visit report on buckingham medical school€¦ · visit report on buckingham medical school this...
TRANSCRIPT
Visit Report on Buckingham Medical School
This visit is part of the 2016/17 visit cycle.
Our visits check that organisations are complying with the standards and requirements as
set out in Promoting Excellence: Standards for medical education and training.
Summary
Medical School Buckingham Medical School
University University of Buckingham
Programmes MBChB
Date of visits
Objective Structured Selection Examination (OSSE):
8 September 2016
Main visit:13-14 September 2016
Objective Structured Clinical Examination (OSCE): 6
January 2017
Second year qualifying OSCE: 21 February
Progression examination board: 1 March 2017
Key Findings
1 The visit carried out in September 2016 was the fifth
visit to Buckingham medical school (the school) since
agreeing to commit resources to begin the process of
a multi-year quality assurance review. We will
continue the rolling cycle of annual quality assurance
visits to the school following the first cohort of
students through to graduation and their first year of
practice.
2 At the time of our visit the school was in phase one
of its curriculum delivery with advanced preparatory
Buckingham Medical School final visit report for 2016/17
2
plans for the delivery of phase two. In line with the
school’s progression through the programme, the
school is growing and currently has 79 students in
year one, 60 students in year two and is planning to
recruit another 85 students commencing in January
2017.
3 During our main visit we met with year one and two
students and a range of staff from different teams
across the school. We observed several teaching
sessions and we visited Milton Keynes University
Hospital NHS Foundation Trust (MKH).
4 The school has made considerable progress since our
last visit in addressing their open requirements and
recommendations. We have therefore closed two
requirements and three recommendations and noted
that two recommendations are partially met. One
requirement and three recommendations remain
open from previous cycles for further monitoring.
5 We have identified an area of good practice and 15
areas that are working well in the school. We found
that students are positive about their experiences at
the school and that staff at the school and MKH are
dedicated and enthusiastic.
6 However, we have also identified requirements and
recommendations for the school to address,
including: streamlining reporting mechanisms from
local education providers (LEPs) to the school,
accelerating the appointment of educational
supervisors for phase two, enhancing the training for
simulated patients and examiners in the OSSEs,
improving communication with students around
clinical placements and encouraging the school to
continue to evaluate their assessment processes.
3
Areas of good practice
We note good practice where we have found exceptional or innovative examples of work
or problem-solving related to our standards. These should be shared with others and/or
developed further.
Number Theme Good practice
1 Theme 3 (R3.2) We heard from all of the groups that we spoke
to about the responsiveness of the school and
the high level of educational and pastoral
support available to students.
Paragraphs 58-62
Areas that are working well
We note areas where we have found that not only our standards are met, but they are
well embedded in the organisation.
Number Theme Areas that are working well
1 Theme 1 (R1.17) The school promotes a culture of learning and
collaboration with other healthcare professions
in the delivery of the curriculum as students
have adequate opportunities to learn from
other healthcare professionals.
Paragraphs 20-22
2 Theme 1 (R1.21) The learning environment is positive with
robust structures in place for educational
support. Students commended the high quality
of support available at the school and noted
high levels of accessibility to teachers and
tutors.
Paragraphs 28-29
3 Theme 2 (R2.1) The school has an effective system of
educational governance which is responsive to
feedback from both learners and educators.
Paragraphs 30-32
4 Theme 2 (R2.3) We note that there has been a significant
4
improvement in the way in which the patient
and public group is constituted and run. The
group is engaged and motivated.
Paragraphs 34-35
5 Theme 2 (R.2.8) We were impressed with the strong working
relationship that the school has fostered with
Health Education England working across
Thames Valley in order to enable their
students to access the Professional Support
Unit.
Paragraphs 45-46
6 Theme 2 (R2.20) The OSSE stations tested a wide range of skills
and attributes which we note are blueprinted
against Good Medical Practice.
Paragraphs 53-56
7 Theme 2 (R.2.20) The school’s selection processes are open and
transparent.
Paragraphs 53-56
8 Theme 2 (R.2.20) The OSSE was well organised, with a high level
of staff involvement and commitment.
Paragraphs 53-56
9 Theme 3 (R3.7) Students were well prepared for the format of
their OSCE. It is evident that they have been
appropriately briefed and supported.
Paragraph 70
10 Theme 4 (R4.1) Educators are well trained and supported in
their roles to meet their education and training
responsibilities.
Paragraphs 75-77
11 Theme 5 (R5.3) Small group teaching is working well and was
commended by students.
Paragraph 88
12 Theme 5 (R5.5) The OSCE stations tested a wide range of skills
and attributes which we note are blueprinted
against outcomes for graduates.
5
Paragraphs 99-101
13 Theme 5 (R5.6) The school’s investment in assessment and
high level of analysis is to be commended.
Paragraph 114
14 Theme 5 (R5.8) We found the OSCE to be well organised, with
a high level of staff involvement and
commitment.
Paragraphs 115 -116
15 Theme 5 (R5.12) We observed clear evidence that reasonable
adjustments have been implemented for the
OSCE by the School.
Paragraphs 117-118
6
Requirements
We set requirements where we have found that our standards are not being met. Each
requirement is:
targeted
outlines which part of the standard is not being met
mapped to evidence gathered during the visit.
We will monitor each organisation’s response and will expect evidence that progress is
being made.
Number Theme Requirements
1 Theme 1 (R1.3) The school must ensure that systems are in
place so that any concerns reported through
placement providers are forwarded in a timely
fashion to a known individual in the LEP who is
responsible for relaying concerns back to the
school.
Paragraph 7-9
2 Theme 4 (R4.2) The school must expedite the appointment of
educational supervisors for phase two to
ensure they are trained and that their job
plans reflect their new role.
Paragraphs 78-80
7
Recommendations
We set recommendations where we have found areas for improvement related to our
standards. They highlight areas an organisation should address to improve, in line with
best practice.
Number Theme Recommendations
1 Theme 2 (R2.20) In OSSE settings, consideration should be
given to further develop consistency in the
simulated patients’ performance, examiners’
interactions with students, examiner training in
relation to the nature of the global score and
also the reliability of the selection event.
Paragraph 56-57
2 Theme 3 (R3.7) The school should improve communication
with current and future cohorts to ensure that
students receive timely and accurate
information about their clinical placements.
Paragraphs 67-69
3 Theme 5 (R5.6) The school should continue to evaluate their
assessment processes through the ongoing
assessment review.
Paragraphs 109-114
8
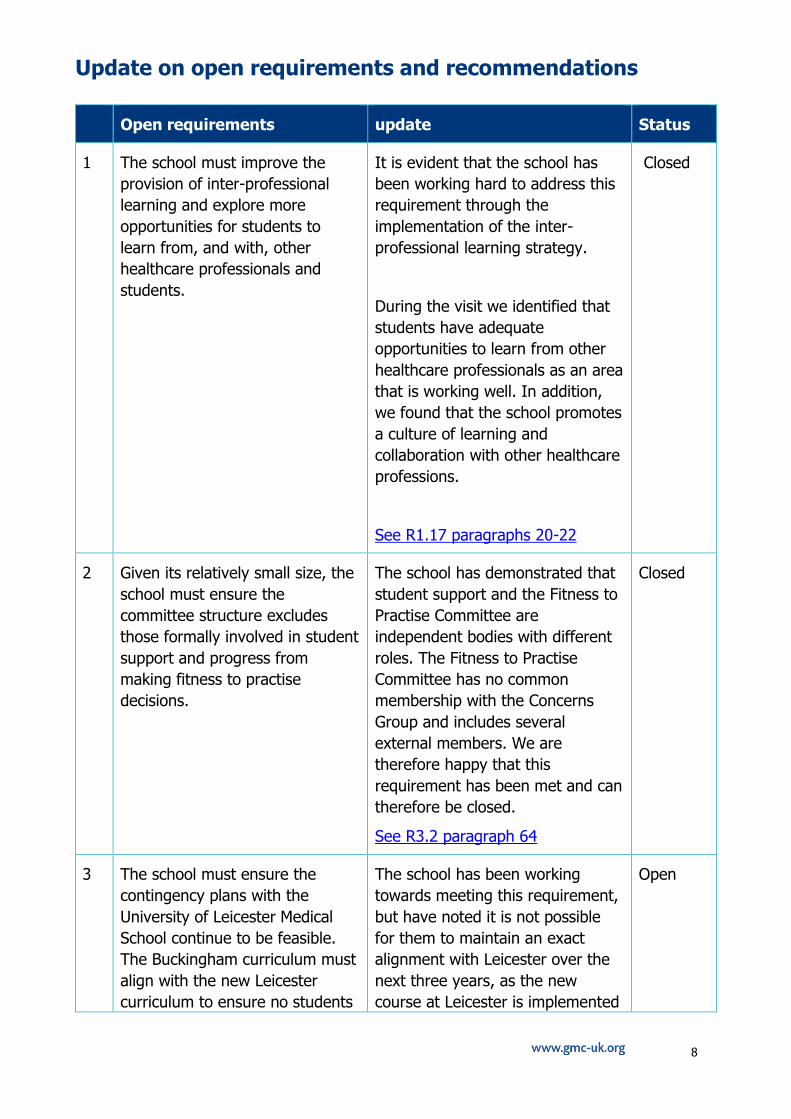
Update on open requirements and recommendations
Open requirements update Status
1 The school must improve the
provision of inter-professional
learning and explore more
opportunities for students to
learn from, and with, other
healthcare professionals and
students.
It is evident that the school has
been working hard to address this
requirement through the
implementation of the inter-
professional learning strategy.
During the visit we identified that
students have adequate
opportunities to learn from other
healthcare professionals as an area
that is working well. In addition,
we found that the school promotes
a culture of learning and
collaboration with other healthcare
professions.
See R1.17 paragraphs 20-22
Closed
2 Given its relatively small size, the
school must ensure the
committee structure excludes
those formally involved in student
support and progress from
making fitness to practise
decisions.
The school has demonstrated that
student support and the Fitness to
Practise Committee are
independent bodies with different
roles. The Fitness to Practise
Committee has no common
membership with the Concerns
Group and includes several
external members. We are
therefore happy that this
requirement has been met and can
therefore be closed.
See R3.2 paragraph 64
Closed
3 The school must ensure the
contingency plans with the
University of Leicester Medical
School continue to be feasible.
The Buckingham curriculum must
align with the new Leicester
curriculum to ensure no students
The school has been working
towards meeting this requirement,
but have noted it is not possible
for them to maintain an exact
alignment with Leicester over the
next three years, as the new
course at Leicester is implemented
Open
9
would be placed at a
disadvantage in terms of
assessment.
in stages. A transfer of students
from Buckingham to Leicester in
phase one would not put students
at a disadvantage. However, we
were made aware that changes to
the Leicester phase two curriculum
are greater and the finer details
are less well developed. We note
that while parts of the curriculum
are similar others are not and
acknowledge that alignment is
challenging. However, potential
issues with transfer points have
been noted and are on the school’s
radar. We will therefore continue
to monitor this item during future
QA cycles.
See R5.3 paragraphs 89-90
Open recommendations update Status
1 We would like to see evidence of
how the medical school building
and the new education centre will
accommodate two cohorts of
students.
During the visit we found that
while the medical school building is
crowded during lesson
changeover, there is adequate
space for teaching.
Building work on the education
centre at MKH was due to
commence in August 2016, with an
occupation date of September
2017. At the time of our visit in
September 2016, the site had been
cleared but building had not yet
begun. The school told us that
contingency plans are in place for
March to August 2017 when phase
two students will be on placement
at MKH. We will continue to
monitor this recommendation.
See R1.19 paragraphs 23-26
Open
10
2 We recommend to set out clear
guidance of the thresholds that
would trigger fitness to practise
procedures
The school has been working to
refine their FtP procedures and
thresholds in advance of receiving
a case. Since our last visit
Buckingham has considered GMC
guidance on Professionalism and
has incorporated it into their FtP
training and procedures and they
now have a framework by which
evidence and reports from
hearings will be collected and
presented. We will keep this item
open for further monitoring until
the process has been utilised more
to ensure changes are sustainable.
See R2.18 paragraph 52
Open
3 We recommend that in the OSCEs
the school requests examiner
written feedback for all students,
not only for the ones assigned a
failing grade
During the year two OSCE we
found that examiners now
complete written feedback for all
students. Therefore, this item can
now be closed.
See R3.13 paragraph 73
Closed
4 The school should increase the
number of options available as
student selected components
(SSCs) and provide clearer links
to how they meet the learning
outcomes defined in Tomorrow’s
Doctors
During the 2015/16 cycle of visits
the visit team concluded that this
recommendation was partially met
as the school has mapped all of its
SSCs to the learning outcomes in
Tomorrow’s Doctors and we noted
that we will continue to monitor
the increase in SSC options.
Since our last visit it is clear that
the school has been working
towards meeting the rest of this
recommendation through working
on increasing the number of SSCs
available to their students. The
school currently offers eight taught
SSCs and 73 library projects.
Additionally, there are five new
SSCs in development with further
proposals for new units under
Partially
met
11
scrutiny. We will continue to
monitor this recommendation.
See R5.3 paragraphs 91-94
5 The school should develop robust
procedures to manage patient
participation at general practices,
as they will be heavily relied upon
during the first year.
The 2016/17 cycle of visits found
no concerns in relation to
procedures around patient
participation at general practices.
The second year students that we
met told us that their GP
placements are going well, they
are well organised and they are
enjoying the narrative medicine
strand. In addition, the school
noted that there has been no
evidence of outstanding issues
from their quality information. This
recommendation can therefore be
closed.
See R5.3 paragraph 95
Closed
6 We understand the small group
activities will be evaluated - and
we recommend careful
consideration is given to how
often the groups should be
changed
The school has taken steps to
evaluate their small group
activities. Student representatives
were asked to consult informally
with the student groups to identify
initial thoughts and feelings
amongst the student body. At the
time of our visit in September 2016
the school planned to formally
consult with the student body
regarding potential changes to the
small activity groups, aiming to
implement an outcome in early
2017. We will therefore follow up
on this recommendation in the
next cycle of visits.
See R5.3 paragraphs 96
Partially
met
7 The ratio of new questions and
tested questions should be
reviewed in the initial runs of the
assessments throughout the
programme.
The school has been addressing
this item and has generated large
numbers of questions for each
assessment and these are
progressively filing their question
bank, such that Leicester questions
Closed
12
are now seldom used. The school
has quality systems in place,
including external scrutiny of their
assessments. Overall the
psychometric analysis of written
and OSCE examinations
constructed with the school’s own
items are satisfactory and the
school is responding to the few
questions with less favourable
psychometric characteristics. We
are therefore satisfied that this
item has now been met.
See R5.6 paragraph 103
8 In an OSCE setting, consideration
should be given to further
develop consistency in the
simulated patients’ performance,
examiners’ interactions with
students and in the calibration of
students’ marks/outcomes.
The school has taken steps to
address standardisation and has
developed an examiner briefing
clarifying that simulated patients
should not contribute to marking in
any way. The school has also
taken steps to develop consistency
in examiners’ interactions with
students and we note the
calibration exercise is a welcome
development.
Although we acknowledge that the
school has taken steps to address
the issues, this item will be kept
open for further monitoring.
See R5.6 paragraphs 104-108
Open
13
Findings
The findings below reflect evidence gathered in advance of and during our visit, mapped
to our standards.
Please note that not every requirement within Promoting Excellence is addressed. We
report on ‘exceptions’, e.g. where things are working particularly well or where there is a
risk that standards may not be met.
Theme 1: Learning environment and culture
Standards
S1.1 The learning environment is safe for patients and supportive for learners and educators. The culture is caring, compassionate and provides a good standard of care and experience for patients, carers and families.
S1.2 The learning environment and organisational culture value and support education and training so that learners are able to demonstrate what is expected in Good medical practice and to achieve the learning outcomes required by their curriculum.
Raising concerns (R1.1) Dealing with concerns (R1.2) Learning from mistakes (R1.3)
7 The school is making good progress towards meeting these requirements. We found
that there is transparency around raising concerns at both the school and MKH.
Students are encouraged to raise any concerns relating to patient safety or education
and training and told us that they feel comfortable in doing so. Moreover, students
are aware of how to report a patient safety concern and understand their
responsibility to do so.
8 The senior management team at MKH told us they have processes in place for
students to raise concerns about patient safety or education and training. Students
are encouraged to speak to a clinician in the first instance, but if this is not possible
then students are encouraged to raise a DATIX. The school told us they have an
agreement in place with MKH which stipulates that all concerns raised by students
must be relayed back to the school. MKH confirmed they send all DATIX reports from
students back to the school.
9 Although we found the foundations for raising concerns are in place at both the
school and MKH, we identified that concerns raised at MKH are not collated by a
known individual at the trust who is responsible for reporting concerns back to the
school. We encourage the school to work with its placement providers to ensure that
feeding concerns back to the school is streamlined.
Requirement 1: The school must ensure that systems are in place so that any
concerns reported through placement providers are forwarded in a timely fashion to a
14
known individual in the LEP who is responsible for relaying concerns back to the
school.
Seeking and responding to feedback (R1.5)
10 During the visit we heard from a number of individuals about how the school
encourages and responds to feedback from learners and educators. We also heard
about the subsequent changes.
11 The quality management team told us that the quality unit design feedback forms for
students to complete. In order to do this education provider unit (EPU) leads are
asked to suggest three questions that are specific to them. Each EPU receives their
own individual feedback but there is also an overview of feedback to allow EPUs to
see how their feedback sits in comparison to others. Additionally, the quality
management team noted they have changed the order of some of the units in
response to student feedback.
12 Academic teachers confirmed that students complete feedback forms in order to
identify areas for development and supervisors at MKH told us they also have the
opportunity to feedback to the school on the delivery of the curriculum. The
curriculum team noted the school has regular meetings with placement providers to
scrutinise student feedback and produce a formal action plan.
13 The patient and public group told us they receive student feedback on their sessions.
They added the process is evolving and that sessions are designed in response to
student feedback. We were also told the patient and public group feel confident in
putting forward their suggestions and feel listened to by the school.
14 The selection team noted that following the school’s selection events, the team meet
in order to identify how stations can be developed. Additionally, during our
observation of the OSSE, the school provided evidence that they collect feedback
from candidates and noted they plan to collect feedback from current students.
15 Finally, students confirmed they have ample opportunities to provide feedback to the
school, and year two students told us there is a student forum whereby students can
raise concerns and give their feedback to the school on a wide range of topics
including: academic, facilities, placement and assessments.
Appropriate capacity for clinical supervision (R1.7) & appropriate level of clinical
supervision (R1.8)
16 During our meeting with the senior management team at MKH it was noted that while
the trust has some hard to recruit to posts in certain specialties, they have
appropriate supervision plans to cover these posts. We were also told the clinical staff
body at MKH has grown significantly, meaning there is adequate support for
students.
15
17 The year two students we met told us their placements at MKH are enjoyable as
consultants are welcoming, supportive and keen to teach. The students did not raise
any concerns about supervision or working beyond their competency.
Induction (R1.13)
18 Upon arrival at the school students undergo an induction week in order to fully
introduce them to the course. Induction week covers a wide range of topics including:
careers, student support and fitness to practise.
19 Senior management at MKH told us that they are developing their induction
programme with the school. We were told that most of the induction is face-to-face
and that students have the opportunity to meet with the chief executive (CEO) during
their induction. Key topics including undermining and bullying and support are
explored during student induction at MKH.
Multiprofessional teamwork and learning (R1.17)
20 The school has an open requirement relating to this standard which can now be
closed. Previously we identified that the school must improve the provision of inter-
professional learning and explore more opportunities for students to learn from, and
with, other healthcare professionals and students.
21 It is evident that the school has been working hard to address this requirement
through the implementation of their inter-professional learning strategy. The key
features of this strategy are a set of experiences for students in phase one, plus a
minimum of one inter-professional learning event in each main block in phase two,
and a requirement to reflect on multi-professional working repeatedly in the e-
portfolio.
22 During the visit we identified that students have adequate opportunities to learn from
other healthcare professionals as an area that is working well. We observed a
procedural skills session for year one students which was led by two mid-wives, and
supervisors at MKH told us that students receive input into their learning from a
range of healthcare professions. Students also told us about an inter-professional
learning day which aims to cover working in a multi-disciplinary team. We were told
that there is a range of healthcare workers at these days, including diabetes nurses,
physiologists and radiographers.
Area working well 1: The school promotes a culture of learning and collaboration
with other healthcare professions in the delivery of the curriculum as students have
adequate opportunities to learn from other healthcare professionals.
16
Capacity, resources and facilities (R1.19)
23 The school has an outstanding recommendation relating to this requirement. During
our last visit we highlighted that we would like to see evidence of how the medical
school building and the education centre at MKH will accommodate two cohorts of
students.
24 The school is currently in partnership with MKH to build a new building for education
purposes at MKH. Work was due to commence in August 2016, with an occupation
date of September 2017. At the time of our visit in September 2016, the site had
been cleared but building had not yet begun. The school told us that contingency
plans are in place for March to August 2017 when phase two students will be on
placement at MKH. During our visit to MKH the senior management team advised
they have rented office space to house hospital back office functions such as, IT, HR
and finance, which in turn will make physical space for phase two students.
Additionally, during the visit we examined the physical space of the current education
centre, which while outdated is fit-for-purpose.
25 During the visit the senior management team told us the medical school building is
successfully accommodating two cohorts of students. We heard there is adequate
room to accommodate scheduled teaching but that there is limited space for private
study in the medical school building. We were also told the building is busy during
changeover times. Year two students supported this and told us that the medical
school building is busy but added it functions. They also told us the lack of private
study space in the medical school building is not an issue as they study in the library
or at home. Academic teachers told us despite growing pressures on office space in
the school that all of teachers have their own desk. They noted they have access to
meeting rooms should they want to meet with the students in private.
26 The senior management team at MKH told us they have no concerns about
placement capacity. MKH is also a placement provider for Oxford Medical School, but
it was noted there is no competition for resources between the different groups of
students as there is only a small number of Oxford students on site. Additionally, we
were told by the trust that they are confident they can accommodate increases in
Buckingham student numbers up to 96 students per cohort, and planning has begun
to accommodate this number of students. We will therefore continue to monitor this
recommendation until the education centre at MKH has been built and students are
occupying it.
Accessible technology enhanced and simulation-based learning (R1.20)
27 The curriculum team at the school confirmed that students will have access to
technology enhanced and simulation based learning opportunities during their time at
the school. They added that several units include simulation activities to solve clinical
problems; additionally there is also a simulation suite at MKH that students have
access to, to support their learning.
17
Access to educational supervision (R1.21)
28 The school’s personal tutor system ensures that students receive ongoing routine
support to facilitate their development. The personal tutor system is separate to the
concerns process and pastoral support group which are discussed in more detail
under R3.2. The school has 21 personal tutors who meet with students regularly in
order to oversee their personal and academic development, as well as their e-
portfolio.
29 During our visit students told us they meet with their personal tutor once a semester
but that personal tutors are accessible and responsive should students wish to
arrange additional meetings. Students noted the personal tutor system at the school
is very effective and they feel supported in their studies. They noted that reflecting
on their e-portfolio in meetings with their personal tutor is helpful. Additionally,
students with whom we met at MKH told us they are well supported on placements,
their personal tutors are accessible and they know who to contact should they have
an issue.
Area working well 2: The learning environment is positive with robust structures in
place for educational support. Students commended the high quality of support
available at the school and noted high levels of accessibility to teachers and tutors.
18
Theme 2: Education governance and leadership
Quality manage/control systems and processes (R2.1)
30 The school has operational and functional educational governance systems and
processes in place to manage and control the quality of education and training. EPUs
are a group of staff responsible for parts of the curriculum delivered in the university,
at an NHS or other body delivering clinical education and are responsible for quality
control. EPUs feed into the quality group responsible for quality management. The
risk registers and action plans from this group are combined into a live global
document and feed into the board of studies which is the body responsible for the
governance of quality for the programme.
31 The quality management team noted there is an understanding and engagement with
the school’s educational governance system amongst staff at the school. Additionally,
quality processes are continuing to develop in line with GMC developments as the
school’s risk register has been configured to match the standards outlined in
Promoting Excellence.
32 The school told us feedback is central to their quality management processes and
during our visits we heard examples of changes that have been made in response to
feedback. Please see R1.5 which details the different types of feedback that the
school collects.
Area working well 3: The school has an effective system of educational
governance which is responsive to feedback from both learners and educators.
Accountability for quality (R2.2)
33 The school is clearly demonstrating accountability for educational governance through
their processes and structures. The director of medical education (DME) holds
responsibility for quality of the MB ChB programme and is accountable to the vice
chancellor. Responsibility for quality management processes are delegated to the
quality unit which checks that each EPU has adequate quality control mechanisms in
Standards
S2.1 The educational governance system continuously improves the quality and outcomes of education and training by measuring performance against the standards, demonstrating accountability, and responding when standards are not being met.
S2.2 The educational and clinical governance systems are integrated, allowing organisations to address concerns about patient safety, the standard of care, and the standard of education and training.
S2.3 The educational governance system makes sure that education and training is fair and is based on principles of equality and diversity.
19
place. The body responsible for the governance of quality is the board of studies and
they convene at least 3 times a year. The board of studies reports to the Learning
and teaching committee and the university senate.
Considering impact on learners of policies, systems, processes (R2.3)
34 It is clear that the school takes into account the views of patients and the public
when considering the impact of systems, policies and processes. The patient and
public group noted they have been recruited to work with the students to give their
perspective as patients currently going through the healthcare system. The group has
grown since our last visit and now consists of 20 members. There is a diverse mix of
experience in the group and we found those in the group to be enthusiastic and
content with their roles.
35 The patient and public group told us processes are evolving in line with student
feedback. The group added they feel confident in raising their suggestions and
listened to by the school. In the 2013-14 visit report we set a recommendation that
the school should increase the level of patient and public involvement in quality
management. We note the progress the school has made in this area and we now
consider the patient and public group to be an area that is working well.
Area working well 4: We note that there has been a significant improvement in the
way in which the patient and public group is constituted and run. The group is
engaged and motivated.
36 As noted in R2.1, feedback from learners and educators is central to the school’s
quality functions and during the visit we heard examples of how the school takes into
account the views of learners and educators. This is discussed in more detail under
R1.5.
Evaluating and reviewing curricula and assessment (R2.4)
37 There are clear governance structures around the school’s curriculum and assessment
frameworks. The school’s curriculum is managed by the curriculum executive, led by
the DME and formally governed by the board of studies. Management of the school’s
assessment is the responsibility of the assessment lead and decisions about
assessment outcomes for individual students are made by the board of examiners.
38 During the visit we heard evidence that the school evaluates their curriculum and
assessment frameworks in order to drive improvement in the quality of education and
training. It was noted that the quality lead works with the curriculum and assessment
teams to ensure that the quality of the programme is monitored, reviewed and
evaluated. Additionally, the curriculum implementation group meets regularly to
coordinate curriculum delivery and make recommendations for enhancement. The
phase two implementation group focuses on the delivery of clinical education in
phase two and acts as an interface between education providers and the school.
20
39 Senior management and supervisors at MKH told us they have the opportunity to
feedback on how the curriculum is working on the ground. They noted there are
regular face-to-face meetings, as well as more formal meetings to discuss the
school’s curriculum and to ensure supervisors at MKH are well informed about
changes in the curriculum. As noted previously feedback is central to the school’s
quality functions of evaluating and reviewing the success of their program.
Collecting, analysing and using data on quality and on equality and diversity (R2.5)
40 The school has analysed all summative assessments in order to examine student
learning, identify common gaps in knowledge, misunderstandings and mistakes. They
also conduct analysis on assessment results in relation to protected characteristics
and socio economic factors.
Systems and processes to monitor quality on placements (R2.6)
41 The school has Service Level Agreements (SLAs) with current provider hospitals, MKH
and Bedford Hospital NHS Trust, which outline the level of service expected from the
education providers. At the time of our visit the school noted that they are engaging
in discussions around securing additional placements with Buckinghamshire
Healthcare NHS Trust and South Warwickshire NHS Foundation Trust. The
discussions are in advanced stages with Memorandum’s of Understanding in place.
The school is aiming to finalise SLAs with Buckinghamshire Healthcare NHS Trust and
South Warwickshire NHS Foundation Trust by the end of 2016.
42 During the visit the school told us about systems and processes in place to monitor
the quality of placements. One of the ways in which the school monitors quality is
through their quality review visits. Frequency of these visits is determined by a risk
based assessment, and visits to LEPs will normally happen every year, but there must
be one at least every two years. Following a visit, a report and action plan is
produced.
43 The visiting process to monitor general practices is different in that visits are scaled
to reflect the greater number of general practices in comparison to LEPs. General
practices will be visited on average every five years and likewise with the quality
review visits to LEPs a report and action plan will be produced following a visit.
44 Outside of quality review visits, senior management at MKH noted there is a good
flow of information about quality matters between the trust and the school. The
quality management team at the school told us there is a quality management
meeting every month at the trust, which the school quality lead attends.
Sharing and reporting information about quality of education and training (R2.8)
45 Senior management at MKH noted they have a good working relationship with the
school and communicate on a day- to-day basis at all levels. MKH formally engage
21
with the school through the curriculum governance process, a joint executive
committee and joint quality committees. It is through these groups that information
pertaining to the quality of education and training at the trust is shared with the
school.
46 The school also told us they are continuing to develop their relationship with Health
Education England working across Thames Valley (HEETV). The school has an active
SLA with HEETV for students to access careers guidance and the Professional Support
Unit, and to play a part in the broader support of student learning. The school added
that HEETV services are utilised by their students and students confirmed they are
aware of the services provided by HEETV.
Area working well 5: We were impressed with the strong working relationship that
the school has fostered with Health Education England working across Thames Valley
in order to enable their students to access the Professional Support Unit.
Collecting, managing and sharing data with the GMC (R2.9)
47 The school is transparent in their reporting to the GMC. They have adequate
governance systems in place to collect and manage all the necessary data required by
the GMC. They have begun submitting a medical school annual return detailing
quality information and they are responsive to all other document requests from the
GMC.
Systems and processes to ensure a safe environment and culture (R2.11) & Educators for
medical students (R2.13)
48 The school has systems and processes to ensure that learners have appropriate
supervision. They hold SLAs with each of their education providers which outline that
each student should have named educational and clinical supervisors in each block.
The phase two implementation group has approved a set of standards for educational
supervision in line with Promoting Excellence outlining what the school expects from
educational supervisors in LEPs. Likewise, the school has also developed a set of
standards for clinical supervision which are also tailored to Promoting Excellence.
49 The school follow up on access to appropriate clinical and educational supervision
through their quality processes, such as quality review visits and also through
feedback from learners and educators.
Managing concerns about a learner (R2.16)
50 The school has systems in place to identify, support and manage concerns about a
learner. Senior management at the school noted that student support is active and
quality management systems are functional in identifying students who require
additional support. Concerns can be identified through a variety of ways including:
attendance, performance in assessment and concerns raised by staff and students.
22
Once a concern has been identified the concerns group coordinates support for
students and the pastoral support team delivers it either directly or by referral to
specialist providers. There is a low threshold for referral in order to enable early
identification of students in potential difficulty. Please see R3.2 for a more
comprehensive explanation of resources the school provides to support the health
and wellbeing of their learners.
Sharing information of learners between organisations (R2.17)
51 We were assured the school has a transfer of information system in place to
adequately share information about a learner between sites. Student support told us
transfer of information forms are generated by the support lead, signed by the
student and occupational health physician and then passed to the LEPs. Senior
management at the school told us that transfer of information has been
communicated to the LEPs in preparation for phase two, and senior management at
MKH confirmed there is an adequate transfer of information process in place and
communication flow is working well.
Requirements for provisional/full registration with the GMC (R2.18)
52 During the 2015/16 cycle of visits we recommended the school should set out clear
guidance on the thresholds that would trigger fitness to practise procedures. Before
the visit the school told us they have been working to refine their FtP procedures and
thresholds in advance of receiving a case. Since our last visit the school has
considered GMC guidance on Professionalism and has incorporated it into their FtP
training and procedures. They now have a framework by which evidence and reports
from hearings will be collected and presented. We will keep this item open for further
monitoring until the process has been utilised more to ensure changes are
sustainable.
Recruitment, selection and appointment of learners and educators (R2.20)
53 The school’s selection processes operate in two stages. The first stage is an academic
selection and the second is the OSSEs, which are a series of stations with different
tasks to test abilities related to Good Medical Practice. During our OSSE observation
we found that the ten stations were varied and tested a diverse range of skills. It was
also apparent the school has blueprinted the stations against Good Medical Practice.
We therefore noted this as an area working well.
Area working well 6: The OSSE stations tested a wide range of skills and attributes
which we note are blueprinted against Good Medical Practice.
54 The OSSE commenced with assessor and candidate registrations, before leading into
a comprehensive assessors briefing and station allocation. As part of the process
parents and partners of candidates have the opportunity to have an informal chat
23
with the school to ask any questions they may have and also tour the campus and
medical school once candidates have finished their examination.
55 We observed the school’s selection process to be open and transparent. The process
was communicated clearly to all and assessors had an in-depth briefing before
commencing. The rotation around the OSSE stations also accommodated candidates
who required reasonable adjustments of extra time. Additionally, the OSSEs were well
organised and ran smoothly and there were ample staff committed to excellence and
delivering the OSSEs successfully. We therefore identified below as areas that are
working well.
Area working well 7: The School’s selection processes are open and transparent.
Area working well 8: The OSSE was well organised, with a high level of staff
involvement and commitment.
56 Despite observing areas of the OSSEs working well, we observed inconsistencies with
the role of the simulated patients involved in the examinations. During some of the
stations assessors and simulated patients consulted when scoring candidates, while at
other stations assessors did not consult with simulated patients. We also observed
that some examiners interacted with candidates after a station had finished whilst
others did not and that there were discrepancies in examiners’ understanding of the
nature of the global score.
57 The school reviews their selection processes each time they are run. The selection
team told us stations are developed and candidate feedback is analysed with the aim
of making improvements. Psychometric analysis is also completed following each
selection cycle. Previous psychometric reports highlight that Cronbach’s Alpha for the
ten stations is lower than desired. The school has recently increased the number of
OSSE stations to ten but they acknowledge that their Alpha is below the 0.80 desired
thresholds for reliability. For the 2016 intake, 225 candidates sat the OSSEs over five
days. The school has reported diversity in Cronbach’s Alpha across the five days and
therefore plan to consider reasons for stations performing poorly across the different
selection days. While the visiting team accepts that achieving a value greater than
0.80 for Cronbach’s Alpha for a new assessment can be challenging, we encourage
the school to continue to develop this assessment to maintain its aims while also
improving its reliability. We have therefore set a recommendation for the school to
address.
Recommendation 1: In OSSE settings, consideration should be given to further
develop consistency in the simulated patients’ performance, examiners’ interactions
with students, examiner training in relation to the nature of the global score and also
the reliability of the selection event.
24
Theme 3: Supporting learners
Standard
S3.1 Learners receive educational and pastoral support to be able to demonstrate what is expected in Good medical practice and achieve the learning outcomes required by their curriculum.
Learner's health and wellbeing; educational and pastoral support (R3.2)
58 Throughout our visit we were told about the excellent educational and pastoral
support the school offers by both students and staff. The school told us that in order
to deliver highly effective support to students that two main groups interact; the
concerns group and the pastoral support team. The concerns group coordinates all
support for students for concerns such as academic and health or conduct. Concerns
can be identified through a variety of ways including: attendance, performance in
assessment and concerns raised by staff and students. The concerns group does not
deliver support directly, but develops a structured action plan which is implemented
through the pastoral support team. The pastoral support team provides support
either directly or by referral to specialist providers.
59 Referrals to specialist providers include:
Occupational health services at MKH
coaching and mentoring services by the pastoral team
learning support including an assessment by an educational psychologist
academic skills support
direction to the big white wall service, which is an anonymous online platform
guided by trained professionals aiming to help those with mental health
conditions through seeking support from each other by sharing their
experiences
specialist services provided through St Andrew’s outpatient clinic and HEETV.
60 In addition to the school providing their own support services, and as mentioned in
R2.8, students have access to careers guidance and the Professional Support Unit at
HEETV. HEETV services are utilised by Buckingham students and during the last
academic year HEETV saw a number of Buckingham students for careers guidance
and training in language and communication.
61 As well as signposting students to HEETV career services, the school has developed
their own career advice initiatives. Students told us about an interactive lecture on
career options they received. They added staff at the school are very supportive in
helping the students explore their interests. Additionally, we were told student
25
support has created a Moodle page for careers which details information such as:
careers fairs and workshops, professional development conferences and blogs from
various students.
62 Overall, we identified this level of support as an area of good practice. The school
offers a wide range of high standard support to students. We heard consistently from
students that educational and pastoral support at the school is excellent. They told us
staff are accessible, responsive, approachable and that they feel comfortable raising
any issues with them.
Good practice 1: We heard from all of the groups that we spoke to about the
responsiveness of the school and the high level of educational and pastoral support
available to students.
63 We identified student perception of the concerns group is that it is a group aiming to
help students overcome any issues they may be having. The students told us they
feel comfortable accessing the group and are clear the group is wholly supportive and
independent of FtP processes.
64 During the 2015/16 cycle of visits we set a requirement that the school must ensure
the fitness to practise committee structure exclude those formally involved in student
support and progress from making fitness to practise decisions. The school has
demonstrated that student support and the fitness to practise committee are
independent bodies with different roles. The fitness to practise committee has no
common membership with the concerns group and is comprised of several external
members. We are therefore happy that this requirement has been met and can
therefore be closed.
Undermining and bullying (R3.3)
65 When asked about undermining and bullying, supervisors at MKH told us the trust has
a policy on undermining and bullying and they have no examples of such behaviour.
They told us staff and students are able to raise their concerns without fear of
adverse consequences and students are introduced to the policy during their
induction.
Student assistantships and shadowing (R3.6)
66 The school told us they are planning for four week student assistantships in a
secondary care environment in the final year and they will commence shortly after
electives finish. We will further explore the school’s planning for assistantships in the
2017/18 cycle of visits.
26
Information about curriculum, assessment and clinical placements (R3.7)
67 During the visit year one students told us the school has not communicated where
their clinical placements will take place during phase two. They added as there are no
year three and four students in the school they do not know where they are likely to
be placed for their clinical placements. They noted that this situation is causing
difficulties with arranging accommodation for coming years as they are expected to
sign annual housing leases when they do not know where they are going to be
placed.
68 As mentioned in R2.6, the school is currently engaging in discussions around securing
additional placements with Bedford Hospital NHS Trust and Buckinghamshire NHS
Trust and South Warwickshire Foundation Trust. They added once the school
confirms if these placements will go ahead or not then they will be able to confirm
where the year one students will be placed in phase two. They added they are hoping
for contracts to be signed by the end of 2016. In the meantime, all year two students
will be placed at MKH and year one students will be told where they are going for
clinical placements at the end of the first term in year two.
69 While we recognise there are fixed constraints on when year one students can expect
to find out where they are being placed in phase two, we encourage the school to
improve communication with current, as well as future cohorts to ensure students
receive timely and accurate information about their clinical placements.
Recommendation 2: The school should improve communication with current and
future cohorts to ensure that students receive timely and accurate information about
their clinical placements.
70 During our visit observing the year two OSCE we found the students to be well
prepared for the format of the exam. The school submitted documentation noting
students are informed about the OSCE in a variety of ways, including presentations
and on Moodle. They also shared the written brief that students receive before the
exam detailing information on OSCE organisation, OSCE marking and feedback and
general guidance for preparing for the exam. This exam operated smoothly and it
was evident that students had received accurate information prior to their exam.
Area working well 9: Students were well prepared for the format of their OSCE. It
is evident that they have been appropriately briefed and supported.
Out of programme support for medical students (R3.9)
71 The school told us a six week elective period will take place following the final
professional exam. Students then go on to complete their assistantship. Please see
R3.2 for further information on the support that the school offers. In future visits we
will explore the support offered to those students specifically on electives.
27
Feedback on performance, development and progress (R3.13)
72 During the visit we found learners are receiving regular, constructive and meaningful
feedback on their performance, development and progress. The facilitators we met at
MKH told us they give the students constructive feedback following tasks. They noted
they highlight specifics that may have been missed, areas for improvement, any
positives and address professionalism. We heard students also have the opportunity
to reflect on their own performance for development. Students at MKH told us they
are receiving enough feedback to enable their development and they can access
materials such as patient notes to enable their development.
73 Following the 2015/16 cycle of visits and observations, we set the school a
recommendation to request examiner written feedback for all students in their OSCE
and not only for those assigned a failing grade. During the year two 2017 OSCE we
found that examiners provide brief comments on the observation sheets regarding
student performance at the different stations. We are therefore satisfied that this
recommendation has been met and it can now be closed.
Career support and advice (R3.16)
74 During our visit the senior management team told us that the school’s exit degree has
been approved by the university. They noted that it makes up 360 credits and
students can opt to receive the degree at the end of phase one if they are not able to
complete a medical qualification.
28
Theme 4: Supporting Educators
Standards
S4.1 Educators are selected, inducted, trained and appraised to reflect their education
and training responsibilities.
S4.2 Educators receive the support, resources and time to meet their education and
training responsibilities.
Induction, training, appraisal for educators (R4.1)
75 The academic teachers we met told us they have received an induction to their role
and the curriculum. We were told the school has provided training in their roles in
areas such as, delivering group teaching and equality and diversity. It was made clear
that professional development is valued, with some of the academic teachers
highlighting they are studying for a postgraduate certificate in education. Additionally,
academic teachers told us they receive an annual appraisal with the DME.
76 The patient public group told us they have received numerous guidance documents
to support them in their roles. They noted they have had the opportunity to
undertake training in equality and diversity, and added they receive feedback from
students following their sessions. Some told us their sessions have been observed
and noted the feedback and observations contribute to their personal development as
they are able to develop and improve their sessions based on the feedback they
receive.
77 Supervisors at MKH supported the above and told us they have received training for
their roles. They added the trust fund and support those involved in education to
undertake additional training such as a masters and a PGCE.
Area working well 10: Educators are well trained and supported in their roles to
meet their education and training responsibilities.
Time in job plans (R4.2)
78 At the time of our visit the school did not have a full complement of educational
supervisors in post for the delivery of phase two. They added they are hoping to
recruit seven to eight educational supervisors per block and confirmed allocated
educational supervisors will be identified by the end of 2016 in order to undergo
training before starting in post for the delivery of phase two. Additionally, we were
told induction into the curriculum for new supervisors is planned and accounted for.
79 Undergraduate supervisors at MKH told us finding supervisors is a challenge and
supervisors do not all have formal time for teaching embedded into their job plans.
They noted time in job plans is not universal and highlighted discrepancies between
those with teaching responsibilities. Additionally, there is also an uncertainty around if
29
newly appointed supervisors will have adequate time allocated in their job plans for
teaching.
80 Whilst we recognise the school plan to have educational supervisors appointed by the
close of 2016, we encourage the school to expedite the appointment of educational
supervisors for phase two.
Requirement 2: The school must expedite the appointment of educational
supervisors for phase two to ensure they are trained and that their job plans reflect
their new role.
Educators' concerns or difficulties (R4.4)
81 Supervisors at MKH noted there is a process in place with the school to support
educators in dealing with learners in difficulty while on placement. Supervisors told us
if such a situation was ever to arise they would build up a picture of student
performance through documentation and relay this back to the school for support.
Academic teachers also noted they are kept updated on reported concerns regarding
students.
Working with other educators (R4.5)
82 Academic teachers told us they are encouraged to liaise with each other and work as
a team. They added academic teachers at the school support each other and also
interact with clinical teachers that teach at the LEPs the school works with.
Recognition of approval of educators (R4.6)
83 The school has met the formal GMC milestone for the recognition and approval of
educators. The senior management team at MKH supported this and told us that all
their supervisors have completed training in relation to the recognition and approval
of trainers, and that there is a phase two implementation working group that
monitors trainers are compliant with requirements.
30
Theme 5: Developing and implementing curricula and assessments
Informing curricular development (R5.2)
84 The school’s curriculum is informed by a range of stakeholders. During the visit
examples of developments and changes to the curriculum as a result of stakeholder
input were provided. The school also told us about the role of the curriculum
implementation group, who convene regularly and focus on improving the quality of
the school’s curriculum. Members of this group are drawn from across the medical
school and include academic, clinical and administrative staff.
85 The school also uses feedback from learners and educators in order to inform the
curriculum. Supervisors at MKH told us they have the opportunity to provide feedback
to the school on the curriculum through the phase two implementation group. The
GPs we met noted they have found the phase two implementation group a useful tool
to discuss the curriculum. Students also told us they have the opportunity to provide
feedback to inform the curriculum at the end of each unit.
Undergraduate curricular design (R5.3)
86 All of the students we met are content with the organisation and breadth of their
curriculum. Second year students commended the wide range of learning
opportunities and noted they enjoy the early patient contact in phase one as it
enables them to link the theory they learn to practice.
87 The school delivers a unit in narrative medicine which aims to teach students to see
patients as humans with individual stories experiencing illness in their social context.
During the narrative medicine unit students are assigned a patient whom they see
once a term. Students spoke highly of the narrative medicine unit as it offers them
the opportunity to gain insight into the longitudinal journey of a patient.
88 All of the students we met valued the small group teaching sessions. They told us
they are effective learning tools as they identify areas for improvement. Students
noted they enjoy applying their learning through example exam questions and case
studies in the small group teaching sessions. Students also praised the small group
sessions for anatomy noting they are effective in developing their learning. We
therefore identified the small group teaching sessions as an area that is working well.
Standard
S5.1 Medical school curricula and assessments are developed and implemented so that medical students are able to achieve the learning outcomes required by graduates.
S5.2 Postgraduate curricula and assessments are implemented so that doctors in training are able to demonstrate what is expected in Good medical practice and to achieve the learning outcomes required by their curriculum.
31
Area working well 11: Small group teaching is working well and was commended
by students.
89 The school has one open requirement and three open recommendations that fall
under this requirement. During the 2014/15 cycle of visits we set a requirement for
the school to ensure that contingency plans with the University of Leicester continue
to be feasible, and that the Buckingham curriculum must align with the new Leicester
curriculum. The school has been working towards meeting this requirement, but have
noted that it is not possible for them to maintain an exact alignment with Leicester
over the next three years as the new course at Leicester is being implemented in
stages. Phase one of the course in Buckingham is the same length as phase one in
the Leicester curriculum and the phase one clinical course at Leicester is also similar
to that at Buckingham. The school noted a potential transfer of students from
Buckingham to Leicester in phase one would not put them at a disadvantage.
90 The Leicester curriculum changes to phase two are greater and the finer details are
less well developed. While parts of the curricula are similar others are not, however,
potential issues with transfer points have been noted and are on the school’s radar.
We will therefore continue to monitor this item during future QA cycles.
91 The 2013/14 cycle of visits identified the recommendation that the school should
increase their number of SSCs and provide clearer links to how they meet the
learning outcomes defined in Tomorrow’s Doctors. During the 2015/16 cycle of visits
the visit team concluded this recommendation was partially met as the school has
mapped all of its SSCs to the learning outcomes in Tomorrow’s Doctors.
92 SSCs in phase one of the curriculum run in terms five and six and since the 2015/16
cycle of visits the term five SSCs have now run for the first time. SSCs are organised
into two components, taught units and library projects and students must complete
one of each in either term five or six. In term five the school delivered three taught
SSCs and students had a choice of 73 university sourced library projects. Students
also had the option to source their own library projects. Students are already
allocated to their term six SSCs with the school planning to deliver five taught SSCs
and the option of 73 library projects. In total the school has 8 taught SSCs across
term five and six.
93 Year two students who had completed their term five SSCs at the time of our visit
told us that the choice of SSCs complement the course and their learning. Feedback
on their SSCs was generally positive and students noted they were clear and well-
structured and supervisors were easy to access throughout. Some students however
noted they would prefer greater diversity in the taught SSCs. The senior management
team told us there are up to five new SSCs in development with additional proposals
for new units under scrutiny.
94 Since our last visit it is clear that the school has been working towards meeting the
rest of this recommendation through working towards increasing the number of SSCs
32
on offer to their students and delivering the first round of SSCs. In addition, feedback
from year two students on their SSCs was generally positive but some students made
reference to the diversity available for the taught SSCs. We will continue to monitor
this item until the additional SSCs in development have been finalised.
95 In our 2013-14 visit report we made a recommendation for the school to develop
robust procedures to manage patient participation at general practices. During the
2015/16 visit report we noted that general practices have been provided with detailed
scheduling templates to allow them to plan patient participation. However, there had
been limited patient contact at the time of the visit. During the 2016/17 cycle of visits
no concerns were highlighted in relation to procedures around patient participation at
general practices. The year two students we met told us their GP placements are
going well, they are well organised and they are enjoying the narrative medicine
strand. In addition, the school told us there is no evidence of outstanding issues from
their quality information. This recommendation can therefore be closed.
96 The 2015/16 cycle of visits recommended that the school should carefully consider
how often small activity groups are changed. Currently students stay in the same
peer groups for the whole of phase one. However, the school planned to carry out an
evaluation of the small group activities to enable consideration into changing the
student groups. Student representatives were asked to consult informally with the
student groups and identified mixed views, in that some groups have formed strong
bonds, while others would welcome a change. At the time of our visit in September
2016 the school planned to formally consult with the student body regarding potential
changes to the small activity groups with an aim to implement an outcome in early
2017. We will therefore follow up on this recommendation in the next cycle of visits.
Undergraduate programmes and clinical placements (R5.4)
97 The school currently has SLAs with MKH and Bedford Hospital NHS Trust and are
hoping to secure additional placements with Buckinghamshire Healthcare NHS Trust
and South Warwickshire NHS Foundation Trust. The LEPs that the school works with
are working to different timelines in terms of receiving students. During phase one
students undertake placements at MKH. Phase two students will commence
placements at St Andrews in early 2017, and during our meeting with representatives
from St Andrews they noted they are familiar with Buckingham’s curriculum and they
are prepared for students to arrive. It’s planned that students will begin clinical
placements at Bedford Hospital during 2018. The school told us the recruitment of
GPs to accommodate phase two has been successful and there have been no issues
with attracting GPs.
98 Year two students told us both their primary and secondary care placements are
enjoyable and well organised and structured. They noted that placements are well
linked to small group activity sessions and support their learning at the school.
Additionally, they noted both consultants and GPs are keen to teach the students and
make them feel welcome.
33
Assessing GMC outcomes for graduates (R5.5)
99 The school utilises a whole course assessment blueprint to outcomes for graduates to
ensure that students experience outcomes in different contexts across assessments
from the first to the final year. At the time of our visit the school was in the advanced
stages of planning for the delivery of phase two. They told us they have reviewed the
outcomes of each block and mapped them to the outcomes for graduates to ensure
outcomes are explicitly met in each block.
100 The school are continuously refining their assessment processes as they continue to
deliver and perform psychometric analysis on their assessments. However, it is clear
the school is aware of the importance of mapping their assessments to outcomes for
graduates as they note the whole course blueprint is the starting point for the
development of all the written and OSCE assessments.
101 The second year OSCE that we observed tested learning from the whole of phase one
and is clearly blueprinted to outcomes for graduates. We found the 12 station OSCE
samples a wide range of the outcomes in a variety of patient presentations and many
of these stations are advanced for the students’ stage of learning. We have therefore
noted this as an area that is working well.
Area working well 12: The OSCE stations tested a wide range of skills and
attributes which we note are blueprinted against outcomes for graduates.
Fair, reliable and valid assessments (R5.6)
102 The school takes adequate steps to scrutinise and ensure their assessments are fair,
reliable and valid. They use the borderline regression method of standard setting for
the end of year OSCEs and the modified Angoff method of standard setting for the
qualifying exam OSCEs. They use Cronbach’s Alpha as a measure of internal
consistency of examinations and aim for a sore of 0.80 or greater. Previous
assessment reports for the OSCEs have found that Cronbach’s Alpha is either slightly
above or slightly below 0.80, and closer to 0.90 for end of term assessments.
Additionally, item-total correlation is used to evaluate performance on the different
questions in written examinations. So far, the school has identified several questions
with poor item-total correlations which have been reviewed by the assessment team.
103 The school has two open recommendations relating to this requirement. The 2014/15
cycle of visits identified that the ratio of new and tested questions should be reviewed
during the initial run of the assessments throughout the process. To begin with the
school used Leicester’s assessment items; however, Leicester questions are now
seldom used and the school has developed an approach that generates large
numbers of questions which are progressively filing their question bank. Staff
involved in teaching input by suggesting questions, a paper is then created by the
deputy assessment lead, scrutinised by the appropriate groups of staff before being
submitted to an external examiner for comment. The school noted that psychometric
34
analysis of previous examinations found that assessments constructed with the
school’s own items are robust and reliable and the school is responding to the few
questions with less favourable psychometric characteristics. We are therefore satisfied
that this item can now be closed.
104 The 2015/16 OSCE observation identified that consideration should be given to
further develop consistency in the simulated patients’ performance, examiners’
interactions with students and the calibration of students’ marks and outcomes. The
second year 2017 OSCEs highlighted that the school has begun to take steps to
address this. The OSCE began with a briefing for examiners and simulated patients
which highlighted the importance of portraying their roles in a consistent fashion,
scoring candidates and general house rules for the OSCE. This was followed by a
calibration and familiarisation exercise during which assessors and simulated patients
practised their roles. This aimed to ensure consistency in simulated patient acting
between the two loops, and develop a shared common understanding of the marking
system amongst the assessors of the different stations and loops.
105 However, we observed some discrepancies between the examiners and simulated
patients in the OSCE marking process, with some of the simulated patients
contributing considerably to marking whilst others did not. This varied across the
stations and between the loops. We also observed that some of the examiners
intervened by stopping the students to ensure there was adequate time to answer
the ‘optional’ questions at the end of a station whilst others did not.
106 We fed this back to the school after our observation of the first year two OSCE, and it
was evident that the school had taken steps to further address these discrepancies
for the year two qualifying exam OSCE. We observed a clearer briefing to examiners
which emphasised that simulated patients should not contribute to marking in any
way. Following this we observed that simulated patients did not contribute to the
marking process or attempt to influence the marking process as advised in the
morning training session. The school also changed the briefing and documentation to
make clear that the questions at the end of the station are not optional and the
student should be stopped with adequate time to answer the questions.
107 During the 2016/17 second year OSCE we observed the competency and global
marking and discussed this with some examiners. We are concerned that this may
not be borderline regression for standard setting because it appears that the
competency marks are being used directly to calculate the global score. The school
had taken steps to address this in the second year qualifying exam OSCE and we feel
there has been some improvement. The school has clarified the independence of the
global score and the competency marks with examiners and we encourage the school
to continue their efforts in ensuring that competencies are objectively marked and
regressed against the global score.
108 We also found inconsistencies amongst examiners in their understanding of the
thresholds for passing. Some described the global score of pass being equivalent to a
35
competent FY1 and a global score of excellent being equivalent to an excellent FY1.
However, other examiners described pass as not quite at FY1 level and excellent as
equivalent to a competent FY1. Therefore, there may not be a shared vision of what
constitutes a pass and also it may be unrealistic to expect a year two student to
perform at FY1 level in order to pass. At the second year qualifying exam OSCE the
standards expected for the global scores of pass and excellent were covered
thoroughly in the early morning briefing and we observed an understanding amongst
examiners in the thresholds for passing. Although we have observed some
improvements with this issue and note the school are addressing concerns we will
keep this recommendation open to ensure that changes made are sustainable.
109 The school told us they are conducting a review of their assessment processes in
order to continuously enhance the way in which assessments are delivered. For a
given type of assessment the school has decided that students must pass a set
number of short answer questions or OSCE stations in order to pass the assessment
overall. The methodology used to decide the number of questions needed to pass, is
not explicit. The visit team encourage the school to consider this in their assessment
review.
110 The school currently combine the OSCE and multiple choice questions to decide if a
pass or fail should be awarded in the qualifying exam; however they do not adopt
this method for term exams. The school has noted they are keeping the differences
between the term and qualifying exam method under review. Additionally, by the end
of the academic year students who fail a component, or cannot take an exam due to
mitigating circumstances are required to sit the qualifying exam that covers the full
year, rather than resit only the exams they have failed. Again we encourage the
school to keep this under review.
111 The school analyses item-total correlations to assess student performance across
different stations or questions in an assessment. The visit team notes that some
items in both written exams and OSCEs have had a low item-total correlation and
encourages ongoing analysis of this in their assessment review.
112 The board of examiners meeting that we observed discussed if students who had
taken the second year qualifying exam were able to progress to phase two of the
course. High performing students from the whole of phase one were also considered
for an award. Overall, the meeting was well run with input from appropriate areas of
expertise. The school had adequate external representation, including a lay
representative and an external examiner who had considered the assessment analysis
for the qualifying exam and concluded that it is reliable. From the meeting and
papers it is apparent that the school undertakes rigorous scrutiny of its exams
including previously mentioned psychometric analysis and double marking of short
answer questions with moderation/checking.
113 However, we consider the school is awarding a large number of distinctions and
merits, out of keeping with the sector norms. In 2016, 20% distinctions and 40%
36
merits were awarded to year one and two students. The external examiner also noted
this as an area for consideration. The school is aware of this and is looking to address
it in future cohorts. Considering that these points contribute to a possible honours
degree we encourage the school to address this and the above four areas listed in
paragraphs 109-113 through their assessment review.
Recommendation 2: The school should continue to evaluate their assessment
processes through their ongoing assessment review.
114 The year two OSCEs identified that the school invests heavily in their assessment
processes. They conduct psychometric analysis following each examination to test the
reliability of their assessment processes. Results are then considered at the board of
examiners meetings. The visit team noted this as an area that is working well in the
school and we encourage the school to continue to develop their assessment
processes.
Area working well 13: The school’s investment in assessment and high level of
analysis is to be commended
Examiners and assessors (R5.8)
115 Assessors are selected from medical school staff, clinical staff and partner
organisations such as general practices and LEPs. All assessors undertake a
comprehensive training session related to the OSCEs which covers OSCE scoring,
standard setting, bias and video calibration. The school also use recorded stations
with candidates being role played by others, for training and calibration of marking by
examiners.
116 During the 2016/17 second year OSCEs we observed the assessors briefing followed
by the calibration exercise. Following this we made some suggestions to the school
and during the qualifying exam it was evident that the school had improved their
assessors briefing. Additionally, the calibration exercise is a welcome development to
ensure a high level of consistency and judgement between assessors.
Area working well 14: We found the OSCE to be well organised, with a high level
of staff involvement and commitment.
Reasonable adjustments in the assessment and delivery of curricula (R5.12)
117 The school has a process in place for dealing with students who require reasonable
adjustments. An educational psychologist reassesses all students accepted onto the
programme who have disclosed a learning support need at application. Reasonable
adjustments are confirmed following a discussion between the educational
psychologist and occupational health services. Those who have not disclosed a
learning support need at application are referred to the educational psychologist
through the concerns group. Following the identification of a support need, the
37
assessment teams, unit leads and personal tutors monitor student performance with
regard to the adjustment.
118 During our observation of the OSCE it was evident that reasonable adjustments had
been implemented as some students had extra reading time before commencing a
station. We noted this as an area that is working well.
Area working well 15: We observed clear evidence that reasonable adjustments
have been implemented for the OSCE by the School.
38
University of Buckingham Medical School’s response to the GMC’s visit
report
The University of Buckingham Medical School (UBMS) thanks our GMC visiting team
for a reasonable and constructive approach to our ongoing quality assurance process.
The School is content to accept the conclusions of the report, and is heartened by the
recognition of considerable strengths in our developing provision. We are already
addressing the few requirements and recommendations made and look forward to
demonstrating this to the team in the next cycle.
It is always our aim to meet, and preferably exceed, the standards for medical
education prescribed by the General Medical Council. We welcome constructive
feedback that will enable us to do so, and we aim to act upon that feedback as
quickly as we can. In reality, we believe, most issues identified in this report were
already addressed before we received it.
We will continue to cooperate as best we can with our ongoing quality assurance
process.
39
Team leader Dr Nick Bishop
Visitors Dr Bruno Rushforth
Dr Carol Gray
Mr Faisel Alam
Prof Helen Cameron
Dr Jessie Sohal-Burnside
GMC staff Emily Saldanha (QA Programme Manager)
Jessica Ormshaw (Education Quality Analyst)
Evidence
base
Doc 161: UBMS term two risk register – October 2015
Doc 162: UBMS update on the academic building at MKH – November
2015
Doc 163: UBMS update on clinical capacity – November 2015
Doc 164: Examples of narrative medicine reflective accounts –
November 2015
Doc 165: UBMS substantive term three OSCE report – December 2015
Doc 166: UBMS substantive term three written paper report –
December 2015
Doc 167: UBMS term three OSCE examiner correlations – December
2015
Doc 168: UBMS updated global risk register – June 2016
Doc 169: Quality management & enhancement in year two – June 2016
Doc 170: Progress report on open issues – August 2016
Doc 171: Progress report on resources and staffing – August 2016
Doc 172: Progress report on the implementation of Phase two – August
2016
Doc 173: Progress report on assessments - August 2016
Doc 174: Progress report of student support – August 2016
Doc 175: Briefing document for the year two OSCE observation –
January 2017
Doc 176: Briefing document for QE2OSCE observation – February 2017
40
Doc 177: Exam board report MED15 QE year two – March 2017
Doc 178: Exam Board meeting agenda – March 2017
Doc 179: Board of examiners minutes for MED16, ETA3 and QE
Doc 180: OSSE performance report 2015 selection cycle