laboratories.docx · web viewindications. enlive is a high-calorie, fat-free alternative to...
TRANSCRIPT

1
MEDICAL NUTRITIONALS ADULT FORMULAS
ENLIVE ®GeneralClear Liquid NutritionComposition- Clear liquid nutrition- Fortified with 21 essential vitamins and minerals.- Excellent source of protein-10 g/8.1 fl oz- Refreshing tangy flavors provide taste alternative.Not for parenteral useNutrient FactsNutrient density (Cal/ml)
1.25
Protein (% Cal) 13.3
Carbohydrate (% Cal) 86.7
Fat, (Cal) 0Water (g/8.1 fl oz) 191Kosher YesGluten-free YesLactose-free YesLow residue YespH 3.1
NUTRITION INFORMATION %
Per 8.1 fl oz
(Apple) Dv
Calories 300
Protein, g 10 20TMI Carbohydrate, g 65 22
Sugars, g 15
Total Fat, g 0 0Saturated Fat, g 0 0 0
Cholesterol, mg <5 <2
Vitamin A, IU 1250 25Vitamin D, IU 60 15Vitamin E, IU 9 30Vitamin K, mcg 20 25Vitamin C, mg 24 40Folic Acid, mcg 60 15Thiamin (Vitamin B1), mg 0.38 25Riboflavin (Vitamin B2), mg 0.34 20Vitamin B6, mg 0.4 20Vitamin B12, mcg 1.2 20Niacin, mg 2.0 10Biotin, mcg 30 10Pantothenic Acid, mg 0.8 8
Sodium, mg 65(2.8 mEq) 3
Potassium, mg 40(1.0 mEq) 1
Chloride, mg 340(.6 mEq) 10
Calcium, mg 60 6Phosphorus, mg 20 2Magnesium, mg 8.0 2Iodine, mcg 45 30Manganese, mg 0.9 45Copper, mg 0.3 15Zinc, mg 3.8 25Iron, mg 2.7 15Selenium, mcg 14 20Chromium, mcg 18 15Molybdenum, mcg 33.7 45

2
IndicationsENLIVE is a high-calorie, fat-free alternative to sweeter-tasting creamy supplements.ENLIVE is an ideal choice for people on clear-liquid, pre- and postsurgical, cancer, bowel-prep, fat-malabsorptive, fat restricted, low-sodium, or low cholesterol diets.For supplemental oral nutritionPackaging27 brik packs/case.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
ENRICH ®CompositionProtein: 9.4 g/250 ml, (Na, Ca) caseinate, soy protein isolate.Fat: 8.8 g/250 ml corn oil.Carbohydrate: 38.3 g/250 ml, hydrolyzed corn starch, sucrose, soy polysaccharide.Minerals & Vitamins: meet RDA in 2000 Kcal.Water: 209.5 ml/250 ml, Calories: 260 Kcal/250 ml = 1.04 Kcal/ml.PropertiesComplete balanced feeding: with fiber; oral or with nasogastric tube; Lactose and gluten free; Vanilla flavor; Osmolality: 439 mOsm/kg of water. IndicationsPatients who do not require low residue diet, monitoring diarrhea or constipation.Packaging24 cans of 250 ml/case.Av M.E.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
ENSURE HN ®GeneralCompositionProtein: 10.5 g/250 ml. (Na, Ca) caseinate, soy protein isolate.Fat: 8.4 g/250 corn oil.Carbohydrate: 33.4 g/250 ml hydrolyzed corn starch, sucrose.Minerals & Vitamins: meet RDA in 2000 Kcal.Water: 212.5 ml/250 ml.Calories: 250 Kcal/250 ml = 1 Kcal/ml.PropertiesComplete balanced feeding: low residue; oral or with nasogastric tube.Lactose and gluten free, Vanilla flavor, Osmolality: 414 mOsm/kg of water.IndicationsMalnourished, elderly, surgical pre/post, psychological, barium enema examination and colonoscopy preparation.Packaging24 cans of 250 ml/case.Av M.E.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
ENSURE ®GeneralComplete, Balanced NutritionComposition- Excellent source of 24 essential vitamins and minerals- Low in saturated fat (0.5 g/8 fl oz)- 500 mcg (0.50 mg) of lutein per 8 fl oz to help support eye health (retail only).Nutrient FactsNutrient density (Cal/ml) 1,06Protein (% Cal) 14.1Carbohydrate (% Cal) 63.9Fat (% Cal) 22.0Nutrient base (Cal) 1000Nutrient base (ml) 948Total Cal/g nitrogen 178:1Nonprotein Cal/g nitrogen 153:1Water (g/8 fl oz) 200Kosher YesGluten-free YesLactose-free YesLow residue YesRenal sol. load (mOsm/L) 326OsmolaIity (m0sm/kg H20)
590
ENSURElngredients (Vanilla-Instit.): U-D Water. Sugar (Sucrose), Corn Syrup, Corn Maltodextrin, Calcium Caseinate, High Oleic Safflower Oil, Canola Oil, Soy Protein Isolate, Whey Protein Concentrate, Corn Oil, Potassium Citrate,Calcium Phosphate, Magnesium Phosphate, Natural and Artificial Flavor, Soy Lecithin, Sodium Citrate, Magnesium Chloride, Salt (Sodium Chloride), Choline Chloride, Carrageenan, Potassium Chloride, Ascorbic Acid, Ferrous Sulfate, dl-Alpha-Tocopheryl Acetate, Zinc Sulfate,

3
Niacinamide, Calcium Pantothenate, Manganese Sulfate, Cupric Sulfate, Vitamin A Palmitate, Thiamine Chloride Hydrochloride, Pyridoxine Hydrochloride, Riboflavin, Folic Acid, Chromium Chloride, Biotin, Sodium Molybdate, Sodium Selenate, Potassium Iodide, Phylloquinone, Vitamin D3 and Cyanocobalamin. (7837-03).Nutrition Per
% DV*
Information 8 fl ozCalories 250Protein, g 8.8
18
Total Carbohydrate, g 40.0
13
Sugars, g 18Total Fat, g 6.1
9
Saturated Fat, g 0.5
3
Cholesterol, mg <5 <2Vitamin A, IU 1250
25
Vitamin D, IU 100
25
Vitamin E, IU 7.5
25
Vitamin K, mcg 20
25
Vitamin C, mg 30
50
Folic Acid, mcg 100
25
Thiamin (Vitamin B1), 0.38
25
mgRiboflavin, mg 0.43
25
Vitamin B6, mg 0.50
25
Vitamin B12, mcg 1.5
25
Niacin, mg 5.0
25
Choline, mg 100
†
Biotin, mcg 75
25
Pantothenic Acid, mg 2.5
25
Sodium, mg 200
8
(8.7 mEq)Potassium, mg 370
11
(9.5 mEq)Chloride, mg 310
10
(8.8 mEq)Calcium, mg 300
30
Phosphorus, mg 250
25
Magnesium, mg 100
25
Iodine, mcg 38
25
Manganese, mg 1.3
60
Copper, mg 0.50
25
Zinc, mg 3.8
25
Iron, mg 4.5
25
Selenium, mcg 18
25
Chromium, mcg 30
25

4
Molybdenum, mcg 38
50
*For adults and children 4 or more years of age.† DV not establishedNot for parenteral useIndicationsRich, creamy-tasting ENSURE provides complete, balanced nutrition for supplemental use between or with meals. ENSURE can benefit people who are on modified diets, at nutrition risk, experiencing involuntary weight loss, recovering from illness or surgery, or on low-residue diets.- For oral or sole-source feeding- Retail product for supplemental oral nutrition.Packaging8-fl-oz cans: 24/caseVanillaChocolateButter PecanStrawberryCoffeeEggnogBlack WalnutVanillaChocolateButter PecanStrawberryCoffee Latte8-fl-oz bottles; 24/caseVanillaChocolateButter PecanStrawberryCoffee Latte32-fl-oz cans; 6/caseVanilla32-fl-oz bottles; 6/caseVanillaChocolate
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
ENSURE FIBER WITH FOS ®GeneralComplete, Balanced NutritionComposition- 2.8 g of dietary fiber/8 fl oz- Includes 1.0 g of FOS/8 fl oz. FOS are prebiotics that stimulate the growth of beneficial bacteria in the colon.- Excellent source of 24 essential vitamins and minerals.Nutrient density (Cal/ml) 1.06Protein (% Cal) 14.1Carbohydrate (% Cal) 63.9Fat (% Cal) 22.0Nutrient base (Cal) 1000Nutrient base (ml) 948
Total Cal/g nitrogen 178:1
Nonprotein Cal/g nitrogen 153:1
Water (g/8 fl oz) 195Kosher YesGluten-free YesLactose-free YesLow residue YesRenal sol. load (mOsm/L) 327OsmolaIity (mOsm/kg H2O) 500
Min. tube size for gravity 10/8pump feeding (Fr) lngredients (Vanilla): U-D Water, Corn Maltodextrin, Sugar (Sucrose), Sodium and Calcium Caseinates, High Oleic Safflower Oil, Canola Oil, Soy Protein Isolate, Oat Fiber, Corn Oil, Fructooligosacharides, Soy Fiber, Calcium Phosphate, Magnesium Chloride, Potassium Citrate, Cellulose Gel, Soy Lecithin, Potassium Phosphate, Sodium Citrate, Natural and Artificial Flavors, Magnesium Phosphate, Choline Chloride, Ascorbic Acid, Cellulose Gum, Carrageenan, Potassium Chloride, Ferrous Sulfate, dl-Alpha-Tocopheryl Acetate, Zinc Sulfate, Niacinamide, Calcium Pantothenate, Cupric Sulfate, Vitamin A Palmitate, Thiamine Chloride Hydrochloride, Pyridoxine Hydrochloride, Riboflavin, Folic Acid, Chromium Chloride, Biotin, Sodium Molybdate, Sodium Selenate, Potassium Iodide, Phylloquinone, Vitamin D3 and Cyanocobalamin.Nutrition Information Per 8 fl oz % DV*

5
Calories 250
Protein, g 8.8 18Total Carbohydrate, g 42.0 14Dietary Fiber, g† 2.8 12
Soluble Fiber, g 1
Sugars, g 12
Total Fat, g 6.1 9Saturated Fat, g 0.5 3Cholesterol, mg <5 <2Vitamin A, IU 1250 25Vitamin D, IU 100 25Vitamin E, IU 7.5 25Vitamin K, mcg 20 25Vitamin C, mg 30 50Folic Acid, mcg 100 25Thiamin (Vitamin B1), mg 0.38 25Riboflavin (Vitamin B2), mg 0.43 25Vitamin B6, mg 0.50 25Vitamin B12, mcg 1.5 25Niacin, mg 5.0 25Choline, mg 100 ‡Biotin, mcg 75 25Pantothenic Acid, mg 2.5 25Sodium, mg 200 (8.7 mEq) 8Potassium, mg 370 (9.5 mEq) 11Chloride, mg 320 (9.0 mEq) 10Calcium, mg 350 35Phosphorus, mg 300 30Magnesium, mg 100 25Iodine, mcg 38 25Manganese, mg 1.3 60Copper, mg 0.50 25Zinc, mg 3.8 25Iron, mg 4.5 25Selenium, mcg 18 25Chromium, mcg 30 25Molybdenum, mcg 38 50*For adults and children 4 or more years of age.† 1.8 g of total dietary fiber from oat and soy fibers and 1.0 g of FOS‡ DV not established Not for parenteral useIndicationsFiber With FOS is complete, balanced nutrition with FOS for people who can benefit from increased dietary fiber and nutrients. The fiber blend with FOS, a prebiotic, helps maintain digestive tract health. Ensure Fiber with FOS can benefit people who are on modified diets, at nutrition risk, experiencing involuntary weight loss, or recovering from illness or surgery.- For oral or sole-source feedingPackaging8-fl-oz cans; 24/caseVanillaChocolateVanillaChocolate
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
ENSURE PLUS HN ®CompositionProtein: 15.6 g/250 ml, (Na, Ca) caseinate, soy protein isolate.Fat: 12.5 g/250 ml corn oil.Carbohydrate: 50.0 g/250 ml hydrolyzed corn starch, sucrose.Minerals and Vitamins: meet RDA in 2000 Kcal.Water: 192.2 ml/250 mlCalories: 1.5 Kcal/ml PropertiesComplete balanced feeding, high caloric, high nitrogen; oral or with nasogastric tube; Lactose and gluten free; Vanilla flavorOsmolality: 650 mOsm/kg of water.Indications

6
Patients who are intolerant to high-volume feedings and requiring increased levels of calories and protein to meet metabolic needs.Packaging24 cans of 250 ml/case.Av M.E.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
ENSURE POWDER ®GeneralComplete, Balanced NutritionComposition- Good source of 24 essential vitamins and minerals.- Convenient, easy to mix.Nutrient FactsAt standard dilution: 1/2 cup mixed with 3/4 cup cold water (one 8-fl-oz serving).Nutrient density (Cal/ml) 1.06Protein (% Cal) 14.0Carbohydrate (% Cal) 54.4Fat (% Cal) 31.6Nutrient base (Cal) 2000Nutrient base (ml) 1887
Total Cal/g nitrogen 178:1
Nonprotein Cal/g nitrogen 153:1
Kosher YesGluten-free YesLactose-free YesLow residue YesRenal sol. load (mOsm/L) 326OsmolaIity (mOsm/kg H2O) 470
lngredients: U-D Corn Syrup Maltodextrin, Sugar (Sucrose), Corn Oil, Sodium and Calcium Caseinates, Soy Protein Isolate, Potassium Citrate, Artificial Flavor, Magnesium Chloride, sodium Citrate, Calcium Phosphate Tribasic, Potassium Chloride, Soy Lecithin, Ascorbic Acid, Choline Chloride, Zinc Sulfate, Ferrous Sulfate, Alpha-Tocopheryl Acetate, Niacinamide, Calcium Pantothenate, Manganese Sulfate, Thiamine Chloride Hydrochloride, Cupric Sulfate, Pyridoxine Hydrochloride, Riboflavin, Vitamin A Palmitate, Folic Acid, Biotin, Sodium Molybdate, Chromium Chloride, Potassium Iodide, Sodium Selenate, Phylloquinone, Cyanocobalamin and Vitamin D3.Nutrition Information Per 8 fl oz DV* %
Calories 250
Protein, g 9 18
Total Carbohydrate, g 34 11
Sugars, g 13
Total Fat, g 9 14
Saturated Fat, g 1.5 8
Cholesterol, mg <5 <2
Water, g† 200
Vitamin A, IU 650 15
Vitamin D, IU 50 15
Vitamin E, IU 5.63 20
Vitamin K, mcg 10 15
Vitamin C, mg 37.5 60
Folic Acid, mcg 100 25
Thiamin (Vitamin B1), mg 0.38 25
Riboflavin (Vitamin B2), mg 0.43 25
Vitamin B6, mg 0.50 25
Vitamin B12, mcg 1.5 25
Niacin, mg 5.0 2

7
5Choline, mg 75 ‡
Biotin, mcg 75 25
Pantothenic Acid, mg 2.5 25
Sodium, mg 200 (8.7 mEq) 8
Potassium, mg 370 (9.5 mEq) 11
Chloride, mg 310 (8.8 mEq) 10
Calcium, mg 125 15
Phosphorus, mg 125 15
Magnesium, mg 50 15
Iodine, mcg 18.8 15
Manganese, mg 0.62 30
Copper, mg 0.25 15
Zinc, mg 2.82 20
Iron, mg 2.25 15
Selenium, mcg 9 15
Chromium, mcg 13 15
Molybdenum, mcg 19 25
*For adults and children 4 or more years of age.† When reconstituted per instructions on can.‡ DV not establishedNot for parenteral useIndicationsEnsure Powder (reconstituted with water) is complete, balanced nutrition for supplemental use between or with meals. When consumed in appropriate amounts, reconstituted Ensure Powder can be used as a sole source of nutrition. It may benefit people who are on modified diets, at nutrition risk, experiencing involuntary weight loss, recovering from illness or surgery, or on low-residue diets.- For oral or sole-source feeding.Packaging14-oz (397-g) cans;6/case; 7 servings/canVanilla.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
GLUCERNA ®GeneralComposition- Provides 100% of the DVs for 24 essential vitamins and minerals in 1420 Calories- 14.4 g of dietary fiber/L. Fiber helps modulate bowel function and may be useful in the dietary management of diarrhea and constipation.- Fat blend is high in monounsaturated fatty acids- Meets American Heart Association recommendations for fatty acid profile favoring mono-unsaturated fat to improve lipid profiles.
Nutrient Facts
Nutrient density (Cal/ml) 1.0Protein (%Cal) 16.7Carbohydrate (% Cal) 34.3Fat (% Cal) 49.0Nutrient base (Cal) 1420Nutrient base (ml) 1420
Total Cal/g nitrogen 150:1
Nonprotein Cal/g nitrogen 125:1
Water (g/L) 853Kosher YesGluten-free YesLactose-free Yes

8
Low residue NoRenal sol. Load (m0sm/L) 360Osmolality (m0sm/kg H20) 355
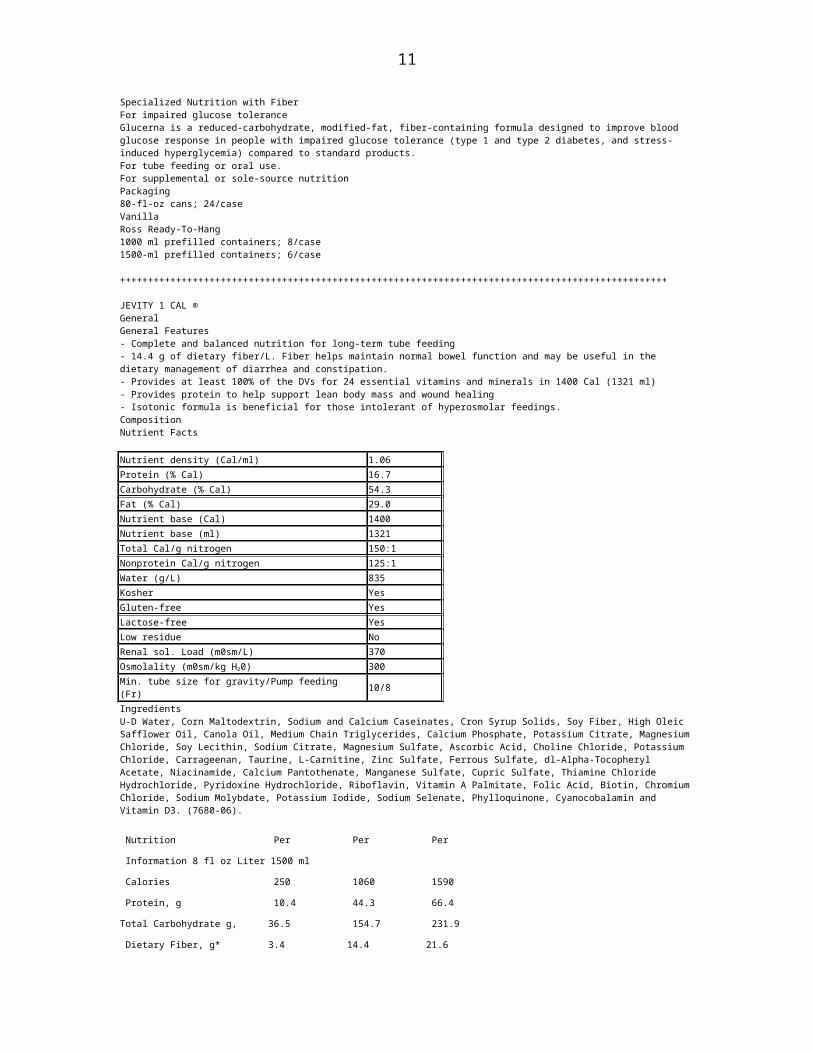
Min. tube size for gravity/ 10/8Pump feeding (Fr) Ingredients: U-D Water, Corn Maltodextrin, High Oleic Safflower Oil, Sodium and Calcium Caseinates, Soy Fiber, Fructose, Canola Oil, Soy Lecithin, Magnesium Chloride, Calcium Phosphate, Sodium Citrate, Natural and Artificial Flavor, m-Inositol, Potassium Citrate, Ascorbic Acid, Potassium Phosphate, Potassium Chloride, Choline Chloride, Carrageenan, L-Carnitine, Taurine, Zinc Sulfate, dl-Alpha-Tecopheryl Acetate, Ferrous Sulfate, Niacinamide, Calcium Pantothenate, Manganese Sulfate, Cupric Sulfate, Thiamine Chloride Hydrochloride, Pyridoxine Hydrochloride, Riboflavin, Vitamin A Palmitate, Beta-Carotene, Folic Acid, Biotin, Chromium Chloride, Sodium Molybdate, Potassium Iodide, Sodium Selenate, Phylloquinone, Cyanocobalamin and Vitamin D3. (7678-02).Nutrition Information Per 8 fl oz Per Liter Per1500 mlCalories 237 1000 1500Protein, g 9.9 41.8 62.7Total Carbohydrate, g 22.8 95.6 143.2Dietary Fiber, g 3.4 14.4 21.6Total Fat, g 12.9 54.4 81.7Water, g 202 853 1280Vitamin A, IU† 1500 6300 9510Vitamin D, IU 67 285 425Vitamin E, IU 7.5 32 48Vitamin K, mcg 14 57 85Vitamin C, mg 50 215 320Folic Acid, mcg 100 425 635Thiamin (Vitamin B1), mg 0.38 1.6 2.4Riboflavin (Vitamin B2), mg 0.43 1.8 2.7Vitamin B6, mg 0.50 2.2 3.2Vitamin B12, mcg 1.5 6.4 9.5Niacin, mg 5.0 22 32Choline, mg 100 425 635Biotin, mcg 75 320 475m-Inositol 0.20 g 850 mg 1300 mgPantothenic Acid, mg 2.5 11 16Sodium, mg 220 (9.6 mEq) 930 (40.4 mEq) 1400 (60.9 mEq)Potassium, mg 370 (9.5 mEq) 1570 (40.3 mEq) 2350 (60.3 mEq)Chloride, mg 340 (9.6 mEq) 1440 (40.6 mEq) 2160 (60.9 mEq)Calcium, mg 170 705 1060Phosphorus, mg 170 705 1060Magnesium, mg 67 285 425Iodine, mcg 25 110 160Manganese, mg 0.84 3.6 5.3Copper, mg 0.34 1.5 2.2Zinc, mg 3.8 16 24Iron, mg 3.0 13 19Selenium, mcg 12 50 74Chromium, mcg 20 85 130Molybdenum, mcg 25 110 160L-Carnitine, mg 34 145 215Taurine, mg 25 110 160* 3.4 g/8 fl oz (14.4 g/L and 21.6 g/1500 ml) of dietary fiber as soy fiber.† 660 IU/8 fl oz (2780 IU/L and 4240 IU/1500 ml) of vitamin A activity supplied by 0.50 mg/8 fl oz (2.1 mg/L and 3.2 mg/1500 ml) of β-carotene.Not for parenteral use. IndicationsSpecialized Nutrition with FiberFor impaired glucose toleranceGlucerna is a reduced-carbohydrate, modified-fat, fiber-containing formula designed to improve blood glucose response in people with impaired glucose tolerance (type 1 and type 2 diabetes, and stress-induced hyperglycemia) compared to standard products.For tube feeding or oral use.For supplemental or sole-source nutritionPackaging80-fl-oz cans; 24/caseVanillaRoss Ready-To-Hang1000 ml prefilled containers; 8/case1500-ml prefilled containers; 6/case
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++

9
JEVITY 1 CAL ®GeneralGeneral Features- Complete and balanced nutrition for long-term tube feeding- 14.4 g of dietary fiber/L. Fiber helps maintain normal bowel function and may be useful in the dietary management of diarrhea and constipation.- Provides at least 100% of the DVs for 24 essential vitamins and minerals in 1400 Cal (1321 ml)- Provides protein to help support lean body mass and wound healing- Isotonic formula is beneficial for those intolerant of hyperosmolar feedings.CompositionNutrient Facts Nutrient density (Cal/ml) 1.06Protein (% Cal) 16.7Carbohydrate (% Cal) 54.3Fat (% Cal) 29.0Nutrient base (Cal) 1400Nutrient base (ml) 1321Total Cal/g nitrogen 150:1Nonprotein Cal/g nitrogen 125:1Water (g/L) 835Kosher YesGluten-free YesLactose-free YesLow residue NoRenal sol. Load (m0sm/L) 370Osmolality (m0sm/kg H20) 300Min. tube size for gravity/Pump feeding (Fr) 10/8IngredientsU-D Water, Corn Maltodextrin, Sodium and Calcium Caseinates, Cron Syrup Solids, Soy Fiber, High Oleic Safflower Oil, Canola Oil, Medium Chain Triglycerides, Calcium Phosphate, Potassium Citrate, Magnesium Chloride, Soy Lecithin, Sodium Citrate, Magnesium Sulfate, Ascorbic Acid, Choline Chloride, Potassium Chloride, Carrageenan, Taurine, L-Carnitine, Zinc Sulfate, Ferrous Sulfate, dl-Alpha-Tocopheryl Acetate, Niacinamide, Calcium Pantothenate, Manganese Sulfate, Cupric Sulfate, Thiamine Chloride Hydrochloride, Pyridoxine Hydrochloride, Riboflavin, Vitamin A Palmitate, Folic Acid, Biotin, Chromium Chloride, Sodium Molybdate, Potassium Iodide, Sodium Selenate, Phylloquinone, Cyanocobalamin and Vitamin D3. (7680-06).
Nutrition Per Per Per
Information 8 fl oz Liter 1500 ml
Calories 250 1060 1590
Protein, g 10.4 44.3 66.4
Total Carbohydrate g, 36.5 154.7 231.9
Dietary Fiber, g* 3.4 14.4 21.6
Total Fat, g 8.2 34.7 52.1
Water, g 197 835 1244
Vitamin A, IU 895 3790 5690
Vitamin D, IU 72 305 460
Vitamin E, IU 8.3 35 53
VITAMIN K, MCG 15 61 92
Vitamin C, mg 55 230 345
Folic Acid, mcg 110 455 690
Thiamin (Vitamin B1), mg 0.41 1.7 2.6
Riboflavin (Vitamin B2), mg 0.48 2.0 3.0
Vitamin B6, mg 0.55 2.3 3.5
Vitamin B12, mcg 1.7 6.9 11
Niacin, mg 5.5 23 35
Choline, mg 110 455 685

10
Biotin, mcg 82 345 520
Pantothenic Acid, mg 2.9 12 18
Sodium, mg 220 930 1400
(9.6 mEq) (40.4 mEq) (60.9 mEq)
Potassium, mg 375 1570 2360
(9.6 mEq) (40.2 mEq) (60.5 mEq)
Chloride, mg 310 1310 1970
(9.8 mEq) (37 mEq) (55.6 mEq)
Calcium, mg 215 910 1370
Phosphorus, mg 180 760 1140
Magnesium, mg 72 305 460
Iodine, mcg 28 115 175
Manganese, mg 0.9 3.8 5.7
Copper, mg 0.37 1.6 2.4
Zinc, mg 4.3 18 27
Iron, mg 3.3 14 21
Selenium, mcg 13 54 81
Chromium, mcg 22 91 140
Molybdenum, mcg 28 115 175
L-Carnitine, mg 28 115 175
Taurine, mg 28 115 175
* 3.4 g/8 fl oz (14.4 g/L and 21.6 g/1500 ml) of total dietary fiber from soy fiber. Not for parenteral use.IndicationsIsotonic Nutrition with FiberJevity 1 Cal is a fiber-fortified, high-nitrogen liquid tube-feeding formula.- For tube feeding- For supplemental or sole-source nutrition- May be used for oral feeding of patients with altered taste perception.* 3.4 g/8 fl oz (14.4 g/L and 21.6 g/1500 ml) of total dietary fiber from soy fiber.Not for parenteral use.Packaging8-fl-oz cans; 24/case32-fl-oz cans; 6/caseRoss Ready-To-Hang1000-ml prefilled containers; 8/case1500-ml prefilled containers; 6/case
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
NEPRO ®GeneralFeatures- Complete, balanced nutrition for people on dialysis.- 8 fl oz provides 475 Cal (2.0 Cal./ml) and at least 25% of the recommended levels of vitamins/minerals for people on dialysis- 1900 Cal (four 8-fl-oz cans) provides at least 100% of the DVs for 18 key vitamins and minerals.- Low in vitamins A and D and high in folic acid and vitamin B6 to accommodate the altered metabolism of people on dialysis.- High in calcium, low in phosphorus; 2:1 Ca/P ratio to help optimize calcium and phosphorus balance- Moderate protein content to replace protein and amino acids lost during dialysis and to help prevent catabolism of tissue proteins.- Includes 3.7 g of FOS/8 fl oz (15.6 g/L). FOS are prebiotics that stimulate the growth of beneficial bacteria in the colon.
Nutrient Facts
Nutrient density (Cal/ml) 2.0Protein (% Cal) 14.0Carbohydrate (% Cal) 43.0Fat (% Cal) 43.0Nutrient base (Cal) 1900Nutrient base (ml) 947
11
Total Cal/g nitrogen 179:1
Nonprotein Cal/g nitrogen 154:1
Water (g/L) 699Kosher YesGluten-free YesLactose-free YesLow residue YesRenal sol. Load (m0sm/L) 491Osmolality (mOsm/kg H20) 665Min. tube size for gravity Pump feeding (Fr) 10/8
Ingredients (Vanilla): U-D Water, Corn Syrup Solids, High-Oleic Safflower Oil, Caseinates (Calcium, Magnesium and Sodium), Canola Oil, Sugar (Sucrose), Milk Protein Isolate, Fructooligosacharides, Soy Lecithin, Natural and Artificial Flavors, Potassium Citrate, Calcium Carbonate, Sodium Citrate, Cellulose Gel, Choline Chloride, Salt (Sodium Chloride), Ascorbic Acid, L-Carnitine, Taurine, Calcium Phosphate Tribasic, Cellulose Gum, Zinc Sulfate, Alpha-Tocopheryl Acetate, Ferrous Sulfate, Niacinamide, Gellan Gum, Calcium Pantothenate, Manganese Sulfate, Pyridoxine Hydrochloride, Cupric Sulfate, Thiamine Chloride Hydrochloride, Riboflavin, Beta-Carotene, Folic Acid, Vitamin A Palmitate, Biotin, Potassium Iodide, Sodium Selenate, Phylloquinone, Cyanocobalamin and Vitamin D3. Nutrition Information Per 8 fl oz Per LiterCalories 475 2000Protein, g 16.7 70Total Carbohydrate, g 52.8 222.7Dietary Fiber, g* 3.7 15.6Total Fat, g 22.7 95.6Water, g 166 699Vitamin A, IU 1000 4215Vitamin D, IU 20 85Vitamin E, IU 12 48Vitamin K, mcg 20 85Vitamin C, mg 25 105Folic Acid, mcg 250 1055Thiamin (Vitamin B1), mg 0.60 2.6Riboflavin (Vitamin B2), mg 0.68 2.9Vitamin B6, mg 2.1 8.9Vitamin B12, mcg 2.4 11Niacin, mg 8 34Choline, mg 150 635Biotin, mcg 120 510Pantothenic Acid, mg 4.0 17Sodium, mg 200 (8.7 mEq) 845 (36.7 mEq)Potassium, mg 250 (6.4 mEq) 1055 (27.1 mEq)Chloride, mg 240 (6.8 mEq) 1010 (28.5 mEq)Calcium, mg 325 1370Phosphorus, mg 165 695Magnesium, mg 50 215Iodine, mcg 38 160Manganese, mg 1.3 5.3Copper, mg 0.50 2.1Zinc, mg 5.7 24Iron, mg 4.5 19Selenium, mcg 24 105L-Carnitine, mg 62 261Taurine, mg 38 160* 3.7 g/8 fl oz (15.6 g/L) of FOS† 750 IU/8 fl oz (3160 IU/L) of vitamin A activity supplied by 0.57 mg/8 fl oz(2.4 mg/L) of β-carotene.Not for parenteral use.IndicationsSpecialized Complete Nutrition with FOSFor electrolyte and fluid restrictionsNepro is specifically designed to meet the nutrient needs and altered metabolism of people on dialysis.For tube or oral feeding.For supplemental or sole-source nutritionPackaging8-fl-oz-cans: 24/caseRoss Ready-To-Hang1000-ml. prefilled containers; 8/case

12
1500-ml prefilled containers; 6/case
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
OSMOLITE ®GeneralIsotonic NutritionFeatures- Complete and balanced nutrition - Low-residue, isotonic formula for those intolerant of hyperosmolar feedings- Provides at least 100% of the DVs for 24 essential vitamins and minerals in 2000 Cal (1887mL)Nutrient FactsNutrient density (Cal/ml) 1.06 Kosher YesProtein (% Cal) 14.0Gluten-free YesCarbohydrate (% Cal) 57.0Lactose-free YesFat (% Cal) 29.0Low residue YesNutrient base (Cal) 2000Renal sol load (mOsm/L) 289Nutrient base (ml) 1887Osmolality 300(mOsm/kg H20)Total Cal/g nitrogen 178:1Min. tube size for gravity/ Nonprotein Cal/g nitrogen 153:1Pump feeding (Fr) 8/5Water (g/L) 841Ingredients: (U)-D Water, Corn Maltodextrin, Sodium and Calcium Caseinates, High Oleic Sunflower Oil, Canola Oil, Soy Protein Isolate, Medium Chain Triglycerides, Potassium Citrate, Soy Lecithin, Magnesium Chloride, Calcium Phosphate, Ascorbic Acid, Carrageenan, Choline Chloride, Magnesium Sulfate, Sodium Citrate, Taurine, L-Carnitine, Zinc Sulfate, Ferrous Sulfate, dl-Alpha-Tocopheryl Acetate, Niacinamide, Calcium Pantothenate, Manganese Sulfate, Thiamine Chloride Hydrochloride, Cupric Sulfate, Pyridoxine Hydrochloride, Riboflavin, Vitamin A Palmitate, Folic Acid, Biotin, Chromium Chloride, Sodium Molybdate, Potassium Iodide, Sodium Selenate, Phyfloquinone, Cyanocobalamin and vitamin D3 (7682-08)IndicationsOSMOLITE is an isotonic, low-residue tube feeding.- For tube feeding- For supplemental or sole-source nutrition- May be used for oral feeding of patients with altered taste perceptionNutrition Per PerInformation 8 Fl oz LiterCalories 250 1060Protein, g 8.8 3 7.1Total Carbohydrate, g 35.6 151.1Total Fat, g 8.2 34.7Water, g 199 841Vitamin A, IU 625 2660Vitamin D, IU 50 215Vitamin E, IU 5.7 24Vitamin K, mcg 10 43Vitamin C, mg 38 160Folic Acid, mcg 100 425Thiamin 0.38
1.6
(Vitamin B1), mgRiboflavin 0.43 1.9(Vitamin B2), mgVitamin B6, mg 0.50 2.2Vitamin B12, mcg 1.5 6.4Niacin, mg 5.0 22Choline, mg 75 320Biotin, mcg 75 320Pantothenic Acid, mg 2.5 11Sodium, mg 150 1020
(6.5mEq)
(26.1 mEq)
Chloride, mg 200 850
(5.6 mEq)
(24 mEq)
Calcium, mg 125 535Phosphorus, mg 125 535Magnesium, mg 50 215Iodine, mcg 19 80Manganese, mg 0.62 2.7

13
Copper, mg 0.25 1.1Zinc, mg 2.9 12Iron, mg 2.3 9.6Selenium, mcg 9.0 38Chromium, mcg 15 64Molybdenum, mcg 19 80L-Carnitine, mg 19 80Taurine, mg 19 80Not for parenteral use.Packaging8-fl-oz cans;24/case32-fl-oz cans;6/caseRoss-Ready-To-Hang®1000-ml prefilled containers; 8/case
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
OXEPA ®GeneralFeatures- Calorically dense (1.5 Cal/ml)-to meet the elevated energy needs of patients who may not tolerate large-volume feeding- Unique, patented oil blend-contains 4.6g of EPA* and 4g of GLA,* fatty acids associated with the production of less proinflammatory eicosanoids- High in protein (62.7g/L)-a level to support protein synthesis and tissue repair- Elevated levels of antioxidants=needed during conditions of oxidative stress- Provides 100% of the DVs for 24 essential vitamins and minerals in 1420 Cal (4 cans)
Nutrient Facts
Nutrient density (Cal/ml) 1.5Protein (%Cal) 16.7Carbohydrate (% Cal) 28.1Fat (% Cal) 55.2Nutrient base (Cal) 1420Nutrient base (ml) 946
Total Cal/g nitrogen 150:1
Nonprotein Cal/g nitrogen 125:1
Water (g/L) 785Kosher YesGluten-free YesLactose-free YesLow residue YesRenal sol. Load (mOsm/L) 512Osmolality (mOsm/kg H20) 535Min. tube size for gravity/pump feeding (Fr) 10/8
Ingredients: (U)-D Water, Sodium and Calcium Caseinates, Sugar (Sucrose), Corn Maltodextrin, Canola Oil, Medium Chain Triglycerides, Refined Deodorized Sardine Oil, Borage Oil, Magnesium Chloride, Calcium Phosphate, Soy Lecithin, Potassium Citrate, Sodium Citrate, Potassium Phosphate, Ascorbic Acid, Natural and Artificial Flavor, Choline Chloride, Taurine, d-Alpha-Tocopheryl Acetate, L-Carnitine, Salt (Sodium Chloride),Gellan Gum, Zinc Sulfate, Ferrous Sulfate, Niacinamide, Calcium Pantothenate, Manganese Sulfate, Cupric Sulfate, Thiamine Chloride Hydrochlor, Pyridoxine Hydrochloride, Riboflavin, Beta-Carotene, Vitamin A Palmitate, Folic Acid, Biotin, Chromium Chloride, Sodium Molybdate, Potassium lodide, Sodium Selenate, Phylloquinone, Cyanocobalamin and Vitamin D3.Nutrition Information Per 8 fl oz Per LiterCalories 355 1500Protein, g 14.8 62.7Total Carbohydrate, g 25.0 105.3Total Fat, g 22.2 93.8Water, g 186 785Vitamin A, IU† 2820 11,910Vitamin D, IU 100 425Vitamin E, IU 75 320Vitamin K, mcg 20 85Vitamin C, mg 200 850Folic Acid, mcg 200 850Thiamin (Vitamin B1), mg 0.75 3.2Riboflavin (Vitamin B2), mg 0.85 3.6Vitamin B6 mg 1.0 4.3Vitamin B12 mcg 3.0 13Niacin, mg 10 43Choline, mg 150 635

14
Biotin, mcg 150 635Pantothenic Acid, mg 5.0 22Sodium, mg 310 (13.5 mEq) 1310 (57.0 mEq)Potassium, mg 465 (11.9 mEq) 1960 (50.1 mEq)Chloride, mg 400 (11.3 mEq) 1690 (47.7 mEq)Calcium, mg 250 1060Phosphorus, mg 250 1060Magnesium, mg 100 425Iodine, mcg 38 160Manganese, mg 1.3 5.3Copper, mg 0.50 2.2Zinc, mg 5.7 24Iron, mg 4.5 20Selenium, mcg 18 74Chromium, mcg 30 130Molybdenum, mcg 38 160L-Carnitine, mg 43 185Taurine, mg 75 320* EPA = eicosapentaenoic acid (from sardine oil), and GLA = gamma-linolenic acid (from borage oil).† 1590 IU/8 fl ox (6625 IU/L) of vitamin A activity supplied by 1.2 mg/8 fl oz (5.0 mg/L) of B-carotene.Not for parenteral use.IndicationsSpecialized Nutritionfor modulating inflammation in the mechanically ventilated, critically illOXEPA is a unique formula clinically shown to modulated the inflammatory response in critically ill patients (APACHE II >15) with SIRS (systemic inflammatory response syndrome), sepsis, ALI (acute lung injury), or ARDS (acute respiratory distress syndrome).- For tube feeding- For sole-source nutritionPackaging8-fl-ox cans; 24/caseRoss Ready-To-Hang ®100-ml, prefilled containers; 8/case
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
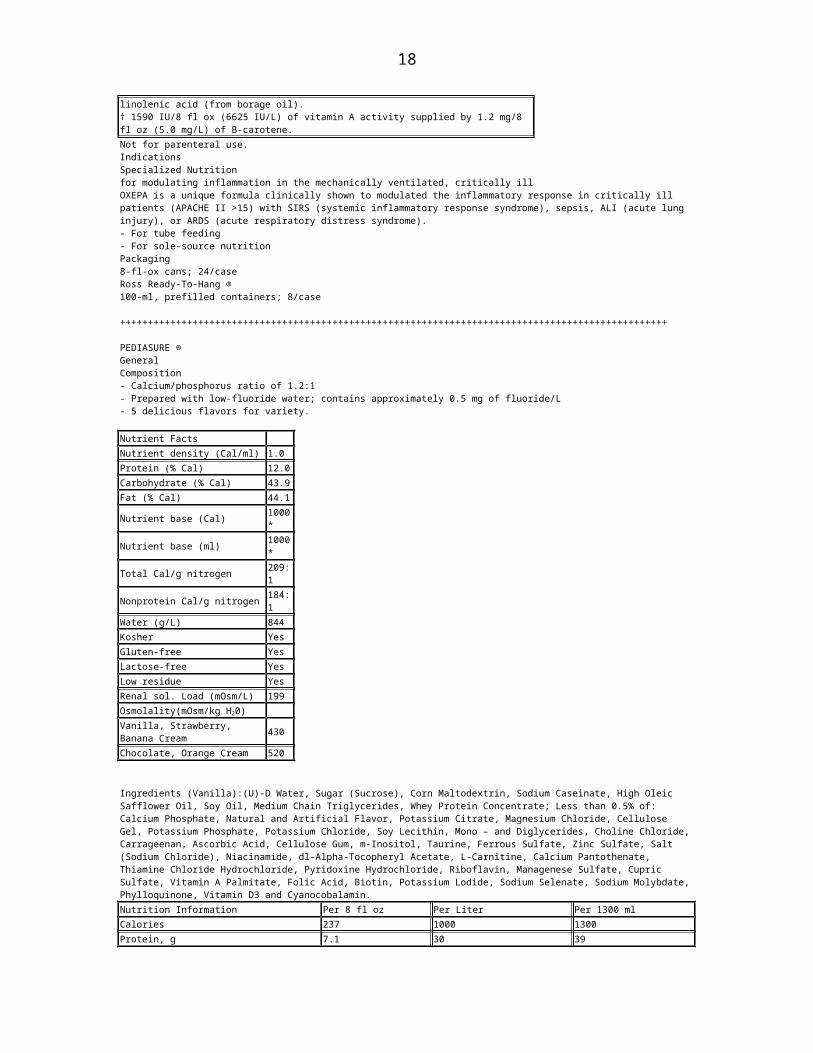
PEDIASURE ®GeneralComposition- Calcium/phosphorus ratio of 1.2:1- Prepared with low-fluoride water; contains approximately 0.5 mg of fluoride/L- 5 delicious flavors for variety.
Nutrient Facts
Nutrient density (Cal/ml) 1.0Protein (% Cal) 12.0Carbohydrate (% Cal) 43.9Fat (% Cal) 44.1Nutrient base (Cal) 1000*Nutrient base (ml) 1000*
Total Cal/g nitrogen 209: 1
Nonprotein Cal/g nitrogen 184:1Water (g/L) 844Kosher YesGluten-free YesLactose-free YesLow residue YesRenal sol. Load (mOsm/L) 199
Osmolality(mOsm/kg H20)
Vanilla, Strawberry, Banana Cream 430
Chocolate, Orange Cream 520 Ingredients (Vanilla):(U)-D Water, Sugar (Sucrose), Corn Maltodextrin, Sodium Caseinate, High Oleic Safflower Oil, Soy Oil, Medium Chain Triglycerides, Whey Protein Concentrate; Less than 0.5% of: Calcium Phosphate, Natural and Artificial Flavor, Potassium Citrate, Magnesium Chloride, Cellulose Gel, Potassium Phosphate, Potassium Chloride, Soy Lecithin, Mono – and Diglycerides, Choline Chloride, Carrageenan, Ascorbic Acid, Cellulose Gum, m-Inositol, Taurine, Ferrous Sulfate, Zinc Sulfate, Salt (Sodium Chloride), Niacinamide, dl-Alpha-Tocopheryl Acetate, L-Carnitine, Calcium Pantothenate, Thiamine Chloride Hydrochloride, Pyridoxine Hydrochloride, Riboflavin,

15
Managenese Sulfate, Cupric Sulfate, Vitamin A Palmitate, Folic Acid, Biotin, Potassium Lodide, Sodium Selenate, Sodium Molybdate, Phylloquinone, Vitamin D3 and Cyanocobalamin.Nutrition Information Per 8 fl oz Per Liter Per 1300 mlCalories 237 1000 1300Protein, g 7.1 30 39Total Carbohydrate, g 26.0 109.7 142.6Total Fat, g 11.8 49.8 64.7Water, g 200 844 1097Vitamin A, IU 610 2574 3346Vitamin D, IU 120 506 658Vitamin E, IU 5.4 23 30Vitamin K, mcg 9.0 38 49Vitamin C, mg 24 101 132Folic Acid, mcg 88 371 483Thiamin (Vitamin B1), mg 0.64 2.7 3.5Riboflavin (Vitamin B2), mg 0.50 2.1 2.7Vitamin B6, mg 0.62 2.6 3.4Vitamin B12, mcg 1.4 5.9 7.7Niacin, mg 4.0 17 22Choline, mg 71 300 389Biotin, mcg 76 321 417Pantothenic Acid, mg 2.4 10 13m-Inositol, mg 19 80 104Sodium, mg 90 (3.9mEq) 380 (16.5mEq) 494 (21.5 mEq)Potassium, mg 310 (7.9mEq) 1308 (33.5 mE1q) 1700 (43.5 mEq)Chloride, mg 240 (6.7 mEq) 1013 (28.6 mEq) 1316 (37.1 mEq)Calcium, mg 230 970 1262Phosphorus, mg 190 802 1042Magnesium, mg 47 198 258Iodine, mcg 23 97 126Manganese, mg 0.24 1.0 1.3Copper, mg 0.24 1.0 1.3Zinc, mg 2.8 12 15Iron, mg 3.3 14 18Selenium, mcg 5.4 23 30Chromium, mcg 7.1 30 39Molybdenum, mcg 8.5 36 47L-Carnitine, mg 4 17 22Taurine, mg 17 72 93* PEDIASURE meets or exceeds 100% of the NAS/NRC RDAs for children 1 to 6 years of age in 1000 Calories (1000mL) and for children 7 to 10 years of age in 1300 Calories (1300 ml).Not for parenteral useIndicationsComplete, Balance Nutrition ®for children 1-10 yearsGreat-tasting, “Kid Approved” PEDIASURE encourages compliance among children who are orally fed. It is designed as a source of complete, balanced nutrition for children who may be undernourished due to illness or poor appetite. PEDIASURE is formulated to support catch-up growth in children with failure-to-thrive and is well tolerated.Great-tasting “Kid Approved” recipes are available in PediaSure.com- For supplemental or sole-source oral nutrition- NOT for children with galactosemiaPackaging8-fl-ox cans; 24/caseVanillaChocolateStrawberryBanana CreamOrange CreamVanillaChocolateStrawberryBanana CreamOrange Cream
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
PEDIASURE ENTERAL ®GeneralComposition- Calcium/phosphorus ratio of 1.2:1- Prepared with low-fluoride water; contains approximately 0.5mg of fluoride/L- Provides 1.9 g of dietary fiber/8 fl oz

16
- Includes 0.7g of FOS/8 fl oz (3.0 g/L and 4.5g/1500mL). FOS are prebiotics that stimulate the growth of beneficial bacteria in the colon (see page 9 for more about FOS)Nutrient FactsNutrient density (Cal/ml) 1.0Protein (% Cal) 12.0Carbohydrate (% Cal) 53.0Fat (% Cal) 35.0
Nutrient base (Cal) 1000*
Nutrient base (ml) 1000*
Total Cal/g nitrogen 209:1Nonprotein Cal/g nitrogen 184:1Water (g/L) 848Kosher YesGluten-free YesLactose-free YesLow residue NoLow residue NoOsmolality (mOsm/kg H2O) 345Min. tube size for gravity/pump feeding (Fr) 10/8
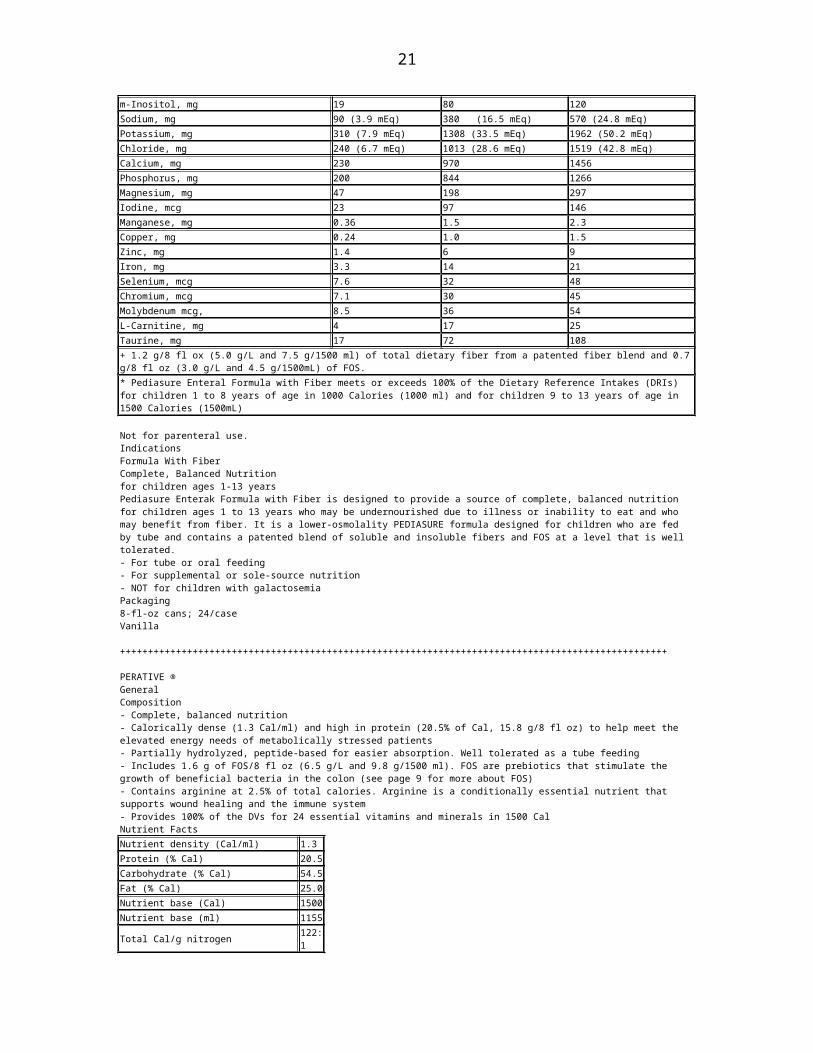
Ingredients: (U)-D Water, Corn Maltodextrin, Milk Protein Concentrate, Sugar (Sucrose), High Oleic Safflower oil, Soy Oil, Medium Chain Triglycerides; Less than 0.5% of: Fructooligosaccharides, Natural and Artificial Flavor, Oat Fiber, Dextrose, Soy Fiber, Potassium Citrate, Magnesium Phosphate, Gum Arabic, Salt (Sodium Chloride), Potassium Chloride, Calcium Phosphate, Potassium Phosphate, Cellulose Gum, Choline Chloride, Soy Lecithin, Mono-and Diglycerides, Ascorbic Acid, Carrageenan, m-Inositol, Taurine, Ferrous Sulfate, Dl-Alpha-Tocopheryl Acetate, L-Carnitine, Zinc Sulfate, Calcium Pantothenate, Niacinamide, Manganese Sulfate, Thiamine Chloride Hydrochloride, Pyridoxine Hydrochloride, Riboflavin, Cupric Sulfate, Vitamin A Palmitate, Folic Acid, Biotin, Chromium Chloride, Potassium Iodide, Sodium Selenate, Sodium Molybdate, Phylloquinone, Vitamin D3 and Cyanocobalamin.Nutrition Information per 8 fl oz Per Liter Per 1500 mlCalories 237 1000 1500Protein, g 7.1 30 44.9Total Carbohydrate, g 32.7 138.0 207.0Dietary Fiber, g† 1.9 8.0 12.0Total Fat, g 9.4 39.7 59.5Water, g 201 848 1272Vitamin A, IU 380 1603 2405Vitamin D, IU 120 506 759Vitamin E, IU 5.4 22.8 34.2Vitamin K, mcg 14 59 89Vitamin C, mg 24 101 152Folic Acid, mcg 71 300 449Thiamin (Vitamin B1), mg 0.64 2.7 4.1Riboflavin (Vitamin B2), mg 0.50 2.1 3.2Vitamin B6, mg 0.62 2.6 3.9Vitamin B12, mcg 1.4 5.9 8.9Niacin, mg 2.4 10 15Choline, mg 71 300 449Biotin, mcg 76 321 481Pantothenic Acid, mg 2.4 10 15m-Inositol, mg 19 80 120Sodium, mg 90 (3.9 mEq) 380 (16.5 mEq) 570 (24.8 mEq)Potassium, mg 310 (7.9 mEq) 1308 (33.5 mEq) 1962 (50.2 mEq)Chloride, mg 240 (6.7 mEq) 1013 (28.6 mEq) 1519 (42.8 mEq)Calcium, mg 230 970 1456Phosphorus, mg 200 844 1266Magnesium, mg 47 198 297Iodine, mcg 23 97 146Manganese, mg 0.36 1.5 2.3Copper, mg 0.24 1.0 1.5Zinc, mg 1.4 6 9Iron, mg 3.3 14 21Selenium, mcg 7.6 32 48Chromium, mcg 7.1 30 45Molybdenum mcg, 8.5 36 54L-Carnitine, mg 4 17 25Taurine, mg 17 72 108+ 1.2 g/8 fl ox (5.0 g/L and 7.5 g/1500 ml) of total dietary fiber from a patented fiber blend and 0.7 g/8 fl oz (3.0 g/L and 4.5 g/1500mL) of

17
FOS.* Pediasure Enteral Formula with Fiber meets or exceeds 100% of the Dietary Reference Intakes (DRIs) for children 1 to 8 years of age in 1000 Calories (1000 ml) and for children 9 to 13 years of age in 1500 Calories (1500mL) Not for parenteral use.IndicationsFormula With FiberComplete, Balanced Nutritionfor children ages 1-13 yearsPediasure Enterak Formula with Fiber is designed to provide a source of complete, balanced nutrition for children ages 1 to 13 years who may be undernourished due to illness or inability to eat and who may benefit from fiber. It is a lower-osmolality PEDIASURE formula designed for children who are fed by tube and contains a patented blend of soluble and insoluble fibers and FOS at a level that is well tolerated.- For tube or oral feeding- For supplemental or sole-source nutrition- NOT for children with galactosemiaPackaging8-fl-oz cans; 24/caseVanilla
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
PERATIVE ®GeneralComposition- Complete, balanced nutrition- Calorically dense (1.3 Cal/ml) and high in protein (20.5% of Cal, 15.8 g/8 fl oz) to help meet the elevated energy needs of metabolically stressed patients- Partially hydrolyzed, peptide-based for easier absorption. Well tolerated as a tube feeding- Includes 1.6 g of FOS/8 fl oz (6.5 g/L and 9.8 g/1500 ml). FOS are prebiotics that stimulate the growth of beneficial bacteria in the colon (see page 9 for more about FOS)- Contains arginine at 2.5% of total calories. Arginine is a conditionally essential nutrient that supports wound healing and the immune system- Provides 100% of the DVs for 24 essential vitamins and minerals in 1500 CalNutrient FactsNutrient density (Cal/ml) 1.3Protein (% Cal) 20.5Carbohydrate (% Cal) 54.5Fat (% Cal) 25.0Nutrient base (Cal) 1500Nutrient base (ml) 1155
Total Cal/g nitrogen 122:1
Nonprotein Cal/g nitrogen 97:1Water (g/L) 790Kosher YesGluten-free YesLactose-free YesLow residue YesRenal sol. Load (mOsm/L) 516Osmolality (mOsm/kg H2O) 460Min. tube size for gravity/Pump feeding (Fr) 10/8
Ingredients: (U)-D Water, Corn Maltodextrin, Partially Hydrolyzed Sodium Caseinate, Hydrolyzed Lactalbumin, Canola Oil, Medium Chain Triglycerides, Fructooligosaccharides, L-Arginine, Corn Oil, Magnesium Chloride, Potassium Citrate, Calcium Phosphate, Citric Acid, Soy Lecithin, Ascorbic Acid, Potassium Phosphate, Choline Chloride, Carrageenan, Potassium Chloride, Taurine, L-Carnitine, Zinc Sulfate, Ferrous Sulfate, dl-Alpha-Tocopheryl Acetate, Niacinamide, Calcium Pantothenate, Manganese Sulfate, Cupric Sulfate, Thiamine Chloride Hydrochloride, Pyridoxine Hydrochloride, Beta-Carotene, Riboflavin, Vitamin A Palmitate, Folic Acid, Biotin, Chromium Chloride, Sodium Molybdate, Potassium Lodide, Sodium Selenate, Phylloquinone, Cyanocobalamin and Vitamin D3.Nutrition Information Per 8 fl oz Per Liter Per 1500mLCalories 308 1300 1950Protein, g 15.8 66.7 100.0Total Carbohydrate, g 42.8 180.3 270.4Dietary Fiber, g* 1.6 6.5 9.8Total Fat, g 8.8 37.3 56.0Water, g 187 790 1185Vitamin A, IU† 2055 8675 13,005Vitamin D, IU 83 350 525Vitamin E, IU 9.3 40 60Vitamin K, mcg 17 70 105Vitamin C, mg 62 260 395Folic Acid, mcg 125 520 785Thiamin (Vitamin B1), mg 0.47 2.0 3.0
18
Riboflavin (Vitamin B2), mg 0.53 2.3 3.4Vitamin B6, mg 0.62 2.6 3.9Vitamin B12, mcg 1.9 7.9 12Niacin, mg 6.2 27 4 0Choline, mg 125 520 785Biotin, mcg 93 395 590Pantothenic Acid, mg 3.1 14 20Sodium, mg 245 (10.7mEq) 1040 (45.2 mEq) 1560 (67.9 mEq)Potassium, mg 410 (10.5 mEq) 1735 (44.5 mEq) 2600 (66.5 mEq)Chloride, mg 390 (11.0 mEq) 1650 (46.5 mEq) 2470 (69.7 mEq)Calcium, mg 210 870 1305Phosphorus, mg 210 870 1305Magnesium, mg 83 350 525Iodine, mcg 31 135 200Manganese, mg 1.1 4.4 6.5Copper, mg 0.42 1.8 2.6Zinc, mg 4.7 20 30Iron, mg 3.7 16 24Selenium, mcg 15 61 92Chromium, mcg 25 105 160Molybdenum, mcg 31 135 200L-Carnitine, mg 31 135 200Taurine, mg 31 135 200* 1.6 g/8 fl oz (6.5 g/L and 9.8 g/1500 ml) of FOS.† 1325 IU/8 fl oz (5565 IU/L and 8350 IU/1500 ml) of vitamin A activity supplied by 1.0 mg/8 fl oz (4.2 mg/L and 6.3 mg/1500mL) of β-carotene.Not for parenteral use.IndicationsSpecialized Nutritionwith partially hydrolyzed proteins and FOS for metabolic stress.Perative is a complete, balanced, ready-to-feed formula designed for metabolically stressed patients with pressure ulcers, multiple fractures, wounds, burns, or surgery who can benefit from supplemental arginine. When used in the critically ill, PERATIVE is for patients with an APACHE II score <15 and without pneumonia, sepsis, or SIRS (systemic inflammatory response syndrome).- For tube feeding- For supplemental or sole-source nutritionPackaging- 8-fl-oz cans; 24/case- Ross Ready-To-Hang® 100-ml prefilled containers; 8/case- 1500-ml prefilled containers; 6/case
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
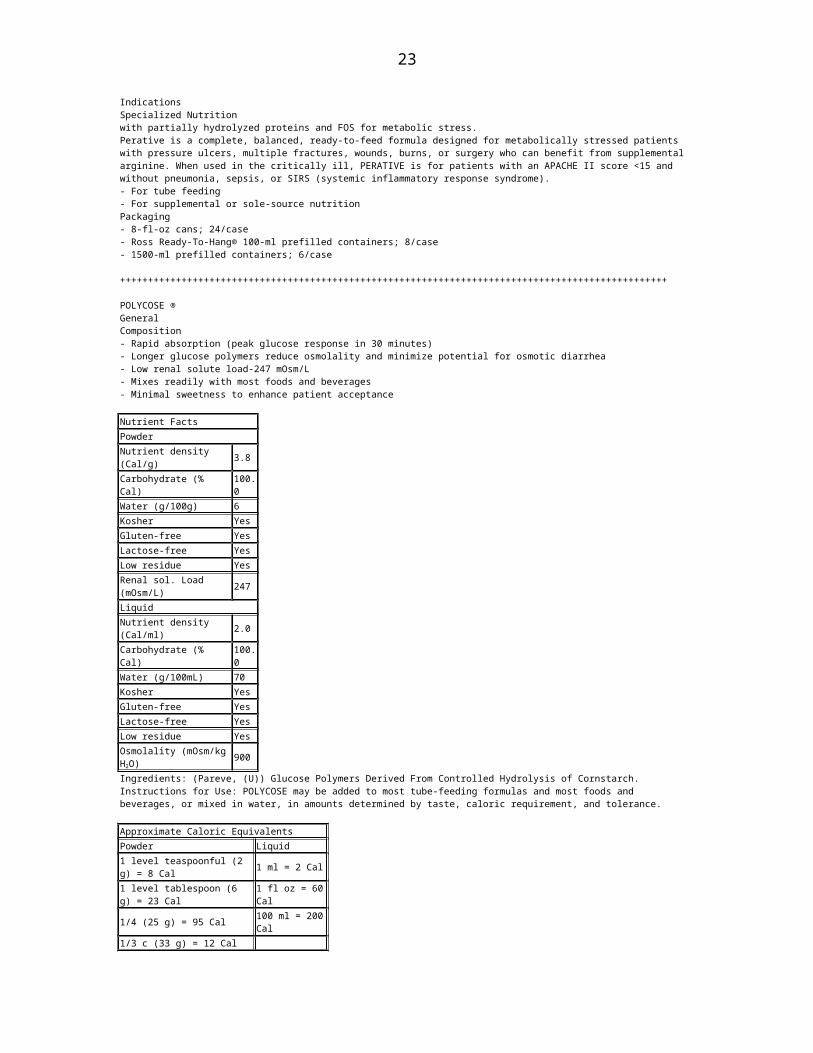
POLYCOSE ®GeneralComposition- Rapid absorption (peak glucose response in 30 minutes)- Longer glucose polymers reduce osmolality and minimize potential for osmotic diarrhea- Low renal solute load-247 mOsm/L- Mixes readily with most foods and beverages- Minimal sweetness to enhance patient acceptance Nutrient FactsPowderNutrient density (Cal/g) 3.8
Carbohydrate (% Cal) 100.0
Water (g/100g) 6Kosher YesGluten-free YesLactose-free YesLow residue YesRenal sol. Load (mOsm/L) 247LiquidNutrient density (Cal/ml) 2.0
Carbohydrate (% Cal) 100.0
Water (g/100mL) 70Kosher YesGluten-free YesLactose-free YesLow residue Yes

19
Osmolality (mOsm/kg H2O) 900
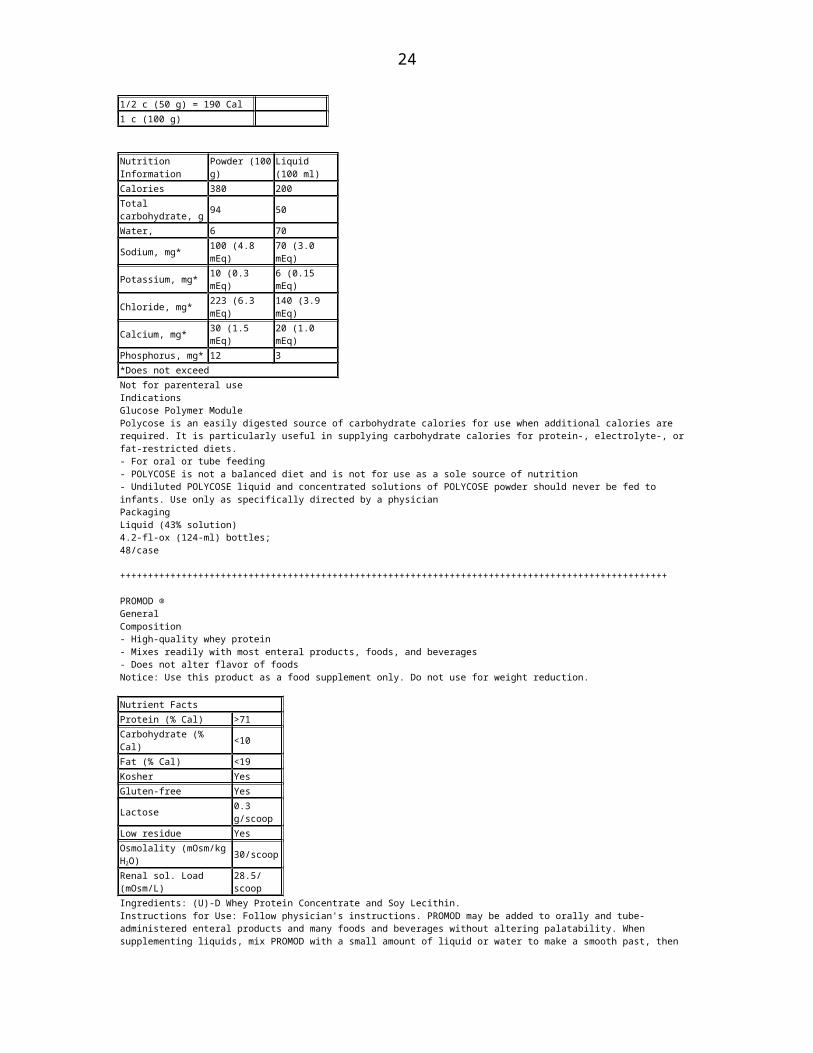
Ingredients: (Pareve, (U)) Glucose Polymers Derived From Controlled Hydrolysis of Cornstarch.Instructions for Use: POLYCOSE may be added to most tube-feeding formulas and most foods and beverages, or mixed in water, in amounts determined by taste, caloric requirement, and tolerance. Approximate Caloric EquivalentsPowder Liquid1 level teaspoonful (2 g) = 8 Cal 1 ml = 2 Cal1 level tablespoon (6 g) = 23 Cal 1 fl oz = 60 Cal
1/4 (25 g) = 95 Cal 100 ml = 200 Cal
1/3 c (33 g) = 12 Cal
1/2 c (50 g) = 190 Cal
1 c (100 g)
Nutrition Information Powder (100 g)
Liquid (100 ml)
Calories 380 200Total carbohydrate, g 94 50
Water, 6 70Sodium, mg* 100 (4.8 mEq) 70 (3.0 mEq)Potassium, mg* 10 (0.3 mEq) 6 (0.15 mEq)Chloride, mg* 223 (6.3 mEq) 140 (3.9 mEq)Calcium, mg* 30 (1.5 mEq) 20 (1.0 mEq)Phosphorus, mg* 12 3*Does not exceedNot for parenteral useIndicationsGlucose Polymer ModulePolycose is an easily digested source of carbohydrate calories for use when additional calories are required. It is particularly useful in supplying carbohydrate calories for protein-, electrolyte-, or fat-restricted diets.- For oral or tube feeding- POLYCOSE is not a balanced diet and is not for use as a sole source of nutrition- Undiluted POLYCOSE liquid and concentrated solutions of POLYCOSE powder should never be fed to infants. Use only as specifically directed by a physicianPackagingLiquid (43% solution)4.2-fl-ox (124-ml) bottles;48/case
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
PROMOD ®GeneralComposition- High-quality whey protein- Mixes readily with most enteral products, foods, and beverages- Does not alter flavor of foodsNotice: Use this product as a food supplement only. Do not use for weight reduction. Nutrient FactsProtein (% Cal) >71Carbohydrate (% Cal) <10Fat (% Cal) <19Kosher YesGluten-free Yes
Lactose 0.3 g/scoop
Low residue YesOsmolality (mOsm/kg H2O) 30/scoop
Renal sol. Load (mOsm/L) 28.5/scoopIngredients: (U)-D Whey Protein Concentrate and Soy Lecithin.Instructions for Use: Follow physician's instructions. PROMOD may be added to orally and tube-administered enteral products and many foods and beverages without altering palatability. When supplementing liquids, mix PROMOD with a small amount of liquid or water to make a smooth past, then gradually add the remaining liquid while stirring. For blender mixing, combine PROMOD with the desired amount of liquid and briefly blend at the lowest speed to minimize foaming. Mix PROMOD directly into prepared foods such as soup, gravy, oatmeal, yogurt, mashed potatoes, or cottage cheese.

20
Approximate Protein Equivalents for Household MeasuresAmount of PROMOD Protein Supplement
Amount of Protein (g)
1 scoop (6.6g) 51 Level teaspoonful (1.3g) 11 level tablespoonful (4.0g) 31/4 cup (16 g) 121/3 cup (22 g) 161/2 cup (32 g) 241 cup (64 g) 48
Nutrition Information Per 5 g Protein (One 6.6-g Scoop)
Calories 28Protein, g 5.0Total carbohydrates, g* 0.67
Total fat, g* 0.60Water, g* 0.60Sodium, mg* 25 (1.09 mEq)Potassium, mg* 45 (1.15 mEq)Calcium, mg* 65 (3.24 mEq)Phosphorus, mg* 35 Amino acid ProfileEssential g/
100gProtein g/
100gNonessential ProteinHistidine 1.9 Alamine 5.3Isoleucine 6.2 Arginine 2.6Leucine 10.8 Aspartic Acid 11.2Lysine 9.3 Cystine 2.6
Methionine 2.2 Glutamic Acid 18.2
Phenylalanine 3.6 Glycine 2.1
Threonine 7.3 Proline 6.5Tryptophan 1.9 Serine 5.6Valine 6.0 Tyrosine 3.4*Does not exceedNot for parenteral useIndicationsProtein ModulePROMOD is a source of concentrated, high-quality whey protein for people with increased protein needs for people with increased protein needs or those unable to meet their protein needs with a normal diet.- For use with oral diets or tube feedings- PROMOD is not a balance diet and is not for use as a sole source of nutritionRoss is a proud sponsor of America's Walk for Diabetes.PackagingPowder (41 scoops/can)9.7-oz (275-g) cans; 6/case
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
PROSURE THERAPEUTIC NUTRITION ™GeneralCompositionPer 8-fl-oz can:- 1 g of EPA to help normalize metabolism- 16 g of protein to help build lean body mass- 5 g of dietary fiber, including 2.4 g of FOS.FOS are prebiotics that stimulate the growth of beneficial bacterial in the colon (see page 9 for more about FOS)- 2 flavors-Vanilla and Banana- selected by people with cancerNutrient FactsNutrient density (Cal/ml) 1.27Protein (% Cal) 21Carbohydrate (% Cal) 61Fat (% Cal) 18
Total Cal/g nitrogen 117.1
21
Nonprotein Cal/g nitrogen 92.1Water (g/8 fl oz) 186Gluten-free YesLactose-free YesRenal sol. Load (mOsm/L) 545Osmolality (mOsm/kg H2O) 635
Ingredients (Vanilla): Water, Corn Syrup Solids, Sodium Caseinate, Hydrolyzed Sodium Caseinate, Maltodextrin (Corn), Sugar (Sucrose), Sardine Oil, Fructooligosaccharides, Gum Arabic, Whey Protein Concentrate, Medium-Chain Triglycerides (Franctionated Coconut Oil), Calcium Phosphate Tribasic, Potassium Citrate, Natural and Artificial Flavors, Magnesium Chloride, Canola Oil, Soy Fiber, Sodium Citrate, Soybean Oil, Lecithin, Ascorbic Acid, Choline Chloride, Magnesium Sulfate, Taurine, Alpha-Tecopheryl Acetate, L-Carnitine, Zinc Sulfate, Ferrous Sulfate, Gellan Gum, Niacinamide, Calcium Pantothenate, Manganese Sulfate, Cupric Sulfate, Thiamine Chloride Hydrochloride, Pyridoxine Hydrochloride, Beta-Carotene, Riboflavin, Vitamin A Palmitate, Folic Acid, Biotin, Chromium Chloride, Sodium Molybdate, Sodium Selenate, Potassium Lodide, Phylloquinone, Vitamin D3 and Cyanocobalamin.Nutrition Information Per 8 fl ozCalories 300Protein, g 16Total Carbohydrate, g* 48Dietary Fiber, g 5Sugars, g 8Total Fat, g 6Saturated Fat, g 2Vitamin A, IU+ 2524Vitamin D, IU 160Vitamin E, IU 75Vitamin K, mcg 20Vitamin C, mg 105Folic Acid, mcg 300Thiamin (Vitamin B1), mg 0.60Riboflavin (Vitamin B2), mg 0.68Vitamin B6, mg 0.80Vitamin B12, mcg 2.40Niacin, mg 2.40Choline, mg 120Biotin, mg 120Pantothenic Acid, mg 4Sodium, mg 360 (15.7mEq)Potassium, mg 470 (12.0 mEq)Chloride, mg 360 (10.2 mEq)Calcium, mg 350Phosphorus, mg 250Magnesium, mg 100Iodine, mcg 37.5Manganese, mg 1.3Copper, mg 0.5Zinc, mg 6Iron, mg 4.5Selenium, mcg 17.5Chromium, mcg 30Molybdenum, mcg 37.5L-Carnitine, mg 30Taurine, mg 45
* 2.6 g of total dietary fiber from a fiber blend and 2.4 g of FOS.+1460 IU of vitamin A activity supplied by 1.1 mg of B-carotene.
Not for parental use.IndicationsPROSURE is the only therapeutic nutritional clinically shown to help build muscle and increase strength in those who gained weight. Unlike other nutritional beverages, PROSURE is a specialized, patented formula that is high in protein and contains the omega-3 fatty acid eicosapentaenoic acid (EPA)- shown to help normalize metabolism, promote weight gain, and build lean body mass.A clinical study among people with cancer showed that drinking PROSURE daily as part of overall care promoted weight gain and increased strength in those who gained weight, helped build muscle, increased physical activity level, and improved quality of life.Results in some patients may be seen in as few as 3 weeks with as little as 2 cans daily.- For use with oral diets or tube feedings- Not for use as a sole source of nutritionPackaging

22
8-fl-oz cans;4 cans/carton;24/caseVanillaVanillaBanana
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
PULMOCARE ®GeneralComposition- Complete, balance nutrition- Contains 20% of fat as MCTs to enhance fat absorption- Meets 100% of the DVs for 24 essential vitamins and minerals in 4 cans- Provides a balanced mixture of polyunsaturated, monounsaturated, and saturated fatty acids.- Fortified with the antioxidants all-natural vitamin E/R,R,R-alpha-tocopherol and beta-carotene. Nutrient FactsNutrient density (Cal/ml) 1.5Protein (% Cal) 16.7Carbohydrate (% Cal) 28.2Fat (% Cal) 55.1Nutrient base (Cal) 1420Nutrient base (ml) 947
Total Cal/g nitrogen 150: 1
Nonprotein Cal/g nitrogen 125:1Water (g/L) 785Kosher YesGluten-free YesLactose-free YesLow residue YesRenal sol. Load (mOsm/L) 512Osmolality (mOsm/kg H2O) 475Min, tube size for gravity/pump feeding (Fr) 10/8
Ingredients: (U)-D Water, Sodium and Calcium Caseinates, Sugar (Sucrose), Canola Oil, Corn Maltodextrin, Medium Chain Triglycerides, Corn Oil, High Oleic Safflower Oil, Magnesium Choride, Calcium Phosphate, Soy Lecithin, Potassium Citrate, Natural and Artificial Flavors, Sodium Citrate, Potassium Phosphate, Choline Chloride, Ascorbic Acid, Carrageenan, Taurine, L-Carnitine, Salt (Sodium Chloride), Zinc Sulfate, d-Alpha-Tocopheryl Acetate, Ferrous Sulfate, Niacinamide, Calcium Pantothenate, Manganese Sulfate, Cupric Sulfate, Thiamine Chloride Hydrochloride, Pyridoxine Hydrochloride, Riboflavin, Beta-Carotene, Vitamin A Palmitate, Folic Acid, Biotin, Chromium Chloride, Sodium Molybdate, Potassium Iodide, Sodium Selenate, Phylloquinone, Cyanocobalamin and Vitamin D3. Nutrition Information Per 8 fl oz Per LiterCalories 355 1500Protein, g 14.8 62.6Total Carbohydrate (% Cal) 25.0 105.7Total Fat, g 22.1 93.3Water, g 186 785Vitamin A, IU* 2840 11,910Vitamin D, IU 100 425Vitamin E, IU 20 85Vitamin K, mcg 20 85Vitamin C, mg 75 320Folic Acid, mcg 200 850Thiamin (Vitamin B1), mg 0.75 3.2Riboflavin (Vitamin B2), mg 0.85 3.6Vitamin B6, mg 1.0 4.3Vitamin B12, mcg 3.0 13Niacin, mg 10 43Choline, mg 150 635Biotin, mcg 150 635Pantothenic Acid, mg 5.0 22Sodium, mg 310 (13.5mEq) 1310 (57.0 mEq)Potassium, mg 465 (11.9 mEq) 1960 (50.1 mEq)Chloride, mg 400 (11.3 mEq) 1690 (47.7 mEq)Calcium, mg 250 1060Phosphorus, mg 250 1060Magnesium, mg 100 425
23
Iodine, mcg 38 160Manganese, mg 1.3 5.3Copper, mg 0.50 2.2Zinc, mg 5.7 24Iron, mg 4.5 19Selenium, mcg 18 74Chromium, mcg 30 130Molybdenum, mcg 38 160L-Carnitine, mg 36 160Taurine, mg 36 160* 1590 IU/8 fl oz (6625 IU/L) of vitamin A activity supplied by 1.2 mg/8 fl oz (5.0 mg/L) of β-carotene.Not for parenteral use.IndicationsSpecialized Nutrition for Pulmonary PatientsPULMOCARE is a low-carbohydrate formula specifically designed to reduce carbon dioxide production, thereby minimizing CO2 retention resulting from chronic obstructive pulmonary disease, cystic fibrosis, or respiratory failure. PULMOCARE is appropriate for ambulatory or ventilator-dependent patients.- For tube or oral feeding- For supplemental or sole-source nutritionCOPD is a chronic condition affecting 16 million people in the US. Pulmocare was the first enteral nutritional product designed to meet the needs of patients with COPD!Packaging8-fl-oz cans; 24/caseVanillaStrawberryRoss Ready-To-Hang®1000-ml prefilledcontainers; 8/case
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
SUPLENA ®GeneralComposition- Complete, balanced nutrition for people with chronic or acute kidney failure who are not receiving dialysis.- Calorically dense-2 Cal/ml- Low in protein- 8 fl oz provides at least 25% of recommended levels of vitamins/minerals for pre-dialysis patients- Low in vitamins A and D and high in folic acid and vitamin B6 to accommodate the altered metabolism of people with kidney failure who are not on dialysis- High in calcium, low in phosphorus; 1.9:1 Ca/P ratio to help optimize calcium and phosphorus balanceNutrient FactsNutrient density (Cal/ml) 2.0Protein (% Cal) 6.0Carbohydrate (% Cal) 51.0Fat (% Cal) 43.0Nutrient base (Cal) 1900Nutrient base (ml) 947
Total Cal/g nitrogen 418:1
Nonprotein Cal/nitrogen 393:1
Water (g/L) 713Kosher YesGluten-free YesLactose-free YesLow residue YesRenal Sol. Load (m)sm/L) 260Osmolality (mOsm/kg H2O) 600Min. tube size for gravity/Pump feeding (Fr) 10/8
Ingredients: (U)-D Water, Maltodextrin (Corn), High-Oleic Safflower Oil, Sodium Caseinate, Sugar (Sucrose), Soy Oil, Calcium Caseinate, Soy Lecithin, Natural and Artificial Flavors, Calcium Carbonate, Potassium Citrate, Magnesium Phosphate Dibasic, Calcium Phosphate Tribasic, Choline Chloride, Salt (Sodium Chloride), Ascorbic Acid, Taurine, Carrageenan, L-Carnitine, Potassium Chloride, Zinc Sulfate, Alpha-Tocopheryl Acetate, Ferrous Sulfate, Niacinamide, Calcium Pantothenate, Manganese Sulfate, Pyridoxine Hydrochloride, Cupric Sulfate, Thiamine Chloride Hydrochloride, Riboflavin, Folic Acid, Vitamin A Palmitate, Biotin, Potassium Iodine, Sodium Selenite, Phylloquinone, Cyanocobalamin and Vitamin D3.Nutrition Information Per 8 fl oz Per LiterCalories 475 2000Protein, g 7.1 30.0Total Carbohydrate, g 60.6 255.2
24
Total Fat, g 22.7 95.6Water, g 169 713Vitamin A, IU 250 1060Vitamin D, IU 20 85Vitamin E, IU 12 48Vitamin K, mcg 20 85Vitamin C, mg 25 86Folic Acid, mcg 250 1060Thiamin (Vitamin B1), mg 0.60 2.6Riboflavin (Vitamin B2), mg 0.68 2.9
Vitamin B6, mg 2.1 8.5Vitamin B12, mcg 2.4 11Niacin, mg 8.0 34Choline, mg 150 635Biotin, mcg 120 510Pantothenic Acid, mg 4.0 17
Sodium, mg 185 (8.0 mEq) 790 (34.3 mEq)
Potassium, mg 265 (6.8 mEq)
1120 (28.6 mEq)
Chloride, mg 220 (6.2 mEq) 935 (26.3 mEq)
Calcium, mg 330 1390Phosphorus, mg 175 730Magnesium, mg 50 215Iodine, mcg 38 160Manganese, mg 1.3 5.3Copper, mg 0.50 2.1Zinc, mg 5.6 24Iron, mg 4.5 19Selenium, mcg 18 78L-Carnitine, mg 38 158Taurine, mg 38 158Not for parenteral use.IndicationsSpecialized Nutritionfor low protein, electrolyte and fluid requirementsSUPLENA is a low-protein, nutritionally complete formula with a vitamin/mineral profile specifically designed for people with chronic or acute kidney failure who are not receiving dialysis- For tube or oral feeding- For supplemental or sole-source nutritionPackaging8-fl-oz cans; 24/caseVanillaMETABOLIC DISORDERS FORMULAS
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
METABOLIC DISORDERS FORMULAS
CYCLINEX-1 ®CompositionAmino acid-modified medical food with iron.PropertiesSupplemented with L-Carnitine (190 mg/100 g) and Taurine (65 mg/100 g) to supply amounts normally found in human milk and foods of animal origin.Provides 47% of energy as fat; 3.5% of energy as linoleic acid; 40% of energy as carbohydrate; supplemented with selenium, calcium and phosphorus.IndicationsWhen a non-essential amino acid-free medical food is needed for nutrition support of infants and toddlers with a defect in a urea cycle enzyme or with gyrate atrophy of the choroid and retina.PrecautionsNot for parenteral use.Packagingtn: 12.3 oz (350 g).Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
CYCLINEX-2 ®CompositionAmino acid-modified medical food.Indications

25
When a non-essential amino acid-free medical food is needed for nutrition support of children and adults with a defect in a urea cycle enzyme or with gyrate atrophy of the choroid and retina. Supplemented with L-Carnitine (370 mg/100 g) and Taurine (110 mg/100 g). Provides 39% of energy as fat to help satisfy energy needs; supplemented with selenium, calcium and phosphorus. PrecautionsNot for parenteral use.Packagingtn: 11.4 oz (325 g).Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
GLUTAREX-1 ®CompositionAmino acid-modified medical food with iron.PropertiesFortified with L-Carnitine (900 mg/100 g); supplemented with Taurine (60 mg/100 g); provides 45% of energy as fat, 3.4% of energy as linoleic acid, supplemented with selenium, calcium and phosphorus.IndicationsWhen a lysine-and tryptophan-free medical food is needed for nutrition support of infants and toddlers with glutaric aciduria type 1.PrecautionsNot for parenteral use.Packagingtn: 12.3 oz (350 g).Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
GLUTAREX-2 ®CompositionAmino acid-modified medical food.PropertiesFortified with L-Carnitine (1800 mg/100 g).Supplemented with Taurine (85 mg/100 g).Provides 34% of energy as fat supplemented with selenium, calcium and phosphorus.IndicationsWhen a lysine-and tryptophan-free medical food is needed for nutrition surt of children and adults with glutaric aciduria type 1.Side EffectsNot for parenteral use.Packagingtn: 11.4 oz (325 g).Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
HOMINEX-1 ®CompositionAmino acid-modified medical food with Iron.PropertiesMethionine-free. Supplemented with L-cystine, in a soluble form. Supplemented with L-Carnitine (20 mg/100 g) and Taurine (60 mg/100 g).Provides 45% of energy as fat, 3.4% of energy as linoleic acid. Supplemented with selenium, calcium and phosphorus. IndicationsWhen a methionine-free medical food is needed for nutrition support of infants and toddlers with vitamin B6 non-responsive homocystinuria or hypermethioninemia.PrecautionsNot for parenteral use.Packagingtn: 12.302 (350 g).Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
HOMINEX-2 ®CompositionAmino acid-modified medical food. PropertiesSupplemented with L-cystine, in a soluble form. Supplemented with L-Carnitine (40 mg/100 g) and Taurine (85 mg/100 g).Provides 34% of energy as fat supplemented with selenium, calcium and phosphorus.IndicationsWhen a methionine-free medical food is needed for nutrition support of infants and toddlers with vitamin B6 non-responsive homocystinuria or hypermethioninemia.PrecautionsNot for parenteral use.Packagingtn: 11.4 oz (325 g).Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++

26
I-VALEX-1 ®CompositionAmino acid-modified medical food with iron.PropertiesLeucine-free, contains isoleucine and valine.Fortified with L-Carnitine (900 mg/100 g).Fortified with glycine (1000 mg/100 g) low in tryptophan.Supplemented with Taurine (60 mg/100 g).Provides 45% of energy as fat, provides 3.4% of energy as linoleic acid. Supplemented with selenium, calcium and phosphorus.IndicationsWhen a leucine-free medical food is needed for nutrition support of infants and toddlers with isovaleric acidemia or other disorders of leucine catabolism.PrecautionsNot for parenteral use.Packagingtn: 12.3 oz (350 g).Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
I-VALEX-2 ®CompositionAmino acid-modified medical food.PropertiesLeucine-Free contains isoleucine and valine. Fortified with L-Carnitine (1800 mg/100 g). Fortified with glycine (3020 mg/100 g). Low in tryptophan.Supplemented with Taurine (85 mg/100 g). Provides 34% of energy as fat.Supplemented with selenium, calcium and phosphorus.PrecautionsNot for parenteral use.Packagingtn: 11.4 oz (325 g).Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
KETONEX-1 ®CompositionAmino acid-modified medical food with iron.PropertiesSupplemented with L-Carnitine (100 mg/100 g) and Taurine (60 mg/100 g). Provides 45% of energy as fat, provides 3.4% of energy as linoleic acid, protein-to-energy ratio that avoids excess energy intake.Supplemented with selenium, calcium and phosphorus.IndicationsWhen a branched chain amino acid-free medical food is needed for nutrition support of infants and toddlers with branched-chain ketoaciduria (maple syrup urine disease -MSUD).PrecautionsNot for parenteral use.Packagingtn: 12.3 oz (350 g).Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
KETONEX-2 ®CompositionAmino acid-modified medical food.PropertiesSupplemented with L-Carnitine (200 mg/ 100 g) and Taurine (85 mg/100 g).Provides 34% of energy as fat.Protein to-energy ratio that avoids excess energy intake.Supplemented with selenium, calcium and phosphorus.PrecautionsNot for parenteral use.Packagingtn: 11.4 oz (325 g).Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
PHENEX-1 ®CompositionAmino acid-modified medical food with iron.PropertiesPhenylalanine-free. Fortified with L-tyrosine, supplemented with L-glutamine, supplemented with L-Carnitine (20 mg/100 g) and Taurine (60 mg/100 g). Provides 45% of energy as fat.3.4% of energy as linoleic acid, supplemented with selenium, calcium and phosphorous.Indications

27
When a phenylalanine-free medical food is needed for nutrition support in infants and toddlers with phenylketonuria (PKU) or hyperphenylalaninemia.PrecautionsNot for parenteral use.Packagingtn:325 g.Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
PHENEX-2 ®CompositionAmino acid-modified medical food.PropertiesPhenylalanine-free. Fortified with L-tyrosine, supplemented with L-glutamine, L-Carnitine (40 mg/100 g) and Taurine (85 mg/100 g).Provides 34% of energy as fat.Supplemented with selenium, calcium and phosphorous.IndicationsWhen a phenylalanine-free medical food is needed for nutrition support of children and adults with phenylketonuria (PKU) or hyperphenylalaninemia.Side EffectsNot for parenteral use.Packagingtn: 11.4 oz (325 g).Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
PRO-PHREE ®CompositionProtein-free energy module with iron, vitamins and minerals.PropertiesProtein-free. Supplemented with L-Carnitine (25 mg/100 g) and Taurine (75 mg/100 g), provides 54% of energy as fat. Provides 3.9% of energy as linoleic acid, supplemented with selenium calcium and phosphorous.IndicationsWhen a protein-free medical food is needed for nutrition support of infants and toddlers requiring reduced protein intake, specific mixture of L-amino acids or increased energy, minerals and vitamins.PrecautionsNot for parenteral use.Packagingtn: 12.3 oz (350 g).Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
PROPIMEX-1 ®CompositionAmino acid-modified medical food with iron.PropertiesMethionine-and valine-free, fortified with L-Carnitine (900 mg/100 g) low in tryptophan. Supplemented with Taurine (60 mg/100 g).Provides 45% of energy as fat, provides 3.4% of energy as linoleic acid, supplemented with selenium, calcium and phosphorous.IndicationsWhen a methionine-and valine-free, low-isoleucine and low-threonine medical food is needed for nutrition support of infants and toddlers with propionic or methylmalonic acidemia.PrecautionsNot for parenteral use.Packagingtn: 12.3 oz (350 g).Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
PROPIMEX-2 ®CompositionAmino acid-modified medical food.PropertiesMethionine - and valine-free, low in isoleucine and threonine. Fortified with L-Carnitine (1800 mg/100 g) low in tryptophan. Supplemented with Taurine (85 mg/100 g).Provides 34% of energy as fat. Supplemented with selenium, calcium and phosphorous.IndicationsWhen a methionine-and valine-free, low-isoleucine and low-threonine medical food is needed for nutrition support of children and adults with propionic or methylmalonic acidemia.Side EffectsNot for parenteral use.Packagingtn: 11.4 oz (325 g).

28
Av S.A., Gulf
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
PROVIMIN ®CompositionProtein-vitamin-mineral formula component with iron.IndicationsFor use as the protein base in the preparation of liquid diets for feeding infants and children with chronic diarrhea and other malabsorptive disorders that require restriction of fat and carbohydrate intake.Contains a high-quality source of protein (casein); virtually carbohydrate and fat-free; meets (NAS-NRC) RDAs; calcium to phosphorous ratio of 1.4:1; fortified with L-Carnitine, Taurine and selenium.PrecautionsNot for parenteral use.Packagingtn: 5.3 oz (150 g).Av S.A., Gulf
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
RCF ®CompositionRoss carbohydrate free low-iron soy formula base.PropertiesCarbohydrate-free; soy protein isolate.IndicationsFor use in the dietary management of persons unable to tolerate the type or amount of carbohydrates in milk or conventional infant formulas.Packagingtn: 13-fl-oz concentrated.Av S.A.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
TYREX-2 ®CompositionAmino acid-modified medical food.PropertiesPhenylalanine and tyrosine-free. Supplemented with L-Carnitine (40 mg/100 g) and Taurine (85 mg/100 g). Provides 34% of energy as fat.Supplemented with selenium, calcium and phosphorous.IndicationsWhen a phenylalanine and tyrosine-free medical food is needed for nutrition support of children and adults with tyrosinemia type II. PrecautionsNot for parenteral use.Packagingtn: 11.4 oz (325 g).Av S.A., Gulf
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
TYROMEX-1 ®CompositionAmino acid-modified medical food with iron.PropertiesPhenylalanine tyrosine and methionine free.Supplemented with L-Carnitine (20 mg/100 g) and Taurine (60 mg/100 g).Provides 45% of energy as fat.Provides 3.4% of energy as linoleic acid.Supplemented with calcium and phosphorous.IndicationsWhen a phenylalanine-tyrosine and methionine free medical food is needed for nutrition support of infants and toddlers with tyrosinemia type I.PrecautionsNot for parenteral use.Packagingtn: 12.3 oz (350 g).Av S.A., Gulf
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
PEDIATRIC NUTRITIONALS INFANT FORMULAS
GAIN PLUS IQ ®CompositionMilk-based, follow-on milk formula fortified with Probiotics and Fructo-oligosaccharide (FOS), also fortified with DHA and A.A.

29
Fat: 36.2 c g/lCarbohydrate: 75 g/l Protein: 28 g/l Minerals: 7 g/l Taurine: 50 mg/l Energy: 738 Kcal/lIron: 12 mg/L.IndicationsGainPlus is specially formulated to complement solid food in providing a nutritionally balanced diet for children 18 months and over. It contains high quality protein, calcium, essential vitamins & minerals to promote the healthy growth. Made with a unique vegetable oil blend, it is easily digested and absorbed, providing an essential fatty acid profile important for brain and retinal development. GainPlus IQ contains Probiotic (Lactobacillus & Bifidus) & FOS (Factor-oligosaccharides) which enhance the maintenance of micro flora balance. ContraindicationsHypersensitivity to cow's milk protein. Dosage AdministrationTo prepare a single serving, add four level scoops of GainPlus IQ to a glass containing 240 ml of previously boiled potable water. Mix well and feed immediately or store up to 24 hours in the refrigerator. Packagingtn: 400 g, 900 gm. Av: SA, ME, Gulf NOTE: Full prescribing information is available upon request.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
ISOMIL 1 ®CompositionSoy based lactose-free infant formula in powder form.IndicationsTo be used as cow's milk-free feeding and post-diarrhea infant feeding. In patients with cow's milk allergy or disorders where lactose should be avoided.ContraindicationsSoy protein allergy.Side EffectsNot likely to occur when instructions are followed.Dosage AdministrationFrom 0-6 months1 measuring scoop of powder for each 60 ml produces a standard dilution (20 cal/30 ml).The physician will recommend according to age/weight the volume of meals and the number of feedings.Packagingtn: 400 g.Av M.E., S.A., GulfNOTE: Full prescribing information is available on request.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
ISOMIL 2 ®CompositionSoy based lactose-free infant formula in powder form.IndicationsTo be used as cow's milk-free feeding and post-diarrhea infant feeding. In patients with cow's milk allergy or disorders where lactose should be avoided.ContraindicationsNot recommended for long-term feeding of very low birth weight infants.Side EffectsNot likely to occur when instructions are followed.Dosage AdministrationFrom 6 months onwards1 measuring scoop of powder for each 60 ml produces a standard dilution (20 cal/30 ml).The physician will recommend according to age/weight the volume of meals and the number of feedings.Packagingtn: 400 g.Av M.E., S.A., GulfNOTE: Full prescribing information is available on request.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
SIMILAC ADVANCE WITH IRON ®CompositionPowdered, homogenized, modified milk products fortified with total potentially available levels of nucleotides found in breast milk.IndicationsUsed if discontinuation of breast feeding is required, if supplement to breast feeding is needed or as a routine feeding if breast feeding is not adopted.Similac with iron is used when an iron-containing formula is needed.ContraindicationsMilk allergy.Side EffectsNot likely to occur if instructions are closely followed.Dosage Administration

30
One measuring scoop of powder for each 60 ml of water produces a standard dilution (20 cal/30 ml). The volume of meals and number of feedings will be adjusted, according to age/weight, by the physician.Packagingtn: 400 gAv M.E., S.A., GulfNOTE: Full prescribing information is available on request.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
SIMILAC ADVANCE IQ ®CompositionPowdered, homogenized, modified milk products fortified with total potentially available levels of nucleotides found in breast milk 72 mg/L. Also fortified with DHA and AA.IndicationsUsed if discontinuation of breast feeding is required, if supplement to breast feeding is needed or as a routine feeding if breast feeding is not adopted.ContraindicationsMilk allergy.Side EffectsNot likely to occur if instructions are closely followed.Dosage AdministrationOne measuring scoop of powder for each 60 ml of water produces a standard dilution (20 cal/30 ml). The volume of meals and number of feedings will be adjusted, according to age/weight, by the physician.Packagingtn: 400 g & 900 gmAv M.E., S.A., GulfNOTE: Full prescribing information is available on request.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
SIMILAC GAIN IQ ®CompositionPowdered, homogenized modified follow-on formula milk fortified with Total Potentially Available level of Nucleotides found in breast milk 72 mg/l. Also fortified with DHA and A.A. Fat: 36.2g/l.Carbohydrate: 75 g/l.Proteins: 28 g/l.Minerals: 7 g/l.Taurine: 50 mg/l.Calories: 738 Kcal/l and nucleotides 72 mg/l.IndicationsSpecially formulated to complement solid food in providing a nutritionally balanced diet for children 6 months and over. Contains high quality protein, calcium and all essential vitamins and minerals to promote the healthy growth. Made with a unique vegetable oil blend is easily digested and absorbed, providing an essential fatty acid profile important for brain and retinal development. Similac Gain IQ is uniquely fortified with nucleotides and clinical research suggest nucleotides may help strengthen a baby's developing immune system.ContraindicationsMilk allergy.Dosage AdministrationOne level scoop of powder to each 60 ml of previously boiled water. Mix well and feed immediately, or store in the refrigerator for no longer than 24 hours.Packagingtn: 400 g & 900 g.Av Gulf, SA, ME.NOTE: Full prescribing information is available on request.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
SIMILAC LF ®CompositionMilk-based lactose-free formula in powder form.IndicationsTo be used as lactose-free milk-based feeding for infants with disorders where lactose should be avoided.ContraindicationsMilk allergy.Side EffectsNot likely to occur when instructions are followed.Dosage AdministrationOne measuring scoop of powder for each 60 ml water produces a standard dilution (20 cal/30 ml). The physician will recommend according to age and weight the volume of meals and the number of feedings.Packagingtn: 375 g.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
SIMILAC NEOSURE IQ ®CompositionSpecial formula contains higher nutrient and vitamin levels than standard milk-based standard formulas. Also fortified with DHA and AA.PropertiesHigher levels of proteins, vitamins and minerals per 100 kcal than standard term formula.

31
More calcium and phosphorus than standard term formula.Well absorbed fat blend than contains 25% added medium-chain triglycerides (MCTs).Powder mixable to various caloric concentrations: 20, 22, 24, 27 kcal/30 ml.IndicationsSpecial formula intended for the first year of life for conditions such as low-birth-weight or prematurity. Similac NeoSure IQ plays an important role in meeting the nutritional needs of premature or low-birth-weight infants who have joined their families at home. Similac NeoSure contains higher nutrient levels than standard milk-based term formulas, but lower levels than formulas fed to premature infants in the hospital, thus extending the nutritional support initiated there.Use only as directed by a physician. Packagingp: 370 g Powder (Case x 24).
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
PHARMACEUTICAL PRODUCTS
BRUFEN SYRUP ®GeneralBottles of 100ml with dispensing spoonCompositionBrufen Syrup: Each teaspoonful contains100mg5ml Ibuprofen BPPropertiesBrufen Syrup: Orange colored, Orange flavoured Syrupy SuspensionPharmacodynamicIbuprofen is a propionic acid derivative with analgesic, anti-inflammatory and antipyretic activity. The drug's therapeutic effects as an NSAID are thought to result from its activity on prostaglandin synthesis.PharmacokineticIbuprofen is rapidly absorbed from the gastrointestinal tract, peak serum concentrations occurring 1-2 hours after administration. The elimination half-life is approximately 2 hours. Ibuprofen is metabolized in the liver to two inactive metabolites and these, together with unchanged ibuprofen, are excreted by the kidney either as such or as conjugates. Excretion by the kidney is both rapid and complete. Ibuprofen is extensively bound to plasma proteins.IndicationsBrufen is indicated for its analgesic and anti-inflammatory effects in the treatment of rheumatoid arthritis (including juvenile rheumatoid arthritis or Still's disease), ankylosing spondylitis, osteoarthritis and other non-rheumatoid (seronegative) arthropathies.In the treatment of non-articular rheumatic conditions, Brufen is indicated in periarticular conditions such as frozen shoulder (capsulitis), bursitis, tendinitis, tenosynovitis and low back pain; Brufen can also be used in soft tissue injuries as sprains and strains.Brufen Syrup: Brufen Syrup is indicated in short-term use for the treatment of pyrexia in children over one year of age.ContraindicationsPatients with a history of, or active, peptic ulceration.Patients who have previously shown hypersensitivity reactions (e.g. asthma, rhinitis or urticaria) in response to ibuprofen, aspirin or other NSAIDs.Severe heart failure.Side EffectsGastrointestinal: The most commonly-observed adverse events are gastrointestinal in nature. Nausea, vomiting, diarrhoea, dyspepsia, abdominal pain, melaena, haematemesis , ulcerative stomatitis and gastrointestinal haemorrhage have been reported following ibuprofen administration. Less frequently, gastritis, duodenal ulcer, gastric ulcer and gastrointestinal perforation have been observed. Epidemiological data indicate that of the seven most widely-used oral, non-asprin NSAIDs, ibuprofen presents the lowest risk of upper gastrointestinal toxicity.Hypersensitivity: Hypersensitivity reactions have been reported following treatment with ibuprofen. These may consist of (a) non-specific allergic reaction and anaphylaxis, (b) respiratory tract reactivity comprising asthma, aggravated asthma, bronchospasm or dyspnoea, or (c) assorted skin disorders, including rashes of various types, pruritus, urticaria, purpura, angioedema and, less commonly, bullous dermatoses (including epidermal necrolysis and erythema multiforme).Cardiovascular: Oedema has been reported in association with Ibuprofen treatment. Oedema, hypertension, and cardiac failure, have been reported in association with NSAID treatment.Clinical trial and epidemiological data suggest that use of ibuprofen, particularly at high dose (2400mg daily), and in long term treatment may be associated with a small increased risk of arterial thrombotic events (for example myocardial infarction or stroke).Other adverse events reported less commonly and for which causality has not necessarily been established include:Renal: Nephrotoxicity in various forms, including interstitial nephritis, nephritic syndrome and renal failure.Hepatic: Abnormal liver function, hepatitis and jaundice.Neurological & special senses: Visual disturbances, optic neuritis, headaches, paraesthesia, depression, confusion, hallucinations, tinnitus, vertigo, dizziness, malaise, fatigue and drowsiness.Haematological: Thrombocytopenia, neutropenia, agranulocytosis, aplastic anaemia and haemolytic anaemia.Dermatological: Photosensitivity.PrecautionsUndesirable effects may be minimized by using the lowest effective dose for the shortest duration necessary to control symptoms. Caution is required if Brufen is administered to patients suffering from, or with a previous history of, bronchial asthma since Ibuprofen has been reported to cause bronchospasm in such patients, Brufen should only be given with care to patients with a history of gastrointestinal disease.Caution is required in patients with renal, hepatic or cardiac impairment since the use of NSAIDs may result in deterioration of renal function. The dose should be kept as low as possible and renal function should be monitored in these patients.Brufen should be given with care to patients with a history of heart failure or hypertension since oedema has been reported in association with ibuprofen administration.Cardiovascular and cerebrovascular effects: Appropriate monitoring and advice are required for patients with a history of hypertension and/or mild to moderate congestive heart failure as fluid retention and oedema have been reported in association with NSAID therapy.Clinical trial data suggest that use of ibuprofen, particularly at a high dose (2400mg daily) and in long term treatment may be associated with a small increased risk of arterial thrombotic events (for example myocardial infarction or stroke). Overall, epidemiological studies do not suggest that low dose ibuprofen (e.g.≤1200mg daily) is associated with an increased risk of myocardial infarction.Patients with uncontrolled hypertension, congestive heart failure, established ischaemic heart disease, peripheral arterial disease, and/or cerebrovascular disease should only be treated with ibuprofen after careful consideration. Similar consideration should be made before

32
initiating longer-term treatment of patients with risk factors for cardiovascular events (e.g. hypertension, hyperlipidaemia, diabetes mellitus, smoking)Pregnancy and LactationWhilst no teratogenic effects have been demonstrated in animal toxicology studies, the use of ibuprofen during pregnancy should, if possible, be avoided. Congenital abnormalities have been reported in association with ibuprofen administration in man; however, these are low in frequency and do not appear to follow any discernible pattern. In view of the known effects of NSAIDs on the foetal cardiovascular system (closure of ductus arteriosus), use in late pregnancy should be avoided. In the limited studies so far available, ibuprofen appears in the breast milk in very low concentrations and is unlikely to adversely affect the breast-fed infant.Effects On Ability To Drive And Use MachinesNo adverse effects known.OverdosageSymptoms include nausea, vomiting, dizziness and rarely, loss of consciousness. Large overdoses are generally well tolerated when no other drugs are involved. Treatment consists of gastric lavage and, if necessary, correction of serum electrolytes and appropriate supportive measures. There is no specific antidote to ibuprofen.Drug InteractionsCare should be taken in patients treated with any of the following drugs as interactions have been reported in some patients.Antihypertensives: Reduced antihypertensive effect.Diuretics: Reduced diuretic effect. Diuretics can increase the risk of nephrotoxicity of NSAIDsCardiac glycosides: NSAIDs may exacerbate cardiac failure, reduce GFR and increase plasma cardiac glycoside levels.Lithium: Decreased elimination of lithium.Methotrexate: Decreased elimination of methotrexate.Cyclosporin: Inreased risk of nephrotoxicity with NSAIDs.Mifepristone: NSAIDs should not be used for 8-12 days after mifepristone administration as NSAIDs can reduce the effects of mifepristone.Other analgesics: Avoid concomitant use of two or more NSAIDs. Corticosteroids: Increased risk of gastrointestinal bleeding. Anticoagulants: Enhanced anticoagulant effect.Quinolone antibiotics: Animal data indicate that NSAIDs can increase the risk of convulsions associated with quinolone antibiotics. Patients taking NSAIDs and quinolones may have an increased risk of developing convulsions.IncompatibilitiesNone.Dosage AdministrationBrufen Syrup: The daily dosage of Brufen is 20 mg/kg of bodyweight in divided doses. This can be achieved as follows:1-2 years: One 2.5 ml spoonful (50 mg), 3-4 times daily.3-7 years: One 5 ml spoonful (100 mg), 3-4 times daily.8-12 years: Two 5 ml spoonfuls (200 mg), 3-4 times daily.Brufen is not recommended for children weighing less than 7 kg.In juvenile rheumatoid arthritis, up to 40 mg/kg of bodyweight daily in divided doses may be taken.PackagingBrufen syup: Bottles of 100ml with dispensing spoon
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
HUMIRA ®General(Adalimumab)Humira 40 mg solution for injection in pre-filled syringeCompositionEach 0.8 ml single dose pre-filled syringe contains 40 mg of adalimumab.Adalimumab is a recombinant human monoclonal antibody expressed in ChineseHamster Ovary cells.PropertiesSolution for injection in pre-filled syringe.PharmacodynamicMechanism of actionAdalimumab binds specifically to TNF and neutralizes the biological function of TNF by blocking its interaction with the p55 and p75 cell surface TNF receptors.Adalimumab also modulates biological responses that are induced or regulated by TNF, including changes in the levels of adhesion molecules responsible for leukocytemigration (ELAM-1, VCAM-1, and ICAM-1 with an IC50 of 1-2 X 10-10 M).Pharmacodynamic effectsAfter treatment with Humira, a rapid decrease in levels of acute phase reactants of inflammation (C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR)) and serum cytokines (IL-6) was observed compared to baseline in patients with rheumatoid arthritis. Serum levels of matrix metalloproteinases (MMP-1 and MMP-3) that produce tissue remodelling responsible for cartilage destruction were also decreased after Humira administration. Patients treated with Humira usually experienced improvement in haematological signs of chronic inflammation. A rapid decrease in CRP levels was also observed in patients with Crohn’s disease.PharmacokineticAfter subcutaneous administration of a single 40 mg dose, absorption and distribution of adalimumab was slow, with peak serum concentrations being reached about 5 days after administration. The average absolute bioavailability of adalimumab estimated from three studies following a single 40 mg subcutaneous dose was 64%.After single intravenous doses ranging from 0.25 to 10 mg/kg, concentrations were dose proportional. After doses of 0.5 mg/kg (~40 mg), clearances ranged from 11 to 15 ml/hour, the distribution volume (Vss) ranged from 5 to 6 litres and the mean terminal phase half-life was approximately two weeks. Adalimumab concentrations in the synovial fluid from several rheumatoid arthritis patients ranged from 31-96% of those in serum.Following subcutaneous administration of 40 mg of Humira every other week the mean steady-state trough concentrations were approximately 5 μg/ml (without concomitant methotrexate) and 8 to 9 μg/ml (with concomitant methotrexate), respectively. The serum adalimumab trough levels at steady-state increased roughly proportionally with dose following 20, 40 and 80 mg every other week and every week subcutaneous dosing.In patients with Crohn’s disease, the loading dose of 80 mg Humira on week 0 followed by 40 mg Humira on week 2 achieves serum adalimumab trough concentrations of approximately 5.5 μg/ml during the induction period. A loading dose of 160 mg Humira on week 0 followed by 80 mg Humira on week 2 achieves serum adalimumab trough concentrations of approximately 12 μg/ml during the induction period. Mean steady-state trough levels of approximately 7 μg/ml were observed in Crohn’s disease patients who received a maintenance dose of 40 mg Humira every other week.

33
Population pharmacokinetic analyses with data from over 1300 patients revealed a trend toward higher apparent clearance of adalimumab with increasing body weight.After adjustment for weight differences, gender and age appeared to have a minimal effect on adalimumab clearance. The serum levels of free adalimumab (not bound to anti-adalimumab antibodies, AAA) were observed to be lower in patients with measurable AAA. Humira has not been studied in children or in patients with hepatic or renal impairment.IndicationsRheumatoid ArthritisHumira in combination with methotrexate, is indicated for:- the treatment of moderate to severe, active rheumatoid arthritis in adult patients when the response to disease-modifying anti-rheumatic drugs including methotrexate has been inadequate.- the treatment of severe, active and progressive rheumatoid arthritis in adults not previously treated with methotrexate.- Humira can be given as monotherapy in case of intolerance to methotrexate or when continued treatment with methotrexate is inappropriate.Humira has been shown to reduce the rate of progression of joint damage as measured by X-ray and to improve physical function, when given in combination with methotrexate.Psoriatic ArthritisHumira is indicated for the treatment of active and progressive psoriatic arthritis in adults when the response to previous disease-modifying anti-rheumatic drug therapy has been inadequate.Ankylosing spondylitisHumira is indicated for the treatment of adults with severe active ankylosing spondylitis who have had an inadequate response to conventional therapy.Crohn’s diseaseHumira is indicated for treatment of severe, active Crohn’s disease, in patients who have not responded despite a full and adequate course of therapy with a corticosteroid and/or an immunosuppressant; or who are intolerant to or have medical contraindications for such therapies. For induction treatment, Humira should be given in combination with corticosteroids. Humira can be given as monotherapy in case of intolerance to corticosteroids or when continued treatment with corticosteroids is inappropriate.ContraindicationsHypersensitivity to the active substance or to any of the excipients.Active tuberculosis or other severe infections such as sepsis, and opportunistic infections.Moderate to severe heart failure (NYHA class III/IV).Side EffectsClinical TrialsHumira was studied in 5293 patients in controlled and open label trials for up to 60 months. These trials included rheumatoid arthritis patients with short term and long standing disease as well as psoriatic arthritis, ankylosing spondylitis and Crohn’s disease patients. The data in Table 1 is based on the controlled Studies (I-IX,CLASSIC I, GAIN AND CHARM). involving 3271 patients receiving Humira and 1809 patients receiving placebo or active comparator during the controlled period.Adverse events at least possibly causally-related to adalimumab for Studies I-IX, CLASSIC I, GAIN and CHARM, both clinical and laboratory, are displayed by system organ class and frequency (very common ≥ 1/10; common ≥ 1/100 < 1/10; uncommon ≥ 1/1000 to ≤ 1/100) and rare < 1/1000 in Table 1 below. Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness.(see Table 1)HUMIRA Table 1 Undesirable Effects in Clinical StudiesSystem Organ Class Frequency Adverse Reaction
Infections and infestations
Commonlower respiratory infections (including pneumonia, bronchitis), viral infections (including influenza, herpes infections), candidiasis, bacterial infections (including urinary tract infections), upper respiratory infection
Uncommonopportunistic infections (including tuberculosis, histoplasmosis), sepsis, abscess, joint infection, wound infection, skin infection (including cellulitis and impetigo), superficial fungal infections (including skin, nail and foot)
Rare necrotising fasciitis, viral meningitis, diverticulitisNeoplasms benign and malignant (including cysts and polyps)
Uncommon skin papilloma
Rare lymphoma, solid organ tumours (including breast, ovarian, testicular), squamous cell carcinoma of the skin
Blood and the lymphatic system disorders
Common lymphopaenia
Uncommon neutropaenia (including agranulocytosis), leucopaenia, thrombocytopaenia, anaemia, lymphadenopathy, leucocytosis
Rare pancytopaenia, idiopathic thrombocytopaenia purpura
Immune system disordersUncommon systemic lupus erythematosus, angioedema, drug hypersensitivity, seasonal allergyRare serum sickness
Endocrine disorders Rare thyroid disorder (including goitre)Metabolism and nutrition disorders
Uncommon Hypokalaemia, lipids increased, appetite disorders (including anorexia), hyperuricaemiaRare hypercalcaemia
Psychiatric disorders Uncommon mood disorders, anxiety (including nervousness and agitation)
Nervous system disordersCommon dizziness (including vertigo), headache, neurologic sensation disorders (including
paraesthesias)Uncommon syncope, migraine, tremor, sleep disturbancesRare multiple sclerosis
Eye disordersCommon infection, irritation or inflammation of the eyeUncommon vision disorder, ocular sensation disordersRare Panophthalmitis, iritis, glaucoma
Ear and labyrinth disordersUncommon tinnitus, ear discomfort (including pain and swelling)Rare hearing loss
Cardiac disordersUncommon arrhythmias, tachycardia, palpitationsRare cardiac arrest, coronary artery insufficiency, angina pectoris, pericardial effusion
Vascular disorders Uncommon hypertension, flushing, haematoma

34
Rare vascular occlusion, aortic stenosis, thrombophlebitis, aortic aneurysm
Respiratory, thoracic and mediastinal disorders
Common cough, nasopharyngeal painUncommon asthma, dyspnoea, dysphonia, nasal congestionRare pulmonary oedema, pharyngeal oedema, pleural effusion, pleurisy
Gastrointestinal disordersCommon diarrhoea, abdominal pain, stomatitis and mouth ulceration, nauseaUncommon rectal haemorrhage, gastritis, vomiting, dyspepsia, abdominal bloating, constipationRare intestinal stenosis, colitis, enteritis, oesophagitis
Hepato-biliary disordersCommon hepatic enzymes increasedRare hepatic necrosis, hepatitis
Skin and subcutaneous tissue disorders
Common rash, dermatitis and eczema, pruritus, hair lossUncommon urticaria, psoriasis, ecchymosis and increased bruising, purpuraRare erythema multiforme, panniculitis
Musculoskeletal, connective tissue and bone disorders
Common musculoskeletal painRare rhabdomyolysis
Renal and urinary disordersCommon haematuria, renal impairment, bladder and urethral symptomsRare proteinuria, renal pain
Reproductive system and breast disorders Uncommon menstrual cycle and uterine bleeding disorders
General disorders and administration site conditions
Very Common injection site reaction (including pain, swelling, redness or pruritus)
Common pyrexia, fatigue (including asthenia and malaise)Uncommon chest pain, oedema, influenza like illness
Investigations Uncommon blood creatine phosphokinase increased, activated partial thromboplastin time prolonged, autoantibodies present
Injury and poisoning Uncommon accidental injury, impaired healing Injection site reactionsIn the twelve controlled trials, 16% of patients treated with Humira developed injection site reactions (erythema and/or itching, haemorrhage, pain or swelling), compared to 10% of patients receiving placebo or active control. Injection site reactions generally did not necessitate discontinuation of the medicinal product.InfectionsIn the twelve controlled trials, the rate of infection was 1.49 per patient year in the Humira treated patients and 1.42 per patient year in the placebo and active control-treated patients. The infections consisted primarily of upper respiratory tract infections, bronchitis and urinary tract infections. Most patients continued on Humira after the infection resolved. The incidence of serious infections was 0.03 per patient year in Humira treated patients and 0.03 per patient year in placebo and active control-treated patients.In controlled and open label studies with Humira, serious infections (including fatal infections, which occurred rarely) have been reported, which include reports of tuberculosis (including miliary and extra-pulmonary locations) and invasive opportunistic infections (e.g. disseminated histoplasmosis, pneumocystis carinii pneumonia, aspergillosis and listeriosis). Most of the cases of tuberculosis occurred within the first eight months after initiation of therapy and may reflect recrudescence of latent disease.Malignancies and lymphoproliferative disordersDuring the controlled portions of ten Humira trials at least 12 weeks in duration (I-IX and CHARM) in patients with moderately to severely active rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis and Crohn’s disease, malignancies, other than lymphoma and non-melanoma skin cancer, were observed at a rate (95% confidence interval) of 5.7 (3.3, 10.1) per 1000 patient-years among 2887 Humira treated patients versus a rate of 4.1 (1.5, 10.9) 1 per 1000 patient-years among 1570 control patients (median duration of treatment was 5.7 months for Humira and 5.5 months for control-treated patients). The rate (95% confidence interval) of non-melanoma skin cancers was 7.6 (4.7, 12.4) per 1000 patient-years among Humira treated patients and 2.0 (0.5, 8.2) per 1000 patient-years among control patients. Of these skin cancers, squamous cell carcinomas occurred at rates (95% confidence interval) of 2.4 (1.0, 5.7) per 1000 patient-years among Humira-treated patients and 0 per 1000 patient-years among control patients. The rate (95% confidence interval) of lymphomas was 1.0 (0.2, 3.8) per 1000 patient-years among Humira-treated patients and 1.0 (0.1, 7.3) per 1000 patient-years among control patients.When combining controlled portions of ten trials (I-IX and CHARM) and ongoing open label extension studies with a median duration of approximately 2. years including 4843 patients and over 13000 patient-years of therapy, the observed rate of malignancies, other than lymphoma and non-melanoma skin cancers is approximately 13.6 per 1000 patient years. The observed rate of non-melanoma skin cancers is approximately 9.0 per 1000 patient years, and the observed rate of lymphomas is approximately 1.2 per 1000 patient years.In post-marketing experience from January 2003, predominately in patients with rheumatoid arthritis, the reported rate of malignancies other than lymphomas and non-melanoma skin cancers is approximately 1.7 per 1000 patient years. The reported rates for non-melanoma skin cancers and lymphomas are approximately 0.2 and 0.4 per 1000 patient years, respectively.AutoantibodiesPatients had serum samples tested for autoantibodies at multiple time points in rheumatoid arthritis Studies I-V. In these trials, 11.9% of patients treated with Humira and 8.1% of placebo and active control-treated patients that had negative baseline anti-nuclear antibody titres reported positive titres at week 24. Two patients out of 3441 treated with Humira in all rheumatoid arthritis and psoriatic arthritis studies developed clinical signs suggestive of new-onset lupus-like syndrome. The patients improved following discontinuation of therapy. No patients developed lupus nephritis or central nervous system symptoms.Liver Enzyme ElevationsRheumatoid arthritis clinical trials: in controlled rheumatoid arthritis clinical trials (Studies I–IV), elevations of ALT were similar in patients receiving adalimumab or placebo. In patients with early rheumatoid arthritis (disease duration of less than 3 years) (Study V), elevations of ALT were more common in the combination arm (Humira/methotrexate) compared to the methotrexate monotherapy arm or the Humira monotherapy arm.Psoriatic arthritis clinical trials: elevations in ALT were more common in psoriatic arthritis patients (Studies VI-VII) compared with patients in rheumatoid arthritis clinical studies.In all studies (I-VII), patients with raised ALT were asymptomatic and in most cases elevations were transient and resolved on continued treatment.Crohn’s disease clinical trials: in controlled clinical trials, elevations of ALT were similar in patients receiving adalimumab or placebo.Additional Adverse Reactions from Postmarketing Surveillance or Phase IV Clinical TrialsThe additional adverse reactions in Table 2 have been reported from postmarketing surveillance of Phase IV clinical trials:HUMIRA Table 2 Undesirable Effects in Postmarketing Surveillance and Phase IV Clinical

35
StudiesSystem Organ Class Adverse ReactionHepatobiliary Disorders reactivation of hepatitis BNervous system disorders demyelinating disorders (eg optic neuritis)Respiratory, thoracic and mediastinal interstitial lung disease, includingdisorders pulmonary fibrosisSkin and subcutaneous tissue disorders cutaneous vasculitisImmune system disorders anaphylaxis PrecautionsInfectionsPatients must be monitored closely for infections including tuberculosis, before, during and after treatment with Humira. Because the elimination of adalimumab may take up to five months, monitoring should be continued throughout this period.Treatment with Humira should not be initiated in patients with active infections including chronic or localized infections until infections are controlled.Patients who develop a new infection while undergoing treatment with Humira should be monitored closely. Administration of Humira should be discontinued if a patient develops a new serious infection until infections are controlled. Physicians should exercise caution when considering the use of Humira in patients with a history of recurring infection or with underlying conditions which may predispose patients to infections including the use of concomitant immunosuppressive medications.Serious infections, sepsis, tuberculosis and other opportunistic infections, including fatalities, have been reported with Humira.Serious infections:In clinical trials an increased risk of serious infections in patients receiving Humira has been shown, and reports from the post-marketing setting support this finding.Of particular importance are infections such as pneumonia, pyelonephritis, septic arthritis and septicaemia.Tuberculosis:There have been reports of tuberculosis in patients receiving Humira. It should be noted that in the majority of those reports, tuberculosis was extra-pulmonary, i.e. disseminated.Before initiation of therapy with Humira, all patients must be evaluated for both active or inactive (latent) tuberculosis infection. This evaluation should include a detailed medical history with a personal history of tuberculosis or possible previous exposure to patients with active tuberculosis and previous and/or current immunosuppressive therapy. Appropriate screening tests, i.e. tuberculin skin test and chest x-ray, should be performed in all patients (local recommendations may apply). It is recommended that the conduct of these tests should be recorded in the patient’s alert card.Prescribers are reminded of the risk of false negative tuberculin skin test results, especially in patients who are severely ill or immunocompromised.If active tuberculosis is diagnosed, Humira therapy must not be initiated.If latent tuberculosis is diagnosed, appropriate anti-tuberculosis prophylaxis in accordance with local recommendations must be initiated before starting treatment with Humira. In this situation, the benefit/risk balance of therapy with Humira should be very carefully considered.Patients should be instructed to seek medical advice if signs/symptoms (eg, persistent cough, wasting/weight loss, low grade fever) suggestive of a tuberculosis infection occur during or after therapy with Humira.Other opportunistic infections:There have been reports of serious and severe opportunistic infections associated with Humira therapy, for example pneumocystis carinii pneumonia, disseminated histoplasmosis, listeriosis and aspergillosis.If a patient receiving Humira shows prolonged/atypical symptoms/signs of infections or general deterioration, prevalent opportunistic conditions must be considered.Hepatitis B ReactivationReactivation of hepatitis B has occurred in patients receiving a TNF-antagonist including Humira, who are chronic carriers of this virus. Some cases have had fatal outcome. Patients at risk for HBV infection should be evaluated for prior evidence of HBV infection before initiating Humira therapy. Carriers of HBV who require treatment with Humira should be closely monitored for signs and symptoms of active HBV infection throughout therapy and for several months following termination of therapy.Adequate data of treating patients who are carriers of HBV with anti-viral therapy in conjunction with TNF-antagonist therapy to prevent HBV reactivation are not available. In patients who develop HBV reactivation, Humira should be stopped and effective anti-viral therapy with appropriate supportive treatment should be initiated.Neurological eventsTNF-antagonists including Humira have been associated in rare cases with new onset or exacerbation of clinical symptoms and/or radiographic evidence of demyelinating disease. Prescribers should exercise caution in considering the use of Humira in patients with pre-existing or recent-onset central nervous system demyelinating disorders.Allergic reactionsSerious allergic adverse reactions have not been reported with subcutaneous administration of Humira during clinical trials. Non-serious allergic reactions associated with Humira were uncommon during clinical trials. In postmarketing,serious allergic reactions including anaphylaxis have been reported very rarely following Humira administration. If an anaphylactic reaction or other serious allergic reaction occurs, administration of Humira should be discontinued immediately and appropriate therapy initiated.The needle cover of the syringe contains natural rubber (latex). This may cause severe allergic reactions in patients sensitive to latex.Immunosuppression In a study of 64 patients with rheumatoid arthritis that were treated with Humira, there was no evidence of depression of delayed-type hypersensitivity, depression of immunoglobulin levels, or change in enumeration of effect or T-and B cells and NKcells, monocyte/macrophages, and neutrophils.Malignancies and lymphoproliferative disordersIn the controlled portions of clinical trials of TNF-antagonists, more cases of lymphoma have been observed among patients receiving a TNF-antagonist compared with control patients. However, the occurrence was rare, and the follow up period of placebo patients was shorter than for patients receiving TNF-antagonist therapy.Furthermore, there is an increased background lymphoma risk in rheumatoid arthritis patients with long-standing, highly active, inflammatory disease, which complicates the risk estimation. With the current knowledge, a possible risk for the development of lymphomas or other malignancies in patients treated with a TNF-antagonist cannot be excluded.No studies have been conducted that include patients with a history of malignancy or that continue treatment in patients who develop malignancy while receiving Humira. Thus additional caution should be exercised in considering Humira treatment of these patients.In an exploratory clinical trial evaluating the use of another anti-TNF agent, infliximab, in patients with moderate to severe chronic obstructive pulmonary disease (COPD), more malignancies, mostly in the lung or head and neck, were reported in infliximab-treated patients compared with control patients. All patients had a history of heavy smoking. Therefore, caution should be exercised when using any TNFantagonist in COPD patients, as well as in patients with increased risk for malignancy due to heavy smoking.

36
Haematologic reactionsRare reports of pancytopenia including aplastic anaemia have been reported with TNF blocking agents. Adverse events of the haematologic system, including medically significant cytopoenia (e.g. thrombocytopaenia, leucopaenia) have been infrequently reported with Humira. All patients should be advised to seek immediate medical attention if they develop signs and symptoms suggestive of blood dyscrasias (e.g. persistent fever, bruising, bleeding, pallor) while on Humira. Discontinuation of Humira therapy should be considered in patients with confirmed significant haematologic abnormalities.VaccinationsSimilar antibody responses to the standard 23-valent pneumococcal vaccine and the influenza trivalent virus vaccination were observed in a study in 226 adult subjects with rheumatoid arthritis who were treated with adalimumab or placebo. No data are available on the secondary transmission of infection by live vaccines in patients receiving Humira. Patients on Humira may receive concurrent vaccinations, except for live vaccines.Congestive heart failureIn a clinical trial with another TNF antagonist worsening congestive heart failure and increased mortality due to congestive heart failure have been observed. Cases of worsening congestive heart failure have also been reported in patients receiving Humira. Humira should be used with caution in patients with mild heart failure (NYHA class I/II). Humira is contraindicated in moderate or severe heart failure.Treatment with Humira must be discontinued in patients who develop new or worsening symptoms of congestive heart failure.Autoimmune processesTreatment with Humira may result in the formation of autoimmune antibodies. The impact of long-term treatment with Humira on the development of autoimmune diseases is unknown. If a patient develops symptoms suggestive of a lupus-like syndrome following treatment with Humira and is positive for antibodies against double-stranded DNA, further treatment with Humira should not be given.Concurrent administration of TNF-alpha inhibitor and anakinra. Serious infections were seen in clinical studies with concurrent use of anakinra and another TNF-antagonist, etanercept, with no added clinical benefit compared to etanercept alone. Because of the nature of the adverse events seen with the combination of etanercept and anakinra therapy, similar toxicities may also result from the combination of anakinra and other TNF-antagonists. Therefore, the combination of adalimumab and anakinra is not recommended.SurgeryThere is limited safety experience of surgical procedures in patients treated with Humira. The long half-life of adalimumab should be taken into consideration if a surgical procedure is planned. A patient who requires surgery while on Humira should be closely monitored for infections, and appropriate actions should be taken. There is limited safety experience in patients undergoing arthroplasty while receiving Humira.Small bowel obstructionFailure to respond to treatment for Crohn’s disease may indicate the presence of fixed fibrotic stricture that may require surgical treatment. Available data suggest that Humira does not worsen or cause strictures.Pregnancy and LactationFor Humira, no clinical data on exposed pregnancies are available.In a developmental toxicity study conducted in monkeys, there was no indication of maternal toxicity, embryotoxicity or teratogenicity. Preclinical data on postnatal toxicity and fertility effects of adalimumab are not available.Due to its inhibition of TNFα, adalimumab administered during pregnancy could affect normal immune responses in the newborn. Administration of adalimumab is not recommended during pregnancy. Women of childbearing potential are strongly recommended to use adequate contraception to prevent pregnancy and continue its use for at least five months after the last Humira treatment.Use during lactationIt is not known whether adalimumab is excreted in human milk or absorbed systemically after ingestion.However, because human immunoglobulins are excreted in milk, women must not breast-feed for at least five months after the last Humira treatment.Effects on ability to drive and use machinesNo studies on the effects on the ability to drive and use machines have been performed.How to use HumiraAlways take Humira exactly as your doctor has instructed you. You should check with your doctor or pharmacist if you are unsure.Humira is injected under the skin (subcutaneous use). The usual dose for adults with rheumatoid arthritis is 40 mg adalimumab given every other week as a single dose.You should continue to inject Humira for as long as instructed by your doctor.Methotrexate is continued while using Humira. If your doctor determines that methotrexate is inappropriate, Humira can be given alone.If you do not receive methotrexate with your Humira therapy, your doctor may decide to give 40 mg adalimumab every week.OverdosageNo dose-limiting toxicity was observed during clinical trials. The highest dose level evaluated has been multiple intravenous doses of 10 mg/kg.Drug InteractionsHumira has been studied both in rheumatoid arthritis and psoriatic arthritis patients taking Humira as monotherapy and those taking concomitant methotrexate. Antibody formation was lower when Humira was given together with methotrexate in comparison with use as monotherapy. Administration of Humira without methotrexate resulted in increased formation of antibodies, increased clearance and reduced efficacy of adalimumab.IncompatibilitiesIn the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products.Dosage AdministrationHumira treatment should be initiated and supervised by specialist physicians experienced in the diagnosis and treatment of rheumatoid arthritis, psoriatic arthritis or ankylosing spondylitis or Crohn’s disease. After proper training in injection technique, patients may self-inject with Humira if their physician determines that it is appropriate and with medical follow-up as necessary.During treatment with Humira, other concomitant therapies (e.g., corticosteroids and/or immunomodulatory agents) should be optimised.AdultsRheumatoid ArthritisThe recommended dose of Humira for adult patients with rheumatoid arthritis is 40 mg adalimumab administered every other week as a single dose via subcutaneous injection. Methotrexate should be continued during treatment with Humira.Glucocorticoids, salicylates, nonsteroidal anti-inflammatory drugs, or analgesics can be continued during treatment with Humira. Regarding combination with disease modifying anti-rheumatic drugs other than methotrexate see special warnings/precautions for use and pharmacodynamic properties section.In monotherapy, some patients who experience a decrease in their response to Humira may benefit from an increase in dose intensity to 40 mg adalimumab every week.Psoriatic Arthritis and ankylosing spondylitisThe recommended dose of Humira for patients with psoriatic arthritis and ankylosing spondylitis is 40 mg adalimumab administered every other week as a single dose via subcutaneous injection.

37
For all of the above indications, available data suggest that the clinical response is usually achieved within 12 weeks of treatment. Continued therapy should be carefully reconsidered in a patient not responding within this time period.Crohn’s diseaseThe recommended Humira induction dose regimen for adult patients with severe Crohn’s disease is 80 mg at week 0 followed by 40 mg at week 2. In case there is a need for a more rapid response to therapy, the regimen 160 mg at week 0 (dose can be administered as four injections in one day or as two injections per day for two consecutive days), 80 mg at week 2, can be used with the awareness that the risk for adverse events is higher during induction.After induction treatment, the recommended dose is 40 mg every other week via subcutaneous injection. Alternatively, if a patient has stopped Humira and signs and symptoms of disease recur, Humira may be re-administered. There is little experience from re-administration after more than 8 weeks since the previous dose.During maintenance treatment, corticosteroids may be tapered in accordance with clinical practice guidelines.Some patients who experience decrease in their response may benefit from an increase in dose intensity to 40 mg Humira every week.Some patients who have not responded by week 4 may benefit from continued maintenance therapy through week 12. Continued therapy should be carefully reconsidered in a patient not responding within this time period.Elderly patientsNo dose adjustment is required.Children and adolescentsThere is no experience in children.Impaired renal and/or hepatic function Humira has not been studied in these patient populations. No dose recommendations can be made.Instructions for preparing and giving an injection of Humira:The following instructions explain how to inject Humira. Please read the instructions carefully and follow them step by step. You will be instructed by your doctor or his/her assistant on the technique of self-injection. Do not attempt to self-inject until you are sure that you understand how to prepare and give the injection. After proper training, the injection can be self-administered or given by another person, for example a family member or friend.This injection should not be mixed in the same syringe or vial with any other medicine.1) Setting up- Wash your hands thoroughly- Set up the following items on a clean surface- One pre-filled syringe of Humira for injection- One alcohol pad- Look at the expiry date on the syringe.Do not use the product after the month and year shown.2) Choosing and preparing an injection site- Choose a site on your thigh or stomach.- Each new injection should be given at least 3 cm from the last injection site.- Do not inject in an area where the skin is reddened, bruised, or hard. This may mean there is an infection.- Wipe the injection site with the enclosed alcohol pad, using a circular motion.- Do not touch the area again before injecting.3) Injecting Humira- Remove cap from needle syringe, being careful not to touch the needle or let it touch any surface.- With one hand, gently grasp the cleaned areas of skin and hold firmly.- With the other hand, hold syringe at 45-degree angle to skin, with the grooved side up.- With one quick, short motion, push needle all the way into skin.- Release the skin with the first hand.- Push plunger to inject solution – it can take from 2 to 5 seconds to empty the syringe.- When the syringe is empty, remove the needle from skin, being careful to keep it at the same angle as when it was inserted.- Using your thumb or a piece of gauze, apply pressure over the injection site for 10 seconds. A little bleeding may occur. Do not rub the injection site. Use a plaster if you want to.4) Throwing away supplies- The Humira syringe should NEVER be reused. NEVER recap a needle.- After injecting Humira, immediately throw away the used syringe in a special container as instructed by your doctor, nurse or pharmacist.- Keep this container out of the reach of children.If you use more Humira than you should:If you accidentally inject Humira more frequently than told to by your doctor, you should call your doctor. Always take the outer carton of medicine with you, even if it is empty.If you forget to take Humira:If you forget to give yourself an injection, you should inject the next dose of Humira as soon as you remember. Then take your next dose as you would have on your originally scheduled day, had you not forgotten a dose.The proportion of patients who discontinued treatment due to adverse events during the double-blind, controlled portion of Studies I-IX, CLASSIC I, GAIN and CHARM was 5.7% for patients taking Humira and 5.3% for control treated patients.StorageStore in a refrigerator (2°C – 8°C). Keep the syringe in the outer carton.Do not freeze.The shelf life is 18 months.PackagingHumira 40 mg solution for injection in single-use pre-filled syringe (type I glass) for patient use is available in packs of:- 1 pre-filled syringe (0.8 ml sterile solution) with 1 alcohol pad in a blister.- 2 pre-filled syringes (0.8 ml sterile solution), each with 1 alcohol pad, in a blister.- 4 pre-filled syringes (0.8 ml sterile solution), each with 1 alcohol pad, in a blister.- 6 pre-filled syringes (0.8 ml sterile solution), each with 1 alcohol pad, in a blister.Not all pack sizes may be marketed.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
ISOPTIN (80 MG & 240 MG) ®GeneralCompositionIsoptin 80 mgOne film-coated tablet contains 80 mg of verapamil hydrochlorideIsoptin SR 240 mg

38
1 prolonged-release tablet contains 240 mg of verapamil hydrochloridePropertiesPharmacodynamicVerapamil hydrochloride belongs to the class of calcium channel blockers. These substances inhibit the influx of calcium through muscle cell membranes. Verapamil hydrochloride acts as a calcium channel blocker on smooth muscle cells, especially in the blood vessels and gastrointestinal tract. Its effect on the smooth muscles manifests as vasodilatation. As a calcium channel blocker, verapamil hydrochloride also has a marked effect on the myocardium. Its effect on the AV node manifests as a prolongation of conduction time. A negative inotropic effect may arise in the working myocardium. In man, verapamil hydrochloride reduces total peripheral resistance as a result of vasodilatation. without a reflectory increase of cardiac output. This lowers the blood pressure accordingly.PharmacokineticFollowing oral administration, 80% to 90% of the verapamil dose is rapidly absorbed from the small intestine. Owing to an extensive first pass metabolism bioavailability is only approximately 20%. Peak plasma levels are achieved 1 to 2 hours after oral dosing. Plasma protein binding of verapamil hydrochloride is approximately 90%.IndicationsSymptomatic coronary artery disease:chronic stable angina pectoris (exercise-induced angina)unstable angina pectoris (crescendo angina, angina at rest)Vasospastic angina pectoris (Prinzmetal‘s angina, variant angina)Post-myocardial infarction angina pectoris in patients without heart failure if beta-blockers are not indicated.For treatment of cardiac arrhythmia in:paroxysmal supraventricular tachycardiaAtrial fibrillation/atrial flutter with rapid atrioventricular conduction (except in Wolff-Parkinson-White syndrome).Hypertension.ContraindicationsIsoptin may not be used in the following cases: Hypersensitivity (allergy) to the active substance verapamil hydrochloride or any of the other ingredients of Isoptin, Cardiovascular shock, Acute myocardial infarction with complications (bradycardia, hypotension, left heart failure), Severe conduction disorders (such as 2nd or 3rd degree SA or AV block), Sick sinus syndrome, Manifest heart failure, Atrial fibrillation and/or flutter accompanied by WPW syndrome (increases risk of triggering ventricular tachycardia). Concomitant intravenous administration of beta-blockers is not recommended in patients receiving Isoptin (except in an intensive care setting).Side EffectsThe side effects given below may occur during Isoptin treatment. The classification of side effects is based on their rate of incidence as listed below:Very common: > 10 %,Common: > 1 % - < 10 %,Uncommon: > 0.1 % - < 1 %Rare: > 0.01 % - < 0.1 %,Very rare: < 0.01%, including isolated casesNote: In patients with pacemakers, the pacing and sensing threshold may be raised while on verapamil hydrochloride treatment. Undesirable EffectsMetabolism Uncommon Reduction of glucose tolerancePsychological Common Fatigue, nervousness.
Nervous System CommonVery rare
Dizziness or lightheadedness, paresthesia, neuropathy and tremor Extrapyramidal symptoms (Parkinson's syndrome, choreoathetosis, dystonic syndromes): experience indicates that these side effects resolve when Isoptin is discontinued
Cardiovascular system
CommonUncommonVery rare
Development of heart failure or exacerbation of existing heart failure. Excessive lowering of blood pressure and/or postural hypotension, sinus bradycardia, 1st degree AV block, ankle oedema, flushing, reddening of the skin and a sensation of warmth Palpitations, tachycardia, 2nd or 3rd degree AV block Sinus arrest with asystole
Respiratory tract Uncommon BronchospasmEar and vestibular system Uncommon Tinnitus
Gastrointestinaltract
Very commonUncommonVery rare
Nausea, bloating, constipationVomitingIleus, gingival hyperplasia (gingivitis, bleeding gums): resolves when Isoptin is discontinued
Liver UncommonReversible elevation of hepatic enzymes, probably as a manifestation of allergic hepatatis
Skin and mucosa (allergic reactions)
CommonRareVery rare
Allergic reactions such as erythema, pruritus, urticaria, maculopapular exanthema, erythromelalgia Purpura Angioneurotic edema, Stevens-Johnson syndrome, photodermatitis
Musculoskeletalsystem
RareVery rare
Arthralgia, myalgia, weak musclesExacerbation of myasthenia gravis, of Lambert-Eaton syndrome or of advanced Duchenne's muscular dystrophy

39
Breast and reproductive organs
UncommonRareVery rare
Erectile dysfunction Gynecomastia in the long-term treatment of elderly patients: Past experience indicates that this condition resolves when Isoptin is discontinued Elevation of prolactin levels, galactorrhea
General Common HeadachePrecautionsParticularly close medical supervision is necessary in the presence of: 1st degree AV block, Hypotension (systolic BP below 90 mmHg), Bradycardia (heart rate below 50 beats per minute), Severely impaired liver function, Conditions associated with impairment of neuromuscular transmission (myasthenia gravis, Lambert-Eaton syndrome, advanced Duchenne's muscular dystrophy).Drug interactions: Verapamil is a substrate and inhibitor of the P450 3A4 cytochrome. If given at the same time as simvastatin, a substance which is metabolised via the P450 3A4 cytochrome, verapamil may increase simvastatin levels in the blood, and may thereby increase the risk of muscular toxicity. The simvastatin dose should therefore be adjusted accordingly (see manufacturer's product information).Pregnancy and LactationPregnancy: Verapamil hydrochloride crosses the placental barrier. Plasma concentrations in umbilical cord blood are 20% - 92% of those in the mother's blood. The database on verapamil hydrochloride use during pregnancy is insufficient. However, data from a limited number of pregnancies in women receiving oral treatment does not suggest that verapamil hydrochloride is teratogenic. Animal studies have demonstrated reproductive toxicity. Therefore, verapamil hydrochloride should not be taken during the first and second trimesters of pregnancy. Verapamil hydrochloride may be taken during the third trimester of pregnancy only if strictly necessary and if the benefits exceed the risks to the mother and child.Breastfeeding: Since active substance is excreted into breast milk (concentration in milk: approximately 23% that in the maternal plasma) verapamil hydrochloride should not be taken during the lactation period. There is evidence to indicate that verapamil hydrochloride may cause hyperprolactinemia and galactorrhea in isolated cases.Effects on ability to drive and use machinesTreatment with Isoptin should be monitored at regular intervals by the physician. Depending on the individual response, Isoptin may affect judgment and motor skills to the point of impairing the ability to drive a vehicle, operate machinery, or work under hazardous conditions. This applies particularly at the beginning of treatment, on increasing the dose, or when switching to another medication as well as when alcohol is consumed simultaneously.OverdosageSymptoms of overdosage: The symptoms of verapamil hydrochloride overdosing will depend on the amount taken, the time at which countermeasures are initiated and age-related myocardial contractility. The following symptoms are observed in severe cases of verapamil poisoning: Severe drop in blood pressure, heart failure, bradycardia or tachycardia (e.g. junctional escape rhythm with AV dissociation and high-grade AV block) which can result in cardiovascular shock and cardiac arrest. Clouding of consciousness to the point of coma, hyperglycemia, hypokalemia, metabolic acidosis, hypoxia, cardiogenic shock with pulmonary edema, impairment of kidney function and seizures. There have been occasional reports of fatalities.Management of overdosage: The main therapeutic aims are to achieve elimination of the compound and to re-instate stable cardiovascular function. The therapeutic measures to be taken will depend upon the time and route of administration as well as the type and severity of the symptoms. In cases of poisoning with large quantities of prolonged-release formulations, it is important to note that drug may be released and absorbed in the intestine for more than 48 hours after intake. Gastric lavage is advised for oral overdosing with verapamil hydrochloride, even if more than 12 hours have elapsed since ingestion, if no gastrointestinal motility (bowel sounds) is evident. If overdosage with prolonged release products is suspected, a variety of countermeasures are indicated, e.g. induced vomiting, gastric and small intestine lavage monitored by endoscopy, intestinal lavage, purgatives and high colonic enemas. Haemodialysis is not recommended as verapamil hydrochloride is not amenable to dialysis. Haemofiltration and, possibly, plasmapheresis (extensive plasma protein binding of the calcium channel blockers) are, however, recommended. Standard intensive care resuscitation measures such as extrathoracic cardiac massage, ventilation, defibrillation and pacemaker therapy.Specific measures: Elimination of cardiodepressant effects, hypotension and bradycardia:Bradycardia is treated symptomatically by administering atropine and/or beta sympathomimetics (isoprenaline, orciprenaline). Life-threatening bradycardia requires short-term pacemaker therapy. Calcium is a specific antidote, e.g. 10 – 20 mL of a 10% calcium gluconate solution intravenously (2.25 to 4.5 mmol), repeated as necessary or given by continuous infusion (e.g. 5 mmol/hour). Hypotension as a result of cardiogenic shock and arterial vasodilation is treated with dopamine (up to 25 µg per kg of body weight per minute), dobutamine (up to 15 µg per kg of body weight per minute), epinephrine or norepinephrine. Dosage of these drugs depends solely on the response achieved. Serum calcium levels should be maintained at upper normal limits or slightly above. Owing to the arterial dilatation, fluids should be substituted (Ringer's or saline solution) in the early stages of detoxification.Drug InteractionsThe following interactions with this medicinal product must be kept in mind:Antiarrhythmics, beta receptor blockers, inhaled anesthetics: Mutual potentiation of cardiovascular effects (high grade atrioventricular block, marked lowering of heart rate, occurrence of heart failure, excessive blood pressure lowering). Concomitant intravenous administration of beta-blockers is not recommended in patients receiving Isoptin (except in an intensive care setting).Antihypertensives, diuretics, vasodilators: Potentiation of the antihypertensive effect.Digoxin: Elevation of digoxin plasma levels as a result of diminished renal excretion (monitor for symptoms of digoxin overdose and reduce the glycoside dose if necessary, after having determined digoxin plasma levels as appropriate).Quinidine: Excessive blood pressure lowering is possible. Pulmonary edema may occur in subjects with hypertrophic obstructive cardiomyopathy. Elevation of quinidine plasma level.Carbamazepine: Potentiation of carbamazepine effect. Enhanced neurotoxicity.Lithium: Diminished lithium efficacy. Increased lithium neurotoxicity.Muscle relaxants: Verapamil hydrochloride may potentiate the effects of these medicinal products.Acetylsalicylic acid: Increased bleeding propensity.Ethanol: Delayed ethanol breakdown and elevation of ethanol plasma levels, resulting in enhancement of the effect of alcohol through verapamil.Interactions due to cytochrome P450 isoenzyme 3A4Verapamil hydrochloride is primarily metabolized by cytochrome P450 isoenzyme 3A4 in the liver and inhibits this enzyme. The following interactions must be observed in this regard:Other inhibitors of the cytochrome P450 isoenzyme 3A4, such as, azole antifungals (e.g. clotrimazole and ketoconazole), protease inhibitors (e.g. ritonavir and indinavir), macrolides (e.g. erythromycin and clarithromycin) and cimetidine: Elevation of verapamil hydrochloride plasma levels and/or plasma levels of these medicinal products owing to (mutual) effects on drug metabolism.Inducers of the cytochrome P450 isoenzyme 3A4 such as phenytoin, rifampicin, phenobarbital, carbamazepine: Lowering of verapamil hydrochloride plasma levels andattenuation of the effect of verapamil hydrochloride.

40
Cytochrome P450 isoenzyme 3A4 substrates, such as, antiarrhythmic agents (e.g. amiodarone and quinidine), CSE inhibitors (e.g. lovastatin and atorvastatin), midazolam, cyclosporin, theophylline, prazosine: Elevation of the plasma levels of these medicinal products.Simvastatin: The risk of myopathy/rhabdomyolysis is increased when higher doses of verapamil and simvastatin are given concomitantly. The simvastatin dose should therefore be adjusted accordingly (see manufacturer's product information).Note: Patients taking Isoptin should avoid foods and drinks containing grapefruit. Grapefruit can increase verapamil hydrochloride plasma levels.IncompatibilitiesNot applicableDosage AdministrationVerapamil hydrochloride, the active substance in Isoptin, should be dosed individually in accordance with the severity of disease. Long-standing clinical experience shows that the average daily dose in almost all indications is between 240 mg and 360 mg. A daily dosage of 480 mg should not be exceeded in long-term therapy; short-term increases are possible.Unless otherwise prescribed, the following dosage guidelines apply:For Isoptin 80 mg:Adults and adolescents weighing more than 50 kg:Coronary heart disease: The recommended daily dosage is 240 mg – 480 mg verapamil hydrochloride in 3 – 4 doses, as follows: 1 Isoptin 80 mg film-coated tablet 3 to 4 times daily (equivalent to 240 mg – 320 mg verapamil hydrochloride per day). For patients requiring higher dosages (e.g. 360 mg – 480 mg verapamil hydrochloride/day), formulations with a more suitable active drug content should be used.Hypertension: The recommended daily dosage is 240 mg – 360 mg verapamil hydrochloride in 3 doses, as follows: 1 Isoptin 80 mg film-coated tablet 3 times daily (equivalent to 240 mg verapamil hydrochloride per day). For patients requiring higher doses (e.g. 360 mg verapamil hydrochloride/day), formulations with a more suitable active drug content should be used.Paroxysmal supraventricular tachycardia, atrial fibrillation/atrial flutter: The recommended daily dosage is 240 mg – 480 mg verapamil hydrochloride in 2 – 5 doses, as follows: 1 Isoptin 80 mg film-coated tablet 3 to 4 times daily (equivalent to 240 mg – 320 mg verapamil hydrochloride per day). For patients requiring higher dosages (e.g. 360 mg - 480 mg verapamil hydrochloride/day), formulations with a more suitable active drug content should be used.Children: (only for cardiac arrhythmia):Older preschool children up to age 6: The recommended daily dosage is 80 mg – 120 mg verapamil hydrochloride in 2 – 3 doses.Schoolchildren aged 6 - 14: The recommended daily dosage is 80 mg - 360 mg verapamil hydrochloride in 2 – 4 doses, as follows: 1 Isoptin 80 mg film-coated tablet 2 to 4 times daily (equivalent to 160 mg – 320 mg verapamil hydrochloride per day). Isoptin 80 mg is used if lower doses (e.g. 80 mg verapamil hydrochloride per day) have not produced a satisfactory response. For patients requiring higher doses (e.g. 360 mg verapamil hydrochloride/day), formulations with a more suitable active drug content should be used.For Isoptin SR 240 mg:Adults and adolescents weighing more than 50 kg:Coronary heart disease: The recommended daily dosage is 240 mg – 480 mg verapamil hydrochloride in 2 doses, as follows: ½ - 1 Isoptin SR 240 mg tablet 2 times daily (equivalent to 240 mg – 480 mg verapamil hydrochloride per day). Isoptin SR 240 mg is used if lower doses (e.g. 240 mgverapamil hydrochloride per day) have not produced a satisfactory response.Hypertension: The recommended daily dosage is 240 mg – 480 mg verapamil hydrochloride in 1 – 2 doses, as follows: 1 Isoptin SR 240 mg tablet once a day in the morning (equivalent to 240 mg verapamil hydrochloride per day). If the response is unsatisfactory, add ½ - 1 Isoptin SR 240 mg tablet in the evening (equivalent to 360 mg - 480 mg verapamil hydrochloride per day).Paroxysmal supraventricular tachycardia, atrial fibrillation/atrial flutter: The recommended daily dosage is 240 mg – 480 mg verapamil hydrochloride in 2 doses, as follows: ½ - 1 Isoptin SR 240 mg tablet 2 times daily (equivalent to 240 mg – 480 mg verapamil hydrochloride per day). Isoptin SR 240 mg is used if lower doses (e.g. 240 mg verapamil hydrochloride per day) have not produced a satisfactory response.Impaired liver function:In patients with impaired hepatic function, the effect of verapamil hydrochloride is enhanced and prolonged due to slower metabolism of the drug depending on the degree of impairment. Therefore, the dosage needs to be adjusted with special caution in such cases, and low doses should be given initially (e.g. 40 mg verapamil hydrochloride 2 – 3 times daily in subjects with impaired liver function, equivalent to 80 mg – 120 mg verapamil hydrochloride per day).The tablets are taken whole without being chewed or sucked, and with sufficient liquid (e.g. a glass of water; not grapefruit juice), preferably with or shortly after meals. Do not take Isoptin while lying down. Verapamil hydrochloride must not be administered to post-myocardial infarction patients with angina pectoris until 7 days after the acute myocardial infarction event. The product may be taken indefinitely. Isoptin should not be discontinued abruptly after long-term use. Tapering off the dosage is recommended.StorageIsoptin 80 mg:Do not store above 25°C.Isoptin SR 240 mg:Do not store above 25°C.Store in the original pack.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
ITRIN ®CompositionTerazosin hydrochloride is a selective blocking drug with a long-lasting action towards the adrenergic receptors alpha-1. Chemically it is a derivative of quinazoline having the following formula: 2-[4-(tetrahydro-2-furanyl)-carbonyl] 1-piperazinyl 6,7-dimethoxy-4-quinazolineamine monohydrochloride dihydrate.PropertiesPharmacodynamics Terazosin is a competitive/selective alpha-1-blocking agent producing reduction of the peripheral vascular resistance and smooth muscle relaxation.Benign Prostatic Hyperplasia (BPH):The symptoms associated with BPH are related to bladder outlet obstruction, which is comprised of two underlying components: a static component due to an increase in prostate size and a dynamic component which is due to an increase in smooth muscle tone in the prostate and bladder neck, leading to constriction of the bladder outlet. Since the bladder body contains few alpha-1-adrenoreceptors while the bladder neck and the prostate contain high density of alpha-1-adrenoreceptors, selective alpha-1-blockade following administration of terazosin decrease the dynamic component of BPH by decreasing bladder outlet resistance without impairing bladder contraction and decreasing prostate muscular tone leading to reduction in symptoms of BPH and improvement of urine flow rates. Clinical studies have demonstrated that the size of the prostate does not correlate with the severity of BPH.Hypertension: Since terazosin develops a selective alpha-1 blocking action, it causes a decrease in blood pressure by decreasing total peripheral vascular resistance. Terazosin decreases blood pressure gradually within 15 minutes following oral administration. The

41
hypotensive action of the drug produced by its daily single dose is clinically manifested in an appreciable way during the whole period of 24 hours. The reduction of blood pressure following the oral daily dose manifests itself gradually; the eventual occurrence of orthostatic effects during the first day of therapy is comparable to that observed with other quinazoline derivatives. Terazosin has proved to possess the same efficiency as other antihypertensive preparations with a clear therapeutic activity.BPH and HypertensionOn long-term therapy, terazosin did not induce tolerance in any of the two indications. It is known that quinazoline derivatives, like terazosin, induce positive effects on the serum lipids, decreasing significantly total cholesterol, LDL, VLDL, and LDL/cholesterol ratio and a favourable reduction of the triglyceride levels. This action represents an advantage with respect to diuretics and beta-blocking drugs which, as known, have unfavourable effects on these parameters.Since the arterial hypertension and the increase of serum lipids are strictly related to the pathology of the coronary, the positive effect exerted by terazosin both on the arterial pressure and on the lipids, may result in reduction of the risk factors for coronary pathies.The long term therapy with terazosin does not produce any clinical significant changes in the most important laboratory parameters as (glycemia, uricemia, creatininemia, azotemia and transaminasemia); therefore, the drug can be safely used in diabetics, hyperuricemics, and elderly patients.Pharmacokinetics Terazosin administered orally is proved to be completely absorbed in man. The effect of food on the absorption of the drug is negligible. The plasma levels of the drug reach the peak concentration within one hour after oral administration, and then decline with a half-life of approximately 12 hours, thus maintaining levels of therapeutic effect allowing the drug to be administered only once daily.IndicationsTerazosin HCL is indicated in the symptomatic treatment of Benign Prostatic Hyperplasia (BPH) and in the therapy of mild to moderate hypertension as single therapy or associated with other antihypertensive drugs.ContraindicationsAscertained or presumed hypersensitivity to quinazoline derivatives, history of orthostatic hypotension and in pregnancy and lactation.Side EffectsBenign Prostatic Hyperplasia (BPH):The following side effects have been reported: asthenia, palpitations, nausea, dizziness, somnolence, nasal congestion and blurred vision. Like all quinazoline derivatives, it can cause orthostatic hypotension, particularly associated with the first dose.Hypertension:The following side effects have been reported: vertigo, headache, fever outsets; abdominal, cervical and thoracic pains. In most cases such symptoms disappear by carrying on the therapy without requiring reduction of dosage.As with all quinazoline derivatives, troubles of postural nature can occur, as a result of the first dose. Also other symptoms have been reported, but they are not distinguishable clearly from those possibly occurring by themselves in hypertensive subjects not under terazosin therapy, particularly: depression, insomnia, irritability and paresthesia.PrecautionsSafety and effectiveness in children have not been ascertained. Since in some cases signs of drowsiness or vertigo have been manifested, it is recommended to be careful in driving motor cars and/or operating machinery requiring particular attention for at least 12 hours after the administration of the starting dose or in case the dose is increased. In case of overdosage and consequent hypotension, keep the patient lying on his back with the head in downward position.While treating BPH, should ITRIN be administered in combination with antihypertensive drugs, their dosage should be adjusted, following the physician's advice. Keep out of reach of children.Drug InteractionsInteractions with the following drugs were observed : thiazide diuretics, beta-blocking drugs, analgesics, non-steroidal anti-inflammatory drugs, hypoglycemic drugs, antibiotics, anxiolytics and bronchodilators.Dosage AdministrationBenign Prostatic Hyperplasia (BPH):The usual recommended dose range is 5 to 10 mg administered once a day. Treatment should always be initiated with 1 mg dose (half -2 mg tablet) given at bed time, then the daily dose should be doubled every two weeks up to 5 mg or 10 mg per day.If the drug administration is discontinued for several days, therapy should be reinstituted using the initial dosage regimen.HypertensionThe dosage of ITRIN must be adjusted following the behaviour of the blood pressure values. It is advisable to start treatment with 1 mg (half -2 mg tablet) at bedtime as a starting dose. After one to two weeks of treatment, the daily single dose can be increased to 2 mg, and then to 5 or 10 mg daily, until the desired value of the blood pressure is achieved. In case of complementing the therapy with a thiazide diuretic or a beta-blocking agent, it may be necessary to reduce the Itrin dose.PackagingBlisters of 30 tablets of 2mg eachBlisters of 14 tablets of 5mg each
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
KALETRA ®GeneralLopinavir /RitonavirKaletra 200 mg/50 mg film-coated tabletsCompositionEach film-coated tablet contains 200 mg of lopinavir co-formulated with 50 mg of ritonavir as a pharmacokinetic enhancer.PropertiesFilm-coated tabletPharmacodynamicMechanism of action: Lopinavir provides the antiviral activity of Kaletra. Lopinavir is an inhibitor of the HIV-1 and HIV-2 proteases. Inhibition of HIV protease prevents cleavage of the gag-pol polyprotein resulting in the production of immature, non-infectious virus.Antiviral activity in vitro: the in vitro antiviral activity of lopinavir against laboratory and clinical HIV strains was evaluated in acutely infected lymphoblastic cell lines and peripheral blood lymphocytes, respectively. In the absence of human serum, the mean EC50 of lopinavir against five different HIV-1 laboratory strains was 19 nM. In the absence and presence of 50% human serum, the mean EC50 of lopinavir against HIV-1IIIB in MT4 cells was 17 nM and 102 nM, respectively. In the absence of human serum, the mean EC50 of lopinavir was 6.5 nM against several HIV-1 clinical isolates.ResistanceHIV-1 isolates with reduced susceptibility to lopinavir have been selected in vitro. HIV-1 has been passaged in vitro with lopinavir alone and with lopinavir plus ritonavir at concentration ratios representing the range of plasma concentration ratios observed during Kaletra therapy.

42
Genotypic and phenotypic analysis of viruses selected in these passages suggest that the presence of ritonavir, at these concentration ratios, does not measurably influence the selection of lopinavir-resistant viruses. Overall, the in vitro characterisation of phenotypic cross-resistance between lopinavir and other protease inhibitors suggest that decreased susceptibility to lopinavir correlated closely with decreased susceptibility to ritonavir and indinavir, but did not correlate closely with decreased susceptibility to amprenavir, saquinavir, and nelfinavir. Genotypic correlates of reduced phenotypic susceptibility to lopinavir in viruses selected by other protease inhibitors. The in vitro antiviral activity of lopinavir against 112 clinical isolates taken from patients failing therapy with one or more protease inhibitors was assessed. Within this panel, the following mutations in HIV protease were associated with reduced in vitro susceptibility to lopinavir: L10F/I/R/V, K20M/R, L24I, M46I/L, F53L, I54L/T/V, L63P, A71I/L/T/V, V82A/F/T, I84V and L90M. The median EC50 of lopinavir against isolates with 0 − 3, 4 − 5, 6 − 7 and 8 − 10 mutations at the above amino acid positions was 0.8, 2.7 13.5 and 44.0-fold higher than the EC50 against wild type HIV, respectively. The 16 viruses that displayed > 20-fold change in susceptibility all contained mutations at positions 10, 54, 63 plus 82 and/or 84. In addition, they contained a median of 3 mutations at amino acid positions 20, 24, 46, 53, 71 and 90.Antiviral activity of Kaletra in patients failing protease inhibitor therapy: the clinical relevance of reduced in vitro susceptibility to lopinavir has been examined by assessing the virologic response to Kaletra therapy, with respect to baseline viral genotype and phenotype, in 56 patients previous failing therapy with multiple protease inhibitors. The EC50 of lopinavir against the 56 baseline viral isolates ranged from 0.6 to 96-fold higher than the EC50 against wild type HIV. After 48 weeks of treatment with Kaletra, efavirenz and nucleoside reverse transcriptase inhibitors, plasma HIV RNA ≤ 400 copies/ml was observed in 93% (25/27), 73% (11/15), and 25% (2/8) of patients with < 10-fold, 10 to 40-fold, and > 40-fold reduced susceptibility to lopinavir at baseline, respectively. In addition, virologic response was observed in 91% (21/23), 71% (15/21) and 33% (2/6) patients with 0 − 5, 6 − 7, and 8 − 10 mutations of the above mutations in HIV protease associated with reduced in vitro susceptibility to lopinavir. Since these patients had not previously been exposed to either Kaletra or efavirenz, part of the response may be attributed to the antiviral activity of efavirenz, particularly in patients harbouring highly lopinavir resistant virus. The study did not contain a control arm of patients not receiving Kaletra.Selection of viral resistance during Kaletra therapy: in Phase II studies of 227 antiretroviral treatment naïve and protease inhibitor experienced patients, isolates from four patients with quantifiable (> 400 copies/ml) viral load following treatment with Kaletra for ≥ 12 weeks displayed significantly reduced susceptibility to lopinavir compared to the corresponding baseline viral isolates. The mean EC50 of lopinavir against the four baseline isolates was 2.8 fold (range: 0.7 to 5.2 fold) higher than the EC50 against wild type HIV, and each of the four baseline isolates contained four or more mutations in HIV protease associated with resistance to protease inhibitors. Following treatment of the four patients with Kaletra, the mean EC50 of lopinavir increased to 55-fold (range: 9.4 to 99-fold) compared to wild type HIV, and 2 − 3 additional mutations at amino acids 10, 24, 33, 46, 54, 63, 71 and/or 82 were observed. In a Phase II study (M97-720) through 204 weeks of treatment, genotypic analysis of viral isolates was successfully conducted in 11 of 16 patients with confirmed HIV RNA above 400 copies/ml revealed no primary or active site mutations in protease (amino acids at positions 8, 30, 32, 36, 47, 48, 50, 82, 84 and 90) or protease inhibitor phenotypic resistance.Cross-resistance: at this stage of development, little information is available on the cross-resistance of viruses selected during therapy with Kaletra. Isolates from 4 patients previously treated with one or more protease inhibitors that developed increased lopinavir phenotypic resistance during Kaletra therapy either remained or developed cross-resistance to ritonavir, indinavir, and nelfinavir. All rebound viruses either remained fully sensitive or demonstrated modestly reduced susceptibility to amprenavir (up to 8.6-fold concurrent with 99-fold resistance to lopinavir). The rebound isolates from the two patients with no prior saquinavir treatment remained fully sensitive to saquinavir.Clinical pharmacodynamic dataThe effects of Kaletra (in combination with other antiretroviral agents) on biological markers (plasma HIV RNA levels and CD4 counts) have been investigated in a controlled study of Kaletra of 48 weeks duration, and in additional studies of Kaletra of 204 weeks duration.Adult UsePatients without prior antiretroviral therapyStudy M98-863 is a randomised, double-blind trial of 653 antiretroviral treatment naïve patients investigating Kaletra (400/100 mg twice daily) compared to nelfinavir (750 mg three times daily) plus nucleoside reverse transcriptase inhibitors. By intent to treat analysis where patients with missing values are considered virologic failures, the proportion of patients at 48 weeks with HIV RNA < 400 copies/ml in the Kaletra arm was 75% and 63% in the nelfinavir arm. Mean baseline CD4 cell count was 259 cells/mm3 (range: 2 to 949 cells/ mm3) and mean baseline plasma HIV-1 RNA was 4.9 log10 copies/ml (range: 2.6 to 6.8 log10 copies/ml). Through 48 weeks of therapy, the proportion of patients in the Kaletra arm with plasma RNA < 50 copies/ml was 67% and 52% in the nelfinavir arm. The mean increase from baseline in CD4 cell count was 207 cells/mm3 in the Kaletra arm and 195 cells/mm3 in the nelfinavir arm. Through 48 weeks of therapy, a statistically significantly higher proportion of patients in the Kaletra arm had HIV RNA < 50 copies/ml compared to the nelfinavir arm. Sustained virological response to Kaletra (in combination with lamivudine and stavudine) has been also observed in a small Phase II study (M97-720) through 204 weeks of treatment. Through 204 weeks of treatment, the proportion of patients with HIV RNA < 400 (< 50) copies/ml was 71% (70%) [n=100 including 40 patients having received the recommended dose of Kaletra for the entire 204 weeks], and the corresponding mean increase in CD4 cell count was 440 cells/mm3. Twenty-eight patients (28%) discontinued the study, including nine (9%) discontinuations due to adverse events and one (1%) death.Patients with prior antiretroviral therapyStudy M97-765 is a randomised, double-blind trial evaluating Kaletra at two dose levels (400/100 mg and 400/200 mg, both twice daily) plus nevirapine (200 mg twice daily) and two nucleoside reverse transcriptase inhibitors in 70 single protease inhibitor experienced, non-nucleoside reverse transcriptase inhibitor naïve patients. Median baseline CD4 cell count was 349 cells/mm3 (range 72 to 807 cells/mm3) and median baseline plasma HIV-1 RNA was 4.0 log10 copies/ml (range 2.9 to 5.8 log10 copies/ml). By intent to treat analysis where patients with missing values are considered virologic failures, the proportion of patients with HIV RNA < 400 (< 50) copies/ml at 24 weeks was 75% (58%) and the mean increase from baseline in CD4 cell count was 174 cells/mm3 for the 36 patients receiving the 400/100 mg dose of Kaletra. M98-957 is a randomised, open-label study evaluating Kaletra treatment at two dose levels (400/100 mg and 533/133 mg, both twice daily) plus efavirenz (600 mg once daily) and nucleoside reverse transcriptase inhibitors in 57 multiple protease inhibitor experienced, non-nucleoside reverse transcriptase inhibitor naïve patients. Between week 24 and 48, patients randomised to a dose of 400/100 mg were converted to a dose of 533/133 mg. Median baseline CD4 cell count was 220 cells/mm3 (range 13 to 1030 cells/mm3). By intent-to-treat analysis of both dose groups combined (n=57), where patients with missing values are considered virologic failures, the proportion of patients with HIV RNA < 400 copies/ml at 48 weeks was 65% and the mean increase from baseline CD4 cell count was 94 cells/mm3.Paediatric UseM98-940 is an open-label study of a liquid formulation of Kaletra in 100 antiretroviral naïve (44%) and experienced (56%) paediatric patients. All patients were non-nucleoside reverse transcriptase inhibitor naïve. Patients were randomised to either 230 mg lopinavir/57.5 mg ritonavir per m2 or 300 mg lopinavir/75 mg ritonavir per m2. Naïve patients also received nucleoside reverse transcriptase inhibitors. Experienced patients received nevirapine plus up to two nucleoside reverse transcriptase inhibitors. Safety, efficacy and pharmacokinetic profiles of the two dose regimens were assessed after 3 weeks of therapy in each patient. Subsequently, all patients were continued on the 300/75 mg per m2 dose. Patients had a mean age of 5 years (range 6 months to 12 years) with 14 patients less than 2 years old and 6 patients one year or less. Mean baseline CD4 cell count was 838 cells/mm3 and mean baseline plasma HIV-1 RNA was 4.7 log10 copies/ml. Through 48 weeks of therapy, the proportion of patients with HIV RNA < 400 copies/ml was 84% for antiretroviral naïve patients and 75% for antiretroviral experienced patients and the mean increases from baseline in CD4 cell count were 404 cells/mm3 and 284 cells/mm3 respectively.

43
PharmacokineticThe pharmacokinetic properties of lopinavir co-administered with ritonavir have been evaluated in healthy adult volunteers and in HIV-infected patients; no substantial differences were observed between the two groups. Lopinavir is essentially completely metabolised by CYP3A. Ritonavir inhibits the metabolism of lopinavir, thereby increasing the plasma levels of lopinavir. Across studies, administration of Kaletra 400/100 mg twice daily yields mean steady-state lopinavir plasma concentrations 15 to 20-fold higher than those of ritonavir in HIV-infected patients. The plasma levels of ritonavir are less than 7% of those obtained after the ritonavir dose of 600 mg twice daily. The in vitro antiviral EC50 of lopinavir is approximately 10-fold lower than that of ritonavir. Therefore, the antiviral activity of Kaletra is due to lopinavir.Absorption: multiple dosing with 400/100 mg Kaletra twice daily for 3 to 4 weeks and without meal restriction produced a mean ± SD lopinavir peak plasma concentration (Cmax) of 9.6 ± 4.4 µg/ml, occurring approximately 4 hours after administration. The mean steady-state trough concentration prior to the morning dose was 5.5 ± 4.0 µg/ml. Lopinavir AUC over a 12 hour dosing interval averaged 82.8 ± 44.5 µg•h/ml. The absolute bioavailability of lopinavir co-formulated with ritonavir in humans has not been established.Effects of food on oral absorption: Administration of a single 400/100 mg dose of Kaletra tablets under fed conditions (high fat, 872 kcal, 56% from fat) compared to fasted state was associated with no significant changes in Cmax and AUCinf. Therefore, Kaletra tablets may be taken with or without food. Kaletra tablets have also shown less pharmacokinetic variability under all meal conditions compared to Kaletra soft capsules.Distribution: at steady state, lopinavir is approximately 98 − 99% bound to serum proteins. Lopinavir binds to both alpha-1-acid glycoprotein (AAG) and albumin, however, it has a higher affinity for AAG. At steady state, lopinavir protein binding remains constant over the range of observed concentrations after 400/100 mg Kaletra twice daily, and is similar between healthy volunteers and HIV-positive patients.Metabolism: in vitro experiments with human hepatic microsomes indicate that lopinavir primarily undergoes oxidative metabolism. Lopinavir is extensively metabolised by the hepatic cytochrome P450 system, almost exclusively by isozyme CYP3A. Ritonavir is a potent CYP3A inhibitor which inhibits the metabolism of lopinavir and therefore, increases plasma levels of lopinavir. A 14C-lopinavir study in humans showed that 89% of the plasma radioactivity after a single 400/100 mg Kaletra dose was due to parent drug. At least 13 lopinavir oxidative metabolites have been identified in man. The 4-oxo and 4-hydroxymetabolite epimeric pair are the major metabolites with antiviral activity, but comprise only minute amounts of total plasma radioactivity. Ritonavir has been shown to induce metabolic enzymes, resulting in the induction of its own metabolism, and likely the induction of lopinavir metabolism. Pre-dose lopinavir concentrations decline with time during multiple dosing, stabilising after approximately 10 days to 2 weeks.Elimination: after a 400/100 mg 14C-lopinavir/ritonavir dose, approximately 10.4 ± 2.3% and 82.6 ± 2.5% of an administered dose of 14C-lopinavir can be accounted for in urine and faeces, respectively. Unchanged lopinavir accounted for approximately 2.2% and 19.8% of the administered dose in urine and faeces, respectively. After multiple dosing, less than 3% of the lopinavir dose is excreted unchanged in the urine. The effective (peak to trough) half-life of lopinavir over a 12 hour dosing interval averaged 5 − 6 hours, and the apparent oral clearance (CL/F) of lopinavir is 6 to 7 l/h.Special PopulationsPaediatrics:There are limited pharmacokinetic data in children below 2 years of age. The pharmacokinetics of Kaletra oral solution 300/75 mg/m2 twice daily and 230/57.5 mg/m2 twice daily have been studied in a total of 53 paediatric patients, ranging in age from 6 months to 12 years. The lopinavir mean steady-state AUC, Cmax, and Cmin were 72.6 ± 31.1 µg•h/ml, 8.2 ± 2.9 µg/ml and 3.4 ± 2.1 µg/ml, respectively after Kaletra oral solution 230/57.5 mg/m2 twice daily without nevirapine (n=12), and were 85.8 ± 36.9 µg•h/ml, 10.0 ± 3.3 µg/ml and 3.6 ± 3.5 µg/ml, respectively after 300/75 mg/m2 twice daily with nevirapine (n=12). The 230/57.5 mg/m2 twice daily regimen without nevirapine and the 300/75 mg/m2 twice daily regimen with nevirapine provided lopinavir plasma concentrations similar to those obtained in adult patients receiving the 400/100 mg twice daily regimen without nevirapine.Gender, Race and Age:Kaletra pharmacokinetics have not been studied in the elderly. No age or gender related pharmacokinetic differences have been observed in adult patients. Pharmacokinetic differences due to race have not been identified.Renal Insufficiency:Kaletra pharmacokinetics have not been studied in patients with renal insufficiency; however, since the renal clearance of lopinavir is negligible, a decrease in total body clearance is not expected in patients with renal insufficiency.Hepatic Insufficiency:The steady state pharmacokinetic parameters of lopinavir in HIV-infected patients with mild to moderate hepatic impairment were compared with those of HIV-infected patients with normal hepatic function in a multiple dose study with lopinavir/ritonavir 400/100 mg twice daily. A limited increase in total lopinavir concentrations of approximately 30% has been observed which is not expected to be of clinical relevance.IndicationsKaletra is indicated for the treatment of HIV-1 infected adults and children above the age of 2 years, in combination with other antiretroviral agents. Most experience with Kaletra is derived from the use of the product in antiretroviral therapy naïve patients. Data in heavily pretreated protease inhibitor experienced patients are limited. There are limited data on salvage therapy on patients who have failed therapy with Kaletra. The choice of Kaletra to treat protease inhibitor experienced HIV-1 infected patients should be based on individual viral resistance testing and treatment history of patients.ContraindicationsHypersensitivity to the active substances or to any of the excipients.Patients with severe hepatic insufficiency.Kaletra contains lopinavir and ritonavir, both of which are inhibitors of the P450 isoform CYP3A. Kaletra should not be co-administered with medicinal products that are highly dependent on CYP3A for clearance and for which elevated plasma concentrations are associated with serious and/or life threatening events. These medicinal products include astemizole, terfenadine, midazolam, triazolam, cisapride, pimozide, amiodarone, ergot alkaloids (e.g. ergotamine, dihydroergotamine, ergonovine and methylergonovine).Herbal preparations containing St John’s wort (Hypericum perforatum) must not be used while taking lopinavir and ritonavir due to the risk of decreased plasma concentrations and reduced clinical effects of lopinavir and ritonavir.Rifampicin should not be used in combination with Kaletra because co-administration may cause large decreases in lopinavir concentrations which may in turn significantly decrease the lopinavir therapeutic effect.Side EffectsThe safety of Kaletra has been investigated in 612 patients in Phase II/III clinical trials, of which 442 have received a dose of 400/100 mg twice daily. In some studies, Kaletra was used in combination with efavirenz or nevirapine. The most common adverse reaction associated with Kaletra therapy was diarrhoea and was generally of mild to moderate severity. Discontinuation due to adverse reactions was 4.5% (naïve patients) and 9% (experienced patients) over a 48 week period. It is important to note that cases of pancreatitis have been reported in patients receiving Kaletra, including those who developed hypertriglyceridaemia. Furthermore, rare increases in PR interval have been reported during Kaletra therapy. Increased CPK, myalgia, myositis, and rarely, rhabdomyolysis have been reported with protease inhibitors, particularly in combination with nucleoside reverse transcriptase inhibitors. Combination antiretroviral therapy has been associated with redistribution of body fat (lipodystrophy) in HIV patients including the loss of peripheral and facial subcutaneous fat, increased intra-abdominal and visceral fat, breast hypertrophy and dorsocervical fat accumulation (buffalo hump). Combination antiretroviral therapy has been associated with metabolic abnormalities such as hypertriglyceridaemia, hypercholesterolaemia, insulin resistance, hyperglycaemia

44
and hyperlactataemia. In HIV-infected patients with severe immune deficiency at the time of initiation of combination antiretroviral therapy (CART), an inflammatory reaction to asymptomatic or residual opportunistic infections may arise.Adult patientsThe following adverse reactions of moderate to severe intensity with possible or probable relationship to Kaletra have been reported. The adverse reactions are displayed by system organ class. Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness: very common > 1/10, common > 1/100, < 1/10, uncommon > 1/1000, < 1/100.KALETRA TABS Table 1. Undesirable Effects in Clinical Studies in Adult PatientsInfections and infestations Uncommon Otitis media, bronchitis, sinusitis, furunculosis, bacterial infection, viral infectionNeoplasms benign, malignant and unspecified (including cysts and polyps)
Uncommon Skin benign neoplasm, cyst
Blood and lymphatic system disorders Uncommon Anaemia, leucopenia and lymphadenopathy
Endocrine disorders Uncommon Hypogonadism male, Cushing syndrome, hypothyroidismMetabolic and nutritional disorders Uncommon Avitaminosis, dehydration, oedema, increased appetite, lactic acidosis, obesity, anorexia,
diabetes mellitus, hyperglycaemia, hypocholesteremia
Psychiatric disordersCommon Insomnia
Uncommon Abnormal dreams, agitation, anxiety, confusion, depression, dyskinesia, emotional lability, decreased libido, nervousness, abnormal thinking
Nervous system disorders
Common Headache
UncommonDizziness, amnesia, ataxia, encephalopathy, facial paralysis, hypertonia, neuropathy, paresthesia, peripheral neuritis, somnolence, tremor, taste loss, taste perversion, migraine, extrapyramidal syndrome
Eye disorders Uncommon Abnormal vision, eye disorderEar and labyrinth disorders Uncommon TinnitusCardiac disorders Uncommon Palpitation, lung oedema, myocardial infarct1
Vascular disorders Uncommon Hypertension, thrombophlebitis, vasculitis, varicose vein, deep thrombophlebitis, vascular disorder
Respiratory, thoracic and mediastinal disorders Uncommon Dyspnea, rhinitis, cough increased
Gastrointestinal disorders
Very common Diarrhoea
Common Nausea, vomiting, abdominal pain, abnormal stools, dyspepsia, flatulence, gastrointestinal disorder
UncommonAbdomen enlarged, constipation, dry mouth, dysphagia, enterocolitis, eructation, oesophagitis, faecal incontinence, gastritis, gastroenteritis, haemorrhagic colitis, mouth ulcerations, pancreatitis2, sialadenitis, stomatitis, ulcerative stomatitis, periodontitis
Hepatobiliary disorders Uncommon Cholecystitis, hepatitis, hepatomegaly, liver fatty deposit, liver tenderness
Skin and subcutaneous tissue disorders
Common Rash, lipodystrophy
Uncommon Alopecia, dry skin, eczema, exfoliative dermatitis, maculopapular rash, nail disorder, pruritis, seborrhea, skin discoloration, skin ulcer, face oedema, acne, sweating, skin striae
Musculoskeletal and connective tissue disorders Uncommon Arthralgia, arthrosis, myalgia, back pain, joint disorder
Renal and urinary disorders Uncommon Kidney calculus, urine abnormality, albuminuria, hypercalcinuria, nephritis, hyperuricemiaReproductive system and breast disorders Uncommon Abnormal ejaculation, amenorrhea, breast enlargement, gynecomastia, impotence,
menorrhagia
General disorders and administration site conditions
Common Asthenia
Uncommon Chest pain, chest pain substernal, chills, fever, flu syndrome, malaise, pain, peripheral oedema, drug interaction
Investigations
Very common(Grade 3 or 4)
Increased triglycerides, increased total cholesterol, increased GGT
Common(Grade 3 or 4
Increased glucose, increased amylase, increased SGOT/AST, increased SGPT/ALT, liver function tests abnormal
Uncommon Decreased glucose tolerance, weight gain, weight loss, increased bilirubin, hormone level altered, lab test abnormal
1 This event had a fatal outcome.2 See special warnings and precautions: pancreatitis and lipidsPaediatric patientsIn children 2 years of age and older, the nature of the safety profile is similar to that seen in adults.KALETRA TABS Table 2. Undesirable Effects in Clinical Studies in Paediatric PatientsInfections and infestations Common Viral infection
Nervous system disorders Common Taste perversion
Gastrointestinal disorders Common Constipation, vomiting, pancreatitis*
Hepatobiliary disorders Common HepatomegalySkin and subcutaneous tissue disorders Common Rash, dry skin
General disorders and Common Fever

45
administration site conditions
InvestigationsCommon(Grade 3 or 4)
Increased activated partial thromboplastin time, decreased haemoglobin, decreased platelets, increased sodium, increased potassium, increased calcium, increased bilirubin, increased SGPT/ALT, increased SGOT/AST, increased total cholesterol, increased amylase, increased uric acid, decreased sodium, decreased potassium, decreased calcium, decreased neutrophils
*see warnings and precautions: pancreatitis and lipidsPost marketing experienceHepatitis, and rarely jaundice, have been reported in patients on Kaletra therapy in the presence or absence of identifiable risk factors for hepatitis.PrecautionsPatients with coexisting conditionsLiver disease: the safety and efficacy of Kaletra has not been established in patients with significant underlying liver disorders. Kaletra is contraindicated in patients with severe liver impairment. Patients with chronic hepatitis B or C and treated with combination antiretroviral therapy are at an increased risk for severe and potentially fatal hepatic adverse events. In case of concomitant antiviral therapy for hepatitis B or C, please refer to the relevant product information for these medicinal products. Patients with pre-existing liver dysfunction including chronic hepatitis have an increased frequency of liver function abnormalities during combination antiretroviral therapy and should be monitored according to standard practice. If there is evidence of worsening liver disease in such patients, interruption or discontinuation of treatment should be considered.Renal disease: since the renal clearance of lopinavir and ritonavir is negligible, increased plasma concentrations are not expected in patients with renal impairment. Because lopinavir and ritonavir are highly protein bound, it is unlikely that they will be significantly removed by haemodialysis or peritoneal dialysis.Haemophilia: there have been reports of increased bleeding, including spontaneous skin haematomas and haemarthrosis in patients with haemophilia type A and B treated with protease inhibitors. In some patients additional factor VIII was given. In more than half of the reported cases, treatment with protease inhibitors was continued or reintroduced if treatment had been discontinued. A causal relationship had been evoked, although the mechanism of action had not been elucidated. Haemophiliac patients should therefore be made aware of the possibility of increased bleeding.Lipid elevationsTreatment with Kaletra has resulted in increases, sometimes marked, in the concentration of total cholesterol and triglycerides. Triglyceride and cholesterol testing is to be performed prior to initiating Kaletra therapy and at periodic intervals during therapy. Particular caution should be paid to patients with high values at baseline and with history of lipid disorders. Lipid disorders are to be managed as clinically appropriate.PancreatitisCases of pancreatitis have been reported in patients receiving Kaletra, including those who developed hypertriglyceridaemia. In most of these cases patients have had a prior history of pancreatitis and/or concurrent therapy with other medicinal products associated with pancreatitis. Marked triglyceride elevation is a risk factor for development of pancreatitis. Patients with advanced HIV disease may be at risk of elevated triglycerides and pancreatitis. Pancreatitis should be considered if clinical symptoms (nausea, vomiting, abdominal pain) or abnormalities in laboratory values (such as increased serum lipase or amylase values) suggestive of pancreatitis should occur. Patients who exhibit these signs or symptoms should be evaluated and Kaletra therapy should be suspended if a diagnosis of pancreatitis is made.HyperglycaemiaNew onset diabetes mellitus, hyperglycaemia or exacerbation of existing diabetes mellitus has been reported in patients receiving protease inhibitors. In some of these the hyperglycaemia was severe and in some cases also associated with ketoacidosis. Many patients had confounding medical conditions some of which required therapy with agents that have been associated with the development of diabetes mellitus or hyperglycaemia.Fat redistribution and metabolic disordersCombination antiretroviral therapy has been associated with redistribution of body fat (lipodystrophy) in HIV patients. The long-term consequences of these events are currently unknown. Knowledge about the mechanism is incomplete. A connection between visceral lipomatosis and protease inhibitors (PIs) and lipoatrophy and nucleoside reverse transcriptase inhibitors (NRTIs) has been hypothesised. A higher risk of lipodystrophy has been associated with individual factors such as older age, and with drug related factors such as longer duration of antiretroviral treatment and associated metabolic disturbances. Clinical examination should include evaluation for physical signs of fat redistribution. Consideration should be given to measurement of fasting serum lipids and blood glucose. Lipid disorders should be managed as clinically appropriate.Immune Reactivation SyndromeIn HIV-infected patients with severe immune deficiency at the time of institution of combination antiretroviral therapy (CART), an inflammatory reaction to asymtomatic or residual opportunistic pathogens may arise and cause serious clinical conditions, or aggravation of symptoms. Typically, such reactions have been observed within the first few weeks or months of initiation of CART. Relevant examples are cytomegalovirus retinitis, generalised and/or focal mycobacterial infections, and Pneumocystis carinii pneumonia. Any inflammatory symptoms should be evaluated and treatment instituted when necessary.Interactions with medicinal productsKaletra contains lopinavir and ritonavir, both of which are inhibitors of the P450 isoform CYP3A. Kaletra is likely to increase plasma concentrations of medicinal products that are primarily metabolised by CYP3A. These increases of plasma concentrations of co-administered medicinal products could increase or prolong their therapeutic effect and adverse events.Particular caution must be used when prescribing sildenafil in patients receiving Kaletra. Co-administration of Kaletra with sildenafil is expected to substantially increase sildenafil concentrations and may result in an increase in sildenafil-associated adverse events including hypotension, syncope, visual changes and prolonged erection.The HMG-CoA reductase inhibitors simvastatin and lovastatin are highly dependent on CYP3A for metabolism, thus concomitant use of Kaletra with simvastatin or lovastatin is not recommended due to an increased risk of myopathy including rhabdomyolysis. Caution must also be exercised and reduced doses should be considered if Kaletra is used concurrently with atorvastatin, which is metabolised to a lesser extent by CYP3A4. If treatment with a HMG-CoA reductase inhibitor is indicated, pravastatin or fluvastatin is recommended.Particular caution must be used when prescribing Kaletra and medicinal products known to induce QT interval prolongation such as: chlorpheniramine, quinidine, erythromycin, clarithromycin. Indeed, Kaletra could increase concentrations of the co-administered medicinal products and this may result in an increase of their associated cardiac adverse events. Cardiac events have been reported with Kaletra in preclinical studies; therefore, the potential cardiac effects of Kaletra cannot be currently ruled out.Rifampicin should not be used in combination with Kaletra because this may cause large decreases in lopinavir concentrations which may in turn significantly decrease the lopinavir therapeutic effect.Co-administration of efavirenz, nevirapine, nelfinavir or amprenavir with Kaletra tablets 400/100 mg is not recommended. If co-administration of these medicinal products with Kaletra tablets is clinically indicated, a dose increase of Kaletra tablets to 600/150 mg twice daily may be considered. However, as the safety of high doses of Kaletra has not been established, safety should be closely monitored when Kaletra tablets 600/150 mg twice daily is administered.

46
Oral Contraceptives: since levels of ethinyl oestradiol may be decreased when oestrogen-based oral contraceptives are co-administered with Kaletra alternative or additional contraceptive measures are to be used.OtherKaletra is not a cure for HIV infection or AIDS. It does not reduce the risk of passing HIV to others through sexual contact or blood contamination. Appropriate precautions should be taken. People taking Kaletra may still develop infections or other illnesses associated with HIV disease and AIDS.Concomitant use of Kaletra and fluticasone or other glucocorticoids that are metabolised by CYP3A4 is not recommended unless the potential benefit of treatment outweighs the risk of systemic corticosteroid effects, including Cushing’s syndrome and adrenal suppression.Pregnancy and LactationThere are no data from the use of Kaletra in pregnant women. Studies in animals have shown reproductive toxicity. The potential risk for humans is unknown. Kaletra should not be used during pregnancy unless clearly necessary. Studies in rats revealed that lopinavir is excreted in the milk. It is not known whether this medicinal product is excreted in human milk. HIV infected women must not breast-feed their infants under any circumstances to avoid transmission of HIV.Effects on ability to drive and use machinesNo studies on the effects on the ability to drive and use machines have been performed.OverdosageTo date, there is limited human experience of acute overdose with Kaletra. The adverse clinical signs observed in dogs included salivation, emesis and diarrhoea/abnormal stool. The signs of toxicity observed in mice, rats or dogs included decreased activity, ataxia, emaciation, dehydration and tremors. There is no specific antidote for overdose with Kaletra. Treatment of overdose with Kaletra is to consist of general supportive measures including monitoring of vital signs and observation of the clinical status of the patient. If indicated, elimination of unabsorbed active substance is to be achieved by emesis or gastric lavage. Administration of activated charcoal may also be used to aid in removal of unabsorbed active substance. Since Kaletra is highly protein bound, dialysis is unlikely to be beneficial in significant removal of the active substance.Drug InteractionsKaletra contains lopinavir and ritonavir, both of which are inhibitors of the P450 isoform CYP3A in vitro. Co-administration of Kaletra and medicinal products primarily metabolised by CYP3A may result in increased plasma concentrations of the other medicinal product, which could increase or prolong its therapeutic and adverse effects. Kaletra does not inhibit CYP2D6, CYP2C9, CYP2C19, CYP2E1, CYP2B6 or CYP1A2 at clinically relevant concentrations.Kaletra has been shown in vivo to induce its own metabolism and to increase the biotransformation of some medicinal products metabolised by cytochrome P450 enzymes and by glucuronidation. This may result in lowered plasma concentrations and potential decrease of efficacy of co-administered medicinal products.Medicinal products that are contraindicated specifically due to the expected magnitude of interaction and potential for serious adverse events are listed in “Contra indications”.All interaction studies, when otherwise not stated, were performed using Kaletra capsules, which gives an approximately 20% lower exposure of lopinavir than the tablets.Antiretroviral agentsNucleoside reverse transcriptase inhibitors (NRTIs):Stavudine and Lamivudine: no change in the pharmacokinetics of lopinavir was observed when Kaletra was given alone or in combination with stavudine and lamivudine in clinical studies.Didanosine: it is recommended that didanosine be administered on an empty stomach; therefore, didanosine may be co-administered with Kaletra tablets without food.Zidovudine and Abacavir: Kaletra induces glucuronidation, therefore Kaletra has the potential to reduce zidovudine and abacavir plasma concentrations. The clinical significance of this potential interaction is unknown.Non-nucleoside reverse transcriptase inhibitors (NNRTIs):In a study performed in healthy volunteers to explore the interaction between Kaletra tablets (400/100 mg twice daily) and efavirenz (600 mg once daily), efavirenz has been shown to decrease the lopinavir concentrations by 30 - 40%. Therefore, the co-administration of Kaletra tablets 400/100 mg with efavirenz is not recommended, since it could expose patients to sub-optimal lopinavir concentrations. When Kaletra tablet dosages were increased to 600/150 mg twice daily during co-administration of efavirenz 600 mg once daily, lopinavir levels increased by 28 – 44% and ritonavir plasma levels by 62 – 95% compared to Kaletra tablets 400/100 mg twice daily alone. Because the safety of these high exposures of lopinavir has not been established, safety aspects of co-administration of Kaletra tablets 600/150 mg with efavirenz should be closely monitored. Similar pharmacokinetic interactions are expected for the co-administration of Kaletra tablets with the NNRTI nevirapine and with the protease inhibitors nelfinavir and amprenavir. The same recommendations for monitoring apply in these cases of co-administration.Co-administration with other HIV protease inhibitors (PIs):Kaletra (400/100 mg twice daily) has been studied in combination with reduced doses of amprenavir, indinavir, nelfinavir and saquinavir in steady-state controlled healthy volunteer studies relative to clinical doses of each HIV protease inhibitor in the absence of ritonavir. Comparisons to published pharmacokinetic data with ritonavir-enhanced amprenavir and saquinavir regimens are also described. Additionally, the effect of additional ritonavir on the pharmacokinetics of lopinavir are discussed. Note that the historical comparisons to ritonavir-enhanced protease inhibitor regimens should be interpreted with caution (see details of combinations below). Appropriate doses of HIV-protease inhibitors in combination with Kaletra with respect to safety and efficacy have not been established. Therefore, the concomitant administration of Kaletra with PIs requires close monitoring.Amprenavir: see recommendations described for Kaletra tablets co-administration with efavirenz.Indinavir: indinavir 600 mg twice daily in combination with Kaletra produces similar indinavir AUC, higher Cmin (by 3.5-fold) and lower Cmax relative to indinavir 800 mg three times daily alone. Furthermore, concentrations of lopinavir do not appear to be affected when both drugs, Kaletra and indinivir, are combined, based on historical comparison with Kaletra alone.Nelfinavir: see recommendations described for Kaletra tablets co-administration with efavirenz.Saquinavir: saquinavir 800 mg twice daily co-administered with Kaletra produces an increase of saquinavir AUC by 9.6-fold relative to saquinavir 1200 mg three times daily given alone. Saquinavir 800 mg twice daily co-administered with Kaletra resulted in an increase of saquinavir AUC by approximately 30% relative to saquinavir/ritonavir 1000/100 mg twice daily, and produces similar exposure to those reported after saquinavir/ritonavir 400/400 mg twice daily. When saquinavir 1200 mg twice daily was combined with Kaletra, no further increase of concentrations was noted. Furthermore, concentrations of lopinavir do not appear to be affected when both drugs, Kaletra and saquinavir, are combined, based on historical comparison with Kaletra alone.Ritonavir: Kaletra co-administered with an additional 100 mg ritonavir twice daily resulted in an increase of lopinavir AUC and Cmin of 33% and 64%, respectively, as compared to Kaletra alone.Other medicinal products:Antiarrhythmics: (bepridil, systemic lidocaine and quinidine): concentrations may be increased when co-administered with Kaletra. Caution is warranted and therapeutic concentration monitoring is recommended when available.Anticoagulants: warfarin concentrations may be affected when co-administered with Kaletra. It is recommended that INR (international normalised ratio) be monitored.Anticonvulsants: (phenobarbital, phenytoin, carbamazepine): will induce CYP3A4 and may decrease lopinavir concentrations.

47
Dihydropyridine calcium channel blockers: (e.g. felodipine, nifedipine, nicardipine): may have their serum concentrations increased by Kaletra.HMG-CoA reductase inhibitors: HMG-CoA reductase inhibitors which are highly dependent on CYP3A4 metabolism, such as lovastatin and simvastatin, are expected to have markedly increased plasma concentrations when co-administered with Kaletra. Since increased concentrations of HMG-CoA reductase inhibitors may cause myopathy, including rhabdomyolysis, the combination of these medicinal products with Kaletra is not recommended. Atorvastatin is less dependent on CYP3A for metabolism. When atorvastatin was given concurrently with Kaletra, a mean 4.7-fold and 5.9-fold increase in atorvastatin Cmax and AUC, respectively, was observed. When used with Kaletra, the lowest possible dose of atorvastatin should be administered. Results from an interaction study with Kaletra and pravastatin reveal no clinically significant interaction. The metabolism of pravastatin and fluvastatin is not dependent on CYP3A4, and interactions are not expected with Kaletra. If treatment with a HMG-CoA reductase inhibitor is indicated, pravastatin or fluvastatin is recommended.Dexamethasone: may induce CYP3A4 and may decrease lopinavir concentrations.Sildenafil: co-administration of sildenafil 100 mg single dose with ritonavir 500 mg twice daily at steady-state resulted in a 1000% increase in sildenafil plasma AUC. On the basis of these data, concomitant use of sildenafil with Kaletra is not recommended and in no case should the starting dose of sildenafil exceed 25 mg within 48 hours.Cyclosporin, sirolimus (rapamycin) and tacrolimus: concentrations may be increased when co-administered with Kaletra. More frequent therapeutic concentration monitoring is recommended until plasma levels of these products have been stabilised.Ketoconazole and itraconazole: may have serum concentrations increased by Kaletra. High doses of ketoconazole and itraconazole (> 200 mg/day) are not recommended.Clarithromycin: moderate increases in clarithromycin AUC are expected when co-administered with Kaletra. For patients with renal or hepatic impairment dose reduction of clarithromycin should be considered.Methadone: Kaletra was demonstrated to lower plasma concentrations of methadone. Monitoring plasma concentrations of methadone is recommended.Oral Contraceptives: since levels of ethinyl oestradiol may be decreased when oestrogen-based oral contraceptives are co-administered with Kaletra alternative or additional contraceptive measures are to be used.Rifabutin: when rifabutin and Kaletra were co-administered for 10 days, rifabutin (parent drug and active 25-O-desacetyl metabolite) Cmax and AUC were increased by 3.5- and 5.7-fold, respectively. On the basis of these data, a rifabutin dose reduction of 75% (i.e. 150 mg every other day or 3 times per week) is recommended when administered with Kaletra. Further reduction may be necessary.Rifampicin: due to large decreases in lopinavir concentrations, rifampicin should not be used in combination with Kaletra.St John’s wort: serum levels of lopinavir and ritonavir can be reduced by concomitant use of the herbal preparation St John’s wort (Hypericum perforatum). This is due to the induction of drug metabolising enzymes by St John’s wort. Herbal preparations containing St John’s wort should therefore not be combined with lopinavir and ritonavir. If a patient is already taking St John’s wort, stop St John’s wort and if possible check viral levels. Lopinavir and ritonavir levels may increase on stopping St John’s wort. The dose of Kaletra may need adjusting. The inducing effect may persist for at least 2 weeks after cessation of treatment with St John’s wort.Fluticasone propionate (interaction with ritonavir): in a clinical study where ritonavir 100 mg capsules twice daily were co − administered with 50 µg intranasal fluticasone propionate (4 times daily) for seven days in healthy subjects, the fluticasone propionate plasma levels increased significantly, whereas the intrinsic cortisol levels decreased by approximately 86% (90% confidence interval 82 − 89%). Greater effects may be expected when fluticasone propionate is inhaled. Systemic corticosteroid effects including Cushing's syndrome and adrenal suppression have been reported in patients receiving ritonavir and inhaled or intranasal administered fluticasone propionate; this could also occur with other corticosteroids metabolised via the P450 3A pathway eg budesonide. Consequently, concomitant administration of Kaletra and these glucocorticoids is not recommended unless the potential benefit of treatment outweighs the risk of systemic corticosteroid effects. A dose reduction of the glucocorticoid should be considered with close monitoring of local and systemic effects or a switch to a glucocorticoid, which is not a substrate for CYP3A4 (eg beclomethasone). Moreover, in case of withdrawal of glucocorticoids progressive dose reduction may have to be performed over a longer period. The effects of high fluticasone systemic exposure on ritonavir plasma levels is yet unknown.Based on known metabolic profiles, clinically significant interactions are not expected between Kaletra and fluvastatin, dapsone, trimethoprim/sulfamethoxazole, azithromycin or fluconazole.IncompatibilitiesNot applicable.Dosage AdministrationKaletra should be prescribed by physicians who are experienced in the treatment of HIV infection.Adult and adolescent use: the recommended dosage of Kaletra tablets is two 200/50 mg tablets twice daily taken with or without food. Kaletra tablets should be swallowed whole and not chewed, broken or crushed. Oral solution is available to patients who have difficulty swallowing.Paediatric use (2 years of age and above): the adult dose of Kaletra tablets (400/100 mg twice daily) may be used in children 40 kg or greater or with a Body Surface Area (BSA)* greater than 1.3 m2. For children weighing less than 40 kg or with a BSA of less than 1.3 m2, please refer to the Kaletra oral solution insert.* Body surface area can be calculated with the following equation:BSA (m2) = √ (Height (cm) X Weight (kg) / 3600)Children less than 2 years of age: Kaletra is not recommended for use in children below 2 years of age due to insufficient data on safety and efficacy.Hepatic impairment: In HIV-infected patients with mild to moderate hepatic impairment, an increase of approximately 30% in lopinavir exposure has been observed but is not expected to be of clinical relevance. No data are available in patients with severe hepatic impairment. Kaletra should not be given to these patients.Renal impairment: no dose adjustment is necessary in patients with renal impairment. Caution is warranted when Kaletra is used in patients with severe renal impairment.StorageThis medicinal product does not require any special storage conditions.2 years.PackagingHigh density polyethylene (HDPE) bottles closed with propylene caps. Each bottle contains 120 tablets.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
KLACID 500MG TABLETS ®CompositionKLACID 500mg tablets: yellow, ovaloid, film-coated tablet containing 500mg clarithromycinPropertiesPharmacodynamic Clarithromycin is a semi-synthetic derivative of erythromycin A. It exerts its antibacterial action by binding to the 50s ribosomal sub-unit of susceptible bacteria and suppresses protein synthesis. It is highly potent against a wide variety of aerobic and anaerobic gram-positive and

48
gram-negative organisms. The minimum inhibitory concentrations (MICs) of clarithromycin are generally two-fold lower than the MICs of erythromycin. The 14-hydroxy metabolite of clarithromycin also has antimicrobial activity. The MICs of this metabolite are equal or two-fold higher than the MICs of the parent compound, except for H. influenzae where the 14-hydroxy metabolite is two-fold more active than the parent compound.Clarithromycin is usually active against the following organisms in vitro:-Gram-positive Bacteria: Staphylococcus aureus (methicillin susceptible); Streptococcus pyogenes (Group A beta-hemolytic streptococci) alpha-hemolytic streptococci (viridans group); Streptococcus (Diplococcus) pneumoniae; Streptococcus agalactiae; Listeria monocytogenes.Gram-negative Bacteria: Haemophilus influenzae, Haemophilus parainfluenzae, Moraxella (Branhamella) catarrhalis, Neisseria gonorrhoeae; Legionella pneumophila, Bordetella pertussis, Helicobacter pylori; Campylobacter jejuni.Mycoplasma: Mycoplasma pneumoniae; Ureaplasma urealyticum.Other Organisms: Chlamydia trachomatis; Mycobacterium avium; Mycobacterium leprae; Mycobacterum kansasii; Mycobacterium chelonae; Mycobacterium fortuitum; Mycobacterium intracellulare.Anaerobes: Macrolide-susceptible Bacteroides fragilis; Clostridium perfringens; Peptococcus species; Peptostreptococcus species; Propionibacterium acnes. Clarithromycin has bactericidal activity against several bacterial strains. The organisms include Haemophilus influenzae, Streptococcus pneumoniae, Streptococcus pyogenes, Streptococcus agalactiae, Moraxella (Branhamella) catarrhalis, Neisseria gonorrhoeae, H. pylori and Campylobacter spp. The activity of clarithromycin against H. pylori is greater at neutral pH than at acid pH.Pharmacological Further information: H. pylori is associated with acid peptic disease including duodenal ulcer and gastric ulcer in which about 95% and 80% of patients respectively are infected with the agent. H. pylori is also implicated as a major contribution factor in the development of gastritis and ulcer recurrence in such patients. In a well controlled study, clarithromycin 500mg tid for 14 days administered with omeprazole 40gm od for 28 days eradicated in excess of 80% of H. pylori isolates in patients with duodenal ulcer. Clarithromycin has been used in small numbers of patients in other treatment regimens. Possible kinetic interactions have not been fully investigated. These regimens include: Clarithromycin plus tinidazole and omeprazole; clarithromycin plus tetracycline, bismuth subsalicylate and ranitidine; clarithromycin plus ranitidine alone. Clinical studies using various different H. pylori eradication regimens have shown that eradication of H. pylori prevents ulcer recurrence.Pharmacokinetic Clarithromycin is rapidly and well absorbed from the gastro-intestinal tract after oral administration of Clarithromycin tablets. The microbiologically active metabolite 14-hydroxyclarithromycin is formed by first pass metabolism. Clarithromycin may be given without regard to meals as food does not affect the extent of bioavailability of Clarithromycin tablets. Food does slightly delay the onset of absorption of clarithromycin and formation of the 14-hydroxymetabolite. The pharmacokinetics of clarithromycin are non linear; however, steady-state is attained within 2 days of dosing. At 250 mg b.i.d. 15-20% of unchanged drug is excreted in the urine. With 500 mg b.i.d. daily dosing urinary excretion is greater (approximately 36%).The 14-hydroxyclarithromycin is the major urinary metabolite and accounts for 10-15% of the dose. Most of the remainder of the dose is eliminated in the faeces, primarily via the bile. 5-10% of the parent drug is recovered from the faeces. When clarithromycin 500 mg is given three times daily, the clarithromycin plasma concentrations are increased with respect to the 500 mg twice daily dosage. Clarithromycin provides tissue concentrations that are several times higher than the circulating drug levels. Increased levels have been found in both tonsillar and lung tissue. Clarithromycin is 80% bound to plasma proteins at therapeutic levels. Clarithromycin also penetrates the gastric mucus. Levels of clarithromycin in gastric mucus and gastric tissue are higher when clarithromycin is co-administered with omeprazole than when clarithromycin is administered alone.IndicationsTreatment of infections caused by susceptible organisms. Indications include:Upper respiratory tract infections for example, sinusitis, tonsillitis and pharyngitis.Lower respiratory tract infections for example, acute and chronic bronchitis, and pneumonia.Skin and soft tissue infections of mild to moderate severity for example, impetigo, erysipelas, folliculitis, furunculosis, and infected wounds.Clarithromycin in the presence of acid suppression effected by omeprazole or lansoprazole is indicated for the eradication of H. pylori in patients with duodenal ulcers. ContraindicationsClarithromycin is contra-indicated in patients with known hypersensitivity to macrolide antibiotic drugs. Clarithromycin and ergot derivatives should not be co-administered. Concomitant administration of clarithromycin and any of the following drugs is contraindicated: cisapride, pimozide and terfenadine. Elevated cisapride, pimozide and terfenadine levels have been reported in patients receiving either of these drugs and clarithromycin concomitantly. This may result in QT prolongation and cardiac arrhythmias including ventricular tachycardia, ventricular fibrillation and Torsade de Pointes. Similar effects have been observed with concomitant administration of astemizole and other macrolides.Side EffectsClarithromycin is generally well tolerated. Side effects include nausea, dyspepsia, diarrhoea, vomiting, abdominal pain and paraesthesia. Stomatitis, glossitis, oral monilia and tongue discolouration have been reported. Other side-effects include headache, arthralgia, myalgia and allergic reactions ranging from urticaria, mild skin eruptions and angioedema to anaphylaxis have been reported. There have been reports of Stevens-Johnson syndrome / toxic epidermal necrolysis with orally administered clarithromycin. Reports of alteration of the sense of smell, usually in conjunction with taste perversion have also been received. There have been reports of tooth discolouration in patients treated with clarithromycin. Tooth discolouration is usually reversible with professional dental cleaning. There have been reports of transient central nervous system side-effects including dizziness, vertigo, anxiety, insomnia, bad dreams, tinnitus, confusion, disorientation, hallucinations, psychosis and depersonalisation. There have been reports of hearing loss with clarithromycin which is usually reversible on withdrawal of therapy.Pseudomembranous colitis has been reported rarely with clarithromycin, and may range in severity from mild to life threatening. There have been rare reports of hypoglycaemia, some of which have occurred in patients on concomitant oral hypoglycaemic agents or insulin. There have been very rare reports of uveitis mainly in patients treated with concomitant rifabutin, most of these were reversible. Isolated cases of leukopenia and thrombocytopenia have been reported. As with other macrolides, hepatic dysfunction (which is usually reversible) including altered liver function tests, hepatitis and cholestasis with or without jaundice, has been reported. Dysfunction may be severe and very rarely fatal hepatic failure has been reported. Cases of increased serum creatinine, interstitial nephritis, renal failure, pancreatitis and convulsions have been reported rarely. As with other macrolides, QT prolongation, ventricular tachycardia and Torsade de Pointes have been rarely reported with clarithromycin. There have been post-marketing reports of colchicine toxicity with concomitant use of clarithromycin and colchicine especially in the elderly, some of which occurred in patients with renal insufficiency. Deaths have been reported in some such patients. PrecautionsClarithromycin is principally excreted by the liver and kidney. Caution should be exercised in administering this antibiotic to patients with impaired hepatic or renal function. Prolonged or repeated use of clarithromycin may result in an overgrowth of non-susceptible bacteria or fungi. If super-infection occurs, clarithromycin should be discontinued and appropriate therapy instituted. H. pylori organisms may develop resistance to clarithromycin in a small number of patients. There have been post-marketing reports of colchicine toxicity with concomitant

49
use of clarithromycin and colchicine, especially in the elderly, some of which occurred in patients with renal insufficiency. Deaths have been reported in some such patients.Pregnancy and LactationThe safety of clarithromycin during pregnancy and breast feeding of infants has not been established. Clarithromycin should thus not be used during pregnancy or lactation unless the benefit is considered to outweigh the risk. Some animal studies have suggested an embryotoxic effect, but only at dose levels which are clearly toxic to mothers. Clarithromycin has been found in the milk of lactating animals and in human breast milk.Effects on ability to drive and use machinesNone known.OverdosageReports indicate that the ingestion of large amounts of clarithromycin can be expected to produce gastro-intestinal symptoms. One patient who had a history of bipolar disorder ingested 8 grams of clarithromycin and showed altered mental status, paranoid behaviour, hypokalemia and hypoxemia. Adverse reactions accompanying overdosage should be treated by gastric lavage and supportive measures. As with other macrolides, clarithromycin serum levels are not expected to be appreciably affected by haemodialysis or peritoneal dialysis.Drug InteractionsClarithromycin has been shown not to interact with oral contraceptives. As with other macrolide antibiotics the use of clarithromycin in patients concurrently taking drugs metabolised by the cytochrome P450 system (eg. Cilostazol, methylprednisolone, oral anticoagulants (eg warfarin), quinidine, sildenafil, ergot alkaloids, alprazolam, triazolam, midazolam, disopyramide, lovastatin, rifabutin, phenytoin, cyclosporine vinblastine, valproate and tacrolimus.) may be associated with elevations in serum levels of these other drugs. Rhabdomyolysis, co-incident with the co- administration of clarithromycin, and lovastatin or simvastatin has been reported. The administration of clarithromycin to patients who are receiving theophylline has been associated with an increase in serum theophylline levels and potential theophylline toxicity. The use of clarithromycin in patients receiving warfarin may result in potentiation of the effects of warfarin. Prothrombin time should be frequently monitored in these patients. The effects of digoxin may be potentiated with concomitant administration of Clarithromycin. Monitoring of serum digoxin levels should be considered. Clarithromycin may potentiate the effects of carbamazepine due to a reduction in the rate of excretion. Simultaneous oral administration of clarithromycin tablets and zidovudine to HIV infected adult patients may result in decreased steady-state zidovudine levels. This can be largely avoided by staggering the doses of Clarithromycin and zidovudine by 1 -2 hours. No such reaction has been reported in children. Ritonavir increases the area under the curve (AUC), Cmax and Cmin of clarithromycin when administered concurrently. Because of the large therapeutic window for clarithromycin, no dosage reduction should be necessary in patients with normal renal function. However, for patients with renal impairment, an immediate release form of Clarithromycin should be used. The following dosage adjustments should be considered: For patients with CLCR 30 to 60 ml/min the dose of clarithromycin should be reduced by 50%. For patients with CLCR <30ml/min the dose of clarithromycin should be decreased by 75%. Doses of clarithromycin greater than 1g/day should not be coadministered with ritonavir. There have been postmarketed reports of Torsade de Pointes occurring with the concurrent use of clarithromycin and quinidine or disopyramide. Levels of these medications should be monitored during clarithromycin therapy. Post-marketing reports also indicate that co-administration of clarithromycin with ergotamine or dihydroergotamine has been associated with acute ergot toxicity characterized by vasospasm and ischaemia of the extremities and other tissues including the central nervous system. Klacid 500mg tabs: Although the plasma concentrations of clarithromycin and omeprazole may be increased when they are administered concurrently, no adjustment to the dosage is necessary. At the dosages recommended, there is no clinically significant interaction between clarithromycin and lansoprazole. Increased plasma concentrations of clarithromycin may also occur when it is co-administered with Maalox or ranitidine. No adjustment to the dosage is necessary. IncompatibilitiesNone known.Dosage AdministrationKLACID 250mg tablets and 500mg tablets: Adults: The usual dose is 250 mg twice daily for 7 days. This may be increased to 500mg twice daily for up to 14 days in severe infections.Children older than 12 years: As for adults.KLACID 500mg tablets for eradication of H. pylori in patients with duodenal ulcers:Adults:Dual Therapy (14 days):The usual dose of Clarithromycin is 500 mg three times daily for 14 days. Clarithromycin should be administered with oral omeprazole 40 mg once daily. The pivotal study was conducted with omeprazole 40 mg once daily for 28 days. Supportive studies have been conducted with omeprazole 40 mg once daily for 14 days.Triple Therapy (7 - 14 days):Clarithromycin 500mg twice daily and lansoprazole 30mg twice daily should be given with amoxycillin 1000mg twice daily for 7 - 14 days.Triple Therapy (7 days):Clarithromycin 500mg twice daily and lansoprazole 30mg twice daily should be given with metronidazole 400mg twice daily for 7 days.Triple Therapy (7 days):Clarithromycin 500mg twice daily and omeprazole 40mg daily should be given with amoxycillin 1000mg twice daily or metronidazole 400mg twice daily for 7 days.Triple Therapy (10 days):Clarithromycin 500mg twice daily should be given with amoxycillin 1000mg twice daily and omeprazole 20mg daily for 10 days.Elderly: As for adults.Renal impairment: Dosage adjustments are not usually required except in patients with severe renal impairment (creatinine clearance < 30 ml/min). If adjustment is necessary, the total daily dosage should be reduced by half, e.g. 250 mg once daily or 250 mg twice daily in more severe infections.KLACID 250mg tablets and 500mg tablets maybe given without regard to meals as food does not affect the extent of bioavailability.PackagingKlacid 500mg tablets: blister packs containing 14 tablets and 20 tablets
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
KLACID XL 500MG TABLETS ®CompositionKLACID XL 500mg tablets: yellow, ovaloid, film-coated tablet containing 500mg clarithromycin in a modified-release preparation.PropertiesPharmacodynamic Clarithromycin is a semi-synthetic derivative of erythromycin A. It exerts its antibacterial action by binding to the 50s ribosomal sub-unit of susceptible bacteria and suppresses protein synthesis. It is highly potent against a wide variety of aerobic and anaerobic gram-positive and gram-negative organisms. The minimum inhibitory concentrations (MICs) of clarithromycin are generally two-fold lower than the MICs of

50
erythromycin. The 14-hydroxy metabolite of clarithromycin also has antimicrobial activity. The MICs of this metabolite are equal or two-fold higher than the MICs of the parent compound, except for H. influenzae where the 14-hydroxy metabolite is two-fold more active than the parent compound.Clarithromycin is usually active against the following organisms in vitro:-Gram-positive Bacteria: Staphylococcus aureus (methicillin susceptible); Streptococcus pyogenes (Group A beta-hemolytic streptococci) alpha-hemolytic streptococci (viridans group); Streptococcus (Diplococcus) pneumoniae; Streptococcus agalactiae; Listeria monocytogenes.Pharmacological Gram-negative Bacteria: Haemophilus influenzae, Haemophilus parainfluenzae, Moraxella (Branhamella) catarrhalis, Neisseria gonorrhoeae; Legionella pneumophila, Bordetella pertussis, Helicobacter pylori; Campylobacter jejuni.Mycoplasma: Mycoplasma pneumoniae; Ureaplasma urealyticum.Other Organisms: Chlamydia trachomatis; Mycobacterium avium; Mycobacterium leprae; Mycobacterum kansasii; Mycobacterium chelonae; Mycobacterium fortuitum; Mycobacterium intracellulare.Anaerobes: Macrolide-susceptible Bacteroides fragilis; Clostridium perfringens; Peptococcus species; Peptostreptococcus species; Propionibacterium acnes. Clarithromycin has bactericidal activity against several bacterial strains. The organisms include Haemophilus influenzae, Streptococcus pneumoniae, Streptococcus pyogenes, Streptococcus agalactiae, Moraxella (Branhamella) catarrhalis, Neisseria gonorrhoeae, H. pylori and Campylobacter spp. Pharmacokinetic Klacid XL: The kinetics of orally administered modified-release clarithromycin have been studied in adult humans and compared with clarithromycin 250mg and 500mg immediate release tablets. The extent of absorption was found to be equivalent when equal total daily doses were administered. The absolute bioavailability is approximately 50%. Little or no unpredicted accumulation was found and the metabolic disposition did not change in any species following multiple dosing. Based upon the finding of equivalent absorption the following in vitro and in vivo data are applicable to the modified-release formulation. (A) In vitro: Results of in vitro studies showed that the protein binding of clarithromycin in human plasma averaged about 70 % at concentrations of 0.45 - 4.5 g/mL. A decrease in binding to 41% at 45.0 g/mL suggested that the binding sites might become saturated, but this only occurred at concentrations far in excess of therapeutic drug levels. (B) In vivo: Clarithromycin levels in all tissues, except the central nervous system, were several times higher than the circulating drug levels. The highest concentrations were found in the liver and lung tissue, where the tissue to plasma ratios reached 10 to 20. The pharmacokinetic behaviour of clarithromycin is non-linear. In fed patients given 500mg clarithromycin modified-release daily, the peak steady state plasma concentration of clarithromycin and 14 hydroxy clarithromycin were 1.3 and 0.48 g/mL, respectively. When the dosage was increased to 1000mg daily, these steady-state values were 2.4 g/mL and 0.67 g/mL respectively. Elimination half-lives of the parent drug and its metabolite were approximately 5.3 and 7.7 hours respectively. The apparent half-lives of both clarithromycin and its 14-hydroxyl metabolite tended to be longer at higher doses. Urinary excretion accounted for approximately 40% of the clarithromycin dose. Faecal elimination accounts for approximately 30%IndicationsTreatment of infections caused by susceptible organisms. Indications include:Upper respiratory tract infections for example, sinusitis, tonsillitis and pharyngitis.Lower respiratory tract infections for example, acute and chronic bronchitis, and pneumonia.Skin and soft tissue infections of mild to moderate severity for example, impetigo, erysipelas, folliculitis, cellulitis, furunculosis, and infected wounds.ContraindicationsClarithromycin is contra-indicated in patients with known hypersensitivity to macrolide antibiotic drugs. Clarithromycin and ergot derivatives should not be co-administered. Concomitant administration of clarithromycin and any of the following drugs is contraindicated: cisapride, pimozide and terfenadine. Elevated cisapride, pimozide and terfenadine levels have been reported in patients receiving either of these drugs and clarithromycin concomitantly. This may result in QT prolongation and cardiac arrhythmias including ventricular tachycardia, ventricular fibrillation and Torsade de Pointes. Similar effects have been observed with concomitant administration of astemizole and other macrolides.Klacid XL: As the dose cannot be reduced from 500mg daily, Klacid XL is contraindicated in patients with creatinine clearance less than 30 mL/min. Side EffectsClarithromycin is generally well tolerated. Side effects include nausea, dyspepsia, diarrhoea, vomiting, abdominal pain and paraesthesia. Stomatitis, glossitis, oral monilia and tongue discolouration have been reported. Other side-effects include headache, arthralgia, myalgia and allergic reactions ranging from urticaria, mild skin eruptions and angioedema to anaphylaxis have been reported. There have been reports of Stevens-Johnson syndrome / toxic epidermal necrolysis with orally administered clarithromycin. Reports of alteration of the sense of smell, usually in conjunction with taste perversion have also been received. There have been reports of tooth discolouration in patients treated with clarithromycin. Tooth discolouration is usually reversible with professional dental cleaning. There have been reports of transient central nervous system side-effects including dizziness, vertigo, anxiety, insomnia, bad dreams, tinnitus, confusion, disorientation, hallucinations, psychosis and depersonalisation. There have been reports of hearing loss with clarithromycin which is usually reversible on withdrawal of therapy. Pseudomembranous colitis has been reported rarely with clarithromycin, and may range in severity from mild to life threatening. There have been rare reports of hypoglycaemia, some of which have occurred in patients on concomitant oral hypoglycaemic agents or insulin. There have been very rare reports of uveitis mainly in patients treated with concomitant rifabutin, most of these were reversible. Isolated cases of leukopenia and thrombocytopenia have been reported. As with other macrolides, hepatic dysfunction (which is usually reversible) including altered liver function tests, hepatitis and cholestasis with or without jaundice, has been reported. Dysfunction may be severe and very rarely fatal hepatic failure has been reported. Cases of increased serum creatinine, interstitial nephritis, renal failure, pancreatitis and convulsions have been reported rarely. As with other macrolides, QT prolongation, ventricular tachycardia and Torsade de Pointes have been rarely reported with clarithromycin. There have been post-marketing reports of colchicine toxicity with concomitant use of clarithromycin and colchicine especially in the elderly, some of which occurred in patients with renal insufficiency. Deaths have been reported in some such patients. PrecautionsClarithromycin is principally excreted by the liver and kidney. Caution should be exercised in administering this antibiotic to patients with impaired hepatic or renal function. Prolonged or repeated use of clarithromycin may result in an overgrowth of non-susceptible bacteria or fungi. If super-infection occurs, clarithromycin should be discontinued and appropriate therapy instituted. There have been post-marketing reports of colchicine toxicity with concomitant use of clarithromycin and colchicine, especially in the elderly, some of which occurred in patients with renal insufficiency. Deaths have been reported in some such patients. Klacid XL and peadiatric suspension: patients with rare hereditary problems of fructose intolerance, glucose-galactose malabsorption or sucrase-isomaltase insufficiency should not take this medicine.Pregnancy and LactationThe safety of clarithromycin during pregnancy and breast feeding of infants has not been established. Clarithromycin should thus not be used during pregnancy or lactation unless the benefit is considered to outweigh the risk. Some animal studies have suggested an

51
embryotoxic effect, but only at dose levels which are clearly toxic to mothers. Clarithromycin has been found in the milk of lactating animals and in human breast milk.Effects on ability to drive and use machinesNone known.OverdosageReports indicate that the ingestion of large amounts of clarithromycin can be expected to produce gastro-intestinal symptoms. One patient who had a history of bipolar disorder ingested 8 grams of clarithromycin and showed altered mental status, paranoid behaviour, hypokalemia and hypoxemia. Adverse reactions accompanying overdosage should be treated by gastric lavage and supportive measures. As with other macrolides, clarithromycin serum levels are not expected to be appreciably affected by haemodialysis or peritoneal dialysis.Drug InteractionsClarithromycin has been shown not to interact with oral contraceptives. As with other macrolide antibiotics the use of clarithromycin in patients concurrently taking drugs metabolised by the cytochrome P450 system (eg. Cilostazol, methylprednisolone, oral anticoagulants (eg warfarin), quinidine, sildenafil, ergot alkaloids, alprazolam, triazolam, midazolam, disopyramide, lovastatin, rifabutin, phenytoin, cyclosporine vinblastine, valproate and tacrolimus.) may be associated with elevations in serum levels of these other drugs. Rhabdomyolysis, co-incident with the co- administration of clarithromycin, and lovastatin or simvastatin has been reported. The administration of clarithromycin to patients who are receiving theophylline has been associated with an increase in serum theophylline levels and potential theophylline toxicity. The use of clarithromycin in patients receiving warfarin may result in potentiation of the effects of warfarin. Prothrombin time should be frequently monitored in these patients. The effects of digoxin may be potentiated with concomitant administration of Clarithromycin. Monitoring of serum digoxin levels should be considered. Clarithromycin may potentiate the effects of carbamazepine due to a reduction in the rate of excretion. Interaction studies have not been conducted with Clarithromycin XL and Zidovudine. If concomitant administration of clarithromycin and zidovudine is required, then an immediate release formulation of clarithromycin should be used. Ritonavir increases the area under the curve (AUC), Cmax and Cmin of clarithromycin when administered concurrently. Because of the large therapeutic window for clarithromycin, no dosage reduction should be necessary in patients with normal renal function. However, for patients with renal impairment, an immediate release form of clarithromycin should be used. Doses of clarithromycin greater than 1g/day should not be coadministered with ritonavir. There have been postmarketed reports of Torsade de Pointes occurring with the concurrent use of clarithromycin and quinidine or disopyramide. Levels of these medications should be monitored during clarithromycin therapy. Post-marketing reports also indicate that co-administration of clarithromycin with ergotamine or dihydroergotamine has been associated with acute ergot toxicity characterized by vasospasm and ischaemia of the extremities and other tissues including the central nervous systemIncompatibilitiesNone known.Dosage AdministrationAdults: The usual recommended dosage is one 500mg modified-release tablet daily to be taken with food. In more severe infections, the dosage can be increased to two 500mg modified-release tablets daily. The usual duration of treatment is 7 to 14 days.Children older than 12 years: As for adults.Renal impairment: Klacid XL should not be used in patients with renal impairment (creatinine clearance less than 30 mL/min). Klacid immediate release tablets may be used in this patient population. PackagingKlacid XL tablets: blister packs containing 7 tablets and 14 tablets
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
KLACID GRANULES 125MG/5ML ®CompositionKLACID granules 125mg/5ml: white to off - white granules for oral suspension. After mixing each 5ml of suspension contains 125mg clarithromycinPropertiesPharmacodynamic Clarithromycin is a semi-synthetic derivative of erythromycin A. It exerts its antibacterial action by binding to the 50s ribosomal sub-unit of susceptible bacteria and suppresses protein synthesis. It is highly potent against a wide variety of aerobic and anaerobic gram-positive and gram-negative organisms. Clarithromycin is usually active against the following organisms in vitro:- Gram-positive Bacteria: Staphylococcus aureus (methicillin susceptible); Streptococcus pyogenes (Group A beta-hemolytic streptococci) alpha-hemolytic streptococci (viridans group); Streptococcus (Diplococcus) pneumoniae; Streptococcus agalactiae; Listeria monocytogenes.Pharmacological PropertiesGram-negative Bacteria: Haemophilus influenzae, Haemophilus parainfluenzae, Moraxella (Branhamella) catarrhalis, Neisseria gonorrhoeae; Legionella pneumophila, Bordetella pertussis, Helicobacter pylori; Campylobacter jejuni.Mycoplasma: Mycoplasma pneumoniae; Ureaplasma urealyticum.Other Organisms: Chlamydia trachomatis; Mycobacterium avium; Mycobacterium leprae; Mycobacterum kansasii; Mycobacterium chelonae; Mycobacterium fortuitum; Mycobacterium intracellulare.Propionibacterium acnes.Pharmacokinetic properties Clarithromycin is rapidly and well absorbed from the gastro-intestinal tract after oral administration of Clarithromycin tablets. The microbiologically active metabolite 14-hydroxyclarithromycin is formed by first pass metabolism. Clarithromycin may be given without regard to meals as food does not affect the extent of bioavailability of Clarithromycin tablets. Food does slightly delay the onset of absorption of clarithromycin and formation of the 14-hydroxymetabolite. The pharmacokinetics of clarithromycin are non linear; however, steady-state is attained within 2 days of dosing. At 250 mg b.i.d. 15-20% of unchanged drug is excreted in the urine. With 500 mg b.i.d. daily dosing urinary excretion is greater (approximately 36%).The 14-hydroxyclarithromycin is the major urinary metabolite and accounts for 10-15% of the dose. Most of the remainder of the dose is eliminated in the faeces, primarily via the bile. 5-10% of the parent drug is recovered from the faeces. When clarithromycin 500 mg is given three times daily, the clarithromycin plasma concentrations are increased with respect to the 500 mg twice daily dosage. Clarithromycin provides tissue concentrations that are several times higher than the circulating drug levels. Increased levels have been found in both tonsillar and lung tissue. Clarithromycin is 80% bound to plasma proteins at therapeutic levels. Clarithromycin also penetrates the gastric mucus. Levels of clarithromycin in gastric mucus and gastric tissue are higher when clarithromycin is co-administered with omeprazole than when clarithromycin is administered alone.IndicationsTreatment of infections caused by susceptible organisms. Indications include:Upper respiratory tract infections for example, sinusitis, tonsillitis and pharyngitis.Lower respiratory tract infections for example, acute and chronic bronchitis, and pneumonia.

52
Skin and soft tissue infections of mild to moderate severity for example, impetigo, erysipelas, folliculitis, furunculosis, and infected wounds.Treatment of acute otitis mediaContraindicationsClarithromycin is contra-indicated in patients with known hypersensitivity to macrolide antibiotic drugs. Clarithromycin and ergot derivatives should not be co-administered. Concomitant administration of clarithromycin and any of the following drugs is contraindicated: cisapride, pimozide and terfenadine. Elevated cisapride, pimozide and terfenadine levels have been reported in patients receiving either of these drugs and clarithromycin concomitantly. This may result in QT prolongation and cardiac arrhythmias including ventricular tachycardia, ventricular fibrillation and Torsade de Pointes. Similar effects have been observed with concomitant administration of astemizole and other macrolides.Side EffectsClarithromycin is generally well tolerated. Side effects include nausea, dyspepsia, diarrhoea, vomiting, abdominal pain and paraesthesia. Stomatitis, glossitis, oral monilia and tongue discolouration have been reported. Other side-effects include headache, arthralgia, myalgia and allergic reactions ranging from urticaria, mild skin eruptions and angioedema to anaphylaxis have been reported. There have been reports of Stevens-Johnson syndrome / toxic epidermal necrolysis with orally administered clarithromycin. Reports of alteration of the sense of smell, usually in conjunction with taste perversion have also been received. There have been reports of tooth discolouration in patients treated with clarithromycin. Tooth discolouration is usually reversible with professional dental cleaning. There have been reports of transient central nervous system side-effects including dizziness, vertigo, anxiety, insomnia, bad dreams, tinnitus, confusion, disorientation, hallucinations, psychosis and depersonalisation. There have been reports of hearing loss with clarithromycin which is usually reversible on withdrawal of therapy. Pseudomembranous colitis has been reported rarely with clarithromycin, and may range in severity from mild to life threatening. There have been rare reports of hypoglycaemia, some of which have occurred in patients on concomitant oral hypoglycaemic agents or insulin. There have been very rare reports of uveitis mainly in patients treated with concomitant rifabutin, most of these were reversible. Isolated cases of leukopenia and thrombocytopenia have been reported. As with other macrolides, hepatic dysfunction (which is usually reversible) including altered liver function tests, hepatitis and cholestasis with or without jaundice, has been reported. Dysfunction may be severe and very rarely fatal hepatic failure has been reported. Cases of increased serum creatinine, interstitial nephritis, renal failure, pancreatitis and convulsions have been reported rarely. As with other macrolides, QT prolongation, ventricular tachycardia and Torsade de Pointes have been rarely reported with clarithromycin. There have been post-marketing reports of colchicine toxicity with concomitant use of clarithromycin and colchicine especially in the elderly, some of which occurred in patients with renal insufficiency. Deaths have been reported in some such patients. PrecautionsClarithromycin is principally excreted by the liver and kidney. Caution should be exercised in administering this antibiotic to patients with impaired hepatic or renal function.Prolonged or repeated use of clarithromycin may result in an overgrowth of non-susceptible bacteria or fungi. If super-infection occurs, clarithromycin should be discontinued and appropriate therapy instituted. There have been post-marketing reports of colchicine toxicity with concomitant use of clarithromycin and colchicine, especially in the elderly, some of which occurred in patients with renal insufficiency. Deaths have been reported in some such patients. Klacid XL and peadiatric suspension: patients with rare hereditary problems of fructose intolerance, glucose-galactose malabsorption or sucrase-isomaltase insufficiency should not take this medicine.OverdosageReports indicate that the ingestion of large amounts of clarithromycin can be expected to produce gastro-intestinal symptoms. One patient who had a history of bipolar disorder ingested 8 grams of clarithromycin and showed altered mental status, paranoid behaviour, hypokalemia and hypoxemia. Adverse reactions accompanying overdosage should be treated by gastric lavage and supportive measures. As with other macrolides, clarithromycin serum levels are not expected to be appreciably affected by haemodialysis or peritoneal dialysis.Drug InteractionsClarithromycin has been shown not to interact with oral contraceptives. As with other macrolide antibiotics the use of clarithromycin in patients concurrently taking drugs metabolised by the cytochrome P450 system (eg. Cilostazol, methylprednisolone, oral anticoagulants (eg warfarin), quinidine, sildenafil, ergot alkaloids, alprazolam, triazolam, midazolam, disopyramide, lovastatin, rifabutin, phenytoin, cyclosporine vinblastine, valproate and tacrolimus.) may be associated with elevations in serum levels of these other drugs. Rhabdomyolysis, co-incident with the co- administration of clarithromycin, and lovastatin or simvastatin has been reported. The administration of clarithromycin to patients who are receiving theophylline has been associated with an increase in serum theophylline levels and potential theophylline toxicity. The use of clarithromycin in patients receiving warfarin may result in potentiation of the effects of warfarin. Prothrombin time should be frequently monitored in these patients. The effects of digoxin may be potentiated with concomitant administration of Clarithromycin. Monitoring of serum digoxin levels should be considered. Simultaneous oral administration of clarithromycin tablets and zidovudine to HIV infected adult patients may result in decreased steady-state zidovudine levels. This can be largely avoided by staggering the doses of Clarithromycin and zidovudine by 1 -2 hours. No such reaction has been reported in children. Ritonavir increases the area under the curve (AUC), Cmax and Cmin of clarithromycin when administered concurrently. Because of the large therapeutic window for clarithromycin, no dosage reduction should be necessary in patients with normal renal function. However, for patients with renal impairment, the following dosage adjustments should be considered: For patients with CLCR 30 to 60 ml/min the dose of clarithromycin should be reduced by 50%. For patients with CLCR < 30 ml/min the dose of clarithromycin should be decreased by 75%. Doses of clarithromycin greater than 1g/day should not be coadministered with ritonavir. There have been postmarketed reports of Torsade de Pointes occurring with the concurrent use of clarithromycin and quinidine or disopyramide. Levels of these medications should be monitored during clarithromycin therapy. Post-marketing reports also indicate that co-administration of clarithromycin with ergotamine or dihydroergotamine has been associated with acute ergot toxicity characterized by vasospasm and ischaemia of the extremities and other tissues including the central nervous system. IncompatibilitiesNone known.Dosage AdministrationKLACID granules 125mg/5ml: For infants 6 months and above, the recommended daily dosage is 15 mg/kg/day in two divided doses. The dose can be increased according to the severity of illness and physician's opinionChild weight (kg) Dosage (ml) bid
5-10 2.5ml
11-20 5ml
21-30 7.5mlRenal impairment: Dosage adjustments are not usually required except in patients with severe renal impairment (creatinine clearance < 30 ml/min). If adjustment is necessary, the total daily dosage should be reduced by half, e.g. 250 mg once daily or 250 mg twice daily in more severe infections.

53
PackagingKlacid granules 125mg/5ml: 60ml and 100ml bottles with dispenser
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
KLACID GRANULES 250MG/5ML ®CompositionKLACID granules 250mg/5ml: white to off - white granules for oral suspension. After mixing each 5ml of suspension contains 250mg clarithromycinPropertiesPharmacodynamic propertiesClarithromycin is a semi-synthetic derivative of erythromycin A. It exerts its antibacterial action by binding to the 50s ribosomal sub-unit of susceptible bacteria and suppresses protein synthesis. It is highly potent against a wide variety of aerobic and anaerobic gram-positive and gram-negative organisms. The minimum inhibitory concentrations (MICs) of clarithromycin are generally two-fold lower than the MICs of erythromycin. The 14-hydroxy metabolite of clarithromycin also has antimicrobial activity. The MICs of this metabolite are equal or two-fold higher than the MICs of the parent compound, except for H. influenzae where the 14-hydroxy metabolite is two-fold more active than the parent compound.Pharmacological PropertiesClarithromycin is usually active against the following organisms in vitro:-Gram-positive Bacteria: Staphylococcus aureus (methicillin susceptible); Streptococcus pyogenes (Group A beta-hemolytic streptococci) alpha-hemolytic streptococci (viridans group); Streptococcus (Diplococcus) pneumoniae; Streptococcus agalactiae; Listeria monocytogenes.Gram-negative Bacteria: Haemophilus influenzae, Haemophilus parainfluenzae, Moraxella (Branhamella) catarrhalis, Neisseria gonorrhoeae; Legionella pneumophila, Bordetella pertussis, Helicobacter pylori; Campylobacter jejuni.Mycoplasma: Mycoplasma pneumoniae; Ureaplasma urealyticum.Other Organisms: Chlamydia trachomatis; Mycobacterium avium; Mycobacterium leprae; Mycobacterum kansasii; Mycobacterium chelonae; Mycobacterium fortuitum; Mycobacterium intracellulare.Anaerobes: Macrolide-susceptible Bacteroides fragilis; Clostridium perfringens; Peptococcus species; Peptostreptococcus species; Propionibacterium acnes. Clarithromycin has bactericidal activity against several bacterial strains. The organisms include Haemophilus influenzae, Streptococcus pneumoniae, Streptococcus pyogenes, Streptococcus agalactiae, Moraxella (Branhamella) catarrhalis, Neisseria gonorrhoeae, H. pylori and Campylobacter spp. Pharmacokinetic properties Clarithromycin is rapidly and well absorbed from the gastro-intestinal tract after oral administration of Clarithromycin tablets. The microbiologically active metabolite 14-hydroxyclarithromycin is formed by first pass metabolism. Clarithromycin may be given without regard to meals as food does not affect the extent of bioavailability of Clarithromycin tablets. Food does slightly delay the onset of absorption of clarithromycin and formation of the 14-hydroxymetabolite. The pharmacokinetics of clarithromycin are non linear; however, steady-state is attained within 2 days of dosing. The 14-hydroxyclarithromycin is the major urinary metabolite and accounts for 10-15% of the dose. Most of the remainder of the dose is eliminated in the faeces, primarily via the bile. 5-10% of the parent drug is recovered from the faeces. Clarithromycin provides tissue concentrations that are several times higher than the circulating drug levels. Increased levels have been found in both tonsillar and lung tissue. Clarithromycin is 80% bound to plasma proteins at therapeutic levels. IndicationsTreatment of infections caused by susceptible organisms. Indications include:Upper respiratory tract infections for example, sinusitis, tonsillitis and pharyngitis.Lower respiratory tract infections for example, acute and chronic bronchitis, and pneumonia.Skin and soft tissue infections of mild to moderate severity for example, impetigo, erysipelas, folliculitis, furunculosis, and infected wounds.Treatment of acute otitis media ContraindicationsClarithromycin is contra-indicated in patients with known hypersensitivity to macrolide antibiotic drugs. Clarithromycin and ergot derivatives should not be co-administered. Concomitant administration of clarithromycin and any of the following drugs is contraindicated: cisapride, pimozide and terfenadine. Elevated cisapride, pimozide and terfenadine levels have been reported in patients receiving either of these drugs and clarithromycin concomitantly. This may result in QT prolongation and cardiac arrhythmias including ventricular tachycardia, ventricular fibrillation and Torsade de Pointes. Similar effects have been observed with concomitant administration of astemizole and other macrolides.Side EffectsClarithromycin is generally well tolerated. Side effects include nausea, dyspepsia, diarrhoea, vomiting, abdominal pain and paraesthesia. Stomatitis, glossitis, oral monilia and tongue discolouration have been reported. Other side-effects include headache, arthralgia, myalgia and allergic reactions ranging from urticaria, mild skin eruptions and angioedema to anaphylaxis have been reported. There have been reports of Stevens-Johnson syndrome / toxic epidermal necrolysis with orally administered clarithromycin. Reports of alteration of the sense of smell, usually in conjunction with taste perversion have also been received. There have been reports of tooth discolouration in patients treated with clarithromycin. Tooth discolouration is usually reversible with professional dental cleaning. There have been reports of transient central nervous system side-effects including dizziness, vertigo, anxiety, insomnia, bad dreams, tinnitus, confusion, disorientation, hallucinations, psychosis and depersonalisation. There have been reports of hearing loss with clarithromycin which is usually reversible on withdrawal of therapy. Pseudomembranous colitis has been reported rarely with clarithromycin, and may range in severity from mild to life threatening. There have been rare reports of hypoglycaemia, some of which have occurred in patients on concomitant oral hypoglycaemic agents or insulin. There have been very rare reports of uveitis mainly in patients treated with concomitant rifabutin, most of these were reversible. Isolated cases of leukopenia and thrombocytopenia have been reported. As with other macrolides, hepatic dysfunction (which is usually reversible) including altered liver function tests, hepatitis and cholestasis with or without jaundice, has been reported. Dysfunction may be severe and very rarely fatal hepatic failure has been reported. Cases of increased serum creatinine, interstitial nephritis, renal failure, pancreatitis and convulsions have been reported rarely. As with other macrolides, QT prolongation, ventricular tachycardia and Torsade de Pointes have been rarely reported with clarithromycin. There have been post-marketing reports of colchicine toxicity with concomitant use of clarithromycin and colchicine especially in the elderly, some of which occurred in patients with renal insufficiency. Deaths have been reported in some such patients. PrecautionsClarithromycin is principally excreted by the liver and kidney. Caution should be exercised in administering this antibiotic to patients with impaired hepatic or renal function. Prolonged or repeated use of clarithromycin may result in an overgrowth of non-susceptible bacteria or fungi. If super-infection occurs, clarithromycin should be discontinued and appropriate therapy instituted.

54
There have been post-marketing reports of colchicine toxicity with concomitant use of clarithromycin and colchicine, especially in the elderly, some of which occurred in patients with renal insufficiency. Deaths have been reported in some such patients. Klacid XL and peadiatric suspension: patients with rare hereditary problems of fructose intolerance, glucose-galactose malabsorption or sucrase-isomaltase insufficiency should not take this medicine.Pregnancy and LactationThe safety of clarithromycin during pregnancy and breast feeding of infants has not been established. Clarithromycin should thus not be used during pregnancy or lactation unless the benefit is considered to outweigh the risk. Some animal studies have suggested an embryotoxic effect, but only at dose levels which are clearly toxic to mothers. Clarithromycin has been found in the milk of lactating animals and in human breast milk.Effects on ability to drive and use machinesNone known.OverdosageReports indicate that the ingestion of large amounts of clarithromycin can be expected to produce gastro-intestinal symptoms. One patient who had a history of bipolar disorder ingested 8 grams of clarithromycin and showed altered mental status, paranoid behaviour, hypokalemia and hypoxemia. Adverse reactions accompanying overdosage should be treated by gastric lavage and supportive measures. As with other macrolides, clarithromycin serum levels are not expected to be appreciably affected by haemodialysis or peritoneal dialysisDrug InteractionsAs with other macrolide antibiotics the use of clarithromycin in patients concurrently taking drugs metabolised by the cytochrome P450 system (eg. Cilostazol, methylprednisolone, oral anticoagulants (eg warfarin), quinidine, sildenafil, ergot alkaloids, alprazolam, triazolam, midazolam, disopyramide, lovastatin, rifabutin, phenytoin, cyclosporine vinblastine, valproate and tacrolimus.) may be associated with elevations in serum levels of these other drugs. Rhabdomyolysis, co-incident with the co- administration of clarithromycin, and lovastatin or simvastatin has been reported. The administration of clarithromycin to patients who are receiving theophylline has been associated with an increase in serum theophylline levels and potential theophylline toxicity. The use of clarithromycin in patients receiving warfarin may result in potentiation of the effects of warfarin. Prothrombin time should be frequently monitored in these patients. The effects of digoxin may be potentiated with concomitant administration of Clarithromycin. Monitoring of serum digoxin levels should be considered. Clarithromycin may potentiate the effects of carbamazepine due to a reduction in the rate of excretion. Simultaneous oral administration of clarithromycin tablets and zidovudine to HIV infected adult patients may result in decreased steady-state zidovudine levels. No such reaction has been reported in children. Ritonavir increases the area under the curve (AUC), Cmax and Cmin of clarithromycin when administered concurrently. Because of the large therapeutic window for clarithromycin, no dosage reduction should be necessary in patients with normal renal function. However, for patients with renal impairment, the following dosage adjustments should be considered: For patients with CLCR 30 to 60 ml/min the dose of clarithromycin should be reduced by 50%. For patients with CLCR <30ml/min the dose of clarithromycin should be decreased by 75%. Doses of clarithromycin greater than 1g/day should not be coadministered with ritonavir. There have been postmarketed reports of Torsade de Pointes occurring with the concurrent use of clarithromycin and quinidine or disopyramide. Levels of these medications should be monitored during clarithromycin therapy. Post-marketing reports also indicate that co-administration of clarithromycin with ergotamine or dihydroergotamine has been associated with acute ergot toxicity characterized by vasospasm and ischaemia of the extremities and other tissues including the central nervous system. IncompatibilitiesNone known.Dosage AdministrationKLACID granules 250mg/5ml: The usual duration of treatment is for 5 to 10 days depending on the pathogen involved and the severity of the condition. The recommended daily dosage of Klacid Paediatric Suspension 250mg/5ml in children is given in the following table and is based on a 7.5mg/kg twice a day dosage regimen. Doses up to 500mg twice a day have been used in the treatment of severe infections.Dosage in ChildrenWeight *(kg) Approx Age(yrs) Dosage (ml) bid
8-11 1 - 2 1.25
12-19 3 - 6 2.5
20-29 7 - 9 3.75
30-40 10 - 12 5
* Children < 8 kg should be dosed on a per kg basis (approx. 7.5 mg/kg twice a day)PackagingKlacid granules 250mg/5ml: 100ml bottle with dispenser
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
LUPRON DEPOT 3.75 MG ®General(Leuprolide acetate for depot suspension).CompositionLeuprolide acetate is a synthetic nonapeptide analog of naturally occurring gonadotropin releasing hormone (GnRH or LH-RH). The analog possesses greater potency than the natural hormone. The chemical name is 5-Oxo-L-prolyl-L-histidyl-L-tryptophyl-L-seryl-L-tyrosyl- D-leucyl-L-leucyl-L-arginyl-N-ethyl-L-prolinamide acetate (salt) with the following structural formula (see Figure 1).

55
Lupron Depot 3.75 Figure 1.Structural formulaLUPRON DEPOT is supplied in a vial containing sterile Iyophilized microspheres, which when mixed with diluent, become a suspension, which is intended as a monthly intramuscular injection.The single-dose vial contains leuprolide acetate (3.75 mg), purified gelatin (0.65 mg), DL-lactic and glycolic acids copolymer (33.1 mg), and D-mannitol (6.6 mg). The accompanying ampule of diluent contains carboxymethylcellulose sodium (10 mg), D-mannitol (100 mg), polysorbate 80 (2 mg), water for injection, USP, and glacial acetic acid, USP to control pH.During the manufacturing process of LUPRON DEPOT, acetic acid is lost, leaving the peptide.PropertiesClinical PharmacologyLeuprolide acetate is a long-acting GnRH analog. A single monthly injection of LUPRON DEPOT results in an initial stimulation followed by a prolonged suppression of pituitary gonadotropins. Repeated dosing at monthly intervals results in decreased secretion of gonadal steroids; consequently, tissues and functions that depend on gonadal steroids for their maintenance become quiescent. This effect is reversible on discontinuation of drug therapy.Leuprolide acetate is not active when given orally. Intramuscular injection of the depot formulation provides plasma concentrations of leuprolide over a period of one month. In female volunteers receiving a single dose of LUPRON DEPOT 3.75 mg IM, there was an initial burst of leuprolide in plasma. Mean plasma leuprolide levels of approximately 0.23 ng/mL to 0.34 ng/mL were maintained over a period of four to five weeks, and then slowly tapered off becoming undetectable eight weeks after injection. Absolute bioavailability from the 3.75 mg dose was estimated to be about 80%.The metabolism, distribution and excretion of leuprolide in humans have not been fully determined.The pharmacokinetics of the drug in hepatic- and renal-impaired patients have not been determined.Clinical StudiesIn controlled clinical studies, LUPRON DEPOT 3.75 mg monthly for six months was shown to be comparable to danazol 800 mg/day in relieving the clinical symptoms of endometriosis (pelvic pain, dysmenorrhea, dyspareunia, pelvic tenderness, and induration) and in reducing the size of endometrial implants as evidenced by laparoscopy. The clinical significance of a decrease in endometriotic lesions is not known at this time, and in addition laparoscopic staging of endometriosis does not necessarily correlate with the severity of symptoms.LUPRON DEPOT 3.75 mg monthly induced amenorrhea in 74% and 98% of the patients after the first and second treatment months respectively. Most of the remaining patients reported episodes of only light bleeding or spotting. In the first, second and third post-treatment months, normal menstrual cycles resumed in 7%, 71% and 95% respectively, of those patients who did not become pregnant.Figure 2 illustrates the percent of patients with symptoms at baseline, final treatment visit and sustained relief at 6 and 12 months following discontinuation of treatment for the various symptoms evaluated during the study. This included all patients at end of treatment and those who elected to participate at the follow-up periods. This might provide a slight bias in the results at follow-up as 75% of the original patients entered the follow-up study and 36% were evaluated at 6 months and 26% at 12 months respectively.

56
LUPRON DEPOT 3,75 Figure 2. Percent of patients with symptoms at baseline, final treatment visit, and after 6 and 12 months of follow-upThere is no evidence that pregnancy rates are enhanced or adversely affected by the use of LUPRON DEPOT.IndicationsExperience with LUPRON DEPOT in females has been limited to women 18 years of age and older treated for 6 months.LUPRON DEPOT 3.75 mg is indicated for management of endometriosis, including pain relief and reduction of endometriotic lesions.Contraindications1. Hypersensitivity to GnRH, GnRH agonist analogs or any of the excipients in LUPRON DEPOT.2. Undiagnosed abnormal vaginal bleeding.3. LUPRON DEPOT is contraindicated in women who are or may become pregnant while receiving the drug. LUPRON DEPOT may cause fetal harm when administered to a pregnant woman. Major fetal abnormalities were observed in rabbits but not in rats after administration of LUPRON DEPOT throughout gestation. There was increased fetal mortality and decreased fetal weights in rats and rabbits (see Pregnancy section). The effects on fetal mortality are expected consequences of the alterations in hormonal levels brought about by the drug. If this drug is used during pregnancy or if the patient becomes pregnant while taking this drug, she should be apprised of the potential hazard to the fetus.4. Use in women who are breast feeding (see Pregnancy and Lactation section).5. A report of an anaphylactic reaction to synthetic GnRH (Factrel) has been reported in the medical literature.Side EffectsEstradiol levels may increase during the first weeks following the initial injection, but then decline to menopausal levels. This transient increase in estradiol can be associated with a temporary worsening of signs and symptoms (see Warnings section).As would be expected with a drug that lowers serum estradiol levels, the most frequently reported adverse reactions were those related to hypoestrogenism.In controlled studies comparing LUPRON DEPOT 3.75 mg monthly and danazol (800 mg/day), or placebo, adverse reactions most frequently reported and thought to be possibly or probably drug-related are shown in Figure 3.

57
LUPRON 3,75 Figure 3. Adverse events reported during 6 months of treatment with Luproin Depot 3,75 mgCardiovascular System – Palpitations, Syncope, Tachycardia; Gastrointestinal System – Dry mouth, Thirst, Appetite changes; Central/Peripheral Nervous System – Anxiety,* Personality disorder, Memory disorder, Delusions; Integumentary System – Ecchymosis, Alopecia, Hair disorder; Urogenital System – Dysuria,* Lactation; Miscellaneous – Ophthalmologic disorders,* Lymphadenopathy.In other clinical trials involving patients with prostate cancer and during postmarketing surveillance, the following adverse reactions were reported to have a possible, probable, or unknown relationship to LUPRON as ascribed by the treating physician. Often, it is difficult to assess causality in patients with prostate cancer. Reactions considered not drug related have been excluded.Cardiovascular System – Congestive heart failure, ECG changes/ischemia, High blood pressure, Murmur, Phlebitis/thrombosis, Angina, Cardiac arrhythmias, Myocardial infarction, Pulmonary emboli, Hypotension, Transient ischemic attack/stroke; Gastrointestinal System – Dysphagia, Gastrointestinal bleeding, Peptic ulcer, Rectal polyps, Hepatic dysfunction; Endocrine System – Decreased testicular size, Gynecomastia, Impotence, Libido increase, Thyroid enlargement; Hemic and Lymphatic System – Anemia, Decreased WBC, Hemoptysis; Musculoskeletal System – Bone pain; Central/Peripheral Nervous System – Peripheral neuropathy, Syncope/blackouts, Hearing disorder, Spinal fracture/paralysis; Respiratory System – Dyspnea, Sinus congestion, Cough, Pleural rub, Pneumonia, Pulmonary fibrosis, Respiratory disorders; Urogenital System – Frequency/urgency, Hematuria, Urinary tract infection, Bladder spasms, Incontinence, Testicular pain, Urinary obstruction, Penile swelling, Prostate pain; Miscellaneous – Diabetes, Fever, Hypoglycemia, Increased BUN, Increased calcium, Increased creatinine, Inflammation.Changes in Bone Density:A controlled study in endometriosis patients showed that vertebral bone density as measured by dual energy x-ray absorptiometry (DEXA) decreased by an average of 3.9% at six months compared with the pretreatment value. Earlier studies in endometriosis patients, utilizing quantitative computed tomography (QCT), demonstrated that in the few patients who were retested at six and 12 months, partial to complete recovery of bone density was recorded in the post-treatment period. Use of LUPRON DEPOT for longer than six months or in the presence of other known risk factors for decreased bone mineral content may cause additional bone loss.Changes in Laboratory Values During Treatment:Plasma enzymes: During clinical trials with LUPRON DEPOT, regular laboratory monitoring revealed that SGOT levels were more than twice the upper limit of normal in only one patient. There was no other clinical or laboratory evidence of abnormal liver function.Lipids: At enrollment, 4% of the LUPRON DEPOT patients and 1% of the danazol patients had total cholesterol values above the normal range. These patients also had cholesterol values above the normal range at the end of treatment.Of those patients whose pretreatment cholesterol values were in the normal range, 7% of the LUPRON DEPOT patients and 9% of the danazol patients had post-treatment values above the normal range.The mean (±SEM) pretreatment values for total cholesterol from all patients were 178.8 (2.9) mg/dL in the LUPRON DEPOT group and 175.3 (3.0) mg/dL in the danazol group. At the end of treatment, the mean values for total cholesterol from all patients were 193.3 mg/dL in the LUPRON DEPOT group and 194.4 mg/dL in the danazol group. These increases from the pretreatment values were statistically significant (p<0.03) in both groups.Triglycerides were increased above the upper limit of normal in 12% of the patients who received LUPRON DEPOT and in 6% of the patients who received danazol.At the end of treatment, HDL cholesterol fractions decreased below the lower limit of the normal range in 2% of the LUPRON DEPOT patients compared with 54% of those receiving danazol. LDL cholesterol fractions increased above the upper limit of the normal range in 6% of the patients receiving LUPRON DEPOT compared with 23% of those receiving danazol. There was no increase in the LDL/HDL ratio in patients receiving LUPRON DEPOT, but there was approximately a twofold increase in the LDL/HDL ratio in patients receiving danazol.Other changes: In comparative studies, the following changes were seen in approximately 5% to 8% of patients. LUPRON DEPOT was associated with elevations of LDH and phosphorus, and decreases in WBC counts. Danazol therapy was associated with increases in hematocrit, platelet count, and LDH.PrecautionsSafe use of leuprolide acetate in pregnancy has not been established clinically. Before starting treatment with LUPRON DEPOT, pregnancy must be excluded.When used monthly at the recommended dose, LUPRON DEPOT usually inhibits ovulation and stops menstruation. Contraception is not insured, however, by taking LUPRON DEPOT. Therefore, patients should use nonhormonal methods of contraception. Patients should be advised to see their physician if they believe they may be pregnant. If a patient becomes pregnant during treatment, the drug must be discontinued and the patient must be apprised of the potential risk to the fetus.

58
During the early phase of therapy, sex steroids temporarily rise above baseline because of the physiologic effect of the drug. Therefore, an increase in clinical signs and symptoms may be observed during the initial days of therapy, but these will dissipate with continued therapy.Information for Patients: An information pamphlet for patients is included with the product. Patients should be aware of the following information:Since menstruation should stop with effective doses of LUPRON DEPOT, the patient should notify her physician if regular menstruation persists. Patients missing successive doses of LUPRON DEPOT may experience breakthrough bleeding.Patients should not use LUPRON DEPOT if they are pregnant, breast feeding, have undiagnosed abnormal vaginal bleeding, or are allergic to any of the ingredients in LUPRON DEPOT.Safe use of the drug in pregnancy has not been established clinically. Therefore, a nonhormonal method of contraception should be used during treatment. Patients should be advised that if they miss successive doses of LUPRON DEPOT, breakthrough bleeding or ovulation may occur with the potential for conception. If a patient becomes pregnant during treatment, she should discontinue treatment and consult her physician.Those adverse events occurring in clinical studies with LUPRON DEPOT are associated with hypoestrogenism; like hot flashes, headaches, emotional lability, decreased libido, acne, myalgia, reduction in breast size, and vaginal dryness. Estrogen levels returned to normal after treatment was discontinued.The induced hypoestrogenic state results in a small loss in bone density over the course of treatment, some of which may not be reversible. For a period up to six months, this bone loss should not be important. In patients with major risk factors for decreased bone mineral content such as chronic alcohol and/or tobacco use, strong family history of osteoporosis, or chronic use of drugs that can reduce bone mass such as anticonvulsants or corticosteroids, LUPRON DEPOT therapy may pose an additional risk. In these patients, the risks and benefits must be weighed carefully before therapy with LUPRON DEPOT is instituted. Repeated courses of therapy with gonadotropin-releasing hormone analogs beyond six months are not advisable in patients with major risk factors for loss of bone mineral content.Retreatment cannot be recommended since safety data beyond 6 months are not available.Drug InteractionsNo pharmacokinetic-based drug–drug interaction studies have been conducted with LUPRON DEPOT. However, because leuprolide acetate is a peptide that is primarily degraded by peptidase and not by cytochrome P-450 enzymes as noted in specific studies, and the drug is only about 46% bound to plasma proteins, drug interactions would not be expected to occur.Drug/Laboratory Test Interactions: Administration of LUPRON DEPOT in therapeutic doses results in suppression of the pituitary-gonadal system. Normal function is usually restored within one to three months after treatment is discontinued. Therefore, diagnostic tests of pituitary gonadotropic and gonadal functions conducted during treatment and up to one to two months after discontinuation of LUPRON DEPOT therapy may be misleading.Carcinogenesis, Mutagenesis, Impairment of Fertility: A two-year carcinogenicity study was conducted in rats and mice. In rats, a doserelated increase of benign pituitary hyperplasia and benign pituitary adenomas was noted at 24 months when the drug was administered subcutaneously at high daily doses (0.6 to 4 mg/kg). There was a significant but not dose-related increase of pancreatic islet-cell adenomas in females and of testicular interstitial cell adenomas in males (highest incidence in the low dose group). In mice, no leuprolide acetateinduced tumors or pituitary abnormalities were observed at a dose as high as 60 mg/kg for two years. Patients have been treated with leuprolide acetate for up to three years with doses as high as 10 mg/day and for two years with doses as high as 20 mg/day without demonstrable pituitary abnormalities.Mutagenicity studies have been performed with leuprolide acetate using bacterial and mammalian systems. These studies provided no evidence of a mutagenic potential.Clinical and pharmacologic studies in adults with leuprolide acetate and similar analogs have shown full reversibility of fertility suppression when the drug is discontinued after continuous administration for periods of up to six months. Although no clinical studies have been completed in children to assess the full reversibility of fertility suppression, animal studies (prepubertal and adult rats and monkeys) with leuprolide acetate and other GnRH analogs have shown functional recovery.Pediatric Use: See LUPRON DEPOT-PED® (leuprolide acetate for depot suspension) labeling for the safety and effectiveness in children with central precocious puberty.Pregnancy and LactationPregnancy, Teratogenic Effects: Pregnancy Category X. (See Contraindications section.) When administered on day 6 of pregnancy at test dosages of 0.00024, 0.0024, and 0.024 mg/kg (1/300 to 1/3 the human dose) to rabbits, LUPRON DEPOT produced a dose related increase in major fetal abnormalities. Similar studies in rats failed to demonstrate an increase in fetal malformations. There was increased fetal mortality and decreased fetal weights with the two higher doses of LUPRON DEPOT in rabbits and with the highest dose (0.024 mg/kg) in rats.Nursing Mothers: It is not known whether LUPRON DEPOT is excreted in human milk. Because many drugs are excreted in human milk, and because the effects of LUPRON DEPOT on lactation and/or the breastfed child have not been determined, LUPRON DEPOT should not be used by nursing mothers.OverdosageIn rats subcutaneous administration of 250 to 500 times the recommended human dose, expressed on a per body weight basis, resulted in dyspnea, decreased activity, and local irritation at the injection site. There is no evidence at present that there is a clinical counterpart of this phenomenon. In early clinical trials using daily subcutaneous leuprolide acetate in patients with prostate cancer, doses as high as 20 mg/day for up to two years caused no adverse effects differing from those observed with the 1 mg/day dose.Dosage AdministrationLUPRON DEPOT Must Be Administered Under The Supervision Of A Physician.The recommended dose of LUPRON DEPOT is 3.75 mg, incorporated in a depot formulation. The Iyophilized microspheres are to be reconstituted and administered monthly as a single intramuscular injection, in accord with the following directions:- Using a syringe with a 22 gauge nee-dle, withdraw 1 mL of diluent from the ampule, and inject it into the vial. (Extra diluent is provided; any remaining should be discarded.)- Shake well to thoroughly disperse particles to obtain a uniform suspension. The suspension will appear milky.- Withdraw the entire contents of the vial into the syringe and inject it at the time of reconstitution.Although the suspension has been shown to be stable for 24 hours following reconstitution, since the product does not contain a preservative, the suspension should be discarded if not used immediately.The recommended duration of administration is six months. Retreatment cannot be recommended since safety data for retreatment are not available. If the symptoms of endometriosis recur after a course of therapy, and further treatment with LUPRON DEPOT is contemplated, it is recommended that bone density be assessed before retreatment begins to ensure that values are within normal limits.As with other drugs administered by injection, the injection site should be varied periodically.The vial of LUPRON DEPOT and the ampule of diluent may be stored at room temperature.PackagingLUPRON DEPOT 3.75 mg is available in a single use kit (NDC 0300- 3639-01) and in a six pack of drug only (NDC 0300-3639-06). Each vial contains sterile lyophilized microspheres which is leuprolide incorporated in biodegradable copolymer of lactic and glycolic acids. When mixed with 1 mL of diluent, LUPRON DEPOT 3.75 mg is administered as a single monthly IM injection.No refrigeration necessary. Protect from freezing.

59
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
LUPRON DEPOT 11.25 MG ®GeneralLeuprolide Acetate for Depot SuspensionLUPRON DEPOT-3 Month 11.25 mg is a formulation of leuprolide acetate supplied in a vial containing sterile Iyophilized microspheres. When mixed with diluent, it becomes a suspension which is administered as an intramuscular or subcutaneous injection every three months.CompositionActive/lnactive Ingredients:The single-dose vial of LUPRON DEPOT-3 Month 11.25 mg contains leuprolide acetate (11.25 mg), a polymer, poly (Dllactic acid) 99.3 mg and D-mannitol 19.45 mg. The compound is easily soluble in polar solutions such as water and anhydrous ethanol and propylene glycol. It is nearly insoluble in chloroform. The pH value of a solution containing 100 mg dry powder of leuprolide acetate in one mL of solution is approximately five to seven.The accompanying ampule of diluent used for reconstitution with the leuprolide acetate powder contains a clear, colorless, slightly viscous solution of carboxymethylcellulose (10 mg), D-mannitol (100 mg), polysorbate 80 (2 mg), water for injection (2 mL) and glacial acetic acid to control pH. (see Figure 1).
Lupron Depot 11.25 Figure 1. Structural formulaPropertiesLeuprolide acetate is a synthetic nonapeptide analog of naturally occurring gonadotrophin releasing hormone (GnRH or LHRH). The analogue possesses greater potency than the natural hormone.The chemical name is 5-oxo-L-prolyl-L-histidyl-L-tryptophyl-L-seryl-L-tyrosyl-D-leucyl-L-leucyl-L-arginyl-N-ethyl-L-prolinamide acetate (salt) and the structural formula isas follows:This is combined labeling:- General information.- Information on endometriosis.- Information on uterine fibroids.Clinical PharmacologyLeuprolide acetate is a long-acting GnRH analog. A single injection of LUPRON DEPOT-3 Month 11.25 mg will result in an initial stimulation followed by a prolonged suppression of pituitary gonadotropins. Repeated dosing at quarterly (LUPRON DEPOT-3 Month 11.25 mg) intervals results in decreased secretion of gonadal steroids; consequently, tissues and functions that depend on gonadal steroids for their maintenance become quiescent. This effect is reversible on discontinuation of drug therapy. Leuprolide acetate is not active when given orally.PharmacokineticsAbsorption: Following a single injection of the three month formulation of LUPRON DEPOT-3 Month 11.25 mg in female subjects, a mean plasma leuprolide concentration of 36.3 ng/mL was observed at 4 hours. Leuprolide appeared to be released at a constant rate following the onset of steadystate levels during the third week after dosing and mean levels then declined gradually to near the lower limit of detection by 12 weeks. The mean (± standard deviation) leuprolide concentration from 3 to 12 weeks was 0.23 ±0.09 ng/mL. However, intact leuprolide and an inactive major metabolite could not be distinguished by the assay which was employed in the study. The initial burst, followed by the rapid decline to a steady-state level, was similar to the release pattern seen with the monthly formulation.Distribution: The mean steady-state volume of distribution of leuprolide following intravenous bolus administration to healthy male volunteers was 27 L. In vitro binding to human plasma proteins ranged from 43% to 49%.Metabolism: In healthy male volunteers, a 1 mg bolus of leuprolide administered intravenously, revealed that the mean systemic clearance was 7.6 L/h, with a terminal elimination half-life of approximately 3 hours based on a two compartment model. In rats and dogs, administration of 14C-labeled leuprolide was shown to be metabolized to smaller inactive peptides, a pentapeptide (Metabolite I), tripeptides (Metabolites II and lIl) and a dipeptide (Metabolite IV). These fragments may be further catabolized.In a pharmacokinetic/pharmacodynamic study of endometriosis patients, intramuscular 11.25 mg LUPRON DEPOT (n=19) every 12 weeks or intramuscular 3.75 mg LUPRON DEPOT (n=15) every 4 weeks was administered for 24 weeks. There was no statistically significant difference between the 2 treatment groups in trough plasma concentrations of leuprolide or M-l collected from weeks 4 through 24. No accumulation of plasma leuprolide or M-l concentrations was observed with multiple dosing of either treatment group. There was also no statistically significant difference in changes of serum estradiol concentration from baseline between the 2 treatment groups.M-l plasma concentrations measured in 5 prostate cancer patients reached maximum concentration 2 to 6 hours after dosing and were approximately 6% of the peak parent drug concentration. One week after dosing, mean plasma M-l concentrations were approximately 20% of mean leuprolide concentrations.

60
Excretion: Following administration of LUPRON DEPOT 3.75 mg to 3 patients, less than 5% of the dose was recovered as parent and M-l metabolite in the urine.Special Populations: The pharmacokinetics of the drug in hepatically and renally impaired patients have not been determined.Drug Interactions: No pharmacokinetic-based drug-drug interaction studies have been conducted with LUPRON DEPOT. However, because leuprolide acetate is a peptide that is primarily degraded by peptidase and not by cytochrome P-450 enzymes as noted in specific studies, and the drug is only about 46% bound to plasma proteins, drug interactions would not be expected to occur.Clinical StudiesIn a pharmacokinetic/pharmacodynamic study of healthy female subjects (N=20), the onset of estradiol suppression was observed for individual subjects between day 4 and week 4 after dosing. By the third week following the injection, the mean estradiol concentration (8 pg/mL) was in the menopausal range. Throughout the remainder of the dosing period, mean serum estradiol levels ranged from the menopausal to the early follicular range.Serum estradiol was suppressed to ≤ 20 pg/mL in all subjects within four weeks and remained suppressed (≤ 40 pg/mL) in 80% of subjects until the end of the 12-week dosing interval, at which time two of those subjects had a value between 40 and 50 pg/mL. Four additional subjects had at least two consecutive elevations of estradiol (range 43-240 pg/mL) levels during the 12-week dosing interval, but there was no indication of luteal function for any of the subjects during this period.LUPRON DEPOT-3 Month 11.25 mg induced amenorrhea in 85% (N=17) of subjects during the initial month and 100% during the second month following the injection. All subjects remained amenorrheic through the remainder of the 12-week dosing interval. Episodes of light bleeding and spotting were reported by a majority of subjects during the first month after the injection and in a few subjects at later time-points. Menses resumed on average 12 weeks (range 2.9 to 20.4 weeks) following the end of the 12-week dosing interval.LUPRON DEPOT-3 Month 11.25 mg produced similar pharmacodynamic effects in terms of hormonal and menstrual suppression to those achieved with monthly injections of LUPRON DEPOT 3.75 mg during the controlled clinical trials for the management of endometriosis and the anemia caused by uterine fibroids.Endometriosis: In a Phase IV pharmacokinetic/pharmacodynamic study of patients, LUPRON DEPOT-3 Month 11.25 mg (N=21) was shown to be comparable to monthly LUPRON DEPOT 3.75 mg (N=20) in relieving the clinical signs/symptoms of endometriosis (dysmenorrhea, nonmenstrual pelvic pain, pelvic tenderness and pelvic induration).
LUPRON 11,25 Figure 2. Percent of patients with signs/symptoms of endometriosis at baseline, final treatment visit and after 6 and 12 months of follow-upIn both treatment groups, suppression of menses was achieved in 100% of the patients who remained in the study for at least 60 days. Suppression is defined as no new menses for at least 60 consecutive days.In controlled clinical studies, LUPRON DEPOT 3.75 mg monthly for six months was shown to be comparable to danazol 800 mg/day in relieving the clinical sign/symptoms of endometriosis (pelvic pain, dysmenorrhea, dyspareunia, pelvic tenderness, and induration) and in reducing the size of endometrial implants as evidenced by laparoscopy.The clinical signficance of a decrease in endometriotic lesions is not known at this time, and in addition laparoscopic staging of endometriosis does not necessarily correlate with the severity of symptoms.LUPRON DEPOT 3.75 mg monthly induced amenorrhea in 74% and 98% of the patients after the first and second treatment months respectively. Most of the remaining patients reported episodes of only light bleeding or spotting. In the first, second and third post-treatment months, normal menstrual cycles resumed in 7%, 71% and 95% respectively, of those patients who did not become pregnant. Figure 2 illustrates the percent of patients with symptoms at baseline, final treatment visit and sustained relief at six and 12 months following discontinuation of treatment for the various symptoms evaluated during the two controlled clinical studies. A total of 166 patients received LUPRON DEPOT 3.75 mg. Seventy-five percent (N=125) of these elected to participate in the follow-up periods. Of these patients, 36% and 24% are included in the six month and 12 month follow-up analysis, respectively. All the patients who had a pain evaluation at baseline and at minimum of one treatment visit, are included in the Baseline (B) and final treatment visit (F) analysis.Hormonal replacement therapy: Clinical studies suggest that the addition of hormonal replacement therapy (estrogen and/or progestin) to LUPRON is effective in reducing loss of bone mineral density which occurs with LUPRON, without compromising the efficacy of LUPRON in relieving symptoms of endometriosis. The optimal drug/dose is not established.Uterine Leiomyomata (Fibroids): LUPRON DEPOT 3.75 mg for a period of three to six months was studied in four controlled clinical trials. In one of these clinical studies, enrollment was based on hematocrit ≤ 30% and/or hemoglobin ≤10.2 g/dL.

61
Administration of LUPRON DEPOT 3.75 mg, concomitantly with iron, produced an increase of ≥6% hematocrit and ≥2g/dL hemoglobin in 77% of patients at three months of therapy. The mean change in hematocrit was 10.1% and the mean change in hemoglobin was 4.2 g/dL. Clinical response was judged to be a hematocrit of ≥36% and hemoglobin of ≥12 g/dL, thus allowing for autologous blood donation prior to surgery. At two and three months respectively, 71% and 75% of patients met this criterion (Table 1). These data suggest however, that some patients may benefit from iron alone or 1 to 2 months of LUPRON DEPOT 3.75 mg. (See Table 1)LUPRON DEPOT 11.25 Table 1: Percent of patients achieving Hematocrit ≥36% and haemoglobin ≥ 12 gm/mlTreatment Group Week 4 Week 8 Week 12
LUPRON DEPOT 3.75 mg
with Iron (N=104) 40* 71** 75**Iron Alone (N=98) 17 39 49* p-Value < 0.01** p-Value < 0.001Excessive vaginal bleeding (menorrhagia or menometrorrhagia) decreased in 80% of patients at three months.Episodes of spotting and menstrual-like bleeding were noted in 16% of patients at final visit.25% was seen in uterine and myoma volumes in 60% and 54% of patients respectively. The mean fibroid diameter was 6.3 cm at pretreatment and decreased to 5.6 cm at the end of treatment. LUPRON DEPOT 3.75 mg was found to relieve symptoms of bloating, pelvic pain, and pressure. ≥ In this same study, a decrease ofIn the other controlled clinical trials, enrollment was not based on hematologic status. Mean uterine volume decrease by 41% and myoma volume decreased by 37% at final visit as evidenced by ultrasound or MRI. The mean fibroid diameter was 5.6 cm at pretreatment and decreased to 4.7 cm at the end of treatment. These patients also experienced a decrease in symptoms including excessive vaginal bleeding and pelvic discomfort. Ninety-five percent of these patients became amenorrheic with 61%, 25%, and 4% experiencing amenorrehea during the first, second, and third treatment months respectively.In addition, post treatment follow-up was carried out in one clinical trial for a small percentage of LUPRON DEPOT 3.75 mg patients (N=46) among the 77% who demonstrated a ≥ 25% decrease in uterine volume while on therapy.Menses usually returned within two months of cessation of therapy. Mean time to return to pretreatment uterine size was 8.3 months. Regrowth did not appear to be related to pretreatment uterine volume.There is no evidence that pregnancy rates are enhanced or adversely affected by the use of LUPRON DEPOT.IndicationsEndometriosis: LUPRON DEPOT-3 Month 11.25 mg is indicated for management of endometriosis, including pain relief and reduction of endometriotic lesions. Experience with LUPRON DEPOT in females has been limited to women 18 years of age and older treated for no more than 6 months.Uterine Leiomyomata (Fibroids): LUPRON DEPOT-3 Month 11.25 mg concomitantly with iron therapy is indicated for the preoperative hematologic improvement of patients with anemia caused by uterine leiomyomata. The clinician may wish to consider a one-month trial period on iron alone in as much as some of the patients will respond to iron alone (see Table 1, Clinical Studies section). LUPRON may be added if the response to iron alone is considered inadequate. Recommended therapy is a single injection of LUPRON DEPOT-3 Month 11.25 mg. This dosage form is indicated only for women for whom three months of hormonal suppression is deemed necessary.Experience with LUPRON DEPOT in females has been limited to women 18 years of age and older treated for no more than 6 months.ContraindicationsHypersensitivity to GnRH, GnRH agonist analogs or any of the excipients in LUPRON DEPOT. A report of an anaphylactic reaction to synthetic GnRH (Factrel) has been reported in the medical literature.1LUPRON DEPOT is contraindicated in women who are or may become pregnant while receiving the drug. LUPRON DEPOT may cause fetal harm when administered to a pregnant woman. Major fetal abnormalities were observed in rabbits but not in rats after administration of LUPRON DEPOT throughout gestation. There was increased fetal mortality and decreased fetal weights in rats and rabbits (see Pregnancy and Lactation section). The effects on fetal mortality are expected consequences of the alterations in hormonal levels brought about by the drug. If this drug is used during pregnancy or if the patient becomes pregnant while taking this drug, she should be apprised of the potential hazard to the fetus.Use in women who are breast feeding (see Pregnancy and Lactation section).Undiagnosed abnormal vaginal bleeding.Side EffectsThe monthly formulation of LUPRON DEPOT 11.25 mg was utilized in controlled clinical trials that studied the drug in 166 endometriosis and 166 uterine fibroids patients. Adverse events reported in ≥ 5% of patients in either of these populations and thought to be potentially related to drug are noted in the following table. (See Table 2).LUPRON DEPOT 11,25 Table 2: Adverse Events Reported to be Causally Related to Drug ≥ 5% of Patients
Endometriosis (2 Studies) Uterine Fibroids (4 Studies)LUPRON DEPOT Danazol Placebo LUPRON DEPOT Placebo3.75 mg N=136 N=31 3.75 mg N=163N=166 N (%) N (%) N=166 N (%)
N (%) N (%)
Body as a WholeAsthenia 5 (3) 9 (7) 0 (0) 14 (8.4) 8 (4.9)General Pain 31 (19) 22 (16) 1 (3) 14 (8.4) 10 (6.1)Headache* 53 (32) 30 (22) 2 (6) 43 (25.9) 29 (17.8)Cardiovascular SystemHot flashes/sweats* 139 (84) 77 (57) 9 (29) 121 (72.9) 29 (17.8)Gastrointestinal SystemNausea/vomiting 21 (13) 17 (13) 1 (3) 8 (4.8) 6 (3.7)GI disturbances* 11 (7) 8 (6) 1 (3) 5 (3.0) 2 (1.2)Metabolic and Nutritional DisordersEdema 12 (7) 17 (13) 1 (3) 9 (5.4) 2 (1.2)Weight gain/loss 22 (13) 36 (26) 0 (0) 5 (3.0) 2 (1.2)Endocrine System

62
Acne 17 (10) 27 (20) 0 (0) 0 (0) 0 (0)Hirsutism 2 (1) 9 (7) 1 (3) 1 (0.6) 0 (0)Musculoskeletal SystemJoint disorder* 14 (8) 11 (8) 0 (0) 13 (7.8) 5 (3.1)Myalgia* 1 (1) 7 (5) 0 (0) 1 (0.6) 0 (0)Nervous SystemDecreased libido* 19 (11) 6 (4) 0 (0) 3 (1.8) 0 (0)Depression/emotinal lability* 36 (22) 27 (20) 1 (3) 18 (10.8) 7 (4.3)Dizziness 19 (11) 4 (3) 0 (0) 3 (1.8) 6 (3.7)Nervousness* 8 (5) 11 (8) 0 (0) 8 (4.8) 1 (0.6)Neuromuscular disorders* 11 (7) 17 (13) 0 (0) 3 (1.8) 0 (0)Paresthesias 12 (7) 11 (8) 0 (0) 2 (1.2) 1 (0.6)Skin and AppendagesSkin reactions 17 (10) 20 (15) 1 (3) 5 (3) 2 (1.2)Urogenital SystemBreast changes /tenderness/pain* 10 (6) 12 (9) 0 (0) 3 (1.8) 7 (4.3)Vaginitis* 46 (28) 23 (17) 0 (0) 19 (11.4) 3 (1.8)In these same studies, symptoms reported in < 5% of patients included: Body as a Whole - Body odor, Flu syndrome, Injection site reactions; Cardiovascular System - Palpitations, Syncope, Tachycardia; Digestive System - Appetite changes, Dry mouth, Thirst; Endocrine System - Androgen-like effects; Hemic and Lymphatic Systems - Ecchymosis, Lymphadenopathy; Nervous System - Anxiety,* Insomnia/Sleep disorders,* Delusions, Memory disorder, Personality disorder; Respiratory System - Rhinitis; Skin and Appendages - Alopecia, Hair disorder, Nail disorder; Special Senses - Conjunctivitis, Ophthalmologic disorders,* Taste perversion; Urogenital System - Dysuria,* Lactation, Menstrual disorders.* = Physiologic effect of the drug.In one controlled clinical trial utilizing the monthly formulation of LUPRON DEPOT, patients diagnosed with uterine fibroids received a higher dose (7.5 mg) of LUPRON DEPOT. Events seen with this dose that were thought to be potentially related to drug and were not seen at the lower dose included glossitis, hypesthesia, lactation, pyelonephritis, and urinary disorders. Generally, a higher incidence of hypoestrogenic effects was observed at the higher dose. In a pharmacokinetic trial involving 20 healthy female subjects receiving LUPRON DEPOT-3 Month 11.25 mg, a few adverse events were reported with this formulation that were not reported previously. These included face edema, agitation, laryngitis, and ear pain. In a Phase IV study involving endometriosis patients receiving LUPRON DEPOT 3.75 mg (N=20) or LUPRON DEPOT-3 Month 11.25 mg (N=21), similar adverse events were reported by the two groups of patients. In general the safety profiles of the two formulations were comparable in this study.Changes in Bone Density:1% from baseline and showed statistically significantly (P-value²In controlled clinical studies, patients with endometriosis (six months of therapy) or uterine fibroids (three months of therapy) were treated with Leuprolide Depot 3.75 mg. In endometriosis patients, vertebral bone density as measured by dual energy x-ray absorptiometry (DEXA) decreased by an average of 3.2% at six months compared with the pretreatment value. In this same study, LUPRON DEPOT 3.75 mg alone and LUPRON DEPOT 3.75 mg plus three different hormonal add-back regimens were compared for one year. All add-back groups demonstrated mean changes in bone mineral density of <0.001) less loss of bone density than the group treated with LUPRON DEPOT 3.75 mg alone, at all time points. Clinical studies suggest that the addition of hormonal replacement therapy (estrogen and/or progestin) to LUPRON is effective in reducing loss of bone mineral density which occurs with LUPRON, without compromising the efficacy of LUPRON in relieving symptoms of endometriosis. The optimal drug/dose is not established. In the Phase IV, six-month pharmacokinetic/pharmacodynamic study in endometriosis patients who were treated with LUPRON DEPOT 3.75 mg or LUPRON DEPOT-3 Month 11.25 mg, vertebral bone density measured by DEXA decreased compared with baseline by an average of 3.0% and 2.8% at six months for the two groups, respectively.When LUPRON DEPOT 3.75 mg was administered for three months in uterine fibroid patients, vertebral trabecular bone mineral density as assessed by quantitative digital radiography (QDR) revealed a mean decrease of 2.7% compared with baseline. Six months after discontinuation of therapy, a trend toward recovery was observed. Use of LUPRON DEPOT for longer than three months (uterine fibroids) or six months (endometriosis) or in the presence of other known risk factors for decreased bone mineral content may cause additional bone loss and is not recommended.Changes in Laboratory Values During Treatment:Liver EnzymesThree percent of uterine fibroid patients treated with LUPRON DEPOT 3.75 mg, manifested posttreatment transaminase values that were at least twice the baseline value and above the upper limit of the normal range. None of the laboratory increases were associated with clinical symptoms.LipidsTriglycerides were increased above the upper limit of normal in 12% of the endometriosis patients who received LUPRON DEPOT 3.75 mg and in 32% of the subjects receiving LUPRON DEPOT-3 Month 11.25 mg.Of those endometriosis and uterine fibroid patients whose pretreatment cholesterol values were in the normal range, mean change following therapy was +16 mg/dL to +17 mg/dL in endometriosis patients and +11 mg/dL to +29 mg/dL in uterine fibroid patients. In the endometriosis treated patients, increases from the pretreatment values were statistically significant (p<0.03). There was essentially no increase in the LDL/HDL ratio in patients from either population receiving LUPRON DEPOT 3.75 mg.ChemistrySlight to moderate mean increases were noted for glucose, uric acid, BUN, creatinine, total protein, albumin, bilirubin, alkaline phosphatase, LDH, calcium, and phosphorus. None of these increases were clinically significant.Postmarketing:During postmarketing surveillance with other dosage forms and in the same and/or different populations, the following adverse events were reported. Like other drugs in this class, mood swings, including depression, have been reported as a physiologic effect of decreased sex steroids. There have been very rare reports of suicidal ideation and attempt. Many, but not all, of these patients had a history of depression or other psychiatric illness. Patients should be counseled on the possibiiity of worsening of depression.Symptoms consistent with an anaphylactoid or asthmatic process have been reported. Rash, urticaria, and photosensitivity reactions have also been reported.Localized reactions including induration and abscess have been reported at the site of injection.Symptoms consistent with fibromyalgia (eg: joint and muscle pain, headaches, sleep disorders, gastrointestinal distress, and shortness of breath) have been reported individually and collectively.Cardiovascular System - Hypotension, Pulmonary embolism Hemic and Lymphatic System - Decreased WBC. Central/Peripheral Nervous System - Peripheral neuropathy, Spinal fracture/paralysis; Musculoskeletal System - Tenosynovitis-like symptoms; Urogenital System - Prostate pain.

63
See other LUPRON DEPOT and LUPRON Injection package inserts for other events reported in the same and different patient populations.PrecautionsAs the effects of LUPRON DEPOT-3Month 11.25 mg are present throughout the course of therapy, the drug should only be used in patients who require hormonal suppression for at least three months.Experience with LUPRON DEPOT in females has been limited to six months; therefore, exposure should be limited to six months of therapy.When used at the recommended dose and dosing interval, LUPRON DEPOT usually inhibits ovulation and stops menstruation. Contraception is not insured, however, by taking LUPRON DEPOT. Therefore, patients should use nonhormonal methods of contraception. Patients should be advised to see their physician if they believe they may be pregnant. If a patient becomes pregnant during treatment. The drug must be discontinued and the patient must be apprised of the potential risk to the fetus (see Contraindications section).During the early phase of therapy, sex steroids temporarily rise above baseline because of the physiologic effect of the drug. Therefore, an increase in clinical signs and symptoms may be observed during the initial days of therapy, but these will dissipate with continued therapy.Information for Patients: Patients should be aware of the following information:Since menstruation should stop with effective doses of LUPRON DEPOT, the patient should notify her physician if regular menstruation persists. Patients missing successive doses of LUPRON DEPOT may experience breakthrough bleeding.Patients should not use LUPRON DEPOT if they are pregnant, breast feeding, have undiagnosed abnormal vaginal bleeding, or are allergic to any of the ingredients in LUPRON DEPOT.LUPRON DEPOT is contraindicated for use during pregnancy. Therefore, a nonhormonal method of contraception should be used during treatment. Patients should be advised that if they miss successive doses of LUPRON DEPOT, breakthrough bleeding or ovulation may occur with the potential for conception. If a patient becomes pregnant during treatment, she should discontinue treatment and consult her physician.Adverse events occurring in clinical studies with LUPRON DEPOT that are associated with hypoestrogenism include: hot flashes, headaches, emotional lability, decreased libido, acne, myalgia, reduction in breast size, and vaginal dryness. Estrogen levels returned to normal after treatment was discontinued.The induced hypoestrogenic state also results in a small loss in bone density over the course of treatment, which may not be fully reversible. In patients with major risk factors for decreased bone mineral content such as chronic alcohol and/or tobacco use, strong family history of osteoporosis, or chronic use of drugs that can reduce bone mass such as anticonvulsants or corticosteroids, LUPRON DEPOT therapy may pose an additional risk. In those patients, the risks and benefits must be weighed carefully before therapy with LUPRON DEPOT is instituted. Clinical studies suggest that the addition of hormonal replacement therapy (estrogen and/or progestin) to LUPRON is effective in reducing loss of bone mineral density which occurs with LUPRON, without compromising the efficacy of LUPRON in relieving symptoms of endometriosis. The optimal drug/dose is not established.Treatment for more than six months cannot be recommended since safety data beyond six months are not available.
Drug Interactions Drug/Laboratory Test Interactions: Administration of LUPRON DEPOT in therapeutic doses results in suppression of the pituitary-gonadal system. Normal function is usually restored within three months after treatment is discontinued. Due to the suppression of the pituitary-gonadal system by LUPRON DEPOT, diagnostic tests of pituitary gonadotropic and gonadal functions conducted during treatment and for up to three months after discontinuation of LUPRON DEPOT may be affected.Carcinogenesis, Mutagenesis, Impairment of Fertility: A two-year carcinogenicity study was conducted in rats and mice. In rats, a dose-related increase of benign pituitary hyperplasia and benign pituitary adenomas was noted at 24 months when the drug was administered subcutaneously at high daily doses (0.6 to 4 mg/kg). There was a significant but not dose-related increase of pancreatic islet-cell adenomas in females and of testicular interstitial cell adenomas in males (highest incidence in the low dose group). In mice, no leuprolide acetate-induced tumors or pituitary abnormalities were observed at a dose as high as 60 mg/kg for two years. Patients have been treated with leuprolide acetate for up to three years with doses as high as 10 mg/day and for two years with doses as high as 20 mg/day without demonstrable pituitary abnormalities.Mutagenicity studies have been performed with leuprolide acetate using bacterial and mammalian systems. These studies provided no evidence of a mutagenic potential.Clinical and pharmacologic studies in adults (> 18 years) with leuprolide acetate and similar analogs have shown reversibility of fertility suppression when the drug is discontinued after continuous administration for periods of up to 24 weeks.Pregnancy and LactationPregnancy, Teratogenic Effects: Pregnancy Category X. (See Contraindications section.) When administered on day 6 of pregnancy at test dosages of 0.00024, 0.0024, and 0.024 mg/kg (1/300 to 1/3 the human dose) to rabbits, LUPRON DEPOT produced a dose-related increase in major fetal abnormalities. Similar studies in rats failed to demonstrate an increase in fetal malformations. There was increased fetal mortality and decreased fetal weights with the two higher doses of LUPRON DEPOT in rabbits and with the highest dose (0.024 mg/kg) in rats.Nursing Mothers: It is not known whether LUPRON DEPOT is excreted in human milk. Because many drugs are excreted in human milk, and because the effects of LUPRON DEPOT on lactation and/or the breast-fed child have not been determined, LUPRON DEPOT should not be used by nursing mothers.Pediatric Use: Safety and effectiveness of LUPRON DEPOT- 3 Month 11.25 mg have not been established in pediatric patients. See LUPRON DEPOT-PED® (leuprolide acetate for depot suspension) labeling for the safety and effectiveness in children with central precocious puberty.OverdosageIn clinical trials using daily subcutaneous leuprolide acetate in patients with prostate cancer, doses as high as 20 mg/day for up to two years caused no adverse effects differing from those observed with the 1 mg/day dose.StorageThe shelf life for this product is 36 months unopened. No refrigeration is necessary, store at room temperature, not exceeding 25°C. Once reconstituted with the sterile diluent, the suspension should be administered immediately. However, the suspension is considered stable for up to 24 hours at 25°C. Protect from light.Dosage AdministrationLUPRON DEPOT Must Be Administered Under the Supervision of a Physician.Endometriosis: The recommended dose of LUPRON DEPOT- 3 Month 11.25 mg is one injection every three months, for a maximum recommended duration of six months. Retreatment cannot be recommended since safety data for retreatment are not available. If the symptoms of endometriosis recur after a course of therapy, and further treatment with LUPRON DEPOT-3 Month 11.25 mg is contemplated, it is recommended that bone density be assessed before retreatment begins to ensure that values are within normal limits.Uterine Leiomyomata (Fibroids): The recommended dose of LUPRON DEPOT-3 Month 11.25 mg is one injection. The symptoms associated with uterine leiomyomata will recur following discontinuation of therapy. If additional treatment with LUPRON DEPOT-3 Month 11.25 mg is contemplated, bone density should be assessed prior to initiation of therapy to ensure that values are within normal limits.Reconstitution:

64
The vial of Leuprolide Acetate Depot Suspension - 3 Month 11.25 mg should be reconstituted immediately prior to administration and administered every three months as a single subcutaneous or intramuscular injection in accordance with the following directions:Using a syringe with a 23 gauge needle, withdraw two mL of diluent from the ampule, and inject it into the vial of leuprolide acetate depot suspension using aseptic technique.Shake well to thoroughly disperse particles to obtain a uniform suspension. The suspension will appear milky.Withdraw the entire contents of the vial into the syringe and inject it at the time of reconstitution. Although the solution has been shown to be stable for 24 hours following reconstitution, since the product does not contain a preservative, the suspension should be discarded if not used immediately.No other fluid should be used for reconstitution of leuprolide acetate depot suspension 3-month 11.25 mg powder.HOW SUPPLIEDLUPRON DEPOT-3 Month 11.25 mg is available in a single dose administration kit. Each kit contains one vial of sterile Iyophilized microspheres of leuprolide acetate incorporated in a biodegradable polymer of polylactic acid; one ampule of diluent; one syringe; two 23 gauge needle and one alcohol wipe.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
LUPRON DEPOT 22.5 MG ®GeneralLeuprolide Acetate for Depot SuspensionCompositionLeuprolide acetate is a synthetic nonapeptide analog of naturally occurring gonadotrophin releasing hormone (GnRH or LHRH). The analogue possesses greater potency than the natural hormone.The chemical name is 5-oxo-L-prolyl-L-histidyl-L-tryptophyl- L-seryl-L-tyrosyl-D-leucyl-L-leucyl-L-arginyl-Nethyl- L-prolinamide acetate (salt) with the following structural formula: (see Figure 1).LUPRON DEPOT-3 Month 22.5 mg is a formulation of leuprolide acetate supplied in a vial containing sterile Iyophilized microspheres. When mixed with diluent, it becomes a suspension which is administered as a single intramuscular injection every three months.
Lupron Depot 22.5 Figure 1. Structural formulaActive/lnactive Ingredients:The single-dose vial of LUPRON DEPOT-3 Month 22.5 mg contains leuprolide acetate (22.5 mg), polylactic acid (198.6 mg) and D-Mannitol (38.9 mg). The accompanying ampule of diluent contains carboxymethylcellulose sodium (10 mg), D-mannitol (100 mg), polysorbate 80 (2 mg), water for injection (2 mL), and glacial acetic acid to control pH. During the manufacture of LUPRON DEPOT-3 Month 22.5 mg, acetic acid is lost leaving the peptide.PropertiesClinical PharmacologyLeuprolide acetate, an LH-RH agonist, acts as a potent inhibitor of gonadotropin secretion when given continuously and in therapeutic doses. Animal and human studies indicate that following an initial stimulation, chronic administration of leuprolide acetate results in suppression of ovarian and testicular steroidogenesis. This effect is reversible on discontinuation of drug therapy. Administration of leuprolide acetate has resulted in inhibition of the growth of certain hormone dependent tumors (prostatic tumors in Noble and Dunning male rats and DMBA-induced mammary tumors in female rats), as well as atrophy of the reproductive organs.In humans, administration of leuprolide acetate results in an initial increase in circulating levels of luteinizing hormone (LH) and follicle stimulating hormone (FSH), leading to a transient increase in levels of the gonadal steroids (testosterone and dihydrotestosterone in males, and estrone and estradiol in premenopausal females). However, continuous administration of leuprolide acetate results in decreased levels of LH and FSH. In males, testosterone is reduced to castrate levels. In premenopausal females, estrogens are reduced to postmenopausal levels. These decreases occur within two to four weeks after initiation of treatment, and castrate levels of testosterone in prostatic cancer patients have been demonstrated for more than five years.Leuprolide acetate is not active when given orally.PharmacokineticsAbsorption:Following a single injection of the three month formulation of LUPRON DEPOT-3 Month 22.5 mg in patients, mean peak plasma leuprolide concentration of 48.9 ng/mL was observed at 4 hours and then declined to 0.67 ng/mL at 12 weeks. Leuprolide appeared to be released at a constant rate following the onset of steady-state levels during the third week after dosing, providing steady plasma concentrations through the 12-week dosing interval. However, intact leuprolide and an inactive major metabolite could not be distinguished by the assay which was employed in the study. Detectable levels of leuprolide were present at all measurement points in all patients. The initial burst, followed by the rapid decline to a steady-state level, was similar to the release pattern seen with the monthly formulation.

65
Distribution:The mean steady-state volume of distribution of leuprolide following intravenous bolus administration to healthy male volunteers was 27 L. In vitro binding to human plasma proteins ranged from 43% to 49%.Metabolism:In healthy male volunteers, a 1 mg bolus of leuprolide administered intravenously revealed that the mean systemic clearance was 7.6 L/h, with a terminal elimination half-life of approximately 3 hours based on a two compartment model.In rats and dogs, administration of 14C-labeled leuprolide was shown to be metabolized to smaller inactive peptides, a pentapeptide (Metabolite I), tripeptides (Metabolites II and III) and dipeptide (Metabolite IV). These fragments may be further catabolized.The major metabolite (M-l) plasma concentrations measured in 5 prostate cancer patients reached maximum concentration 2 to 6 hours after dosing and were approximately 6% of the peak parent drug concentration. One week after dosing, mean plasma M-l concentrations were approximately 20% of mean leuprolide concentrations.Excretion:Following administration of LUPRON DEPOT 3.75 mg to 3 patients, less than 5% of the dose was recovered as parent and M-l metabolite in the urine.Special Populations:The pharmacokinetics of the drug in hepatically and renally impaired patients have not been determined.Clinical StudiesIn clinical studies, serum testosterone was suppressed to castrate levels within 30 days in 87 of 92 (95%) patients and within an additional two weeks in three patients. Two patients did not suppress for 15 and 28 weeks. respectively. Suppression was maintained in all of these patients with the exception of transient minimal testosterone elevations in one of them, and in another an increase in serum testosterone to above the castrate range was recorded during the 12 hour observation period after a subsequent injection. This represents stimulation of gonadotropin secretion.3.99 ng/mL) in 63% of the patients.²90% was reported in 71% of the patients and a change to within the normal range (³An 85% rate of “no progression” was achieved during the initial 24 weeks of treatment. A decrease from baseline in serum PSA ofPeriodic monitoring of serum testosterone and PSA levels is recommended, especially if the anticipated clinical or biochemical response to treatment has not been achieved. It should be noted that results of testosterone determinations are dependent on assay methodology. It is advisable to be aware of the type and precision of the assay methodology to make appropriate clinical and therapeutic decisions.IndicationsLUPRON DEPOT-3 Month 22.5 mg is indicated in the palliative treatment of advanced prostatic cancer. It offers an alternative treatment of prostatic cancer when orchiectomy or estrogen administration are either not indicated or unacceptable to the patient. In clinical trials, the safety and efficacy of LUPRON DEPOT-3 Month 22.5 mg were similar to that of the original daily subcutaneous injection and the monthly depot formulation.ContraindicationsA report of an anaphylactic reaction to synthetic GnRH (Factrel) has been reported in the medical literature. LUPRON DEPOT is contraindicated in women who are, or may become pregnant while receiving the drug.When administered on day 6 of pregnancy at test dosages of 0.00024, 0.0024 and 0.024 mg/kg (1/600 to 1/6 of the human dose) to rabbits, the monthly formulation of LUPRON DEPOT produced a dose-related increase in major fetal abnormalities. Similar studies in rats failed to demonstrate an increase in fetal malformations. There was increased fetal mortality and decreased fetal weights with the two higher doses of the monthly formulation of LUPRON DEPOT in rabbits and with the highest dose in rats. The effects on fetal mortality are logical consequences of the alterations in hormonal levels brought about by this drug. Therefore, the possibility exists that spontaneous abortion may occur if the drug is administered during pregnancy.Side EffectsIn the majority of patients testosterone levels increased above baseline during the first week, declining thereafter to baseline levels or below by the end of the second week of treatment. Potential exacerbations of signs and symptoms during the first few weeks of treatment is a concern in patients with vertebral metastases and/or urinary obstruction or hematuria which, if aggravated, may lead to neurological problems such as temporary weakness and/or paresthesia of the lower limbs or worsening of urinary symptoms (see WARNINGS section).In two clinical trials of LUPRON DEPOT-3 Month 22.5 mg, the following adverse reactions were reported to have a possible or probable relationship to drug as ascribed by the treating physician in 5% or more of the patients receiving the drug. Often, causality is difficult to assess in patients with metastatic prostate cancer.Reactions considered not drug-related are excluded. (See Table 1).LUPRON DEPOT 22.5 Table 1. Side EffectsLUPRON DEPOT-3 Month 22.5 mg
N=94 (Percent)
Body As a WholeAsthenia 7 ( 7.4%)General Pain 25 (26.6%)Headache 6 (6.4%)Injection Site Reaction 13 (13.8%)Cardiovascular SystemHot flashes/Sweats* 55 (58.5%)Digestive SystemGl Disorders 15 (16.0%)Musculoskeletal SystemJoint Disorders 11 (11.7%)Central/Peripheral Nervous SystemDizziness/Vertigo 6 (6.4%)Insomnia/Sleep Disorders 8 (8.5%)Neuromuscular Disorders 9 (9.6%)Respiratory SystemRespiratory Disorders 6 (6.4%)Skin and AppendagesSkin Reaction 8 (8.5%)Urogenital System

66
Testicular Atrophy* 19 (20.2%)Urinary Disorders 14 (14.9%)In these same studies, the following adverse reactions were reported in less than 5% of the patients on LUPRON DEPOT-3 Month 22.5 mg.Body As A Whole - Enlarged abdomen, Fever; Cardiovascular System - Arrhythmia, Bradycardia, Heart failure, Hypertension, Hypotension, Varicose vein; Digestive System - Anorexia, Duodenal ulcer, Increased appetite, Thirst/dry mouth; Hemic and Lymphatic System - Anemia, Lymphedema; Metabolic and Nutritional Disorders - Dehydration, Edema; Central/Peripheral Nervous System - Anxiety, Delusions, Depression, Hypesthesia, Libido decreased*, Nervousness, Paresthesia; Respiratory System - Epistaxis, Pharyngitis, Pleural effusion, Pneumonia; Special Senses - Abnormal vision, Amblyopia, Dry eyes, Tinnitus; Urogenital System - Gynecomastia, Impotence*, Penis disorders, Testis disorders.Laboratory:Abnormalities of certain parameters were observed, but are difficult to assess in this population. The following were recorded in 5% of patients: Increased BUN, Hyperglycemia, Hyperlipidemia (total cholesterol, LDL-cholesterol, triglycerides), Hyperphosphatemia, Abnormal liver function tests, Increased PT, Increased PTT. Additional laboratory abnormalities reported were:Decreased platelets, Decreased potassium and Increased WBC.* Physiologic effect of decreased testosteronePost-Marketing:During postmarketing surveillance, which includes other dosage forms, the following adverse events were reported.Symptoms consistent with an anaphylactoid or asthmatic process have been rarely reported. Rash, urticaria, and photosensitivity reactions have also been reported.Localized reactions including induration and abscess have been reported at the site of injection.Hemic and Lymphatic System - Decreased WBC; Central/Peripheral Nervous System - Peripheral neuropathy, Spinal fracture/paralysis: Musculoskeletal System - Tenosynovitis-like symptoms; Urogenital System - Prostate pain.See other LUPRON DEPOT and LUPRON Injection package inserts for other events reported in different patient populations.PrecautionsIsolated cases of worsening of signs and symptoms during the first weeks of treatment have been reported with LH-RH analogs. Worsening of symptoms may contribute to paralysis with or without fatal complications. For patients at risk, the physician may consider initiating therapy with daily LUPRON® (leuprolide acetate) Injection for the first two weeks to facilitate withdrawal of treatment if that is considered necessary.Patients with metastatic vertebral lesions and/or with urinary tract obstruction should be closely observed during the first few weeks of therapy (see Warnings section).Laboratory Tests:Response to LUPRON DEPOT-3 Month 22.5 mg should be monitored by measuring serum levels of testosterone, as well as prostate-specific antigen and prostatic acid phosphatase. In the majority of patients, testosterone levels increased above baseline during the first week, declining thereafter to baseline levels or below by the end of the second week of treatment. Castrate levels were reached within two to four weeks and once achieved were maintained for as long as the patients received their injections.Carcinogenesis, Mutagenesis, Impairment of Fertility:Two-year carcinogenicity study were conducted in rats and mice. In rats, a dose-related increase of benign pituitary hyperplasia and benign pituitary adenomas was noted at 24 months when the drug was administered subcutaneously at high daily doses (0.6 to 4 mg/kg). There was a significant but not dose related increase of pancreatic islet-cell adenomas in females and of testicular interstitial cell adenomas in males (highest incidence in the low dose group). In mice, no pituitary abnormalities were observed at a dose as high as 60 mg/kg for two years. Patients have been treated with leuprolide acetate for up to three years with doses as high as 10 mg/day and for two years with doses as high as 20 mg/day without demonstrable pituitary abnormalities.Mutagenicity studies have been performed with leuprolide acetate using bacterial and mammalian systems. These studies provided no evidence of a mutagenic potential.Clinical and pharmacologic studies in adults ( 18 years) with leuprolide acetate and similar analogs have shown reversibility of fertility suppression when the drug is discontinued after continuous administration for periods of up to 24 weeks.Pediatric Use:See LUPRON DEPOT-PED® (leuprolide acetate for depot suspension) labeling for the safety and effectiveness of the monthly formulation in children with central precocious puberty.Pregnancy and LactationPregnancy Category X: (See CONTRAINDICATIONS section.)OverdosageIn rats subcutaneous administration of 250 to 500 times the recommended human dose, expressed on a per body weight basis, resulted in dyspnea, decreased activity, and local irritation at the injection site. There is no evidence at present that there is a clinical counterpart of this phenomenon. In early clinical trials with daily subcutaneous leuprolide acetate, doses as high as 20 mg/day for up to two years caused no adverse effects differing from those observed with the 1 mg/day dose.Drug InteractionsNo pharmacokinetic-based drug-drug interaction studies have been conducted with LUPRON DEPOT. However, because leuprolide acetate is a peptide that is primarily degraded by peptidase and not by cytochrome P-450 enzymes as noted in specific studies, and the drug is only about 46% bound to plasma proteins, drug interactions would not be expected to occur.Drug/Laboratory Test Interactions:Administration of LUPRON DEPOT 3.75 mg in women results in suppression of the pituitary-gonadal system. Normal function is usually restored within three months after leuprolide acetate depot treatment is discontinued. Therefore, diagnostic tests of pituitary gonadotropic and gonadal functions conducted during treatment and up to three months after discontinuation of LUPRON DEPOT 3.75 mg therapy may be misleading.StorageThe vial of Leuprolide Acetate Depot Suspension - 3 Month and the ampule of diluent may be stored at room temperature not exceeding 25°C. No refrigeration necessary. Protect from freezing.Dosage AdministrationLUPRON DEPOT Must Be Administered Under The Supervision Of A Physician.The recommended dose of LUPRON DEPOT-3 Month 22.5 mg to be administered is one injection every three months (84 days). Due to different release characteristics, a fractional dose of this 3-month depot formulation is not equivalent to the same dose of the monthly formulation and should not be given.Reconstitution:Incorporated in a depot formulation the lyophilized microspheres are to be reconstituted and administered every three months as a single intramuscular injection, in accord with the following directions:1. Using a syringe with a 22 gauge needle, withdraw 1.5 mL of diluent from the ampule, and inject it into the vial. (Extra diluent is provided; any remaining should be discarded).

67
2. Shake well to thoroughly disperse particles to obtain a uniform suspension. The suspension will appear milky.3. Withdraw the entire contents of the vial into the syringe and inject it at the time of reconstitution. The suspension settles very quickly following reconstitution; therefore, it is preferable that LUPRON DEPOT-3 Month 22.5 mg be mixed and used immediately. Reshake suspension if settling occurs.Although the potency of the reconstituted suspension has been shown to be stable for 24 hours, since the product does not contain a preservative, the suspension should be discarded if not used immediately.As with other drugs administered by injection, the injection site should be varied periodically.PackagingLeuprolide Acetate Depot Suspension - 3 Month is available in a single dose kit. Each kit contains a vial of sterile Iyophilized microspheres which is leuprolide acetate incorporated in a biodegradable polymer of polylactic acid. When mixed with 1.5 mL of accompanying diluent, Leuprolide Acetate Depot Suspension - 3 Month is administered as a single l.M. injection every three months.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
ODRIK ®GeneralTRANDOLAPRILOdrik 0.5 mg, capsulesOdrik 1 mg, capsulesOdrik 2 mg, capsulesCompositionOdrik 0.5 mg: 1 capsule contains 0.5 mg of trandolaprilOdrik 1 mg: 1 capsule contains 1.0 mg of trandolaprilOdrik 2 mg: 1 capsule contains 2.0 mg of trandolaprilPropertiesCapsulesPharmacodynamic Trandolapril is an efficacious, non-sulphydryl, orally active angiotensin converting enzyme (ACE) inhibitor which exerts its action in the plasma and tissue, especially in the vascular system, heart and adrenals. After oral administration and absorption, trandolapril is primarily converted by hydrolysis into its active diacidic metabolite, trandolaprilat. ACE is a peptidyl-dipeptidase which catalyses the transformation of angiotensin I into vasoconstrictive angiotensin II and the degradation of bradykinin to inactive fragments. Low concentrations of trandolapril suffice to produce a potent inhibitory effect on ACE, thus preventing the formation of angiotensin II. Suppression of negative feedback causes a reduction in aldosterone secretion and an increase in plasma renin activity. Hence, trandolapril has an effect on the renin-angiotensin-aldosterone system which plays a decisive role in the regulation of blood volume and pressure. Other mechanisms of action which may be related to the vasodilatory activity of this ACE inhibitor include the inhibition of bradykinin degradation and prostaglandin release as well as an attenuation of sympathetic nervous system activity. The combination of these properties of trandolapril may be responsible for the regression of cardiac hypertrophy and improvement of vascular compliance observed in humans. In hypertensive patients trandolapril produces a reduction of the systolic and diastolic blood pressure. This antihypertensive efficacy is maintained, even when plasma renin levels are low. The decrease in peripheral resistance induced by trandolapril is not accompanied by either water or sodium retention nor by tachycardia. Trandolapril's antihypertensive effect sets in about one hour after dose administration, and peak efficacy is, as a rule, reached after 4 to 6 hours. The effect is sustained for at least 24 hours without affecting circadian blood pressure rhythm. Antihypertensive efficacy is maintained in long-term treatment without the development of tolerance. There is no rebound effect on discontinuation of treatment. Combination with a diuretic or a calcium channel blocker may potentiate the antihypertensive efficacy of trandolapril. No pharmacokinetic interactions have been observed with the following drug products: frusemide, digoxin, nifedipine, warfarin. No clinical interactions have been observed in myocardial infarction patients with left ventricular dysfunction receiving concomitant therapy with the following agents: thrombolytics, acetylsalicylic acid, beta blockers, nitrates, anticoagulants, diuretics, digoxin. In a placebo-controlled study on 1749 patients with left ventricular dysfunction (LVEF ≤ 35%) after myocardial infarction, trandolapril (when treatment was started between day 3 to day 7 after the infarction) significantly prolonged survival time (primary outcome criterion) and reduced cadiovascular morbidity. During treatment with trandolapril the incidence of sudden cardiac death decreased and the development of severe heart failure (secondary outcome criterion) was delayed as compared with placebo. Patients receiving trandolapril displayed fewer clinical symptoms of heart failure, such as, peripheral oedema, dyspnoea, orthopnoe and fatigue than patients receiving placebo.Pharmacokinetic Peak plasma levels (Cmax) are observed 30 minutes (Tmax) after administration of trandolapril. Trandolapril clears rapidly from the plasma. It has a half-life of less than one hour. The compound is converted by hydrolysis into trandolaprilat. The amount of trandolaprilat that results from this conversion is not affected by food intake. The peak plasma concentration of trandolaprilat is reached after 4 to 6 hours. More than 80% of trandolaprilat binds to plasma proteins. Binding is saturable with a high affinity to the converting enzyme. On repeated daily dosing of trandolapril, steady state is reached on average after four days in healthy volunteers as well as in young and elderly hypertensive patients and in patients with heart failure. The calculated effective cumulative half-life of trandolapril ranges from 16 to 24 hours. About 10 to 15% of the administered trandolapril dose is excreted as unchanged trandolaprilat with the urine. After oral administration of the labelled compound in man, 33% of the radioactivity is recovered in the urine and 66% in the feces. Patients at risk: Patients with renal failure: The renal clearance of trandolaprilat is proportional to creatinine clearance. In patients in whom creatinine clearance is 30 ml/min or below, trandolaprilat plasma concentrations are significantly higher. On repeated dosing in patients with chronic renal failure, however, steady state is reached after an average of four days, regardless of the severity of the renal failure.Patients with impaired liver function: In patients with impaired liver function, the reduction in metabolic clearance of both the parentcompound, trandolapril, and the active metabolite, trandolaprilat, leads to a marked increase in trandolapril plasma levels and, to a lesser extent, to an increase in the trandolaprilat concentrations. Therefore, treatment should start with a dose of 0.5 mg of trandolapril (equivalent to 1 capsule Odrik 0.5 mg) once daily under close monitoring by the physician.In view of the data provided above, patients with severe kidney failure (creatinin clearance below 30 ml/min) and/or severe liver function impairment should not be treated with trandolapril.Elderly patients: In a kinetics study on repeated dosing of trandolapril in hypertensive patients over 65 years of age whose renal function was in keeping with their age, it was found that no dose adjustment is necessary.Trandolapril is very rapidly absorbed after oral administration. The absorbed amount lies between 40 to 60 % of the administered dose and is not affected by food intake. Absolute bioavailability of the active metabolite trandolaprilat, administered in the form of trandolapril, is 13%.Indications- Essential hypertension- Left ventricular dysfunction after myocardial infarction in clinically stable patients with an ejection fraction of ≤ 35%ContraindicationsOdrik may not be used in patients with the following conditions: Hypersensitivity to trandolapril or any of its other ingredients, a history of angioneurotic edema (e.g. related to previous ACE inhibitor therapy), arteriostenosis of the kidneys (both right and left or one-sided in

68
patients with only one kidney), after kidney transplant, hemodynamically relevant aortic or mitral valve stenosis and/or hypertrophic cardiomyopathy, shock, systolic blood pressure < 100 mmHg, idiopathic hyperaldosteronism, pregnancy and breastfeedingSince experience in its use in the following conditions is insufficient to date, Odrik should not be administered in the following cases: Unstable angina pectoris, severe liver function impairment/liver cirrhosis with ascites, severe renal function impairment (creatinine clearance below 30 ml/min), dialysis, untreated, decompensated heart failure not resulting from myocardial infarction to children.Patients being treated with Odrik may not undergo dialysis or hemofiltration using poly (acrylonitrile sodium-2-methallylsulfonate) high flux membranes (e.g. “AN 69”). If dialysis or hemofiltration are required as emergency measures, the patient must either be switched to another antihypertensive agent - a non-ACE inhibitor - before the intervention or an alternative membrane must be used in the dialysis equipment. Life-threatening anaphylactoid reactions may occur in patients taking ACE inhibitors who are subjected to LDL (low density lipoprotein) apheresis using dextran sulphate. In patients undergoing desensitization therapy to insect venoms (e.g. bee or wasp stings) there may be life-threatening anaphylactoid reactions (such as, severe drop in blood pressure, respiratory distress, vomiting, allergic skin reactions) if ACE inhibitors are given simultaneously. Patients requiring LDL apheresis and/or desensitization therapy against insect venoms should be switched temporarily from the ACE inhibitor to an alternative medication.A very critical risk/benefit assessment should be made before prescribing Odrik to patients with the following conditions and their relevant clinical and lab parameters should be monitored at regular intervals: clinically relevant proteinuria ( more than 1 g/day) clinically relevant electrolyte disorders, impaired immune reaction or collagen vascular disease (such as, lupus erythematosus and scleroderma, simultaneous treatment with immunosuppressants (such as, steroids, cytostatics, antimetabolites), allopurinol, procainamide or lithium.Side EffectsThe following adverse reactions have been observed in patients being treated with Odrik or other ACE inhibitors: The classification of side effects is based on their rate of incidence as follows:Very common (≥1/10), Common (≥1/100 to ≤ 1/10), Uncommon (≥1/1.000 to ≤ 1/100), Rare (≥1/10.000 to ≤ 1/1.000),Very rare (≥1/10.000)CardiovascularOccasionally, especially at the onset of Odrik therapy and in patients with hyponatraemia and/or dehydration (e.g. previous treatment with diuretics), heart failure, severe hypertension, and also when increasing the dosage of Odrik and/or diuretics, there may be an excessive drop in blood pressure (hypotension, orthostatic hypotension) accompanied by symptoms such as dizziness, feeling weak, vision impairment and, rarely, fainting (syncope). There have been individual reports of the following side effects after taking ACE inhibitors accompanied by a sharp drop in blood pressure: tachycardia, bradycardia, palpitations, cardiac arrhythmias, angina pectoris, myocardial infarction, cardiac arrest, TIA and cerebrovascular accident. In cases where Odrik was administered within the first few days of an infarction, there have been rare reports of 2nd and 3rd degree AV block, marked hypotension and shock.RenalOccasionally, renal function disorders may occur or be aggravated, in some individuals there may even be acute kidney failure. Proteinuria has seldom been reported, in some cases this has been accompanied by a deterioration of kidney function. There have been isolated reports of non-bacterial interstitial nephritis after ACE inhibitors.Respiratory SystemThere have been occasional reports of dry cough and bronchitis; rarely, sore throat, respiratory distress, sinusitis, rhinitis, isolated bronchospasm, glossitis and dry mouth. Isolated cases of ACE inhibitors triggering angio-oedema affecting the larynx, pharynx and/or tongue have been reported (see Emergency measures section ). Isolated cases of alveolar inflammation (allergic alveolitis, eosinophilic pneumonia) have been observed for ACE inhibitors.GastrointestinalThere have been occasional reports of nausea, epigastric discomfort and gastrointestinal disorders; rarely, vomiting, diarrhea, constipation or loss of appetite. Isolated cases of ileus during ACE inhibitor therapy have been reported.LiverIsolated cases of liver function disorders (increases in liver enzymes including SGOT and SGPT), hepatitis, and pancreatitis have been reported for patients receiving ACE inhibitor therapy. A syndrome beginning with cholestatic icterus and progressing to hepatic necrosis (sometimes fatal) has rarely been observed in patients being treated with ACE inhibitors. Its relationship to treatment is not clear. Patients who experience icterus or in whom there is a clear increase in liver enzymes are to discontinue treatment with the ACE inhibitor and their progress is to be monitored by the physician.Skin, vesselsAllergic skin reactions such as exanthema and pruritus may occur occasionally; urticaria and angioneurotic oedema affecting the lips, face and/or extremities seldom occur. Serious skin reactions, such as, erythema multiforme, Stevens-Johnson syndrome and toxic epidermal necrolysis have rarely been reported. Skin disorders may be accompanied by fever, muscular pain, arthralgia/arthritis, vasculitis, eosinophilia, leucocytosis, and/or elevated antinuclear antibody (ANA) titers. The attending physician must be informed immediately if there are signs of a serious skin reaction and treatment with Odrik may have to be discontinued. Isolated cases of psoriatic skin disorders, photosensitivity, alopecia, onycholysis and aggravation of Raynaud's syndrome have been observed in patients on ACE inhibitor therapy. Isolated cases of male mammary gland enlargement (gynecomastia) have been observed in connection with ACE inhibitors.Nervous SystemHeadache and fatigue may occur occasionally; dizziness, depression, sleep disorders, impotence, tingling, agitation, sweating, hot flushes, paraesthesia, muscular pain, disorders of balance, confusion, ringing ears, blurred vision and changes in the sense of taste or temporary loss of taste are rare.Lab parametersOccasionally, there may be a drop in haemoglobin levels, haematocrit, leukocyte or thrombocyte counts. Anaemia, thrombocytopenia, neutropenia, eosinophilia are seldom, but may occur, especially in patients whose kidney function is impaired, who have collagen disease or are receiving concomitant therapy with allopurinol, procainamide or certain medications which suppress immune responses; there have also been isolated reports of agranulocytosis and pancytopenia. Isolated cases of haemolysis/haemolytic anaemia, also with G-6-PDH deficiency, have been reported; however, a causal relationship with ACE inhibitor therapy has not been established. Serum uric acid, urea, creatinine and potassium (hyperkalaemia) levels may be increased, especially in patients with impaired kidney function, and serum sodium levels may drop; incidence, however, is rare.In patients with diabetes, increases in serum potassium levels have been observed. Proteinuria may be more pronounced. Bilirubin and liver enzyme concentrations may be increased in isolated cases.NoteThe above-mentioned lab parameters should be checked before treatment with Odrik is initiated and at regular intervals throughout. Serum electrolyte and serum creatinine concentrations should be checked and blood count should be performed especially before initiating therapy and at short intervals in patients at risk (i.e. patients with kidney failure, collagen diseases, patients on immunosuppressants, cytostatics, allopurinol or procainamide). Should symptoms such as fever, swelling of the lymph nodes and/or sore throat occur in the course of Odrik therapy, the patient's white blood cell count must be determined immediately. PrecautionsKidney function must be checked before prescribing Odrik. Blood pressure and/or the relevant lab parameters should be closely monitored, especially in the initial stages of Odrik therapy, in patients who: are suffering from hyponatraemia and/or dehydration, have impaired kidney

69
function, have severe hypertension, are over 65 years of age and have heart failure. Emergency dialysis or haemofiltration using poly(acrylonitrile, sodium-2-methallylsulfonate) high flux membranes (e.g. “AN 69”) in patients on Odrik can cause anaphylactoid reactions that may even lead to life-threatening shock. Odrik must not be used during LDL apheresis with dextran sulfate or in patients undergoing desensitization therapy against insect venoms.Pregnancy and LactationOdrik is contraindicated during pregnancy and while breastfeeding. Pregnancy has to be ruled out in women of child-bearing age before administering an ACE inhibitor such as trandolapril. These women have to use adequate contraception during treatment with Odrik. Should a patient on Odrik become pregnant, therapy has to be switched under the supervision of the attending physician to another substance involving fewer risks for the child because administration of Odrik may cause damage to the foetus, or may even prove to be fatal, in particular during the last 6 months of pregnancy. Trandolapril is excreted in breast milk. No information is available on human use while breastfeeding.Effects On The Ability To Drive And Use MachinesTreatment with this medicinal product should be monitored at regular intervals by the physician. Depending on the individual, the ability to drive a vehicle, operate machinery or work safely under precarious conditions may be affected to various degrees. This applies particularly at the beginning of treatment and when switching to another medication as well as when alcohol is consumed simultaneously.Overdosagea) Symptoms of overdosing: The highest trandolapril doses used in clinical studies were 32 mg, given as a single dose to healthy subjects, and 16 mg, given to hypertensive patients as a repeated daily dose. Trandolapril was tolerated without any symptoms of overdosing. Depending on the extent of overdosing with ACE inhibitors, the following symptoms may be observed: severe hypotension, stupor, bradycardia, circulatory shock, electrolyte imbalances, renal failure.b) Treatment of overdosing: 1. If the patient displays life-threatening angioneurotic oedema involving the tongue, glottis and/or larynx as well as severe anaphylactoid reactions (shock), the following emergency measures are recommended: Immediate subcutaneous administration of 0.3 – 0.5 mg epinephrine or slow intravenous administration of 0.1 mg epinephrine (paying special attention to the dilution instructions!) while monitoring ECG, pulse rate and blood pressure, followed by systemic administration of a glucocorticoid (e.g. 250 - 1000 mg of methylprednisolone). In addition, the intravenous administration of antihistamines and H2 receptor antagonists is recommended. In C1-inactivator-deficient patients, administration of a C1 inactivator, in addition to epinephrine, is recommended. 2. In cases of overdosing or poisoning, the therapeutic measures will depend on the type and time of administration and the type and severity of the symptoms. Apart from general measures which enhance the elimination of trandolapril (e.g. gastric lavage, administration of adsorbents and sodium sulfate within 30 minutes of taking trandolapril), the vital parameters must be monitored or corrected under intensive care conditions. No appreciable amounts of trandolapril and trandolaprilat are cleared by dialysis. In the event of hypotension, sodium replenishment and volume expansion are recommended once the patient has been placed in the supine position. If these measures fail to produce the desired effect, catecholamines should be administered intravenously. Treatment with angiotensin II can also be considered.Refractory bradycardia should be counteracted by pace-maker therapy.Serum electrolyte and creatinine concentrations should be monitored at all times.Drug InteractionsThe following interactions between Odrik and other ACE inhibitors have been observed when these agents are used concomitantly:Sodium: attenuation of the antihypertensive efficacy of Ordik and its positive effect on the symptoms of heart failureAntihypertensive agents: enhancement of the antihypertensive efficacy of trandolapril, especially with diureticsAnalgesics, antiphlogistics (e.g. acetylsalicylic acid, indomethacin): possible attenuation of the antihypertensive efficacy of Udrik and its positive effect on the symptoms of heart failurePotassium, potassium-sparing diuretics (e.g. spirolactone, amiloride, triamterene) and other medications which cause serum potassium levels to rise (e.g. heparin): exacerbated increase in serum potassium levels.Antacids: reduction of ACE inhibitor bioavailability.Lithium: increase in serum lithium levels (check at regular intervals).Alcohol: increase in ACE inhibitor bioavailability.Hypnotics, narcotics, anaesthetics: enhanced blood pressure reduction (anaesthetist must be informed if the patient is taking Odrik);Sympathomimetics: affect the antihypertensive efficacy of ACE inhibitors. Patients should be carefully monitored to establish whether the desired effect is achievedAllopurinol, cytostatics, immunosuppressants, systemic steroids, procainamide: reduction of leukocyte count in the blood; leukopenia.Oral antidiabetics (sulfonyl urea/biguanides), insulin: in rare cases, ACE inhibitors may enhance the blood glucose lowering efficacy of antidiabetic agents in patients with diabetes mellitus, particularly at the beginning of treatment. In these cases, it may be necessary to adjust the dose of the blood glucose lowering medication or of Odrik.IncompatibilitiesNot applicable.Dosage AdministrationNotePatients who are sodium-or volume-depleted (e.g. as a result of vomiting/diarrhea, diuretic therapy) or suffering from heart failure, left ventricular dysfunction after myocardial infarction or severe hypertension may experience an excessive drop in blood pressure, especially in the early stages of treatment with Odrik. As far as possible, sodium-and/or volume-depletion should be compensated before initiating Odrik therapy, and the existing diuretic dose should be reduced or discontinued, as necessary. These patients are to be started on the smallest single dose of 0.5 mg trandolapril (i.e. 1 capsule Odrik 0.5 mg) taken in the morning. After administration of the first dose, and whenever the Odrik and/or loop diuretic dosage is increased, patients must be monitored for about 6 hours to ensure that any undue drops in blood pressure are kept under control. Patients suffering from malignant hypertension, left ventricular dysfunction after myocardial infarction or severe heart failure should be hospitalized during titration on Odrik. Otherwise, the following dosing guidelines apply:Essential hypertensionAs a rule, the initial dose is 1 mg of trandolapril once daily. If blood pressure does not return to normal, the dose can be increased to 2 mg trandolapril once daily. Dose increases should not be attempted until the patient has been receiving treatment for 3 weeks. As a rule, the maintenance dose is 1-2 mg trandolapril once daily, the maximum dose is 4 mg trandolapril once daily. No dose adjustments are required for elderly patients with normal kidney function.Left ventricular dysfunction after myocardial infarctionTreatment should not be initiated until 3 days after the infarction at the earliest. The initial dose is 1 capsule of Odrik 0.5 mg (0.5 mg trandolapril) once daily. If this dose is well tolerated, then the dose on the following day should be increased to 1 mg trandolapril as a single dose, i.e. 2 capsules of Udrik 0.5 mg or 1 capsule of Odrik 1 mg. Depending on tolerability, the dose should then be progressively increased to a maximum maintenance dose of 2 capsules of Odrik 2 mg (i.e. 4 mg of trandolapril) once daily. Should symptomatic hypotension occur, dose incrementation may be temporarily interrupted. In cases of hypotension all concomitant antihypertensive medications (e.g. nitrates, diuretics) have to be checked and the doses reduced as appropriate. The Odrik dose should only be reduced if the previously mentioned measures have proved ineffective or are not applicable.Dosage in patients with moderately impaired renal function (creatinine clearance 30 – 60 ml/min or serum creatinine concentrations > 1.2 - < 1.8 mg/dl):
70
Patients in whom creatinine clearance is > 30 ml/min do not require a dose reduction. However, close monitoring of the relevant lab parameters is recommended in patients with impaired renal function. Patients in whom renal function is severely impaired (creatinine clearance < 30 ml/min) and/or who require dialysis should not be treated with Odrik.Dosage in patients with moderate liver function impairment:The initial dose is 0.5 mg of trandolapril (i.e. 1 capsule Odrik 0.5 mg capsule) taken in the morning. The dosage may only be increased gradually depending on the patient's individual response to therapy. The maximum dose of 2 mg trandolapril per day (i.e. 1 capsule Odrik 2 mg or 2 capsules Odrik 1 mg or 4 capsules Odrik 0.5 mg) must not be exceeded. Patients suffering from severe liver function disorder or cirrhosis are not to be treated with Odrik. Odrik is taken at the same time each morning before, during or after breakfast with plenty of liquid.Left ventricular dysfunction after myocardial infarctionOdrik (trandolapril) therapy should not be initiated until 3 days after myocardial infarction at the earliest and no later than day 7 after acute infarction at the latest. If trandolapril is well tolerated, therapy should be continued for at least 2 years after the infarction. Any increase in the Odrik dose will depend on tolerability, in particular on the occurrence of hypotension. Concomitant administration of Odrik and other drug products (e.g. beta-blockers, acetylsalicylic acid) usually given after myocardial infarction is possible. Odrik is contraindicated in children.StorageStore at temperatures below 25°C.PackagingOdrik 0.5 mg: blister packs of 28 capsules eachOdrik 1 mg: blister packs of 28 capsules eachOdrik 2 mg: blister packs of 28 capsules each
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
REDUCTIL ®GeneralReductil® 10 mg capsules.Reductil® 15 mg capsules.CompositionReductil 10mg: Each capsule contains 10mg Sibutramine hydrochloride monohydrate (equivalent to 8.37 mg Sibutramine). Reductil 15mg: Each capsule contains 15mg Sibutramine hydrochloride monohydrate (equivalent to 12.55 mg Sibutramine).PropertiesCapsule, hard.PharmacodynamicSibutramine produces its therapeutic effects predominantly via its active secondary and primary amine metabolites (metabolite 1 and metabolite 2) which are inhibitors of noradrenaline, serotonin (5- hydroxytryptamine; 5-HT) and dopamine reuptake. In human brain tissue, metabolite 1 and metabolite 2 are ~3-fold more potent as in vitro inhibitors of noradrenaline and serotonin reuptake than of dopamine reuptake. Plasma samples taken from sibutramine-treated volunteers caused significant inhibition of both noradrenaline reuptake (73%) and serotonin reuptake (54%) with no significant inhibition of dopamine reuptake (16%). Sibutramine and its metabolites are neither monoamine-releasing agents nor are they monoamine oxidase inhibitors. They have no affinity with a large number of neurotransmitter receptors, including serotonergic (5-HT1, 5-HT1A, 5-HT1B, 5-HT2A, 5- HT2C), adrenergic (β1, β2, β3, α1, α2), dopaminergic (D1-like, D2-like), muscarinic, histaminergic (H1), benzodiazepine and NMDA receptors. In animal models using lean growing and obese rats, sibutramine produces a reduction in bodyweight gain. This is believed to result from its impact on food intake, i.e. by enhancing satiety, but enhanced thermogenesis also contributes to weight loss. These effects have been shown to be mediated by the inhibition of serotonin and noradrenaline re-uptake. In clinical trials in man, Reductil was shown to effect weight loss by enhancing satiety. Data are also available which demonstrate a thermogenic effect of Reductil by attenuating the adaptive decline in resting metabolic rate during weight loss. Weight loss induced by Reductil is accompanied by beneficial changes in serum lipids and glycaemic control in patients with dyslipidaemia and type 2 diabetes, respectively. In obese patients with type 2 diabetes mellitus weight loss with sibutramine was associated with mean reductions of 0.6% (unit) in HbA1c. Similarly, in obese patients with dyslipidaemia, weight loss was associated with increases in HDL cholesterol of 12-22% and reductions in triglycerides of 9-21%.Pharmacokinetic propertiesSibutramine is well absorbed and undergoes extensive first-pass metabolism. Peak plasma levels (Cmax) were achieved 1.2 hours after a single oral dose of 20 mg of sibutramine hydrochloride monohydrate. The half-life of the parent compound is 1.1 hours. The pharmacologically active metabolites 1 and 2 reach Cmax in three hours with elimination half-lives of 14 and 16 hours, respectively. Linear kinetics have been demonstrated over the dose range of 10 to 30 mg, with no dose-related change in the elimination half-lives but a dose-proportionate increase in plasma concentrations. On repeated dosing, steady-state concentrations of metabolites 1 and 2 are achieved within 4 days, with an approximately 2-fold accumulation. The pharmacokinetics of sibutramine and its metabolites in obese subjects are similar to those in normal weight subjects. The relatively limited data available so far provide no evidence of a clinically relevant difference in the pharmacokinetics of males and females. The pharmacokinetic profile observed in elderly healthy subjects (mean age 70 years) was similar to that seen in young healthy subjects. In subjects with moderate hepatic impairment, bioavailability of the active metabolites was 24% higher after a single dose of sibutramine. Plasma protein binding of sibutramine and its metabolites 1 and 2 amounts to approximately 97%, 94% and 94%, respectively. Hepatic metabolism is the major route of elimination of sibutramine and its active metabolites 1 and 2. Other (inactive) metabolites are excreted primarily via the urine, at a urine: faeces ratio of 10 : 1. In vitro hepatic microsome studies indicated that CYP3A4 is the major cytochrome P450 isoenzyme responsible for sibutramine metabolism. In vitro, there was no indication of an affinity with CYP2D6, a low capacity enzyme involved in pharmacokinetic interactions with various drugs. Further in vitro studies have revealed that sibutramine has no significant effect on the activity of the major P450 isoenzymes, including CYP3A4. The CYP450s involved in the further metabolism of metabolite 2 were shown (in vitro) to be CYP3A4 and CYP2C9. Although there are no data at present, it is likely that CYP3A4 is also involved in further metabolism of metabolite 1.IndicationsReductil is indicated as adjunctive therapy within a weight management programme for: 1. Patients with nutritional obesity and a body mass index (BMI) of 30 kg/m2 or higher. 2. Patients with nutritional excess weight and a BMI of 27 kg/m2 or higher, if other obesity-related risk factors such as type 2 diabetes or dyslipidaemia are present.NOTE: Reductil may only be prescribed to patients who have not adequately responded to an appropriate weight-reducing regimen alone, i.e. patients who have difficulty achieving or maintaining >5% weight loss within 3 months.Treatment with Reductil should only be given as part of a long-term integrated therapeutic approach for weight reduction under the care of a physician experienced in the treatment of obesity. An appropriate approach to obesity management should include dietary and behavioural modification as well as increased physical activity. This integrated approach is essential for a lasting change in eating habits and behaviour which is fundamental to the long-term maintenance of the reduced weight level once Reductil is stopped. Patients should change their lifestyle while on Reductil so that they are able to maintain their weight once drug treatment has ceased. They should be informed that, if they fail to do so, they may regain weight. Even after cessation of Reductil continued monitoring of the patient by the physician should be encouraged.

71
ContraindicationsKnown hypersensitivity to sibutramine hydrochloride monohydrate or to any of the excipients; organic causes of obesity; history of major eating disorders; PSYCHIATRIC ILLNESS: Sibutramine has shown potential antidepressant activity in animal studies and therefore it cannot be excluded that sibutramine could induce a manic episode in bipolar patients; Gilles de la Tourette’s syndrome; concomitant use, or use during the past two weeks, of monoamine oxidase inhibitors or of other centrally-acting drugs for the treatment of psychiatric disorders (such as antidepressants, antipsychotics) or for weight reduction, or tryptophan for sleep disturbances; history of coronary artery disease, congestive heart failure, tachycardia, peripheral arterial occlusive disease, arrhythmia or cerebrovascular disease (stroke or TIA); inadequately controlled hypertension (>145/90 mmHg; see “Warnings and precautions”); hyperthyroidism; severe hepatic impairment; severe renal impairment; benign prostatic hyperplasia with urinary retention; phaeochromocytoma; narrow angle glaucoma; history of drug, medication or alcohol abuse; pregnancy and lactation (see “Pregnancy and lactation”); children and young adults up to the age of 18 years and patients above 65 years of age due to insufficient data.Side EffectsMost side effects reported with sibutramine occurred at the start of treatment (during the first 4 weeks). Their severity and frequency diminished over time. They were generally not serious, did not entail discontinuation of treatment, and were reversible.The side effects observed in phase II/III clinical trials are listed below by body system (very common >1/10, common <1/10 and >1/100):REDUCTIL Table 1. Side EffectsBody system Frequency Undesirable effects
Cardiovascular system(see detailed information below) Common
TachycardiaPalpitationsRaised blood pressure/hypertensionVasodilation (hot flush)
Gastrointestinal system
Very common Constipation
Common NauseaHaemorrhoid aggravation
Central nervous system Very common Dry mouth Insomnia
Common
Light-headednessParaesthesiaHeadacheAnxiety
Skin Common SweatingSensory functions Common Taste perversionCardiovascular system: A mean increase in resting systolic and diastolic blood pressure of 2-3 mmHg, and a mean increase in heart rate of 3-7 beats per minute have been observed. Higher increases in blood pressure and heart rate cannot be excluded in isolated cases. Any clinically significant increase in blood pressure and pulse rate tends to occur early on in treatment (first 4-12 weeks). Therapy should be discontinued in such cases (see “Warnings and precautions.”). For use of Reductil in patients with hypertension, see “Contraindications” and “Warnings and precautions”. Clinically significant adverse events seen in clinical studies and during postmarketing surveillance are listed below by body system:Blood and lymphatic system disorders: Thrombocytopenia, Henoch- Schonlein purpura.Cardiovascular disorders: Atrial fibrillation, paroxysmal supraventricular tachycardia.Immune system disorders: Allergic hypersensitivity reactions ranging from mild skin eruptions and urticaria to angioedema and anaphylaxis have been reported.Psychiatric disorders: Agitation, depression in patients both with and without a prior history of depression (see “Warnings and precautions”).Nervous system disorders: Seizures, serotonin syndrome in combination with other agents affecting serotonin release (see “Drug Interactions”), transient short-term memory disturbance.Eye disorders: Blurred vision.Gastrointestinal disorders: Diarrhoea, vomiting.Skin and subcutaneous tissue disorders: Alopecia, rash, urticaria.Renal and urinary disorders: Acute interstitial nephritis, mesangiocapillary glomerulonephritis, urinary retention.Reproductive system and breast disorders: Abnormal ejaculation/ orgasm, impotence, menstrual cycle disorders, metrorrhagia.Investigations: Reversible increases in liver enzymes.Other: Withdrawal symptoms such as headache and increased appetite have rarely been observed.PrecautionsBlood pressure and pulse rate should be monitored in all patients on Reductil, as sibutramine has caused clinically relevant increases in blood pressure in some patients. In the first three months of treatment, these parameters should be checked every 2 weeks; between month 4 and 6 these parameters should be checked once monthly and regularly thereafter, at maximum intervals of three months. Treatment should be discontinued in patients who have an increase, at two consecutive visits, in resting heart rate of > 10 bpm or systolic/diastolic blood pressure of > 10 mmHg. In previously well-controlled hypertensive patients, if blood pressure exceeds 145/90 mmHg at two consecutive readings, treatment should be discontinued (see “Side effects, cardiovascular system”). In patients with sleep apnoea syndrome particular care should be taken in monitoring blood pressure. For use of sibutramine concomitantly with sympathomimetics, please see “Drug Interactions”. Although sibutramine has not been associated with primary pulmonary hypertension, it is important, in view of general concerns with antiobesity drugs, to be on the look out for symptoms such as progressive dyspnoea, chest pain and ankle oedema in the course of routine check-ups. The patient should be advised to consult a doctor immediately if these symptoms occur.Reductil should be given with caution to patients with epilepsy.Increased plasma levels have been observed in the assessment of sibutramine in patients with mild to moderate hepatic impairment. Although no adverse effects have been reported, Reductil should be used with caution in these patients.Although only inactive metabolites are excreted by the renal route, Reductil should be used with caution in patients with mild to moderate renal impairment.Reductil should be given with caution to patients who have a family history of motor or verbal tics. Women of child-bearing potential should employ adequate contraception whilst taking Reductil.There is the possibility of drug abuse with CNS-active drugs. However, available clinical data have shown no evidence of drug abuse with sibutramine.There are general concerns that certain anti-obesity drugs are associated with an increased risk of cardiac valvulopathy. However, clinical data show no evidence of an increased incidence with sibutramine.Patients with a history of major eating disorders, such as anorexia nervosa and bulimia nervosa, are contraindicated. No data are available for sibutramine in the treatment of patients with binge (compulsive) eating disorder.

72
Sibutramine should be given with caution to patients with open angle glaucoma and those who are at risk of raised intraocular pressure, e.g. family history.In common with other agents that inhibit serotonin reuptake, there is a potential for an increased risk of bleeding in patients taking sibutramine. Sibutramine should, therefore, be used with caution in patients predisposed to bleeding events and those taking concomitant medications known to affect haemostasis or platelet function.Cases of depression, suicidal ideation and suicide have been reported rarely in patients on sibutramine treatment. Special attention is therefore required in patients with a history of depression. If signs or symptoms of depression occur during the treatment with sibutramine, the discontinuation of sibutramine and commencement of an appropriate treatment should be considered.Reductil contains lactose and therefore should not be used in patients with rare hereditary problems of galactose intolerance, Lapp lactase deficiency or glucose-galactose malabsorption.Pregnancy and LactationUse in pregnancy: Sibutramine should not be used during pregnancy. It is generally considered inappropriate for weight-reducing drugs to be used during pregnancy, so women of childbearing potential should employ an adequate method of contraception while taking sibutramine and notify their physician if they become pregnant or intend to become pregnant during therapy. No controlled studies with Reductil have been conducted in pregnant women.Use in lactation: It is not known whether sibutramine is excreted in human breast milk and therefore administration of Reductil is contraindicated during lactation.Effects on ability to drive and use machinesAlthough sibutramine did not affect psychomotor or cognitive performance in healthy volunteers, any centrally-acting drug may impair judgement, thinking or motor skills. Therefore, patients should be cautioned that their ability to drive a vehicle, operate machinery or work in a hazardous environment may be impaired when taking Reductil.OverdosageThere is limited experience of overdosing with sibutramine. No specific therapeutic measures are recommended and there is no specific antidote. Treatment should consist of the general measures employed in the management of overdosing, such as keeping airways unobstructed, monitoring of cardiovascular functions and general symptomatic and supportive measures. Early administration of activated charcoal may delay the absorption of sibutramine. Gastric lavage may also be of benefit. Cautious use of beta-blockers may be indicated in patients with elevated blood pressure or tachycardia. There are a number of reports of overdose in humans (including accidental ingestion by children as young as 18 months) where doses of up to 500 mg sibutramine hydrochloride monohydrate were ingested. A heart rate of 160 beats per minute was observed in one patient who took 500 mg sibutramine hydrochloride monohydrate. Except in one case of multiple drug intoxication with alcohol (where the patient died, possibly due to inhalation of vomit), there were no complications and the individuals made a full recovery.Drug InteractionsSibutramine and its active metabolites are eliminated by hepatic metabolism; the main enzyme involved is CYP3A4, and CYP2C9 and CYP1A2 can also contribute. Caution should be exercised on concomitant administration of Reductil with drugs which affect CYP3A4 enzyme activity (see “Pharmacokinetic properties”). CYP3A4 inhibitors include ketoconazole, itraconazole, erythromycin, clarithromycin, troleandomycin and cyclosporin. Co-administration of ketoconazole or erythromycin with sibutramine increased plasma concentrations (AUC) of sibutramine active metabolites (23% or 10% respectively) in an interaction study. Mean heart rate increased by up to 2.5 beats per minute more than on sibutramine alone. Rifampicin, phenytoin, carbamazepine, phenobarbital and dexamethasone are CYP3A4 enzyme inducers and may accelerate sibutramine metabolism, although this has not been studied experimentally. The simultaneous use of several drugs, each of which increases levels of serotonin in the brain, may give rise to serious interactions. This phenomenon is called serotonin syndrome and may occur in rare cases in connection with the simultaneous use of a selective serotonin reuptake inhibitor [SSRI] together with certain antimigraine drugs (such as sumatriptan, dihydroergotamine), or along with certain opioids (such as pentazocine, pethidine, fentanyl, dextromethorphan), or in the case of simultaneous use of two SSRIs. As sibutramine inhibits serotonin reuptake (among other effects), Reductil should not be used concomitantly with other drugs which also raise serotonin levels in the brain. Concomitant use of Reductil with other drugs which may raise the blood pressure or heart rate (e.g. sympathomimetics) has not been systematically evaluated. Drugs of this type include certain cough, cold and allergy medications (e.g. ephedrine, pseudoephedrine), and certain decongestants (e.g. xylometazoline). Caution should be taken when prescribing Reductil to patients who use these medicines. Reductil does not impair the efficacy of oral contraceptives. At single doses, there was no additional impairment of cognitive or psychomotor performance when sibutramine was administered concomitantly with alcohol. However, the consumption of alcohol is not compatible with the recommended dietary measures as a general rule. No data on the concomitant use of Reductil with orlistat are available. Two weeks should elapse between stopping sibutramine and starting monoamine oxidase inhibitors.IncompatibilitiesNot applicable.Dosage AdministrationAdults: The initial dose is one capsule of Reductil 10 mg swallowed whole, once daily, in the morning, with liquid (eg. a glass of water). The capsule can be taken with or without food. In those patients with an inadequate response to Reductil 10mg (defined as less than 2 kg weight loss after four weeks treatment), the dose may be increased to one capsule of Reductil 15 mg once daily, provided that Reductil 10mg was well tolerated. Treatment must be discontinued in patients who have responded inadequately to Reductil 15 mg (defined as less than 2 kg weight loss after four weeks treatment). Non-responders are at a higher risk of undesirable effects (see “Side Effects”).DURATION OF TREATMENT: Treatment must be discontinued in patients who have not responded adequately, i.e. whose weight loss stabilises at less than 5% of their initial bodyweight or whose weight loss within three months after starting therapy has been less than 5% of their initial bodyweight. Treatment should not be continued in patients who regain 3 kg or more after previously achieved weight loss. In patients with associated co-morbid conditions, it is recommended that treatment with Reductil 10 mg / 15 mg should only be continued if it can be shown that the weight loss induced is associated with other clinical benefits, such as improvements in lipid profile in patients with dyslipidaemia or glycaemic control of type 2 diabetes. Reductil should only be given for periods up to one year. Data on use over one year is limited.StorageShelf life is 3 years.Do not store above 25°C.Store in the original package.PackagingReductil 10 mg: Blister packs containing 28 capsules.Reductil 15 mg: Blister packs containing 28 capsules.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
SEVOFLURANE ®GeneralInhalationAnaesthetic

73
CompositionSevoflurane is a non-flammable, pleasant smelling, volatile liquid. It is comprised only of the active ingredient (Sevoflurane)It is 1, 1, 1, 3, 3, 3-hexafluoro-2-fluoromethoxypropane and has the following structural formula:Some physical constants of Sevoflurane are:
Relative molecular mass 200.05
Boiling point at 760mmHg 58.6°C
Refractive index n20 1.2740 - 1.2760
Specific gravity at 20°C 1.520 - 1.525
Vapour pressure Temp °C mmHg
20 157
25 197
36 317
Partition coefficients at 37°C
Water/gas 0.36
Blood/gas 0.63 -0.69
Olive Oil/gas 47.2 - 53.9
Mean partition coefficientsat 25°C - component/gas
Conductive rubber 14.0
Butyl rubber 7.7
Polyvinylchloride 17.4
Polyethylene 1.3
Purity by gas chromatography99.9875% or better
Flammability Not flammable
ExcipientsWater (as a Lewis Acid Inhibitor)PropertiesPharmacodynamicChanges in the clinical effects of Sevoflurane rapidly follow changes in the inspired concentration.Cardiovascular EffectsAs with all other inhalation agents Sevoflurane depresses cardiovascular function in a dose related fashion. In one volunteer study, increases in Sevoflurane concentration resulted in decrease in mean arterial pressure, but there was no change in heart rate. Sevoflurane did not alter plasma noradrenaline concentrations in this study.Nervous System EffectsNo evidence of seizure was observed during the clinical development programme. In patients with normal intracranial pressure (ICP),
Sevoflurane had minimal effect on ICP and preserved CO2 responsiveness. The safety of Sevoflurane has not been investigated in patients with a raised ICP. In patients at risk for elevations of ICP, Sevoflurane should be administered cautiously in conjunction with ICP-reducing manoeuvres such as hyperventilation.PharmacokineticThe low solubility of Sevoflurane in blood should result in alveolar concentrations which rapidly increase upon induction and rapidly decrease upon cessation of the inhaled agent. In humans <5% of the absorbed Sevoflurane is metabolised. The rapid and extensive pulmonary elimination of Sevoflurane minimises the amount of anaesthetic available for metabolism. Sevoflurane is defluorinated via cytochrome P450(CYP)2E1 resulting in the production of hexafluoroisopropanol (HFIP) with release of inorganic fluoride and carbon dioxide (or a one carbon fragment). HFIP is then rapidly conjugated with glucuronic acid and excreted in the urine. The metabolism of Sevoflurane may be increased by known inducers of CYP2E1 (e.g. isoniazid and alcohol), but it is not inducible by barbiturates. Transient increases in serum inorganic fluoride levels may occur during and after Sevoflurane anaesthesia. Generally, concentrations of inorganic fluoride peak within 2 hours of the end of Sevoflurane anaesthesia and return within 48 hours to pre-operative levels.IndicationsSevoflurane is indicated for induction and maintenance of general anaesthesia in adult and paediatric patients for inpatient and outpatient surgery.Contraindications
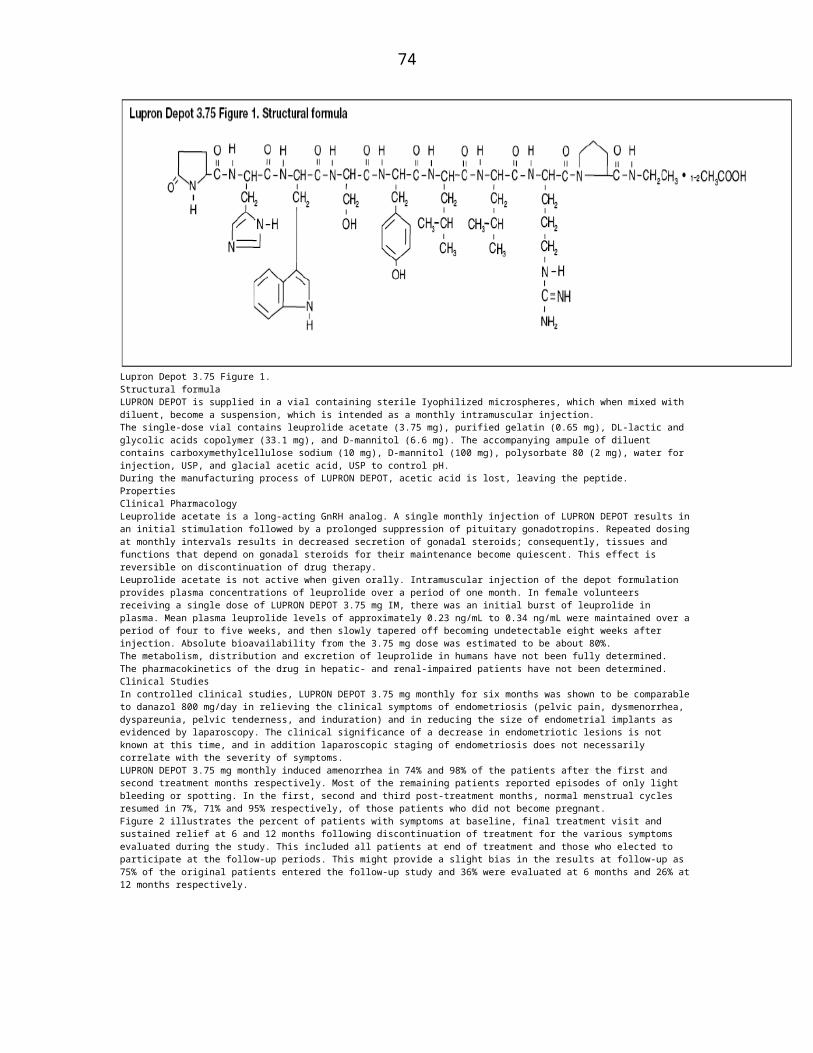
74
Sevoflurane should not be used in patients with known sensitivity to Sevoflurane. Sevoflurane is also contraindicated in patients with known or suspected genetic susceptibility to malignant hyperthermia.Side EffectsAs with all potent inhaled anaesthetics, Sevoflurane may cause dose-dependent cardio-respiratory depression. Most adverse events are mild to moderate in severity and are transient. Nausea and vomiting are commonly observed in the post-operative period, at a similar incidence to those found with other inhalation anaesthetics. These effects are common sequelae of surgery and general anaesthesia which may be due to the inhalational anaesthetic, other agents administered intra-operatively or post-operatively and to the patient’s response to the surgical procedure. Adverse event data are derived from controlled clinical trials conducted in the United States and Europe in over 3,200 patients. The type, severity and frequency of adverse events in Sevoflurane patients were comparable to adverse events in patients treated with other inhalation anaesthetics.The most frequent adverse events associated with Sevoflurane overall were nausea (24%) and vomiting (17%). Agitation occurred frequently in children (23%). Other frequent adverse events (>10%) associated with Sevoflurane administration overall were: increased cough and hypotension.In addition to nausea and vomiting, other frequent adverse events (>10%) by age listings were: in adults, hypotension; in elderly, hypotension and bradycardia; in children, agitation and increased cough. Less frequent adverse events (1-<10% overall) associated with Sevoflurane administration were: agitation, somnolence, chills, bradycardia, dizziness, increased salivation, respiratory disorder, hypertension, tachycardia, laryngismus, fever, headache, hypothermia, increased SGOT. Occasional (<1% overall) adverse events occurring during clinical trials included: arrhythmias, increased LDH, increased SGPT, hypoxia, apnoea, leukocytosis, ventricular extrasystoles, supraventricular extrasystoles, asthma, confusion, increased creatinine, urinary retention, glycosuria, atrial fibrillation, complete AV block, bigeminy, leucopenia Malignant hyperthermia and acute kidney failure have been reported very rarely. Rare reports of allergic reactions, such as rash, urticaria, pruritus, bronchospasm, anaphylactic or anaphylactoid reactions have been reported. Rare reports of post-operative hepatitis exist, but with an uncertain relationship to Sevoflurane. Convulsions may occur extremely rarely following Sevoflurane administration, particularly in children. There have been very rare reports of pulmonary oedema. As with other anaesthetic agents, cases of twitching and jerking movements with spontaneous resolution have been reported in children receiving Sevoflurane for induction of anaesthesia with an uncertain relationship to Sevoflurane.Laboratory findings:Transient elevations in glucose and white blood cell count may occur as with use of other anaesthetic agents. Occasional cases of transient changes in hepatic function tests were reported with Sevoflurane.PrecautionsSevoflurane should be administered only by persons trained in the administration of general anaesthesia. Facilities for maintenance of a patent airway, artificial ventilation, oxygen enrichment and circulatory resuscitation must be immediately available. Sevoflurane should be delivered via a vaporiser specifically calibrated for use with Sevoflurane so that the concentration delivered can be accurately controlled. Hypotension and respiratory depression increase as anaesthesia is deepened. During the maintenance of anaesthesia, increasing the concentration of Sevoflurane produces dose-dependent decreases in blood pressure. Excessive decrease in blood pressure may be related to depth of anaesthesia and in such instances may be corrected by decreasing the inspired concentration of Sevoflurane. The recovery from general anaesthesia should be assessed carefully before patients are discharged from the recovery room.Malignant Hyperthermia: In susceptible individuals, potent inhalation anaesthetic agents may trigger a skeletal muscle hypermetabolic state leading to high oxygen demand and the clinical syndrome known as malignant hyperthermia. Treatment includes discontinuation of triggering agents (e.g. Sevoflurane), administration of intravenous dantrolene sodium, and application of supportive therapy.Renal failure may appear later, and urine flow should be monitored and sustained if possible. Because of the small number of patients with renal insufficiency (baseline serum creatinine greater than 133μmol/litre) studied, the safety of Sevoflurane administration in this group has not been fully established.Therefore, Sevoflurane should be used with caution in patients with renal insufficiency. Sevoflurane produces low levels of Compound A (pentafluoroisopropenyl fluoromethyl ether (PIFE)) and trace amounts of Compound B (pentafluoromethoxy isopropyl fluoromethyl ether (PMFE)), when in direct contact with CO2 absorbents. Levels of Compound A increase with:- increase in canister temperature; increase in anaesthetic concentration; decrease in gas flow rate and increase more with the use of Baralyme rather than Soda lime. In some studies in rats, nephrotoxicity was seen in animals exposed to levels of Compound A in excess of those usually seen in routine clinical practice. The mechanism of this renal toxicity in rats is unknown and its relevance to man has not been established. Rare cases of extreme heat, smoke, and/or spontaneous fire in the anaesthesia machine have been reported during Sevoflurane use in conjunction with the use of desiccated CO2 absorbent, specifically those containing potassium hydroxide (e.g Baralyme). An unusually delayed rise or unexpected decline of inspired Sevoflurane concentration compared to the vaporizer setting may be associated with excessive heating of the CO2 absorbent canister. When a clinician suspects that the CO2 absorbent may be desiccated, it should be replaced. The colour indicator of most CO2 absorbents does not necessarily change as a result of desiccation. Therefore, the lack of significant colour change should not be taken as an assurance of adequate hydration. CO2 absorbents should be replaced routinely regardless of the state of the colour indicator. An exothermic reaction, enhanced Sevoflurane degradation, and production of degradation products can occur when CO2 absorbent becomes desiccated, such as after an extended period of dry gas flow through the CO2 absorbent canisters. Sevoflurane degradants (methanol, formaldehyde, carbon monoxide, and Compounds A, B, C and D) were observed in the respiratory circuit of an experimental anaesthesia machine using desiccated CO2 absorbents and maximum Sevoflurane concentrations (8%) for extended periods of time (≥ 2 hours). Concentrations of formaldehyde observed at the anaesthesia respiratory circuit (using sodium hydroxide containing absorbents) were consistent with levels known to cause mild respiratory irritation. The clinical relevance of the degradants observed under this extreme experimental model is unknown. Experience with repeat exposure to Sevoflurane is very limited. However, there were no obvious differences in adverse events between first and subsequent exposures.Pregnancy and LactationWith the exception of one study in Caesarean Section there are no other studies in pregnant women, including in labour and delivery. Experience in Caesarean section is limited to one trial in a small number of patients. Reproduction studies have been performed in rats and rabbits at doses up to 1 MAC. No effects on male and female reproductive capabilities were observed. Reduced foetal body weights concomitant with increased skeletal variations were noted in rats only at maternally toxic concentrations. No adverse foetal effects were observed in rabbits. Sevoflurane was not teratogenic. Therefore, Sevoflurane should be used during pregnancy only if clearly needed. It is not known whether Sevoflurane is excreted in human milk therefore caution should be exercised when Sevoflurane is administered to a nursing woman.Effects on Ability to Drive and Use MachinesAs with other agents, patients should be advised that performance of activities requiring mental alertness, such as operating hazardous machinery, may be impaired for some time after general anaesthesia. Patients should not be allowed to drive for a suitable period after Sevoflurane anaesthesia.OverdosageIn the event of overdosage, the following action should be taken: Stop drug administration, establish a clear airway and initiate assisted or controlled ventilation with pure oxygen and maintain adequate cardiovascular function.Drug InteractionsThe action of non-depolarising muscle relaxants is markedly potentiated with Sevoflurane, therefore, when administered with Sevoflurane, dosage adjustments of these agents should be made. Sevoflurane is similar to isoflurane in the sensitisation of the myocardium to the

75
arrhythmogenic effect of exogenously administered adrenaline. MAC values for Sevoflurane decrease with the addition of nitrous oxide as indicated in the table on ‘Effect of Age on MAC of Sevoflurane’.As with other agents, lesser concentrations of Sevoflurane may be required following use of an intravenous anaesthetic e.g. propofol.The metabolism of Sevoflurane may be increased by known inducers of CYP2E1 (e.g. isoniazid and alcohol), but it is not inducible by barbiturates.IncompatibilitiesSevoflurane is stable when stored under normal room lighting conditions. No discernible degradation of Sevoflurane occurs in the presence of strong acids or heat. Sevoflurane is not corrosive to stainless steel, brass, alumimum, nickel-plated brass, chrome-plated brass or copper beryllium alloy. Chemical degradation can occur upon exposure of inhaled anaesthetics to CO2 absorbent within the anaesthesia machine. When used as directed with fresh absorbents, degradation of Sevoflurane is minimal and degradants are undetectable or non-toxic. Sevoflurane degradation and subsequent degradant formation are enhanced by increasing absorbent temperature, desiccated CO2 absorbent (especially potassium hydroxide-containing, e.g. Baralyme), increased Sevoflurane concentration and decreased fresh gas flow. Sevoflurane can undergo alkaline degradation by two pathways. The first results from the loss of hydrogen fluoride with the formation of pentafluoroisopropanyl fluoromethyl ether (PIFE or more commonly known as Compound A). The second pathway for degradation of Sevoflurane occurs only in the presence of desiccated CO2 absorbents and leads to the dissociation of Sevoflurane into hexafluoroisopropanol (HFIP) and formaldehyde. HFIP is inactive, non-genotoxic, rapidly glucoronidated, cleared and has toxicity comparable to Sevoflurane. Formaldehyde is present during normal metabolic processes. Upon exposure to a highly desiccated absorbent, formaldehyde can further degrade into methanol and formate. Formate can contribute to the formation of carbon monoxide in the presence of high temperature. Methanol can react with compound A to form the methoxy addition product Compound B. Compound B can undergo further HF elimination to form Compounds C, D and E. With highly desiccated absorbents, especially those containing potassium hydroxide (e.g Baralyme) the fomation of formaldehyde, methanol, carbon monoxide, Compound A and perhaps some of its degradants, Compounds B, C and D may occur.Dosage AdministrationSevoflurane should be delivered via a vaporiser specifically calibrated for use with Sevoflurane so that the concentration delivered can be accurately controlled. MAC (minimum alveolar concentration) values for Sevoflurane decrease with age and with the addition of nitrous oxide.Table 1 indicates average MAC values for different age groups.SEVOFLURANE Table 1 : Effect of age on MAC of Sevoflurane.Age of Patient Sevoflurane in Sevoflurane in(years) Oxygen 65% N2O/35%O2*<3 3.3 - 2.6% 2.0%3 - <5 2.5% Not available5 - 12 2.4% Not available25 2.5% 1.4%35 2.2% 1.2%40 2.05% 1.1%50 1.8% 0.98%60 1.6% 0.87%80 1.4% 0.70%* In paediatric patients, 60% N2O/ 40% O2 was used.Induction:Dosage should be individualised and titrated to the desired effect according to the patient’s age and clinical status. A short acting barbiturate or other intravenous induction agent may be administered followed by inhalation of sevoflurane. Induction with sevoflurane may be achieved in oxygen or in combination with oxygen-nitrous oxide mixtures. In adults inspired concentrations of up to 5% Sevoflurane usually produce surgical anaesthesia in less than 2 minutes. In children, inspired concentrations of up to 7% Sevoflurane usually produce surgical anaesthesia in less than 2 minutes. Alternatively, for induction of anaesthesia in unpremedicated patients, inspired concentrations of up to 8% Sevoflurane may be used.Maintenance:Surgical levels of anaesthesia may be sustained with concentrations of 0.5 - 3% Sevoflurane with or without the concomitant use of nitrous oxide.Elderly: As with other inhalation agents, lesser concentrations of Sevoflurane are normally required to maintain surgical anaesthesia. Emergence:Emergence times are generally short following Sevoflurane anaesthesia. Therefore, patients may require early post operative pain relief.Instructions for Use/HandlingSevoflurane should be administered via a vaporiser calibrated specifically for Sevoflurane using a key filling system designed for Sevoflurane specific vaporisers or other appropriate Sevoflurane specific vaporiser filling systems. Carbon dioxide absorbents should not be allowed to dry out when inhalational anaesthetics are being administered. Some halogenated anaesthetics have been reported to interact with dry carbon dioxide absorbent to form carbon monoxide. However, in order to minimise the risk of formation of carbon monoxide in re-breathing circuits and the possibility of elevated carboxyhaemoglobin levels, CO2 absorbents should not be allowed to dry out. There have been rare cases of excessive heat production, smoke and fire in the anaesthetic machine when Sevoflurane has been used in conjunction with a desiccated (dried out) CO2 absorbent. If the CO2 absorbent is suspected to be desiccated it should be replaced.StorageDo not store above 25°C. Do not refrigerate. Keep cap tightly closed.Packaging100ml and 250ml amber polyethylene napthalate (PEN) bottles.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
SIMDAX™GeneralLevosimendan 2.5 mg/mLCompositionLevosimendan 2.5 mg/mL concentrate for solution for infusion, Conc. Sol. Inf. Short term Sterile ConcentrateTrade NamesSimdax™, Ximdan™, Daxim™, Simevo™, Tropodan™, Zendan™, Simtac™.Description

76
Levosimendan, the active pharmaceutical ingredient in levosimendan 2.5 mg/mL concentrate, is a member of a new class of cardiotonic agents, the calcium sensitizers, which increase cardiac contractility by enhancing the sensitivity of the heart to calcium. As a result, levosimendan produces positive inotropic effects that are independent of beta-receptors or cyclic AMP. Levosimendan is chemically named as (-)-(R)-[[4-(1,4,5,6- tetrahydro-4-methyl-6-oxo-3- pyridazinyl)-phenyl]hydrazono]- propanedinitrile. It is a yellow to brownish yellow powder with a molecular weight of 280.3, an empirical formula of C14H12N6O, and the following structure: Levosimendan is a moderately lipophilic compound. Its solubility in distilled water is 0.04 mg/mL, in ethanol 7.8 mg/mL, and at a pH of 8 in phosphate buffer (67 mM) 0.9 mg/mL. Levosimendan 2.5 mg/mL concentrate is available in 5 mL and 10 mL vials. Each mL contains 2.5 mg of levosimendan. Inactive ingredients include: povidone, anhydrous citric acid, and anhydrous ethanol. Levosimendan 2.5 mg/mL concentrate is a clear, yellow or orange solution for dilution prior to administration.PropertiesPharmacodynamicsLevosimendan enhances the calcium sensitivity of contractile proteins by binding to cardiac troponin C in a calcium- dependent manner. Levosimendan increases the contraction force but does not impair ventricular relaxation. In addition, levosimendan opens ATP-sensitive potassium channels in vascular smooth muscle, thus inducing vasodilatation of systemic and coronary arterial resistance vessels and systemic venous capacitance vessels. Levosimendan is a selective phosphodiesterase III inhibitor in vitro. The relevance of this at therapeutic concentrations is unclear. In patients with heart failure, the positive inotropic and vasodilatory actions of levosimendan result in an increased contractile force, and a reduction in both preload and after load, without adversely affecting diastolic function. Levosimendan activates stunned myocardium in patients after PTCA or thrombolysis. Levosimendan generates within the recommended dose range one therapeutically active metabolite which produces similar hemodynamic effects to levosimendan. However, these effects last for up to seven to nine days after discontinuation of a 24 hour levosimendan infusion. Levosimendan infusion increases coronary blood flow in patients recovering from coronary surgery and improves myocardial perfusion in patients with heart failure. These benefits are achieved without a significant increase in myocardial oxygen consumption. Treatment with Levosimendan infusion significantly decreases circulating levels of endothelin-1 in patients with congestive heart failure. It does not increase plasma catecholamine levels at recommended infusion rates.Clinical TrialsLevosimendan has been shown to lead to dose-dependent increases in cardiac output and stroke volume as well as dose-dependent decreases in pulmonary capillary wedge pressure, mean arterial pressure and total peripheral resistance. In a double-blind multicenter trial, 203 patients with severe low output heart failure (ejection fraction <0.35, cardiac index <2.5 L/min/m2, pulmonary capillary wedge pressure (PCWP) >15 mmHg) and in need of inotropic support received levosimendan (loading dose 24 mcg/kg over ten minutes followed by a continuous infusion of 0.1 to 0.2 mcg/kg/min) or dobutamine (5 to 10 mcg/kg/min) for 24 hours. The etiology of heart failure was ischemic in 47% of the patients; 45% had idiopathic dilative cardiomyopathy. Seventy-six percent of the patients had dyspnea at rest. Major exclusion criteria included systolic blood pressure below 90 mmHg and heart rate above 120 beats per minute. The primary endpoint was an increase in cardiac output by > 30% and a simultaneous decrease of PCWP by >25% at 24 hours. This was reached in 28% of levosimendan treated patients compared with 15% after dobutamine treatment (p=0.025). Sixty-eight percent of symptomatic patients had an improvement in their dyspnea scores after levosimendan treatment, compared with 59% after dobutamine treatment. Improvement in fatigue scores were 63% and 47% after levosimendan and dobutamine treatment, respectively. All-cause 31 day mortality was 7.8% for levosimendan and 17% for dobutamine treated patients. In a further double-blind multicenter trial carried out primarily to evaluate safety, 504 patients with decompensated heart failure after acute myocardial infarction who were assessed to require inotropic support, were treated with levosimendan or placebo for six hours. There were no significant differences in the incidence of hypotension and ischemia between the treatment groups. No adverse effect on survival up to six months was observed in a retrospective analysis of these two major trials.PharmacokineticsGeneralThe pharmacokinetics of levosimendan are linear in the therapeutic dose range 0.05 to 0.2 mcg/kg/min.DistributionThe volume of distribution of levosimendan (Vss) is approximately 0.2 L/kg. Levosimendan is 97 to 98% bound to plasma proteins, primarily to albumin. The protein binding of the active metabolite (OR-1896) is 40%.MetabolismLevosimendan is completely metabolized and negligible amounts of unchanged parent drug are excreted in urine and feces. Levosimendan is primarily metabolized by conjugation to cyclic or N-acetylated cysteinylglycine and cysteine conjugates. Approximately 5% of the dose is metabolized in the intestine by reduction to aminophenylpyridazinone (OR-1855), which after reabsorption is metabolized by N-acetyltransferase to the active metabolite OR- 1896. The acetylation level is genetically determined. In rapid acetylators, the concentrations of the metabolite OR- 1896 are slightly higher than in slow acetylators. However, this has no implication for the clinical hemodynamic effect at recommended doses. In vitro studies have shown that levosimendan could have a mild inhibitory effect of CYP2D6 (Ki: 5 microM), while levosimendan, OR-1855, and OR-1896 do not inhibit CYP1A2, 2A6, 2C19, 2E1, or 3A4 at concentrations achieved by the recommended dosing. In addition levosimendan does not inhibit CYP1A1, and neither OR-1855 or OR-1896 inhibit CYP2C9 or CYP2D6. The results of drug interaction studies in humans with warfarin, felodipine, and itraconazole confirmed that levosimendan does not inhibit CYP3A4 or CYP2C9.Elimination and excretionClearance is about 3.0 mL/min/kg and the half-life about one hour. Fifty-four percent of the dose is excreted in urine and 44% in feces. More than 95% of the dose is excreted within one week. Negligible amounts (<0.05 % of the dose) are excreted as unchanged levosimendan in the urine. The circulating metabolites OR-1855 and OR-1896 are formed and eliminated slowly. Peak plasma concentration is reached about two days after termination of a levosimendan infusion. The half-lives of the metabolites are about 75 to 80 hours. The elimination of the active metabolite OR-1896 has not been completely investigated. Potential interactions cannot be predicted.Special PopulationsChildren: Limited data indicate that the pharmacokinetics of levosimendan after a single dose in children (age three months to six years) are similar to those in adults. The pharmacokinetics of the active metabolite have not been investigated in children. Levosimendan should not be administered to children.Renal impairment: The pharmacokinetics of levosimendan are similar in healthy subjects and in subjects with mild to moderate renal impairment. The effect of hemodialysis on the pharmacokinetics of levosimendan has not been determined. There is limited data on the pharmacokinetics of the active metabolite in renal impairment.Hepatic impairment: Elimination of levosimendan is slightly reduced in patients with mild hepatic impairment due to cirrhosis. The effect of moderate to severe hepatic impairment on the pharmacokinetics of levosimendan has not been evaluated. The pharmacokinetics of the active metabolite have not been investigated in hepatic impairment.Population analysis has shown no effects of age, ethnic origin or gender on the pharmacokinetics of levosimendan.However, the same analysis revealed that volume of distribution and total clearance are dependent on weight.IndicationsLevosimendan concentrate for solution for infusion is indicated for short-term treatment of acutely decompensated severe chronic heart failure.Levosimendan concentrate for solution for infusion should only be used as add-on therapy in situations where conventional therapy with e.g. diuretics, ACE-inhibitors, and digitalis is not sufficient and where there is a need for inotropic support.Contraindications

77
Hypersensitivity to levosimendan or to any of the excipients. Marked mechanical obstructions affecting ventricular filling or outflow or both. Severe renal impairment (creatinine clearance <30 mL/min) and severe hepatic impairment.Severe hypotension and tachycardia. History of Torsades de Pointes.Side EffectsThe most common adverse reactions in clinical trials were headache and hypotension (both 5%). In levosimendan treated patients, extrasystoles were reported in 1.3% of patients, atrial fibrillation in 1.4%, tachycardia in 2.4%, ventricular tachycardia in 1%, palpitations in 0.9%, and myocardial ischemia in 2%. Of all reported reactions, 83% occurred during levosimendan therapy and 17% after end of therapy. The majority of adverse reactions (98.6%) were seen within three days after start of the infusion.SIMDAX Table 1: Adverse Reactions
Common(>1/100, <1/10)
Red blood cell disorders:Hemoglobin decreaseMetabolic and nutritional disorders:HypokalemiaCentral and peripheral nervous system disorders: DizzinessCardiovascular disorders, general:HypotensionMyo-, endo-, pericardial & valve disorders: myocardial ischemiaHeart rate and rhythm disorders: extrasystoles, fibrillation atrial, tachycardia, tachycardia ventricularGastro-intestinal system disorders: Nausea, vomitingBody as a whole – general disorders: Headache
Uncommon(>1/1000, <1/100)
Heart rate and rhythm disorders:Palpitation
PrecautionsHemodynamically favorable effects on cardiac output and pulmonary capillary wedge pressure persist for at least 24 hours after discontinuation of (a 24-hour) infusion. The exact duration of all hemodynamic effects has not been determined. However, the effects on blood pressure generally last for three to four days, and the effects on heart rate for seven to nine days. This is partly due to the presence of an active metabolite, which reaches its maximum plasma concentration about 48 hours after the infusion has been stopped. Interactions with the elimination of the active metabolite cannot be predicted and could lead to a more pronounced and prolonged effect on heart rate (see Drug Interactions). Non-invasive monitoring for at least three days after the end of infusion or until the patient is clinically stable is recommended. In patients with mild to moderate renal or mild to moderate hepatic impairment monitoring is recommended for at least five days. ECG, blood pressure, and heart rate must be monitored continuously during the treatment and the urine output measured. Symptoms of heart failure should be followed and invasive hemodynamic monitoring is recommended during infusion. Levosimendan infusion should be used cautiously in patients with mild to moderate renal or hepatic impairment. The elimination of the active metabolite has not been investigated in patients with impaired hepatic function and only limited data are available in patients with impaired renal function. Impaired hepatic or renal function may lead to increased concentrations of the metabolite, which may result in a more pronounced and prolonged effect on heart rate. (see Pharmacodynamics) Levosimendan infusion may cause a decrease in serum potassium concentration. Thus, low serum potassium concentrations should be corrected prior to the administration of levosimendan, and serum potassium should be monitored during treatment. As with other medicinal products for heart failure, infusions of levosimendan may be accompanied by decreases in hemoglobin and hematocrit, andcaution should be exercised in patients with ischemic cardiovascular disease and concurrent anemia. Levosimendan infusion should be used cautiously in patients with hypotension, tachycardia or atrial fibrillation with rapid ventricular response. Severe hypovolemia should be corrected prior to levosimendan infusion. If excessive changes in blood pressure or heart rate are observed, the rate of infusion should be reduced or the infusion discontinued. There is limited experience of administration of inotropic agents (except digoxin) concomitantly with levosimendan or after a levosimendan infusion (see Drug Interactions). Thus, such administration is not recommended, and benefit and risk should be assessed for the individual patient. In patients with severely compromised cardiac function, levosimendan must be administered under continuous monitoring of cardiac output and filling pressure. Patients with sustained ventricular tachycardia, nonsustained tachycardia not related to reperfusion, or life-threatening arrhythmia should be treated for the arrhythmia and stabilized prior to administration of levosimendan. Levosimendan concentrate should be used cautiously and under close ECG monitoring in patients with ongoing coronary ischemia, long QTc interval regardless of etiology, or when given concomitantly with medicinal products that prolong the QTc interval. (see OVERDOSAGE) No information is available on the use of levosimendan in the following disorders: restrictive cardiomyopathy, hypertrophic cardiomyopathy, severe mitral valve insufficiency, myocardial rupture, cardiac tamponade, right ventricular infarction, and potentially life threatening arrhythmias within the last three months. There is no experience of use of levosimendan in children and adolescents under 18 years of age. Only limited experience is available on the use of levosimendan in the following conditions and special caution should therefore be exercised: Acute heart failure related to a recent onset of a noncardiac condition; serious deterioration of heart failure after surgery; and severe heart failure in patients awaiting heart transplantation.Pregnancy and LactationThere is no experience of using levosimendan in pregnant women. Animal studies have shown toxic effects on reproduction (see Carcinogenesis, Mutagenesis, and Impairment of Fertility). Therefore, levosimendan should be used in pregnant women only if the benefits for the mother outweigh the possible risks to the fetus.Nursing MothersIt is not known whether levosimendan is excreted in human milk. Therefore, women receiving levosimendan should not breastfeed within 14 days after infusion.OverdosageOverdose of levosimendan may induce hypotension and tachycardia. In clinical trials with levosimendan, hypotension has been successfully treated with vasopressors (e.g., dopamine in patients with congestive heart failure and adrenaline in patients following cardiac surgery). Excessive decreases in cardiac filling pressures may limit the response to levosimendan and can be treated with parenteral fluids. High doses (at or above 0.4 mcg/kg/min) and infusions over 24 hours increase the heart rate and are sometimes associated with prolongation of the QTc interval. In the event of an overdose of levosimendan, continuous ECG monitoring, repeated determinations of serum electrolytes, and invasive hemodynamic monitoring should be undertaken. Levosimendan overdose leads to increased plasma concentrations of the active metabolite, which may lead to a more pronounced and prolonged effect on heart rate requiring a corresponding extension of the observation period.Drug InteractionsIn vitro studies utilizing human liver microsomes have shown that levosimendan is unlikely to cause significant drug-drug interactions with agents metabolized by cytochrome P450 (CYP) enzymes due to its apparent low affinity to various CYP-isoforms. The elimination of the active metabolite has not been completely evaluated, and potential interactions with the elimination of this metabolite cannot be predicted. A possible interaction could lead to a more pronounced and prolonged effect on heart rate. The duration of this effect could be longer than the seven to nine days normally seen after a levosimendan infusion. No pharmacokinetic interactions have been observed in a population

78
analysis of patients receiving digoxin and levosimendan infusion. Levosimendan infusion can be used in patients receiving beta-blocking agents without loss of efficacy. Coadministration of isosorbide mononitrate and levosimendan in healthy volunteers resulted in significant potentiation of the orthostatic hypotensive response. No potentiation of the decrease in blood pressure after concomitant administration of nitrates and levosimendan was found in patients.Carcinogenesis, Mutagenesis, Impairment of FertilityConventional studies on general toxicity and genotoxicity revealed no special hazard for humans in short term use. In animal studies, levosimendan was not teratogenic, but it caused a generalized reduction in the degree of ossification in rat and rabbit fetuses with anomalous development of the supraoccipital bone in the rabbit. When administered before and during early pregnancy, levosimendan decreased the number of corpora lutea, implantations and pups per liter, and increased the number of early resorptionsand post-implantation losses in the female rat. The effects were seen at clinical exposure levels. In animal studies, levosimendan was excreted into maternal milk.IncompatibilitiesThis medicinal product must not be mixed with other medicinal products or diluents except those stated inDosage and Administration/Compatibilities.After DilutionChemical and physical in-use stability has been demonstrated for 24 hours at 25° C. From a microbiological point of view, the product should be used immediately. If not used immediately, in-use storage times and conditions prior to use are the responsibility of the user. Storage and in-use time after dilution should never exceed 24 hours.Dosage AdministrationMethod of AdministrationLevosimendan concentrate is for in-hospital use only. It should be administered in a hospital setting where adequate monitoring facilities and expertise with the use of inotropic agents are available. Levosimendan 2.5 mg/mL concentrate is to be diluted prior to administration. Levosimendan 2.5 mg/mL concentrate for solution for infusion is intended for single use only. As for all parenteral medicinal products, inspect the diluted solution visually for particulate matter and discoloration prior to administration. The color of the concentrate may turn to orange during storage, but there is no loss of potency, and the product may be used until the indicated expiration date if storage instructions have been followed. The infusion can be administered by the peripheral or central intravenous route.DosingThe dose and duration of treatment should be individualized according to the patient’s clinical condition and response. The treatment should be initiated with a loading dose of 12 to 24 mcg/kg infused over ten minutes, followed by a continuous infusion of 0.1 mcg/kg/min. A loading dose of 24 mcg/kg will produce a stronger hemodynamic response but may be associated with a transient increased incidence of adverse reactions. The response of the patient should be assessed after 30 to 60 minutes. If the response is deemed excessive (hypotension, tachycardia), the rate of the infusion may be decreased to 0.05 mcg/kg/min or discontinued. If the initial dose is tolerated and an increased hemodynamic effect is required, the rate of the infusion can be increased to 0.2 mcg/kg/min. The recommended duration of infusion in patients with acute decompensation of severe chronic heart failure is 24 hours. No signs of development of tolerance or rebound phenomena have been observed following discontinuation of levosimendan infusion. Hemodynamic effects persist for at least 24 hours and may be seen up to nine days after discontinuation of a 24 hour infusion.ElderlyNo dose adjustment is required for elderly patients.Renal impairmentLevosimendan must be used with caution in patients with mild to moderate renal impairment. Levosimendan should not be used in patients with severe renal impairment (creatinine clearance <30 mL/min) (see Contraindications, Precautions and Pharmacokinetics).Hepatic impairmentLevosimendan must be used with caution in patients with mild to moderate hepatic impairment Levosimendan should not be used in patients with severe hepatic impairment (see Contraindications, Precautions and Pharmacokinetics).ChildrenLevosimendan should not be administered to children and adolescents under 18 years of age (see Precautions and Pharmacokinetics).There is no experience of repeated administration of levosimendan concentrate and experience of concomitant use with other inotropic agents (except digoxin) is limited. To prepare the 0.05 mg/mL infusion, mix 10 mL of levosimendan 2.5 mg/mL concentrate for solution for infusion with 500 mL of 5% glucose (dextrose) solution. Table provides detailed infusion rates for both the loading and maintenance infusion doses of a 0.05 mg/mL preparation of levosimendan infusion:SIMDAX Table 2. Detailed infusion rates for both the loading and maintenance infusion doses of a 0.05 mg/mL preparation of levosimendan infusionPatient’s Infusion Rate for Loading Continuous Infusion rate (mL/h)
Weight (kg) Dose Infused Over 10 min (mL/h)
12 mcg/kg 24 mcg/kg 0.05 mcg/kg/min 0.1 mcg/kg/min 0.2 mcg/kg/min
40 58 mL/h 115 mL/h 2 5 1050 72 144 3 6 1260 86 173 4 7 1470 101 202 4 8 1780 115 230 5 10 1990 130 259 5 11 22100 144 288 6 12 24110 158 317 7 13 26120 173 346 7 14 29 To prepare the 0.025 mg/mL infusion, mix 5 mL of levosimendan 2.5 mg/mL concentrate for solution for infusion with 500 mL of 5% glucose (dextrose) solution. Table 3 provides detailed infusion rates for both the loading and maintenance infusion doses for a 0.025 mg/mL preparation of levosimendan infusion:SIMDAX Table 3. Detailed infusion rates for both the loading and maintenance infusion dosesfor a 0.025 mg/mL preparation of levosimendan infusionPatient’s Infusion Rate for Loading Continuous Infusion rate (mL/h)
Weight (kg) Dose Infused Over 10 min (mL/h)
12 mcg/kg 24 mcg/kg 0.05 mcg/kg/min 0.1 mcg/kg/min 0.2 mcg/kg/min

79
40 115 mL/h 230 mL/h 5 10 1950 144 288 6 12 2460 173 346 7 14 2970 202 403 8 17 3480 230 461 10 19 3890 259 518 11 22 43100 288 576 12 24 48110 317 634 13 26 53120 346 691 14 29 58 CompatibilitiesThe following medicinal products can be given simultaneously with levosimendan in connected intravenous lines:- Furosemide 10 mg/mL- Digoxin 0.25 mg/mL- Nitroglycerine (or Glyceryl trinitrate) 0.1 mg/mLStorageTwo years if stored as recommendedStore at 2 to 8° C (36 to 46° F) in a refrigerator. Do not freeze.The color of the concentrate may turn to orange during storage, but there is no loss of potency, and the product may be used until the indicated expiration date if storage instructions have been followed.Packaging- 5 or 10 mL, Type I glass vials containing 2.5 mg levosimendan/mL.- Chlorobutyl Rubber Closure with Fluoropolymer Coating.Packaging Sizes- 1, 4, 10 vials of 5 mL- 1, 4, 10 vials of 10 mL
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
SURVANTA ®General(beractant)intratracheal suspensionSterile Suspension for Intratracheal Administration OnlyCompositionSURVANTA (beractant) Intratracheal Suspension is a sterile, non-pyrogenic pulmonary surfactant intended for intratracheal use only. It is a natural bovine lung extract containing phospholipids, neutral lipids, fatty acids, and surfactant-associated proteins to which colfosceril palmitate (dipalmitoylphosphatidylcholine), palmitic acid, and tripalmitin are added to standardize the composition and to mimic surface-tension lowering properties of natural lung surfactant. The resulting composition provides 25 mg/mL phospholipids (including 11.0-15.5 mg/mL disaturated phosphatidylcholine), 0.5-1.75 mg/mL triglycerides, 1.4-3.5 mg/mL free fatty acids, and less than 1.0 mg/mL protein. It is suspended in 0.9% sodium chloride solution, and heat-sterilized. SURVANTA contains no preservatives. Its protein content consists of two hydrophobic, low molecular weight, surfactantassociated proteins commonly known as SP-B and SP-C. It does not contain the hydrophilic, large molecular weight surfactant-associated protein known as SP-A. Each mL of SURVANTA contains 25 mg of phospholipids. It is an off-white to light brown liquid supplied in single-use glass vials containing 4 mL (100 mg phospholipids) or 8 mL (200 mg phospholipids).PropertiesClinical PharmacologyEndogenous pulmonary surfactant lowers surface tension on alveolar surfaces during respiration and stabilizes the alveoli against collapse at resting transpulmonary pressures. Deficiency of pulmonary surfactant causes Respiratory Distress Syndrome (RDS) in premature infants. SURVANTA replenishes surfactant and restores surface activity to the lungs of these infants.ActivityIn vitro, SURVANTA reproducibly lowers minimum surface tension to less than 8 dynes/cm as measured by the pulsating bubble surfactometer and Wilhelmy Surface Balance. In situ, SURVANTA restores pulmonary compliance to excised rat lungs artificially made surfactant-deficient. In vivo, single SURVANTA doses improve lung pressure-volume measurements, lung compliance, and oxygenation in premature rabbits and sheep.Animal MetabolismSURVANTA is administered directly to the target organ, the lungs, where biophysical effects occur at the alveolar surface. In surfactant-deficient premature rabbits and lambs, alveolar clearance of radio-labelled lipid components of SURVANTA is rapid. Most of the dose becomes lung-associated within hours of administration, and the lipids enter endogenous surfactant pathways of reutilization and recycling. In surfactant-sufficient adult animals, SURVANTA clearance is more rapid than in premature and young animals. There is less reutilization and recycling of surfactant in adult animals.Limited animal experiments have not found effects of SURVANTA on endogenous surfactant metabolism. Precursor incorporation and subsequent secretion of saturated phosphatidylcholine in premature sheep are not changed by SURVANTA treatments.No information is available about the metabolic fate of the surfactant-associated proteins in SURVANTA. The metabolic disposition in humans has not been studied.Clinical StudiesClinical effects of SURVANTA were demonstrated in six single-dose and four multiple-dose randomized, multi-center, controlled clinical trials involving approximately 1700 infants. Three open trials, including a Treatment IND, involved more than 8500 infants. Each dose of SURVANTA in all studies was 100 mg phospholipids/ kg birth weight and was based on published experience with Surfactant TA, a lyophilized powder dosage form of SURVANTA having the same composition.Prevention StudiesInfants of 600-1250 g birth weight and 23 to 29 weeks estimated gestational age were enrolled in two multiple-dose studies. A dose of SURVANTA was given within 15 minutes of birth to prevent the development of RDS. Up to three additional doses in the first 48 hours, as often as every 6 hours, were given if RDS subsequently developed and infants required mechanical ventilation with an FiO2 ≥ 0.30. Results of the studies at 28 days of age are shown in Table 1.SURVANTA Table 1. Results of the studies at 28 days of ageStudy 1Number infants studied SURVANTA Control P-Value

80
Incidence of RDS (%)Death due to RDS (%)Death or BPD due to RDS (%)Death due to any cause (%)Air Leaksa (%)Pulmonary interstitial emphysema (%)
11927.62.548.77.65.920.8
12463.519.552.822.821.740.0
<0.001<0.0010.5360.0010.0010.001
Study 2b
Number infants studiedIncidence of RDS (%)Death due to RDS (%)Death or BPD due to RDS (%)Death due to any causec (%)Air Leaksa (%)Pulmonary interstitial emphysema (%)
SURVANTA9128.61.127.516.514.526.5
Control9648.310.544.213.719.633.2
P-Value0.0070.0060.0180.6330.3740.298
a Pneumothorax or pneumopericardiumb Study discontinued when Treatment IND initiatedc No cause of death in the SURVANTA group was significantly increased; the higher number of deaths in this group was due to the sum of all causes.Rescue Studies0.30. Results of the studies at 28 days of age are shown in Table 2. Infants of 600-1750 g birth weight with RDS requiring mechanical ventilation and an FiO2 ≥ 0.40 were enrolled in two multiple-dose rescue studies. The initial dose of SURVANTA was given after RDS developed and before 8 hours of age. Infants could receive up to three additional doses in the first 48 hours, as often as every 6 hours, if they required mechanical ventilation and an FiO2 ≥SURVANTA Table 2. . Results of the studies at 28 days of ageStudy 3a
Number infants studiedDeath due to RDS (%)Death or BPD due to RDS (%)Death due to any cause (%)Air Leaksb(%)Pulmonary interstitial emphysema (%)
SURVANTA19811.659.121.711.816.3
Control19318.166.826.429.534.0
P-Value0.0710.1020.285<0.001<0.001
Study 4
Number infants studied Death due to RDS (%)Death or BPD due to RDS (%)Death due to any cause (%)Air Leaks b (%)Pulmonary interstitial emphysema (%)
SURVANTA2046.443.615.211.220.8
Control20322.363.428.22.244.4
P-Value<0.001<0.0010.0010.005<0.001
a Study discontinued when Treatment IND initiatedb Pneumothorax or pneumopericardiumAcute Clinical EffectsMarked improvements in oxygenation may occur within minutes of administration of SURVANTA. All controlled clinical studies with SURVANTA provided information regarding the acute effects of SURVANTA on the arterial-alveolar oxygen ratio (a/APO2), FiO2, and mean airway pressure (MAP) during the first 48 to 72 hours of life. Significant improvements in these variables were sustained for 48-72 hours in SURVANTA-treated infants in four single-dose and two multiple-dose rescue studies and in two multiple-dose prevention studies. In the single-dose prevention studies, the FiO2 improved significantly.IndicationsSURVANTA is indicated for prevention and treatment (“rescue”) of Respiratory Distress Syndrome (RDS) (hyaline membrane disease) in premature infants. SURVANTA significantly reduces the incidence of RDS, mortality due to RDS and air leak complications.ContraindicationsNone known.PreventionIn premature infants less than 1250 g birth weight or with evidence of surfactant deficiency, give SURVANTA as soon as possible, preferably within 15 minutes of birth.RescueTo treat infants with RDS confirmed by x-ray and requiring mechanical ventilation, give SURVANTA as soon as possible, preferably by 8 hours of age.Side EffectsThe most commonly reported adverse experiences were associated with the dosing procedure. In the multiple-dose controlled clinical trials, each dose of SURVANTA was divided into four quarter-doses which were instilled through a catheter inserted into the endotracheal tube by briefly disconnecting the endotracheal tube from the ventilator. Transient bradycardia occurred with 11.9% of doses. Oxygen desaturation occurred with 9.8% of doses. Other reactions during the dosing procedure occurred with fewer than 1% of doses and included endotracheal tube reflux, pallor, vasoconstriction, hypotension, endotracheal tube blockage, hypertension, hypocarbia, hypercarbia, and apnea. No deaths occurred during the dosing procedure, and all reactions resolved with symptomatic treatment. The occurrence of concurrent illnesses common in premature infants was evaluated in the controlled trials. The rates in all controlled studies are in Table 3.SURVANTA Table 3. Side effect rates in all controlled studies
All Controlled StudiesSURVANTA
Control

81
Concurrent Event (%) (%) P-Valuea
Patent ductus arteriosus 46.9 47.1 0.814Intracranial hemorrhage 48.1 45.2 0.241Severe intracranial hemorrhage 24.1 23.3 0.693Pulmonary air leaks 10.9 24.7 <0.001Pulmonary interstitial emphysema 20.2 38.4 <0.001
Necrotizing enterocolitis 6.1 5.3 0.427Apnea 65.4 59.6 0.283Severe apnea 46.1 42.5 0.114Post-treatment sepsis 20.7 16.1 0.019Post-treatment infection 10.2 9.1 0.345Pulmonary hemorrhage 7.2 5.3 0.166a P-value comparing groups in controlled studiesWhen all controlled studies were pooled, there was no difference in intracranial hemorrhage. However, in one of the single-dose rescue studies and one of the multiple-dose prevention studies, the rate of intracranial hemorrhage was significantly higher in SURVANTA patients than control patients (63.3% v 30.8%, P = 0.001; and 48.8% v 34.2%, P = 0.047, respectively). The rate in a Treatment IND involving approximately 8100 infants was lower than in the controlled trials. In the controlled clinical trials, there was no effect of SURVANTA on results of common laboratory tests: white blood cell count and serum sodium, potassium, bilirubin, creatinine. More than 4300 pretreatment and post-treatment serum samples from approximately 1500 patients were tested by Western Blot Immunoassay for antibodies to surfactant-associated proteins SP-B and SP-C. No IgG or IgM antibodies were detected. Several other complications are known to occur in premature infants. The following conditions were reported in the controlled clinical studies. The rates of the complications were not different in treated and control infants, and none of the complications were attributed to SURVANTA. Respiratory: lung consolidation, blood from the endotracheal tube, deterioration after weaning, respiratory decompensation, subglottic stenosis, paralyzed diaphragm, respiratory failure.Cardiovascular: hypotension, hypertension, tachycardia, ventricular tachycardia, aortic thrombosis, cardiac failure, cardio-respiratory arrest, increased apical pulse, persistent fetal circulation, air embolism, total anomalous pulmonary venous return.Gastrointestinal: abdominal distention, hemorrhage, intestinal perforations, volvulus, bowel infarct, feeding intolerance, hepatic failure, stress ulcer.Renal: renal failure, hematuria.Hematologic: coagulopathy, thrombocytopenia, disseminated intravascular coagulation.Central Nervous System: seizures.Endocrine/Metabolic: adrenal hemorrhage, inappropriate ADH secretion, hyperphosphatemia.Musculoskeletal: inguinal hernia.Systemic: fever, deterioration.Follow-Up EvaluationsTo date, no long-term complications or sequelae of SURVANTA therapy have been found.Single-Dose StudiesSix-month adjusted-age follow-up evaluations of 232 infants (115 treated) demonstrated no clinically important differences between treatment groups in pulmonary and neurologic sequelae, incidence or severity of retinopathy of prematurity, rehospitalizations, growth, or allergic manifestations.Multiple-Dose StudiesSix-month adjusted age follow-up evaluations have been completed in 631 (345 treated) of 916 surviving infants. There were significantly less cerebral palsy and need for supplemental oxygen in SURVANTA infants than controls. Wheezing at the time of examination was significantly more frequent among SURVANTA infants, although there was no difference in bronchodilator therapy. Final twelve-month follow-up data from the multiple-dose studies are available from 521 (272 treated) of 909 surviving infants. There was significantly less wheezing in SURVANTA infants than controls, in contrast to the six-month results. There was no difference in the incidence of cerebral palsy at twelve months.Twenty-four month adjusted age evaluations were completed in 429 (226 treated) of 906 surviving infants. There were significantly fewer SURVANTA infants with rhonchi, wheezing, and tachypnea at the time of examination. No other differences were found.PrecautionsSURVANTA is intended for intratracheal use only. SURVANTA CAN RAPIDLY AFFECT OXYGENATION AND LUNG COMPLIANCE.Therefore, its use should be restricted to a highly supervised clinical setting with immediate availability of clinicians experienced with intubation, ventilator management, and general care of premature infants. Infants receiving SURVANTA should be frequently monitored with arterial or transcutaneous measurement of systemic oxygen and carbon dioxide. DURING THE DOSING PROCEDURE, TRANSIENT EPISODES OF BRADYCARDIA AND DECREASED OXYGEN SATURATION HAVE BEEN REPORTED. If these occur, stop the dosing procedure and initiate appropriate measures to alleviate the condition. After stabilization, resume the dosing procedure.GeneralRales and moist breath sounds can occur transiently after administration. Endotracheal suctioning or other remedial action is not necessary unless clearcut signs of airway obstruction are present. Increased probability of post-treatment nosocomial sepsis in SURVANTA treated infants was observed in the controlled clinical trials (Table 3). The increased risk for sepsis among SURVANTA-treated infants was not associated with increased mortality among these infants. The causative organisms were similar in treated and control infants. There was no significant difference between groups in the rate of post-treatment infections other than sepsis. Use of SURVANTA in infants less than 600 g birth weight or greater than 1750 g birth weight has not been evaluated in controlled trials. There is no controlled experience with use of SURVANTA in conjunction with experimental therapies for RDS (eg, high-frequency ventilation or extracorporeal membrane oxygenation). No information is available on the effects of doses other than 100 mg phospholipids/kg, more than four doses, dosing more frequently than every 6 hours, or administration after 48 hours of age.Carcinogenesis, Mutagenesis, Impairment of FertilityCarcinogenicity studies have not been performed with SURVANTA. SURVANTA was negative when tested in the Ames test for mutagenicity. Using the maximum feasible dose volume, SURVANTA up to 500 mg phospholipids/kg/day (approximately one-third the premature infant dose based on mg/m2/day) was administered subcutaneously to newborn rats for 5 days. The rats reproduced normally and there were no observable adverse effects in their offspring.OverdosageOverdosage with SURVANTA has not been reported. Based on animal data, overdosage might result in acute airway obstruction. Treatment should be symptomatic and supportive.Rales and moist breath sounds can transiently occur after SURVANTA is given, and do not indicate overdosage. Endotracheal suctioning or other remedial action is not required unless clear-cut signs of airway obstruction are present.

82
Dosage AdministrationFor intratracheal administration only. SURVANTA should be administered by or under the supervision of clinicians experienced in intubation, ventilator management, and general care of premature infants. Marked improvements in oxygenation may occur within minutes of administration of SURVANTA. Therefore, frequent and careful clinical observation and monitoring of systemic oxygenation are essential to avoid hyperoxia. Review of audiovisual instructional materials describing dosage and administration procedures is recommended before using SURVANTA. Materials are available upon request from Ross Products Division.Each dose of SURVANTA is 100 mg of phospholipids/kg birth weight (4 mL/kg).The SURVANTA Dosing Chart shows the total dosage for a range of birth weights.SURVANTA Table 4. Survanta dosing chart
WEIGHT(grams)
TOTAL DOSE(mL)
WEIGHT(grams)
TOTAL DOSE(mL)
600- 650 2.6 1301- 1350 5.4
651- 700 2.8 1351- 1400 5.6
701- 750 3.0 1401- 1450 5.8
751- 800 3.2 1451- 1500 6.0
801- 850 3.4 1501- 1550 6.2
851- 900 3.6 1551- 1600 6.4
901- 950 3.8 1601- 1650 6.6
951- 1000 4.0 1651- 1700 6.8
1001- 1050 4.2 1701-
1750 7.0
1051- 1100 4.4 1751-
1800 7.2
1101- 1150 4.6 1801-
1850 7.4
1151- 1200 4.8 1851-
1900 7.6
1201- 1250 5.0 1901-
1950 7.8
1251- 1300 5.2 1951-
2000 8.0
Four doses of SURVANTA can be administered in the first 48 hours of life. Doses should be given no more frequently than every 6 hours.Directions for UseC). Date and time need to be recorded in the box on front of the carton or vial, whenever SURVANTA is removed from the refrigerator. Before administration, SURVANTA should be warmed by standing at room temperature for at least 20 minutes or warmed in the hand for at least 8 minutes. ARTIFICIAL WARMING METHODS SHOULD NOT BE USED. If a prevention dose is to be given, preparation of SURVANTA should begin before the infant’s birth.°SURVANTA should be inspected visually for discoloration prior to administration. The color of SURVANTA is off-white to light brown. If settling occurs during storage, swirl the vial gently (DO NOT SHAKE) to redisperse. Some foaming at the surface may occur during handling and is inherent in the nature of the product. SURVANTA is stored refrigerated (2-8Unopened, unused vials of SURVANTA that have been warmed to room temperature may be returned to the refrigerator within 24 hours of warming, and stored for future use. SURVANTA SHOULD NOT BE REMOVED FROM THE REFRIGERATOR FOR MORE THAN 24 HOURS. SURVANTA SHOULD NOT BE WARMED AND RETURNED TO THE REFRIGERATOR MORE THAN ONCE. Each single-use vial of SURVANTA should be entered only once. Used vials with residual drug should be discarded. SURVANTA DOES NOT REQUIRE RECONSTITUTION OR SONICATION BEFORE USE.Dosing ProceduresGeneralSURVANTA is administered intratracheally by instillation through a 5 French endhole catheter. The catheter can be inserted into the infant’s endotracheal tube without interrupting ventilation by passing the catheter through a neonatal suction valve attached to the endotracheal tube. Alternatively, SURVANTA can be instilled through the catheter by briefly disconnecting the endotracheal tube from the ventilator. The neonatal suction valve used for administering SURVANTA should be a type that allows entry of the catheter into the endotracheal tube without interrupting ventilation and also maintains a closed airway circuit system by sealing the valve around the catheter. If the neonatal suction valve is used, the catheter should be rigid enough to pass easily into the endotracheal tube. A very soft and pliable catheter may twist or curl within the neonatal suction valve. The length of the catheter should be shortened so that the tip of the catheter protrudes just beyond the end of the endotracheal tube above the infant’s carina. SURVANTA should not be instilled into a mainstem bronchus.To ensure homogenous distribution of SURVANTA throughout the lungs, each dose is divided into four quarter-doses. Each quarter-dose is administered with the infant in a different position. The recommended positions are:- Head and body inclined 5-10 down, head turned to the right- Head and body inclined 5-10 down, head turned to the left- Head and body inclined 5-10 up, head turned to the right- Head and body inclined 5-10 up, head turned to the leftThe dosing procedure is facilitated if one person administers the dose while another person positions and monitors the infant.First DoseDetermine the total dose of SURVANTA from the SURVANTA dosing chart based on the infant’s birth weight. Slowly withdraw the entire contents of the vial into a plastic syringe through a large-gauge needle (eg, at least 20 gauge). DO NOT FILTER SURVANTA AND AVOID SHAKING.Attach the premeasured 5 French end-hole catheter to the syringe. Fill the catheter with SURVANTA. Discard excess SURVANTA through the catheter so that only the total dose to be given remains in the syringe.

83
BEFORE ADMINISTERING SURVANTA, assure proper placement and patency of the endotracheal tube. At the discretion of the clinician, the endotracheal tube may be suctioned before administering SURVANTA. The infant should be allowed to stabilize before proceeding with dosing.In the prevention strategy, weigh, intubate and stabilize the infant. Administer the dose as soon as possible after birth, preferably within 15 minutes. Position the infant appropriately and gently inject the first quarter-dose through the catheter over 2-3 seconds.After administration of the first quarter-dose, remove the catheter from the endotracheal tube. Manually ventilate with a hand-bag with sufficient oxygen toprevent cyanosis, at a rate of 60 breaths/minute, and sufficient positive pressure to provide adequate air exchange and chest wall excursion.In the rescue strategy, the first dose should be given as soon as possible after the infant is placed on a ventilator for management of RDS. In the clinical trials, immediately before instilling the first quarter-dose, the infant’s ventilator settings were changed to rate 60/minute, inspiratory time 0.5 second, and FiO2 1.0.Position the infant appropriately and gently inject the first quarter-dose through the catheter over 2-3 seconds. After administration of the first quarterdose, remove the catheter from the endotracheal tube and continue mechanical ventilation.In both strategies, ventilate the infant for at least 30 seconds or until stable. Reposition the infant for instillation of the next quarter-dose. 00Instill the remaining quarter-doses using the same procedures. After instillation of each quarter-dose, remove the catheter and ventilate for at least 30 seconds or until the infant is stabilized. After instillation of the final quarter-dose, remove the catheter without flushing it. Do not suction the infant for 1 hour after dosing unless signs of significant airway obstruction occur.AFTER COMPLETION OF THE DOSING PROCEDURE, RESUME USUAL VENTILATOR MANAGEMENT AND CLINICAL CARE.Repeat DosesThe dosage of SURVANTA for repeat doses is also 100 mg phospholipids/kg and is based on the infant’s birth weight. The infant should not be reweighed for determination of the SURVANTA dosage. Use the SURVANTA DOSING CHART to determine the total dosage. The need for additional doses of SURVANTA is determined by evidence of continuing respiratory distress. Using the following criteria for redosing, significant reductions in mortality due to RDS were observed in the multipledose clinical trials with SURVANTA.Dose no sooner than 6 hours after the preceding dose if the infant remains intubated and requires at least 30% inspired oxygen to maintain a PaO2 less than or equal to 80 torr.Radiographic confirmation of RDS should be obtained before administering additional doses to those who received a prevention dose.Prepare Survanta and position the infant for administration of each quarter-dose as previously described. After instillation of each quarter-dose, remove the dosing catheter from the endotracheal tube and ventilate the infant for at least 30 seconds or until stable.In the clinical studies, ventilator settings used to administer repeat doses were different than those used for the first dose. For repeat doses, the FiO2 was increased by 0.20 or an amount sufficient to prevent cyanosis. The ventilator delivered a rate of 30/minute with an inspiratory time less than 1.0 second. If the infant’s pretreatment rate was 30 or greater, it was left unchanged during SURVANTA instillation.Manual hand-bag ventilation should not be used to administer repeat doses.DURING THE DOSING PROCEDURE, VENTILATOR SETTINGS MAY BE ADJUSTED AT THE DISCRETION OF THE CLINICIAN TO MAINTAIN APPROPRIATE OXYGENATION AND VENTILATION. AFTER COMPLETION OF THE DOSING PROCEDURE, RESUME USUAL VENTILATOR MANAGEMENT AND CLINICAL CARE.Dosing PrecautionsIf an infant experiences bradycardia or oxygen desaturation during the dosing procedure, stop the dosing procedure and initiate appropriate measures to alleviate the condition. After the infant has stabilized, resume the dosing procedure.Rales and moist breath sounds can occur transiently after administration of Survanta. Endotracheal suctioning or other remedial action is unnecessary unless clear-cut signs of airway obstruction are present.PackagingSurvanta (beractant) Intratracheal Suspension is supplied in single-use glass vials containing 4 mL (NDC 0074-1040-04) or 8 mL of Survanta (NDC 0074- 1040-08). Each milliliter contains 25 mg of phospholipids suspended in 0.9% sodium chloride solution. The color is off-white to light brown.Store unopened vials at refrigeration temperature (2-8˚C). Protect from light. Store vials in carton until ready for use. Vials are for single use only. Upon opening, discard unused drug.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
SYNAGIS ®GeneralPropertiesPharmacodynamicPalivizumab is a humanized IgG1 monoclonal antibody directed to an epitope in the A antigenic site of the fusion protein of respiratory synctial virus (RSV). This humanized monoclonal antibody is composed of human (95%) and murine (5%) antibody sequences. It has potent neutralizing and fusion-inhibitory activity against both RSV subtype A and B strains.Palivizumab serum concentrations of approximately 30mcg/ml have been shown to produce a mean 99% reduction in pulmonary RSV replication in the cotton rat model.PharmacokineticIn studies in adult volunteers, Palivizumab had a pharmacokinetic profile similar to a human IgG1 antibody with regard to volume of distribution (mean 57mL/kg) and half-life (mean 18 days). In prophylactic studies in premature and bronchopulmonary dysplasia paediatric populations, the mean half-life of Palivizumab was 20 days and monthly intramuscular doses of 15mg/kg achieved mean 30 day trough serum drug concentrations of approximately 40mcg/ml after the first injection, approximately 60mcg/ml after the second injection, and approximately 70mcg/ml after the third and fourth injection.In the congenital heart disease study, monthly intramuscular doses of 15 mg/kg achieved mean 30 day trough serum drug concentrations of approximately 55 mcg/ml after the first injection and approximately 90 mcg/ml after the fourth injection.Among 139 children in the congenital heart disease study receiving palivizumab who had cardio-pillmonary bypass and for whom paired serum samples were available, the mean serum palivizumab concentration was approximately 100mcg/ml pre-cardiac bypass and declined to approximately 40mcg/ml after bypass.IndicationsSynagis® is indicated for the prevention of serious lower respiratory tract disease requiring hospitalization caused by respiratory synctial virus (RSV) in pediatric patients at high risk of RSV disease:Children born at 35 weeks of gestation or less and less than 6 months of age at the onset of the RSV seasonChildren less than 2 years of age and requiring treatment for bronchopulmonary dysplasia within the last 6 monthsChildren less than 2 years of age with haemodynamically significant congenital hear diseaseContraindicationsPalivizumab is contraindicated in patients with known hypersensitivity to palivizumab or any component of the formulation , or other humanized monoclonal antibodies.Side Effects

84
Adverse drug reactions (ADRs) reported in the prophylactic paediatric studies were similar in the placebo and palivizumab groups. The majority of ADRs were transient and mild to moderate in severity.Adverse events at least possibly casually-related to palivizumab, both clinical and laboratory are displayed by system organ class and frequency (common>1/100 ≤ 1/10; uncommon >1/1000 ≤ 1/100) in studies conducted in premature and bronchopulmonary dysplasia paediatric patients, and congenital heart disease patients (Tables 1 and 2, respectively).SYNAGIS TABLE 1 Undesirable Effects in Prophylactic Clinical Studies with Premature and Bronchopulmonary Dysplasia Paediatric Population
Infections and Infestations Uncommon Upper Respiratory InfectionViral Infection
Blood and lymphatic system disorders Uncommon LeucopaeniaPyschiatric disorders Uncommon Nervousness
Respiratory,thoracic and mediastinal disorders UncommonRhinitisCoughWheeze
Gastrointestinal disorders Uncommon DiarrhoeaVomiting
Skin and subcutaneous tissue disorders Uncommon Rash
General disorders and administration site conditions UncommonFeverInjection Site reactionPain
Investigations UncommonAST increaseAbnormal liver function testALT increase
SYNAGIS TABLE 2. Undesirable Effects in the Prophylactic Paediatric Congenital Heart Disease Clinical Study
Infections and Infestations Uncommon Upper Respiratory InfectionGasteroenteritis
Pyschiatric disorders Uncommon Nervousness
Nervous system Uncommon SomnolenceHyperkinesia
Vascular disorders Uncommon HaemorrhageRespiratory,thoracic and mediastinal disorders Uncommon Rhinitis
Gastrointestinal disorders UncommonDiarrhoeaVomitingConstipation
Skin and subcutaneous tissue disorders Uncommon RashEczema
General disorders and administrationsite conditions Uncommon
Injection Site reactionFeverAsthenia
No medically important differences were observed during the prophylactic studies carried out in the premature and bronchopulmonary dysplasia paediatric populations in ADRs by body system or when evaluated in subgroups of children by clinical category, gender, age, gestational age, country, race/ethnicity or quartile serum palivizumab concentration.No significant difference in safety profile was observed between children without active RSV infection and those hospitalized for RSV. Permanent discontinuation of palivizumab due to ADRs was rare (0.2%). Deaths were balanced between the integrated placebo and palivizumab groups and were not drug-related.In the congenital heart disease study, no medically important differences were observed in ADRs by body system or when evaluated in subgroups of children by clinical category. The incidence of serious adverse events was significantly lower in the palivizumab group compared to the placebo group. No serious adverse events related to palivizumab were reported. The incidence of cardiac surgeries classified as planned, earlier than planned or urgent were balanced between the groups. Deaths associated with RSV infection occurred in 2 patients in the palivizumab group and 4 patients in the placebo group and were not drug-related.Rare ADRs (> 1/10,000, < 1/1,000): apnoeaVery rare ADRs (< 1/10,000): anaphylaxis, urticariaPost-marketing serious spontaneous adverse events reported during palivizumab treatment between 1998 and 2002 covering four RSV seasons were evaluated. A total of 1291 serious reports were received where palivizumab had been administered as indicated and the duration of therapy was within one season. The onset of the adverse event occurred after the sixth or greater dose in only 22 of these reports (15 after the sixth dose, 6 after the seventh doses and 1 after the eight dose). These events are similar in character to those after the initial five doses.Palivizumab treatment schedule and adverse events were monitored in a group of nearly 20,000 infants tracked through a patient compliance registry between 1998 and 2000. Of this group 1250 enrolled infants had 6 injections, 183 infants had 7 injections, and 27 infants had either 8 or 9 injections. Adverse events observed in patients after a sixth or greater dose were similar in character and frequency to those after the initial 5 doses.Human anti-human antibody (HAHA) response:Antibody to palivizumab was observed in approximately 1% of patients in the IMpact-RSV during the first course of therapy. This was transient, low titre, resolved despite continued use (first and second season), and could not be detected in 55/56 infants during the second season (including 2 with titres during the first season). Therefore, HAHA responses appear to be of no clinical relevance.Immunogenicity was not studied in the congenital heart disease study.PrecautionsAllergic reactions including very rare anaphylaxis have been reported following palivizumab administration (see Undesirable effects, Post marketing experience).Medications for the treatment of severe hypersensitivity reactions, including anaphylaxis should be available for immediate use following administration of palivizumab.

85
A moderate to severe acute infection of febrile illness may warrant delaying the use of palivizumab, unless, in the opinion of the physician, withholding palivizumab entails a greater risk. A mild febrile illness, such as mild upper respiratory infection, is not usually reason to deter administration of palivizumab.As with any other intramuscular injection, palivizumab should be given with caution to patients with thrombocytopaenia or any coagulation disorder.The single-use vial of palivizumab does not contain a preservative. Injections should be given within 3 hours after reconstitution.The efficacy of palivizumab when administered to patients as a second course of treatment during an ensuing RSV season has not been formally investigated in a study performed with this objective. The possible risk of enhanced RSV infection in the season following the season in which the patients were treated with palivizumab has not been conclusively ruled out by studies performed aiming at this particular point.Interactions with other medicinal products and other forms of interactionNo formal drug-drug interactions studies were conducted, however no interactions have been described to date. In the phase III Impact-RSV study in the premature and bronchopulmonary dysplasia paediatric populations, the proportions of patients in the placebo and palivizumab groups who received routine childhood vaccines, influenza vaccine,bronchodilators or corticosteroids were similar and no incremental increase in adverse reactions was observed among patients receiving these agents.Since the monoclonal antibody is specific for RSV, palivizumab is not expected to interfere with the immune response to vaccines.Pregnancy and LactationNot applicableEffect on ability to drive and use of machineNot applicableOverdosageIn clinical studies, three children received an overdose of more than 15mg/kg. These doses were 20.25mg/kg,21.1 mg/kg and 22.27 mg/kg. No medical consequences were identified in these instances.IncompatibilitiesPalivizumab should not be mixed with any medications or diluents other than Water for Injections.Dosage AdministrationRecommended doseThe recommended dose of Synagis ® is 15mg/kg of body weight, given once a month during anticipated periods of RSV risk in the community. Where possible, the first dose should be administered prior to commencement of the RSV season. Subsequent doses should be administered monthly throughout the RSV season.The majority of experience including the pivotal phase III clinical trials with palivizumab has been gained with 5 injections during one season (see Pharmacodynamic properties). Data, although limited, are available on greater than 5 doses (see Undesirable Effects and Pharmacodynamic properties), therefore the benefit in terms of protection beyond 5 doses has not been established.To reduce risk of rehospitalisation, it is recommended that children receiving palivizumab, who are hospitalized with RSV continue to receive monthly doses of palivizumab for the duration of the RSV season.For the children undergoing cardiac bypass, it is recommended that a 15mg/kg injection of palivizumab be administered as soon as stable after surgery to ensure adequate palivizumab serum levels. Subsequent doses should resume monthly through the remainder of the RSV season for children that continue to be high risk of RSV disease (see Pharmacokinetic properties)Method of AdministrationPalivizumab is administered in a dose of 15mg/kg once a month intramuscularly, preferably in the anterolateral aspect of the thigh. The gluteal muscle should not be used routinely as an injection site because of the risk of damage to the sciatic nerve. The injection should be given using aseptic technique. Injection volumes over 1ml should be given as divided dose.For information on reconstituting Synagis, see “Instructions for Handling”Instructions for Use, Handling and DisposalSLOWLY add 0.6 ml of Water for Injections for the 50mg vial or 1.0ml of Water for Injections for the 100mg vial along the inside wall of the vial to minimise foaming. After the water is added, tilt the vial slightly and gently rotate the vial for 30 seconds. DO NOT SHAKE VIAL. Palivizumab solution should stand at room temperature for a minimum of 20 minutes until the solution clarifies. Palivizumab solution does not contain a preservative and should be administered within 3 hours of preparation. Any remaining contents should be discarded after use.When reconstituted as recommended, the final concentration is 100 mg/ml.StorageShelf life is 3 years.Solution: must be administered within 3 hours of preparation.Store in a refrigerator (2ºC to 8ºC). Do not freeze.Store in the original container.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
TARKA 180/2 ®GeneralCompositionTarka 180 mg/2 mgEach tablet contains 180 mg of verapamil hydrochloride and 2 mg of trandolapril.Pink, oval, marked with the Knoll logo and “182” on one sidePropertiesModified-release tabletPharmacodynamicTarka is a fixed combination of the heart-rate lowering calcium antagonist verapamil and the ACE inhibitor trandolapril.VerapamilThe pharmacologic action of verapamil is due to inhibition of the influx of calcium ions through the slow channels of the cell membrane of vascular smooth muscle cells and of the conductile and contractile cells in the heart.The mechanism of action of verapamil produces the following effects:1. Arterial vasodilation.Verapamil reduces arterial pressure both at rest and at a given level of exercise by dilating peripheral arterioles. This reduction in total peripheral resistance (afterload) reduces myocardial oxygen requirements and energy consumption.2. Reduction of myocardial contractility.The negative inotropic activity of verapamil can be compensated by the reduction in total peripheral resistance. The cardiac index will not be decreased unless in patients with preexisting left ventricular dysfunction.Verapamil does not interfere with sympathetic regulation of the heart because it does not block the beta-adrenergic receptors. Spastic bronchitis and similar conditions, therefore, are not contraindications to verapamil.Trandolapril

86
Trandolapril suppresses the plasma renin-angiotensin-aldosterone system (RAS). Renin is an endogenous enzyme synthesized by the kidneys and released into the circulation where it converts angiotensinogen to angiotensin Ι a relatively inactive decapeptide. Angiotensin Ι is then converted by angiotensin converting enzyme, a peptidyldipeptidase, to angiotensin ΙΙ. Angiotensin ΙΙ is a potent vasoconstrictor responsible for arterial vasoconstriction and increased blood pressure, as well as for stimulation of the adrenal gland to secrete aldosterone. Inhibition of ACE results in decreased plasma angiotensin ΙΙ, which leads to decreased vasopressor activity and to reduced aldosterone secretion. Although the latter decrease is small, small increase in serum potassium concentrations may occur, along with sodium and fluid loss. The cessation of the negative feedback of angiotensin ΙΙ on the renin secretion results in an increase of the plasma renin activity.Another function of the converting enzyme is to degrade the potent vasodilating kinin peptide bradykinin to inactive metabolites. Therefore inhibition of ACE results in an increased activity of circulating and local kallikrein-kinin system which contributes to peripheral vasodilation by activating the prostaglandin system. It is possible that this mechanism is involved in the hypotensive effects of ACE inhibitors and is responsible for certain adverse reactions. In patients with hypertension administration of ACE inhibitors results in a reduction of supine and standing blood pressure to about the same extent with no compensatory increase of the heart rate. Peripheral arterial resistance is reduced with either no change or an increase in cardiac output.There is an increase in renal blood flow and glomerular filtration rate is usually unchanged. Achievement of optimal blood pressure reduction may require several weeks of therapy in some patients. The antihypertensive effects are maintained during long term therapy. Abrupt withdrawal of therapy has not been associated with a rapid increase in blood pressure.The antihypertensive effect of trandolapril sets in one hour post-dose and lasts for at least 24 hours, but trandolapril does not interfere with the circadian blood pressure pattern.TarkaNeither animal studies nor healthy volunteer studies could demonstrate pharmacokinetic or RAS interactions between verapamil and trandolapril. The observed synergistic activity of these two active substances must therefore be due to their complementary pharmacodynamic actions.In clinical trials Tarka was more effective in reducing high blood pressure than either active substance alone. In long-term trials, Tarka proved to be safe and well tolerable.PharmacokineticTarka tablets are film-coated and composed of a layer designed for sustained release of verapamil hydrochloride and a separate layer intended for immediate release of trandolapril.VerapamilAbsorption:About 90% of orally administered verapamil is absorbed. The mean bioavailability is as low as 22% because of extensive hepatic first-pass extraction, and shows great variation (10-35%). The mean bioavailability following repeated administration may increase to 30%.Food, especially fat food, may delay the absorption of verapamil from the tablet, which results in higher Tmax values and lower Cmax values, without influence on the bioavailability of verapamil. To prevent a potential delayed absorption it is recommended to take Tarka half an hour before breakfast.Distribution and biotransformation:The mean time to peak plasma concentration is 4 hours. The peak plasma concentration of norverapamil is attained about 6 hours post-dose. Steady state after multiple once daily dosing is reached after 3-4 days. Plasma protein binding of verapamil is about 90%.Elimination:The mean elimination half-life after repeated administration is 8 hours. 3-4% of a dose is excreted renally as unchanged drug. Metabolite excretion is in the urine (70%) and in the faeces (16%). Norverapamil is one of 12 metabolites identified in urine, has 10-20% of the pharmacologic activity of verapamil, and accounts for 6% of excreted drug. The steady-state plasma concentrations of norverapamil and verapamil are similar. Verapamil kinetics is not altered by renal function impairment.The bioavailability and elimination half-life of verapamil are increased in patients with liver cirrhosis. Verapamil kinetics is, however, unchanged in patients with compensated hepatic dysfunction. Kidney function has no effect on verapamil elimination.TrandolaprilAbsorption:Orally administered trandolapril is absorbed rapidly. Absorption is 40-60% and independent of the presence of food.The time to peak plasma concentration is about 30 minutes.Distribution and biotransformation:Trandolapril disappears very rapidly from plasma, and its half-life is less than one hour.Trandolapril is hydrolysed in plasma to form trandolaprilat, a specific angiotensin converting enzyme (ACE) inhibitor. The amount of trandolaprilat formed is independent of food intake.The time to peak plasma concentration of trandolaprilat is 4-6 hours.Plasma protein binding of trandolaprilat is greater than 80%. Trandolaprilat binds with great affinity to ACE, and this is a saturable process. Most of circulating trandolaprilat binds to albumin in a non saturable process. Steady state after multiple once daily dosing is reached after about 4 days in healthy volunteers as well as in younger and elderly hypertensive patients.The effective half-life calculated from accumulation is 16-24 hours.Elimination:10-15% of an administered trandolapril dose is excreted as unchanged trandolaprilat in urine. Following oral administration of radioactively labelled trandolapril, one third of radioactivity is recovered in urine and two thirds in faeces.The renal clearance of trandolaprilat shows a linear correlation with creatinine clearance. The trandolaprilat plasma concentration is significantly higher in patients whose creatinine clearance is [≤] 30 ml/min. Following repeated administration to patients with chronic renal dysfunction, steady state is, however, also reached after four days, independently of the extent of kidney function impairment.The trandolapril plasma concentration may be 10 times higher in patients with liver cirrhosis than in healthy volunteers. The plasma concentration and renal excretion of trandolaprilat are also increased in cirrhotic patients, albeit to a lesser extent.Trandolapril(at) kinetics are unchanged in patients with compensated hepatic dysfunction.TarkaAs there are no known kinetic interactions between verapamil and trandolapril or trandolaprilat, the single active substance kinetic parameters of these two active substances apply to the combination product as well.IndicationsEssential hypertension in patients whose blood pressure has been normalised with the individual components in the same proportion of doses.ContraindicationsKnown hypersensitivity to trandolapril or any other ACE inhibitor and/or verapamil or to any of the excipientsHistory of angioneurotic oedema associated with previous ACE inhibitor therapyHereditary/idiopathic angioneurotic oedemaCardiogenic shockRecent myocardial infarction with complicationsSecond- or third-degree AV block without a functioning pacemaker

87
SA blockSick sinus syndrome in patients without a functioning pacemakerCongestive heart failureAtrial flutter/fibrillation in association with an accessory pathway (e.g. WPW-syndrome)Severe renal impairment (creatinine clearance < 10 ml/min)DialysisLiver cirrhosis with ascitesAortic or mitral stenosis, obstructive hypertrophic cardiomyopathyPrimary aldosteronismPrgnancyLactationUse in children and adolescents (< 18 years)
Side EffectsThe adverse drug reactions for Tarka are consistent with those known for its components or the respective class of medicinal products. The most commonly reported adverse drug reactions are cough, headache, constipation, vertigo, dizziness and hot flushes (see table below).
TARKA Table 1 Side EffectsSystem Organ Class Frequency Undesirable Effects
Blood and lymphatic system disorders very rare-leukopenia-pancytopenia-thrombocytopenia
Immune system disorders
uncommon -allergic reaction, unspecified
very rare -increase in gammaglobulin-hypersensitivity, unspecified
Metabolism and nutritional disordersuncommon -hyperlipidaemia
rare -anorexia
Psychiatric disorders
uncommon -somnolence
very rare
-aggression-anxiety-depression-nervousness
Nervous system disorders
common -dizziness-vertigo
uncommon -tremor
rare -collapse
very rare
-impaired balance-insomnia-paresthesia or hyperesthesia-syncope or acute circulatory failures with loss of consciousness-taste aberration-weakness
Eye disorders very rare -abnormal/blurred vision
Cardiac disorders/vascular disorders
common -hot flushesuncommon
-AV block, first degree-Palpitation
very rare
-angina pectoris-atrial fibrillation-AV block, complete-AV block, unspecified-bradycardia-cardiac arrest-cerebral haemorrhage-oedema, peripheral-oedema, unspecified-flushing-heart failure-hypotensive events including orthostasis or fluctuation of blood pressure-tachycardia
Respiratory, thoracic and mediastenal disorders
common -cough
very rare
-asthma-bronchitis-dyspnea-sinus congestion
Gastrointestinal disorders common -constipationuncommon
-abdominal pain-diarrhoea-gastrointestinal disorders unspecified-nausea

88
very rare-dry mouth/throat-pancreatitis-vomiting
Hepatobiliary disorders very rare
-cholestasis-hepatitis-increase in γGT-increase in LDH-increase in lipase-jaundice
Skin and subcutaneous tissue disorders
uncommon
-facial oedema-pruritus-rash-sweating increased
rare-alopecia-herpes simplex-skin disorders, unspecified
very rare
-angioneurotic oedema-erythema multiforme-exanthema or dermatitis-psoriasis-urticaria
Musculoskeletal connective tissue and bone disorders very rare
-arthralgia-myalgia-myasthenia
Renal and urinary disordersuncommon -polyuria
very rare -acute renal failure
Reproductive system and breast disorders very rare -gynecomastia-impotence
General disorders and administration site conditions
common -headacheuncommon -chest pain
very rare -fatigue or asthenia
Investigations
uncommon -liver function test, abnormal
rare -hyperbilirubinemia
very rare-increase in alkaline -phosphatase-increase in serum potassium-increase in transaminases
Adverse events either reported spontaneously or observed in clinical trials are depicted in the following table. Within each system organ class, the ADRs are ranked under headings of frequency, using the following convention: common (>1/100, <1/10), uncommon (>1/1,000, <1/100), rare (>1/10,000, <1/1.000), very rare (<1/10,000), including isolated reports.The following adverse reactions have not yet been reported in relation to Tarka, but are generally accepted as being attributable to ACE inhibitors:Blood and lymphatic system disorders: decreases in haemoglobin and hematocrit, and in individual cases agranulocytosis. Isolated cases of hemolytic anaemia have been reported in patients with congenital G-6-PDH deficiency.Psychiatric disorders: occasionally confusion.Nervous system disorders: rarely, sleep disorders.Ear and labyrinth disorders: rarely, problems with balance, tinnitus.Cardiac disorders/vascular disorders: Individual cases of arrhythmia, myocardial infarction and transient ischemic attacks have been reported for ACE inhibitors in association with hypotension.Respiratory, thoracic and mediastinal disorders: Rarely, sinusitis, rhinitis, glossitis, and bronchospasm.Gastrointestinal disorders: occasionally indigestion. Individual cases of ileus.Hepatobiliary disorders: individual cases of cholestatic icterus.Skin and subcutaneous tissue disorders: occasionally allergic and hypersensitivity reactions such as Stevens-Johnson syndrome, toxic epidermic necrolysis. This can be accompanied by fever, myalgia, arthralgia, eosinophilia and / or increased ANA - titers.Investigations: increases in blood urea and plasma creatinine may occur especially in the presence of renal insufficiency, severe heart failure and renovascular hypertension. These increases are however reversible on discontinuation.Symptomatic or severe hypotension has occasionally occurred after initiation of therapy with ACE inhibitors. This occurs especially in certain risk groups, such as patients with a stimulated renin-angiotensin-aldosterone system.The following adverse reactions have not yet been reported in relation to Tarka, but are generally accepted as being attributable to phenylalkylamine calcium-channel blockers:Nervous system disorders: in some cases, there may be extrapyramidal symptoms (Parkinson’s disease, choreoathetosis, dystonic syndrome). Experience so far has shown that these symptoms resolve once the medicinal product is discontinued. There have been isolated reports of exacerbation of myasthenia gravis, Lambert-Eaton syndrome and advanced cases of Duchenne’s muscular dystrophy.Gastrointestinal disorders: gingival hyperplasia following long-term treatment is extremely rare and reversible after discontinuation of therapy.Skin and subcutaneous tissue disorders: Stevens-Johnson syndrome and erythromelalgia have been described. In isolated cases allergic skin reactions like erythema.Reproductive system and breast disorders: Hyperprolactinemia and galactorrhea have been described.Excessive hypotension in patients with angina pectoris or cerebrovascular disease treated with Verapamil may result in myocardial infarction or cerebrovascular accident.PrecautionsSymptomatic hypotension:
89
Under certain circumstances, Tarka may occasionally produce symptomatic hypotension. This risk is elevated in patients with a stimulated renin-angiotensin-aldosterone system (e.g., volume or salt depletion, due to the use of diuretics, a low-sodium diet, dialysis, dehydration, diarrhoea or vomiting; decreased left ventricular function, renovascular hypertension)Such patients should have their volume or salt depletion corrected beforehand and therapy should preferably be initiated in a hospital setting. Patients experiencing hypotension during titration should lie down and may require volume expansion by oral fluid supply or intravenous administration of normal saline. Tarka therapy can usually be continued once blood volume and pressure have been effectively corrected.Kidney function impairment:Patients with moderate renal impairment should have their kidney function monitored.Tarka may produce hyperkalemia in patients with renal dysfunction.Acute deterioration of kidney function (acute renal failure) may occur especially in patients with pre-existing kidney function impairment, or congestive heart failure.There is insufficient experience with Tarka in secondary hypertension and particularly in renal vascular hypertension. Hence, Tarka should not be administered to these patients, especially since patients with bilateral renal artery stenosis or unilateral renal artery stenosis in individuals with a single functioning kidney (e.g., renal transplant patients) are endangered to suffer an acute loss of kidney function.Proteinuria:Proteinuria may occur particularly in patients with existing renal function impairment or on relatively high doses of ACE inhibitors.Severe impairment:Since there is insufficient therapeutic experience in patients with severe hepatic impairment as such, the use of Tarka cannot be recommended. Tarka is contraindicated in patients with liver cirrhosis with ascites.Angioneurotic oedema:Rarely, ACE inhibitors (such as trandolapril) may cause angioneurotic oedema that includes swelling of the face, extremities, tongue, glottis, and/or larynx. Patients experiencing angioneurotic oedema must immediately discontinue trandolapril therapy and be monitored until oedema resolution.Angioneurotic oedema confined to the face will usually resolve spontaneously. Oedema involving not only the face but also the glottis may be life-threatening because of the risk of airway obstruction.Compared to non-black patients a higher incidence of angioedema has been reported in black patients treated with ACE inhibitors.Angioneurotic oedema involving the tongue, glottis or larynx requires immediate subcutaneous administration of 0.3-0.5 ml of epinephrine solution (1:1000) along with other therapeutic measures as appropriate.Caution must be exercised in patients with a history of idiopathic angioneurotic oedema, and Tarka is contraindicated if angioneurotic oedema was an adverse reaction to an ACE inhibitor.Neutropenia/agranulocytosis:The risk of neutropenia appears to be dose-and type-related and is dependent on the patient’s clinical status. It is rarely seen in uncomplicated patients but may occur in patients with some degree of renal impairment especially when it is associated with collagen vascular disease e.g. systemic lupus erythematosus, scleroderma and therapy with immunosuppressive medicinal products. It is reversible after discontinuation of the ACE inhibitor.Cough:During treatment with an ACE inhibitor a dry and non-productive cough may occur which disappears after discontinuation.Hyperkalemia:Hyperkalemia may occur during treatment with an ACE inhibitor, especially in the presence of renal insufficiency and/or heart failure. Potassium supplements or potassium sparing diuretics are generally not recommended, since they may lead to significant increases in plasma potassium. If concomitant use of the above mentioned medicinal products is deemed appropriate, they should be used with frequent monitoring of serum potassium.Elderly:Tarka has been studied in a limited number of elderly hypertensive patients only. Pharmacokinetic data show that the systemic availability of Tarka is higher in elderly compared to younger hypertensives. Some elderly patients might experience a more pronounced blood pressure lowering effect than others. Evaluation of the renal function at the beginning of treatment is recommended.Surgical patients:In patients undergoing major surgery requiring general anaesthesia, ACE inhibitors may produce hypotension, which can be corrected by plasma volume expanders.Conduction disturbances:Treatments should be used with caution in patients with first degree atrioventricular block.Bradycardia:Tarka should be used with caution in patients with bradycardia.Diseases in which neuromuscular transmission is affected:Tarka should be used with caution in patients with diseases in which neuromuscular transmission is affected (myasthenia gravis, Lambert-Eaton syndrome, advanced Duchenne muscular dystrophy).Haemodialysis patientsPatients on concurrent ACE inhibitor therapy and haemodialysis with polyacrylonitrile methallyl sulfonate high-flux membranes (e.g. ‘AN 69’) have experienced anaphylactoid reactions. Such membranes should therefore not be used in these patients.Desensitisation:Anaphylactoid reactions (in some cases life threatening) may develop in patients receiving ACE inhibitor therapy and concomitant desensitisation against animal venoms.LDL-aphaeresis:Life threatening anaphylactoid reactions have been noted when patients on LDL-aphaeresis take ACE inhibitors at the same time.Evaluation of the patients should include assessment of renal function prior to initiation of therapy and during treatment.Blood pressure readings for evaluation of therapeutic response to Tarka should always be taken before the next dose.LactoseTarka tablets contain lactose.Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicinal product.SodiumThis medicinal product contains 1.12 mmol (or 25.76 mg) sodium per dose. To be taken into consideration by patients on a controlled sodium diet.Pregnancy and LactationThe use of Tarka in pregnancy is contraindicatedThe safe use of Tarka in pregnant women is inadequately documented. However, there have been anecdotal reports of neonatal lung hypoplasia, intra-uterine growth retardation, persistent ductus arteriosus, and cranial hypoplasia following exposure of foetuses to ACE inhibitors. In addition, the pharmacologic activity of ACE inhibitors is compatible with the possibility of foetal hypotension, which may be associated with foetal/neonatal oliguria/anuria and oligohydramnios.

90
Teratogenic effects are primarily expected when ACE inhibitors are used in the second and third trimesters of pregnancy, and it is not known whether exposure of the embryo/foetus to an ACE inhibitor only in the first trimester is teratogenic or embryotoxic/foetotoxic. Women who wish to get pregnant or are pregnant must consult their doctor without delay, so an alternative pharmacologic treatment can be prescribed.Women of child-bearing potentialDoctors should instruct women of child-bearing potential accordingly before prescribing an ACE inhibitor.Tarka is contraindicated when breastfeedingEffects on ability to drive and use machinesWhile no effect on the ability to drive and use machinery has been established, impairment of alertness cannot be ruled out altogether, since Tarka may produce dizziness and fatigue.OverdosageThe highest dose used in clinical trials was 16 mg of trandolapril. This dose produced no signs or symptoms of intolerance.The most important symptom to be expected after a significant overdose is hypotension. Administration of normal saline solution is recommended in this case.The most important signs and symptoms of a verapamil overdose are due to its pharmacologic activity in the cardiovascular system and include hypotension arising from peripheral vasodilation and a negative inotropic effect, depression of impulse generation in the sinus node and cardiac impulse conduction disturbances that may result in sinus bradycardia, sinus arrest, AV block, and asystole.Following oral verapamil overdosage, the patient must be monitored and treated in an intensive care setting. Overdose management must be aimed at preventing the further absorption of verapamil from the gastrointestinal tract, providing symptomatic treatment of the toxic effects (see above), and compensating for the calcium-antagonistic effects of this active substance. Further absorption of verapamil from the gastrointestinal tract can be prevented by gastric lavage, administration of adsorbent material (activated charcoal) and a cathartic (sodium sulphate). Apart from general supportive measures in response to severe hypotension (to the point of shock), i.e., maintenance of an adequate circulating blood volume by administering plasma or a plasma expander, it may be necessary to stimulate the heart muscle with such positive inotropic medicinal products drugs as dopamine, dobutamine or isoproterenol.Atropine (or methylatropine) may be useful in the management of sinus bradycardia. AV block should be treated with sympathomimetic medicinal products (isoproterenol or metaproterenol) or a pacemaker. Asystole should be handled by the usual measures including cardiopulmonary resuscitation, cardiac pacing, etc. The calcium-antagonistic effect can be offset by parenteral administration of calcium, for instance as calcium gluconate.Drug InteractionsNot recommended association- Potassium sparing diuretics or potassium supplements: ACE inhibitors attenuate diuretic induced potassium loss. Potassium sparing diuretics e.g. spironolactone, triamterene, or amiloride, potassium supplements, or potassium containing salt substitutes may lead to significant increases in serum potassium, particularly in the presence of renal function impairment. If concomitant use is indicated because of demonstrated hypokalemia they should be used with caution and with frequent monitoring of serum potassium.Dantrolene: The simultaneous use of verapamil with dantrolene is not recommended.Precaution for useAntihypertensive medicinal products: increase of the hypotensive effect of Tarka.Diuretics: patients on diuretics and especially those who are volume-and / or salt depleted may experience an excessive reduction of blood pressure after initiation of therapy with an ACE inhibitor. The possibility of hypotensive effects can be reduced by discontinuation of the diuretic, by increasing volume or salt intake prior to intake and by initiation of therapy with low doses. Further increases in dosage should be performed with caution.Lithium: there have been reports of both an increase and a reduction in the effects of lithium used concurrently with verapamil. The concomitant administration of ACE inhibitors with lithium may reduce the excretion of lithium. Serum lithium levels should be monitored frequently.Anaesthetics: Tarka may enhance the hypotensive effects of certain anaesthetic medicinal products.Narcotics/antipsychotics: postural hypotension may occur.Allopurinol, cytostatic or immunosuppressive medicinal products, systemic corticosteroids or procainamide: concomitant administration with ACE inhibitors may lead to an increased risk for leucopenia.Cardiodepressive medicinal products: the concurrent use of verapamil and cardiodepressives, i.e., medicinal products that inhibit cardiac impulse generation and conduction (e.g., beta-adrenergic blockers, antiarrhythmics, inhalation anesthetics), may produce undesirable additive effects.Quinidine: the concomitant use of quinidine and oral verapamil in patients with hypertrophic (obstructive) cardiomyopathy has resulted in hypotension and pulmonary oedema in a small number of cases.Digoxin: concurrent use of digoxin and verapamil has been reported to result in 50-75% higher digoxin plasma concentrations, requiring reduction of the digoxin dosage.Muscle relaxants: the effect of muscle relaxants may be enhanced.Tranquillisers/antidepressants: as with all antihypertensives, there is an elevated risk of orthostatic hypotension when combining Tarka with major tranquillisers or antidepressant medicinal products containing imipramine.Take into accountNon-steroidal anti-inflammatory drugs (NSAIDs): the administration of a non-steroidal anti-inflammatory drug may reduce the antihypertensive effect of an ACE inhibitor. Furthermore it has been described that NSAIDs and ACE inhibitors exert an additive effect on the increase in serum potassium, whereas renal function may decrease. These effects are in principle reversible, and occur especially in patients with compromised renal function.Antacids: induce decreased bioavailability of ACE inhibitors.Sympathomimetics: may reduce the antihypertensive effects of ACE inhibitors; patient should be carefully monitored to confirm that the desired effect is being obtained.Alcohol: enhances the hypotensive effect.Verapamil may increase the plasma concentrations of carbamazepine, cyclosporin, and theophylline thus increasing risk of toxicity from these compounds.Rifampin, phenytoin, and phenobarbital reduce the plasma concentrations of verapamil, whereas cimetidine may increase the plasma concentrations of verapamil.Antidiabetics: a dose adjustment of antidiabetics or of Tarka may be necessary in individual cases especially at the start of therapy due to increased reduction of blood glucose.Grapefruit juice has been shown to increase the plasma levels of verapamil, which is a component of Tarka. Grapefruit juice should therefore not be ingested with Tarka.Food has been shown to decrease the rate but not the extent of absorption of verapamil. It is therefore recommended to take the medicinal product half an hour before breakfastIncompatibilitiesNot applicableDosage Administration

91
The usual dosage is one tablet once daily, taken in the morning half an hour before breakfast. The tablets should be swallowed whole.Dosage in children: Tarka is contraindicated in children and adolescents (<18 years).Dosage in the elderly: As systemic availability is higher in elderly patients compared to younger hypertensives, some elderly patients might experience a more pronounced blood pressure lowering effect.Dosage in renal failure: Tarka is contraindicated in severe renal impairment.Dosage in hepatic insufficiency: the use of Tarka is not recommended in patients with severe hepatic impairment; Tarka is contraindicated in patients with liver cirrhosis with ascitesPackagingBlister packs of 14, 28, 30, 50, 56, 98, 280 modified-release tabletsNot all pack sizes maybe marketed.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++