vëllimi 15, nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 ... stomat mars dhjetor 2017-web.pdf ·...
TRANSCRIPT

i Fakultetit të Mjekësisë Dentare
STOMATOLOGJIKEVëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 ISSN 2308-5290
Albanian Dental JournalOfficial Publication of Faculty of Dental Medicine, UMT
Executive Editorial BoardEditor In-ChiefEdit XHAJANKA
Deputy EditorsXhina Mulo, Gerta KAÇANI
Xhina MuloRamazan ISuFI
lindita XHEMNICAAdem AluSHI
Rozarka BuDINARuzhdie QAFMollA
Fejzi KERAJEdit XHAJANKABesnik GAVAZI
Merita BARDHoSHIDorjan HYSIEtleva QElI
Çeliana ToTI Agron METoKoço GJIlo
Gerta KAÇANI Alketa QAFMollA
Rozela RRoÇoEnida PETRo Fatmir lElA
Kreshnik KERAJSilvana BARA
Aldo VANGJElIEsat BARDHoSHIPrunela PolIÇIAndis QENDRo
Edlira DEDAJErda QoRRI
Florian BEuER Peter PoSPIECHNorina FoRNA
Bruno GIARDINAGiovanni ARCuDI
Francesco INCHINGolo Ioanis GEoRGAKoPouloS
Vincenzo CAMPANEllAFiladelfio CoNIGlIoNE
Philipp EBERlSanja PANCHEVSKA
Teuta PuSTINAGloria STAKA
Ali GASHIMerita BARANI Nedim KASAMI
lorena QAFMollA, lavdërim FERHATIEditorial office
National Editorial Board International Editorial Board
Me Revistën Stomatologjike Shqiptare bashkëpunojnë:Shoqata Dentare shqiptare
Shoqata Kirurgjikale oromaxillo-FacialeShoqata e ortodontëve shqiptarë
Shoqata Shqiptare e Pedodontisë dhe Profilaksisëuniversiteti i Prishtinës Departamenti i Stomatologjisë
Shoqëria Stomatologjike ApoloniaShoqata e Protezistëve shqiptarë
Adresa: Fakultetit të Mjekësisë Dentare, Universiteti i Mjekësisë, Rr. Dibrës, 371, Tiranë, Shqipëri.
Address: Faculty of Dental Medicin at the Medical University of Tirana, Rr. Dibrës, 371, Tirana, Albania.
e-mail: [email protected]
Revista Stomatologjike Shqiptare2
© Revista Stomatologjike ShqiptareDesign: Arben Hamzallari
Qëllimi
Revista Stomatologjike Shqiptare synon t’ u mundësojë studentëve dhe profesionstëve të shëndetit të njihen e të vlerësojnë prurjet më të reja dhe zhvillimet më të fundit të shkencave në fushën dentare e stomatologjike, të mbështesë klinicistët dhe kërkuesit në zhvillimin e vazhdueshëm profesional, në zgjerimin e dijeve, efektivitetit dhe produktivitetit të tyre. Artiujt e përfshirë në këtë revistë adresojnë zhvillimet më të rëndësishme dhe të spikatura në stomatologji kryesisht brenda vendit.
Struktura dhe formati
Revista Stomatologjike Shqiptare botohet dy herë në vit. Në të publikohen editoriale, recensa, artikuj origjinalë, raporte klinike, raportime të shkurtra, ide dhe mendime, vlerësime librash, produkte seminaresh, simpoziumesh dhe evente shkencore të ndryshme. Struktura e secilit variant të publikuar përfshin seksione të përcaktuara nga Redaksia dhe reflekton pikëpamjet e Bordit Editorial.
Ekspertiza editoriale
Bordi Editorial i Revistës Stomatologjike Shqiptare është i përbërë nga ekspertë të kualifikuar në fushën e stomatologjisë. Vlerësimi peer-review i artikujve organizohet nëpërmjet ekspertësh të përzgjedhur për ekspertizën e tyre të lartë në fushat që mbulojnë.
Për autorët
Të gjitha dorëshkrimet dërgohen në Redaksinë e revistës nëpërmjet postës elektronike në adresën: [email protected]. Jeni të lutur të konsultoheni me faqet e fundit të revistës ne hapësirën udhëzime për autorët. Artikujt e botuar në këtë revistë janë të mbrojtura me të drejta autoriale, të cilat mbulojnë të drejtat e përkthimit dhe të drejtën ekskluzive për të riprodhuar dhe shpërndarë të gjithë artikujt e shtypur në revistë. Asnjë material i botuar në revistë nuk mund te ruhet në mikrofilm, videokasetë ose në bazat e të dhënave elektronike ose të riprodhohet fotografikisht pa lejen paraprake me shkrim të Revistës Stomatologjike Shqiptare.
Aprovimi
Për informacione mbi marrjen e lejes dhe fitimin e së drejtës për të riprodhuar artikuj/informacione të publikuara në këtë revistë, jeni të lutur të kontaktoni Zyrën Editoriale.
Politikat e publikimit të reklamave
Revista pranon publikimin për disa kategori reklamash. Tarifimet mbi sasi publikimesh dhe pozicionimin në revistë janë të mundshme. Revista rezervon të drejtën të refuzojë çdo reklamë të konsideruar të papërshtatshme sipas politikave të përcaktuara të saj. Shfaqja e produkteve të reklamuara apo informacioneve shoqëruese në sektorë të ndryshëm të revistës nuk shpreh asnjë përgjegjësi të Revistës apo Entit Publikues mbi cilësinë apo vlerën e produktit.
Qartësim
Informacioni dhe opinionet e përfshira në artikujt e Revistës reflektojnë pikëpamjen e autorit dhe jo të Revistës, Bordit Editorial apo të Publikuesit. Publikimi në vetvete nuk to të thotë që revista ka të njëjtin qëndrim apo mban përgejgjësi për përmbajtjen e artikullit.
Abonimet
Revista publikohet dy herë në vit dhe është e disponeshme për abonim. Për më tepër informacion kontaktoni me Zyrën Editoriale.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 3
© Revista Stomatologjike ShqiptareDesign: Arben Hamzallari
Aims and Scope
Albanian dental journal enables time- pressured dentiststo stay abreast of key advances and opinion in dental sciences in order to support clinicians and related healthcare professionals in continuously developing their knowledge, effectiveness and productivity. The journal comprises balanced and comprehensive articles, addressing the most important and salient development in dental medicine.
Structure and Format
Albanian dental journal is a biannual journal and comprises editorials, reviews, original articles, case reports, short report, ideas and opinions, book reviews, seminars, symposium, ethics and rights, health care policy and management, practice guides. The structure of each edition of the publication comprises section categories determined by Editor and reflects the views of the Editorial Board.
Editorial Expertise
Editorial Board consist of leading authorities from a variety and respective fields of Dental medicine. Peer-review conducted by expert appointed for their experience and knowledge of a specific topic.
Important notice for Author
All manuscripts must be submitted to the Editorial office by electronic mail, email address: [email protected]. Please check the last pages on each edition the column “Instruction for author”. the work shall not be published elsewhere in any language without the written consent of the Board. The articles published in this journal are protected by copyright, which cover translation rights and the exclusive to reproduce and distribute all the articles printed in electronic database and the like or reproduced photographically without the prior written permission of the Albanian Dental Journal.
Permissions
For information on how to request permissions to reproduce articles/information from this journal please contact Editorial office.
Advertising policies
The journal accepts advertising. Frequency discounts and special positions are available. The journal reserves the right to reject any advertisement considered unsuitable according to the set policies of the journal. The appearance of advertising of product information in the various sections in the journal does not constitute an endorsement of approval by the journal and/or its publisher of the quality or value of the said product or of claims made for it by its manufacturer.
Disclaimer
The information and opinions presented in the Albanian dental journal reflects the views of the author and not of the Journal or its Editorial Board or the Publisher. Publication does not constitute endorsement by the journal
Subscriptions
Albanian dental journal is published two times a year and is available on subscription. For further information contact the Editorial office.

4
ReviSta Stomatologjike ShqiptaRevëllimi 15 Nr. 1 (56) mars 2017
përmbajtjamalokluzioni dhe ndikimi psikosocial 10Fatime Elezi, Edlira Subashi, Rudin Kusi, Andri Çabeli
Rebazimi i protezës totale në kushte të zvogëlimit të dimensionitvertikal- përshkrimi i një rasti klinik 22Sanja Panchevska, Darko Gjorgjievski, Sasho Elenchevski, Nadica Janeva, Faton Vojnika
trajtimi i klasës së iii me kafshim të kyqëzuar anterior me aparatfiks self-ligating. Rast klinik 28Manjola Gusho, Xhina Mulo
laminatet keramike jo invazive si një alternativë për ruajtjen e strukturës së dhëmbitsi dhe zgjatimi vertikal i dhëmbëve me anë të gingivoplastikës për arritjen e estetikës 38Mefail Sulejmani, Florina Sulejmani, Bashkim Saiti
Frekuenca e sëmundjeve të rrezikut te pacientët e trajtuar me punime protetike 47Sherif Shaqiri, Kaltrina Beqiri
Rezistenca ndaj frakturës e dhëmbëve të trajtuar endodontikisht me kavitete hyrëskonservativë të restauruar me materiale të ndryshme kompozite 55Almira Isufi, Gianluca Plotino, Nicola Maria Grande, Pietro Ioppolo, luca Testarelli, Rossella Bedini,
Gianluca Gambarini
teknika e zonës neutrale dhe masa terciare 76Neada Hysenaj, Edit Xhajanka, Merita Bardhoshi, Koço Gjilo
osteotomia Sagitale Bilaterale e Ramusit mandibular 83Renato Isufi, Algen Isufi, Aurora Isufi, Ramazan Isufi
agenezia e incizivit lateral të përhershëm në fëmijët josindromik me kleft unilaterale të buzës/alveolës/palatumit 95Bisela Asllanaj

5
table of Contents
volume 15 No. 1 (56) march 2017
alBaNiaN StomatologiCal jouRNal
malocclusion and psychosocial impact 16Fatime Elezi, Edlira Subashi, Rudin Kusi, Andri Çabeli
Complete dentures rebasing in case of decreased vertical dimension. Case report 25Sanja Panchevska, Darko Gjorgjievski, Sasho Elenchevski, Nadica Janeva, Faton Vojnika
treatment of Class iii malocclusion and anterior crossbite withthe use of self-ligating Brackets System. Case Report 33Manjola Gusho, Xhina Mulo
Non-invasive ceramic veneers as an alternative to preserve tooth structure and crownlengthening via gingivoplasty in achieving aesthetics 41Mefail Sulejmani, Florina Sulejmani, Bashkim Saiti
preservation of the alveola for implanting dental implants with ReSoRBa® DeNtal 44lj. Simjanovska, A. Trajkovski, S.Simjanovski, F.Azizi, S.Simjanovska
the frequency of systemic diseases by patients treated with prosthetic appliances 51Sherif Shaqiri, Kaltrina Beqiri
Fracture resistance of endodontically treated teeth with conservative access cavitiesrestored with different composite materials 61Almira Isufi, Gianluca Plotino, Nicola Maria Grande, Pietro Ioppolo, luca Testarelli, Rossella Bedini,
Gianluca Gambarini
tissue support and implant retention overdenture in mandible: a simply, smart and predictable treatment. a case report. 67Roberto Scrascia, luigi Secondo
Neutral zone technique and third impression 80Neada Hysenaj, Edit Xhajanka, Merita Bardhoshi, Koço Gjilo
the Bilateral Sagittal Split mandibular Ramus osteotomy 89Renato Isufi, Algen Isufi, Aurora Isufi, Ramazan Isufi
agenesis of the permanent lateral incisor in nonsyndromic children with unilateral cleft lip/ alveolus / palate 99Bisela Asllanaj

6
vëllimi 15 Nr. 2 (57) Nëntor 2017përmbajtjaNiveli plazmatik i markerave të inflamacionit, si shprehës i ndërlidhjessë periodontitit me arterosklerozën 102Saimir Heta, Ilma Robo, ortodonte Ermelinda Gina, Dariel Thereska, Nevila Alliu
vlerësim klinik i 34 rasteve të implantuara me ngritje të sinusit maksilar 110Florian Bllaca
mbyllja e diastemës nëpërmjet përdorimit të fasetave të gatshme të kompozitit.(Raportim rasti) 118Stela Panteqi, Adem Alushi, orges Simeon
morfologjia e sistemit kanalar në molarin e parë maksilar 126Xhanina Gavazi
Një këndvështrim mbi trajtimin kirugjikal dhe konservator të frakturave të kondilit 138Jakup Vrioni, Renato Isufi, Ramazan Isufi
Rast klinik i një kanini maksilar të impaktuar, i trajtuarnë mënyrë ortodontike-kirurgjikale 146Iris Çaçani, Xhina Mulo, Rudin Kusi
trajtimi kirurgjikalo-ortodontik i kaninit të impaktuar (raportim rasti) 154Nineta Fino, Ramazan Isufi, Adela Alushi
Dhëmbët multiple inkluzë-Rishikimi i literaturës dhe raportim rasti 162Remi likaj, Alba likaj
kurorёzohet me sukses proçesi i akreditimit institucional tё universitetit tё mjekёsisё, tiranё, duke u vlerёsuar me maksimumin e plotёsimit tё standarteve 166Finalizohet bashkëpunimi ndërmjet Fakultetit të mjekësisëDentare dhe Bashkisë së tiranës 167marrëveshje bashkëpunimi midis universitetit të prishtinës “hasan prishtina” dhe universitetit të mjekësisë, tiranë 168Një delegacion shqiptar viziton ndërmarrjen italiane Rhein 83 169Zhvillimi i konferencës së iv të Shkencave mjekësore të universitetit të mjekësisë, tiranë, 21- 23 prill 2017 170
NekRologjiprof.asoc. afërdita BaSha 172Dr.Shahin joka 173Dr. kujtim likaj 174

7
table of Contentsvolume 15 No. 2 (57) November 2017
plasma level of inflammatory markers, as an expressionof the connection of periodontitis with arteriosclerosis 106Saimir Heta, Ilma Robo, ortodonte Ermelinda Gina, Dariel Thereska, Nevila Alliu
implant placement in maxillary sinus area.outcome of 34 cases with sinus lifting 114Florian Bllaca
Diastema closure by using pre-fabricated composite veneers.(Case report) 122Stela Panteqi, Adem Alushi, orges Simeon
morphology of root canal system in the first maxillary molar 132Xhanina Gavazi
a point of view in the chirurgical and conservator treatment of the condyle 142Jakup Vrioni, Renato Isufi, Ramazan Isufi
Case report of a maxillary impacted canine treated in a surgical-orthodontic way 150Iris Çaçani, Xhina Mulo, Rudin Kusi
Surgical - orthodontic treatment of impacted canines (case report) 158Nineta Fino, Ramazan Isufi, Adela Alushi
management of multiple inclused teeth- Review of literature and case report 164Remi likaj, Alba likaj

Revista Stomatologjike Shqiptare8

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 9
Editorial
Të nderuar kolegë, profesionistë e dashamirës të fushës së stomatologjisë!Revista Stomatologjike Shqiptare, e botuar periodikisht prej 17 vitesh, përbën organin
shkencor kryesor të Fakultetit të Mjekësisë Dentare. Me kalimin e Departamentit të Stomatologjisë nga departament i Fakultetit të Mjekësisë, në Fakultet më vete, edhe Revista është fuqizuar dhe ka evoluar ndjeshëm. Niveli cilësor i saj është rritur vazhdimisht, duke pasqyruar përparimin e shërbimit stomatologjik në Shqipëri dhe të rejat profesionale bashkëkohore, tashmë të inkluduara në praktikën profesionale të shumë stomatologëve dhe profesionistëve në Shqipëri.
Kemi riorganizuar këtë revistë, me shpresën dhe dëshirën që çdo profesionist të motivohet për të publikuar në të sfidat e profesionit, të rejat bashkëkohore, rezultatet e punës kërkimore-shkencore, eksperimentale, raste klinike interesante etj, duke e ndjerë veten të përfshirë në rrugën e progresit dhe të inovacionit.
Sigurisht, nëpërmjet shkëmbimit të eksperiencave profesionale, Revista Stomatologjike Shqiptare do të shërbejë si një ndërlidhje ndërmjet profesionistëve stomatologë të disiplinave të ndryshme, si dhe ndërmjet pedagogëve dhe studentëve, duke u dhënë mundësinë edhe studentëve ekselentë të mund të botojnë punën e tyre shkencore, temat e diplomës që paraqesin interes, raste klinike interesante etj.
Për herë të parë në bordin e Revistës Stomatologjike Shqiptare bëjnë pjesë figura akademike të shquara ndërkombëtare, Profesorë të nderuar nga Gjermania, Italia, Kosova, Maqedonia etj, duke rritur nivelin shkencor të këtij organi shkencor të FMD.
Shpresoj që kjo revistë të përmbushë kërkesat tuaja për t’ju njohur me risitë e fushës së stomatologjisë dhe, nëpërmjet kontributit të stafit akademik dhe të gjithë profesionistëve, të rrisë nivelin cilësor dhe standartet e saj.
Me respekt dhe konsideratё tё veçantё,
Prof. Asoc. Edit XHAJANKA, Dekane e FMD.

Revista Stomatologjike Shqiptare10
AbstraktObjektivi: Për të vlerësuar ndikimin psikosocial te estetikës dentare duke përdorur “Pyetësorin e ndikimit psikosocial te estetikës dentare [‘Psychosocial Impact of Dental Aesthetics
Questionnaire’ (PIDAQ)] dhe komponentin vetë-vlerësues estetik (AC) të indeksit të nevojës së trajtimit ortodontik [self-rated Aesthetic Component (AC) of the Index of orthodontic Treatment Need (IoTN)].
Lloji i studimt: Studimi është Cross-sectional.
Vendi dhe Kohëzgjatja e studimit: Fakulteti i Mjekësisë, Fakulteti i Mjekësisë Dentare, Klinikat private, për një periudhë kohore, (shkurt 2014- maj 2016).
Metodologjia: Të rriturit pa trajtim paraprak ortodontik u pyetën për të plotësuar një version të modifikuar të “Pyetësorit të ndikimit psikosocial të estetikës dentare (PIDAQ). u përdor një total prej katër variablave, duke përfshirë “Vetë-besimi ‘’dentar”, “Ndikimi social”, “Ndikimi psikologjik” dhe “Nevoja e perceptuar për trajtim ortodontik”, ndërsa estetika dentare u vlerësua nga të anketuarit duke përdorur komponentin estetik të IoTN-së (vetë-vlerësimin IoTN-AC).
Testi Kruskal-Walli u aplikua për të përcaktuar domethënien.
Rezultatet: Të anketuarit ishin 160 të rritur (90 femra dhe 70 meshkuj, të moshës 22.3 vjeç), tek të cilët të katër variablat matëse të lartpërmendura mbi ndikimin psikologjik treguan korrelacione pozitive dhe të rëndësishme, perceptuar kjo me rendimin e malokluzionit, sikurse përshkruhet nga komponenti estetik (AC) i indeksit të nevojës së trajtimit ortodontik (IoTN), me vlere (p ) prej me pak se 0.05 për të gjitha variablat.
Konkluzioni: Rezultatet tregojnë ndikimin e fortë psikosocial të estetikës te ndryshuar dentare në gjendjen emocionale të një individi. Shoqërimi midis gradave vetë-vlerësuese të IoTN-AC me mirëqenien psikosociale ekziston, duke treguar se estetika e perceptuar e malokluzionit mund të jetë një faktor i rëndësishëm në përcaktimin e trajtimit te malokluzionit.
Fjalët kyçe:
Ndikimi
psikosocial,
estetika
dentare, indeksi
i nevojës
se trajtimit
ortodontik.
Fatime elezi1, edlira Subashi2 , Rudin kusi2, andri çabeli
malokluzioni dhe ndikimi psikosocial
1Shefe shërbimi në shërbimin Psikiatrik në QSUT; 2 Mjeke stomatologe në klinikën private
HyrjePerceptimet personale estetike të kompleksit
dentofacial dhe ndikimi shoqërues psiko-social janë me pasoja të mëdha për pacientët ortodontike. Fytyra është tipari më lehtë i dukshem dhe në këtë mënyrë është karakteristika më e rëndësishme fizike në zhvillimin e vetë-imazhit dhe vetë-vlerësimin. Ndërkohë që në ndërveprimet sociale ka rezultuar që një fytyrë e pranueshme rrit marrëdhëniet ndërpersonale dhe krijon më shumë vetë-konfidencë (1, 2, 23).
Një malokluzion, veçanërisht i pranishëm në pjesen anteriore, është shpesh i dukshëm, gjë që ngjall reagime sociale të pakëndshme (3,4,5). Maggregor deklaronte se: “një malokluzion është një handikap fizik pasi ai kufizon stereotipin dhe mundësitë sociale të një personi « (6).
Të jesh pjesë e një rrjeti social, ka një nevojë te natyrshme për tu ndjerë i pranuar. Çdo shmangie e konsiderueshme nga norma mund të rezultojë në ndjenjen e pasigurisë në lidhje me pamjen, pengesë në kontaktet sociale dhe krahasimi i vetes me të tjerët që konsiderohen ‘superior’, të cilat mund të ndikojnë negativisht në cilësinë e jetës së individuale (7,8,9).
Trajtimi ortodontik mund të ndikohet më shpesh nga kërkesa se sa nga nevoja (10,11).
Në të kaluarën, nevoja për trajtim ortodontik vlerësohej nga një perspektive strikte profesionale, duke marrë edhe mendimin e prindërve. Megjithatë, disa studime kanë treguar se aparenca e dhëmbëve e vetë-perceptuar është gjithashtu e rëndësishme në vendimin për të kërkuar trajtim ortodontik (11,12). Indekse të ndryshme, të tilla si Indeksi i Nevojës për Trajtim ortodontik (IoTN), Indeksi Estetik Dentar (DAI) , etj, janë zhvilluar si sisteme për të vlerësuar malokluzionet dhe ndikimin e tyre tek pacientët (12,13,14, 23).
IoTN është një sistem matës që i rendit malokluzionet në bazë të tipareve okluzale për shëndetin oral dhe ndikimin estetik. Komponenti estetik (AC) i IoTN-së është përdorur zakonisht për të vlerësuar nevojën për trajtim për arsye estetike (të vlerësuar nga dentistët ose vetë pacientët) (15,16). Megjithatë, që kur është një fakt i pranuar se pasojat psiko-sociale për shkak të estetikës papranueshme të dhëmbëve mund të jetë aq serioze, apo edhe më serioze se problemet biologjike, indekset

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 11
aktualisht në përdorim janë kritikuar për mungesë të një komponenti psiko-social (5,10,17).
Filozofët duke studjuar konceptin e vetëvlerësimit, konkluduan që, edhe pse vetë-vlerësimi zhvillohet gjatë gjithë jetës, është eksperienca jonë gjatë fëmijërisë që luan një rol të madh në vitet më vonë, ndërsa ne ndërtojme një imazh të vetes nga përvojat në situata të ndryshme dhe me njerëz të ndryshëm. “Ndikimi psiko-social” i malokluzionit është një fenomen që mund të provokojë një reagim emocional që manifestohet si pasiguri në lidhje me pamjen, pengesë në kontaktet sociale, ndjenjë trishtimi dhe krahasim të vetes me të tjerët. Korrigjimi i aparencës së dhëmbëve është faktor kryesor motivues për shumicën e pacientëve ortodontike; megjithatë, vetëm kohët e fundit faktorët psiko-social të tilla si ato që vlerësojne vetë-imazhin janë përfshirë në vlerësimin e malokluzioneve.
Ky studim u ndërmor me qëllim për të përcaktuar ndikimin psikologjik si dhe atë social të estetikës dentare duke përdorur pyetësorin e impaktit psikosocial te estetikës dentare (PIDAQ) dhe Komponentin estetik (AC) të indeksit të nevojës për trajtim ortodontik (IoTN), të dyja këto metoda të aprovuara dhe të përdorura në kërkimet shkencore ortodontike mbarë botërore.
MetodologjiaKy ishte një studim cross-sectional i kryer nga
shkurti 2014 deri në maj 2016. Grupi i studimit përbëhej nga mjekët e ketij studimi (të fushës së mjekësisë dhe stomatologjisë), shoqëruesit e pacientëve dhe pacientët ortodontike. Ndër kriteret përfshirëse ishin: pacientët të qenë mbi 18 vjeç dhe pa histori të mëparshme të trajtimit ortodontik. Kriteret e përjashtimit ishin pacientët ortodontike me prani të sindromave ose anomalive kraniofaciale.
Pyetësori i përdorur në këtë studim mbi impaktin psikosocial të estetikës dentare (PIDAQ), zhvilluar nga Klages dhe bp. është modifikuar pak për këtë studim (1,17). Analizat e besueshmërisë së katër faktorëve ishin shumë të qëndrueshme siç konfirmohet nga Cronbach me vlerat që variojnë nga 0.83-0.92 (17). Pyetësori është vetë-administruar nga subjektet, me shkallën e likert-it duke vlerësuar përgjigjet në një shkallë që varion nga 0 (mosmarrëveshje totale) me 4 (marrëveshje totale).
Një total prej katër variablash të përfshirë “Vetë-besimi dentar”, “Ndikimi social”, “Ndikimi psikologjik” dhe “Nevoja e perceptuar për trajtim ortodontik” u vlerësuan nga një seri deklaratash përkatëse (Fig. 1) (15,17).
Nga ky pyetësor:Pyetja 1-4 është variabli “Vetë-besimi dentar”,Pyetja 5-10 është variabli “Ndikimi social”,Pyetja 11-18 është variabli “Ndikimi psikologjik”,Pyetja 19-21 është variabli “Nevoja e perceptuar për trajtim ortodontik”.
Estetika dentare u vlerësua duke përdorur IoTN-në, komponenti estetik (AC). Subjekteve ju paraqitën 10 fotografi bardh e zi të dhëmbëve anteriorë me shkallë të ndryshme të malokluzionit (fig. 2), dhe u pyetën për të treguar se në cilën fotografi (1 në 10), ata mendonin se ngjante denticioni i tyre.
IoTN-AC vetë-vlerësues u përdor për të kategorizuar në grupet përkatëse subjektet e studimit.
Fig.1: Pyetësori mbi impaktin psikosocial të estetikës dentare (PIDAQ)

Revista Stomatologjike Shqiptare12
Sipas 10 fotografive bardhë e zi të dhëmbëve anteriorë, tregoni se cila fotografi ju e ndjeni se ngjan më shumë me destinacionin tuaj?
Sipas këtyre fotove bëhet kjo ndarje:Grada 1 (foto 1)-jo anomaliGrada 2 (foto 2)-anomali e lehtëGrada 3 (foto 3)-anomali e mesmeGrada 4 (foto 4-10)-shumë anomali.
1 6
2 7
3 8
4 9
5 10
Testi Kruskal-Wallis u aplikua për të përcaktuar dallimet midis rezultateve për të gjitha grupet e subjekteve (1 në 4 +) për secilin nga katër variablat sipas studimit. Vlera-p e barabartë ose më pak se 0.05 është marrë si statistikisht e rëndësishme. Analizat statistikore ishin kryer duke përdorur SPSS për Windows (version 14.0).
Për të vlerësuar ndikimin psikosocial të estetikës dentare mbi gjëndjen emocionale të një individi, vlerat mesatare u krahasuan midis katër grupeve të subjekteve për secilin nga variablat.
RezultatetTë anketuarit ishin 160 adultë, me nje mesatare të
moshës 22.3 vjeç (SD + 2,8 vjeç) dhe kryesisht femra.Në figurën 3 dhe 4 paraqiten përgjigjet e të anketuarve
për pyetësorin dhe IoTN:
Fig. 2: Indeksi IOTN-AC

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 13
Fig. 3: Përgjigjet e pyetësorit
Fig. 4: Përgjigjet e IOTN-së
Fig. 5: Shpërndarja e të anketuarve sipas gradave të IOTN-AC
15% e të anketuarve vlerësuan pamjen e tyre dentare si grada 1 e IoTN-AC (përbëjnë:
Grupi 1), 16.3% vendosën veten si grada 2 e IoTN-AC (Grupi 2), 17.5% vlerësuan veten si grada 3 e IoTN-AC (Grupi 3), ndërsa 51.3% e subjekteve vlerësuan estetikën e tyre dentare si grada 4 deri në 10 e IoTN-AC (Grupi 4).(Fig. 5).
Mbizotëron grada 4 me ndryshim sinjifikant me gradat e tjera, (χ2 = 61.03 p=0.0001).
Rezultatet e 4 variableve treguan:“Vetë-besimi dentar” u gjet më i lartë për subjektet e
vendosura tek grada 1 e IoTN-AC (vlera mesatare 12.9), dhe më e ulët tek grada 4 e IoTN-AC (vlera mesatare
4.2), ne gradat 2 dhe 3 te IoTN-AC (vlerat mesatare 9.7 dhe 8.0 përkatësisht) duke treguar ndryshime të mëdha ndërmjet grupeve (P = 0.000).
“Ndikimi social” ishte më i madh për të anketuarit që klasifikuan veten në gradën 4 të IoTN-AC (vlera mesatare 9.4), dhe më pak për ata që vlerësuan aparencën e dhëmbëve të tyre tek grada 1 e IoTN-AC (vlera mesatare 3.1), në gradat 2 dhe 3 të IoTN-AC vlerat mesatare ishin 4.2 dhe 5.7 respektivisht, (p = 0.004).
“Ndikimi psikologjik“ është gjetur të jetë i lartë në individët të cilët vlerësuan veten në gradën 4 të IoTN-AC

Revista Stomatologjike Shqiptare14
(vlera mesatare 15.3) , dhe më i ulët tek ata që vlerësuan veten tek grada 1 e IoTN - AC (vlera mesatare 4.9) , e ndjekur nga gradat 2 dhe 3 të IoTN - AC (vlerat mesatare 8.9 dhe 11.1 respektivisht ), (P = 0.000).
“Nevoja e perceptuar për trajtim ortodontik” ishte më e lartë në gradën 4 të IoTN - (vlera mesatare 5.2) , duke rënë në mënyrë progresive së bashku me gradat e IoTN - AC (vlera mesatare 3.8 për gradën 3 të IoTN – AC dhe 2.9 për graden 2 ) , dhe më pak për gradën 1 të IoTN – AC (vlera mesatare 2.8 ) , duke qenë sinjifikisht e ndryshme gjatë grupeve (p = 0.007).
Ndërkohë që duke analizuar këto variable midis gjinive, rezultoi se (Fig. 6):
Vetvlerësimi dentarNdikimi socialNdikimi psikologjik
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
Scor
e
FemraMeshkuj
Fig.6: Krahasimi i nënshkallëve të pyetësorit sipas gjinisë
Vërehet që tek meshkujt, ndikimi psikologjik (p=0.04), social (p=0.004) dhe vetëvlerësimi dentar (p=0.0009), është më i ulët se tek femrat.
DiskutimiVlerësimi i faktorëve psiko-social të malokluzionit
kohët e fundit është konsideruar si një pjesë e rëndësishme e trajtimit ortodontik tek adultët (1,3,4,7 , 9 , 12,17-19).
Për sa i përket kategorizimit të IoTN - AC siç perceptohet nga vetë subjektet, u gjet se shumica e tyre e vendosnin veten në gradën 4 të IoTN-AC (51,3 % ), e ndjekur nga grada 3 e IoTN - AC, grada 2, dhe numri më i pakët i të anketuarve vendosnin veten tek grada 1 e IoTN - AC.
Klages dhe bp. kanë gjetur se numri më i madh i subjekteve e vlerësuan veten ne graden 1 të IoTN - AC (33.5 % ) , vetëm 8.8 % e të anketuarve e vendosur veten ne gradën 4 IoTN-AC (17). Kerosuo dhe bp. demonstruan gjithashtu vlera të përafërta.
Për secilin nga variablat, domethënë, “Vetë-besimi ‘’dentar”, “Ndikimi social”, “Ndikimi psikologjik” dhe “Nevoja e perceptuar për trajtim ortodontik”, krahasimi i vlerave mesatare midis katër grupeve të subjekteve (vetë-vlerësimi IoTN-AC 1 deri 4 +) në mënyrë të qartë tregon ndikimin e fortë psiko-social të estetikës ndryshuar dentare.
“Vetë-besimi dentar”, tregon nivelin e kënaqësisë apo pakënaqësisë me paraqitjen e denticionit të secilit dhe synon të masë ndikimin e estetikës dentare në vetë-imazhin e një individi. Aparenca e gojës dhe buzëqeshja luan një rol të rëndësishëm në vlerësimin e atraktivitetit të fytyrës, e cila pa dyshim kontribuon në vetë-vlerësimin (1-3). Rezultatet e këtij studimi treguan një trend të vetë-konfidencës së ulët dentare me nivelin e rritur të estetikës së ndryshuar, siç perceptohet nga vetë të anketuarit duke përdorur IoTN-AC. Klages dhe bp. kanë treguar rezultate të ngjashme në studimin e tyre.
“Ndikimi Social” ka për qëllim të vlerësojë problemet e mundshme që një individ mund të përballë në situata sociale për shkak të një aparence subjektivisht të pafavorshme dentare. Studimet e mëparshme kanë vërejtur se individët e perceptuar të jenë tërheqës kanë më shumë eksperienca pozitive sociale dhe vlerësime nga bashkëmoshatarët (1-3). Klages dhe bp. kanë treguar një efekt të drejtpërdrejtë të estetikës së dhëmbëve për shëndetin e pergjithshëm.
Në këtë studim, një ndikim gjithnjë e më i lartë social është vënë në dukje gjatë të anketuarve duke vlerësuar veten në gradën 4 të IoTN-AC, duke theksuar ndikimin negativ të estetikës së pakëndshme në ndërveprimet sociale. Kjo mund të shpjegohet me fenomenin e “krahasimit social’” ku paraqitja e fytyrës, e lidhur me vetë-konceptimin mund të preket në masën e të qënit një handikap social (3).
Sipas onyeaso dhe bp., mbi 40% e të anketuarve raportuan ndjenja më pak konfidente si rezultat i malokluzionit të tyre, me aktivitete normale të kufizuara në disa nga subjektet, duke përfshirë të qeshurën në publik, takimin me njerëzit dhe formimin e relacioneve (20).
“Ndikimi psikologjik” vlerëson ndjenjat e inferioritetit ose pakënaqësisë sidomos krahasuar me të tjerët. Sipas Tung dhe Kiyak, “hulumtuesit kanë gjetur vazhdimisht se vetë-konceptimi është i lidhur më shumë me perceptimet individuale të vlerësimeve të të tjerëve, se sa me vlerësimet objektive nga të tjerët “ (3).
onyeaso dhe bp. kanë raportuar në lidhje me depresionin e lidhur me estetikën dentare në 27% të subjekteve të tyre (20).
Studimi tregoi dallime statistikisht të rëndësishme tek grupet, ku mirëqenia psikologjike zvogëlohej me estetikën gjithnjë e më të keqe të dhëmbëve.
Klages dhe bp. tregojnë rezultate të ngjashme me studimin tonë, ku gradat 1 deri 4 të IoTN-AC demonstrojnë një trend në rritje të efektit psikologjik përgjatë spektrit të IoTN-AC (17).
“Nevoja e perceptuar për trajtim ortodontik”, vlerëson nevojën subjektive për vëmendje ortodontike, dhe rezultatet tregojnë, se kjo është gjetur më e lartë në individë që e klasifikojnë veten në gradën 4 të IoTN-AC.
Shoqërimi i rritjes së nevojës së perceptuar për trajtim ortodontik me rritjen e ashpërsisë së malokluzionit, është treguar nga Mandall dhe bp., i cili arriti në përfundimin se fëmijët të cilët janë të ngacmuar në lidhje me dhëmbët e

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 15
1. Bos A, Hoogstraten J, Prahl-Andersen B. Expectations of treatment and satisfaction with dentofacial appearance in orthodontic patients. Am J orthod Dentofacial orthop 2003; 123:127-32.
2. Social thought and social behaviour. In: Baron RA. Essen-tials of psychology. 2nd ed. Massachusetts: Allyn & Bacon; 1999.p.535-66.
3. Tung AW, Kiyak HA. Psychological influences on the timing of orthodontic treatment. Am J orthod Dentofacial orthop 1998; 113:29-39.
4. Marques lS, Ramos-Jorge Ml, Paiva SM, Pordeus IA. Maloc-clusion: esthetic impact and quality of life among Brazilian school children. Am J orthod Dentofacial orthop 2006; 129:424-7.
5. Soh J, Chew MT, Chan YH. Perceptions of dental esthetics of Asian orthodontists and laypersons. Am J orthod Dentofa-cial orthop 2006; 130: 170-6.
6. Rinchuse DJ, Rinchuse DJ. orthodontics justified as a pro-fession. Am J orthod Dentofacial orthop 2002; 121:93-6.
7. Sarver DM, Proffit WR. Special considerations in diagnosis and treatment planning. In: Graber TM, Vanarsdall Rl, Vig KW, (edi). orthodontics: current principles and techniques. 4th ed. Missouri: Elsevier; 2005.p.4-9.
8. Morphopsychology and esthetics. In: Rufenacht CR. Funda-mentals of esthetics. Illinois: Quintessence Publishing Co; 1990.p.59-66.
9. Klages u, Bruckner A, Zentner A. Dental aesthetics, self-awareness, and oral health-related quality of life in young adults. Eur J orthod 2004; 26:507-14.
10. Jarvinen S. Indexes for orthodontic treatment need. Am J orthod Dentofacial orthop 2001; 120:237-9.
11. Bernabe E, Kresevic VD, Cabrejos SC, Flores-Mir F, Flores-Mir C. Dental esthetic self-perception in young adults with and without previous orthodontic treatment. Angle orthod 2006; 76: 412-6.
12. Espeland lV, Stenvik A. Perception of personal dental ap-pearance in young adults: relationship between occlusion, awareness, and satisfaction. Am J orthod Dentofacial or-thop 1991;100: 234-41.
13. Brook PH, Shaw WC. The development of an index of orth-odontic treatment priority. Eur J orthod 1989; 11:309-20.
14. Firestone AR, Beck FM, Beglin FM, Vig KW. Validity of the Index of Complexity, outcome and Need (ICoN) in deter-mining orthodontic treatment need. Angle orthod 2002; 72:15-20.
15. Grzywacz I. The value of the aesthetic component of the index of orthodontic treatment need in the assessment of subjec-tive orthodontic treatment need. Eur J orthod 2003; 25:57-63.
16. Hunt o, Hepper P, Johnston C, Stevenson M, Burden D. The aesthetic component of the index of orthodontic treat-ment need validated against lay opinion. Eur J orthod 2002; 24:53-9.
17. Klages u, Claus N, Wehrbein H, Zentner A. Development of a questionnaire for assessment of the psychosocial impact of dental aesthetics in young adults. Eur J orthod 2006; 28:103-11.
18. Kerosuo H, Al Enezi S, Kerosuo E, Abdulkarim E. As-sociation between normative and self-perceived orth-odontic treatment need among Arab high school stu-dents. Am J orthod Dentofacial orthop 2004; 125:373-8.
19. Klages u, Bruckner A, Guld Y, Zentner A. Dental esthetics, orthodontic treatment, and oral-health attitudes in young adults. Am J orthod Dentofacial orthop 2005; 128:442-9.
20. onyeaso Co, utomi Il, Ibekwe TS. Emotional effects of malocclusion in Nigerian orthodontic patients. J Contemp Dent Pract 2005; 6: 64-73.
21. Varela M, Garcia-Camba JE. Impact of orthodontics on the psychologic profile of adult patients: a prospective study. Am J orthod Dentofacial orthop 1995; 108:142-8.
22. Mandall NA, Wright J, Conboy F, Kay E, Harvey l, o’Brien KD. Index of orthodontic treatment need as a predictor of orthodontictreatment uptake. Am J orthod Dentofacial or-thop 2005; 128:703-7.
23. Munizeh Khan and Mubassar Fida, Assessment of Psycho-social Impact of Dental Aesthetics, Journal of The College of Physicians and Surgeons Pakistan 2008, Vol. 18 (9): 559-564.
REFERENCA
tyre kanë më shumë gjasa për të marrë trajtim ortodontik (21). onyeaso dhe bp. raportoi se 56.6% e të gjithë subjekteve të tyre raportuan për trajtim ortodontik për arsye estetike (20).
“Vetë-besimi Dentar” dhe “Ndikimi psikologjik” demonstruan dallime të rëndesishme midis grupeve të IoTN-AC nën shqyrtim; këto rezultate janë paralele me ato të arritura nga Klages dhe bp., (17), duke demonstruar se efektet sociale dhe psikologjike të estetikës dentare janë faktorë të pavarur.
Dallimet midis grupeve në “Ndikimin social” dhe “Nevojën e perceptuar për trajtim ortodontik”, ishin më të vogla, por ende të rëndësishme. Varela dhe Garcia-CAMBA nuk raportuan ndryshime të rëndësishme në vetë-konceptim dhe veçanërisht në vetë-vleresim mbas trajtimit ortodontik (21). Disa studime kanë demonstruar efektet e dëmshme të estetikës së varfër dentare në
gjëndjen emocionale të një individi (3,9,17,18,22). Rezultatet nga ky studim janë gjithashtu konkluzive
në theksimin e faktit të ndikimit psikologjik dhe social të malokluzionit, me një shoqërim invers midis gradave të IoTN-AC me mirëqenien psikosociale. Kështu, IoTN-AC mund të konsiderohet si një mjet efektiv në vlerësimin e ndikimit psiko-social ne estetikën dentare.
KonkluzionTrajtimi ortodontik duhet të vlerësohet jo vetëm nga
ortodonti, por edhe subjektivisht duhet të perceptohet nga pacienti.
Ekziston nje shoqërim i rëndësishëm midis gradave të IoTN-AC me mirëqenien psiko-sociale, duke treguar se estetika e perceptuar e malokluzionit mund të jetë një faktor i rëndësishëm në përcaktimin e nevojës së trajtimit.

Revista Stomatologjike Shqiptare16
AbstraktObjective: To evaluate the psychosocial impact of malocclusion, determine its relationship with the severity of malocclusion using the ‘Psychosocial Impact of Dental Aesthetics Questionnaire’ (PIDAQ) and self-rated Aesthetic Component (AC) of the Index of orthodontic Treatment Need (IoTN).
Study Design: Cross-sectional study.
Place and Duration of Study: Faculty of Medicine, Faculty of Dentstry, Private Clinics, from February 2014 to May 2016.
Methodology: A random sample of adults with no prior orthodontic treatment were asked to complete a modified version of the “Psychosocial Impact of Dental Aesthetics Questionnaire” (PIDAQ). A total of four variables including “Dental Self-confidence”, “Social impact”, “Psychological impact” and “Perceived orthodontic treatment need” were assessed by a series of statements, whereas dental aesthetics were assessed by the respondents using the IoTN Aesthetic Component (self-rated IoTN-AC).
Kruskal-Walli’s test was applied to determine significance.
Results: The respondents were 160 adults (90 females and 70 males; mean age 22.3 years), all four of the above mentioned variables measuring psychosocial impact showed positive and significant correlations with the perceived severity of malocclusion as depicted by the Aesthetic Component (AC) of Index of orthodontic Treatment Need (IoTN), with p-value of less than 0.05 for all variables.
Conclusion: The results indicate the strong psychosocial impact of altered dental aesthetics on the emotional state of an individual. The association between self-rated IoTN-AC grading with psychosocial well-being stands established, indicating that the perceived aesthetics of malocclusion may be as significant a factor in determining treatment need as
the degree of malocclusion. Malocclusion has a psychological impact in adolescents and this impact increases with the severity of malocclusion. Psychological impact seems to be greater among girls.
Psychosocial impact. Dental aesthetics. Index of orthodontic treatment need.
key woRDS:
Ndikimi
psikosocial,
estetika
dentare, indeksi
i nevojës
se trajtimit
ortodontik.
Fatime elezi1, edlira Subashi2 , Rudin kusi2, andri çabeli
malocclusion and psychosocial impact
1Head in Psychiatric service in QSUT; 2 Dental doctor in private clinic (0682128811)
IntroductionMalocclusion affects many people worldwide.
orthodontists traditionally consider restored oral health, function, and aesthetics as the principal therapeutic goals. However, improved aesthetics and its positive psychosocial impact are increasingly being accepted as important benefits of treatment.Personal aesthetic perceptions of the dentofacial complex and the associated psychosocial impact are of great consequence to orthodontic patients. The face is the most readily apparent feature and thus is said to be the most important physical characteristic in the
development of self-image and self-esteem, as positive social interactions have been shown to result in better interpersonal relationships and more self-confidence (1, 2, 23).
As malocclusion, particularly that present in the anterior region, is often conspicuous, it may elicit unpleasant social reactions and a poor self-concept (3-
5). Any significant deviations from the norm may result in feelings of insecurity related to appearance, inhibition in social contacts, and comparison of self with others considered to be ‘superior’, all of which may negatively
affect the quality of life of the individual (7-9).orthodontic treatment may be more often influenced
by demand than by need (10,11). In the past, the need for orthodontic treatment was assessed from a strictly professional perspective, taking on a more paternalistic approach from the caregiver. However, several studies have stated that self-perceived dental appearance is also important in the decision to seek orthodontic
Attention (11,12). Different scales, such as the Index of orthodontic Treatment Need (IoTN), the Dental Aesthetic Index (DAI), and the Index of Complexity outcome and Need (ICoN) were developed as a scoring system for malocclusion, and may be used to screen potential patients (10,13,14, 23).
The IoTN is a scoring system that ranks malocclusion

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 17
based on occlusal traits for oral health and aesthetic impairment. The Aesthetic Component (AC) of the IoTN has commonly been used to evaluate treatment need on aesthetic grounds assessed by dentists (operator-rated) or patients (self-rated) (15,16). However, since it is an accepted fact that psychosocial consequences due to unacceptable dental aesthetics may be as serious, or even more serious, than the biologic problems, the indices currently in use have been criticized as lacking a psychosocial Component (5,10,17).
The ‘psychosocial impact’ of malocclusion is a phenomenon that may provoke an emotional reaction manifested as insecurities related to appearance, inhibition in social contacts, feelings of unhappiness and comparison of self with others (4,9).
The present study was undertaken with the objective to determine the psychological as well as social impact of dental aesthetics using the ‘Psychosocial Impact of Dental Aesthetics Questionnaire’ (PIDAQ) and self rated Aesthetic Component (AC) of the Index of orthodontic Treatment Need (IoTN).
MethodologyThis was a cross-sectional study
conducted from February 2014 to May 2016. The study group consisted of doctors (medical and dental), and orthodontic patients.
The inclusion criteria of this study was that the patients being above 18 years of age and having no previous history of orthodontic treatment. The exclusion criteria included patients without previous orthodontic treatment, and presence of craniofacial syndromes or anomalies.
The ‘Psychosocial Impact of Dental Aesthetics Questionnaire’ (PIDAQ) developed by Klages et al. was slightly modified for this study (17).
The reliability analyses of the four factorial analysisderived scales were highly consistent as confirmed by Cronbach’s a values ranging from 0.83-0.92 (17).
The questionnaire was self-administered by the subjects, with the likert scale being used to rate the responses on a scale ranging from 0 (total disagreement) to 4 (total agreement). A total of four variables including ‘Dental Self-confidence’, ‘Social impact’, ‘Psychological impact’ and ‘Self-perceived orthodontic treatment need’ were assessed by a series of relevant statements (Fig. 1) (15,17).
Fig. 1: Questionnaire on Psychosocial Impact of Dental Aesthetics (PIDAQ)
From this questionnaire:Question 1-4 is ‘Dental Self-confidence’ variable, Question 5-10 is ‘Social impact’ variable,Question 11-18 is ‘Psychological impact’ variable,Question 19-21 is ‘Self-perceived orthodontic treatment need’ variable.
Dental aesthetics were assessed using the IoTN Aesthetic Component (AC).The subjects were presented with 10 black and white photographs of anterior teeth displaying varying degrees of malocclusion (fig. 2), and were asked to indicate which grade of photograph (1 to 10) they thought most closely resembled their own dentition.

Revista Stomatologjike Shqiptare18
According to the 10 black and white photographes of anterior teeth shown to you, which photograph do tou feel resembles your dentition most closely?
Based on these photographs:Grade 1 (photo 1)-no abnomality,Gradae 2 (photo 2)-light abnomality,Grade 3 (photo 3)-middle abnomality,Grade 4 (photos 4-10)-severe abnomality.
The Kruskal-Wallis test was applied to determine differences between the mean scores for all the subject groups (1 to 4+) for each of the four variables under study. P-value equal to or less than 0.05 was taken as statistically significant. Statistical analyses were performed using SPSS for Windows (version 14.0).
To assess the psychosocial impact of dental aesthetics on the emotional state of an individual, the mean values were compared amongst the four subject groups for each of the variables.
Results
1 6
2 7
3 8
4 9
5 10
The sample consisted of 160 adults with a mean age of 22.3 years (SD + 2.8 years), and a predominantly female.
of the total sample, 15% of respondents rated their dental appearance as IoTN-AC grade 1 (constituting Group 1), 16,3% placed themselves as IoTN-AC grade 2 (Group 2), 17,5% rated themselves as IoTN-AC grade 3 (Group 3), whereas 51.3% of the subjects rated their dental aesthetics as IoTN-AC grades 4 to 10. (Fig. 3).
Fig. 2: Index IOTN-AC

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 19
Fig. 3: Distribution of subjects based on grades of IOTN-AC
Fig. 4: Përgjigjet e IOTN-së
Fig. 4: Distribution of subjects based on grades of IOTN-AC
Highest is grade 4, with significant change comparing with other grades, (χ2 = 61.03 p=0.0001).
‘Dental Self-confidence’ was found to be highest for subjects rating themselves as IoTN-AC grade 1 (mean score 12.9), and lowest for IoTN-AC grades 4 and above.
‘Social impact’ was greatest for respondents scoring themselves as IoTN-AC grades 4 and above (mean score 9.4), and least for those evaluating their dental appearance as IoTN-AC grade 1 (mean score 3.1), with IoTN-AC grades 2 and 3 again scoring in between with mean scores of 4.2 and 5.7 respectively, (p=0.004).
‘Psychological impact’ was found to be of highest in
individuals who rated themselves as resembling IoTN-AC grades 4 and above (mean score 15.3), and lowest in those rating themselves as IoTN-AC grade 1 (mean score 4.9), followed by IoTN-AC grades 2 and 3 (mean scores 8.9 and 11.1 respectively) (p=0.000).
‘Self-perceived orthodontic treatment need’ was determined to be highest in IoTN-AC grades 4 and above (mean score 5.2), progressively decreasing along the IoTN-AC scale (mean score 3.8 for IoTN-AC grade 3 and 2.9 for grade 2), and being the least for IoTN-AC grade 1 (mean score 2.8), being significantly different amongst the groups (p=0.007).

Revista Stomatologjike Shqiptare20
Analysing these variables between genders, the results was (Fig. 4):
Fig. 4: Comparison of variables between gendersIn male, psychosocial Impact (p=0.04), social (p=0.004)
and dental self-confidence’ (p=0.0009), is lower than female.
DiscussionAssessment of psychosocial factors of malocclusion
has usually concentrated on children, and only recently have psychosocial evaluations been considered an important part of the orthodontic examination in adults (1,3,4,7, 9, 12,17-19).
With respect to IoTN-AC grading as perceived by the subjects themselves (self-rated IoTN-AC), it was found that the majority of raters placed themselves as IoTN-AC grades 4 or higher (51,3%), followed by IoTN-AC grade 3, grade 2, and the least number of respondents placed themselves as IoTN-AC grade 1.
Klages et al. found that although the greatest number of subjects evaluated themselves as IoTN-AC 1 (33.5%), only 8.8% of respondents placed themselves as IoTN-AC grades 4 or above.
For each of the variables, namely, ‘Dental Selfconfidence’, ‘Social impact’, ‘Psychological impact’ and ‘Perceived orthodontic treatment need’, the comparison between mean values amongst the four subject groups (self-rated IoTN-AC 1 to 4+) clearly indicate the strong psychosocial impact of altered dental aesthetics. ‘Dental Self-confidence’ indicates the level of satisfaction or dissatisfaction with the appearance of one’s dentition, and aims to measure the influence of dental aesthetics on the self-image of an individual.
The results of the present study suggest a trend of decreasing dental self-confidence with increasing levels of altered aesthetics, as perceived by the respondents themselves using the IoTN-AC. Klages et al. showed similar results in their study, corroborating that a set of well-aligned teeth (as depicted by lower scores on the IoTN-AC scale) may be associated with more favourable
oral-health attitudes, and a higher degree of satisfaction regarding dental attractiveness resulting in better self-concept (17,19).
‘Social impact’ aims to assess the potential problems an individual may face in social situations due to a subjectively unfavourable dental appearance. In the present study, an increasingly high social impact has been noted in respondents denoting themselves as IoTN-AC grades 4 and above, highlighting the negative influence of unpleasant aesthetics in social interactions.
‘Psychological impact’ evaluates feelings of inferiority
or unhappiness related to an individual’s comparison of self with others. The highly statistically significant group differences in the study shows the relationship of diminishing psychological well-being with increasingly poor dental aesthetics. Klages et al. show results in parallel to ours, with IoTN-AC grades 1 to 4 and above demonstrating an increasing trend of psychological effect along the IoTN-AC spectrum, (17, 23). ‘Perceived orthodontic treatment need’ assesses the subjective need for orthodontic attention, and as the results indicate, is found to be highest in individuals classifying themselves as IoTN-AC grade 4 and above. onyeaso et al. reported that 56.6% of all their subjects reported for orthodontic treatment for aesthetic purposes (20).
The results from this study are also conclusive in denoting the psychological as well as social impacts of malocclusion, with an inverse association being perceived between the IoTN-AC grading with psychosocial well-being. Thus, the IoTNAC may be considered an effective tool in assessing the psychosocial impact of dental aesthetics.
ConclusionMalocclusion has a psychological impact in
adolescents and adults. This impact increases with the severity of malocclusion. Social class may not influence this association, but gender has some effect, because the psychological impact is greater in girls.
It seems prudent to endorse the benefits of orthodontic treatment based on the need as assessed normatively by the orthodontist and subjectively as perceived by the patient.
The association between self-rated IoTN-AC grading with psychosocial well-being stands established, indicating that the perceived aesthetics of the malocclusion may be as significant a factor in determining treatment need as the degree of malocclusion. Although, the AC is effective in determining the detrimental effects of altered dental aesthetics, the recommendations for an index incorporating a psychometric scale for assessment of orthodontic-specific aspects of quality of life still stand strong.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 21
1. Bos A, Hoogstraten J, Prahl-Andersen B. Expectations of treatment and satisfaction with dentofacial appearance in orthodontic patients. Am J orthod Dentofacial orthop 2003; 123:127-32.
2. Social thought and social behaviour. In: Baron RA. Essen-tials of psychology. 2nd ed. Massachusetts: Allyn & Bacon; 1999.p.535-66.
3. Tung AW, Kiyak HA. Psychological influences on the timing of orthodontic treatment. Am J orthod Dentofacial orthop 1998; 113:29-39.
4. Marques lS, Ramos-Jorge Ml, Paiva SM, Pordeus IA. Maloc-clusion: esthetic impact and quality of life among Brazilian school children. Am J orthod Dentofacial orthop 2006; 129:424-7.
5. Soh J, Chew MT, Chan YH. Perceptions of dental esthetics of Asian orthodontists and laypersons. Am J orthod Dentofa-cial orthop 2006; 130: 170-6.
6. Rinchuse DJ, Rinchuse DJ. orthodontics justified as a pro-fession. Am J orthod Dentofacial orthop 2002; 121:93-6.
7. Sarver DM, Proffit WR. Special considerations in diagnosis and treatment planning. In: Graber TM, Vanarsdall Rl, Vig KW, (edi). orthodontics: current principles and techniques. 4th ed. Missouri: Elsevier; 2005.p.4-9.
8. Morphopsychology and esthetics. In: Rufenacht CR. Funda-mentals of esthetics. Illinois: Quintessence Publishing Co; 1990.p.59-66.
9. Klages u, Bruckner A, Zentner A. Dental aesthetics, self-awareness, and oral health-related quality of life in young adults. Eur J orthod 2004; 26:507-14.
10. Jarvinen S. Indexes for orthodontic treatment need. Am J orthod Dentofacial orthop 2001; 120:237-9.
11. Bernabe E, Kresevic VD, Cabrejos SC, Flores-Mir F, Flores-Mir C. Dental esthetic self-perception in young adults with and without previous orthodontic treatment. Angle orthod 2006; 76: 412-6.
12. Espeland lV, Stenvik A. Perception of personal dental ap-pearance in young adults: relationship between occlusion, awareness, and satisfaction. Am J orthod Dentofacial or-thop 1991;100: 234-41.
13. Brook PH, Shaw WC. The development of an index of orth-odontic treatment priority. Eur J orthod 1989; 11:309-20.
14. Firestone AR, Beck FM, Beglin FM, Vig KW. Validity of the Index of Complexity, outcome and Need (ICoN) in deter-mining orthodontic treatment need. Angle orthod 2002; 72:15-20.
15. Grzywacz I. The value of the aesthetic component of the index of orthodontic treatment need in the assessment of subjec-tive orthodontic treatment need. Eur J orthod 2003; 25:57-63.
16. Hunt o, Hepper P, Johnston C, Stevenson M, Burden D. The aesthetic component of the index of orthodontic treat-ment need validated against lay opinion. Eur J orthod 2002; 24:53-9.
17. Klages u, Claus N, Wehrbein H, Zentner A. Development of a questionnaire for assessment of the psychosocial impact of dental aesthetics in young adults. Eur J orthod 2006; 28:103-11.
18. Kerosuo H, Al Enezi S, Kerosuo E, Abdulkarim E. As-sociation between normative and self-perceived orth-odontic treatment need among Arab high school stu-dents. Am J orthod Dentofacial orthop 2004; 125:373-8.
19. Klages u, Bruckner A, Guld Y, Zentner A. Dental esthetics, orthodontic treatment, and oral-health attitudes in young adults. Am J orthod Dentofacial orthop 2005; 128:442-9.
20. onyeaso Co, utomi Il, Ibekwe TS. Emotional effects of malocclusion in Nigerian orthodontic patients. J Contemp Dent Pract 2005; 6: 64-73.
21. Varela M, Garcia-Camba JE. Impact of orthodontics on the psychologic profile of adult patients: a prospective study. Am J orthod Dentofacial orthop 1995; 108:142-8.
22. Mandall NA, Wright J, Conboy F, Kay E, Harvey l, o’Brien KD. Index of orthodontic treatment need as a predictor of orthodontictreatment uptake. Am J orthod Dentofacial or-thop 2005; 128:703-7.
23. Munizeh Khan and Mubassar Fida, Assessment of Psycho-social Impact of Dental Aesthetics, Journal of The College of Physicians and Surgeons Pakistan 2008, Vol. 18 (9): 559-564.
REFERENCES

Revista Stomatologjike Shqiptare22
AbstraktZvogëlimi i dimensionit vertikal tek pacientët me proteza totale shpeshherë përcillet me probleme funksionale dhe estetike. Ky problem më shpesh është prezent tek pacientë të cilët kanë proteza të vjetra (më tepër se 10 vjet), por mund të paraqitet edhe tek pacientë me proteza të cilat nuk janë më të vjetra se 5 vjet.
Qëllimi i prezantimit është mundësia për rekonstruim të dimensionit vertikal të zvogëluar tek pacientët me proteza totale të punuara më parë, pa i ndërruar të njejtat.
Në QKu Klinika për protetikë mobile stomatologjike- Shkup është pranuar pacient 72 vjeçar me anodonci (padhëmbësi) totale në nofullën e sipërme dhe atë të poshtme e sanuar me proteza totale. Gjashtë vite pas punimit të protezave totale, pacienti ankohet për “kollabim të protezës” (fundosje të protezës), por nuk dakordohet të punohen proteza të reja. Zgjidhja është rebazimi indirekt i protezës së poshtme njëkohësisht duke e zmadhuar dimensionin vertikal.
Me këtë veprim me sukses është arritur korigjimi i raportit të çrregulluar ndërnofullor, përmirësimi i estetikës dhe funksioni i sistemit stomatognat.
Fjalët kyçe:
Rebazim,
mbushje,
raport
ndërnofullor,
proteza totale.
Sanja panchevska, Darko gjorgjievski, Sasho elenchevski, Nadica janeva, Faton vojnika
Rebazimi i protezës totale në kushte të zvogëlimit të dimensionit vertikal- përshkrimi i një rasti klinik
Universiteti “Sh. Qirili dhe Metodi” Fakulteti i Stomatologjisë- Shkup
Përcaktimi i saktë i dimensionit vertikal (DV) tek bartësit e protezave totale është i një rëndësie të veçantë për funksionet e sistemit stomatognat por, edhe për një estetikë dhe profilaksë të indeve biologjike tek këta pacientë. Për shkak se resorbimi i kreshtës alveolare residuale është proces kronik dhe nuk ndalet me punimin e protezave totale, me kalimin e kohës vjen deri tek ndryshimet në DV (Knezovic-Zlataric D 2002). Abrazioni i dhëmbëve artificial të protezës totale gjatë funksionit është një nga faktorët që sjellin në zvogëlimin e DV dhe kjo rezulton me humbjen e stabilitetit dhe retencionin e protezës. E gjithë kjo çon deri te çrregullimi i funksionit mastikator, por edhe i funksioneve tjera të sistemit stomatognat. Ndryshimet e këtilla janë shkak për ankesa të shpeshta të pacientëve për ndjenjën në rritje të paqëndrueshmërisë dhe diskomforit të protezave. Tek pacientët të cilët i mbajnë të njëjtat proteza një kohë më të gjatë (10 vjet apo më gjatë) zvogëlimi i DV është aq i shprehur saqë vjen deri te ndryshimi i pozicionit të mandibulës, d.m.th. ajo rrëshqet sipër dhe përpara dhe vjen në pozitën e dhëmbëve teh më teh ose në kafshim progenik (Hadjieva H. 2014). Ndryshimet estetike mund të përcillen me praninë e fisurave dhe ragadave në këndet e gojës apo të buzëve. Problemet e shfaqura mund të zgjidhen me mbushje (shtuarje të një shtrese të re të akrilatit), rebazim (zëvendësim të akrilatit të vjetër me akrilat të ri, vetëm dhëmbët mbeten) ose tek rastet më të vështira me punimin e protezave të reja.
Humbja e retencionit dhe stabilitetit, kollapsi dimensionit vertikal, paksimi i shikueshmërisë së dhëmbëve gjatë të folurit, degjenerimi i bazës dentale dhe zvogëlimi i ekstensionit të protezës në pjesët mukobukale janë kriteriumet të cilat na udhëzojnë në vendimin tonë për mbushje apo rebazim të protezave totale (Christensen G. 1995).
Qëllimi i këtij punimi është të prezantojmë metodë të modifikuar të rebazimit të protezave totale si mënyrë për korigjim të zvogëlimit (prishjes) të DV.
Përshkrimi i rastitNë QKu Klinika për protetikë mobile stomatologjike-
Shkup është pranuar pacient 72 vjeçar me anodonci (padhëmbësi) totale në nofullën e sipërme dhe atë të poshtme e sanuar me proteza totale. Gjashtë vite pas punimit të protezave totale, pacienti ankohet për “kollabim të protezës”, ndjenjën e lëvizshmërisë dhe diskomfortit të shtuar. Pacienti nuk është dakord të punohen proteza të reja sepse deri para pak kohe ka qenë i kënaqur me funksionin dhe estetikën e protezave totale. Mungesa e abrazionit të dhëmbëve prej akrilati të protezës si dhe gjendja e mirë e protezave (baza e akrilatit e padëmtuar, higjiena e mirë) janë faktorë të cilët ndikojnë në vendimin tonë që të mos punohen proteza të reja, ndërsa ndjenja e diskomfortit dhe lëvizshmërisë në rritje e protezës totale të poshtme të zgjidhet me rebazimin e saj.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 23
Pacienti ka një resorbim të theksuar të kreshtës alveolare reziduale të poshtme dhe zvogëlim të dimensionit vertikal (f. 1 dhe f. 2a e 2b).
Për tu arritur zmadhimi i dëshiruar i DV, pas kontrollit të okluzionit, vendosen mbrojtës të hapësirës nga masa termoplastike duke u kujdesur që pacienti të mbyll gojën në okluzion qendror (f. 3a dhe 3b). Mbajtësit e hapësirës janë të vendosur nga një në regjionin distal dhe një në pjesën frontale. Për shkak se tehet e protezës së poshtme tani nuk kanë kontakt me mukozën e gojës nuk ka nevojë të gdhenden. Hapsira ndërmjet mbajtësve mbushet me masë termoplastikie të zbutur dhe në pozicion të okluzionit qendror pacienti kryen lëvizje funkcionale
(f. 4a dhe 4b). Pas kontrollit të DV pason marrja e masës funkcionale në okluzion me masë elastomere. Procedura në laboratorin stomatologjik është e njejtë me rebazimin indirekt klasik ndërrohet i gjithë akrilati dhe mbeten vetëm dhembët e protezës (f. 5a, 5b dhe 6).
Diskutim Edhe tek protezat e punuara në mënyrë ideale pas një
periudhe kohore mund të vijë deri tek zvogëlimi i retencionit dhe stabilitetit si pasojë e resorbimit të zmadhuar të kreshtës alveolare. Nuk ekziston një përgjigje e saktë në pyetjen nëse protezat që shkaktojnë ndjenjën e diskomforit tek pacienti
duhet të mbushen, rebazohen apo të zëvendësohen me të reja. Knechtel dhe loney theksojnë se per një numër të madh të pacientëve mbushja dhe rebazimi i protezave si metodë për përmirësimin e retencionit dhe stabilitetit kanë domethënie ekonomike. Sipas Garret dhe bashkëpunëtorëve të tij, gati të gjithë pacientët pas mbushjes tregojnë se kanë rritje të komforit, përmirësim të mastikacionit dhe me të edhe pakësim të vështirësive gjatë ngrënies të ushqimit të fortë, ndërsa shumica prej tyre vërejnë edhe përmirësim të të folurit si dhe ndjenjë sigurie gjatë mbajtjes së protezave.
PërfundimKontrollet e rregullta të pacientëve me proteza tek
specialisti (njëherë në vit), janë të domosdoshme me qëllim që indet e buta të hapësirës së gojës të mbahen në gjendje të mirë, të ndiqet shkalla e resorbimit kockor dhe të gjitha me qëllim të kontrollohen ndryshimet e DV që të mund të kryhen korigjime të caktuara përpara se të ndodhin ndryshime në funksionin e sistemit stomatognat. Në raste kur është evident ndryshimi i DV, rebazimi i protezave totale i kryer në mënyrën e përshkruar jep mundësi për korigjimin e tij, njëkohësisht përmirëson estetikën dhe të folurit, por para së gjithash retencionin dhe stabilitetin. E gjithë kjo sjell deri te zmadhimi i ndjenjës së komforit tek bartësit e protezave totale.
Fig. 1: Kreshta reziduale e poshtme e resorbuar Fig. 2: Zvogëlimi i dimensionit vertikal
Fig. 3: a) Mbajtës të hapësirës b) Masa në okluzion qëndror
a) b)

Revista Stomatologjike Shqiptare24
1. Knezovic-Zlataric D, Celebic A, lazic B. Resorptive changes of maxillary and mandibular bone structures in removable denture wearers. Acta stomat Croat. 2002; 36(2): 261-265.
2. Hadjieva H, Dimova M, Hadjieva E, Todorov S. Changes in the vertical dimension of occlusion during different periods of complete denture wear – a comparative study. J of IMAB. 2014; 20(3): 546-549.
3. Christensen JG. Relining, rebasing partial and complete dentures. JADA 1995; 126(40): 503-506.
4. Anderson F. Monica. Reline, rebase or remake: The denture dilemma. 2009; www. drbicuspid.com
5. Knechtel EM and loney WR. Improving the outcome of denture relining. JCDA 2007; 73(7): 587-591.
6. Garret NR, Kapur KK, Perez P. Effects of improvement of poorly fitting dentures and new dentures on patient satis-faction. J Prosthet Dent 1996; 76(4): 403-13.
REFERENCA
Fig. 4: a) Masë me material termoplastik b) Masë funksionale
Fig. 5: DV i rregulluar (restauruar) pas rebazimit Fig. 6: Proteza totale pas rebazimit.
a) b)

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 25
Abstract The decrease of the vertical dimension in patients with complete dentures often is followed by functional and aesthetic problems. This problem is bigger in patients which dentures are much older (some times more than 10 years) but it could also happen in patients with mush newer dentures (less than 5 years).
The aim of this report is to present the possibility to correct the decreased vertical dimension in patients with complete dentures without making new one.
A 72 years old completely edentulous patient was admitted at the uDCC - Department for removable dentures in Skopje. The patient’s complete dentures were made six years ago and he complains of „dentures meltdown“. The patient does not accept to make new ones. Method of choice is increasing the vertical dimension during the indirect rebasing of the lower complete denture.
With this procedure the correction of the vertical dimension was successful as well as the improvement of the aesthetic and the function of the stomatognatic system.
keywoRDS:
rebasing,
relining,
intermaxillary
relationship,
complete
dentures.
Sanja pancevska, Darko gjorgjievski, Sasho elençevski, Nadica janeva, Faton vojnika
Complete dentures rebasing in case of decreased vertical dimensionCase report
Department for prosthodontics - PDO Dental Care
The precise determination of the vertical dimension (VD) in complete denture wearers is of great significance to the maintenance of stomatognatic function, the prophylaxis of oral soft tissues and jawbone, as well as the preservation of their esthetic integrity. Because the resorption of the residual alveolar ridge is a chronic process and does not stop during the use of complete dentures, a change in the VD occurs with time (Knezovic-Zlataric D 2002)1. The wasting of artificial teeth in complete dentures is another factor that contributes in the reduction of VD, resulting in a loss of stability and retention. All of this leads to disturbances in the masticatory and other functions of the stomatognatic system. These changes are the reason for the frequent patient complaints regarding the increase in discomfort and looseness of the dentures. In patients who have been using the same dentures for longer periods of time (>10 years), the reduction in VD is pronounced to the point of mandibular propulsion (Hadjieva H. 2014)2. The esthetic changes may be emphasized by fissures and angular chelitis. These problems can be solved by relining (adding a new layer of acrylic resin), rebasing (replacing the entire acrylic base), or in the most difficult cases with a completely new complete dentures. The loss of retention and stability, reduction in VD, decreased visibility of the teeth during speech, degeneration of the dental base and reduced extension of the dentures in the muco-buccal segments are the criteria which
should guide us in the decision to reline or rebase the removable dentures (ChristensenG. 1995)3.
The goal of this study is to present a modified method for rebasing existing complete dentures, as a way of restoring the VD.
Case-reportA 72 year old complete denture wearer was seen
at the uDCC Clinic for removable dentures – Skopje, presenting with lowered dentures, a feeling of looseness, and increased discomfort. The patient is not consenting to the fabrication of new dentures due to a certain level of satisfaction by the current complete dentures. The absence of abrasion on the artificial teeth, as well as the overall condition of the dentures (no visible damage on the acrylic base, well preserved oral hygiene) contribute to our decision not to fabricate new dentures, but to solve the problem of increased discomfort and looseness by rebasing the lower complete denture. The patient has a severe resorption of the lower alveolar ridge and a decrease in VD, and in such conditions the method of choice is indirect rebasing of the lower complete denture, therefore providing an increase in VD. (fig. 1, fig.2)
In order to achieve the increase in VD, after evaluation of the occlusion, gap holders from a thermoplastic compound were placed on the oral surface of the lower denture (fig. 3). Two gap holders were placed bilaterally

Revista Stomatologjike Shqiptare26
in the post canine region, and one in the front. In this position, the denture is not in contact with the oral mucosa, therefore there is no need for shortening of the denture flanges. The gap between the holders is filled with a softened thermoplastic compound, and in central occlusion, the patient is instructed to make functional movements (fig. 4). After control of the VD, a functional impression in central occlusion was taken with impression material. The procedure in the dental laboratory is identical to the one used in classic indirect rebasing (fig. 5, fig. 6)
DiscussionEven in perfectly manufactured dentures, a reduction
in retention and stability can appear as a result of the increased resorption of the alveolar ridge. Currently, there is no definitive answer on whether to reline, rebase or completely replace dentures that are causing discomfort4. As described by Knechtel & loney, for most patient, denture relining is an economical means of improving a
dentures stability and retention, the overall occlusal VD, and in some cases facial appearance5. Increased comfort, improved mastication, and improvement of the ability to consume solid foods, as well as an improvement in speech and the overall attitude of the patient towards the dentures can be seen in the majority of the patients after denture relining (Garret et al)6.
ConclusionRegular prosthodontics check-ups (once per year)
are essential for complete denture wearers in order to preserve the soft tissues and to track the rate and severity of alveolar resorption. The goal of this is to control the changes in VD, and to make certain adjustments before stomatognatic function is compromised. In cases where there is a noticeable reduction in VD, using the method described in this paper allows for certain adjustments, resulting in improved esthetics and speech, but above all, improved retention and stability. All of this leads to an increase in the denture wearers comfort.
Fig. 1: Resorbed residual alveolar ridge Fig. 2: a) A reduction in the vertical dimension (VD) b) Intraoral view
Fig. 3: a) Gap holders b) impression in central occlusion
a) b)

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 27
1. Knezovic-Zlataric D, Celebic A, lazic B. Resorptive changes of maxillary and mandibular bone structures in removable denture wearers. Acta stomat Croat. 2002; 36(2): 261-265.
2. Hadjieva H, Dimova M, Hadjieva E, Todorov S. Changes in the vertical dimension of occlusion during different periods of complete denture wear – a comparative study. J of IMAB. 2014; 20(3): 546-549.
3. Christensen JG. Relining, rebasing partial and complete dentures. JADA 1995; 126(40): 503-506.
4. Anderson F. Monica. Reline, rebase or remake: The denture dilemma. 2009; www. drbicuspid.com
5. Knechtel EM and loney WR. Improving the outcome of denture relining. JCDA 2007; 73(7): 587-591.
6. Garret NR, Kapur KK, Perez P. Effects of improvement of poorly fitting dentures and new dentures on patient satis-faction. J Prosthet Dent 1996; 76(4): 403-13.
REFERENCES
Fig. 4 - a) impression with thermoplastic compound b) functional impression
Fig. 5 – A restored vertical dimension after rebasing
Fig. 6 –Complete denture after rebasing
a) b)

Revista Stomatologjike Shqiptare28
AbstraktKafshimi i kryqëzuar anterior është një nga anomalitë mjaft të ndeshura tek fëmijët, të cilët janë në periudhën e rritjes. Hapi i parë që duhet të bëjmë atëherë kur trajtojmë një kafshim të kryqëzuar anterior është të përcaktojmë nëse ai është me natyrë dentare apo skeletale. Atëherë kur anomalia është me natyrë dentare, akset e incisivëve superiorë nuk janë të pozicionuar korrekt, ndërsa kur anomalia është me natyrë skeletale mund të hasim retrognaci maksilare, prognaci mandibulare ose një kombinim të të dyjave.
Korrigjimi i kafshimit të kryqëzuar anterior është një procedurë mjaft e zakonshme në ortodonci dhe një nga mënyrat e trajtimit është dhe me aparate fikse. Trajtimi i kësaj anomalie rekomandohet me qëllim ruajtjen nga frakturat e dhëmbëve fontalë, mbrojtjen nga abrazioni, parandalimin e patologjive parodontale, për të përmirësuar estetikën dhe për të patur një okluzion korrekt. Diagnoza diferenciale ndërmjet një kafshimi të kryqëzuar anterior me natyrë dentare dhe asaj me natyrë skeletale është thelbësore në trajtimin e anomalisë. Për të vendosur një diagnozë precize duhet të marrim parasysh: ekzaminimin klinik, studimin e radiografive dhe analizën e modeleve.
Fjalët kyçe:
Kafshim i
kryqëzuar
anterior,
denticion miks
i vonët, briketa
self-ligating
Damon Q,
trajtim eficient
dhe i shkurtër.
manjola gusho, Xhina mulo
trajtimi i klasës së iii me kafshim të kyqëzuar anterior me aparat fiks self-ligating. Rast klinik
Fakulteti i Mjekësisë Dentare
HyrjeTrajtimi i anomalisë së klasës së III fillon me diagnozën
diferenciale të kafshimit të kryqëzuar. Situatat intraorale, të cilat i hasim në një klasë III mund të jenë:
a) Proklinim i incisivëve frontalë inferiorë dhe retroinklinim i atyre superiorë. Mandibulën në këtë rast e gjejmë në një pozicion më anterior, gjë e cila përkufizohet si një pseudo klasë III. Për fat të keq studimi i cefalometrisë nuk na jep gjithmonë një përgjigje nëse anomalia është për defekt të maksilës apo mandibulës. Më shumë informacion na jep gjendja intraorale e pacientit.
b) Retroinklinimi i incisivëve inferiorë dhe proklinimi i atyre superiorë si dhe kontakti frontal ndërmjet këtyre, majë më majë apo kafshim i kryqëzuar anterior. Këto fenomene njihen dhe si fenomene kompensuese në ortodonci.
Trajtimi i hershëm i klasës së III mund të na ndihmojë në minimizimin e fenomeneve kompensuese që sapo folëm më lart.
Ekzistojnë disa protokolle pune për të trajtuar kafshimet e kryqëzuara anteriore. Ai që do të prezantojmë në këtë artikull është trajtimi me një fazë të vetme, me aparate fikse self-ligating, Damon Q.
QëllimiTrajtimi ka për qëllim të stimulojë rrijen e maksilarit,
korigjimin e kafshimit të kryqëzuar anterior, të ruhet klasa e I dentare në nivel molar dhe të arrihet klasa e I në nivel të kaninëve, të realizohet përputhja e vijës mediane inferiorë me atë superiorë, të zgjidhen grumbullimet dentare në maksilar dhe të përmirësohet estetika e pacientit për sa i përket buzëqeshjes dhe profilit.
Materiale dhe MetodaAnamneza:Pacienti l.B, i seksit mashkull, 11 ½ vjeç, me denticion
mikst të vonët. Prindi i pacientit kërkon trajtim ortodontik me qëllim korigjimin e kafshimit të kryqëzuar anterior. Higjiena dentare e pacientit paraqitet e kënaqshme.
Diagnoza dhe etiologjiaPacienti paraqet fytyrë brahifaciale, simetria e
fytyrës është e ruajtur, profil konkav të shoqëruar me inkompetencë labiale dhe shkallë të buzëve të inversuar (Fig. 1).

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 29
Pacienti (prindi) kërkon trajtim ortodontik për të korrigjuar kafshimin e kryqëzuar anterior. Në harkun dentar maksilar vihen re grumbullime të mëdha dentare, me mungesë totale për rreshtimin e kaninit djathtas dhe në harkun mandibular grumbullime dentare minimale. Pacienti paraqet klasë I dentare në nivel molar majtas dhe djathtas, të shoqëruar me kafshim të kryqëzuar anterior dhe diskrepancë Co-CR. Vija mediane inferiore është e devijuar djathtas me 2 mm në Co (Fig.2). Nga studimi i panorameksit vihet re që denticioni permanent është normal i zhvilluar, me prezencë të mugureve të molarëve të pjekurisë (Fig.3).
Fig. 1. Fotot ekstraorale para trajtimit
Nga ekzaminimi klinik u vu re një denticion mikst i vonët me persistencë të molarëve të dytë të qumështit mandibular (Fig. 2).
Fig. 2. Fotot intraorale para trajtimit
Fig.3. Panorameks - para trajtimit
Nga studimi i cefalometrisë rezultoi një tendencë për klasë të III (ANB = -1mm), rritje skeletale normodivergente (FM = 27mm, MM = 28mm). Aksi i incisivëve superiorë paraqitet normal (Inc sup to Max Pl = 1090), ndërsa i incisivëve inferiorë më i zvogëluar (Inc inf to Mand Pl = 860) (Fig. 4).
Fig. 4. Cefalometri – para trajtimit
Albanian Stomatological Journal30
Babai i pacientit paraqet një kafshim me mbimbulim minimal të dhëmbëve frontalë inferiorë.
Etiologjia e anomalisë mendohet të jetë me natyrë të kombinuar: e trashëguar si dhe për shkak të faktorëve të tjerë mjedisorë.
Plani i trajtimitMeqënëse pacienti është në periudhën e rritjes,
qëllimi kryesor i trajtimit është të korrigjohet kafshimi i kryqëzuar anterior nëpërmjet stimulimit të rritjes së maksilarit.
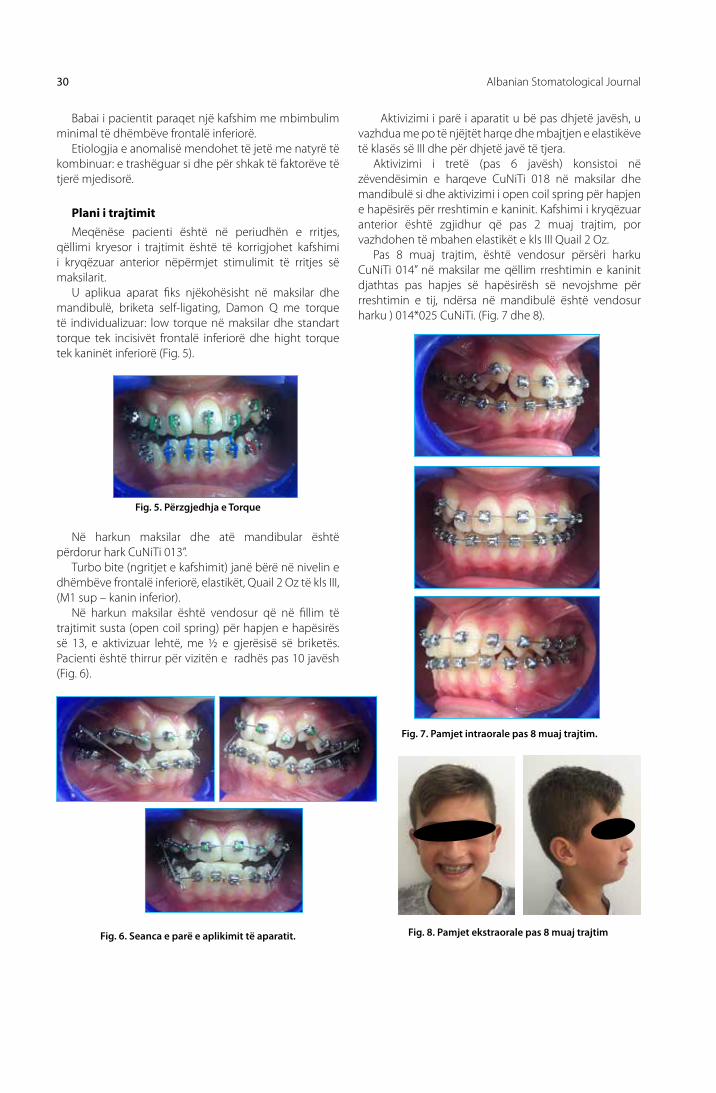
u aplikua aparat fiks njëkohësisht në maksilar dhe mandibulë, briketa self-ligating, Damon Q me torque të individualizuar: low torque në maksilar dhe standart torque tek incisivët frontalë inferiorë dhe hight torque tek kaninët inferiorë (Fig. 5).
Fig. 5. Përzgjedhja e Torque Në harkun maksilar dhe atë mandibular është
përdorur hark CuNiTi 013”. Turbo bite (ngritjet e kafshimit) janë bërë në nivelin e
dhëmbëve frontalë inferiorë, elastikët, Quail 2 oz të kls III, (M1 sup – kanin inferior).
Në harkun maksilar është vendosur që në fillim të trajtimit susta (open coil spring) për hapjen e hapësirës së 13, e aktivizuar lehtë, me ½ e gjerësisë së briketës. Pacienti është thirrur për vizitën e radhës pas 10 javësh (Fig. 6).
Fig. 6. Seanca e parë e aplikimit të aparatit.
Fig. 7. Pamjet intraorale pas 8 muaj trajtim.
Aktivizimi i parë i aparatit u bë pas dhjetë javësh, u vazhdua me po të njëjtët harqe dhe mbajtjen e elastikëve të klasës së III dhe për dhjetë javë të tjera.
Aktivizimi i tretë (pas 6 javësh) konsistoi në zëvendësimin e harqeve CuNiTi 018 në maksilar dhe mandibulë si dhe aktivizimi i open coil spring për hapjen e hapësirës për rreshtimin e kaninit. Kafshimi i kryqëzuar anterior është zgjidhur që pas 2 muaj trajtim, por vazhdohen të mbahen elastikët e kls III Quail 2 oz.
Pas 8 muaj trajtim, është vendosur përsëri harku CuNiTi 014” në maksilar me qëllim rreshtimin e kaninit djathtas pas hapjes së hapësirësh së nevojshme për rreshtimin e tij, ndërsa në mandibulë është vendosur harku ) 014*025 CuNiTi. (Fig. 7 dhe 8).
Fig. 8. Pamjet ekstraorale pas 8 muaj trajtim

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 31
Sekuenca e harqeve të përdorur ishte 014*025 CuNiTi në maksilar dhe 018*025 CuNiTi në mandibulë, në këtë moment u bënë dhe ripozicionimet e briketave të disa dhëmbëve me qëllim paralelizimin e rrënjëve të dhëmbëve.
Pasi u rreshtuan plotësisht dhëmbët, u përdor hark TMA 019*025 në maksilar dhe TMA 017*025 në mandibulë.
Fig. 9. Pamjet intraorale në fund të trajtimit.
RezultateNga krahasimi i radiografive, modeleve dhe profilit
të fillimit të trajtimit dhe fundit të trajtimit u vu re që objektivat ishin përmbushur: u ruajt klasë e I dentare në nivel molar dhe u arrit dhe klasë e I në nivel kanin, vijat mediane koincidojnë në fund të trajtimit, grumbullimet dentare si në maksilar dhe në mandibulë janë zgjidhur si dhe estika e pacientit, buzëqeshja dhe profili janë përmirësuar në mënyrë të ndjeshme.
Fig.10. Panorameks në fund të trajtimit
Në përfundim të trajtimit, i cili zgjati për rreth 24 muaj, (Fig. 9), u aplikua retainer fiks në mandibulë dhe maksilar si dhe Essix në maksilar.
Pacientit iu dhanë shpjegimet e duhura për mirëmbajtje e retainer, essix do të mbahet vetëm natën dhe pacienti duhet të paraqitet në vizita pas tre, gjashtë dhe një vit pas heqjes së aparatit.
Panorameks në fund të trajtimit tregon një paralelizëm të rrënjëve të dhëmbëve, pa rezorbime të tyre apo kockës përreth. (Fig. 10)
Nga krahasimi i cefalometrisë para dhe pas trajtimit, u vu re që maksilari kishte avancuar anterior me 40. Gjithashtu u vu re dhe një proklinim i incisivëve superiorë më qëllim korigjimin e kafshimit të kryqëzuar anterior (Fig. 11 dhe tabela 1)
Fig. 11. Cefalometria para dhe pas trajtimit

Albanian Stomatological Journal32
Tabela 1.
Fig. 12. Buzëqeshja dhe profili i pacientit para dhe pas trajtimit.
KonkluzionePacientët të cilat paraqesin një kafshim të kryqëzuar
anterior janë të lehtë për t’u identifikuar. Atëherë kur kemi një klasë të III skeletale të lehtë dhe denticion miks të vonët ose permanent të hershëm, trajtimi me aparate
fikse ka rezultuar i suksesshëm. Kur kafshimi i kryqëzuar anterior është me natyrë dentare është më lehtë për t’u korigjuar dhe për t’u mbajtur. Korigjimi i kafshimit të kryqëzuar lejon një zhvillim normal të maksilarit.
1. Proffit WR, Fields HW Jr. Contemporary orthodontics. 3rd ed. St. louis, Mo: Mosby; 2000:185-191.
2. McNamara JA Jr. An orthopedic approach to the treatment of Class III malocclusion in young patients. J Clin orthod 1987;21:598–608.
3. lin JX, Huang JF, Zeng Xl. A cephalometric evaluation of hard and soft tissue changes during Class III traction. Eur J orthod 1985;7:201–204.
4. Isabella T, Tiziano B, lorenzo F. Mandibular skeletal changes induced by early functional treatment of Class III malocclu-sion: a superimposition study. Am J orthod Dentofacial or-thop 1995;108:525–532.
5. Rabie ABM, Yan G. Diagnostic criteria for pseudo-Class III mal-occlusion. Am J orthod Dentofacial orthop 2000;117:1-9.
6. Benham NR: Treatment of simple anterior crossbite using a fixed appliance technique. J Dent Child 42:487-88. 1975.
7. Valentine F, Howitt JW: Implications of early anterior cross-bite correction. J Dent Child 37:420-27, 1970.
8. lee BD: Correction of crossbite. Dent Clin North Am 22:647- 68, 1978.
REFERENCA

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 33
AbstractAnterior crossbites are one of the most common orthodontic problems we observe in growing children. When treating an anterior crossbite first of all we should determine if it is dental or skeletal pattern. In dental factors, upper incisor axes are not correctly positioned, meanwhile in skeletal pattern we can find maxillary retrognathia (maxillary retrusion), mandibular prognathism or a combination. This article shows the treatment of Class III malocclusion by correcting anterior dental crossbite with the use of a fixed appliance, self-ligating braces.
This treatment has been recommended for the prevention of fractures of anterior teeth, abnormal enamel abrasions, periodontal pathology, and to produce a more esthetic dentofacial complex with a better occlusion.
Differential diagnosis between dental and skeletal pattern is fundamental for treatment purposes. The diagnose should be based on: clinical exam, radiographs interpretations and study models. A better understanding of features and dental effects of class III malocclusion is thus necessary to establish as an additional base for effective treatment planning.
keywoRDS:
Anterior
crossbite,
late mixed
dentition,
Self -ligating
Damon Q
brackets,
short effective
treatment
manjola gusho, Xhina mulo
treatment of Class iii malocclusion and anterior crossbite with the use of self-ligating Brackets System. Case Report
Fakulteti i Mjekësisë Dentare
Intraoral1- lower incisors proclined and upper incisors
retroclined. Anterior position of the mandible will name it Pseudo class III. unfortunately cephalometric exam cannot always determine if it is maxillary or mandibular deficiency. oral exam major factor for accurate diagnosis.
2- upper incisor proclined and the lower incisors retroclined, premature contact into maximal interdigitation, edge to edge or anterior crossbite. All this clinical findings are part of dento-alveolar compensation which reduces the severity of the incisor relationship.
Early treatment of class III may help minimize the compensation effects mentioned above.
There are many protocols for anterior crossbite treatments; we are going to elaborate one phase treatment, self-ligating system, Damon Q brackets.
The AimThe specific treatment objectives were to stimulate
the growth of the maxilla, eliminate the functional shift and correct the anterior crossbite, maintain the Class I molar and achieve a Class I canine relationship, correct the mandibular dental midline, alleviate the maxillary anterior crowding, procline the maxillary incisors, and improve the smile esthetics.
Materials and methodsPatient’s initials l.B. male 11½ year’s old, late mixed
dentition. Father’s chief complaint is “the under bite”. His oral hygiene was good.
Diagnosis and etiology The patient presented with brachiocephalic,
symmetrical face and a concave type profile, lips incompetent and inversed. (Figure 1).

Albanian Stomatological Journal34
Fig.1. Pre-treatment facial photographs.
Patient’s father presents edge to edge anteriors. The etiology of the malocclusion was determined to be a combination of heredity and environmental factors.
Fig. 2. Pre-treatment intraoral views).
Fig. 3. Pre-treatment panoramic
Clinical Findingslate mixed dentition, over retained deciduous second
molars, maxillary severe crowding, ectopic eruption upper right 3, total inadequate space in the maxillary arch, mild mandibular crowding. (Figure 2)
Right and left molar classification Class I, anterior Crossbite, discrepancy Co-CR. lower midline is deviated 2 mm to the right. Panoramic interpretations determines normal dental growth with the presence of wisdoms follicles. (Figure 3)
Cephalometric analysis revealed a skeletal Class III tendency (ANB= -1o) with normodivergent growth pattern (FM = 27mm, MM = 28mm), (Inc sup to Max Pl = 1090), (Inc inf to Mand Pl = 860). (Figure 4)
Fig. 4. Lateral cephalometric radiographs

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 35
Treatment PlanThe intention during this treatment plan is to
stimulate maxillary growth which will lead to anterior crossbite treatment.
Comprehensive treatment, bond upper and lower, self-ligating bracket with individual torque, low torque for the maxillary, standard torque lower incisors, and high torque lower canines. (Figure 5.)
Fig. 6. First visit
Fig. 8. Ekstraoral view after 8 months in treatment
Fig.7. Intraoral view after 8 months of treatment
First Adjustment after 10 weeks, Retie, same wires and continue elastic use.
Next Adjustment after 6 weeks. Wires u/l CuNiTi 018’ activate open coil for the ectopic
upper right canine, After 2 months anterior crossbite is treated, continue elastic Quail 2 oz
After 8 months maxillaryCuNiTi 014’ to align the upper right canine since we have enough space, for the mandibular wire 014*025 CuNiti. (Fig 7 and 8).
Wires: upper/lower CuNiTi 013’Anterior Turbos, Elastics Quail 2 oz Class IIIupper right 2 to upper right 4 open coil slightly active,
half a bracket length. Next visit after 10 weeks. (Figure 6.)
Fig. 5. Torque selection

Revista Stomatologjike Shqiptare36
Fig. 9. Post-treatment intraoral views
Post-treatment panoramic radiograph showed proper space closure and acceptable root parallelism with no signs of bone or root resorption. (Figure 10.)
Cephalometric interpretation shows: Maxillary anterior advancement 4°, proclined maxillary incisors (Figure 11.)
ResultsRadiographies before and after, intraoral and extra
oral photos and study models show that the purpose of the treatment is accomplished.
After treatment: Molar Class I, canine class I, midlines matches, no more crowding, improved smile, aesthetic, and profile.
Fig.10. Post-treatment. Fig.11. post-treatment lateral cephalometric
Arch wires sequence 012*025 CuNiTi Maxillary and 018*025 CuNiTi mandibular, repositioned some brackets to achieve root parallelism for specific teeth.
At the time that all the teeth were positioned in the arches upgraded to maxillary TMA 019*025 and 017*025
mandibulararch wires.Debond after 24 months, applied fixed mandibular
and maxillary retainer, plus Essix for the Maxilla. (Figure 9.)Stressed home care, Essix night time only and keep
following up after 3, 6, 12 months.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 37
Tabel 1.
Fig. 12. Post-treatment facial photographs.
ConclusionsAnterior crossbite malocclusion patients are easy
to detect. In skeletal patterns, late mixed dentition or early permanent dentitions, comprehensive treatment has shown to be successful. Early diagnosis facilitates
optimum treatment and all but the most severe cases can be offered treatment in the mixed dentition. Anterior crossbite associated with dental factors are generally more cooperative to orthodontic treatments.
1. Proffit WR, Fields HW Jr. Contemporary orthodontics. 3rd ed. St. louis, Mo: Mosby; 2000:185-191.
2. McNamara JA Jr. An orthopedic approach to the treatment of Class III malocclusion in young patients. J Clin orthod 1987;21:598–608.
3. lin JX, Huang JF, Zeng Xl. A cephalometric evaluation of hard and soft tissue changes during Class III traction. Eur J orthod 1985;7:201–204.
4. Isabella T, Tiziano B, lorenzo F. Mandibular skeletal changes induced by early functional treatment of Class III malocclu-sion: a superimposition study. Am J orthod Dentofacial or-thop 1995;108:525–532.
5. Rabie ABM, Yan G. Diagnostic criteria for pseudo-Class III mal-occlusion. Am J orthod Dentofacial orthop 2000;117:1-9.
6. Benham NR: Treatment of simple anterior crossbite using a fixed appliance technique. J Dent Child 42:487-88. 1975.
7. Valentine F, Howitt JW: Implications of early anterior cross-bite correction. J Dent Child 37:420-27, 1970.
8. lee BD: Correction of crossbite. Dent Clin North Am 22:647- 68, 1978.
REFERENCES

Revista Stomatologjike Shqiptare38
AbstraktRehabilitimi i një fronti duke ruajtur principet bazë për ruajtjen e strukturës së dhëmbëve si dhe përshtatjen e funksionit dhe estetikës është një nga hapat më human dhe që korespondon me etikën mjekësore. Stomatologjia estetike në veçanti ka arritur kulminacionin ku në mënyrën më invazive dhe më imituese natyrore të përshtas rastet,gjë që rezulton me pacient të lumtur dhe të kënaqur si dhe rikthim të vetbesimit dhe buzëqeshjes. Aplikimi i kësaj metode mbështetet në teknologjinë bashkëkohore, avansimi ekiporë si dhe zbulimin e bondeve speciale që mënjanojnë mbështetjen mekanike me atë kimike dhe sigurojnë stabilitet.
Fjalët kyçe:
laminatet e
keramikes,
metoda jo
invasive,
gingivoplastika,
bondimi.
mefail Sulejmani¹, Florina Sulejmani¹, Bashkim Saiti²
laminatet keramike jo invazive si një alternativë për ruajtjen e strukturës së dhëmbit si dhe zgjatimi vertikal i dhëmbëve me anë të gingivoplastikës për arritjen e estetikës
¹OPSH”M Dental Group’’ ²OPSH “Bashkim&Co”
Hyrjelaminatet jo invazive paraqesin një alternativë ku me anë të
së cilave krahas kursimit të strukturave të dhëmbit dhe arritjen e funksionit, vjen deri te estetika e planifikuar. (2, 9)
Duke u bazuar në etikën mjekësorë fillimisht po edhe duke bërë prevenimin me lënien e dhëmbit në formën e tij natyrale dhe intakte zvoglohen mundësitë e përhapjes së florës bakteriale, sepse dekortikimi i shtresës së zmaltit rrit mundësitë për përhapje të infeksionit në brendi të dhëmbëve.
Duke qënë se goja paraqet një pjesë të lëvizshme të kokës , këtu ndërlidhen shumë elemente si pamja e dhëmbëve si njëra nga elementet që së bashku me gingivat dhe buzët ndërtojnë një shprehje estetike që ndikon te karakteri dhe bukuria drejtpërsëdrejti. (10, 11)
Materiali dhe metodaPaciente, 30 vjeçare erdhi për konsultim për të
korigjuar dhëmbët e sipërm frontal nga shkaqe estetike. Pacientja raportoi në lidhje me shqetësimet e saj dhe përveç raportimit të këtyre problemeve specifike,
pacienti kërkoi një përmirësim të përgjithshëm të buzëqeshjes së saj.
Një shqetësim kryesor i pacientit ishte se të gjitha trajtimet duhet të bëhen pa preparuar asnjë nga dhëmbët e saj. Pas një observimi klinik intraoral u konstatua se te pacientja ekziston kafshimi thellë shkaku si dhe distema te dhëmbët frontal me gjërësi 1mm deri 1, 5mm. Për të analizuar rastin në detaje tek pacientja morëm një masë për studio model. Pas analizës së detajuar së dhëmbëve dhe kafshimit vendosëm që ka kushte për rregullimin e estetikës pa mos dekortikuar dhëmbët, vetëm se korigjimi i gjatësisë së dhëmbëve shkaku i kafshimit të thellë të bëhet në drejtim vertikal duke bërë ndërhyrje invasive në gingivën margjinale të dhëmbëve frontal dhe duke e shkurtuar për 1mm prej dhëmbit 14 deri te dhëmbi 24. Nënvizuam me anë të një lapsi me ngjyrë duke caktuar linjën e kuqe kundrejt të bardhës dhe duke krijuar një simetri të nivelit gingivar në të dyanët e frontit. (12)
Fig. 2Fig. 1

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 39
Ndërhyrja kirurgjikale u bë me anë të një instrumenti gjysëm hënë adekuat për prerje të gingivave duke fituar harkun e gingivës në mënyrë proporcionale dhe të drejtë përreth dhëmbit dhe duke ruajtur estetikën e gingivës.
Mbas një përpunimi të mirefilltë dhe mbas nje polirimi me anë të gomave , disqeve dhe brushave pacientes i është rekomanduar për një observim mbas dy javë.
RezultatiNë fotografinë mund të vëreni raportin e gingivave
në korelacion me laminatet e vendosura. Një estetikë maksimale i cili ndryshim i formës së dhëmbëve është bërë mbas formës së kontureve të fytyrës gjë që rezultoi me kënaqësi nga ana e pacientes dhe rikthim të vetbesimit.
Fig. 8Rasti mbas 6 muaj.
Fig. 9KonkuzioniMetoda jo invasive me laminate keramike konsiderohet
si një zgjidhje koservative për rastet që janë indikacion, si mbyllja e diastemave, përmirësimin e formës, ngjyrës ose pozicionit të tyre. Mbulimi i dhëmbëve në këtë mënyrë krahas ruajtjes së strukturës ndikon drejtpërsëdrejti edhe në personalitetin dhe karakterin e njeriut, ku rrit vetëbesimin si dhe shfaqë interes për përkujdesje më të madhe ndaj shëndetit oral.
Fig. 3
Fig. 4
Fig. 5
Pacientit iu rekomandua pushim prej 2 javë dhe shpërlarje të gojës me chlorhexidine dhe ruajtje të higjienës.
Mbas dy javë pacientit i aplikuam për marje të masës Nr. 1 dhe morëm masë me anë të materialeve elastomere me dy fazë dhe dy komponent. Mënyra e përgatitjes së bazës së laminateve u bë me anë të skanerit 3D dhe realizimi me CAD-CAM- në mënyrë shumë preçise dhe me trashësi 0. 2mm kurse pjesa e fasetimit në mënyrën konvencionale. (4, 5)
Gjatë proçesit të bondimit kemi bërë fillimisht izolim të frontit me anë të ruberdamit dhe kemi përdorur përgatitje të sipërfaqeve me thartirë ortofosforike 37% si dhe acid hydrofluorik 9% për keramikën si dhe silant për kondicionim të sipërfaqeve të dhëmbëve dhe të laminateve të porcelanit. (1, 3, 7)Pas përgatitjes së sipërfaqeve kemi përdorur nano bond të gjeneratës së VII Peak Bond për lyerjen e sipërfaqeve në shtresa fare të holla si dhe nano kompozit të lëngshëm Genial Flow. Mbas aplikimit të kompozitit të lëngshëm laminatet janë ngjitur dhe janë polimerizuar me llampë 3200 mW/cm2 të gjitha nga 3 sek. (6, 7)
Fig. 6
Fig. 7

Revista Stomatologjike Shqiptare40
1. Magne P, Belser uC. Bonded Porcelain Restorations in the Anterior Dentition-a Biomimetic Approach. Chicago: Quin-tessence Publishing Co; 2002.
2. Radz GM. Minimum thickness anterior porcelain res-torations. Dent Clin North Am. 2011;55(2):353–370. ix. [PubMed]
3. Wells DJ. “No-prep” veneers. Inside Dent. 2010;6(8):56–60.
4. Ferrari M, Patroni S, Balleri P. Measurement of enamel thickness in relation to reduction for etched laminate ve-neers. Int J Periodontics Restorative Dent. 1992;12(5):407–413. [PubMed]
5. Parmeijer CH. Porcelain laminate veneers. J Calif Dent As-soc. 1991;19(4):59–62. [PubMed]
6. Pini NP, Aguiar FH, lima DA, lovadino JR, Terada RS, Pascotto RC. Advances in dental veneers: materials, applications, and techniques. Clin Cosmet Investig Dent. 2012;4:9–16. [PMC free article][PubMed]
7. Strassler HE, Weiner S. Seven to ten-year clinical evaluation of porcelain laminate veneers. J Dent Res. 1995;74:176
8. D’Arcangelo C, De Angelis F, Vadini M, D’Amario M. Clinical evaluation on porcelain laminate veneers bonded with light-cured composite: results up to 7 years. Clin oral In-vestig. 2012;16(4):1071–1079. [PubMed]
9. Belser u. C. , Magne P. , Magne M. Ceramic laminate veneers: continuous evolution of indications. Journal of Esthetic Dentistry. 1997;9(4):197–207. doi: 10. 1111/j. 1708-8240. 1997. tb00941. x. [PubMed][Cross Ref ]
10. Rotoli B. T. , lima D. A. N. l. , Pini N. P. , Aguiar F. H. B. , Pereira G. D. S. , Paulillo l. A. M. S. Porcelain veneers as an alternative for esthetic treatment: clinical report. opera-tive Dentistry. 2013;38(5):459–466. doi: 10. 2341/12-382-t. [PubMed] [Cross Ref ]
11. Pincus C. R. Building mouth personality. Journal of the Cali-fornia Dental Association. 1938;14:125–129.
12. Kan J. Y. K. , Morimoto T. , Rungcharassaeng K. , Roe P. , Smith D. H. Gingival biotype assessment in the esthetic zone: vi-sual versus direct measurement. The International journal of periodontics & restorative dentistry. 2010;30(3):237–243. [PubMed]
REFERENCA

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 41
AbstractFrontal rehabilitation by preserving basic principals in saving tooth structure as well as adapting function and esthetics is one of the most humanistic approach that corresponds to medical ethics. Esthetic dentistry in particular achieved its culprit, where invasively and via emulation cases are adapted, resulting in happy and satisfied patients, meanwhile reestablishing self-confidence and smile. Application of above techniques is based in contemporary technology, in team advancement and invention of special adhesives, substituting mechanical retention with chemical one, thereof establishing stability.
key woRDS:
Ceramic veneers,
non-invasive
method,
gingivoplasty,
bonding.
mefail Sulejmani¹, Florina Sulejmani¹, Bashkim Saiti²
Non-invasive ceramic veneers as an alternative to preserve tooth structure and crown lengthening via gingivoplasty in achieving aesthetics
¹PHF “M Dental Group’’²PHF “Bashkim & Co”
IntroductionNoninvasive veneers are representing an alternative
approach, where apart from saving tooth structure and establishing function, desired esthetic is achieved, too.(2,9)
Based on medical ethics, first, yet also by preserving tooth intact and natural structure, spread of oral bacteria is reduced, since enamel removal increases infection potential among teeth.
Since mouth represents a mobile part of the head, many elements are related, like dental appearance, who, along with gums and lips, construct an esthetical expression, directly affecting human character and beauty.(10,11)
Materials and Methods30 years old patient showed at our practice asking
frontal dental correction for esthetical purposes. Patient explained her complaints and asked for overall improvement of esthetics, for a better smile.
Her only request was a noninvasive, grinding no teeth structure, while achieving desired results. upon intraoral evaluation, deep bite was found, along with 1-1.5mm in width frontal teeth diastema. For a detailed approach, a study cast was obtained. upon detailed evaluation, a noninvasive dental approach was set, yet for crown lengthening an invasive approach one of gingivalplasty was set, respectively shortening marginal gingiva in 1mm from teeth 14 to 24. Bordering was marked, separating red line from the white one, thus producing symmetric gingival level bilaterally.(12)
Fig. 2Fig. 1

Albanian Stomatological Journal42
Surgery was performed via semilunar scalpel, adequate to obtain gingival arch like shape in direct and proportional way, thus saving its esthetics.
upon fine grinding and polishing with rubbers, discs and brushes, the patient was scheduled for a two week follow up.
ResultsImages show gingiva veneer relations. Maximal
esthetics attained in accordance to facial contours, resulting in patient satisfaction and self-esteem.
Fig. 86 months recall.
Fig. 9ConclusionNon invasive approach with ceramic veneers is
conisdered as an conservative solution in certain inidtications, as diastema closure, improving teeth shape, color and position, thereof beside structure preservation, directly influencing personality and human character, simultaneosuly increasing self confidence and oral health maintainance arised awareness.
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Fig. 7
Patient was scheduled for 2 week follow up and advised to flush with chlorehexidine solution and brush teeth in regular basis.
After two weeks, impression thread was applied, whereof two phasic, two component dental impression was taken. Dental cast was 3D scanned, veneers produced via CAD CAM, with high accuracy of 0.2mm, while porcelain layering was performed in a conventional manner.(4,5) In adhesive phase during the bonding process we first made the isolation of the front by ruberdamit and we have37% orthophosphoric and 9% sodiumfluoride acids where utilized, as well as conditioning sealant for teeth and veneer surfaces, and finally VIIth generation very thin bonding was applied.(1,3,7) Veneers were applied using genial flow composite, polymerized via 3200mW/cm2 curing light for 3 sec. (6,8)

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 43
1. Magne P, Belser uC. Bonded Porcelain Restorations in the Anterior Dentition-a Biomimetic Approach.Chicago: Quin-tessence Publishing Co; 2002.
2. Radz GM. Minimum thickness anterior porcelain restora-tions. Dent Clin North Am. 2011;55(2):353–370. ix. [PubMed]
3. Wells DJ. “No-prep” veneers. Inside Dent. 2010;6(8):56–60.
4. Ferrari M, Patroni S, Balleri P. Measurement of enamel thickness in relation to reduction for etched laminate ve-neers. Int J Periodontics Restorative Dent. 1992;12(5):407–413. [PubMed]
5. Parmeijer CH. Porcelain laminate veneers. J Calif Dent As-soc. 1991;19(4):59–62. [PubMed]
6. Pini NP, Aguiar FH, lima DA, lovadino JR, Terada RS, Pascotto RC. Advances in dental veneers: materials, applications, and techniques. Clin Cosmet Investig Dent. 2012;4:9–16. [PMC free article][PubMed]
7. Strassler HE, Weiner S. Seven to ten-year clinical evaluation of porcelain laminate veneers. J Dent Res. 1995;74:176
8. D’Arcangelo C, De Angelis F, Vadini M, D’Amario M. Clini-cal evaluation on porcelain laminate veneers bonded with light-cured composite: results up to 7 years. Clin oral Inves-tig. 2012;16(4):1071–1079. [PubMed]
9. Belser u. C., Magne P., Magne M. Ceramic laminate ve-neers: continuous evolution of indications. Journal of Esthetic Dentistry. 1997;9(4):197–207. doi: 10.1111/j.1708-8240.1997.tb00941.x. [PubMed][Cross Ref ]
10. Rotoli B. T., lima D. A. N. l., Pini N. P., Aguiar F. H. B., Pereira G. D. S., Paulillo l. A. M. S. Porcelain veneers as an alter-native for esthetic treatment: clinical report. operative Dentistry. 2013;38(5):459–466. doi: 10.2341/12-382-t. [PubMed] [Cross Ref ]
11. Pincus C. R. Building mouth personality. Journal of the Cali-fornia Dental Association. 1938;14:125–129.
12. Kan J. Y. K., Morimoto T., Rungcharassaeng K., Roe P., Smith D. H. Gingival biotype assessment in the esthetic zone: vi-sual versus direct measurement. The International journal of periodontics & restorative dentistry. 2010;30(3):237–243. [PubMed]
REFERENCES

Albanian Stomatological Journal44
AbstractAim: Because the height and the width of the alveolar ridge are major factors for the future implanting, the RESoRBA® DENTAl material is used with aim to save the alveola for further implanting of the same.
Material and methods: We show a few cases in which RESoRBA® DENTAl material was used, after extraction of the maxillary incisives. After the successful osteointegration of the material in the jaw bone, dental implant was placed and after four months of the procedure, a dental prosthetic construction was made. osteointegration of the material was determined according to objective clinical examination of the patient, the subjective symptoms and RTG. In the meantime while waiting, for the esthetic moment the empty space is filed with temporary prosthetic construction.
Results: The alloplastic material has remarkable attributes of defending the alveolar ridge from atrophy, because of that the healing of the alveola went very good. Post extraction complications in our cases were missing and not evidenced. The height and the width of the ridge were on satisfying level and we had successful implanting.
Conclusion: With RESoRBA® DENTAl material, bone resorption is prevented and we have many benefits:
• The extraction wound heals faster
• The material provides stability of the blood coagulum (no bleeding)
• long-range success of the dental construction.
key woRDS:
RESoRBA®
DENTAl,
endooseal
implants,
alveolar ridge,
osteointegration,
implanting,
extraction wound
lj. Simjanovska, a. trajkovski, S.Simjanovski, F.azizi, S.Simjanovska
preservation of the alveola for implanting dental implants with ReSoRBa® DeNtal
Faculty of Dentistry St. Ciryl and Metodij Skopje, PHF D-r Aleksandar Trajkovski, , PHF Denta, PHF Picasso.
Introduction In this study we will show, preservation of the alveola
as very important procedure for future implanting. Also there will be a few cases with successful integration of bone material and implants. The loss of the teeth can cause defects on the ridges, which present a base of any kind of prosthetic construction. Sanitation of the bone defect in and out of the alveola after the extraction lasts 3-6 months. In that period of time often, serious problems appear like changes in the height and width of the ridges. To provide and get good alveolar ridge, especially if the vestibular side is damaged, augmentation of the lost bone needs to be done to prevent the collapse of the vestibular side. However an adequate width of the ridge must be provided because of the implant which must have great stability (1,4). With that the implant can’t be loosened and the force used for tightening the implant will be much stronger. The material for augmentation is chosen by the doctor. The usage of bone material with or without membrane depends form the defects and the foramens in the jaws.
Many times for preservation of the place we have to put sutura and membrane must be placed.
With that procedure except width, we also get height. The height presents one of the biggest problems.
The width and the height of the alveolar ridge are major factors for further implantation. We used RESoRBA® DENTAl bone material.
Material and methods: In this case we will show cases (10) with applied alloplastic material RESoRBA® DENTAl (PARASoRB® + Cone) in the alveola (picture 1). After the successful osteointegration of the material in the jaw, dental implants were implanted. After 4 months adequate prosthetic construction was made.
Slika br 1. RESORBA ® DENTAL / (PARASORB® + Cone)http://www.admedsol.com/our-brands/resorba /

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 45
RESORBA® DENTAL as a material for preservation of the alveola we applicate immediate after the extraction. In every case there was a risk of a defect of dehiscence of the side of the ridge. The extracted teeth were usually with big destructions of the crown and placed intact. Also the preservation was made at the molar region for strengthening the alveola and the sinus wall. (5).
In the front existed a chance for a fracture of the lamina which was very thin.
In every quadrant of the both jaws there were indications for augmentation.
In many of the cases, after the application of the material, we applicate membrane -RESoDoNT® for protection. The removal of the suture was after 10 days and the patients also were controlled. Before and after every intervention RTG was made. The osteointegration of the material was determinated according to the objective examination of the patient, the subjective symptoms and the RTG.
In the meantime (along osteointegration) because of the esthetic moment, a permanent dental construction was made. The dental construction must not make any pressure.
Results and discussion: While the extraction of the teeth, shortly after, the aproximal alveolar ridge towards the next teeth is rapidly sliding and the other teeth are leaning into the hollow places. With that the height of the alveola is lost (picture 2).
Picture 2 A Extracted tooth B Scheme of lost of the height of the alveola
one of the basic criteria for success of the implanting is the volume of the bone supporting the osteointegration. In contraire the surgeon would do an augmentation or grafting of the bone. The procedure of the transplantation is transplantation or adding of nature or synthetic bone in the jaw. After that the material joins the existing bone
A
B
(usually 6 to 9 months, rarely 12 months). The materials used for transplantation can be divided
into several categories. In 2006 laurencin gave the following classification.
According of the shape the materials divide to: granules, bounded tissue, membranes and slabs.
According to the nature:• Autogenous bones, taken from the patients, from
their chin, skull, thy …• Allograft or human bones• Animal bones called xenografts (Capacity inferior
compared with the autografts and allografts) • Synthetic bones classified into three groups:
demineralized bone matrix, ceramics, composite (mixed) materials.
RESORBA ® DENTAL like alloplastic material has collagen fibrils and owns great characteristics for protection of the coagulum. The collagen matrix increases the coagulum and prevents the soft tissue to join with the extraction wound, defends the ridge from atrophy and is good for regeneration. The patient’s organism accepted the material without any complications, pain, swallowing, edema or other. The height and the width of the ridge were satisfying and the implantation was successful (picture 3).
Picture 3 a) Healthy alveolar ridge
b) RTGc) Abatment
A
B
C

Revista Stomatologjike Shqiptare46
This kind of augmentation acts osteoconductive on the bone and has physical effect for forming a new bone.
Picture 4 RTG of ready supra structure with done preservation a)Molar region , b) Frontal region
Picture 5RTG of dental implants after augmentation with RESORBA ®
DENTAL
A B
Picture 6 Healty alveolar ridge http://www.resorba.com/
RESoRBA ® DENTAl as a dental material for bone grafting is a collagen which possesses many great characteristics (9,11).
Reduction of the atrophy of the alveolar ridgeStabilizes the alveola and supports the thin vestibular
laminaProvides stability of the alveolar procesus Esthetic and functional results If not prevented the after later interventions are
expensive and took long period, also are painfull.Working with this material also provides:Comfort of the doctor and the patients Simple usageEliminates the surgical later manipulationAcceptable price Successful regenerationFor a short time we have a stable bone area and long
term success
ConcusionWith the usage of the RESoRBA ® DENTAl we
successfully prevent the bone resorption of the ridge and we have many benefits like stability of the coagulum. The coagulum stripe is more effective than the gelatin sponges or the cellulose. With all that we have great future and successful dental prosthetic construction.
1. American Society for Bone and Mineral Research, Bone Cur-riculum
2. Bauer Tomas W MD, PhD and Muschler, George F. MD An overvieW of the Basic Science.
Clinical ortopedics & Related Research, February 2000.3. British Dental Journal, Vol186, No. 5,: Tooth surface loss; Part
3: oclusion and splint therapy. 4. Dominic o’Sullivan BDS, FDS, RCS,lars Sennerby DDS, PhD, Measurements Comparing the Initial Stability of Five De-
signs of Dental Implants: A Human Cadaver Study. First published: April 2000Full publication history
5. luarencin C, Khan Y, El Amin Bone graft substitutes. Expert Rev Med Devices. Jan 2006
6. Pär-olov Östman, Mats Hellman, lars Sennerby, Direct Im-plant loading in the Edentulous Maxilla using a Bone Den-sity–Adapted Surgical Protocol and Primary Implant Stabil-ity Criteria for Inclusion June 2005
7. Richard l. Burguete, Richard B. Johns, Toby King, Eann A. Patterson.
Tighening characteristics for screved joints in osseointe-grated dental implants. (J Prosthet Dent 1994; 71: 592-9).
8. Sam Khoury. Human Bone& Graft Material in Dentistry. January 20099. http://www.resorba.com/ 10. http://www.admedsol.com/our-brands/resorba /11. http://www.admedsol.com/our-divisions/branded-distrib-
uted/resorba/
REFERENCES

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 47
AbstraktSëmundjet e organizmit të njeriut në përgjithsi dhe ata sistemike në veçanti, me rritjen e shpejtë dhe agresivitetin e tyre, si kurrë më parë paraqesin probleme serioze shëndetësore për popullatën, si dhe për institucionet përgjegjëse relevanteQëllimi i studimit tonë është që:
- Të përcaktohet përqindja e pacientëve me sëmundje sistemore të trajtuar në pikëpamje protetike- Të përcaktohet frekuenca e sëmundjeve të rrezikut te pacientët e pajisur me punime protetike - Të përcaktohet përqindja e pacientëve me sëmundje rreziku që marrin terapi dhe atyre që nuk marrin terapi dhe të vërtetohet korelacioni mes tyre
Materiali dhe MetodatPër këtë studim janë ndjekur në vazhdimësi të dhënat e përftuara nga pacientë të ekzaminuar në klinikën dentare specialistike “Protetika Ag” në Tetovë në periudhën kohore 2013-2015.Rezultatet Rezultatet e fituara tregojnë se: Sëmundjet kardiovaskularë marrin pjesë me 46.15%, Sëmundjet reumatizmale me 21.64%, Diabetes mellitus me 9.13%, Sëmundjet e SNQ-së me 7.72%, Sëmundjet neuro psiqike me 4.62%.Përfundim Njohuritë mbi marrjen e terapisë nga ana e pacientëve me sëmundje të rrezikut janë me rëndësi për shkak të interaksionit të mundshëm mes intervenimit stomatologjik, anestezionit dhe barërave të cilët i përshkruan stomatologu. Duke i patur të dhënat për sëmundjet e rrezikut, është e mundur që të planifikohen ndërhyrjet në sistemin stomatognatik. Vlera e t-testit dhe e koeficientit të probabilitetit, tregojnë për lidhje statistikisht të rëndësishme mes marrjes së terapisë dhe mosmarrjes terapi sipas sëmundjeve të rrezikut te pacientët e ekzaminuar. Në rezutatet e këtij studimi vërehet se ekziston një lidhje e dobët në midis përqindjes së pacientëve me sëmundje sistemike të cilët trajtohen me terapi dhe pacientëve me sëmundje sistemike të cilët nuk trajtohen me terapi.
SheRiF ShaqiRi 1,2 kaltRiNa BeqiRi 1
Frekuenca e sëmundjeve të rrezikut te pacientët e trajtuar me punime protetike
1Klinika specialistike për protetikë “Protetika AG” Tetovë2Departamenti i Stomatologjisë, Fakulteti i Shkencave Mjekësore, Universiteti Shtetëror i Tetovës
HyrjeSëmundjet e organizmit të njeriut në përgjithsi
dhe ata sistemike në veçanti, me rritjen e shpejtë dhe agresivitetin e tyre, si kurrë më parë paraqesin problem serioze shëndetësore për popullatën, si dhe për institucionet përgjegjegjëse relevante(1).
Këto sëmundje janë definuar si sëmundje kronike të qëndrueshme, me kohëzgjatje prej më shumë se 3 muaj që ndikojnë në jetën e individit dhe kërkojnë trajtim të vazhdueshëm mjekësor(2). Këto sëmundje luajnë rol kryesor në përcaktimin e opsionit të mundshëm të trajtimit në stomatologji. Te këto raste proçedurat protetike duhet të gjykohen me kujdes dhe të planifikohen sipas statusit sistemik të pacientit(3)
Ekzistojnë sëmundje të ndryshme shqetësuese në lidhje me Protetikën. Këto së bashku me menaxhimin e tyre janë përshkruar si:- sëmundje kardiovaskulare të cilat e përbëjnë
kategorinë më të përhapur të sëmundjeve sistemike në pothuajse të gjitha vende e botës, prevalenca e
të cilave rritet me moshën, ku bëjnë pjesë: angina pectoris, infarctus myicardi, endocarditis bacterialis subacuta, dëmtimet kongestive të zemrës, hipertensioni
- sëmundjet endokrine si diabetes mellitus, që është sindromë klinike e karakterizuar nga hiperglikemia për shkak të mungesës absolute ose relative të insulinës(2).
- sëmundjet e gjëndrës tiroide- sëmundjet e gjëndrave mbiveshkore- sëmundjet e traktit respirator- sëmundjet e mëlçisë si: ceroza- sëmundjet hematologjike si: anemia dhe leukopenia- sëmundjet e eshtrave si: osteoporoza, displazia
fibrotike dhe osteoitis deformans- sëmundjet neuro-psiqike si: sëmundja e Parkinsonit
dhe sindroma e gojës djegëse- sëmundjet autoimune si: artriti reumatizmal
ku kyçet tëmtho-nofullore janë më shpesh të prekura(2,3).
Fjalët kyçe:
Frekuenca,
sëmundjet e
rrezikut, pajisjet
protetike,
pacientët e
trajtuar

Revista Stomatologjike Shqiptare48
Sa i përket trajtimit protetik te pacientët me sëmundje sistemike, në varshmëri nga lloji dhe shkalla e lëngimit nga këto sëmundje, stomatologu protezist gjatë trajtimit protetik duhet t’i monitorojë shenjat vitale dhe të mbajë llogari: - për përdorimin e kufizuar të vazokonstriktorëve
(angina pectoris) dhe afatin kohorë nga paraqitja e sëmundjes deri te trajtimi protetik, si dhe procedurat e gjata të trajtimit duhet ndarë dhe rregulluar në procedura të shkurtra (infractus myocardi). Për këta pacientë me prirje për angina pectoris ose për infarctus myocardi, mjeku stomatolog ofrues i trajtimit protetik duhet të jetë i pregatitur për dallimin dhe menaxhimin e rreziqeve dhe në këtë mënyrë t’i parandalojë këta raste(3,4, 5);
- që të ketë njohuri se në cilat situata është kundër indikacion vendosja e punimeve protetike mobile dhe marrja e kopjes orale (endocarditis bacterialis subacuta);
- që të ketë kujdesë dhe të jëtë i gatshëm për prevenimin e ekzacerbimit akut të sëmundjeve kronike (dëmtimet kongestive të zemrës);
- që të zbatojë protokoll për uljen e stresit (hipertensioni).Falë kësaj llogari mbajtjeje, stomatologu protezist gjatë
menaxhimit të pacientit me sëmundje kardiovaskulare gjatë terapisë protetike është i siguruar se ndryshimet hemodinamike të krijuara gjatë trajtimeve protetike nuk e tejkalojnë rezervën kardiovaskulare të pacientit(6,7);- që të përdorë teknikë për kopje e cila do të krijojë
kompatibilitet fiziologjik maksimal ndërmjet bazës së protezës dhe strukturave mbështetëse të nofullës, të kryejë korigjime okluzale të kujdesshme me qëllim të eleminimit të gjitha interferencave, t’i jap pacientit instruksione të detajuara mbi shprehitë e të ushqyerit dhe higjienës orale, të bëjë vlerësimin e shpeshtë mbi gjendjen e protezave dhe pacientëve të cilët kanë prirje për infeksione dhe komplikime vaskulare, t’ ju përshkruajë profilaksë me antibiotikë para trajtimit protetik me qëllim të parandalimit të infeksioneve të mëvonshme (diabetes mellitus), ndërsa pacientët e të gjitha moshave të trajtuar në pikëpamje protetike duhet të kuptojnë se ky çrregullim metabolik i vendosur mund të ketë një ndikim të konsiderueshëm në rezultatin përfundimtar të trajtimit protetik(3,4,8,9,10,11,12);
- që pacientët me frymëmarrje të vështirësuar gjatë angazhimit si dhe ata të cilët përdorin terapi bronhodilatatore duhet t’i nënshtrohen kontrollit mjekësor, ndërsa përdorimi i epinefrinës dhe vazokonstriktorëve në anestezion ose në perin për retraksion të gingivës nuk sugjerohet (sëmundjet e mushkërive)(13);
- se stomatologu protezist është në pozitë strategjike për evidentimin e hershëm të osteoporozës dhe t’i edukojë pacientët geriatrikë për ushqyerje të mirë. Disenjimi i protezave të plota për këtë kategori të pacientëve kërkon një konsideratë të veçantë me qëllim të ruajtjes së konstruksionit themelorë të strukturave indore sa më shumë të jetë e mundur (osteoporoza)(2);
- që te rastet si apopleksia, sinkopa dhe insultet duhet marrë anamnezë të saktë dhe listën e barërave, si dhe të konsultohet mjeku i cili e trajton pacientin (sëmundjet neuro-psiqike)(3);
- që te rastet e sëmundjeve reumatizmale të cilat paraqesin çrregullime muskuloskalatale të karakterizuara me inflamim të kyçeve, trajtimi duhet të fokusohet kryesisht në medikamentet antireumatike, pasiqë proçedurat protetike nuk mund ta shërojnë sëmundjen dhe për këtë arsye ata janë sekundare, ndërsa kur sëmundja ndodhet mes fazës akute dhe asaj kronike, atëherë trajtimi ireverzibil me proteza fikse nuk duhet të realizohet derisa sëmundja nuk është e shëruar (sëmundjet reumatizmale)(2,8). Problem i hasur në rehabilitimin protetik të pacientëve me artrit reumatoid të kyçit tëmtho-nofullorë është ndryshimi i okluzionit dhe relacioni nofullor(8).
Menaxhimi me sukses i pacientit fillon pikërisht nga anamneza mjekësore deri te plani i trajtimit, ku shumë më tepër konsideratë duhet patur për statusin sistemik të individit. Stomatologu protezist i cili në anamnezë e neglizhon statusin sistemik, ai do të futet në komplikime serioze në dëm të jetës së pacientit(3)
QëllimiQëllimi i studimit tonë është që përmes të dhënave të
përfituara nga ekzaminimet klinike të:- Përcaktohet përqindja e pacientëve me sëmundje
sistemike të trajtuar në pikëpamje protetike,- Përcaktohet frekuenca e sëmundjeve të rrezikut te
pacientët e pajisur me punime protetike, - Përcaktohet përqindja e pacientëve me sëmundje të
rrezikut që marrin dhe atyre që nuk marrin terapi dhe të vërtetohet korelacioni mes tyre.
Materiali dhe metodatPër këtë studim janë ndjekur në vazhdimsi të
dhënat e përfituara nga pacientë të ekzaminuar në klinikën dentare specialistike “Protetika Ag” në Tetovë në periudhën kohore 2013-2015, të cilët kanë ardhur në klinikën tonë duke shprehur ankesat e tyre që kanë të bëjnë me sistemin stomatognatik
Nga ky grupim 943(52.83%) e tyre ishin pacientë të gjinisë mashkullore ndërsa 842(47.17%) e tyre ishin paciente të gjinisë femërore. Mosha e të ekzaminuarve ishte prej 13 gjer 82 vjeç, me moshë mesatare 48.2 vjeç.
Përmes anamnezës u siguruan të dhënat mbi sëmundjet si:
- Sëmundjet kardiovaskulare,- Sëmundjet neuro-psiqike,- Diabetes mellitus,- Sëmundjet reumatizmale,- Sëmundjet e Sistemit Nervor Qendror (SNQ) dhe - Patologjive të tjera. Të dhënat e fituara janë futur në kartela të pacientit
duke e përdorur formën e modifikuar të vlerësimit të shëndetit oral sipas oBSH-së. (World Health organization), të përshtatur dhe modifikuar me natyrën e studimit tonë.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 49
Të dhënat e fituara, pas përpunimit statistikor i kemi paraqitur me anë të grafikëve dhe tabelave, ndërsa ata të rëndësisë së veçantë janë treguar me anë të T-testit, koefiçientit të probabilitetit (p) dhe koefiçientit të korelacionit (Rxy).
RezultatetPërqindjen e pacientëve tanë të ekzaminuar me
sëmundje të rrezikut të paraqitur në grafikët dhe në tabelë e kemi fituar nga historia mjekësore e secilit pacient veç e veç.
Në grafikun 1 janë paraqitur rezultatet për pacientët e trajtuar të “shëndoshë” dhe ata që lëgojnë nga sëmundje të ndryshme. Nga ky grafik shihet se nga numri i përgjithshëm i pacientëve te ekzaminuar, 975(54.62%) ishin pacientë që vuanin sëpaku nga një sëmundjet dhe 810(45.38%) ishin pacientë që nuk lëngonin nga asnjë sëmundje.
Fig. 1. Pacientët që lëngojnë dhe ata të cilët nuk lëngojnë nga
sëmundje të ndryshme
Rezultatet për pacientët me sëmundje të rrezikut dhe ata të cilët vuanin nga sëmundje tjera janë paraqitur në grafikun 2. Nga ky grafik shihet se nga numri i përgjithshëm (975) i pacientëve që vuanin nga sëmundje të ndryshme, 841(86.26%) ishin pacientë që vuanin sëpaku nga një sëmundje e rrezikut dhe 134(13.74%) ishin pacientë që lëngonin nga sëmundje tjera.
Fig. 2. Pacientët që lëngojnë nga sëmundjet sistemike dhe ata të cilët lëngojnë nga sëmundje të tjera
Në grafikun 3 i kemi paraqitur rezultatet e pacientëve me sëmundje të rrezikut. Nga këto rezultate shihet qartë se pacientët me sëmundje kardiovaskulare janë në numër
më të madh 450 dhe përqindje më të lartë 46.15%, të ndjekur nga pacientët me sëmundje reumatizmale me 21.64% (211), pacientët me diabetes mellitus me 9.13% (89), pacientët me sëmundje të SNQ-së me 7.72% (46) dhe pacientët me sëmundje neuro-psikike me 4.62%(45).
Fig. 3. Pacientët që lëngojnë nga sëmundjet e ndryshme sistemike
Në tabelën 1 janë paraqitur pacientët me sëmundje të rrezikut të trajtuar në klinikën tonë. Nga rezultatet e kësaj tabele shohim se pacientët me sëmundje kardiovaskulare në 341 (75.78%) raste marrin terapi, ndërsa në 109 (24.22%) raste nuk marrin terapi, të ndjekur nga pacientët me sëmundje reumatizmale, nga të cilët 76 (30.02%) marrin terapi ndërsa 135 (63.98%) nuk marrin terapi, pacientë me sëmundje të tjera, nga të cilët 61 (45.52%) marrin terapi dhe 73 (54.48%) nuk marrin terapi, pacientët me diabetes mellitus ku të gjithë (100%) marrin terapi, pacientët me sëmundje të SNQ-së të gjithë (100%) marrin terapi dhe pacientët me sëmundje neuro-psikike, ku gjithashtu të gjithë (100%) marrin terapi.
Diskutimi Shërimi me sukses i atyre sëmundjeve të cilat do të
ndikojnë në prognozën e çdo punimi protetik duhet të jetë vija e frontit gjatë trajtimit të pacientëve nga ana e stomatologut protezist. Rezultatet e sipër përmendura tregojnë se pavarësisht sëmundjeve të ndryshme, nevoja për kurim dhe rehabilitim të sistemit stomatognatik ngel si një sfidë konstante për stomatologët.
Këtë problematikë e kanë studiuar dhe për të kanë debatuar autorë të ndryshëm. Kështu autori Bokhari me bashkp.(14), në studimin e tyre mbi dhëmbët e humbur dhe të pakompensuar te pacientët me sëmundje kardiake në Institutin e Penxhabit, vë në dukje se te popullata e studiuar 86.95% nuk kishin kompensime protetike për dhëmbët e tyre mungues, ndërsa 12.65% e pacientëve me sëmundje kardiake dhe 13.57% e pacientëve të shëndoshë kishin kompensime protetike për dhëmbët e tyre mungues. Po ashtu, Sotosek me bashkp.(15), në studimin e tyre mbi statusin e përgjithshëm shëndetësor të pacientëve stomatologjikë, nga ekzaminimi i 2045 pacientëve kanë arritur në rezultatet se 30.1% e tyre vuanin nga ndonjë sëmundje sistemike, ndërsa 42,2% e të ekzaminuarve merrnin barëra.
Nga sëmundjet sistemike, autori Akar me bashkp.(16),
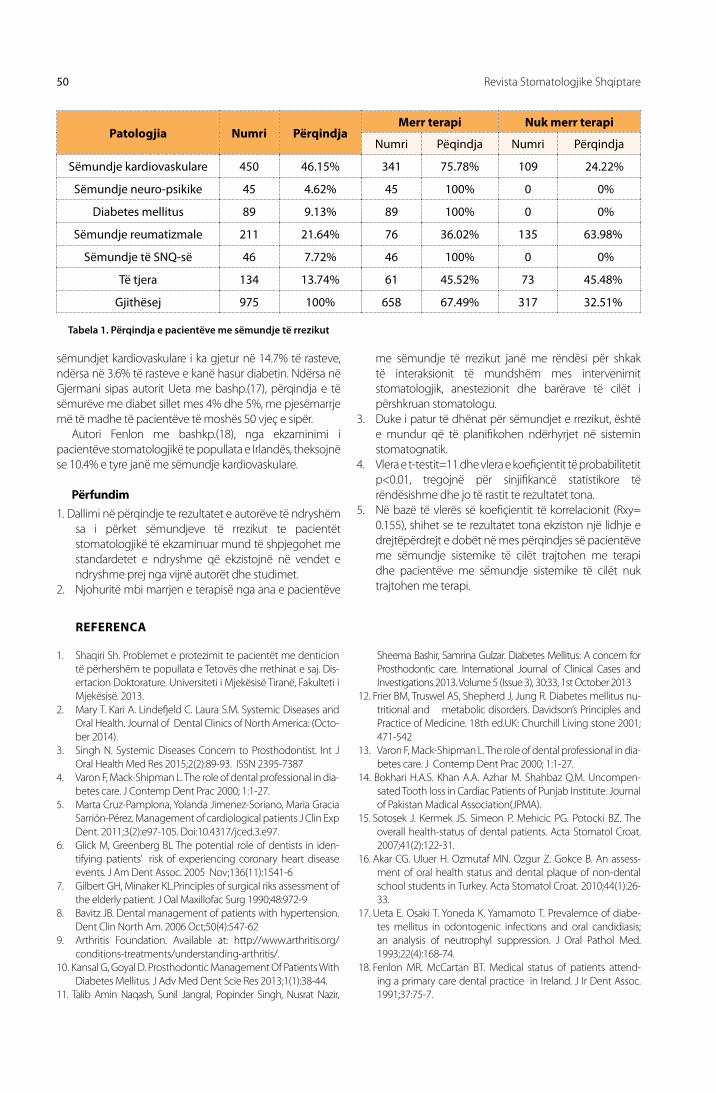
Revista Stomatologjike Shqiptare50
sëmundjet kardiovaskulare i ka gjetur në 14.7% të rasteve, ndërsa në 3.6% të rasteve e kanë hasur diabetin. Ndërsa në Gjermani sipas autorit ueta me bashp.(17), përqindja e të sëmurëve me diabet sillet mes 4% dhe 5%, me pjesëmarrje më të madhe të pacientëve të moshës 50 vjeç e sipër.
Autori Fenlon me bashkp.(18), nga ekzaminimi i pacientëve stomatologjikë te popullata e Irlandës, theksojnë se 10.4% e tyre janë me sëmundje kardiovaskulare.
Përfundim1. Dallimi në përqindje te rezultatet e autorëve të ndryshëm
sa i përket sëmundjeve të rrezikut te pacientët stomatologjikë të ekzaminuar mund të shpjegohet me standardetet e ndryshme që ekzistojnë në vendet e ndryshme prej nga vijnë autorët dhe studimet.
2. Njohuritë mbi marrjen e terapisë nga ana e pacientëve
me sëmundje të rrezikut janë me rëndësi për shkak të interaksionit të mundshëm mes intervenimit stomatologjik, anestezionit dhe barërave të cilët i përshkruan stomatologu.
3. Duke i patur të dhënat për sëmundjet e rrezikut, është e mundur që të planifikohen ndërhyrjet në sistemin stomatognatik.
4. Vlera e t-testit=11 dhe vlera e koefiçientit të probabilitetit p<0.01, tregojnë për sinjifikancë statistikore të rëndësishme dhe jo të rastit te rezultatet tona.
5. Në bazë të vlerës së koefiçientit të korrelacionit (Rxy= 0.155), shihet se te rezultatet tona ekziston një lidhje e drejtëpërdrejt e dobët në mes përqindjes së pacientëve me sëmundje sistemike të cilët trajtohen me terapi dhe pacientëve me sëmundje sistemike të cilët nuk trajtohen me terapi.
1. Shaqiri Sh. Problemet e protezimit te pacientët me denticion të përhershëm te popullata e Tetovës dhe rrethinat e saj. Dis-ertacion Doktorature. universiteti i Mjekësisë Tiranë, Fakulteti i Mjekësisë. 2013.
2. Mary T. Kari A. lindefjeld C. laura S.M. Systemic Diseases and oral Health. Journal of Dental Clinics of North America: (octo-ber 2014).
3. Singh N. Systemic Diseases Concern to Prosthodontist. Int J oral Health Med Res 2015;2(2):89-93. ISSN 2395-7387
4. Varon F, Mack-Shipman l. The role of dental professional in dia-betes care. J Contemp Dent Prac 2000; 1:1-27.
5. Marta Cruz-Pamplona, Yolanda Jimenez-Soriano, Maria Gracia Sarrión-Pérez. Management of cardiological patients J Clin Exp Dent. 2011;3(2):e97-105. Doi:10.4317/jced.3.e97.
6. Glick M, Greenberg Bl The potential role of dentists in iden-tifying patients’ risk of experiencing coronary heart disease events. J Am Dent Assoc. 2005 Nov;136(11):1541-6
7. Gilbert GH, Minaker Kl.Principles of surgical riks assessment of the elderly patient. J oal Maxillofac Surg 1990;48:972-9
8. Bavitz JB. Dental management of patients with hypertension. Dent Clin North Am. 2006 oct;50(4):547-62
9. Arthritis Foundation. Available at: http://www.arthritis.org/conditions-treatments/understanding-arthritis/.
10. Kansal G, Goyal D. Prosthodontic Management of Patients With Diabetes Mellitus. J Adv Med Dent Scie Res 2013;1(1):38-44.
11. Talib Amin Naqash, Sunil Jangral, Popinder Singh, Nusrat Nazir,
Sheema Bashir, Samrina Gulzar. Diabetes Mellitus: A concern for Prosthodontic care. International Journal of Clinical Cases and Investigations 2013. Volume 5 (Issue 3), 30:33, 1st october 2013
12. Frier BM, Truswel AS, Shepherd J, Jung R. Diabetes mellitus nu-tritional and metabolic disorders. Davidson’s Principles and Practice of Medicine. 18th ed.uK: Churchill living stone 2001; 471-542
13. Varon F, Mack-Shipman l. The role of dental professional in dia-betes care. J Contemp Dent Prac 2000; 1:1-27.
14. Bokhari H.A.S. Khan A.A. Azhar M. Shahbaz Q.M. uncompen-sated Tooth loss in Cardiac Patients of Punjab Institute. Journal of Pakistan Madical Association(JPMA).
15. Sotosek J. Kermek JS. Simeon P. Mehicic PG. Potocki BZ. The overall health-status of dental patients. Acta Stomatol Croat. 2007;41(2):122-31.
16. Akar CG. uluer H. ozmutaf MN. ozgur Z. Gokce B. An assess-ment of oral health status and dental plaque of non-dental school students in Turkey. Acta Stomatol Croat. 2010;44(1):26-33.
17. ueta E. osaki T. Yoneda K. Yamamoto T. Prevalemce of diabe-tes mellitus in odontogenic infections and oral candidiasis; an analysis of neutrophyl suppression. J oral Pathol Med. 1993;22(4):168-74.
18. Fenlon MR. McCartan BT. Medical status of patients attend-ing a primary care dental practice in Ireland. J Ir Dent Assoc. 1991;37:75-7.
REFERENCA
Patologjia Numri PërqindjaMerr terapi Nuk merr terapi
Numri Pëqindja Numri Përqindja
Sëmundje kardiovaskulare 450 46.15% 341 75.78% 109 24.22%
Sëmundje neuro-psikike 45 4.62% 45 100% 0 0%
Diabetes mellitus 89 9.13% 89 100% 0 0%
Sëmundje reumatizmale 211 21.64% 76 36.02% 135 63.98%
Sëmundje të SNQ-së 46 7.72% 46 100% 0 0%
Të tjera 134 13.74% 61 45.52% 73 45.48%
Gjithësej 975 100% 658 67.49% 317 32.51%
Tabela 1. Përqindja e pacientëve me sëmundje të rrezikut

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 51
AbstractThe diseases of human organism in generally, and systemic diseases specially, with their fast growth and aggressively, as never before represent a serious health problem for population, also for adequate and relevant institutions too. The scope of our study is to:- determine the per cent of patients with systemic diseases prosthetically treated, - determine the frequency of risk diseases by patients with prosthetic appliances, - determine the per cent of patients with risk diseases treated with therapy and patients
without therapy, and correlation between them.Material and MethodsFor this study were follow up getting data from patients examined in the clinic for prosthetic dentistry “Protetika AG” in Tetova in a period from 2013 to 2015 year.Through the history were providet data for general diseases like: cardiovascular diseases, neuro-physiatric diseases, diabetes mellitus, rheumatic arthrytis, the diseases of CNS, and other pathologies. The getting data are presented with tables and graphics, meanwhile those with special importance are showed with T-test, coefficient of probability (p), and coefficient correlation (Rxy).Resultats The getting results showed that: cardiovascular diseases are present with 46.15%, rheumatic diseases with 21.64%, diabetes mellitus with 9.13%, diseases of CNS with 7.72%, neuro-physiatric diseases with 4.62%.Conclusion The cnowledges about taking therapy from patients with risk diseases are importante becouse of possible interaction between stomatological intervention, anesthesya and drugs prescribet from the side of dentist. Havin data for risk diseases, there is possible to planification intervention in stomatognathic system. The value of t-test and the coeffitient of probability, showed a high statistically and importante significance of results between taking and no taking therapy according the risk diseases by examined patients. According to the value of coefficient of correlation (Rxy= 0.155), in this study there is shoowed that there is a weakened direct connection between the per cent of patients with systemic diseases which are treated with therapy, and patients with systemic diseases not treated.
SheRiF ShaqiRi 1,2 kaltRiNa BeqiRi 1
the frequency of systemic diseases by patients treated with prosthetic appliances
1SPECIALISED CLINIC FOR PROSTHODONTICS“PROTETIKA AG” TETOVA2SCHOOL OF DENTISTRY, FACULTY OF MEKDICAL SCIENCES, UNIVERSITY OF TETOVA
Introduction The diseases of human organism in generally, and
systemic diseases specially, with their fast growth and aggressively, as never before represent a serious health problem for population, also for adequate and relevant institutions too(1). These diseases are defined like resistant chronically diseases, with time limit more than 3 months which affect in life of person and need continuing medical treatment(2).
These diseases play a pivotal role in deciding treatment options in dentistry. By these cases, prosthodontics procedures need to be carefully judged and planned according the systemic status of the patient (3).
There are various disease that of concern in Prosthodontics. These along with their management have been described as under: - cardiovascular diseases which make the most
divulgated category of sistemic diseases, almost in
all countries of the world, which prevalence increase with age, where participate: angina pectoris, infarctus myicardi, endocarditis bacterialis subacuta, congestive heart desorders, hypertension;
- endocrine disorders like diabetes mellitus, which is a clinic syndrome caracterised with hyperglicemia cosed from the absolute or relative lack of insuline(2);
- thyroid diseases;- adrenal gland diseases;- respiratory tractus diseases;- liver diseases like cyrosis;- hematologic diseases like anemy and leuciplaky; - bone diseases like osteoporosis, fobrotic dysplasia
and osteoitis deformans;- neuro-psyhiatric diseases like Parkinson and mouth
burning syndroma;- autoimmune diseases like rheumatic arthritys, where
ATM are frequently affectet(2,3,).
key woRDS:
Frequency,
risk diseases,
prosthetic
appliances,
treated
patients

Albanian Stomatological Journal52
Concerning the prosthetic treatment by patients with sistemic diseases, in dependence from the kind and digree of suffering from these diseases, dentist prosthetist during the treatment must monitoring the vital sings and to take care about: - limitet using of vasoconstrictors(angina pectoris)
and time limit from disease representation till the prosthodontics treatment, and long prosthetics procedures mus be devited and regullated in shortened procedures(infractus myocardi). For these patients prone for angina pectoris or infarctus myocardi, the dentist offers of prosthodontics treatment must be ready for distinction and menage of risks, and in this manner to prevent these cases(3, 4, 5);
- to have knowledges in which situations is contraindication to provide with mobile prosthetic appliances and to take oral impression(endocarditis bacterialis subacuta);
- to take care, and to be ready for prevention of acute exacerbation of chronic diseases (congestive cardiac diseases);
- to apply the protocill for discrease the stres(hipertension);
The primary management goal for the patient with cardiovascular disease during dental therapy is to ensure that hemodynamic changes produced during dental treatments does not exceed the cardiovascular reserve of the patient(6, 7); - to use an impression technique that will produce
maximum physiologic compatibility of the denture base with supporting structure, careful occlusal correction should be accomplished to remove all interferences, the food table should be small and the patient should be given detailed instructions on eating habits and oral hygiene, frequent evaluation of denture is necessary and patients which are prone to develop infections and vascular complication so an antibiotic prophylaxis before prosthodontics therapy to prevent subsequent infection is advised(diabetes mellitus), and patients from all ages prosthetically treated must anderstand that this established metabilic disorder could have an impact on the outcom result of prosthetic treatment(3,4,8,9,10,11,12);
- patients with difficulty in breathing upon exertion and using bronchodilator therapy should undergo medical examination, and use of epinephrine or vasoconstrictors in anesthetics or gingival retraction cord is not advised(pulmonary diseases)(13);
-that prosthodontists are in a strategic position to intercept early evidence of osteoporosis and educate the geriatric patient towards good nutrition. Designing complete denture requires special consideration for these patients to preserve the underlying tissue structure as much as possible(osteoporosis)(2);
- that neurologic emergencies like stroke, syncope and seizures require thorough history and list of medications, and consultation with physician is helpful in treating these patients(neuro-psyhiatric
diseases)(3); - that cases with rheumatismal diseases which are
a musculoskeletal disorder characterized by the inflammation of joints, treatment should be primarily focused on antirheumatic medications as the prosthetic procedures do not cure the joint disease and are therefore secondary, since the disease commonly occurs between acute and chronic stages, the irreversible treatment like fixed prosthesis should not be given until the disease is cured(rheumatoid diseases)(2,8). The problem encountered in the prosthodontics rehabilitation of patients with rheumatoid arthritis of TMJ is manifested with changes in occlusion and jaw relation(8).
The successful management of patient begins right from the medical history to the treatment plan in which much consideration has to be given to the systemic status of individual. Prosthodontist neglecting the systemic status in the history will step into more serious complication at the cost of individual life(3)
Aim of the studyThe aim of our study is that through collected data
from clinical examination to:- determine the per cent of patients with systemic
diseases prosthetically treated,- determine the frequency of risk diseases by patients
provided with prosthetic appliances, - determine the frequency of patients with risk diseases
treated with therapy and those without therapy treatment, and to verify the correlation between them.
Material and methodsFor this study are follow up the getting data from
examined patients in the specialised dental clinic “Protetika Ag” in Tetova from 2013 to 2015 year, which came in our clinic for expressing their complaints concerning the stomatognatic system. From this group, 943(52.83%) of them were males, and 842(47.17%) were females, and the age of examinated patients were from 13 to 82 year old, with average age from 48.2 year.
Through the history were providet data for diseases like: - cardiovascular diseases,- neuro-psyhiatric diseases, - diabetes mellitus,- rheumatoid diseases- CNS diseases and - other pathologies.
The getting data are evidenced in patient chart using the modificated forme of evaluation of oral health according WHo(World Health organization), adapted and modificated accordin of nature of our study. The getting data after their statistically elaboration are showed with graphics and tables, while data with importance are showed with T-test, coefficient of probability (p) and coefficient of correlation (Rxy)
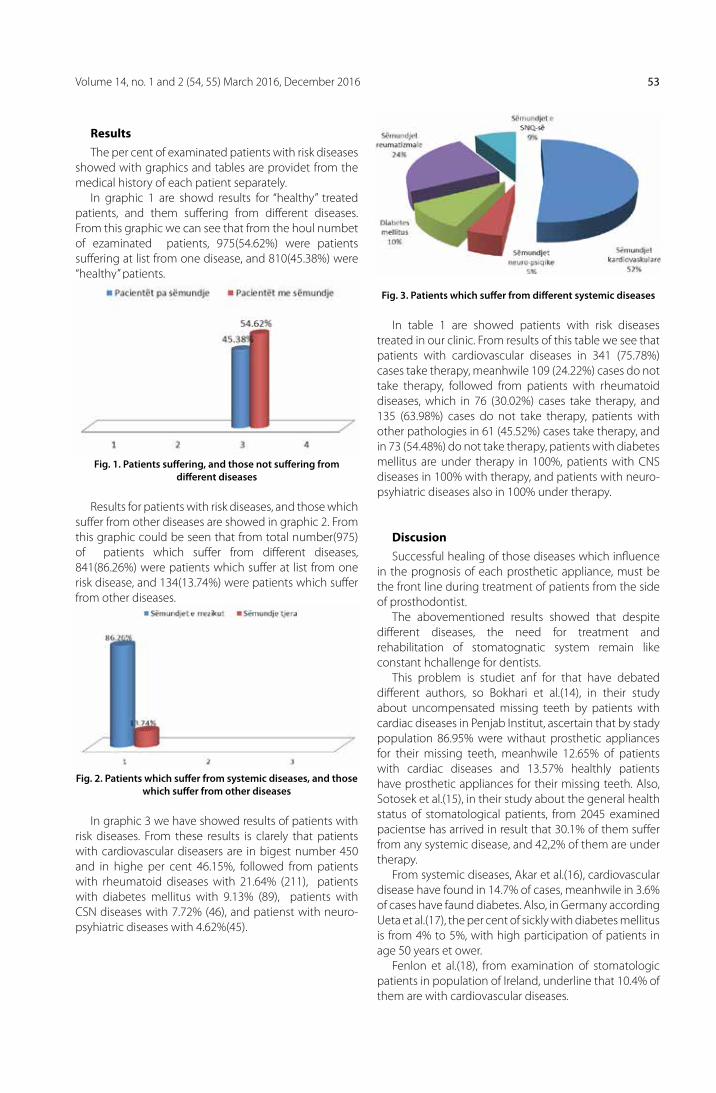
Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 53
ResultsThe per cent of examinated patients with risk diseases
showed with graphics and tables are providet from the medical history of each patient separately.
In graphic 1 are showd results for “healthy” treated patients, and them suffering from different diseases. From this graphic we can see that from the houl numbet of ezaminated patients, 975(54.62%) were patients suffering at list from one disease, and 810(45.38%) were “healthy” patients.
Fig. 1. Patients suffering, and those not suffering from different diseases
Results for patients with risk diseases, and those which suffer from other diseases are showed in graphic 2. From this graphic could be seen that from total number(975) of patients which suffer from different diseases, 841(86.26%) were patients which suffer at list from one risk disease, and 134(13.74%) were patients which suffer from other diseases.
Fig. 2. Patients which suffer from systemic diseases, and those which suffer from other diseases
In graphic 3 we have showed results of patients with risk diseases. From these results is clarely that patients with cardiovascular diseasers are in bigest number 450 and in highe per cent 46.15%, followed from patients with rheumatoid diseases with 21.64% (211), patients with diabetes mellitus with 9.13% (89), patients with CSN diseases with 7.72% (46), and patienst with neuro-psyhiatric diseases with 4.62%(45).
Fig. 3. Patients which suffer from different systemic diseases
In table 1 are showed patients with risk diseases treated in our clinic. From results of this table we see that patients with cardiovascular diseases in 341 (75.78%) cases take therapy, meanhwile 109 (24.22%) cases do not take therapy, followed from patients with rheumatoid diseases, which in 76 (30.02%) cases take therapy, and 135 (63.98%) cases do not take therapy, patients with other pathologies in 61 (45.52%) cases take therapy, and in 73 (54.48%) do not take therapy, patients with diabetes mellitus are under therapy in 100%, patients with CNS diseases in 100% with therapy, and patients with neuro-psyhiatric diseases also in 100% under therapy.
Discusion Successful healing of those diseases which influence
in the prognosis of each prosthetic appliance, must be the front line during treatment of patients from the side of prosthodontist.
The abovementioned results showed that despite different diseases, the need for treatment and rehabilitation of stomatognatic system remain like constant hchallenge for dentists.
This problem is studiet anf for that have debated different authors, so Bokhari et al.(14), in their study about uncompensated missing teeth by patients with cardiac diseases in Penjab Institut, ascertain that by stady population 86.95% were withaut prosthetic appliances for their missing teeth, meanhwile 12.65% of patients with cardiac diseases and 13.57% healthly patients have prosthetic appliances for their missing teeth. Also, Sotosek et al.(15), in their study about the general health status of stomatological patients, from 2045 examined pacientse has arrived in result that 30.1% of them suffer from any systemic disease, and 42,2% of them are under therapy.
From systemic diseases, Akar et al.(16), cardiovascular disease have found in 14.7% of cases, meanhwile in 3.6% of cases have faund diabetes. Also, in Germany according ueta et al.(17), the per cent of sickly with diabetes mellitus is from 4% to 5%, with high participation of patients in age 50 years et ower.
Fenlon et al.(18), from examination of stomatologic patients in population of Ireland, underline that 10.4% of them are with cardiovascular diseases.

Albanian Stomatological Journal54
Conclusion1. The difference in per cent by results of different
authors concerning the risk diseases by examined stomatological patients can be explaned with different standards which exist in different countries from which came authors and studies.
2. The cnowledges about taking therapy from patients with risk diseases are importante becouse of possible interaction between stomatological intervention, anesthesya and drugs prescribet from the side of dentist.
3. Having data for risk diseases, there is possible planification of intervention in stomatognathic system.
4. The value of t-test=11, and the value of coeffitient of probability p<0.01, showed for a high statistically and importante significance of results between taking and withaut taking therapy according the risk diseases by examined patients.
5. According to the value of coefficient of correlation (Rxy= 0.155), could be seen that by our results exist a wakened direct connection between the per cent of patients with systemic diseases which are treated with therapy, and patients with systemic diseases not treated with therapy.
1. Shaqiri Sh. Problemet e protezimit te pacientët me denti-cion të përhershëm te popullata e Tetovës dhe rrethinat e saj. Disertacion Doktorature. universiteti i Mjekësisë Tiranë, Fakulteti i Mjekësisë. 2013.
2. Mary T. Kari A. lindefjeld C. laura S.M. Systemic Diseases and oral Health. Journal of Dental Clinics of North America: (october 2014).
3. Singh N. Systemic Diseases Concern to Prosthodontist. Int J oral Health Med Res 2015;2(2):89-93. ISSN 2395-7387
4. Varon F, Mack-Shipman l. The role of dental professional in diabetes care. J Contemp Dent Prac 2000; 1:1-27.
5. Marta Cruz-Pamplona, Yolanda Jimenez-Soriano, Maria Gra-cia Sarrión-Pérez. Management of cardiological patients J Clin Exp Dent. 2011;3(2):e97-105. Doi:10.4317/jced.3.e97.
6. Glick M, Greenberg Bl The potential role of dentists in iden-tifying patients’ risk of experiencing coronary heart disease events. J Am Dent Assoc. 2005 Nov;136(11):1541-6
7. Gilbert GH, Minaker Kl.Principles of surgical riks assessment of the elderly patient. J oal Maxillofac Surg 1990;48:972-9
8. Bavitz JB. Dental management of patients with hyperten-sion. Dent Clin North Am. 2006 oct;50(4):547-62
9. Arthritis Foundation. Available at: http://www.arthritis.org/conditions-treatments/understanding-arthritis/.
10. Kansal G, Goyal D. Prosthodontic Management of Pa-tients With Diabetes Mellitus. J Adv Med Dent Scie Res 2013;1(1):38-44.
11. Talib Amin Naqash, Sunil Jangral, Popinder Singh, Nusrat Nazir, Sheema Bashir, Samrina Gulzar. Diabetes Mellitus: A concern for Prosthodontic care. International Journal of Clinical Cases and Investigations 2013. Volume 5 (Issue 3), 30:33, 1st october 2013
12. Frier BM, Truswel AS, Shepherd J, Jung R. Diabetes mellitus nutritional and metabolic disorders. Davidson’s Principles and Practice of Medicine. 18th ed.uK: Churchill living stone 2001; 471-542
13. Varon F, Mack-Shipman l. The role of dental professional in diabetes care. J Contemp Dent Prac 2000; 1:1-27.
14. Bokhari H.A.S. Khan A.A. Azhar M. Shahbaz Q.M. uncom-pensated Tooth loss in Cardiac Patients of Punjab Institute. Journal of Pakistan Madical Association(JPMA).
15. Sotosek J. Kermek JS. Simeon P. Mehicic PG. Potocki BZ. The overall health-status of dental patients. Acta Stomatol Croat. 2007;41(2):122-31.
16. Akar CG. uluer H. ozmutaf MN. ozgur Z. Gokce B. An as-sessment of oral health status and dental plaque of non-dental school students in Turkey. Acta Stomatol Croat. 2010;44(1):26-33.
17. ueta E. osaki T. Yoneda K. Yamamoto T. Prevalemce of dia-betes mellitus in odontogenic infections and oral candi-diasis; an analysis of neutrophyl suppression. J oral Pathol Med. 1993;22(4):168-74.
18. Fenlon MR. McCartan BT. Medical status of patients attend-ing a primary care dental practice in Ireland. J Ir Dent Assoc. 1991;37:75-7.
REFERENCES
Patology Number PercentageTherapy No therapy
Number Percentage Number Percentage
Cardiovascular diseases 450 46.15% 341 75.78% 109 24.22%
Neurologic diseases 45 4.62% 45 100% 0 0%
Diabetes mellitus 89 9.13% 89 100% 0 0%
Rheumatism 211 21.64% 76 36.02% 135 63.98%
CNQ diseases 46 7.72% 46 100% 0 0%
Other 134 13.74% 61 45.52% 73 45.48%
Total 975 100% 658 67.49% 317 32.51%
Table 1. The percentage of patients with risk diseases

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 55
AbstraktQëllimi: Përcaktimi dhe krahasimi i rezistencës ndaj frakturës së dhëmbëve të trajtuar endodontikisht të restauruar me materiale të ndryshme kompoziti. Materiale e Metoda: 40 molarë maksilarë dhe 40 mandibularë pas trajtimit endodontik dhe procedurave adezive u ndanë në 3 nëngrupe për çdo tip dhëmbi (n=10): Grupi A: grupi I kontrollit (dhëmbë intaktë); Grupi B: kavitetet hyrës u restauruan me rezinë kompozite tradicionale (EsthetX; Dentsply-Italy, Rome, Italy); Grupi C: kavitetet hyrës u restauruan me kompozitbulkfill flow (SDR; Dentsply-Italy) ; Grupi D: kavitetet hyrës u restauruan me kompozitbulkfill (SonicFill; Kerr-California, uSA). Kampionët iu nënshtruan forcës kompresive për testimin statik deri sa të ndodhte fraktura, forca maksimale për frakturën e kampionëve u mat (N) dhe u regjistrua tipi i frakturës. Të dhënat u analizuan statistikisht me analizën e vaiancës (ANoVA) dhe testet Bonferroni (P<0.05).Rezultate: Asnjë diferencë statistikisht e rëndësishme nuk u gjet ndërmjet grupeve të dhëmbëve intaktë në krahasim me dhëmbët e trajtuar endodontikisht në të gjitha grupet (P<0.05). Asnjë diferencë statistikisht e rëndësishme nuk u gjet në rezistencën ndaj frakturës dhe ndërmjet dy grupeve të restauruar me kompozite bulkfill SDR e SonicFill.Konkluzione: Rezistenca ndaj frakturës e dhëmbëve të restauruar me rezinë kompozite tradicionale dhe me kompozite bulkfill ishte e ngjashme në molarët maksilarë e mandibularë dhe nuk tregoi asnjë zvogëlim të rezistencës ndaj frakturës krahasuar me kampionët intaktë.
almira isufi1,2 gianluca plotino1, Nicola maria grande3, pietro ioppolo4, luca testarelli1 , Rossella Bedini4, gianluca gambarini1
Rezistenca ndaj frakturës e dhëmbëve të trajtuar endodontikisht me kavitete hyrës konservativë të restauruar me materiale të ndryshme kompozite
1Departementi i Endodontisë, Sapienza Universitàdi Roma, Rome, Itali2Fakulteti i Mjekesisë Dentare, Universiteti i Mjekësisë Tiranë, Shqipëri3Università Cattolica del Sacro Cuore, Rome, Itali4Istituto Superiore di Sanità, Dipartimento di Tecnologie e Sanità, Rome, Itali
Fjalët kyçe:
Rezistenca
ndaj frakturës,
trajtim
endodontik,
kompozit
bulkfill, rezinë
kompozite
Hyrje
Rehabilitimi funksional dhe estetik i dhëmbëve të trajtuar endodontikisht ka qënë objekt i studimeve të ndryshme (1). Restaurimi duhet jo vetëm të sigurojë funksionin, estetikën dhe vulosjen marginale, por edhe të mbrojë strukturën e mbetur të dhëmbit (2,3). Studime të ndryshme kanë treguar se përgatitja e kaviteteve hyrës endodontike zvogëlon fortësinë e dhëmbëve, për shkak të përgatitjeve të kaviteteve të thella dhe të zgjeruara të cilat zvogëlojnë në mënyrë kritike sasinë e dentinës (4-8) dhe rrisin deflektimin kuspal gjatë funksionit (9). Rëndësia e ruajtjes së dentinës u shfaq në ruajtjen e integritetit strukturor dhe në prognozën e dhëmbëve endodontik të restauruar (10-13), pasi rezistenca ndaj frakturës dhe shpërndarja e stresit të dhëmbëve të trajtuar endodontikisht ndikohet drejtpërdrejt nga sasia e dentinës koronale të mbetur (4, 14-18).
Në përgatitjet posteriore, sidomos kur margo cervikale është në dentinë, efektet e tkurrjes së polimerizimit mund të jenë të rëndësishme, duke prodhuar defekte marginale dhe boshllëqe, pavarësisht aplikimit të kujdesshëm (19). Janë propozuar teknika të ndryshme dhe shumëllojshmëri e materialeve restaurative, të cilët do të minimizonin streset e krijuara në ndërfaqen e restaurimit duke modifikuar disa veti fizike dhe mekanike
për të reduktuar efektet e tkurrjes së polimerizimit (20-22). Për më tepër, polimerizimi i pamjaftueshëm përgjatë restaurimit mund të kompromentojë vetitë e tij fizike dhe mund të çojë në efekte të padëshirueshme, të tilla si formimi i boshllëqeve, rrjedhje marginale, karies rekurent (23-26). Ajo gjithashtu mund të ndikojë negativisht në indet e pulpës dhe mund të çojë në dështimin e parakohshëm të restaurimit (27,28).
Prodhues të ndryshëm kanë zhvilluar dhe prezantuar kohët e fundit lloje të reja rezina kompozite, të ashtuquajturat materiale “bulkfill”, të cilat mund të aplikohen në kavitet dhe të polimerizohen me dritë në shtresa me një trashësi maksimale prej 4-5 mm (29-32) me përforcim të polimerizimit, tkurrjes dhe vetive fizike (33). Kompozitet bulkfill flow përdoren bashkë me kompozitet konvencionale për restaurimet estetike në dhëmbët posteriorë, duke patur stres polimerizimi më të ulët, rrjedhshmëri më të mirë me vendosje të lehtë, një përshtatje të shkëlqyer me muret e zgavrës dhe modul të ulët të elasticitetit, të cilat mund të zvogëlojnë stresin e gjeneruar në muret e kavitetit (34).
Qëllimi i këtij studimi in vitro ishte të krahasojë rezistencën ndaj frakturës të molarëve të sipërm dhe të poshtëm të trajtuar endodontikisht të restauruar me

Albanian Stomatological Journal56
restaurime të drejtpërdrejtë rezine kompozite të ndryshme, tradicionale dhe bulkfill. Hipoteza e zerose testuar ishte që ka një ndryshim në rezistencën ndaj frakturës dhe në mënyrën e frakturës midis molarëve maksilarë dhe mandibularë të trajtuar endodontikisht dhe të restauruar me rezinë kompozite tradicionale dhe bulkfill.
Materiale e metoda
Tetëdhjetë molarë maksilarë dhe mandibularë të ekstraktuar, intaktë, me apekse të formuar plotësisht janë përdorur në këtë studim in vitro. Kriteret e përjashtimit për dhëmbët e testuar ishin prania e kariesit, restaurime të mëparshme dhe linja të dukshme thyerje ose krisje. Pas një debridement me instrumente dore dhe pastrimit me pomice, dhëmbët u ruajtën në kontejnerë të numëruar në mënyrë individuale me 0.1% sol thymol në 4 ° C deri kur u përdorën. 40 molarë maksilarë me tri rrënjë të veçanta dhe 40 molarë mandibularë me dy rrënjë të ndara u përzgjodhën bazuar në lartësi të ngjashme anatomike të kurorës, matur nga sipërfaqja okluzale në junksionin cemento-smalt në të katër anët e dhëmbëve, dhe dimensionet bucco-lingual (Bl), mesio-distal (MD) në sipërfaqen okluzale. Matjet e dhëmbëve janë bërë me një kalibër dixhital. Radiografitë paraprake janë bërë në dy drejtime perpendikulare (MD dhe Bl) për të përcaktuar anatominë e kanaleve të rrënjëve dhe për të matur gjatësinë dhe gradën e kurbaturës së kanalit duke përdorur metodën Schneider (35). Kampionët më pas u caktuan në 4 grupe (n = 10), për secilin lloj të dhëmbëve duke krijuar grupe homogjene duke konsideruar mesataren e dimensioneve të dhëmbëve për të minimizuar ndikimin e madhësisë dhe variacioneve në formë në rezultate:• Grupi A, grupi i kontrollit negativ, i cili përfshin 10
molarë maksilarë dhe 10 molarë mandibularë që janë lënë të paprekur për testimin e thyerjes, pa asnjë përgatitje kaviteti apo trajtim të kanalit të rrënjës;
• Grupi B, i cili përfshin 10 molarë maksilarë dhe 10 molarë mandibularë, në të cilët janë përgatitur kavitetet hyrës endodontikë dhe u janë nënshtruar procedurave endodontike dhe janë restauruar me rezinë kompozite (EsthetX; Dentsply-Itali, Romë, Itali);
• Grupi C, i cili përfshin 10 molarë maksilarë dhe 10 molarë mandibularë, në të cilët janë përgatitur kavitetet hyrës endodontikë dhe u janë nënshtruar procedurave endodontike dhe janë restauruar me një kompozit bulkfill flowable (SDR; Dentsply-Itali), meinkremente 4mm, me përjashtim të shtresës 1.5 mm të sipërfaqes okluzale që u restaurua me të njëjtën rezinë kompozite si grupi B.
• Grupi D, i cili përfshin 10 molarë maksilarë dhe 10 molarë mandibularë, në të cilët janë përgatitur kavitetet hyrës endodontikë dhe u janë nënshtruar procedurave endodontike dhe janë restauruar me kompozit bulkfill (SonicFill; Kerr-California, uSA) me shtresa inkrementale 5mm.
Të gjithë kavitetet hyrës janë përgatitur sipas principeve konservative të përshkruara nga Clark e Khademi (36). Kaviteti hyrës është përgatitur duke përdorur freza të rrumbullakëta dhe cilindrike dhe fund-jo-prerës me diametra të ndryshme, të diamantuara, të ftohura me ujë, të montuara në turbinë. Kanalet radikulare janë negociuar me K-file me madhësi 10 (Flexofile, Dentsply Maillefer, Ballaigues, Switzerland) deri në foramen apikal dhe kanalet u instrumentuan në gjatësi pune me instrumente rrotulluese NiTi (Mtwo; Sweden& Martina, Padova, Italy) deri në file me madhësinë tip 0.25 dhe taper 0.06. Gjatë trajtimit endodontik është përdorur irrigimi në mënyrë intermitente me 5.25% hipoklorit natriumi (Niclor 5, ogna, Muggio Milano, Italy) duke përdorur ProRinse me agë me dalje anësore 30 G (DENTSPlY Tulsa Dental Specialties, Tulsa, oK). Kanalet u thanë me kone letre dhe u mbushën me guta-percha (single-kon # 25 / 0.06 taper) dhe një cement endodontik me bazë rezinoze (AH-Plus, DENTSPlY Maillefer, Ballaigues, Zvicër). Pas procedurave të pastrimit, përpunimit dhe mbushjes, dhëmbët iu nënshtruan radiografive post-operative në dy dimensione perpendikulare (MD dhe Bl) për të vlerësuar trajtimin endodontik. Pastaj smalti dhe dentina e kavitetit hyrës u acidifikuan me acid fosforik 37% për 30 dhe 15 sekonda, respektivisht, u shplanë për 30 sekonda me një spray ujë/ajër, dhe u thanë me kujdes për të shmangur mbi-tharjen. Një adeziv primer-bond i polimerizueshëm me dritë (XP Bond,, Dentsply International, York, uSA) u aplikua, u përdor ajër me kujdes dhe u ekspozua ndaj polimerizit lED për 40 sekonda. Në grupin B kavitetet hyrës u restauruan me rezinë kompozite të drejtpërdrejtë (EsthetX) me shtresa inkrementale maksimale të materialit 2mm. Kampionët në grupin C u restauruan me një kompozit bulkfill flowable me trashësi maksimale inkrementale prej 4mm (SDR), me përjashtim të 1.5 mm shtresë e sipërfaqes okluzale që u restaurua me të njëjtën rezinë kompozite si grupin B (Fig. 1).
Fig.1. Acidifikim me acidi fosforik 37% të smaltit e dentinës së kaviteteve hyrës (A), aplikimi i adezivit primer-bond
të fotopolimerizueshëm(B),aplikimi i kompozitit bulkfill flowable SDR me shtresa inkrementale 4mm (C), restaurimi
final i siperfaqes okluzale (D)

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 57
“i pafavorshëm”, sepse jo-i restaurueshëm, kur dështimet shtriheshin nën nivelin e simulimit të kockës (vendi i frakturës nën rezinën akrilike).
Të dhënat u verifikuan me testin Kolmogorov-Smirnov për normalitetin e shpërndarjes dhe testin levene për homogjenitetin e variancës. Kështu, ata janë vlerësuar statistikisht nga analiza e variancës dhe testimi Student-Newman-Keuls për krahasime multiple (Prism 5.0; GraphPad Software, Inc, la Jolla, CA), me nivel të rëndësisë të vendosur në 5% (P <.05).
Rezultate
Mesatarja e dimensioneve bucco-linguale (Bl) dhe mesio-distale (MD) në sipërfaqen okluzale dhe lartësisë anatomike të kurorës së dhëmbëve të testuar janë paraqitur në Tabelën 1. Asnjë dallim i rëndësishëm nuk u gjet në krahasimin e të gjitha dimensioneve të dhëmbëve në grupet e kontrollit dhe të testuar (P> 05).
Asnjë ndryshim statistikisht i rëndësishëm nuk u gjet ndërmjet grupeve (P <0.05). Rezistenca ndaj frakturës së dhëmbëve të trajtuar endodontikisht të restauruar me një rezinë kompozite tradicionale dhe me kompozite bulkfill (SDR e SonicFill) ishte e ngjashme në molarët maksilarë (Grupi B: 1185 ± 482N, Grupi C: 1268 ± 354N, Grupi D:1308 ± 418N) dhe mandibularë (Grupi B: 1416 ± 307N, Grupi C: 1535± 432N, Grupi D: 1613± 372N). Dhëmbët e restauruar nuk treguan rënie të konsiderueshme në rezistencën ndaj frakturës në krahasim me kampionët intaktë në molarët maksilarë (Grupi A: 1234 ± 315N) dhe molarët mandibularë (Grupi A: 1684 ± 232N) (Tabela 2).
61,25% e frakturave në total ishin të pafavorshme (Grupi B 70%, Grupi C 75%, Grupi D75%, grupi i kontrollit, 25%). Nuk u vunë re ndryshime të mëdha në llojin e frakturës së dhëmbëve të restauruar ndërmjet grupeve të dhëmbëve të restauruar, ndërsa dhëmbët intaktë shfaqën në mënyrë të konsiderueshme fraktura më të favorshme në krahasim me frakturat e kampionëve të restauruar.
Diskutime
Hipoteza zero e hetuar në këtë studim mund të hidhet poshtë, pasi rezultatet e arritura tregojnë që nuk ka dallim në rezistencën ndaj frakturës dhe në llojin e frakturës ndërmjet molarëv emaksilarë dhe molarëve mandibularë të trajtuar endodontikisht të restauruar me një rezinë kompozite bulkfill (SDR e SonicFill) ose një rezinë kompozite tradicionale.
Predispozita për frakturë e dhëmbëve të trajtuar endodontikisht ndikohet kryesisht nga sasia e mbetur e dentinës (4, 38), dhe kjo nuk është e lidhur me vetitë e saj biomekanike pas trajtimit endodontik, si fortësia dhe rezistenca (39). Disa studime kanë treguar se reduktimi i strukturës së dhëmbit rezulton në dhëmbë të dobët për shkak të procedurave restaurative (6-8). Megjithatë, sipas Reeh et al. (4), procedurat endodontike kanë
Kampionët në grupin D u restauruan me një kompozit bulkfill me trashësi maksimale inkrementale prej 4mm (SonicFill), me përjashtim të 1.5 mm shtresë e sipërfaqes okluzale që u restaurua me të njëjtën rezinë kompozite si grupin B. Të gjithë kampionët u shënuan 2 mm nën lidhjen smalt-cement dhe u mbuluan me një shtresë dylli me trashësi rreth 0.25 mm. Kampionët u vendosën në rezinë akrilike auto polimerizuese (SR Ivolen, Ivoclar Vivadent, Schaan, lichtenstein) në forma metalike cilindrike në pozicionin e aksit të tyre gjatësor paralel me atë të formave cilindrike. Për të simuluar ligamentin periodontal, në shenjat e para të fillimit të polimerizimit, dhëmbët u hoqën nga blloqet e rezinës dhe dylli u pastrua nga sipërfaqet e rrënjëve. Një shtresë standarde silikoni u krijua duke përdorur një material mase light-body silicon-based (Aquasilultra light bodies, Dentsply International, York, SHBA) e cila u injektua në bazat e rezinës qe po polimerizohej. Dhëmbët me sipërfaqen e rrënjëve tani pa dyll u vendosën në bazat e rezinës menjëherë pas injektimit të silikonit (37). Të gjithë kampionët u ruajtën në solucion fiziologjik plus 1.5% thymol në temperaturë dhome (24-28°C) deri në proçedurën e testimit të frakturës. Të gjitha kampionët u vendosën në një makinë universale të testimit të ngarkesës (lR30K; lloyd Instruments ltd, Fareham, uK). Dhëmbët u ngarkuan në fossan qëndrore të tyre në një kënd 30° me boshtin gjatësor të dhëmbit (Fig.2).
30°
150°
Fig.2. Simulimi i ngarkesës okluzale duke përdorur një sferë çeliku me diameter 6mm e vendosur në fosën qëndrore
me orientim lingual në linjë aksio-okluzale me kënd 30° me aksin gjatësor të një molari mandibular.
Forca e vazhdueshme kompresive me një shpejtësi cross-head 1.6 mm/s u aplikua me një kokë kompresive çeliku me fund në formë topi me diametër 6 mm deri sa u vunë re prova të dukshme apo të dëgjueshme të frakturës. Forca e frakturës u mat në Newton (N) dhe lloji i frakturës u regjistrua si “i favorshëm” për arsye të restaurimit, kur dështimet ishin mbi nivelin e simulimit të kockës (vendi i frakturës mbi rezinën akrilike) dhe si

Revista Stomatologjike Shqiptare58
vetëm një efekt të vogël në dhëmb, duke reduktuar rigiditetin relativ me 5%, që i detyrohet tërësisht kavitetit hyrës. Procedurat restauruese dhe, në veçanti, humbja e integritetit të kreshtave marginale, ishin kontribuesit më të mëdhenj për humbjen e rezistencës së dhëmbit. Humbja e 1 kreshte marginale rezultoi me një humbje prej 46% në rigiditetin e dhëmbëve, dhe një përgatitje MoD rezultoi në një humbje mesatare prej 63% në rigiditetin relativ kuspal.
Disa studime janë kryer për të përcaktuar materialet dhe teknikat ideale për të restauruar dhëmbët e trajtuar endodontikisht sepse prognoza e tyre afat-gjatë varet nga cilësia e restaurimit final (40-43). Zakonisht, për të restauruar dhëmbët e trajtuar endodontikisht janë të nevojshme disa inkremente rezine për të mbushur kavitetin e preparuar për shkak të vëllimit të madh të restaurimit. Kështu, klinicisti duhet të kompensojë tkurrjen e polimerizimit të rezinave kompozite tradicionale, duke i mbushur kavitetet në disa inkremente (44). Një kategori e re e rezinave kompozite është prezantuar si material bulkfill base që mund të aplikohet në bulks 4mm të trashë në vend të përdorimit të teknikës inkrementale, pa ndikuar negativisht në tkurrjen e polimerizimit,
përshtatjen në kavitet apo gradën e konvertimit (30-32).Rezultatet e këtij studimi tregojnë se nuk ka pasur
dallime të mëdha në rezistencën e frakturës statike të molarëve të trajtuar endodontikisht të restauruar me rezinë kompozite bulkfill (SDR e SonicFill) dhe me rezinë kompozite tradicionale. Për më tepër, ngarkesa mesatare e frakturës së dhëmbëve të restauruar me SDR dhe SonicFill është më e lartë krahasuar me ngarkesën mesatare të frakturës së kampionëve të restauruar me rezinë kompozite tradicionale, pa ndonjë ndryshim me rëndësi statistikore. Për më tepër, rezultatet e këtij studimi treguan se nuk ka ndonjë ndryshim të rëndësishëm ndërmjet dhëmbëve të restauruar me rezinë kompozite bulkfill (Surefil SDR e SonicFill) dhe dhëmbëve intaktë. Këto rezultate mund t’i atribuohen efektit elastik buffer të përdorimit të viskozitetit të ulët të kompoziteve, stresit të ulët të tkurrjes dhe modulit të ulët të elasticitetit (45,46).
Në studim 75% e kampionëve të grupit të kontrollit të lënë intaktë paraqitën fraktura të favorshme, me një ndryshim të rëndësishëm statistikor krahasuar me grupet e kampionëve të restauruar. Në fakt, shumica e dhëmbëve restauruar me SDR (75%), SonicFill (75%) dhe me kompozite tradicionale (70%) paraqitën
GRuPI KONTROLLKOMPOZIT BuLKFILL
FLOwABLE (SDR)
KOMPOZIT BuLKFILL
(SONICFILL)
REZINë KOMPOZITE
TRADICIONALE
Tipi i
Dhëmbit
(n=10)
Sipërfaqja
okluzale
lartësia
e Kurorës
Anatomike
Sipërfaqja okluzalelartësia
e Kurorës
Anatomike
Sipërfaqja
okluzale
lartësia
e Kurorës
Anatomike
Sipërfaqja
okluzale
lartësia
e Kurorës
Anatomike MD Bl MD Bl MD Bl MD Bl
Molarë
Maksilarë 9.9 a (0.6)
10.1 a
(0.9)5.4 (0.4)b
10.0 a
(0.5)
10.1 a
(1.0)5.5 (0.6)b
10.0 a
(0.5)
10.1 a
(0.9)5.6 (0.6)b
9.9 a
(0.5)
10.1 a
(0.8)5.3 (0.4)b
Molarë
Mandibularë
10.6 a
(1.1)
10.1 a
(0.8)5.7 (0.6)b
10.5 a
(0.9)
10.2 a
(0.7)5.5 (0.4)b
10.7 a
(1.2)
10.2 a
(0.8)5.6 (0.5)b
10.5a
(1.1)
10.1 a
(0.7)5.6 (0.6)b
Shkronja e njëjtë në të njëjtin rresht tregon se nuk ka diferenca statistikisht të rëndësishme (P >.05).
Tabela 1. Mesatarja dhe (Deviacioni Standart) i dimensioneve Mezio–Distal (MD) dhe Buko–Lingual (BL) dhe lartësia anatomike e kurorës (e matur në të katër anët e dhëmbit) e dhëmbëve të testuar në secilin grup
TIPI I
DHëMBIT
(N=10)
FORCA E FRAKTuRëS (N)LLOJI I FRAKTuRëS
Grupi A Grupi B Grupi C Grupi D
Grupi A Grupi B Grupi C Grupi D F P F P F P F P
Molarë
Maksilarë 1234 (315)a 1185 (482)a 1268 (354)a 1308 (418)a 8a 2b 3b 7a 3b 7a 3b 7a
Molarë
Mandibularë1684 (232)a 1416 (307)a 1535 (432)a 1613 (372)a 7a 3b 3b 7a 2b 8a 2b 8a
Shkronja e njëjtë në të njëjtin rresht tregon se nuk ka diferenca statistikisht të rëndësishme (P >.05).
Tabela 2. Forca e frakturës (mesatarja ± deviacioni standart) dhe lloji i frakturës, i Favorshëm (F) ose i Pafavorshëm (P) për dhëmbët intaktë (kontroll, Grupi A), dhe dhëmbët e restauruar me rezina kompozite tradicionale (Grupi B), me kompozit bulkfill flowable SDR
(Grupi C), ose me kompozit bulkfill SonicFill (Grupi D), e vlerësuar pas testit statik duke përdorur Instron universal Machine.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 59
1. Meyenberg K. The ideal restoration of endodontically treat-ed teeth - structural and esthetic considerations: a review of the literature and clinical guidelines for the restorative clinician. Eur J Esthet Dent. 2013;8(2):238-268.
2. Steele A, Johnson BR. In vitro fracture strength of endodon-tically treated premolars. J Endod1999;25:6-8.
3. Krejci I, Duc o, Dietschi D, de Campos E. Marginal adapta-tion, retention and fracture resistance of adhesive com-posite restorations on devital teeth with and without posts. oper Dent 2003;28:127-135.
4. Reeh ES, Messer HH, Douglas WH. Reduction in tooth stiff-ness as a result of endodontic and restorative procedures. J Endod1989;15:512-516.
5. owen CP (1986) Factors influencing the retention and re-sistance of preparations for cast intracoronal restorations. J Prosthet Dent 55(6) 674-677.
6. Fokkinga WA, Kreulen CM, Vallittu PK, Creugers NH. A struc-tured analysis of in vitro failure loads and failure modes of fiber, metal, and ceramic post-and-core systems. Int J Prosthodont2004;17:476–482.
7. Panitvisai P, Messer HH. Cuspal deflection in molars in re-lation to endodontic and restorative procedures. J Endod 1995;21(2):57-61.
8. Mondelli J, Steagall l, Ishikiriama A, de lima Navarro MF, Soares FB. Fracture strength of human teeth with cavity preparations. J Prosthet Dent 1980;43:419-422.
9. Tang W, Wu Y, Smales RJ. Identifying and reducing risks for potential fractures in endodontically treated teeth. J En-dod2010;36:609-617.
10. Ree M, Schwartz RS. The endo-restorative interface: Current concepts. Dent Clin North Am. 2010;54:345-374.
11. Huang TJ, Shilder H, Nathason D. Effects of moisture con-tent and endodontic treatment on some mechanical prop-erties of human dentin. J Endo 1992;18:209-215.
13. Tzimpoulas NE, Alisafis MG, Tzanetakis GN, Kontakiotis EG. A prospective study of the extraction and retention inci-dence of endodontically treated teeth with uncertain prog-nosis after endodontic referral. J Endod. 2012;38:1326-1329.
14. Ichim I, Kuzmanovic DV, love RM. A finite element analysis of ferrule design on restoration resistance and distribution of stress within a root. IntEndod J 2006;39:443-452.
15. libman WJ, Nicholls JI. load fatigue of teeth restored with cast posts and cores and complete crowns. Int J Prostho-dont 1995;8: 155-161.
16. Akkayan B. An in vitro study evaluating the effect of fer-rule length on fracture resistance of endodontically treated teeth restored with fiber-reinforced and Zirconia dowel sys-tems. J Prosthet Dent 2004;92:155-162.
17. Kishen A, Kumar GV, Chen NN. Stress-strain response in hu-man dentine: rethinking fracture predilection in postcore restored teeth. Dent Traumatol 2004;20:90-100.
18. Da Silva NR, Raposo lH, Versluis A, Fernandes-Neto AJ, Soares CJ. The effect of post, core, crown type, and ferrule presence on the biomechanical behavior of endodontically treated bo-vine anterior teeth. J Prosthet Dent 2010;104:306-317.
19. Dietschi D, Scampa u, Campanile G, Holz J. Marginal ad-aptation and seal of direct and indirect Class II composite resin res- torations: an in vitro evaluation. Quintes- sen-ceInt1995;26:127-138.
20. Furness A, Tadros MY, looney SW, Rueggeberg FA. Effect of bulk/incremental fill on internal gap formation of bulk-fill composites. J Dent. 2014;42(4):439-449.
REFERENCA
thyerje të pafavorshme. Megjithatë, nuk u vunë re ndryshime të rëndësishme në llojin e frakturës ndërmjet dhëmbëve të restauruar. Për më tepër, të gjitha frakturat e dhëmbëve të restauruar ishin fraktura kohezive, pavarësisht nga lloji i restaurimit. Moduli i ulët i elasticitetit mund të shpjegojë llojin e frakturës së pafavorshme të paraqitur në grupet e dhëmbëve të restauruar. Këto rezultate janë në përputhje me studime të mëparshme që kanë gjetur një rritje të frekuencës dhe gravitetit të frakturës kuspale për shkak të largimit të dentinës cervikale (47).
Kufizimet e këtij studimi duhet të njihen. Metodat eksperimentale të përdorura për studimet in vitro nuk pasqyrojnë me saktësi kushtet intraorale, në të cilat frakturat ndodhin kryesisht për shkak të lodhjes (fatigue). Studimet e ardhshme në këtë fushë duhet të përdorin ngarkimin ciklik dhe simulime të tjera lodhëse (fatigue) për të riprodhuar më saktë mjedisin klinik. Studime të tjera klinike janë të nevojshme për të përcaktuar prognozën afatgjatë të molarëve maksilarë dhe mandibularë të trajtuar endodontikisht të restauruar me rezina kompozite bulkfill.
Konkluzione
Brenda kufizimeve të këtij studimi in vitro, molarët maksilarë e mandibularë të trajtuar endodontikisht të restauruar me rezina kompozite bulkfill (SDR e SonicFill) paraqitën një rezistencë ndaj frakturës nën simulimin e forcës kompresive statistikisht jo të ndryshme nga ajo e restaurimeve tradicionale me rezinë kompozite. Dhëmbët e restauruar nuk treguan ulje të konsiderueshme në rezistencën e frakturës në krahasim me kampionët intaktë. Për më tepër, nuk u gjetën ndryshime në llojin e frakturës ndërmjet dhëmbëve të restauruar, ndërsa dhëmbët e paprekur paraqitën fraktura statistikisht më të favorshme.
Rëndësia klinike
Kompozitet bulkfill mund të përdoren për të restauruar dhëmbët posteriorë të trajtuar endodontikisht duke përdorur inkremente 4-5 mm maksimale, pasi kjo nuk do të zvogëlonte rezistencën mekanike të dhëmbëve të restauruar, duke i bërë procedurat e punës më të lehta, më pak stresuese dhe duke reduktuar kohëne punës në poltron.

Revista Stomatologjike Shqiptare60
21. lindberg A, van Dijken JW, lindberg M. Nine-year evalua-tion of a polyacid-modified resin composite/resin com-posite open sandwich technique in Class II cavities. J Dent. 2007;35(2):124-129.
22. Aguiar FH1, Ajudarte KF, lovadino JR. Effect of light curing modes and filling techniques on microleakage of posterior resin composite restorations. oper Dent. 2002;27(6):557-562.
23. Ruyter IE, oysaed H. Conversion in different depths of ultra-violet and visible light activated composite materials. Acta odontolScand 1982;40:179–192.
24. Ferracane Jl, Mitchem JC, Condon JR, Todd R. Wear and mar-ginal breakdown of composites with various degrees of cure. J Dent Res 1997;76:1508–1516.
25. PoskuslT, Placido E, Cardoso PE. Influence of placement techniques on Vickers and Knoop hardness of class II com-posite resin restorations. Dent Mater 2004;20:726–732.
26. Sideridou ID, Achilias DS. Elution study of unreacted Bis-GMA, TEGDMA, uDMA, and Bis-EMA from light-cured den-tal resins and resin composites using HPlC. J Biomed Mater Res B ApplBiomater2005;74:617–626.
27. Musanje l, Darvell BW. Curing-light attenuation in filled-resin restorative materials. Dental Materials 2006;22:804–817.
28. Ferracane Jl, Greener EH. The effect of resin formulation on the degree of conversion and mechanical properties of dental restorative resin. Journal of Biomedical Materials Re-search1986;20:121–131.
29. Quixfil Scientific Compendium. Dentsply DeTrey; 2003.
30. Surefil SDR flow Directions For use. Dentsply Caulk; 2009.
31. Venus Bulk Fill Product Profile. Heraeus Kulzer; 2011.
32. TetricEvoCeram Bulk Fill Press Release. IvoclarVivadent; 2011.
33. Ilie N, HickelR. Investigations on a methacrylate-based flowable composite based on the SDR technology. Dental Materials 2011;27:348–355.
34. Carrilho MR, Tay FR, Pashley DH, Tjäderhane l, Carvalho RM. Mechanical stability of resin-dentin bond components. Dent Mater. 2005;21(3):232-241.
35. Schneider SW. A comparison of canal preparations in straight and curved root canals. oral Surg oral Med oral Pathol 1971; 32:271-275.
36. Clark D, Khademi J (2010a) Modern molar endodontic ac-cess and directed dentin conservation. Dental clinics of North America 54:249-73. doi: 10.1016/j.cden.2010.01.001 20
37. Plotino G, Buono l, Grande NM, lamorgese V, Somma F. Fracture resistance of endodontically treated molars re-stored with extensive composite resin restorations. J Pros-thet Dent. 2008;99(3):225-232.
38. Asundi A, Kishen A. Digital photoelastic investigations on the tooth-bone interface. J Biomed opt 2001;6:224-230.
39. Sedgley CM, Messer HH. Are endodontically treated teeth more brittle? J Endod. 1992;18:332-335.
40. Korasli D, Ziraman F, ozyurt P, Cehreli SB. Microleakage of self-etch primer/adhesives in endodontically treated teeth. J Am Dent Assoc 2007;138(5):634-640.
41. Galvan RR Jr, West lA, liewehr FR, Pashley DH. Coronal mi-croleakage of five materials used to create an intracoronal seal in endodontically treated teeth. J Endod 2002;28(2):59- 61.
42. Gencoglu N, Pekiner FN, Gumru B, Helvacioglu D. Periapical status and quality of root fillings and coronal restorations in an adult Turkish subpopulation. Eur J Dent 2010;4(1):17-22.
43. Fathi B, Bahcall J, Maki JS. An in vitro comparison of bacterial leakage of three common restorative materials used as an intracoronal barrier. J Endod 2007; 33(7):872-874.
44. Carvalho RM1, Pereira JC, Yoshiyama M, Pashley DH. A re-view of polymerization contraction: the influence of stress development versus stress relief. oper Dent. 1996;21(1):17-24.
45. Braga RR, Ballester RY, Ferracane Jl. Factors involved in the development of polymerization shrinkage stress in resin-composites: a systematic review. Dent Mater 2005;21:962–970.
46. leprince JG, Palin WM, Vanacker J, Sabbagh J, Devaux J, leloup G. Physico-mechanical characteristics of commercially available bulk-fill composites. J Dent. 2014;42(8):993-1000.
47. Hansen EK, Asmussen E. Cusp fracture of endodontically treated posterior teeth restored with amalgam: teeth re-stored in Denmark before 1975 versus after 1979. Acta odontolScand1993;51:73-77.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 61
AbstractAim: To determine and compare the fracture resistance of endodontically treated teeth restored with different resin composites. Materials and Methods: After endodontic treatment and adhesive procedures, 40 maxillary and 40 mandibulary molarswere assigned into4subgroups for each tooth type (n=10): Group A: control group(intact teeth); Group B: access cavities were restored with a traditional resin composite (EsthetX; Dentsply-Italy, Rome, Italy); Group C: access cavities were restored with a bulkfill flowable composite (SDR; Dentsply-Italy), except 1.5 mm layer of the occlusal surface that was restored with the same resin composite as Group B;Group D: access cavities were restored with a bulkfill composite(SonicFill; Kerr-California, uSA).The specimens were subjected to compressive force in a material static-testing machine until fracture occurred, the maximum fracture load of the specimens was measured (N) and the type of fracturewas recorded as favorable or unfavorable. The data were statistically analyzed with one-way analysis of variance (ANoVA) and Bonferroni tests (P<0.05). Results: No statistically significant differences were found among groups of intact teeth when compared with all endodontically treated teeth groups (P<0.05). Also, no statistically significant differences were found in the fracture resistance between the two groups restored with bulkfill composites, SDR and SonicFill.Conclusions: Fracture resistance of endodontically treated molars restored with traditional resin composite restorations andbulkfill composite restorations was similar in maxillary and mandibular molars and did not show any reduction on the fracture resistance when compared to intact teeth.
almira isufi1,2 gianluca plotino1, Nicola maria grande3, pietro ioppolo4, luca testarelli1 , Rossella Bedini4, gianluca gambarini1
Fracture resistance of endodontically treated teeth with conservative access cavities restored with different composite materials
1Departmentof Endodontics, Sapienza University of Rome, Rome, Italy2Faculty of Medical Dentistry, University of Medicine of Tirana, Albania3Catholic University of Sacred Heart, Rome, Italy4Italian National Institute of Health, Technology and Health Department, Rome, Italy
key woRDS:
Fracture
resistance,
endodontic
treatment,
bulkfil
composite,
resine
composite
Introduction
The functional and esthetic rehabilitation of endodontically treated teeth has been the subject of different studies (1).The restoration should not only provide function, esthetic and marginal sealing, but also protect the remaining tooth structure (2, 3). Different studies have shown that the preparation of endodontic access cavities reduces the strength of the teeth, because of deep and extended cavity preparations which critically reduce the amount of dentin (4-8) and increase cuspal deflection during function (9). The importance of conserving the bulk of dentin was demonstrated in maintaining the structural integrity and in the prognosis of endodontically restored teeth (10-13), as the fracture resistance and stress distribution of endodontically treated teeth is directly affected by the amount of residual coronal dentin (4, 14-18).
In posterior preparations, especially when the cervical margin is located in dentin, the polymerization shrinkage effects can be significant, producing marginal defects and gaps despite careful application (19). Several techniques and a variety of restorative materials, which would minimize
the stresses generated on the interface of the restoration by modifying some physical and mechanical properties have been proposed to reduce the effects of polymerization shrinkage (20-22). Furthermore, inadequate polymerization throughout the restoration may compromise its physical properties and increase elution of monomer(23-26) and may lead to undesirable effects, such as gap formation, marginal leakage, recurrent caries. It may also, negatively affect pulp tissue and may lead to premature failure of the restoration (27, 28).
Several manufacturers have recently developed and introduced new types of resin composites, so-called “bulkfill” materials, which can be applied to the cavity and light cured to a maximal increment thickness of 4 mm (29-32) with enhanced curing, shrinkage and physical properties (33). Bulk fill flowable resin composites are used in association with conventional composites for esthetic restorations in posterior teeth, having lower polymerization stress, better flow with easy placement, an excellent adaptation to the cavity walls and low modulus of elasticity, which can reduce the stress generated on the cavity walls (34).

Revista Stomatologjike Shqiptare62
The purpose of this in vitro study was to compare the fracture resistance of endodontically treated upper and lower molars restored with direct traditional and bulkfill resin composite restorations. The null hypothesis tested was that there was a difference in the fracture resistance and the type of failure between endodontically treated maxillary and mandibular molars restored with traditional and bulkfill resin composite.
Materials and methods
Eighty intact recently extracted human maxillary and mandibular molars with completely formed apices were used in this in vitro study. The exclusion criteria for tested teeth were the presence of caries, previous restoration and visible fracture lines or cracks. After a debridement with hand scaling instruments and cleansing with rubber cup and pomice, the teeth were storedin individually numbered containers with 0.1% thymol solution at 4° C until used. Forty maxillary first molars with three separate roots and 30 mandibular first molars with two separate roots were selected based on similar anatomical crown height, measured from the occlusal surface to the cementoenamel junction on the four sides of the teeth, and bucco-lingual (Bl), mesio-distal (MD) dimensions at the occlusal surface. Tooth measurements were taken with a digital caliper.Preliminary radiographs were taken in two perpendicular directions (MD and Bl) to determine root canal anatomy and measure the length and degree of canal curvature using the Schneider method (35). Specimens were subsequently assigned to 4 groups (n=10) for each tooth type creating homogenous groups considering the average of teeth dimensions in order to minimize the influence of size and shape variations on the results: • Group A, the negative control group, which included
10 maxillary and 10 mandibular molars thatwere left intact for fracture testing, without any cavity preparation or root canal treatment;
• Group B, which included 10 maxillary and 10 mandibular molars, which were subjected to endodontic access cavity and endodontic procedures and were restored with a resin composite (EsthetX; Dentsply-Italy, Rome, Italy);
• Group C, which included 10 maxillary and 10 mandibular molars, which were subjected to endodontic access cavity and endodontic procedures and were restored with a bulk fill flowable composite (SDR; Dentsply-Italy), except 1.5 mm layer of the occlusal surface that was restored with the same resin composite as Group B;
• Group D, which included 10 maxillary and 10 mandibular molars, which were subjected to endodontic access cavity and endodontic procedures and were restored with a bulkfill composite (SonicFill; Kerr-California, uSA)with 5mm increments.
All access cavities were prepared according to the
conservative principles described by Clarck and Khademi (36). The access cavity was prepared using water-cooled round-ended cylindrical diamond burs and non-endcutting diamond burs mounted on a high-speed hand piece with different diameters. Root canals were negotiated with size 10 K-type files (Flexofile; Dentsply Maillefer, Ballaigues, Switzerland) to the major apical foramen and canals instrumented to length with NiTi rotary instruments (Mtwo; Sweden & Martina, Padova, Italy) up to the #25 tip size and 0.06 taper file. During the endodontic treatment 5.25% sodium hypochlorite (Niclor 5, ogna, Muggiò Milan, Italy) for irrigation was intermittently deposited using Pro Rinse side-vented 30-G needles (Dentsply Tulsa Dental Specialties, Tulsa, oK). The canals were dried with paper points and filled with gutta-percha (single-cone #25/0.06 taper) and a resin-based endodontic sealer (AH-Plus, Dentsply Maillefer, Ballaigues, Switzerland). After the cleaning, shaping and filling procedures, the teeth were subjected to post-operative radiographs in the two perpendicular dimensions (MD and Bl) to evaluate the endodontic treatment. Then, the enamel and dentin of the access cavity were etched with 37% phosphoric acid for 30 and 15 seconds respectively, rinsed for 30 seconds with a water/air spray, and gently air-dried to avoid desiccation. A light-polymerizing primer-bond adhesive (XP Bond, Dentsply International, York, uSA) was applied, gently air-thinned and exposed to lED polymerization for 40 seconds. In group B access cavities were restored with direct resin composite (EsthetX; Dentsply-Italy, Rome, Italy) with material increments of maximum 2 mm. The specimens in group C were restored with a bulk fill flowable composite with maximal increment thickness of 4 mm (SDR; Dentsply-Italy), except for 1.5 mm layer of the occlusal surface that was restored with the same resin composite as Group B (Fig. 1).
Fig.1. Etching enamel and dentineof the cavity with phosphoric acid 37% (A), applying primer-bond
(B),applyingcomposite bulkfill flowable SDR in 4mm layers (C), final restoration of occlusal surface (D)

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 63
The specimens in group D were restored with a bulkfill composite with maximal increment thickness of 5 mm.
All the specimens were marked 2 mm below the cemento-enamel junction and were covered with approximately 0.25 mm-thick wax. The specimens were embedded in autopolymerizing acrylic resin (SR Ivolen; IvoclarVivadent, Schaan, lichtenstein) in metallic cylindrical molds in position with their long axis parallel to that of the cylindrical molds. To simulate the periodontal ligament, at the first signs of the beginning of polymerization, the teeth were removed from the resin blocks and the wax was cleaned from the root surfaces. A standardized silicone layer was created using a light-body silicone-based impression material (Aquasilultra light bodies, Dentsply International, York, uSA) which was injected into the polymerizing resin bases. The teeth with now wax-free root surfaces were inserted into the resin bases immediately after the silicone injection (37). All the specimens were stored in buffered salineplus1.5% thymol at room temperature (24-28° C) until the fracture testing procedure.
All of the 60 specimens were mounted in a universal load testing machine (lR30K; lloyd Instruments ltd, Fareham, uK). The teeth were loaded at their central fossa at a 30° angle to the long axis of the tooth (Fig. 2).
extending below the level of bone simulation (site of fracture below the acrylic resin). The data were verified with the Kolmogorov-Smirnov test for the normality of the distribution and the levene test for the homogeneity of variances. Thus, they were statistically evaluated by the analysis of variance test and Student-Newman-Keuls test for multiple comparisons (Prism 5.0; GraphPad Software, Inc, la Jolla, CA) with the significance level established at 5% (P <.05).
Results
The mean of the bucco-lingual (Bl) and mesio-distal (MD) dimensions at the occlusal surface and the anatomical crown height of the teeth tested are presented in Table 1. No significant difference was found comparing all teeth dimensions in control and test groups (P >.05). Mesatarja e dimensioneve bucco-linguale (Bl) dhe mesio-distale (MD) në sipërfaqen okluzale dhe lartësisë anatomike të kurorëssë dhëmbëve tëtestuar janë paraqitur në Tabelën 1. Asnjë dallim irëndësishëmnuk u gjet nëkrahasimine të gjitha dimensioneve të dhëmbëve në grupete kontrollit dhe të testuar (P> 05).
No statistically significant differences were found among groups (P<0.05). Fracture resistance of endodontically treated teeth restored with a traditional resin composite and with bulkfill composites(SDR e SonicFill) was similar in both maxillary (Group B: 1185 ± 482N, Group C: 1268 ± 354N, Group D:1308 ± 418N) and mandibular molars(Group B: 1416 ± 307N, Group C: 1535 ± 432N, Group D: 1613± 372N). Restored teeth showed no significant decrease in fracture resistance compared to intact specimens similar in both maxillary (Group A: 1234 ± 315N) and mandibular molars (Group A: 1684 ± 232N) (Tab. 2).
61,25% of the failures in total were unfavorable (Group B 70%, Group C 75%, Group D75%, control group, 25%). No significant differences were found in the mode of failure of the differently restored teeth, while intact teeth presented significantly more favorable fractures compared to restored specimens.
Discussion
The null hypothesis investigated in the present study can be rejected, as the results obtained support that there is no difference in the fracture resistance and in the mode of failure between endodontically treated maxillary and mandibular molars restored with a bulkfill resin composite (SDR and SonicFill) or a traditional resin composite.
Fracture susceptibility of root-filled teeth is affected mostly by the amount of the remaining dentin (4, 38) and it is not related to its biomechanical properties after endodontic treatment, such as hardness and toughness (39). Some studies have shown that the reduction of tooth structure results in weaker teeth due to restorative
30°
150°
Fig.2. Occlusal load simulation by a stainless steel sphere with 6mm diameter positioned in the central fossa and
with lingual orientation and a 30° with the main axis of a mandibular molar.
The continuous compressive force at a crosshead speed of 1.6 mm/s was applied with a 6 mm diameter ball-ended steel compressive head until visible or audible evidence of fracture was shown. The force at fracture was measured in Newton (N) and type of fracture was recorded as “favorable” because restorable, when the failures were above the level of bone simulation (site of fracture above the acrylic resin) and as “unfavorable” because non-restorable, when the failures were

Revista Stomatologjike Shqiptare64
procedures (6-8). However, according to Reeh et al. (4), endodontic procedures have only a small effect on the tooth, reducing the relative rigidity by 5%, which is contributed entirely by the access opening. Restorative procedures and, particularly, the loss of marginal ridge integrity, were the greatest contributors to loss of tooth resistance. The loss of 1 marginal ridge resulted in a 46% loss in tooth rigidity, and a MoD preparation resulted in an average loss of 63% in relative cuspal rigidity.
Several studies were conducted to determine the ideal materials and techniques to restore endodontically treated teeth because their long-term prognosis depends on the quality of the final restoration (40-43). usually, to restore endodontically treated teeth several resin increments are required to fill the cavity preparation because of the large volume of the restoration. Thus, the clinician must compensate the polymerization shrinkage of traditional resin-based composite, by filling the cavities in several increments (44). A new category of resin-based composites has been introduced as bulkfill base material that can be applied in 4mm thick bulks instead of using the incremental placement technique, without negatively affecting the polymerization shrinkage, cavity
adaptation or the degree of conversion (30-32). The results of our study show that there were no
significant differences in the static fracture resistance of endodontically treated molars restored with bulkfill resin composites (SDR and SonicFill) and a traditional resin composite. Moreover, the mean fracture load for teeth restored with SDR and SonicFillwas higher compared with the mean fracture load of specimens restored with traditional resin composites, without any statistical significance. Furthermore, the results of this study showed that there was no significant difference between teeth restored with bulkfill resin composite (Surefil SDRand SonicFill) and intact teeth. These findings may be attributed to the elastic buffer effect of using low viscosity composites and the characteristic low contraction stress and low modulus of elasticity (45, 46).
In the present study 75% of the samples in the intact control teeth presented favorable fracture type that was an important statistical difference with the restored groups. In fact, the majority of the teeth restored with SDR (75%), SonicFill (75%) and with a traditional resin composite (70%) reported unfavorable type of fracture. However, no significant differences were found in the
Tabela 1. Average mean value and standard deviation of mesial- distal dimensions and bucal lingual dimensions, vertical dimension of anatomical crown of each teeth
GROuP CONTROLBuLKFILL FLOwABLE
COMPOSITE (SDR)
BuLKFILL COMPOSITE
(SONICFILL)
TRADITIONAL
COMPOSITE RESIN
Type of tooth
(n=10)
occlusal surface Vertical
dimension of
anatomical
crown
occlusal surfaceVertical
dimension
of
anatomical
crown
occlusal
surface
Vertical
dimension
of
anatomical
crown
occlusal
surface
Vertical
dimension
of
anatomical
crown
MD Bl MD Bl MD Bl MD Bl
Maxillary
Molar 9.9 a (0.6)
10.1 a
(0.9)5.4 (0.4)b
10.0 a
(0.5)
10.1 a
(1.0)5.5 (0.6)b
10.0 a
(0.5)
10.1 a
(0.9)5.6 (0.6)b
9.9 a
(0.5)
10.1 a
(0.8)5.3 (0.4)b
Mandibular
Molar
10.6 a
(1.1)
10.1 a
(0.8)5.7 (0.6)b
10.5 a
(0.9)
10.2 a
(0.7)5.5 (0.4)b
10.7 a
(1.2)
10.2 a
(0.8)5.6 (0.5)b
10.5a
(1.1)
10.1 a
(0.7)5.6 (0.6)b
Shkronja e njëjtë në të njëjtin rresht tregon se nuk ka diferenca statistikisht të rëndësishme (P >.05).
Tabela 2. Fracture strength (average mean ± standard deviation) and type of fracture, Favorable (F) or not Favorable (P) for intact teeth (control, Group A),and restored teeth with traditional resin composite (Group B), bulkfill flowable composite SDR
(Group C), or bulkfill composite SonicFill (Group D), rated after the static test by using Instron universal Machine
TyPE OF
TOOTH
(N=10)
FRAKTuRE STRENGTH (P)TyPE OF FRACTuRE
Group A Group B Group C Group D
Group A Group B Group C Group D F P F P F P F P
Maxillary
Molar 1234 (315)a 1185 (482)a 1268 (354)a 1308 (418)a 8a 2b 3b 7a 3b 7a 3b 7a
Mandibular
Molar1684 (232)a 1416 (307)a 1535 (432)a 1613 (372)a 7a 3b 3b 7a 2b 8a 2b 8a
Shkronja e njëjtë në të njëjtin rresht tregon se nuk ka diferenca statistikisht të rëndësishme (P >.05).
Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 65
1. Meyenberg K. The ideal restoration of endodontically treat-ed teeth - structural and esthetic considerations: a review of the literature and clinical guidelines for the restorative clinician. Eur J Esthet Dent. 2013;8(2):238-268.
2. Steele A, Johnson BR. In vitro fracture strength of endodon-tically treated premolars. J Endod1999;25:6-8.
3. Krejci I, Duc o, Dietschi D, de Campos E. Marginal adapta-tion, retention and fracture resistance of adhesive com-posite restorations on devital teeth with and without posts. oper Dent 2003;28:127-135.
4. Reeh ES, Messer HH, Douglas WH. Reduction in tooth stiff-ness as a result of endodontic and restorative procedures. J Endod1989;15:512-516.
5. owen CP (1986) Factors influencing the retention and re-sistance of preparations for cast intracoronal restorations. J Prosthet Dent 55(6) 674-677.
6. Fokkinga WA, Kreulen CM, Vallittu PK, Creugers NH. A struc-tured analysis of in vitro failure loads and failure modes of fiber, metal, and ceramic post-and-core systems. Int J Prosthodont2004;17:476–482.
7. Panitvisai P, Messer HH. Cuspal deflection in molars in re-lation to endodontic and restorative procedures. J Endod 1995;21(2):57-61.
8. Mondelli J, Steagall l, Ishikiriama A, de lima Navarro MF, Soares FB. Fracture strength of human teeth with cavity preparations. J Prosthet Dent 1980;43:419-422.
9. Tang W, Wu Y, Smales RJ. Identifying and reducing risks for potential fractures in endodontically treated teeth. J En-dod2010;36:609-617.
10. Ree M, Schwartz RS. The endo-restorative interface: Current concepts. Dent Clin North Am. 2010;54:345-374.
11. Huang TJ, Shilder H, Nathason D. Effects of moisture con-tent and endodontic treatment on some mechanical prop-erties of human dentin. J Endo 1992;18:209-215.
13. Tzimpoulas NE, Alisafis MG, Tzanetakis GN, Kontakiotis EG. A prospective study of the extraction and retention inci-dence of endodontically treated teeth with uncertain prog-nosis after endodontic referral. J Endod. 2012;38:1326-1329.
14. Ichim I, Kuzmanovic DV, love RM. A finite element analysis of ferrule design on restoration resistance and distribution of stress within a root. IntEndod J 2006;39:443-452.
15. libman WJ, Nicholls JI. load fatigue of teeth restored with cast posts and cores and complete crowns. Int J Prostho-dont 1995;8: 155-161.
16. Akkayan B. An in vitro study evaluating the effect of fer-rule length on fracture resistance of endodontically treated teeth restored with fiber-reinforced and Zirconia dowel sys-tems. J Prosthet Dent 2004;92:155-162.
17. Kishen A, Kumar GV, Chen NN. Stress-strain response in hu-man dentine: rethinking fracture predilection in postcore restored teeth. Dent Traumatol 2004;20:90-100.
18. Da Silva NR, Raposo lH, Versluis A, Fernandes-Neto AJ, Soares CJ. The effect of post, core, crown type, and ferrule presence on the biomechanical behavior of endodontically treated bovine anterior teeth. J Prosthet Dent 2010;104:306-317.
19. Dietschi D, Scampa u, Campanile G, Holz J. Marginal ad-aptation and seal of direct and indirect Class II composite resin res- torations: an in vitro evaluation. Quintes- sen-ceInt1995;26:127-138.
20. Furness A, Tadros MY, looney SW, Rueggeberg FA. Effect of bulk/incremental fill on internal gap formation of bulk-fill composites. J Dent. 2014;42(4):439-449.
21. lindberg A, van Dijken JW, lindberg M. Nine-year evalu-ation of a polyacid-modified resin composite/resin com-posite open sandwich technique in Class II cavities. J Dent. 2007;35(2):124-129.
REFERENCES
mode of failure between restored teeth. Furthermore, all failures of the restored teeth were cohesive fractures, regardless of the type of restoration. The low elastic modulus may explain the severity of fracture type presented in restored teeth groups and the occurrence of unfavorable fracture. These findings are in agreement with previous reports that found an increased frequency and severity of cuspal fracture due to removal of cervical dentin (47).
The limitations of this study must be recognized. The experimental methods used for in vitro analyses do not accurately reflect intraoral conditions, in which failures occur primarily due to fatigue. Future research in this area should use cyclic loading and other fatiguing simulation to more accurately reproduce the clinical environment. Additional clinical studies are necessary to determine the long-term prognosis of endodontically treated maxillary and mandibular molars restored with bulkfill resin composites.
Conclusions
Within the limitations of this in vitro study, endodontically treated upper and lower molars restored with bulkfill resin composites (SDR and SonicFill) presented a resistance to fracture under simulated compressive force not significantly different than that of traditional resin composite restorations. Restored teeth showed no significant decrease in fracture resistance compared to intact specimens. Furthermore, no differences were found in the mode of failure of the differently restored teeth, while intact teeth presented statistically more favorable fractures.
Clinical relevance
Bulkfill composites can be used to restore endodontically treated posterior teeth using 4-5 mm maximum increments because this does not reduce the mechanical resistance of the restored teeth, while making the procedure easier, less stressful and with a reduced chair side time.

Revista Stomatologjike Shqiptare66
22. Aguiar FH1, Ajudarte KF, lovadino JR. Effect of light curing modes and filling techniques on microleakage of posterior resin composite restorations. oper Dent. 2002;27(6):557-562.
23. Ruyter IE, oysaed H. Conversion in different depths of ultra-violet and visible light activated composite materials. Acta odontolScand 1982;40:179–192.
24. Ferracane Jl, Mitchem JC, Condon JR, Todd R. Wear and marginal breakdown of composites with various degrees of cure. J Dent Res 1997;76:1508–1516.
25. PoskuslT, Placido E, Cardoso PE. Influence of placement techniques on Vickers and Knoop hardness of class II com-posite resin restorations. Dent Mater 2004;20:726–732.
26. Sideridou ID, Achilias DS. Elution study of unreacted Bis-GMA, TEGDMA, uDMA, and Bis-EMA from light-cured den-tal resins and resin composites using HPlC. J Biomed Mater Res B ApplBiomater2005;74:617–626.
27. Musanje l, Darvell BW. Curing-light attenuation in filled-resin restorative materials. Dental Materials 2006;22:804–817.
28. Ferracane Jl, Greener EH. The effect of resin formulation on the degree of conversion and mechanical properties of dental restorative resin. Journal of Biomedical Materials Research1986;20:121–131.
29. Quixfil Scientific Compendium. Dentsply DeTrey; 2003.
30. Surefil SDR flow Directions For use. Dentsply Caulk; 2009.
31. Venus Bulk Fill Product Profile. Heraeus Kulzer; 2011.
32. TetricEvoCeram Bulk Fill Press Release. IvoclarVivadent; 2011.
33. Ilie N, HickelR. Investigations on a methacrylate-based flowable composite based on the SDR technology. Dental Materials 2011;27:348–355.
34. Carrilho MR, Tay FR, Pashley DH, Tjäderhane l, Carvalho RM. Mechanical stability of resin-dentin bond components. Dent Mater. 2005;21(3):232-241.
35. Schneider SW. A comparison of canal preparations in straight and curved root canals. oral Surg oral Med oral Pathol 1971; 32:271-275.
36. Clark D, Khademi J (2010a) Modern molar endodontic ac-cess and directed dentin conservation. Dental clinics of North America 54:249-73. doi: 10.1016/j.cden.2010.01.001 20
37. Plotino G, Buono l, Grande NM, lamorgese V, Somma F. Fracture resistance of endodontically treated molars re-stored with extensive composite resin restorations. J Pros-thet Dent. 2008;99(3):225-232.
38. Asundi A, Kishen A. Digital photoelastic investigations on the tooth-bone interface. J Biomed opt 2001;6:224-230.
39. Sedgley CM, Messer HH. Are endodontically treated teeth more brittle? J Endod. 1992;18:332-335.
40. Korasli D, Ziraman F, ozyurt P, Cehreli SB. Microleakage of self-etch primer/adhesives in endodontically treated teeth. J Am Dent Assoc 2007;138(5):634-640.
41. Galvan RR Jr, West lA, liewehr FR, Pashley DH. Coronal mi-croleakage of five materials used to create an intracoronal seal in endodontically treated teeth. J Endod 2002;28(2):59- 61.
42. Gencoglu N, Pekiner FN, Gumru B, Helvacioglu D. Periapical status and quality of root fillings and coronal restorations in an adult Turkish subpopulation. Eur J Dent 2010;4(1):17-22.
43. Fathi B, Bahcall J, Maki JS. An in vitro comparison of bacterial leakage of three common restorative materials used as an intracoronal barrier. J Endod 2007; 33(7):872-874.
44. Carvalho RM1, Pereira JC, Yoshiyama M, Pashley DH. A re-view of polymerization contraction: the influence of stress development versus stress relief. oper Dent. 1996;21(1):17-24.
45. Braga RR, Ballester RY, Ferracane Jl. Factors involved in the development of polymerization shrinkage stress in resin-composites: a systematic review. Dent Mater 2005;21:962–970.
46. leprince JG, Palin WM, Vanacker J, Sabbagh J, Devaux J, le-loup G. Physico-mechanical characteristics of commercially available bulk-fill composites. J Dent. 2014;42(8):993-1000.
47. Hansen EK, Asmussen E. Cusp fracture of endodontically treated posterior teeth restored with amalgam: teeth re-stored in Denmark before 1975 versus after 1979. Acta odontolScand1993;51:73-77.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 67
tissue support and implant retentionoverdenture in mandible: a simply, smart and predictable treatment.a case report.
keywoRDS:
overdenture, Dental Implants, Dental Prosthesis, low profile attachments.
IntroductionEdentulism can lead to significant functional
impairment as well as unfavorable aesthetic and psychological changes in patients. Problems include restrictions in diet, speech impairment, loss of soft tissues support and decreased vertical dimension. The conventional method for treating edentulism is to provide complete dentures. However, progressive and irreversible loss of basal bone may lead to incrementally increasing difficulties for the denture patient, especially in relation to the mandible, creating problems like loss of retention and stability, hyperplasia and ulceration of the underlying mucosa, soreness and pain, and impaired psychosocial functioning. Removable designs of implant-supported prostheses offers a better retention and improves oral function and patient satisfaction, compared with conventional complete dentures. Rehabilitative treatments based on dental implants can improve the retention and stability of complete dentures in edentulous patients. In this way, two dental implants with two attachments create a tissue support and implant retention overdenture, the new “state of art” in edentulous mandible.
The edentulism is related with several phenomena such as bone remodelling and soft tissues inflammation. The smoking habits can be a disadvantageous factor in edentulous patients as well as all the stress related conditions. The total upper and lower edentulism represents a clinical challenge for every dentist; it must be properly approached, taking in mind the aesthetic requests of patients and their economic availability. The quality of life of edentulous patients subjected to implantology can be improved with the right prosthetic treatment; nowadays, the good treatment is both fixed and removable, depending from clinical and economic reasons. Scientific literature demonstrated that patients
Roberto Scrascia, DDS1, luigi Secondo, Dt1Master Class in Bone Regenerative and Oral Surgery, Master Class in Fixed and removable Prostheses
wearing a removable upper denture can quickly tolerate their new rehabilitative solution, mainly because it typically shows a good stability and makes patients feeling good; conversely, poor stability and masticatory problems are often reported in the lower removable prostheses, because of the complex anatomy of such site that favors a condition of instability. The overdenture mandibular prostheses on implants allow you to get many clinical benefits, such as good aesthetic, correct phonetic and speech, good prosthesis stability and correct masticatory movements. The implant surgery is commonly performed in “safe” areas, such as the symphysis of the jaw, included into the two mental foramens; in such zone, the bone remodeling usually preserves enough amount of bone tissue, allowing to surgeons the correct positioning of 2 to 4 implants. The overdenture (oVD) is an excellent dental prosthesis and its use is growing in the last years. The implant survival rate (ISR) ranges from 92% to 100%, regardless of the type of attachment used or the age of the patients. The surgical protocol to be preferred is the one-stage technique, especially in elderly patients or in patients affected from systemic diseases. The bone healing outcomes are similar to those reported after the two-stage technique, however, the one-stage technique needs only one surgery time, thus reducing the patients stress and allowing an overall costs and time reduction. The modern implant-supported overdentures have been classified into two sub-categories: 1) implant-retained tissue-supported overdenture, retained by different abutment or bar designs, and 2) overdenture implant supported and implant retained, fully supported by implants. The following article aims to show how a minimally invasive work can significantly improve the quality of life of our patients.

Albanian Stomatological Journal68
Case ReportWe treated a 65yo patient reporting a teeth loss due
to a severe periodontitis. She was totally edentulous for a long time and the radiological examinations revealed a strong resorption of the bony crest. our patients showed the typical facial morphology commonly characterizing the edentulous patients: we found that the lips vermilion was almost completely unseen and nasolabial folds were deeper than other folds in different facial zones. Such a dramatic loss of vertical dimension was depending from the resorption of bony crest.After a shared brainstorming with the patient, where we discussed about the clinical case and the therapeutic options, we decided to proceed with a full denture in maxilla and removable prosthesis rehabilitation in mandible, thus stabilizing the lower prosthesis with two interforaminal dental implants. Patient need prosthetic flanges to give scaffold to soft tissue of the face but she need more stability to her lower denture. Implant surgery was performed with one-stage surgery, with a simultaneous screwing of the healing abutments, in order to shorten the treatment duration. The lower denture was customized in order to fit with the implants position: we used a direct technique, properly perfectioned by using F.I.T.T. (Functional Impression Tissue Toner) gel to get a lower trauma to soft tissues. When we choose to use this technique, it is preferable to check our patient within 48 hours after the application of F.I.T.T., in order to soften any roughnedges created by the progressive hardening of this material. According to the international
guidelines, the sutures were removed after 7 to 10 days from the surgery: it’s important to plan a follow-up every 2 weeks with the aim to modify the prosthesis, so to ensure an optimal healing of gingival tissues after the surgery. An import event must to be underline, the hygienic aspect of the treatment. our patient lose all her teeth because she isn’t the best cleaner ever, and in this way we need to have a prosthetic treatment that is so simply to clean. With two low profile attachments the cleaning steps are so simply to do. 3 months after the implant-surgery we are quite sure that the bone healing process is completed: we are thus ready to load dental implants with two low-profile attachments; in our case-report, we used oT Equator (Rhein83, Bologna, Italy) to stabilize the lower denture with a size measuring 2mm in the 4.3 position and 1mm in the 3.3 position. The steps were the following ones: first panoramic impression, then precision impression with personalized spoon and through the use of the transfers of the Equator. This is an important and raccomanded step, because through an functionalized impression we can build the denture but through the transfers we have the possibility to have the three dimension position of the implant and in this way we can build the metal reinforcement of the denture to give more strength to the final work. All the steps of the classical denture were used to go to the final work but we use the direct technique to load the Equator. With the precision impression we have the possibility to load the Equator in the indirect way, to put the retention caps and steel housing at the laboratory but we prefer to build the metal reinforcement e to leave a free space under the denture to fill in the direct way in the mouth of the patient because in this way we can have the possibility to handle the resilience of the soft tissue of the oral cavity. 2 weeks after the positioning of the prosthesis, we performed an accurate follow-up to evaluate the aesthetic and function of the prosthetic rehabilitation. At the time of loading of the low profile attachments we have been used the yellow (extra-soft) elastic matrices, the less retentive of the system. one mouth after prosthesis delivery yellow retentive caps were replaced with other type. We have various retentive powers. from yellow, which corresponds to 600g until the purple that releases 2.7 kg. In the middle we are pink 1.2 kg and white 1.8 kg. Clinical experience shows that not always the most retentive matrix is the best. We must proceed
Pic.1 Tipical facial edentulous in female patient. Pic.1a Rx OPT at the beginning.
Pic.2 we need scaffold of soft tissue of the lower third of the face.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 69
step by step to assess the situation that works best, in equilibrium between mucous support and implant retention. We recorded an excellent patient’s satisfaction about her new denture, in fact, the good aesthetic and the restored chewing function led great benefit from a clinical and psychological point of view. Instructions were given to the patients, recall visits were scheduled for occlusal adjustments and oral hygiene quality control every 6 months, and for retentive caps replacement every one year. Prostheses were built carefully about occlusal schemes, the rule that was followed sees driving the occlusion from the prosthesis “weaker”. For example in a mouth with lower overdentures and dentures in the maxilla, guide the occlusal scheme of the total prosthesis. overjet was left purposely broad, from 2 mm to 5 mm in order to avoid interferences during the function. To load the Equator directly in the mouth the steps are the following ones: separator disks on the attachments to take away undercuts stell housing over the attachments acrylic resin under the denture.A successful prosthetic treatment is measured in the follow-up: compared to complex structures such as the implant bars, when we
plan an overdenture supported by implants and mucosa, it is crucial to check whether the internal prosthesis profile is congruent with the profile of the edentulous ridge. In our case, follow-ups have been performed up to 4 years, showing an overdenture prosthesis stable and clinically performing. The bone around the implants remained quite stable, without signs of resorption, and the mucosal tissues around the implants remained in excellent health. In this clinical case we had used oT Equator attachment. It is stable retention, resilient and self-aligning attachment system. oT Equator attachments allow to angle compensation up to 30 degrees that may be helpful in severe atrophic patients with different degree of mandibular atrophy and lingual concavities that may compromise the ability to place axial implants with bone reconstruction. The 30 degrees are guaranteed with the standard steel cages, with the new metallic cages called SmartBox, thanks to a patented internal system, we can compensate for up to 50 degrees the dental implants.The findings of this study support the established evidence base for an improvement in edentulous patients’ satisfaction with their prostheses
Pic.4 Picture of the maxilla.
Pic.6 Parallelized mirror to put implant parallel.
Pic.5 A resorbed mandible. More retention for the denture.
Pic.7 Split crest of a small bone in intraforaminal space.
Pic.7a Rx OPT with pin of parallelism. Pic.8 Osstem TSIII in action.

Albanian Stomatological Journal70
when two implants are used to retain their mandibular complete denture, even in severe atrophic patients. Two implants in the lower jaw, to retain a full denture is the new standard of treatment for edentulous, in a historical moment where the average age of patients has increased, and also increased their demands, it is
important to have in our hands a streamlined treatment, safe and predictable. Treatment that can greatly improve performance of quality in life of patients, above all in those patients where there is a strong bone atrophy and thus the classic denture may not be sufficient to ensure function and aesthetics, so a good quality of life.
Pic.9 Healing abutment after 2 months. Pic.9a OT Equator.
Pic.10 OT Equator mounted in oral cavity.
Pic.11 Model study and personalized trays.
DiscussionPatients’ life is rapidly increasing in expectations and
duration; their requirements related to a prosthetic treatment are clear and peremptory: they need to have a fast, safe, practical, valuable treatment and, more than everything all, they require aesthetics at low cost. The literature analysis reports that a mandibular overdenture supported by 2 or more implants has a
high implant and prosthetic success rate, moreover, the one-stage surgery and the modern materials allow to achieve good aesthetics in a short-time treatment; all such characteristics make the overdenture a highly valuable prosthetic treatment. The positive feedback of the patient reported in our case is paradigmatic of the great versatility of overdenture, without renouncing to comfort and aesthetics, at cheap costs comparing
Pic.12 OT Equator tranfers.
Pic.14 Occlusion trays. Pic.13 Master models.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 71
to other kinds of prostheses. The change in aesthetics and function leads towards a complete amelioration of the overall quality of life of patients rehabilitated with a dental prosthesis. We strongly think that patient demands and needs are the principal reading key of our treatment, and everything must be built around such requests. For example, in this clinical case, only two dental implants and a very good upper full denture have been charged on the treatment plan, offering to patient a low-expensive treatment with a high rate of success and an amazing increasing in the quality of life.A spontaneous question could be: why, thus, we propose a prosthetic treatment supported by more than 2 dental implants? This is a question that would require a deep and complex discussion, and the reply is a sum of anatomic, functional and aesthetic factors. In this reported case, if we had opted for upper and lower fixed prostheses, we would have ensured function, of course, but not the aesthetics and the predictability of the long-time outcomes. In fact, a fixed prosthesis needs specific requirements related to the maintenance of a proper hygiene, consequently, the perioral tissues would not have the right support. only the prosthesis with flanges can ensure the correct scaffold of soft tissue, and in this way on full denture and overdenture have this propriety, This last aspect is particularly important in the upper prostheses, because
of their need to concretely support the upper lips. In our clinical case here reported we had choice full denture in upper jaw for economic reasons. The lower jaw would have been rehabilitated by a fixed prosthesis or not less than four implants, but it would not have been the best treatment for our patient, because she required an aesthetically guided work and a rehabilitative solution easy to clean. Single attachments are instead the gold standard in our reported case, because they allow an easy hygiene without complex cleaning maneuvers.
ConclusionsIn our case report, the “take-home-message” is that
the mandibular implant-supported overdentures can be a reliable and predictable prosthetic choice, in such edentulous patients with low economic budget and high aesthetic expectations. The treatment must be carefully planned and shared with patients and dental technicians. our main goal is to provide an adequate support to the perioral soft tissues, in fact, the loss of hard and soft tissues in edentulous patients can be severe.
Conflict of interestAuthors disclose no conflicts of interest and no
financial interest.
Pic.15 Phonetics tests.
Pic.17 Facial arch.
Pic.16 Camper plane.
Pic.18 Laboratory step of maxilla prosthetic space.

Albanian Stomatological Journal72
Pic.19 Aesthetics tray in.
Pic. 21 Full teeth set up.
Pic. 23 Prosthetics space and bone resorption.
Pic. 20 Aesthetics tray in mouth.
Pic. 22 Occlusion.
Pic. 24 Occlusal view.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 73
Pic. 25 Occlusion tests.
Pic. 26 Mandible prosthetics with free space for direct loading of the low profile attachments.
Pic. 29 SatisfyPic. 28 OT Equator after polishing.
Pic. 25a Aestethics full denture and overdenture
Pic. 27 Acrylic resin to load the attachments.

Albanian Stomatological Journal74
REFERENCES1. Zitzmann Nu, Marinello CP, Sendi P. A cost-effective-
ness analysis of implant overdentures. J Dent Res. 2006 Aug;85(8):717-21.
2. Marrelli M, Gentile S, Palmieri F, Paduano F, Tatullo M. Cor-relation between Surgeon’s experience, surgery complex-ity and the alteration of stress related physiological param-eters. PloS one. 2014 Nov 7;9(11):e112444.
3. Albrektsson, T., Blomberg, S., Branemark, A. & Carlsson, G.E. (1987) Edentulousness–an oral handicap. Patient reactions to treatment with jawbone-anchored prostheses. Journal of oral Rehabilitation 14: 503–511.
4. Allen, P.F. (2005) Association between diet, social resources and oral health related quality of life in edentulous patients. Journal of oral Rehabilitation 32: 623–628.
5. Ellis JS, Burawi G, Walls A, Thomason JM. Patient satisfac-tion with two designs of implant supported removable overdentures; ball attachment and magnets. Clinical oral Implants Research 2009;20:1293–8.
6. Harris D, Hofer S, o’Boyle CA, Sheridan S, Marley J, Bening-ton IC, et al. A comparison of implant-retained mandibular overdentures and conventional dentures on quality of life in edentulous patients: a randomized, prospective, within-subject controlled clinical trial. Clinical oral Implants Re-search 2011;24:96–103.
7. Chiapasco M, Abati S, Romeo E, Vogel G. Implant-retained mandibular overdentures with Brånemark System MKII implants: a prospective comparative study between de-layed and immediate loading. Int J oral Maxillofac Implants 2001;16:537-546.
8. Romeo E, Chiapasco M, lazza A, Casentini P, Ghisolfi M, Iorio M, et al. Implant-retained mandibular overdentures with ITI implants. Clin oral Implants Res 2002;13:495-501.
9. Turkyilmaz I, Tumer C. Early versus late loading of unsplint-ed Tiunite surface implants supporting mandibular over-dentures: a 2-year report from a prospective study. J oral Rehabil 2007;34:773-780.
10. Hyland R, Ellis J, Thomason M, El-Feky A, Moynihan P. A qual-itative study on patient perspectives of how conventional and implant-supported dentures affect eating. J Dent 2009;37:718–23.
11. Thomason JM, Kelly SAM, Bendkowski A, Ellis JS. Two im-plant retained overdentures--a review of the literature sup-porting the McGill and York consensus statements. J Dent 2012;40:22–34.
12. Pozzi A, Tallarico M, Moy PK. Four-implant overdenture fully supported by a CAD-CAM titanium bar: A single cohort prospective 1-year preliminary study. The Journal of Pros-thetic Dentistry 2016;116:516–23.
13. Weinländer M, Piehslinger E, Krennmair G. Removable im-plant-prosthodontic rehabilitation of the edentulous man-dible: five-year results of different prosthetic anchorage concepts. Int J oral Maxillofac Implants 2010;25:589–97.
14. Cawood JI, Howell RA. A classification of edentulous jaws. Int J oral Max- illofac Surg 1998;17:232-6.
15. Elm von E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, STRoBE Initiative. Strengthening the Re-porting of observational Studies in Epidemiology (STRoBE) statement: guidelines for reporting observational studies. BMJ 2007;335:806-8.
16. Tallarico M, Vaccarella A, Marzi GC. Clinical and radiological outcomes of 1- versus 2-stage implant placement: 1-year results of a randomised clinical trial. Eur J oral Implantol 2011;4:13–20.
17. Tallarico M, Meloni SM. open-cohort prospective study on early implant failure and physiological marginal remodel-ing expected using sandblasted and acid-etched bone lev-el implants featuring an 11° Morse taper connection within one year after loading. J oral Science Rehabilitation. 2017 Mar;3(1):68–79.
18. Elsyad MA, Khairallah AS, Shawky AF. Changes in the eden-tulous maxilla with ball and telescopic attachments of implant-retained mandibular overdentures: A 4-year retro-spective study. Quintessence Int 2013;44:487–495.
19. Geertman ME, Boerrigter EM, Van Waas MA, van oort RP. J Prosthet Dent. 1996 Feb;75(2):194-204. Roberto Branchi.
20. Berglundh T, Persson l, Klinge B. A systematic review of the incidence of biological and technical complications in im-plant dentistry reported in prospective longitudinal studies of at least 5 years. J Clin Periodontol. 2002; 29: 197-212.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 75
INNOVATIVE DESIGN AND FUNCTIONALITY ON YOUR IMPLANTThe Smallest Dimensional Titanium Abutment in the Market
STAINLESS STEEL HOUSING2,1mm HEIGHT - 4,4mm DIAMETER
RETENTIVE NYLONCAPSHOCK ABSORBING FUNCTIONALITY
TIN COATED TITANIUM1600 VICKERS HARDNESS
C. Borromeo
RETENTIVE CAPS LINEELASTICITY AND MECHANICAL RETENTION TO ENSURE A SUPERIOR FUNCTIONALITY FOR THE PROSTHESIS
THE OT EQUATOR ATTACHMENTS ARE AVAILA-BLE FOR THE MAJOR IMPLANT BRANDS.UPON REQUEST WE CAN CUSTOMIZE THEM FOR ANY KIND OF IMPLANTS. WHEN ORDERING, PLEASE ALWAYS INDICATE: IMPLANT BRAND, IMPLANT DIAMETER AND CUFF HEIGHT. CUFF AVAILABLE UP TO 7mm.
COMPATIBLE TO ALLIMPLANT PLATFORMS
STAINLESS STEELHOUSING
STRONGRETENTION
STANDARDRETENTION
SOFTRETENTION
EXTRA SOFTRETENTION
TITANIUMHOUSING
PROCESSING
METAL TO METAL ROTATIONAL CORE
TITANIUM ANODIZED HOUSING
TITANIUM LINER
ELASTIC CAP
CORRECT DIVERGENCY UP TO 50°
THE SELF-ALIGNINGOT EQUATOR HOUSING
DORINA MELE Co. Sh. p.k.Rruga “ Prokop Myzeqari” N.8
1000 TIRANA- ALBANIA00355 4 2259425
Ot Equator+Smartbox_A4_ENG_Luglio_2017.indd 1 10/10/2017 11:27:01

Albanian Stomatological Journal76
AbstraktProblemi kryesor i protezave të plota mbetet qëndrueshmëria e tyre, veçanërisht në nofullën e poshtme. Janë përdorur metoda të ndryshme për të rritur qëndrueshmërinë e tyre, një nga këto metoda është dhe masa terciare apo regjistrimi i zonës neutrale.Qëllimi. Ndikimi i teknikës së regjistrimit të zonës neutrale nëpërmjet masës terciare në rritjen e qëndrueshmërisë dhe retensionit në protezat e lëvizshme totale.Materiali dhe metoda. Në Klinikën Stomatologjike universitare, Tiranë, u përzgjodhën 17 pacientë; 10 meshkuj dhe 7 femra. Si kriter kryesor për përzgjedhjen shërbeu shkalla mesatare dhe e avancuar e rezorbimit të proçesit alveolar si dhe problemet me protezat ekzistuese. Për secilin pacient u realizuan 2 proteza: të parat u realizuan me metodën tradicionale, të dytat me teknikën e zonës neutrale dhe masës terciare. Të dy protezat u aplikuan nga një muaj në secilin pacient. Pacientët plotësuan një formular rreth qëndrueshmërisë dhe retensionit të dy llojeve të protezave.Rezultatet. Pas përpunimit statistikor të të dhënave të pyetësorëve, rezultuan vlera më të larta të qëndrueshmërisë dhe retensionit në protezat me regjistrim të zonës neutrale, në krahasim me protezat tradicionale.Konkluzioni. Në konstruktimin e protezave të lëvizshme, sidomos në rastet me proçese alveolare shumë të rezorbuara, regjistrimi i zonës neutrale nëpërmjet masës terciare jep rezultate mjaft të mira. Përdorimi i kësaj metode rezulton në përshtatje më të mirë , retension dhe qëndrueshmëri më të madhe të protezave totale.
1 Neada hysenaj, 2 edit Xhajanka, 2 merita Bardhoshi, 2 koço gjilo
teknika e zonës neutrale dhe masa terciare
1Klinika Stomatologjike Universitare, Tiranë2Fakulteti i Mjekësisë Dentare, Tiranë
Fjalët kyçe:
proteza të
lëvizshme,
qëndrueshmëri,
retensioni, zona
neutrale.
Hyrje Rezorbimi i kockës alveolare është pasojë e mungesës
së dhëmbëve për një kohë të gjatë.1 Ky problem është më i theksuar në moshat e treta 2, si rrjedhojë lëvizshmëria e protezave të poshtme është një problem madhor. Një nga metodat e zgjidhjes së këtij problemi është riformimi i sipërfaqeve mbështetëse të protezave të poshtme, në mënyrë që të regjistrohen impresionet e muskujt rrethues.3
Kjo metodë u përshkrua për herë të parë nga Wilfred Fish.4 Sipas tij, proteza përmban 3 sipërfaqe, ku secila prej tyre luan një rol të pavarur në qëndrueshmërinë dhe retensionin e protezave. Wilfred Fish e përshkroi regjistrimin e zonës neutrale si një zgjidhje tjetër të mundshme për protezimin në nofullat me proçese alveolare të rezorbuara.5 Zona neutrale përshkruhet si hapësira ndërmjet faqeve dhe buzëve nga njëra anë dhe gjuhës nga ana tjetër, zonë ku forcat ekuilibrojnë njëra tjetrën.6 Dhëmbët artificialë duhet të rreshtohen në këtë zonë, në mënyrë që forcat të jenë të balancuara.7 Zona neutrale mbështetet në parimin që çdo forcë ka një kundër-forcë në drejtim të kundërt, por të barabartë në vlerë.8 Protezat, si pjesë e kavitetit oral, duhet të jenë në harmoni me funksionin neuro-muskular normal.9 Muskujt rrethues nuk duhet të zhvendosin protezat nga pozicioni i tyre dhe forcat e ushtruara nga gjuha duhet të balancohen me forcat e ushtruara nga buzët dhe faqet.10 Është e rëndësishme që të regjistrohet saktë zona neutrale, në mënyrë që të rivendosim të gjjtha funksionet normale si: të folurën, mastikacionin, përtypjen, të qeshurit; si dhe të rrisim maksimalisht qëndrueshmërinë dhe retensionin e protezave, sidomos në rastet ku proçeset alveolare janë shumë të rezorbuar.11
Materiali dhe Metoda Pas një ekzaminimi të hollësishëm, u përjashtuan
nga përzgjedhja pacientët me çrregullime temporo-mandibulare, kserostomi, çrregullime të motorrikës oro-faciale, hiposalivacion, pacientët me patologji ekstra dhe intra-orale, pacientë me manifestime orale të sëmundjeve të ndryshme sistemike, si dhe pacientë me probleme psikologjike apo psikiatrike.
Fig.1, a,b – Ekzaminimi intraoral dhe përzgjedhja sipas gradës së dytë dhe të tretë të atrofisë

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 77
Nga pacientët e paraqitur në Klinikën Stomatologjike universitare u përzgjodhën 17 pacientë; 10 meshkuj dhe 7 femra. Mosha mesatare ishte rreth 70 vjeç. Ato u trajtuan me proteza totale të lëvizshme. Kriter për përzgjedhjen e pacientëve ishte rezorbimi i proçeseve alveolare në shkallë të mesme dhe të avancuar. (Fig.1, a,b)
Për të përcaktuar shkallën e rezorbimit kockor u përdor grafia panoramike (Fig. 2). Pacientët, të cilët ishin të protezuar më parë, paraqitën si ankesë kryesore lëvizshmërinë dhe qëndrueshmërinë e ulët të protezave ekzistuese.
Fig. 2- Ekzaminimi shtesë nëpërmjet grafisë panoramike
Pas parapërgatitjes së gojës, u mor masa anatomike dhe u formuan dy lugët individuale përkatëse për secilin nga modelet (Fig.3 a,b).
Fig.3, a,b - Modeli anatomik dhe luga individuale
Fig.4, a,b- Përgatitja e protezave totale tradicionale
Për protezat tradicionale puna vazhdoi si në vijim: Masa funksionale u mor me pastë oksid zink eugenoli, pasi u realizua bordazhi i lugëve me teknikën seksionale. u përcaktua okluzioni qëndror sipas metodës tradicionale. u realizua prova me dhëmbë, muflimi dhe polimerizimi i protezave. (Fig.4, a,b )

Revista Stomatologjike Shqiptare78
Në protezat provë, pra të konstruktuara nëpërmjet regjistrimit të zonës neutrale, u proçedua në këtë mënyrë: Në bazën e shabllonit u vendos një spirale, ( Fig.5, a ) , mbi të cilën vendosëm vinil siloksan (heavy body). (Fig.5,b). Zona neutrale u regjistrua nga impresionet që la muskulatura përreth nga lëvizjet funksionale të buzëve, faqeve dhe gjuhës. laboranti realizoi rreshtimin e dhëmbëve duke u bazuar në zonën neutrale të regjistruar.
Në provën me dhëmbë u kontrollua okluzioni qëndror, estetika dhe fonetika e pacientit. Në protezat provë u hoq dyll nga sipërfaqja labiale, bukale dhe linguale duke krijuar hapësirën e nevojshme për materialin e masës. Dhëmbët u lyen me vazelinë, që mos të ngjitnin me materialin e masës. Si material mase përdorëm pastën e oksid zink eugenolit. Fillimisht materiali u aplikua në pjesën labiale dhe bukale, ku pacientët u instruktuan të realizojnë lëvizjet funksionale, sipas të cilave lanë impresione faqet dhe buza e poshtme. E njëjta proçedurë u ndoq për pjesën linguale, ku gjuha la impresionet e saj gjatë gëlltitjes. Pas eliminimit të pjesës së tepërt të materialit, proteza e poshtme ishte e gatshme për muflim.
Fig.5, a, b, c, d- Regjistrimi i zonës neutrale
fillimisht me silikon A (polivinilsiloksan) dhe më pas me pastë oksid zink eugenoli.
Muflimi u realizua sipas metodës tradicionale. Protezat u përpunuan dhe u lustruan. Pacientëve ia aplikuan protezat e zakonshme për një muaj, duke mos i informuar cilat nga protezat u aplikuan. Pacientët u instruktuan për mirëmbajtjen e protezave. Pas 1 muaji u aplikuan tek pacientët protezat provë, të cilat u përdorën gjatë një muaji në vazhdim. (Fig. 6). Pacientët plotësuan një formular ku ju përgjigjën pyetjeve rreth qëndrueshmërisë dhe retensionit të protezave të të dy llojeve. Përgjigjet varionin nga 0-3, ku 0 tregonte përgjigje maksimale pozitive, 3 përgjigje maksimale negative. Të dhënat u vlerësuan nga një klinicist. Gjithashtu, u regjistruan vizitat për retushe dhe ankesat e pacientëve.
Fig. 6- Proteza e konstruktuar sipas teknikës së regjistrimit të zonës neutrale
Rezultatet. Në shumë raste protezat e lëvizshme mbeten një mundësi e rëndësishme trajtimi. Për të dy llojet e protezave u krahasuan të dhënat e pyetësorëve dhe u realizua përpunimi statistikor i tyre. Sipas të dhënave, qëndrueshmëria dhe retensioni i protezave provë rezultuan në vlera më të larta (76,4 %), krahasuar me protezat tradicionale (47%). Gjithashtu , numri i vizitave dhe retushet për korigjim të protezave ishte më i madh në rastin e protezave tradicionale (64,7 %) krahasuar me protezat me regjistrim të zonës neutrale ( 35,2 %).
DiskutimMungesa e qëndrueshmërisë dhe retensionit të
protezave të poshtme është një problem madhor, sidomos në pacientët me kockë alveolare shumë të rezorbuar. Pacientët u ndoqën për 2 vite, ku ishte e qartë zgjedhja e protezave provë. Pacientët shfaqën rehati dhe përshtatshmëri më të shpejtë me protezat provë. Gjithashtu, numri i korigjimeve të protezave tradicionale ishte më i madh. Në ndjekjen e vazhdueshme të pacientëve u vu re një numër më i madh i ngacmimeve mekanike të mukozës, kur pacientët përdorën protezat e zakonshme. Ka studime, sipas të cilave vetëm përdorimi i teknikës së zonës neutrale rrit qëndrueshmërinë dhe retensionin e protezave12, ndërsa studime të tjera mbështesin kombinimin e teknikës së zonës neutrale me impresionet e sipërfaqeve mbështetëse.13
KonkluzionNë konstruktimin e protezave të lëvizshme teknika e
regjistrimit të zonës neutrale rekomandohet të realizohet e kombinuar me masën e sipërfaqeve mbështetëse, sidomos në pacientët me proçese alveolare shumë të rezorbuara. Përdorimi i kësaj metode rezulton në përshtatshmëri, retension dhe qëndrueshmëri më të madhe të protezave, si dhe në reduktim të dekubituseve dhe të ngacmimeve mekanike të mukozës. Kjo teknikë realizohet lehtë dhe jep rezultate më të mira kryesisht në mandibul, ku është problem qëndrueshmëria e protezave totale.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 79
1. Makzoume JE. Morphologic comparison of two NZ impres-sion techniques: a pilot study. J Prosthet Dent.2004;92:563–568. doi: 10.1016/j.prosdent.2004.09.010.
2. Glossary of Prosthodontic terms. (2005) 8th ed. J Prosthet Dent 94:46
3. Gahan MJ, Walmsley AD. The NZ impression revisited. Br Dent J. 2005;198:269–272. doi: 10.1038/sj.bdj.4812118.
4. Beresin VE, Schiesser FJ. The neutral zone in complete den-tures. J Prosthetic Dent. 2006;95:93-101. doi: 10.1016/j.pros-dent.2005.10.005
5. Tinker A. Ageing in the united Kingdom what does this mean for dentistry? Br Dent J 2003; 194: 369-372.
6. Kursoglu P, Ari N, Calikkocaoglu S. using tissue conditioner material in NZ technique. NY State Dent J.2007;73(40):42.
7. Sadighpour l, Geramipanah F, Falahi S, Memarian M. using NZ concept in prosthodontic treatment of a pa-tient with brain surgery: a clinical report. J Prosthodont Res. 2011;55:117–120. doi: 10.1016/j.jpor.2010.03.003.
REFERENCA
8. Kokubo Y, Fukushima S, Sato J, Seto K. Arrangement of ar-tificial teeth in the NZ after surgical reconstruction of the mandible: a clinical report. J Prosthet Dent. 2002;88:125–127. doi: 10.1067/mpr.2002.127951.
9. ohkubo C, Hanatani S, Hosoi T, Mizuno Y. Neutral zone ap-proach for denture fabrication for a partial glossectomy pa-tient: A clinical report. J Prosthet Dent2000; 84: 390-393.
10. Agarwal S, Gangadhar P, Ahmad N, Bhardwaj A. A simpli-fied approach for recording NZ. J Indian Prosthodont Soc. 2010;10:102–104. doi: 10.1007/s13191-010-0019-8.
11. Ikebe K, okuno I, Nokubi T. Effect of adding impression material to mandibular denture space in Piezography. J oral Rehabil. 2006;33:409–415. doi: 10.1111/j.1365-2842.2005.01582.
12. Allen Pf, Wilson Nhf. Teeth for life for older Adults. Quintes-sence;2002.
13. Raja Hz Sm. Relationship of Neutral Zone and Alveolar Ridge with Edentulous Period. J Coll Physicians Surg Pak. 2010;20(6):395-9.

Albanian Stomatological Journal80
AbstractThe purpose of this study: To evaluate neutral zone technique and polished surface impression effect in the stability and retention of total removable dentures.Materials and methods. 17 patients, 10 men and 7 female, were selected in the university Dental Clinic, Tirana. The scale of bone resorbtion was the main criteria of patients selection. For every patient, two kind of dentures were constructed: the first ones were realized in the traditional way, while the others with neutral zone technique and polished surface impression. Each denture was applied for one month, patients fulfilled a questionnaire about the stability and retention of their denture.Results. After the statistical evaluation of the data, the test dentures resulted with higher values of stability and retention, compared to the traditional dentures.Conclusion. The neutral zone technique is recommended to be used with polished surface impression. This combination leads in increased retention, stability and adaptability of removable dentures, especially in resorbed alveolar ridge.
1 Neada hysenaj, 2 edit Xhajanka, 2 merita Bardhoshi, 2 koço gjilo
Neutral zone technique and third impression
1University Dental Clinic, Tirana, Albania 2 Faculty of Dental Medicine, Tirana, Albania
key woRDS:
removable
dentures,
stability,
retention,
neutral zone.
Introduction The resorbtion of alveolar ridge is closely related to
the loss of teeth for a long time. 1 loose dentures are a main problem, especially for elderly people.2 one of the methods for the solution of this problem is reshaping the sorrounding surfaces, so the muscles can leave their impressions.3
First this method was described by Sir Wilfred Fish.4 According to him, prostheses contains three surfaces, where each of them plays an independent role in the stability and retention of prostheses. Sir Wilfred describes neutral zone as another possible solution for resorbed alveolar ridge.5 Neutral zone is described as the space between the tounge in one side and cheeks and lips, on the other side, the zone where forces equalizes each other.6 Artificial teeth should be aligned in this zone, in order that the surrounding forces are compensated.7
Neutral zone is based in the concept that every force has its opponent, in the same value but in the opposite direction.8 Prostheses as part of the oral cavity, should be in full harmony with the normal function of neuro-muscular function.9 Surrounding muscles should not move dentures, and the forces caused by tounge should be compensated by the forces caused by cheek and lips.10
It is important to register correctly the neutral zone in order to have normal functions of speech, mastication, swallowing, laughing; and to increase the retention and stability of dentures, especially in resorbed mandibular ridge.11
Materials and Methods After a careful examination, patients with temporo-
mandibular disorders, xerostomia, disfunction of oro-facial system, hyposalivation, patients with extra and
intra oral pathology, patients with oral manifestations of systemic diseases, psychologic and psychiatric problems were excluded from the study.
Fig.1, a,b Intra-oral examination and the pre-selection according to II and III grade of bone resorbtion
17 patients, 10 men and 7 female were selected from the university Dental Clinic, Tirana, with an average age of 70 years old. They were treated with complete removable dentures. As a main criteria for the selection of patients was the scale of resorbtion of alveolar ridge. (Fig.1, a,b)
Panoramex was used to define the scale of bone resorbtion (Fig. 2). The main complain of the patients who had previously dentures, was the feeling of loose and unstable dentures.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 81
Fig. 2-Complementary examination through panoramex film
First impression was made and two individual trays for each cast were made (Fig.3, a,b ).
Fig.3, a,b –Primary cast and individual tray
Fig.4, a,b-Traditional denture preparation
These were the steps that were followed for the traditional dentures:
Functional impression with zinc oxide eugenol, after border molding. Centric occlusion, try-in stage and flasking procedure were realized according to the traditional manner (Fig.4, a,b).
In test dentures the following steps were realized: in the base a wire spurs was installed (Fig.5,a ), over which vinyl siloxane (heavy body) was positioned. (Fig.5,b). Neutral zone was registered by the impressions made from the surrounding muscles during the functional movements of cheeks, lips and tounge. The dental technician aligned the teeth based on the neutral zone that was registered.

Albanian Stomatological Journal82
1. Makzoume JE. Morphologic comparison of two NZ impres-sion techniques: a pilot study. J Prosthet Dent.2004;92:563–568. doi: 10.1016/j.prosdent.2004.09.010.
2. Glossary of Prosthodontic terms. (2005) 8th ed. J Prosthet Dent 94:46
3. Gahan MJ, Walmsley AD. The NZ impression revisited. Br Dent J. 2005;198:269–272. doi: 10.1038/sj.bdj.4812118.
4. Beresin VE, Schiesser FJ. The neutral zone in complete den-tures. J Prosthetic Dent. 2006;95:93-101. doi: 10.1016/j.pros-dent.2005.10.005
5. Tinker A. Ageing in the united Kingdom what does this mean for dentistry? Br Dent J 2003; 194: 369-372.
6. Kursoglu P, Ari N, Calikkocaoglu S. using tissue conditioner ma-terial in NZ technique. NY State Dent J.2007;73(40):42.
7. Sadighpour l, Geramipanah F, Falahi S, Memarian M. using NZ concept in prosthodontic treatment of a patient with brain surgery: a clinical report. J Prosthodont Res. 2011;55:117–120. doi: 10.1016/j.jpor.2010.03.003.
REFERENCES
8. Kokubo Y, Fukushima S, Sato J, Seto K. Arrangement of artificial teeth in the NZ after surgical reconstruction of the mandible: a clinical report. J Prosthet Dent. 2002;88:125–127. doi: 10.1067/mpr.2002.127951.
9. ohkubo C, Hanatani S, Hosoi T, Mizuno Y. Neutral zone ap-proach for denture fabrication for a partial glossectomy pa-tient: A clinical report. J Prosthet Dent2000; 84: 390-393.
10. Agarwal S, Gangadhar P, Ahmad N, Bhardwaj A. A simpli-fied approach for recording NZ. J Indian Prosthodont Soc. 2010;10:102–104. doi: 10.1007/s13191-010-0019-8.
11. Ikebe K, okuno I, Nokubi T. Effect of adding impression mate-rial to mandibular denture space in Piezography. J oral Reha-bil. 2006;33:409–415. doi: 10.1111/j.1365-2842.2005.01582.
12. Allen Pf, Wilson Nhf. Teeth for life for older Adults. Quintes-sence;2002.
13. Raja Hz Sm. Relationship of Neutral Zone and Alveolar Ridge with Edentulous Period. J Coll Physicians Surg Pak. 2010;20(6):395-9.
In the try-in stage centric occlusion, esthetics and fonetics were controlled. In the try-in stage, wax was removed from the labial, buccal and lingual surface, in order to create the necessary space for the impression material, zinc oxide eugenol. Teeth were covered with Vaseline, in order to be easily separated from the impression material. The material was first applied in buccal and labial surfaces, were patients were instructed to realize the functional movements. The same procedure was followed for the lingual surface, where tounge left its impression during swallowing. After eliminating the excessive material, lower denture was ready for flasking.
Fig.5, a, b, c, d-Neutral zone registration through vinyl
siloxane, then through zinc oxide eugenol
Flasking procedure was realized according to the traditional manner. Dentures were cleaned and polished. The traditional dentures were first applied for 1 month, without informing the patients which denture was applied. Patients were instructed about dentures hygiene. After 1 month, the test dentures were applied. (Fig. 6). Patients answered to a questionnaire about the stability, retention of dentures. Answers ranged from 0-3, where 0 was maximal satisfaction, while 3 negative evaluation. The answers were evaluated from a clinician. Follow up visits and complaints were registered.
Results. In cases of contra-indications of surgical
interventions removable dentures are an important treatment option. The data extracted from the questionnaire were analyzed and compared. According to the statistical evaluation, retension and stability of test dentures showed higher values compared to the traditional dentures. The number of follow-ups for the complaints of patients with test dentures were lower compared to the traditional dentures.
Fig. 6- Test denture constructed through
neutral zone technique registration
Discussionloss of stability and retention are a common
problem, especially for patients with resorbed alveolar ridge. Patients were followed for 2 years, where their choice for test dentures was clear. Patients expressed faster adaptability and comfort with test dentures. The number of denture corrections was higher in traditional dentures, also redness and ulceration was more obvious in traditional dentures. There are studies were the use of neutral zone technique increases the retention and stability of dentures12, while other studies reports the increase effect of neutral zone technique combined with the polished surface impression.13
ConclusionThe neutral zone technique is recommended to be
used with polished surface impression. This combination leads in increased retention, stability and adaptability of removable dentures, especially in resorbed alveolar ridge.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 83
AbstraktKorigjimi i anomalive dentofaciale kërkon një plan trajtimi të saktë si për ortodoncinë dhe kirurgjinë ortognatike.Gjithashtu është e domosdoshme që korigjimi kirurgjikal të bëhet me saktësi për të garantuar rezultatin përfundimtar.Në këtë artikull do të mundohemi të përshkruajmë tekniken e osteotomisë sagitale te ramusit mandibular për zgjidhjen e deformimeve të ndryshme të mandibules si dhe të deformimeve të kombinuara në te dyja nofullat.Në vitin 1970, J M Ferrer ka thënë: “ Duhet të dihet se në cdo operacion kirurgu ne menyrë të pa evitueshme e dëmton pacientin ,ky demtim mund dhe duhet të minimizohet nga një teknike kirurgjikale e sakte , e butë dhe e kujdesshme” Megjithëse anatomia dhe forma e mandibules së njeriut çon vetvetiu në një ndarje në planin sagital , osteotomia kirurgjikale e mandibules vazhdon të mbetet një proçedurë sfiduese.Gjate 30 viteve të fundit ka pasur modifikime të shumta të teknikës kirurgjikale të përshkruar për hërë të parë nga obwegeser dhe Trauner në 1955,zbulimi i instrumentave të rinj dhe përmiresimi i aftësive kirurgjikale kanë bërë të mundur që të arrihen rezultate kirurgjikale të shpejta dhe atraumatike.Qëllimi: Çdo kirurg duhet të aplikojë një teknikë bashkëkohore me të cilën është familjarizuar dhe ka garantuar rezultate për disa vite.
Renato isufi1, algen isufi1, aurora isufi2, Ramazan isufi1
osteotomia Sagitale Bilaterale e Ramusit mandibular
1Departamenti i Kirurgjisë Orale dhe Maksilofaciale, Fakulteti i Mjëksisë Dentare , QSUT “Nënë Tereza”2Isufi Royal Dental(Specializantë në Ortodonci)
Fjalët kyçe:
osteotomi
Sagitale, deformime mandibulare, disekim
Teknika Hapi 1- Infiltrimi i indeve të buta me
vazokonstriktor. Buzët duhet të jenë të lubrifikuara gjatë proçedurës
kirurgjikale. Zona e disekimit infiltrohet me anestetik lokal që përmban vazokonstriktor (1:100 000) 10 minuta përpara kirurgjisë.
Fig1
Hapi 2- Incizioni në indet e buta Incizioni bëhet nëpërmjet mukozës, muskulit dhe
periostit,lingualisht linjës oblike eksterne,në gjysmën e sipërme të ramust mandibular nga lart deri në mesin e molarit të dytë poshtë. Te paktën 5 mm mukoze e pakeratinizuar duhet të lihet në pjesën bukale të poshtme të incizionit për të lehtësuar suturimin.
Fig 2
Fig 3
Hapi 3- Disekimi bukal subperiostalShkëputet periosti nga trupi dhe pjesa anteriore
e ramusit të mandibules për të lejuar një pamje të mjaftueshme. Disekimi duhet të jetë subperiostal, i saktë dhe i pastër. Nuk është e nevojshme të shkëputet i gjithë muskuli maseter nga kendi i mandibules. Shkëputja totale e këtij muskuli do të çoje në hapsirë të vdekur dhe do te stimulojë edemën dhe hematomën.

Revista Stomatologjike Shqiptare84
Fig 4
Fig 5
Hapi 4- Disekmi subperiostal superior Shkëputen fibrat e poshtme të muskulit temporal nga
bordi i përparshem i ramusit. Disekohet periosti nga linja oblike interne duke vazhduar poshtë në pjesen meziale të zonës retromolare. Vendoset një ekartor në formë bishtë dallandysheje mbi bordin anterior dhe tërhiqet lart për një pamje më të mirë.
Fig. 6
Fig 7Hapi 5 – Ekspozimi i Lingulës Fillohet disekimi mezial nga sipër dhe me pas
vazhdohet duke disekuar inferiorisht. Qëndrohet subperiostal gjatë gjithë kohës. Identifikohet me kujdes lingula për të siguruar pamjen. Perforimi i periostit në këtë
zonë mund të shkaktojë shumë hemoragji (zakonisht nga muskuli pterygoid mezial);gjithësesi ajo ndalon në mënyre spontane.
Fig 8
Fig9
Hapi 6 – Osteotomia meziale e ramusit Mund të përdoret një frezë linderman ose një frezë
fissure 701, shenjohet e ngritura e lingulës dhe mbahet osteotomia paralel me planin e okluzionit. Konveksiteti i linjës oblike interne mund të fshehi lingulën. Nëse pamja është e veshtirë, kreshta duhet të reduktohet me një frezë të madhe rond. Fillohet osteotomia direkt mbi lingulë në fose.
Fig 10 Fig 11
Fig12

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 85
Hapi 7- Osteotomia sagitalePërdoret piezo, sharra ose nje freze fissure 701,fillohet
sipër në osteotomine meziale-horzontale dhe qendrohet brenda korteksit bukal te trupit dhe te ramusit mandibular. Sigurohemi qe osteotomia eshte bere perms korteksit(afersisht 5 mm ). Prezenca e nje molari te trete mund mund te ndikoje (molaret e trete duhet te hiqen minimalisht 9 muaj perpara kirurgjise,ose gjate nderhyrjes.
Fig 13
Fig 14
Fig 15
Hapi 8-Osteotomia bukale e trupit te mandibules. Hiqet ekartori ne formen e bishtit te dallandyshes
dhe vendoset ekatrori obëegeser në bordin e poshtëm të trupit të mandibules. Fillohet osteotomia bukale në bordin e poshtëm dhe bashkohet sipër me osteotomine sagitale. Sigurohemi që korteksi i bordit të poshtëm është i përfshirë në osteotomi. Fillimi i ndarjes duhet
të jetë në bordin e poshtëm dhe të perfshijë korteksin lingual. Pritet në drejtim të pjesës së vestibulare të mandibules,gjithësesi duhet treguar kujdes që të mos demtohet nervi alveolar inferior.
Fig 16
Fig 17
Hapi 9 – Shpohen vrimat për telat fiksuesePozicionimi i kondilit në fosen glenoide është hapi më
i rëndësishem i kësaj proçedure dhe duhet konsideruar si një hap i veçantë përpara vendosjes së fiksimit rigid. Përdorimi i telave fiskuese është opsional sepse disa kirurgë perdorin klemat kockor për fiksimin e segmenteve te prera.
Hapi 10- LavazhiShplahet zona kirurgjikale me fiziologjik me shumicë
dhe vendoset pak sponge ne te. Kur osetotomia përfundon në njërën anë është e rekomandueshme që të perfundohet dhe osteotomia e anës tjetër përpara se të fillohet me ndarjen e mandibules sepse në këtë mënyrë do evitohet dëmtimi i nervit alveolar inferior gjatë levizshmërisë së fragmenteve të prera.
Fig 18

Revista Stomatologjike Shqiptare86
Fig 20 Fig 21
Fig 23
Fig 22
Fig 24
Hapi 11- Lirimi i OsteotomisePërdoret një osteotom i hollë 10 mm për të goditur
lehtë gjatë linjës së osteotomisë vertikale, nga osteotomia meziale dhe vazhdohet poshtë tek ajo bukale. Është shumë e rëndësishme të mbështetet mandibula kur bëhet ndarja në anën e kundërt për të parandaluar dëmtimin e indeve të forta dhe të buta në anën e ndarë. Fillohet gradualisht lirimi i fragmenteve të prera.
Fig 19
Hapi 12 – Ndarja e mandibules Mandibula duhet të suportohet gjatë gjithë kohës
nga ekartori obëegeser dhe me dorë për të mbrojtur artikulacionin temporomandibular. Vendoset një osteotom i madh 10 mm sipër në osteotomine sagitale dhe një osteotom i vogël Reyneke në osteotominë bukale. Rrotullohen të dy instrumentat me kujdes por të kontrolluar. Shikohet për tu siguruar nëse tufa neurovaskulare është intakte dhe e ndarë nga segmenti proksimal.
Tani osteotomi i madh zëvendësohet nga osteotom obëegeser dhe osteotomi Reyneke nga një osteotom më i madh në mënyre që të bëhet ndarja e plotë e mandibules.
Hapi 13 – Limohen zonat e kontaktit të segmeneteve
Për të zbutur zonat e kontaktit midis segmenteve përdoret një frezë rond. Duhet treguar kujdes që të mos dëmtohet nervi alveolar inferior.
Fig25
Hapi 14- Mobilizimi i segmeneteve kockore Shtyhet segmenti proksimal me gishtin tregues dhe
terhiqet segmenti distal me kujdes përpara. Mobilizimi i mjaftueshëm do të sigurojë që indet e buta do të lejojnë pozicionimin e segmentit distal. Gjatë kësaj manovre nuk duhet të përdoret forcë dhe duhet të sigurohemi që proçeset artikulare janë në fose. Në disa raste lind nevoja e një osteotomie të murit lingual për të bërë adaptimin më te mirë të segementeve të prera.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 87
Hapi 15- Vendosen dhëmbët në okluzionin e planifikuar
Përdoret splinti i parapëergatitur më pas fiksohen dhëmbët në okluzion.
Fig26
Hapi 16- Fiksimi rigidGjate fiksimit rigid duhet të merren në konsideratë
disa faktorë si: pozicioni i nervit alveolar inferior,rrënja distale e molarit të dytë të poshtëm,trashësia e kockës për të përcaktuar gjatësinë e vidës,të sigurohemi që freza do ti shpojë të dy kortikalet e kockës dhe të vendosen mjaftueshëm vida.
Përdoret një frezë e mprehtë duke e shtyrë me dorë kur shpon vrimat,duhet treguar kujdes me ushtrimin e forcës sepse mund të spostojë segmentet, kondilet apo të ndryshojë okluzionin. Përdoret shumë fiziologjik për ftohje. Zgjidhet nje pllake e përshtatshme për të lejuar vendosjen e të paktën dy vidave në secilën anë të osteotomisë. Mund të përdoren një ose dy pllaka,gjithësesi shumica e kirurgëve përdorin vetëm një pllakë 2. 0 mm. Përshtatet pllaka që të qëndroje mirë në kockë dhe vendoset në menyrë të tillë që të lejojë vendosjen e vidave posterior përpara. Në disa raste lind nevoja e vendosjes së vidave me troakar me rrugë ekstraorale.
Fig27
Fig28
Hapi 17-Hiqet fiksimi intermaksilar dhe kontrollohet okluzioni
Per tu siguruar që kondilet janë në pozicionin e duhur, okluzioni nuk duhet të kontrollohet direkt pas heqjes së fiksimit intermaksilar por duhet pritur disa minuta.
Hapim dhe mbyllim me kujdes gojën dhe lëvizim mandibulën nga njëra anë në tjetren. Mbyllim gojën me kujdes dhe kontrollojmë okluzionin. Në raste të dyshimta për pozicionin e kycit duhet të bëhet grafi kontrolli pas zgjimit të semurit dhe duhet prashikuar rifutja në sallë.
Fig29
Hapi 18 –Vendosen drenat dhe suturimi i plagësPër të evituar hematomat që në disa raste janë
problematike mund të vendosim dren intra apo ekstraoral. Më mirë është të përdoren drena ekstraoral aspirativ. Më pas bëhet suturimi i plages.
Fig30

Revista Stomatologjike Shqiptare88
Hapi 19-Vendosen elastikët intermaksilarElastiket vendosen në mënyrë trekëndore zakonisht
në zonën kanine. Drejtimi i elastikëve duhet të perforcojë levizjet kirurgjikale. Elastikët përdoren 4-6 javë në varësi të osteotomive pas tyre vazhdohen me mjekimin ortodontik.
Fig31
Hapi 20 – Vendosja e kompresave të ftohtaKompresat e ftohta rekomandohen për 24 orëKonkluzione:Aplikimi i kësaj teknike përreth 15 vite në Shërbimin
e Kirugjisë oMF ka zgjidhur kërkesat e mjaft pacientëve me anomali dentomaksilofaciale.
Përveç eksperiencës së kirurgut per garantimin e kësaj teknike kërkohet dhe instrumentariumi përkatës pa nënvlerësuar piezokirurgjine e cila është e pazëvendësueshme për të garantuar mos dëmtimin e paketin neurovascular mandibular.
Për të evituar ndërlikimet të cilat në disa raste janë të paevitueshme përveç njohjes me egzaktësi të hapave të teknikës kërkohet dhe eksperiencë e cila do te arrihet nëpërmjet studimit të shumtë, asistencave të shumta si dhe numrit të rasteve të operuara në mënyrë të pavarur.
1. Isufi R ;Qendro A: Bardhoshi E: “Kirurgjia orale dhe Maksilo-faciale” Vol II,Tiranë, 2010
2. Kademani D;Tiëana P: “Atlas of oral and Maxilofacial Sur-gery” 2015
3. Hunsuck EE. A modified intraoral sagittal splitting tech-nique for the correction of mandibular prognathism. J oral Surg 1968;26:249e50.
4. Epker BN. Modifications in the sagittal split osteotomy of the mandible. J oral Surg 1977;35:157e9.
5. obëegeser H, Trauner R, obëegeser H. Zur operationstech-nik bei der Progenia und anderen unterkieferanomalien. Dtsch Zahn Mund Kieferhlkd 1955;23:11e25.
6. Reyneke JP. Essentials in orthognathic surgery. Chapter 4. 2nd edition. Chicago: Quintessence; 2010. p. 209e18. 5. Reyneke JP. Basic guidelines for the surgical correction of mandib- ular anteroposterior deficiency and excess. Clin Plast Surg 2007;34: 501e17.
7. Reyneke JP. The sagittal split mandibular ramus osteotomy surgical manual. Jacksonville (Fl): Ëalter lorenz Surgical; 1999. 7. Reyneke JP, Ferretti C. Intraoperative diagnosis of condylar sag after bilateral sagittal split ramus osteotomy. Br J oral Maxillofac Surg 2002;40:285e92.
REFERENCA

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 89
AbstractThe correction of dentofacial deformities demands accurate treatment planning for the orthodontic preparation and subsequent surgery. It is also mandatory that the surgical correction be performed accurately to ensure the final outcome. In this article ëe ëill describes the technique for the sagittal split mandibular ramus osteotomy to correct different deformities in mandible or combined deformities in both jaës. In 1970, J M Ferrer said: “it must be recognized that at every operation the surgeon inevitably injures the patient; this injury can and must be minimized by the use of careful, gentle, and accurate surgical technique. ” Although the anatomy and shape of the human mandible lends itself to splitting in a sagittal plane, the surgical osteotomy of the mandible remains a challenging procedure. over the last 30 years, the modificationsto the original technique as described by obëegeser and Trauner in 1955,development of special instruments,and improvement of surgical skills have made it possible to achieve surgical goals relatively quickly and atraumatically. Aim: Each surgeon should apply a contemporary techniquewith ëhich it is familiar and has guaranteed results for several years.
Dr.Renato isufi1; Dr.algen isufi1; Dr.aurora isufi2; prof.Dr.Ramazan isufi1
the Bilateral Sagittal Split mandibular Ramus osteotomy
1Department of Oral and Maxillofacial Surgery, Faculty of Dental Medicine, UHC Mother Theresa 2 Isufi Royal Dental(Orthodontic Resident)
key woRDS:
osteotomy
Sagittale,deformities mandible
Technique
Step 1-Infiltrate the soft tissue with vasoconstrictor
The lips should be kept lubricated throughout the surgical procedure. The area of dissection is infiltrated with a local anesthetic containing a vasoconstrictor ( 1:100,000) 10 minutes before surgery.
Fig1
Step 2-The soft tissue incision An incision is made through the mucosa, muscle,
and periosteum from just lingual to the external oblique ridge, halfway up the mandibular ramus superiorly to mesial of the second molar inferiorly. At least 5 mm of nonkeratinized mucosa should be left buccally at the lower end of the incision for ease of suturing later.
Fig 2
Fig 3
Step 3-Buccal subperiosteal dissection Strip the periosteum from the body and anterior
aspect of the mandibular ramus to allow for adequate visualization. Dissection must remain subperiosteal, decisive,and clean.
It is not necessary to strip the entire masseter muscle attachment off the mandibular angle. Total stripping of the muscle will result in dead space and encourage swelling and hematoma formation.

Revista Stomatologjike Shqiptare90
Fig4
Fig5
Step 4-Superior subperiosteal dissection Strip the lower fibers of the temporalis muscle off the
anterior border of the ramus. Dissect the periosteum from the internal oblique ridge down to the medial aspect of the retromolar area. Place a swallowtail retractor over the anterior border and pull upwards for good visualization.
Fig6
Fig 7
Step 5-Exposure of the lingula Start the medial dissection from above and then
dissect inferiorly. Stay subperiosteal at all times. Carefully identify the lingula and ensure visualization. Perforation of the periosteum in this area may cause brisk hemorrhage (usually from the medial pterygoid muscle); however it often subsides spontaneously.
Fig8
Fig9
Step 6-Medial ramus osteotomy use a lindeman or 701 fissure bur, aim at the notch
of the ligula and angle the osteotomy parallel to the occlusal plane. The convexity of the internal oblique ridge may obscure the lingula. If visualization is difficult, the ridge should be reduced with a large trimming burr. Terminate the osteotomy just above to the lingula into the fossa.
Fig 10 Fig 11

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 91
Fig12
Step 7-Sagittal osteotomy use piezo,a saw or 701-fissure bur; start at the medial
horizontal osteotomy superiorly, and stay just inside the buccal cortex of the mandibular ramus and body.
Ensure the osteotomy is made through the cortex (approximately 5 mm).
The presence of an impacted third molar tooth may interfere (ideally impacted third molars should be removed at least 9 months before surgery or inside surgery.
Fig 13
Fig 14
Fig 15
Step 8 - Buccal osteotomy of the mandibular body
Remove the swallowtail retractor and place a obwegeser retractor at the lower border of the body. Start the buccal osteotomy at the lower border, and join it superiorly with the sagittal osteotomy. Ensure that the cortex of the lower border is included in the osteotomy. The actual start of the split should be at the lower border and include the lingual cortex.
Cut toward the mandible and feel the bur perforate the cortex; however, be careful not to damage the inferior alveolar nerve.
Fig 16
Fig 17
Step 9-Drill holes for a holding wire Positioning the condyle in the glenoid fossa is the
most important step of the procedure and should be performed as a separate step prior to placement if rigid fixation. The use of a holding wire is optional; because some surgeons make use of a bone clamp to hold the segments in position.

Albanian Stomatological Journal92
Step 10-Lavage Wash the surgical area thoroughly with saline
solution and gently place a small sponge in it. once the osteotomy cuts have been completed on one side, it is recommended that the other side to be completed before proceeding to split the mandible because this will avoid damange to inferior alveolar nerv from segments repositioning.
Fig18
Step 11-Define the osteotomy use a 10 mm wide osteotome to tap along the vertical
osteotomy line from the medial osteotomy downward to the buccal osteotomy below. It is important to support the mandible when splitting the contralateral side to
prevent hard and soft tissue damage on the side already split. Start gradually to separate the segments.
Fig 19
Step 12-Splitting the mandible The mandible should be supported at all times by
the obwegeser retractor and digital pressure to protect the temporomandibular joint. Place a large 10 mm osteotome superiorly into the sagittal osteotomy and a small Reyneke splitter into the buccal osteotomy to engage the lower border of the mandible
Rotate the 2 instruments gently but firmly. Visualize and ensure that: The neurovascular bundle is
intact and separates from the proximal segment. The osteotome is now replaced by a larger obwegeser
osteotome and the small Reyneke splitter by the larger splitter; the split can now be completed.
Fig 20 Fig 21
Fig 23
Fig 22
Fig 24

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 93
Step 13-Smooth the contact areas of the segments
use a large round bur to smooth contact areas. Take care not to damage the inferior alveolar nerve.
Fig25
Step 14-Mobilize the bone segments Support the proximal segment with the index finger
and pull the distal segment gently but firmly anteriorly. Adequate mobilization will ensure that the soft tissue drape will allow free positioning of the distal segment. Should not use to much force and must ensure that the condyle are in articular fossa. In some cases is needed an osteotomy to lingual wall to make a good segments adaption.
Step 15-Place the teeth into the planned occlusion
use of a splint is optional and fixate the teeth into occlusion.
Fig 26
Step 16-Rigid fixation During placement of ridged fixation several factors
should be considered: The position of the inferior alveolar neurovascular bundle;The distal root of the lower second molar; Thickness of the bone to estimate the length of the screws;Ensure that the drill perforate both bone cortices;Place enough screws for adequate fixation. use a sharp drill and apply light pressure when drilling the holes. undue pressure may displace the bone segments, the condyle or the occlusion. use copious water cooling. An appropriate plate is selected to allow for at least 2 screws to be placed on each side of the osteotomy. one or 2 plates may be used; however, most surgeons use only one 2. 0 mm plate. Bend the plate to fit accurately to the bone and position the plate to allow for placement of the posterior screws first. In some cases we use the troacar to place the screws extraorally.
Fig 27
Fig 28
Step 17-Remove the intermaxillary fixation and check the occlusion
To ensure that the condyles will settle and have been positioned correctly, the occlusion should not be checked immediately following removal of the intermaxillary fixation. Wait a few minutes. Gently open and close the mouth and translate the mandible from side to side. With light finger pressure, the mouth is closed and the occlusion checked. In suspeciuos cases for condyle position should do a control x-ray and maybe re-entered in operation room.
Fig 29

Albanian Stomatological Journal94
Step 18-Place sutures To avoid hematoms in difficult cases we can use inta
or extraoral drain. Better are aspirative extraorally drains, after make the sutures.
Fig30
Step 19-Place intermaxillary elastics Elastics are placed in a triangular fashion usually in
the canine region. The direction of the elastics should reinforce the surgical movement. Elastics are used for 4-6 weeks after that begin the orthodontic treatment.
Fig31
Step 20-Apply a pressure bandage The pressure bandage are recommended for 24 hours
Conclusions:Application of this technique for 15 years in ower
Service of oral and Maxilofacial Surgery has resolved the demands of many patients with dentomaxilofacial anomalies.
Regardless of the surgeon’s experience, to guarantee this technique, the required instrumentation is needed, without understimation piezo-surgery, which is irreplaceable to ensure that the mandibular neurovascular package is not damaged.
In order to avoid complications which in some cases are inevitable, besides knowing the exactness of the steps of the technique is required and experience which will be achieved through numerous studies, numerous assistance and the number of cases operated independently
1. Isufi R ; Qendro A: Bardhoshi E: “Kirurgjia orale dhe Maksilo-faciale” Vol II, Tiranw, 2010
2. Kademani D; Tiwana P: “Atlas of oral and Maxilofacial Sur-gery” 2015
3. Hunsuck EE. A modified intraoral sagittal splitting tech-nique for the correction of mandibular prognathism. J oral Surg 1968;26:249e50.
4. Epker BN. Modifications in the sagittal split osteotomy of the mandible. J oral Surg 1977;35:157e9.
5. obwegeser H, Trauner R, obwegeser H. Zur operation-stechnik bei der Progenia und anderen unterkieferanoma-lien. Dtsch Zahn Mund Kieferhlkd 1955;23:11e25.
6. Reyneke JP. Essentials in orthognathic surgery. Chapter 4. 2nd edition. Chicago: Quintessence; 2010. p. 209e18. 5. Reyneke JP. Basic guidelines for the surgical correction of mandib- ular anteroposterior deficiency and excess. Clin Plast Surg 2007; 34: 501e17.
7. Reyneke JP. The sagittal split mandibular ramus osteotomy surgical manual. Jacksonville (Fl): Walter lorenz Surgical; 1999. 7. Reyneke JP, Ferretti C. Intraoperative diagnosis of condylar sag after bilateral sagittal split ramus osteotomy. Br J oral Maxillofac Surg 2002;40:285e92.
REFERENCES

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 95
AbstraktBackground: Pacientët me kleft të buzës/ alveolës/ palatumit shpesh kanë probleme me sistemin dentar. Qëllimi i këtij studimi ishte të vlerësonte agenezinë e incizivit lateral në bazë të komplikacionit të kleftës.Metodologjia: Në këtë studim retrospektivë të dhënat u morën për pacientët e lindur midis 5 Prill 1992 dhe 10 Dhjetor 2005 nga Erasmus Medical Center, Rotterdam, the Netherlands dhe Radboud university Medical Center në Nijmegen, the Netherlands. Agenezia e incizivit lateral u vlerësua në bazë të radiografive panoramike dhe kartelës klinike të pacientëve.Rezultati: Sa më e shtrirë ishte klefta në buzë aq më e madhe ishte prevalenca e agenezisë së incizivit lateral. Në mënyrë sinjifikante ishte e lidhur agenezia e incizivit lateral të përhershëm me kleftën komplete të buzës ( oR= 32.6, p< 0.001). lidhje sinjifikante u gjetën midis agenezisë së incizivit lateral dhe me kleftën e shtrirë në gjatësinë1/3-2/3 të buzës (oR=10.4, p= 0.02).Konkluzioni: Për fëmijët me kleft complete të buzës, agenezia e incizivit lateral të përhershëm ishte e pranishme në mënyrë sinjifikante. Ky studim tregon se ku pritet të gjendet më tepër agenezia e incizivit lateral në pacientët me kleft të buzës.
Bisela asllanaj1
agenezia e incizivit lateral të përhershëm në fëmijët josindromik me kleft unilaterale të buzës/alveolës/palatumit
1Departamenti i kirurgjisë oro-maxilo-faciale,Qëndra Spitalore Universitare ‘’Nënë Tereza’’ (QSUT)
Fjalët kyçe:
klefta e buzës,
agenezi,
incizivi lateral,
odontogjeneza
HyrjaAnomalitë dentare janë të shumta në pacientët e lindur
me kleft josindromike unilaterale të buzës/ alveolës/ palatumit në krahasim me popullatën në përgjithësi.[1-4] Incizivi lateral i lokalizuar në zonën e kleftës në vecanti, shfaqet me variacione të shumta anatomike nga normal, medialisht, distalisht, medialisht dhe distalisht deri në mungesë në lidhje me regjionin e kleftës. Dihet se ndërprimi kompleks reciprok epitelial-mezenkimal kontribuon në mënyrë sinjifikante në morfogjenezën, diferencimin dhe pozicionin anatomikë të incizivit lateral.[5] Megjithatë, mekanizmat që janë pas këtij ndërveprimi janë akoma të panjohura plotësisht. Identifikimi i hershëm i prezencës apo mungesës së incizivit lateral është i rëndësishëm për planifikimin e trajtimit të duhur sipas rastit përkatës. Qëllimi i këtij studimi është ti shtojë njohuritë në këtë fushë duke investiguar lidhjen midis shtrirjes së kleftës dhe agenezisë së incizivit lateral të përhershëm në pacientët josindromik me kleft unilaterale të buzës/alveolës/ palatumit. Hipoteza e testuar është nëse rritja e shtrijes së kleftës është e lidhur me mungesën e incizivit lateral.
Materialet dhe MetodatKy studim retrospektivë u ndërmor për të identifikuar
472 pacient me kleft komplete dhe jokomplete të buzës/ premaksilës/ palatumit duke parë kartelat klinike dhe arkivën spitalore. Të gjithë pacientët janë lindur midis 5 Prill 1992 dhe 10 Dhjetor 2005. Në total, 345 pacient i përmbushnin kriteret e përfshirjes:• Pacient me kleft josindromike unilaterale të buzës/
alveolës/ qiellzës• Foto preoperatore• Radiografitë e denticionit të përhershëm
Njëqind e njëzet e shtatë pacient nuk u perfshinë bazuar në kriteret e përjashtimit:• Pacient me kleft bilaterale të buzës/ alveolës/
palatumit• Pacientët sindomik• Mungesa e fotove preoperative• Mungesa e radiografive të denticionit të përhershëm
Për të gjithë pacientët informacionet e mëposhtme u futën nëMS Excel spreadsheet: numri i pacientëve, data e lindjes, gjinia, klinika, morfologjia e kleftës së buzës, morfologjia e kleftës së alveolës, morfologjia e kleftës së qiellzës dhe pozicioni i incizivit lateral.
Fotot preoperatore u përdorën për klasifikimin e morfologjisë së buzës në katër grupe:I) vermillion notch; II) 1/3 - 2/3 kleft e buzës; III) 2/3 - subtotal kleft e buzës; IV) kleft komplete e buzës; dhe defekti alveolar në katër grupe: I) alveolë normale; II) alveoli hipoplastike; III) kleftin komplete e alveoles; IV) kleft komplete e alveolës. Për arsye statistike defekti i alveolës u kategorizua në tre grupe: I) alveoli normale dhe hipoplastike; II) kleft inkomplete alveolare; III) kleft komplete alveolare.
Radiografitë e pacientëve të marra në moshën 6 vjecare dhe më vonë nga Erasmus Medical Center, Rotterdam, the Netherlands dhe Radboud university Medical Center në Nijmegen, the Netherlands u përdorën për të identifikuar pozicionin e incizivit lateral.
Shkronja Z u vendos kur incizivi lateral i përhershëm ishte në pozicionin normal në alveolë. Shkronjat X, Y and XY u vendosën përkatësisht sipas pozicionit të incizivit lateral mezialisht, distalisht dhe njëkohësisht mezialisht dhe distalisht zonës së kleftës. Shkronja AB u vendos kur incizivi lateral mungonte.
Informacioni për palatumin primarë dhe sekondarë u kategorizua në dy grupe: 1) kleft inkomplete

Revista Stomatologjike Shqiptare96
në palatumin primarë dhe 2) kleft komplete në palatumin primarë; dhe për palatumin sekondarë në katër grupe:1) palatum sekondarë normal, 2)
palatum sekondarë submukozal, 3) kleft inkomplete në palatumin sekondarë dhe 4) kleft komplete në palatumin sekondarë.
Analiza StatistikoreSë pari, për cdo karakteristikë të subjekteve ne
krahasuam pozicionet e incizivit lateral duke përdorur testet Chi-square dhe Fisher. Së dyti, ne eksploruam lidhjet e pozicionit të incizivit lateral me secilën karakteristikë të subjekteve duke përdorur modelin e regresionit multinomial. Ne testuam rolin e: 1) kleftës, gjinisë, klinikës; 2) defektit alveolarë; 3) defektit të palatumit. Variablet u përfshinë në model bazuar në lidhjen e tyre në studimet e mëparshme me pozicionin në denticion të përhershëm ose një ndryshimi në vlerësimin e efektit > 10%. Hipoteza u testua në nivelin e sinjifikancës 5%. odds ratio (oR) u llogarit në 95% CI për të matur fuqinë e lidhjes midis pozicionit në denticion të përhershëm dhe cdo variabli.Analizat statistikore u performuan duke përdorur Paketën Statistikore të Shkencës Sociale version 21.0 (SPSS Inc., Chicago, Il, uSA).
RezultatiPrevalenca e pacientëve me vermilion notch dhe me
presence të incizivit lateral të përhershëm medialisht ose distalisht kleftës ishte 25%. Ndërkohë prevalence e pacientëve me shtrirje të kleftës në vermilion notch dhe
me praninë e incizivit lateral medialisht dhe distalisht kleftës ishte 30.8%. Një prevalencë prej 11.7% u gjet e agenezisë së incizivit lateral në pacientët me kleft të buzës në vermilion notch. Në pacientët me kleft të buzës të shtrirë në gjatësinë 1/3-2/3 prevalencën më të madhe e kishte pozicioni medialisht dhe distalisht i incizivit lateral 43.6%. Pozicioni i incizivit lateral të përhershëm medialisht ose distalisht kleftës kishte prevalencë më të madhe dhe në pacientët me shtrirje të kleftës në gjatësinë 2/3 në subtotal. Agenezia e incizivit lateral ishte me prevalencë më të madhe 52.7% në pacientët me kleft komplete të buzës. Subfenotipet e kleftës së buzës u krahasuan duke u bazuar në prevalencë e agenezisë e incizivit lateral për denticionin e përhershëm, në shtrirjen e kleftës në alveolë dhe palatum. Të gjitha grupet e kleftës së buzës dallonin dukshëm nga shtrirja e kleftës. Pacientët me kleft komplete të buzës ishin në mënyrë sinjifikante të lidhur me agenezinë e incizivit lateral të përhershëm ( oR= 32.6, p< 0.001), dhe më pas renditeshin pacientët me kleft 2/3 në subtotal, më pas pacientët kleft 1/3 në 2/3 e buzës, përkatësisht (oR=10.4, p= 0.02; oR= 6.5, p=0.04).
Fig.1. Grafiku i subjekteve të përfshira në studim.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 97
Tabela 1. Karakteristika të pacientëve me kleft unilaterale të buzës/ alveolës/ qiellzës(n (%))
Denticion i përhershëm
Totali X/ Y XY AB Z p-value+
n = 345 n = 113 n = 77 n = 120 n=35
Karakteristikat
Klinika
Rotterdam 158 69 35 54 0
Nijmegen 187 44 42 66 35 <0.001
Gjinia
Mashkull 227 75 50 77 25
Femër 118 38 27 43 10 0.882
Klefta e buzës
Vermillion notch 68 17 21 8 22
Kleft 1/3 - 2/3 55 11 24 7 13
Kleft 2/3 - subtotal 59 23 17 19 0
Kleft komplete e buzës 163 62 15 86 0 <0.001
Defektialveolës
Normal 104 22 38 9 35
Hypoplastik 3 1 1 1 0
Inkomplete 47 16 17 14 0
Komplete 191 74 21 96 0 <0.001
Palatumi primar
Kleft inkomplete 145 34 54 22 35
Kleft komplete 200 79 23 98 0 <0.001
Palatumisekondarë
Normal 266 92 62 78 34
Kleft Submucous 1 1 0 0 0
Kleft inkomplete 9 3 3 2 1
Kleft komplete 69 17 12 40 0 0.001
Klefta në Palatum
Vetëm në primare 266 92 62 78 34
Primare + Sekondare 79 21 15 42 1 <0.001
vlerat pjanë bazuar në testet Chi-squared dhe Fisher
Diskutim Ky studim tregon se gjatësia e shtrirjes së kleftës në
buzë lidhet me pozionet e ndryshme të prezencës së incizivit lateral të përhershëm. Ky informacion mund të përdoret për të planifikuar dhe menaxhuar trajtimin e pacientëve me kleft por edhe për të informuar prindërit e pacientëve.
Studimet tregojnë se prevalenca e mungesës së dhëmbëve në pacientët me kleftë është në mënyrë sinjifikante më e lartë (45-77%;[6]) krahasuar me pacientët pa kleft (3.2- 7.6%; [7]). Studimet gjithashtu kanë treguar që kjo mund të lidhet me proçedurat kirurgjikale specifike të cilave u nënshtrohen pacientët me kleft [8, 9].
Në studimin tonë prevalenca e agenezisë së incizivit lateral ishte 34.7%. Raportohet që agenezia e incizivit lateral në popullatë normale është 2%.[7, 10]
Në këtë studim tregohet se një numër i lartë i pacientëve me agenezi të incizivit lateral gjenden me prezencë të shtrirjes komplete të kleftës. Një shpjegim i këtij rezultati mund të jetë fakti që anomalitë dentare kanë të njëjtët faktor etiolgjik me kategorinë e kleftës së buzës ku ato gjenden. Prandaj faktorët kritikë që ndikojnë në patogenezën e kleftës së buzës kanë ndikim edhe në odontogenezën e incizivit lateral po ashtu. Një shpjegim tjetër mund të jetë fakti që ndyshimet

Revista Stomatologjike Shqiptare98
REFERENCA
1 . Ranta, R., A review of tooth formation in children with cleft lip/palate. American Journal of orthodontics and Dentofa-cial orthopedics. 90(1): p. 11-18.
2. letra, A., et al., Defining Subphenotypes for oral Clefts Based on Dental Development. Journal of Dental Research, 2007. 86(10): p. 986-991.
3. Congenitally Missing Teeth in the Israeli Cleft Population. The Cleft Palate-Craniofacial Journal, 2005. 42(3): p. 314-317.
4. Jordan, R.E., B. Kraus, and C. Neptune, Dental abnormalities associated with cleft lip and/or palate. The Cleft palate jour-nal, 1966. 3: p. 22.
5. Vastardis, H., The genetics of human tooth agenesis: new discoveries for understanding dental anomalies. Ameri-can Journal of orthodontics and Dentofacial orthopedics, 2000. 117(6): p. 650-656.
6. Böhn, A., Dental anomalies in harelip and cleft palate. Acta odontologica Scandinavica, 1963. 21: p. SuPPl38: 1.
7. Polder, B.J., et al., A meta-analysis of the prevalence of den-tal agenesis of permanent teeth. Community dentistry and oral epidemiology, 2004. 32(3): p. 217-226.
8. lekkas, C., et al., The adult unoperated cleft patient: ab-sence of maxillary teeth outside the cleft area. The Cleft palate-craniofacial journal, 2000. 37(1): p. 17-20.
9. da Silva Filho, o.G., A.D.C. Normando, and l. Capelozza Filho, Mandibular growth in patients with cleft lip and/or cleft palate—the influence of cleft type. American Journal of orthodontics and Dentofacial orthopedics, 1993. 104(3): p. 269-275.
10. Stamatiou, J. and A.l. Symons, Agenesis of the permanent lateral incisor: distribution, number and sites. J Clin Pediatr Dent, 1991. 15(4): p. 244-6.
11. van den Boogaard, M.-J.H., et al., MSX1 mutation is associ-ated with orofacial clefting and tooth agenesis in humans. Nature genetics, 2000. 24(4): p. 342.
12. Vieira, A.R., et al., Medical sequencing of candidate genes for nonsyndromic cleft lip and palate. PloS Genet, 2005. 1(6): p. e64.
13. ooé, T., on the early development of human dental lamina. okajimas folia anatomica Japonica, 1957. 30(2-3): p. 197-210_1.
14. Hovorakova, M., et al., one odontogenic Cell-Population Contributes to the Development of the Mouse Incisors and of the oral Vestibule. PloS one, 2016. 11(9): p. e0162523.
që ndodhin në fazat e hershme të zhvillimit çojnë në formimin e një klefte komplete të buzës dhe dëmtojnë dhe embrionogjenezën e dhëmbëve gjithashtu. Kjo mund të shpjegohet dhe me ndikimin e dëmtimeve gjenetike të njëjta që çojnë në fenotipe të njëjta.[11, 12]. Më shumë rëndësi ka shpjegimi me ndikimin e pozicionit të lamina dentare, e cila kontrollon origjinën, formën, pozicionin dhe kohën e erupsionit të incizivit lateral, në pikat e lidhjes midis proçeseve nasal medial dhe maksilarë.[13, 14]
Gjetjet në studimin tonë mund të ndihmojnë në shpjegimin dhe kuptimin e lidhjeve të gjetura në studimet e mëparshme midis prezencës së dhëmbëve në pacientët me kleft. Në bazë të njohurive tona ky studim është i pari që merret me lidhjen midis agenezisë së incizivit lateral dhe kleftës unilaterale të buzës në pacientët jo sindromik. Për më tepër ky studim mund të shpjegoj lidhjen midis fenotipeve dhe hartës gjenetike të pacientëve me kleft të vlerësuar në studimet e fundit kërkimore gjenetike.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 99
AbstractBackground: Patients with cleft lip / alveolus / palate often have dental problems. The purpose of this study was to assess the agenesis of lateral incisor based on the cleft morphology.Methods: In this retrospective study data were taken for patients born between 5 April 1992 and 10 December 2005 from the Erasmus Medical Center, Rotterdam, the Netherlands and Radboud university Medical Center, Nijmegen, the Netherlands. Agenesis of lateral incisor was assessed on the basis of panoramic X-rays and patient records.Results: The more extended the cleft type was associated with a higher prevalence of lateral incisor agenesis. Agenesis of lateral incisor was significantly associated with complete cleft lip (oR = 32.6, p <0.001). This study showed a significantly association between the lateral incisor agenesis and children born with cleft 1/3-2/3 of the lip (oR = 10.4, p = 0.02).Conclusion: Children born with complete cleft lip tended to have agenesis of permanent lateral incisor. This study shows the phenotype of cleft lip where is expected to appear more agenesis of lateral incisor in patients with cleft lip.
Bisela asllanaj1
agenesis of the permanent lateral incisor in nonsyndromic children with unilateral cleft lip/ alveolus / palate
1Departament of Oral and Maxillofacial Surgery, University Hospital Center ‘Mother Teresa’ (UHC)
keywoRDS:
cleft lip,
agenesis,
lateral incisor,
odontogenesis
IntroductionDental abnormalities are higher in patients born with
nonsyndromic unilateral cleft lip/alveolus/palate(uCl/A/P)in comparison with the general population.[1-4]The lateral incisors located at the cleft side in particular,showsa range of anatomic positions from normal, medial, distal, medial and distal to absent in relation with the cleft side. It is noteworthy thatcomplex reciprocal epithelial-mesenchymal interactions contribute significantly tomorphogenesis, differentiation and anatomic position of the teeth.[5]However, the mechanism behind this association remains largely unknown. It is therefore important to determine the presence or absence of permanent lateral incisor at an earlyage and then to plan treatment accordingly. our aim is to add to the knowledge by investigating the association between the cleft lip severity and agenesis of the permanent lateral incisor in nonsyndromic uCl/A/P patients.We tested one hypothesis: (i) that theextent of the cleft is associated with the absence of permanent lateral incisor.
Materials and MethodsThis retrospective study was undertaken to identify
472 patientswith complete and incomplete cleft of the lip/premaxilla/palate by reviewing medical records and hospitals archives. All patients were born between 5 April 1992 and 10 December 2005. In total, 345 patients met the following inclusion criteria:• Nonsyndromic uCl/A/P patients• Preoperative photograph• Radiographsof permanent dentition
one hundred twenty-seven patients were excluded following the exclusion criteria:
• Bilateral Cl/A/Ppatients• Syndromic patients• Missing preoperative photograph• Missing Radiographs of permanent dentition
For all patients the following informationwas entered into an MS Excel spreadsheet: patients number,date of birth, gender, clinic, Cl morphology, alveolus morphology and lateral incisor patterns.Preoperative photograph were used to categorized lip morphology into four groups:I) vermillion notch; II) 1/3 to 2/3 Cl; III) 2/3 till subtotal Cl; IV) complete Cl; and alveolar defects into four groups: I) normal alveolus; II) hypoplastic alveolus; III) incomplete alveolar cleft; IV) complete alveolar cleft. For statistically reasons the alveolar defects in two dentitions were categorized into three groups: I) normal alveolus and hypoplastic alveolus; II) incomplete alveolar cleft; III) complete alveolar cleft.Radiographs of the patients taken at 6 years old and later from the Erasmus Medical Center, Rotterdam, the Netherlands and the Radboud university Medical Center in Nijmegen, The Netherlands were used to assess five groups of lateral incisor patterns.The pattern Z was transcribed when the permanent lateral incisor was in normal position in normal alveolar arch. The patterns X, Y and XY weretranscribed with respect to the positionof the lateral incisor mesial, distal and both mesial and distal to the cleft side. The pattern AB was transcribed when the lateral incisor was absent.Available information of the primary and secondary palate categorized the primary palate in two groups: 1) incomplete cleft in the primary palate and 2) complete cleft in the primary palate; and the secondary palate into four groups: 1) normal secondary palate, 2) submucuous secondary palate, 3) incomplete cleft in the secondary palate and 4) complete cleft in the secondary palate.

Albanian Stomatological Journal100
Statistical AnalysesFirst, for each subject characteristics we compared
the differentlateral incisor patterns using Chi-square and Fisher exact tests. Second, we explored the associations of permanent dentition patterns with each subject characteristics by using multinomial regression model. We tested the role of: 1) Cl, gender, clinic; 2) alveolar defects; 3) palate defects. Covariates were included in the model based on their associations with permanent patterns in previous studies or a change in effect estimates of > 10%.The hypothesis was tested at the 5% level of significance. The odds ratio (oR) was calculated at the 95% CI to measure the strength of associations between permanent dentition patterns and eachcovariates. Statistical analyses were performed using Statistical Package of Social Sciences version 21.0 (SPSS Inc., Chicago, Il, uSA).
ResultsThe prevalence of patients born with the vermillion
notch and having the patterns X or Y was 25%. While the prevalence of patients with vermillion notch and the presence of patterns X and Y was 30.8%. The prevalence of 11.7% was found in patients having vermillion notch and pattern AB at the same time. In patients with 1/3-2/3 Cl the prevalence of patterns X and Y was 43.6%. Meanwhile the prevalence of having patterns X or Y was higher in patients with 2/3 in subtotal Cl. The higher prevalence of 52.7% of pattern AB was in patients with complete Cl. Subdivisions of Cl were compared regarding the prevalence of AB pattern, the alveolar defect and the palate defect. All Cl groups differed significantly from the extension of the cleft. Patients born with complete Cl, subtotal to 2/3 Cland 1/3 to 2/3 Cl were significantly associatedwith pattern AB, respectively (oR = 32.6, p <0.001; oR = 10.4, p = 0.02; oR = 6.5, p = 0.04).
DiscussionThis study shows that the agenesis of permanent lateral
incisor clearly differ with respect to the ‘severity’ or ‘extent’ of the cleft.This information can be used to plan and manage treatment, and also to informpatients and their parents.
Studies show that the prevalence of agenesis of teeth in patients with cleft is significantly higher (45-77%; [6]) compared with patients without cleft (3.2- 7.6%; [7]). Studies also showed that specific surgical procedures in cleft patients mayhave an effect on agenesis of teeth [8, 9].
In our study, the prevalence of agenesis of the lateral incisor was 34.7%. Agenesis of lateral incisor is 2% in normal population. [7, 10]
In this study it is shown that the extent of the cleft was significantly associated with the prevalence of lateral incisor agenesis.An explanation for this result is that these dental anomalies have the same etiologic factors with the lip categories they occur. Therefore, we suggest that critical factors in pathogenesis of the cleft lip impact the odontogenesis of lateral incisor as well. Another explanation may be that many alterations in early development lead to a complete cleft lip and hamper teeth embryogenesis as well.Another possible explanation may be the similar genetic aberrations can yield similar phenotypes. [11, 12] Importantly, this may be explain by the position of dental lamina ,which controls in terms of origin, shape, position and time of eruption lateral incisor, in connection point between medial nasal and maxillary process explanation.[13, 14]
The findings in our study may help in explaining and understanding the association found in previous studies between the presences of teeth in patients with cleft. Based on our knowledge this study assesses for the first time the association between agenesis of lateral incisor and cleft in non syndromic patients with unilateral Cl/ A/ P.Furthermore, this study would be useful to explain conjunction between phenotype and gene mapping of cleft patients highlighted by recent genetic research studies.
Fig. 1 Flowchart of subjects enrolled in the study.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 101
Table 1. Sample characteristics of patients with unilateral CL/A (n (%))Permanent patterns
Total X/ Y XY AB Z p-value+
n = 345 n = 113 n = 77 n = 120 n=35CharacteristicClinic
Rotterdam 158 69 35 54 0Nijmegen 187 44 42 66 35 <0.001
GenderMale 227 75 50 77 25
Female 118 38 27 43 10 0.882Cleft lip
Vermillion notch 68 17 21 8 22Cleft 1/3 to 2/3 55 11 24 7 13
Cleft 2/3 to subtotal 59 23 17 19 0Complete cleft lip 163 62 15 86 0 <0.001
Alveolar defectNormal 104 22 38 9 35
Hypoplastic 3 1 1 1 0Incomplete 47 16 17 14 0Complete 191 74 21 96 0 <0.001
Primary palateIncomplete cleft 145 34 54 22 35Complete cleft 200 79 23 98 0 <0.001
Secondary palateNormal 266 92 62 78 34
Submucous cleft 1 1 0 0 0Incomplete cleft 9 3 3 2 1Complete cleft 69 17 12 40 0 0.001
Cleft in PalateOnly in Primary 266 92 62 78 34
Primary + Secondary 79 21 15 42 1 <0.001
p values are based on Chi-squared and Fisher exact tests
REFERENCES
1. Ranta, R., A review of tooth formation in children with cleft lip/palate. American Journal of orthodontics and Dentofacial or-thopedics. 90(1): p. 11-18.
2. letra, A., et al., Defining Subphenotypes for oral Clefts Based on Dental Development. Journal of Dental Research, 2007. 86(10): p. 986-991.
3. Congenitally Missing Teeth in the Israeli Cleft Population. The Cleft Palate-Craniofacial Journal, 2005. 42(3): p. 314-317.
4. Jordan, R.E., B. Kraus, and C. Neptune, Dental abnormalities as-sociated with cleft lip and/or palate. The Cleft palate journal, 1966. 3: p. 22.
5. Vastardis, H., The genetics of human tooth agenesis: new discoveries for understanding dental anomalies. American Journal of orthodontics and Dentofacial orthopedics, 2000. 117(6): p. 650-656.
6. Böhn, A., Dental anomalies in harelip and cleft palate. Acta odontologica Scandinavica, 1963. 21: p. SuPPl38: 1.
7. Polder, B.J., et al., A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community dentistry and oral epidemiology, 2004. 32(3): p. 217-226.
8. lekkas, C., et al., The adult unoperated cleft patient: absence of maxillary teeth outside the cleft area. The Cleft palate-cranio-facial journal, 2000. 37(1): p. 17-20.
9. da Silva Filho, o.G., A.D.C. Normando, and l. Capelozza Filho, Mandibular growth in patients with cleft lip and/or cleft pal-ate—the influence of cleft type. American Journal of ortho-dontics and Dentofacial orthopedics, 1993. 104(3): p. 269-275.
10. Stamatiou, J. and A.l. Symons, Agenesis of the permanent lat-eral incisor: distribution, number and sites. J Clin Pediatr Dent, 1991. 15(4): p. 244-6.
11. van den Boogaard, M.-J.H., et al., MSX1 mutation is associated with orofacial clefting and tooth agenesis in humans. Nature genetics, 2000. 24(4): p. 342.
12. Vieira, A.R., et al., Medical sequencing of candidate genes for nonsyndromic cleft lip and palate. PloS Genet, 2005. 1(6): p. e64.
13. ooé, T., on the early development of human dental lamina. okajimas folia anatomica Japonica, 1957. 30(2-3): p. 197-210_1.
14. Hovorakova, M., et al., one odontogenic Cell-Population Con-tributes to the Development of the Mouse Incisors and of the oral Vestibule. PloS one, 2016. 11(9): p. e0162523.

Albanian Stomatological Journal102
AbstraktQëllimi: Faktorët risk për periodontitin, kombinuar me faktorët etiologjik dhe genetik, paraqesin pamjen klinike orale dhe sistemike, ndihmëse në nxitjen e shfaqjes së arterosklerozës. Nivelet plazmatike të markerave të inflamacionit janë shprehës të ndërlidhjes së periodontitit ekzistues me arterosklerozën avancuese.Ky studimi synon vlerësimin e efektit të trajtimit jo kirurgjikal periodontal, shprehur në nivelet e indekseve periodontal, në korelacion me nivelin sasiorw dhe cilësorw, të markerave plazmatik të inflamacionit.Materiale dhe metoda: Faza e parë e studimit është aplikimi i protokollit të hartuar të punës, në mostrën eksperimentale prej 10 pacientësh. Faza e dytë, aktuale, është reflektimi i korelacioneve të shprehura më parë, në mostër më të madhe pacientësh, rreth 54 pacientë. Pacientët janë vlerësuar për përqindje të sipërfaqeve të gjakosura dhe thellësi sondimi tek dhëmbët e Ramfjord-it. Analiza e gjakut dhe vlerësimi periodontal i statusit të pacientëve u krye para trajtimit dhe 1 javë post-trajtim, ose në epatën fundore të trajtimit. Vlera p≤ 0.0002 tregon relacion statistikisht të rëndësishëm.Rezultate: Të dhënat klinike treguan që mesatarja e zonave të gjakosura dhe thellësia e sondimit u reduktua me 62% dhe 2.5mm, reskeptivisht. Trajtimi jo kirurgjikal periodontal redukton ndjeshëm nivelin e markerave inflamator në gjak, në kufijtë 10-20Mg/dl.Konkluzioni: Mikroflora orale është burim potencial i bakteremisë së përkohëshme periodontale, me potencialin e nxitjes së tromboemblizmit, arterosklerozës, nëpërmjet bashkëveprimit me rruazat e shtuara në gjak. Trajtimi jo kirurgjikal periodontal redukton ndjeshëm nivelin e fibrinogenit, njohur si faktor risk për zhvillimin e tromboembolizmit arterial.
Saimir heta1, ilma Robo2, ortodonte ermelinda gina2, Dariel thereska1, Nevila alliu1
Niveli plazmatik i markerave të inflamacionit, si shprehës i ndërlidhjes së periodontitit me arterosklerozën
1Qëndra Spitalore Universitare “Nënë Tereza”, Tiranë 2Albanian University, Fakulteti i Shkencave Mjekësore, Tiranë, Albania
Fjalë kyçe:
fibrinogen,
periodontit
refraktar,
arteroskleroza
HyrjeSëmundjet inflamatore kanë ngjashmëri të dukshme
në mekanizmat bazë të veprimit të faktorëve risk. Periodontiti si një prej këtyre sëmundjeve, është i prezantuar në kavitetin oral me shenjat tipike klinike, të veprimit të faktorëve risk, të tillë si duhanpirja, diabeti dhe pllaka bakteriale. Kontrolli ndaj veprimit të faktorëve risk kryhet me anë të studimeve longitudinale, me qëllimin e gjetjes së kombinimit të mundshëm me përcaktuesit e riskut, parashikuesit e riskut dhe të indikatorëve të riskut. A janë këta elemente, kombinimi i të cilëve siguron veprimin e faktorëve të riskut?
Përcaktuesit e riskut veprojnë në mënyrë horizontale tek subjekti që flasim dhe veprimi i tyre kontrollohet me anë të studimeve longitudinale. Tek përcaktuesit e riskut janë përfshirë duhanpirja, diabeti, hipertensioni dhe dislipidemia. Të katër këta elementë janë veprues të drejtpërdrejtë tek enët e gjakut, në aftësinë e tyre për vazokonstriksion dhe vazodilatacion, në ngushtimin e lumenit dhe në elasticitetin e mureve. Treguesit e riskut përfshijnë: kariesin, lezionet periapikale, periodontitin dhe perikoronaritin. Këta elementë vlerësohen me anë të studimeve kros-seksionale. Parashikuesit e riskut për arteriosklerozën përfshijnë elementet: sasia e fibrinogenit, shtimin e rruazave të bardha të gjakut dhe raportin lDl/VlDl. Parashikuesit e riskut ndryshe nga treguesit e riskut janë elementë që vlerësohen me studime longitudinale.
Koha
DuhanpirjaDiabeti
HipertensioniDislipidemia
Përcaktuesit e
riskut
Hos
ti
Karieslezionet
PeriapikalePeriodontiti
Perikoronariti
Mik
roflo
ra
Fibrinogeni Shtimi i rruazave
të bardha të gjakut
Raporti lDl/VlDl
Parashikuesit e riskut
Die
ta
organizuar nga Dr.Ilma Robo
Treguesit e riskut
Të gjitha këto elementë janë të paraqitur në tabelën 1. Në këtë tabelë janë treguar kombinimi i këtyre tre elementëve dhe mënyra e vlerësimit të tyre në bazë të studimeve kros-seksionale dhe longitudinale.
Tabela 1. Rruga e analizimit të përcaktuesve të riskut, të parashikuesve të riskut dhe të indikatorëve të riskut, sipas
llojit të studimit ku mund t’i aplikojmë ata.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 103
Materiali dhe metodaNga diversiteti i periodontopative, përzgjedhim
periodontitin refraktar dhe atë agresiv. Tek të dyja sëmundjet, shkaktari i sëmundjes është kombinimi i A. actinomycetemcomitans, P. gingivalis, T. forsythia, P. intermedia and F. nucleatum. Raportet në porcione të përqëndrimit të këtyre baktereve, tregojnë nëse jemi përballur me periodontit të lokalizuar agresiv, apo me periodontit të gjeneralizuar, ose kronik.(1)
Ky studim ka për qëllim vlerësimin e efektit të trajtimit jo kirurgjikal periodontal në reduktimin e shenjave klinike të inflamacionit periodontal dhe në nivel të markerave të inflamacionit dhe në plazmën e gjakut (niveli i fibrinogenit dhe i numrit të qelizave të bardha të gjakut).
Për këtë arsye u formatua konsenti për pacientit. Pacientëve të përfshirë në studim i është marrë
mostër gjaku për analizë gjaku, me qëllimin e vlerësimit të nivelit të fibrinogenit dhe të numrit të rruazave të gjakut. Pacientët i janë nënshtruar 2 analizave të gjakut para trajtimit jo kirurgjikal periodontal dhe 10 ditë post trajtimit. Tek të dyja analizat janë përmbledhur të dhënat në vlera për fibrinogenin dhe për rruazat e bardha të gjakut. Vlerësimi i statusit periodontal të pacientëve
është kryer me ndihmën e indeksit të gjakosjes gingivale Mühlerman dhe sondimit të dhëmbëve të Ramfjord-it. Sondimi është kryer me sondën Williams.
Terapia me antibiotikë sistemik duket më e parashikueshme se administrimi lokal në zhdukjen e patogenëve periodontal nga xhepat e thellë periodontal,(2) duke treguar rol primar të absorbimit të medikamentit të administruar në ofrimin e këtyre antibiotikëve sistemik në vendin e veprimit të terapisë periodontale.(3) Theksojmë se trajtimi periodontal nuk përfshinte marrjen e antibiotikëve, si element ndihmës. Trajtimi periodontal përfshinte kyretazhin e thellë periodontal dhe aplikimin e solucioneve shpëlarës periodontal që aplikohen në poltronin dentar, vetëm nga stomatologu.
RezultateRezultatet e grumbulluara nga studimi janë
shpërndarë sipas specifikave nëpër tabelat më poshtë. Tek tabela 2 pacientët janë të ndarë në varësi të gjinisë dhe të moshës. Mosha 40 vjeçare është përzgjedhur mbështetur në karakteristikat e periodontitit agresiv dhe në elementin që është moshë e nivelit kufi, ku procedurat karioze fillojnë të reduktohen në shpeshtësinë e tyre dhe procedurat periodontale të shtojnë aktivitetin.
Pacientët Mosha nën 40 vjeç
Shprehur në %
Mosha mbi 40 vjeç
Shprehur në % Totali Totali në
% Vlera p
Femra 9 16.7% 10 18.51% 19 35.21%
0.3915 Meshkuj 12 22.2% 23 42.59% 35 64.79%
Totali 21 38.9% 33 61.1% 54 100%
Mosha mesatare e pacientëve është 42 vjeçare. Në tabelën 2 janë përmbledhur pacientët të klasifikuar si të
shëndetshëm dhe të sëmurë mbështetur në bazë të vlerave të regjistruara për indeksin PMA dhe për vlerat e sondimit.
Tabela 2. Në tabelë paraqiten pacientët e ndarë sipas gjinisë dhe moshës. Korelacioni është shprehur me përllogaritjen e vlerës p.
Tabela 3. Korelacioni midis numrit të pacientëve të përfshirë në studim ndarë në bazë të vlerësimeve sipas indeksit PMA dhe vlerave të sondimit.
Pacientët Të sëmurë sipas vlerave të sondimit
Të shëndetshëm sipas vlerave të sondimit Vlera p
Të sëmurë sipas indeksit PMA 11 16 0.0003
Të shëndetshëm sipas indeksit PMA 0 27
Totali 11 43
Në tabelën 4 është pasqyruar grupi i pacientëve në bazë të luhatjes së nivelit plazmatik të regjistruar të fibrinogenit, 10 ditë post trajtimit.
Tabela 4. Luhatjet e fibrinogenit në intervale të matshme.
Pacientët 0-10Mg/dL 10-20Mg/dL 20-Mg/dL
Të sëmurë sipas indeksit PMA 11 5 11
Të shëndetshëm sipas indeksit PMA 5 11 11
Totali 16 16 22

Revista Stomatologjike Shqiptare104
Indeksi gingival pëson luhatje në 1 vlerë vlerësimi pas trajtimit jo kirurgjikal korrekt periodontal. Të dhënat klinike tregojnë se mesatarja e zonave të
gjakosura dhe thellësia e sondimit reduktohen me 60% dhe me 2mm-ra.
Në figurat më poshtë pasqyrohen rastet klinike të pacientëve të përfshirë në studim.
Fig. 2. Pacienti para dhe pas trajtimit jo kirurgjikal periodontal. Në figurë është pasqyruar zona e incizivëve mandibular.
Fig. 3. Pacienti i pasqyruar pas trajtimit në zonën e maksilës dhe pas trajtimit në zonën mandibulare. Ky pacient është diagnostikuar me periodontit agresiv.
Fig. 4. Rast klinik ku dallohet ndjeshëm aftësia ripërtëritëse e indeve gingivale tek pacientët e shëndetshëm, që nuk vuajnë
nga sëmundje sistemike.DiskutimeStudimet mё tё fundit epidemiologjike kanё treguar
se inflamimi ёshtё lidhja mes sёmundjeve peridontale dhe komplikacioneve kardiovaskulare. Këto studime vlerёsojnë efektin e trajtimit jo-kirurgjikal periodontal nё nivelet e markerave tё inflamacionit tё hasur nё plazmёn e pacientёve me periodontit tё gravuar dhe refraktar.
Terapia periodontale ёshtё efektive nё reduktimin e nivelit plazmatik tё fibrinogenit.(4)
Nëse përpiqemi të analizojmë periodontitet si sëmundje inflamatore, shkaktuar nga flora ekzistuese orale, elementi bazë i klasifikimit të pacientëve të prekur, është mosha. Kufiri 40 vjeçar i moshës përcakton limitin kohor të ekstraksioneve orale shkaktuar nga destruksioni i dhëmbëve, si pasojë e kariesit.(5)
Pas kësaj moshe, efekti i periodontitit është akoma më i ndjeshëm në shkakun e mirëfilltë të ekstraksioneve

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 105
si pasojë e sëmundjeve periodontale. Nëse në këtë moshë përpiqemi të ndjejmë efektin e gjinisë (raporti meshkuj:femra), si në rastin e studimit tonë, vlera p e gjetur tregon se nuk ka një korelacion të ndjeshëm të kufirit moshor dhe gjinisë. Periodontitet e shfaqin njëlloj efektin e tyre pavarësisht florës orale të njëjtë, përkatësisht sipas diagnozës së vendosur. Terapia peridontale jo kirurgjikale redukton ndjeshëm përbërjen bakteriale subgingivale dhe porcionet e baktereve gram-negative, por jo deri në nivelin e reduktimit në sasi totale të A. actinomycetemcomitans.(4) Në studimin tonë përzgjodhëm rastet e periodontiteve agresive dhe refraktare për të matur ndryshimet e ndjeshme nëse ekzistojnë, tek markerat e inflamacionit në gjakun e pacientëve të prekur. Mosha mesatare 42 vjeçare e pacientëve të prekur në studimin tonë tregon edhe njëherë për një përzgjedhje rastësore, mbështetur në vullnetin e pacientëve.
Qëllimi tjetër i studimit qëndronte në gjetjen e korrelacionit që rezulton statistikisht i rëndësishëm, mbi vlerësimin e pacientëve sipas dy indekseve periodontale. E gjithë kjo vetëm në mbështetje të faktit që për të vlerësuar si të shëndetshëm apo të sëmurë një pacient nga pikëpamja periodontale, duhet të bazohemi në dy indekse periodontale. Njëri prej tyre të jetë vlera e sondimit dhe tjetri një indeks i përshtatshëm për vlerësimin e statusit
gingival, apo të shkaktarit kryesor të shfaqes lokale të gingiviteve, siç është pllaka bakteriale. Për shkak se sëmundja periodontale shoqërohet me zhvillimet e arteriosklerozës, është e rëndësishme të kuptohet reagimi lokal imun ndaj P. gingivalis.(5)
Fibrinogeni është faktor koagulimi me përqëndrim normal në gjak 1.5 – 4g/l. Ai luan rol kyç në hemostazën primare dhe sekondare.(6) luhatjet e ndjeshme në nivelin e fibrinogenit në gjak, para trajtimit dhe 10 ditë post-trajtim jo kirurgjikal periodontal, flasin edhe njëherë për ndërlidhjen sistemike të inflamacionit gingival–periodontal me mundësinë e shfaqes së arteriosklerozës, për arsyen e thjeshtë të ndikimit që ka inflamacioni i indeve të butë në luhatjen e nivelit plazmatik të fibrinogenit.
KonkluzioneTrajtimi periodontal jo kirurgjikal redukton dukshëm
nivelin e markerave jo inflamator në gjak.Shëndeti oral redukton ndjeshëm burimin potencial
për bakteremi periodontale, me potencialin e nxitjes së tromboembolizmit, me anë të ndërveprimit midis tromboblasteve.
Trajtimi jo kirugjikal periodontal redukton ndjeshëm nivelin e fibrinogenit, i njohur si faktor risk i zhvillimit të tromboembolizimit arterial.
1. Goodson JM.; “Antimicrobial strategies for treatment of periodontal diseases”; Periodontol 2000. 1994;5:142–68. [PubMed]
2. Slots J, Rams TE; “Antibiotics in Periodontal therapy: Advan-tages and disadvantages”; J Clin Periodontol. 1990;17:479–93. [PubMed]
3. Sakkelari D, Goodson JM, Kolokotronis A.; “Concentration of 3 tetracyclines in plasma, GCF and Saliva”; J Clin Periodon-tol. 2000;27:53–60. [PubMed]
4. Vidal F1, Figueredo CM, Cordovil I, Fischer RG; ”Periodontal therapy reduces plasma levels of interleukin-6, C-reactive protein, and fibrinogen in patients with severe periodonti-tis and refractory arterial hypertension”; J Periodontol. 2009
REFERENCA
May;80(5):786-91. doi: 10.1902/jop.2009.080471.
5. Michael G.Neëman, DDS, Henry H.Takey, DDS, Ms.Fermin A.Carranza, Dr.odont; “Clinical Periodontology; Ninth edi-tion”; 2004 Mosby.
6. Hussain M1, Stover CM1, Dupont A2; “P. gingivalis in Peri-odontal Disease and Atherosclerosis - Scenes of Action for Antimicrobial Peptides and Complement”; Front Immunol. 2015 Feb 10;6:45. doi: 10.3389/fimmu.2015.00045. eCollec-tion 2015.
7. Mackie IJ, Kitchen S, Machin SJ, loëe GD; “Haemostais and Thrombosis Task Force of the British Committee for stan-dards in Haematology. Guidelines for fibrinogen assays”; Br J Haemotol 2003;121:396-304.
Albanian Stomatological Journal106
AbstractPurpose: Risk factors for periodontitis, combined with genetic and etiologic factors, affecting the oral and systemic clinical view of the patient, assisting in promoting of atherosclerosis. Plasma levels of markers of inflammation are expressive, in interconnection of existing periodontitis, with advancing arteriosclerosis.This study aims to assess the effect of non-surgical periodontal treatment, expressed in levels of periodontal indices, correlated with the quantitative and qualitative level, of the plasma markers of inflammation.Materials and methods: The first phase of the study is the application of the designed protocol at experimental sample of 10 patients. The second phase, current, is the reflection of correlations expressed before, in the biggest sample of patients, about 54 patients. Patients were evaluated for percentage of bleeding surfaces and probing depth to Ramfjord teeth. Blood analysis and evaluation of periodontal status of patients was performed before treatment and 1 week post-treatment or after the terminal stage of treatment. P value ≤ 0.0002 indicates statistically significant relationship.Results: The data showed that the average of clinical bleeding areas and probing depth are reduced by 62% and 2.5mm, respectively. Non-surgical periodontal treatment significantly reduces the level of fibrinogen in the blood, in the range 10-20 mg/dl.Conclusion: Microoral flora is a potential source of temporary periodontal bacteremia, with the potential of promoting atherosclerosis, through increased interaction with blood cells. Non-surgical periodontal treatment significantly reduces the level of fibrinogen, known as risk factor for the development of arterial arteriosclerosis.
Saimir heta1, ilma Robo2, ortodonte ermelinda gina2, Dariel thereska1, Nevila alliu1
plasma level of inflammatory markers, as an expression of the connection of periodontitis with arteriosclerosis
1University Hospital Center “Mother Teresa“ , Tirana, Albania 2Albanian University, Faculty of Medical Sciences, Tirana, Albania
keywoRDS:
fibrinogen,
probing depth,
bleeding
gingival surfaces
Entry Inflammatory diseases have obvious similarities to
the underlying mechanisms of action of risk factors. Periodontitis as one of these diseases is presented in oral cavity with typical clinical signs of risk factors, such as smoking, diabetes, and bacterial plaques. Control of the risk factor action is carried out through longitudinal studies, with the aim of finding a possible combination with risk determinants, risk proponents and risk indicators. Are these elements the combination of which provides contact and action of risk factors?
Risk determinants act horizontally at the subject we speak and their action is controlled by longitudinal studies. Risk factors include smoking, diabetes, hypertension and dyslipidaemia. All four of these elements are direct acting in the blood vessels, their ability to vasoconstriction and vasodilation, the narrowing of the lumen and the elasticity of the walls. Risk indicators include: caries, periapical lesions, periodontitis and pericoronitis. These elements are evaluated through cross-sectional studies.
Risk factors for arteriosclerosis include the elements: the amount of fibrinogen, the addition of white blood cells, and the lDl / VlDl ratio. Risk projections different from risk indicators and they are the elements that we can evaluat with longitudinal studies. All of these elements are presented in Table 1. This table shows the combination
of these three elements and the way of their evaluation based on cross-sectional and longitudinal studies.
Table 1. Analyzing risk determinants, risk proponents and risk indicators, by the type of study
where we can apply them.
Tim
e
SmokingDiabetes
HypertensionDyslipidemia
Risk Determinants
Hos
t
CariesPeriapical
lesionsPeriodontitis
Pericoronaritis
Mic
roflo
ra
FibrinogenWhite blood
cellslDl / VlDl
ratio
Risk proponents
Die
t
organized by, Dr.Ilma Robo
Risk Indicators
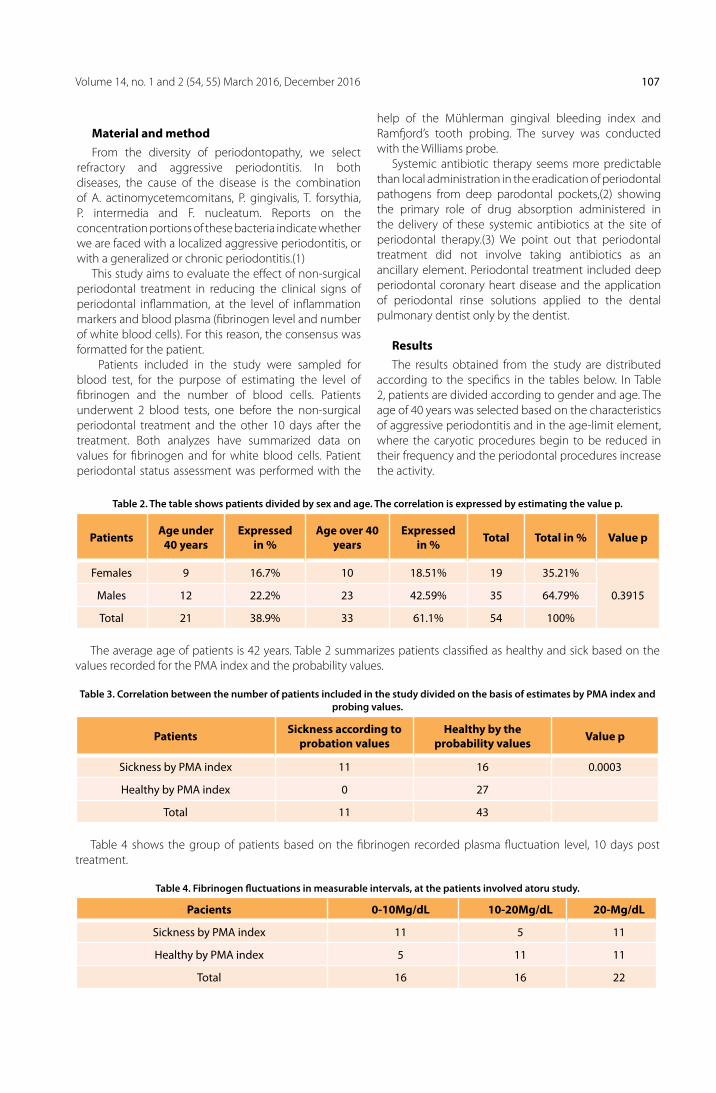
Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 107
Material and method From the diversity of periodontopathy, we select
refractory and aggressive periodontitis. In both diseases, the cause of the disease is the combination of A. actinomycetemcomitans, P. gingivalis, T. forsythia, P. intermedia and F. nucleatum. Reports on the concentration portions of these bacteria indicate whether we are faced with a localized aggressive periodontitis, or with a generalized or chronic periodontitis.(1)
This study aims to evaluate the effect of non-surgical periodontal treatment in reducing the clinical signs of periodontal inflammation, at the level of inflammation markers and blood plasma (fibrinogen level and number of white blood cells). For this reason, the consensus was formatted for the patient.
Patients included in the study were sampled for blood test, for the purpose of estimating the level of fibrinogen and the number of blood cells. Patients underwent 2 blood tests, one before the non-surgical periodontal treatment and the other 10 days after the treatment. Both analyzes have summarized data on values for fibrinogen and for white blood cells. Patient periodontal status assessment was performed with the
help of the Mühlerman gingival bleeding index and Ramfjord’s tooth probing. The survey was conducted with the Williams probe.
Systemic antibiotic therapy seems more predictable than local administration in the eradication of periodontal pathogens from deep parodontal pockets,(2) showing the primary role of drug absorption administered in the delivery of these systemic antibiotics at the site of periodontal therapy.(3) We point out that periodontal treatment did not involve taking antibiotics as an ancillary element. Periodontal treatment included deep periodontal coronary heart disease and the application of periodontal rinse solutions applied to the dental pulmonary dentist only by the dentist.
ResultsThe results obtained from the study are distributed
according to the specifics in the tables below. In Table 2, patients are divided according to gender and age. The age of 40 years was selected based on the characteristics of aggressive periodontitis and in the age-limit element, where the caryotic procedures begin to be reduced in their frequency and the periodontal procedures increase the activity.
Table 2. The table shows patients divided by sex and age. The correlation is expressed by estimating the value p.
Patients Age under 40 years
Expressed in %
Age over 40 years
Expressed in % Total Total in % Value p
Females 9 16.7% 10 18.51% 19 35.21%
0.3915 Males 12 22.2% 23 42.59% 35 64.79%
Total 21 38.9% 33 61.1% 54 100%
The average age of patients is 42 years. Table 2 summarizes patients classified as healthy and sick based on the values recorded for the PMA index and the probability values.
Table 3. Correlation between the number of patients included in the study divided on the basis of estimates by PMA index and probing values.
Patients Sickness according to probation values
Healthy by the probability values Value p
Sickness by PMA index 11 16 0.0003
Healthy by PMA index 0 27
Total 11 43
Table 4 shows the group of patients based on the fibrinogen recorded plasma fluctuation level, 10 days post treatment.
Table 4. Fibrinogen fluctuations in measurable intervals, at the patients involved atoru study.
Pacients 0-10Mg/dL 10-20Mg/dL 20-Mg/dL
Sickness by PMA index 11 5 11
Healthy by PMA index 5 11 11
Total 16 16 22

Revista Stomatologjike Shqiptare108
The gingival index undergoes 1 oscillation after non-surgical periodontal surgery. Clinical data show that the average of bleeding areas and the depth of the probe are
reduced by 60% and 2mm. The figures below reflect the clinical cases of the patients involved in the study.
Fig. 2. Patient in fotos are before and after non-surgical periodontal treatment. The figure shows the area of mandibular incisors.
Fig. 3. Reflected patient after treatment in the maxillary area and after treatment in the mandibular area. This patient is diagnosed with aggressive periodontitis.
Fig.4. Clinical case that shows how the resilience of gingivitis tissue resembling at a healthy person, who does not suffer from systemic disease, that is significantly distinguished.
DiscussionsRecent epidemiological studies have shown that
inflammation is the connection between peripheral neoplasms and cardiovascular complications. These studies evaluate the effect of non-surgical periodontal treatment at the levels of inflammatory markers in the plasma of patients with agraved and refracted periodontal problems. Periodontal therapy is effective in reducing plasma fibrinogen level.(4)
If we try to analyze periodontitis as inflammatory disease, caused by existing oral flora, the basic element of the classification of affected patients is age. The 40-year-old limit determines the time limit of oral extravasations, caused by the destruction of the teeth due to caries.(5)
After this age, the effect of periodontitis is even more pronounced in the true cause of extractions due to periodontal diseases. If at this age we try to sense the effect of gender (male ratio: female), as in our case study,

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 109
the observed value indicates that there is no significant correlation between the age limit and the gender. Periodontitis exhibits the same effect regardless of the same oral flora, respectively according to the established diagnosis. Non-surgical peridontal therapy significantly reduces subgingival bacterial composition and Gram-negative bacterial portions, but not up to the level of total A. actinomycetemcomitans reduction.(4) In our study we selected cases of agressive and refractory periodontitis to measure changes in visible mode, if any, to the markers of inflammation in the blood of the affected patients. The 42-year average of the patients affected in our study shows once again for a random selection, based on the patient’s will.
The other purpose of the study was to find the correlation statistically significant, on the evaluation of patients according to two periodontal indexes. All this only in support of the fact that to evaluate as healthy or sick a patient from the periodontal point of view, we have to rely on two periodontal indices. one of them is the value of the probe, and the other an index suitable for the evaluation of gingival status, or the main cause of the local gingivitis display, such as bacterial plaque. Because
periodontal disease is associated with arteriosclerosis, it is important to understand the local immune response to P. gingivalis.(5)
Fibrinogen is a coagulation factor with a normal blood concentration of 1.5 to 4 g / l. It plays a key role in primary and secondary hemostazes.(6) Significant fluctuations in blood fibrinogen level, prior to treatment and 10 days of non-surgical periodontal posttreatment, once again reveal systemic linkage of gingival-periodontal inflammation with the possibility of arteriosclerosis , for the influence of soft tissue inflammation on fluctuating plasma fibrinogen level.
ConclusionsNon-surgical periodontal treatment significantly reduces
the level of non-inflammatory markers in the blood.oral health significantly reduces the potential
source of periodontal bacteria, with the potential of promoting thromboembolism, by interaction between thrombocytes.
Non-surgical periodontal treatment significantly reduces the level of fibrinogen, known as a risk factor for the development of arterial thromboembolism.
1. Goodson JM.; “Antimicrobial strategies for treatment of periodontal diseases”; Periodontol 2000. 1994;5:142–68. [PubMed]
2. Slots J, Rams TE; “Antibiotics in Periodontal therapy: Advan-tages and disadvantages”; J Clin Periodontol. 1990;17:479–93. [PubMed]
3. Sakkelari D, Goodson JM, Kolokotronis A.; “Concentration of 3 tetracyclines in plasma, GCF and Saliva’; J Clin Periodontol. 2000;27:53–60. [PubMed]
4. Vidal F, Figueredo CM, Cordovil I, Fischer RG; ”Periodontal therapy reduces plasma levels of interleukin-6, C-reactive protein, and fibrinogen in patients with severe periodonti-tis and refractory arterial hypertension”; J Periodontol. 2009 May; 80(5):786-91. doi: 10.1902/jop.2009.080471.
REFERENCES
5. Michael G.Newman, DDS, Henry H.Takey, DDS, Ms.Fermin A.Carranza, Dr.odont; “Clinical Periodontology; Ninth edi-tion”; 2004 Mosby.
6. Hussain M, Stover CM, Dupont A; “P. gingivalis in Periodon-tal Disease and Atherosclerosis - Scenes of Action for An-timicrobial Peptides and Complement”; Front Immunol. 2015 Feb 10;6:45. doi: 10.3389/fimmu.2015.00045. eCollec-tion 2015.
7. Mackie IJ, Kitchen S, Machin SJ, lowe GD; “Haemostais and Thrombosis Task Force of the British Committee for stan-dards in Haematology. Guidelines for fibrinogen assays”; Br J Haemotol 2003;121:396-304.

Revista Stomatologjike Shqiptare110
Hyrjenë implantimin dentar pamjaftueshmëria e kockës
është një problem i rëndesishëm. Humbje e dhëmbëve posteriore për një kohë të gjatë i hap rrugën rezorbimit të proçesit alveolar dhe pneumatizimit të sinusit maksilar duke e bërë implantimin dentar të veshtirë. Në të kaluarën sinusi maksiler është konsideruar thjesht një hapësire anatomike e pavlerë dhe që nuk shërbente në proliferimin kockor. Këto mendime janë kaluar tashmë në sajë të teknikave të ndryshme kirurgjikale4*. Metodat e përdorura për rigjenerimin e proçeseve atrofike përfshijnë rigjenerimin e guiduar kockor inlay grafted dhe ngritje e sinusit maksilar. Kjo e fundit është një teknike e përkryer për të siguruar një qëndrueshmëri afatgjatë të implanteve 5, 6*. Ka një numër të madh studimesh mbi ngritjen e sinusit maksilar në terma anatomike teknikave rezultateve klinike dhe histologjike të bazuara në qëndrimin klinik dhe llojeve të implanteve5*. Teknika e ngritjes së dyshemese së sinusit maksilar për implantimin dentar në zonën pasteriore maksilare u prezantua7( dhe raportua për herë të parë me 1980 8( nga Ëallace et al9(. Shumë faktorë ndërhyjne në shkallën e suksesit implantar pas ngritjes se sinusit. Këtu përshkruhen materiali e implantit, përpunimi i sipërfaqes, implantimi në një ose dy faza sipërfaqja e kontaktit midis graftit dhe kockës autologe, ushqyeshmëria e lembos dhe koha e pritjes10, 11. Ky artikull vlerson përdorimin e grafteve kockore në ngritjen e sinusit maksilar për të determinuar kriteret e përshtatshme në implantimin dentar në maksilën posteriore.
Materiale dhe metodaKy artikull përfshin 34 pacientë tek të cilët u aplikua
ngritja e sinusit maksilar për implantim dentar në maksilen posteriore në periudhën 2007-2012. Pacientët janë ndjekur për një periudhë dy vjecare pas protezimit. Janë 21 meshkuj dhe 13 femra me një moshë mesatare 53. 6 vjec. Janë vendosur gjithësej 68 implante
Fig. 1 Hyrja laterale
Fig. 2 Preparimi membranes
AbstraktQëllimi i studimit: Rezorbimi i proçesit alveolar të maksiles e komplikon vendosjen e implanteve në regjonin posterior të saj.Në ditët e sotme ngritja e sinusit maksilar nuk e bën të pamundur implantimin e kësaj zone.Shumë studime janë bërë në drejtim të permirësimit të cilësisë dhe sasisë së kockës së përdorur për këtë qëllim dhe grada e suksesit ndryshon nga njëri material në tjetrin.Metoda: Janë marë në studim 34 pacientë të cilet ju vendosen imlplante në regjonin posterior të maksilës me ngritje të sinusit maksilar nga 2007-2012.Pacientët janë mbajtur nën kontroll për 2 vjet pas vendosjes së dhëmbëve.Kanë qënë 21 meshkuj dhe 13 femra me një moshë mesatare 53.6 vjec.Janë vendosur gjithsej 68 implante.Rezultatet: Ky studim vlerëson shkallën e suksesit pas ngritjes së sinusit me autografte,ksenografte dhe b-TCP.Nga 2007-2012,janë vendosur 68 implante në 34 pacientë në klinikën “Albdental” duke përdorur teknikën e ngritjes së sinusit maksilar.Shkalla e suksesit të implanteve ka qënë 91.2%.Konkluzione: Në kontrollet më të fundit 62 implante janë plotësisht të integruara me asnjë shenjë klinike apo radiologjike levizshmërie.Diametri më i perdorur ka qënë 3.8.Materiali më i përdorur dhe me i suksesshëm ka qënë kombinimi kockë autologe + b-TCPn (autograft+b-TCP) dhe ksenograft +autograft.
FloRiaN BllaCa
vlerësim klinik i 34 rasteve të implantuara me ngritje të sinusit maksilar
Klinika Dentare “AlbdentaL” Durrës Albania
Fjalë kyçe:
Sinusi maksilari,
graft kockor,
implant,
trikalcium
fosfat

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 111
Hyrja laterale është përdorur për pacientë me kreshtë reziduale më të madhe se 4 mm fig1, fig2. Ku niveli i kreshtës alveolare ka qënë me i vogël se 4 mm është aplikuar më parë ngritja e sinusit dhe vendosja e implanteve është bërë në një fazë të dytë. Për rastet me gjatesi të 4-7mm të kreshtës alveolare ngritja e sinusit dhe implantimi janë bërë në të njëjtën fazë.
Ndërhyrjët janë bërë përgjithësisht me anestezi lokale. Pas ngritjes së lembos mukoperiostale në madhësi të tillë që të mbyllë plotësisht dritaren e krijuar, është hapur sinusi me freze round të madhe ose me piezzo 2-3 mm mbi dysheme. Është preparuar dhe ngritur membrana sinuzale. fig2. Grafti është vendosur pas preparimit të sitit implanter gjithashtu dhe pas vendosjes së implanteve duke mbushur hapsirat e mbetura subantrale, meziale dhe laterale. Është vendosur membranë kolagjenoze e absorbueshme në dritaren vestibulare e absorbueshme në te gjitha rastet. fig4. Në fund është aplikuar suture e thjeshtë.
Materialet e përdorura për grafte kanë qenë: 1. Ksenograft2. Allograft3. Ksenograft+autograft4. Allograft+autograft5. Tcp+autograft ne raport 1: 1 nga regjoni retromolar
dhe tuberi.
Fig3 Vendosja e graftit
Fig4 Membranë kolagjenoze
Materiale Pacientë Nr. tot impanteve /Nr implanteve të integruar Shkalla e suksesit
Xenograft 6 8/4 50. 0
Tcp+autograft 14 22/22 100
Xenograft+autograft 6 24/22 91. 6
Autograft 4 8/8 100
Te tjerë 4 6/6 100
Total 34 68/62 91. 1%
Implantet e përdorura kanë qënë Tiolox, Innovazione, DIo implant dhe VIS implant. Diametri më i përdorur ka qënë 3. 8mm (22 implante) dhe 3. 75 e 4. 0 (20 implante), ndërsa gjatësia më e përdorur ka qënë l. 10mm (28 implante).
Vlerësimi i mbijetesës së implanteve është bërë në varësi të pesë kritereve të vendosura nga Albrektsson (22) dhe shkalla e suksesit është vlerësuar në përputhje me llojin e implantit diametrin dhe gjatësinë e tij si dhe koha e ndërhyrjes kirurgjikale të dyte ku ka patur.
Table 1. Shkalla e suksesit në varësi të llojit të graftit
Janë vendosur gjithësej 68 implante në 34 pacientë me një përqindje suksesi 91, 1%. Ksenografti ka qënë i suksesshëm në 4 nga 6 rastet e aplikuara ndërsa kombinimi TCP+autograft dhe ai ksenograft + autograft ka qënë me i suksesshmi dhe më i përdoruri në 19 nga 20 rastet e aplikuara(95%). Tabela 1. Humbja e implanteve ka ndodhur me tepër kur implantimi është bërë para 6 muajve të ngritjes së sinusit. Tabela2

Albanian Stomatological Journal112
Fig, 5, 6 Një vitë pas kirurgjisë
Fig7 Rezultati final
Tabela3. Shkalla e suksesit në raport me diametrin e implantit.
Përmbledhje e diskutimeSinusi maksilar lidhet me kavitetin nazal nëpërmjet
meatusit inferior në 1/3 e sipërme të murit të brëndshëm të sinusit. Në qoftë se në bëjmë ngritje të madhe të mukozës kjo zonë mund të ekspozohet. Ky komplikacion duhet shmangur. Pas lindjes sinusi maksilar zmadhohet dhe zë një pjesë të madhe të maksiles. Në adoleshencë sinusi shtrihet nga kanini tek molari i tretë dhe superiorisht nga orbita deri tek rrënja e kaninit maksilar. Si rrjedhojë sinusi maksilar ndërhyn tek vendosja e implanteve pas regjionit të kaninit kështu që në mungesë ëe kockës disponibël nevojitet ngritje e mukozës së tij. Misch dhe aut. 13) kanë raportuar një shkallë suksesi deri në 98% në 170 implante të vendosura me ngritje të sinusit maksilar
Diametri implanteve
Nr i pacientëve
Nr i implanteve
Implante të humbura
2. 9 2 4 -
3. 25 2 4 -
3. 5 6 8 2
3. 75 2 10 -
3. 8 12 22 2
4. 0 6 10 2
4. 5 6 6 -
5. 0 2 2 -
6. 0 2 2 -
Shuma 68 6
Gjatësia e implantit
Nr. i pacienteve
Nr. I implanteve
Implante të humbura
10 20 28 2
11. 5 9 16 2
12 9 12 2
13 4 8 -
14 - - -
15 1 4 -
Perqindje 100% 8. 8%
Shuma 68 6
Tabela2. Shkalla e suksesit në raport me kohën e pritjes
Koha në muaj Nr i implanteve Implante të humbura
Less then 5 months 10 4
6 8 2
7 8 -
10 12 -
12 30 -

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 113
me TCP të përzier me kockë të demineralizuar dhe gjak. Kockë autogjene mund të përdoret gjithashtu si material për grafte sinusi.
Kockat allogjenike, heterologe apo sintetike më vete ose të përziera janë gjithashtu të efektshme në varësi të situatave klinike. 14). Graftet e perdorura në formë blloku dhe ato të bluara në përqindje respektive 80. 4% dhe 94. 83% kanë vërtetuar avantazhin e këtyre të fundit si dhe një mbijetesë më të lartë implantare. 15). Kocka autogjene është standarti i arte për shkak të vetive osteokonduktive dhe osteoinduktive teë saj. 16). Megjithatë ajo ka disa mangeëi që përfshijnë kohën e nevojshme të qëndrimt në spitalë një plagë kirurgjikale e dytë si dhe ri pneumatizimin e sinusit të shkaktuar nga rezorbimi i graftit. Në menyrë paralele prodhimi i zevendësuesëve kockorë është në rritje. 10). Allograftet janë kocka kortikale apo spongioze të perfituara nga kadavrat apo donatorë të tjere. Kocka sterilizohet dhe ruhet në banka kockore. Trajtimi adekuat duhet gjykuar në bazë të avantazheve dhe të metave të kockes autologe dhe asaj jo autologe. Avantazhet e këtyre të fundit janë grada e ulët e infeksionit postoperator, qëndrueshmëria e graftit ndaj rezorbimit dhe gjithashtu nuk kemi një plagë te dytë operatore. Periudha e gjatë e shërimit, teknikat preçize kirurgjikale dhe mungesa e vetive osteoinduktive janë të metat e këtyre grafteve. Autograftet kërkojne një periudhë sëerimi më të shkurtër, nuk kanë kosto dhe
kanë veti osteoinduktive. Rezorbimi i graftit dhe prania e një plage operatore të dytë janë disavantazhet e këtyre grafteve18). Studimet e fundit nuk kanë treguar ndonjë lidhje të rëndësishme midis materialit implantar dhe incidencës së komplikacioneve në ngritjen e dyshemesë së sinusit maksilar, dhe në formimin e kockes së re brënda një mesatareje prej 6 muajsh. Përveç kësaj nuk është vërejtur ndonjë diferencë në pamjen radiologjike ndërmjet kockës autologe dhe asaj sintetike të përzier me autologe. 19)
KonkluzioneNgritja e mukozës së sinusit maksilar është bërë në
34 pacientë, janë vendosur gjithësej 68 implante dhe graftet e përdorura kanë qënë Ksenografte, Allografte, Sintetike dhe autologe. Në ndjekjen 2 vjeçare të bërë më pas mbeten të integruara 62 implante pa shenja radiologjike apo klinike inflamacioni. Këta pacientë kanë mundur të përtypin pa komplikacione në një përqindje suksesi 91. 2%1. Për ksenografte+autografte shkalla e suksesit ka
qënë 91. 6%(24/22)2. Diametrat implantare më i përdorur kanë qënë 3. 8, 4.
0 dhe 4. 5 në një shkallë suksesi 89. 4%3. Gjatësia implantare më e përdorur ka qënë l. 10 dhe
shkalla e peëgjithëshme e mbijetesës implantare ka qënë 91. 2%(68/62)
1. Ëheeler Sl, Holmes RE, Calhoun CJ. Six-year clinical and histologic study of sinus-lift grafts. Int J oral Maxillofac Im-plants 1996;11: 26-34.
2. Butz SJ, Huys lË. long-term success of sinus augmentation using a synthetic alloplast: a 20 patients, 7 years clinical re-port. Implant Dent 2005;14: 36-42.
3. Krauser JT, Rohrer MD, Wallace SS. Human histologic and histomorphometric analysis comparing osteoGraf/N with PepGen P-15 in the maxillary sinus elevation procedure: a case report. Implant Dent 2000;9: 298-302.
4. Tadjoedin ES, de lange Gl, Bronckers Al, lyaruu DM, Burg-er EH. Deproteinized cancellous bovine bone (Bio-oss) as bone substitute for sinus floor elevation. A retrospective, histomorphometrical study of five cases. J Clin Periodontol 2003;30: 261-270.
5. Wallace SS, Froum SJ, Cho SC, Elian N, Monteiro D, Kim BS, Tarnow DP. Sinus augmentation utilizing anorganic bovine bone (Bio-oss) with absorbable and nonabsorbable mem-branes placed over the lateral ëindoë: histomorphometric and clinical analyses. Int J Periodontics Restorative Dent 2005;25: 551-559.
6. Hurzeler MB, Kirsch A, Ackermann Kl, Quinones CR. Re-construction of the severely resorbed maxilla with dental implants in the augmented maxillary sinus: a 5-year clinical investigation. Int J oral Maxillofac Implants 1996;11: 466-475.
7. Tatum oH Jr, lebowitz MS, Tatum CA, Borgner RA. Sinus augmentation. Rationale, development, long-term results. N Y State Dent J 1993;59: 43-48.
8. Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marroë and bone. J oral Surg 1980;38: 613-616.
9. Wallace SS, Froum SJ, Tarnow DP. Histologic evaluation of a sinus elevation procedure: a clinical report. Int J Periodon-tics Restorative Dent 1996;16: 46-51.
10. Del Fabbro M, Testori T, Francetti l, Weinstein R. Systematic reviewof survival rates for implants placed in the grafted maxillary sinus. Int J Periodontics Restorative Dent 2004;24: 565-577.
11. Kahnberg KE, Nystrom E, Bartholdsson l. Combined use of bone grafts and Branemark fixtures in the treatment of severely resorbed maxillae. Int J oral Maxillofac Implants 1989;4: 297-304.
12. Kim SG. Sinus Bone Graft, Narae Publishing Inc, 2004. 13. Misch CE. Maxillary sinus augmentation for endosteal im-
plants: organized alternative treatment plans. Int J oral Im-plantol 1987;4: 49-58.
14. Jensen oT, Shulman lB, Block MS, Iacono VJ. Report of the Sinus Consensus Conference of 1996. Int J oral Maxillofac Implants1998;13: 11-45.
15. Ëallace SS, Froum SJ. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic revieë. Ann Periodontol 2003;8: 328-343.
16. Schlegel KA, Fichtner G, Schultze-Mosgau S, Wiltfang J. His-tologic findings in sinus augmentation with autogenous bone chips versus a bovine bone substitute. Int J oral Max-illofac Implants 2003;18: 53-58.
17. Garg AK. Bone Biology, Harvesting, and Grafting for Dental Implants. 1st edition, 2005.
18. Fugazzotto PA, Pikos MA. Guided bone regeneration and sinus augmentation in the absence of autogenous bone grafting. Implant Dent 2001;10: 158-161.
19. Barone A, Santini S, Sbordone l, Crespi R, Covani u. A clini-cal study of the outcomes and complications associated with maxillary sinus.
REFERENCA

Albanian Stomatological Journal114
Introduction In implant placement, the insufficient bone height
causes several problems. In the posterior maxilla, the bone loss on the buccolingual side and apical region that follows
the loss of a tooth and pneumatization of the maxillary sinus floor make implantation difficult. In the past, the maxillary sinus floor was considered merely an unnecessary anatomical space that was of no help in bone proliferation. However, these thoughts has been overcome by various surgical techniques4). The methods used to regenerate an atrophied ridge include guided bone regeneration (GBR) followed by onlay bone transplant, le Fort I osteotomy and bone transplantation, maxillary sinus floor elevation and bone grafting. The last appears to be an excellent method promoting the long-term retention of implants5, 6). There have been numerous reports about maxillary sinus floor elevation in terms of the anatomy, technical factors, clinical and histological results based on the clinical approach, and implant materials5). A maxillary sinus floor elevation technique for placing an implant in a recessed maxillary molar area was first introduced7), and reported in1980 8) by Wallace et al. 9)
Many variables affect the success rate of implant placement after maxillary sinus floor elevation, including the implant material, implant surface treatment, one- or two-stage implant placement, the contact surface between the grafted and autologous bone, the blood supply to the elevated flap, and the time since surgery10, 11). This article evaluated maxillary floor elevation using various bone substitutes to determine the criteria for successful implant placement in the maxillary molar area.
Patients and methodsThis study included 34 patients who underwent
maxillary sinus floor elevation during implant placement in the maxillary molar area from 2007 to 2012. The patients were followed up for at least 2 years after completion of the prosthesis. There were 21 males and 13 females, with an overall mean age of 53. 6 years. In total, 68 implants were placed.
Fig. 1 Lateral approach
Fig. 2
AbstractAims of Study: Alveolar bone absorption after missing of tooth leads to problems when placing posterior maxillary implants. Because of sinus lifting, an unfavorable architecture of the maxillary sinus no longer contraindicates the implant placement. Many investigators have examined the ways to improve bone quality and quantity and the success rates differ for different bone grafting materials.Method: This study included 34 patients who underwent maxillary sinus floor elevation during implant placement in the maxillary molar area from 2007 to 2012. The patients were followed up for at least 2 years after completion of the prosthesis. There were 21 males and 13 females,with an overall mean age of 53.6 years. In total,68 endoseus implants were placed.Results: This study evaluates the success rate of implant after sinus grafting with autografts,xenografts and b-TCP. From 2007 to 2012, 68 endosseous implants were placed in 34 patients at “Albdental” private practice using sinus lifting techniques. The survival rate for the implants was 91.1%.Conclusion: At the last follow-up, 62 implants remained attached to the upper prosthesis with no radiological or clinical signs of inflammation or mobility. The most common implant diameter was 3.8. The most common and successful augmentation material used was autograft+b-TCP.
FloRiaN BllaCa
implant placement in maxillary sinus area.outcome of 34 cases with sinus lifting
AlbdentaL “Private Practice Durres Albania
key woRDS:
Maxillary sinus,
Bone graft,
Dental implant,
tricalcium
phosphate.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 115
A lateral approach was used for patients with more than 4 mm of residual alveolar bone fig1, fig2. When the height of the residual alveolar bone was less than 4 mm, two-stage surgery was performed, while one-stage surgery was performed for the cases with 4-7 mm of residual alveolar bone.
under local anesthesia, a full thickness flap was prepared to fit the window, and an oval window was created in the area 2~3 mm above themaxillary sinus floor. The maxillary sinus membrane was dissected, and elevated. fig2. Graft material was placed in the subantral space on the mesial, inner, and lateral sides, the implants were placed, and any remaining space was filled. Collagenous membrane was used in all the cases. fig. 4
Finally, the flap was sutured. The used materials were as follows: 1. Xenograft 2. Allograft 3. Xenograft + autogenous bone4. Allograft +autogenous bone(autograft)5. Tcp mixed with autogenous bone from the
retromolar area and tuber maxillae in 1: 1 ratio.
Fig3 Vendosja e graftit
Fig3 Graft placement Fig4 Collagenous membrane
The implants used in accordance with the manufacturer included 68 fixtures of Tiolox (dentaurum), Innovazione, DIo and VIS implants. The most frequently used diameters were 3. 8 (22 implants) and 3. 75 mm and 4. 0 mm (20 implants), and the most frequently used lengths were 10 mm.
Implant success rate was evaluated using the five criteria suggested by Albrektsson (22), and the success rate was evaluated according to implant type, the length and
diameter of the implant, and the time of second surgery. Results (Tables 1~4)overall, 68 implants were placed in 34 patients with
an 91. 1% success rate. Xenograft (Bio-oss, BioCera, BBP) was successful in 4 of 6 cases applied, while Xenograft + Autograft and Tcp+Autograft were successful in 19 of 20 cases applied(95%) (Table 1). The implant failure rate was much higher when the second surgery was performed within 6 months Table 2.
Table 1. Success rate of the various graft materials
Materials Patients Nr.of total impl/Nr of success implants Success rates
Xenograft 6 8/4 50. 0
Tcp+autograft 14 22/22 100
Xenograft+autograft 6 24/22 91. 6
Autograft 4 8/8 100
others 4 6/6 100
Total 34 68/62 91. 1%

Revista Stomatologjike Shqiptare116
Fig, 5, 6. One year after surgery.
Fig7 Final result
Table3. Success rate according to implant diameter.
Summary and discussionThe maxillary sinus is connected to the nasal cavity
through one or two inferior nasal meatusin the upper 1/3 of the internal wall of the maxillary sinus. If the maxillary sinus is elevated excessively, this area may be exposed, and care must be taken to avoid this. After birth, the maxillary sinus enlarges continuously and comes to occupy much of the maxilla. At adolescence, the maxillary sinus extends from the canine to the 3rd molar, and from the floor of the orbit superiorly to the root of the maxillary canine inferiorly. Consequently, the maxillary sinus interferes with implant placement near the maxillary canine. Therefore, implant placement requires elevation of the maxillary sinus mucosa.
Misch et al. 13) reported a 98% success rate for 170 implants with maxillarysinus grafts consisting of tricalcium
Implant diameter
Nr of patients
Nr of implants
Lost implants
2. 9 2 4 -
3. 25 2 4 -
3. 5 6 8 2
3. 75 2 10 -
3. 8 12 22 2
4. 0 6 10 2
4. 5 6 6 -
5. 0 2 2 -
6. 0 2 2 -
Total 68 6
Implant length
Nr. of patients
Nr of implants
Lost ImplantsSuccs
10 20 28 2
11. 5 9 16 2
12 9 12 2
13 4 8 -
14 - - -
15 1 4 -
Percent 100% 8. 8%
Total 68 6
Table 4. Success rate according to implant length
Table2. Success rate according to elapsed time
Time in months Nr of implants Lost implants
Less then 5 months 10 4
6 8 2
7 8 -
10 12 -
12 30 -

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 117
phosphate mixed with demineralized bone and blood. Autogenous bone can be used for sinus grafting.
Heterologous, allogenic, or synthetic bone used alone or in combination is effective implant material depending on the clinical situation14). The block pattern and particle shape were seen in 80. 4% and 94. 83% of grafts, respectively, and the particle pattern had a higher implant success rate15). Autogenous bone is the gold standard for bone grafting in the oral cavity because of its osteoconduction and osteo-induction properties16). However, it has several shortcomings, including the additional hospital stay required for collecting extraoral bone, the need for a second surgery, and repneumatization of the maxillary sinus caused by resorption of the bone graft.
Consequently, the use of bone substitutes is increasing10). Allografts include cortical or spongiose bone and are mainly obtained from cadavers or other donors. The bone is sterilized and stored in a bone bank. Technical problems are relatively requent, and include the accuracy required to place the graft mass to the donor area, the need for firm fixation for successful fusion with the host bone, infection, non-union, and the possible fracture of the allograft. Allograft bone is not osteogenic, and when used in combination with autologous bone, osteogenesis is slower than when using autogenous bone alone.
Synthetic grafts are natural products orsynthetic materials, and heal exclusively via osteoconduction. Such graft materials serve as scaffolds to accelerate the repair and growth of bone tissues. using allogenic bone or synthetic graft materials in combination with autologous bone for maxillary sinus grafts decreases the amount of autogenous bone needed, although osteogenesis may be insufficient or slow17). The appropriate treatment method should be chosen after considering the advantages and shortcomings of autogenous and non autogenous bone
grafts. The advantages of non autogenous bone are that no additionous surgery in another area is required, the postoperative infection rate is reduced, and the grafted bone is not resorbed during the healing period. Its shortcomings are that a longer bone regeneration period is required, and precise surgical techniques and appropriate selection of implant material are required to obtain the best result. The advantages of autogenous bone graft are that the period of bone regeneration is shorter than with a non-autogenous bone graft and the cost of non-autologous implant materials is avoided. The shortcomings are that additional surgery is required and slight bone loss occurs during the healing period18). Recent studies have failed to detect significant associations between implant materials and the incidence of complications in maxillary floor elevation, and new bone developed within 6 months on average. In addition, no radiological differences were detected comparing autogenous bone alone to autogenous bone in combination with synthetic grafts19).
ConclusionsMaxillary mucosa elevation surgery was performed with
xenogenic, allogenic, synthetic, and autogenous bone grafts, and 68 implants were placed. At the last follow-up, 62 implants remained attached to the upper prosthesis with no radiological or clinical signs of inflammation or mobility, and the patients could chew successfully, for an 91. 2% success rate. 1. For xenograft +autograft , the success rate was 91. 6%
(24/22). 2. The most common implant diameters were 3. 8, 4. 0
and 4. 5 mm and the success rate was 89. 4%3. Implants of 10 mm in length were used most frequently,
and the overall success rate was 91. 1% (62/68).
1. Wheeler Sl, Holmes RE, Calhoun CJ. Six-year clinical and histologic study of sinus-lift grafts. Int J oral Maxillofac Implants 1996;11: 26-34.
2. Butz SJ, Huys lW. long-term success of sinus augmentation using a synthetic alloplast: a 20 patients, 7 years clinical report. Implant Dent 2005;14: 36-42.
3. Krauser JT, Rohrer MD, Wallace SS. Human histologic and histomor-phometric analysis comparing osteoGraf/N with PepGen P-15 in the maxillary sinus elevation procedure: a case report. Implant Dent 2000;9: 298-302.
4. Tadjoedin ES, de lange Gl, Bronckers Al, lyaruu DM, Burger EH. De-proteinized cancellous bovine bone (Bio-oss) as bone substitute for sinus floor elevation. A retrospective, histomorphometrical study of five cases. J Clin Periodontol 2003;30: 261-270.
5. Wallace SS, Froum SJ, Cho SC, Elian N, Monteiro D, Kim BS, Tarnow DP. Sinus augmentation utilizing anorganic bovine bone (Bio-oss) with absorbable and nonabsorbable membranes placed over the lateral window: histomorphometric and clinical analyses. Int J Periodontics Restorative Dent 2005;25: 551-559.
6. Hurzeler MB, Kirsch A, Ackermann Kl, Quinones CR. Reconstruction of the severely resorbed maxilla with dental implants in the augmented maxillary sinus: a 5-year clinical investigation. Int J oral Maxillofac Im-plants 1996;11: 466-475.
7. Tatum oH Jr, lebowitz MS, Tatum CA, Borgner RA. Sinus augmenta-tion. Rationale, development, long-term results. N Y State Dent J 1993; 59: 43-48.
8. Boyne PJ, James RA. Grafting of the maxillary sinus floor with autog-enous marrow and bone. J oral Surg 1980;38: 613-616.
9. Wallace SS, Froum SJ, Tarnow DP. Histologic evaluation of a sinus el-evation procedure: a clinical report. Int J Periodontics Restorative Dent 1996;16: 46-51.
10. Del Fabbro M, Testori T, Francetti l, Weinstein R. Systematic reviewof survival rates for implants placed in the grafted maxillary sinus. Int J Periodontics Restorative Dent 2004;24: 565-577.
11. Kahnberg KE, Nystrom E, Bartholdsson l. Combined use of bone grafts and Branemark fixtures in the treatment of severely resorbed maxillae. Int J oral Maxillofac Implants 1989;4: 297-304.
12. Kim SG. Sinus Bone Graft, Narae Publishing Inc, 2004. 13. Misch CE. Maxillary sinus augmentation for endosteal implants: orga-
nized alternative treatment plans. Int J oral Implantol 1987;4: 49-58. 14. Jensen oT, Shulman lB, Block MS, Iacono VJ. Report of the Sinus Con-
sensus Conference of 1996. Int J oral Maxillofac Implants1998;13: 11-45.
15. Wallace SS, Froum SJ. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann Peri-odontol 2003;8: 328-343.
16. Schlegel KA, Fichtner G, Schultze-Mosgau S, Wiltfang J. Histologic findings in sinus augmentation with autogenous bone chips versus a bovine bone substitute. Int J oral Maxillofac Implants 2003;18: 53-58.
17. Garg AK. Bone Biology, Harvesting, and Grafting for Dental Implants. 1st edition, 2005.
18. Fugazzotto PA, Pikos MA. Guided bone regeneration and sinus aug-mentation in the absence of autogenous bone grafting. Implant Dent 2001;10: 158-161.
19. Barone A, Santini S, Sbordone l, Crespi R, Covani u. A clinical study of the outcomes and complications associated with maxillary sinus.
REFERENCES

Revista Stomatologjike Shqiptare118
Hyrje Sot është koha e Dentistrisë Estetike. Individët që
janë të pashëm në paraqitje janë më të lumtur. Ata janë më të sigurtë në vetvete,të sjellshëm, miqësor, dhe rrjedhimisht më te suksesshëm në karrierën e tyre. Për të realizuar pikat e lart përmëndura duhet të kujdesemi të kemi ose të kërkojme buzëqeshje të bukura. Ka shumë komponent interaktiv që ndikojnë në një buzëqeshje të bukur: koka, qafa dhe fytyra ; struktura të veçanta të fytyrës; forma, funksioni dhe gjëndja e indeve të buta të një të tretës së poshtme të fytyrës, veçanërisht buzet; ndërtimi dhe shëndeti i gingivave; dhe e fundit,por jo më pak e rëndësishmje; denticioni si një trup i vetëm dhe forma,gjëndja,ngjyra,funksioni, dhe mardhënia e dhëmbëve të veçantë. T’i krijosh një pacienti një buzëqeshje të bukur, bën të lumtur jo vetëm pacientin por njëkohësisht inkurajon edhe të tjerët përqarkë të buzëqeshin. Dizenjimi i buzëqeshjeve të bukura ka qënë një sfidë për vite me radhë dhe “shpikja” e fasetave ka qënë një ndër pikat kyce të kësaj sfide.
Në 1937 u “zbulua” aplikimi i fasetave në dhëmbët anterior nga Dr. Pincus(1), por më popullor u bë nga mesi i viteve 70 duke përdorur tre mënyra kryesore: bondimi direkt duke përdorur kompozite rezinoze, faseta kompoziti të para fabrikuara, dhe faseta intirekte porcelan të punuara në laborator(2).
Nga fund i viteve 70 dhe fillimi i viteve 80 kjo teknikë u ndoq dhe u përmirësua më tej nga l.Rochette(3).
Stomatologjia ka ndryshuar rrënjësisht këto 30 vitet e fundit dhe ky ka qënë një ndryshim i karakterizuar nga faktor të ndryshëm. Siç e dimë ka mënyra të ndryshme për të krijuar një buzëqeshje të bukur, si psh: përdorimi i kurorave të plota metal-porcelan, restaurimet komplet porcelan, si edhe teknika të tjera direkte.Kurorat tradicionale metal-qeramikë kanë një histori suksesi të qëndrueshme, por lënë për të dëshiruar në aspektin
estetik.Rritja e kërkesës nga ana e pacientëve për një buzëqeshje sa më estetike, ka çuar në zhvillimin
e sistemeve të përpunimit të qeramikës. Restaurimet estetike direkte kërkojnë aftësi teknike
të kombinuara me aftësi krijuese dhe artistike. Kjo kërkon një kohë të konsiderueshme në poltronin e dentistit. Teknikat indirekte të cilat kërkojnë proçedura laboratorike kanë aftësinë të përmirësojnë estetikën dhe të krijojnë restaurime jetëgjata. Në krahasim me teknikën direkte, teknika indirekte tradicionalisht kërkon më shumë preparim të dhëmbit për të krijuar hapsirën e nevojshme për trashesinë e materialit si dhe për të parandaluar mbikonturimin. Gjithashtu këto restaurime kanë një kosto të shtuar dhe kanë nevojë për të paktën dy seanca klinike, restaurime provizore dhe tarifën shtesë të laboratorit.
Përdorimi i fasetave këto vitet e fundit është bërë e modës dhe pacientët së bashku me stomatologun duhet të zgjedhin midis fasetave të porcelanit dhe atyre të kompozitit. Nëse përdoret teknika indirekte duhet të marrim në konsideratë kostot e shtuara të këtyre restaurimeve dhe kohën e shpenzuar për ti përgatitur ato. Megjithëse nuk kemi evidenca klinike të përshtatshmërisë së kompozitëve të përdorur në mënyrë indirekte, gjenerata e fundit e kompozitëve që përdoret në mënyre indirekte në dhëmbët anterior shfaq disa karakteristika interesante si: rezistencë mekanike adekuate ndaj stresit, estetikë ekselente, dhe të lejon riparimin intraoral(4).
Në ditët e sotme teknikat direkte janë përmirësuar ndjeshëm me gjeneratën e re të kompozitëve, duke na dhënë ne mundësinë për të përdorur sistemin e fasetave të kompozitit të parafabrikuara. Këto lloj fasetash janë zbuluar rreth 35 vjet më parë duke përdorur matriksin e metil-metakrilatit dhe grimcat mbushëse të mëdha si në rastin e kompoziteve rezinoze, por me sukses
AbstraktQëllimi i studimit: Ky artikull fokusohet mbi përdorimin e fasetave të parafabrikuara të kompozitit me grimca nano-hibride në një nga indikacionet e tyre si: mbyllje ose minimizim diasteme dhe rikthim e përmirësim te estetikes. Materiali dhe Metoda: Sistemi CoMPoNEER është një klasë e re fasetash direkte kompoziti, me avantazhe të dyaneshme. Trashësia prej 0,3mm lejon preparim minimal, duke i bere këto faseta minimalisht invasive.Konkluzione: Kjo teknike trajtimi rezultoi e përballueshme financiarisht për të rikthyer estetikën. Kryhet në një seancë, shmang laboratorin, shumë komode per mjekun dhe pacientin. Si me te gjitha teknikat e reja duhet kohe per të konfirmuar efikasitetin si një zgjidhje afatgjatë.
1 Stela panteqi, 2adem alushi, 3orges Simeon
mbyllja e diastemës nëpërmjet përdorimit të fasetave të gatshme të kompozitit. (Raportim rasti)
1,2,3Fakulteti i Shkencave Dentare, Universiteti Aldent 2Fakulteti i Mjekësisë Dentare, Universiteti i Mjekësisë
Falë kyçe:
Faseta,
Kompozit,
Estetikë

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 119
të limituar për shkak të kufizimeve teknologjike dhe pranisë së poroziteteve në sipërfaqe(5). Me avancimin e teknologjisë, ne tani kemi një klasë të re të fasetave të kompozitit të parafabrikuara me karakteristika të përmirësuara.
Fasetat e kompozitit të parafabrikuara janë prezantuar së fundmi nga Coltene. Këto guaska kompoziti të holla (0,3mm cervikalisht dhe 0,6-1mm në buzën prerëse), janë të prodhuara nga kompozit nano-hibrid i parapolimerizuar Synergy D6 (Coltene). Çementimi i tyre realizohet me të njëjtin kompozit me të cilin ato janë prodhuar gjë që e bën restaurimin një trup të vetëm pas çementimit. Këto faseta mund të përshtaten dhe ngjiten direkt në sipërfaqen e dhëmbit duke përdorur kompozitin hibrid. one-Coat Bond (Coltene), është adezivi i dentinës i përfshirë në sistem i cili përdoret për ngjitjen e guaskave të parafabrikuara në sipërfaqën e dhembit.
PREZANTIM RASTIDiagnoza klinikeMarrja e anamnezës duhet të përfshijë informacione
esenciale si: emri, gjinia, datëlindja, adresa, kontakti, përfshirë këtu edhe ndonjë informacion të veçantë për persona me aftësi të kufizuara. Qëllimet e Dentistrisë
Estetike janë si më poshtë:1. Të plotësojë pritshmëritë reale të pacientëve.2. Të ofrojë stabilitet estetik dhe funksional për një kohë
të gjatë.3. Të arrijë qëllimet e trajtimit nëpërmjet aplikimit të
metodave minimalisht invasive.
Për të përmbushur këto qëllime dentisti duhet të mbledhë të gjithë informacionin e nevojshëm të historisë mjekësore të pacientit dhe të dëgjojë në mënyrë të kujdesshme ankesat dhe shqetësimet e pacientëve në mënyrë që të gjitha problemet e ngritura nga pacienti të jenë lehtësisht të investigueshme.
Sipas Chalifoux (6) ka tre kategori anomalish në Estetikën dentare të cilat e shtyjnë pacientin të kërkojë ndërhyrje estetike. Këto janë:• Ngjyra• Pozicioni• Forma
Përveç këtyre tre anomalive në rutinën dentare, ne ndeshemi edhe me sfida të tjera si:• Të zgjasim dhëmbët anterior• Të korigjojmë dhëmbët e keqpozicionuar• Të maskojmë ngjyrimet• Të mbyllim ose minimizojmë diastemat• Të restaurojmë lezionet karioze me shtrirje të gjërë
dhe dhëmbët e frakturuar• Të korigjojmë restaurimet e mëdha e të vjetra në
dhëmbët anterior.Kur të gjitha mundësitë tjera të trajtimit janë të
pa aplikueshme për pacientin për arsye nga më të ndryshmet, ne rekomandojmë fasetat e kompozitit të parafabrikuara.
Qëllimi i këtij artikulli është të përshkruaj një nga këto sfida siç është minimizimi ose mbyllja e një diasteme dhe rikthimi i një pamje sa më estetike të dhëmbëve anterior.
Rasti klinikPacientja E.N, 34 vjeç, paraqitet në klinikë me ankesën
kryesore mbi praninë e diastemës së theksuar dhe pozicionin e centralëve të saj maksilar (Fig. 1).
Fig 1. Pamje preoperative me hapës goje. Vërejmë praninë e diastemës.
Një ekzaminim klinik i kujdesshëm na paraqet një paciente me higjenë orale shumë të mirë. Centralët e saj maksilar ishin te shëndetshëm pa asnjë mbushje kështu që mundësitë e trajtimit ishin të lehta për tu diskutuar. Për shkak të kufizimeve financiare fasetat e kompozitit të parafabrikuara u zgjodhën si trajtimi më i përshtatshëm. u përcaktua të aplikohen dy faseta në incizivët central maksilar për të minimizuar diastemën dhe për të korrigjuar keqpozicionimin. Përmasa “l” u zgjodh me ndihmën e “Contour guide”(Fig. 2), A2/B2 u zgjodh si ngjyra e përshtatshme e dentinës dhe Enamel universal u zgjodh si ngjyra e përshtatshme e smaltit. Këto ngjyra u përcaktuan duke përdorur çelësin e ngjyrave Synergy D6 (Fig. 3).
Fig 2. Çelësi i madhësisë Componeer

Revista Stomatologjike Shqiptare120
Fig 3. Çelësi i ngjyrave Componeer
Pas preparimit të dhëmbit, 2 faseta kompoziti të parafabrikuara u pershtatën me disk abraziv (SëissFlex, Coltene) dhe u provuan mbi dhëmb për të kontrolluar përputhjen e madhësisë dhe formës. Acidi fosforik 35% u përdor për të acidifikuar sipërfaqen e dhëmbit dhe “one coat Bond” u përdor si sistemi adeziv i përfshirë në sistemin Componeer. Pas vendosjes së fillit retraktues, fasetat u çementuan me të njëjtin kompozit hibrid me të cilin janë prodhuar. (Fig. 4).
Fig 4. Pamje postoperative. Vendosja e 2 fasetave mbi dy centralët maksilar duke mbyllur diastemën.
Stripsat abraziv u përdorën për lëmimin e sipërfaqeve proksimale, ndersa disqet abrasive fleksibël (3M/ESPE) u përdorën për margon incizale.
Diskutime Fasetat e kompozitit të para-fabrikuara janë në
dispozicion në ngjyra dhe madhësi të ndryshme të cilat përputhen me kërkesat e pacientëve. Një nga avantazhet kryesore të këtyre fasetave është nevoja e vetëm një vizite tek dentisti, e cila ul koston shtesë për restaurimet e përkohshme dhe/ose proçedurat laboratorike. Fasetat janë lehtësisht të lëmueshme dhe mund të riparohen brënda në gojë. Megjithatë ka ende nevojë për të kryer
studime shtesë për vetitë mekanike dhe estetike të këtyre fasetave ndërkohë që teknologjia përmirësohet çdo ditë, sidomos duke krahasuar fasetat direkte me ato indirekte si dhe materialet e ndryshme që përdoren për të krijuar ato.
Një studim vlerësoi 318 faseta porcelani në 84 pacientë mbi 10 vjet. Fasetat e porcelanit ofrojnë një restaurim të parashikueshëm dhe të suksesshëm me një probabilitet mbijetese të vlerësuar prej rreth 93,5% mbi 10 vjet. Normat e dështimit të rritura në mënyrë të konsiderueshme ishin të lidhura me bruksizmin dhe jovitalitetin e dhëmbëve, dhe njollat marginale ishin më të theksuara në pacientët duhanpirës (7).
Megjithatë lloji dhe vendndodhja e restaurimit janë faktorët përcaktues për integritetin marginal (8).
Një tjetër arsye përse fasetat e para-fabrikuara janë shpesh një zgjedhje shumë e mirë trajtimi është për shkak se pavarësisht se janë një alternativë më pak e shtrenjtë se porcelani, nga pikëpamja biologjike materialet me bazë rezinoze e konsumojnë më pak smaltin antagonist se sa porcelani, nje tregues ky mjaft i rëndësishëm per këte material ( 9).
Shumë studime individuale kanë vlerësuar mbijetesën e vetëm të fasetave të porcelanit ose vetëm të fasetave të kompositit, pa krahasuar performancën e tyre në të njëjtën gojë. Nuk ka asnjë evidencë të besueshme për të treguar një avantazh ose perfitim të një lloji të restaurimit me faseta (direkt ose indirekt) në lidhje me llojin tjetër të fasetave për sa i perket jetëgjatësisë se restaurimit (10).Gjithashtu ka shumë pak informacion në lidhje me mbijetesën afatgjatë të sistemeve të ndryshme të fasetave indirekte (11).
Teknika dhe materialet e përshkruara në këtë punim mbeten një mundësi shumë e mirë për pacientët tanë. Kjo teknike mund të përdoret për të mbyllur ose minimizuar diastemat, për të rifituar simetrinë dhe formën e dhëmbëve frontal, për të rivendosur një pamje jetike të dhëmbëve jo vitale si dhe për të drejtuar dhëmbët e keqpozicionuar. Ky sistem, nëse përdoret siç duhet, në përputhje me udhëzimet e tij, mund të arrijë rezultate shumë të mira në Dentistrine Estetike dhe Restorative të cilat mund të jenë të dobishme si për dentistët ashtu dhe pacientët.
KonkluzioniKjo teknikë e re e trajtimit rezultoi të jetë një mënyrë
mjaft e volitshme për të rifituar estetikën. Dentisti mund ta përdorë këtë teknikë në një numër të gjerë rastesh. Një nga avantazhet kryesore të këtyre fasetave është nevoja e vetëm një vizite tek dentisti, e cila ul koston shtesë për restaurimet e përkohshme dhe/ose proçedurat laboratorike, gjë që e bën atë shumë të rehatshme si për dentistin ashtu dhe për pacientin. Si me të gjitha teknikat e reja, ka ende shumë rrugë përpara, për të konfirmuar efektivitetin e saj si një zgjidhje afatgjatë në Dentistrinë Estetike.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 121
1. Pincus Cl. “Building mouth personality”. A paper presented at: California State Dental Association, 1937:San Jose, Cali-fornia.
2. Faunce FR, Myers DR. laminate veneer restoration of per-manent incisors. JADA 1976;93:790–792.
3. A ceramic restoration bonded by etched enamel and resin for fractured incisors Dr.Sc.odont., M.D. Alain l. Rochette 16 Ave. Paul Doumer 83700 Saint Raphael France
4. The use of indirect composite veneers to rehabilitate pa-tients with dental erosion: a case report. European Journal of Esthetic Dentistry. Autumn2013, Vol. 8 Issue 3, p414-431. 18p. 44 Color Photographs, 6 Black and White Photographs.
5. Jensen o.E., Soltys, J.l. “Six month clinical evaluation of prefabricated veneer restorations after partial enamel re-moval.” J oral Rehab 1986;13:49–55
6. Narin H. F. Wilson. Essentials of Esthetic Dentistry, Principles and practice of Esthetic Dentistry. Vol.1. pg.50.
7. Clinical performance of porcelain laminate veneers for up to 20 years,Beier uS, Kapferer I, Burtscher D, Dumfahrt HInt J Prosthodont, 2012.
8. The 5-year clinical performance of direct composite addi-tions to correct tooth form and position. I. Esthetic quali-ties Peumans M, Van Meerbeek B, lambrechts P, Vanherle G Article Clin oral Investig, 1997
9. Krämer N1, Kunzelmann KH, Taschner M, Mehl A, Garcia-Godoy F, Frankenberger R. Antagonist enamel wears more than ceramic inlays. J Dent Res.2006 Dec; 85 (12):1097-100
10. Wakiaga J1, Brunton P, Silikas N, Glenny AM. Direct versus indirect veneer restorations for intrinsic dental stains. Co-chrane Database Syst Rev. 2004;(1):CD004347
11. RoeteMeijering AC1, Creugers NHrs FJ, Mulder J. Survival of three types of veneer restorations in a clinical trial: a 2.5-year interim evaluation.J Dent. 1998 Sep;26(7):563-8.
REFERENCA

Revista Stomatologjike Shqiptare122
IntroductionEsthetic dentistry is here to stay. Individuals who are
beautiful are happier, and they are more confident, kind, friendly, popular, and successful than their less attractive peers. Having or acquiring an attractive smile can make an important contribution to realizing this goal. There are many interactive components to an attractive smile: the head, neck and face in which it is set; facial structures and features; the nature, form, functions and condition of , in particular, the soft tissues of the lower third of the face, specifically the lips; the architecture and health of the gingival tissue; and last, but by no means least , the shapes, condition, shades, relationships and function of individual teeth, and the dentition as a whole. Giving an individual a smile that is beautiful, makes the patient happy, and encourages others to smile, is what Esthetic Dentistry should aim to achieve.
Designing beautiful smiles has been a challenge for many years and the “invention” of dental veneering has been a crucial feature of this challenge. While the “invention” of veneering anterior teeth by Dr. Pincus (1) was presented in 1937, it became more popular in the mid-seventies, using three different approaches: direct bonding using resin composites, prefabricated composite veneers and indirect, custom-made porcelain veneer (2).
In the late 1970, early 1980s this technique was followed and improved by l Rochette (3)
Dentistry has changed dramatically over the past 30 years. It has been an evolutionary development catalysed by various factors. As we already know there are lots of other options for achieving a beautiful smile such as: full metal-ceramic restorations, all-ceramic restorations and other direct techniques.
Traditional metal-ceramic restorations have predictable strength and a history of long term success, but typically less than ideal esthetics. The increasing demand from patients for improved esthetics has driven the development of all ceramic systems.
Direct esthetic restorations require careful techniques combined with creative and artistic skills. This involves considerable chairside time. Indirect techniques using laboratory manufactured restoration outsource the skills to provide an esthetic restoration, and may improve the long term esthetics and performance. In comparison to direct procedures, indirect approaches traditionally require more tooth preparation to create the space required for the necessary thickness of material and to prevent over contouring. There is also the added cost of these restorations given the need for at least 2 appointments, temporary restorations and the laboratory fee.
Veneering is the trend of these last years and both professionals and patients have to choose between ceramic veneers and composite veneers. If the indirect technique is used we do have to consider the extra cost of these restorations and also the time spent to prepare them.
Even though there is no clinical evidence of the appropriateness of indirect composites in these treatments, the latest generation of composites used indirectly in the anterior teeth exhibits some interesting characteristics: it supports mechanical stress adequately, has an excellent esthetic result and can be repaired intra orally (4).
Nowadays, direct techniques have improved a lot with the new generation of composites giving us the possibility to use the pre-fabricated composite
AbstraCtObjective: This article is focused on the use of pre-fabricated nano-hybrid-composite veneers to close or minimize diastema in order to enhance esthetics.Clinical consideration: CoMPoNEER system is a new class of direct composite veneers. They are polymerized, composite enamel-shells, which combine the advantages of direct restorations with those of lab-made veneers.The extremely thin veneer (0.3 mm) allows a high level of conservation of hard tooth substance during preparation.Conclusions: This treatment is an affordable way to regain esthetics. It’s a one session treatment, very comfortable for dentist and patients. As with all new techniques, there’s still a lot to be done, to confirm its effectiveness as a long term solution.
1msc Stela panteqi, 2prof.Dr. adem alushi, 3msc orges Simeon
Diastema closure by using pre-fabricated composite veneers. (Case report)
1,2,3Fakulteti i Shkencave Dentare, Universiteti Aldent 2Fakulteti i Mjekësisë Dentare, Universiteti i Mjekësisë
key woRDS:
Veneers,
Composite,
Esthetics

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 123
veneer systems. This kind of veneers (Mastique®, Caulk) was explored about 35 years ago, using a methyl-methacrylate matrix and large glass fillers, such as used in resin composites but with limited success due to technological limitations and poor surface qualities (5).
As technology improves everyday we now have a new class of pre-fabricated composite veneers with improved properties.
Pre-fabricated composite veneers have been recently introduced. Componeer. (Coltene, Altstatten,Swisterland) pre- fabricated veneers are thin composite shells (0,3 mm cervically and 0,6-1 mm to the incisal edge). These prefabricated veneers are made of pre-polymerized nano-hybrid composite resin, Synergy D6 (Coltene). The veneers are cemented with the same hybrid composite resin that they are made from, which has the potential of making the complete restoration as a mono block unit. These veneers can be trimmed and bonded to the tooth structure using direct hybrid composite resin. one-Coat Bond (Coltene), is the dentine adhesive included in the system, which is used to bond the prefabricated composite shells to the tooth structure, using an etch and rinse bonding strategy.
CASE PRESENTATIONClinical diagnosisThe taking of a patient history should include
recording essential data such as name, gender, date of birth, address and contact details, together with any information in respect of special needs when attending for dental care. • The goals of esthetic dental care include the
following:• Meet the realistic expectations of the patients• obtain long term functional and esthetic
stability Achieve the treatment goals through the application
of minimal intervention approaches In order to fulfill these goals the professionals should
gather all the necessary medical patient history, listen attentively to the complaints and concerns of the patients so all the issues raised by the patient are fully investigated.
According to Chalifoux (6) there are three categories of “dental esthetic imperfections“that encourage patients to seek esthetic interventions. These relate to anomalies in tooth:• Color• Position• Shape
Besides these three main anomalies in our daily practice we face several challenges such as:
To lengthen anterior teethTo correct malpositioned teethTo mask discoloration To close or minimize diastemasTo restore extensive caries lesions and tooth fractureTo correct large, old anterior restorations.
When other treatment options are out of reach for the patient we recommend pre-fabricated composite veneers.
The purpose of this case report paper is to describe one of these challenges such as closing or minimizing diastema by giving the teeth an esthetic appearance.
Clinical CaseA 34 year-old female patient presented herself with a
major complaint about her diastema and the position of her maxillary central incisors. (Figure 1).
Fig.1. Preoperative retracted view. Note the presence of the diastema.
A careful clinical examination revealed a healthy patient with a perfect oral hygiene. Her maxillary frontal teeth were intact without any restoration so the treatment options were easy to discuss. Due to financial limitations pre-fabricated composite veneers were chosen as the perfect option. It was decided to put two veneers on the maxillary central incisors to minimize the diastema and to align them both. Size “l” was chosen with the help of contour guide (Figure 2) and A2/B2 was chosen as the appropriate dentin shade, while the enamel shade was Enamel universal. These shades were determined by using Synergy D6 color guide (Figure 3).
Fig. 2. Componeer contour guide.

Revista Stomatologjike Shqiptare124
Fig. 3. Componeer Synergy D6 shade guide.
After tooth preparation, two pre-fabricated composite veneers were trimmed with abrasive discs ( SwissFlex, Coltene) and tried in to match the size and shape of the desired restoration. 35 % phosphoric acid was used to etch the tooth surface and one Coat Bond was used as the adhesive system included in the Componeer system. After the placement of the retraction cord, the veneers were cemented with the same hybrid composite resin that they are made from (Figure 4).
Fig 4 . Postoperative non-retracted view. Placement of two veneers on both maxillary central incisors to close the
diastema.
Finishing and polishing strips were used for interproximal areas and flexible abrasive discs (3M/ESPE) were used for the incisal edge.
Discussion Pre-fabricated composite veneers are available
in different shades and sizes which matches the requirements of the patients. one of the major
advantages of these veneers is the need of one-visit appointment, which lowers the extra cost for provisional restorations or laboratory procedures. They are easily finished and polished and can be repaired intra-orally. There is still need to perform additional studies for mechanical and esthetic properties of these veneers as technology improves every day especially comparing direct and indirect veneers and also different materials used to create them.
A study evaluated 318 ceramic veneers in 84 patients over 10 years. Porcelain laminate veneers offer a predictable and successful restoration with an estimated survival probability of 93.5% over 10 years. Significantly increased failure rates were associated with bruxism and nonvital teeth, and marginal discoloration was worse in patients who smoked (7).
However the type and location of the restoration are determining factors for marginal integrity (8).
Another reason why pre-fabricated composite veneers is often a very good treatment choice is because despite being a less expensive option than ceramics, from a biological point of view resin based materials wear the antagonist enamel less than ceramics do, indicating potential for this material (9).
A lot of individual studies evaluated the survival of either only ceramics or only resin composites as the laminate veneer material, without comparing their performance in the same mouth. There is no reliable evidence to show a benefit of one type of veneer restoration (direct or indirect) over the other with regard to the longevity of the restoration (10).
There is little information about long term survival of different indirect laminate systems (11).
The technique and materials described in this paper remains a pretty good option for our patients. It can be used to close diastemas, to regain symmetry of the shape of frontal teeth, to restore a vital look to non vital teeth, to align malpositioned teeth. This system if properly used, according to the system guidelines, can achieve very good results in Esthetic and Restorative Dentistry which can be useful for both professionals and patients.
Conclusion This new technique of treatment resulted to be
an affordable way to regain esthetics. It allows the practitioner to use this technique in a various number of cases. It is a one session treatment and requires no lab sessions, which makes it very comfortable for both dentist and patients. As with all new techniques, there is still a lot to be done, to confirm its effectiveness as a long term solution in Esthetic Dentistry.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 125
1. Pincus Cl. “Building mouth personality”. A paper presented at: California State Dental Association, 1937:San Jose, Cali-fornia.
2. Faunce FR, Myers DR. laminate veneer restoration of per-manent incisors. JADA 1976;93:790–792.
3. A ceramic restoration bonded by etched enamel and resin for fractured incisors Dr.Sc.odont., M.D. Alain l. Rochette 16 Ave. Paul Doumer 83700 Saint Raphael France
4. The use of indirect composite veneers to rehabilitate pa-tients with dental erosion: a case report. European Journal of Esthetic Dentistry. Autumn2013, Vol. 8 Issue 3, p414-431. 18p. 44 Color Photographs, 6 Black and White Photographs.
5. Jensen o.E., Soltys, J.l. “Six month clinical evaluation of prefabricated veneer restorations after partial enamel re-moval.” J oral Rehab 1986;13:49–55
6. Narin H. F. Wilson. Essentials of Esthetic Dentistry, Principles and practice of Esthetic Dentistry. Vol.1. pg.50.
7. Clinical performance of porcelain laminate veneers for up to 20 years,Beier uS, Kapferer I, Burtscher D, Dumfahrt HInt J Prosthodont, 2012.
8. The 5-year clinical performance of direct composite addi-tions to correct tooth form and position. I. Esthetic quali-ties Peumans M, Van Meerbeek B, lambrechts P, Vanherle G Article Clin oral Investig, 1997
9. Krämer N1, Kunzelmann KH, Taschner M, Mehl A, Garcia-Godoy F, Frankenberger R. Antagonist enamel wears more than ceramic inlays. J Dent Res.2006 Dec; 85 (12):1097-100
10. Wakiaga J1, Brunton P, Silikas N, Glenny AM. Direct versus indirect veneer restorations for intrinsic dental stains. Co-chrane Database Syst Rev. 2004;(1):CD004347
11. RoeteMeijering AC1, Creugers NHrs FJ, Mulder J. Survival of three types of veneer restorations in a clinical trial: a 2.5-year interim evaluation.J Dent. 1998 Sep;26(7):563-8.
REFERENCES

Revista Stomatologjike Shqiptare126
HyrjeQëllimi i një terapie të suksesshme endodontike
është pastrimi i plotë mekanik dhe kimik i të gjithë sistemit të kanalit te rrënjës dhe mbushja e tij e plotë me material mbushës inert. Së bashku me diagnozën dhe planifikimin e trajtimit, njohja e plotë e morfologjisë së kanalit të rrënjës dhe ndryshimi i saj është një kërkesë themelore për terapinë e suksesshme endodontike (1, 2). Kështu, njohja e morfologjisë së brendshme të sistemit të kanalit të rrënjës, është çështje jashtëzakonisht e rëndësishme, në lidhje me planifikimin dhe ekzekutimin e terapisë endodontike. Ndryshimet në anatominë e dhëmbëve gjenden në të gjitha grupet e dhëmbëve dhe njohja e këtyre ndryshimeve është çelësi i terapisë endodontike të suksesshme, pasi aftësia për të gjetur dhe trajtuar si duhet këto kanale mund të parandalojë dështimet e ardhshme (6). Molarët e parë maksilar janë veçanërisht të rëndësishëm për variacionet anatomike të kanalit të rrënjës. Forma më e zakonshme e molarit të parë maksilar është ajo me 3 rrënjë dhe 3 kanale. Sipas rishikimit të literaturës, molari i parë maksilar ka 3 rrënjë në 95.9% raste dhe 3 kanale në 56.8% dhe 4 kanale në 43.1% të rasteve respektivisht. Prezenca e kanalit të 4-t zakonisht raportohet në rrënjën meziobukale në 95.6% të rasteve (5, 6). Më pak ndryshime ndodhin në rrënjën distobukale dhe palatinale që përmbajnë 1 kanal në 98.3% dhe 99% të rasteve respektivisht. Dështimi i terapisë është për shkak të pranisë së kanalit të katërt
MB2, shtesë që nuk arrihet të zbulohet. Hess et al. (1925) tregoi praninë e 4 kanaleve në 54% të molarëve të parë maksilar (10). Wein et al. (1969) raportoi se incidenca e kanalit MB2 mund të jetë 62% në molarët e parë maksilar (4). Pineda dhe Kuttler (1972) raportuan një incidencë prej 51.5% të kanaleve shtesë në molarin e parë dhe të dytë (11). Anatomia kanalare është studiuar in vivo (metoda klinike) dhe in vitro (metoda laboratorike). Metodat in vivo përfshijnë trajtimin klinik të një dhëmbi, pasuar nga vlerësimi radiologjik i anatomisë së kanalit të rrënjës. Metodat in vitro përfshijnë vëzhgimin e drejtpërdrejtë, vëzhgimin mikroskopik, seksionet makroskopike, seksionet mikroskopike, dekalcifikimin, tomografi e kompjuterizuar me rreze konike. Në krahasimin e gjetjeve laboratorike dhe klinike, Seidberg et al. (1973) vuri në dukje një incidencë 62% kundrejt një incidence prej 33.3% të dy kanaleve në rrënjën meziobukale të molarëve të parë maksilar (3). Një ndihmë e rëndësishme për gjetjen e kanalit të rrënjës është mikroskopi dentar operativ (DoM), i cili u prezantua në endodonti nga Bauman në 1997 për të siguruar ndriçim dhe shikueshmëri më të madhe. Ai sjell detaje të vogla dhe një pamje të qartë (13). Teknika e kthjellimit të dhëmbëve është një tjetër metodë laboratorike për të analizuar anatominë kanalare. Avantazhi i kësaj metode është fakti se kjo metodë lejon vlerësimin e detajuar të kanaleve dhe komunikimin interkanalar në formë 3D (7). Weller et al (1995) studioi morfologjinë e rrënjës MB të
AbstraktHyrje: Trajtimi i suksesshëm endodontik përfshin diagnozë të saktë, njohje të mirë të parimeve biologjike dhe ekzekutim të shkëlqyer të trajtimit. Ndryshimet në anatominë e dhëmbëve gjenden në të gjitha grupet e dhëmbëve dhe njohja e këtyre ndryshimeve është çelësi i terapisë endodontike të suksesshme, pasi aftësia për të gjetur dhe trajtuar si duhet këto kanale mund të parandalojë dështimet e ardhshme.Qëllimi: Qëllimi i këtij studimi është të dallojmë karakteristikat anatomike të dhomës pulpare dhe të sistemit kanalar në molarin e parë maksilar në popullatën tonë dhe të krahasojmë rezultatet me studimet në vende të tjera.Materiali dhe metoda: Janë mbledhur në mënyrë rastësore 80 molarë të parë maksilar të hequr në Shërbimin e Kirurgjisë, pranë Klinikës Stomatologjike universitare, Tiranë. Dhëmbët u dekalcifikuan me acid nitrik 5% dhe u dehidruan me alkool me përqendrime të përshkallëzuara. u injektua ngjyra dhe morfologjia e kanalit të rrënjës u ekzaminua me stereomikroskop. Ky studim është bazuar në klasifikimin e Vertuccit.Rezultatet: Pas analizimit 90% e dhëmbëve rezultuan me tre rrënjë, nga të cilët 52.5% kishin tre kanale dhe 37.5% kishin 4 kanale. 10% e molarëve të parë maksilar rezultuan me dy rrenjë dhe tre kanale. Në këtë studim nuk u gjetën dhëmbë me 5 kanale. Kanali MB2 u gjet në 37.5% të rasteve.Konkluzioni. Rrënja mezio bukale shfaq një kompleksitet të morfologjisë kanalare. Tipi i parë u vu re në 35% të rasteve, tipi i dytë në 35% të rasteve, tipi i katërt në 20 % të rasteve, tipi i pestë në 3.75% të rasteve, tipi i gjashtë në 6.25 % të rasteve dhe tipi i shtatë në 1.25% të rasteve. Në rrënjën meziobukale u pa një foramen apikal në 70% të rasteve dhe dy foramen apikal në 30% të rasteve.Fjalët kyce: Sistemi kanalar, molari i parë maksilar, kanali i dytë meziobukal, indi pulpar.
Xhanina gavazi
morfologjia e sistemit kanalar në molarin e parë maksilar
Fakulteti i Mjekësise Dentare, Universiteti i Mjekësisë, Tiranë
Falë kyçe:
fëmijë,
dhëmbët e
qumështit,
higjena orale,
karies

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 127
molarit maksilar duke përdorur teknikën e kthjellimit të dhëmbëve dhe tregoi se 60% e rrënjëve meziobukale kishin 2 kanale me konfigurim të kanalit të tipit të 2-të.
Qëllimi i studimit: Qëllimi i këtij studimi in vitro është të dallojmë karakteristikat anatomike të dhomës pulpare dhe të sistemit kanalar në molarin e parë maksilar në popullatën tonë dhe të krahasojmë rezultatet me studimet në vende të tjera.
Materiali dhe metoda: Janë mbledhur 80 molarë të parë maksilar të hequr në Shërbimin e Kirurgjisë, pranë Klinikës Stomatologjike universitare, Tiranë. Dhëmbët u hoqën për karies të pa trajtuar, sëmundje periodontale, nga traumat ose për arsye protezimi. Kriteret e përzgjedhjes ishin: dhëmbë me kurorë intakte, rrënjë e formuar mirë dhe pa fraktura, pa rezorbim të brendshëm ose të jashtëm. Indet e buta të mbetura, fragmentet kockore, gurëzat u pastruan me kyreta.
Dhëmbët e përzgjedhur u shpëlanë në ujë të rrjedhshëm dhe u ruajtën në 5.25% hipoklorit natriumi për 30 min për heqjen e substancës organike. Dhëmbët u ruajtën në temperaturën e dhomës në formalinë 10% deri në momentin e përdorimit.
Për secilin dhëmb është bërë përgatitja e kavitetit hyrës duke përdorur freza të gjata rrumbullake diamanti
dhe orificiumet e kanaleve u lokalizuan. Më pas u vendosën në enë prej 5.25% hipoklorit natriumi për 24 orë për të hequr mbetjet organike. Protokolli i teknikës së kthjellimit u miratua nga një metodë e përshkruar më parë (7). Këto mostra u vendosën përsëri në acid nitrik 5% për dekalcifikim për 4 ditët e ardhshme në temperaturën e dhomës (Fig.1). Acidi nitrik u ndryshua çdo ditë. Për të parë shkallën e dekalcifikimit u përdor testi i gjilpërës dhe radiografia në seri (Fig.2, 3).Pas dekalcifikimit këto mostra u lanë dhe u dehidruan në alkool etilik 70%për 12 orë, pasuar nga alkool 90% për 1 orë dhe alkool etilik 100% shpëlarje për një orë secila. Mostrat duhet të vendosen në xylene për dy orë për t’u ngurtësuar para vendosjes në metil salicilat për t’i bërë ato transparente. Dhëmbët u vendosën në metil salicilat për 15-30 minuta për 3 ditë. Në fund të ditës së tretë këto dhëmbë bëhen plotësisht transparent. Më pas u injektua ngjyra e blu metilenit në kanalet e rrënjes me ndihmën e një gjilpëre 27-gauge. Pasi boja u tha morfologjia e kanalit të rrënjës u analizua për të regjistruar kanalet me stereomikroskop me zmadhim x 10. leximet u tabeluan dhe u analizuan duke përdorur softuerin SPSS (SPSS, Versioni 18.0, SPSS, Chicago, Il, uSA) SPSS.
Figura nr.1. Dhëmbët pas vendosjes në acid nitrik 5%.
Figura nr.3. Shkalla e dekalcifikimit në shkallën e dekalcifikimit. radiografi.
Figura nr. 4. Molari i parë maksilar Figura nr.5. Komunikimi ndër kanalar në rrënjën pas injektimit të bojës
meziobukale të molarit të parë maksilar.
Figura nr.2. Testi i gjilpërës për të parë

Revista Stomatologjike Shqiptare128
Tabela nr. 1 Numri i rrënjëve dhe kanaleve te rrënjes në molarin e parë maksilar.
Numri i rrënjëve në
molarin e parë maksilar
Numri i dhëmbëve
me 3 kanale%
Numri i dhëmbëve
me 4 kanale
%Numri i
dhëmbëve me 5 kanale
% Totali %
2 rrënjë 8 10% - - - - 8 10%
3 rrënjë 42 52.5% 30 37.5% - - 72 90%
Totali 50 62.5% 30 37.5% - - 80 100%
Tabela nr. 2 Tipet e ndryshme të konfigurimit të kanalit të rrënjës në molarin e parë maksilar.
Tipi i kanalitRrënja
meziobukalenr %
Rrënja distobukalenr %
Rrënja palatinalenr %
Rrënja meziobukale 2nr %
Tipi 1 28 35% 69 86.25% 77 96.25% - -
Tipi 2 28 35% 11 13.75% 3 3.75% 16 20%
Tipi 3 - - - - - - 14 17.5%
Totali me nje kanal në
apeks56 70% 80 100% 80 100% 30 37.5%
Tipi 4 16 20% - - - - - -
Tipi 5 3 3.75% - - - - - -
Tipi 6 4 5% - - - - - -
Tipi 7 1 1.25 - - - - - -
Totali me dy kanale në
apeks24 30% - - - - - -
Tipi 8 - - - - - - - -Totali me tre
kanale në apeks
- - - - - - - -
Totali 80 100% 80 100% 80 100% 30 37.5%
RezultatetPas analizimit me tre rrenjë rezultuan 90% e dhëmbëve
nga të cilët 52.5% kishin tre kanale dhe 37.5% kishin 4 kanale. 10% e molarëve të parë maksilar rezultuan me dy rrënjë dhe tre kanale. Në këtë studim nuk patëm dhëmbë me 5 kanale (Tabela.nr.1). Ekzaminimi i sistemit kanalar në këtë studim është bazuar në klasifikimin e Vertuccit. Rrënja meziobukale paraqet disa tipe të konfigurimit të kanalit të rrënjës. Tipi I u gjet në 35% të rasteve, tipi II në 35% të rasteve, tipi IV në 20 % të rasteve, tipi V në 3.75% të rasteve,tipi VI në 5 % dhe tipi i shtatë në 1.25% të rasteve. Në rrënjën meziobukale u pa një foramen apikal në 70% te rasteve dhe dy foramen apikale në 30% të rasteve (Tabela nr. 2). Kanali MB2 u gjet në 37.5% të rasteve. Rrënja distobukale në 86.2% të rasteve paraqet tipin e I-rë dhe në 13.8% tipin e II-të të konfigurimit të kanalit dhe në 100% ka një foramen apikal. Rrënja
palatinale në 96.3% paraqet tipin e parë të konfigurimit të kanalit dhe në 3.7% tipin e dytë të konfigurimit kanalar dhe ka një foramen apikal në 100% të rasteve (Tabela nr.1). Kanalet laterale u panë ne rrënjen meziobukale në të treten apikale në 15% të rasteve, dhe në të tretën e mesme ne 5% te rasteve (Tabela nr.3).
Në rrënjen distobukale, kanalet laterale u panë në 6.2% të rasteve në të tretën apikale dhe në të tretën e mesme në 1.2% te rasteve (Tabela nr.4). Në rrenjën palatinale,kanalet laterale u panë në të treten apikale në 13.7% të rasteve dhe në të tretën e mesme në 7.5% të rasteve (Tabela nr.5). Komunikimi ndër kanalar u pa në rrenjën meziobukale, në të tretën koronale në 8.75% te rasteve, në te tretën koronale dhe të tretën e mesme në 12.5% te rasteve, në të treten e mesme në 1.25% dhe në të tretën e mesme dhe të tretën apikale në 2.5% të rasteve (Tabela nr.6).

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 129
Tabela nr.3 Kanalet laterale në rrënjën meziobukale të molarit të parë maksilar.
Kanalet laterale në rrënjën
meziobukale
Numri i dhëmbëve
me 3 kanale
%Numri i
dhëmbëve me 4 kanale
%
Numri i dhëmbëve
me 5 kanale
% Totali %
Asnjë 38 47.5% 26 32.5% - - 64 80%
Në të tretën apikale 11 13.75% 1 1.25% - - 12 15%
Në të tretën koronare - - - - - - - -
Në të tretën e mesme 1 1.25% 3 3.75% - - 4 5%
Totali 50 62.5 30 37.5% - - 80 100%
Tabela nr.4 Kanalet laterale në rrënjën distobukale të molarit të parë maksilar.
Kanalet laterale në rrënjën
distobukale
Numri i dhëmbëve
me 3 kanale
%
Numri i dhëmbëve
me 4 kanale
%
Numri i dhëmbëve
me 5 kanale
% Totali %
Asnjë 48 60% 26 32.5% - - 74 92.5%
Në të tretën apikale 2 2.5% 3 3.75% - - 5 6.25%
Në të tretën koronale - - - - - - - -
Në të tretën e mesme - - 1 1.25% - - 1 1.25%
Totali 50 62.5% 30 37.5% - - 80 100%
Tabela nr. 5 Kanalet laterale në rrënjën palatinale të molarit tëe parë maksilar.
Kanalet laterale
në rrënjën palatinale
Numri i dhëmbëve
me 3 kanale%
Numri i dhëmbëve
me 4 kanale
%
Numri i dhëmbëve
me 5 kanale
% Totali %
Asnjë 40 50% 23 28.75% - - 63 78.75%
Në të treten apikale 7 8.75% 4 5% - - 11 13.75%
Në të tretën koronare - - - - - - - -
Në të tretën e mesme 3 3.75% 3 3.75% - - 6 7.5%
Totali 50 62.5% 30 37.5% - - 80 100%

Revista Stomatologjike Shqiptare130
Tabela nr.6 Komunikimi ndër kanalar në rrënjën meziobukale të molarit të parë maksilar
Koronale,në të tretën e
mesme dhe apikale
Tipi i parë
1 kanal
Tipi i dytë 2-1
kanale
Tipi i tretë 1-2-1
kanale
Tipi i katërt
2-2 kanale
Tipi i pestë
1-2 kanale
Tipi i gjashtë
1-2-1 kanale
Tipi i shtatë 1-2-1-2 kanale
Tipi i tetë
3 kanale
Totali
Asnjë 35% 20% - 11.25% 2.5% 6.25% - - 75%
Në të tretën koronare - 3.75% - 5% - - - - 8.75%
Koronare dhe të
tretën e mesme
- 10% - 1.25% 1.25% - - - 12.5%
Në të tretën e mesme - 1.25% - - - - - - 1.25%
Në të tretën e
mesme dhe të tretën apikale
- - - 2.5% - - - - 2.5%
Totali 35% 35% - 20% 3.75% 6.25% - - 100%
DiskutimeVariabiliteti i morfologjisë kanalare në dhëmbët
me shumë rrënjë paraqet një sfidë të vazhdueshme të diagnozës dhe trajtimit endodontik. Molari i parë maksilar konsiderohet si një dhëmb me tre rrënjë, rrenjen palatinale, distobukale dhe mezio-bukale. Në këtë studim, molari i parë maksilar rezultoi me tre rrënjë në 90% të rasteve nga të cilat 52.5% kishin tre kanale dhe 37.5% kishin 4 kanale. 10% e molarëve të parë maksilar rezultuan me dy rrënjë dhe tre kanale. Studimet e mëparshme gjithashtu raportuan incidencë të lartë të molarëve maksilar me tre rrënjë. Neg et al. raportoi se 100% e molarëve të parë maksilar kishin tre rrënjë në popullatën burmeze. (14, 15). Pecora et al. ka gjetur 86.4% me tre rrënjë, 7.9% me rrënjën bukale të bashkuar, 5% të rasteve rrënja linguale dhe distobukale shkrihen së bashku, dhe 0.7% e dhëmbëve me të gjitha rrënjët e bashkukara së bashku nga 140 molarë të parë maksilar. Thomas et al. raportoi se, nga 216 molarë maksilar 204 kishin tre rrënjë, 9 nga të cilat , rrënjët distobukale dhe palatinale ishin të bashkuara, dhe 3 nga të cilat rrënja distobukale dhe meziobukale janë të bashkuara.
Teknika e kthjellimit të dhëmbëve ka vlerë të konsiderueshme në studimin e anatomisë së sistemit të kanalit të rrënjës, sepse ndryshe nga imazhet radiografike, ajo siguron një pamje tre-dimensionale të kavitetit pulpar në raport me pjesën e jashtme të dhëmbit (7). llojet e kanaleve të vërejtura në rrënjën meziobukale janë komplekse. Tipi i I është parë në 35% te rasteve,tipi
i II në 35% të rasteve, tipi i IV në 20 % të rasteve, tipi i V në 3.75% të rasteve dhe tipi i VI në 6.25 % të rasteve. lloji i konfigurimit të kanalit të rrënjës meziobukale në studimin aktual tregon ngjashmëri të ngushtë me studimin e Shahriar Shahi et al. në një popullsi iraniane dhe raportoi tipin e I në (37.96%), tipin e II në (24.08%), tipin e IV në (24.18%), tipin e V në (9.5%), dhe tipin e VI në (4.38%) të konfigurimit kanalar (15, 16).
Në mënyrë të ngjashme, një studim i Wasti et al. të molarit të parë maksilar në popullsinë Pakistane të Azisë Jugore në 30 mostra raportuan se sistemi i kanalit të rrënjes në rrënjën meziobukale ishte tipi i I (33.3%), tipi i II (23.3%), tipi i IV (23.3%), tipi i V (13.3%), dhe tipi i VI (6.8%). Vertucci ka raportuar konfigurimin kanalar të 100 dhëmbëve molar të parë maksilar në rrënjën meziobukale, tipi i I (45%), tipi i II (37%), tipi i III (0) dhe tipi i IV (18%) të rasteve (19, 20).
Ndërkohë, Weine et al. raportoi 30.4% nga 293 molarë të parë maksilar dhe Alavi et al. raportoi 44.2% nga 52 molarë të parë maksilare të tipit IV. Kjo përqindje më e lartë e tipit IV konsiderohet një tip i popullsisë Mongoloide (13).
KonkluzioneDivergjenca raciale mund të jetë e pergjegjshme për
variacione të tilla. Studime të mëtejshme me kampione më të mëdha në numër nevojiten për të bërë një përshkrim më preciz të anatomisë kanalare.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 131
1. Vertucci FJ. Root canal morphology and its relationship to end-odontic procedures. Endodontic Topics. 2005; 10 (1):3–29.
2. Neelakantan P, Subbarao C, Ahuja R, Chandragiri VS, Gut-mann Jl. Cone-beam computed tomography study of root and canal morphology of maxillary first and second molars in an Indian population. J Endod. 2010; 36:1622–7.
3. Alavi AM, opasanon A, Ng Yl, Gulabivala K. Root and canal morphology of Thai maxillary molars.Int Endod J. 2002;35(5):478–85.
4. Weine FS, Hayami S, Hata G, Toda T. Canal configuration of the mesiobuccal root of the maxillary first molar of a Japa-nese sub-population. Int Endod J. 1999;32(2):79–87.
5. lee K-W, Kim Y, Perinpanayagam H, lee J-K, Yoo Y-J, lim S-M, Chang SW, Ha B-H, Zhu Q, Kum K-Y. Comparison of Alterna-tive Image Reformatting Techniques in Micro–Computed Tomography and Tooth Clearing for Detailed Canal Mor-phology. J Endod. 2014;40(3):417–22.
6. okumura T. Anatomy of root canals. Tokyo Dental College; 1927.
7. Robertson D, leeb IJ, McKee M, Brewer E. A clearing technique for the study of root canal systems. J En-dod. 1980;6(1):421–4.
8. Thomas RP, Moule AJ, Bryant R. Root canal morphology of maxillary permanent first molar teeth at various ages. Int Endod J. 1993;26:257–67.
9. Cleghorn BM, Christie WH, Dong CS. Root and root canal morphology of the Human permanent maxillary first molar; a literature review. J Endod. 2006;32:813–21.
10. Hess W, Zu¨rcher E. The Anatomy of Root Canals of the Teeth of the Permanent and Deciduous Dentitions. New York: William Wood & Co, 1925.
11. Pineda F, KuĴ ler Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root ca-nals. oral Surg oral Med oral Pathol 1972;33:101-10. 9.
12. Pomeranz HH, Fishelberg G. The secondary mesiobuccal canal of maxillary molars. J Am Dent Assoc 1974;88:119-24.
13. Weine FS. Endodontic Therapy, 5th edn. St louis: Mosby-Yearbook Inc., 1996: 243.
14. Stropko JJ. Canal morphology of maxillary molars, clinical observations of canal configurations. J Endod 1990: 25: 446–450.
15. Baldassari-Cruz lA, lilly JP, Rivera EM. The influence of dental operating microscopes in locating the mesiolingual canal orifices. oral Surg oral Med oral Pathol oral Radiol Endod 2002: 93: 190–194.
16. Coelho de Carvalho MC, Zuolo Ml. orifice locating with a microscope. J Endod 2000: 26: 532–534.
17. Go¨rduysus Mo, Gorduysus M, Friedman S. operating mi-croscope improves negotiation of second mesiobuc cal canals in maxillary molars. J Endod 2001: 27:
18. Kerekes K, Tronstad l. Morphometric observations on root canals of human molars. J Endod 1977: 3: 114–118.
19. Schwarze T, Baethge C, Stecher T, Geurtsen W. Iden-tification of second canals in the mesiobuccal root of maxillary first and second molars using magnify-ing loupes or an operating microscope. Aust Endod J 2002: 28: 57–60.
20. Buhrley lJ, Barrows MJ, BeGole EA, Wenckus CS. Effect of magnification on locating the MB2 canal in maxillary mo-lars. J Endod 2002: 28: 324–327.
REFERENCA

Revista Stomatologjike Shqiptare132
IntroductionThe aim of successful endodontic therapy is the
complete mechanical and chemical cleaning of the entire root canal system and its full filling with inert filler material. Along with diagnosis and treatment planning, a full knowledge of root canal morphology and its variations is a fundamental requirement for a successful endodontic therapy (1.2). Thus, the recognition of the internal complex morphology of the root canal system is an extremely important issue regarding the planning and application of endodontic therapy. Dental anatomy variations are found in all dental groups and knowledge of these changes is the key to successful endodontic therapy as the ability to locate and treat them properly can prevent future failures (6). Regarding the anatomical variations of the root canal the first maxillary molars are particularly important. The most common form of the first maxillary molar includes 3 roots and 3 canals. According to the literature reviews, the first maxillary molar owns 3 roots in 95.9% of cases and 3 channels at 56.8% and 4 channels in 43.1% of cases respectively. The presence of the 4th canal is usually reported at the meziobucal root in 95.6% of cases (5.6). less variations are present with in the distal and palatal root containing so 1 canal at 98.3% and 99% respectively. The reason for endodontic therapy failure is often due to the presence of the fourth MB2 canal, which is hard to be detected. Hess et al. (1925) showed the presence of 4th canals in 54% of the first
maxillary molars (10). Wein et al. (1969) reported that the incidence of the MB2 canal could be 62% in the first maxillary molars (4). Pineda and Kuttler (1972) reported an incidence of 51.5% of the additional canal in the first and second molars (11). Canal anatomy has been studied in vivo (clinical methods) and in vitro (laboratory methods). In vivo methods include the clinical treatment of a tooth, followed by the radiological evaluation of the root canal anatomy. In vitro methods include direct observation, microscopic observation, macroscopic sections, microscopic sections, decalcification, computerized micro tomography. Comparing laboratory and clinical findings, Seidberg et al. (1973) noted an incidence of 62% versus 33.3% of the two canals at the mesiobuccal root of the first maxillary molars (3). An important aid in finding root canals is the DoM, which was introduced by Bauman in 1997 to provide greater lighting and visibility. It brings small details and a clear picture (13). Finding the canal morphology through the clearing technique is another laboratory method. The advantages of this method is that this method allows us to evaluate in detail the canals and inter canal communications in 3D form (7). Weller et al. (1995) studied the MB root morphology of the maxillary molar using the clearing technique of the teeth and showed that 60% of mesiobuccal roots had 2 canal with a type 2 configuration pattern.
Purpose: The purpose of this in vitro study is to distinguish the anatomical characteristics of the pulp
AbstractIntroduction: Successful endodontic treatment includes accurate diagnosis, good understanding of biological principles, and excellent treatment performance. Anatomic variations of the teeth are present on all tooth groups, so knowledge of these variations is the key of successful endodontic therapy.Purpose: The purpose of this study is to distinguish the anatomical characteristics of the pulp chamber and the root canal system in the first maxillary molar in our population and compare the results with studies in other countries.Material and Method: 80 first maxillary molars were extracted and collected randomly, at the Dental Clinic, university of Dentistry, Tirana. The teeth were decalcified with 5% nitric acid and dehydrated with alcohol with escalated concentrations. The dye was then injected and the morphology of the root canal were then examined with a stereomicroscope. This study is based on the Vertucci ’s classification.Results: 90% of the teeth resulted with three roots configurations, of which 52.5% own three canals and 37.5% own 4 canals. 10% of the first maxillary molars resulted with two roots and three canals. In this study there were no 5 canals configuration. MB2 canal was found in 37.5% of cases.Conclusion: The mesiobuccal root shows a complexity of canal morphology. The first type was seen in 35% of cases, the second type in 35% of cases, type four in 20% of cases, type five in 3.75% of cases and type six in 6.25% of cases. In the mesiobuccal root, an apical foramen was seen in 70% of cases and two apical foramen in 30% of cases.
Xhanina gavazi
morphology of root canal system in the first maxillary molar
Faculty of Dental Medicine, University of Medicine, Tirana
key woRDS:
The canal
system, the first
maxillary molar,
the second
mesiobuccal
canal, the pulp
tissue.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 133
chamber and the canal system in the first maxillary molar in our population and compare the results with studies in other countries.
Material and Method: 80 first maxillary molars were extracted near by Dental Clinic, university of Dentistry, Tirana. Teeth were extracted for untreated caries, periodontal disease, trauma, or prosthesis. Selection criteria were: teeth with intact crowns, well formed, fractures free roots and without internal or external resorption. The residual soft tissues, bone fragments were cleansed properly.
The selected tooth was dispersed in running water and stored in 5.25% sodium hypochlorite for 30 min for the removal of organic substances. The teeth were stored at room temperature in 10% formalin until the time of use.
For each of the tooth, the preparation of the access cavity was made using long diamond round bur and the canal orifice was located. They were then placed in containers of 5.25% sodium hypochlorite for 24 hours in order to remove organic wastes. The clearing technique
protocol was approved by a previously described method (7). These samples were again put into 5% nitric acid for decalcification for the next 4 days at room temperature (Figure 1). Nitric acid was changed every day. In order to evaluate the decalcification level the needle to crown test and X-rays in series were applied (Figure. 2, 3). After decalcification, these samples were again browned and dehydrated at 70% ethyl alcohol for 12 hour, followed by 90% for 1 hour and 100% ethyl alcohol and rinsed in running water for one hour. Samples should be placed in xylene for two hours to be hardened prior to placement in methyl salicylates solution to make them transparent. The teeth were placed in methyl salicylates for 15-30 minutes for 3 days. At the end of the third day, the teeth are fully transparent. The methylene blue dye was then injected into the root canals with the aid of a 27-gauge needle. once the dye was dried the root canal morphology was analyzed with a stereo microscope x 10 magnification to evaluate the root canal numbers. The given datas were analyzed using SPSS (SPSS, Version 18.0, SPSS, Chicago, Il, uSA) SPSS software.
Fig. 1. Teeth after settling in 5% nitric acid.
Fig.3. The decalcification disk on the degree of decalcification.
radiography
Fig.4. Maxillary first molar after dye injection
Fig. 5. Communication between canals in the mesiobuccal root of the first
maxillary molar
Fig. 2.The needle test to see

Revista Stomatologjike Shqiptare134
Table 1. Number of roots and root canals of maxillary first molars.
Numer of roots of maxillary first molar
Number of teeth 3
canals%
Number of teeth 4
canals%
Number of teeth 5
canals% Total %
2 rooted 8 10% - - - - 8 10%
3 rooted 42 52.5% 30 37.5% - - 72 90%
Total 50 62.5% 30 37.5% - - 80 100%
Tabela nr. 2 Tipet e ndryshme të konfigurimit të kanalit të rrënjës në molarin e parë maksilar.
Types of canal
Mesiobuccalrootnr %
Distobuccal rootnr %
Palatal rootnr %
Mesiobuccalroot 2nr %
Type 1 28 35% 69 86.25% 77 96.25% - -
Type 2 28 35% 11 13.75% 3 3.75% 16 20%
Type 3 - - - - - - 14 17.5%
Total with one canal at
apex56 70% 80 100% 80 100% 30 37.5%
Type 4 16 20% - - - - - -
Type 5 3 3.75% - - - - - -
Type 6 4 5% - - - - - -
Type 7 1 1.25 - - - - - -
Total no with two canal at
apex24 30% - - - - - -
Type 8 - - - - - - - -
Total with three canal at
apex- - - - - - - -
Total 80 100% 80 100% 80 100% 30 37.5%
Results90% of the teeth resulted with three roots, of
which 52.5% had three canals and 37.5% had 4 canals. 10% of the first maxillary molars resulted with two roots and three canals. In this study there were no 5 canals root configuration Table 1. The examination of root canal system in this study is based on Vertucci’s classification. The mesiobuccal root represents some types of root canal configuration. The first type is seen in 35% of cases, the second type in 35% of cases, type 4 in 20% of cases, type 5 in 3.75% of cases, type 6 in 5% of cases and type 7 in 1.25% of cases. In the mesiobuccal root there was seen an apical foramen in 70% of cases and two apical foramens in 30% of cases Table. 2. MB2 canal was found in 37.5% of cases. Distobuccal root in 86.2% of cases has type 1 canal configuration and in 13.8% has the second type of
canal configuration and in 100% of cases there is an apical foramen. Palatinal root at 96.3% represents the first type of canal configuration and in the 3.7% the second type of canal configuration and an apical foramen in 100% of the cases. Table 1. The lateral canals were seen in the mesiobuccal root in the apical third in 15% of cases, and in the middle third in 5% of the cases. Tabela .3.In the distobuccal root the lateral canals were seen in 6.2% of cases in the apical third and in the middle third in 1.2% of cases. Table 4. In the palatinal root lateral canals were found in to apical third in 13.7% of the cases and in the middle third in 7.5% of the cases. The communication between the canals (Figure 5) was observed in the mesiobuccal root, in the coronal third 8.75%, in the coronarl and middle third in 12.5% of cases, in the middle third in 1.25% and in the middle and in the apical third in 2.5% of cases Table 6.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 135
Table 3. Lateral canals in the mesiobuccal root of the maxillary first molar.
Lateral canals in the mesiobuccal
root.
Number of teeth 3
canals% Number of
teeth 4 canals %Number
of teeth 5 canals
% Totali %
None 38 47.5% 26 32.5% - - 64 80%
Apical third 11 13.75% 1 1.25% - - 12 15%
Coronal third - - - - - - - -
Middle third 1 1.25% 3 3.75% - - 4 5%
Totali 50 62.5 30 37.5% - - 80 100%
Table 4. Lateral canals in the distobuccal root of the maxillary first molar.
Lateral canals in the distobuccal
root
Number of teeth 3
canals%
Number of teeth 4
canals%
Number of teeth 4
canals% Totali %
None 48 60% 26 32.5% - - 74 92.5%
Apical third 2 2.5% 3 3.75% - - 5 6.25%
Coronal third - - - - - - - -
Middle third - - 1 1.25% - - 1 1.25%
Total 50 62.5% 30 37.5% - - 80 100%
Table 5. Lateral canals in the palatinal root of the maxillary first molar.
Lateral canals in the palatal
root
Number of teeth 3 canals %
Number of teeth 4
canals%
Number of teeth 5
canals% Totali %
None 40 50% 23 28.75% - - 63 78.75%
Apical third 7 8.75% 4 5% - - 11 13.75%
Coronal third - - - - - - - -
Middle third 3 3.75% 3 3.75% - - 6 7.5%
Total 50 62.5% 30 37.5% - - 80 100%

Revista Stomatologjike Shqiptare136
Table 6. Intercanal communications of mesiobuccal root of maxillary first molar
Coronal, middle,
apical third
Type1
canal
Type2
2-1 canals
Type3
1-2-1 canals
Type4
2-2 canals
Type5
1-2 canals
Type6
1-2-1 canals
Type7
1-2-1-2 canals
Type8 3
canals
Total
None 35% 20% - 11.25% 2.5% 6.25% - - 75%
Coronal third - 3.75% - 5% - - - - 8.75%
Coronal-middle third - 10% - 1.25% 1.25% - - - 12.5%
Middle third - 1.25% - - - - - - 1.25%
Middle-apical third - - - 2.5% - - - - 2.5%
Total 35% 35% - 20% 3.75% 6.25% - - 100%
DiscussionsThe variability of root canal morphology of multi-
rooted teeth represents a constant challenge to diagnosis and endodontic treatment. The first maxillary molars are usually considered a three-rooted tooth, with palatal, distobucal, and mesio-buccal roots. In this study, the first maxillary molar resulted with three roots in 90% of cases, of which 52.5% had three canals and 37.5% had 4 canals. 10% of the first maxillary molars resulted in two roots and three canals (14, 15). Earlier studies also reported high incidence of three rooted maxillary molars. Neg et al. reported that 100% of the first molar molars had three roots in the Burmese population (14, 15). Pecora et al found 86.4% with three roots, 7.9% with united roots, 5% where lingual and distobuccal roots melts together, and 0.7% of all roots with roots together by 140 maxillary molars. Thomas et al. reported that from 216 maxillary molars 204 had three roots, 9 of which, the distobular and palatal roots are united, and 3 of which distobuccal and mesiobuccal roots are united.
The technique of dental cleaning has a considerable value in studying the anatomy of the root canal system, because unlike radiographic images, it provides a three-dimensional view of the pulp cavity in relation to the tooth (7). The types of canals observed at the mesiobuccal root are complex. The first type is observed in 35% of cases, the second type in 35% of cases, type
four in 20% of cases, type five in 3.75% of cases and type six in 6.25% of cases. The type of configuration of the mesiobuccal root canal in the present study shows close similarity with the study of Shahriar Shahi et al. in a Iranian population reporting Type I (37.96%), Type II (24.08%), Type IV (24.18%) Type V (9.5%), and Type VI (4.38% ), (16).
Similarly, a study by Wasti et al. reported Type I (33.3%), Type II (23.3%), Type IV (23.3%), Type V (13.3%), and Type VI (6.8%) of cases. Vertuci reported the canal configuration of 100 maxillary first molar and observed Type I in (45%) of cases, Type II (37%), Type III (0) and Type IV (18%) of cases (19, 20).
Meanwhile, Weine et al. reported 30.4% of the 293 maxillary first molars and Alavi et al. reported 44.2% of the 52 first maxillary molars with type IV of root canal configuration. This higher type IV spread can be considered as a type of Mongoloid population (13).
Conclusions Racial divergence may be responsive to such
variations. Further studies with larger sample numbers are needed to make a precise description of the canals anatomy.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 137
1. Vertucci FJ. Root canal morphology and its relationship to end-odontic procedures. Endodontic Topics. 2005; 10 (1):3–29.
2. Neelakantan P, Subbarao C, Ahuja R, Chandragiri VS, Gut-mann Jl. Cone-beam computed tomography study of root and canal morphology of maxillary first and second molars in an Indian population. J Endod. 2010; 36:1622–7.
3. Alavi AM, opasanon A, Ng Yl, Gulabivala K. Root and canal morphology of Thai maxillary molars.Int Endod J. 2002;35(5):478–85.
4. Weine FS, Hayami S, Hata G, Toda T. Canal configuration of the mesiobuccal root of the maxillary first molar of a Japa-nese sub-population. Int Endod J. 1999;32(2):79–87.
5. lee K-W, Kim Y, Perinpanayagam H, lee J-K, Yoo Y-J, lim S-M, Chang SW, Ha B-H, Zhu Q, Kum K-Y. Comparison of Alterna-tive Image Reformatting Techniques in Micro–Computed Tomography and Tooth Clearing for Detailed Canal Mor-phology. J Endod. 2014;40(3):417–22.
6. okumura T. Anatomy of root canals. Tokyo Dental College; 1927.
7. Robertson D, leeb IJ, McKee M, Brewer E. A clearing technique for the study of root canal systems. J En-dod. 1980;6(1):421–4.
8. Thomas RP, Moule AJ, Bryant R. Root canal morphology of maxillary permanent first molar teeth at various ages. Int Endod J. 1993;26:257–67.
9. Cleghorn BM, Christie WH, Dong CS. Root and root canal morphology of the Human permanent maxillary first molar; a literature review. J Endod. 2006;32:813–21.
10. Hess W, Zu¨rcher E. The Anatomy of Root Canals of the Teeth of the Permanent and Deciduous Dentitions. New York: William Wood & Co, 1925.
11. Pineda F, KuĴ ler Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root ca-nals. oral Surg oral Med oral Pathol 1972;33:101-10. 9.
12. Pomeranz HH, Fishelberg G. The secondary mesiobuccal canal of maxillary molars. J Am Dent Assoc 1974;88:119-24.
13. Weine FS. Endodontic Therapy, 5th edn. St louis: Mosby-Yearbook Inc., 1996: 243.
14. Stropko JJ. Canal morphology of maxillary molars, clinical observations of canal configurations. J Endod 1990: 25: 446–450.
15. Baldassari-Cruz lA, lilly JP, Rivera EM. The influence of dental operating microscopes in locating the mesiolingual canal orifices. oral Surg oral Med oral Pathol oral Radiol Endod 2002: 93: 190–194.
16. Coelho de Carvalho MC, Zuolo Ml. orifice locating with a microscope. J Endod 2000: 26: 532–534.
17. Go¨rduysus Mo, Gorduysus M, Friedman S. operating mi-croscope improves negotiation of second mesiobuc cal canals in maxillary molars. J Endod 2001: 27:
18. Kerekes K, Tronstad l. Morphometric observations on root canals of human molars. J Endod 1977: 3: 114–118.
19. Schwarze T, Baethge C, Stecher T, Geurtsen W. Iden-tification of second canals in the mesiobuccal root of maxillary first and second molars using magnify-ing loupes or an operating microscope. Aust Endod J 2002: 28: 57–60.
20. Buhrley lJ, Barrows MJ, BeGole EA, Wenckus CS. Effect of magnification on locating the MB2 canal in maxillary mo-lars. J Endod 2002: 28: 324–327.
REFERENCES

Revista Stomatologjike Shqiptare138
HyrjeFiksimi intermaksilar i shoqëruar me fizioterpi është
përdorur gjerësisht në të shkuarën.Disavantazhet e shumta (okluzion abnormal si pasojë
e fiksimit jokorrekt, apo mosfunksionimi drejtë i artikulacionit temporo-mandibular pasojë
e atrofisë muskulare) kanë bërë që vëmendja të shkojë drejt osteosintezës me minipllaka. Studiues të shumtë rekomandojnë fiksimin intermaksillar për trajtimin e frakturave të kondilit.1 2 3
Megjithatë, është akoma e diskutueshme përzgjedhja e njërës apo tjetrës teknikë. Kjo varet nga vështirësia apo zona e frakturës. Klotch & Lundy4 and Widmark et al.5 raportuan që osteosinteza me minipllaka duhet të bëhet kur kondili mandibular i frakturuar është shumë i zhvendosur, dhe fiksimi intermaksilar duhet të kryhet duke konsideruar një sërë faktorësh si mosha e pacientit, stabiliteti i siguruar i okluzionit, vështirësi në trajtimin me teknikën e osteosintezës me minipllaka për shkak të anestezisë gjenerale. Haug & Asseal6 raportuan se nuk ka asnjë të dhënë me rëndësi statistikore mbi statusin e okluzionit apo komplikimeve si limitim i lëvizjes mandibulare mes fiksimit intermaksilar dhe osteosintezës me mini pllaka. Sipas Ellis et al.7 janë parë më shumë komplikime (si: gjakderdhje intraoperatore, infeksion postoperator, paralizë e nervit facial, çrregullim funksional i nervit aurikulo-temporal, dhe çrregullim në rritjen kondilare) gjatë osteosintezës me minipllaka. Sipas tij është më e favorshme teknika e fiksimit intermaksilar. Ndërkohë Brown & Jones8 përdorën fiksimin me minipllakat dhe panë që nuk ishte i nevojshëm fiksimi intermaksilar. Tu & Tenhulzen9 arritën në konkluzionin që fiksimi i frakturës duke përdorur minipllakat dhe vidat shkurton periudhën e fiksimit intermaksilar
dhe parandalon atrofinë e muskulit mastikator. Jeter et al.10 arriti në konkulzionin që fiksimi mandibular mund të sjelli komplikime si çrregullime të hapjes së gojës, dhimbje temporomandibulare dhe çrregullime funksionale. Rekomandohet rikonsturktimi i frakturës me osteosintezë me minipllaka. Të gjitha këto opinione na bëjnë që të jemi të vëmendshëm dhe të kujdesshëm në zgjedhjen e mënyrës së trajtimit të kësaj frakture.
Materiali dhe metoda:Trajtimi i frakturave kondilare1-Fiksimi intermaksilar dhe terapia funksionale
MetodaFiksimi intermaksilar realizohet nëpërmjet përdorimit
të shinës dhe telave. Ky fiskim midis maksilës dhe mandibulës mbahet rreth 2-4 javë. Mbasi arrihet një bashkim i qëndrueshëm i zonës së frakturuar, telat hiqen dhe zëvendësohen ose jo me llastiqe. Për dy javë rekomandohet dietë me lëngje dhe ushqime të buta. Po gjatë kësaj periudhe bëhet terapia funksionale që përfshin ushtrime për lëvizjen e mandibulës dhe hapjes së gojës.
Ushtrimi i hapjes së gojës: veprohet duke qëndruar mbrapa pacientit dhe duke mbajtur gishtat tek molarët dhe tek bordi mandubular i anës së frakturuar. Në të njëjtën kohë pacienti hap gojën vet dhe me dorë poshtë mjekrës ushtron forcë për të evituar devijimin e mandibulës. Koha e fiksimit intermaksilar varion në literaturë. Shumë autor shpjegojnë se në frakturën interkapsulare mbahet 2 javë për pacientët nën 5 vjeç dhe 4 javë për ata mbi. Ndërsa për frakturën extra-kapsulare 2 javë për pacientët nën 8 vjeç.
AbstraktFrakturat e kondilit zënë një gamë të gjerë në frakturat e regjionit maxillofacial. Që në kohët më të hershme të trajtimit të këtyre frakturave është parë veshtirësia si në trajtimin imediat ashtu dhe në pasojat pas trajtimit. Aktualisht me zhvillimin e mjekësisë dhe mënyrave të reja të fiksimit është bërë që të kemi një rezultat gati perfekt në trajtimin e fragmenteve dhe me komplikacione minimale në kohë. Gjithsesi akoma dhe sot qëndrimi para një frakture të kondilit sidomos në disa zona të tij është akoma kontrovers dha has diskutime të shumta. Për trajtimin e frakturës së kondilit mund të përdoren si teknika konservative ajo e fiksimitintermaksilar ashtu edhe trajtimi kirurgjikal i osteosintezës me minipllaka. Menaxhimi ikësaj frakture mbetet një temë mjaft e diskutueshme në traumën orale dhe maksilo-faciale.Për çdo tip të frakturës së kondilit, metoda e trajtimit duhet zgjedhur duke u marrë nëkonsideratë një sërë faktorësh si: prezenca e dhëmbëve, lartësia e frakturës, devijimi imandibulës etj. Fiksimi intermaksilar i shoqëruar me fizioterapi është përdorur gjerësisht në të shkuarën. Qëllimi: Qëllimi i këtij artikulli është të vlersojë ndryshimet kryesore që përcaktojnë zgjedhjen e njërës teknikë apo tjetrës, duke identifikuar avantazhet dhe disavantazhet si dhe ecurinë afatgjatë dhe komplikacionet e afërta dhe të largëta.
jakup vrioni, Renato isufi, Ramazan isufi
Një këndvështrim mbi trajtimin kirugjikal dhe konservator të frakturave të kondilit
Klinika oro maxilofaciale Spitali Francez, QSUT “Nene Tereza”, Tiranë
Falë kyçe:
Frakturë, fiksim intermaksilar, fizioterapi, klasifikimi i frakturës se qafës se kondilit

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 139
AvantazhetFiksimi intermaksilar shoqëruar me terapi funksionale
është një trajtim mjaft i sigurt. Nuk ndodh asnjë dëmtim në nerva apo vaza, dhe asnjë komplikim postoperativ si infeksion apo shenjë e plagës. Më e rëndësishmja është që komplikimet si fraktura, humbja apo vonesë në eruptim tek pacientët pediatrik janë të evitueshme.11
DisavantazhetFiksimi intermaksilar mund të dëmtojë indin
periodontal dhe mukosën vestibulare. Mund të kemi gjithashtu vështirësi në mbajtjen e higjenës, vështirësi në shqiptim, probleme nutritive, çrregullime në hapjen e gojës dhe çrregullime respiratore.12 13 Çrregullimi i rritjes dhe rritja e tepërt e anës së dëmtuar mund të ndodh si rezultat i mos reponimit në mënyrën e duhur të fragmenteve kockore të thyera.14 15 Gjithashtu mund të kemi dhe devijim mendibular gjatë hapjes (Shumë studime kanë vërtetuar që tek pacientët e moshave 10-15 vjeç mund të shihet asimetri faciale apo patologji të ATM-sësi pasojë e çrregullimeve të rritjes apo funksionale. Veçanërisht çrregullimet e rritjes dhe funksionale të ATM-së ndodhin në 20-25%të pacientëve të moshës 7-10 vjeç.)
Klasifikimi i frakturës se qafës se kondilit sipas Spiessl dhe Schroll
Tipi I: frakturë e qafës së kondilit pa dislokim Tipi II: frakturë e thellë e qafës me zhvendosjeTipi III: frakturë e lartë e qafës së kondilit me zhvendosjeTipi IV: frakturë e thellë e qafës së kondilit me zhvendosje
dhe rotullimTipi V: frakturë e lartë e qafës së kondilit me zhvendosje
dhe rotullimTipi VI: frakturë intrakapsulare
2-Osteosinteza me mini-pllakaTeknikat operatoreKa lloje të ndryshme medotash operative për
osteosintezën me mini-pllaka në trajtimin e frakturës kondilare. Në varësi të zonës së frakturës apo gradës së zhvendosjes së fragmenteve kockore incisioni mund të jetë periaurikular, retroaurikulare , submandibulare , retromandibular apo i kombinuar. Trajtimi duhet zgjedhur duke marrë parasysh moshën e pacientit, preferencën, tipin e frakturës, nësë ka fraktura dhe në zona të tjera dhe gjendjen e dhëmbëve.etj
AvantazhetAvantazhi kryesor është vendosja e fragmenteve të
frakturuara në mënyrë anatomike ideale. Si rrjedhojë mund të parandalojë komplikacionet e ndryshme, asimetrite, okluzionin , çrregullime respiratore, të shqiptimit.etj
Disavantazhetosteosinteza me mini pllaka kërkon një trajtim mjaft
invaziv, i cili mund të shkaktojë dëmtim të nervave
dhe vazave përreth. Mund të shkaktojë dhe infeksion postoperativ. Edhe pse incizioni bëhet duke konsideruar estetikën shenja gjithsesi mbetet.
Për të arritur të kryejmë osteosintezën kirurgu duhet të ketë një akses sa më të mire të fushës operatore dhe fragmenteve të frakturës. Për të arritur këtë në varësi dhe të linjës së thyerjes së kondilit kemi disa linja prerjeje që vendosen në zona të ndryshme të fytyrës. Po japim disa më të rëndësishmet gjithmonë duke e lidhur ngushtë dhe me linjën e frakturës.
Incizioni PreaurikularIncizioni bëhet 3-4 cm nga bordi inferior i tragusit
drejt kanalit auditiv ekstern. Përdoret zakonisht në frakturat e larta kondilare si
fraktura interkapsulare.Veçanërisht ky incizion kryhet kur fragmenti i kondilit
zhvendoset antero-mezialisht nga tërheqja e pterigoidit medial.
Incizioni retroaurikulareBëhet nga një zonë 3 mm poshtë regjionit të kthyer
retroaurikulare dhe duke vazhduar përgjatë saj. Bëhet një incizion tjetër në proçesin mastoid dhe në pjesën e sipërme të veshit. Edhe kjo metodë përdoret për frakturat e larta kondilare. Ka avantazh estetik dhe për shkak se hyrja është mbrapa veshit eviton dëmtimin e nervit facial dhe arteries temporale sipërfaqësore. Risk të ulët në dëmtimin e parotisit. Disavantazhet janë vështirësia në përdorimin e instrumentave kirurgjikal dhe komplikime si stenoza e kanalit auditiv ekstern, tinitus, infeksion dhe nekrozë e kërcit aurikolar, parestesi aurikolare si pasojë e dëmtimit të kanalit auditiv ekstern, si dhe shërim më i avashtë i plagës krahasuar me incizionin preaurikolar.
Incizioni submandibularIncizioni bëhet nga një zonë 2-3 cm poshtë bordit
inferior të mandibulës duke vazhduar paralelisht me të. Ky incizion të jep një pamje të gjerë të ramusit mandibular, kondilit mandibular dhe proçesit koronoid. Për këtë arsye është mjaft i përdorur. Ka si disavantazh dëmtimin e nervit facial alveolar, vështirësi në arritjen e zonave të larta të frakturës së kondilit, dhe vështirësi në ekzaminimin e pjeses intrakapsulare të ATM-së.
Incizioni RisdonKy incizion është i përafërt me atë submandibular.
Mundëson pamje të regjionit inferior, ramusit, këndit gonial, dhe trupit posterior të kondilit mandibular. Në qoftë se lemboja superior divergohet mirë mund të shihen dhe frakturat e qafës së kondilit. Njëlloj si dhe incizioni submandibular kërkon traksion të fortë për të parë frakturën kondilare të lart.19
Incizioni i kombinuarËshtë një kombinim i incizionit preaurikolar dhe

Revista Stomatologjike Shqiptare140
submandibular. Kjo metodë është mjaft e dobishme kur duam të arrijmë frakturën e qafës së kondilit nëpërmjet incizionit preaurikular dhe behet fiksimi i fragmenteve kockore duke tërhequr mandibulën poshtë.
Për shkak të përdorimit të dy incizioneve ka mjaft disavantazhe si: kohë operative më e gjatë, formimi i një shenje më të madhe, risk i lartë për dëmtimin e nervit facial, dhe risk për zhvillimin e një patologjie sekondare të ATM-së.
Incizioni intraoralNëpërmjet kësaj metode arrihet kondili mandibular
njëlloj si në osteotomin e ramusit mandibular. linja e incizionit formohet përgjatë pjesës anteriore të ramusit mandibular dhe sulkusit bukal. Për të arritur pamjen intraoperatore duhet bërë diseksioni i muskulit temporalis. Kjo metodë ka mjaft avantazhe: nuk lë shenjë dhe nuk ka risk për dëmtimin e nervit facial. Përdorimi i instrumentave ka vështirësi prandaj nevojitet endoskopi. Ka vështirësi në mbajtjen e qëndrueshmërisë së fragmenteve kockorë të frakturuar.
Incizioni RetromandibularIncizioni bëhet vertikalisht këndit mandibular duke
ecur 3 cm deri 5 cm poshtë veshit. Kjo metodë lejon fiksimin për frakturën subkondilare. Kjo teknikë siguron një fiksim të mire dhe për frakturat e kokës së kondilit. Shenja e incizionit është mjaft e vogël pra ka avantazh estetik, si dhe të lejon të kesh nje fushë operatore të mirë në ekspozimin e fragmenteve superiore të frakturës. Por gjithashtu ka dhe disavantazhe si: risk për dëmtimin e nervit facial dhe vazeve të gjakut. 20 21
Protokolli trajtimitFraktura kondilare është ndër frakturat mandibulare
që ndeshemi më shumë. Metodat e trajtimit kanë qënë gjithmonë burim diskutimesh. Që kur Zide & Kent raportuan indikacionet relative dhe absolute për frakturat e kondilit në 1983, osteosinteza me mini-pllaka është vënë në diskutim dhe teknikat e reja kirugjikale dhe të fiksimit janë zhvilluar.
Fraktura kondiliare ndodh për shkaqe të ndryshme dhe ka metoda të ndryshme trajtimi në varësi të pozicionit të frakturës, moshës së pacientit dhe tipit të frakturës.
Qëllimi i trajtimit të frakturës kondilare është të arrihet rikthimi i funksionit normal të ATM-së.
Prandaj vlerësimi i trajtimit duhet të mbështetet duke u bazuar në komplikimet e mundshme. Qëllimi final i trajtimit është arritja e stabilitetit okluzal, hapje normale të gojës, lëvizje normale të ATM-së, parandalimi i dhimbjes temporo-madibulare si dhe parandalimin e çrregullime të rritjes.
Kjo arrihet duke analizuar metodën e trajtimit më të favorshme duke zgjedhur mes fiksimit intermaksilar dhe osteosintezës me minipllak
Indikacionet absolute të trajtimit me minipllaka• Zhvendosja në fosën kraniale• Pamundësia për të arritur okluzionin e përshtatshëm
nëpërmjet fiksimit intermaksilar• Zhvendosje laterale ekstra-kapsulare• Kur kemi një trup të huaj
Indikacione Relative• Frakturë bilaterale e kondilit në pacient edentuloz• Frakturë bilatelare ose unilaterale e kondilit ku
splintimi nuk mund të kryhet për arsye mjekësore ose kur mekanoterapia është e pamundur
• Frakturë bilaterale kondilare dhe njëkohësisht fraktura të tjera faciale, apo kur kemi prezence prognatie
• Probleme Periodontale• Humbje të dhëmbëve• Frakturë unilaterale kondililare me bazë jo të
stabilizuar
Protokollet e AAoMS (American Association of oraland Maxillofacial Surgeons) për osteosintezën me mini pllaka (2003)
Në 2003 shoqata Amerikane e kirurgëve oral dhe maksilofacial sugjeroi një protokoll ndërkombëtar në trajtimin e frakturave kondilare.Trajtimi i hapur me osteosintez rekomandohej kryesisht në rastet e konfirmuara si radiologjikisht dhe klinikisht për të parandaluar komplikacione të ndryshme funksionale ose çregullime të rritjes.
Indikacionet për osteosintez sipas AAOMS (2003)• Konfirmimi klinik dhe radiologjik i prezencës së
frakturës• Malokluzion• Prishje apo Pengesë në levizjen e mandibulës• Raporti fuksional i nofullave • Prezenca e trupave të huaj• Dëmtime dhe/ose hemorragji në kanalin
auditivekstern• Prezenca e lëngut cerebral nga veshi • Hemartrozë
Indikacione absolute • Zhvendosje e kondilit në fossa crani media • Prezenca e trupave të huaj• Zhvendosje laterale ekstrakapsulare e kondilit • Pamundësi e rivendosjes së okluzionit me fiksim me
bimaksilare
Indikacione të forta bazuar në evidencën e fakteve për fiksim me osteosintezë • Frakturë bilaterale Kondili • Frakturë kondili me zhvendosje më të madhe se 45
gradë • Reduksion i lartësisë së ramusit mbi 2mm
Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 141
• Frakturë kondilare me shprehur me fraktura të katit të mesëm
• Kur kemi okluzion jo te stabilizuar ( psh dhembe qe levizin ose mungojne )
Trajtim me fiksim bimaksilare me tela ose elastik• Frakturë pa zhvendosje të kondilit ose inkomplete • Frakturë intrakapsulare të izoluar• Frakturë kondilare në femijë (me perjashtim te atyre
absolute )• Sëmundje të ndryshme ku nuk mund ti nënshtrohet
anestezisë gjenerale
Protokolli ynë i trajtimitQëndrimi ynë në trajtimin e frakturat e kondilit është
në linjë me protokollet e mësipërme. Për sa i përket frakturave intrakapsulare pa ndryshime në okluzion terapia që preferojmë është kryesisht koservatore pra me fiksim interemaksilare 2 deri 3 javë në varësi të dëmtimit me fiskim me elasik ose rigid dhe fizioterapi për disa muaj.
Në frakturat interkapsulare me zhvendosje fragmentesh në moshë më të madhe se 10 vjec me prishje okluzioni praninë e trupave të huaj ose fragmenti që pengon hapjen e gojës, veprohet me mënyrën e
hapur pra me osteosintezë me minipllaka. Po kështu dhe në ato bilateralet kur kemi mundësi fiksimi dhe kur nuk kemi dëmtime të fragmentimit të kokës artikulare, fizioterapi për disa muaj.
Në raste të frakturave ekstakapsulare pa ndryshime fiksimi për 3 – 4 javë me elastik ose tela dhe fizioterapi për disa muaj
Në frakturat ekstrakapsulare me ndryshime në okluzion hapsira të fragmenteve kënde me te mëdhenj se 30 gradë të fragmenteve fiksim me osteosintezë me minipllaka.
Gjithashtu në të gjitha rastet e frakturave të hapura dhe me trupa të huaj përdoret osteosintezë me minipllaka.
KonkluzionePër trajtimin e frakturave kondilare mandibulare
përdoren si teknika konservative e fiksimit intermaksilar ashtu si dhe teknika kirurgjikale e osteosintezës me mini pllaka. udhëzimet për njërën apo tjetrën janë akoma në diskutim. lloji i trajtimit duhet të zgjidhet duke konsideruar moshën e pacientit, llojin e frakturës, prezencës e frakturave të tjera, dhëmbët, prezencën e trupave të huaj etj. Avantazhet, disavantazhet dhe komplikimet e mundshme duhet të diskutohen edhe me pacientin për zgjedhjen e planit të trajtimit.
1. Zide MF, Kent JN. Indications for open reduction of mandib-ular condyle fractures. J oral Maxillofac Surg 1983;41: 89-98.
2. Goss AN, Bosanquet AG. The arthroscopic appearance of acute temporomandibular joint trauma. J oral Maxillofac Surg 1990;48:780-3.
3. Wood GD. Assessment of function following fracture of the mandible. Br Dent J 1980;149:137-41.
4. Klotch DW, lundy lB. Condylar neck fractures of the man-dible. otolaryngol Clin North Am 1991;24:181-94.
5. Widmark G, Bagenholm T, Kahnberg KE, et al. open reduc-tion of subcondylar fractures: a study of functional rehabili-tation. Int J oral Maxillofac Surg 1996;25:107-11.
6. Haug RH, Assael lA. outcomes of open versus closed treat-ment of mandibular subcondylar fractures. J oral Maxillofac Surg 2001;59:370-5.
7. Ellis E 3rd, McFadden D, Simon P, et al. Surgical complica-tions with open treatment of mandibular condylar process fractures. J oral Maxillofac Surg 2000;58:950-8.
8. Brown JS, Jones K. Delayed miniplate osteosynthesis for mandibular fractures. Br J oral Maxillofac Surg 1991;29: 286.
9. Tu HK, Tenhulzen D. Compression osteosynthesis of man-dibular fractures: a retrospective study. J oral Maxillofac Surg 1985;43:585-9.
10. Jeter TS, Van Sickels JE, Nishioka GJ. Intraoral open reduc-tion with rigid internal fixation of mandibular subcondylar fractures. J oral Maxillofac Surg 1988;46:1113-6.
11. Kaban lB, Troulis MJ. Pediatric oral and maxillofacial surgery. Philadelphia: Saunders; 2004.
12. Coletti DP, Salama A, Caccamese JF Jr. Application of inter-maxillary fixation screws in maxillofacial trauma. J oral Max-illofac Surg 2007;65:1746-50.
13. Kirurgjia oro Maxillo Faciale. Prof.Dr.Ramazan Isufi, Dr.Andis Qendro, Dr.Esat Bardhoshi
REFERENCA

Revista Stomatologjike Shqiptare142
IntroductionIntermaxilar fixation accompanied by physiotherapy has
been used widely in the past. The disadvantages (abnormal occlusion as a result of a non correct fixation, or bad function of the temporo-mandibular articulation as a result of the muscular atrophy) did the treatment to be focused on the osteosintesis with miniplasts. Many studies recommend intermaxilar fixation for treating condyle’s fractures. 1 2 3
However, it is still discussed the election of the technique. This depends on the difficulties and the area of the fracture. Klotch & Lundy4 and Widmark et al.5 reported that osteosintesis with miniplasts must be done when the fracture mandibulat condyle is too much displaced, and the intermaxilar fixation must be done considering a set of factors like the age of the patient, the secured stabilization of the occlusion, the difficulties on treating it with the technique of osteosintesis with miniplasts because of the general anesthesia.
Haug & Asseal6 reported that there is no data with statistic importance regarding to the occlusion status or complications as a limitation of the mandibul moving between intermaxilar fixation and osteosintesis with miniplasts. According to Ellis et al.7, there has been lot of complications ( like: intraoperative bleeding, post operator infection, paralysis of the facial nerve, dysfunction of the aurikulo-temporaland nerve ) during the osteosintesis with miniplasts. According to him, intermaxilar fixation is more favored. Meanwhile, Brown & Jones8 used the fixation with miniplasts and noticed that the intermaxilar fixation was not necessary. Tu & Tenhulzen9 achieved the conclusion that the fixation of the fracture using miniplasts and screws cuts the intermaxilar fixation time and prevent the atrophy of the musticator muscle. Jeter et al.10 had the conclusion that mandibular fixation might brought complications like dysfunction on opening the mouth, temporomandibular pains and functional dysfunction. They recommend the reconstruction of the fracture using osteosintesis with
miniplasts. All these opinions raise our awareness on using the right technique on treating this kind of fracture.
Materials and Methods:The treatment of the condyles’ fractures1- Intermaxilar fixation and the functional therapy
The methodIntermaxilar fixation is realized by using toothpicks.
This fixation between maxilla and mandibul is kept for 2-4 weeks. After achieving a solid fracture of the fractured area they are removed and might be replaced by the slingshots. For two weeks, it’s recommended a diet full of juices and wet food. During that time also is recommended functional therapy including exercises on moving mandibul and the opening of the mouth.
The exercise on opening the mouth: it is operated by staying in the back of the patient keeping your fingers on the molars and at the mandibular bord of the fractured side. At the same time, the patient open his mouth and with the hand under his chin exercises force in order to avoid the mandibular deviation. The time of the intermaxilar fixation varies depending on the literature. Many studies explain that on the intecapsular fracture is kept 2 weeks for patients under 5 years old and 4 weeks for the others. The extra-capsular farcture is kept 2 weeks for patients under 8 years old.
The advantagesIntermaxilar fixation accompanied by the functional
therapy is a very safe treatment. There is no damage on the nerves and no post-operative complications such as infections or marks. The most important is the fact that complications like fracture, loss in the recuperating on the patients can be deviated.
AbstractCondyle’s fractures maintain the main position regarding to the maxillofacial region. Time ago it was obviously seen the difficulties on immediate treatment of such factures and the consequences after the treatment. Actually, the development of the medicine and the new ways on fixing it made the results already perfect on treating minimal fragments and complications. However the fractures of the condyle still have lots of discussion. For treating condyle’s fracture we can use like conservative techniques that of intermaxilar fixation and the chirurgical treatment of osteosintesis with miniplasts. The discussion of such fracture is still open in the oral and maxi facial trauma. For treating every kind of cobdyle’s fracture we must take in consideration a lot of factors such as: the highness of the fracture, the condition of the teeth, the mandibular deviation.Intermaxilar fixation accompanied by physiotherapy has been used widely in the past.The aim: the purpose of this article is to evaluate principal changes that define the election of the adequate technique identifying the advantages and disadvantages, the long term development and the different complications.
jakup vrioni, Renato isufi, Ramazan isufi
a point of view in the chirurgical and conservator treatment of the condyle
Oro maxi facial clinic French Hospital, QSUT “Mother Teresa” Tirana
key woRDS: Fracture, Intermaxilar fixation, physiotherapyclassification of the Condyle’s neck fracture

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 143
The DisadvantagesIntermaxilar fixation may damage the periodontal
tissue and the vestibular mucous. It might be also difficult to maintain a clear hygiene. , difficulties while speaking, nutritive problems, dysfunction on opening the mouth and breathing dysfunction. The abnormal growth of the damaged side may come as a result of nocorrecting on the right way the damaged fragments. Also, we may notice mandibular deviation while opening the mouth. (Many studies have proved facial asymmetry on the 10-15 years old patients. The growing and ATM dysfunction occurs in 20-25% of the 7-10 years old patients.)
The classification of the Condyle’s Neck Fracture according to Spiessl and SchrollType I: Condyle’s neck fracture without deploymentType II: Deep fracture of the neck with displacementType III: High fracture of Condyle’s neck with displacementType IV: Deep fracture of Condyle’s neck with displacement
and rotationType V: High fracture of Condyle’s neck with displacement
and rotationType VI: Intracapsule fracture
2- Osteosintesis with miniplastsOperative techniquesThere are different types of operative methods for
osteosintesis with miniplasts on treating the Condyle fracture. Depending on the area of the fracture or the grade of the displacement of the fragment bones, the incision might be periauricular, retrourikular, submandibular, retromandibular or combined. The treatment must be elected considering the age of the patient, the type of the fracture, and if there is other fractured areas, the conditions of the teeth.
AdvantagesThe main advantage is the placement of the fractured
fragments in an ideal anatomic way. This may prevent different complications, asymmetries, and occlusion, breathing dysfunctions and speaking ones.
Disadvantagesosteosintesis with miniplasts looks for a very invasive
treatment, which may cause damage of the nerves around it. It may cause even post-operative infection. Even if the incision in made considering the esthetic part, the mark remains within it.
In order to operate with osteosintesis, the chirurgery must have a very detailed access on the operative area and the fractured fragments. To achieve this, depending on the line of the condyle’s fracture,there are different cutting lines in differentareas of the face. The most important regarding to the area of the fracture are:
Preurikular IncisionThe incision is made 3-4 cm away from the inferior bord
of tragus continuing in the extern additive cannel. It is mostly used in the high condyle’s fractures like intercapsular
fracture. Especially this incision is made when the condyle’s fragment is displaced from the withdrawal of medial pterigoid.
Retroaurikular incisionIt is made in an area 3 mm under the retroaurikular
region going through it. It continues with another incision in the mastoid process and in the upper part of the ear. Even this method is used for the high condyle’s fracture. There is the esthetic advantage and having the process after the ear avoid the damage of the facial nerve and the superficial temporal artery. There is low risk on damaging the parotis. Disadvantages are the difficulties on using the chirurgical instruments, and complications like stenosis of the extern auditory canal, tinnitus, infection and necrosis of auricular kercite, parestesis aurikolar as a result of the damage of the extern auditory canal, and lower healing of the marks compare to the preaurikolar incision.
Submandibular incisionThe incision is made in an area 2-3 mm under the inferior
border of the mandibul continuing in a parallel way with it. This incision gives a wide view of the mandibular ramuses, mandibular condyle and the conoroid process. For this reason it’s very used. Its disadvantage is the damage of the alveolar facial nerve, difficulties on the higher areas of the condyle’s fracture and difficulties on examination of the intra caspul part of the ATM.
Combined IncisionThis is a combination between preaurikolar and
submandibular incision. In this method is done the fixation of the fragment bones pulling the mandibular under it. The risk of using two incisions is on longer operative time, a bigger mark, high risk on damaging facial nerve, risk on developing a second pathology of ATM.
Intraoral incisionThrough this method we have the mandibular condyle
the same as in the osteotomus of the mandibular ramuses. The incision is created on the inner part of the mnadibular ramuses and bukal sulkus. To have the intraoperative view we must do the dissection of the temporalis mucle. This method doesn’t leave marks and there is no risk on the damage of the facial nerve. There are difficulties of keeping active the fragment bones fractured.
Retromandibular incisionThe incision is made vertically going 3-5 cm under the
ear. This method permits the fixation of the subcondilare fracture. This technique secures a better fixation of the condyle’s head. There is the estethic advantage and it permits to have a good operative field in the exposition of the superior fragments fractured. Disadvantage is the risk of having the facial nerve damaged.
The protocol of the treatmentCondyle fracture is the most famous of the mandibulare
fractures. The methods on treating them have always been an open discussion. Since when Zide & Kent reported the

Revista Stomatologjike Shqiptare144
relative and absolute indications of the condyle’s fracture in 1983, osteosintesis with miniplats are in discussion even with the evolution of the new ways of fixation and the chirurgical ones.
Condyle’s fracture occurs for different causes and there are different ways of treating it, depending on the position of the fracture, age of the patient and the type of the fracture.
The aim of the fracture treatment is to have the normal function of the ATM. That’s why the evaluation of the treatment should be supported based on the possible complications. The final aim of this treatment is to achieve occlusion stabilization, normal opening of the mouth, and normal movement of the ATM, prevention of the temporo-madibulair pain. This is achieved by analyzing the most favored methods, choosing between intermaxilar fixation and osteosintesis with miniplats.
The absolute indication of the treatment with miniplasts• Displacement in the cranial fose• The inability to reach the right occlusion through
intermaxilar fixation• lateral extra-capsul displacement• Having an anti-body
Reative Indications• Bilateral fracture of the condyle in a edentulous
patient• Bilateral or unilateral fracture of the condyle where
the splint cannot be done for medical reasons or the mecantropy is impossible
• Bilateral condyle fracture and at the same time other facial fractures
• Periodontal problems• loss of the teeth• unilateral condyle fracture with no stabilized base
The AAoMS for osteosintesis with minplasts In 2003 the AAoMS suggested an international protocol on treating the condyle’s fracture. An open treatment with osteosintesis was recommended mostly in the cases that were confirmed as radiological and clinically to prevent different functional complications or growing dysfunctions.
The indications for osteosintesis according to AAOMS (2003)• Clinically and radiological confirmation of the
presence of the facture• Maloclusion• Damage or obstacle in the move of the mandibul• Functional report of the • The presence of anti-bodies• The presence of the cerebral water from the ear• Hermartros
Absolute indications• Displacement of the condyle in the fossa crani media• Te presence of the anti-bodies• Displacement extracapsul lateral of condyle• Inability of placing occlusion with fixation in bimaksilare
Strong indications based in the evidence of the facts for fixation with osteosintesis• Bilateral fracture condyle• Condyle’s fracture with big displacement 45 grade• Height reduction of the ramus up to 2mm• Condyle fracture expressed with fractures of the
middle plan• For not stabilized occlusion ( e.x teeth that are loss or
missed)
Treatment with bimaxilare fixation with wires• Fracture without displacement of the condyle or
incomplete• Intracapsul isolated fracture• Condilar fracture in children • Different diseases where you can’t take general
anesthetic
Our protocol of the treatmentour point of view in the treatment of the condyle’s
fracture is in the same line with the above protocols. Regarding to the intracapsul fractures without changes in the occlusion, the therapy that we desire is mostly conservative, which means with intermaksilar fixation, 2-3 weeks, depending on the damage of fixation with elastic or rigid and physiotherapy for some months.
In interkapsular fractures with displacement of fragments in ages up to 10 years old, we use the open way, so osteosintesis with miniplats. The same even with bilateral when we have the opportunity of fixation and when we don’t have damages of the head fragments, with physiotherapy for some months.
In the cases of the extracapsul fractures without changes we have fixation with 3-4 weeks with elastic or physiotherapy for some months.
In the fractures extracapsul with changes in occlusion we have spaces of the fragments in 30grade using fixation of osteosintesis with miniplats.
Also in the cases of the open fractures and antibodies we use osteosintesis with miniplats.
ConclusionsFor the treatment of the condilaire mandibulaire fractures
use conservative techniques and intermaksilar fixation, as chirurgical techniques of osteosintesis with miniplats. Choosing the technique is still an open discussion. The kind of the treatment used should be elected considering the age of the patient, the presence of other factures, the presence of antibodies, the control of the teeth. The advantages, disadvantages and possible complications must be discussed even with the patient for choosing the way of treatment.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 145
1. Zide MF, Kent JN. Indications for open reduction of mandib-ular condyle fractures. J oral Maxillofac Surg 1983;41: 89-98.
2. Goss AN, Bosanquet AG. The arthroscopic appearance of acute temporomandibular joint trauma. J oral Maxillofac Surg 1990;48:780-3.
3. Wood GD. Assessment of function following fracture of the mandible. Br Dent J 1980;149:137-41.
4. Klotch DW, lundy lB. Condylar neck fractures of the man-dible. otolaryngol Clin North Am 1991;24:181-94.
5. Widmark G, Bagenholm T, Kahnberg KE, et al. open reduc-tion of subcondylar fractures: a study of functional rehabili-tation. Int J oral Maxillofac Surg 1996;25:107-11.
6. Haug RH, Assael lA. outcomes of open versus closed treat-ment of mandibular subcondylar fractures. J oral Maxillofac Surg 2001;59:370-5.
7. Ellis E 3rd, McFadden D, Simon P, et al. Surgical complica-tions with open treatment of mandibular condylar process fractures. J oral Maxillofac Surg 2000;58:950-8.
8. Brown JS, Jones K. Delayed miniplate osteosynthesis for mandibular fractures. Br J oral Maxillofac Surg 1991;29: 286.
9. Tu HK, Tenhulzen D. Compression osteosynthesis of man-dibular fractures: a retrospective study. J oral Maxillofac Surg 1985;43:585-9.
10. Jeter TS, Van Sickels JE, Nishioka GJ. Intraoral open reduc-tion with rigid internal fixation of mandibular subcondylar fractures. J oral Maxillofac Surg 1988;46:1113-6.
11. Kaban lB, Troulis MJ. Pediatric oral and maxillofacial surgery. Philadelphia: Saunders; 2004.
12. Coletti DP, Salama A, Caccamese JF Jr. Application of inter-maxillary fixation screws in maxillofacial trauma. J oral Max-illofac Surg 2007;65:1746-50.
13. Kirurgjia oro Maxillo Faciale. Prof.Dr.Ramazan Isufi, Dr.Andis Qendro, Dr.Esat Bardhoshi
REFERENCES

Revista Stomatologjike Shqiptare146
HYRJE Në regjionin anterior, kaninët janë dhëmbët që
impaktohen më shpesh, me një prevalencë që varion nga 1% deri në 3%. (1)
Këta dhëmbë luajnë një rol të rëndësishëm si në ruajtjen e formës së harkadës dhe në funksion, por edhe një rol të rëndësishëm estetik. (2) Në fakt, mosrekuperimi i kaninëve të impaktuar, lidhet me një sërë problemesh të tjera sic është rezorbimi i rrënjëve të dhëmbëve ngjitur ose spostimi i rrënjëve të tyre (3), humbje në gjatësi e harkut dentar, formimi i kisteve odontogjene, infeksione lokale, etj. (4,5) Për këtë arsye është evidente rëndësia e rekuperimit të këtyre dhëmbëve në harkadat dentare, duke evituar sa më shumë që ti heqim. (6)
Me kalimin e viteve janë propozuar zgjedhje terapeutike të ndryshme për të evituar ekstraksionin e tyre. Një ndër to është edhe autotransplanti i dhëmbit të impaktuar në alveolën e krijuar nga kirurgu. Kjo mënyrë parashikon edhe trajtimin endodontik të këtij dhëmbi për një periudhë kohe. Të dhënat e literatures tregojnë për një sukses prej 90% të rasteve (7). Altonen dhe Myllarniemi (8) në mesin e viteve 70 propozuan një ndërhyrje më konservative që parashikon një ekspozim kirurgjikal të indeve që mbulojnë kurorën e dhëmbit të impaktuar, duke e lënë të hapur (teknika e dritares).
Dhëmbi i ekspozuar në këtë mënyrë, në prani të hapësirës së nëvojshmeka mundësi që të eruptojë vetë, edhe pse jo në vendin e duhur. Ky rezultat klinik ka bërë që të krijohet një bashkpunim i ngushtë i ortodontit dhe kirurgut oral në ekspozimin e dhëmbëve të impaktuar dhe në drejtimin e tyre në pozicionin e duhur final në harkadë (9) Trajtimi i kaninëve të impaktuar në mënyrë ortodontike-kirurgjikale ka pësuar një zhvillim të madh në vitet e fundit duke marrë në konsiderate jo vetëm menaxhimin e indeve të forta (kocka, smalti, dentina)
dhe të buta (gingiva), por edhe të forcave tërheqëse. Më përpara hiqej një pjesë e strukturës së dhëmbit për të vendosur një vidë që do të shërbente për të tërhequr dhëmbin e impaktuar. Me metodat e reja të ngjitësve (kompozitëve) u arrit të mënjanohet dëmtimi i strukturave të dhëmbit dhe ekspozimi i koronës së tij u limitua në një hapësirë të vogël sa për të vendosur braketën (10) Përsa i përket indeve të buta u arrit të kalohej nga teknikat të cilat hiqnin një pjesë të madhe të gingivës (window technique), në teknika të cilat ruajnë si gingivën aderente edhe ate jo aderente me ripozicionimin e saj në pozicionin e mëparshëm (closed technique) (11).
Momenti i fundit që duhet marrë parasysh është tërheqja (forca dhe drejtimi). Sipas Bishara (4) kjo parashikon tërheqjen me forca të lehta (më pak se 60g). lëvizja e dhëmbit arrihet me “rezorbim direkt” të kockës që rrethon kaninin me një balancim të mirë të fenomeneve të rezorbimit dhe formimit të kockës së re.
Drejtimi i forcës duhet të bëhet në mënyrë të tillë që të largohet nga rrënjët e dhëmbëve fqinjë, duke mënjanuar formimin e lezioneve mbi dhëmbët e ankorimit. Por mbi të gjitha duhet të lëjojë eruptimin e kaninit të impaktuar në qëndër të procesit alveolar, duke imituar eruptimin fiziologjik dhe njëkohësisht migrimin e indeve paradontale (12). Qëllimi i këtij punimi është të paraqesim hap pas hapi fazat e trajtimit ortodontiko-kirurgjikal të një kanini maksilar të impaktuar.
Rast klinikPacientja G.K e moshës 21 vjec u paraqit në klinikën
tonë për trajtim ortodontikNë ekzaminimin klinik shihet mungesa e kaninit maksilar të anës së majtë si dhe mungesa respektive e hapësirës në harkun dentar.(fig.1,2,3,4,5,6).
AbstraktTrajtimi i kombinuar ortodontiko-kirurgjikal për nxjerrjen e kaninit të impaktuar është zhvilluar dukshëm në vitet e fundit duke konsideruar jo vetëm menaxhimin e indeve të buta e të forta, por edhe forcat e tërheqjes. Qëllimi i punimit të mëposhtëm është të prezantojmë një rast klinik të një kanini maksilar të impaktuar të trajtuar në mënyrë kirurgjikale-ortodontike.Materiali dhe metoda. Pacienti u paraqit në klinikën tonë për një vizitë ortodontike. Nga kërkimet radiografike u evidentua kanini maksilar 23 i impaktuar dhe u vendos të rekuperohet me anë të një trajtimi të kombinuar ortodontiko-kirurgjikal. Rezultati: kanini u rekuperua në një kohë të pranueshme nga ana e pacientit si dhe u arrit vendosja e tij në harkadë në pozicionin e duhur. Konkluzioni: trajtimi i kaninit të impaktuar me metodën ortodontiko-kirurgjikale ka rezultate të mira dhe për këtë arsye duhet të jetë mëtoda dominuese në trajtimin e tyre.
iris çaçani1, Xhina mulo2, Rudin kusi1
Rast klinik i një kanini maksilar të impaktuar, i trajtuar në mënyrë ortodontike-kirurgjikale
1Klinikë private2Fakulteti i Mjekësisë Dentare
Fjale kyçe: kanin i impaktuar, ekspozim kirurgjikal, trajtim i kombinuar ortodontiko- kirurgjikal

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 147
Fig 1
Fig 3
Fig 5
Fig 2
Fig 4
Fig 6
Fig 7
Analiza radiografike na tregon praninë e 23 të impaktuar (fig 6)
Faza 1: Trajtimi ortodontik fillestar.Faza e parë e trajtimit parashikon vendosjen e aparatit
fiks për të drejtuar dhe ankoruar dhëmbët si dhe për përgatitjen e harkut dentar (për të krijuar hapësirën e nevojshme për kaninin e impaktuar).
Faza 2: Ekspozimi kirurgjikal me ndihmen e mjekut kirurg.1- Pas anestezisë lokale bëhet incizioni në anën
palatinale duke filluar nga pjesa meziale e premolarit të dytë deri në pjesën distale të centralit të anës tjetër. (fig 7)

Revista Stomatologjike Shqiptare148
2- Me lëvizje të ngadalta kryhet shkolitja e periostit dhe krijimi i lembos.
3- Zbulimi i koronës me anë të largimit të kujdesshëm të indeve të buta e të forta duke përdorur freza me shpejtësi të ulët.
4- Shpëlahet dhe thahet sipërfaqja e smaltit të dhëmbit të impaktuar. Për të shmangur hemorragjinë aplikohet një garzë e ngopur me solucion anestetik me vazokonstrigjentë ose me ujë të oksigjenuar dhe shtypet për disa minuta. Nuk ka nevojë për elektrokoagulim. Më pas vazhdohet me ngjitjen e një brakete te lidhur me një zinxhir metalik me anë të të cilit do të tërheqim dhëmbin e impaktuar.
5- Mbyllja dhe suturimi i lembos.
Tërheqja ortodontikeTërheqja ortodontike arrihet me përdorimin e fijeve
elastike direkt mbi harkun e fortë të aparatit fiks. Forca tërheqëse ishte rreth 50-60 g, me zevendësimin e fijes elastike cdo 15-20 ditë. Kontrolli radiografik rreth 4 muaj pas ndërhyrjes kirurgjikale (fig. 8).
Fig 8
Faza 3- Trajtimi ortodontik përfundimtar.Pas daljes së kaninit të impaktuar vazhdohet me
drejtimin dhe vendosjen e tij në harkun dentar si dhe merifiniturat e nevojshme për përfundimin e trajtimit të rastit. ( fig. 9,10, 11, 12, 13, 14)
Fig 9
Fig 11
Fig 10
Fig 12

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 149
Fig 13 Fig 14
1. Peck S, Peck l, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle orthod 1994; 64(4):249-56.
2. Kuftinec MM, Shapira Y. The impacted maxillary canine: Re-view of concepts, ASDC J Dent Child 1995; 62(5): 317-24.
3. Brin I, Becker A, Zilberman Y. Resorbed lateral incisors ad-jacent to impacted canines have normal crown size. Am J orthod Dentofacial orthop 1993; 104(1): 60-6.
4. Bishara SE. Impacted maxillary canines; a review Am J or-thod Dentofacial orthop 1992; 101(2): 159-71.
5. Cozza P, Mucedero M, Ricchiuti MR, Baccetti T. Il canino su-periore. Diagnosi e terapia basate sull’evidenza scientifica. Bologna: Edizioni Martina; 2010.
6. Quiryen M, op Heij DG, Adriansens A, opdebeeck HM, van Steenberghe D. Periodontal health of orthodontically ex-truded impacted teeth. A split-mouth, long-term clinical evaluation. J Periodontol 2000;71(11):1708-14.
7. Berglund l, Kurol J, Kvint S. orthodontic pre-treatment prior to autotransplantion of palatally impacted maxillary ca-nines: case reports on a new approach. Eur J orthod 1996; 18(5): 449-56.
8. Altonen M, Myllarniemi S. Results of surgical exposure of impacted cuspids and bicuspids in relation to patients’ so-matic and dental maturation. Int J oral Surg 1976;5(4): 180-6.
9. Wisth PJ, Norderval K, Booe oE. Comparison of two surgi-cal methods in combined surgical-orthodontic correc-tion of impacted maxillary canines. Acta odontol Scand 1976;34(1):53-7.
10. Gensior AM, Strauss RE. The direct bonding technique ap-plied to the management of the maxillary impacted canine. J Am Dent Assoc 1974;89(6):1332-7.
11. Crescini A, Nieri M, Buti J, Bacceti T, Mauro S, Prato GP. Short and long-term periodontal evaluation of impacted canines treated with a closed surgical-orthodontic approach. J Clin Periodontol 2007;34(3):232-42.
12. Crescini A, Clauser C Giorgetti R, Cortellini P, Pini Prato GP. Tunnel traction of infraosseous impacted maxillary canines. A thrre-year periodontal follow-up. Am J orthod Dentofa-cial orthop 1994;105(1):61-72.
13. McDonald F, Yap Wl. The surgical exposure and applica-tion of direct traction of unerupted teeth. Am J orthod 1986;89(4):331-40.
14. Kohavi D, Becker A, Zilberman Y. Surgical exposure, orthodontiv movement, and final tooth position as factors in periodontal breakdown of treated palatally impacted ca-nines. Am J orthod 1984;85(1):72-7.
15. Boyd Rl. Clinical assessment of injuries in orthodontic movement of impacted teeth. II. Surgical recommenda-tions. Am J orthod 1984;86(5):407-18.
REFERENCA

Revista Stomatologjike Shqiptare150
IntroductionCanines are the most frecuently impacted teeth in the
anterior region of the dental arch, with a prevalence of 1%-3% (1). These teeth have an important role in the shape of dental arch, in function and an important esthetic role (2). Impacted canines are associated with other anomalies such as root resorbtion of closedby teeth (3), decrease of the length of dental arch, odontogenic cists, local infections, ect (4,5). Therefore it is very important to reposition these teeth in the dental arch and to not extract them (6). During the last years, several ways of treatment for the impacted canines have been proposed. one of them is autotransplantion of the impacted canine in an alveola created by the surgeon. This includes the endodontic tretment of this tooth and the fixation of this tooth for an important period. In the literature we find a success of 90% (7). Altonen and Myllarniemi (8) in the middle of years ’70 proposed a conservative exposition of the canine with the open window technique. This tooth, in the presence of a neccessary space in the dental arch has the possibility to erupt, although not in the proper location. This result has made it possible to combine the orthodontic treatment with the surgical help (9). The surgical-orthodontic treatment of impacted canines has advanced significantly in the recent years, regarding the management of both hard (bone, enamel, dentine) and
soft tissues (gum) and forces of traction. In the past, a big amount of dental structure was sacrificed so that the pin could attach to the tooth. Nowdays, with the evolution of adhesive composites, we can expose a small part of the corona and attach the bracket to the tooth (10).
As for the soft tissues, it is not neccessary to open a big part of the gum (window technique) but with the closed techniques the soft tissues are conservated (11).
As for the forces of traction, light forces (less than 60g) are being used for the traction of the impacted teeth (4). The direction of the traction forces should be away of the roots of the addiacent teeth, to avoid lesions in the anchored teeth.
It is important that the impacted tooth erupts in the middle of the alveolar bone, imitating the fisiological eruption (12). The aim of this report is to describe all the fases of the surgical-orthodontic treatment of an impacted maxillary canine.
Case Report:Patient G.K, 21 years, has come at our clinic for an
orthodontic treatment. In the clinic examination is observed the absence of the left maxillary canine and lack of space in the dental arch (fig. 1,2,3,4,5).
Radiologic evaluation shows the impaction of the canine 23. (fig.6)
AbstractCombined surgical-orthodontic treatment of impacted maxillary canines has advanced significantly in recent years, regarding the management of both hard and soft tissues and forces of traction. The aim of this report is to describe a combined surgical-orthodontic approach used to treat an impacted maxillary canine.Materials and methods: G.K has come at our clinic for orthodontic treatment. Radiographic images showed a maxillary impacted canine (23) and we decided to treat the patient in a combined surgical-orthodontic way.Results: the canine was repositioned in the dental arch in a relatively short expected time.Conclusions: The combined surgical-orthodontic treatment is the right choice for impacted maxillary canines.
iris çaçani1, Xhina mulo2, Rudin kusi1
Case report of a maxillary impacted canine treated in a surgical-orthodontic way
1Private Clinic2 Faculty of Dental Medicine
key woRDS: impacted canine, surgical exposure, surgical- orthodontic treatment

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 151
Fig 1
Fig 3
Fig 5
Fig 2
Fig 4
Fig 6
Fig 7
Fase 1: Initial orthodontic treatment.The first fase of orthodontic treatment includes the
alignment and enchorage of the teeth. We prepared the dental arch and created the space for the canine in the dental arch.
Fase 2: Surgical exposure1- After local anesthesia the surgeon has made an
incision in the palatal side, begining from the mesial part of the second premolar to the distal part of the central tooth of the other side (7).

Revista Stomatologjike Shqiptare152
2- The lembo has been opened with very slow and careful movements.
3- Exposure of the canine by opening the soft and hard tissues, using low speed drills.
4- The surface of the exposed tooth has been irrigated and impregnet with vasoconstrigents to avoid bleeding. A bracket with a chain has been attached to the corona of the tooth with the help of adhesive composites.
5- Closure and suturation of the lembo.
Orthodontic traction.orthodontic traction is achieved by the use of elastic
legatures directly in the strong wires of fixed appliances. The traction forces were 50-60 grams. The elastic legatures were changed once in 15-20 days.
Radiographic evaluation 4 months after exposure (fig 8).
Fig 8
Fase 3: Final orthodontic treatment.After the eruption of the canine, the orthodontic
treatment is combined with the alignment of the tooth and final refinitures to finish the case. (fig.9,10,11,12,13,14)
Fig 9
Fig 11
Fig 10
Fig 12

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 153
Fig 13 Fig 14
1. Peck S, Peck l, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle orthod 1994; 64(4):249-56.
2. Kuftinec MM, Shapira Y. The impacted maxillary canine: Re-view of concepts, ASDC J Dent Child 1995; 62(5): 317-24.
3. Brin I, Becker A, Zilberman Y. Resorbed lateral incisors ad-jacent to impacted canines have normal crown size. Am J orthod Dentofacial orthop 1993; 104(1): 60-6.
4. Bishara SE. Impacted maxillary canines; a review Am J or-thod Dentofacial orthop 1992; 101(2): 159-71.
5. Cozza P, Mucedero M, Ricchiuti MR, Baccetti T. Il canino su-periore. Diagnosi e terapia basate sull’evidenza scientifica. Bologna: Edizioni Martina; 2010.
6. Quiryen M, op Heij DG, Adriansens A, opdebeeck HM, van Steenberghe D. Periodontal health of orthodontically ex-truded impacted teeth. A split-mouth, long-term clinical evaluation. J Periodontol 2000;71(11):1708-14.
7. Berglund l, Kurol J, Kvint S. orthodontic pre-treatment prior to autotransplantion of palatally impacted maxillary ca-nines: case reports on a new approach. Eur J orthod 1996; 18(5): 449-56.
8. Altonen M, Myllarniemi S. Results of surgical exposure of impacted cuspids and bicuspids in relation to patients’ so-matic and dental maturation. Int J oral Surg 1976;5(4): 180-6.
9. Wisth PJ, Norderval K, Booe oE. Comparison of two surgi-cal methods in combined surgical-orthodontic correc-tion of impacted maxillary canines. Acta odontol Scand 1976;34(1):53-7.
10. Gensior AM, Strauss RE. The direct bonding technique ap-plied to the management of the maxillary impacted canine. J Am Dent Assoc 1974;89(6):1332-7.
11. Crescini A, Nieri M, Buti J, Bacceti T, Mauro S, Prato GP. Short and long-term periodontal evaluation of impacted canines treated with a closed surgical-orthodontic approach. J Clin Periodontol 2007;34(3):232-42.
12. Crescini A, Clauser C Giorgetti R, Cortellini P, Pini Prato GP. Tunnel traction of infraosseous impacted maxillary canines. A thrre-year periodontal follow-up. Am J orthod Dentofa-cial orthop 1994;105(1):61-72.
13. McDonald F, Yap Wl. The surgical exposure and applica-tion of direct traction of unerupted teeth. Am J orthod 1986;89(4):331-40.
14. Kohavi D, Becker A, Zilberman Y. Surgical exposure, orthodontiv movement, and final tooth position as factors in periodontal breakdown of treated palatally impacted ca-nines. Am J orthod 1984;85(1):72-7.
15. Boyd Rl. Clinical assessment of injuries in orthodontic movement of impacted teeth. II. Surgical recommenda-tions. Am J orthod 1984;86(5):407-18.
REFERENCES

Revista Stomatologjike Shqiptare154
Hyrje Dhëmb i impaktuar, quhet një dhëmb të cilit i
ka ardhur koha për të dalë në harkadë, ka mbaruar zhvillimin e tij të plote dhe shanset për të dale i ka te pakta ne disa raste edhe nga trajtimi ortodontik, prandaj kërkon trajtim te kombinuar (1). Përqindja e hasjes së dhëmbëve te impaktuar dominohet nga molarët e tretë mandibularë , pastaj vijnë kaninët maksilarë, molarët e tretë maksilarë, kaninët mandibularë dhe premolrët. (1). Incidenca e tyre varion 0.8-5.2 % në vartësi të popullatës (3,4). Ndërkohë që molarët e tretë trajtohen në shumicën e rasteve me ekstraksion kirurgjikal, kaninët paraqesin një sfidë për trajtim konservativ. Trajtimi i tyre për ripozicionim në harkun dentar bëhet i mundur me anën e trajtimit të kombinuar, kirurgjikalo-ortodontik.
Qëllimi i këtij punimi është të paraqesë një rast klinik ku si teknikë kirurgjikale është zgjedhur , zbulimi i kaninit të impaktuar me teknikën e mbyllur të eruptimit.
Metoda e mbyllur indikohet kryesisht kur kanini ka pozicionim palatinal (5). Favorizon një ligament periodontal të shëndëtshëm mbas stimulimit të eruptimit të dhëmbit me anën e tërheqjes me forca ortodontike të kontrolluara.
Etiologjia e dhëmbëve të impaktuar përfshin faktorë lokalë dhe sistemikë (2). Në hasjen e kaninëve të impaktuar luajnë rol trashëgimia, sëmundjet endokrine. Disa sindroma shoqërohen me dhëmbë të impaktuar. Faktorë lokalë mund te jenë: traumat, tumoret ose kistat e regjionit, qëndrimi i gjatë ose
ekstraksioni i parakohshëm i dhëmbit të qumështit, periodontiti kronik apikal i dhëmbit të qumështit, ankilosis,faktori jatrogjene etj. Vihet re se impaktimi labial i kaninëve shoqërohet me mungësë hapësirash ne harkun dentar, kurse impaktimi palatinal i tyre vjen si rezultat i mungesës së guides gjatë rrugës së erruptimit.(5)
Diagnoza e kaninëve te impaktuar është kyç për suksesin e trajtimit, vendoset në bashkepunim midis mjekut ortodont dhe kirurgut oral. Diagnoza arrihet nëpërmjet një anamneze të kujdesshme, ekzaminimi intraoral dhe ekzaminime plotësuese që përfshijnë radiografi panoramike, grafi okluzale, skaner radiografi 3D, shumë të rëndësishmë për lokalizimin e kaninit të impaktuar.
Nga momenti kur mjeku ortodont në vartësi të diagnozës ortodontike dhe orientimit të kaninit të imapktuar në nofull, vendos që mund të sillet në hark dhëmbi, planifikohet koha e ndërhyrjes kirurgjikale. Indikacionet lokale për këtë proçedurë përcaktohen në bazë te pozicionimit të kaninit, raporteve të tij me dhëmbët fqinjë, largesisë nga plani i okluzionit si dhe këndit që formon boshti i kaninit me linjën mediane. Kunderindikacione lokale perveç rasteve të pozicionimit, janë dhe rastet kur janë zhvilluar kiste apo formacione tumorale dhe kur ka dhënë rezorbim të rrënjëve të dhëmbëve fqinje. Kunderindikacione janë dhe rastët kur pacienti ka patologji të përgjithshme që nuk lejojnë ndërhyrje kirurgjikale ( sëmundje gjaku, defiçite imunitare, pacientë që i janë nënështruar kemio apo radioterapise, etj)
AbstraktKaninët e imapktuar hasen shpesh në praktikën stomatologjike. Për shumë kohë trajtimi i tyre ka qenë ekstraksioni kirurgjikal dhe zëvendesimi protetik ose mbajtja nën observim. Sot gjithmonë e më shumë po trajtohen në mënyrë që të ruhet ky dhëmb i rëndësishëm dhe te rreshtohet ne harkadën dentare në pozicionin korrekt. Kjo bëhet e mundur nëpërmjet trajtimit të kombinuar kirurgjikalo-ortodontik. Ndërkohë që indikacionet per trajtim, llojin e apartit ortodontik e percakton mjeku ortodont, sfidë për kirurgun oral është lokalizimi i dhëmbit, rrjedhimisht vëndin dhe teknikën e ndërhyrjes që do mundësojë ekspozimin e kurorës së dhëmbit dhe aplikimin e butonit. Gjithashtu ka rëndësi mosdëmtimi i formacioneve fqinje ose vetë dhëmbi apo ligamenti periodontal.Ne do sjellim një rast klinik që u diagnostikua me kanin maksilar majtas të impaktuar , ekzaminimet e nevojshme dhe ndërhyrjen kirurgjikale me metodën e eruptimit të mbyllur.
Nineta Fino1, Ramazan isufi² , adela alushi³
trajtimi kirurgjikalo-ortodontik i kaninit të impaktuar (raportim rasti )
1SPA, Universiteti “Aldent “2 Prof.Dr, Shef i Derartamentit të Kirurgjisë Oro-Max-Fac, Universiteti i Mjekësisë Dentare.3 Msc, Universiteti “Aldent”
Fjale kyçe: Kanin, impaktim, zbulim kirurgjikal, trajtim.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 155
Tabela e mëposhtme ilustron indikacionet lokale: (7)
Kategoria Prognozë e mirë Mesatare E varfër
Mbivendosje me centralin
Pa mbivendosje Deri ne gjysëm të rrënjës Mbivendosje e plote
lartësia nga plani i okluzionit
Në nivelin e lidhjes zmalto-cement
Në gjysëm të gjatësisë të rrënjës
Me lart së gjatësia e rrënjës
Kendi i boshtit të dhëmbit me linjën
mediane
0-15° 16-30° >30°
Pozicionimi i apeksit
Mbi pozicionin e kaninit Mbi premolarin e parë
Mbi premolarin e dytë
Përdoren disa teknika kirurgjikale për zbulimin e kaninëve të impaktuar:1. Zbulim ekcizional (gingivectomi). Konsiston në
zbulimin e kurorës nga indet e buta ose të forta sipas rastit klinik.
2. Pozicionim apikal i lembos. Konsiston në hapjen e lembos dhe mukoperiostale, zbulim kurore dhe ripozicionim mbi butonin duke mbuluar lidhjen zmalt-cement.
3. Teknika e mbyllur e eruptimit.konsiston në hapjen e lembos mukoperiostale, zbulim i kurorës, ngjitjen e butonit dhe suturim i lembos në pozicionin fillestar, duke realizuar mbulim të plotë.
Zgjedhja e teknikës së duhur do sigurojë eruptim të thjeshtë dhe pa komplikacione.
Rasti klinikPacientja F.P seksi femër, 19 vjeç paraqitet te
stomatologu i përgjithshëm me ankesën se i lëviz kanini ana e majtë sipër (63). Mjeku stomatolog konstaton se dhëmbi që është në hark, është dhëmbi i qumështit dhe se kanini i përhershëm (23) mungon
në harkadë. Rekomandon pacienten për konsultë tek mjeku ortodont.
Pasi u be ekzaminimi intraoral, kontroll me panoramex digital,cefalometri, u vendos diagnoza : 23 i impaktuar i cili ka të dhëna të favorshme për tu sjelle ne harkadë.
Klinikisht u vu re prezenca e kaninit te qumeshtit (63) ne harkade dhe tumefaksion I lehte ne anen e majte palatinale ne nivelin e rrenjeve te dhembeve.
Pacientja kishte pasur një zhvillim normal të sistemit dentar, dalje të dhëmbëve të qumështit ne kohë dhe ndërrim i tyre normal dhe pa çrregullime lokale dhe të përgjithsshme. Nuk kishte vuajtur nga ndonjë sëmundje e përgjithshme në fëmijëri. Nuk kishte patologji të përgjithshme shoqëruese.
Në anamnezën familjare, del se dhe mamaja e pacientes kishte patur po të njëjtin problem, me njerin nga kaninët.
Paraprakisht u fillua me trajtim ortodontik me aparat fiks për të krijuar hapësirë midis lateralit dhe premolarit superior te anës së majtë pak më shumë se sa diametri mezio-distal i kaninit.
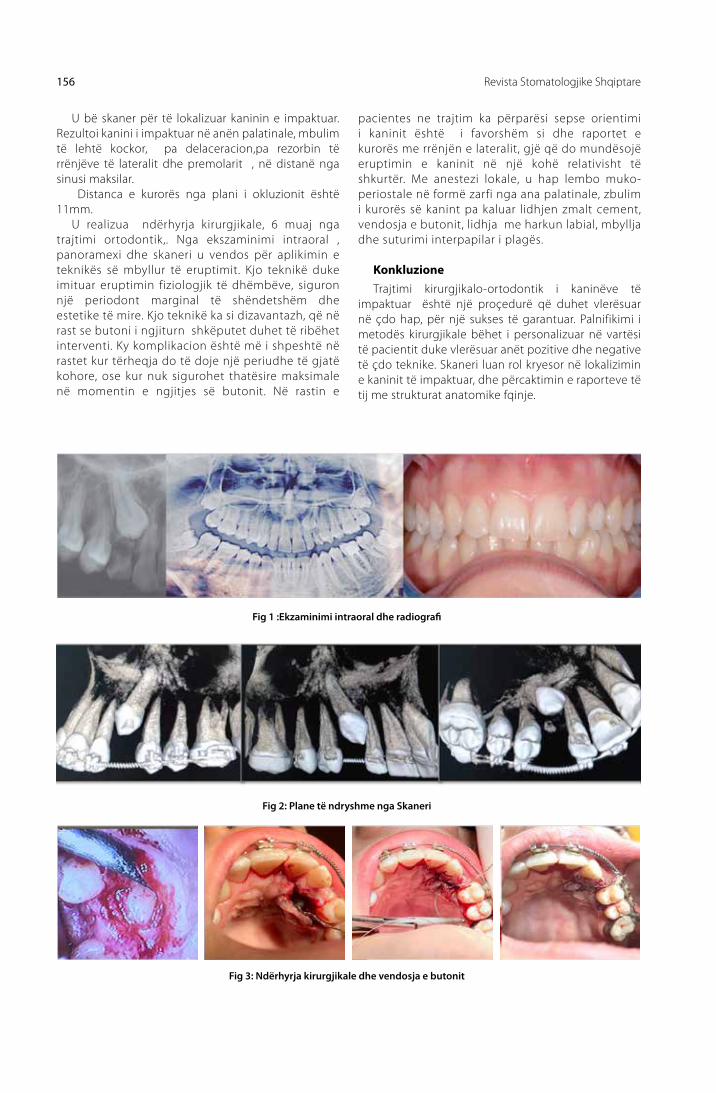
Revista Stomatologjike Shqiptare156
u bë skaner për të lokalizuar kaninin e impaktuar. Rezultoi kanini i impaktuar në anën palatinale, mbulim të lehtë kockor, pa delaceracion,pa rezorbin të rrënjëve të lateralit dhe premolarit , në distanë nga sinusi maksilar.
Distanca e kurorës nga plani i okluzionit është 11mm.
u realizua ndërhyrja kirurgjikale, 6 muaj nga trajtimi ortodontik,. Nga ekszaminimi intraoral , panoramexi dhe skaneri u vendos për aplikimin e teknikës së mbyllur të eruptimit. Kjo teknikë duke imituar eruptimin fiziologjik të dhëmbëve, siguron një periodont marginal të shëndetshëm dhe estetike të mire. Kjo teknikë ka si dizavantazh, që në rast se butoni i ngjiturn shkëputet duhet të ribëhet interventi. Ky komplikacion është më i shpeshtë në rastet kur tërheqja do të doje një periudhe të gjatë kohore, ose kur nuk sigurohet thatësire maksimale në momentin e ngjitjes së butonit. Në rastin e
pacientes ne trajtim ka përparësi sepse orientimi i kaninit është i favorshëm si dhe raportet e kurorës me rrënjën e lateralit, gjë që do mundësojë eruptimin e kaninit në një kohë relativisht të shkurtër. Me anestezi lokale, u hap lembo muko-periostale në formë zarfi nga ana palatinale, zbulim i kurorës së kanint pa kaluar lidhjen zmalt cement, vendosja e butonit, lidhja me harkun labial, mbyllja dhe suturimi interpapilar i plagës.
Konkluzione Trajtimi kirurgjikalo-ortodontik i kaninëve të
impaktuar është një proçedurë që duhet vlerësuar në çdo hap, për një sukses të garantuar. Palnifikimi i metodës kirurgjikale bëhet i personalizuar në vartësi të pacientit duke vlerësuar anët pozitive dhe negative të çdo teknike. Skaneri luan rol kryesor në lokalizimin e kaninit të impaktuar, dhe përcaktimin e raporteve të tij me strukturat anatomike fqinje.
Fig 1 :Ekzaminimi intraoral dhe radiografi
Fig 2: Plane të ndryshme nga Skaneri
Fig 3: Ndërhyrja kirurgjikale dhe vendosja e butonit

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 157
1. ISuFI.R, QËNDRo.A, BARDHoSHI.E, KIRuRGJIA oRAlE DHE MAKSIlo-FACIAlE (2010), ribotim (2015). Vol I
2. PETERSoN’S PRINCIPlES oF oRAl AND MAXIlloFACIAl SuRGERY,second edition. 2004
3. Brin I, Becker A, Shalhav M. Position of the Maxillary Perma-nent Canine in Relation to Anomalous or Missing lateral Incisors: a Population Study. European Journal of ortho-dontics 1986; 8(1) 12-16.
4. Chu FC, li TK, lui VK, Neësome PR, Choë Rl, Cheung lK. Prevalence of Impacte ed Teeth and Associated Patholo-gies-a Radiographic Study of the Hong Kong Chiw nese Population. Hong Kong Medical Journal 2003; 9(3) 158-163.
5. Gazi university, Faculty of Dentistry, Department of ortho-dontics, Ankara, Turkey . Emerging Trends in oral Health Sciences and Dentistry, Clinical Consideration and Man-agement of Impacted Maxillary Canine Teeth http://dx.doi.org/10.5772/59324
6. Prof.Asc Gafur SHTINo, Prof.Dr. Ramazan ISuFI Atlas i Kirurgjisë orale dhe Maksilo- Faciale 2011
7. K. Counihan, Al-Aëadhi, J.Butler. Guideliness for the assess-ment of the impacted maxillary canine 2013 http://www.exodontia.info/files/Dent_update_2013._Guidelines_for_the_Assessment_of_the_Impacted_Maxillary_Canine.pdf
REFERENCA

Revista Stomatologjike Shqiptare158
Introduction Impacted tooth is called a tooth whose time has
come to erupt in dental arch, has completed its full development and chances for eruption are slim also from orthodontic treatment, therefore it requires a combined treatment (1). The percentage of incidence of impacted teeth is dominated mostly by mandibular third molars, followed by maxillary canine, maxillary third molars, mandibular canines and premolars (2). Their incidence varies depending 0.8-5.2% of the population (3, 4). While the third molars in most cases are treated with surgical extraction, canine poses a challenge for conservative treatment. Their treatment for repositioning in the dental arch is made possible through combined surgical-orthodontic treatment.
The purpose of this paper is to present a clinical case where the surgical intervention selected is exposure of impacted canine with erupted closed technique.
Closed technique is indicated mainly when canine is positioned on palatine side (5). Favors a healthy periodontal ligament after stimulation of the tooth erupted through controlled orthodontic force traction.
The etiology of impacted teeth includes local and systemic factors (1), such as heredity role, endocrine diseases. Some syndromes are associated with impacted teeth. local factors can be: trauma, tumor or cyst in the region, the long stay or premature
deciduous tooth extraction tooth, deciduous tooth apical chronic periodontitis, ankylosis, iatrogenic factors etc. It is noted that the impacted canine from labial side is associated with a lack of space in the dental arch, and from palatine side comes as a result of lack of guide along the eruption way. (5)
Diagnosis of impacted canine which is the key to treatment success is based on cooperation between orthodontist and oral surgeon. Diagnosis is achieved through a careful anamnesis, intraoral examination and additional tests that include panoramic radiograph, occlusal x-ray and 3D X-ray scanner, very important for the localization of impacted canine.
From the moment the orthodontist decides that this tooth can be brought to arc based on orthodontic diagnosis and on the orientation of the maxillary impacted canine, then timing of surgery is planned. local indications for this procedure are determined based on the canine position, his relations with the adjacent teeth, distance from the occlusion plan and the angle formed by the axis of the canine with the median line. local contraindications except in cases of positioning are cases where formation of cists or tumors is developed and root resorption of adjacent teeth has happened. Also contraindications are cases when patient has general pathologies that do not allow surgery intervention such as (blood diseases, immune diseases, patients who have undergone chemotherapeutic or radiation therapy, etc.)
AbstractThe impacted canines are frequently encountered in dental practice. For a long period of time, their treatment was surgical extraction and prosthetic replacement or keeping it under observation. Nowadays these clinical cases are being treated more and more in order to preserve this important tooth and aligned it in dental arcade in the correct position. This becomes possible through combined surgical-orthodontic treatment. While the indications for treatment and the type of orthodontic appliance is determined by orthodontist, the challenge for oral surgeon is locating the tooth, thus the place and intervention techniques that will enable the exposure of tooth crown and the application button. Also it is important not to cause damage adjacent formations or the tooth itself and periodontal ligament. We will bring a clinical case that was diagnosed with impacted canine, the necessary examinations and surgical intervention with erupted closed technique.
Nineta Fino1, Ramazan isufi² , adela alushi³
Surgical - orthodontic treatment of impacted canines (case report)
1SPA, Universiteti “Aldent “2 Prof.Dr, Shef i Derartamentit të Kirurgjisë Oro-Max-Fac, Universiteti i Mjekësisë Dentare.3 Msc, Universiteti “Aldent”
keywoRDS: Canine, impacted, surgical exposure, treatment.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 159
The following table illustrates the local indications: (7)
Category Good prognosis Average Poor
overlap of incisor
No horizontal overlap up to half root width Complete overlap
Vertical height
CEJ – halfway up root >half <full root length >full root length
Angulation
0-15° 16-30° >30°
Position of apex
Above canine position Above 1st premolar
Above 2nd premolar
Several surgical techniques are used for exposure of impacted canine: 1. Excisional detection (gingivectomy). It consists in
exposing the crown of tooth from soft or hard tissue depending on the clinical case.
2. Apically positioned flap. It consists on mucoperiosteal flap opening, exposure of crown and reposition of the crown with the button by covering CEJ.
3. The closed eruption technique. It consists on mucoperiosteal flap opening, exposure of crown, attachment of the button and suture of flap in original position, achieving full coverage.
Choosing the proper technique will provide simple eruption and without complications.
Clinical caseFemale patient with initials F.P, 19 years old
is presented at a general dentist office with the complaint that her left maxillary canine tooth is moving. The dentist finds that the tooth in the arch is deciduous tooth and permanent canine (23) is
absent in the dental arch. The dentist recommends the patient for a consult with orthodontist.
After intraoral examination, digital panoramic x-ray, cephalometry, diagnosis is set; tooth nr.23 is impacted however with favorably data to be brought into the dental arch.
Clinically it was observed the presence of deciduous canine (63) in dental arch and a light swelling on left palatine side at roots level.
The patient had a normal development of the dental system; deciduous teeth were erupted and replaced on time without any local or general disorders. Patient had not suffered from any disease overall in childhood and there was no general pathology associated.
In family history, it appears that her mother had the same problem with one of the canines.
Beforehand it started with fixed orthodontic treatment to create space between lateral incisor and premolar on the left side just a little more than mesio - distal diameter of the canine.
The scanner was done to locate the impacted canine. The impacted canine resulted on palatal side,

Revista Stomatologjike Shqiptare160
light cover with hard tissue, without dilacerations without roots resorbtion of lateral and premolar and in good distance from maxillary sinus.
Crown distance from occlusal plane is 11mm. The surgery intervention was done after 6 months
of orthodontic treatment. After intraoral examination, panoramic x-ray and scanner was decided for the application of closed erupted technique. This technique mimics the physiological way of tooth eruption and provides a healthy marginal periodontal tissue and good aesthetic. However this technique has the disadvantage that if the next button detaches the whole intervention needs to be redone. This complication is more frequent when the traction would want a long period of time, or the maximum dryness is not achieved at the time of attachment of the button. In our case the patient has the advantage because canine orientation is favorable and also the
ratio of the crown with the root of lateral, which will enable the canine to erupt in a relatively short time. local anesthesia was used, opened envelope shaped mucoperiostal flap from the palatal side, canine crown was detected without passing CEJ, button was placed, linked with labial bow, and interpapillary suture was used to close the opening.
ConclusionsSurgical-orthodontic treatment of impacted
canine is a procedure that must be assessed at every step, for a guaranteed success. Planning the surgical intervention requires a case by case study depending on the patient by evaluating the pros and cons of each technique. Scanner plays a major role in the localization of impacted canine, and the determination of its relations with the adjacent anatomical structures.
Fig 1
Fig 2
Fig 3

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 161
1. ISuFI.R, QËNDRo.A, BARDHoSHI.E, KIRuRGJIA oRAlE DHE MAKSIlo-FACIAlE (2010), ribotim (2015). Vol I
2. PETERSoN’S PRINCIPlES oF oRAl AND MAXIlloFACIAl SuRGERY,second edition. 2004
3. Brin I, Becker A, Shalhav M. Position of the Maxillary Perma-nent Canine in Relation to Anomalous or Missing lateral Incisors: a Population Study. European Journal of ortho-dontics 1986; 8(1) 12-16.
4. Chu FC, li TK, lui VK, Neësome PR, Choë Rl, Cheung lK. Prevalence of Impacte ed Teeth and Associated Patholo-gies-a Radiographic Study of the Hong Kong Chiw nese Population. Hong Kong Medical Journal 2003; 9(3) 158-163.
5. Gazi university, Faculty of Dentistry, Department of ortho-dontics, Ankara, Turkey . Emerging Trends in oral Health Sciences and Dentistry, Clinical Consideration and Man-agement of Impacted Maxillary Canine Teeth http://dx.doi.org/10.5772/59324
6. Prof.Asc Gafur SHTINo, Prof.Dr. Ramazan ISuFI Atlas i Kirurgjisë orale dhe Maksilo- Faciale 2011
7. K. Counihan, Al-Aëadhi, J.Butler. Guideliness for the assess-ment of the impacted maxillary canine 2013 http://www.exodontia.info/files/Dent_update_2013._Guidelines_for_the_Assessment_of_the_Impacted_Maxillary_Canine.pdf
REFERENCES

Revista Stomatologjike Shqiptare162
HyrjePrevalencën më të lartë të inkluzionit të dhëmbëve
e kanë molarët e tretë dhe kaninët maksilarë, më të ulët e kanë incizivët, premolarët mandibularë etj. Molarët e tretë veçanërisht ata inferiorë kanë një prevalencë inkluzioni rreth 20-30% më të lartë në krahasim me dhëmbët e tjerë. Prevalenca e inkluzionit të kaninit maksilar permanent është 1-2% në popullatë. Këto inkluzione ndodhin si pasojë e faktorëve gjenetikë, defiçencës endokrine, rrezatimit, palatoskizave, disharmonive dento-maksilare dhe ndërmjet premaksilës dhe maksilës, defiçencës transversale të maksilës anteriore, mungesës së hapësirës, faktorëve që lidhen me humbjen e parakohshme të dhëmbëve të qumështit, bllokim i proçesit eruptiv, pozicioni ektopik etj. Plani i trajtimit është multidisiplinar:Kirurgji orale, ortodonci dhe protetikë. Në disa raste të komplikuara, veçanërisht në dhëmbë inkluzë tërësisht horizontal dhe me rrënjë shumë të diverguara, trajtimi ortodontik është i pamundur dhë ekstraksioni i tyre mbetet i vetmi opsion. Ekziston një diferencë e rëndësishme ndërmjet nozologjive retinuar/inkluzë: Dhëmbë inkluzë janë ata dhëmbë që e kanë të formuar rrënjën dhe për këtë nuk eruptojnë më. Dhëmbët e retinuar janë dhëmbët që nuk e kanë të formuar rrënjën dhe
për këtë e kanë mundësinë e proçesit të eruptimit në vazhdim.
Përshkrim i rastitNjë pacient mashkull 27 vjeçar paraqitet në klinikë
për një rehabilitim protetik të dhëmbëve që i mungojnë në regjionin e djathtë maksilar. Nga anamneza pacienti referon që nuk ka ekstraktuar asnjë dhëmb në këtë regjion dhe dyshimet hiqen plotësisht nga imazhi panoramik. Ne imazhin radiologjik vëmë re 3 dhëmbë multiple inkluzë, ku kemi 12 pjesërisht inkluz, 13 dhë 15 totalisht inkluz. Gjithashtu nga ekzaminimi klinik arritëm ne përfundimin qe keto inkluzione dentale ndodhen ne pozicionin vestibular. Është zgjedhur nga vetë pacienti, pas prezantimit të modaliteteve të ndryshme të trajtimit, ekstraksioni i këtyre dhëmbëvë si plan trajtimi përfundimtar dhe vendosja e një punimi protetik fiks për zëvendësimin e dhëmbëve të munguar. Ekstraksioni i dhëmbëve inkluzë është bërë me teknikën konvencionale kirurgjikale nën anestezi lokale:lembo trekëndore mukoperiostale vestibulare, osteotomi me pjesamen të drejtë dhe freza kockore, odontomi, luksimi dhe ekstraksioni me elevator të 12, 13 15;suture e lembos.
AbstraktDhëmbët inkluzë i ndeshim shumë shpesh në praktikën e përditshme klinike. Dhëmbët inkluzë i zbulojmë nga ekzaminimet radiologjike panoramik rutinë sepse jo të gjithë pacientët vijnë nga simptoma(dhimbja). Inkluzionet i ndeshim në dhëmbë të ndryshëm,në regjione të ndryshme,në pozicione të ndryshme,por më të rralla janë rastet kur ndeshim dhëmbë multiple inkluzë në të njëjtin regjion. Në këtë artikull në prezantojmë një rast klinik me 3 dhëmbë inkluzë në regjionin e djathtë maksilar.
Remi likaj, alba likaj
Dhëmbët multiple inkluzë-Rishikimi i literaturës dhe raportim rasti
Klinika dentare private “REAL” Durrës
Fjalët kyçe: dhëmbë multiple inkluzë, pozicion ektopik, ekzaminim radiologjik, dhëmb i retinuar
Fig. 1 Pamje radiologjike e dhëmbëve inkluzë Fig. 2 laterali gjysëm inkluz

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 163
Fig. 3 kanini total inkluz
Rezultate:Dhëmbët inkluzë janë raste të shpeshta në praktikën
klinike vecanërisht molarët e tretë dhe kaninët. Prevalencën më të ulët të inkluzioneve dentare e kanë inçizivët supërior, premolarët mandibularë dhe akoma më të rralla janë rastet që shoqërohen me inkluzione
dentare multiple në të njëjtin regjion siç është dhe ky rast që ne po raportojmë. Ekzaminimet radiologjike panoramike luajnë një rol të rëndësishëm në zbulimin e këtyre inkluzioneve dentare edhe pse jo të gjitha inkluzionet dentare shoqërohen me simptoma.
1. Ajith SD, Shetty S, Hussain H, Nagaraj T, Srinath M. Manage-ment of multiple impacted teeth:A case report and review. J Int oral Health. 2014;6:93-8.
2. Shaw B, Schneider. S. S Zeyer, J. Surgical management of ankylosed impacted maxillary canines. J Am oent Assoc 1981;102:497-500
3. Dachi, S. F. Hawell, F. V. A survey at 3, 874 routine full mouth radiographs. oral Surg oral Med oral Path 1961;14:1165-9
4. Scottish Intercollegiate Guidelines Network (SIGN). SIGN Guidelines:management of unerupted teeth. Edinburgh;SIGN 2001 SIGN publication n. 43).
5. Hupp, James R. , et. al. Contemporary Maxillofacial Surgery, 6E, Elsevier –Mosby, 2014. ISBN 978-0-323-09177.
6. lytle JJ. Etiology and indications for the management of impacted teeth. Northwest Dent. 1995;74:23-32
REFERENCA
Fig. 5 alveolat postestraktive
Fig. 4 premolari i dytë inkluz
Fig. 6 Suturat

Revista Stomatologjike Shqiptare164
IntroductionThe higher prevalence of inclused teeth has third
molars and maxillary canines and the lowers has incizives, mandibular premolars ect. Third molars, espetially inferior molars, have a inclusion prevalence about 20-30 % higher than other teeth. The prevalence of maxillary permanent canine impaction is 1-2% in the general population. This inclusion occur because of genetic factors, endocrine deficiency, irradiation, palatal clefts, dento maxillary disharmony, growth disharmony between premaxilla and maxilla, transverse growth deficiency of the anterior maxilla, overlap of eruption process, ectopic position, factors that are connecting with early loss of deciduos teeth ect. The plan of treatment is multidisciplinary:oral surgery, orthodoncy and prosthodonty. In complicated cases, espetially in cases where the inclusion teeth are totally horizontal or their roots are divergent, is very difficult orthodontic treatment and oral surgery is the only option. It is very important to understand the difference between retention/inclusion: The radix of inclused teeth is shaped and for this reason their
eruption is not possible. The radix of reteined teeth is not shaped and for this reason their eruption is possible continually.
Case reportA 27 years old man visited the dental clinic for
prosthetic rehabilitation in the right maxillary region. From anamneses, the patient refered that he had never extracted any tooth and suspicions are eleminated from panoramic radiographs. In the X-ray we see 3 teeth inclused:12 partial inclused, 13 and 15 totally inclused. Also from clinic and x-ray examination we verified that teeth are inclused in vestibular position. The patients choice was the extraction of teeth as the final plan of treatment and a metal- ceramic bridge placement, after we have introduced alternative treatments. The extraction of inclused teeth is realized with conventional surgical tecnic:triangular mucoperiostal lembo, osteotomy with straight handpiece and cutter osseous, odontomy, luxation and final extraction with elevator of 12, 13 15, suture of lembo.
AbstractThe inclusion of teeth is very frequently in our dental practice.Screening commonly includes clinical examination as well as x-rays such as panoramic radiographs because not all the patients came from pain(symptoms). The dental inclusions occur in different teeth,in different regions,but more rarely are the cases where these multiple inclused teeth occur in the same region.In this article we report a clinical case with multiple inclused teeth in the right maxillary region.
Remi likaj, alba likaj
management of multiple inclused teeth- Review of literature and case report
Private dental clinic “REAL” Durres
keywoRDS: multiple inclused teeth, ectopic position, radiographic examination, reteined teeth.
Fig.1 Radiological view of inclusions Fig.2 Lateral partially incluse

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 165
Fig.3 canine totally inclused
Fig. 5 Postextraction alveols
Fig. 4 Premolar totally inclused
Fig. 6 Suture
ConclusionsThe inclusion of teeth are routine cases in our
dental practice,espetially third molars and canines.The lower prevalence has superior incizives,mandibular
premolars and more rarely are the cases with multiple inclused teeth in the same region as this case report.Routine panoramic radiographs are very important in exploration of inclusions even not all the dental inclusions occur with symptoms.
1. Ajith SD, Shetty S, Hussain H, Nagaraj T, Srinath M. Manage-ment of multiple impacted teeth:A case report and review. J Int oral Health. 2014;6:93-8.
2. Shaw B, Schneider. S. S Zeyer, J. Surgical management of ankylosed impacted maxillary canines. J Am oent Assoc 1981;102:497-500
3. Dachi, S. F. Hawell, F. V. A survey at 3, 874 routine full mouth radiographs. oral Surg oral Med oral Path 1961;14:1165-9
4. Scottish Intercollegiate Guidelines Network (SIGN). SIGN Guidelines:management of unerupted teeth. Edinburgh;SIGN 2001 SIGN publication n. 43).
5. Hupp, James R. , et. al. Contemporary Maxillofacial Surgery, 6E, Elsevier –Mosby, 2014. ISBN 978-0-323-09177.
6. lytle JJ. Etiology and indications for the management of impacted teeth. Northwest Dent. 1995;74:23-32
REFERENCES

Revista Stomatologjike Shqiptare166
kuRoRЁZohet me SukSeS pRoçeSi i akReDitimit iNStituCioNal tЁ uNiveRSitetit tЁ mjekЁSiSЁ, tiRaNЁ, Duke u vleRЁSuaR me makSimumiN
e plotЁSimit tЁ StaNDaRteve Nё datёn 21 shtator 2017, Agjensia e Akreditimit tё
Arsimit Tё lartё (APAAl), nё bashkёpunim me Agjencinё Britanike tё Akreditimit (QAA), dha rezultatin definitiv tё Akreditimit Institucional tё universitetit tё Mjekesisё, Tiranё: universiteti i Mjekёsisё fiton akreditimin 5 vjeçar!
Proçesi i akreditimi tё uMT u zhvillua nё kuadrin e akreditimit tё pёrgjithshёm institucional tё tё gjitha Institucioneve tё Arsimit tё lartё nё Shqipёri. Ky proçes u zhvillua me disa etapa dhe, pas njё pune kolosale lidhur me hartimin dhe sistemimin e dokumentacionit tё detajuar mbi veprimtarinё e uMT, nё 10-12 maj 2017 u zhvilluan takime intensive direkte tё Ekspertёve tё Akreditimit tё APAAl dhe tё Agjencisё Britanike (QAA), me Rektorin dhe stafin drejtues tё universitetit tё Mjekёsisё dhe tё Fakulteteve tё Mjekёsisё, Mjekёsisё Dentare dhe tё Shkencave Mjekёsore Teknike; me stafin akademik dhe administrativ tё uMT, si dhe me studentё tё tё gjitha cikleve tё studimit.
lajmi i akreditimit institucional tё uMT nё vendin e parё tё universiteteve shqiptare me maksimumin e plotёsimit tё standarteve ёshtё konfirmimi mё i mirё i performancës dhe nivelit tё lartё tё stafit akademik dhe administrativ,
rrjetit formues tё qendrave spitalore universitare tё Tiranёs, tё studentёve tanё, tё cilёt pёrbёjnё elitёn e nxёnёsve tё sistemit arsimor shqiptar; vizionit europian tё shtetit shqiptar dhe mbi tё gjitha, tё traditёs mёsimdhёnёse 65 vjeçare tё Fakultetit tё Mjekёsisё, i organizuar prej 4 vjetёsh si universiteti i Mjekёsisё, Tiranë.
Sigurisht qё njё meritё tё madhe ka stafi i Rektoratit tё uMT, grupi i punёs dhe pёrfaqёsuesit e çdo fakulteti, tё cilёt pёrballuan me pёrgjegjshmёri tё lartё dhe pёrkushtim ngarkesёn e madhe tё njё pune tё gjatё, tё vёshtirё dhe voluminoze.
urime dhe falenderime pёr çdo pjesёtar tё stafit akademik dhe administrativ tё uMT dhe tё Fakultetit tё Mjekёsisё Dentare, si dhe pёr tё gjithё studentёt dhe ata qё kontribuan nё çdo hallkё e nё çdo detaj tё kёtij procesi, duke ndihmuar dhe ndikuar nё zhvillimin e suksesshёm tё procesit kaq tё rёndёsishёm tё Akreditimit.
Nder, pёrgjegjёsi dhe ndёrgjegjёsim qё kemi ende shumё pёr tё bёrё!
Urime tё gjithёve dhe suksese tё mёtejshme!

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 167
FiNaliZohet BaShkëpuNimi NDëRmjet Fakultetit të mjekëSiSë DeNtaRe Dhe BaShkiSë Së tiRaNëS
Në vijim të bisedave ndërmjet Dekanes së Fakultetit të Mjekësisë Dentare, Prof.Asc.Edit Xhajanka dhe Këshilltares së Kryetarit të Bashkisë së Tiranës, u vendos që të krijohen mundësi bashkëpunimi ndërmjet Fakultetit të Mjekësisë Dentare dhe Bashkisë së Tiranës.
Ky bashkëpunim konsiston në organizimin e një Projekti të përbashkët për “Edukimin Shëndetësor dhe Promocionin mbi shëndetin dentar dhe oral në fëmijët e çerdheve, kopshteve dhe shkollave 9 vjeçare të Tiranës”. Projekti do të realizohet me angazhimin e studentëve të FMD, kryesisht të viteve të larta, të stafit akademik dhe drejtuesve të dy institucioneve. Një rol të rëndësishëm do të ketë në këtë projekt edhe “Shoqata e Dentistrisë Pediatrike Shqiptare”, me kryetare Dr. Shk. Manola Kelmendi.
Në datën 11 tetor 2017, në ambjentet e Bashkisë së Tiranës, u realizua një takim ndërmjet Kryetarit të Bashkisë, Z. Erion Veliaj, Dekanes, Prof. Asoc. Edit Xhajanka, dhe Zv. Dekanes së Fakultetit të Mjekësisë Dentare, Prof. Vergjini
Mulo. Në takim merrnin pjesë dhe një grup studentësh ekselentë, pjesmarrës aktivë në projektin e mësipërm, si dhe koordinatorja e studentëve për projekte të ndryshme sociale, Dr. Neada Hysenaj.
Pas diskutimit mbi detajet e projektit, u nënshkrua një memorandum bashkëpunimi ndërmjet FMD dhe Bashkisë së Tiranës. Kryetari i Bashkisë mori përsipër personalisht ndjekjen e projektit dhe, sigurisht, që marrëveshja do të materializohet me fillimin e vitit akademik 2017-2018. Ky projekt do t’i shërbejë jo vetëm ngritjes së nivelit të profilaksisë dhe promocionit në fëmijët 0-18 vjeç të rrethit të Tiranës, por edhe nxjerrjes së treguesve statistikorë aktualë për Shqipërinë dhe indekseve lidhur me sëmundshmërinë karioze dhe defektet dentare në këtë grupmoshë.
Duke falenderuar stafin e Bashkisë, studentët dhe gjithë personat e përfshirë në projekt, urojmë që bashkëpunimi i Fakultetit të Mjekësisë Dentare me Bashkinë e Tiranës të jetë sa më i suksesshëm dhe t’i shërbejë brezit të ri.

Revista Stomatologjike Shqiptare168
maRRëveShje BaShkëpuNimi miDiS uNiveRSitetit të pRiShtiNëS “haSaN pRiShtiNa” Dhe uNiveRSitetit të mjekëSiSë, tiRaNë.
Në datën 17.07.2017 në ambjentet e Rektoratit të universitetit të Mjekësisë, Tiranë u zhvillua takimi mes përfaqësuesve të universitetit të Prishtinës “Hasan Prishtina” dhe universitetit të Mjekësisë, Tiranë. Në këtë takim ishin të pranishëm Rektorët e dy universiteteve dhe njëkohësisht Zëvendës Rektorët e këtyre të fundit, sikundër përfaqësues të stafit akademik dhe autoritete drejtuese të fakulteteve në uMT. Kryefjala e këtij takimi ishte marrëveshja midis dy universiteteve dhe dobia e nënshkrimit të saj. Përfaqësuesit e universiteteve përkatës diskutuan mbi shkëmbimin e përvojave në programe të ndryshme studimore, si edhe në projekte
të ndryshme të kërkimit shkencor. Shkëmbimi sistematik i stafit akademik dhe i studentëve u nënvizua si faktori thelbësor në zhvillmin e ndërsjelltë institucional.
Në fund të takimit Rektori i universitetit të Mjekësisë, Prof. Dr. Arben Gjata dhe Rektori i universitetit të Prishtinës “Hasan Prishtina”, Prof. Dr. Marjan Dema nënshkruan marrëveshjen e përbashkët.
Në Kongresin e Parë të Fakultetit të Mjekësisë Dentare, në datat 3 dhe 4 Nëntor, 2017 do të na nderojë me pjesëmarrjen e saj prorektorja e universitetit “Hasan Prishtina”, protezistja e nderuar, Prof. Teuta Pustina, si dhe personalitete të tjerë të fushës së shëndetësisë.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 169
Një DelegaCioN ShqiptaR viZitoN NDëRmaRRjeN italiaNe RheiN 83
Në datat 5, 6 dhe 7 tetor një grup dentistësh dhe laborantësh shqiptarë, vizituan selinë e Rhein83 në Bolonja, ku u organizua njё kurs intensiv trainimi me qёllim njohjen e teknologjive bashkёkohore mbi pёrgatitjen e mbiprotezave (overdenture). Në ditët e kursit, të drejtuar nga Dr. Roberto Scrascia, u detajuan të gjithë protokollet e ndjekura për një përdorim korrekt të tyre. Vizita në ndërmarrjen e prodhimit bëri të mundur njohjen e teknologjisë së përdorur për prodhimin e atakeve (lidhjeve) për mbiprotezat. Rhein83 është ndërmarrja ndërkombetare që ka ekskluzivitet në prodhimin e lidhjeve apo atakeve për protezat e lëvizshme, që nga ataket e ngurta për implantet, deri tek linjat dedikuar sistemit CAD-CAM. Në delegacionin shqiptar bënte pjesë edhe Prof. Asoc. Edit Xhajanka, e cila në takimin me Z. Raffaele lombardo, Drejtor komercial i Rhein83, vendosi një marrëdhënie bashkëpunimi me Fakultetin e Mjekësisë Dentare të Tiranës. Dekanes së Fakultetit ju dhurua libri “Aspekte kliniko-teknike të protezës së kombinuar”. u diskutua pёr njё bashkёpunim tё mundshёm ndёrmjet FMD dhe kёsaj firme, me qёllim njohjen e studentёve, tё stafit akademik dhe klinicistёve me tё rejat e protetikёs sё lёvizshme mbi implante apo mbi dhёmbё natyralё, si njё alternativё e thjeshtё, ekonomike dhe e pёrshtatshme pёr kushtet e vendit tonё.
Kёshtu, nё datёn 17 shkurt 2018, nё Fakultetin e Mjekёsisё Dentare, nё sallёn e Leksioneve, do tё zhvillohet njё Konferencё dedikuar protezёs sё lёvizshme (overdenture). Ky seminar do tё ketё si lektor Dr. Roberto Scrascia, kirurg dhe protezist i njohur nga Puglia, relator nё shumё konferenca ndёrkombёtare dhe autor i shumё publikimeve dhe rasteve klinike, tё paraqitura nё revista kombёtare dhe ndёrkombёtare.
“Parimet tradicionale dhe risitё nё protezёn e lёvizshme, me suport implantar”
Abstrakt: Nё 30 vitet e fundit vihet re njё rritje e ndjeshme e moshёs mesatare tё popullatёs. Tё moshuarit kanё njё jetё tё pasur sociale dhe pёrvec funksionit, edhe estetika ka rёndёsi kryesore. Pёrqindja e personave pa dhёmbё ёshtё ulur, megjithatё ёshtё pёrsёri sinjifikante, meqёnёse jeta mesatare ёshtё rritur ndjeshёm. Nё Europё fenomeni i mungesёs sё dhёmbёve haset nё miliona njerёz dhe 40% e tyre kanё vёshtirёsi mastikatore dhe fonetike, si pasojё e protezave totale tё keq adaptuara apo me qёndrueshmёri tё ulёt. literatura ndёrkombёtare prej kohёsh ka pёrcaktuar avantazhet e trajtimit me mbiprotezat tё mbёshtetura mbi implante. Gjatё leksionit do tё paraqiten dhe ilustrohen raste ku proteza me mbёshtetje implantare, e tipologjive tё ndryshme, ёshtё zgjidhja mё e mirё pёr pacientёt si nga aspekti funksional, dhe ekonomik. Teknologjitё dhe materialet e reja i japin mjekut dhe laborantit mundёsitё pёr tё zgjedhur ndёrmjet trajtimeve tё llojeve tё ndryshme dhe sistemeve tё ndryshme retentive. Do tё prezantohet njё protokoll i pёrcaktuar pune, i cili bёn tё mundur pёr pacientin konstruktimin e njё proteze perfekte nga pikёpamja estetike dhe funksionale.

Revista Stomatologjike Shqiptare170
Zhvillimi i koNFeReNCëS Së iv të ShkeNCave mjekëSoRe të uNiveRSitetit të mjekëSiSë, tiRaNë, 21- 23 pRill 2017,
pikëNiSje e BaShkëpuNimit Dhe e NDëRliDhjeS iNStituCioNale NDëRmjet Fakultetit të mjekëSiSë DeNtaRe Dhe qeNDRëS
uNiveRSitaRe “ChaRitÉ BeRliN”
Me ndërhyrjen e Deputetes sё Bundestagut , Zonjёs Iris EBERl, pёrfaqёsuese e CSu/CDu nё Parlamentin Gjerman, në shtator 2016, filloi një ndërlidhje ndërmjet Dekanes së Fakultetit të Mjekësisë Dentare, Prof. Asc. EDIT XHAJANKA dhe zyrës së Znj. Eberl.
Nё vijim tё iniciativёs sё Zonjёs Iris Eberl, nё datat 12-14 mars 2017, në Berlin, me kërkesën e palës gjermane, u zhvilluan takime dhe biseda ndёrmjet pёrfaqёsuesve tё Fakultetit tё Mjekёsisё Dentare, tё pёrfaqёsuar nga Dekania, Prof. Asc. Edit Xhajanka, dhe Prof. Asc. Merita Bardhoshi, Znj. Iris Eberl dhe Drejtorit tё Qendrёs universitare “Charité Berlin”, Prof. Florian Beuer.
Në takime ishte i pranishëm edhe ambasadori shqiptar në Gjermani, Zoti Artur KuKo, i cili mbështeti plotësisht mundësinë e bashkëpunimit, duke e quajtur shumë të vlefshëm për FMD.
Nё qendёr tё bisedimeve ishte tematika e bashkёpunimit ndёrmjet Klinikёs universitare “Charité Berlin”, Klinikё universitare e njohur nё Protetikёn Dentare nё Gjermani, dhe Fakultetit tё Mjekёsisё Dentare, Tiranё. Bashkёpunimi do tё shtrihet nё fushёn
akademike, me shkёmbim tё lektorёve, veçanёrisht me pёrcjelljen e pёrvojёs sё shquar tё akademikёve gjermanё, nё shkёmbim tё studentёve ndёrmjet dy Institucioneve universitare, si dhe nё drejtim tё thellimit tё kёrkimit shkencor, nёpёrmjet zhvillimit tё work-shopeve dhe Konferencave tё ndryshme shkencore. Gjithashtu, pritet miratimi nga GIZ, Ministria Federale Gjermane, i njё projekti tё pёrbashkёt dy vjeçar ndёrmjet dy Institucioneve, kryesisht nё specialitetin e Protetikёs Dentare. Nё mbёshtetje tё kёtij bashkёpunimi do tё jetё edhe Ambasada Shqiptare nё Gjermani.
Materializimi i kёtij bashkёpunimi u bë në Konferencën e Fakultetit tё Mjekёsisё Dentare, të organizuar nё kuadrin e Konferencёs sё uMT, nё datat 21-23 prill 2017. Nё kёtё Konferencё na nderuan me pjesëmarrjen e tyre Deputetja e shquar, Znj. Iris Eberl, Ambasadorja e Gjermanisë në Shqipëri, Znj. Susanne Shutz, si dhe profesorё tё shquar dhe pёrfaqёsues tё Qendrёs universitare “Charité Berlin”, Prof. Peter Pospiech, zëvendës drejtor i “Charité Berlin”, Dr. Philipp Eberl, etj, tё cilёt ishin njёkohёsisht edhe lektorё nё kёtё Konferencё.

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 171
Në ceremoninë e hapjes morën pjesë duke përshëndetur Ministrja e Arsimit, Znj. lindita Nikolla, dhe Ministrja e Shëndetësisë, Znj. ogerta Manastirliu. Gjithashtu, na nderuan me pjesëmarrjen e tyre Kryetarët e urdhërit të Mjekut, të Dentistit dhe të Farmacistit, si dhe Rektorë, Dekanë e drejtues të universiteteve dhe Fakulteteve të tjera në Shqipëri. Konferenca zhvilloi punimet e saj me sukses dhe ishte një ndër konferencat me pjesëmarrjen më masive të profesionistëve të fushës së mjekësisë dhe të shëndetësisë, stafit akademik dhe të studentëve. Numri i pjesëmarrësve arriti në mbi 3000 persona.
Niveli i saj u rrit ndjeshëm nga pjesëmarrja e shumë lektorëve të huaj, profesorë dhe akademikë ndërkombëtarë, si dhe e profesorëve nga Kosova e Maqedonia. Gjatë ditevë të Konferencës, u organizua një takim i Deputetes gjermane Eberl
dhe i profesorёve tё nderuar gjermanё, me Rektorin e universitetit të Mjekёsisë, Tiranё, Prof. Arben Gjata, pёr tё thelluar dhe pёr tё vazhduar mё tej bashkёpunimin e nisur.
Në vijim të edukimit në vazhdim, Fakulteti i Mjekësisë Dentare në bashkëpunim me “Charité Berlin”, Shoqatën e Protetikës Shqiptare, Shoqatën e Kirurgëve oMF, Shoqatën Brainstorm, etj, do të organizojë në datat 3 dhe 4 nëntor 2017 Kongresin e parë me tematikën: “Të rejat bashkëkohore dhe sfidat në stomatologji”.
Ndërsa në 9-11 maj 2019, Fakultetit të Mjekësisë Dentare i është besuar nga Kryesia e Shoqatës Ballkanike të Stomatologjisë (BaSS) organizimi në Shqipëri i Kongresit të 24-rt Ballkanik.
Ftojmë të gjithë profesionistët dhe dashamirësit e fushës së shëndetësisë të marrin pjesë në këto evente shkencore madhore!

Revista Stomatologjike Shqiptare172
Prof.Asoc. Afërdita BASHA
lindur në Tiranë më 30.11.1942Prof. Asoc. Afërdita BASHA ka zhvilluar pjesën
më të madhe të aktivitetit të saj profesional pranë Fakultetit të Mjekësisë, Departamentit të Stomatologjisë, Katedra e ortopedisë Stoma-tologjike .
Pas përfundimit të shkollës së mesme nisi studi-met në fushën e stomatologjisë me një kurs 1 vjeçar për laborante dentare gjatë viteve 1959-1960. Menjëhere në përfundim të kursit, gjatë viteve 1960-1965, ajo vazhdoi studimet e larta universi-tare në Fakultetin e Mjekësisë, Dega Stomatologji.
Pas përfundimit të studimeve të larta me re-zultate të shkëlqyera Prof. Asoc. Afërdita BASHA filloi punë si pedagoge me kohë të plotë në katedrën e ortopedisë Stomatologjike, titullare e lëndës ortodonci. Ajo ka kryer dhe special-izime në lëmin e ortopedisë, 1966, dhe ortod-oncise, 1979. Në vitin 1982 fitoi gradën Kandidat i Shkencave me vendim nr. 62 dhe në 1993 fitoi gradën shkencore “Docent” me vendim nr. 1155.
Në vitin 1993 konform kërkesave të vendimit të Këshillit të Ministrave nr. 351 dhe udhëzimeve nr. 2 dhe nr 3 të KKSH riklasifikohet dosja e plotë e saj dhe në 21.12.1993 iu dha titulli “Profesore e Asociuar”.
Puna e saj në zhvillimin e ortodoncisë shqiptare vazhdoi dhe pas vitit 1996, kohë kur ajo doli në pension. Prof. Asoc Afërdita BASHA ka botuar një numër të konsiderueshëm artikujsh shkencorë si edhe 7 tekste mësimore dhe monografi; Atlasin e ortodoncisë, librin “ortodoncia”, praktikumet klinike dhe paraklinike të ortodoncisë, si dhe teks-tin “Shkaktarët e anomalive dhe parandalimi i tyre”. Gjatë aktivitetit të saj akademik ka kryer shumë re-censa dhe oponenca librash dhe Disertacionesh. Ka qenë vazhdimisht anëtare në Redaksinë e “Bule-tini i Shkencave Mjeksorë”, “Shëndetsia Popullore” dhe Kryetare e Shoqatës Shkencore të Studentëve.
Ajo u nda nga jeta në 12 qershor, 2017, por la pas një kontribut në stomatologji për të cilin do të kujtohet ndër breza.
NekRologji

Vëllimi 15, Nr. 1 dhe 2 (56, 57) mars 2017, nëntor 2017 173
Dr.Shahin JOKA
Shahin Joka lindi në libohovë, më 18 shtator 1952. Shkollën 7-vjeçare dhe të mesme e kreu në Memaliaj. Në vitin 1974 diplomohet si Mjek Stomatolog në universitetin e Tiranës. Në vitin 1974 deri në 1976 emërohet dhe punoi si Mjek Stomatolog në Krujë.
Në vitin 1976 fillon punën si Mjek Stomatolog në qytetin e laçit, deri në vitin 1993. Gjatë këtyre viteve ka ushtruar dhe rolin e Drejtuesit të Shërbimit të Stomatologëve në këtë qytet, kohë në të cilën falë përkushtimit dhe kontributit të tij “Qendra Stomatologjike”, në rrethin e laçit njohu një zhvillim të madh në profesionalizëm dhe infrastrukturë, duke
u kthyer në një nga qëndrat kryesore në rajonin e veriut.
Nga viti 1993 deri në vitin 2017, kaloi në profesion të lirë dhe ushtroi profesionin në klinikat e tij në rrethin e laçit dhe Tiranës. Shahini ka shërbyer si pedagog në Fakultetin e Stomatologjisë, pranë “Albanian university”, për më shumë se 10 vjet.
Në të gjitha vendet ku ka punuar është dalluar për përkushtimin dhe prefesionalizmin e jashtëzakonshëm ndaj profesionit të Mjekut. Ai u nda nga jeta në 21 Qershor 2017, për të mos u harruar kurrë, duke lënë në hidhërim të thellë gruan, fëmijët, shokët, kolegët dhe studentët e tij.
NekRologji

Revista Stomatologjike Shqiptare174
Dr. Kujtim Likaj
Themelues i shërbimit oMF në Spitalin Rajonal Durrës Kr. dr. Kujtim likaj lindi më 22 Korrik 1948, në Vlorë. Është rritur në Tiranë , Pogradec , Koplik dhe përfundimisht në vitin 1960 në qytetin e Durrësit, pasi u transferuan familjarisht nga emërimi ushtarak i të atit, ku ka jetuar deri në fund të jetës së tij. Arsimin 7 vjeçar e ka filluar në vitin 1954 në Koplik të Shkodrës dhe e përfundon në shkollën “ 10 Korriku” Durrës, në vitin 1961. Po në qytetin e Durrësit kryen edhe arsimin e mesëm të përgjithshëm në gjimnazin “ Nako SPIRu “ në vitet 1961 – 1965. Ndjek studimet universitare në Tiranë në vitet 1965 – 1970 dhe mbaron studimet e larta në fakultetin e Mjekësisë, të universitetit Shtetëror të Tiranës - Dega Stomatologji. Aktivizohet në garat atletike gjatë periudhës së fakultetit në ekipin sportiv „STuDENTI“ ku dhe aty dallohet për treguesa të lartë cilësor sportive në garat e shkurtër të vrapit 100 metër.
Në tërë jetën e tij përmendte vazhdimisht afeksionin e veçantë që ka patur për kirurgjinë, muzikën dhe sportin e atletikës.
Fillon aktivitetin si mjek stomatolog duke u emëruar në qytetin e lushnjes. Në këtë qytet janë hedhur hapat e para të punës së tij të palodhshme dhe të dalluar duke punuar në sektorin e kirurgjisë ambulatore. Që në këto vite ka bërë kirurgji orale si:kistë odontogjene dhe jo odontogjene, rezeksionë apikale, dhëmbë inkluzë në pozicionë të ndryshme etj. Në muajin nëntor 1974 transferohet në rrethin e Durrësit, qyteti i Shijakut me një karakteristikë pune të shkëlqyer nga qyteti i lushnjës. Nga viti 1974 – 1975 ka punuar në qytetin e Shjijakut duke u ngritur gjithmonë e më shumë profesionalisht. Në vitin 1975 u transferua nga qyteti i Shijakut dhe u emërua në qytetin e Durrësit, nga u caktua të punojë në Spitalin Rajonal
të Durrësit. Merr pjesë në programin e specializimit të Kirurgjisë oro-Maksilo-Faciale nga dt. 01. 09. 1978 deri më 28. 02. 1980 në Tiranë, duke fituar të drejtën e specialistit Kirurg oMF. Jep provimin përfundimtar dhe vlerësohet student i shkëlqyer. Pas përfundimit me sukses të specializimit themelon shërbimin e kirurgjisë oro-maksilo-faciale në Spitalin Rajonal të qytetit të Durrësit, ku realizon me sukses të plotë të gjitha llojet e operacioneve të të gjitha fushave të Kirurgjisë oMF si: Tumoret beninje dhe malinje të regjionit oMF, patologjitë e gjëndrave të pështymës, patologjite malformative, patologjitë traumatike, ankilozat e artikulacionit temporo -mandibular, por afeksioni i tij më i madh ishin defektet e lindura të buzës dhë qiellzës.
Të gjitha këto operacione janë të dokumentuara me foto dhe me shkrim dore origjinale nga vetë Dr. Kujtim likaj.
Në aktivitetin e tij shkencor ai ka qënë referues dhe pjesëmarrës aktiv të shumë punimeve shkencore. Të gjitha rastet i ka bërë në Durrës me sukses të plotë, duke shënuar kështu hedhjen e bazave të kirurgjisë oro- maksilo –faciale në spitalin rajonal dhe në tërë rrethin e Durrësit.
Për herë të parë në Shqipëri u pajisë në vitin 1993 me liçencën e dy punësimit si kirurg oMF në spital dhe shërbimin stomatologjik privat në klinikën e tij private. Në vitin 1996 u shkëput nga spitali dhe iu kushtua aktivitetit të tij privat si stomatolog dhe kirurg oMF në klinikën e tij private të pajisur me sallë operacioni , ku njëkohësisht thirrej dhe operonte për rastet e ndryshme kirurgjikale të spitalit në rrethin e Durrësit.
Vdiq më 08. 06. 2002 në spitalin Valle De Skote të Sienës –Itali dhe u varros me nderim në qytetin e tij të Durrësit më 13. 06. 2002.
NekRologji