viral-antibody detection by a more sensitive complement-fixation reaction
TRANSCRIPT
754
an increase of the bone isozyme, substantiated by heatinactivation, was also present.
It is well known that intestinal A.P. can be demonstratedin the serum of normal fasting individuals (usually personsof blood-group 0 and B who are secretors).1 With our
techniques we found a frequency of 48% in normal sub-jects, but never was the percentage of this fraction higherthan 20% of total activity. In a reference group of 100
patients with chronic renal failure with different degreesof diminished glomerular filtration, but not necessitatingmaintenance hxmodialysis, the isozyme pattern of A.P.showed an intestinal fraction at a level and a percentageas found in normals, except in 2 cases.The possibility that the observed increase of intestinal
A.P. in patients on maintenance hxmodialysis was due toeating 2 can be excluded in our series. Androgen hormonetherapy is commonly used in this type of patients, andcould be the cause of an increased intestinal A.P.3 However,we could not induce the A.P. increase by administration ofandrogen hormone in patients not presenting this isozyme,nor could we see any change in patients with this serum-A.P. isozyme upon discontinuation of the drug. Therefore,we do not have a definite explanation for these observations.However, in view of the evidence that Ca-dependentA.T.p.-ase and A.P. localised in the brush border of theintestinal epithelium are identical 4 and are involved in theentry of calcium in the cell,5,6 we suggest that there issome relation to the development of secondary hyper-parathyroidism.Department of Nephrology and of
Clinical Chemistry,University Hospital,9000 Gent, Belgium.
M. E. DE BROEV. BOSTEELS*R. J. WIEME.
1. Posen, S., Neale, F. C., Birkens, D. J. J. clin. Path. 1967, 48, 81.2. Langman, M. J. S., Leuthold, E., Robson, E. B., Harris, J., Luffman,
J. E., Harris, H. Nature, 1966, 212, 41.3. Fishman, W. H., Ghosh, N. K. Adv. clin. Chem. 1967, 10, 255.4. Haussler, M. R., Nagode, L. A., Rasmussen, H. Nature, 1970,
228 1199.5. Kodicek, E. Lancet, 1974, i, 325.6. Coburn, J. W., Hartenbower, D. L., Massry, S. G. Kidney Intern.
1973, 4, 96.* Department of Nephrology, Kliniek Maria Voorzienigheid, 8500
Kortrijk, Belgium.
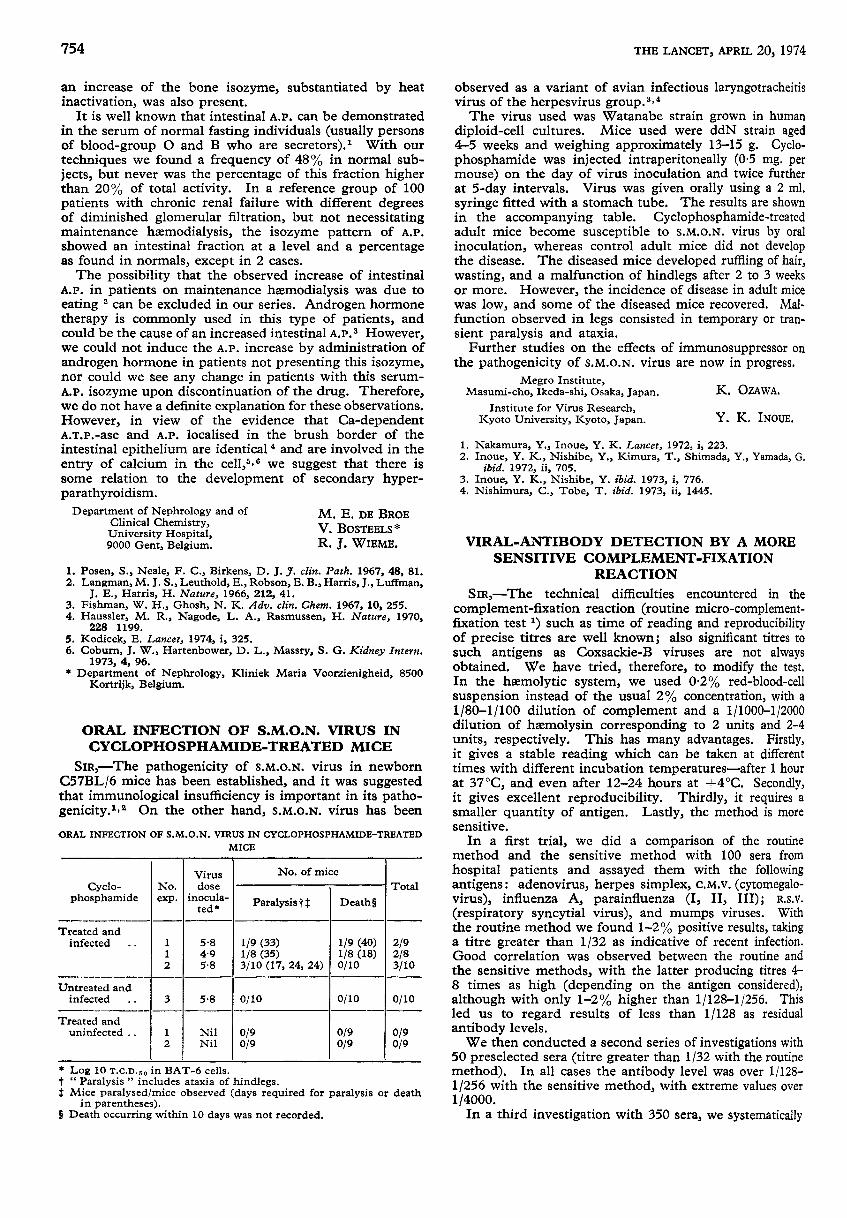
ORAL INFECTION OF S.M.O.N. VIRUS INCYCLOPHOSPHAMIDE-TREATED MICE
SiR,—The pathogenicity of S.M.O.N. virus in newbornC57BL/6 mice has been established, and it was suggestedthat immunological insufficiency is important in its patho-genicity. 2,2 On the other hand, s.M.o.N. virus has been
ORAL INFECTION OF S.M.O.N. VIRUS IN CYCLOPHOSPHAMIDE-TREATED
MICE
* Log 10 2.c.n.bo in BAT-6 cells.t " Paralysis " includes ataxia of hindlegs.t Mice paralysed/mice observed (days required for paralysis or death
in parentheses).§ Death occurring within 10 days was not recorded.
observed as a variant of avian infectious laryngotracheitisvirus of the herpesvirus group.3,4The virus used was Watanabe strain grown in human
diploid-cell cultures. Mice used were ddN strain aged4-5 weeks and weighing approximately 13-15 g. Cyclo-phosphamide was injected intraperitoneally (0-5 mg. permouse) on the day of virus inoculation and twice furtherat 5-day intervals. Virus was given orally using a 2 ml.syringe fitted with a stomach tube. The results are shownin the accompanying table. Cyclophosphamide-treatedadult mice become susceptible to S.M.O.N. virus by oralinoculation, whereas control adult mice did not developthe disease. The diseased mice developed ruffling of hair,wasting, and a malfunction of hindlegs after 2 to 3 weeksor more. However, the incidence of disease in adult micewas low, and some of the diseased mice recovered. Mal-function observed in legs consisted in temporary or tran-sient paralysis and ataxia.
Further studies on the effects of immunosuppressor onthe pathogenicity of S.M.O.N. virus are now in progress.
Megro Institute,Masumi-cho, Ikeda-shi, Osaka, Japan. K. OZAWA.
Institute for Virus Research,Kyoto University, Kyoto, Japan. Y. K. INOUE.
1. Nakamura, Y., Inoue, Y. K. Lancet, 1972, i, 223.2. Inoue, Y. K., Nishibe, Y., Kimura, T., Shimada, Y., Yamada, G.
ibid. 1972, ii, 705.3. Inoue, Y. K., Nishibe, Y. ibid. 1973, i, 776.4. Nishimura, C., Tobe, T. ibid. 1973, ii, 1445.
VIRAL-ANTIBODY DETECTION BY A MORESENSITIVE COMPLEMENT-FIXATION
REACTION
SIR,-The technical difficulties encountered in thecomplement-fixation reaction (routine micro-complement-fixation test 1) such as time of reading and reproducibilityof precise titres are well known; also significant titres tosuch antigens as Coxsackie-B viruses are not alwaysobtained. We have tried, therefore, to modify the test.
In the hasmolytic system, we used 0-2% red-blood-cellsuspension instead of the usual 2% concentration, with a1/80-1/100 dilution of complement and a 1/1000-1/2000dilution of haemolysin corresponding to 2 units and 2-4units, respectively. This has many advantages. Firstly,it gives a stable reading which can be taken at differenttimes with different incubation temperatures-after 1 hourat 37°C, and even after 12-24 hours at +4°C. Secondly,it gives excellent reproducibility. Thirdly, it requires asmaller quantity of antigen. Lastly, the method is moresensitive.
In a first trial, we did a comparison of the routinemethod and the sensitive method with 100 sera from
hospital patients and assayed them with the followingantigens: adenovirus, herpes simplex, C.M.v. (cytomegalo-virus), influenza A, parainfluenza (I, II, III); R.S.V.
(respiratory syncytial virus), and mumps viruses. Withthe routine method we found 1-2% positive results, takinga titre greater than 1/32 as indicative of recent infection.Good correlation was observed between the routine andthe sensitive methods, with the latter producing titres 4-8 times as high (depending on the antigen considered),although with only 1-2% higher than 1/128-1/256. Thisled us to regard results of less than 1/128 as residualantibody levels.We then conducted a second series of investigations with
50 preselected sera (titre greater than 1/32 with the routinemethod). In all cases the antibody level was over 1/128-1/256 with the sensitive method, with extreme values over1/4000.
In a third investigation with 350 sera, we systematically
755
tried to detect anti-Coxsackie-B (1-5) antibodies using bothmethods. These antibodies were not consistently measur-able with the routine method; there was a high proportionof heterotopic reactions. This is in agreement with the
findings of Schmidt and Lennette.2 In contrast, 20 pairedsera examined with the sensitive method showed a fourfoldor greater increase in titres, with values in excess of 1/128.We found some heterotopic reactions also, but alwaysthere was an outstanding predominance of one Coxsackie-Btype. We subsequently found out the origins of these sera.They came from patients who had been admitted withmeningitis, encephalitis, rhinopharyngitis, bronchopneu-monia, bronchitis, pericarditis, or myocarditis. For allthese clinical cases no other aetiology was discovered; theywere possibly due to a Coxsackie-B infection.We feel that this sensitive method will permit standard-
isation of the results of complement-fixation reactions invirology, in view of the greater stability of readings. Italso affords the considerable advantage of allowing detectionof antibodies to viruses for which it is difficult to obtain
good antigens-e.g., Coxsackie-B viruses.Department of Microbiology,
Hospital St-Pierre, and G. ZISSIS.
Department of Virology,Institut Pasteur du Brabant,
Brussels, Belgium. G. CLINET.
1. Sever, J. L. J. Immun. 1962, 88, 320.2. Schmidt, H. J., Lennette, E. H. Prog. med. Virol. 1973, 15, 246.
VIRUS ANTIGEN IN VALVULARHEART-DISEASE
SIR,-Viruses can cause myocarditis and pericarditis. 1Coxsackie B 3-5, Coxsackie A, and echoviruses are com-monly implicated in both myocarditis and pericarditis.Poliovirus, influenza virus, and adenovirus have been moreoften associated with myocarditis alone. Others are lessoften involved. Endocarditis due to virus has been demon-strated in animals; Coxsackie virus B4 produced valvulitisin Cynomolgus monkeys 2 and mice,3 and characteristicinclusion bodies of adenovirus have been shown in mice.4These experimental and clinical findings suggest that
viruses, particularly those of Coxsackie group B, may causesome cases of acquired chronic valve disease.5 Despitethese reasoned arguments, substantial proof has been
lacking; valvular endocarditis due to viruses has not beendemonstrated in patients with valve disease. This mayexplain why viruses have not been more widely acceptedas a possible cause of acquired valve disease.
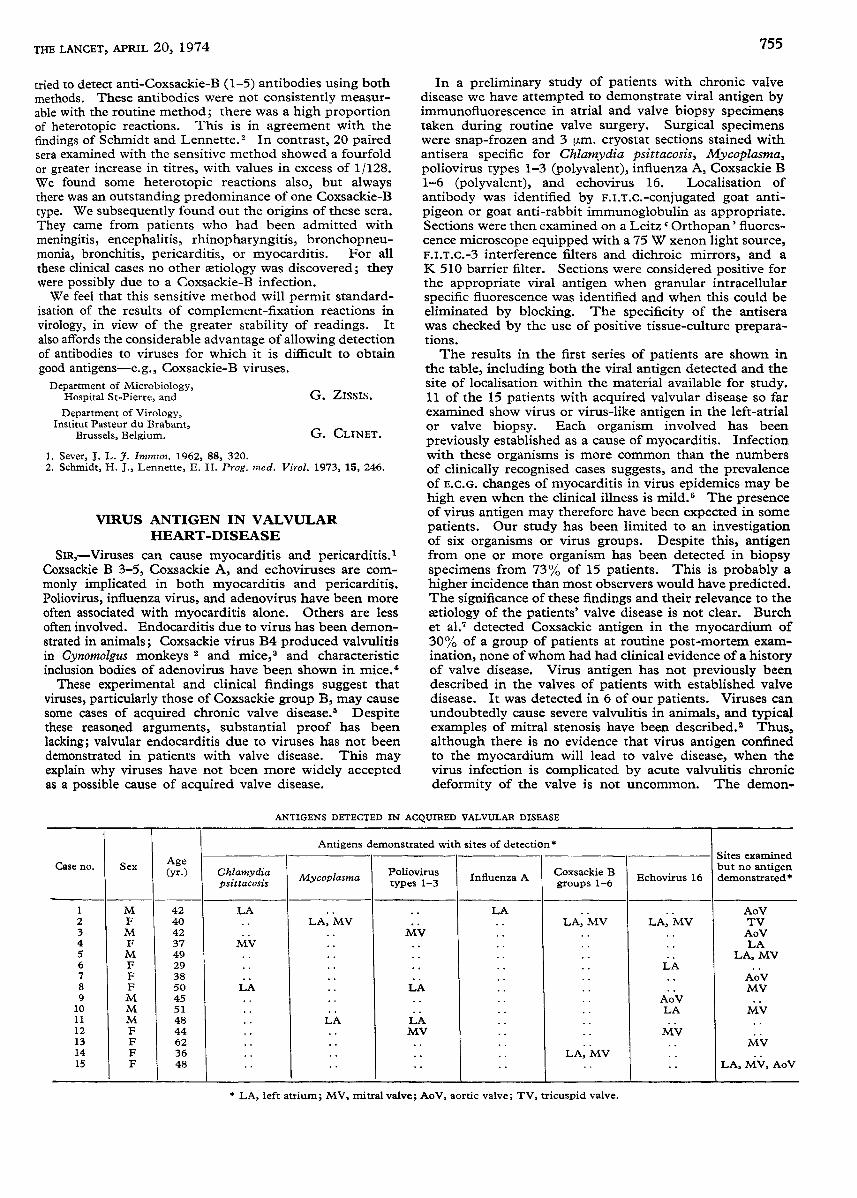
In a preliminary study of patients with chronic valvedisease we have attempted to demonstrate viral antigen byimmunofluorescence in atrial and valve biopsy specimenstaken during routine valve surgery. Surgical specimenswere snap-frozen and 3 .m. cryostat sections stained withantisera specific for Chlamydia psittacosis, Mycoplasma,poliovirus types 1-3 (polyvalent), influenza A, Coxsackie B1-6 (polyvalent), and echovirus 16. Localisation of
antibody was identified by F.l.T.C.-conjugated goat anti-pigeon or goat anti-rabbit immunoglobulin as appropriate.Sections were then examined on a Leitz Orthopan’ fluores-cence microscope equipped with a 75 W xenon light source,F.I.T.C.-3 interference filters and dichroic mirrors, and aK 510 barrier filter. Sections were considered positive forthe appropriate viral antigen when granular intracellularspecific fluorescence was identified and when this could beeliminated by blocking. The specificity of the antiserawas checked by the use of positive tissue-culture prepara-tions.The results in the first series of patients are shown in
the table, including both the viral antigen detected and thesite of localisation within the material available for study.11 of the 15 patients with acquired valvular disease so farexamined show virus or virus-like antigen in the left-atrialor valve biopsy. Each organism involved has been
previously established as a cause of myocarditis. Infectionwith these organisms is more common than the numbersof clinically recognised cases suggests, and the prevalenceof E.C.G. changes of myocarditis in virus epidemics may behigh even when the clinical illness is mild. The presenceof virus antigen may therefore have been expected in somepatients. Our study has been limited to an investigationof six organisms or virus groups. Despite this, antigenfrom one or more organism has been detected in biopsyspecimens from 73% of 15 patients. This is probably ahigher incidence than most observers would have predicted.The significance of these findings and their relevance to theaetiology of the patients’ valve disease is not clear. Burchet al. detected Coxsackie antigen in the myocardium of30% of a group of patients at routine post-mortem exam-ination, none of whom had had clinical evidence of a historyof valve disease. Virus antigen has not previously beendescribed in the valves of patients with established valvedisease. It was detected in 6 of our patients. Viruses can
undoubtedly cause severe valvulitis in animals, and typicalexamples of mitral stenosis have been described.2 2 Thus,although there is no evidence that virus antigen confinedto the myocardium will lead to valve disease, when thevirus infection is complicated by acute valvulitis chronicdeformity of the valve is not uncommon. The demon-
ANTIGENS DETECTED IN ACQUIRED VALVULAR DISEASE
* LA, left atrium; MV, mitral valve; AoV, aortic valve; TV, tricuspid valve.