virushepatititis & leberzirrhose - fomf.at wien... · struktur des hepatitis b virus middle...
TRANSCRIPT

Virushepatititis & Leberzirrhose
Abteilung für Innere Medizin I
Gastroenterologie & Hepatologie, Rheumatologie
Endokrinologie und Diabetologie
Klinikum Wels-Grieskirchen
Harald Hofer

Virushepatitis

Primär hepatotrope Viren Sekundär hepatotrope Viren
- Hepatitis A (HAV)- Hepatitis B (HBV)- Hepatitis C (HCV)- Hepatitis D (HDV)- Hepatitis E (HEV)
Humane Herpesviren- Herpes simplex Virus (HSV)- Zytomegalievirus (CMV) - Epstein-Barr Virus (EBV)- Humanes Herpes Virus 6, 7, 8- Varicella Zoster Virus (VZV)CoxsackievirenParamyxovirusParvovirus B19Exotisch: Dengue, Gelbfieber, Lassa, Ebola
Virale Hepatitiden

Prävalenz der Hepatitis A
• Hepatitis A Virus (HAV): RNA Virus
• Übertragung : – Kontaminierte Nahrungsmittel (fäko-oral)
– Selten sexuelle Übertragung
• Lebermanifestation – Akute Hepatitis (Leberversagen möglich)
– Keine chronischen Verlaufsformen
• Therapie : – Symptomatisch, Impfung!
Virale Hepatitiden – Hepatitis A

HAV fulminante Hepatitis§
HAV - non fulminant
Alter* 35.4 ± 8.9 31 ± 6.6
Männer* 90 % 57 %
C2 Abusus* 20 % 3.3 %
HBs Ag pos.* 40 % 4.1 %
Bilirubin 23.8 ± 16.6 7.0 ± 3.9
AST 5173 ± 2768 2578 ± 2447
INR 3.5 ± 1.4 1.2 ± 0.3
Kreatinin 3.5 ± 2.5 1.1 ± 1.1
Kim et al. Factors influencing the severity of acute viral hepatitis A. Korean J Hepatol 2010;16:295-300
§ definiert durch Encephalopathie < 8 Wo. nachBeginn des Ikterus & INR > 1.5
Jacobsen KH. et al The Global Prevalence of Hepatitis A Virus Infection
and Susceptibility: A Systematic Review. 2009
Fulminante Hepatitis A

Struktur des Hepatitis B Virus
Middle surface Antigen
Nukleokapsid
Small surface Antigen
Large surface Antigen
Lipoprotein Hülle
Genomische DNA
DNA Polymerase
lHBsAg, Prä-S1/S2 Domäne
sHBsAg, S-Domäne, 24kD
mHBsAg, Prä-S2 Domäne

HBV mRNA
HBV
Golgi
ER
HBsAg
CCC
DNA
HBeAg
Hepatitis B Virus Replikationszyklus
Core Assembly/RNA Packaging
plus strand minus strand synthesis
APC
Once Hepatitis B - always
Hepatitis B !

Hepatitis B: Risiko der Reaktivierung unter Immunsuppression
Risk of reactivation
HBsAg(+) and
HBV DNA(-)
HBsAg(+) and
HBV DNA(+)
HBsAg(-), anti-HBc(+),
anti-HBs(±) and HBV DNA(-)
Pre-emptive/prophylact. therapy
(NUCs)
Close monitoring of ALT and
HBV DNA; initiate rescue
therapy where indicated
Serologie/HBV DNA (Replikation) 1,2,3
HBsAg(-),anti-HBc(+),
and HBV DNA(+)
Risiko: hoch>10%, mittel (1-10%), niedrig (<1%)1,2,3
Dauer und Intensität der Immunsuppression (Biologika, Rituximab) 1,2,3
1.Reddy et al., Gastroenterology 2015, 2.Perillo et al., Gastroenterology 2015, 3. EASL Clinical Practice Guidelines 2017

Jahre
HBV
HBV: Natürlicher Verlauf & Therapieindikation
Chronische Hepatitis
Akute Hepatitis
Cirrhosis
hepatis
~5%
HCC
HBsAg Elimination
99% kompensiert50- 70% anikterisch30 - 45% ikterisch
Therapie: NEIN
Akutes Leberversagen
Therapie: JA
Schwere akute, fulminante (<1%)

Jahre
HBV
HBV: Natürlicher Verlauf & Therapieindikation
Chronische Hepatitis
Akute Hepatitis
Cirrhosis
hepatis
~5%
HCC
HBsAg Elimination
99% kompensiert50- 70% anikterisch30 - 45% ikterisch
Therapie: NEIN
Akutes Leberversagen
Therapie: JA
Schwere akute, fulminante (<1%)
HBeAg neg. chron. Hep. B
HBeAg pos. chron. Hep. B
HBeAg neg. chron. Infektion(HBsAg Carrierstatus)
HBeAg pos. chron. Infektion(Immuntoleranter Status)
HBsAg Carrier
Immuntoleranz

Jahre
HBV
HBV: Natürlicher Verlauf & Therapieindikation
Chronische Hepatitis
Akute Hepatitis
Cirrhosis
hepatis
~5%
HCC
HBsAg Elimination
99% kompensiert50- 70% anikterisch30 - 45% ikterisch
Therapie: NEIN
Akutes Leberversagen
Therapie: JA
Schwere akute, fulminante (<1%)
Virussupression
THERAPIE
HBV DNA
nachweisbar
THERAPIE
HBV-DNA (> 2x10³ IU/ml)
ALT (erhöht)
Histologie (>A1/F1)

Hepatitis B – EASL CPG 2017

Substanz Präparat
Nucleosidanaloga Lamivudine (LAM), Zeffix®: 100mg/d
Entecavir (ETV), Baraclude®: 0.5mg/d
Telbivudine (LdT), Sebivo®: 600mg/d
Nucleotidanaloga Adefovir (ADV), Hepsera®: 10mg/d
Tenofovir (TDF), Viread®: 245mg/d
Tenofovir (TAF), Vemlidy®: 25mg/d
Interferon Interferon-a
PEG-IFN a-2a, Pegasys®: 180µg/Woche
Therapie der chronischen Hepatitis B

Hepatitis C Virus (HCV)
• 40-70 nm in diameter
• Envelope proteins E1, E2
• Lipid envelope derived from host cell
• Nucleocapsid containing single-stranded viral RNA and capsid protein
• Identified 1989
• HCV Genotypen
1. Moradpour D et al. Nat Rev Microbiol. 2007;5:453-463.

HCV
Spontane Viruselimination
Chronische
Hepatitis CAkute
Hepatitis C
~85%
Natürlicher Verlauf der HCV Infektion
~15%
Fulminante
Hepatitis
<1%
Ausheilung
Leber-
zirrhoseHCC
Akutes
Leberversagen


HCV Structural proteins HCV Non-structural proteins
HCV Lifecycle StepsDirect-Acting Antiviral
NS3 NS5A NS5B
Viral Entry
Translation
Processing
Replication complex
Replication
Assembly
Release
HCV Genome3
6
4,5
4,5
4,5
1. Gao et al. Nature. 2010;465:96.; 2. Nettles et al. Hepatology. 2011;54:1956; 3. Chevaliez et al. In: Hepatitis C Viruses:
Genomes and Molecular Biology, 2006; 4. He et al. In: Hepatitis C Viruses: Genomes and Molecular Biology, 2006; 5. Gao et al. Curr
Opin Virol 2013;3:514; 6. Jazwinski et al. Gastroenterol Hepatol 2011; 7:154-162
5
6
IFN-freie Therapie - Wirkmechanismus

Drug Abbreviation Class
Grazoprevir GZR NS3/4A protease inhibitor
Paritaprevir PTV NS3/4A protease inhibitor
Simeprevir SMV NS3/4A protease inhibitor
Glecaprevir GLE NS3/4A protease inhibitor
Voxilaprevir VOX NS3/4Aprotease inhibitor
Daclatasvir DCV NS5A inhibitor
Elbasvir EBR NS5A inhibitor
Ledipasvir LDV NS5A inhibitor
Ombitasvir OBV NS5A inhibitor
Velpatasvir VEL NS5A inhibitor
Pibrentasvir PIB NS5A inhibitor
Ruzasvir RZR NS5A inhibitor
Dasabuvir DSV NS5B non-nuc pol inhibitor
Sofosbuvir SOF NS5B nuc pol inhibitor

DAA Therapie - Fixdosiskombinationen
Protease Inhibitor
Polymerase Inhibitor
NS5A Inhibitor
Ledipasvir+
Sofosbuvir
(Harvoni®)
Ombitasvir+
Paritaprevir
(Viekirax®)
+
Dasabuvir
(Exviera®)
Elbasvir+
Grazoprevir
(Zepatier®)
Velpatasvir+
Sofosbuvir
(Epclusa®)
SOF/VEL/VOX
(Vosevi®)
Pibrentasvir+
Glecaprevir
(Maviret®)
Interferon-freie Therapie (DAA)
Ausgezeichnete Verträglichkeit !
Kurze Therapiedauer (8-12 Wochen) !
Heilung der HCV Infektion in 95-100% !
Pangenotypische Therapieregime!

Frühling der Hepatologie 2018, Graz
DAA Therapie der Hepatitis C
HCV ist heilbar...
...alle Genotypen
...alle Zirrhosestadien
...trotz Resistenzen
...trotz Niereninsuffizienz
...auch bei HBV/HIV Koinfektion
...auch bei Transplantation
Flemming et al, Hepatology 2016.

Hughes SA, Wedemeyer H, & Harrison PM Lancet 2011
Delta Hepatitis
• Weltweit ca. 30 Mio. Hep. D Infizierte
• HDV braucht HBV zur Replikation
• Superinfektion bei HBV Infektion oder simulante HBV/HDV Infektion
Jede Hepatitis B zumindest 1x auf Delta testen!

Virale Hepatitiden – Hepatitis D
• Hepatitis D Virus (HDV): RNA Virus
• Übertragung : – Wie Hepatitis B
– Blut-Blut, sexuelle Übertragung
• Lebermanifestation – Akute Hepatitis (Leberversagen möglich)
– Chronische Hepatitis (rasche Progression!!)
• Therapie : – Derzeit Peg-Interferon, Myrcludex ?
– Impfung gegen Hep. B!

Kupferschmidt K Science 2016; 353: 862-863
Hepatitis E Virus (HEV)
Debing Y et al. Update on hepatitis E
virology: Implications for clinical
practice. J Hep 2016
• single strand RNA Virus (27-
34nm)
• 4 (5) HEV Genotypen
– Unterschiedliche globale Verteilung
– GT 3,4 Zoonose

Hepatitis E Übertragung
• HEV Genotyp 1 und 2
– fäkal-oral, person-to-person
– Epidemien durch fäkal-kontaminiertes Trinkwasser oder Speisen
– Bluttransfusionen
– Vertikal auf den Fetus
• HEV Genotyp 3 und 4
– Nahrungsmittel
– Tierkontakte (Schwein, Wild…)
– Bluttransfusionen/Transplant
– Vertikal auf den Fetus

„Hot spots“ in Europe…
1. Thom K, et al. Euro Surveill 2018; 2. Mansuy JM, et al. Hepatology 2016 3. Zaaijer HL. Hepatology 2015 4. Müller B, et al. Transfus Med Hemother 2015, 5. Adlhoch C, et al. J Clin Virol 2016. Lucarelli C, et al. Euro Surveill 2016. Bura M, et al, Int J Infect Dis. 2017, 8. Shrestha AC, et al. Transfusion 2016 9. Hoad VC, et al. Vox Sang 2017; 10. Fearon MA, et al. Transfusion 2017, 11. Zhang L, et al. Transfusion 2017; 12. Matsubayashi K, et al. ISBT Science Series 2011. 14. Stramer SL, et al. Transfusion 2015. Adlhoch et al., J Clin Virol 2016
Häufigste Ursache einer akuten Hepatitis in vielen
europäischen Ländern.

• Akute Hepatitis (meist selbstlimitierend)
– Cholestatische Verlaufsformen möglich1
– Akutes Leberversagen möglich3
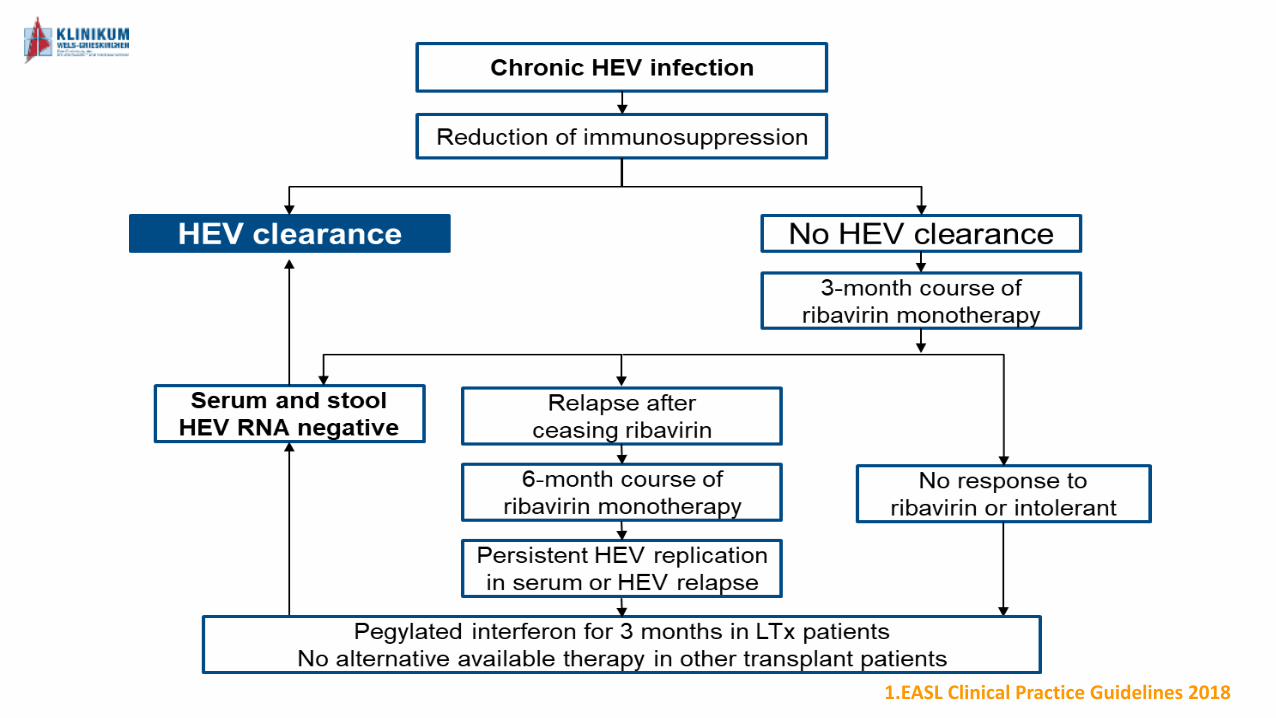
• Chron. Hepatitis bei Immunsuppression
– V.a. Organtransplantatempfänger
– HEV RNA in Serum und Stuhl nachweisbar
– Vorwiegend autochthone GT 3 Infektion
• Extrahepatische Manifestationen
– Neuralgische Schulteramyotrophie
– Guillaine-Barre Syndron
– Renal/hämatologisch…
Hepatitis E Klinische Manifestation
1Chau et al., Am J Gastroenterol 2006, 2Ollier et al., Ann Intern Med, 2009, 3Daltons et al, NEJM 2009

Diagnose der Hepatitis E Infektion
• Inkubationszeit (15-60 Tage)
Bei Immunsuppression ist die Serologie häufig
unzuverlässig (NAT bei Verdacht).

Anti-HEV-IgM (and IgG)and HEV RNA
Positive
Acute hepatitis E
Immunocompetent
Extrahepatic
manifestation?
Immunocompromised
HEV RNA
± serology
Chronic hepatitis E
Elevated liver enzymes
Pre-existing
chronic liver disease?
Acute-on-chronic
liver failure?
Transplant-centre?
Ribavirin?
Positive
HEV-infection
HEV RNA positive
>3 months?
1.EASL Clinical Practice Guidelines 2018
1.EASL Clinical Practice Guidelines 2018

Leberzirrhose

Leberzirrhose & portale Hypertension
Ikterus
Aszites
Spidernävi
Muskelatrophie
Caput Medusae
Komplikationen
- Ösophagusvarizenblutung
- Aszites/spontan bakt. Peritonitis
- Hepatische Enzephalopathie
- Zirkulatorische Dysfunktion
- Hepatorenales Syndrom
- Hepatopulmonales Syndrom

Budd-Chiari Syndrome
Vascular Liver Diseases
Autoimmune Hepatitis (AIH)Alcoholic Liver Disease
Non-alcoholic steatohepatitis (NASH)
Viral Hepatitis C & B/D, E
Hemochromatosis
Wilson Disease
Drug-Induced Liver Injury (DILI)
A1-Antirypsin Deficiency (A1AD)
Portosinusoidal Disease
Primary Biliary Cholangitis (PBC)
Primary Slerocsing Cholangitis (PSC)
Autoimmune Hepatitis (AIH)
Primary Biliary Cholangitis (PBC)
IgG4-associated Disease
Primary Sclerosing Cholangitis (PSC)
Chronic liver disease
Liver Cirrhosis

Klinik bei fortgeschrittener Zirrhose• Aszites?• Beinödeme?• (Skleren) Ikterus?• Blutungen?• Verwirrtheit? HE?• Leberhautzeichen
• Spidernävi• Lacklippen• Palmarerythem
Diagnose der Leberzirrhose
Labor• Synthese: Albumin, PTZ/INR
CHE• Exkretion: Bilirubin• Hepatische Enzephalopathie:
Ammoniak• Portale Hypertension:
Thrombozyten
• Nicht-Invasive Fibrosescores• APRI, FIB-4

• US
• CT
Diagnose der Leberzirrhose
Bildgebung
• Oberfläche?, Aszites?• Raumforderungen?
Histologie
• Fibroseklassifikation• Ludwig F1-F4 (Zirrhose)
Transiente Elastographie

• Child-Pugh Score
• MELD Score (Mayo End Stage Liver Disease): 6-40
10 {0.957 Ln(Krea) + 0.378 Ln(Bili) + 1.12 Ln(INR) + 0.643}
Parameter 1 P. 2 P. 3 P.
Aszites - gering ausgeprägt
Enzephalopathie keine I-II III-IV
Serum-Bilirubin (mg/dL) <2 2-3 >3
PTZ (%) >70 30-70 <30
Serum Albumin (mg/dL) >35 28-35 <28
Child Pugh A: 5-6 B: 7-9, C: 10-15
Prognoseabschätzung: Scores
Schuppan et al., Lancet 2008

Garcia-Tsao (2010, Hepatology), D’Amico (2006, JHEP)
4 Baveno Stadien der
Portalen HypertensionZirrhose Progression (HVPG)
Kompensiert vs. Dekopmensiert
Progression der Zirrhose - Zirrhosestadien

Portale Hypertension

Intrahepatischer
Widerstand
HVPG >10mmHg
Varizen
Splenomegalie &
Thrombopenie
Aszites
HVPG >12mmHg
Varizenblutung
HVPG >16mmHg
Refraktärer Aszites
HVPG >20mmHg
“High-Risk”
Blutung

Diagnosis of Cirrhosis advanced chronic liver disease (TE>15kPa)
Elastographyavailable
TE <15 kPa +PLT >150 G/L
No ScreeningEndoscopy
Repeat TE and
PLT 1x/Year
TE >15kPa orPLT <150 G/L
Screening Endoscopy
No Varices Low-Risk GOVs<5mm
High-Risk GOVs>5mm, Child C or
red spot signs
Primary Prophylaxis
Repeat Endoscopy:- Compensated: 2Y- Decompensated: 1Y
Betablockersor repeat
Endoscopy after 1Y
Billroth III: Screening für CSPH und Varizen
• Carvedilol 12.5mg 1-0-0 for primary prophylaxis• Use EBL if contraindications or refractory ascites

Varizenblutung

Diagnosis of cirrhosis and (suspected) variceal bleeding
Endoscopic treatment (EVL for EV, Glue for cardiofundal Varices)
• Transfusion if Hb<7g/dL
• Somatostatin 6mg/50mL at 4.2mL/h
• 3G-Cephalosphorin/Betalactam
• Erythromycin 250mg

Early TIPS
<72h
No hemostasis
- 2nd
Endoscopy
- Bleeding Stent (or Balloon)
Diagnosis of cirrhosis and (suspected) variceal bleeding
Endoscopic treatment (EVL for EV, Glue for cardiofundal Varices)
• Transfusion if Hb<7g/dL
• Somatostatin 6mg/50mL at 4.2mL/h
• 3G-Cephalosphorin/Betalactam
• Erythromycin 250mg
Child-B + active
bleeding or
Child C10-13

Escorsell et al (Hepatology 2015)
Ballon Tamponade (Sengstaken) – Danis Stent

Early TIPS
<72h
No hemostasis
Hemostasis achieved
Continue vasoactive
drugs for up to 5d
- 2nd
Endoscopy
- Bleeding Stent (or Balloon)
Early rebleeding
<5days
Secondary
prophylaxis
Diagnosis of cirrhosis and (suspected) variceal bleeding
Endoscopic treatment (EVL for EV, Glue for cardiofundal Varices)
• Transfusion if Hb<7g/dL
• Somatostatin 6mg/50mL at 4.2mL/h
• 3G-Cephalosphorin/Betalactam
• Erythromycin 250mg
Child-B + active
bleeding or
Child C10-13
Rebleeding or Failure of secondary prophylaxis:
“rescue” or “elective” TIPS

Sekundärprophylaxe:Kombination von β-Blocker + EBL
Bei wiederholter/schwerer Blutung unter β-Blocker + EBL TIPS evaluieren.

Aszites

Diagnosis and Therapy of Ascites
Uncomplicated Cirrhosis Refractory Ascites
Definition
Grade 1: Mild ascites only detectable by ultrasound
Grade 2: Moderate ascites evident by moderate symmetrical distension of abdomen
Grade 3: Large or gross ascites with marked abdominal distension
Ascites that cannot be mobilized or the early recurrence of which cannot be prevented because of a lack of response to sodium restriction and diuretic treatment; impaired urinary sodium excretion (< 80 mmol/24 h); spot urinary sodium/potassium ratio <2.5
Treatment
Sodium restriction and diureticsSpironolactone 100mg 1-0-0 (1-1-0)
Furosemide 20-20-0 (40-40-0)
Paracentesis, sodium restriction and diuretics
Paracentesis, TIPS, transplantation
Avoid
NSAIDs, angiotensin converting encyme inhibitors, angiotensin receptor blockers, aminoglycosides
NSAIDs, angiotensin converting encyme inhibitors, angiotensin receptor blockers, aminoglycosides, carvedilol, propranolol with caution
Aszites: Graduierung und Therapie

• MA, 7 randomisierte Studien, 305 Patienten
Transplant-freies Überleben HE-Episode
Salerno et al., Gastroenterology 2007; 133: 825
Refraktärer Aszites – TIPS vs. Parezentese
Salerno et al., Gastroenterology 2007; 133: 825

Does This Patient Have Bacterial Peritonitis or Portal Hypertension? How Do I Perform a Paracentesis and Analyze the Results? JAMA, March 12, 2008—Vol 299, No.
10
(diagnostische) Aszitespunktion !!
• Leukozytenzahl (>500/µl), Neutrophilenzahl (>250/µl)
• Kulturen (Ascitic fluid and blood cultures)
• Antibiotische Therapie! (gram-negative coverage (e.g. aminopenicilline/β-lactamase inhibitor, 3rd generation cephalosporin, or quinolone)
• Albuminsubstitution
• Verlaufspunktion
Spontan bakterielle Peritonitis

Hepatorenal Syndrome (Billroth III Konsens)
ICA-AKI Stage 2/3Increase in sCrea >2x
(even if <ULN)
1. Pause Diuretics & nephrotoxic drugs2. Pause NSBB if RR<90 or Na<1303. Renal Ultrasound4. Urinary assessment5. Screening for Infections, paracentesis: check for SBP6. Albumin 1g/kg: 300-500mL 20% HA
Decrease in sCrea after 2 days:Partial Response (decrease in AKI stage)Complete Response (return baseline sCrea
No decrease in sCrea after 2 days:• Continue Albumin 200-300mL 20% HA• Vasoconstrictors:
• Terlipressin 1mg every 6h up to 2mg every 4h (4-12mg/d• Terlipressin 0.2-0.5mg/h, 4mg/40mL: 2-5mL/h• Noradrenaline 5mg/50mL, 2mL-5mL/h
Nonresponse: No decrease in sCrea: Discontinuation after 14daysConsider TIPS in case of severe/refractory ascites (HRS-2, CKD-HRSRRT: as clinically indicated, only in OLTX candidates
48h – 2 days

Zusammenfassung
• Virushepatitis: Große Fortschritte in Diagnostik und Therapie
• HBV: gut kontrollierbar, Reaktivierung!, (an HDV denken!)
• HCV: dauerhaft ausheilbar (Elimination)
• HEV: akute Hepatitis, Immunsuppression
• Leberzirrhose: Diagnose der Ätiologie und Stadium (Scores)
• Portale Hypertension/Komplikationen
• Varizenblutung (prim/sek. Proph., Blutungsmanagement)
• Aszites (SBP, refraktär, TIPS)
• HE, HCC Surveillance, OLT