ventilation modes and current trends
DESCRIPTION
Ventilation Modes and Current Trends. Denny Gish, BSRT, RRT Clinical Specialist, Adult Respiratory Care Legacy Emanuel Hospital and Health Center. Objectives. Review current ventilator modes Mode descriptions Review trends in Respiratory Care ARDS Network recommendations Best PEEP - PowerPoint PPT PresentationTRANSCRIPT
Ventilation Modes and Current Trends
Denny Gish, BSRT, RRTClinical Specialist, Adult Respiratory Care
Legacy Emanuel Hospital and Health Center

Objectives
• Review current ventilator modes– Mode descriptions
• Review trends in Respiratory Care– ARDS Network recommendations – Best PEEP– Recruitment Maneuvers
• Identify various methods of High Frequency Ventilation


Modes of Ventilation
The Critical Question...
How do you choose ?
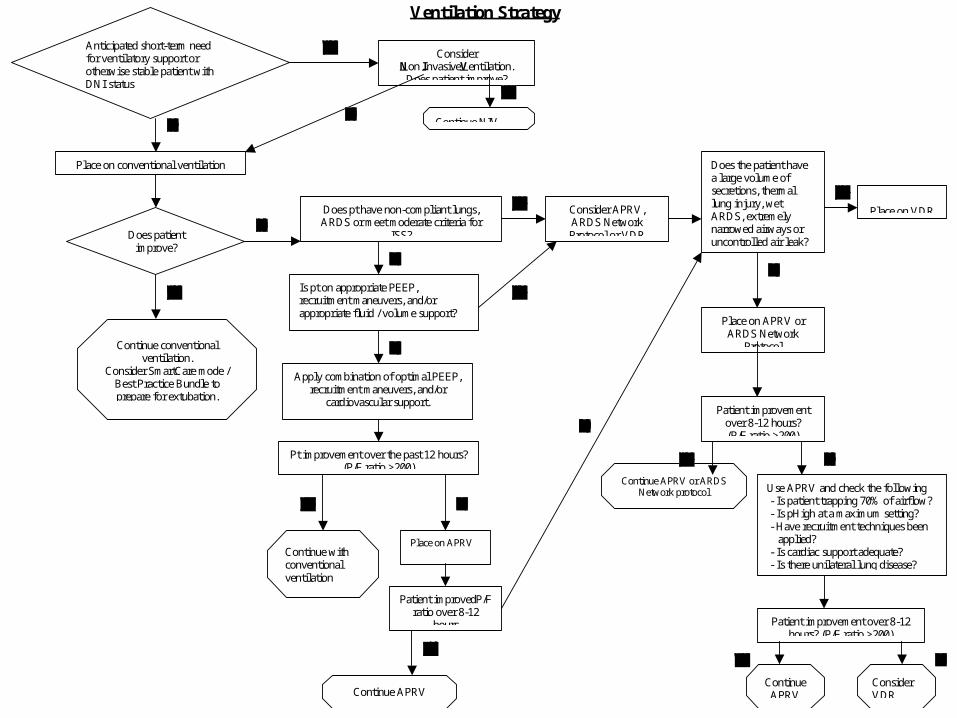
Ventilation Strategy
Anticipated short-term need for ventilatory support or otherwise stable patient with DNI status
Place on conventional ventilation
Does patient improve?
Does pt have non-compliant lungs, ARDS or meet moderate criteria for
ISS?
Is pt on appropriate PEEP, recruitment maneuvers, and/or appropriate fluid / volume support?
Apply combination of optimal PEEP, recruitment maneuvers, and/or
cardiovascular support.
Pt improvement over the past 12 hours? (P/F ratio >200)
Continue with conventional ventilation
Patient improvedP/F ratio over 8-12
hours
Consider APRV, ARDS Network Protocol or VDR
Does the patient have a large volume of secretions, thermal lung injury, wet ARDS, extremely narrowed airways or uncontrolled air leak?
Place on VDR
Place on APRV or ARDS Network
Protocol See attached document
Patient improvement over 8-12 hours? (P/F ratio >200)
Continue APRV
Use APRV and check the following - Is patient trapping 70% of airflow? - Is pHigh at a maximum setting? - Have recruitment techniques been applied? - Is cardiac support adequate? - Is there unilateral lung disease? - Is there severe airway obstruction?
Patient improvement over 8-12 hours? (P/F ratio >200)
Continue APRV
Consider VDR
Consider Non InvasiveVentilation.
Does patient improve?
Continue NIV
Place on APRV
Continue APRV or ARDS Network protocol
Continue conventional ventilation.
Consider SmartCare mode / Best Practice Bundle to prepare for extubation.
What Starts the Breath ?
• Controlled or timed breaths• Controller is really an interval timer• Assisted breaths are triggered by patient
inspiratory effort in addition to Controlled breaths
• Spontaneous breaths allowed in some modes
What Ends the Breath ?
• Preset pressure reached• Preset volume is delivered• Preset time has elapsed

Ventilator Settings• Mode: Volume control, Pressure control, Spontaneous, etc
(how the breath goes in)
• Vt:Tidal Volume (size of breath 8-10 cc/kg, 4-6cc/kg for ARDS)• “Volutrauma” can be as damaging as “Barotrauma”
• f : Frequency (rate # breaths per minute 10-15 bpm)
• PEEP: Positive End Expiratory Pressure (>/= 5 cmH20)
• IP: Inspiratory Pressure (ideally < 30 cmH20)
• FIO2: Fraction of Inspired Oxygen
All ordered by MD or by unit protocol• Ti or V: Inspiratory time or Flowrate (how long it takes the breath
to go in - generally per RT discretion based on pt comfort & condition)
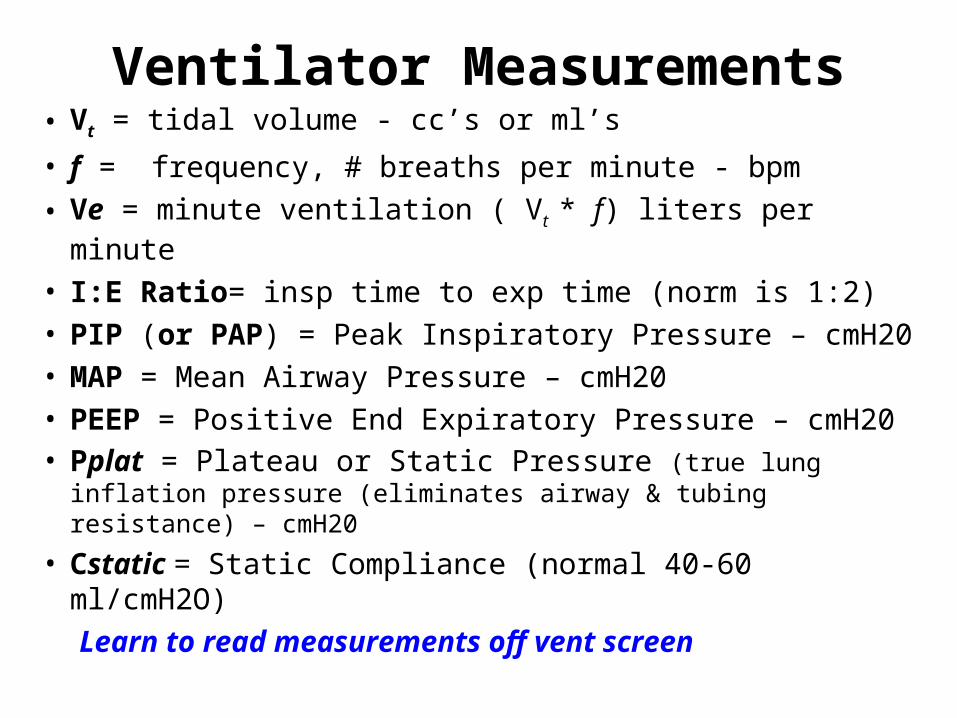
Ventilator Measurements• Vt = tidal volume - cc’s or ml’s
• f = frequency, # breaths per minute - bpm• Ve = minute ventilation ( Vt * f) liters per minute
• I:E Ratio= insp time to exp time (norm is 1:2)• PIP (or PAP) = Peak Inspiratory Pressure – cmH20• MAP = Mean Airway Pressure – cmH20• PEEP = Positive End Expiratory Pressure – cmH20• Pplat = Plateau or Static Pressure (true lung inflation
pressure (eliminates airway & tubing resistance) – cmH20
• Cstatic = Static Compliance (normal 40-60 ml/cmH2O)Learn to read measurements off vent screen
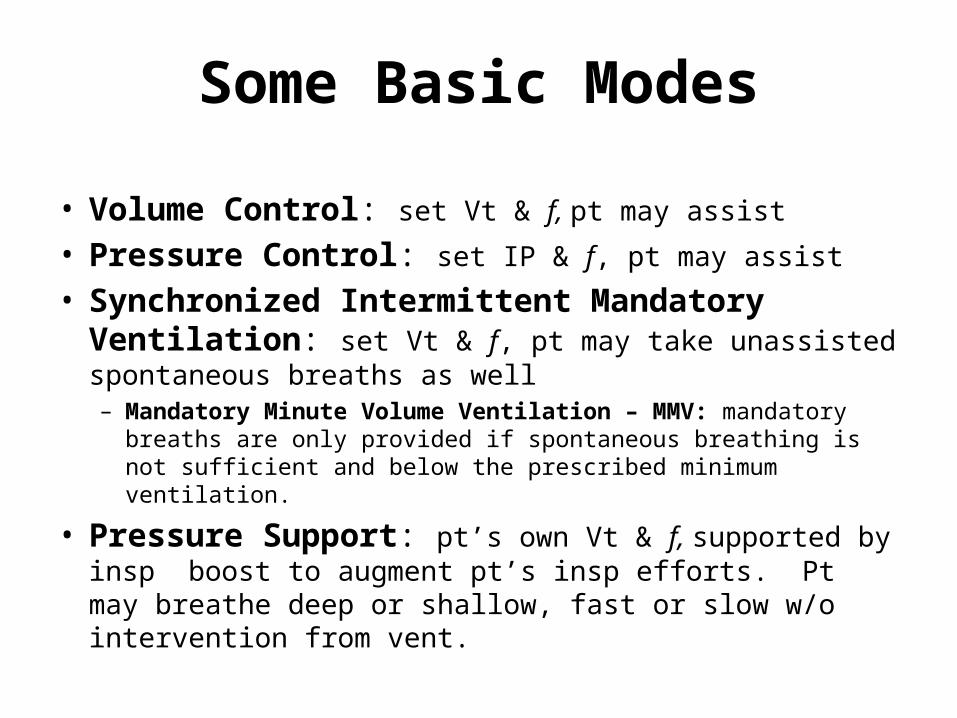
Some Basic Modes
• Volume Control: set Vt & f, pt may assist
• Pressure Control: set IP & f, pt may assist
• Synchronized Intermittent Mandatory Ventilation: set Vt & f, pt may take unassisted spontaneous breaths as well– Mandatory Minute Volume Ventilation – MMV: mandatory breaths
are only provided if spontaneous breathing is not sufficient and below the prescribed minimum ventilation.
• Pressure Support: pt’s own Vt & f, supported by insp boost to augment pt’s insp efforts. Pt may breathe deep or shallow, fast or slow w/o intervention from vent.
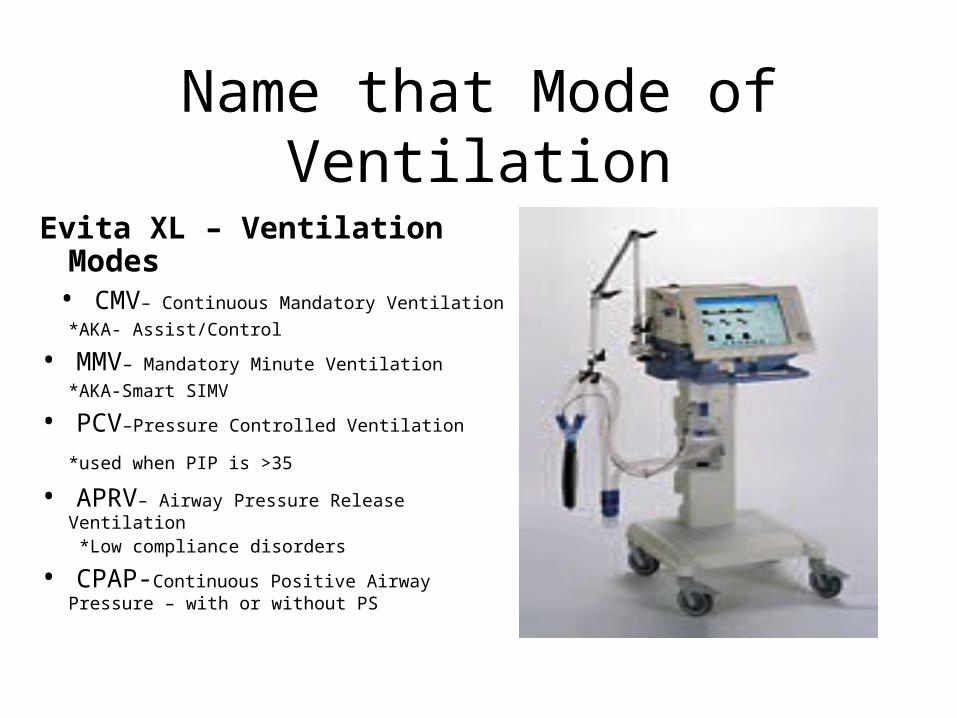
Name that Mode of Ventilation
Evita XL – Ventilation Modes
• CMV– Continuous Mandatory Ventilation
*AKA- Assist/Control
• MMV– Mandatory Minute Ventilation
*AKA-Smart SIMV
• PCV–Pressure Controlled Ventilation
*used when PIP is >35
• APRV– Airway Pressure Release Ventilation
*Low compliance disorders
• CPAP-Continuous Positive Airway Pressure – with or without PS

Draeger V 500Ventilation mode
VC-CMV - Draeger XL has CMV, but it is NOT the same!
VC-AC–Works like CMV on the Draeger XL
VC-MMV-Draeger XL has MMV and it performs exactly like the VC-MMV on the V500
PC-AC – Draeger XL has PCV
PC-APRV with AutoRelease - Draeger XL does not have an autorelease function
SPN-CPAP/PS/VS-Draeger XL has CPAP mode that has Pressure Support capabilities, but no Volume Support

Now…Puritan Bennet 840

Viasys Avea

Servo I buy
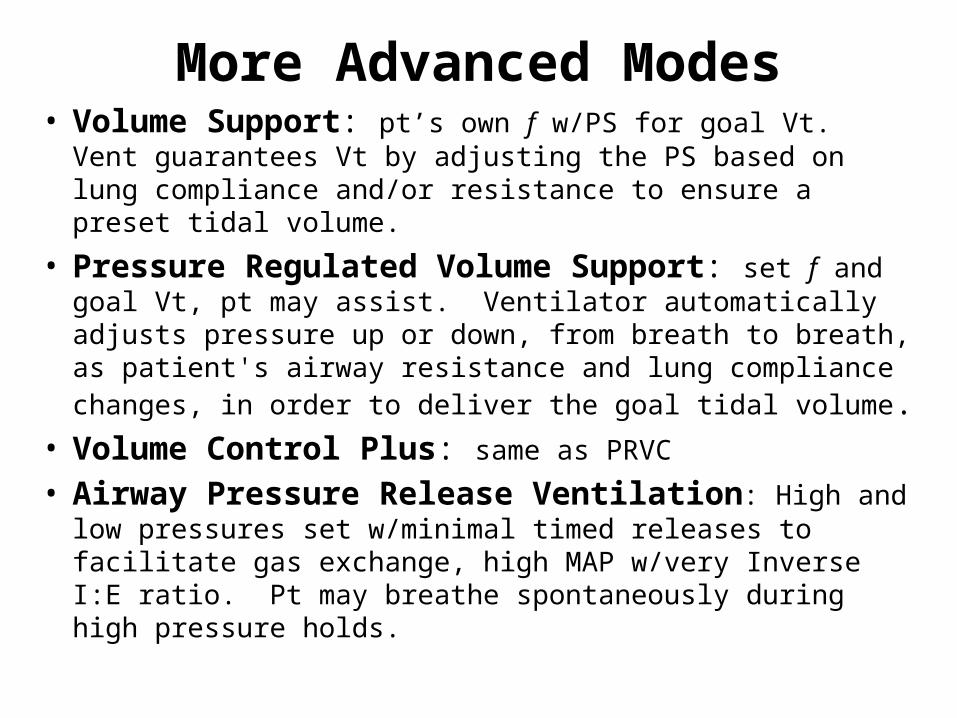
More Advanced Modes• Volume Support: pt’s own f w/PS for goal Vt. Vent
guarantees Vt by adjusting the PS based on lung compliance and/or resistance to ensure a preset tidal volume.
• Pressure Regulated Volume Support: set f and goal Vt, pt may assist. Ventilator automatically adjusts pressure up or down, from breath to breath, as patient's airway resistance and lung compliance changes, in order to deliver the goal tidal volume.
• Volume Control Plus: same as PRVC
• Airway Pressure Release Ventilation: High and low pressures set w/minimal timed releases to facilitate gas exchange, high MAP w/very Inverse I:E ratio. Pt may breathe spontaneously during high pressure holds.

ARDS Current Definition
• Onset - Acute and persistent• Radiographic - Bilateral pulmonary
infiltrates • Oxygenation - regardless of the PEEP, with
a Pao2/Fio2 ratio 300 for ALI and 200 for ARDS
• Exclusion criteria - Clinical evidence of Left Atrial Hypertension or a PAOP of 18 mm Hg.
Bernard GR et al., Am J Respir Crit Care Med 1994
The 1994 North American-European Consensus Conference The 1994 North American-European Consensus Conference (NAECC) Criteria:(NAECC) Criteria:

Tidal Volume Strategies in ARDS
Traditional ApproachTraditional Approach
High priority to traditional High priority to traditional goals of acid-base balance goals of acid-base balance and patient comfortand patient comfort
Lower priority to lung Lower priority to lung protectionprotection
Low Stretch ApproachLow Stretch Approach
High priority to lungHigh priority to lung protectionprotection
Lower priority to Lower priority to traditional goals of acid-traditional goals of acid-base balancebase balance
and comfortand comfort
Physiologic Benefits vs Patient-Important Outcomes
PaO2 improvementPaO2 improvement vs vs Survival BenefitSurvival Benefit• For ARDS, inhaled nitric oxide For ARDS, inhaled nitric oxide improves PaO2, but not improves PaO2, but not
mortalitymortality(Taylor et al, JAMA 2004;291:1603)
• High tidal volumes in patients with ARDS High tidal volumes in patients with ARDS improvesimprovesPaO2PaO2, , but mortality is lower for small tidal volumesbut mortality is lower for small tidal volumes
(ARDSnet, N Engl J Med 2000; 342:1301)
• For ARDS, prone position For ARDS, prone position improves PaO2, but notimproves PaO2, but notmortalitymortality
(Gattinoni, N Engl J Med 2001;345:568)
ARDS Network Low VT Trial
Patients with ALI/ARDS of < 36 hours
Ventilator procedures • Volume-assist-control mode• 6 vs. 12 ml/kg of predicted body weight Vt
(PBW/Measured body weight = 0.83)• Plateau pressure 30 vs. 50 cmH2O• Ventilator rate 6-35 to achieve a pH goal
of 7.3 to 7.45 • Oxygenation goal: PaO2 55 - 80 mmHg, SpO2 88 - 95%
) ARDS Network. N Engl J Med. 2000.
Lung Recruitment
First and foremost performed to provide an arterial oxygen saturation of 90% or greater at an FiO2 of less than 60%
Recruitment of nonaerated lung units (open-lung concept) but risk of regional lung overinflation :
a highly controversial issue!
Recruitment Maneuvers (RMs)Effective in improving arterial oxygenation at low PEEP and small tidal volumes. Recruitment maneuvers may be poorly effective or deleterious, inducing overinflation of the most compliant regions, hemodynamic instability, and an increase in pulmonary shunt resulting from the redistribution of pulmonary blood flow toward nonaerated lung regions.The effect of recruitment may not be sustained unless adequate PEEP is applied to prevent derecruitment.Many questions still need to be answeredMany questions still need to be answered
PEEP in ARDS:How much is enough ?
PEEP, by avoiding repetitive opening and collapse of atelectatic lung units, could be protective against VILIPEEP, has been shown to prevent surfactant loss in the airways and avoid surface film collapse. The lung is kept open by using PEEP to avoid end-expiratory collapse.High PEEP should make the mechanical ventilation less dangerous than low PEEP.
Levy MM. N Engl J Med. 2004.Rouby JJ, et al. Am J Respir Crit Care Med. 2002.Gattinoni L, et al. Curr Opin Crit Care. 2005.
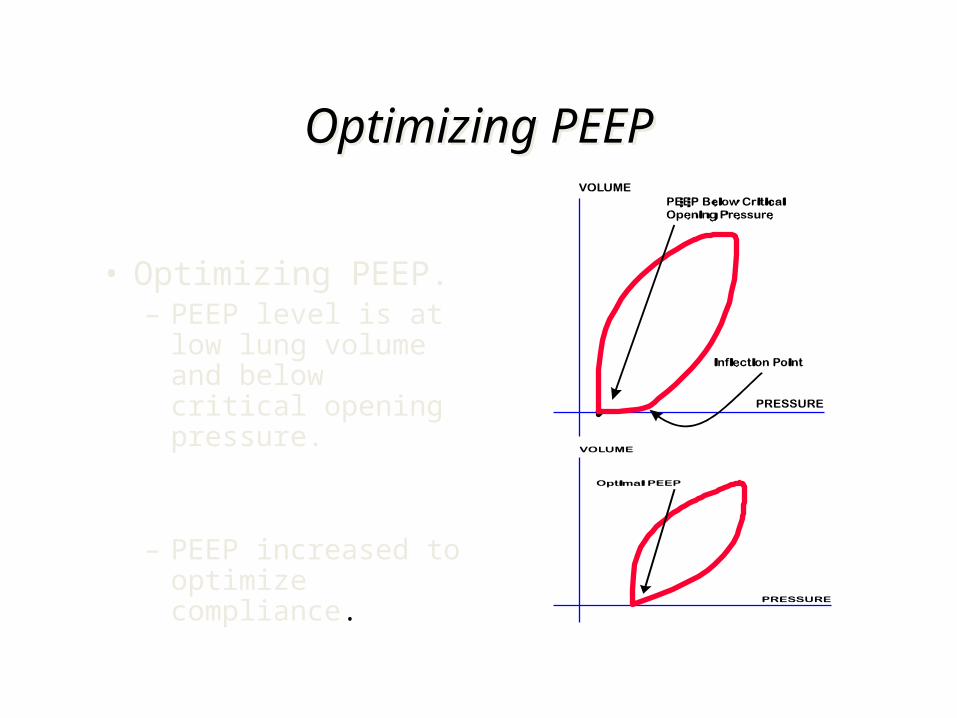
Optimizing PEEPOptimizing PEEP
• Optimizing PEEP.– PEEP level is at low
lung volume and below critical opening pressure.
– PEEP increased to optimize compliance.
larson
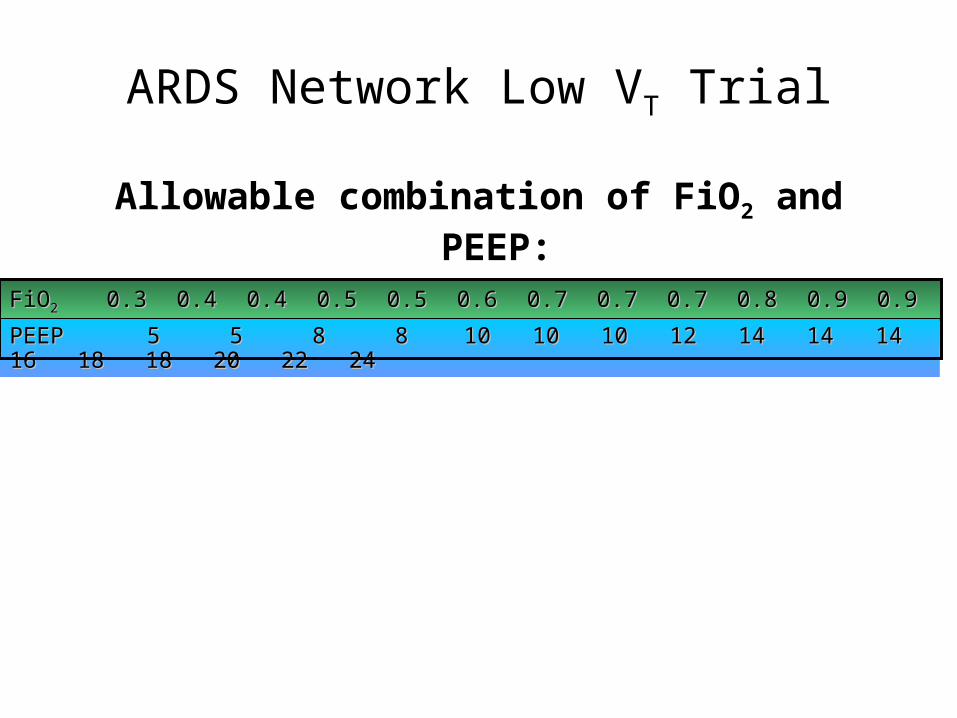
ARDS Network Low VT Trial
Allowable combination of FiO2 and PEEP:
FiOFiO22 0.3 0.4 0.4 0.5 0.5 0.6 0.7 0.7 0.7 0.8 0.9 0.9 0.9 1.0 1.0 1.0 0.3 0.4 0.4 0.5 0.5 0.6 0.7 0.7 0.7 0.8 0.9 0.9 0.9 1.0 1.0 1.0 1.01.0PEEP 5 5 8 8 10 10 10 12 14 14 14 16 18 18 20 22 PEEP 5 5 8 8 10 10 10 12 14 14 14 16 18 18 20 22 2424
APRV Mode
• First described 1987• Baseline airway pressure is the upper CPAP
level, and the pressure is intermittently “released” to a lower level, thus eliminating waste gas
• Time spent at low pressure (short expiratory time): prevents complete exhalation; maintains alveolar distension
APRV Evidence
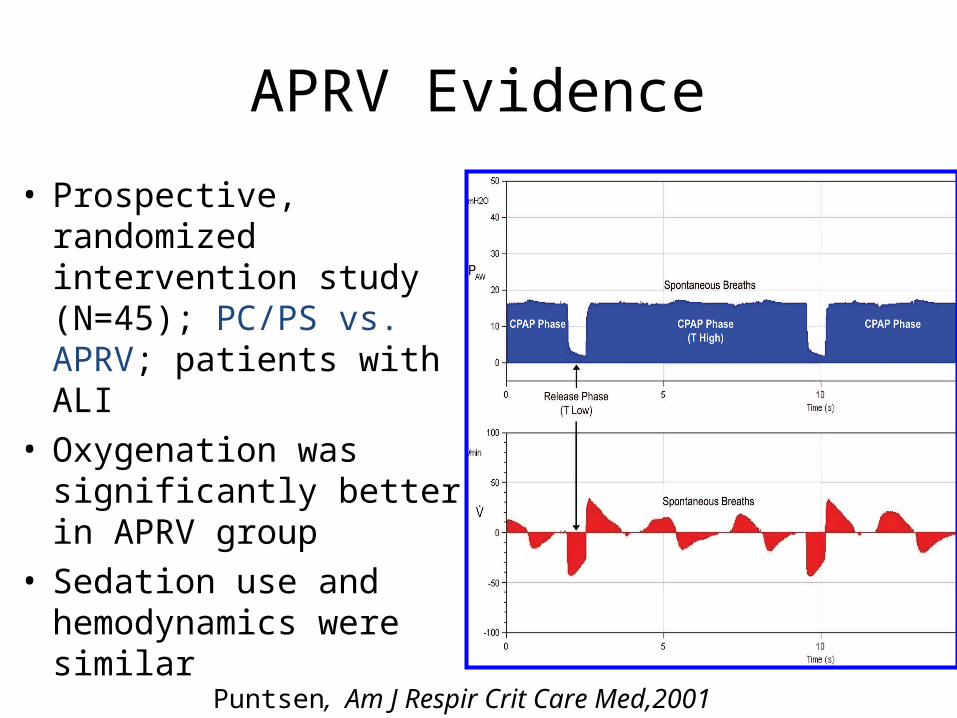
• Prospective, randomized intervention study (N=45); PC/PS vs. APRV; patients with ALI
• Oxygenation was significantly better in APRV group
• Sedation use and hemodynamics were similar
Puntsen, Am J Respir Crit Care Med,2001
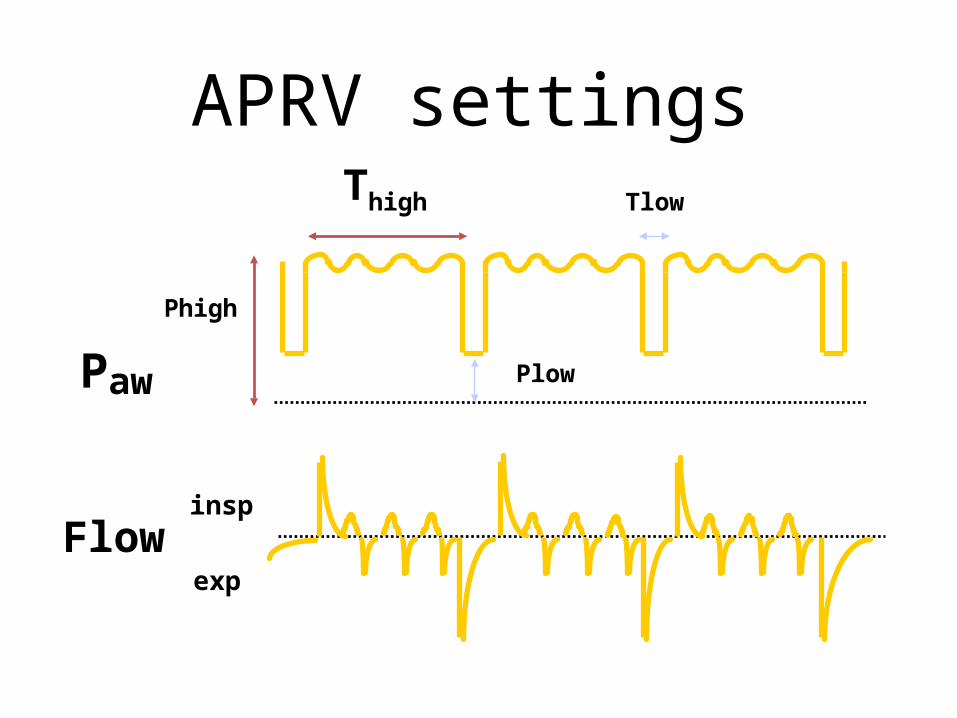
APRV settings
Flow
Paw
Thigh Tlow
Phigh
Plow
insp
exp
“If this...
why not this?”
- John B. Downs, MD

High Frequency Ventilation
HFOVOscillatory
HFJVJET
HFPVPercussive
High Frequency Percussive Ventilation
HFPV
• -High Frequency Percussive Ventilation (HFPV) is a hybrid form of high frequency ventilation.
• -This concept of pneumatic diffusive / convective protocols is not related to high frequency vibration, jet insufflation or electronically controlled crank or magnetically servoed dynamic oscillators.
Rationale for HFV-Based Lung Protective Strategies
• HFV uses very small tidal volumes– Avoids excessive end-inspiratory lung volumes– Allows for higher end-expiratory lung volumes
to achieve better recruitment• HFV uses much higher respiratory rates
– Allows for maintenance of normal PaCO2 even with very small tidal volumes

High-frequency Ventilation• HFOV may improve oxygenation when used as a rescue
modality in adult patients with severe ARDS failing CV.HFOV may be considered for patients with severe ARDS:• FiO2 > 0.60 and/or SpO2 < 88% on CV with PEEP > 15 cm H2O,
or• Plateau pressures (Pplat) > 30 cmH2O, or• Mean airway pressure 24 cm H2O, or• Airway pressure release ventilation Phigh 35 cm H2O
HFOV for adults with ARDS is still in its infancy and requires further evaluations.
Higgins J et al., Crit Care Med 2005
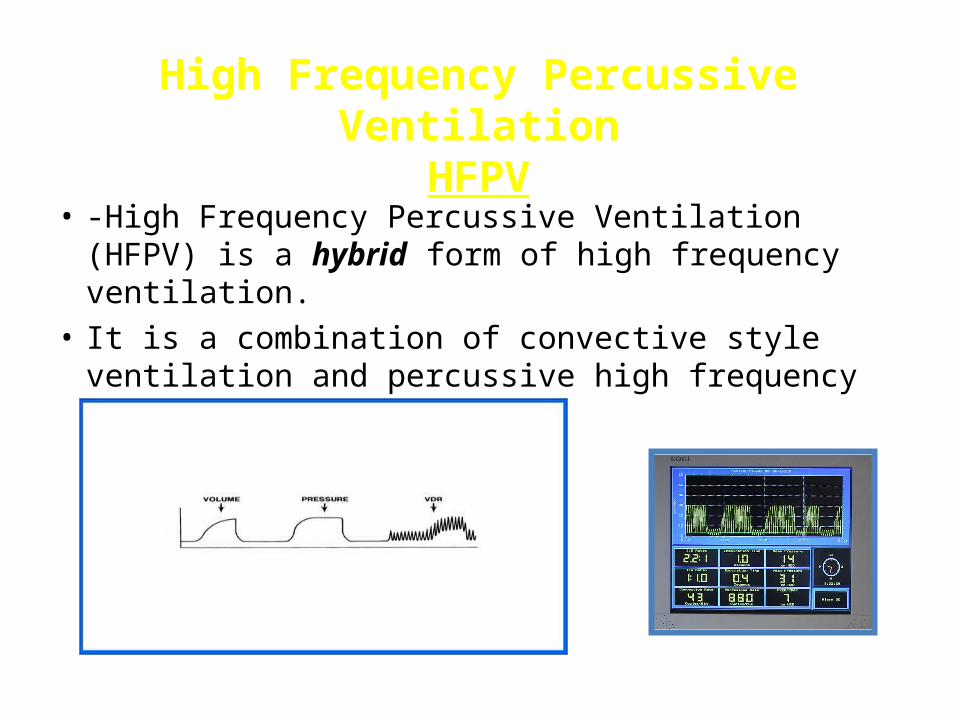
High Frequency Percussive Ventilation
HFPV• -High Frequency Percussive Ventilation (HFPV) is
a hybrid form of high frequency ventilation.• It is a combination of convective style ventilation
and percussive high frequency linked together.

Inverse Ratio Ventilation
• Technique used prior to latest generation of vents• Used in refractory hypoxemia• Another way to increase FRC• Expiratory time is longer than inspiratory time.• Heavy sedation/paralytics required • Fluids, pressors usually needed as well due to
decrease in venous return to thorax
Sometimes occurs inadvertently by erroneous vent changes or pt agitation & high RR. Must be corrected!
Other Advanced InterventionsRequire separate or additional machines
• Inhaled Nitric Oxide selective pulmonary artery vasodilator. Used for pulm htn, lg saddle PE’s, to reduce intrapulmonary shunting & improve V/Q matching. Prohibitively expensive, may cause methemoglobin buildup
• High Frequency Ventilation high frequency (>200 breathes per min) – HFOV, HFJV, HFPV
• Extracorporeal Membrane Oxygenation (ECMO) similar to bypass pump used in cardiac surgery

Adjuncts
• Recruitment Maneuver– PEEP - does not recruit alveoli, but can help
maintain alveolar stability
• Prone positioning – has not changed morbidity or mortality outcomes in ARDS, but has been shown to help improve oxygenation
A man suffered from insomnia and dyslexia. He was also an
agnostic. What did he do?
He stayed up all night wondering if there was a DOG.