ehammonscsudpt.files.wordpress.com viewthe diagnostic process of evaluating a spine patient is an...
TRANSCRIPT

MSE Case Analysis
Evan Hammons
4/6/2016
1. Case Description:
Patient, a 23 y/o female student (Caucasian) and is not currently working, presents with left cervical neck pain that travels to her forehead that causes intense migraine headaches. Onset of problem began in November of 2008 when she fell onto her neck in a high school basketball game that resulted in a concussion. She has been seeing a chiropractor for this problem for 4 years (goes every 3-4 months) and claims her visits relieve her pain. The pain/symptoms will last for ~a couple of days at a time before they subside. She has been taking Relpax (migraine) for pain relief. Patient claimed that in the morning her neck feels stiff and semi-painful but loosens up throughout the day. Patient does not have any impairment’s for functional activity/status, self-care and home management. Patient has been to the emergency room three times for migraine headaches that cause intense pain. The patient has had MRI and X-Rays taken of her cervical spine that shows a slight left rotation/shift malalignment of her atlas (C1). Patient lives at home with her family in a two-story home that has multiple sets of stairs, into house and within house, and railings. She rates her overall health as “excellent”. Patient is a non-smoker who has 1-2 drinks of alcohol per week and exercises 2x/week, which includes 30 minutes of cardio and “core strengthening”. Patient’s family medical history includes hypertension (mother and grandmother), stroke (grandmother), type II diabetes mellitus (grandfather) and cancer (grandfather). Patients relevant past medical history include a head injury (2008 incident). Within the past year, patient has had a cough, fever/chills/sweats and headaches. Patient has had surgery in 2005 for a mole removal.
Patients Goals: Decrease neck pain and headaches. Her headaches have increased her stress levels being a student.
Cardiovascular/Pulmonary System: Heart Rate: 60 BPMRespiratory Rate: 14 breaths per minuteBlood Pressure: 117/85 mm Hg
Integumentary System: No abnormalities.
Musculoskeletal System: No ROM, strength impairments, no asymmetries.
Neuromuscular System: No balance, gait, locomotion, transfer/transition impairments.
Communication, Affect, Cognition, Learning Style: No communication, orientation, or emotional or learning impairments. Patient claims her best learning style includes reading, listening and demonstrations.

2. Background and Purpose
The diagnostic process of evaluating a spine patient is an ever-growing field in physical therapy. Complications, such as neurological, in either area of the spine, upper or lower, can arise from spinal abnormalities of the vertebra. Current evaluation techniques focus primarily on spinal alterations.1,7 Specific diagnosing techniques include technologies such as CT, MRI, X-Ray or evaluation done by a professional such as a physical therapist10. The current issues surrounding diagnosis are focused on the mechanism of injury, which could include trauma, biomechanical sources, degenerative disorders, whiplash, etc. With back pain and neck pain, the goal of the diagnosis is to identify the anatomic pain generators.7,20 Another key factor in today’s evaluation techniques include patient history and interview to narrow down the potential causes of the pain as well as any red flags that can be present. All of these factors in the diagnosing process help to distinguish between competing diagnoses or even identify missed diagnoses.
The diagnostic and examination process needs to be fully understood in a clinical setting in order to provide the patient with the best possible health care or even referral if it is not safe to continue intervention. The ultimate goal is to be as precise as possible and walk the fine line between thorough and being too extensive in offering the patient with a timely diagnosis and treatment. The literature states that approximately 10% of back pain is diagnosable with the current technologies2. The literature also suggests that in an overwhelming percentage of the patient population, that the problems they are being seen for have been aggravating them for an extended period of time4. The patients wait to receive health care because at the onset, the symptoms are usually not life altering or limiting. Therefore, when they come for treatment, it is because their quality of life has been decreased due to their symptoms. The goal of healthcare professionals treating spine problems is to get a better understanding of the patient’s lifestyle, what is limiting them in their lives and therefore, return the patient back to their original quality of life before the symptoms arose.
The purpose of this case report is to demonstrate the diagnostic process that ensues in patients who present with spinal signs and symptoms. This includes a patient interview, an examination process and how certain aspects led to confirming or denying spine diagnoses.
3. Clinical Impression #1
The primary problem presented in this patient’s case is cervical neck pain that is causing her intense migraine headaches that is affecting her normal quality of life. Her primary problem began ~8 years ago due to a neck trauma.
Potential Differential Diagnoses: Neck Pain with Headache (JOSPT)4, Hypermobility/Functional Instability (Kisner)13, Postural Syndrome (Mckenzie/Kisner)13, Neck Pain with Movement Coordination Impairments (JOSPT)4, Neck Pain with Radiating Symptoms (JOSPT).4

Additional information would need to be requested that was not obtained in the patient interview or history. This would include questions as, does the pain travel down your upper extremities, do any specific movements make the pain worse, does sitting in a specific posture cause the pain to subside/increase and in relation to the pain within the neck does it ever occur bilaterally or unilaterally?14 Rating the amount of pain the patient is experiencing, describing the feeling of the pain and “point” specifically to where the pain is originating from is important. These questions help to target where the source of the pain is originating. If the pain does travel more distally down her upper extremities, then it would be suspected that it was a nerve issue rather than a muscular problem. The questions regarding any specific movements or postures that make the pain worse or better would then begin to differentiate between a posture syndrome, hyper-mobility or movement coordination problem. The pain questions will help to further understand the type of tissue being involved and how severe the tissue abnormality is.
4. Examination
(Table 1) Neuro Exam
Procedure Diagnostic Focus
Reliability/ Validity
Rationale Description
Results
UE Dermatomes13
Nerve root function, Neck Pain with Radiating s/s
Not available: Important to include for sensory testing due to pt’s trauma to neck and help clear spinal cord.
To measure intact dermatomes of skin and corresponding nerve roots.
Patient sitting. Have pt close eyes. Use light touch on UE dermatomes and ask pt to say 1) what area is being touched and 2) which side*See Figure 1
All UE dermatomes WNL
UE Myotomes13
Nerve root function, Neck Pain with Radiating s/s
Not available: Important to include for sensory testing due to pt’s trauma to neck and help
To measure intact myotomes of specific muscles of corresponding nerve roots
Patient sitting and have them mimic your movements for correct myotomal
All UE myotomes WNL (pt moves the muscle group and overcomes
clear spinal cord.
testing and test strength of each muscle group *See Figure 2
resistance of examiner normal muscle strength).
UE Deep Tendon Reflexes14
Test for proper muscle tendon reflex/ stretching
Not available: Important to do reflex testing for intact muscular/ tendon stretching
To measure proper/abnormal response to tendon reflex testing
Patient sitting and place UE into proper positioning for testing of deep tendon reflexes
Biceps (C5): 1+
BR (C6): 1+
Triceps (C7-C8): 2+
*All WNL
Postural Analysis Procedure Diagnostic
FocusReliability/
ValidityRationale Descriptio
nResults
Static Sitting14
Postural Syndrome, Neck Pain with Radiating s/s
Not available: Important to assess pt’s posture, which could be causing muscular impairments or nerve root compression
To assess pt’s abnormal posture
Have patient sitting and tell them to sit in their comfortable position as they normally would
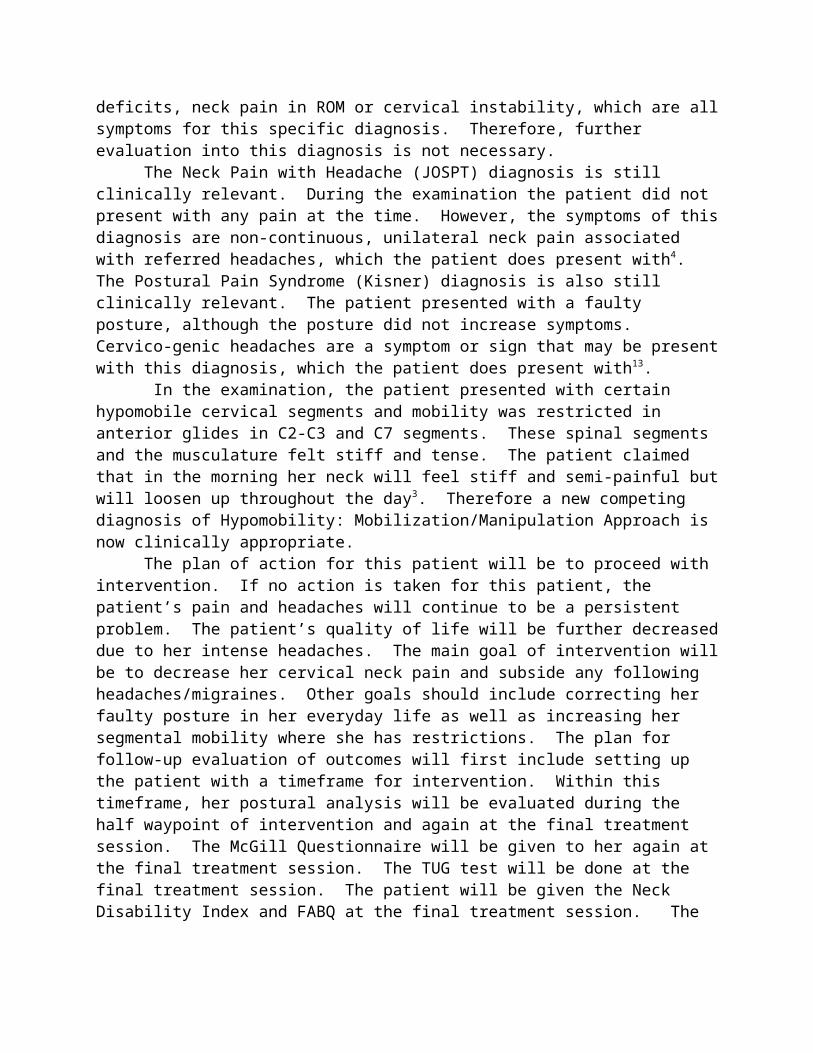
Forward shoulders (rounded), neck placed forward into cervical flexion. Head rotated slightly to right*See Figure 3
Static Standing14
Postural Syndrome, Neck Pain with Radiating s/s
Not available: Important to assess pt’s posture, which could be causing muscular impairments or nerve root compression
To assess pt’s abnormal posture
Have patient stand in front of examiner. Assess from a posterior, anterior and lateral view to see
Left shoulder slightly lower than right. Head slightly rotated to left and side bent to right

if any abnormal deviations from midline
ROM AssessmentProcedure Diagnostic
FocusReliability/
ValidityRationale Descriptio
nResults
Cervical AROM(Flexion, extension, L ROT, R ROT, R SB, L SB)14
Hypermobility Hypomobility Coordination Impairments
Not available: Important to assess pt’s ROM in c-spine to detect any impairments
Important to assess pt’s ROM in c-spine to detect any impairments
Have patient sitting and instruct them in the desired motion for each ROM
ROM for right and left movements all WNL, along with no pain at end range or with overpressure*See Figure 4
Shoulder AROM(Flexion, extension, ABD, ER, IR)14
Hypermobility Hypomobility Coordination Impairments
Not available: Important to assess pt’s ROM in shoulder to detect any underlying impairments
Important to assess pt’s ROM in shoulder to detect any underlying impairments
Have patient sitting and instruct them in the desired motion for each ROM
ROM for each shoulder (bilaterally) all WNL along with no pain at end range
Cervical Spine Mobility Procedure Diagnostic
FocusReliability/ Validity
Rationale Description
Results
Cervical Spine mobility testing12,14
HypermobilityHypomobility Neck Pain with Headaches
Not available: Important to test for hyper- or hypo- mobility of individual spinal segments
To test for hyper- or hypo- mobility of individual spinal segments
Have patient lie prone with neck exposed. Find desired cervical segment and find spinous process
C2-C3: hypomobility
C7: hypomobility
*Both section had muscular tightness.

and apply an anterior glide. Repeat with unilateral transverse process
Special Tests Procedure Diagnostic
FocusReliability/
Validity26Rationale Descriptio
nResults
Upper limb Nerve Tension Tests (radial, median and ulnar)14.18
Shortened nerve length or impingement of specific nerve
Reliability: .76 To test for the presence of cervical radiculopathy
Video link (median)Video link (radial)Video link (ulnar)
Normal pulling, strain, no pain
Sharps Purser14,21
Hypermobility Movement coordination impairments
Reliability: 0.58Specificity: 96%Sensitivity: 69%
Assess integrity of Atlanto-Axial joint (transverse ligament)
Video link Negative
Cervical Distraction14
Nerve compression
Reliability: 0.88 Specificity: 97% Sensitivity: 44%
To test for the presence of cervical radiculopathy
Video link Negative (no symptom relief or provoking)
Spurlings14 Nerve compression
Reliability: 0.60Sensitivity: 50% Specificity: 88%
To test for the presence of cervical radiculopathy
Video link Negative
Vertebral Artery Quadrant14
Test vertebral artery blood flow (any effect on pt’s headaches)
Not enough literature support
Often misdiagnosed as cervical headaches. Test any stenosis of vertebral artery flow.
Video link Negative

Lateral Transverse Shear Test14,22
HypermobilityHypmobility
Reliability 0.5-0.89Sensitivity: 65% Specificity: 98%
To test for hypermobility of atlantoaxial articulation
Video link Negative
Outcome Measures Procedure Diagnostic
FocusReliability /
Validity26Rationale Descriptio
nResults
McGill Pain (VAS)15,25
To assess intensity and quality of pain
Reliability: Not establishedValidity (musculoskeletal pain): 0.70
To assess intensity and quality of pain
Answer questions, locate area of body with pain
(See McGill Form)
The Neck Disability Index14
Assess how neck pain affects patients daily life
Test-Retest Reliability for Neck Pain (Chronic): 0.86Validity for General Neck Pain: 0.45-0.75
Assess how neck pain affects patients daily life
Answer the form
(See Neck Disability Index)
FABQ14 Assess patients fear-avoidance due to pain
Inter-rater Reliability: 0.94Validity: 0.90
Assess patients fear-avoidance beliefs about activity affect/ contribute to pain
Self reported
(See FABQ)
Functional Movement23
Assess patients ability to perform functional movement with/without pain
Not available for age group/testImportant to distinguish patient does not have any pain with movement
Assess patients ability to perform functional movement with/without pain
Patient standing, pick up 10 pounds from ground and place on hip level table. Repeat 10 times for 3 sets
Average of 3 sets: 22.3 seconds (did not experience pain)
TUG Test14 Assess Not available Assess Video link Average of 3

mobility, balance and walking ability
for age group (over 60, average time is 8.2 seconds)
mobility, balance and walking ability
trials: 5.6 seconds
Figure 1:14

Figure 2:14

Figure 3:8,14
Figure 4:2,14

Exam Summary:
Due to the patients normal dermatome, myotome, upper nerve tension tests, deep tendon reflexes, negative distraction test and Spurlings test this would be valid differential diagnosis in order to rule out any kind of neural or nerve diagnosis1. The patient’s abnormal static sitting and standing posture (slight left rotation, slight right side bend, forward neck flexion and rounded shoulders) could allow for further evaluation into these factors facilitating her neck pain and headaches. The patient presents with all normal ROM’s in her cervical spine and bilateral shoulders. The patient presented with hypomobility of C2-C3, which could be due to her lateral shift/rotation of her head. She also has hypomobility of her C7 segment, which could be due to her abnormal posture. The McGill questionnaire shows that her pain is centralized to her neck and forehead and is not radiating. It also shows how she describes her pain, which include severe stabbing, sharp and splitting in her left neck and forehead (where she indicated on the VAS).
5. Clinical Impression #2
Due to the examination procedures, it is clinically relevant to deny the initial impression of any diagnosis that included any nerve or radiating symptoms, such as Neck Pain with Radiating Symptoms (JOSPT).4 The patient was negative in the Spurlings Compression Test, Cervical Distraction Test and Upper Nerve Tension Tests. The patient did not present with any radiating symptoms during ROM, postural analysis or in her VAS form15. The patient did not present with any hypermobility or functional instabilities13. She did not present with any ligament laxity even though the cause of her pain was a neck trauma. It is relevant that radiating pain was not occurring, which is a common symptom of this specific diagnosis. Therefore further evaluation and analysis into this diagnosis is not necessary. Neck Pain with Movement Coordination Impairments4, is also a diagnosis that can be denied. The patient did not present with referred UE pain or any signs of a cervical spine sprain, strain, any strength deficits, neck pain in ROM or cervical instability, which are all symptoms for this specific diagnosis. Therefore, further evaluation into this diagnosis is not necessary.
The Neck Pain with Headache (JOSPT) diagnosis is still clinically relevant. During the examination the patient did not present with any pain at the time. However, the symptoms of this diagnosis are non-continuous, unilateral neck pain associated with referred headaches, which the patient does present with4. The Postural Pain Syndrome (Kisner) diagnosis is also still clinically relevant. The patient presented with a faulty posture, although the posture did not increase symptoms. Cervico-genic headaches are a symptom or sign that may be present with this diagnosis, which the patient does present with13.
In the examination, the patient presented with certain hypomobile cervical segments and mobility was restricted in anterior glides in C2-C3 and C7 segments. These spinal segments and the musculature felt stiff and tense. The patient claimed that in the morning her neck will feel stiff and semi-painful but will loosen up throughout the day3. Therefore a new competing diagnosis of Hypomobility: Mobilization/Manipulation Approach is now clinically appropriate.

The plan of action for this patient will be to proceed with intervention. If no action is taken for this patient, the patient’s pain and headaches will continue to be a persistent problem. The patient’s quality of life will be further decreased due to her intense headaches. The main goal of intervention will be to decrease her cervical neck pain and subside any following headaches/migraines. Other goals should include correcting her faulty posture in her everyday life as well as increasing her segmental mobility where she has restrictions. The plan for follow-up evaluation of outcomes will first include setting up the patient with a timeframe for intervention. Within this timeframe, her postural analysis will be evaluated during the half waypoint of intervention and again at the final treatment session. The McGill Questionnaire will be given to her again at the final treatment session. The TUG test will be done at the final treatment session. The patient will be given the Neck Disability Index and FABQ at the final treatment session. The patients cervical segment mobility will also be assessed at each treatment session to note any change in mobility.
6. Intervention
This patient is presenting with multiple problems that are clinically relevant to guide the intervention strategy. The problems include a faulty posture, mostly in her cervical spine, segmental hypomobility, malalignment of certain cervical spine segments and headaches that are occurring due to vertebrae or musculature abnormalities. These problems are all factors in the leading diagnosis that include 1) Neck Pain with Headaches, 2) Postural Syndrome and 3) Hypomiblity: mobilization/manipulation approach. Due to these problems, the initial problems that should be addressed include (see Table 2 for cervical stabilization with progressive limb loading with emphasis on cervical and thoracic extensors):
Neck Pain with Headache : postural adjustment/correction, upper cervical flexion approach with lower cervical spine extension, cervical and scapular stabilization, upper extremity, cervical and suboccipital stretching13. Mobilizations of cervical spine (mostly C2-C3, C7, but also thoracic spine for cervical extension improvement).5 which also include mobilizations with movement (anterior glide of left transverse process while patient turns head to right).26 The literature supports that thoracic spine manipulation, including high velocity thrusts, has a positive effect on cervical neck pain associated with headaches.5,9,12,19 Transcutaneous Electrical Nerve Stimulation (TENS) unit on neck extensors for relaxation of musculature and tension relief6. Kinesthetic awareness with upper extremities loading (Table 2).13
Postural Syndrome: postural education and ergonomic assessment (changing way patient carries heavy backpack as a student). Deep neck muscular stabilization/relaxation and controlled axial extension with cranio-cervical flexion and lower cervical/upper thoracic extension (Table 2). 12,13 Patient education of awareness of neutral spine position in supine, prone, sitting and standing.13
Hypomobility : mobilizations of cervical spine in extension, rotation and side bending. Muscle energy techniques for cranio-cervical mobility to increase cranio-cervical rotation.12,16,17
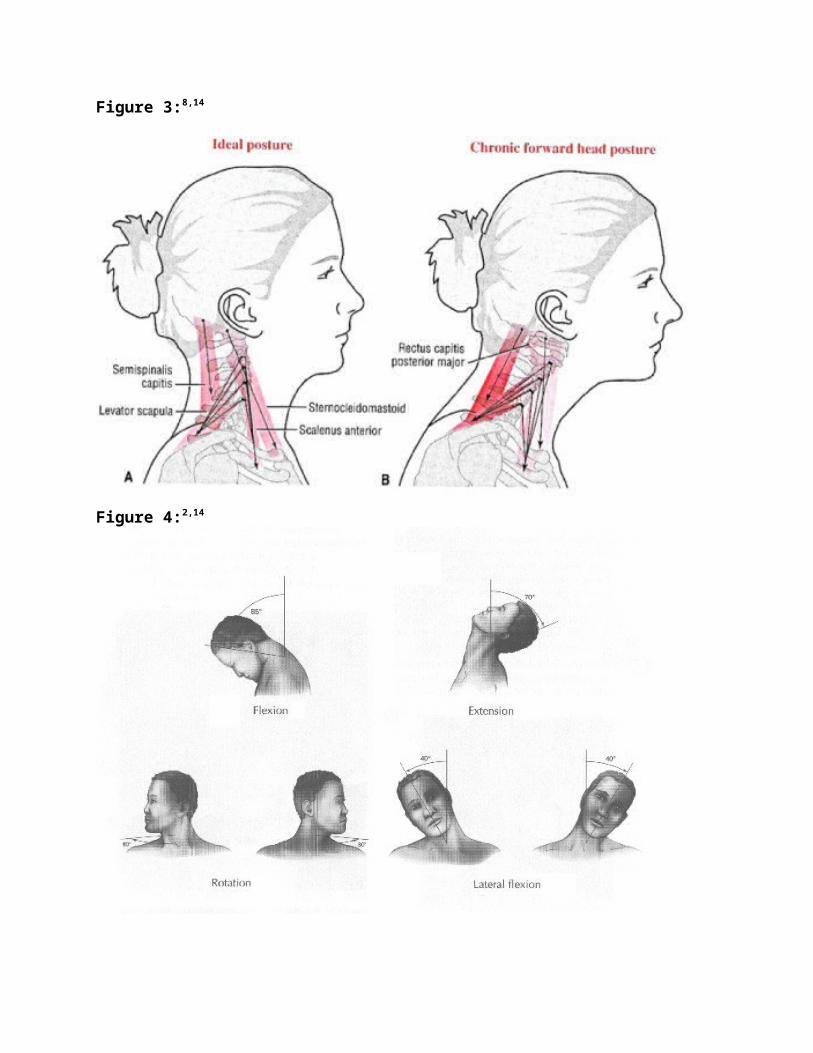
Table 2:13
Max Support----------------------------------------------------------------------Minimum Support

7. Outcomes:14,23,26
McGill Pain (VAS): to assess both the intensity and quality of pain.Neck Disability Index: self-report questionnaire used to determine how neck pain affects a patient’s daily lifeFABQ: Focuses specifically on how a patient’s fear-avoidance beliefs about physical activity and work may affect and contribute to his/her pain (i.e. the cognitive/affective components of pain that are differentiated from specific tissue damage, injury, and nociception) and resulting disability.Functional Movement Testing: to identify improper movement patterns, which can then be addressed by using corrective exercises to restore proper movement. (Patient performed picking up 10 pounds from ground and placing on table, 10 times/3 sets.)
TUG Test: Assesses mobility, balance, walking ability, and fall risk in older adults
(See Examination section for outcome measures reliability and validity and Clinical Impression #2 section for the time points indicated in intervention stages)
8: Discussion:
The analysis of this case study of this patient provides that the competing diagnoses are all of relevance to the underlying problems in this patient’s examination. With thorough investigation into the patient’s problems and what could be causing them or what was not causing them, there was guidance towards specific diagnoses while other diagnoses were dropped from consideration. All of the nerve/neural tests were negative with no radicular symptoms present, which can lead to dismiss any nerve involvement.1,2 The spinal segments or musculature surrounding the cervical spine was not hypermobile or did not have increased laxity, which can therefore dismiss that specific diagnosis. Therefore, it is appropriate to address that the diagnostic dilemma was not technically resolved, but rather improved and further treatment/intervention is necessary to pinpoint the exact causes of the patient’s problems.
The main patient-identified problem (PIP) presented was the patients migraine headaches associated with her neck pain, which would lead the clinician to focus firstly on this impairment. Since the patient presented with a faulty posture or sustained posture and tense muscle contraction in the upper and lower cervical region this would be considered the primary diagnoses. The literature suggests that cervical impairments, which can lead to the headaches, can also arise from faulty thoracic joint mobility.11,19,24 Therefore, there is extensive literature to suggest that thoracic mobilization, in chronic patients, can lead to a decrease in cervical headaches and increased cervical/thoracic mobility.5,8 The patient’s identification of where the pain was occurring, unilaterally in the fronto-temporal region, severely for 4-72 hours at a time, also suggests that it is a migraine headache in comparison to a cluster or tension headache.4
Another comparison according to the literature is the postural syndrome. The patient presented with faulty posture within the cervical spine, specific segment stiffness in cervical spine, muscular tightness in upper trapezius and upper cervical muscles and a lifestyle that involves excessive use of sitting on a laptop (student). These are all contributing factors to her faulty posture and can be another leading cause to her pain/headaches. The literature has suggested that patients with migraines and a faulty neck posture (forward head posture) had a decrease in isometric strength and less endurance compared to those with an absence of headaches.8,24 More recent studies even further back this research, suggesting that patients who present with general cervical lordosis have an increased likelihood of developing cervico-genic headaches.11,24
The last patient abnormality that was addressed was hypomobile segments in the cervical spine. These impairments can either be an effect of faulty posture or the cause of the faulty posture. In either case, the literature suggests that adjusting these hypomobile deficits can lead to a decrease in cervical symptoms, such as headaches.3,8,9,16,17

This specific case suggests that the symptoms of headaches and neck pain that are being provoked from different causes (hypomobility, faulty cervical posture, faulty thoracic posture/mobility). In conclusion it is appropriate to address all of these clinical abnormalities in order to improve the patient’s quality of life in her interventions.
Total Word Count: 4,305Word Count Without References: 3,638Word Count Without References and Table 1: 2,659
References:
1. Binder AL. Cervical pain syndromes. In: Oxford Textbook of Rheumatology, Maddison PJ (Ed), Oxford Medical Publications, Oxford 1993. p.1060
2. Brismée J-M, Phelps V, Sizer P. Differential Diagnosis and Treatment of Chronic Neck and Upper Trapezius Pain and Upper Extremity Paresthesia: A Case Study Involving the Management of an Elevated First Rib and Uncovertebral Joint Dysfunction. Journal of Manual & Manipulative Therapy 2005;13(2):79–90.
3. Cervical and Thoracic Mobilization Versus Manipulation for Mechanical Neck Pain. J Orthop Sports Phys Ther Journal of Orthopaedic & Sports Physical Therapy 2012;42(4).
4. Childs, J. D., Cleland, J. A., Elliott, J. M., Teyhen, D. S., Wainner, R. S., Whitman, J. M., . . . American Physical Therapy, Association. (2008). Neck pain: Clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther, 38(9), A1-A34.
5. Cleland JA, Mintken PE, Carpenter K, et al. Examination of a Clinical Prediction Rule to Identify Patients With Neck Pain Likely to Benefit From Thoracic Spine Thrust Manipulation and a General Cervical Range of Motion Exercise: Multi-Center Randomized Clinical Trial. Physical Therapy 2010;90(9):1239–1250.
6. Chiu TT, Hui-Chan CW, Cheing G. A randomized clinical trial of TENS and exercise for patients with chronic neck pain. clin rehabil Clinical Rehabilitation 2005;19(8):850–860.
7. Douglass AB, Bope ET. Evaluation and Treatment of Posterior Neck Pain in Family Practice. The Journal of the American Board of Family Medicine 2004;17(90001).
8. Farmer PK, Snodgrass SJ, Buxton AJ, Rivett DA. An Investigation of Cervical Spinal Posture in Cervicogenic Headache. Physical Therapy 2014;95(2):212–222.
9. Gross A, et al. Manipulation of mobilization for neck pain: A Cochrane Review. Man Therapy. 2010;15:3315-333
10. Janssen M, Nabih A, Moussa W, Kawchuk GN, Carey JP. Evaluation of Diagnosis Techniques Used for Spinal Injury Related Back Pain. Pain Research and Treatment 2011;2011:1–10.
11. Jull GA. Management of Cervicogenic Headache. Physical Therapy of the Cervical and Thoracic Spine 2002:239–272.
12. Kanlayanaphotporn R, Chiradejnant A, Vachalathiti R. The Immediate Effects of Mobilization Technique on Pain and Range of Motion in Patients Presenting With

Unilateral Neck Pain: A Randomized Controlled Trial. Archives of Physical Medicine and Rehabilitation 2009;90(2):187–192.
13. Kisner C, Kolby LA. Therapeutic Exercise: Foundations and Techniques. 6th edition. F.A. Davis Company. 2012.
14. Magee D. Chapter 3: Cervical Spine. In: Orthopedic Physical Assessment. 6th ed. St. Louis, MO : Elsevier Saunders; 2014:148–223.
15. Melzack, Ronald. "The short-form McGill pain questionnaire." Pain 30.2 (1987): 191-197.
16. Monahan JJ, Waite RJ. Cervical spine. In: Orthopaedics in primary care, Steinberg GG, Akins CM, Baran DT (Eds), Lippincott Williams Wilkins, Baltimore 1999.
17. Mun Cheung Lau H et al. The effectiveness of thoracic manipulation on patients with chronic mechanical neck pain-RCT. Man Ther. 2011; 16:141-147
18. Neurodynamic Assessment. - Physiopedia, universal access to physiotherapy knowledge. Available at: http://www.physio-pedia.com/neurodynamic_assessment. Accessed April 7, 2016.
19. Racicki S, Gerwin S, Diclaudio S, Reinmann S, Donaldson M. Conservative physical therapy management for the treatment of cervicogenic headache: a systematic review. Journal of Manual & Manipulative Therapy 2013;21(2):113–124.
20. Rogers B, Brogan K. Diagnosis and management of acute non-degenerative neck pain. Br J Hosp Med British Journal of Hospital Medicine 2013;74(Sup3).
21. Sharp Purser Test. - Physiopedia, universal access to physiotherapy knowledge. Available at: http://www.physio-pedia.com/sharp_purser_test. Accessed April 7, 2016.
22. Transverse Ligament Stress Test. - Physiopedia, universal access to physiotherapy knowledge. Available at: http://www.physiopedia.com/transverse_ligament_stress_test. Accessed April 7, 2016.
23. Wainner RS, Fritz JM, Irrgang JJ, Boninger ML, Delitto A, Allison S. Reliability and Diagnostic Accuracy of the Clinical Examination and Patient Self-Report Measures for Cervical Radiculopathy. Spine 2003;28(1):52–62.
24. Watson DH, Trott PH. Cervical headache: an investigation of natural head posture and upper cervical flexor muscle performance. Cephalalgia 1993;13(4):272–284.
25. Wilkie, Diana J., et al. "Use of the McGill Pain Questionnaire to measure pain: a meta-analysis." Nursing Research 39.1 (1990): 36-41
26. Wise CH. Orthopaedic Manual Physical Therapy: from Art to Evidence. 1st ed. Philadelphia, PA: F.A. David Company; 2015.