vivek srivastava consultant in acute medicine kings college hospital
TRANSCRIPT

Vivek Srivastava Consultant in Acute Medicine
King’s College Hospital

• 5.9% of emergency admissions considered unnecessary
• 50.7% of hospitals did not have a written handover protocol
• There was a relationship between the quality of the initial assessment and the overall quality of care
• There must be appropriate handover systems in place
Emergency Admissions:A journey in the right direction?
A report of the National Confidential Enquiry into Patient Outcome and Death (2007)
Why

WhyNCEPOD - Deaths in
Acute Hospitals (2009)In 25% of cases there
was, a clinically important delay in the first review by a consultant.
Poor communication between and within clinical teams was identified as an important issue in 13.5% (267/1983) of cases.
SummaryAppropriately trained doctors must see sick
patients in a timely manner
The systems of care need to be overhauled to ensure that emergency patients get a uniformly high standard of care
Communication, documentation and handover must improve

The problemKing’s viewAvoid emergency
referralEarly assessment Admission preventionEarly discharge backMedical plans
Maudsley view
• Escalation
• Too many pathways
• Evaluation
• Transfer to KCH
• The medically deteriorating patient

The pilot - principlesDevelop a pathway that providesEarly recognition of the deteriorating patientPrompt communication with medical teamAppropriate evaluation and management Non-emergency transfer to KCH, if requiredReduced A&E waitingJoint care and discharge planningImproved patient experience

The pilot – the proposalThe service will operate between 10.00-16.00Telephone support Planned assessment by Acute Medicine
(AAU)Assessments at the Maudsley site if there is a
risk associated with transferring to Kings1:1 nursing support for individual service
usersShared teaching provision - SLaM and King’s

The pathwayIn case of a Medical Emergency – follow your hospital protocol
Inpatient in SLaM with concerns about medical health
Nurse in charge to record complete set of observations and calculate Early Warning Score. Inform Junior Doctor caring for the patient
Junior doctor carries out examination, blood tests and ECG
Bleep Medical SpR providing ward cover on KCH bleep 221; orCall Acute Medicine Consultant on 020 3299 5453 (M-F- 10am to 4pm)Details required -Medical issues and clinical findings-Results of bedside and lab tests
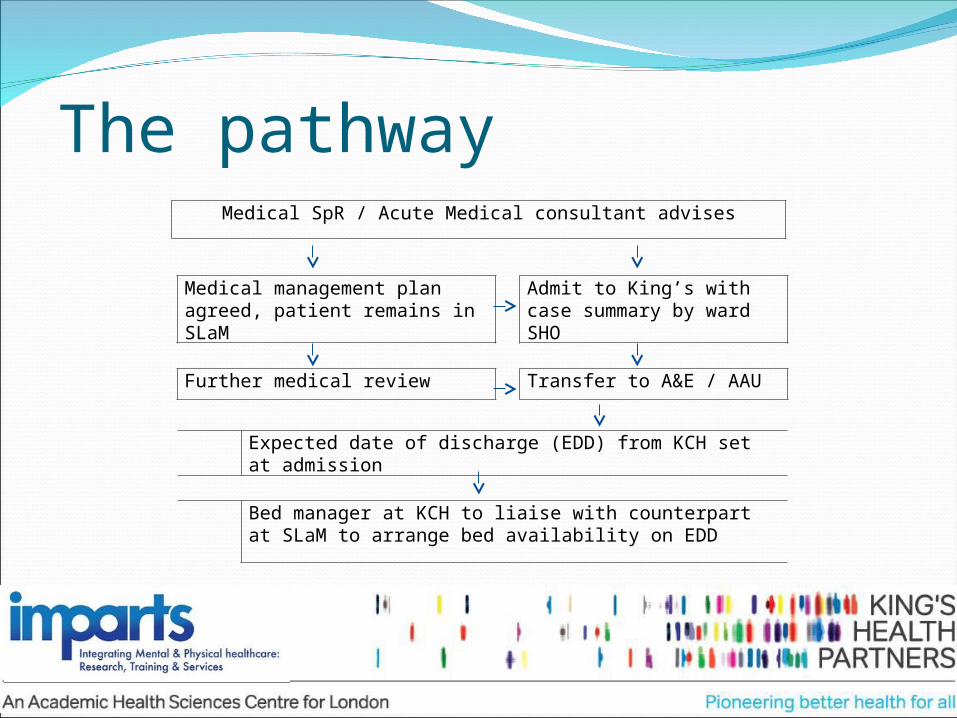
Medical SpR / Acute Medical consultant advises
Medical management plan agreed, patient remains in SLaM
Admit to King’s with case summary by ward SHO
Further medical review Transfer to A&E / AAU
Expected date of discharge (EDD) from KCH set at admission
Bed manager at KCH to liaise with counterpart at SLaM to arrange bed availability on EDD
The pathway

Way forwardEvaluation – define scale of the problem
Measures collected in KCH 1. Total time spent in A&E by SLAM patients. 2. Route of referral 3. Reduced length of stay4. Lag time between being declared clinically fit for discharge and actually leaving KCH5. Same day discharges Length of time in MAU if not admitted6. MAU patient experience feedback 7. Time of day of calls8. Profile of conditions referred SLaM Measures1. Number of people from Maudsley who have to go to KCH2. Number of ambulances between Maudsley and KCH3. Number of 999 calls. 4. Number/ cost of escorts to KCH.5. SLaM PEDIC measure on return. 6. SLaM length of stay 7. Survey of doctor/ nurses including qualitative information benefits to patients and staff at both sites. Measures from both sites1. Improved medicine reconciliation rates 2. Proportion of people for whom SLAM bed managers know KCH EDD on admission3. Quantify the number of people who would have benefitted from assessment on the Maudsley site

Initial results (n=72)Pilot - 14/12/11 – 13/3/12 (n=39)Control - 14/9/11 – 13/12/11 (n=33)Unable to capture tele-referrals39 female : 33 males; Age – 16 – 89y28/72 (38.8%) presented after 5pmSince December increasing evening rather
than late night referrals.Benefits – better communication, appropriate
admissions, early discharges (some). Staff happy

Way forwardChallenges
- Data sharing – IT issues, medico-legal issues- Multidisciplinary working- Medicines reconciliation- Communication and prompt patient transfer
across the road in either direction- Standardising mental-physical interface- Education and training – early progress
SummaryThe overall goal of IMPARTS is to improve
mental healthcare provision within medical settings across KHP.
We suggest the need to improve medical healthcare provision within mental health settings across KCP.
Long term - Medical Liaison team(s) (cf Psych liaison team)
Spread across all acute / mental health trusts