebo(21.8%versus8.3%,P<0.01).Inaddition,cognitiveeffectsindependentoftheantidepressanteffectwereexploredbyas-sessingchangesinscoresforReyAuditoryVerbalLearningTest(RAVLT)andTheDigitSymbolSub-stitutionTest(DSST).Bothduloxetineandvorti-oxetinewereassociatedwithanimprovementinverballearningbutonlyvortioxetinewasassoci-atedwithanimprovementinmemoryandpro-cessingspeedcomparedtoplacebo.Theinvesti-gatorsconcludedthatvortioxetineisbothsafeandef icaciousinelderlypatientsandmayhavepro-cognitiveeffects.
Inadditiontotheshort-termclinicaltrials,a52-weekrelapsepreventionstudywasconduct-edtoassessthelongtermef icacyinpatientwithmoderatetosevereMDDandatleastonepriordepressiveepisode.22Severitywasre lectedinthemeanbaselineMADRStotalscoreof32.5.Thisstudywasconductedin17countries,butwasnotconductedintheUnitedStates.Thestudypopula-tionconsistedof396oftheinitial639partici-pantsbetweentheagesof18and75yearsthatwerediagnosedtobeinremissionbyendofanopen-label, lexibledosingacutetreatmentphase.Remissionwasde inedasaMADRStotalscoreof10orless.Theeligibleparticipantswererandom-izedtoreceiveindividualized ixedtreatmentdose(5mgor10mg)orplacebofor24to46weeks.Theprimaryoutcomewastimetorelapsewithinthe irst24weeksofthedouble-blindphasewhererelapsewasde inedasaMADRSscoreof22orgreater.Thetimetorelapsewastwiceaslongwithvortioxetinecomparedtopla-cebo(HR=2.01,p=0.0035).Therelapserateofthevortioxetinegroupwas13%comparedto26%oftheplacebogroup(p=0.0013).Thedis-continuationrateduetosideeffectswas8%intheopen-label, lexibledosingphasethatallowedeither5mgor10mgtreatmentdoses.Inthedou-ble-blindphase,thediscontinuationrateswere
PharmaNote Volume 29 Issue 6 March 2014 3

8%inthevortioxetinegroupand3%intheplace-bogroup.Theinvestigatorsconcludedvortiox-etinesigni icantlyreducestheriskofrecurrentdepressiveepisodescomparedtoplaceboandiswelltoleratedforlong-termuse.
Therearekeylimitationstothedatafromthesestudies.Althoughhavinganactivecontrolincreasesthevalidityoftheresults,noneofthestudieswerepoweredtodirectlycomparevorti-oxetinetotheactivecontrol.Moreimportantly,similartomostclinicaltrials,generalizabilityof
thedataislimitedsincethetrialsexcludedpa-tientsthatarerepresentativeofthegeneralpa-tientpopulationtreatedinclinicalpractice,suchastreatment-resistantpatientsandpatientswithmultiplecomorbidities.Inaddition,itisunclearofthesigni icanceofthevaryingresultsbetweennon-USpopulationandUS-population.FurtherstudiesconductedintheUSassessingvortiox-etineinpeoplewithtreatment-resistancedepres-sionorwhohaveotherconcomitantdisordersareneeded.
Table3|SummaryofPrimaryOutcomeResultsofthe6to8weekClinicalTrials9,13,17,18,19,20,21
ClinicalTrialLocation
TreatmentGroup Numberofpatients
PrimaryMeasureDepressionRatingScale
MeanBase‐lineScore
LSMeanChangefromBase‐line(SE)
Placebo‐subtractedDifference(95%CI)
Alvarezetal17Non‐USStudy
Vortioxetine5mg/day
Vortioxetine10mg/dayPlacebo
108
100105
MADRS 34.1(2.6)
34.0(2.8)33.9(2.7)
-20.4(1.0)
-20.2(1.0)-14.5(1.0)
-5.9
(-8.6,-3.2)
-5.7
(-8.5,-2.9)
Henigsbergetal18Non‐USStudy
Vortioxetine5mg/day
Vortioxetine10mg/day
Placebo
139
139
139
HAMD-24 32.2(5.0)
33.1(4.8)
32.7(4.4)
-15.4(0.7)
-16.2(0.8)
-11.3(0.7)
-4.1
(-6.2,-2.1)-4.9
(-7.0,-2.9)
Boulengeretal19Non‐USStudy
Vortioxetine15mg/day
Vortioxetine20mg/dayPlacebo
149
151158
MADRS 31.8(3.4)
31.2(3.4)31.5(3.6)
-17.2(0.8)
-18.8(0.8)-11.7(0.8)
-5.5
(-7.7,-3.4)
-7.1
(-9.2,-5.0)
Mahable‐shwarkaretal20USStudy
Vortioxetine15mg/day
Vortioxetine20mg/day
Placebo
145
147
153
MADRS 31.9(4.1)
32.0(4.4)
31.5(4.2)
-14.3(0.9)
-15.6(0.9)
-12.8(0.8)
-1.5
(-3.9,0.9)
-2.8
(-5.1,-0.4)
Jacobsenetal21USStudy
Vortioxetine10mg/day
Vortioxetine20mg/day
Placebo
154
148
155
MADRS 32.2(4.5)
32.5(4.3)
32.0(4.0)
-13.0(0.8)
-14.4(0.9)
-10.8(0.8)
-2.2
(-4.5,0.1)
-3.6
(-5.9,-1.4)
Katonaetal13USandNon‐USStudyElderly
Vortioxetine5mg/day
Placebo
155
145
HAMD-24 29.2(5.0)
29.1(5.1)
-13.7(0.7)
-10.3(0.8)
-3.3
(-5.3,-1.3)
AdaptedfromBrintellix(vortioxetine)packageinsert9
PharmaNote Volume 29 Issue 6 March 2014 4

A E D I
Manyofvortioxetine’sreportedadverseeffectsanddruginteractionsareexpected.Itsmostcommonsideeffectsaregastrointestinalandneurological,suchasnausea,diarrhea,consti-pation,dizzinessandabnormaldreams.OthercommonsideeffectsarelistedinTable4.9Ifpa-tientsexperienceintolerablesideeffects,lower-ingtheinitialdosemaybebene icial.
Ararebutserioussideeffectcharacteristicofallantidepressantsthatmodulateserotoninreuptakeisincreasedriskofsuicide.Short-termtrialsindicatethatonlyparticipantsyoungerthan24yearsoldtakingvortioxetinewereobservedtobeatrisk,butallpatientsshouldbecloselymoni-tored.9Otherserioussideeffectsthatrequiremonitoringincludehypersensitivity,angioedema,andmaniaorhypomania.Thus,patientsshouldbescreenedforriskofbipolardisorderpriortoinitiatingvoritioxetine.9Currentlyavailabledatasuggestsvortioxetineisweightneutral.Onlythemaleparticipantstakingvortioxetinereportedahigherincidenceofsexualdysfunctioncomparedtotheircounterpartstakingplacebo(Table5).9SimilartootherSSRIsandSNRIs,hyponatremiahasbeenreported;patientsconcomitantlytakingdiureticsandelderlypatientsmaybeathigherrisk.Nootherclinicalimportantchangesinlabor-atorytestsandvitalsigns,includingbloodpres-sureandheartrate,havebeenobserved.
Vortioxetinehassomekeydruginterac-tions.PatientsconcomitantlytakingNSAIDS,aspi-rin,oranticoagulantssuchaswarfarinareatin-creasedbleedingrisk.Vortioxetineuseiscontra-indicatedwiththefollowingmedicationsduetoanincreaseriskofserotoninsyndrome:MAOin-hibitors,linezolidandintravenousmethyleneblue.Cautionshouldbeexercisedinpatientscon-comitantlytakingvortioxetineandserotonergicagents;bothmedicationsshouldbediscontinuedifserotoninsyndromedevelops.Sincevortiox-etineisprimarilymetabolizedbytheCYP2D6en-zyme,itsserumdruglevelsmaychangewhentak-enwithmedicationsthatinduceorinhibitCYP2D6.Therecommendedmaximumdoseisreducedby50%to10mgdailyinknownCYP2D6poormetabolizersorpatientsconcomitantlytak-ingastrongCYP2D6inhibitor,suchasbupropion,
luoxetine,paroxetine,orquinidine.Ofnote,con-comitantuseof luoxetineorparoxetinewithvor-tioxetinemayincreaseriskofserotoninsyndromeinadditiontoserumvortioxetineconcentration.Conversely,adoseincreasemaybewarrantedinpatientstakingastrongCYP2C6inducer,suchasrifampin,carbamazepine,orphenytoin,forgreat-erthan14days.9
D
Itisrecommendedthatpatientsinitially
startwith10mgorallyoncedailywithoutregardstofoodandtitrateastolerated.Patientsshouldbetitrateddownto5mgdailyiftheyexperiencein-tolerablesideeffects.Themaximumrecommend-eddoseis20mgdaily.However,forpoorCYP2D6metabolizersorpatientsconcomitantlytakingastrongCYP2C6inhibitor,themaximumrecom-mendeddoseis10mgdaily.Doseincreasesupto
Table4|CommonAdverseReactionsOccur‐ringin≥2%ofPatientsTreatedwithanyVor‐tioxetineDoseandatLeast2%MoreFre‐quentlythanIncidenceinPlacebo‐treatedPa‐tientsinthe6to8WeekPlacebo‐ControlledStudies9
DoseofVortioxetine
5mgperday
10mgperday
15mgperday
20mgperday
N=1013(%)
N=699(%)
N=449(%)
N=455(%)
Gastrointestinaldisorders
Nausea 21 26 32 32
Diarrhea 7 7 10 7
Drymouth 7 7 6 8
Constipation 3 5 6 6
Vomiting 3 5 6 6
Flatulence 1 3 2 1
Nervoussystemdisorders
Dizziness 6 6 8 9
Psychiatricdisorders
Abnormaldreams
6 6 8 9
Pruritus 1 2 3 3
Skinandsubcutaneoustissuedisorders
PharmaNote Volume 29 Issue 6 March 2014 5

Jun;62(6):629-640.7. GelenbergAJ,FreemanMP,MarkowitzJC,etal.Practice
GuidelinefortheTreatmentofPatientsWithMajorDe-pressiveDisorder.3rded.Arlington,VA:AmericanPsy-chiatricAssociation;2010.AmericanPsychiatricAssoci-ation.
8. RichelsonE.Multi-modality:anewapproachforthetreatmentofmajordepressivedisorder.IntJNeuropsy-chopharmacol.2013July;16(6):1433–1442.
9. Brintellix(vortioxetine)packageinsert.Deer ield,IL:TakedaPharmacueticalsAmerica,Inc.;2013Sept.
10. Mohammad-Zadeh,L.F.,Moses,L.,Gwaltney-Brant,S.M.Serotonin:areview.JVetPharmacolTher.2008Jun;31(3):187-99.
11. Buspar(buspirone)packageinsert.Princeton,NJ:Bris-tol-MyersSquibbCompany;2003Nov.
12. Viibryd(vilazodone)packageinsert.St.Louis,MO;For-estPharmaceuticals,Inc.:2012Dec.
13. KatonaC,HansenT,OlsenCK.Arandomized,double-blind,placebo-controlled,duloxetine-referenced, ixed-dosestudycomparingtheef icacyandsafetyofLuAA21004inelderlypatientswithmajordepressivedis-order.IntClinPsychopharmacol.2012Jul;27(4):215-23.
14. FrankE,PrienRF,JarrettRB,KellerMB,KupferDJ,La-voriPW,RushAJ,WeissmanMM:Conceptualizationandrationaleforconsensusde initionsoftermsinmajordepressivedisorder.Remission,recovery,relapse,andrecurrence.ArchGenPsychiatry1991;48:851–5.
15. SnaithRP,HarropFM,NewbyPA,TealeC.GradescoresoftheMontgomery-Asbergdepressionandtheclinicalanxietyscales.BrJPsychiatry.1986;148:599–601.
16. FoodandDrugAdministration.DescriptionoftheHam-iltonDepressionRatingScale(HAMD)andtheMont-gomery-AsbergDepressionRatingScale(MADRS)http://www.fda.gov/ohrms/dockets/ac/07/brie ing/2007-4273b1_04-descriptionofmadrshamddepressionr%281%29.pdf.AccessedNovember172013.
17. AlvarezE,PerezV,DragheimM,LoftH,ArtigasF.Adou-ble-blind,randomized,placebo-controlled,activerefer-encestudyofLuAA21004inpatientswithmajorde-pressivedisorder.IntJNeuropsychopharmacol.2012Jun;15(5):589-600.
18. HenigsbergN,MahableshwarkarAR,JacobsenP,ChenY,ThaseME.Arandomized,double-blind,placebo-controlled8-weektrialoftheef icacyandtolerabilityofmultipledosesofLuAA21004inadultswithmajorde-pressivedisorder.JClinPsychiatry.2012;73:953-959.
19. BoulengerJP,LoftH,OlsenCK.Arandomized,double-blind,placebo-controlled,duloxetine-referencedstudyoftheef icacyandsafetyofvortioxetineinacutetreat-mentofMDD.Programandabstractsofthe166thAn-nualAmericanPsychiatricAssociationMeeting;May18-22,2013;SanFrancisco,California.PosterNR3-054.
20. MahableshwarkarAR,JacobsenPL,SerenkoM,ChenY,TrivediM.Arandomized,double-blind,parallelgroupstudycomparingtheef icacyandsafetyof2dosesofvortioxetineinadultswithmajordepressivedisorder.
threetimestheoriginaldosemaybeconsideredinpatientstakingastrongCYP2D6inducerforgreaterthan14days.Nodoseadjustmentsarerecommendedforgeriatricpatients,renalimpair-mentandmildtomoderatehepaticfailure.
S
Vortioxetineisanewmultimodalantide-
pressantindicatedforMDDinadults.InadditiontobeingaSSRI,vortioxetinehasmodulatingactiv-ityofavarietyofserotoninreceptors.Speci ically,itactsasanantagonistto5-HT3,5-HT1D,and5-HT7receptors,partialagonistat5-HT1Breceptors,andagonistat5-HT1Areceptorsbuttheclinicaleffectsremainsunknown.Itisanewoptionforacuteandlong-termtreatment.However,majori-tyoftheclinicaltrialsusedtosupportitsapprovalwereshort-term,conductedoutsidetheUnitedStatesandexcludedpatientsthatarecommonlyseeninclinicalpractice.Patientsshouldbestart-edon10mgdailyandcanbetitratedupto20mgdaily;somepatientsexperiencingsideeffectsmaybene itfromhavingtheirinitialdosereducedto5mgdaily.Vortioxetinecanbetakenwithoutre-gardtomealsandnodoseadjustmentsareneed-edforage,renalfunctionormildtomoderatehe-paticimpairment.However,thereispotentialfordruginteractions,patientstakingstrongCYP2D6inhibitorsorinducersmayrequiredoseadjust-ments.
R
1. KesslerRC,ChiuWT,DemlerO,etal.Prevalence,severi-
ty,andcomorbidityof12-monthDSM-IVdisordersintheNationalComorbiditySurveyReplication.ArchGenPsychiatry.2005;62(6):617–627.
2. BurcusaSL,IaconoWG.Riskforrecurrenceindepres-sion.ClinPsycholRev.2007;27:959–985.
3. GreenbergPE,KesslerRC,BirnbaumHG,LeongSA,LoweSW,etal.TheeconomicburdenofdepressionintheUnitedStates:howdiditchangebetween1990and2000?JClinPsychiatry.2003:64:1465–147.
4. BelmakerRH,AgamGMajorDepressiveDisorder.NEnglJMed.2008:358:55–68.
5. GeddesJR,CarneySM,DaviesC,etal.Relapsepreven-tionwithantidepressantdrugtreatmentindepressivedisorders:asystematicreview.Lancet.2003;361(9358):653–661.
6. WangPS,LaneM,OlfsonM,PincusHA,WellsKB,Kess-lerRC.TwelvemonthuseofmentalhealthservicesintheUnitedStates.ArchivesofGeneralPsychiatry.2005
PharmaNote Volume 29 Issue 6 March 2014 6

tion.Witheachadditionalmedicationaddedtotheregimen,thesideeffectpro ileincreases,withaboutaquarterofallepilepticpatientsexperienc-ingunnecessarysideeffects.6Inadequatecontrolandsideeffectscontributetoaneconomicandsocialburdenthatmayjeopardizedthequalityoflifeformanypatients.7Thus,researcherscontin-uetostrivefordevelopingAEDsthatpossessesbothhighef icacyandtolerability.
Eslicarbazepineacetate(ESL),manufac-turedbySunovionPharmaceuticalsandmarketedunderthetrademarknameAptiom®,wasap-provedbytheFDAonNovember8th,2013asad-junctivetreatmentforpartial-onsetseizures.8Thisarticlewilldiscussthepharmacology,phar-macokinetics,ef icacy,dosing,andsafetyofESL.
P P
Eslicarbazepineacetatepossessesafew
uniquecharacteristicswhencomparedtootherAEDs.Thoughtheexactmechanismofactionisunknown,ESLisbelievedtocompetitivelyblockinactivehigh-frequencyvoltage-gatedsodiumchannelsatreceptorsite2.Thisprolongsthein-activationperiod,therebyreducingtheabilityofneuronsto ireathighfrequencies.Inaddition,ESLismoreselectiveforrapidly iringneuronsversusrestingneurons,showingathreefoldloweraf inityforrestingsodiumchannelswhencom-paredtocarbamazepine(CBZ).ESLisstructurallysimilartoCBZandoxcarbazepine(OXC)becauseitsharesadibenzazepinenucleus.9However,un-likeCBZ,ESLisnotmetabolizedtoatoxicepoxideduetothemoleculardifferenceofESLatthe10,11-positiononthemolecule.Becauseofthismo-leculardifference,ESLhasmodestenzymeinduc-ingpropertiesand,unlikeCBZ,willnotinduceitsownmetabolism.Additionally,incontrasttoOXC,ESLisaprodrugmetabolizedintoasingleenanti-omerwhereasOXCismetabolizedtobothR-andS-licarbazepine.Thissingleenantiomerisbe-lievedtobemoreef icacious,possessfewersideeffects,andcrossthebloodbrainbarriermoreef icientlythantheR-licarbazepine.10
Table1providesasummaryofseveralim-portantpharmacokineticpropertiesofESL.Themetabolite,eslicarbazepine,isresponsibleforthepharmacologicalactivityofESL.Atdosesof400-1200mg/day,ESLhaslinear,dosedependent
Programandabstractsofthe166thAnnualAmericanPsychiatricAssociationMeeting;May18-22,2013;SanFrancisco,California.PosterNR9-02.
21. JacobsenPL,MahableshwarkarAR,SerenkoM,ChenY,TrivediM.Arandomized,double-blind,placebo-controlledstudyoftheef icacyandsafetyofvortiox-etine10mgand20mginadultswithmajordepressivedisorder.Programandabstractsofthe166thAnnualAmericanPsychiatricAssociationMeeting;May18-22,2013;SanFrancisco,California.PosterNR9-06.
22. BoulengerJP,LoftH,FloreaI.ArandomizedclinicalstudyofLuAA21004inthepreventionofrelapseinpatientswithmajordepressivedisorder.JPsychophar-macol.2012;26(11):1408–1416.
23. Prozac( luoxetine)packageinsert.EliLillyandCompa-ny.Indianaplis,IN;1987.
pilepsyisacommonneurologicaldisor-derthatimpactsthelivesofmany,withanage-adjustedincidenceof44per100,000andaprevalenceof6-8per
1000.1,2Thoughmanyoftheantiepilepticdrugshaveadvancedthetreatmentofepilepsy,manyindividualssufferfrominadequateseizurecontroland/orundesirablesideeffects.Epilepsyisdivid-edintotwocategories:generalizedandpartialseizures.Generalizedseizuresoccurinbothhemi-spheresofthebrainandusuallyresultsinalossofconsciousness.Conversely,partialepilepsyislocalizedtoonehemisphereofthebrain,doesnotleadtoalossofconsciousness,andaccountsfornearly60%ofpeoplewithepilepsy.Partialepi-lepsyencompassessimplepartialseizures,com-plexpartialseizures,andsecondarygeneralizedseizures.3,4
Seizuresarisefromavarietyofcomplexmechanismsthatarenotcompletelyunderstood.Alterationsinionchannels,genetics,andneuro-transmitterimbalancesarebelievedtocontributetothepathophysiologyofseizures.5Antiepilepticdrugs(AEDs)arethemainstayintreatmentforpartialseizures.However,approximately30%oftreatedpatientswithepilepsyhavesuboptimalcontrolandwillberequiredtotakebetween2-4concomitantmedicationstomanagethiscondi-
PharmaNote Volume 29 Issue 6 March 2014 7
Aptiom®(Eslicarbazepineacetate):
AReview John Chichetto, PharmD, Candidate
E
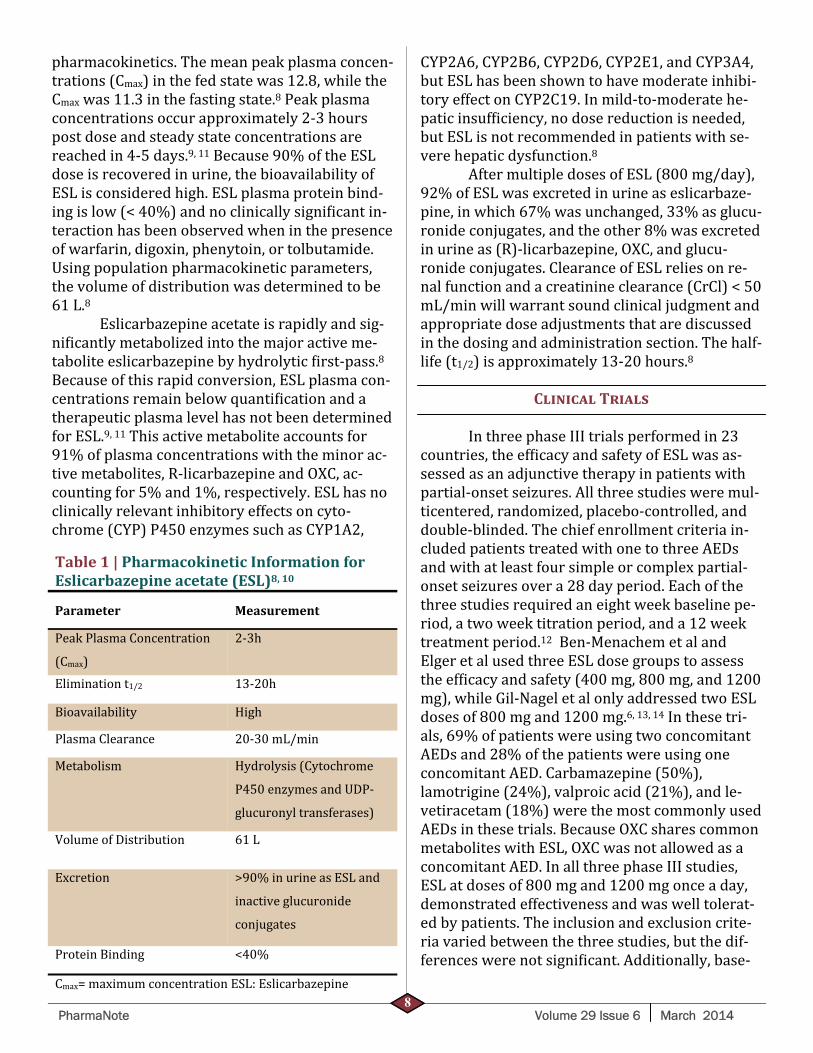
CYP2A6,CYP2B6,CYP2D6,CYP2E1,andCYP3A4,butESLhasbeenshowntohavemoderateinhibi-toryeffectonCYP2C19.Inmild-to-moderatehe-paticinsuf iciency,nodosereductionisneeded,butESLisnotrecommendedinpatientswithse-verehepaticdysfunction.8
AftermultipledosesofESL(800mg/day),92%ofESLwasexcretedinurineaseslicarbaze-pine,inwhich67%wasunchanged,33%asglucu-ronideconjugates,andtheother8%wasexcretedinurineas(R)-licarbazepine,OXC,andglucu-ronideconjugates.ClearanceofESLreliesonre-nalfunctionandacreatinineclearance(CrCl)<50mL/minwillwarrantsoundclinicaljudgmentandappropriatedoseadjustmentsthatarediscussedinthedosingandadministrationsection.Thehalf-life(t1/2)isapproximately13-20hours.8
C T
InthreephaseIIItrialsperformedin23
countries,theef icacyandsafetyofESLwasas-sessedasanadjunctivetherapyinpatientswithpartial-onsetseizures.Allthreestudiesweremul-ticentered,randomized,placebo-controlled,anddouble-blinded.Thechiefenrollmentcriteriain-cludedpatientstreatedwithonetothreeAEDsandwithatleastfoursimpleorcomplexpartial-onsetseizuresovera28dayperiod.Eachofthethreestudiesrequiredaneightweekbaselinepe-riod,atwoweektitrationperiod,anda12weektreatmentperiod.12Ben-MenachemetalandElgeretalusedthreeESLdosegroupstoassesstheef icacyandsafety(400mg,800mg,and1200mg),whileGil-NageletalonlyaddressedtwoESLdosesof800mgand1200mg.6,13,14Inthesetri-als,69%ofpatientswereusingtwoconcomitantAEDsand28%ofthepatientswereusingoneconcomitantAED.Carbamazepine(50%),lamotrigine(24%),valproicacid(21%),andle-vetiracetam(18%)werethemostcommonlyusedAEDsinthesetrials.BecauseOXCsharescommonmetaboliteswithESL,OXCwasnotallowedasaconcomitantAED.InallthreephaseIIIstudies,ESLatdosesof800mgand1200mgonceaday,demonstratedeffectivenessandwaswelltolerat-edbypatients.Theinclusionandexclusioncrite-riavariedbetweenthethreestudies,butthedif-ferenceswerenotsigni icant.Additionally,base-
pharmacokinetics.Themeanpeakplasmaconcen-trations(Cmax)inthefedstatewas12.8,whiletheCmaxwas11.3inthefastingstate.8Peakplasmaconcentrationsoccurapproximately2-3hourspostdoseandsteadystateconcentrationsarereachedin4-5days.9,11Because90%oftheESLdoseisrecoveredinurine,thebioavailabilityofESLisconsideredhigh.ESLplasmaproteinbind-ingislow(<40%)andnoclinicallysigni icantin-teractionhasbeenobservedwheninthepresenceofwarfarin,digoxin,phenytoin,ortolbutamide.Usingpopulationpharmacokineticparameters,thevolumeofdistributionwasdeterminedtobe61L.8
Eslicarbazepineacetateisrapidlyandsig-ni icantlymetabolizedintothemajoractiveme-taboliteeslicarbazepinebyhydrolytic irst-pass.8Becauseofthisrapidconversion,ESLplasmacon-centrationsremainbelowquanti icationandatherapeuticplasmalevelhasnotbeendeterminedforESL.9,11Thisactivemetaboliteaccountsfor91%ofplasmaconcentrationswiththeminorac-tivemetabolites,R-licarbazepineandOXC,ac-countingfor5%and1%,respectively.ESLhasnoclinicallyrelevantinhibitoryeffectsoncyto-chrome(CYP)P450enzymessuchasCYP1A2,
PharmaNote Volume 29 Issue 6 March 2014 8
Table1|PharmacokineticInformationforEslicarbazepineacetate(ESL)8,10
Parameter Measurement
PeakPlasmaConcentration
(Cmax)
2-3h
Eliminationt1/2 13-20h
Bioavailability High
PlasmaClearance 20-30mL/min
Metabolism Hydrolysis(Cytochrome
P450enzymesandUDP-
glucuronyltransferases)
VolumeofDistribution 61L
Excretion >90%inurineasESLand
inactiveglucuronide
conjugates
ProteinBinding <40%
Cmax=maximumconcentrationESL:Eslicarbazepine

linecharacteristicsdidnotdiffersigni icantlybe-tweenthetrials.12
Theprimaryef icacyendpointforallthreetrialswasseizurefrequencyduringthe12weekmaintenanceperiod,whilerelativereductioninseizurefrequency,andresponderrate(≥50%re-ductioninseizurefrequency)wereanalyzedassecondaryendpoints.Ef icacyendpointswereanalyzedusinganintentiontotreatanalysis,whichincludedallpatientsrandomizedandthatreceivedatleastonedoseofESL.AllthreetrialsassessedtheimpactofESLonreducingthenum-berofseizures,whilecontrollingforothervaria-blessuchasconcomitantAEDsandbaselinesei-zurefrequency.Secondaryendpointswereper-formedperprotocolandincludedallpatientsthatcompletedthestudy.12
Elgeretalrandomized402patients,ofwhich102patientswereassignedtotheplacebogroup,100patientswereassignedtoESL400mg/day,98patientswereassignedtoESL800mg/day,and102patientswereassignedtoESL1200mg/day.6Ofthe402patientsthatenteredthetreatmentphase,330(82%)completedthestudy.Ofthe72(18%)patientsthatwerelosttofollow-up,themostcommonreasonwasduetoadverseevents(AEs).Overthe12weektreat-mentphase,theseizurefrequencywasfoundtobesigni icantlylowerintheESL800mg/dayarm
(LeastSquare(LS)Mean5.66,p=0.0028)andintheESL1200mg/dayarm(LSMean5.35,p=0.0003),comparedtotheplacebogroup(LSMean7.64).TheESL400mg/dayarmandplace-bodidnothaveastatisticallysigni icantdifferentLSMean.TheLSMeanseizurefrequencywasad-justedperfourweektimeperiod.Theresponderrate(patientswith≥50%decreaseinseizurefre-quencies)wassigni icantlyhigherintheESL800mg/day(34%,p=0.0359)andintheESL1200mg/dayarm(43%,p=0.009)thanintheplacebogroup(20%).Theincidencesofmild-to-moderateAEsincreasedwithincreasingdoses,andthefrequencyofseriousAEswassimilaracrossallgroupsinthetrial.Theauthorsconclud-edthatboththeESL800mg/dayand1200mg/dayarewelltoleratedandeffectiveinpatientsthathaverefractorypartial-onsetseizures.6
Gil-Nageletalstudiedtheef icacyandsafetyofdailydosesofESL800mgand1200mgasadjunctivetreatmentinpatientswithpartial-onsetseizures.13Afteran8-weekbaselineperiod,253patientswererandomizedintothreearms.Theplacebogroupcontained88patients,theESL800mg/dayarmhad85participants,andtheESL1200mg/daygrouphad80patients.Afteratwoweektitrationperiod,patientsentereda12weekmaintenanceperiod.Thepopulationwasana-lyzedusinganintention-to-treatmethod.The
PharmaNote Volume 29 Issue 6 March 2014 9
Table2|SummaryofESLphaseIIITrials
Author/Year StudyDesignESLdose(mg/
day)ResponderRate(%)
MedianRela‐tiveRiskRe‐ductioninsei‐zurefrequen‐cy(%)
AuthorsConclu‐sion
Elgeretal.(2009)6
MC,DB,R,PC Placebo4008001200
20.023.034.043.0
16.026.036.045.0
ESL800and1200mg/daywelltoler-atedandeffective
Gil‐Nageletal.(2009)13
MC,DB,R,PC
Placebo8001200
22.634.537.7
17.037.941.9
800and1200mg/dayofESLeffectiveandwelltolerated
Ben‐Menachemetal.(2010)14
MC,DB,R,PC Placebo4008001200
13.017.040.037.1
0.818.732.632.8
ESL800and1200mg/daywelltoler-atedandeffective
DB:Double-blind;MC:Multicenter;R:Randomized;PC:Placebocontrolled;ESL:Eslicarbazepineacetate;Responderrate:percentageofpatientswith≥50%decreaseinseizurefrequency;

standardized(per4week)seizurefrequencywassigni icantlylowerforthe800mg/day(LSMean5.7,p=0.048)and1200mg/day(LSMean5.5,p=0.021)armswhencomparedtoplacebo(LSMean7.3).Theresponderratewas22.6%fortheplaceboarm,34.5%(p=0.106)forthe800mg/dayarm,and37.7%(p=0.020)inthe1200mg/dayarm.Theauthorsconcludedthat800mg/dayand1200mg/dayofESLareeffectiveandwelltolerated.13
Ben-MenachemetalcarriedoutatrialsimilartothatofElgeretal.6,14Afteran8-weekbaselineobservationalperiod,395ofthe503pa-tientsthatenteredthestudywererandomizedtoplacebo(n=100),ESL400mg/day(n=96),ESL800mg/day(n=101),or1200mg/day(n=98).Afteratwoweektitrationperiod,thepatientsen-tereda12-weektreatmentperiodfollowedbyatwoweekdiscontinuationphase.Thedatacollect-edwasanalyzedafterthe14weektreatmentpe-riodandthestandardizedseizurefrequency(per4weeks)wassigni icantlylowerintheESL800mg/day(LSMean7.1,p<0.001)andintheESL1200mg/day(LSMean7.4,p<0.001),comparedtotheplaceboarm.Therewasnostatisticallysig-ni icantdifferenceintheplaceboandESL400mg/daygroups.Inaddition,theresponderrateintheESL800mg/daygroup(40.0%,p<0.001)andintheESL1200mg/day(37.1,p<0.01)wassigni -icantlyhigherthantheplacebogroup.Likeprevi-
Table3|DruginteractionswithESLanddoseadjustments8,15
Drug EffectsofESLondrugEffectofdrugonESL
Doseadjustment
Carbamazepine None 21-33%de-creaseinAUC
MayneedanincreaseESLdose
Phenytoin Increase30-35%inAUC 21-33%de-creaseinAUC
MonitorphenytoinlevelsandmayneedanincreaseinESLdose
Phenobarbital None DecreaseAUC MayneedanincreaseinESLdose
Simvastatin Decrease41-61%inAUC None Increaseinsimvastatindosemayberequired
Rosuvastatin DecreaseinAUC None Increaseinrosuvastatindosemayberequired
Ethinylestradiol Decreaseof37%inAUC None Additionalcontraceptionshouldbeused
Levonorgestrel Decreaseof42%inAUC None Additionalcontraceptionshouldbeused
Warfarin Decreaseof23%in(S)-WarfarinAUC
None MonitorINRclosely
AUC:Areaunderthecurve
Table4|Combinedadversereactionsfromthreeclinicaltrials(Events≥2%ofpatientsinESL800mgand1200mgarms)8
Adversereaction
Placebo(%) ESL800mg ESL1200mg
Dizziness 9 20 28
Nausea 5 10 16
Somnolence 8 11 18
Headache 9 13 15
Diplopia 2 9 11
Vomiting 3 6 10
Fatigue 4 4 7
Ataxia 2 4 6
Blurredvision
1 6 5
Tremor 1 2 4
Vertigo 1 2 6
Rash 1 1 3
Hyperten‐sion
1 1 2
Hypo‐natremia
1 2 2
PharmaNote Volume 29 Issue 6 March 2014 10

ous indings,AEsincreasedwithincreasingdosesandthediscontinuationratesduetoAEswere3.0%(placebo),12.5%(400mg),18.8%(800mg),and26.5%(1200mg).ThemostcommonAEsweredizziness,somnolence,headache,nau-sea,anddiplopia.TheauthorsconcludedthattreatmentwithoncedailyESL800mgand1200mgarebothef icaciousandwelltolerated.14Table2summarizestheaforementionedtrials.
D I Manyofthedruginteractionsnotedhave
beenwithconcomitantuseofotherAEDs.Whenphenytoin(PHT)andESLaregivenconcomitant-ly,a30-35%increaseinPHTanda21-33%de-creaseinESLexposureisseen.Similarly,con-comitantlytakingCBZandESLleadstoanin-creaseinCBZplasmaconcentrationsandade-creaseinESLplasmaconcentrations.Therefore,thedoseofPHT,CBZ,andESLmayneedtobead-justedaccordingly.WhenusedconcomitantlywithenzymeinducingAEDs,suchasphenobarbi-talandprimidone,higherdosesofESLmaybeneeded.InteractionswithotherAEDs,suchasle-vetiracetam,valproicacid,andgabapentin,donotappeartobeclinicallyrelevant,notrequiringdoseadjustments.ESLcaninhibitCYP2C19,whichcancauseincreasedplasmaconcentrationsofdrugs,suchasomeprazole,clobazam,andphenytoin.ESLcaninduceCYP3A4,decreasingplasmaconcentrationsofagentsmetabolizedbythisCYPenzyme.Administrationofethyinyles-tradiol/levonorgestrelwithESLleadstoade-creaseof42%inethyinylestradiolanda37%de-creaseinlevonorgestrel.Thisinteractionappearstooccurinadosedependentfashion.Theclinical-lyrelevantinteractions,alongwithappropriatedosingrecommendations,aresummarizedinTa-ble4.15
A E
ESLappearstohaveafavorablesideeffectpro ile.InphaseIIIstudies,mostofthemildtomoderateAEsoccurredmainlyduringtheinitia-tionphaseofESL.Aftersixweeksoftreatment,nosigni icantdifferencesintheoccurrenceofAEswereevidentbetweenESL800mg,1200mg,and
placebogroups.AEsleadingtoattritionduringthetrialswere4.5%intheplaceboarm,8.7%intheESL400mgarm,11.6%intheESL800mgarm,and19.3%intheESL1200mgarm.4Gil-Nageletal,frompooleddata,concludedthat45.3%treatedwithESLreportedtreatmentrelat-edAEs,comparedto24.4%treatedwithplace-bo.12TheoccurrenceofsevereAEs,suchasSte-vens-JohnsonSyndrome,Toxicepidermalnecrol-ysis,andDRESS/MultiorganHypersensitivity,waslowandsimilarineachoftheESLtreatmentarms.Theincidenceofrashwas0.3%inplacebo,0.5%withESL400mg,1.1%withESL800mg,and3.2%withESL1200mg.Hyponatremia,de-inedbyNa+<125mmol/L,wasreportedinfourpatientsand<1%ofthetreatmentarmsexperi-encedbehavioralorpsychiatricAEs.4ThemostcommonAEs,suchasdizziness,nausea,somno-lence,andheadache,aresummarizedinTable4.14
D A
Eslicarbazepineacetatewillbeavailablein
200mg,400mg,600mg,and800mgtablets.ESLcanbetakenwithoutregardtofoodandcrushedifneeded.8Initialdosesshouldbe400mgbymouthdailyforoneweekandtitratedtotherec-ommendedmaintenancedoseof800mgdaily.Thedosecanbefurthertitratedto1200mgdailybasedontolerabilityandclinicalresponse.9,11Ifthedesireddoseis1200mgdaily,themanufac-turerrecommendsstartingwith400mgdailyforoneweek,thenincreasingto800mgdailyforatleastaweek.8Thoughthishasshowntodecreaseseizurefrequency,cliniciansshouldbeawaretheAEsseenwithESLaredosedependent.11There-fore,clinicalresponseandpatienttolerabilitywillbethemostvaluablemethodforassessingtheef-icacyofESLineachpatient.Inpatientswithcom-promisedrenalfunctionCrCl<50mL/min,thedoseshouldbehalfoftherecommendedmainte-nancedose.Themanufacturerrecommendsstart-ingwith200mgdailyfortwoweeksandthenini-tiateESL400mgdailythereafter.8Doseadjust-mentsarenotavailableforCrCl<30mL/minduetoinadequatedata.15IfdiscontinuationofESLiswarranted,abruptwithdrawalshouldbeavoidedandthedoseshouldbegraduallytaperedoverseveralweekstominimizetheriskofseizures.8
PharmaNote Volume 29 Issue 6 March 2014 11

S
Eslicarbazepineacetateisindicatedasanadjuvantforthetreatmentofpartial-onsetsei-zures.ESLwasef icaciousinseveralphaseIIIclinicaltrialsandhasshowngoodtolerabilityinadults,withthemostcommonsideeffectsinclud-ingdizziness,somnolence,headache,nausea,andvomiting.Thoughstructurallysimilartocarbam-azepine,ESLhasamuchlowerpotentialfordrug-druginteractionsandnoautoinduction.Withlessdrug-druginteractions,onceadaydosing,andgoodtolerability,ESLhasthepotentialtoposi-tivelyimpactthelivesofmanypatientssufferingfromseizuresandcontributetoincreasedqualityoflife.
R
1. HauserWA,AnnegersJF,KurlandLT.Incidenceofepi-
lepsyandunprovokedseizuresinRochester,Minneso-ta:1935–1984.Epilepsia.1993;34:453–468.
2. HauserWA,AnnegersJF,KurlandLT.Prevalenceofepi-lepsyinRochester,Minnesota:1940–1980.Epilepsia.1991;32:429–445.
3. Chang,B,Lowenstein,D.Epilepsy.NEngJMed.2003;349:1257-1266.
4. Rauchenzauner,M,Luef,G.Updateontreatmentofpar-tialonsetepilepsy:roleofeslicarbazepine.Neuropsychi‐atricDiseaseandTreatment.2010;6:723-730.
5. Chang,BS,Lowenstein,DH.Mechanismsofdisease:Epi-lepsy.NEnglJMed.2003;349:1257-66.
6. Elger,C,Halasz,P,Almeida,L,etal.Ef icacyandSafetyofeslicarbazepineacetateasadjunctivetreatmentinadultswithrefractorypartial-onsetseizures:arandom-ized,double-blind,placebo-controlled,parallel-groupphaseIIIstudy.Epilepsial.2009;50(3):454-463.
7. Jennum,P,Gyllenborg,J,Kjellberg,J.Thesocialandeco-nomicconsequencesofepilepsy:acontrollednationalstudy.Epilepsia.2011;52(5):949-956.
8. Aptiom®[packageinsert].SunovionPharmaceuticalsInc.November2013.AccessedonDecemeber4,201.http://www.epilepsy.com/pdfs/aptiom_insert.pdf.
9. Almeida,L,Soares-da-Silva,P.Eslocarbazepienacetate(BIA2-093).Neurotherapeutics.2007;4(1):88-96.
10. Singh,R,Asconape,J.Areviewofeslicarbazepineace-tatefortheadjunctivetreatmentofoartial-onsetepi-lepsy.JournalofCentralNervousSystemDisease.2011;3:179-187.
11. Verrotti,A,Loiacono,G,Rossi,A,etal.Eslicarbazepineacetate:anupdateonef icacyandsafetyinepilepsy.EpilepsyRes.(2013),http://dx.doi.org/10.1016/j.eplepsyres.10.005.
12. Gil-Nagel,a,Elger,C,Ben-Menachem,E,etal.Ef icacyandsafetyofeslicarbazepineacetateasadd-ontreat-mentinpatientswithfocal-onsetseizures:integrated
analysisofpooleddatafromdouble-blindphaseIIIclinicalstudies.Epilepsia,2013;54(1):98-107.
13. Gil-Nagel,A,Lopes-Lima,J,Almeida,L,etal.Ef icacyandsafetyof800and1200mgeslicarbazepineacetateasadjunctivetreatmentinadultswithrefractorypar-tial-onsetseizures.ActaNeurolScand.2009;120:281-287.
14. Ben-Menachem,E,Gabbai,AA,Hufnagel,A,etal.Eslicarbazepineacetateasadjunctivetherapyinadultpatientswithpartialepilepsy.EpilepsyResearch.2010;89:278-285.
15. Bialer,M,Soares-da-Silva,P.Pharmacokineticsanddruginteractionsofeslicarbazepineacetate.Epilepsia.2012;53(6):935-946.
PharmaNote Volume 29 Issue 6 March 2014 12
John G. Gums PharmD, FCCP
R. Whit Curry, MD
Nicholas Carris PharmD, BCPS
Editor
Associate Editor
Assistant Editor
The PharmaNote is Published by: The Department of Pharmacy Services, UF Family Practice
Residency Program, Departments of Community Health and Family
Medicine and Pharmacotherapy and Translational Research University of Florida
UPCOMMING ARTICLES: LINACLOTIDE: A NEW OPTION FOR IRRITABLE BOWEL SYNDROME WITH CONSTIPATION (IBS-C) 2013 ACCF/AHA GUIDELINES FOR THE MAN-
AGEMENT OF HEART FAILURE: EXPANDED USE OF NATRIURETIC PEPTIDES AND ALDOSTERONE ANTAGONISTS