healthinafrica.istanbulhealthinafrica.istanbul/.../endemic-diseases-in-africa.docx · web...
TRANSCRIPT

SOCIOECONOMIC BURDEN OF ENDEMIC DISEASES IN AFRICA WITH EMPHYSIS ON
MALARIAProfessor Mustafa Idris Elbashir MD, PhD
Faculty of Medicine, University of Khartoum, [email protected]; [email protected]
Introduction:Good health is important for building vibrant and productive communities, stronger economies, safer nations, and better world. Endemic tropical diseases are the highest contributors to the socioeconomic burden of disease in Africa. Information that is available on real socioeconomic burden of endemic diseases in Africa is fragmentary and sometimes inconsistent. However, years of life lost from premature death, and years of life lived in less than full health, in addition to increased mother, infant, and child mortality as well as decrease in life expectancy are good indicators for the huge socioeconomic burden of endemic diseases in Africa (1). In most sub-Saharan African (SSA) countries, endemic diseases perpetuate poverty which
1

affects the health seeking behaviors, and the approaches employed to manage these diseases by different people. Africans seek care from several health care providers ranging from wandering drug sellers to general hospitals. The proliferation of low level treatment providers such as barefaced medicine dealers, wandering drug sellers, and traditional medicine dealers who diagnose and treat endemic diseases is elicited by weaknesses in the public healthcare system. In many African countries governments are unable to provide adequate and equitable essential healthcare services to the expanding population. People in need of health care might wander between unauthorized practitioners without getting cure for their illnesses. The preference of healthcare provider is usually determined by affordability, nearness to homes, striking unsubstantiated propaganda and advocacy for sold drugs, and the prompt attention and attitudes of service providers (2). Endemic diseases in Africa include the “big three” diseases (malaria, tuberculosis TB, and HIV/AIDS) which have serious direct
2

costs in terms of treatment, treatment seeking, absenteeism from work and school, and funeral expenses in the event of death. HIV/AIDS, malaria and tuberculosis are by far the commonest causes of ill-health and death in the poorest countries of the world which happen to be in the tropics and temperate countries in Africa, Asia and South America. Morbidity and mortality from these three diseases have a major socio-economic impact on individuals, communities and nations, due to the vicious cycle of poverty, ill health and ignorance. If not controlled continuing rise in incidence of HIV/AIDS, malaria and TB may threaten the survival of small enterprises, and ability to attract foreign investments leading to a rise in unemployment. Thus, investments in the improvement of health including HIV/AIDS, malaria and tuberculosis if done well will bring substantial benefits for the national economy including increase in productivity, a better trained workforce, improved economy, strong business enterprises, lower unemployment, fall in disease trends and better social well-being of the population (3). Endemic diseases in Africa also include a group of diseases called,
3

collectively, neglected tropical diseases (NTDs) (4). A consistent description of the socioeconomic burden of endemic diseases and the risk factors that cause them is an important input to health decision-making and planning processes. Evidence-based interventions exist to prevent and control these diseases with very gratifying results, however, the coverage still remains low in the face of many challenges including; shortage of finance, antimicrobial resistance, political instability, power health facilities and records, to name a few (5). This paper presents brief account on the socioeconomic burden of the NTDS, HIV/AIDS, TB and malaria in Africa. It also highlights the collective progress made in the fight against these endemic diseases and the existing challenges. It also proposes the scale up of NGOs role, including the Federation of Islamic Medical Associations (FIMA) and Turkish government and Foundations, in building capacity of local communities in Africa, to empower community-based delivery of medical and
4
health services, and probably the establishment of centers of excellence for basic and applied research on endemic diseases in Africa. This is to be delivered in close collaboration with official bodies involved in health service provision, and with other stakeholders already exerting appreciable efforts to control or eradicate endemic diseases in Africa. Socioeconomic burden of Neglected tropical diseases (NTDs):The concept of NTDs emerged recently and has been recognized as a valid way to categorize diseases that affect the poorest individuals (6). They are defined as a group of infections strongly associated with poverty in tropical and subtropical environments and they are diverse in biological and transmission characteristics. They spread in 149 countries, affecting more than one billion people, costing developing economies billions of dollars every year. NTDs blind, mutilate, disfigure and debilitate hundreds of millions of people in the poorest parts of the world, mainly in Africa. Once widely prevalent globally, these diseases are now restricted to tropical and sub-tropical regions with unsafe water, inadequate hygiene and
5
sanitation, and poor housing conditions. More than 70% of countries and territories that report the presence of NTDs are low or lower-middle income economies with limited access to health services (7).Despite the progress made in relieving the burden of these diseases through successful programs aiming at control, elimination or total eradication, however, there is great need for affordable products in the areas of diagnostics, effective drugs, and insecticides. In addition, challenges such as insecurity and weak health systems continue to prevail in the poorest countries, inhibiting progress in scaling up control or eradication measures. We are still far from achieving the WHO Roadmap goals which were endorsed by member states in a World Health Assembly Resolution in 2013 for minimizing the burden of NTDs by 2020 (8). NTDs have also been included within the Sustainable Development Goal targets (SDG) and are also becoming a crucial component of universal health coverage (UHC) (9). Of the many poverty-related, neglected tropical diseases that exist, the World Health Organization (WHO) initially has selected 17 to be included in the priority list for control of NTDs, and in some cases be eliminated.
6

However, on 28 May 2016, the 69th World Health Assembly approved a resolution recognizing Mycetoma as a neglected tropical disease to be given more attention among the selected list, as well (10). More than 128 countries are burdened by, at least one NTD, and at least 2 billion people are at risk of infection. NTDs are ancient notorious diseases for their disabling and deforming symptoms, and effective treatments exist for many, which explain why they have all but vanished in richer countries, where better funded health care systems and improved sanitation have slowed their spread. Some of these NTDs have painful and stigmatizing symptoms, and others leave no visible mark on the people they infect if treated early. Effective control against NTDs can be achieved when several public health approaches are combined. Thus, interventions guided by local epidemiology and availability of appropriate detection, prevention, and control measures that can be delivered locally with high coverage will lead to achieving the WHO NTD Roadmap targets resulting in the elimination of many diseases and the eradication of some by 2020 (9).
7

NTDs can be transmitted by viruses, bacteria or parasites. They include multi-cellular helminths that are visible to the naked eye or microscopic single-celled protozoa. There are many NTDs, but 18 that have been given priority by WHO include the following: Viruses:
1- Dengue Dengue is a systemic viral infection transmitted between humans by Aedes mosquitoes. Dengue fever is fast-emerging and prone to pandemics. It has been estimated that there are 390 million dengue infections per year and up to 100m infections are estimated to manifest annually in more than 100 endemic countries. It causes flu-like symptoms, joint pains and rashes and is potentially fatal for some patients. It has been predicted that dengue is ubiquitous throughout the tropics, with local spatial variations in risk influenced strongly by rainfall, temperature and the degree of urbanization. Dengue has been ranked as one of the top emerging diseases and is most common in Asia and Latin America, while the analogous virus, chikungunya, which was first isolated from an outbreak in Tanzania, occurs mainly in Africa and Asia (11). Current epidemiological data may not even reflect the true burden of disease due to
8

under-reported figures. Vector control programs have failed to contain the disease and worst of all, no specific treatment is available at the moment, and no licensed vaccines. Substantial vector control efforts which currently going on have not stopped its rapid emergence and global spread. Despite there are numerous vaccine candidates available they could be held back by different aspects in promoting vaccine implementation. Their long-term protective efficacy against each of the 4 dengue virus serotypes remains to be definitively determined (12). Furthermore, for developing nations, logistics and cost are the major hurdles that need to be addressed in order to provide a quick yet affordable medical relief. As an alternative, plant-based vaccine production system is able to offer an attractive prospect given to its advantages of bio containment warranty, low operation cost, rapid scalability and logistics flexibility. Researches that have embarked on this scope are laid out and reviewed in terms of the feasibility of plant system to serve as a biofactory for dengue vaccine (13). WHO target: Reduce cases by more than 25% and deaths by 50% (from 2009-10 baseline) by 2020 (14).
2- Rabies
9

Domestic dogs are the most common reservoir of the rabies virus: more than 95 per cent of human deaths are caused by dog-mediated rabies. The virus is transmitted in the saliva of rabid animals and generally enters the body via a wound or bite. There are two forms: furious and paralytic. Furious is the most common form in humans. It causes hyperactivity, hydrophobia, aerophobia, and death by cardio-respiratory arrest within days. Paralytic rabies causes a slow progression from paralysis to coma to death. Rabies is endemic on all continents except Antarctica. Rabies is one of the most feared human diseases, estimated to cause some 55,000 deaths each year, 95 per cent of them among children and the rural poor people in Asia and Africa (15, 16, 17). The global burden estimates for rabies (931,600 DALYs) more than justify prioritizing rabies control building on the strong advocacy platforms, functioning at local, regional, and global levels (including the Global Alliance for Rabies Control), and commitments from WHO, OIE, and FAO. Simple effective tools for rabies control exist together with blueprints for operationalizing control, yet, despite elimination targets being set, no global affirmative action has been taken. Rabies control demands activities both in the short
10

term and over a long period of time to achieve the desired cumulative gains. Despite the availability of effective vaccines and messaging tools, rabies will not be sustainably controlled in the near future without long-term financial commitment, particularly as disease incidence decreases and other health priorities take hold. While rabies control is usually perceived as a public good, public private partnerships could prove equally effective in addressing endemic rabies through harnessing social investment and demonstrating the cost-effectiveness of control. It is acknowledged that greater attention to navigating local realities in planning and implementation is essential to ensuring that rabies, and other neglected diseases, are controlled sustainably. In the shadows of resource and institutional limitations in the veterinary sector in low- and middle-income countries, sufficient funding is required so that top-down interventions for rabies can more explicitly engage with local project organization capacity and affected communities in the long term. Latin America and the Caribbean have had a substantial reduction in the number of human and animal rabies cases following the implementation of dog rabies control programs. Official reports of cases of
11
human rabies transmitted by dogs decreased from about 250 in 1990 to fewer than 10 in 2010. The Pan American Health Organization has set a target to eliminate dog-mediated rabies from the Americas by 2015(18). WHO target: Elimination in Southeast Asia and the western Pacific by 2020, not in Africa (5).
Bacteria: 3- Yaws
Yaws is an infectious, debilitating and disfiguring disease of poverty that mainly affects children in rural communities in tropical areas. It is caused by the spirochete bacteria Treponema pallidum, subspecies pertenue. It is a chronic skin disease that mainly affects children under 15 (with a peak between six and 10 years). It is closely related to syphilis and one of three endemic non-venereal treponemal diseases. The bacterium causes a chronic relapsing treponematosis characterized by highly contagious primary and secondary cutaneous lesions and non-contagious tertiary destructive lesions of the bones (19). Humans are the primary reservoir for yaws and transmission occurs through skin to skin contact with the exudate of lesions by those who have skin abrasions or cuts. Yaws is usually contracted in childhood (75% of cases
12
occur before age 15) and infectious lesions are infrequent after the age of 30 (20). In the early stage of the disease, which may last from weeks to months, skin lesions are highly contagious and present differently by season with more open infectious lesions and papillomatous frambesides in the wet season and drier, scalier, maculopapular lesions in the dry season. Painful and itching lesions commonly appear on the upper and lower limbs, fingers, toes, soles of the feet, face, genital areas, and buttocks. The early stage is typically characterized by a single elevated primary lesion that develops a crust that is shed, followed by secondary Yaws resurgence on other parts of the body. After 3-4 months lesions subside due to host immune response. The disease then becomes latent. In about 10% of untreated patients, the infection progresses to the tertiary stage characterized by destruction of tissue, bone, and cartilage resulting in disfigurement and disability (21). Symptoms begin with a round, hard swelling of the skin that grows to the size of a golf ball and goes on to form ulcers and affect bones and cartilage. Yaws has been eliminated in many countries, including India in 2006, and is treated with one of two antibiotics: azithromycin or benzathine penicillin. Early detection can avoid
13

disfigurement and disability, which occur in about 10 per cent of cases. WHO target: Eradication of yaws by 2020 (22).
4- Buruli ulcerBuruli ulcer is the third most common mycobacterial infection worldwide and it is related to the ones that cause leprosy and tuberculosis. It is endemic in tropical, subtropical, and temperate climates and has been identified in at least 33 countries in Africa, South America, the Western Pacific region, and Southeast Asia. Buruli ulcers affect people of all ages, but mostly children; more than 50% of these children are under 15 years of age. Those affected usually live in remote rural areas and have limited access to health services. In the year 2014, 2200 new cases were reported (23). Buruli ulcers present in active and inactive clinical forms. The active form is characterized by non- ulcerative lesions including ulcers, nodules, plaques, and edematous indurations. The infection starts as a small nodule that later ulcerates, giving rise to an unsightly ulcer with undermining edges and a cotton wool-like appearance, and thickening and darkening of the skin surrounding the lesion. A scar later develops, which may compromise the function of the affected area. Although it is slowly-growing organism, Mycobacterium
14

ulcerans produces a toxin, mycolactone, which destroys tissue resulting in large ulcers causing debilitating skin disease with ugly morbidity, often requiring reconstructive surgery. Untreated ulcers might result in long-term disability or even mortality. The infection may affect the face, chest wall, abdomen, and back; however, the disease commonly affects the extremities. Mycobacterium ulcerans is an environmental pathogen characterized by multi-host transmission dynamics and that its infectious pathways to humans rely on the local effects of global environmental changes. Land-use changes, climatic patterns and biodiversity alterations contribute to disease emergence in many parts of the world. Prevailing opinion is that humans are infected from; insects, such as mosquitoes, and water-residing biting arthropods, have been proposed as vectors for transmission (24). It is not known how the disease spreads, but early signs of the disease are a painless swelling. Early diagnosis and treatment are the only ways to prevent disability. The treatment duration is usually long and the regimens considered are limited to the combined antibiotics rifampicin and streptomycin. In 2015 the number of cases of Buruli ulcer decreased by 60% compared
15
with 2008 in India. WHO target: 70% cases cured with antibiotics in all endemic countries by 2020 (23).
5- Trachoma Chlamydia trachomatis, an obligate intraocular bacteria causing trachoma, adult and neonatal inclusion conjunctivitis, was the leading cause of blindness in the last century worldwide. Improvement in socioeconomic and living conditions, availability of antibiotics, and introduction of National Trachoma Control Programs reduced the prevalence in developed countries, but it persisted in resource-poor settings of Africa and Asia. Trachoma is transmitted by person-to-person contact, via fomites, or via eye-seeking flies that have been in contact with the ocular discharge of an infected individual, particularly between children and their mothers. Trachoma infection afflicts predominantly young children. It thrives in crowded living conditions where there are shortages of water and poor sanitation. It usually affects both the eyes and symptoms include itching, irritation, discharge, swelling of eyelids, photophobia, and pain. During the initial stage, follicles appear in the upper tarsal conjunctiva which contains white blood cells followed by papillae. Repeated infections lead to scarring of the conjunctiva,
16

ranging from a few linear or stellate scars to thick distorting bands of fibrosis which appear as white lines with split lamp. The scar tissue contracts which results in entropion and trichiasis leading to corneal opacification and ultimately blindness. Through visual disability, and negative impact on the economic livelihoods of those affected, the sub-Saharan Africa region currently bears the largest burden ( 25). In 1990, the WHO reported that 146 million individuals across the globe had active trachoma, 10 million were in need of surgery, and 8 million were blind due to trachoma. In 1995, about 15.5% of the total blindness across the world was due to trachoma and it was the second major cause of global blindness. Therefore, in 1995, the World Health Assembly constituted the Global Alliance for the Elimination of Blinding Trachoma by the year 2020 (GET 2020) by implementation of the SAFE strategy (surgery for TT; antibiotics for C. trachomatis; facial cleanliness; and environmental improvement) with an aim to eliminate trachoma by the year 2020 (26). One of the Alliance major elimination targets is to reduce the prevalence of trachomatous inflammation, follicular (TF) in children aged 1–9 years old to < 5 % in all endemic regions
17

by 2020. Programmatic success is evaluated through follow-up surveys assessing prevalence of TF in 1–9-year-olds, following several annual antibiotic treatment rounds.With the implementation of SAFE strategy, trachoma has decreased in significance as a major cause of blindness. In 2002 and 2003, 84 million people across the world were suffering from active trachoma and ~1.3 million people were blind from trachoma. In 2002, ~3.6% of the total visual impairment was due to trachoma, which was the fourth major cause of blindness. In 2005, as per the WHO report, ~60 million people were suffering from trachoma and in 2008, 40 million people were suffering from active trachoma.The Carter Center's Trachoma Control Program was established in 1998. As a global leader in the fight against trachoma, the Center and partners implement the World Health Organization endorsed Surgery, Antibiotics, Facial cleanliness, and Environmental (SAFE) strategy for trachoma control. The International Task Force for Disease Eradication (ITFDE), hosted and sponsored by Carter center, concluded in 2010 that blindness from trachoma could be eliminated by 2020 by accelerating the pace and scale of interventions. Mounting
18

evidence suggests that some combination of programmatic activity and infrastructure improvement are reducing the burden of trachoma worldwide (27). In Ethiopia and several other endemic countries, the Carter Center has trained and equipped local health workers to surgically correct eyelids deformed by the scarring of multiple trachoma infections, has supported approximately 45 percent of the global output of these types of surgeries. In 2015, The Center supported 83,434 corrective eyelid surgeries. Since 1999, The Center has assisted National Programs in completing 562,109 surgeries, and has assisted in the distribution of over 140 million doses of Zithromax® (donated by Pfizer Inc), an effective trachoma-fighting antibiotic. In 2015, over 16 million doses, about 30 percent of the global total, were distributed in Carter Center-supported areas in Ethiopia. The Center has also provided more than 10,300 villages with ongoing health education and supported the construction of over 319,000 household latrines in 2015. Since 2002, approximately 3.4 million household latrines have been built to help to reduce breeding sites for flies, a principal source of infection. Since 2000, The Carter Center has been a pioneer in the fight against blinding
19
trachoma. The Carter Center has conducted extensive studies in partnerships with ministries of health and others and has published more than 100 papers in scientific journals and peer-reviewed publications (28).In 2013, the WHO reported that trachoma was a major public health problem in only 53 socioeconomically underdeveloped countries of the world in Africa, Central and South America, Asia, Australia, and the Middle East (27). In 2016, as per the WHO report, trachoma is restricted to 42 countries, causing blindness/visual impairment in ~1.9 million people (28). Seven countries, three of them are Africans (China, Gambia, Ghana, the Islamic Republic of Iran, Morocco, Myanmar, and Oman) had submitted reports of achieving 100% elimination goals of trachoma, which was a major milestone in the campaign to eliminate chlamydial infections of the eyes (28).
Significant progress has been achieved in some high burden African countries such as Ethiopia. In 2016, rigorous impact surveys, showed that 143 districts, with a population of 29.7 million persons, reached the elimination target for TF and no longer warranted MDA. At the community level, national trachoma programs and their NGO
20

partners have had local success even in once hyper-endemic communities. In several studies in the Amhara region and the Gurage zone of the Ethiopian Southern Nations, Nationalities, and Peoples' region of Ethiopia, repeated mass antibiotic distributions dramatically reduced infection after 3 to 4 years of treatment. However, despite 7-10 years of programmatic activity region-wide, progress has been slower than anticipated for many districts of Amhara, where TF1-9 prevalence has stabilized at a lower, yet still hyper-endemic level (29). The current antibiotic of choice is oral azithromycin, which is distributed to entire endemic districts meeting the intervention criteria. The WHO recommends that treatment is repeated annually for an initial 3–5-year period, depending on the baseline disease prevalence (30). Data from various sources such as randomized-trials in Ethiopia and cohort studies in other countries, as well as mathematical modeling demonstrate that the situation in other hyper-endemic areas is similar to the experiences in Amhara ( 29 ) . These various sources suggest that in areas which started at a high TF 1-9 prevalence, reaching elimination in five years under the current strategy of annual community-wide
21

MDA is impossible. Several trials testing more intensive antibiotic distributions and non-antibiotic water and hygiene measures are now underway, including two in Amhara. The limiting step to controlling trachoma worldwide may be determining whether a more intensive strategy can control the disease in the most hyper-endemic areas of Ethiopia. Even though the global program is moving in the right direction, it will take years for trachoma to disappear at the current rate of progress in some hyper-endemic areas. Both regression and mathematical transmission models suggest that the 2020 target for elimination of trachoma as a public health problem will not be reached in some of the world’s most affected areas. On one hand, programs have had remarkable success in reducing the clinical signs of trachoma several fold, and even more success in reducing PCR evidence of infection. On the other hand, the most severely affected areas such as Amhara, Ethiopia, despite regional success, have numerous districts where TF1-9 remains 4-fold higher than the target prevalence of less than 5%, despite being at scale with SAFE for a number of years. There has been tremendous progress in scaling up the global trachoma program since the ITFDE last
22

reviewed the disease. The near completion of the TF 1-9 prevalence map for all endemic districts propelled the global community to assess intervention needs, attempt to fill funding gaps, and focus immediate interventions on the countries that will require the most effort. There has been a collaborative effort to identify partners within countries to focus on all aspects of the SAFE. The ITFDE believes that the logic for careful integration of LF and trachoma programs at the local, national, and continental levels, particularly in Africa, is persuasive, with mutual benefits in programmatic terms for both programs, as well as improved operational efficiencies.
6- Leprosy In 1873, in Norway, GH Armauer Hansen discovered Mycobacterium leprae, the first bacterium to be identified as causing disease in humans. Hansen’s disease is now better known as leprosy, a disease that mainly affects the skin, nerves, upper respiratory tract and eyes. Leprosy transmission still occurs continuously in some endemic areas in the world including Africa. The most likely route of transmission of leprosy is through aerosols, with contacts closest to a patient with leprosy, in particular within household contacts, having the highest risk of acquiring
23

the infection. It was once thought to be highly contagious and was treated with mercury, but it is curable with a collection of antibiotics, and early treatment averts most disabilities. Detection of leprosy is based on clinical signs and classified into paucibacillary (PB; ≤5 skin lesions) and multibacillary (MB; >5skin lesions) leprosy. Leprosy in children below 15 years old is a robust indicator of active source of infection in the community where they live. Early diagnosis in children can be hard because of the wide range of clinical aspects of the skin lesions and mainly due to the difficulty of performing the clinical peripheral nerve evaluation. A special focus on children to reduce disabilities and reduce transmission is one of the core areas of interventions of the global leprosy strategy 2016-2020 (31). Global elimination of leprosy has been a target for many years. In 1991, the World Health Assembly set a goal for “elimination of leprosy as a public health problem”, defined as a prevalence of less than 1 per 10,000, by the year 2000. More recently, the World Health Organization (WHO) has formulated new targets for leprosy, which include global interruption of transmission or elimination by 2020, and reduction of grade-2 disabilities in newly detected cases to below
24

1 per million population at global level by 2020. Currently, worldwide, more than 200,000new cases of leprosy are detected annually, with India, Brazil, Indonesia and sub-Saharan Africa. This incidence has remained fairly stable over the past decade (32).Leprosy continues to be a global public health problem, but draws less attention because 'prevalence based elimination' has been misinterpreted as eradication. The ongoing transmission of M. leprae has renewed interest in complete elimination. While many countries claim to have eliminated leprosy, clusters of cases remain, especially in poor and remote communities where stigma is still attached to the disease.Currently, the main strategies to control leprosy are early detection of cases, and treatment with multidrug therapy (32). Ongoing research is trying to develop better diagnostic tests and to advance chemoprophylaxis and immunoprophylaxis approaches. It is important to maintain leprosy expertise and improve the health professionals training for leprosy diagnosis, since we still have a long journey to reach leprosy elimination. The biological and technical feasibility of elimination is not certain and advanced microbiological and
25

operational research is necessary to understand transmission better (33). Helminths :
7- Taeniasis and cysticercosis These are caused by an infection with T. solium or T. saginata, and Swine are the intermediate hosts of T. solium, whereas cattle are the intermediate hosts for T. saginata. They are transmitted by eating raw or insufficiently cooked pork or beaf containing infective larvae. The T. solium parasite occurs most commonly in Southern Africa, China, India, Central America, Chile, Brazil, Papua New Guinea and non-Islamic South East Asia where human feces comes into contact with pigs and where pork may be eaten raw or undercooked. Taeniasis, and cysticercosis have been ranked as the most important food-borne parasitic diseases of humans in terms of public health, socioeconomic and trade impact. In 2010 it was estimated that approximately 300,000 individuals were infected with T. solium cysticercosis globally, resulting in over 28,000 deaths. Between 2.5 and 5 million people are estimated to harbor adult tapeworms of T. solium (34). In humans, the symptoms of taeniasis are subtle and mild and include abdominal distension, abdominal pain, digestive
26
disorders and anal pruritis but humans can also develop cysticercosis from the tapeworm larvae, which can be fatal. After being consumed in undercooked pork or beef that contains cysts, larvae can then migrate through the human body. When cysts develop in the brain, they cause neurocysticercosis (NCC) the symptoms of which include headaches, blindness, convulsions or epileptic seizures, paralysis, dementia, muscular or cardiac lesions may also be present or even death .The myocardial inflammatory response is variable and may result in granuloma formation and fibrosis. This may subsequently lead to arrhythmias and conduction abnormalities either spontaneously or during treatment. Cardiac involvement in cysticercosis has previously been thought to be rare, but autopsy studies have shown a prevalence of 20%–25% in patients with concomitant documented neurocysticercosis. Treatment of the disease can include surgery and/or long courses of the drugs; praziquantel and albendazole. WHO target: Scaled-up interventions in selected countries for control and elimination by 2020 (35, 36).
8- Dracunculiasis
27

Dracunculiasis (better known as guinea-worm disease) is a crippling disease caused by the parasite Dracunculus medinensis. It is long and grows up to a meter in length, a threadlike worm. It is transmitted exclusively when people drink water that has been contaminated with parasite-infected water fleas. After about a year of incubation, the female Guinea worm, one meter long, creates an agonizingly painful lesion on the skin and slowly emerges from the body. The guinea worm migrates through the body under the skin, causing severe pain, and eventually emerges (usually from the feet), causing an ulcer, fever, nausea and vomiting. Guinea worm sufferers may try to seek relief from the burning sensation caused by the emerging worm and immerse their limbs in water sources, but this contact with water stimulates the emerging worm to release its larvae into the water and begin the cycle of infection all over again. Guinea worm is a particularly devastating disease that incapacitates people for extended periods of time, making them unable to care for themselves, work, grow food for their families, or attend school. In 1986, the disease afflicted an estimated 3.5 million people a year in 21 countries in Africa and Asia (37).
28

There is no known curative medicine or vaccine to prevent Guinea worm disease. The same treatment for emerging worms has been used for thousands of years. Traditional removal of a Guinea worm consists of winding the worm around a piece of gauze or small stick and manually extracting it, a slow, painful process that often takes weeks. The skin lesions often develop secondary bacterial infections, which exacerbate the suffering and prolong the period of disability.When Ernesto Ruiz-Tiben, the head of Carter Center to work against guinea worm, began his work to eradicate guinea worm disease more than 30 years ago, he felt “it was going to be like dragging a dead elephant through a swamp by its tail.” But in 1981, health workers exhilarated by the recent eradication of smallpox, the first time in history that a human disease had been eliminated, made guinea worm their next target. Guinea worm disease is set to become the second human disease in history, after smallpox, to be eradicated. It will be the first parasitic disease to be eradicated and the first disease to be eradicated without the use of a vaccine or medicine (38). Through his non-governmental organization, former US President Jimmy Carter
29

championed the cause to eradicate guinea worm disease with corporates and heads of states. He also kept up pressure and accountability by visiting affected countries, even brokering a ceasefire in Sudan in the 1990s to allow health workers access to those at risk. Through a combination of health education, larvicides, water filters and dogged determination Carter program helped cut instances of the disease in 2016 to just 25 cases reported in four countries (South Sudan, Mali, Chad, and Ethiopia) (39). The Center's strategy is to work with ministries of health to stop the spread of Guinea worm disease by providing health education and helping to maintain political will. This has been achieved through community-based interventions to educate and change behavior, such as teaching people to filter all drinking water and preventing transmission by keeping anyone with an emerging worm from entering water sources. In Ghana, for example, the campaign’s success was accelerated by local communities’ commitment. Villagers, for example, deployed guards next to water where the infection was transmitted, and people were fined for wading in. The campaign to eradicate guinea worm offers important pointers to success and shows that
30

the battle against NTDs is far from hopeless (40). The impact and lessons learned from the concerted contribution of different stakeholders in campaign to eradicate guinea worm has set an example which can be followed for other diseases and can be summarized in the following points:
a- Incidences of Guinea worm disease have been reduced from an estimated 3.5 million in 1986 to 25 in 2016.
b- The Guinea worm eradication campaign has averted at least 80 million cases of this devastating disease among the world's poorest and most neglected people.
c- The campaign has helped to establish village-based health delivery systems in thousands of communities that now have networks of health personnel and volunteers who provide health education and interventions to prevent other diseases.
d- The advanced vision and clear road map to the final goal enabled Carter Center to lead the international Guinea worm disease eradication campaign, to compile and distribute case numbers, and to provide technical and financial support to national programs to interrupt Guinea worm disease transmission and bring
31

cases to zero. When transmission is interrupted, the Center provides continued assistance in developing or strengthening surveillance in Guinea worm-free areas and preparing nations for official certification.
e- The confidence imparted on National Ministries of Health in the endemic countries by the success in the campaign achieved annually enabled them to oversee domestic Guinea worm elimination programs and engage and train field workers and supervisory staff.
f-The final say on eradication has been totally assigned to World Health Organization to be responsible for certifying countries as Guinea worm-free, and is the only organization that can officially certify the eradication of a disease.
g- The U.S. Centers for Disease Control and Prevention provides technical assistance and verifies whether worms from final patients are truly Guinea worms.
h- UNICEF mainly assists countries by helping to provide safe sources of drinking water to priority areas identified by the national Guinea worm eradication programs.
32

i- If guinea worm is close to eradication, the last steps are proving extremely difficult since people involved get relaxed and loosen their attention to tackle the few remaining patients which lead to the wake up of the disease again. Thus, sustainability of efforts should be continued until the official declaration of eradication is declared by concerned authorities.
A new challenge to eradication has been the emergence recently of numerous Guinea worm infections in dogs. Guinea worm infections in domestic dogs in Chad were first detected in 2012. Most of those infections were apparently linked to dogs' consumption of fish and fish entrails containing Guinea worm larvae. Volunteers trained by Chad’s Guinea Worm Eradication Program with the Carter Center’s help have been encouraging people in those areas to bury fish discards, and cash rewards are being paid for reporting infected animals and for keeping them away from water sources. Also, researchers are actively seeking a remedy for canine infections, including the use of established veterinary deworming drugs. Substantial nonhuman infections have
33

not occurred in any other country during the eradication campaign. In January–December 2016, Ethiopia reported 14 infected dogs, and Mali reported 11. South Sudan's only known infected dog was reported in 2015 (41, 42).
9- Soil-transmitted helminthiases Soil-transmitted helminthiases by intestinal worms including roundworm, whipworm and hookworm are among the most common infections worldwide. They tend to affect the most deprived communities. They are transmitted by eggs present in human faeces, which in turn contaminate the soil in areas where sanitation is poor and sewage is left untreated. Infected children are physically, nutritionally and cognitively impaired. It is estimated that 576-740 million individuals are infected with hookworms worldwide. Of the infected individuals, about 80 million are severely affected. The major etiology of hookworm infections is due Necator americanus which is found in the Americas, sub-Saharan Africa, and Asia . Ancylostoma duodenale is found in more scattered focal environments, namely Europe and the Mediterranean. Most infected indi-viduals are concentrated in sub-Saharan Africa, East Asia, and the Pacific Islands with each region having estimates of 198 million
34

and 149 million infected individuals, respectively (43). The World Health Organization’s (WHO) policy for control of the soil transmitted helminths (STH) largely centers on two groups, preschool aged children (pre-SAC), and school-aged children (SAC). The strategy for treatment is based on the argument that pre-SAC and SAC often harbor heavy infection which will have a detrimental impact on anemia, child growth, and development. Although this largely holds for Ascaris lumbricoides and Trichuris trichuria, where the intensity of infection is highest in these age groupings, it holds less well for the hookworm species since infection is often greatest in adults (43). The current WHO guidelines focus on SAC, both for monitoring infection and as a target for treatment, although treatment of pre-SAC and women of childbearing age is also recommended where sustainable delivery mechanisms exist, especially in areas of intense transmission. The guidelines recommend treating SAC annually where any STH prevalence falls between 20 % and 50 % and twice a year where it exceeds 50 % (44) .WHO aims to scale up mass drug administration (MDA) for STH, so that by 2020, 75 % of the pre-SAC and SAC in need
35

will be treated regularly. Progress has been good in some areas, but less so in others. Pharmaceutical companies who manufacture the main anthelmintics have continued to increase drug donations. In 2013, global coverage of those in need was 39 % for SAC and 49 % for pre-SAC (45). In 2015, STH moved from yellow to green in the progress score card chart (recently developed by Uniting to Combat NTDs), in part due to better coordination between UNICEF and WHO which has led to an improvement in reporting of coverage for pre-SAC. The coverage in this age grouping now exceeds 50 %. Coverage in SAC is reported as 39 %, which, it is argued in the report, is on track for a 75 % target in 2020 (46).
36

10- Foodborne trematodiasesFoodborne trematodiases are a group of infections caused by trematode worms (known as flatworms or flukes). People become infected by eating raw or poorly cooked fish, crustaceans and vegetables that harbor the minute larvae of the parasites. Recent estimates indicate that at least 56 million people suffer from one or more foodborne trematode infections (clonorchiasis, opisthorchiasis, fascioliasis, paragonimiasis and others). Cases of trematodiases have been reported from more than 70 countries worldwide. However, tropical fasciolosis caused by Fasciola
37

gigantica infection is one of the major diseases infecting ruminants in the tropical regions of Asia and Africa, and causes a significant economic loss in livestock industry in developing and underdeveloped countries for more than 3.2 billion US dollars per annum. The WHO is working to expand preventive chemotherapy to include foodborne trematode infections and ensure that their worst consequences (cancers of the bile duct) are fully prevented. All foodborne trematode infections can be treated with praziquantel or triclabendazole. The WHO has been aiming to control morbidity due to foodborne trematodiases by the inclusion of these infections in the mainstream preventive chemotherapy strategy with the necessary veterinary public-health support. By 2020, 75% of the at-risk population will have been reached by preventive chemotherapy and morbidity associated with foodborne trematode infections will be under control in 100% of the endemic countries (47).
11- Lymphatic filariasisLymphatic filariasis (LF) commonly known as elephantiasis, is a mosquito-transmitted parasitic disease caused by infection with Wuchereria bancrofti, Brugia malayi, or B.
38

timori, in tropical and subtropical regions. The mosquitoes carry the larvae of threadlike worms which nest in the human lymphatic system. People of all ages can be infected and symptoms of an infection in childhood can appear much later in life. These worms live in, and cause blockage of, the lymphatic system that normally returns fluids in our extremities to the circulatory system. This blockage results in fluid collection in the tissues (most commonly the legs and genitalia), severe swellings, and periodic fevers from bacterial infections of the collected fluids. A long-standing infection with lymphatic filariasis results in an irreversible condition called elephantiasis, in which there is a marked enlargement and hardening of the limbs so that they resemble those of an elephant, and patients suffer from persistent recurring fevers (48). Approximately 120 million people are infected by lymphatic filariasis, and 1.1 billion are at risk of infection. In endemic communities as many as 10 percent of women and men can be affected with swollen limbs, and 50 percent of men can suffer from the mutilating disease of their genitals. These physical disfigurations result in social stigma with significant social and economic consequences for patients, families, and
39

communities. The devastating effect on the quality of life of victims, impacts them not only physically but also emotionally and economically (49). Global Program for Elimination of LF (GPELF) was launched in 2000 following a World Health Assembly resolution (WHA50.29) to eliminate lymphatic filariasis as a public health problem. LF was endemic in 73 countries with 1.2 billion individuals at risk of infection and considered by WHO as one of the leading causes of global disability. The global LF elimination strategy includes stopping the spread of infection through annual Mass Drug Administration( MDA) of albendazole together with either ivermectin or diethylcarbamazine (DEC) to eligible individuals in affected areas for 4-6 years, and alleviation of suffering through morbidity management and disability prevention (MMDP). Long-lasting insecticidal nets have also shown to be effective in interrupting LF transmission in areas where anopheles mosquitoes are vectors. MDA has been implemented in 63 of the 73 endemic countries. With 556 million people in 39 countries treated during 2015, the cumulative total of treatments since 2000 now exceeds 6.2 billion (50).
40

In areas that have completed at least five rounds of MDA at effective population coverage (>65%) and lowered infection prevalence in sentinel and spot-check communities to less than 1% microfilaremia or 2% antigenemia, an initial transmission assessment survey-1 (TAS1) is recommended. TAS1 is used to determine whether parasite prevalence has been reduced below sustainable transmission levels and MDA can stop. Additional post-MDA surveys (TAS2 and TAS3) are recommended at 2-3 year intervals to confirm that transmission has not recrudesced or been reintroduced. Since the development of the TAS methodology, 524 surveys have been conducted in 41 countries to evaluate the impact of MDA. Progress in achieving stop-MDA criteria, as measured by the proportion of endemic implementation units (IUs) that have passed TAS1, varies by WHO region: from14% in Africa, to 41% in the Americas, 77% in the Eastern Asia (51). The Carter Center is working with national ministries of health in several countries to eliminate lymphatic filariasis including Ethiopia and, Nigeria which are among the most endemic worldwide. Carter Center assists countries to distribute the drugs Mectizan, donated by Merck, albendazole,
41

donated by GlaxoSmithKline, and DEC, donated by Eisai. These medicines are taken in combination (Mectizan and albendazole in Africa; DEC and albendazole in Hispaniola) to stop mosquitoes from transmitting the parasite from infected to uninfected people. The Center also has assisted in the distribution of long-lasting insecticidal bed nets (LLINs) to protect pregnant women and children who cannot take drug treatment. LLINs have the added benefit of protecting against other mosquito-borne diseases, such as malaria (52).The monitoring and epidemiological assessment of mass drug administration in the global program eliminate lymphatic filariasis showed that in 1,250 Implementation units (IUs) with a cumulative population of 351 million persons there is no longer need for MDA. A total of 18 countries have halted MDA nationwide and six of these (Cambodia, Cook Islands, Maldives, Niue, Sri Lanka and Vanuatu) were acknowledged by WHO as having eliminated LF as a public health problem. Nonetheless, 2,738 IUs across 54 countries, with approximately 946 million people, are still considered to require MDA to achieve elimination targets (51). GPELF currently faces numerous challenges in order to meet the goal of LF elimination by
42

2020. First, 29 countries have either not started MDA or have not achieved 100% geographic coverage of endemic IUs. These countries are not on target to stop MDA by 2020 under current WHO guidelines. Thus, urgent support is needed to initiate MDA in all endemic IUs in these 29 countries. Alternative MDA strategies that could reduce the number of rounds or time required to achieve elimination targets also are needed. Clinical trials are currently underway to determine if combination- triple drug therapy with ivermectin, DEC, and albendazole (IDA) is safe and superior to currently recommended two-drug regimens. These include DEC-albendazole used in areas outside of Africa and ivermectin-albendazole used in Africa, because of the potential for DEC-associated severe adverse reactions in individuals infected with Onchocerca volvulus use of ivermectin with DEC is contraindicated in areas endemic for Loa loa. Data from a pilot study in heavily infected individuals in an MDA-naïve area of Papua New Guinea (PNG) indicate that 100% (n=12) of individuals treated with the triple( IDA) were microfilaremia negative after 12 months compared to only one of 12 individuals treated with DEC plus albendazole. No serious adverse events were observed.
43

Reported adverse events were mild to moderate, resolved within 72 hours, and correlated with baseline levels of microfilaremia. Based on these results, modeling data indicate that IDA would decrease the number of rounds of MDA required to reach elimination thresholds. In 2015, only 75% of IUs achieved effective coverage (>65% of the total population) during MDA. Where effective coverage is not achieved, more MDA rounds are required to reduce infection below elimination thresholds. To maximize coverage WHO recommends to utilize distribution strategies acceptable by the communities targeted and directly observed treatment.
The success of the joint programs has demonstrated that one community-based health education and drug distribution system can support the control and elimination of multiple diseases. In Nigeria: Between 2000 and 2011, The Carter Center and the Nigeria Federal Ministry of Health worked together to protect 4 million people from lymphatic filariasis in Plateau and Nasarawa states through community health education, delivery of LLINs and 33 million drug treatments for lymphatic
44

filariasis and river blindness between 2000 and 2011. In 2012, it was confirmed that lymphatic filariasis transmission had stopped. Post-treatment surveillance is currently underway to assure that the parasite is not reintroduced into the area. In 2014, with support from The Carter Center, the Nigeria Federal Ministry of Health and other partners issued co-implementation guidelines for a coordinated effort to eliminate malaria and lymphatic filariasis. The guidelines called for shared interventions such as health education, community based action, distribution of long-lasting insecticidal bed nets, and mass drug administration. These are the first of their kind in Africa. In Ethiopia: In 2009, The Carter Center began integrating mass drug administration to prevent lymphatic filariasis with river blindness and malaria control in the Gambella Region. Subsequently the program expanded to eighteen districts, and delivered more than 1.1 million treatments in 2015 (51).
45

12- Onchocerciasis
46

Human onchocerciasis or river blindness is caused by the filarial nematode Onchocerca volvulus. Tiny black flies that live by fast-flowing water spread the filarial worms, from person to person. The disease is mostly found in remote villages where inhabitants subsist on farming. Once inside the body, the larvae of the worms migrate to the skin, eyes and other organs, where they grow into adult worms that can live in the body for up to 15 years. The disease causes skin lesions, severe itching and visual impairment, including permanent blindness, reduces an individual's ability to work and learn, and can shorten life expectancy by up to 15 years. More than 99 per cent of infected people live in 31 countries in sub-Saharan Africa (53).
It is earmarked for elimination by the World Health Organization (WHO) as articulated by the 2012 Roadmap (54) and the London Declarationon Neglected Tropical Diseases (55). The principal strategy to achieve elimination is mass drug administration (MDA) with ivermectin. Ivermectin kills the skin-dwelling microfilariae (mf) that are the progeny of adult O. volvulus and are
47

infectious to biting blackfly species vectors. Ivermectin may also kill and/or sterilize adult worms. Multiple rounds of mass treatment are effective in lowering the prevalence and intensity of onchocerciasis, and if given for long enough at high enough coverage, can lead to the interruption of transmission and elimination of the infection. Mass drug administration programs, in which the entire population of an area is treated (biannual, without first being tested for infection, has helped eliminate onchocerciasis (river blindness) from several countries in the Americas. The Carter Center has been working with national ministries of health in Latin America and Africa to eliminate river blindness. Together with the Ministries of Health and partners, the Carter Center's Onchocerciasis Elimination Program for the Americas has successfully eliminated river blindness transmission from Colombia (2013), Ecuador (2014), Mexico (2015), and Guatemala (2016) (56). Good progress towards elimination has also been made in Africa which bears 99% of the onchocerciasis burden, with notable successes in regions of Mali, Senegal, Nigeria, Sudan and eastern Uganda. The Carter Center currently assists ministries of health in six nations to eliminate river
48

blindness through health education and mass distribution of the medicine Mectizan, donated by Merck. The Center and its partners have successfully broken river blindness transmission in Uganda and Sudan by providing twice per year Mectizan treatments. The successes have spurred river blindness elimination projects in Ethiopia and Nigeria. However, there are conspicuous regions of ongoing transmission despite years of intervention in Ghana, Cameroon and northwestern Uganda, and evidence of recrudescence in Burkina Faso also exists (57, 58).
13- Schistosomiasis
49

Schistosomiasis or bilharzia is a water-borne parasitic infection that results in a debilitating chronic disease with extensive morbidity and organ pathology. It is endemic in 76 countries worldwide, with about 207 million people infected of which 123 million are children. The majority (88%) of the people infected with schistosomiasis live on the African continent. There are two major types of schistosomiasis disease manifestations: urogenital schistosomiasis (most prevalent in Africa) caused by Schistosoma haematobium, and intestinal schistosomiasis, caused by, depending on the tropical region of the world, either S. intercalatum, S. mansoni, S. japonicum, S. guineensis or S. mekongi. Schistosomiasis is implicated in several clinical conditions including bladder cancer leading to death, liver cirrhosis, hydronephrosis, reproductive complications, and human immunodeficiency virus (HIV) transmission and fast progression to acquired immune deficiency syndrome (AIDS) in adults. It is the most deadly of the neglected tropical diseases and it is the second most common parasitic disease, after malaria. In children the disease is associated with stunting and reduced ability to learn, malnutrition, poor cognitive development, iron-deficiency anaemia and reduced school
50

performance in the high-risk age group (5–15 years). In terms of socioeconomic and public health impact, schistosomiasis is second only to malaria as the most devastating parasitic disease in tropical countries (59).People are infected during routine agricultural, domestic, occupational and recreational activities which expose them to infested water. It is caught through fresh water that contains the larvae of worms. The parasite can live for years in the veins near the bladder or intestines, laying eggs that pass out of the body in urine or feces and reinfect water sources. Snails are infected when fresh water is contaminated by eggs excreted in human urine and feces. Infected snails release larvae that infect humans when they expose their skin to water contaminated by the snails. In children and infants, the clinical presentation may include fever, rigor, sweating, headache, general muscular pain, gastrointestinal disturbances, enlargement and tenderness of the liver, and eosinophilia. Heavily infected patients are usually very sick with a high fever, which may lead to death. Most subjects with the infection in endemic areas are chronic cases, with the infection reported to have started during the
51

early years of growth and exposure to the infective sources. Most children below the age of five are symptomless, while some are slightly symptomatic and the impact to their general growth is usually not significant. While the preschool age determines the extent of the disease in later age, if not treated in time, the disease may become advanced causing higher morbidity. Other patients may have a latent symptomless infection all their life. Most of the mortality of schistosomiasis is seen in the advanced stage of the disease (59).The clinical assessment of infection and morbidity due to schistosomiasis has mainly been based on haematuria and the presence of eggs in either urine or stool, but regular monitoring is needed to diagnose the disease as it is often asymptomatic. Detailed confirmation of infection for surveillance purposes, however, has been based on prevalence, infection intensity, clinical presentations and mortality. Introduction of mass treatment has resulted in a sharp decrease of the prevalence as well as the intensity of infection, and the morbidity of the disease has significantly declined (60). Nigeria is the most endemic country for schistosomiasis, with approximately 20 million people, mostly children, needing
52

treatment. For schistosomiasis, main control strategy is preventive chemotherapy in which several countries in Africa have now embarked. National schistosome control programs utilizing mass drug administration (MDA) are targeting primary school-aged children following treatment regimens recommended by the World Health Organization (WHO). The Carter Center assists the Nigerian Ministry of Health in providing health education and the drug praziquantel to treat schistosomiasis in six states ; Delta, Ebonyi, Edo, Enugu, Nasarawa, and Plateau; where the burden of the disease is greatest. Schistosomiasis is controlled and treated easily with a single annual dose of praziquantel which can reverse up to 90 percent of the damage caused by the parasite(60). The World Health Organization, Merck (Germany), and many additional partners have made possible the delivery of more than 10 million praziquantel treatments by the Carter Center in Nigeria since 1999. Blood in school children's urine, a telltale sign of schistosomiasis infection, has been reduced by approximately 94 percent in Plateau and Nasarawa states and approximately 88 percent in Delta state.
53

A Carter Center-assisted effort has shown that treatments for schistosomiasis can be delivered at the same time as interventions against lymphatic filariasis and river blindness, helping the ministry of health implementing programs more efficiently through one community-based health education and drug distribution system instead of separate programs for each disease. However, for successful elimination, the approach needs to be strengthened by integrating other control methods such as early diagnosis and coverage of the whole population in endemic areas, as well as integrating these efforts with snail elimination (61). Global control efforts need to be inclusive of other stakeholders such as primary care health centers, family health clinics and primary school health initiatives, as well as other sectors such as agriculture, occupations working in the aquatic environment and, of course, water and sanitation programs. Inclusive preventative chemotherapy programs targeting all sectors of the population including out-of-reach communities and children out of school, together with the control of the snail
54

intermediate host and health education, would have a greater and longer-lasting impact than chemotherapy alone. This also means that for elimination to be successful, all animals and human reservoirs of infection must be targeted for treatment, which translates into targeting whole populations in endemic areas.Furthermore, individuals acquire the infection, usually repeated and heavy, during childhood. However, after schistosomiasis infection control, there is usually successful transmission control, yet individuals can still develop clinical disease. This is likely to occur in young children and individuals with high water contact such as women. Therefore, disease control is still needed in the post-transmission period, in which at-risk populations are monitored. This is a problem in post-mass treatment for schistosomiasis control in the post-transmission period and so surveillance and suitable intervention are needed in areas where transmission is interrupted. Currently, the goals for neglected tropical disease control and research are shifting from control to elimination as articulated in the Sustainable Development Goal ( 62)
55
14- Echinococcosis Human echinococcosis is a zoonotic disease that is caused by parasites, namely tapeworms of the genus Echinococcus. Echinococcosis occurs in 4 forms: cystic echinococcosis, also known as hydatid disease or hydatidosis, caused by infection with Echinococcus granulosus; alveolar echinococcosis, caused by infection with E. multilocularis; polycystic echinococcosis, caused by infection with E. vogeli; and unicystic echinococcosis, caused by infection with E. oligarthrus. The two most important forms, which are of medical and public health relevance in humans, are cystic
56
echinococcosis (CE) and alveolar echinococcosis (AE) (63).The disease has the highest incidence in countries where sheep are raised with the help of dogs. In endemic regions, human incidence rates for HD can reach >50/100,000 person-years, and prevalence levels as high as 5%–10% may occur in parts of East Africa, Central Asia China, Argentina, and Peru. Both cystic echinococcosis and alveolar echinococcosis represent a substantial disease burden. More than 1 million people are affected with echinococcosis at any one time. Echinococcosis is often expensive and complicated to treat, and may require extensive surgery and/or prolonged drug therapy. Many of these people will be experiencing severe clinical syndromes which are life-threatening if left untreated. Even with treatment, people often face reduced quality of life. For cystic echinococcosis, there is an average of 2.2% post-operative death rate for surgical patients, and about 6.5% of cases relapse after an intervention, thereby requiring prolonged recovery time. Unfortunately, in many patients the disease is diagnosed at an advanced stage. As a result, if palliative surgery is carried out without complete and effective anti-infective treatment, frequent relapses will occur.
57

In livestock, the prevalence of cystic echinococcosis found in slaughterhouses in hyperendemic areas of South America varies from 20%–95% of slaughtered animals. The highest prevalence is found in rural areas where older animals are slaughtered. Depending on the infected species involved, livestock production losses attributable to cystic echinococcosis result from liver condemnation and may also involve reduction in carcass weight, decrease in hide value, decrease of milk production, and reduced fertility. The 2015 WHO Foodborne Disease Burden Epidemiology Reference Group (FERG) estimated echinococcosis to be the cause of 19 300 deaths and around 871 000 disability-adjusted life-years (DALYs) globally each year. Annual costs associated with cystic echinococcosis are estimated to be US$ 3 billion for treating cases and losses to the livestock industry. WHO is working towards the validation of effective cystic echinococcosis control strategies by 2020. Prevention programs focus on deworming of dogs and sheep, which are the definitive hosts. In the case of cystic echinococcosis, control measures also include improved food inspection, slaughterhouse hygiene, and public education campaigns. Vaccination of
58
lambs is currently being evaluated as an additional intervention (64). Humans are infected through ingestion of food, water or soil, contaminated with parasite- eggs containing the larval tapeworm (oncosphere) which is produced by the adult tapeworm inhabiting the small intestine of dogs. Eggs excreted in the feces of dogs are dispersed widely in the environment. Human and sheep are intermediate hosts which become infected by accidental consumption of water or food that has been contaminated. Oncospheres penetrate the intestine and are carried through bloodstream where they are filtered out in various organs.The most common hydatid cyst sites in humans are the hepatic filter, 60%–70% of cases, followed by lung and brain. Several distinct genotypes of E. granulosus are recognized, some having distinct intermediate host preferences. Some genotypes are considered species distinct from E. granulosus. Not all genotypes cause infections in humans. The genotype causing the great majority of cystic echinococcosis infections in humans is principally maintained in a dog–sheep–dog cycle, yet several other domestic animals may also be
59
involved, including goats, swine, cattle, camels and yaks. Human infection with E. granulosus leads to the development of one or more hydatid cysts located most often in the liver and lungs, and less frequently in the bones, kidneys, spleen, muscles, central nervous system and eyes. The asymptomatic incubation period of the disease can last many years until hydatid cysts grow to an extent that triggers clinical signs, however approximately half of all patients that receive medical treatment for infection do so within a few years of their initial infection with the parasite. Abdominal pain, nausea and vomiting are commonly seen when hydatids occur in the liver. If the lung is affected, clinical signs include chronic cough, chest pain and shortness of breath. Other signs depend on the location of the hydatid cysts and the pressure exerted on the surrounding tissues. Non-specific signs include anorexia, weight loss and weakness. Alveolar echinococcosis usually occurs in a wildlife cycle between foxes, other carnivores and small mammals (mostly rodents). Domesticated dogs and cats can also be infected. It is characterized by an asymptomatic incubation period of 5–15 years and the slow development of a primary tumor-like lesion which is usually located in
60

the liver. Clinical signs include weight loss, abdominal pain, general malaise and signs of hepatic failure. Larval metastases may spread either to organs adjacent to the liver (for example, the spleen) or distant locations (such as the lungs, or the brain) following dissemination of the parasite via the blood and lymphatic system. If left untreated, alveolar echinococcosis is progressive and fatal. Ultrasonography imaging is the technique of choice for the diagnosis of both cystic echinococcosis and alveolar echinococcosis in humans. This technique is usually complemented or validated by computed tomography (CT) and/or magnetic resonance imaging (MRI) scans. Cysts can be incidentally discovered by radiography. Specific antibodies are detected by different serological tests and can support the diagnosis. Biopsies and ultrasound-guided punctures may also be performed for differential diagnosis of cysts from tumors and abscesses. There are several options for the treatment of cystic echinococcosis: percutaneous treatment of the hydatid cysts with the PAIR (Puncture, Aspiration, Injection, Re-aspiration) technique, surgery, anti-infective
61

drug treatment “watch and wait”. The choice must primarily be based on the ultrasound images of the cyst, following a stage-specific approach, and also on the medical infrastructure and human resources available. For alveolar echinococcosis, early diagnosis and radical (tumor-like) surgery followed by anti-infective prophylaxis with albendazole remain the key elements. If the lesion is confined, radical surgery can be curative. Early detection of E. granulosus and E. multilocularis infections, especially in low-resource settings, is still needed in addition to the evaluation of clinical treatment options. Further assessment and potential commercialization of a vaccine for E. granulosus recombinant oncosphere antigen (EG95) is on trial in sheep to impede E. granulosus infection of lambs. This could supplement control measures such as the treatment of dogs and culling of older sheep. Robust surveillance data is fundamental in order to show burden of disease and to evaluate progress and success of control programs. However, as for other neglected diseases which are focused in underserved populations and remote areas, data is especially scarce and will need more
62

attention if control programs are to be implemented and measured (64).The WHO Informal Working Group on Echinococcosis (WHO-IWGE) continues to identify priorities to develop guidance on detection and clinical management of cystic echinococcosis through improved case detection and management. The group is also working to promote the collection and mapping of epidemiological data. Morocco finished a project aimed at decentralizing diagnostic and therapeutic techniques and promoting the PAIR (puncture, aspiration, injection, re-aspiration) strategy in rural and hyperendemic areas. As a complement, the emphasis needs to be put on prevention in the animal and food safety sector. Mongolia has recognized the importance of echinococcosis as a public-health problem and, at the request of the Ministry of Health, WHO in 2013 conducted an initial situation analysis. The analysis focused on implementing early diagnosis and building a basic surveillance system covering humans and animals to understand the actual burden of the disease. No significant investment for echinococcosis has been made, and therefore programmatic progress has stalled. China is integrating echinococcosis prevention, control and treatment in their economic and
63

development plans to raise attention to the vast problem in the country, especially the Tibetan plateau, as well as in the Central Asian Republics (64).
Protozoa
15- Chagas disease Chagas disease was first described in 1909 by the Brazilian scientist Carlos Ribeiro Justiniano Chagas (1879-1934). It is also known as American trypanosomiasis, and it is potentially life-threatening illness. The etiologic agent that causes Chagas disease is the protozoan parasite Trypanosoma cruzi (T. cruzi). The parasite is transmitted by the reduviid bug, a member of the Triatomine
64

subfamily, popularly known as the kissing bug. Chagas disease is classified as one of the 17 most important neglected diseases by the World Health Organization (WHO). Estimates of the number of infected individuals in the world have decreased from approximately 20 million in 1981, to 7-8 million in 2014. The majority of infected individuals live in 21 countries of Central and South America. Though once confined to the Americas, the disease has spread to other continents over the past century as global population movements have increased. Estimates of mortality attributable to Chagas disease vary considerably (between 0.2% and 19.2% annually) (65, 66).Many people infected show no symptoms during the disease’s initial phases, after which the parasite moves to the muscles of the heart or bowels, where it can cause severe damage to organs. Transmission may also occur by blood or organ transplant, contaminated food, from mother to child and due to laboratory accidents. In humans, Chagas disease manifests in two phases, acute and chronic. The acute phase has mild symptoms that may last for approximately two months. In the chronic phase, the majority of cases are of the asymptomatic indeterminate form, which may last a
65
lifetime. Individuals in the chronic phase of the disease with normal electrocardiogram (EKG) and normal chest and esophagus X- rays are considered individuals in the indeterminate form of the disease, whereas, clinically apparent chronic disease form is divided into a cardiac, gastrointestinal, or combined form. The most important health consequence of Chagas disease is cardiomyopathy, which over a lifetime occurs in 20 to 40% of infected persons with an incidence rate of 1.85% per person-year. There is no vaccine for Chagas disease, although some cases can be treated with the drug benznidazole. WHO target: Prevention of transmission in households in the Americas by 2020 (65, 67).
16- Leishmaniasis Leishmaniasis is a parasitic spectral neglected disease caused by intracellular protozoan parasite, Leishmania and transmitted by the bite of a certain female sandflies of Phlebotomus and Lutzomyia species. It ranks third in disease burden in disability-adjusted life years (DALY) caused by neglected tropical diseases and is the second most frequent cause of parasite-related deaths after malaria. However, most people infected by the leishmania parasite do
66

not develop any symptoms at all, so the term refers to the fact of becoming sick due to an infection and not merely being infected. It is endemic in 98 countries and causes significant morbidity and mortality in both rural and urban areas worldwide. Phenomena such as globalization and human migration, as well as the increased volume of international travel have extended its prevalence in developed countries. In addition, the incidence of leishmaniasis as an opportunistic disease has increased in recent years because of the growing number of patients with immune depression secondary to chronic illness, neoplasm, transplant and HIV infection, thereby constituting a public health problem. Overall, annual prevalence is 12 million and the population at risk is approximately 350 million. Leishmaniasis is classified as cutaneous, visceral and mucocutaneous by clinical manifestations and it is among the world’s six major tropical diseases. Mucocutaneous leishmaniasis (MCL) and visceral leishmaniasis (VL) are associated with significant morbidity and mortality. If left untreated, the fatality rate of VL is as high as 100%; in some areas. Cutaneous leishmaniasis (CL) and visceral leishmaniasis (VL) are present in 14 of the 22 countries of the Eastern Mediterranean
67

Region. Iran is an endemic country for both CL and VL (68, 69).The global burden of visceral leishmaniasis (VL) alone is estimated at 0.2 to 0.4 million cases, resulting in 50,000 deaths every year. Eastern Africa is the second-highest-burdened region, after the Indian subcontinent. VL suppresses the immune response, and epidemics in populations affected by malnutrition or displacement can be severe (70). More than 70% of cutaneous leishmaniasis (CL) cases were reported from Afghanistan, Algeria, Colombia, Brazil, Iran, Syria, Ethiopia, North Sudan, Costa Rica and Peru. CL is endemic in half of the 31provinces of Iran, and is a great health problem. In most countries CL is under-reported, therefore it is difficult to estimate the real number of the cases, however about 0.7-1.2 million cases per year have been estimated. CL common in many parts of Afghanistan and Syria has been spread through the region by the displacement of people in the recent armed conflicts. CL is generally mild but may cause cosmetic disfigurement. Mucocutaneous disease is due to extension of local skin disease into the mucosal tissue via direct extension ( 71).
68
Combined WHO’s Roadmap and the London declaration have accelerated interventions since 2012 with significant levels of progress. There was 82% reduction in reported cases of visceral leishmaniasis (VL) in Bangladesh, India and Nepal. WHO target is the elimination of the visceral form on the Indian subcontinent by 2020 (72).
17- Sleeping sickness
Sleeping sickness (human African trypanosomiasis, HAT) is transmitted by the bite of the Glossina, commonly known as the tsetse fly. Trypanosomes cause a variety of diseases in man and domestic animals in Africa, Latin America and Asia. In the
69

Trypanozoon subgenus, Trypanosoma brucei gambiense and T. b. rhodesiense cause human African trypanosomiasis, while T. b. brucei, T. evansi and T. equiperdum are responsible for nagana, surra and dourine in domestic animals, respectively. The disease mostly affects poor communities in rural Africa and infected people typically suffer fevers, headaches and joint pains followed by confusion, poor co-ordination, numbness and trouble sleeping. HAT is a neglected tropical disease, with a population of 70 million at risk. In the 1930s, colonial administrations established programs to combat the disease, treating millions. By the early 1960s, sleeping sickness had almost been controlled. The rarity of new cases led to retreating of interest and gradually the disease crept back. In the last decade of the 20th century, the number of cases of HAT, reached alarming levels. In reaction to this epidemiological situation of a lethal disease, a number of stakeholders came together to support the affected countries. In the early years of the 21st century, the World Health Organization (WHO) launched a public-private partnership that, together with important efforts from bilateral cooperation and non-governmental organizations (NGOs),
70

enabled to reverse the epidemiological trend. In this process, the key role was played by the National Sleeping Sickness Control Programs (NSSCPs) of endemic countries and their committed health workers. The steady reduction in the number of HAT cases reported during the first decade of the current century prompted first the HAT focal points of endemic countries, then the WHO Strategic and Technical Advisory Group on Neglected Tropical Diseases (NTDs) and finally the WHO Expert Committee on control and surveillance of HAT to set the elimination of HAT as a goal. Combined WHO’s Roadmap and the London declaration have accelerated interventions since 2012 with significant levels of progress after HAT has been included in the WHO NTD roadmap as one of the diseases targeted for elimination as a public health problem by 2020. This progress has been demonstrated by 89% drop in new human African trypanosomiasis (HAT) cases between 2000 and 2015 (73, 74, 75).
71

18- MycetomaMycetoma is a common neglected tropical disease, endemic in many tropical and subtropical regions. It can be caused by bacteria (actinomycetoma) or fungi (eumycetoma) and typically affects poor communities in remote areas. It is an infection of subcutaneous tissues resulting in mass and sinus formation and a discharge that contains grains. The lesion is usually on the foot but all parts of the body can be affected. The causative microorganisms probably enter the body by a thorn prick or other lesions of the skin. Mycetoma has a worldwide distribution but is restricted to specific climate zones. Microbiological diagnosis and characterization of the exact
72
organism causing mycetoma is difficult; no reliable serological test exists but molecular techniques to identify relevant antigens have shown promise. Despite its distressing deformities, disability, high morbidly, and negative socioeconomic impacts on patients, communities, and health authorities it enjoys meagre national and international attention and recognition (76). To date, the actual disease incidence and prevalence and infection route are not well characterized, likewise, its susceptibility, resistance and response to medical treatment. This has been reflected on the available treatment and control modalities which proved to be ineffective. A major problem in mycetoma is that most of the patients are of poor socio-economic and health education status and hence the late presentation, poor treatment compliance and high follow-up dropout rates. The lack of national and international attentiveness and awareness on the disease has led to a massive knowledge gap in mycetoma that had significantly and adversely affected patient care and management and proper planning for mycetoma preventative measures. It is still challenging and hard to treat patients with mycetoma; in particular eumycetoma. The current treatment is still not optimal and
73
disappointing. To cure, this disease both extensive and destructive surgery and prolonged antifungals treatment are necessary. With the current drugs, ketoconazole and itraconazole, improvement has been demonstrated, but cure rates for eumycetoma are still significantly lower than cure rates for actinomycetoma. These drugs need an extended period to affect a partial cure, they have many side effects and contraindicated during pregnancy and lactation. The prolonged use of the available drugs proved to be not cost effective for the health authorities and patients. Surgery is curative in early cases but the fact that patients present late made its outcome to be stigmatizing due to the massive mutilating surgical excisions or amputation (10, 76).
74

The progress in control or elimination of NTDs The WHO has been the major actor and coordinator of efforts to fight against NTDs. It succeeded to bring many global stakeholders together in one forum. The first global partners’ meeting on NTDs was held in 2007, and adopted the theme, “Collaborate. Accelerate. Eliminate”. The meeting marked a turning point in global efforts to control and eliminate these poverty-related diseases. Following the meeting a group of global partners who agreed to tackle NTDs together, a variety of local and international stakeholders have worked alongside ministries of health in endemic countries to
75

deliver quality-assured medicines, and provide people with care and long-term management. In 2012 and inspired by the WHO NTD Roadmap, partners signed the London Declaration on Neglected Tropical Diseases through which they pledged to support WHO in the control and elimination of 10 neglected tropical diseases by 2020 (8, 47, 55). In the most recent Global Partners’ Meeting in Geneva, 19 April 2017, WHO presented the fourth report which showed remarkable achievements in the fight against NTDs. Representatives of Member States, donor agencies, foundations, the private sector, academia and various stakeholders attended the meeting. The fourth report reflected the achievements of the past decade, and declared to sustain support towards the 2020 WHO Roadmap targets, and called on partners to facilitate availability of resources needed beyond 2020. Among the achievements of the past decade an estimated 1 billion people received treatment in 2015 alone. “WHO has observed record-breaking progress towards bringing ancient scourges like sleeping sickness and elephantiasis to their knees,” said WHO EX-Director-General, Dr Margaret Chan. “Over the past 10 years, millions of people have
76

been rescued from disability and poverty, thanks to one of the most effective global partnerships in modern public health”. In a recently published WHO report, Integrating neglected tropical diseases in global health and development, it has been clearly demonstrated how strong political support, generous donations of medicines, and improvements in living conditions have led to sustained expansion of disease control programs in countries where these diseases are most prevalent (9) . The following are the key achievements from 2007 onwards. One billion people were treated for at least one neglected tropical disease in 2015 alone, and 1 billion people in 88 countries have benefited from preventive chemotherapy in 2014. Five hundred and fifty six million people received preventive treatment for lymphatic filariasis (elephantiasis) and more than 114 million people received treatment for onchocerciasis (river blindness); 62% of those requiring it. Only 25 human cases of Guinea-worm disease were reported in 2016, putting eradication within reach. Cases of human African trypanosomiasis (sleeping sickness) have been reduced from 37000 new cases in 1999 to well under 3000 cases in 2015 (9).
77

Trachoma, the world’s leading infectious cause of blindness has been eliminated as a public health problem in Mexico, Morocco, and Oman. More than 185 000 trachoma patients had surgery for trichiasis worldwide and more than 56 million people received antibiotics in 2015 alone (29). Concerning visceral leishmaniasis in 2015, the target for elimination was achieved in 82% of sub-districts in India, in 97% of sub-districts in Bangladesh, and in 100% of districts in Nepal. Only 12 reported human deaths were attributable to rabies in the WHO Region of the Americas in 2015, bringing the region close to its target of eliminating rabies in humans by 2015. However, the report highlights the need to further scale up action in other areas especially Sub Saharan Africa. Besides celebrating 10 years of multi-stakeholder collaboration, the Global Partners’ Meeting (GPM) on NTDs in Geneva, on19 April 2017 marked the 5th anniversary of the WHO NTD Roadmap which established targets and milestones for the global control, elimination, and eradication of many of these diseases. The GPM also followed the progress of the London Declaration of 2012 which has recorded increased commitments of donated drugs for visceral leishmaniasis, lymphatic filariasis, and schistosomiasis, while earlier
78

commitments to provide drugs for fascioliasis, leprosy, leishmaniasis, lymphatic filariasis, onchocerciasis, trypanosomiasis, and soil-transmitted helminthiases at no cost to endemic countries were reinforced as well. The meeting also stressed the importance of integrating NTDs in the Global Health and Development (GHD), and to be part of the Universal Health Coverage (UHC) policy which has been recommended in the 58th World Health Assembly resolution in 2005 (8). Universal health coverage means all people receiving the health services they need, including health initiatives designed to promote better health (such as antitobacco policies), prevent illness (such as vaccinations), and to provide treatment, rehabilitation, and palliative care (such as end-of-life care) of sufficient quality to be effective while at the same time ensuring that the use of these services does not expose the user to financial hardship (9). Thus, countries were encouraged to plan for stepping-up implementation of the UHC which entails integration of NTDs into regular health services. The passage in 2012 of a United Nations General Assembly resolution calling for governments “to accelerate the transition towards universal access to affordable and quality health care services”,
79

confirmed not only the breadth of consensus regarding the urgency of action on UHC, but also the level of concern about the state of the world’s health systems. In 2013, the World Health Assembly approved Resolution WHA 66.12, which defined strategies for NTDs with clear targets and milestones for 17 NTDs, and endorsed the WHO NTDs-Roadmap goals linking NTDs to Universal Health Coverage (UHC). Thus, in this setting NTDs are to be addressed through five strategies: preventive chemotherapy, intensified disease management, vector control, veterinary public health measures for zoonotic neglected diseases, and through improved water and sanitation (8). Preventive chemotherapy, for example, involves regular administration of anthelminthics to all people at risk. There are clear coverage targets and progress against these targets which should be routinely monitored. It has been recommended that country programs achieve full geographical coverage of all endemic districts, and 65–85% preventive chemotherapy coverage in each district, depending on which diseases are endemic. Globally, the coverage target is 80%. While preventive chemotherapy coverage is increasing, it is still low in many countries. For instance, globally, coverage
80

stands at 43% for lymphatic filariasis, for an estimated 1.4 billion people requiring treatment. For schistosomiasis, only 14% of the 250 million people in need of preventive chemotherapy receive it. Monitoring preventive chemotherapy coverage remains key to ensuring that the diseases of the least well-off are being prioritized from the very beginning of the path towards UHC (9).
Main actors in the fight against NTDs:In the fight against NTDs emphasis is placed on building partnerships for change among international agencies, governments, nongovernmental organizations, corporations, national ministries of health, and most of all, with people at the grass roots. This is intended to help people acquire the tools, knowledge, and resources they need to transform their own lives, building a more peaceful and healthier world for all. However, the main partners which their efforts have made real difference include the following:
1- The WHO as the lead health authority within the United Nations (UN) system works to ensure the safety of the air we breathe, the food we eat, the water we drink, and the medicines and vaccines
81

that treat and protect us. The Organization aims to provide every child, woman and man with the best chance to lead a healthier, longer life. WHO has been at the center of or behind dramatic improvements in public health since it was established in 1948, gathering the world’s top health experts, defining solutions, delivering guidelines and mobilizing governments, health workers and partners to positively impact people’s health. Over 7,000 public health experts from all over the globe work for WHO, in most countries worldwide. Concerning NTDs WHO formed the Global partners forum mentioned above.
2- Carter Center Health ProgramsSince 1986, The Carter Center has led the international campaign to eradicate Guinea worm disease, working closely with ministries of health and local communities, the U.S. Centers for Disease Control and Prevention, the World Health Organization, UNICEF, and many others. Inspired by the successful eradication of smallpox in 1977, the International Task Force for Disease Eradication (ITFED) has been formed at The Carter Center in 1988 to evaluate disease control and prevention and to see the potential for
82
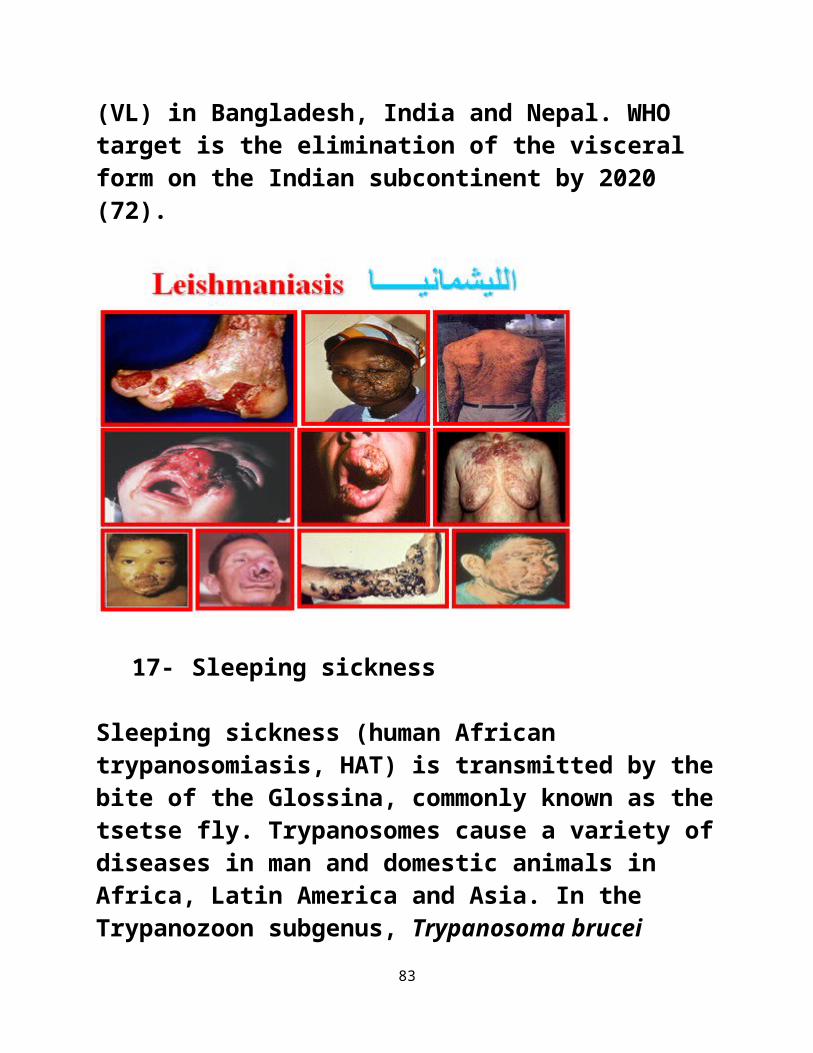
eradicating other infectious diseases. Thus, in addition to sponsoring and hosting the ITFDE meetings, Carter Center health programs address two of the diseases currently identified by the ITFDE for eradication, dracunculiasis and lymphatic filariasis, and three diseases identified for elimination or better control, onchocerciasis,, trachoma, and schistosomiasis. The center uses health education and simple, low-cost methods. Scientists and notable international health organizations serving on the task force have identified additional diseases that potentially could be eradicated, thereby dramatically and permanently improving the quality of life for many millions of the world's poorest people. These diseases include poliomyelitis, mumps, rubella, measles, and yaws. Currently supported by the Bill & Melinda Gates Foundation, the task force reviews progress in the field of disease eradication and the status of diseases selected for control or eradication, and recommends action steps.
3- Drug companies such as Merck and many other pharmaceutical groups have fulfilled the pledges made at the London
83
declaration in 2012 to provide medicines totaling more than 1.8bn treatments a year. They have been supported by non-pharma partners such as DHL, the international logistics company, which has helped with shipments of the donated drugs. Pfizer’s drug azithromycin has been donated free to treat yaws, alongside its existing donations of the drug for trachoma, under which 500m doses have been given away since 1998.
Socioeconomic burden of HIV/AIDS, Tuberclosis and malaria:HIV/AIDS, Tuberclosis and malaria are
considered the three big diseases in tropical Africa. They cause the major socioeconomic burden of endemic diseases in Africa
HIV/AIDS:HIV infection represents a global health concern. It has an extremely uneven geographical distribution, with Sub-Saharan Africa bearing more than two-thirds of the global burden. HIV/AIDS pandemic has a bad implication on life expectancy, and the sustained high prevalence of the disease is considered to be the most significant threat
84

to socioeconomic development. HIV/AIDS is by far the leading cause of premature mortality in sub-Saharan Africa and the fourth-biggest killer worldwide. In sub- Saharan Africa, HIV prevalence among adults had reached around 7.4%, rising to over 20% in some settings. At the end of 2004, an estimated 39 million people globally were living with HIV, and there were 3.1 million AIDS deaths, including 510,000 children. In 2010 the global deaths from HIV/AIDS was about 1.5 million. In 2011, 34 million people were living with HIV globally, 3.3 million were children under 15 years and 16.7 million were women. Adolescents are also vulnerable with estimated 2.1 million cases (aged 10–19 years) living with HIV in 2012 in low- and middle-income countries (LMICs), with the prevalence among young women twice as high as that among young men throughout Sub-Saharan Africa (77- UNAIDS, 2012). Progress has been made on some fronts. In 2003, the World Health Organization (WHO) 3 by 5 initiative called for providing 3 million people living with HIV in LMICs with antiretroviral treatment (ART) by the end of 2005. Despite considerable skepticism regarding the advisability and feasibility of expanding access to ART, by June 2016 around 18.2 million, or 49% of people living
85

with HIV (PLHIV), were taking ART. Efforts to expand access to treatment are supported by scientific evidence that treatment prevents illness and death, reduces human immunodeficiency virus (HIV) transmission, and can decrease health care costs. The United Nations Program on HIV/AIDS (UNAIDS) World AIDS Day Report 2012, reported a 50% reduction in HIV incidence in 25 LMICs between 2001 and 2011, while in Sub- Saharan Africa, the number of newly infected children declined by 24% between 2009 and 2011. However, the Joint UNAIDS estimates that 36.7 million people were living with HIV globally in 2015 and 1.1 million people died in the same year from AIDS resulting from HIV infection. This shows that more efforts are needed to control the pandemic globally, and especially, in sub-Saharan Africa. Although hundreds of millions of HIV tests have been performed, one of the most important barriers to earlier ART and viral suppression is limited HIV diagnosis among PLHIV, of whom only 60% had been diagnosed as of 2015. Initiation of ART has primarily relied on CD4 cell count measurement, with access to the more useful viral load monitoring increasing only recently. It seems that ensuring access to
86
care and successful viral suppression is still a major challenge (78, 79).However, the importance of accelerating access to diagnosis, treatment, and viral suppression as significant elements in ending the epidemic has prompted the Joint UN Program on HIV/AIDS (UNAIDS) to release the HIV 90-90-90 target. The 90-90-90 target states that by 2020, 90% of individuals living with HIV will know their HIV status, 90% of people with diagnosed HIV infection will receive antiretroviral treatment (ART), and 90% of those taking ART will be virally suppressed. The establishment of the 90-90-90 target has placed increased emphasis on accurate monitoring and evaluation of the national continua of care from HIV diagnosis to viral suppression. Consistent methods and routine reporting in the public domain is necessary for tracking progress towards the 90-90-90 target (79). The importance of a standardized monitoring and evaluation framework was reflected in the 2001 UN General Assembly Special Session on HIV/AIDS that called for 13 core national-level indicators for monitoring progress. Data is available on the care scale from 82 countries in the public domain from 2010 to 2016, representing 33.8 million (92%) of the 2015 global estimate of PLHIV. Of the 82
87

countries, only Sweden has achieved the 90-90-90 target. Data on PLHIV diagnosed were available for 51 of 82 countries, data for those on ART indicator for 80 of 82 countries, and data for viral suppression for 53 of 82 countries. Care continua with viral suppression estimates were available in the public domain from only nine countries in sub-Saharan Africa (Kenya, Malawi, Mauritius, Namibia, Rwanda, South Africa, Swaziland, Uganda, and Zimbabwe), representing only 35% of the 2015 HIV burden (78, 79). Unfortunately, research on major health issues, including HIV/AIDS, in Africa is still far behind that of developed countries, mainly due to brain drain, lack of mentorship, inadequate research funding, armed conflicts, and marginal collaboration (81).
Socioeconomic burden of tuberculosis (TB) in Afri ca: Tuberculosis is the second greatest killer worldwide due to a single infectious agent after HIV/AIDS. It kills nearly 1.7 million people annually, most of them in their prime productive years. Over 95% of TB deaths occur in LMICs with the highest burden in Africa and Asia. The African region has 24% of the world’s TB cases and the highest rates
88

of cases and deaths per capita. With the notable exception of sub-Saharan Africa, the incidence of tuberculosis has declined over the past two decades in most regions of the world (82, 83).The emergence of drug- resistant strains of the disease, the spread of HIV/AIDS, which enhances susceptibility to tuberculosis, and the growing number of refugees and displaced persons, have all contributed to its spread. The number of new tuberculosis cases has been growing by about 1% a year, predominantly because of AIDS epidemic in sub- Saharan Africa. In 2003, there were an estimated 8.8 million new cases, including 674,000 in people infected with HIV. There is also the emerging issue of multi-drug resistant TB (MDR- TB), which is rising and reached 60,000 in the 27 high MDR-TB burden countries worldwide in 2011. Although the MDG target to halt and reverse the TB epidemic by 2015 is already achieved, the disease burden remains enormous with resurgence in many areas due to HIV/AIDS. An estimated 13% of the TB cases in 2011 were co-infected with HIV and 430,000 deaths were among the HIV-positive population (82, 83).The burden of multidrug-resistant (MDR) and extensively drug-resistant (XDR) tuberculosis
89

has evolved in several tuberculosis-endemic countries. Approximately 20% of tuberculosis isolates globally are estimated to be resistant to at least one major drug (first-line or group A or B second-line), with approximately 10% resistant to isoniazid. WHO has defined multidrug-resistant (MDR) tuberculosis as resistance to at least isoniazid and rifampicin, when first-line therapy is unlikely to cure the disease and a switch to a second-line drug regimen is recommended. XDR TB is defined as drug-incurable or programmatically incurable tuberculosis (totally drug-resistant tuberculosis). The extensively drug-resistant (XDR) tuberculosis is also resistant to the fluoroquinolones and second-line injectable drugs, indicating the probable failure of the standardized second-line treatment regimen. Globally, approximately 5% of patients with tuberculosis are estimated to have either MDR or XDR types, but the distribution of cases is not uniform; it is substantially higher in some regions, and increasing incidence has been reported in several countries. The high mortality due to most patients remaining untreated is a key reason for this apparently stable estimated global rate of drug-resistant tuberculosis. Approximately 30% of MDR tuberculosis isolates are either
90

fluoroquinolone-resistant or aminoglycoside-resistant, and approximately 10% of MDR tuberculosis isolates can be classed as XDR tuberculosis, or as having resistance to additional drugs beyond XDR tuberculosis (ie, totally drug resistant). Two modes exist by which patients contract drug-resistant tuberculosis. Primary resistance results from infection with a drug-resistant strain, whereas resistance that develops during therapy is referred to as secondary or acquired resistance. Amplification of resistance might occur when resistance to additional drugs emerges during the treatment course, often in association with inadequate therapy (84). This poses several challenges similar to those encountered in the pre-chemotherapy era, including the inability to cure tuberculosis, high mortality, and the need for alternative methods to prevent disease transmission. This phenomenon mirrors the worldwide increase in antimicrobial resistance and the emergence of other MDR pathogens, such as malaria, HIV, and Gram-negative bacteria. MDR and XDR tuberculosis are associated with high morbidity and substantial mortality, are a threat to health-care workers, prohibitively expensive to
91

treat, and are therefore a serious public health problem (84). The traditional view that acquired resistance to antituberculous drugs is driven by poor compliance and programmatic failure is now being questioned, and several lines of evidence suggest that alternative mechanisms, including pharmacokinetic variability, induction of efflux pumps that transport the drug out of cells, and suboptimal drug penetration into tuberculosis lesions, are likely crucial to the pathogenesis of drug-resistant tuberculosis. These factors have implications for the design of new interventions, drug delivery and dosing mechanisms, and public health policy (85).This expansion of resistance has ushered in an era of programmatically incurable tuberculosis, in which insufficient effective drugs remain to construct a curative regimen. The availability of newer drugs, such as bedaquiline and delamanid,3–5 has not averted this problem and resistance to both bedaquiline and delamanid in the same patient has already been reported. The effect on patients is profound, because drug resistant tuberculosis is associated with a higher morbidity than drug-sensitive tuberculosis and is responsible for
92

approximately 20% of the global tuberculosis mortality, with mortality rates estimated at around 40% for patients with MDR tuberculosis and 60% for those with XDR tuberculosis (82).
The socioeconomic burden of Malaria in Africa:Malaria continues to have a severe socioeconomic impact in Sub Saharan Africa and a major impediment to health, where it frequently takes its greatest toll on very young children and pregnant women. A child dies every minute from malaria in Africa where it is estimated that 9 out of 10 malaria deaths occur. The consensus view of recent studies and reviews is that malaria causes at least 20% of all deaths in children under- 5 years of age in Africa. Malaria is transmitted via the bites of infective mosquitoes, but it can also be spread to the fetus during pregnancy as well as before and/or during childbirth. Malaria contracted at this time is called congenital malaria and is a cause of infant death and low birth weight. There are three principal ways in which malaria can contribute to death in young children. First,
93

an overwhelming acute infection, which frequently presents as seizures or coma (cerebral malaria), may kill a child directly and quickly. Second, repeated malaria infections contribute to the development of severe anaemia, which substantially increases the risk of death. Third, low birth weight, frequently the consequence of malaria infection in pregnant women, is the major risk factor for death in the first month of life. In addition, repeated malaria infections make young children more susceptible to other common childhood illnesses, such as diarrhoea and respiratory infections, and thus contribute indirectly to mortality. Although respiratory disease caused by a variety of infectious agents results in a similar proportion of deaths, P. falciparum is the most important single infectious agent causing death among young children (86, 87).With high case-fatality rates due to late presentation, inadequate management, and unavailability or stock-outs of effective drugs, malaria is also a major contributor to deaths among hospital inpatients. It is one of
94

the causes of household poverty because it results in absenteeism from the daily activities of productive living and income generation. Malaria also continues to prevent many school children from attending school due to illness, diminishing their capacity to realize their full potential. Children who survive malaria may suffer long-term consequences of the infection. Repeated episodes of fever and illness reduce appetite and restrict play, social interaction, and educational opportunities, thereby contributing to the burden. Because malaria is such a common disease and well known to the people it affects most, and because many of those who become sick with malaria do not visit health care facilities, thus, assessing the size of the problem, and how it is changing over time, is an enormous challenge. No country in Africa south of the Sahara for which data are available shows a substantial decline in malaria incidence and the burden of sickness and death due to malaria remained high. Available monitoring systems cannot yet reliably track changes in malaria incidence and clinical pattern (86, 87, 88).
95
However, the available data showed that around 81% of the malaria incidence and 91% of the malaria deaths in 2010 occurred in Africa, and 86% involved children under- five years of age. In 2012, malaria was responsible for over 1.1 million deaths globally and was endemic in 104 countries with substantial geographic disparities. In 2013, there were 528 000 deaths from malaria and about 78% of these were children under 5 years of age. In 2015, 88% of global cases and 90% of global deaths were still in the Africa. In all malaria-endemic countries in Africa, 25–40% of all outpatient clinic visits had been for malaria. In these same countries, between 20% and 50% of all hospital admissions are a consequence of malaria (87). However, due to concerted efforts in the
fight against malaria between 2000 and 2015, the number of malaria cases declined by 42% while the malaria death rate declined by 66% in the Africa. This reduction is due to improved availability and use of insecticide-treated nets (ITNs), diagnosis-based treatment with artemisinin-based
96

combination therapy (ACT), engagement of communities in malaria control, and strengthening capacity in vector control for malaria. Despite the successes made the malaria burden is still startling (89).A number of factors account for the
continued malaria burden in Africa, which include climate changes, poverty, weak infrastructure, emerging drug and insecticide resistance, massive population and demographic shifts, and high costs of containment and therapy. In many endemic areas, transmission is seasonal and unstable, with peaks during and just after the rainy season. Due to transmission intensity fluctuation from year to year the pattern of clinical malaria greatly depends on the rainfall patterns. In such areas, unlike the highly endemic areas, epidemic malaria typically affects people of all ages and can have high case- fatality due to the fact that no single age group in the population is immune by repeated infections. However, epidemics can also occur in areas of higher transmission as a result of the abandonment of control programs, immigration of non-
97

immune people, and reduced access to treatment (87, 90). In addition, poor families live in dwellings
that offer little protection against mosquitoes and are less able to afford insecticide-treated nets. Poor people are also less likely to be able to pay either for effective malaria treatment or for transportation to a health facility capable of treating the disease. Both direct and indirect costs associated with a malaria episode represent a substantial burden on the poorer households. A study in northern Ghana found that, while the cost of malaria care was just 1% of the income of the rich, it was 34% of the income of poor households (87). In Africa, most cases of malaria are diagnosed on the basis of clinical symptoms and treatment is presumptive, rather than based on laboratory confirmation. Moreover, malaria parasitaemia is common among clinic attendees in many endemic areas, so that a positive laboratory result does not necessarily mean that the patient is ill with malaria. Reporting from facilities to districts and from districts to the ministry of health
98
varies in its completeness and timeliness from country to country but it is not, yet, satisfactory. Thus, routine reports of the number of malaria cases and deaths have limited value for comparisons of the malaria burden between countries (89). Demographic and health surveys (DHS) and other sources indicate that less than 40% of malaria morbidity and mortality is seen in formal health facilities, a small fraction of the total burden. However, routinely collected data are often the only information available over a prolonged period and over a wide geographical area. While these data are of use for local program planning, major investment in improving both the quality of health information systems and access to health services would be required before their utility for monitoring changes in malaria disease trends could be assessed (88).
99

Insecticide-treated nets (INTs)Insecticide-treated nets (INTs) are highly effective in reducing malaria mortality in young children. They are low- cost and highly effective way of reducing the incidence of malaria in people who sleep under them, and they have been conclusively shown in a series of trials to substantially reduce child mortality in malaria-endemic areas of Africa. By preventing malaria, ITNs reduce the need for treatment and the pressure on health services, which is particularly important in view of the increase in drug-resistant falciparum malaria parasites. At least five large factories in Africa are now producing nets. Almost all malaria-endemic African countries now have active programs under way to encourage ITN use, and most of these support a variety of different mechanisms to increase net coverage. ITNs and the insecticide to treat them can now be
100
purchased in small shops and markets and even on street corners in many endemic African countries. Use of INTs is a major contributor to control, but, the commercial price of nets and insecticide, though falling, still puts this life-saving technology beyond the reach of the poorest income groups of the population. Major efforts are now being made in several African countries to provide subsidized ITNs to the most vulnerable groups, young children and pregnant women. New technological developments promise nets that will retain insecticidal activity for many years, and novel ways of encouraging regular net treatment with insecticide should make it possible to increase the proportion of nets that are effectively treated. Although accurate data from the acceleration of ITN in1980s are not generally available for comparison, it is certain that there are now more children sleeping under nets and a greater use of ITNs in Africa than ever before. Recent survey data showed that approximately 15% of young children slept under a net, but that only about 2% used
101

nets that were treated with insecticide. Untreated nets provide some protection against malaria, but their full protective benefits can be realized only if they are regularly retreated with insecticide. The price of nets has fallen substantially as a result of greater demand, increased competition between producers, and reductions in taxes and tariffs and other obstacles to trade, that many African countries have endorsed after the Abuja Summit in 2000. In response to low re-treatment rates of conventional insecticide-treated nets, especially in Africa, WHO prompted industry to develop long-lasting insecticidal nets (LLINs), ready-to-use, factory-pretreated nets that require no further treatment during their expected lifespan of 4–5 years. This technology obviates the need for re-treatment, and unlike conventional ITNs, LLINs resist washing, and reduces both human exposure (at any given time, most of the insecticide is hidden and not bioavailable) and the risk of environmental contamination. Using the most recent fibre technologies, LLINs are regarded
102

as a major breakthrough in malaria prevention. One LLIN is already commercially available and is recommended by WHO. At a current price of around US$ 5 per net, LLINs are already more cost-effective than conventionally treated nets. Efforts are being made to scale up production capacity to meet demand, which is already high. The Roll Back Malaria (RBM) partnership is facilitating technology transfer and stimulating local production of LLINs in Africa (91).Antimalarial drug resistanceTreated nets and other means of reducing mosquito bites will not totally prevent malaria. People who become ill with the disease need prompt and effective treatment to prevent the development of severe manifestations and death. Antimalarial drug resistance has become one of the greatest challenges in malaria treatment. Since the 1980s, parasite resistance to chloroquine, the cheapest and most widely available antimalarial drug, has emerged as a major challenge since it has lost its clinical effectiveness in most parts of Africa. Average cost of a full course of adult outpatient
103

treatment with Chloroquine is US$ 0.13. In most countries in Eastern, Central, and Southern Africa, chloroquine has lost its clinical effectiveness as a malaria treatment. A similar evolution is taking place, though some years later, in West Africa, and there is indirect, but compelling, evidence that this is giving rise to increasing mortality. Unfortunately, resistance to the most common replacement drug, sulfadoxine–pyrimethamine, has also emerged, especially in Eastern and Southern Africa (92, 93). Over the past few years, 13 countries in Africa have changed their national policies to require the use of more effective antimalarial treatments. Where current monotherapies are failing, WHO recommends artemisinin-based combination therapy (ACT), which is highly efficacious and promises to delay emergence of resistance. So far however, its use is constrained by high costs and limited operational experience in Africa. The combination of multiple drugs enhances clinical efficacy and may delay the development of resistance of parasites. However, these drugs are not yet widely
104

available and not always affordable (91).In many malaria-endemic countries the first treatment for malaria is often purchased from a shop. Data from representative sample surveys indicate that almost half of all children under 5 years of age with fever are treated with an antimalarial drug. Although this is encouraging, some of these treatments may have been with failing drugs or been given too late or in the wrong dosage. Recent studies indicate that home treatment, supported by public information and pre- packaging (as an aid, to ensure that patients take the full treatment course at the right time), can help to reduce malaria mortality in children. Many countries now concentrate on making effective malaria treatment available close to the home, through support to community initiatives and engagement of drug sellers and the pharmaceutical industry. Realizing the full potential of effective treatment as a tool for reducing mortality will require a systems approach, ensuring that effective drugs are affordable (which will often require subsidization) and that they are
105

supported by appropriate education of formal and informal providers as well as mothers, and by quality assurance and regulation. Pre-packaged antimalarial drugs can increase compliance and facilitate home treatment (88). Home-based management of fever (HBMF) is a promising strategy for improving the coverage of prompt effective treatment. Community health workers and mothers of young children are trained in the recognition of symptoms and the benefits of prompt antimalarial treatment. Prepackaged kits of full-course treatments, with appropriate drawn and written instructions, allow mothers to treat children as soon as fever is detected. Programs have been launched in Ghana, Nigeria, and Uganda in June 2002. Uganda has gone to scale with the HBMF approach in more than 10 districts and is rapidly expanding coverage. The impact of HBMF is being evaluated in three districts; interim results suggest that, among children under 5 years, the number of outpatient malaria cases has declined since program implementation (94).
106
Despite the gains made towards elimination of Plasmodium falciparum malaria in the past 15 years, many countries still have endemic transmission, and are increasingly looking to new strategies to accelerate progress. One of the adopted approaches is mass drug administration (MDA) which involves the time-limited distribution of drugs to a target population, irrespective of infection status. It has been used only sporadically against malaria in most settings, and cluster-randomized trials (95, 96). However, MDA has received renewed interest as a strategy to clear chronic asymptomatic infections and rapidly reduce transmission. In September, 2015, WHO’s Malaria Policy Advisory Committee recommended for the first time the use of MDA in specific circumstances: when transmission is close to being interrupted, vector control, effective surveillance, and access to case management are at high coverage, and importation of infection is minimal. This can be applied also in areas which are under threat of multidrug resistance, or for malaria epidemics or during complex emergencies. National malaria control programs and partners need to decide what role, if any, MDA should have in control and elimination strategies. However,
107

the best operational strategies for MDA and how best to combine MDA with other interventions need to be established (96). Malaria Vaccines
During the last thirty years scientists have been working hard to get long lasting vaccines for malaria without any real success so far. Recently, a partially protective vaccine candidate, RTS,S, has been in trials (97). A proof-of-concept Phase IIb trial in Mozambique found that the vaccine offered partial protection for young children, cutting their risk of severe malaria by 58%. Grants have been allocated Phase IIb trials and a Phase III trial in multiple African countries. The trials will study RTS,S in young children as well as infants, and confirm that it is safe when given with other childhood vaccines. “A vaccine is our best long-term hope to defeat malaria, and even a partially-effective vaccine would be a huge step forward,” said Dr. Melinda Moree, director of MVI. “We’re advancing this vaccine through final testing in the hope that it will be available to save lives as soon as possible.”Malaria and pregnancyP. falciparum infection during pregnancy is estimated to cause an estimated 75 000 to
108
200 000 infant deaths each year. Despite the toll that malaria exacts on pregnant women and their infants, this was, until recently, a relatively neglected problem, with less than 5% of pregnant women having access to effective interventions. Nowadays, however, potentially more effective strategies for prevention and control of malaria in pregnancy have been developed and shown to have a remarkable impact on the health of mothers and infants. For many years WHO recommended that pregnant women in malaria endemic areas should receive an initial antimalarial treatment dose on their first contact with antenatal services, followed by weekly chemoprophylaxis (given at less than therapeutic dose) with an effective and safe antimalarial drug. In most countries in Africa, chloroquine (CQ) has been the drug of choice. However, the emergence and spread of CQ-resistant falciparum malaria, poor patient compliance with multiple doses, and a high incidence of CQ-induced pruritus have limited the effectiveness and hence the implementation of this policy (91).
109
It has been shown that the impact of malaria on pregnant women and their newborns can be substantially reduced by the recently recommended use of intermittent preventive treatment (IPT). In 2000, the WHO Expert Committee on Malaria recommended that intermittent treatment with an effective, preferably one- dose, antimalarial drug, should be made available as a routine part of antenatal care to women in their first and second pregnancies in highly endemic areas. This strategy provides at least two treatment doses of an effective antimalarial at routine antenatal clinics to all pregnant women living in areas at risk of endemic falciparum malaria in Africa (irrespective of whether they are actually infected with malaria or not). About two-thirds of pregnant women in Africa south of the Sahara attend clinics for antenatal care, and incorporating IPT for malaria into their routine care should be straightforward. At present, sulfadoxine–pyrimethamine (SP), given at a therapeutic dose, is the single- dose antimalarial with the best overall effectiveness for prevention of malaria in pregnancy in areas with high transmission, and low resistance to SP. Other
110
antimalarials are being evaluated for potential use in IPT. Studies in Kenya and Malawi have shown that IPT with at least two treatment doses of SP is highly effective in reducing the proportion of women with anaemia and placental malaria infection at delivery. The benefits of IPT for both maternal and infant health have been seen in a range of different malaria transmission settings (87). Now an integral part of the “Making Pregnancy Safer” strategy, IPT has been adopted as policy by many countries to replace chemoprophylaxis; most other countries in Africa are reviewing their policies in the light of the new recommendation. The beneficial effects of IPT will probably be additive to the proven benefits of ITNs use by pregnant women. The prevention and management of malaria during pregnancy, therefore, calls for a combination of IPT, support for ITN use, and prompt access to effective treatment. Several countries in Eastern and Southern Africa have recently formed a coalition to reduce the impact of malaria in pregnancy through this combined approach (87).
111

Financial challengesTackling malaria effectively requires substantial resources. At the Abuja Summit in 2000, it was estimated that at least US$ 1 billion is needed from a combination of increased domestic spending and international assistance. Government spending on all health care is low in most African countries, typically less than US$ 15 per person. The costs of malaria control are high: artemisinin-based combination drugs to treat resistant malaria are likely to cost US$ 1–3 per treatment for the drug alone, and ITNs cost around US$ 5. Most of the costs of preventing and treating malaria in Africa today are in fact borne by people themselves which may contribute to poverty. Government support is needed for the most effective interventions and the appropriate regulation to ensure that only safe, effective malaria interventions are sold and that the public is fully informed about their use and effectiveness (88).Partnership in the fight against malariaDuring the 1950s and 1960s, the malaria
eradication campaign successfully eliminated
112

or controlled the disease in countries with temperate climates and in some countries where malaria transmission was low or moderate. However, the emergence of drug and insecticide resistance, coupled with concerns about the feasibility and sustainability of tackling malaria in areas with weak infrastructure and high transmission, brought an end to the eradication era. Thus, the bulk of international funding for malaria has been directed to control and investment in malaria research. Despite international indifference in subsequent years, progress continued to be made in understanding the problem of malaria and strategies for its control. By the early 1990s the international community began to appreciate that the malaria burden was unacceptably high and worsening, particularly in Africa, and that real reductions in malaria mortality and morbidity were possible with existing but under-used tools and strategies.In the last three decades many stakeholders
have already been involved in malaria control. Formal partnerships have been
113

created and a statement of intent issued, indicating what will be achieved, and how. Resources have been mobilized from partners and systems are set up to monitor achievements in rolling back malaria. In 1992, malaria control was re-established as a global health priority by a Conference of Ministers of Health held in Amsterdam. Scientific interest in the disease and its control, political commitment to reducing the burden of malaria, and the financial resources for malaria research and control began to increase rapidly. Between1991-1998 malaria control expertise and capacity were expanded and strengthened, particularly in Africa, especially through the project for Accelerated Implementation of Malaria Control (1997-1998). The project for Accelerated Implementation of Malaria Control represented an unprecedented contribution to the fight against malaria in Africa south of the Sahara, in terms of both technical support and funds. The funding provided for the project over the two years was estimated to have been more than 12 times the contributions made by WHO during
114

the previous decade. This is in addition to the Multilateral Initiative on Malaria formed by WHO/TDR in 1997 (86).In1998 the Roll Back Malaria (RBM) Partnership was launched and consensus on the core technical strategies for tacking malaria established. In 2000 the United Nations declared 2001–2010 the Decade to Roll Back Malaria in developing countries, particularly in Africa (United Nations General Assembly, Resolution 55/284). The goal of Roll Back Malaria is to halve the burden of malaria by 2010. The following targets for specific intervention strategies were established at the Abuja Malaria Summit, April 2000, attended by heads of states in a historic meeting, to express their personal commitment to tackling malaria and to establish targets for implementing the technical strategies to Roll Back Malaria. Prompt access to effective treatment, Insecticide-treated nets (ITNs), Prevention and control of malaria in pregnant women, Malaria epidemic and emergency response. The original Abuja declaration included the recommendation for chemoprophylaxis, as
115

well, but present WHO and RBM policy strongly recommends IPT, and not chemoprophylaxis, for prevention of malaria during pregnancy. In addition the African heads of states participating in the Abuja Summit agreed that by the year 2005 at least 60% of those suffering from malaria should have prompt access to and be able to use correct, affordable, and appropriate treatment within 24 hours of the onset of symptoms (93).Since then the international spending on malaria has more than doubled to approximately US$ 200 million per year. The partners in the Roll Back Malaria efforts include governments of malaria-endemic countries, donor governments, international non- governmental organizations, the private sector, and civil society bodies. They have, so far, supported the introduction of wide range interventions. Roll Back Malaria has been supporting efforts to improve the early recognition of, and effective and timely response to, malaria epidemics. Indoor residual spraying which plays an important role in malaria vector
116

control, especially in the control of epidemics. Malaria early warning systems have been established in Southern Africa to improve outbreak detection and response and are being developed in other epidemic-prone parts of Africa. However, the past decade has seen tremendous expansion in malaria financing and consequent coverage of interventions. Approximately half of countries with ongoing malaria transmission are on track to meet the World Health Assembly (WHA) and Roll Back Malaria (RBM) targets to achieve a 75% reduction in malaria cases by 2015, as compared to those in 2000. Fifteen epidemic-prone countries have developed a preparedness plan of action (87).The present targets of RBM Partners shall be to work together to support achievement of the following goals: By 2020: Malaria mortality rates and incidence is reduced by at least 40% compared with 2015. Malaria does not re-emerge in countries that were malaria-free in 2015. Malaria is eliminated in a further 10 countries compared to 2015 and by 2030 to reduce malaria incidence and
117

mortality rates globally by at least 90% compared with 2015 levels, in addition to elimination of malaria from at least 35 countries in which malaria was transmitted in 2015, and to prevent re-establishment of malaria in all countries that are malaria free (86). In 2017 the unofficially issued yet RBM mission is to support malaria-affected countries to achieve the goals of WHO’s Global Technical Strategy and contribute to a malaria-free world by 2030. This can be achieved by; convening Partners focused on this common cause, coordinating Partners to maximize alignment, facilitate cooperation and ensure that common challenges are addressed cooperatively, mobilizing resources by identifying resource requirements and creating humanitarian and business cases to support the mobilization of resources, facilitating communication between Partners to identify and address opportunities and challenges; share experience and best practice with one another providing mission critical support to malaria-affected countries and regions by
118
supporting critical enablers required to enhance political will, and providing targeted support where it is needed most.
The business community is also increasingly playing a role in the Roll Back Malaria partnership and providing vital resources and expertise to support malaria control programs. Partnerships have been forged with the drug industry, companies with major investments in malaria-endemic countries whose workers are at risk from malaria, and manufacturers of nets and insecticides. In addition, companies have provided funds for training and collaborating with young scientists and medical officers to allow them to gain valuable experience in the field. International expenditures on malaria increased substantially over the years. The Bill & Melinda Gates Foundation announced three grants totaling $258.3 million for advanced development of a malaria vaccine, new drugs, and innovative mosquito control methods to help defeat malaria. “Millions of children have died from malaria because they were not protected by an insecticide-treated bed net, or did not receive effective treatment,” said Gates. “If we expand malaria control programs, and
119

invest what’s needed in R&D, we can stop this tragedy.”The Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM) is a major new source of grant funding for tackling malaria in Africa. In 2001 resources for controlling malaria were significantly boosted with the establishment of the Global Fund to Fight AIDS, Tuberculosis and Malaria. Twenty-five countries and one multi-country group have submitted successful proposals to the GFATM. Almost all of these proposals have been built on the national malaria control plans developed by these countries with the support of the Roll Back Malaria Partnership during the period 1999–2001. The countries have been awarded a total of US$ 256 million for an initial two years to scale up malaria control activities. Depending on success, it is expected that additional funds will be made available for a total period of five years. Commitments from the Global Fund to Fight AIDS, Tuberculosis and Malaria have significantly increased the financial resources for malaria control in Africa. The challenge now is for countries to develop the capacity
120
to spend the money efficiently and for the international community to support Africa in that effort (98).
The International Consortium to Target Malaria-Transmitting MosquitoesThe Innovative Vector Control Consortium (IVCC), led by the Liverpool School of Tropical Medicine was offered $50.7 million, five-year grant to develop safer, more effective, and longer-lasting insecticides for mosquito control. The consortium will also develop improved bed nets and other insecticide-treated materials, and help health authorities determine how to deploy insecticides and bed nets for maximum impact. “Historically, controlling mosquitoes has been key to controlling malaria, but mosquitoes are developing resistance to insecticides,” said Dr. Janet Hemingway, Director of the Liverpool School of Tropical Medicine. “We need new insecticides that are up to the task today, and that are safe for humans and the environment.” Need for reliable data
With the renewed international commitment to fighting malaria, the need for regular and reliable information on the global malaria situation is greater than it has ever been.
121

The general indifference of the past has given way to an urgent demand for information that can be used to define and analyze the malaria situation and measure progress towards the goals established by the international community and by national control programs. The World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) are committed to meeting this demand. WHO has established 126 sentinel surveillance sites in 36 African countries that monitor the efficacy of locally used antimalarial drugs by following up patients in the clinics. According to standard protocol, results are expressed as i) early treatment failure (ETF); ii) late clinical failure (LCF); late parasitological failure (LPF), as well. Public health success stories, such as the guinea worm eradication, Onchocerciasis Control Program, and the polio eradication campaign, have depended on the combination of country commitment and international support translating into impact on the ground. There is good reason to believe that similar progress can be achieved in malaria (86.
122

Existing Challenges in the fight against endemic diseases:Meeting the following challenges will require not only the continued commitment of the various stakeholders working to combat endemic diseases but also increased collaboration and partnerships to exploit synergies and optimize use of resources. Much has been achieved, however, significant challenges remain:
1- WHO estimates that 2.4 billion people still lack basic sanitation facilities such as toilets and latrines, while more than 660 million continue to drink water from “unimproved” sources, such as surface water.
2- The lack of robust, sustained international and domestic financing.
3- The need to accelerate progress is improving the inadequate performance of health systems in most of affected African countries.
4- Many of the people who harbor infections remain asymptomatic or undiagnosed and act as potential reservoirs.
5- In some parts of Africa, vector-control tools cannot effectively protect against a disease given the diversity of vectors and the differences in their behaviors
123

6- The emergence of resistance to medicines and insecticides is major concern. New combinations of drugs and innovative, faster-acting medicines with fewer side-effects are needed. The lack of financial incentives for pharmaceutical companies has tended to discourage research and development in the area of endemic diseases.
7- Lack of capacity to implement effective surveillance and monitoring compromises getting reliable data which is needed to expose coverage inequities, and to make sure whether people receive the services they need, and also takes into account the quality of services provided, and the ultimate impact on health.
8- Disruptive armed conflicts in many African countries
9- Barriers to accessing needed health services that range from poverty to stigmatization.
10- Once you move towards elimination, communities forget the burden of the contained disease. We have to remind the community to remain alert and report cases to make sure that the diseases could not come back.
124

11- Eliminating transmission of NTDs and ensuring that the delivery of health services meets the needs of those still living with NTD-related disease.
12- Lack of a strong political voice. People affected by endemic diseases in Africa are generally overlooked
13- How to overcome endemic zoonotic diseases through strategies of veterinary public health activities and the One Health approach which recognizes that the health of people is connected to the health of animals and the environment.
Role of NGOs and Turkish foundations in Eradicating Endemic Diseases:NGOs including the Federation of Islamic Medical Associations (FIMA) and Turkish Foundations can have influential role in building capacity of local communities in Africa to fight endemic diseases. They can be involved in programs to empower community-based delivery of medical and health services. This is to be achieved in close collaboration with official bodies involved in health service provision, and with other stakeholders already exerting appreciable efforts to control or eradicate
125

endemic diseases in Africa.
The Turkish government can help in establishing centers of excellence for research and training on endemic diseases control in several African countries. These centers can carry epidemiological studies on prevalence, vulnerability and spread of endemic diseases in Africa using modern technological tools. Such studies can give sold data on the magnitude and perception of the burden of the endemic diseases in Africa. The centers can help in the design and availability of effective and practical interventions to combat endemic disease. Such interventions could include research on vaccines or other primary preventive measures, curative treatments with new effective drugs, or new means of eliminating vectors. Ideally, intervention should be effective, safe, inexpensive, long-lasting, and easily deployed. Carter center has demonstrated feasibility of elimination of endemic diseases by mobilizing efforts of many stakeholders. Also the generous funding by The Bill & Melinda Gates Foundation has made real appreciable difference in the fight against endemic diseases in Africa. Why not relatively wealthy Islamic countries such Turkey make such a
126

move to establish centers of excellence in Africa bearing in mind the majority of the affected people in Africa are Muslims.
References:
1- World Health Organization: The global burden of disease: 2004 update. 2008. Geneva: World health organization; 2011.
2- Harris M, Reza JN: Global Report for Research on Infectious Diseases of Poverty. Geneva, Switzerland: World Health Organization; 2012.
3- Makinen, M., Waters, H., Rauch, M., Almagambetova, N., Bitran, R., Gilson, L., McIntyre, D., Pannarunothai, S., Prieto, A.L., Ubilla, G. & Ram, S. 2000. Inequalities in health care use and expenditures: empirical data from eight developing countries in transition. Bulletin of the World Health Organization, 78:55-65.
4- Liese B, Rosenberg M, Schratz A. Programmes, partnerships, and governance for elimination and control of neglected tropical diseases. Lancet 2010; 375: 67–76
5- Molyneux DH, Savioli L, Engels D. Neglected tropical diseases: progress towards addressing the chronic pandemic. Lancet (2017)
127

389(10066) :312–25. doi:10.1016/S0140-6736(16)30171-4
6- Liese B, Rosenberg M, Schratz A. Programmes, partnerships, and governance for elimination and control of neglected tropical diseases. Lancet 2010; 375: 67–76
7- Hotez PJ, Fenwick A, Savioli L, Molyneux DH. Rescuing the bottom billion through control of neglected tropical diseases. Lancet 2009; 373: 1570–75.
8- World Health Organization. Investing to overcome the global impact of neglected tropical diseases: WHO third report on neglected tropical diseases. Geneva: WHO, 2015. https://www.yumpu.com/en/document/ view/ 37074971/1 a9bnbk/5 (accessed Sept 1, 2015).
9- World Health Organization 2017. Integrating neglected tropical diseases into global health and development: fourth WHO report on neglected tropical diseases. ISBN 978-92-4-156544-8
10- Zijlstra EE, van de Sande WW, Welsh O, Mahgoub el S, Goodfellow M, Fahal AH. Mycetoma: a unique neglected tropical disease. Lancet Infect Dis. 2016 Jan;16(1):100-12. doi: 10.1016/S1473-3099(15)00359-X. Review.PMID:26738840
128
11- Bhatt S, Gething PW, Brady OJ, et al. The global distribution and burden of dengue. Nature 2013; 496:504–7.
12- Low, JGH, Ooi,EE, Vansudevan, SG Current status of Dengue therapeutics research and development Journal of Infectious Diseases 2017; 215(S2) :S 96-102
13- Towards development of a universal dengue vaccine How close are we? 2017 Asian Pacific Journal of Tropical Medicine http://dx.doi.org /10.1016/ j.apjtm.2017.03.003
14- World Health Organization, strategy for dengue prevention and control 2012-2020, Geneva, WHO 2012a.
15- Knobel DL, Cleaveland S, Coleman PG, Fèvre EM, Meltzer MI, Miranda ME, et al. Re-evaluating the burden of rabies in Africa and Asia. Bull World Health Organ (2005) 83:360–8. doi:10.1590/S0042-96862005000500012
16- Sambo M, Cleaveland S, Ferguson H, Lembo T, Simon C, Urassa H, et al. The burden of rabies in Tanzania and its impact on local communities. PLoS Negl Trop Dis (2013) 7:e2510. doi:10.1371/ journal.pntd.0002510
17- Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, et al.
129

Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis (2015) 9:e0003786. doi:10.1371/journal.pntd.0003709
18- Velasco-Villa, A , Escobar, L, Sanchez, A et al. Successful strategies implemented towards the elimination of canine rabies in the Western Hemisphere Antiviral Research 143 (2017) 1e12
19- Mitja O, Asiedu K, Mabey D. Yaws. The Lancet. 2013: 381: 763±773
20- Kazadi WM, Asiedu KB, Agana N, Mitja O. Epidemiology of yaws: an update. Clinical Epidemiology 2014: 6 119±128. https://doi.org/ 10.2147/ CLEP.S44553 PMID: 24729728
21- Boock AU, Awah PK, Mou F, NichterM (2017) Yaws resurgence in Bankim, Cameroon:The relative effectiveness of different means of detection in rural communities. PLoS Negl Trop Dis11(5): e0005557. https://doi.org/10.1371/journal.pntd.0005557
22- World Health Organization. Eradication of yaws the Morges Strategy. Wkly Epidemiol Rec2012:87:189±94. PMID: 24340400
23- World Health Organization. Buruli ulcer disease (Mycobacterium ulcerans
130

infection). Geneva: WHO, 2017. Available at: http://www.who .int /media- centre/factsheets/fs199/en/index.html.
24- Combe M , Velvin CJ, Morris A, Garchitorena A, Carolan K, Sanhueza D, Roche B, Couppié P, Guégan JF, Gozlan RE, Global and local environmental changes as drivers of Buruli ulcer emergence. Emerg Microbes Infect. 2017 Apr 26;6(4):e22. doi: 10.1038/emi.2017.7.
25- Hu VH, Harding-Esch EM, Burton MJ, Bailey RL, Kadimpeul J, Mabey DC. Epidemiology and control of trachoma: Systematic review. Trop Med Int Health. 2010;15:673–91. [PMCID: PMC3770928] [PubMed: 20374566]
26- World Health Organization. Report of the First Meeting of the WHO Alliance for the Global Elimination of Trachoma. Geneva, Switzerland: World Health Organization; 1997.
27- World Health Organization. Global WHO alliance for the elimination of blinding trachoma by 2020. Wkly Epidemiol Rec. 2013;88:241–56.
28- World Health Organization, 2016. Generic framework for control, elimination and eradication of neglected tropical diseases. Geneva: WHO. Available at http: //
131

www.who.int/neglected_diseases/ resources/ WHO_HTM_NTD_2016.6/ en/, accessed January 2017.
29- Pinsent A, Burton MJ, Gambhir M. Enhanced antibiotic distribution strategies and the potential impact of facial cleanliness and environmental improvements for the sustained control of trachoma: a modeling study. BMC Medicine 2016:14(71).
30- World Health Organization (WHO). Report of the 3rd global scientific meeting on trachoma. Johns Hopkins University, Baltimore, Maryland, 19–20 July 2010. WHO: Geneva; 2010.
31- Barreto JG, Frade MAC, Bernardes Filho F, da Silva MB, Spencer JS, Salgado CG Leprosy in Children. Curr Infect Dis Rep. 2017 Jun;19(6):23. doi: 10.1007/s11908-017-0577-6.
32- WHO global leprosy update 2015, No 35, 91 http://www.who.int/ wer
33- Rao PN Global leprosy strategy 2016-2020: Issues and concerns. Indian J Dermatol Venereol Leprol. 2017 Jan-Feb;83(1):4-6. doi:10.4103/0378-6323.195075. PMID: 27917842
34- Torgerson PR, Devleesschauwer B, Praet N, Speybroeck N, Willingham AL,
132

Kasuga F, et al. World Health Organization Estimates of the Global and Regional Disease Burden of 11 Foodborne Parasitic Diseases, 2010: A Data Synthesis. PLoS Med. 2015;12:1–22.
35- Murrell KD, Dorny P, Flisser A, Geerts S, Kyvsgaard NC, McManus DP, et al.WHO/FAO/OIE Guidelines for the surveillance, prevention and control of taeniosis/cysticercosis. OIE (World Organisation for Animal Health), WHO (World Health Organization) and FAO (Food and Agriculture Organization); 2005.
36- Wu HW, Ito A, Ai L, Zhou XN, Acosta LP, Lee WA. Cysticercosis/ taeniasis endemicity in Southeast Asia: Current status and control measures. Acta Trop Elsevier BV. 2015;165:121–32.
37- World Health Assembly. Elimination of dracunculiasis: resolution of the 39th World Health Assembly. Geneva, Switzerland: World Health Organization; 1986. Resolution WHA 39.21. http://www.who.int/ neglected_diseases/mediacentre/WHA_39.21_Eng.pdf
38- World Health Organization. Meeting of the International Task Force for Disease
133

Eradication, April 2015. Wkly Epidemiol Rec 2015;90:384–92.
39- World Health Organization. Dracunculiasis eradication: global surveillance summary, 2015. Wkly Epidemiol Rec 2016;91:219–36.
40- Hopkins DR, Ruiz-Tiben E, Eberhard ML, Roy SL. Progress toward global eradication of dracunculiasis—January 2014–June 2015. MMWR Morb Mortal Wkly Rep 2015;64:1161–5.
41- Eberhard ML, Ruiz-Tiben E, Hopkins DR, et al. The peculiar epidemiology of dracunculiasis in Chad. Am J Trop Med Hyg 2014;90:61–70.
42- Eberhard ML, Yabsley MJ, Zirimwabagabo H, et al. Possible role of fish and frogs as paratenic hosts of Dracunculus medinensis, Chad. Emerg Infect Dis 2016;22:1428–30.
43- Brooker S, Bethony J, Hotez PJ. Human
hookworm infection in the 21st century. Adv Parasitol. 2004;58:197–288.
44- WHO. Preventive Chemotheraphy in Human Helminthiasis. Geneva, Switzerland: World Health Organization; 2006.
45- WHO: Investing to overcome the global impact of neglected tropical diseases: third WHO report on neglected
134

tropical diseases. In. Edited by Holmes P. Geneva: WHO press; 2015: 191
46- Truscott, JE, Turner, HC, and Anderson, RM What impact will the achievement of the current World Health Organisation targets for anthelmintic treatment coverage in children have on the intensity of soil transmitted helminth infections? Parasites & Vectors (2015) 8:551 DOI 10.1186/s 13071-015-1135-4
47- WHO. Accelerating work to overcome the global impact of neglected tropical diseases: a roadmap for implementation. Geneva, Switzerland: World Health Organization; 2012.
48- Addiss DG, Brady MA. Morbidity management in the Global Programme to Eliminate Lymphatic Filariasis: a review of the scientific literature. Filaria J 2007: 6: 2.
49- World Health Organization. Lymphatic filariasis: Managing Morbidity and Preventing Disability [Internet], 2013. (Available from: http://apps.who.int/iris/bitstream/10665/85347/1/9789241505291_eng.pdf
50- World Health Organization, 2016. Responding to failed transmission assessment surveys. Report of an ad hoc meeting.Geneva: WHO. Available at:
135

http://www.who.int/lymphatic_filariasis/ resources/ 9789241511292/ en/accessed November 2016.
51- World Health Organization, 2017. Validation of elimination of lymphatic filariasis as a public health problem. Geneva: WHO. Available at http:// www.who.int/lymphatic_filarias is/resources/97 9241511957/en/.
52- World Health Organization 2010. LF progress report and strategic plan 2010–2020 of the Global Programme to EliminateLymphatic filariasis: halfway towards eliminating lymphatic filariasis,
53- Kelly-Hope LA, Unnasch TR, Stanton MC, Molyneux DH. Hypo-endemic onchocerciasis hotspots: defining areas of high risk through micro-mapping and environmental delineation. Infect Dis Poverty. 2015;4:36.
54- World Health Organization, 2012. Accelerating Work to Overcome the Global Impact of Neglected Tropical Diseases A Roadmap for Implementation Executive Summary. WHO/HTM/NTD/2012.1. World Health Organization, Geneva, Switzerland
55- London Declaration on Neglected Tropical Diseases, 2012. Ending the neglect and reaching 2020 goals,
136
Available at: http://unitingto combatntds .org/ downloads/press/ntd event London declaration on ntds.pdf
56- Walker,M, Stolkc, WA, Dixonc MA, Bottomley C, Diawarae L, Traoréf MO, de Vlasc SJ, Basá˜nez MG, Modelling the elimination of river blindness using long-term epidemiological and programmatic data from Mali and Senegal http://dx.doi.org/10.1016/j.epidem.2017.02.005
57- Tekle, A.H., Zouré, H.G., Noma, M., Boussinesq, M., Coffeng, L.E., Stolk, W.A.,Remme, J.H.F., 2016. Progress towards onchocerciasis elimination in theparticipating countries of the African Programme for Onchocerciasis Control:epidemiological evaluation results. Parasites Vectors 5, 66, http://dx.doi.org/10.1186/s40249-016-0160-7.
58- Koala, L., Nikiema, A., Post, R.J., Paré, A.B., Kafando, C.M., Drabo, F., Traoré, S., 2017.Recrudescence of onchocerciasis in the Comé valley in Southwest Burkina Faso.Acta Trop. 166, 96–105, http://dx.doi.org /10.1016/j.actatropica.2016.11.003.
137

59- World health Organization. Report of a meeting to review the results of studies on the treatment of schistosomiasis in pre-school-age children.Geneva: World Health Organization; 2012.
60- Chitsulo LD, Engels D, Montresor A, Savioli L. Global status of schistosomiasis. Acta Trop. 2000;77:41–51.
61- World Health Organization. Prevention and Control of Schistosomiasis and Soil-transmitted Helminthiasis. Geneva: World Health Organization; 2002.
62- MduluzaT, and Mutapi F Putting the treatment of paediatric schistosomiasis into context Infectious Diseases of Poverty (2017) 6:85 DOI 10.1186/s40249-017-0300-8
63- Papanikolaou A. Osseous hydatid disease. Trans R Soc Trop Med Hyg. 2008;102:233–8.
64- Echinococcosis Fact Sheet No. 377. World Health Organization; March. 2016. [Last retrieved on 2017 May 29]. http://www.who.int /mediacentre/factsheets/fs377/en/
65- WHO. Working to overcome the global impact of neglected tropical diseasesÐSummary. Wkly Epidemiol Rec.
138

2011; 86(13):113±20. Epub 2011/03/29. PMID: 21438440
66- Andrade DV, Gollob KJ, Dutra WO. Acute Chagas Disease: New Global Challenges for an Old Neglected Disease. PLoS Negl Trop Dis. 2014; 8(7):e3010. Epub 2014/08/01. PNTD-D-14-00148 [pii]. PubMed Central PMCID: PMC4117453. https://doi.org/10.1371/ journal .pntd. 0003010 PMID: 25077613
67- Capuani L, Bierrenbach AL, Pereira Alencar A, Mendrone A, Jr., Ferreira JE, Custer B, etal. (2017) Mortality among blood donors seropositive and seronegative for Chagas disease (1996±2000) in São Paulo, Brazil: A death certificate linkage study. PLoS Negl Trop Dis 11(5): e0005542. https://doi.org/10.1371/journal.pntd.0005542
68- Control of the leishmaniases. Report of a meeting of the WHO Expert Committee on the control of Leishmaniases. World Health Organ Tech Rep Ser No. 949, 2010; p. 1–187.
69- lvar J, Velez ID, Bern C, Herrero M, Desjeux P, Cano J, Jannin J, den Boer M. Leishmaniasis worldwide and global estimates of its incidence. PLoS One. 2012;7:e35671.
139

70- Postigo JA. Leishmaniasis in the World Health Organization Eastern Mediterranean Region. Int J Antimicrob Agents 2010; 36(1): 62–5.
71- Hailu A, Dagne DA, Boelaert M. Leishmaniasis In: Gyapong J, Boatin B, editors. Neglected Tropical Diseases—Sub-Saharan Africa. Cham: Springer International Publishing; 2016. pp. 87–112.
72- Akhtardanesh B, Mohammadi IS, Mostafavi M, Hakimmipour M& Pourafshar NG, Feline visceral leishmaniasis in Kerman, southeast of Iran: Serological and molecular study J Vector Borne Dis 54, March 2017, pp. 96–102
73- WHO (2013) Report of a WHO meeting on elimination of African trypanosomiasis (Trypanosoma brucei gambiense). Geneva: World Health Organization. ttp://apps.who.int/iris/bitstream/10665/79689/1/ WHO_HTM_NTD_IDM_2013.4_eng.pdf?ua=1.
74- WHO (2015) Report of the first WHO stakeholders meeting on rhodesiense human African trypanosomiasis Geneva: World Health Organization. http://apps.who.int/iris/bitstream/10665/181167/1/9789241508650_eng.pdf.
140

75- Franco JR, Cecchi G, Priotto G, Paone M, Diarra A, Grout L, et al. (2017) Monitoring the elimination of human African trypanosomiasis: Update to 2014. PLoS Negl Trop Dis 11(5): e0005585. https://doi.org /10.1371/journal. pntd.0005585
76- Fahal AH Mycetoma: A global medical and socio-economic dilemma PLoS Negl Trop Dis. 2017 Apr; 11(4): e0005509. Published online 2017 Apr 20. doi: 10.1371/journal.pntd.0005509 PMCID: PMC5398501
77- UNAIDS. World AIDS Day report: Results, 2012, Joint United Nations Programme on HIV/AIDS (UNAIDS): Geneva, Switzerland. 2012, Available at http://www.unaids.org/en/resources/publications /2012/name,76120,en.asp.
78- Joint United Nations Program on HIV/AIDS (UNAIDS). AIDS by the numbers 2016. http://www.unaids.org/sites/default/files/media_ asset / AIDS-by-the-numbers-2016_en.pdf. Accessed 30 Jan 2017.
79- Granich R, Gupta S, Hall I, Aberle-Grasse J, Hader S, Mermin J (2017) Status and methodology of publicly available national HIV care continua and 90-90-90 targets: A systematic review. PLoS Med
141

14(4): e1002253. doi:10.1371/journal.pmed.1002253
80- Joint UN Program on HIV/AIDS (UNAIDS). 90-90-90 An ambitious treatment target to help end the AIDS epidemic. Geneva, Switzerland 2014. http://www.unaids.org/sites/default/files/media_asset/90-90-90_ en_0.pdf.
81- UNAIDS Report on the Global AIDS Epidemic2013. Available at http://www.unaids.org/en/resources/campaigns/ globalreport2013 /globalreport/.
82- WHO. Global tuberculosis report. Geneva: World Health Organization, Dec 3, 2015.
83- Dheda K, Barry CE , Maartens G. Tuberculosis. Lancet 2016; 387: 1211–26.
84- Dheda K, Gumbo T, Gandhi NR, et al. Global control of tuberculosis: from extensively drug-resistant to untreatable tuberculosis. Lancet Respir Med 2014; 2: 321–38
85- Dheda K, Gumbo T, Maartens G, Dooley KE et al. The epidemiology, pathogenesis, transmission, diagnosis, and management of multidrug-resistant, extensively drug-resistant, and incurable tuberculosis Lancet Respir Med 2017; 5: 291–360 http://dx.doi.org /10.1016/ S2213-2600(17)30079-6
142

86- Snow RW. Global malaria eradication and the importance of Plasmodium falciparum epidemiology in Africa. BMC Med. 2015;13:23.
87- World Health Organization. World Malaria Report. Geneva: World Health Organization; 2016. http://www.who.int/malaria /publications/ world-malaria-report-2016/report/en/.
88- Hamilton M, Mahiane G, Werst E, Sanders R, Briët O, Smith T, Cibulskis R, Cameron E, Bhatt S, Weiss DJ, Gething PW, Pretorius C, Korenromp EL. Spectrum-Malaria: a user-friendly projection tool for health impact assessment and strategic planning by malaria control programs in sub-Saharan Africa. Malar J. 2017 Feb 10;16(1):68. doi: 10.1186/s12936-017-1705-3.
89- WHO. Global technical strategy for malaria 2016–2030. Geneva: World Health Organization; 2015.
90- Giha HA, Elghazali G, A-Elgadir TM, A-Elbasit IE, Eltahir EM, Baraka OZ, Khier MM, Adam I, Troye-Blomberg M, Theander TG, Elbashir MI. Clinical pattern of severe Plasmodium falciparum malaria in Sudan in an area characterized by seasonal and unstable malaria transmission Trans R Soc Trop Med Hyg. 2005;99(4):243-51
143

91- Bhatt S, Weiss DJ, Cameron E, et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 2015; 526: 207–11
92- Osman ME, Mockenhaupt FP, Bienzle U, Elbashir MI, Giha HA. Field-based evidence for linkage of mutations associated with chloroquine (pfcrt/pfmdr1) and sulfadoxine-pyrimethamine (pfdhfr/pfdhps) resistance and for the fitness cost of multiple mutations in P. falciparum. Infect Genet Evol. 2007; 7(1):52-9.
93- World Health Organization. World malaria report. Geneva: World Health Organization; 2015. http://www.who.int/malaria/publications/ world-malaria-report-2015/report/en/.
94- Walker PGT, Griffin JT, Ferguson NM, Ghani AC. Estimating the most efficient allocation of interventions to achieve reductions in Plasmodium falciparum malaria burden and transmission in Africa: a modelling study. Lancet Glob Health 2016; 4: e474–84.
95- Newby G, Hwang J, Koita K, et al. Review of mass drug administration for malaria and its operational challenges. Am J Trop Med Hyg 2015; 93: 125–34.
144

96- Brady OJ, Slater HC, Pemberton-Ross P, Edward Wenger E et al., Role of mass drug administration in elimination of Plasmodium falciparum malaria: a consensus modelling study Lancet Glob Health 2017 http://dx.doi.org/10.1016/ S2214-109X(17)30220-6
97- van den Berg RA, Coccia M, Ballou WR, Kester KE, Ockenhouse CF, Vekemans J, Jongert E, Didierlaurent AM and van der Most RG (2017) Predicting RTS,S Vaccine-Mediated Protection from Transcriptomes in a Malaria-Challenge Clinical Trial. Front. Immunol. 8:557. doi: 10.3389/fimmu.2017.00557
98- Yan I, Korenromp E, Bendavid E. Mortality changes after grants from the global fund to fight AIDS, tuberculosis and malaria: an econometric analysis from 1995 to 2010. BMC Public Health. 2015;15: 977.
145