virginia opioid addiction echo* - vcuhealth.org july 27th presentation.pdf · nanah fofanah, mph,...
TRANSCRIPT
Virginia Opioid Addiction ECHO*
Project ECHO:July 27th
*ECHO: Extension of Community Healthcare Outcomes

Agenda
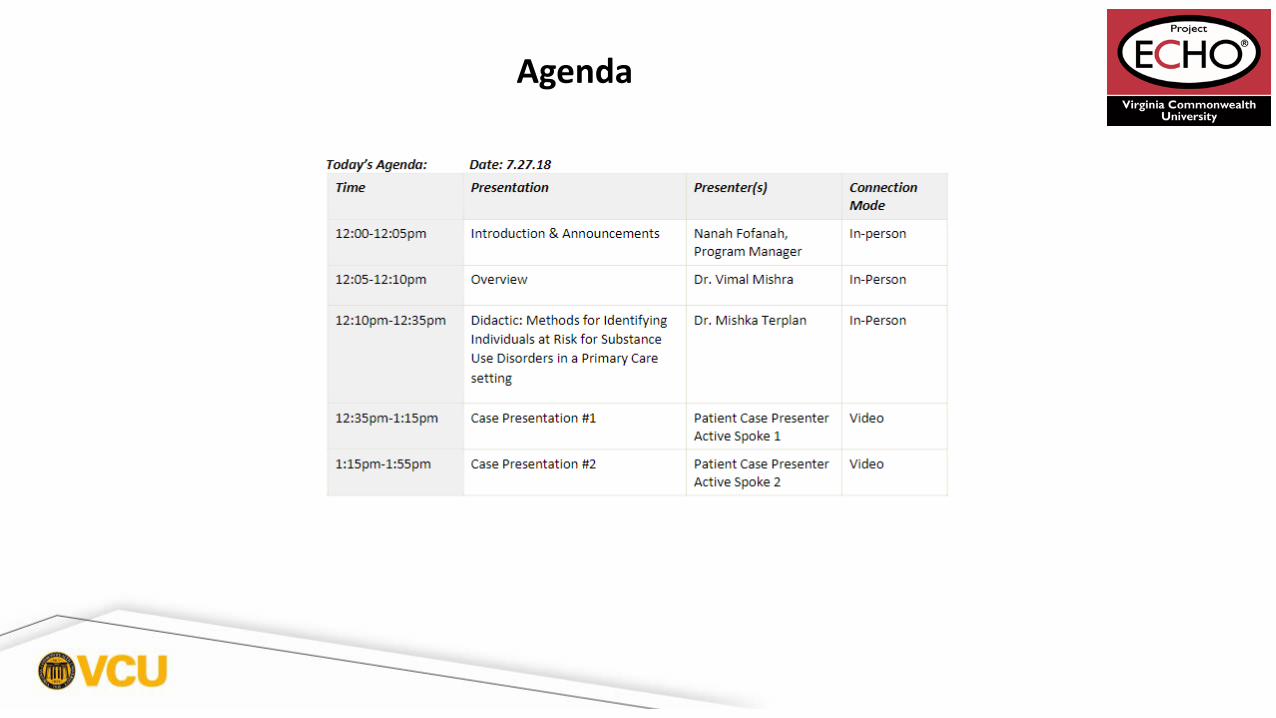
Agenda
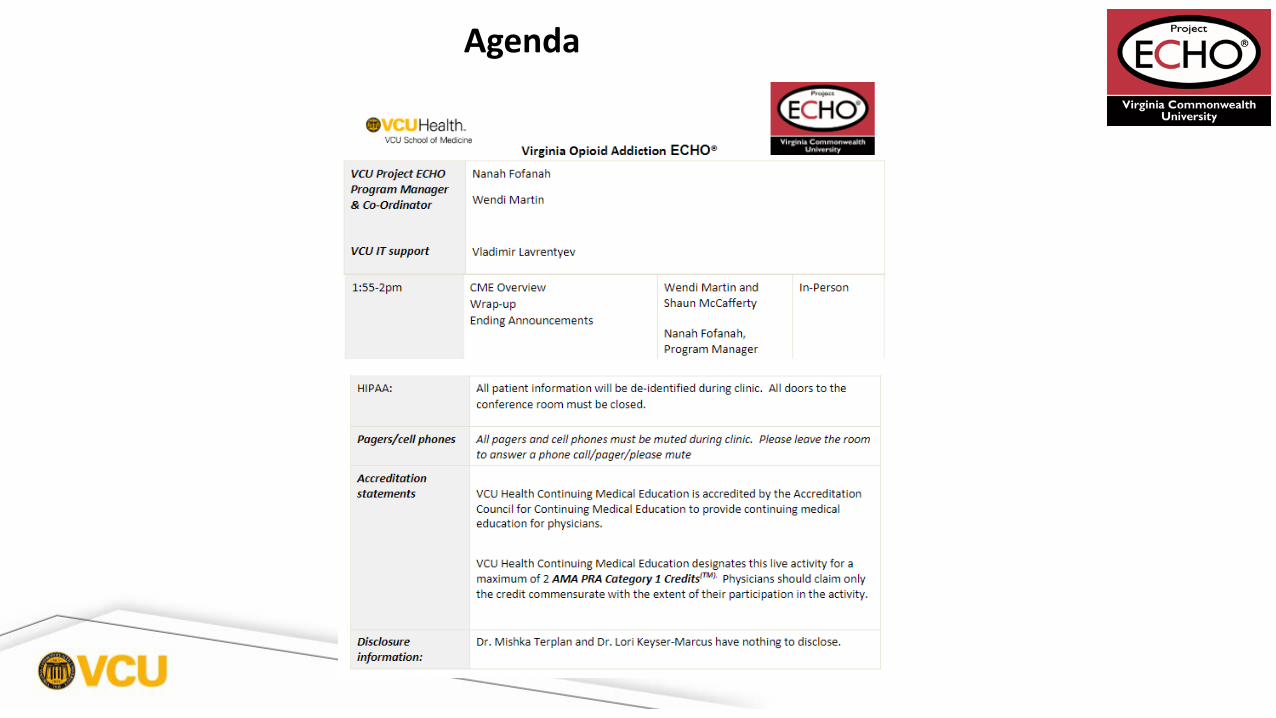
Agenda

VCU Team Clinical Director Mishka Terplan, MD, MPH, FACOG, FASAM
Administrative Medical Director ECHO Hubs and Principal Investigator
Vimal Mishra, MD, MMCi
Clinical Expert
Program Manager
Practice Administrator
IT Support
Lori Keyser-Marcus, PhD
Nanah Fofanah, MPH, CPH
David Collins, MHA
Vladimir Lavrentyev, MBA
Introductions

Fatal drug overdose has been the leading cause of unnatural death in Virginia since 2013
Opioid Epidemic and Virginia
At least 1,420 people died last year due to drug overdose
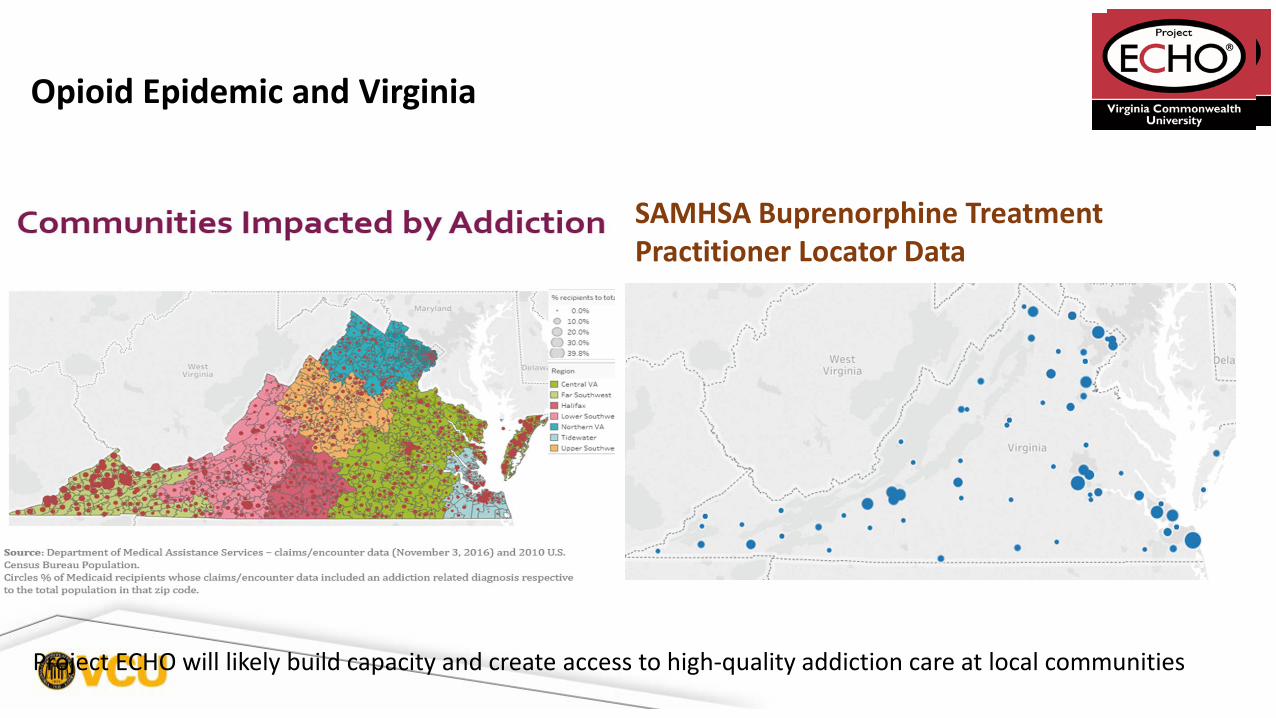
Project ECHO will likely build capacity and create access to high-quality addiction care at local communities
SAMHSA Buprenorphine Treatment Practitioner Locator Data
Opioid Epidemic and Virginia


Statewide Administrator
Academic hub Academic hub Academic hub
Clinical hub will rotate every 12-16 weeksBi-Weekly 2 hour tele-ECHO Clinics
Every tele ECHO clinic includes a 30-minute talk followed by case discussions
Talks will be developed and delivered by inter-professional experts in substance use disorder
https://www.vcuhealth.org/explore-vcu-health/for-medical-professionals/project-echo
Project ECHO Clinical LeadershipClinical Directors Mishka Terplan, MD, MPH, FACOG, FASAM (VCU)
Richard Lawrence Merkel, MD, PhD (UVA)
Cheri W. Hartman, PhD (Virginia Tech Carilion)
Administrative TeamAdministrative Medical Director ECHO Hub and Principal Investigator
Program Manager
Practice Administrator
IT Support
Vimal Mishra, MD, MMCi
Nanah Fofanah, MPH, CPH
David Collins, MHA
Vladimir Lavrentyev, MBA
Benefits to Participating Clinicians
• Free continuing education credit
• Opportunity to present actual patient cases, in a de-identified format, and receive specialty input
• Addiction treatment training, including management of naloxone/ buprenorphine (e.g. Suboxone)
• Access to a virtual learning community for access to treatment guidelines, tools, and patient resources
• Professional interaction with colleagues with similar interest

• Recording: By participating in this clinic you are consenting to be recorded. If you do not wish to be
recorded, please email [email protected]
• Protect Patient Privacy
• Participation and discussion is welcomed
Helpful Reminders
• Rename your ZOOM screen: Please rename your screen with your full name
• All participants are Muted during the call, Please Unmute yourself before speaking. If you have a
question, use the ‘hand-raised’ future in ZOOM or type your question in the Chat box.
• Speak to the Camera, avoid distractions and for ZOOM issues (such as echoing, audio level etc.), use the
chat function to speak with the clinic IT team (Vlad)
Helpful Reminders

What to Expect
I. Overview
II. Introductions
III. Didactic Presentation
IV. Case presentationsI. Case1
I. Case summary II. Clarifying questions III. Recommendations
II. Case 2 I. Case summary II. Clarifying questionsIII. Recommendations
V. Closing and questions
Lets get started!Didactic Presentation

Virginia Opioid Addiction ECHO: Didactic Presentation
Open to all practicing and licensed M.D.s, D.O.s, and Community-based clinicians
Disclosures
Dr. Mishka Terplan and Dr. Lori Keyser-Marcus have no financial conflicts of interest to disclose
There is no commercial or in-kind support for this activity.
Objectives
• Compare and contrast the medications commonly used for treatment of Opioid use disorders including indications, side effects, and regulatory concerns
• Plan strategies to integrate medication for Opioid use disorders into practice

Pharmacotherapy for OUDMedications for the Treatment of OUD
Presenter: Dr. Mishka Terplan
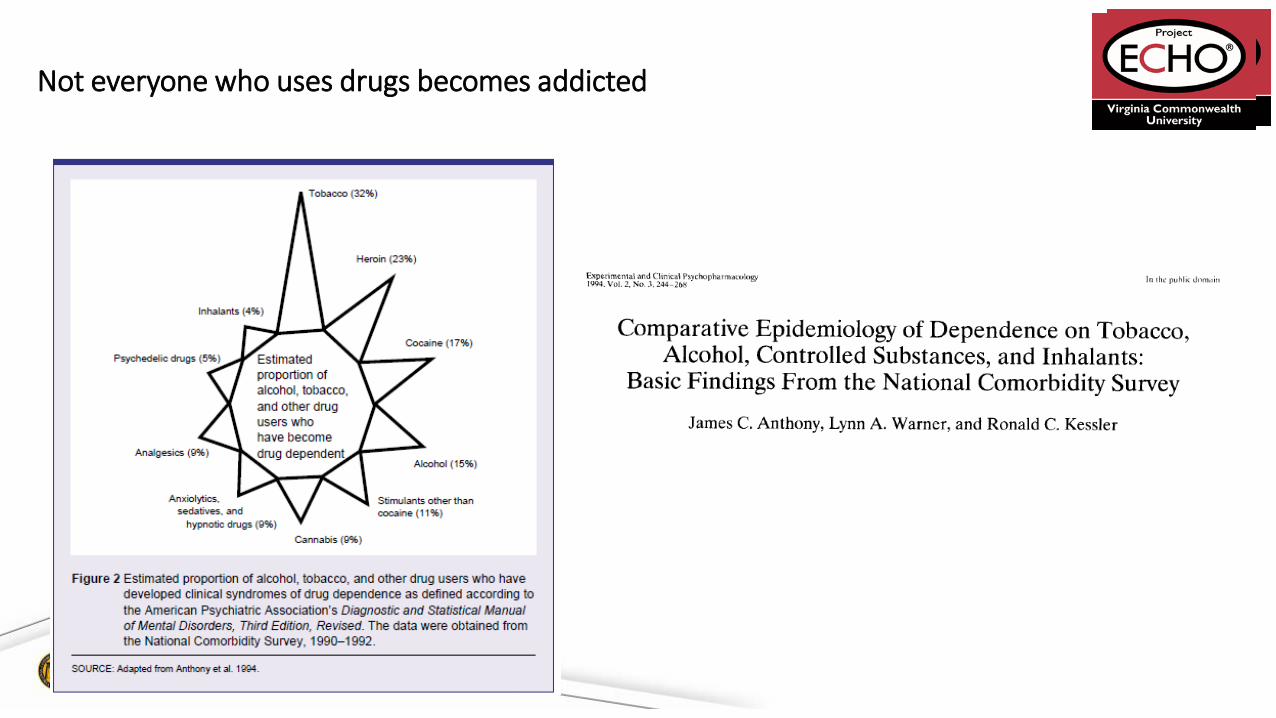
Not everyone who uses drugs becomes addicted

Heroin addiction is a disease – a “metabolic disease” – of the brain with resultant
behaviors of “drug hunger” and drug self-administration, despite negative
consequences to self and others. Heroin addiction in not simply a criminal behavior
or due along to antisocial personality or some other personality disorder

Why do people use opioids?W
ithdr
awal
Nor
mal
Euph
oria
Chronic useAcute use
Tolerance and Physical Dependence
To feel good
To feel better

Maintenance Treatment for Severe Opioid Use DisorderW
ithdr
awal
Nor
mal
Euph
oria
Chronic use Maintenance
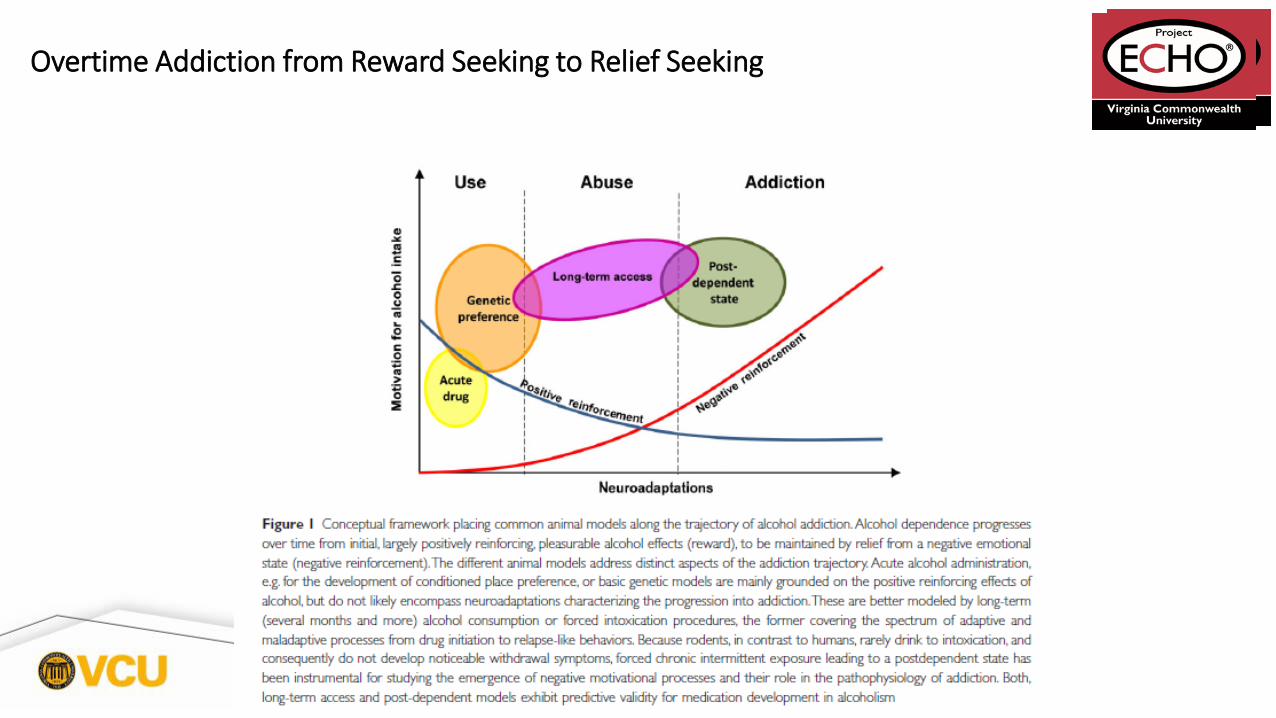
Overtime Addiction from Reward Seeking to Relief Seeking

-10 -9 -8 -7 -6 -5 -40
10
20
30
40
50
60
70
80
90
100
% Efficacy
Log Dose of Opioid
Full Agonist(Methadone)
Partial Agonist(Buprenorphine)
Antagonist (Naloxone)
Opioid Efficacy: Full Agonist, Partial Agonist, Antagonist

How does buprenorphine work?
• High affinity, but low activity at the mu opioid receptor
• Low activity is enough activity to TREAT WITHDRAWAL and REDUCE CRAVINGS
• Low activity results in a CEILING EFFECT• Euphoria is unusual• Overdose occurs only with other drugs of
abuse• Opioid dependent patients FEEL NORMAL• High affinity means it is a BLOCKER, more
active opioids can not stimulate the receptor in presence of buprenorphine
SAMHSA/CSAT TIP #40 page13
Withdrawal relief
Pain relief
Euphoria
Respiratory depression
Death
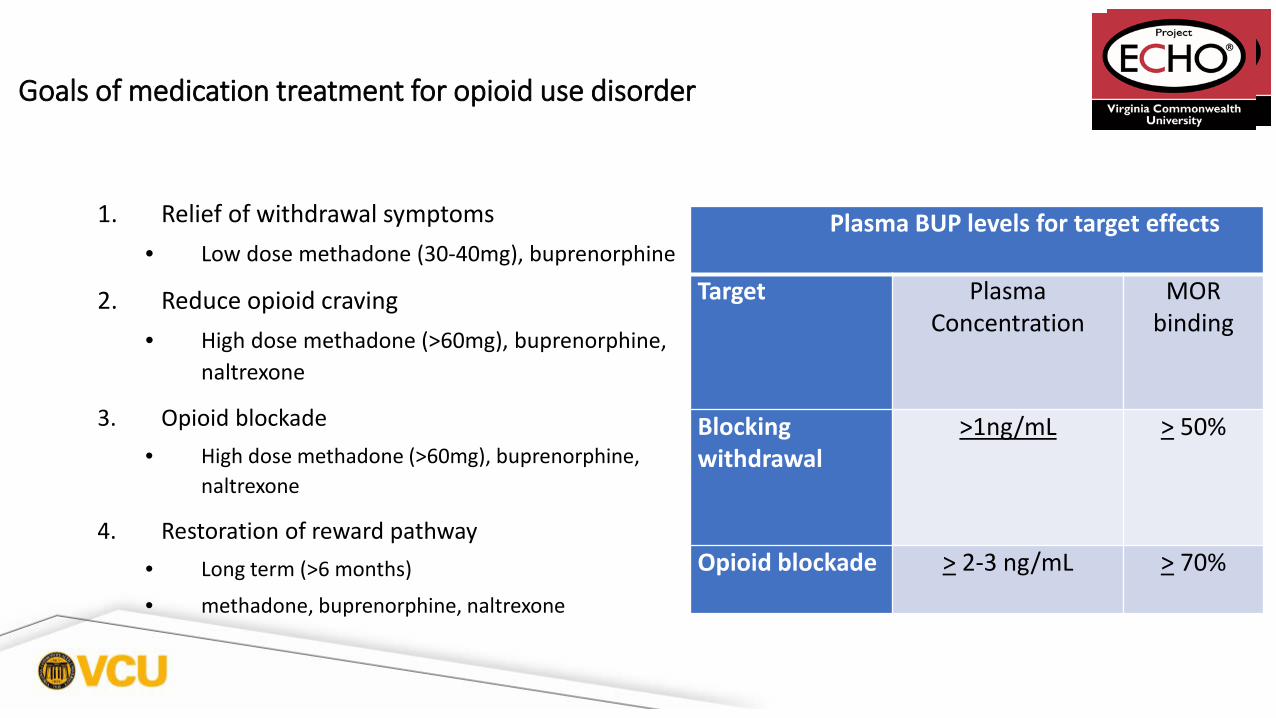
Goals of medication treatment for opioid use disorder
1. Relief of withdrawal symptoms • Low dose methadone (30-40mg), buprenorphine
2. Reduce opioid craving• High dose methadone (>60mg), buprenorphine,
naltrexone
3. Opioid blockade• High dose methadone (>60mg), buprenorphine,
naltrexone
4. Restoration of reward pathway• Long term (>6 months)
• methadone, buprenorphine, naltrexone
Plasma BUP levels for target effects
Target Plasma Concentration
MOR binding
Blocking withdrawal
>1ng/mL > 50%
Opioid blockade > 2-3 ng/mL > 70%
How do buprenorphine + naloxone work?
• Buprenorphine has good sublingual and IV bioavailabilty but poor GI
bioavailability
• Naloxone (Narcan) has good IV bioavailabilty, but poor GI and sublingual
bioavailability
• The combination results in decreased abuse and diversion for IV use
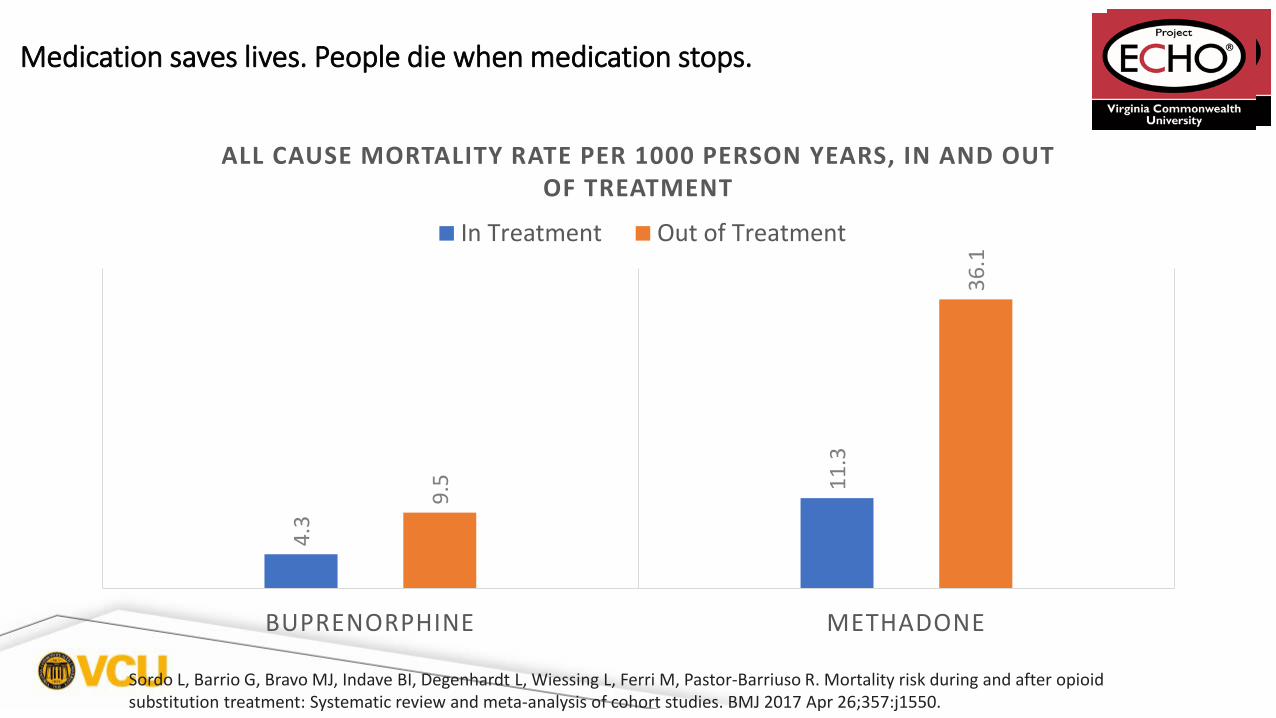
Medication saves lives. People die when medication stops.
4.3
11.3
9.5
36.1
BUPRENORPHINE METHADONE
ALL CAUSE MORTALITY RATE PER 1000 PERSON YEARS, IN AND OUT OF TREATMENT
In Treatment Out of Treatment
Sordo L, Barrio G, Bravo MJ, Indave BI, Degenhardt L, Wiessing L, Ferri M, Pastor-Barriuso R. Mortality risk during and after opioid substitution treatment: Systematic review and meta-analysis of cohort studies. BMJ 2017 Apr 26;357:j1550.
Deaths per 100-person-years

• Pure opioid antagonist • Injectable naltrexone (Vivitrol®)
• Monthly IM injection• FDA approved 2010• Patients must be opioid free for a minimum
of 7-10 days before treatment • Oral naltrexone
• Well tolerated, safe• Duration of action 24-48 hours• FDA approved 1984• 2008 Cochrane Review
• No clear benefit in treatment retention or relapse at follow up over placebo
• Physicians > 80% abstinence at 18 months
Naltrexone
Outcomes NTX placebo
Trial completion 53% 38%
Abstinence at 24 weeks 90% 35%
Change in craving score -10.1 0.7
Krupitsky E, et al. Lancet, 2011

Opioid Detox Outcomes
• Low rate of retention in treatment
• High rates of relapse post treatment
< 50% abstinent at 6 months
< 15% abstinent at 12 months
Increased rates of overdose due to decreased tolerance
O’Connor PG JAMA 2005Mattick RP, Hall WD. Lancet 1996Stimmel B et al. JAMA 1977
So, how long should maintenance treatment last?Long enough

Matching Patients to Pharmacotherapy
• The choice between methadone, buprenorphine or naltrexone depends upon:
• Patient preference - Past experience
• Access to treatment setting
• Ease of withdrawal
• Risk of overdose
• Care = Evidence-Based and Person-Centered

New Formulations
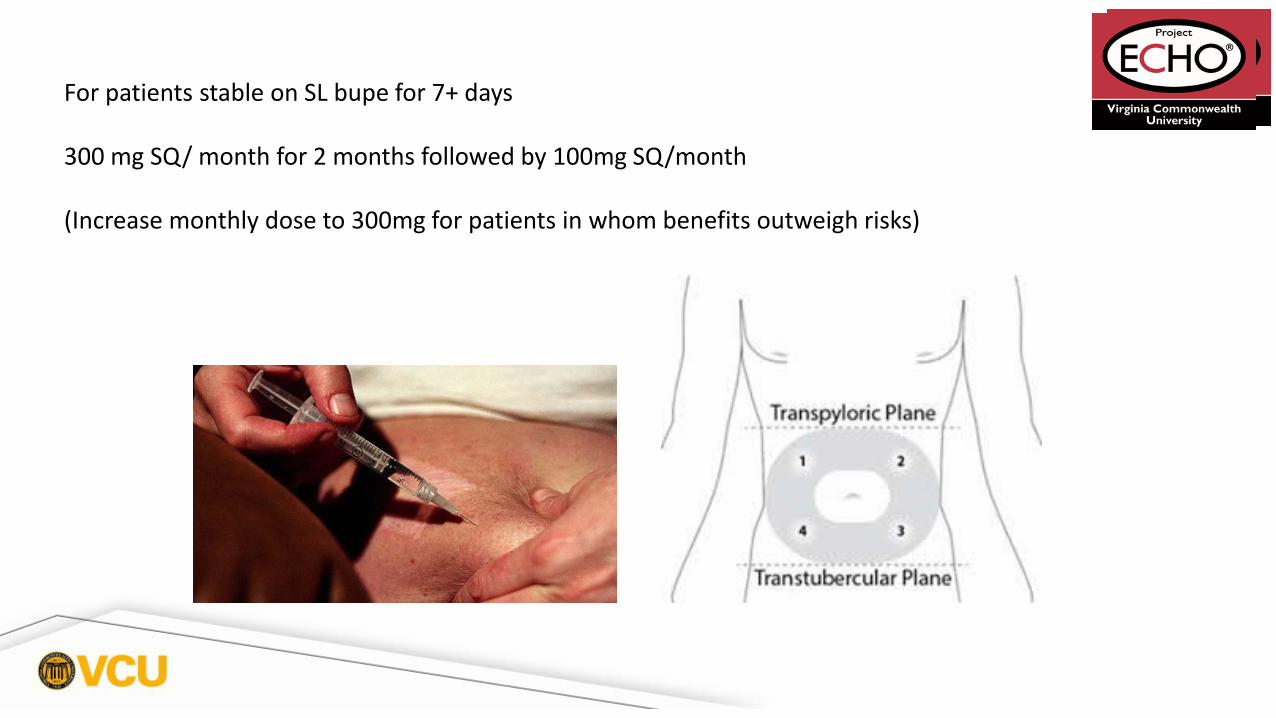
For patients stable on SL bupe for 7+ days
300 mg SQ/ month for 2 months followed by 100mg SQ/month
(Increase monthly dose to 300mg for patients in whom benefits outweigh risks)

SQ Bupe Blockade
Positron Emission Tomography
(PET) study with SUBLOCADE in 2
subjects (one subject receiving 200
mg SC injections and one subject
receiving 300 mg SC injections):
75 to 92% occupancy of the mu-
opioid receptors in the brain was
maintained for 28 days following
the last dose under steady-state
conditions.
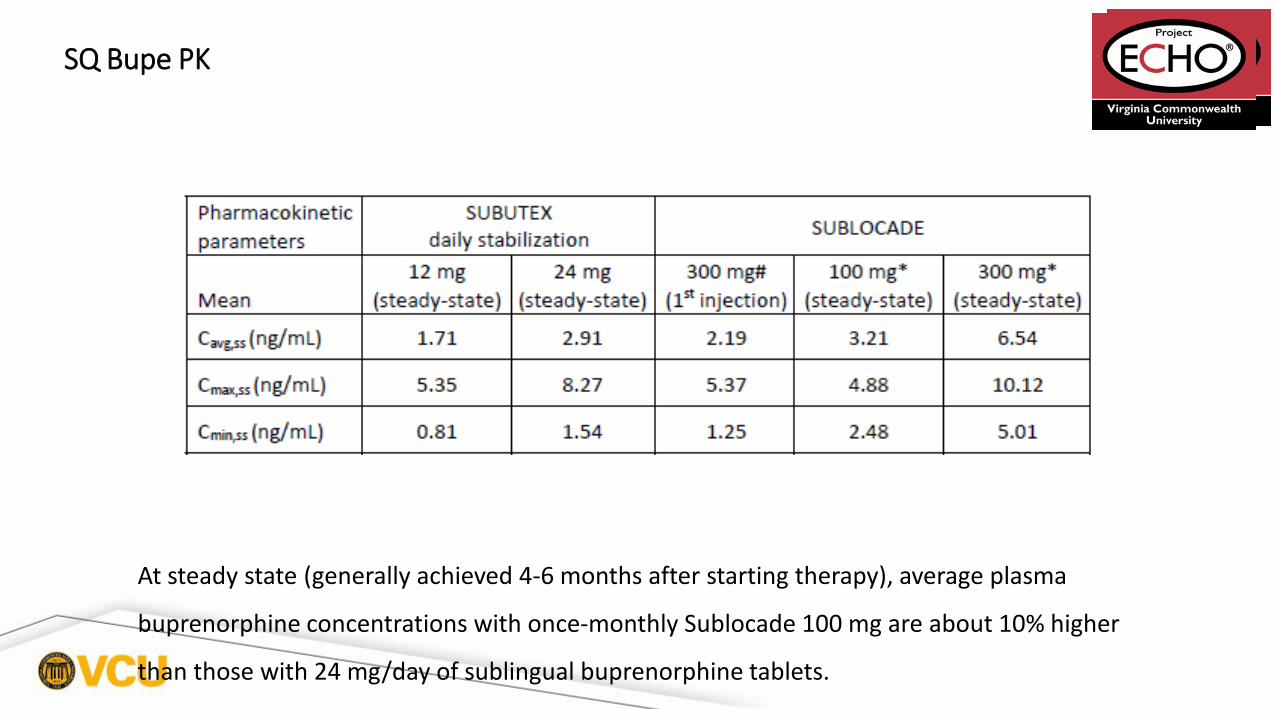
SQ Bupe PK
At steady state (generally achieved 4-6 months after starting therapy), average plasma
buprenorphine concentrations with once-monthly Sublocade 100 mg are about 10% higher
than those with 24 mg/day of sublingual buprenorphine tablets.

Efficacy

Cost

Diversion

Relative Risks/Strengths Diverted Opioids
Relative Risks/Strengths Diverted Opioids
OxyContin
Buprenorphine
Methadone
Questions ?

Reference
Mattick RP, Breen C, Kimber J, Davoli M.,Buprenorphine maintenance versus placebo ormethadonemaintenance for opioid dependence.Cochrane Database of Systematic Reviews 2014, Issue 2. Art. No.: CD002207.
DOI: 10.1002/14651858.CD002207.pub4.

Case #1
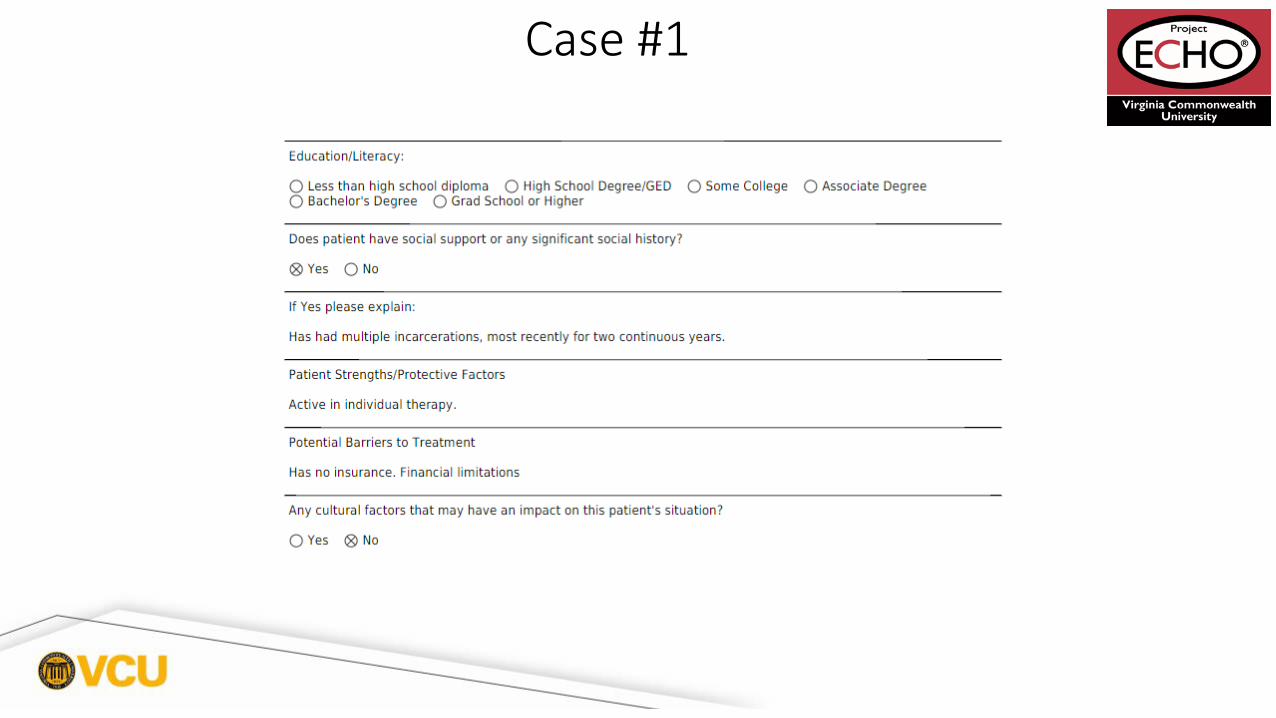
Case #1

Case #1
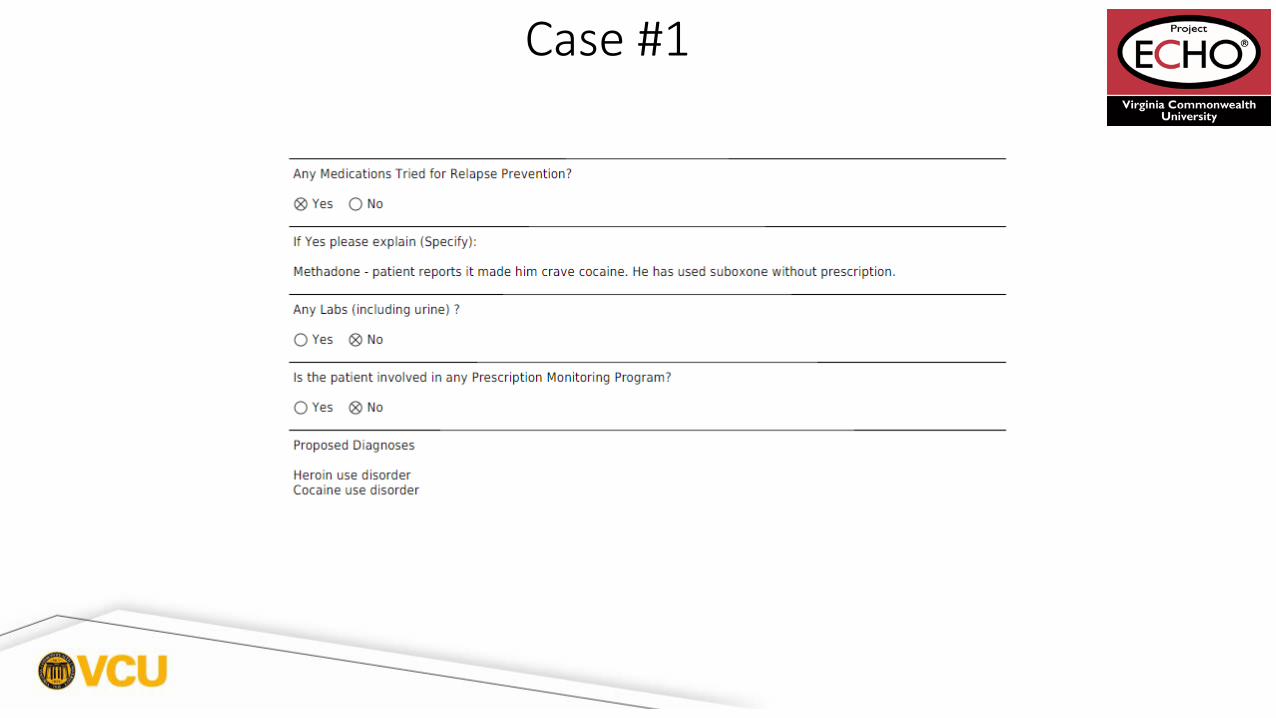
Case #1

Case #1
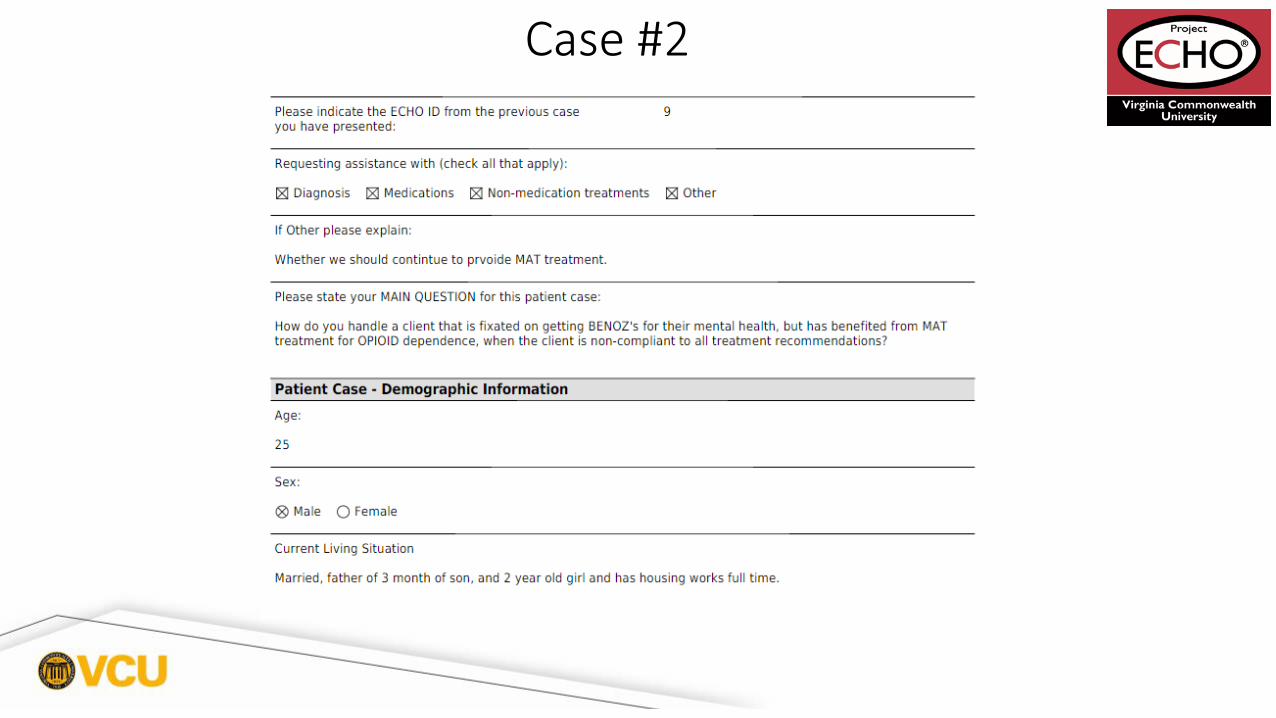
Case #2

Case #2

Case #2
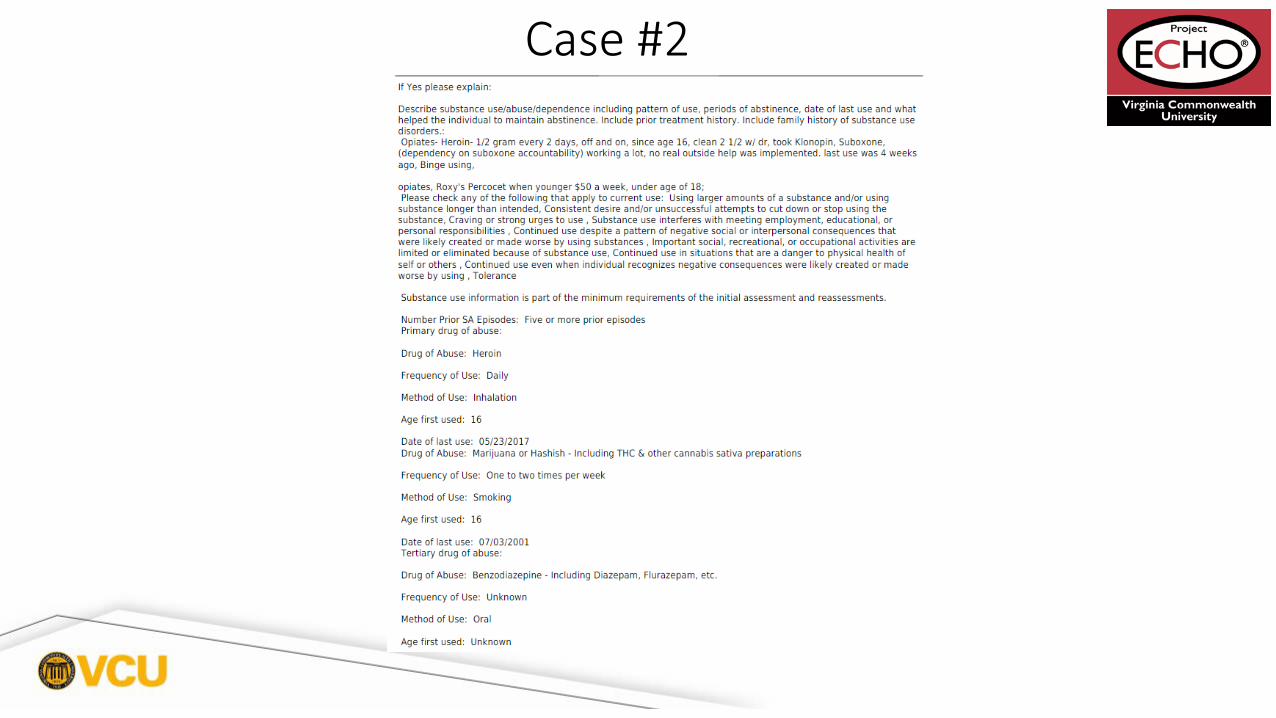
Case #2

Case #2
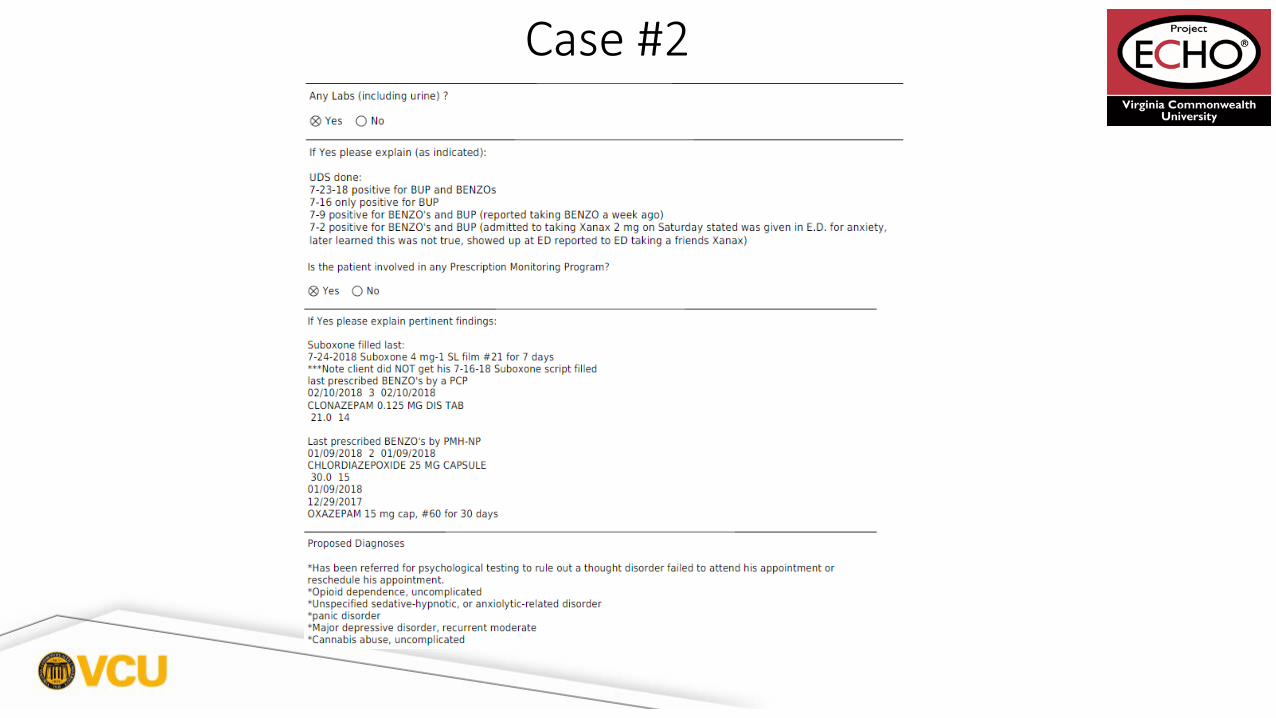
Case #2
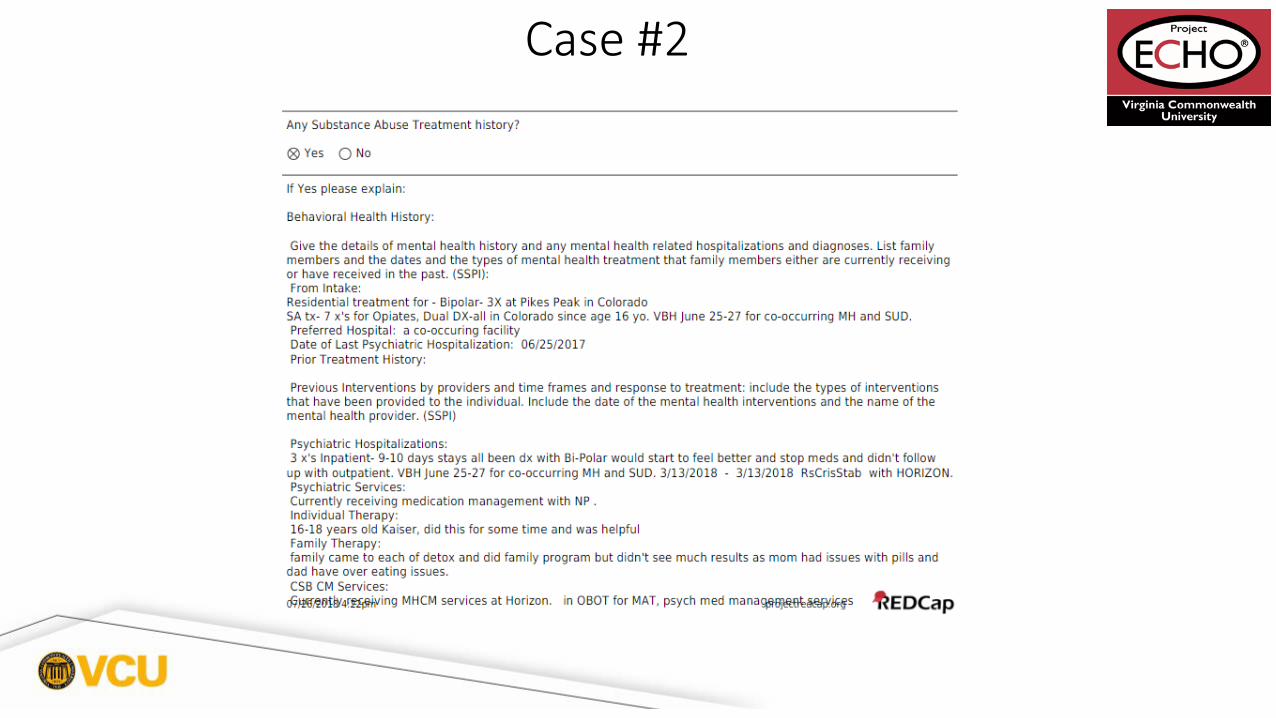
Case #2
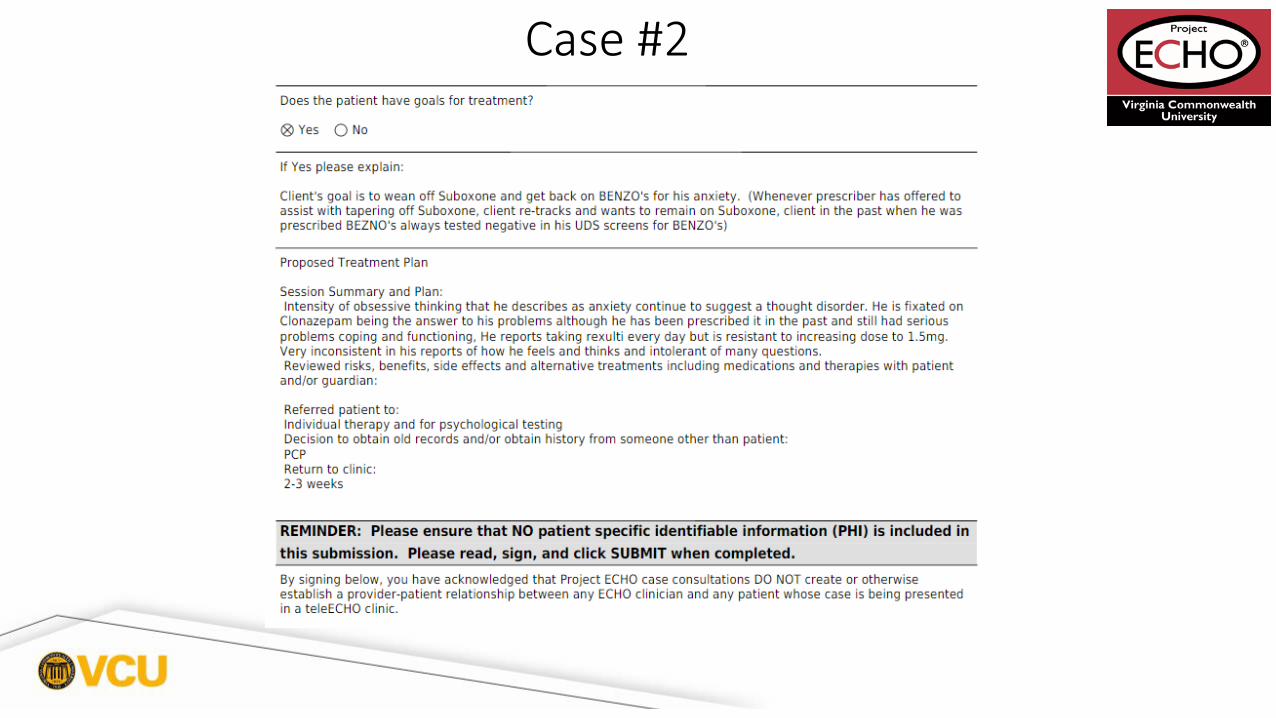
Case #2

Scheduled TeleECHO Clinics
Bi-Weekly Fridays 12-2pm
1. May 18: Introduction to Opioid Use Disorder2. June 1: Harm Reduction of Opioids3. June 15: Counselling and Other Support for Treatment of Opioid Use Disorders
4. June 29: Introduction to Motivational Interviewing5. July 13: Identifying Addiction in Primary Care6. July 27: Medications for Treatment of Opioid Use Disorders

How to Access Your Evaluation and Claim Your CME
Shaun McCafferty
Step 1 - Go to https://vcu.cloud-cme.com/aph.aspx and click “Sign In” on the top left
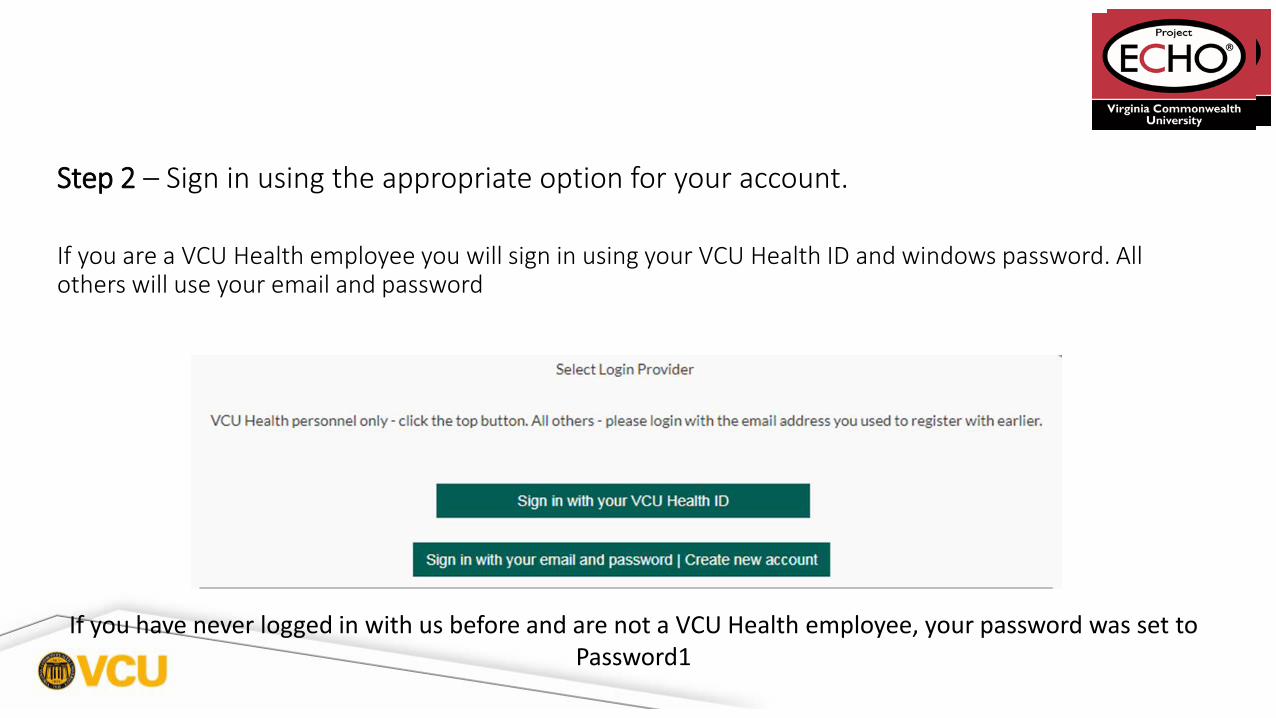
Step 2 – Sign in using the appropriate option for your account.
If you are a VCU Health employee you will sign in using your VCU Health ID and windows password. All others will use your email and password
If you have never logged in with us before and are not a VCU Health employee, your password was set to Password1
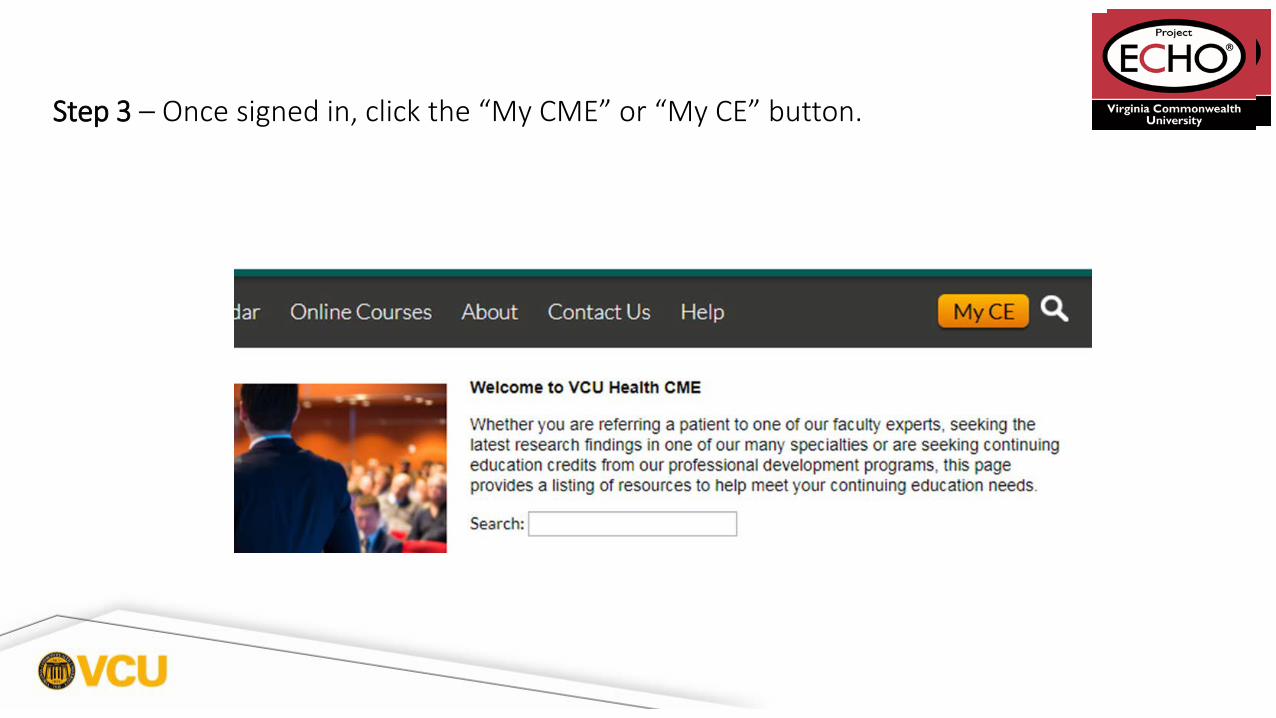
Step 3 – Once signed in, click the “My CME” or “My CE” button.
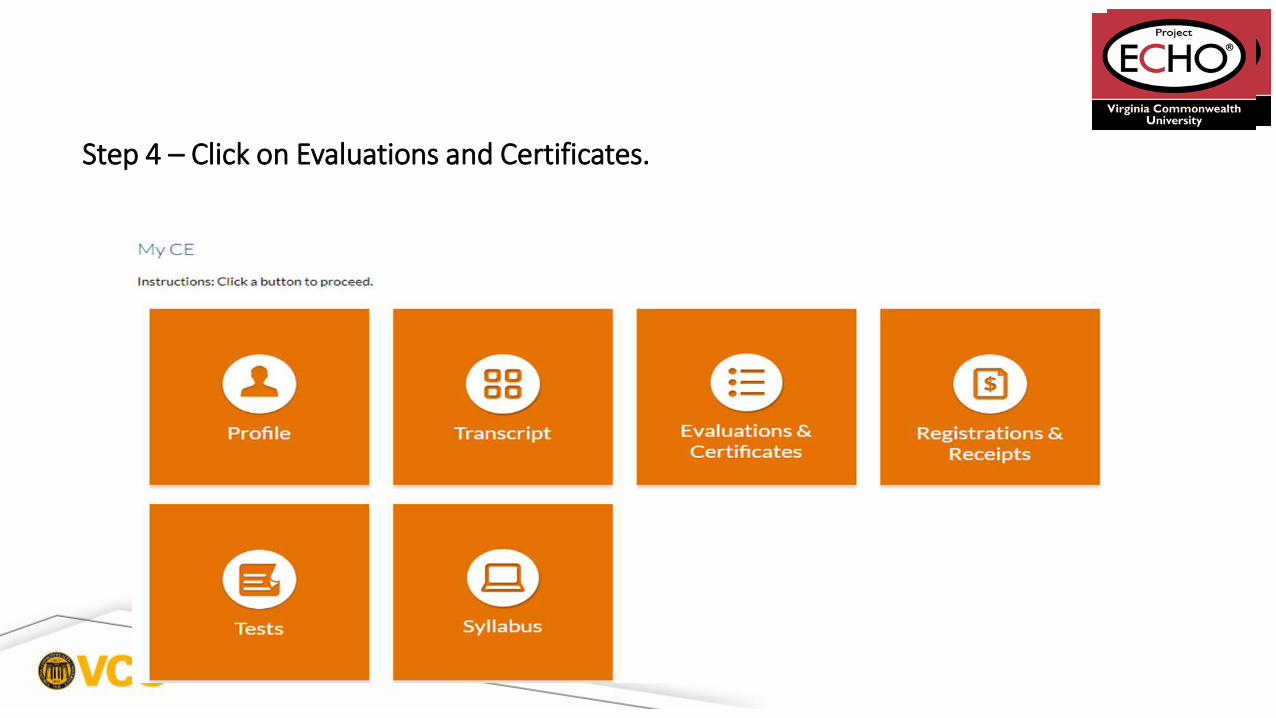
Step 4 – Click on Evaluations and Certificates.

• Evaluations and Certificates – This option allows you to view evaluations that need to be completed for existing activities you have attended and also allows you to view, print or email certificates for activities you have already completed an evaluation for in CloudCME. This is where you will claim credit, fill out evaluations, and download your certificates.
Please contact VCU Health CME directly with any problems or questions at (804) 828-3640 or [email protected]
Scheduled TeleECHO Clinics
Bi-Weekly Fridays 12-2pm
1. May 18: Introduction to Opioid Use Disorder2. June 1: Harm Reduction of Opioids3. June 15: Counselling and Other Support for Treatment of Opioid Use Disorders
4. June 29: Introduction to Motivational Interviewing5. July 13: Identifying Addiction in Primary Care6. July 27: Medications for Treatment of Opioid Use Disorders

THANK YOU!