vasa dialysis access symposium xiv
TRANSCRIPT

114th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
VASA OFFICERS & BOARD OF DIRECTORSThomas M. Vesely, MD PresidentSurendra Shenoy, MD, PhD President-ElectMitchell Henry, MD Immediate Past PresidentJack Work, MD SecretaryTheodore F. Saad, MD TreasurerDeborah J. Brouwer-Maier RN, CNNIngemar J. Davidson, MDDirk M. Hentschel, MDBrian G. LaMendola, RN, MBAJeffery H. Lawson, MD, PhDCharmaine Lok, MDEric K. Peden, MDHaimanot Wasse, MD, MPH
VASA DIALYSIS ACCESS SYMPOSIUM 2014 PROGRAM COMMITTEETheodore F. Saad, MD, ChairmanJohn Aruny, MDLynda Ball, MSN, RN, CNNDavid Cull, MDCharmaine Lok, MD
PURPOSE & OBJECTIVESThis symposium is convened to gather individuals who are interested in vascular access and to promote excellence in the care of patients with end stage kidney disease.
FACULTY PRESENTATIONS At the conclusion of this symposium, the participant should be able to:
1. Describe optimal use of arteriovenous fistulas, grafts, and venous catheters for hemodialysis access.
2. Recognize the role for peritoneal dialysis and techniques for PD catheter insertion
3. Recite how to manage venous stenosis associated with grafts & fistulas, including optimal use of venous stents
4. Explain how to avoid and manage fistula needle site aneurysms
5. Discuss cardiologic issues related to arteriovenous hemodialysis access
6. Tell about dialysis access management and health care delivery systems in other countries
7. Describe changes in regulatory and reimbursement models that may affect dialysis access management in the USA
8. Demonstrate how to monitor & improve dialysis access outcomes to deliver high quality care and minimize risk
ABSTRACT PRESENTATIONS 1. Examine techniques for creation, maintenance, or
salvage of dialysis vascular access2. Explain strategies for achieving optimal dialysis
vascular access outcomes in clinical practice or healthcare delivery systems
3. Recognize novel devices or technologies for achieving successful vascular access
DISCLOSURE INFORMATIONIn compliance with ACCME Accreditation Criteria, the American College of Surgeons, as the accredited provider of this activity, must ensure that anyone in a position to control the content of the educational activity has disclosed all relevant financial relationships with any commercial interest. All reported conflicts are managed by a designated official to ensure a bias-free presentation. Each speaker will disclose any conflict of interest at the time of their presentation.
ELECTRONIC EVALUATIONSElectronic Evaluations must be completed in order to successfully complete and claim Continuing Education for this event. Visit www.vasamd.org/2014resources to evaluate each session for which you are claiming credit. Speaker presentations can also be found online using this website.
VASA DIALYSIS ACCESS SYMPOSIUM XIV14th Biennial Symposium on Dialysis Access

214th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
AMA PRAThis activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of the University of Kentucky College of Medicine, and Vascular Access Society of the Americas. The University of Kentucky College of Medicine is accredited by the ACCME to provide continuing medical education for physicians.
The University of Kentucky College of Medicine designates this live activity for a maximum of 12.75 AMA PRA Category 1 Credit(s)™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
The University of Kentucky College of Medicine presents this activity for educational purposes only. Participants are expected to utilize their own expertise and judgment while engaged in the practice of medicine. The content of the presentations is provided solely by presenters who have been selected for presentations because of recognized expertise in their field.
The University of Kentucky is an Equal Opportunity University
To receive AMA PRA credit, at the conclusion of this activity:1. Open your Internet browser (Internet Explorer, Firefox,
Safari, AOL, etc.) and go to www.CECentral.com/getcredit. 2. In the box marked ‘Activity Code’, enter MLS14139 and
click ‘Search’.3. The appropriate activity details will display; click ‘Proceed
to Credit’ on the right hand side.4. If you are not signed into CECentral.com, you will either
need to log in or create an account (free of charge).a. Create ID by filling out the one time information
screen. b. If you are not automatically logged in, please return to
step 1 and proceed from there.5. CECentral will ask you to check all the sessions you
attended. Please do so to receive a complete, correct certificate.
6. Check the box at the bottom verifying your attendance and click Submit
7. Complete the evaluation and click submit.8. Your certificate will appear; you can print it or view it later
by clicking ‘Transcript’ in the grey bar at the top of the page.
If you experience any difficulty in claiming credit online, please call CECentral at (859) 257-5320 between 8:00 am - 4:30 pm ET, Monday-Friday.
IMPORTANT! The deadline to claim credit online is June 2, 2014.
ARRT-RECOGNIZED CONTINUING EDUCATION EVALUATION MECHANISM (RCEEM)This continuing education activity is approved by the AVIR for 15.5 Category A+ CEs. Participants must complete the entire activity as designed and approved to earn the credit. A certificate of attendance will be provided at the conclusion of the event for your personal records.
ANCC CREDITThe University of Kentucky, College of Nursing is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
This activity is offered for up to a maximum of ANCC 13.0 contact hours. In order to receive credit for this 2 day conference, participants will complete the CNE activity and submit a credit application and evaluation form online. Certificates may be printed once the evaluation is completed.
Accessing Certificate – You must complete the program evaluation at the event prior to logging on to access your certificate1. Log onto http://moodle.ukconce.org; enter your user
name and password; create an account if you do not have an existing account for this site
2. Select “Evaluation and CE Request for Live Courses”3. Select “VASA Dialysis Access Symposium” and your date/s
of attendance4. Enter enrollment key: 001675. Download the nursing CE certificate.
QUESTIONS – Email the College of Nursing Continuing Education office at [email protected].
ASCP CMLE CREDITThis continuing medical laboratory education activity is recognized by the American Society for Clinical Pathology for CMLE credit. ASCP CMLE credits are acceptable for the ASCP Board of Registry Certification Maintenance Program.
TEXAS BME CREDITThe Vascular Access Society of the Americas Dialysis Access Symposium: Legal and Ethical Issues in Vascular Access session was approved for one hour of Medical Ethics/Professional Responsibility designation by the Texas Medical Board.
314th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
INVITED FACULTY
PROGRAM CHAIR
Theodore F. Saad, MDNephrology Associates, PAChief, Section of Renal & Hypertensive DiseasesChristiana Care Health SystemNewark, Delaware
Program Committee Members John E. Aruny, MDLynda K. Ball, MSN, RN, CNNDavid L. Cull, MD, FACSCharmaine Lok, MD
FACULTY
John Aruny, MDCo-Director, Vascular & Interventional RadiologyYale University School of Medicine New Haven, CT
Lynda K. Ball, MSN, RN, CNNQuality Improvement Director FMQAI: ESRD Network 13Oklahoma City, OK
Deborah J Brouwer-Maier RN CNNDirector of Dialysis Access InitiativesFMS- Medical OfficeWarrendale, PA
Lee L. Cameron, Jr, EsqPartner at Wilson, Elser, Moskowitz, Edelman, & Dicker, LLPDallas, TX
Eric Chemla, MD Chair of the Division of Specialist Medicine and Cardiovascular Sciences University of London, St George’s Medical School London, UK
Timothy Clark, MDAssociate Professor of Clinical Radiology University of Pennsylvania School of Medicine Philadelphia, PA
David Cull, MD Vice-Chair Academic AffairsProfessor of SurgeryUniversity of South Carolina School of Medicine- Greenville Greenville, SC
Ingemar Davidson, MD Professor of Surgery University of Texas - Southwestern Medical Center Dallas, TX
Maurizio Gallieni, MD Director, Nephrology and Dialysis Unit Ospedale San Carlo Borromeo Milan, Italy
Dirk M. Hentschel, MDInterventional Nephrology, Brigham and Women’s Hospital Assistant Professor of Medicine, Harvard Medical SchoolCambridge, Massachusetts
Nicholas Inston, MD, PhD Clinical Lead for Renal Surgery and Transplantation Queen Elizabeth Hospital Birmingham, UK
Jeffrey Lawson, MD Professor of Surgery Duke University School of Medicine Durham, NC
Charmaine Lok, MD Professor, Faculty of Medicine University of Toronto Toronto, ON, CA
Dugan Maddux, MD, FACPVP Kidney Disease InitiativesFresenius Medical ServicesWaltham, MA
Jan Malik, MDVascular Access CenterFirst Faculty of Medicine, Charles UniversityGeneral University HospitalPrague, Czech Republic
Eric Peden, MD Chief of Vascular Surgery Methodist DeBakey Heart and Vascular Center at The Methodist Hospital Houston, TX
Robert Provenzano, MD Vice President Medical AffairsDaVitaDenver, CO
Dorian Schatell, MS Executive DirectorMedical Education Institute, Inc.Madison, WI
Larry Scher, MD Vascular SurgeonMontefiore Medical CenterBronx, NY
Fred Schild, MD Professor of SurgeryFlorida International University Miami, FL

414th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
Jeffrey Schussler, MD, FACC, FSCAI Medical Director: CVICU - Baylor Heart and Vascular Hospital Professor of Medicine: Texas A&M School of Medicine Dallas, TX
Surendra Shenoy, M.D., Ph.D. Professor of Surgery Washington University School of Medicine St Louis, MO
Jaime Velez, MD Vascular Surgeon Clinica Amiga Cali, Colombia
Thomas Vesely, MDInterventional Radiologist Vascular Access Center of Frontenac GroveSt Louis, MO
Haimanot Wasse, MD Associate Professor of MedicineEmory University School of Medicine Atlanta, GA
Jack Work, MD Professor of Medicine, EmeritusEmory University School of MedicineAtlanta, GA

514th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
EXHIBITORSARTEGRAFT, INC. ARTEGRAFT® collagen vascular graft is like a Fistula in a Bottle™ -ideal for fistula salvage and repair. JVS published 3-year randomized, prospective study by Massachusetts General Hospital confirms superior primary patency and lower intervention rates of the Bovine Carotid Artery Graft™ to ePTFE. Artegraft is pulsatile, available for access within 10 days. Triple pressure tested to insure quality and reliability. Superior surgical handling and anastomotic compliance with no suture line bleeding.
Contact: Rick Gibson206 N. Center DriveNorth Brunswick, NJ 08902Tel: (800) [email protected]
BRAINTREE Our main focus at Braintree is to accelerate productivity for specialty outpatient procedure centers through our medical software applications. Our products are meant to deliver integrated, end-to-end software solutions and professional services that can help transform the way you interact with referring physicians, manage your workflow, position your business in your markets, and give high quality patient care.
Through our medical software applications, we help ensure your success in today’s competitive healthcare environment by streamlining your business and clinical workflow with digital images and information solutions. The end goal is to make your medical facility a completely paperless system with cutting-edge technology that will improve efficiency and your bottom line.
Contact: Sunil ReddyPO Box 272000Corpus Christi, TX 78427Tel: (512) [email protected]
CR BARD PERIPHERAL VASCULAR, INC. Bard Peripheral Vascular, Inc. provides a range of interventional medical devices specifically designed for the treatment of peripheral arterial, hemodialysis access and venous disease. These products include; Flair® Endovascular Stent Graft approved for dialysis access and market leading offerings of Peripheral PTA Dilatation Catheters and dialysis catheters.
Contact: Kristen Nedoba 1625 W 3rd Street Tempe, AZ 85281Tel: (480) [email protected]
CRYOLIFECryoLife® is a leader in the development and implementation of advanced technologies associated with vascular allograft processing and cryopreservation. CryoLife also has the HeRO Graft (Hemodialysis Reliable Outflow). HeRO Graft is the ONLY fully subcutaneous AV access solution clinically proven to maintain long-term access for hemodialysis patients with central venous stenosis.
Contact: Stephanie Amburn1655 Roberts BlvdKennesaw, GA 30144Tel: (770) [email protected]

614th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
DIRECTACCESS MEDICAL DirectACCESS Medical Is dedicated to developing innovative solutions to specifically address the unique needs of the dialysis access patient and clinicians. We work with all of the larger access center management companies as well as independently owned and operated facilities to deliver advancements in all aspects of dialysis access.
Our initial products, that are now commercially available, are the FirstChoice UHP PTA line of balloon catheters. From concept to launch, the FirstChoice products were purpose built to address the wide range of lesions that present in access. They are the strongest first line utility balloons available on the market and are designed to deliver superior trackability. With FirstChoice, clinicians are now able to treat the majority of access related lesions with a single line of PTA catheters.
Contact: Chris PeeleFounder & PrincipalDirectACCESS Medical, LLCTel: (614) 893-3096 [email protected]
FORGE MEDICAL, INC.Forge Medical, Inc., based in Philadelphia, PA was founded in 2009 to develop innovative solutions for clinical challenges in vascular care. Our team of dedicated physicians, nurses, engineers and regulatory professionals offer a unique blend of experience in the interventional medical device community. This combination of years of inventing, designing, developing and clinically using innovative medical devices has impacted the lives of thousands of patients worldwide. Contact: Timothy Clark 8516 Parkwood Lane, Suite 100 Philadelphia, PA 19128Tel: (877) 466-0109 [email protected]
FRESENIUS VASCULAR CAREFresenius Vascular Care (FVC) is the largest owner/operator of freestanding vascular centers in the US. We’re primarily dedicated to the care of dialysis vascular access, but treat a variety of medical conditions, including Peripheral Arterial Disease (PAD), Venous Insufficiency/Varicose Veins and Uterine Fibroids. We are committed to improving the standard of care and quality of life for our patients and are “Dedicated to the Exceptional Patient Experience.”
Contact: Ellen Ferreira 400 Connell Drive – Suite 2200Berkeley Heights, NJ 07922Tel: (908) [email protected]
GORE MEDICAL PRODUCTS DIVISIONThe Gore Medical Products Division has provided creative therapeutic solutions to complex medical problems for three decades. During that time, more than 35 million innovative Gore Medical Devices have been implanted, saving and improving the quality of lives worldwide. The extensive Gore Medical family of products includes vascular grafts, endovascular and interventional devices, surgical materials for hernia repair, soft tissue reconstruction, staple line reinforcement and sutures for use in vascular, cardiac and general surgery. Gore was recently named one of the best companies to work for by Fortune magazine for the 17th consecutive year. For more information, visit http://www.goremedical.com.
Contact: Elaine Silashki1505 N Fourth Street Flagstaff, AZ 86004Tel: (928) [email protected]

714th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
LEMAITRE VASCULARLeMaitre Vascular was founded in 1983 by George D. LeMaitre, M.D., a vascular surgeon and the inventor of our first product, the valvulotome. Over the years we have remained focused on the needs of vascular surgeons when they work in peripheral vessels. We develop, manufacture, and market disposable and implantable vascular devices for use in both open vascular surgery and minimally invasive endovascular procedures. Our product lines consist of well-known brand name products used in arteries and veins outside of the heart and are supported by a growing, specialized and highly trained organization of vascular sales professionals.
Contact: Chance KrieselDirector of Sales - West 63 Second AvenueBurlington, MA 01803Tel: (602) 505-8321 [email protected] www.lemaitre.com
MAQUET MEDICAL SYSTEMSMAQUET Medical Systems, USA is a market leader offering a comprehensive portfolio of products utilized in the Hybrid OR, ICU, Cath Lab which are designed to meet the needs of clinical professionals in the areas of: surgery, cardiac intervention, peripheral intervention, dialysis, perfusion, anesthesia, and respiratory. MAQUET is focused on improving patient care and quality of life, providing clinicians with future-oriented technology that fits their daily practice and investing in the development of innovative technologies and solutions that will help further advance clinical practice and significantly improve patient outcomes.
Contact: Tammie Jarry45 Barbour Pond Drive Wayne, NJ 07470Tel: (650) [email protected]
MARVAO MEDICAL DEVICES LIMITEDMarvao Medical Devices is introducing the FDA-cleared NexSite Tunnelled Dialysis Catheter featuring the NexSite DISC (Dermal Ingrowth Support Collar). The NexSite DISC includes a polyester tissue ingrowth scaffold that is placed under the skin and is aligned with the long polyester cuff on the catheter shaft which is placed through the skin. The combination of the polyester DISC and catheter cuff facilitates tissue ingrowth, which is considered important in reducing the source of extraluminal infection in patients requiring long term catheterization. Dr. John Ross of is presenting First-In-Man data on NexSite at VASA 2014.
Contact: Jonathan Bouchier-HayesDirector of Business DevelopmentIBE at GMIT Dublin Road Galway, IrelandTel: 353 87 325 9728Jonathan.bouchier-hayes@marvaomedical.comwww.marvaomedical.com
MEDICAL COMPONENTSMedcomp® is the premier developer, manufacturer and supporter of cutting-edge vascular access devices that meet and exceed the clinical demands of today’s medical specialties, particularly in the fields of interventional medicine and dialysis.
In everything we do, from research and development to manufacture, packaging, delivery and support, our first consideration is the patient. By continually improving on existing technology, Medcomp is able to provide a catheter to suit every medical requirement while also considering the patient’s comfort. Patients, physicians and nurses can rely on a Medcomp device to do its job.
Contact: Karen Bacher1499 Delp DriveHarleysville, PA 19438Tel: (215) [email protected] www.medcompnet.com

814th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
MEDISTIMMedistim offers validated technologies that reduce post-CABG MACCE. The VeriQ C™ provides a novel combination of our proven transit time flow assessment along with a 15 MHz ultrasound probe, specifically designed for epiaortic and epicardial imaging.
Contact: Keely Cogswell14000 25th Ave N. Ste. 108Plymouth, MN 55447Tel: (763) 208-9852 [email protected]
TRANSONIC For clinicians, researchers and specialty solution developers seeking quantitative data to improve their outcomes and results, Transonic provides those measurement solutions. For three decades, the unprecedented resolutions of Transonic measurements has made the Transonic name synonymous with gold standard diagnostic and research measurement tools.
Contact: Miriam Tenorio34 Dutch Mill RoadIthaca, NY 14850Tel: (607) 257-5300 [email protected]
VASCULAR FLOW TECHNOLOGIES Vascular Flow Technologies is focused on the research, development and commercialisation of vascular devices based on a new understanding of blood flow dynamics – Spiral Laminar Flow (SLF technology). The technology is currently applied to two synthetic grafts, SLF PV graft and SLF AV graft. Vascular Flow grafts are the only grafts proven
to induce Spiral Laminar Flow, the body’s natural blood flow pattern, improving graft patency and helping to prevent disease progression.
Contact: Peter Fox Prospect Business CentreGemini Crescent Dundee, DD2 1TY UKTel: (602) [email protected]
VITAL ACCESS CORPORATION Vital Access designs and manufactures surgical and interventional technologies to improve vascular access for patients and their caregivers. Vascular access challenges have driven the company to develop the VWING Vascular Needle Guide, which is currently approved for use in markets such as the United States, Canada, Europe and New Zealand.Vital Access and its employees are committed to quality and improving patient care. Our focus is developing solutions for access surgeons, clinicians and patients.
Contact: Emmy Kermott 2302 S Presidents Drive Suite C Salt Lake City, UT 84120Tel: (801) 433-9390 [email protected]

914th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
SCHEDULE AT-A-GLANCE
7:00 AM - 8:00 AM Continental Breakfast with Exhibitors (Texas A)
8:00 AM - 8:05 AM Introduction from Program Directors (Texas C) Theodore F. Saad, MD; John E. Aruny, MD; Lynda K. Ball, MSN, RN, CNN; David L. Cull, MD, FACS; Charmaine Lok, MD
8:05 AM - 8:15 AM President’s Address (Texas C) Thomas M. Vesely, MD, President of VASA
8:15 AM - 8:25 AM VASA 10th Anniversary (Texas C) Fred Schild, MD
8:25 AM - 9:05 AM Faculty Presentations: ARTERIOVENOUS FISTULAE (Texas C)Fistula “Balloon Maturation”: Facts & Fiction: Theodore F. Saad, MD
Prevention of Needle-Site Aneurysms: Lynda K. Ball, MSN, RN, CNN
Aneurysmorrhaphy: Surendra Shenoy, MD
9:05 AM - 9:45 AM Faculty Presentations: STENTS (Texas A)Update on Stent-Graft Trials: RENOVA, REVISE, RESCUE: John Aruny, MD
Stents for AV Fistulae: Past, Present, & Future: Timothy Clark, MD
Stents or Stent-Grafts for Central Vein Disease: Dirk Hentschel, MD
9:45 AM - 10:15 AM Morning Break (Texas A)
10:15 AM - 11:45 AM Abstracts (#1-10) (Texas C)
11:45 AM - 12:00 PM Vascular Access in the UK: Focus on Quality and Outcomes (Texas C) Eric Chemla, MD
12:00 PM - 1:00 PM Lunch (Texas A)
12:00 PM - 1:00 PM Satellite Symposium (San Antonio 4-6) Presented by Gore and Associates
1:00 PM - 1:40 PM Faculty Presentations: ARTERIOVENOUS GRAFTS (Texas C)Mythbuster Part-1: Are Grafts as “Bad” as We Think?: David Cull, MD
Synthetic & Biological Grafts: What’s New?: Eric Peden, MDThe Science of Vascular Access: New Frontiers: Nicholas Inston, MD, PhD
1:40 PM - 2:20 PM Faculty Presentations: CARDIAC ISSUES IN AV ACCESS (Texas C)Radial Artery Cardiac Catheterization: Jeffrey Schussler, MD, FACC, FSCAI
CHF & Pulmonary Hypertension Associated with AV Hemodialysis Access: Jan Malik, MD
Cardiovascular Implantable Electronic Devices & Hemodialysis Access: Haimanot Wasse, MD
2:20 PM - 2:30 PM Dialysis & Vascular Access in Colombia: Lessons for the USA (Texas C) Jaime Velez, MD
2:30 PM - 3:00 PM Afternoon Break (Texas A)
3:00 PM - 4:30 PM Abstracts (#11-20) (Texas C)
4:30 PM - 5:00 PM Video Presentations (Texas C) Suren Shenoy, MD
5:30 PM - 7:00 PM VASA Networking Reception (Texas A)
FRIDAY, MAY 2, 2014
6:00 PM – 7:30 PM Welcome Reception (Texas A)
THURSDAY, MAY 1, 2014
1014th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
SCHEDULE AT-A-GLANCE
7:00 AM - 8:00 AM Continental Breakfast with Exhibitors (Texas A)
7:00 AM - 8:00 AM Satellite Symposium (San Antonio 4-6) Presented by CR Bard
8:00 AM - 8:05 AM Introduction (Texas C) Program Committee Members
8:05 AM - 8:15 AM Nephrology Oral History Project (Texas C) Dugan Maddux, MD, FACP
8:15 AM - 8:45 AM Faculty Presentations: PERITONEAL DIALYSIS (Texas C) Patient Selection is Key to Success: Ingemar Davidson, MD
Methods of PD Catheter Insertion: Maurizio Gallieni, MD
8:45 AM - 9:25 AM Faculty Presentations: VENOUS HEMODIALYSIS CATHETERS (Texas C) Mythbuster Part 2: Are Catheters as Bad as We Think?: Charmaine Lok, MD
Catheter Designs, Materials, Coatings: What Really Matters?: Jack Work, MD
Catheter Exit-Site: The Real Achilles Heel?: Deborah J. Brouwer-Maier, RN, CNN
9:25 AM - 9:45 AM ESRD Vascular Access Services in a Risk-Driven Payment System (Texas C) Robert Provenzano, MD
9:45 AM - 10:15 AM Morning Break (Texas A)
10:15 AM - 11:45 AM Abstracts (#21-32) (Texas C)
10:15 AM - 12:00 PM Nurses & Techs Breakout Session (San Antonio 1-3)Dori Schatell, MS; Lynda Ball,MSN, RN, CNN
11:45 AM - 11:55 AM Journal Club: Important Publications in Vascular Access 2012-2014 (Texas C) Thomas Vesely, MD
12:10 AM - 1:00 PM Lunch (Texas A)
12:10 AM - 1:00 PM Business Meeting Luncheon (San Antonio 4-6)
1:00 PM - 1:05 PM Introduction of Dr. Shenoy, Incoming VASA President (Texas C)
1:05 PM - 1:20 PM Henry Lecture: Bioengineered Grafts (Texas C) Introduction: Mitchell Henry, MD Jeffrey Lawson, MD
1:20 PM - 2:50 PM Abstracts (#33-40) (Texas C)
2:50 PM - 3:10 PM Afternoon Break (Texas A)
3:10 PM - 4:10 PM Legal & Ethical Issues in Vascular Access (Texas C) Larry Scher, MD
Risk Reduction in Hemodialysis Access Surgery Practice: Lee L. Cameron, Jr, Esq
Minimizing Risk and Liability of Venous Catheter Access: Maurizio Gallieni, MD
End of Life Issues in Dialysis: Dorian Schatell, MS
Legal Cases & Considerations in Vascular Access: Larry Scher, MD
4:10 PM - 4:15 PM Conclude (Texas C)
SATURDAY, MAY 3, 2014

1114th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
SCIENTIFIC PROGRAM
THURSDAY, MAY 1, 2014 4:00 PM Registration Opens
6:00 PM - 7:30 PM Welcome Reception
FRIDAY, MAY 2, 20147:00 AM - 8: 00 AM Breakfast in Exhibit Hall
8:00 AM - 8:05 AM Introduction from Program Directors
Theodore F. Saad, MD; John E. Aruny, MD; Lynda K. Ball, MSN, RN, CNN; David L. Cull, MD, FACS; Charmaine Lok, MD
8:05 AM - 8:15 AM President’s AddressThomas M. Vesely, MD, President of VASA
8:15 AM - 8:25 AM VASA 10th Anniversary
A Frederick Schild, MD, VASA President 2004-2006, Professor of Surgery, Florida International University, Miami, FL
SESSION I: FACULTY PRESENTATIONS ARTERIOVENOUS FISTULAE
Moderators: David L. Cull, MD, FACS; Surendra Shenoy, MD, PhD; Gregg Miller, MD
8:25 AM - 8:27 AM Introduction/Oral History
8:28 AM - 8:37 AM Fistula “Balloon Maturation:” Facts & Fiction Theodore F. Saad, MD, Interventional NephrologyNewark, Delaware
8:38 AM - 8:47 AM Prevention of Needle-Site Aneurysms Lynda K. Ball, MSN, RN, CNN, Quality Improvement Director, FMQAI: ESRD Network 13, Edmond, OK
8:48 AM - 8:57 AM AneurysmorrhaphySurendra Shenoy, MD, PhD, Professor of Surgery, Washington University School of Medicine, St. Louis, MO
8:57 AM - 9:05 AM Q&A
STENTS Moderators: Gerald A. Beathard, MD, PhD, FASN;
Thomas Vesely, MD
9:05 AM - 9:07 AM Introduction/Oral History
9:08 AM - 9:17 AM Update on Stent-Graft Trials: RENOVA, REVISE, RESCUEJohn Aruny, MD, Co-Director, Vascular & Interventional Radiology, Yale University School of Medicine, New Haven, CT
9:18 AM - 9:27 AM Stents for AV Fistulae: Past, Present, & FutureTimothy Clark, MD, Associate Professor of Clinical Radiology, University of Pennsylvania School of Medicine, Philadelphia, PA
9:28 AM - 9:37 AM Stents or Stent-Grafts for Central Vein StenosisDirk Hentschel, MD, Interventional Nephrology, Brigham and Women’s Hospital, Assistant Professor of Medicine, Harvard Medical School, Cambridge, Massachusetts
9:37 AM - 9:45 AM Q&A
9:45 AM - 10:15 AM Morning Break

1214th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
SESSION I: SCIENTIFIC ABSTRACT PRESENTATIONS Moderators: John Aruny, MD; Jack Work, MD; Earl Schuman, MD 10:15 AM -10:21 AM 1.1 Forearm Basilic Vein Transposition Provides
Functional Autogenous Access after Failed Ipsilateral Proximal AV Access
Toufic Safa, MD, Surgery, St Francis Hospital, Great Neck, NY
10:24 AM -10:30 AM1.2 First Week Postoperative Flow Measurements
are Highly Predictive of Primary Patency of Radiocephalic Arteriovenous Fistulas
Eric Ladenheim, MD; Dzenan Lulic, MD; Craig Lum, MD; Nathan Chadwick—LDAC Vascular Centers, Fresno, CA
10:33 AM - 10:39 AM1.3 Description and Outcomes of a Simple
Surgical Technique for Treating Arteriovenous Fistula Pseudoaneurysms
Angela L. Gucwa, MD; Christopher G. Carsten,III, MD; David L. Cull, MD—Greenville Health System, Greenville, SC
10:42 AM - 10:48 AM1.4 The Heterotopic Transplantation of the
Shunt Vein - Maintenance of an Autologous Puncture Segment in Case of Irreversible Loss of the Ipsilateral Central Venous Drainage
Franziska Frizen, MD, Vascular Access Surgery, DKD Wiesbaden, Wiesbaden, Germany
10:51 AM - 10:57 AM1.5 Prevention and Treatment of Aneurysms of
Autogenous Dialysis Accesses Stephen L. Hill, MD, Physicians Care of Virginia,
Roanoke, VA
11:00 AM - 11:06 AM1.6 Covered Stents in the Management of
Central Venous Stenosis Marc G. Webb, MD; Katherina Savoka, GNC-BC; Tripti
Nagar—Michigan Vascular Access, Livonia, MI
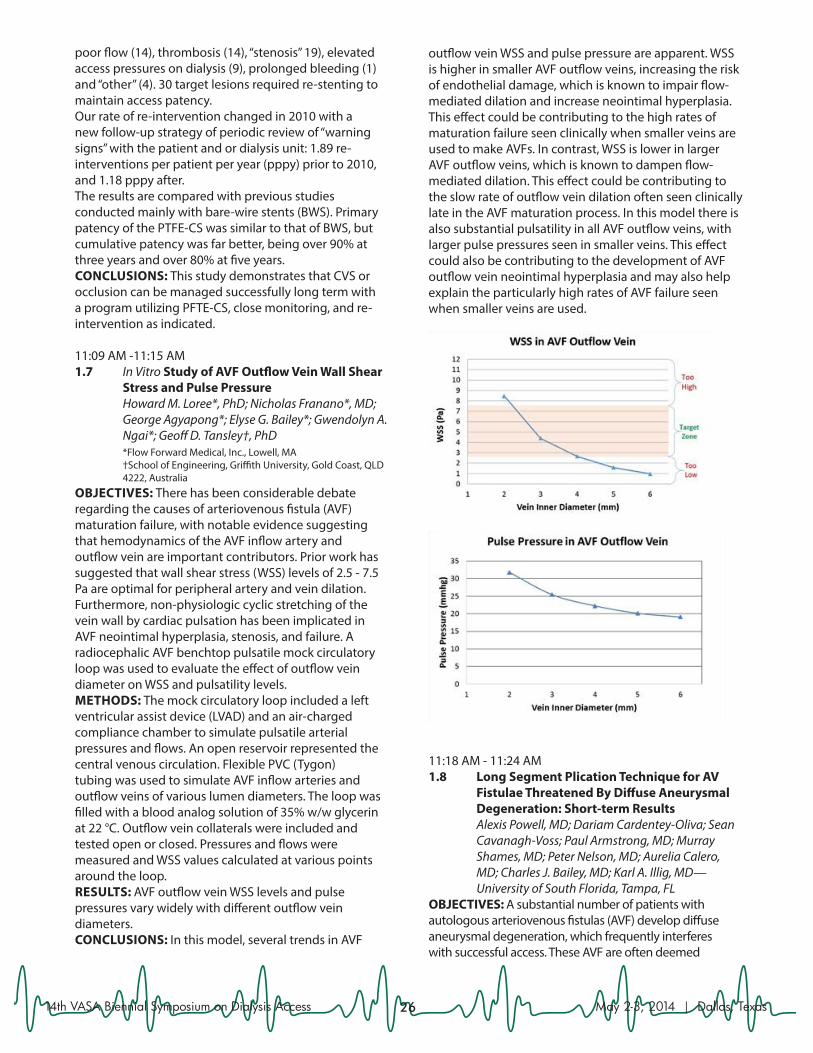
11:09 AM -11:15 AM1.7 In Vitro Study of AVF Outflow Vein Wall Shear
Stress and Pulse Pressure Howard M. Loree*, PhD; Nicholas Franano*, MD;
George Agyapong*; Elyse G. Bailey*; Gwendolyn A. Ngai*; Geoff D. Tansley†, PhD
*Flow Forward Medical, Inc., Lowell, MA †School of Engineering, Griffith University, Gold Coast, QLD
4222, Australia
11:18 AM - 11:24 AM1.8 Long Segment Plication Technique for AV
Fistulae Threatened By Diffuse Aneurysmal Degeneration: Short-term Results
Alexis Powell, MD; Dariam Cardentey-Oliva; Sean Cavanagh-Voss; Paul Armstrong, MD; Murray Shames, MD; Peter Nelson, MD; Aurelia Calero, MD; Charles J. Bailey, MD; Karl A. Illig, MD—
University of South Florida, Tampa, FL
11:27 AM - 11:33 AM1.9 Outcomes of Arteriovenous Fistula Created
Before Dialysis Start Vesna Gerasimovska , PhD; Biljana Gerasimovska-
Kitanovska, PhD; Aleksandar Sikole, PhD— Vascular Access Unit, Clinic of Nephrology, Skopje, Macedonia, The Former Yugoslav Republic
11:36 AM - 11:42 AM1.10 ‘Fistula Fast’ - Initial Experience from a New,
Rapid Access Arteriovenous Fistula Pathway Damian McGrogan; Yazin Marie; Susan Freckleton;
Helen Eddington, PhD; Clara Day; Nicholas Inston PhD—Queen Elizabeth Hospital, Birmingham, United Kingdom
11:45 AM - 11:55 AM Vascular Access in the UK, Focus on Quality and OutcomesEric Chemla, MD, Chair of the Division of Specialist Medicine & Cardiovascular Sciences, University of London, St. George’s Medical School, London, UK
11:55 AM - 12:00 PM Q&A
12:00 PM - 1:00 PM Lunch Break
1314th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
SESSION II: FACULTY PRESENTATIONS ARTERIOVENOUS GRAFTS
Moderators: Eric Chemla, MD; Jeffrey Lawson, MD, PhD
1:00 PM -1:02 PM Introduction/Oral History
1:03 PM -1:12 PM Mythbuster Part-1: Are Grafts as “Bad” as We
Think? David Cull, MD, Vice-Chair Academic Affairs, Professor of Surgery, University of So. Carolina
School of Medicine- Greenville, Greenville, SC
1:13 PM -1:22 PM Synthetic & Biological Grafts: What’s New? Eric Peden, MD, Chief of Vascular Surgery,
Methodist DeBakey Heart &Vascular Center at The Methodist Hospital, Houston, TX
1:23 PM -1:32 PM The Science of Vascular Access: New Frontiers Nicholas Inston, MD, PhD, Clinical Lead for Renal
Surgery and Transplantation, Queen Elizabeth Hospital, Birmingham, UK
1:32 PM -1:40 PM Q&A
CARDIAC ISSUES IN AV ACCESS Moderators: Theodore F. Saad, MD; Jan Malik,
MD; Marc Glickman
1:40 PM -1:42 PM Introduction/Oral History
1:43 PM -1:52 PM Radial Artery Cardiac Catheterization Jeffrey M Schussler, MD, Medical Director: CVICU
- Baylor Heart and Vascular Hospital, Professor of Medicine: Texas A&M School of Medicine, Dallas, TX
1:53 PM - 2:02 PM CHF & Pulmonary Hypertension Associated
with AV Hemodialysis Access Jan Malik, MD, Vascular Access Center, First
Faculty of Medicine, Charles University, General University Hospital, Prague, Czech Republic
2:03 PM -2:12 PM Cardiovascular Implantable Electronic
Devices & Hemodialysis Access Haimanot Wasse, MD, Associate Professor of
Medicine, Emory University School of Medicine, Atlanta, GA
2:12 PM -2:19 PM Q&A
2:20 PM - 2:30 PM Dialysis & Vascular Access in Colombia.
Lessons for the USA Jaime Velez, MD, Vascular Surgeon, Clinica Amiga,
Cali, Colombia
2:30 PM - 3:00 PM Afternoon Break
SESSION II: SCIENTIFIC ABSTRACT PRESENTATIONS Moderators: David L. Cull, MD, FACS; Haimanot Wasse, MD 3:00 PM -3:06 PM 2.1 Initial Experience on Early Cannulation Using
a New Tri-Layer Graft for Vascular Access Matteo Tozzi, MD; Gabriele Piffaretti, PhD; Marco
Franchin, MD; Gabriele Soldini, MD; Mattia Cavagna, MD; Giulio Carcano, MD—Surgical and Morphological Sciences, University of Insubria, Varese, Italy
3:09 PM - 3:15 PM2.2 An Immediate Access Dialysis Graft that
Prevents Traumatic Cannulation Related Injuries
Shawn M. Gage, PA; Roberto J. Manson, MD; Jeffrey H. Lawson, MD, PhD—Duke University Medical Center, Durham, NC
3:18 PM - 3:24 PM2.3 The Cost to Creation and Maintenance
of Functional Arteriovenous Fistulas and Financial Losses in Capitated Models
Steven Abramowitz, MD; Robert A. Lookstein, MD; Harry Schanzer, MD; Peter L. Faries, MD; Michael M. Marin, MD; Victoria J. Teodorescu, MD—Mount Sinai Medical Center, New York, NY
3:27 PM - 3:33 PM2.4 Optimal Hemodialysis Access from Start to
Finish Earl S. Schuman, MD; Amy Ronfeld, RN; Carolyn
Beall, RN—Kaiser Northwest, Portland, OR
3:36 PM - 3:42 PM2.5 Evaluation and Treatment of High Flow
Arteriovenous Fistulas after Successful Renal Transplantation
George Gkotsis*, MD; William Jennings, MD†; Alexandros Mallios* MD; Kevin Taubman*, MD
*University of Oklahoma, Tulsa, OK †St John Medical Center, Tulsa, OK
1414th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
3:45 PM - 3:51 PM2.6 AV Fistula Salvage with Novel Patch-Wrap
Technique Jose Zamora II MD FACS, Balboa Transplant
Institute, San Diego, CA
3:54 PM - 4:00 PM2.7 Use of the Artegraft in Salvage of
Arteriovenous Fistulas for Dialysis (Free) David B. Leeser*, MD; Silke Niederhaus*, MD;
Patricia Rosenberry†, RN; Eugene Schweitzer*, MD *University of Maryland Medical School, Baltimore, MD †Shore Regional Health System, Baltimore, MD
4:03 PM - 4:09 PM2.8 Ipsilateral Replacement Grafts - Using an
Early Cannulation Graft to Avoid Catheter Exposure
Marc G. Webb, MD; Ramsis Georgi—Michigan Vascular Access, Livonia, MI
4:12 PM - 4:18 PM2.9 Cost Analysis of the Creation and
Maintenance of Functional Arteriovenous Grafts for Hemodialysis
Neeraja Konuthula; Steven D. Abramowitz, MD; Harry Schanzer, MD; Peter L. Faries, MD; Michael M. Marin; Victoria J. Teodorescu, MD— Mount Sinai Medical Center, New York, NY
4:21 PM -4:27 PM2.10 Avoiding the Use of a Femoral Bridging
Hemodialysis Catheter in Selected Patients Using a Two-Stage HeRO Graft Implantation Technique
William J. Yoon, MD; David R. Lorelli, MD— Department of Surgery, Division of Vascular Surgery, St. John Hospital and Medical Center, Detroit, MI
4:30 PM -5:00 PM Video Presentations Moderator: Surendra Shenoy, MD, PhD
5:00 PM Adjourn Scientific Program
5:30 PM -7:00 PM VASA RECEPTION
SATURDAY, MAY 3, 20147:00 AM - 8: 00 AM Breakfast in Exhibit Hall
8:00 AM - 8:05 AM Introduction from Program Committee
8:05 AM - 8:15 AM Nephrology Oral History Project Dugan Maddux, MD, VP Kidney Disease Initiatives, Fresenius Medical Services, Waltham, MA
SESSION III: FACULTY PRESENTATIONS PERITONEAL DIALYSIS
Moderators: Brian LaMendola, RN, MBA; Jack Work, MD
8:15 AM - 8:17 AM Introduction/Oral History
8:19 AM - 8:28 AM Patient Selection is Key to Success Ingemar Davidson, MD, Professor of Surgery,
University of Texas - Southwestern Medical Center, Dallas, TX
8:29 AM - 8:38 AM Methods of PD Catheter Insertion Maurizio Gallieni, MD, Director, Nephrology and
Dialysis Unit, Ospedale San Carlo Borromeo, Milan, Italy
8:38 AM - 8:45 AM Q&A
VENOUS HEMODIALYSIS CATHETERS Moderators: Maurizio Gallieni, MD; Deborah
Brouwer-Maier, RN, CNN; John Ross, MD
8:45 AM - 8:47 AM Introduction/Oral History
8:48 AM - 8:57 AM Mythbuster Part 2: Are Catheters as Bad as
We Think? Charmaine Lok, MD, Assistant Professor, Faculty of
Medicine, University of Toronto, Toronto, ON, CA
8:58 AM - 9:07 AM Catheter Designs, Materials, and Coatings:
What Really Matters? Jack Work, MD, Professor of Medicine, Emeritus,
Emory University School of Medicine, Atlanta, GA
1514th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
9:08 AM - 9:17 AM Catheter Exit-Site: The Real Achilles Heel? Deborah Brouwer-Maier, RN, CNN, Director of
Dialysis Access Initiatives, FMS- Medical Office, Warrendale, PA
9:17 Am - 9:25 AM Q&A
9:25 AM - 9:40 AM ESRD Vascular Services in a Risk-Driven
Payment System Robert Provenzano, MD, Vice President Medical
Affairs, DaVita, Denver, CO
9:40 AM - 9:45 AM Q&A
9:45 AM -10:15 AM Morning Break
NURSES & TECHS BREAKOUT SESSION
10:15 AM - 10:25 AM Patient Perspectives on Vascular Access Dorian Schatell, MS, Executive Director, Medical
Education Institute, Madison, WI
10:25 AM - 11:10 AM Fatal Vascular Access Hemorrhage Lynda K. Ball, MSN, RN, CNN, Quality Improvement
Director, FMQAI: ESRD Network 13, Edmond, OK
11:10 AM - 11:30 AM Case Study on Access Hemorrhage Lynda Ball,MSN, RN, CNN
11:30 AM - 11:50 AM Speaker Panel: Q & A on Vascular Access Dori Schatell, MS; Lynda Ball,MSN, RN, CNN
SESSION III: SCIENTIFIC ABSTRACT PRESENTATIONS Moderators: Charmaine Lok, MD; Surendra Shenoy, MD, PhD, 10:15 AM - 10:21 AM3.1 Venous Outflow Stenosis: A Single Entity or
Is the Cephalic Arch Different? Andrew J. Jackson, MD; Emma L. Aitken, MD; Ram
Kasthuri, MD; David B. Kingsmore, MD— Department of Transplantation, Glasgow, United
Kingdom
10:24 AM -10:30 AM3.2 Seasonal Variability of Fistula Thrombosis in
a Temperate Climate Andrew J. Jackson, MD; Emma L. Aitken, MD,
David B. Kingsmore, MD—Department of Transplantation, Glasgow, United Kingdom
10:33 AM -10:39 AM3.3 The Role of Exogenous Nitrates in
Arteriovenous Fistula Maturation John Yerxa*; Mostafa A. Gabr†, MD; Aamna Ali*,
MD; Shawn M. Gage†; Roberto J. Manson†, MD; James C. Otto†, PhD; Jeffrey H. Lawson†, MD
*Duke University School of Medicine, Durham, NC †Duke University Department of Surgery, Durham, NC
10:42 AM - 10:48 AM3.4 Single-Site Puncture Technique for Lateral
Internal Jugular Vein Tunneled Hemodialysis Catheter Placement
Rodney S. Florek*, MD; Gabriel Rivera*, MD; Trac Le*, MD; M. Molina*, MD; Juan Gomez†, MD; Eva Wasilewska*, MD; Michael Helm*, MD
*West Jefferson Medical Center, Metairie, LA †Tulane University Medical Center, New Orleans, LA
10:51 AM - 10:57 AM3.5 Outcomes of 500 Consecutive Arteriovenous
Fistulas Performed by a Single Surgeon John F. Lucas,III, MD; Rebecca McGlawn, RN— Greenwood Leflore Hospital, Greenwood, MS
11:00 AM - 11:06 AM3.6 Novel Approach to Percutaneous
Thrombolysis in Large Caliber Clotted Vascular Access Using Ultrasound Accelerated Thrombolysis Technology
Jessica A. Zagory, MD; Paul E. Perkowski, MD; London Guidry, MD; Jon V. Schellack, MD—
Louisiana State University Health Sciences Center New Orleans, New Orleans, LA
11:09 AM - 11:15 AM3.7 Utility and Safety of Pneumatic Tourniquet
for Surgical Procedures of Hemodialysis Access Under Conscious Sedation
Shouwen Wang, MD, Surgery Center, Arizona Kidney Disease and Hypertension Center, Phoenix, AZ
11:18 AM - 11:24 AM3.8 A Randomised Controlled Trial Comparing
Continuous to Interrupted Sutures for Radiocephalic Arteriovenous Fistulae
Emma Aitken, MD; Edward Jeans, MD; David Kingsmore, MD— Western Infirmary, Glasgow, United Kingdom
1614th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
11:27 AM - 11:33 AM3.9 Outcomes of Combined Rheolytic and
Rotational Mechanical Thrombectomy for Total Venous Circuit Thrombosis in Hemodialysis Patients
Nicholas J. Petruzzi*, MD; Raphael Cohen†, MD; Mark Mantell†, MD; Timothy W. Clark†, MD
*Interventional Radiology, Hospital of the University of Pennsylvania, Philadelphia, PA
†Penn Presbyterian Medical Center, Philadelphia, PA
11:36 AM - 11:42 AM3.10 Overnight Low Dose Thrombolysis Increases
Primary Patency Rate Of Upper Extremity Dialysis Grafts in Recanalization of Proximal Subclavian Vein Occlusion
Rodney S. Florek, MD Radiology*; Juan Paredes MD, Vascular Surgery*; Gabriel Rivera MD, Nephrology†; Trac Le MD, Nephrology†; Miguel Molina MD, Nephrology†
*Lourdes Regional Medical Center, Lafayette, LA †West Jefferson Medical Center, Marrero, LA
11:45 AM -11:55 AM Journal Club: Important Publications in
Vascular Access 2012-2014 Thomas Vesely, MD, Vascular Access Center of
Frontenac Grove, St Louis, MO
12:10 PM - 1:00 PM VASA MEMBER BUSINESS LUNCH (Members Only)
1:00 PM -1:05 PM Introduction of Dr. Shenoy, Incoming
VASA President Surendra Shenoy, MD, PhD, VASA President, 2014-
2016
1:05 PM -1:20 PM Henry Lecture: Bioengineered Grafts Introduction: Mitchell Henry, MD, Chief, Division
of Transplantation Surgery, Department of Surgery, Ohio State University, Wexner Medical Center, Columbus, OH
Jeffrey Lawson, MD, PhD, Professor of Surgery, Duke University School of Medicine, Durham, NC
SESSION IV: SCIENTIFIC ABSTRACT PRESENTATIONS Moderators: Mitchell Henry, MD; Dirk Hentschel, MD
1:20 PM - 1:26 PM 4.1 The Exit Site Management Catheter - A
Retrospective Evaluation of the First in Human Use of the NexSite HD Catheter
John Ross, MD, The Regional Medical Center, Orangeburg, SC
1:29 PM - 1:35 PM4.2 Severity of Swing-Segment Stenosis
Following Stage 1 Basilic Vein Transposition Is Not Predictive of Outcome in 2-Stage Basilic Vein Transposition
Mostafa A. Gabr, MD; John Yerxa; James C. Otto, PhD; Aamna Ali, MD; Shawn M. Gage; Jeffrey H. Lawson, MD—Duke University, Durham, NC
1:38 PM - 1:44 PM4.3 Suction Lipectomy of AVF and AVG
Dramatically Reduces Central Venous Catheter Exposure
Gregg Miller*, MD; Walead Latif†, MD; Yevgeny Savransky††, MD; Elsie Koh, MD**; Dean Preddie*, MD; Aleksandr Khariton*, MD
*Fresenius Vascular Care of Brooklyn, Brooklyn, NY †Fresenius Vascular Care of Union, Union, NJ ** Fresenius Vascular Care of Woodland Park, Woodland
Park, NJ †† Fresenius Vascular Care of Bellmore, Bellmore, NY
1:47 PM - 1:53 PM4.4 Surgical Treatment of Thrombosed
Arteriovenous Fistulas and Grafts by Nephrologist
Andrey Yankovoy; Alexsandr Sinutin; Alexsandr Smoliacov; Victor Grankin; Vadim Stepanov—
Moscow Regional Clinical Institut, Moscow, Russian Federation
1:56 PM - 2:02 PM4.5 Impact of Ambulatory Dialysis Access
Center Approach to Conversion of Catheter Dependent Hemodialysis Patients to Arteriovenous Access
George Blessios, MD, Surgery, Catholic Health System, Buffalo, NY

1714th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
2:05 PM - 2:11 PM4.6 Cutting Angioplasty Balloon in Native Av
Fistulas - A Seven Year Experience Aurangzaib Khawaja; Robert Jones; Nicholas
Inston; Andrew Willis; Ian Maccafferty; Peter Riley—New Queen Elisabeth Hospital, Birmingham, United Kingdom
2:14 PM - 2:20 PM4.7 Retrograde Jugular Vein Access from the
Inside-out: A Safer New Paradigm for Obtaining First Attempt Central Venous Access Even in High Risk Patients
Lakshmikumar Pillai*, MD; Thomas Lawson*, PhD; Patrick Burt*; Anatole Besarab†, MD; Mark H. Wholey**, MD
*Vascular Access Technologies, Inc., Palo Alto, CA †Henry Ford Hospital, Detroit, MI **Pittsburgh Vascular Institute, Pittsburgh, PA
2: 23 PM - 2:29 PM4.8 Projecting Medical System Assets to Improve
Access in Rural Areas David B. Leeser*, MD; Patricia M. Rosenberry†, RN;
Silke Niederhaus*, MD; Eugene Schweitzer, MD *University of Maryland Medical School, Baltimore, MD †Shore Regional Health System, Baltimore, MD
2: 32 PM - 2:38 PM4.9 Hemodialysis Associated Left Innominate
Vein Compression Syndrome Yaxue Shi, Jiejun Cheng; Wei Liang; Meng Ye;
Yiping Zhao; Hao Zhang; Jiwei Zhang— Department of Vascular Surgery, Shanghai RenJi
Hospital, Shanghai, China
2:41 PM - 2:47 PM4.10 “TV-Contrast Dump” For Central Vein
Visualization During Peripheral Venograms Da-Hee Park; Prakrati Kumar, MD; Dirk M.
Hentschel, MD—Brigham and Women’s Hospital, Boston, MA
2:50 PM -3:10 PM Afternoon Break
LEGAL & ETHICAL ISSUES IN VASCULAR ACCESS Moderator: Larry Scher, MD
3:10 PM - 3:30 PM Risk Reduction in Hemodialysis Access
Surgery Practice Lee L. Cameron, Jr, Esq, Partner at Wilson, Elser,
Moskowitz, Edelman, & Dicker, LLP, Dallas, TX
3:30 PM -3:40 PM Minimizing Risk and Liability of Venous
Catheter Access Maurizio Gallieni, MD, Director, Nephrology and
Dialysis Unit, Ospedale San Carlo Borromeo, Milan, Italy
3:40 PM - 3:55 PM End of Life Issues in Dialysis Dorian Schatell, MS, Executive Director, Medical
Education Institute, Madison, WI
3:55 PM -4:10 PM Legal Cases & Considerations in Vascular
Access Larry Scher, MD, Professor of Clinical Surgery,
Albert Einstein College of Medicine, Bronx, NY
4:10 PM -4:15 PM SESSION ADJOURNS

1814th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
NOTES

1914th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
NOTES

2014th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
NOTES
2114th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
NOTES

2214th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
NOTES

2314th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
FRIDAY, MAY 2, 2014SESSION I: SCIENTIFIC ABSTRACT PRESENTATIONS Moderators: John Aruny, MD Jack Work, MD Earl Schuman 10:15 AM -10:21 AM 1.1 Forearm Basilic Vein Transposition Provides
Functional Autogenous Access after Failed Ipsilateral Proximal AV Access
Toufic Safa, MD, Surgery, St Francis Hospital, Great Neck, NY
OBJECTIVES: In the era of “fistula first initiative”, vascular surgeons are under increasing pressure to create functional autogenous AV fistulas for their long term hemodialysis patients. A strategy of forearm fistula first followed by a more proximal AV access is usually followed. Forearm basilic vein transposition is often underutilized but can provide an excellent alternative for autogenous access. Patients with poor superficial venous anatomy often undergo multiple failed attempts at creating a functional autogenous fistula. Many of these patients have proximal arm or thigh AV grafts placed or are dialyzed using tunneled catheters for long term access. Basilic vein transposition can provide a secondary option for access in these patients as well.This report discusses our experience with seven patients who underwent successful forearm basilic vein transposition after failure of proximal, ipsilateral AV access. Two patients had previous radiocephalic fistulas and upper arm AV grafts that failed. Three patients had antecubital primary fistulas followed by an upper arm basilic vein fistula that failed. Two patients had forearm fistulas, antecubital fistulas, and a proximal AV graft that failed as well.METHODS: All seven patients underwent successful forearm basilic vein transposition followed by a percutaneous balloon assisted maturation procedure in 3-4 weeks after the surgery. RESULTS: All patients had arms deemed not suitable for an autogenous access by other surgeons yet all developed a mature and functional forearm transposition used successfully for hemodialysis access within a 5-14 week period. CONCLUSIONS: We conclude that it is incumbent upon access surgeons to consider all options available to create a functional autogenous AV access in their patients, including those with previous failed access
procedures. Forearm basilic vein transposition is often underutilized. It can provide an excellent option for autogenous access both as a primary procedure or as a secondary procedure after failed proximal ipsilateral grafts or fistulas.
10:24 AM -10:30 AM1.2 First Week Postoperative Flow Measurements
are Highly Predictive of Primary Patency of Radiocephalic Arteriovenous Fistulas
Eric Ladenheim, MD; Dzenan Lulic, MD; Craig Lum, MD; Nathan Chadwick—LDAC Vascular Centers, Fresno, CA
OBJECTIVES: The purpose of this study was to learn what factors might predict early failure of radiocephalic arteriovenous fistulas (RCAVF). We were particularly interested in the relative predictive value of the intraoperative volume flow rate (VFR) and the VFR at the first postoperative visit. Our goal was to find factors that would help us identify patients with arteriovenous fistulas (AVFs) that would require closer follow up and/or early intervention to aid maturation.METHODS: This was a retrospective case series study of 68 patients who received RCAVFs from 2007-2013. We measured the VFR after AVF creation but before closing the surgical incision. Postoperative VFRs were measured at the first postoperative visit and then as clinically needed. All VFR measurements were performed by duplex methodology. We defined primary patency as the number of days between operation and the endpoint of thrombosis, balloon angioplasty, or surgical revision. Primary patency of AVFs was described with survival analysis using Kaplan Meier Curves. To determine the contribution of independent variables to the dependent variable of loss of primary patency, multivariate survival analysis Cox Proportional Hazard Regression was used.RESULTS: The overall primary patency of the RCAVFs was 30% at one year (Fig. 1). We found that flow on the first postoperative visit was a highly statistically significant predictor (P=0.0022) of survival (Table 1). We found intraoperative flow was not a significant predictor of primary patency (P=0.44). When patients were stratified according to whether they had at least a two-fold increase in flow from intraoperative to the first postoperative visit, we found a significant difference in their primary patency. Patients whose flow more than doubled had higher primary patency (P=.009) (Fig 2).CONCLUSION: Of all the factors we studied, the most important one was the flow on the first postoperative
ABSTRACTS

2414th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
visit. This study demonstrates that it is possible to identify patients as soon as the first postoperative visit who would benefit from early intervention or closer follow-up. This should help with reducing the use of bridging hemodialysis catheters and minimize the risks of catheter dependency. Further study is needed to establish the feasibility and safety of earlier postoperative interventions.
10:33 AM - 10:39 AM1.3 Description and Outcomes of a Simple
Surgical Technique for Treating Arteriovenous Fistula Pseudoaneurysms
Angela L. Gucwa, MD; Christopher G. Carsten,III, MD; David L. Cull, MD—Greenville Health System, Greenville, SC
OBJECTIVES: Several methods for treating AV fistula (AVF) pseudoaneurysms (PSA) are described in case reports and small case series. Surgical techniques often require placement of tunneled dialysis catheters (TDC) or use of prosthetic to repair/bypass the PSA. Series reporting outcomes for endovascular treatment of AVF PSA are conflicting with some reporting good results in selected patients and others reporting poor outcomes. A technique for treating AVF PSA is described which involves resecting the lateral/ulcerated wall of the PSA and repairing the AVF primarily. The purpose of this study is to describe the technique and its long-term outcome.METHODS: Vascular access database and medical records were reviewed to identify patients who underwent surgical management of an AVF PSA between 2001 and 2013. Endpoints included technical success, functional patency, and complications. RESULTS: During the study period, 24 surgical repairs of AVF PSA were performed in 20 patients. Indications included skin necrosis/erosion (17), pain (2), bleeding (2), limited sites for cannulation (2), and infection (1). Three procedures were emergent. Mean follow-up was 36 months. Four patients had a concomitant outflow stenosis which was treated at the time of PSA repair. Technical success was achieved in 96% (23/24) of cases. One patient required AVF ligation for infection and bleeding on postoperative day 14. One patient had perioperative bleeding requiring return to the operating room. One patient had perioperative bleeding requiring readmission to the hospital. One patient had perioperative thrombosis of the fistula requiring thrombectomy and vein patch angioplasty. Seven patients required temporary placement of a TDC. The secondary patency rate at 12 months was 85%. Secondary interventions to maintain access patency were required in 10 patients, however, none occurred in the zone of the PSA repair. No late AVF failure resulted from a complication at the repair site.CONCLUSIONS: We describe a simple surgical procedure to salvage AVF with PSA including those with ulceration and infection. It avoids the need for placement of prosthetic material, does not require placement of a TDC in most cases, and obviates the disadvantages of endovascular intervention. This procedure should be considered a first-line treatment for AVF PSA.
2514th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
10:42 AM - 10:48 AM1.4 The Heterotopic Transplantation of the
Shunt Vein - Maintenance of an Autologous Puncture Segment in Case of Irreversible Loss of the Ipsilateral Central Venous Drainage
Franziska Frizen, MD, Vascular Access Surgery, DKD Wiesbaden, Wiesbaden, Germany
OBJECTIVES: In patients with loss of the centralvenous drainage by irreversible occlusion and severe swelling of the shuntarm, we explant the well developed shunt vein and transplant it to the other arm or the upper leg.METHODS: We present the cases of 9 patients, 6 women and 3 men and the follow up from 08/2005 to 11/2013. The average age was 51. Indication was the irreversible loss of the ipsilateral centralvenous outflow with monstrous edema of the shunt arm. In one patient we transplanted the vein to the upper leg because of cava superior thrombosis. While the explanted shunt vein is established, it is possible to use the vein immediately after operation for dialyse, punctured by the surgeon itsself.RESULTS: One patient died with open vascular access. One shunt was lost by irreversible thrombosis, 7 accesses are still working.CONCLUSIONS: The hypertrophic dilated shunt vein is the main goal in vascular access surgery. The human body needs months and even years to create this biologic high quality structure. Therefore its heterotopic use in cases of orthotop irreversible loss of drainage is obvious for a longlasting vascular access plan and even without alternative.
10:51 AM - 10:57 AM1.5 Prevention and Treatment of Aneurysms of
Autogenous Dialysis Accesses Stephen L. Hill, MD, Physicians Care of Virginia,
Roanoke, VAOBJECTIVES: The increase in construction of autogenous dialysis accesses over the past decade has brought with it many improvements. There are fewer infections, increased patency, and fewer hospitalizations. However, it has also brought with it an increase in the development of aneurysmal dilatation of the native vein due to the characteristics of the vein. Previously, prosthetic grafts would develop aneurysms only due to infection or degradation of the prosthetic material. METHODS: The presence and development of aneurysmal dilatation was reviewed over an eleven year period in one surgeon’s practice. Essentially all autogenous fistulae show some component of aneurysmal dilatation, but only those aneurysmal dilatations which reached significant proportions to require evaluation (> 4 cm) were included. RESULTS: There were a total of 571 autogenous fistulae constructed over the eleven year period; 174 Cimino fistulae, 269 brachial cephalic fistulae, 36 transposition of the midforearm cephalic vein, and 92 basilic vein
transpositions. There were 22 patients with 24 (4.2%) significant aneurysms. There were three in Cimino fistulae, 16 aneurysms in 15 patients with brachial cephalic fistulae and five occurring in four patients with basilic vein transpositions. Treatment consisted of observation, ligation, interventional stent placement or dilatation and operative placement of a prosthetic interposition graft or saphenous vein graft. CONCLUSIONS: The development of significant aneurysmal dilatation in an autogenous fistula is a serious complication which frequently heralds the end of that autogenous fistula. There are ways to preserve the fistula but most are temporizing procedures which involve the use of prosthetic material negating many of the advantages of an autogenous fistula. The best treatment is proactive, control hypertension, emphasize rotation of dialysis needles, and frequent screening of fistulae looking for possible stenoses which can be dilated to slow or stop the progression of aneurysmal dilatation. It is the characteristics of native vein combined with hypertension, turbulence, stenosis and repetitive sticks which, once established, can lead to the inevitable loss of the access much in the way infections in the prosthetic grafts ultimately required a new access.
11:00 AM - 11:06 AM1.6 Covered Stents in the Management of
Central Venous Stenosis Marc G. Webb, MD; Katherina Savoka, GNC-BC; Tripti
Nagar—Michigan Vascular Access, Livonia, MIOBJECTIVES: Central venous stenosis (CVS) is a consequence of prolonged central venous catheterization, and complicates efforts to provide dialysis access, creating unacceptable manifestations of venous hypertension of the extremity and limiting hemodialysis options. Management may include “moving on” to an uninvolved extremity, repeated central venoplasty with or without stenting, abandoning hemodialysis for CAPD, and perhaps utilizing the HeRO graft catheter. Our strategy includes aggressively recanalizing central venous occlusions as possible with repeated venoplasty, and stenting as indicated.METHODS: A retrospective review of patients with CVS managed with PTFE covered stents (PTFE-CS) was conducted, with follow-up exceeding one year in every case, up to seven years. All interventions subsequent to the stent placement were entered into an online data analysis tool (Medrio, Inc) for analysis.RESULTS: 125 patients were followed over an average of 3.9 (up to seven) years. Ages ranged from 31 to 96, averaging 67 years.Indications for PTFE-CS included: (1) inability to achieve an acceptable result with venoplasty alone - elastic stenosis, persistently elevated pressures or persistent collateralization; (2) rupture with expanding hematoma; (3) long segment recanalization with risk for more serious, irretrievable re-occlusion; and (4) recurrence of a CVS in less than three months.Reintervention was indicated for limb swelling (21),
2614th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
poor flow (14), thrombosis (14), “stenosis” 19), elevated access pressures on dialysis (9), prolonged bleeding (1) and “other” (4). 30 target lesions required re-stenting to maintain access patency.Our rate of re-intervention changed in 2010 with a new follow-up strategy of periodic review of “warning signs” with the patient and or dialysis unit: 1.89 re-interventions per patient per year (pppy) prior to 2010, and 1.18 pppy after.The results are compared with previous studies conducted mainly with bare-wire stents (BWS). Primary patency of the PTFE-CS was similar to that of BWS, but cumulative patency was far better, being over 90% at three years and over 80% at five years.CONCLUSIONS: This study demonstrates that CVS or occlusion can be managed successfully long term with a program utilizing PFTE-CS, close monitoring, and re-intervention as indicated.
11:09 AM -11:15 AM1.7 In Vitro Study of AVF Outflow Vein Wall Shear
Stress and Pulse Pressure Howard M. Loree*, PhD; Nicholas Franano*, MD;
George Agyapong*; Elyse G. Bailey*; Gwendolyn A. Ngai*; Geoff D. Tansley†, PhD
*Flow Forward Medical, Inc., Lowell, MA †School of Engineering, Griffith University, Gold Coast, QLD
4222, AustraliaOBJECTIVES: There has been considerable debate regarding the causes of arteriovenous fistula (AVF) maturation failure, with notable evidence suggesting that hemodynamics of the AVF inflow artery and outflow vein are important contributors. Prior work has suggested that wall shear stress (WSS) levels of 2.5 - 7.5 Pa are optimal for peripheral artery and vein dilation. Furthermore, non-physiologic cyclic stretching of the vein wall by cardiac pulsation has been implicated in AVF neointimal hyperplasia, stenosis, and failure. A radiocephalic AVF benchtop pulsatile mock circulatory loop was used to evaluate the effect of outflow vein diameter on WSS and pulsatility levels.METHODS: The mock circulatory loop included a left ventricular assist device (LVAD) and an air-chargedcompliance chamber to simulate pulsatile arterial pressures and flows. An open reservoir represented the central venous circulation. Flexible PVC (Tygon)tubing was used to simulate AVF inflow arteries and outflow veins of various lumen diameters. The loop was filled with a blood analog solution of 35% w/w glycerin at 22 °C. Outflow vein collaterals were included andtested open or closed. Pressures and flows were measured and WSS values calculated at various points around the loop.RESULTS: AVF outflow vein WSS levels and pulse pressures vary widely with different outflow vein diameters. CONCLUSIONS: In this model, several trends in AVF
outflow vein WSS and pulse pressure are apparent. WSS is higher in smaller AVF outflow veins, increasing the risk of endothelial damage, which is known to impair flow-mediated dilation and increase neointimal hyperplasia.This effect could be contributing to the high rates of maturation failure seen clinically when smaller veins are used to make AVFs. In contrast, WSS is lower in larger AVF outflow veins, which is known to dampen flow-mediated dilation. This effect could be contributing to the slow rate of outflow vein dilation often seen clinically late in the AVF maturation process. In this model there is also substantial pulsatility in all AVF outflow veins, with larger pulse pressures seen in smaller veins. This effect could also be contributing to the development of AVF outflow vein neointimal hyperplasia and may also helpexplain the particularly high rates of AVF failure seen when smaller veins are used.
11:18 AM - 11:24 AM1.8 Long Segment Plication Technique for AV
Fistulae Threatened By Diffuse Aneurysmal Degeneration: Short-term Results
Alexis Powell, MD; Dariam Cardentey-Oliva; Sean Cavanagh-Voss; Paul Armstrong, MD; Murray Shames, MD; Peter Nelson, MD; Aurelia Calero, MD; Charles J. Bailey, MD; Karl A. Illig, MD—
University of South Florida, Tampa, FLOBJECTIVES: A substantial number of patients with autologous arteriovenous fistulas (AVF) develop diffuse aneurysmal degeneration, which frequently interferes with successful access. These AVF are often deemed

2714th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
unsalvageable. We hypothesize that long segment plication in these patients can be performed safely with acceptable short-term AVF salvage rates.METHODS: We reviewed a prospectively maintained database to identify all patients with extensive AVF aneurysmal disease operated on for this problem.RESULTS: Thirty-five patients, 25 (71%) male and 10 (29%) female were operated upon between July 2012 and January 2014. AVFs included 23 (66%) brachiocephalic, 5 (14%) radiocephalic, and 7 brachiobasilic (20%) fistulae (one first stage only but in use). The cohort had one or a combination of local pain, arm edema, cannulation issue, recurrent thrombosis, dysfunctional during dialysis, or extreme tortuousity. Time range for AVF creation to consultation ranged from 3 months to 11 years.All underwent long segment plication over a 20Fr Bougie with or without segmental vein resection; 3 underwent concomitant first rib resection for costoclavicular stenosis. 21 patients had tunneled catheter placement for use while healing, while 13 were allowed segmental use of their AVF during the perioperative period (one patient was not yet on dialysis). Early in our experience AVF were left under the wound, while all but one repaired since early 2013 were left under a lateral flap.All patients were followed by clinical exam and duplex. In the 30 day postoperative period, 2 AVF (5.7%) became infected requiring excision, 2 occluded (5.7%), one day 1 and the other at 24 days out, 1 patient developed steal and required DRIL one week post operatively, and 1 patient died, unrelated to his surgery. Postoperative functional primary patency was 88% (30 of 34). Of the patients needing temporary access catheter, median time to first fistula use was 44 days. No wound or bleeding complications have occurred in repaired AVF left under skin flaps.CONCLUSIONS: In this group of patients whose access was threatened by diffuse aneurysmal degeneration, long-segment placation allowed salvage of 88% of fistulae with relatively low morbidity. Fewer complications are associated by covering the revised fistula with intact skin.
11:27 AM - 11:33 AM1.9 Outcomes of Arteriovenous Fistula Created
Before Dialysis Start Vesna Gerasimovska , PhD; Biljana Gerasimovska-
Kitanovska, PhD; Aleksandar Sikole, PhD— Vascular Access Unit, Clinic of Nephrology, Skopje, Macedonia, The Former Yugoslav Republic
OBJECTIVES: Starting renal replacement therapy with an arteriovenous fistula (AVF) increases patient survival following dialysis initiation. AVF creation should occur at least six months prior to anticipated hemodialysis (HD) initiation to allow for AVF maturation. Therefore, early creation of an AVF is strongly recommendedMethods: A 2-year single institution experience of the success rate, survival and complications of arteriovenous fistula (AVF) creation before dialysis initiation is reported.
Study cohort : all patients (pts) who underwent AVF creation before need for dialysis ( n =141, averaged age 61 year,male 76 and female 65) divided in three groups(gr) - diabetic (AVFd = 47 ), -hypertensive pts (AVFh = 49) and others (AVFo=45).RESULTS: Mean glomerul filtration rate (eGFR) at creation in AVFd group was higher (15,04 ± 4,5 ml/min vs. 13 ± 3,2 ml/min, p=0,005).Only 17 pts underwent second AVF and 4 pts had a third AVF creation (more frequently in females). During the study period, in 72% (n=101) of all pts a mature fistula was used as their first dialysis access, 16% (n=22) were still without dialysis and 12% (n=18) started HD with central venous catheters. Median time to first cannulation of AVF were: gr AVFd =203 ±114 days, gr AVFh= 197±97,5 days and AVFo=176±114 days. No significant difference was found for median time to first cannulation of AVF in different groups (p=0,29) Significant difference was found in kreatinin level when HD was stared, hematocrit and albumin level and eGFR when pts started with HD (AVFd =11,70 ± 6,05ml/min , AVFh= 7,8±3,2 ml/min and AVFo= 8,2±2,2 ml/min)(ANOVA p=0,049 ,p=0,000..).Sixty five pts were elderly >65 years (AVFd=27 ,AVFh=29 and AVFo=9)No significant difference was registered in the survival of AVF in patients with started HD in comparison to those that have not started hemodialysis, adjusted for diabetes mellitus (log-rank 0,16.)Greater hematocrit (HR,1.04;95%CI,1.01 to 1.09) and albumin level (HR,1,79;95%CI,1,37 to 2.33)showed an independent association with survival.CONCLUSIONS: In conclusion, the success rate of early AVF creation is reasonable and complications, when identified on time, can be remedied without the need for a catheter, thus ultimately maximizing the use of AVF in dialysis patients, especially diabetic.
11:36 AM - 11:42 AM1.10 ‘Fistula Fast’ - Initial Experience from a New,
Rapid Access Arteriovenous Fistula Pathway Damian McGrogan; Yazin Marie; Susan Freckleton;
Helen Eddington, PhD; Clara Day; Nicholas Inston PhD—Queen Elizabeth Hospital, Birmingham, United Kingdom
OBJECTIVES: The current pathway for patients requiring autogenous arteriovenous fistula (AVF) involves referral by nephrologist to assessment clinic to operative intervention and finally post-operative follow-up. The United Kingdom average time taken to achieve definitive AVF is over 3 months from referral. The aim of the ‘Fistula Fast’ program is to reduce delays in the pathway from referral to definitive AVF.METHODS: ‘Fistula Fast’ is a rapid vascular access clinic run by a trainee surgeon competent in vascular mapping supported by specialist AVF nurse. This clinic has 8 available patient appointments with 4 ‘on the day’ referrals from the concurrently run low clearance renal clinic.

2814th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
RESULTS: One hundred and three patients have been reviewed in the ‘Fistula Fast’ clinic between 3rd September 2013 and 21st January 2014 with 64 referred for new fistula creation. Thirty-four patients have completed the cycle from referral to post operative follow up, 7 are awaiting follow up, 12 are awaiting surgery and 11 have had their cycle interrupted due to various uncontrolled events.Comparison of the 34 ‘Fistula Fast’ patients to those patients being managed through the standard pathway (n = 46) shows a significant difference in progression from referral to review.Mean time from referral by nephrologist to vascular access assessment was shorter by 2.7 weeks (p = 0.0001), time from vascular access assessment to operative intervention shorter by 2.2 weeks (p = 0.001), time from referral by nephrologist to operative intervention shorter by 6.3 weeks (p = 0.0001) and time from operative intervention to follow-up shorter by 2.1 weeks (p = 0.0001). Cumulative time from referral to follow up was 7.7 weeks shorter (p = 0.0001). Comparison of primary function between the ‘Fistula Fast’ (62%) and standard pathways (74%) was not statistically significant (p = 0.33).CONCLUSIONS: Patients seen at ‘Fistula Fast’ clinic experience a significantly shorter pathway from referral by nephrologist to post operative follow-up than those on the standard pathway. The evidence supporting reduced mortality and morbidity of patients commencing haemodialysis on native AVF as opposed to central venous catheters supports the use of this new pathway. In addition the early review identifies AVF at risk and may allow early intervention to assist maturation.
SESSION II: SCIENTIFIC ABSTRACT PRESENTATIONS Moderators: David Cull Haimanot Wasse, MD 3:00 PM -3:06 PM 2.1 Initial Experience on Early Cannulation Using a
New Tri-Layer Graft for Vascular Access Matteo Tozzi, MD; Gabriele Piffaretti, PhD; Marco
Franchin, MD; Gabriele Soldini, MD; Mattia Cavagna, MD; Giulio Carcano, MD—Surgical and Morphological Sciences, University of Insubria, Varese, Italy
OBJECTIVES: The aim of our study is to report the early results of the use of a new tri-layer ePTFE graft for prosthetic vascular access (pVA) in patients with end-stage renal disease on hemodialysis.METHODS: Between October 2011 and October 2013, 30 patients with end-stage renal disease underwent implantation of a new ePTFE tri-layer grafts. Primary and secondary patency, complications and survival were recorded.RESULTS: We treated 30 patients; 18 (60%) were males,
mean age was 60 ± 12 years (range, 34-85). PVAs loop were as follow: radial-basilic (n = 12, 40%), brachial-basilic (n = 10, 33.3 %), radial-cephalic (n = 2, 6.7%), radial-antecubital forearm (n = 2, 6.7%), brachial-axillary (n = 1, 3.3%), and femoro-femoral (n = 3, 10.0%). The mean follow-up time was 6.3 ± 5.9 months (range, 1-24; median, 5). Mean latency between pVA implantation and cannulation was 2.4 ± 1.2 days (range, 1-15). Permanent graft failure was 0% at 24 months. Local complications included access thrombosis (n = 8, 16.6%) and skin erosion (n = 1, 3.3%): early (< 30 days) thrombosis occurred in 1 (3.3%) patient, late (> 30 days) thrombosis occurred in 4 (13.3 %) patients. Cause of late thrombosis were intimal hyperplasia at the venous outflow (n = 4, 13.3%), stenosis of the arterial anastomosis (n = 1, 3.3%) and graft thrombosis with no anastomotic defects (n = 3, 3.3%). Primary patency was 92% ± 5 and 61% ± 13 at 1 and 12 months, respectively; secondary patency was 100% and 92% ± 8 at 1 and 12 months.CONCLUSIONS: In our experience the new tri-layer graft Acuseal® (W.L Gore - Flagstaff; AZ - USA) proved to be safe and effective. Cannulation-related complications were absent and patency rates are superior if compared to the standard grafts used for vascular accesses.
3:09 PM - 3:15 PM2.2 An Immediate Access Dialysis Graft that
Prevents Traumatic Cannulation Related Injuries
Shawn M. Gage, PA; Roberto J. Manson, MD; Jeffrey H. Lawson, MD, PhD—Duke University Medical Center, Durham, NC
OBJECTIVES: Complications plague prosthetic vascular access, most commonly, thrombosis, infection, bleeding, and pseudoaneurysm formation. Patients can suffer from significant pain secondary to an expanding hematoma, and bleeding from a ruptured pseudoaneurysm or excoriated graft can lead to graft loss or rapid exsanguination and death. Hospitalization costs and cannulation related complications lead to millions in healthcare expenditures. To address this problem, we have developed a novel, immediate cannulation graft that is easily identifiable, self-sealing, and prevents posterior wall penetration. Currently, there is no FDA approved arteriovenous graft (AVG) that offers immediate access and specific protection from injury.METHODS: The study graft (SG) features a puncture resistant lateral and posterior surface, which assures access to the flow lumen without concern for posterior wall injury, hematoma, or patient harm. In bench top testing, both a study and control graft (CG) (standard ePTFE) were placed on a closed circuit pump, accessed with a standard dialysis needle, and evaluated for water leakage post cannulation and posterior wall penetration. The two grafts were then compared in a porcine model. Over the course of 2 weeks, both grafts were accessed 60 times per site, equivalent to 5 months of regular dialysis.RESULTS: The needle easily penetrated the anterior and

2914th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
posterior walls of the CG resulting in unceasing water spray from both puncture sites. The SG resisted posterior wall puncture, as the anterior wall exhibited miniscule water droplets that ceased quickly. The animal model highlighted the features of the SG by resisting posterior wall puncture, hematoma formation, and hemorrhage. Conversely, the CG sustained significant posterior wall injury, developed large hematomas, with rapid blood loss. SG hemostasis times were on the order of 15 times less than the CG with no application of pressure.CONCLUSIONS: SG performance was superior to that of the control in all areas tested. The SG design would mitigate several clinical failures of vascular access grafts such as: immediate cannulation, technician cannulation errors, graft degeneration, bleeding, and infection. The economic implications include the reduction of access related health care costs and facilitation of home hemodialysis.
3:18 PM - 3:24 PM2.3 The Cost to Creation and Maintenance
of Functional Arteriovenous Fistulas and Financial Losses in Capitated Models
Steven Abramowitz, MD; Robert A. Lookstein, MD; Harry Schanzer, MD; Peter L. Faries, MD; Michael M. Marin, MD; Victoria J. Teodorescu, MD—Mount Sinai Medical Center, New York, NY
OBJECTIVES: The Affordable Care Act encourages Accountable Care Organization (ACO) and capitated payment models. We sought to explore the economic impact of multi-institution hemodialysis access care.METHODS: A retrospective analysis of a prospectively-maintained database identified 300 patients who underwent access creation at our institution with two years of documented functional patency. Medical records were reviewed for central venous catheter events and access-related diagnostic imaging and procedures. Provider documentation of or radiographic evidence of interval events by outside care providers was also recorded. Current Procedural Terminology® codes were used to calculate the unadjusted Medicare, or “national average,” reimbursement in 2013 US dollars for these events as outpatient hospital encounters.RESULTS: Statistically significant differences in cost based on gender and age are identified in Table 1. 324 (97 outside institution) and 432 (136 outside intuition) maturation or maintenance procedures and 228 and 366 diagnostic imaging events were performed during the first and second year, respectively. 30.8% of known secondary access procedures were not performed at our institution at an estimated cost of $3,886,422, or an average redistribution of over $11,000 per patient. Patients with outside intervention had statistically significant higher number of known access-related procedures than those with single institution care (1.8 v 1.3, p = 0.03).CONCLUSION: Multi-institution hemodialysis access care may present economic challenges to ACO or capitated model cost-control measures.
3:27 PM - 3:33 PM2.4 Optimal Hemodialysis Access from Start to
Finish Earl S. Schuman, MD; Amy Ronfeld, RN; Carolyn
Beall, RN—Kaiser Northwest, Portland, OROBJECTIVE: To present an algorithm for patient centered hemodialysis access creation that improves the initial access while achieving goals for fistula prevalence and optimal access long term. METHODS: This is a retrospective review of 1812 patients. Most (1422) had access created from 2000-2010 allowing for possibility of a 3 year follow-up. This led to an algorithm that considers patient age, renal function (GFR), co-morbidities, vessel size and characteristics based on ultrasound mapping. Vessels between 2.5 and 3 mm were considered borderline Calcified arteries <3mm were avoided. GFR > 20 allowed use of vessels down to 2.5mm. GFR of 15-20 required a more conservative approach . If transposition or procedures were needed that increased maturation time, the patient’s GFR must be followed closely. When GFR is less than 15 only fistulas that will mature in less than 3months are considered. If patient’s vessels are inadequate consider placing a graft. This approach was evaluated by data from 290 prevalent patients in 2013.RESULTS: The retrospective review showed fistulas and grafts had similar functional patencies at 2 (23 vs 19%) and 3 years (14.8 vs 12.8%). Females comprised 45% of the study population yet received 60% of the grafts.Most patients in the past year initiated hemodialysis as an inpatient (53%) and most of them (60%) started with a catheter. Fistulas were used at the start of treatment in 32% and grafts in 8%.

3014th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
At the end of the year 67% were using fistulas for their access, 26% grafts and 7% catheters. Brachiocephalic fistulas were the predominant type. Multiple types of grafts were used. Grafts matured faster than fistulas.CONCLUSIONS: Although Fistula First encourages use of native fistulas in most patients, a fistula at all costs strategy can lead to increased catheter use, both initially and in the prevalent data. This has been shown to have deleterious consequences.. This study showed long term patencies of fistulas and grafts are similar, giving assurance that graft placement is a good choice in a patient approaching end stage disease or on dialysis with poor vessels for fistula creation. Immediate use grafts can replace catheters for dialysis initiation.An algorithm that considers a multitude of individual patient data can improve the quality of access for both the incident and prevalent populations.
3:36 PM - 3:42 PM2.5 Evaluation and Treatment of High Flow
Arteriovenous Fistulas after Successful Renal Transplantation
George Gkotsis*, MD; William Jennings, MD†; Alexandros Mallios* MD; Kevin Taubman*, MD
*University of Oklahoma, Tulsa, OK †St John Medical Center, Tulsa, OKOBJECTIVES: Observation versus ligation of a functional AVF following successful renal transplantation (SRT) has been debated. Cardiac disease including congestive heart failure and pulmonary hypertension are common in dialysis patients and more common when access flows exceed 1200-1500 ml/min. Transplant failure may occur in up to 66% of patients after 5 years, so maintaining a moderate flow AVF appears warranted. We review SRT patients with high flow AVFs where a precision inflow banding procedure was used.METHODS: Patients referred for high flow AVF evaluation post SRT were identified. In addition to physical examination, each patient had ultrasound AVF flow measurement before and after temporary AVF compression (AVF-comp) of the access by digital occlusion for 2-3 minutes. Pulse rate and the presence or absence of cardiac murmurs were noted before and after AVF-comp. Pre and post-banding flow rates were included in the analysis.RESULTS: Twelve patients were identified. Eight (66%) were male, and one (8%) obese. Ages were 15-73 years (mean=42). The AVFs were established 24-86 months previously. The mean pulse rate declined after AVF-comp from 90/min to 72/min (range 110-78). Six patients had a pre-compression cardiac systolic flow murmur that disappeared with temporary AVF-comp. One patient with poor cardiac function underwent immediate AVF ligation with dramatic improvement in cardiac status. All other patients underwent a precision banding
procedure with real-time flow monitoring. Mean access flow was 2280ml/min (range 3320-1148ml/min) before access banding and was 598 ml/min (range 876-481) after flow reduction. All AVFs remained patent although one individual later requested ligation for cosmesis. Two patients had renal transplant failure and later successfully used the AVF. Follow-up post banding was 1-18 months (mean=12).CONCLUSIONS: Hemodialysis vascular access patients with high flow AVFs had successful resolution of high cardiac output findings and maintenance of access patency using a precision banding procedure. Yearly examination of transplanted patients with access flow measurement seems warranted. Flow reduction in symptomatic patients or when AVF flow exceeds 1200-1500 ml/min is recommended. Further study is warranted to substantiate these recommendations.
3:45 PM - 3:51 PM2.6 AV Fistula Salvage with Novel Patch-Wrap
Technique Jose Zamora II MD FACS, Balboa Transplant
Institute, San Diego, CAOBJECTIVE: Aneurismal arteriovenous fistulae (AVF) develop due to causes including outflow stenoses and needle trauma. AVF dilatation can lead to high flows resulting in congestive heart failure and/or steal syndrome. A unified strategy to address these problems has not been reported. Preliminary results from our unified approach to impending AVF failure are presented.We used a 4-tiered approach to AVF salvage. 1. easing of outflow obstruction using percutaneous intervention, 2. banding excessive inflow using Transonic® flow probe (TFP) measurement, 3. novel Patch-Wrap (ZPW) using a graft to correct, strengthen, and band aneurismal portion of the AVF, and 4. place the wrapped AVF under new skin.METHODS: Outflow stenoses were radiologically found and treated. AVF flow was measured intraop using either 2-crystal or 4-crystal Confidence TFP. The aneurysmal wall of the AVF is either excised/repaired or involuted to create a size like the non-aneurismal portion of AVF. ZPW uses longitudinally cut PTFE or Artegraft® grafts to tubular or spiral wrap the AVF depending on AVF size. The wrap limits inflow for AVF’s with flow>1500cc/min or symptomatic steal. The modified AVF is repositioned under a lateral sub-Q flap for better coverage and cannulation.RESULTS: 105 procedures were performed in 81 patients since 2005; 55 used PTFE and 50 had Artegraft. Indications included aneurysmal dilatation (66), steal (13), hemorrhage (6), and central occlusion (5). 18 required multiple ZPW’s and the majority continue to function long-term.

3114th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
CONCLUSIONS: Optimizing blood flow can save centrally occluded AVF’s, correct steal, and prevent surgical intervention of cephalic arch stenoses by matching inflow and outflow. Intraoperative flow measurement by TFP aids precise banding for correction of steal and lower intra-AVF pressure. ZPW for fistula salvage is adaptable to circumstances. By keeping the patient’s blood in contact with autogenous vein wall lifespan of the conduit should be optimized. Our novel ZPW technique salvages failing AVF’s by supporting them with external graft material thereby extending the life of the AVF. This technique prevents or delays aneurismal recurrence due to persistent stenoses and ongoing needle trauma. The dysfunctional AVF is salvaged rather than replaced with graft decreasing long-term morbidity.
3:54 PM - 4:00 PM2.7 Use of the Artegraft in Salvage of
Arteriovenous Fistulas for Dialysis David B. Leeser*, MD; Silke Niederhaus*, MD;
Patricia Rosenberry†, RN; Eugene Schweitzer*, MD *University of Maryland Medical School, Baltimore, MD †Shore Regional Health System, Baltimore, MDOBJECTIVES: Patients with arteriovenous fistulas for hemodialysis can develop problems including steal, congestive heart failure (CHF), prolonged bleeding post cannulation and aneurysmal dilation. We present a series of 14 patients with fistula problems that were repaired using artegraft wraps around the fistula to decrease flow in the cases of CHF and steal, to prevent redilation of the fistula following plication or to provide a substrate around the fistula on which clot can form for hemostasis. METHODS: The charts of 14 patients who underwent revision of their fistulas were reviewed. Of the charts reviewed, 5 patients had steal, 2 CHF, 6 aneurysmal dilation and 1 patient with prolonged post cannulation bleeding without outflow obstruction. The artegraft was used as a 1cm band in the case of steal syndrome or CHF and as a complete wrap of the fistulae following plication. The degree of narrowing by the band was determined using flow probes to halve the flow combined with palpation of the radial pulse and pulse oximetry measurements of the hand. RESULTS: None of the fistulas thrombosed and all were able to continue to be used as the patients’ primary access. All cases of steal and CHF resolved following banding with artegraft. The patient with prolonged post cannulation bleeding is doing well with excellent hemostasis following dialysis. CONCLUSIONS: The artegraft provides a safe and simple biological material for revision and salvage of native arteriovenous fistulas.
4:03 PM - 4:09 PM2.8 Ipsilateral Replacement Grafts - Using an
Early Cannulation Graft to Avoid Catheter Exposure
Marc G. Webb, MD; Ramsis Georgi—Michigan Vascular Access, Livonia, MI
OBJECTIVES: Using early cannulation grafts to avoid catheter exposure has been one of the “Holy Grail” goals of access surgery, but use of these grafts has traditionally been fraught with difficulties, complications and disappointment. We report a series of 37 patients whose worn, dysfunctional or thrombosed accesses were replaced with an ipsilateral early cannulation graft with the intent to use that graft for the next dialysis session and avoid the necessity of catheter placement. METHODS: 37 patients with problem accesses and without catheters were offered this option. Accesses replaced included 25 arm grafts, 6 brachiocephalic fistulas (two previously revised with graft interpositions), four brachiobasilic transpositions, one wrist fistula and one forearm graft. One access was acutely clotted and the remainder were patent and usable but dysfunctional. In 26 (70%) patients a fistulogram or intraoperative venogram was included to define the vasculature or to optimize the venous runoff.RESULTS: 36 of 37 patients in this cohort were able to use their newly placed access on the next dialysis day and successfully avoided catheter exposure (36/37 = 97%). One patient early in the series had laceration of the graft requiring early replacement and ended up with permacath placement.Replacements used (1) old inflow and outflow sections (pure interposition), (2) a new anastomosis to the artery above, below, or at the previous anastomosis, (3) a new venous anastomosis above the previous, to a parallel vein, or end to end to the previously stented outflow, or (4) some combination.CONCLUSIONS: Although historical experience with early cannulation grafts has been uneven and disappointing for some surgeons, newer products are easier to use, and may change surgical practices. In particular, extensive revision or ipsilateral replacement of a dysfunctional access no longer requires interval exposure to a catheter during weeks of “healing” in most cases.
4:12 PM - 4:18 PM2.9 Cost Analysis of the Creation and
Maintenance of Functional Arteriovenous Grafts for Hemodialysis
Neeraja Konuthula; Steven D. Abramowitz, MD; Harry Schanzer, MD; Peter L. Faries, MD; Michael M. Marin; Victoria J. Teodorescu, MD— Mount Sinai Medical Center, New York, NY
OBJECTIVES: Creating and maintaining arteriovenous grafts for hemodialysis access is a challenge for vascular surgeons and a significant healthcare expense. We sought to capture the total patient cost of maintaining

3214th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
arteriovenous graft functional patency. To do this, we analyzed all directly related costs from creation to failure of arteriovenous grafts.METHODS: A prospectively maintained institutional database identified 218 patients who underwent arteriovenous graft placement as initial access for hemodialysis between 2007 and 2013. All patients had documented follow up at our institution from access creation to failure. Medical records were analyzed for central venous catheter events, access-related diagnostic imaging and access-related procedures including those pertaining to access maintenance and revision. Current Procedural Terminology® (CPT) codes were used to calculate the unadjusted Medicare, or “national average,” reimbursement in 2013 US dollars for these events as outpatient hospital encounters. Bivariate analysis using linear modeling and one-way analysis of variance was used to assess differences in mean cost by access anatomic location and patient demographics. RESULTS: The average cumulative cost of functionally patent arteriovenous grafts at one year was $12,685. The average creation cost of an arteriovenous graft in our study group, including pre-operative vein mapping, was $3,969. Central venous catheter costs averaged $2,471 per patient per arteriovenous graft. Functionally patent arteriovenous grafts had an average yearly non-invasive diagnostic imaging cost of $508 and an average yearly procedural cost of $5,737. If two years of functional patency was reached, the average total cost was $39,524, with $24,887 spent in the second year. The vast majority of additional cost was due to procedural expenditures.CONCLUSION: The cost of creating and maintaining arteriovenous grafts for hemodialysis include expenses related to creation and maintenance diagnostics and procedures. Understanding the true cost of hemodialysis access is an important step in working to limit healthcare expenditures.
4:21 PM -4:27 PM2.10 Avoiding the Use of a Femoral Bridging
Hemodialysis Catheter in Selected Patients Using a Two-Stage HeRO Graft Implantation Technique
William J. Yoon, MD; David R. Lorelli, MD— Department of Surgery, Division of Vascular Surgery, St. John Hospital and Medical Center, Detroit, MI
OBJECTIVE: To evaluate a novel 2-stage HeRO implantation technique that avoids the use of a femoral bridging hemodialysis (HD) catheter versus the conventional 1-stage technique requiring a bridging catheter in selected patients.METHODS: A retrospective review was performed on 20 end-stage renal disease patients with an internal jugular vein (IJV) catheter selected for 2-staged HeRO
implantation at our institution between January 2010 and March 2013. The arterial graft component (AGC) was implanted without anastomosing it to the target artery (1st stage). After AGC incorporation, the venous outflow component was inserted (2nd stage). Instead of creating a new femoral bridging catheter, the preexisting IJV catheter was maintained for HD access during the inter-stage period. Patient characteristics, patency using Kaplan-Meier method, and infection rates were analyzed.
RESULTS: A total of 17 patients completed the 2-staged procedure. The mean age was 59 years (range, 25-86 years), 12 were females (71%), 14 were African-American (82%), and 12 had diabetes (71%). The axillary artery was the most frequently used arterial anastomosis site (71%). During the inter-stage period (mean 12 weeks, range 4-22 weeks), no graft- or surgery-related infection occurred. The need of a femoral bridging catheter (published infection rate range 3.6-6.9/1,000 days) was avoided by utilizing the preexisting IJV dialysis catheter. The accumulated HeRO days was 3,916 days with a mean follow-up of 7.7 months (range 1-22.6 months). The HeRO-related infection rate was 0.3/1,000 days. The primary-assisted and secondary patency at 6-month were 69% and 82%, respectively, which were similar to those of arteriovenous grafts: 68% and 76%, respectively. Staging conferred immediate vascular accessibility.CONCLUSIONS: Avoiding the use of a femoral bridging HD catheter using the 2-stage technique may lower infection rate, with comparable primary-assisted and secondary patency to arteriovenous grafts and added benefit of immediate cannulatability in this subset of patients.
SATURDAY, MAY 3, 2014SESSION III: SCIENTIFIC ABSTRACT PRESENTATIONS Moderators: Charmaine Lok Surendra Shenoy 10:15 AM - 10:21 AM3.1 Venous Outflow Stenosis: A Single Entity or
Is the Cephalic Arch Different? Andrew J. Jackson, MD; Emma L. Aitken, MD; Ram
Kasthuri, MD; David B. Kingsmore, MD— Department of Transplantation, Glasgow, United
KingdomOBJECTIVES: Cephalic arch stenosis (CAS) is emerging as an important cause of brachiocephalic fistula (BCF) failure. The optimal management strategy for dysfunctional AVF as a result of CAS is yet to be defined. Endovascular management is generally employed as first line treatment based upon success in other venous stenosis sites. We compare the outcomes of
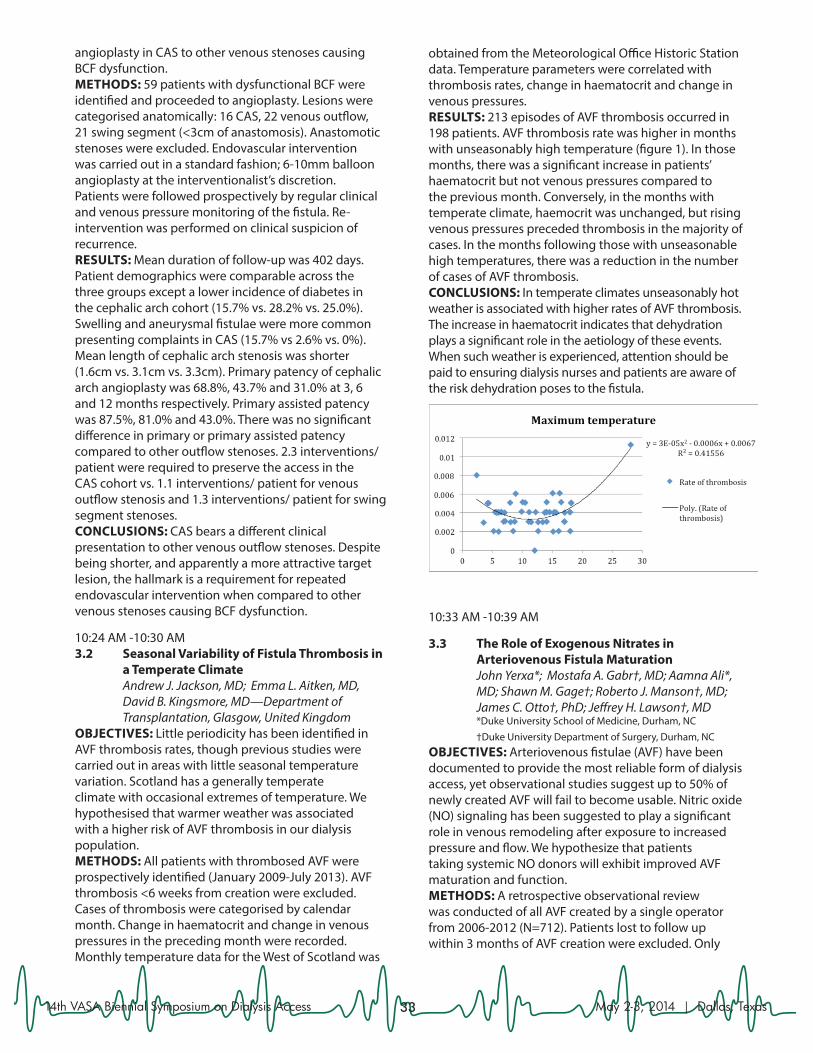
3314th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
angioplasty in CAS to other venous stenoses causing BCF dysfunction. METHODS: 59 patients with dysfunctional BCF were identified and proceeded to angioplasty. Lesions were categorised anatomically: 16 CAS, 22 venous outflow, 21 swing segment (<3cm of anastomosis). Anastomotic stenoses were excluded. Endovascular intervention was carried out in a standard fashion; 6-10mm balloon angioplasty at the interventionalist’s discretion. Patients were followed prospectively by regular clinical and venous pressure monitoring of the fistula. Re-intervention was performed on clinical suspicion of recurrence. RESULTS: Mean duration of follow-up was 402 days. Patient demographics were comparable across the three groups except a lower incidence of diabetes in the cephalic arch cohort (15.7% vs. 28.2% vs. 25.0%). Swelling and aneurysmal fistulae were more common presenting complaints in CAS (15.7% vs 2.6% vs. 0%). Mean length of cephalic arch stenosis was shorter (1.6cm vs. 3.1cm vs. 3.3cm). Primary patency of cephalic arch angioplasty was 68.8%, 43.7% and 31.0% at 3, 6 and 12 months respectively. Primary assisted patency was 87.5%, 81.0% and 43.0%. There was no significant difference in primary or primary assisted patency compared to other outflow stenoses. 2.3 interventions/ patient were required to preserve the access in the CAS cohort vs. 1.1 interventions/ patient for venous outflow stenosis and 1.3 interventions/ patient for swing segment stenoses. CONCLUSIONS: CAS bears a different clinical presentation to other venous outflow stenoses. Despite being shorter, and apparently a more attractive target lesion, the hallmark is a requirement for repeated endovascular intervention when compared to other venous stenoses causing BCF dysfunction.
10:24 AM -10:30 AM3.2 Seasonal Variability of Fistula Thrombosis in
a Temperate Climate Andrew J. Jackson, MD; Emma L. Aitken, MD,
David B. Kingsmore, MD—Department of Transplantation, Glasgow, United Kingdom
OBJECTIVES: Little periodicity has been identified in AVF thrombosis rates, though previous studies were carried out in areas with little seasonal temperature variation. Scotland has a generally temperate climate with occasional extremes of temperature. We hypothesised that warmer weather was associated with a higher risk of AVF thrombosis in our dialysis population. METHODS: All patients with thrombosed AVF were prospectively identified (January 2009-July 2013). AVF thrombosis <6 weeks from creation were excluded. Cases of thrombosis were categorised by calendar month. Change in haematocrit and change in venous pressures in the preceding month were recorded. Monthly temperature data for the West of Scotland was
obtained from the Meteorological Office Historic Station data. Temperature parameters were correlated with thrombosis rates, change in haematocrit and change in venous pressures. RESULTS: 213 episodes of AVF thrombosis occurred in 198 patients. AVF thrombosis rate was higher in months with unseasonably high temperature (figure 1). In those months, there was a significant increase in patients’ haematocrit but not venous pressures compared to the previous month. Conversely, in the months with temperate climate, haemocrit was unchanged, but rising venous pressures preceded thrombosis in the majority of cases. In the months following those with unseasonable high temperatures, there was a reduction in the number of cases of AVF thrombosis. CONCLUSIONS: In temperate climates unseasonably hot weather is associated with higher rates of AVF thrombosis. The increase in haematocrit indicates that dehydration plays a significant role in the aetiology of these events. When such weather is experienced, attention should be paid to ensuring dialysis nurses and patients are aware of the risk dehydration poses to the fistula.
10:33 AM -10:39 AM
3.3 The Role of Exogenous Nitrates in Arteriovenous Fistula Maturation
John Yerxa*; Mostafa A. Gabr†, MD; Aamna Ali*, MD; Shawn M. Gage†; Roberto J. Manson†, MD; James C. Otto†, PhD; Jeffrey H. Lawson†, MD
*Duke University School of Medicine, Durham, NC †Duke University Department of Surgery, Durham, NCOBJECTIVES: Arteriovenous fistulae (AVF) have been documented to provide the most reliable form of dialysis access, yet observational studies suggest up to 50% of newly created AVF will fail to become usable. Nitric oxide (NO) signaling has been suggested to play a significant role in venous remodeling after exposure to increased pressure and flow. We hypothesize that patients taking systemic NO donors will exhibit improved AVF maturation and function. METHODS: A retrospective observational review was conducted of all AVF created by a single operator from 2006-2012 (N=712). Patients lost to follow up within 3 months of AVF creation were excluded. Only
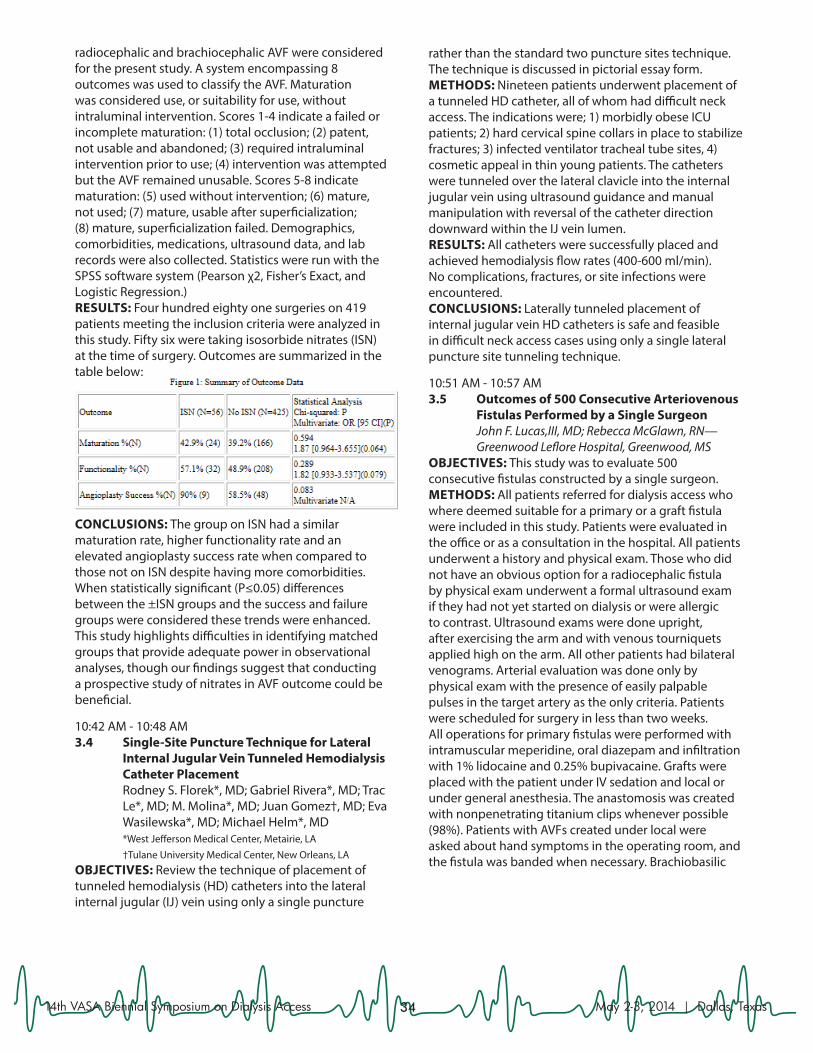
3414th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
radiocephalic and brachiocephalic AVF were considered for the present study. A system encompassing 8 outcomes was used to classify the AVF. Maturation was considered use, or suitability for use, without intraluminal intervention. Scores 1-4 indicate a failed or incomplete maturation: (1) total occlusion; (2) patent, not usable and abandoned; (3) required intraluminal intervention prior to use; (4) intervention was attempted but the AVF remained unusable. Scores 5-8 indicate maturation: (5) used without intervention; (6) mature, not used; (7) mature, usable after superficialization; (8) mature, superficialization failed. Demographics, comorbidities, medications, ultrasound data, and lab records were also collected. Statistics were run with the SPSS software system (Pearson χ2, Fisher’s Exact, and Logistic Regression.) RESULTS: Four hundred eighty one surgeries on 419 patients meeting the inclusion criteria were analyzed in this study. Fifty six were taking isosorbide nitrates (ISN) at the time of surgery. Outcomes are summarized in the table below:
CONCLUSIONS: The group on ISN had a similar maturation rate, higher functionality rate and an elevated angioplasty success rate when compared to those not on ISN despite having more comorbidities. When statistically significant (P≤0.05) differences between the ±ISN groups and the success and failure groups were considered these trends were enhanced. This study highlights difficulties in identifying matched groups that provide adequate power in observational analyses, though our findings suggest that conducting a prospective study of nitrates in AVF outcome could be beneficial.
10:42 AM - 10:48 AM3.4 Single-Site Puncture Technique for Lateral
Internal Jugular Vein Tunneled Hemodialysis Catheter Placement
Rodney S. Florek*, MD; Gabriel Rivera*, MD; Trac Le*, MD; M. Molina*, MD; Juan Gomez†, MD; Eva Wasilewska*, MD; Michael Helm*, MD
*West Jefferson Medical Center, Metairie, LA †Tulane University Medical Center, New Orleans, LAOBJECTIVES: Review the technique of placement of tunneled hemodialysis (HD) catheters into the lateral internal jugular (IJ) vein using only a single puncture
rather than the standard two puncture sites technique. The technique is discussed in pictorial essay form. METHODS: Nineteen patients underwent placement of a tunneled HD catheter, all of whom had difficult neck access. The indications were; 1) morbidly obese ICU patients; 2) hard cervical spine collars in place to stabilize fractures; 3) infected ventilator tracheal tube sites, 4) cosmetic appeal in thin young patients. The catheters were tunneled over the lateral clavicle into the internal jugular vein using ultrasound guidance and manual manipulation with reversal of the catheter direction downward within the IJ vein lumen. RESULTS: All catheters were successfully placed and achieved hemodialysis flow rates (400-600 ml/min). No complications, fractures, or site infections were encountered. CONCLUSIONS: Laterally tunneled placement of internal jugular vein HD catheters is safe and feasible in difficult neck access cases using only a single lateral puncture site tunneling technique.
10:51 AM - 10:57 AM3.5 Outcomes of 500 Consecutive Arteriovenous
Fistulas Performed by a Single Surgeon John F. Lucas,III, MD; Rebecca McGlawn, RN— Greenwood Leflore Hospital, Greenwood, MSOBJECTIVES: This study was to evaluate 500 consecutive fistulas constructed by a single surgeon.METHODS: All patients referred for dialysis access who where deemed suitable for a primary or a graft fistula were included in this study. Patients were evaluated in the office or as a consultation in the hospital. All patients underwent a history and physical exam. Those who did not have an obvious option for a radiocephalic fistula by physical exam underwent a formal ultrasound exam if they had not yet started on dialysis or were allergic to contrast. Ultrasound exams were done upright, after exercising the arm and with venous tourniquets applied high on the arm. All other patients had bilateral venograms. Arterial evaluation was done only by physical exam with the presence of easily palpable pulses in the target artery as the only criteria. Patients were scheduled for surgery in less than two weeks.All operations for primary fistulas were performed with intramuscular meperidine, oral diazepam and infiltration with 1% lidocaine and 0.25% bupivacaine. Grafts were placed with the patient under IV sedation and local or under general anesthesia. The anastomosis was created with nonpenetrating titanium clips whenever possible (98%). Patients with AVFs created under local were asked about hand symptoms in the operating room, and the fistula was banded when necessary. Brachiobasilic

3514th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
fistulas were followed with U/S at monthly intervals until the vein was 6 mm in diameter. The vein was then transposed under general anesthesia.RESULTS: 500 consecutive fistulas created between January 1, 2012 and June 30, 2013 were followed for at least 6 months. These patients had the following previous access surgery: grafts in 8%, fistulas in 38% and basilic vein transpositions in 7%. New fistulas were 91% primary, 3% prosthetic AVGs and 6% AV biografts. Two-stage basilic fistulas were done in 31%. The units where these patient dialyze have a greater than 75% primary fistula rate with 85% being catheter-free. This is better than the national average of 60% and 80%, respectively.CONCLUSIONS: Using physical exam, U/S mapping, venograms and predominantly local anesthesia, it is possible to achieve over 75% primary fistulas in a large patient population. Age, race, sex and comorbidities are unimportant compared to the quality of the target artery and vein.
11:00 AM - 11:06 AM3.6 Novel Approach to Percutaneous
Thrombolysis in Large Caliber Clotted Vascular Access Using Ultrasound Accelerated Thrombolysis Technology
Jessica A. Zagory, MD; Paul E. Perkowski, MD; London Guidry, MD; Jon V. Schellack, MD—
Louisiana State University Health Sciences Center New Orleans, New Orleans, LA
OBJECTIVES: Ultrasound accelerated thrombolysis (USAT) is a technique widely described in the treatment of deep vein thrombosis (DVT), pulmonary embolism (PE), embolic stroke, and arterial occlusions as a safe and effective technique for clot lysis by increasing the clot permeability and penetration of the thrombolytic agent into the thrombus. The risk of clot propagation into the pulmonary circulation in percutaneous declotting is a reported complication. The application of USAT in large caliber clotted AVF has yet to be reported.METHODS: Consecutive patients with thrombosis of dialysis vascular access that extended to large and/or central veins (axillary, subclavian, innominate) were chosen to undergo USAT. Patients were excluded if they had contraindications to thrombolysis.RESULTS: Six patients underwent USAT. Ages were 23 to 74 (mean 47.8), with 2 males. Time since fistula creation was 25 days to 1762 days (average 475.2). Follow up ranged from 3 to 6.5 months, with no adverse events. One patient had rethrombosis at 11 days.Adequate thrombolysis was achieved in five patients. One patient required percutaneous balloon thombectomy to resolve remaining clot in the fistula. All patients had an associated procedure (percutaneous transluminal angioplasty and/or stent placement).CONCLUSIONS: The use of USAT has already been shown to be effective and safe in large vein thrombolysis
in the setting of DVT and PE. In select patients with extensive clotting of dialysis access, the short- and long-term outcomes are favorable toward maintenance of the vascular access and may have advantages over percutaneous or open thrombectomy.
11:09 AM - 11:15 AM3.7 Utility and Safety of Pneumatic Tourniquet
for Surgical Procedures of Hemodialysis Access Under Conscious Sedation
Shouwen Wang, MD, Surgery Center, Arizona Kidney Disease and Hypertension Center, Phoenix, AZ
OBJECTIVES: Pneumatic tourniquet has been utilized in various surgical specialties to facilitate surgeries on the extremities, including surgical procedures of hemodialysis access by some surgeons. However, its use has been limited and often confined to the hospital settings under general anesthesia or regional nerve block in the United States. The objectives of this study are to demonstrate the utility and safety of pneumatic tourniquet for a variety of surgical procedures of hemodialysis access under conscious sedation and local anesthesia, and to compare the sedation requirements and procedure durations of arteriovenous fistula creations with and without tourniquet use. METHODS: The clinical data of 550 various surgical procedures of hemodialysis access performed using pneumatic tourniquet were reviewed. For comparing the sedation requirements and procedure durations with and without tourniquet use, an additional 336 cases of arteriovenous fistula creations performed without tourniquet were reviewed. A single operator performed these surgical procedures in an outpatient surgery center. To avoid ischemic pain and other potential complications, the continuous tourniquet inflation time was limited to <30 minutes. RESULTS: The pneumatic tourniquet is well tolerated under conscious sedation and no significant tourniquet-associated adverse event has been encountered during its use in 550 various surgical procedures of hemodialysis access (Table 1). Comparing arteriovenous fistula creations with and without tourniquet (377 and 336 cases respectively), the average amounts of sedation medications given are significantly less (midazolam = 2.54+1.29 mg versus 2.97+1.31 mg, p<0.001; fentanyl = 73.14+46.33 mcg versus 91.85+45.33 mcg, p<0.001). Importantly, the average procedure duration is reduced by 33% (37.2+8.6 min versus 55.8+16.5 min, p<0.001). CONCLUSIONS: Pneumatic tourniquet can be safely employed under conscious sedation in an outpatient setting. It offers many advantages: less dissection, shortened procedure duration, reduced vascular trauma and potentially improved clinical outcomes. Given these advantages, the author recommends the routine use of pneumatic tourniquet during surgical procedures of hemodialysis access in suitable patients.
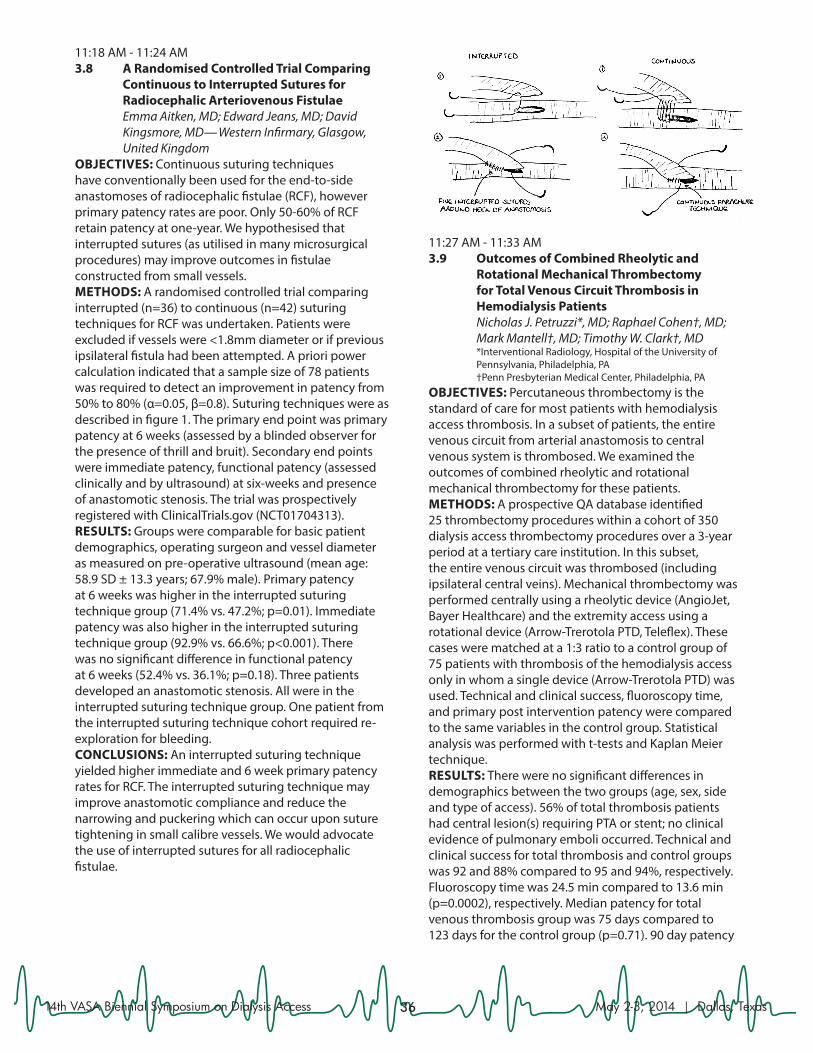
3614th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
11:18 AM - 11:24 AM3.8 A Randomised Controlled Trial Comparing
Continuous to Interrupted Sutures for Radiocephalic Arteriovenous Fistulae
Emma Aitken, MD; Edward Jeans, MD; David Kingsmore, MD— Western Infirmary, Glasgow, United Kingdom
OBJECTIVES: Continuous suturing techniques have conventionally been used for the end-to-side anastomoses of radiocephalic fistulae (RCF), however primary patency rates are poor. Only 50-60% of RCF retain patency at one-year. We hypothesised that interrupted sutures (as utilised in many microsurgical procedures) may improve outcomes in fistulae constructed from small vessels.METHODS: A randomised controlled trial comparing interrupted (n=36) to continuous (n=42) suturing techniques for RCF was undertaken. Patients were excluded if vessels were <1.8mm diameter or if previous ipsilateral fistula had been attempted. A priori power calculation indicated that a sample size of 78 patients was required to detect an improvement in patency from 50% to 80% (α=0.05, β=0.8). Suturing techniques were as described in figure 1. The primary end point was primary patency at 6 weeks (assessed by a blinded observer for the presence of thrill and bruit). Secondary end points were immediate patency, functional patency (assessed clinically and by ultrasound) at six-weeks and presence of anastomotic stenosis. The trial was prospectively registered with ClinicalTrials.gov (NCT01704313).RESULTS: Groups were comparable for basic patient demographics, operating surgeon and vessel diameter as measured on pre-operative ultrasound (mean age: 58.9 SD ± 13.3 years; 67.9% male). Primary patency at 6 weeks was higher in the interrupted suturing technique group (71.4% vs. 47.2%; p=0.01). Immediate patency was also higher in the interrupted suturing technique group (92.9% vs. 66.6%; p<0.001). There was no significant difference in functional patency at 6 weeks (52.4% vs. 36.1%; p=0.18). Three patients developed an anastomotic stenosis. All were in the interrupted suturing technique group. One patient from the interrupted suturing technique cohort required re-exploration for bleeding.CONCLUSIONS: An interrupted suturing technique yielded higher immediate and 6 week primary patency rates for RCF. The interrupted suturing technique may improve anastomotic compliance and reduce the narrowing and puckering which can occur upon suture tightening in small calibre vessels. We would advocate the use of interrupted sutures for all radiocephalic fistulae.
11:27 AM - 11:33 AM3.9 Outcomes of Combined Rheolytic and
Rotational Mechanical Thrombectomy for Total Venous Circuit Thrombosis in Hemodialysis Patients
Nicholas J. Petruzzi*, MD; Raphael Cohen†, MD; Mark Mantell†, MD; Timothy W. Clark†, MD
*Interventional Radiology, Hospital of the University of Pennsylvania, Philadelphia, PA
†Penn Presbyterian Medical Center, Philadelphia, PAOBJECTIVES: Percutaneous thrombectomy is the standard of care for most patients with hemodialysis access thrombosis. In a subset of patients, the entire venous circuit from arterial anastomosis to central venous system is thrombosed. We examined the outcomes of combined rheolytic and rotational mechanical thrombectomy for these patients.METHODS: A prospective QA database identified 25 thrombectomy procedures within a cohort of 350 dialysis access thrombectomy procedures over a 3-year period at a tertiary care institution. In this subset, the entire venous circuit was thrombosed (including ipsilateral central veins). Mechanical thrombectomy was performed centrally using a rheolytic device (AngioJet, Bayer Healthcare) and the extremity access using a rotational device (Arrow-Trerotola PTD, Teleflex). These cases were matched at a 1:3 ratio to a control group of 75 patients with thrombosis of the hemodialysis access only in whom a single device (Arrow-Trerotola PTD) was used. Technical and clinical success, fluoroscopy time, and primary post intervention patency were compared to the same variables in the control group. Statistical analysis was performed with t-tests and Kaplan Meier technique.RESULTS: There were no significant differences in demographics between the two groups (age, sex, side and type of access). 56% of total thrombosis patients had central lesion(s) requiring PTA or stent; no clinical evidence of pulmonary emboli occurred. Technical and clinical success for total thrombosis and control groups was 92 and 88% compared to 95 and 94%, respectively. Fluoroscopy time was 24.5 min compared to 13.6 min (p=0.0002), respectively. Median patency for total venous thrombosis group was 75 days compared to 123 days for the control group (p=0.71). 90 day patency
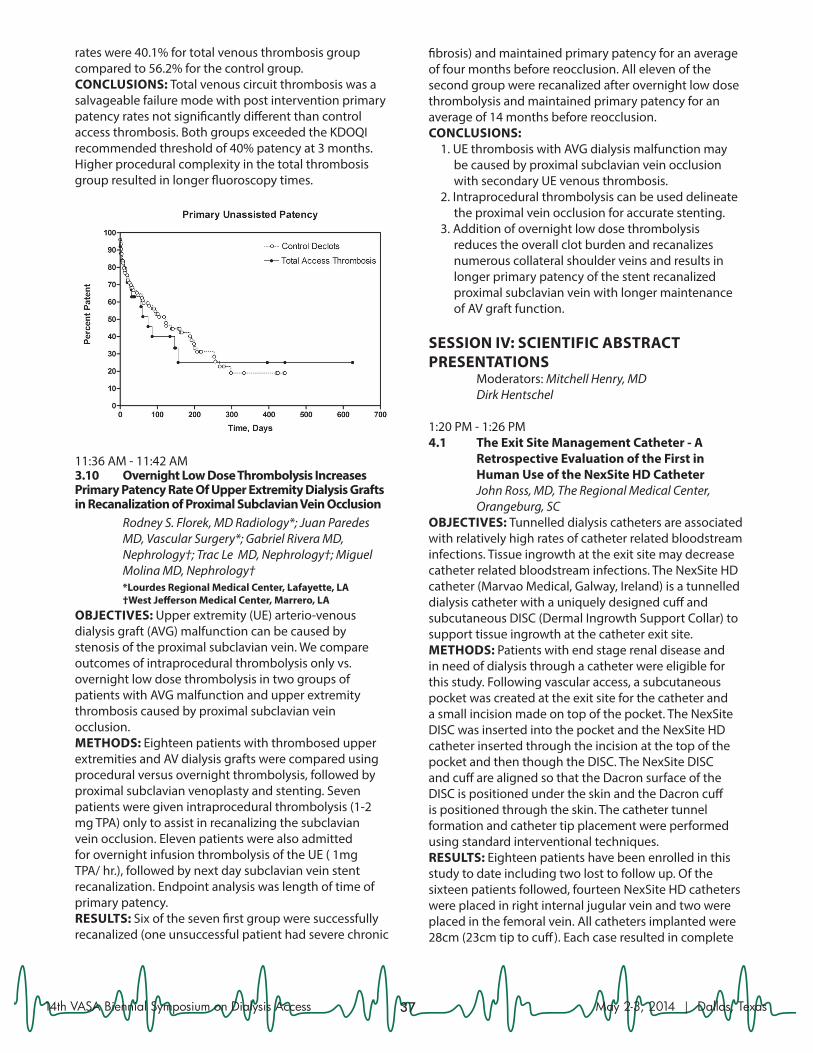
3714th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
rates were 40.1% for total venous thrombosis group compared to 56.2% for the control group.CONCLUSIONS: Total venous circuit thrombosis was a salvageable failure mode with post intervention primary patency rates not significantly different than control access thrombosis. Both groups exceeded the KDOQI recommended threshold of 40% patency at 3 months. Higher procedural complexity in the total thrombosis group resulted in longer fluoroscopy times.
11:36 AM - 11:42 AM 3.10 Overnight Low Dose Thrombolysis Increases Primary Patency Rate Of Upper Extremity Dialysis Grafts in Recanalization of Proximal Subclavian Vein Occlusion Rodney S. Florek, MD Radiology*; Juan Paredes
MD, Vascular Surgery*; Gabriel Rivera MD, Nephrology†; Trac Le MD, Nephrology†; Miguel Molina MD, Nephrology†
*Lourdes Regional Medical Center, Lafayette, LA †West Jefferson Medical Center, Marrero, LAOBJECTIVES: Upper extremity (UE) arterio-venous dialysis graft (AVG) malfunction can be caused by stenosis of the proximal subclavian vein. We compare outcomes of intraprocedural thrombolysis only vs. overnight low dose thrombolysis in two groups of patients with AVG malfunction and upper extremity thrombosis caused by proximal subclavian vein occlusion.METHODS: Eighteen patients with thrombosed upper extremities and AV dialysis grafts were compared using procedural versus overnight thrombolysis, followed by proximal subclavian venoplasty and stenting. Seven patients were given intraprocedural thrombolysis (1-2 mg TPA) only to assist in recanalizing the subclavian vein occlusion. Eleven patients were also admitted for overnight infusion thrombolysis of the UE ( 1mg TPA/ hr.), followed by next day subclavian vein stent recanalization. Endpoint analysis was length of time of primary patency.RESULTS: Six of the seven first group were successfully recanalized (one unsuccessful patient had severe chronic
fibrosis) and maintained primary patency for an average of four months before reocclusion. All eleven of the second group were recanalized after overnight low dose thrombolysis and maintained primary patency for an average of 14 months before reocclusion.CONCLUSIONS:
1. UE thrombosis with AVG dialysis malfunction may be caused by proximal subclavian vein occlusion with secondary UE venous thrombosis.
2. Intraprocedural thrombolysis can be used delineate the proximal vein occlusion for accurate stenting.
3. Addition of overnight low dose thrombolysis reduces the overall clot burden and recanalizes numerous collateral shoulder veins and results in longer primary patency of the stent recanalized proximal subclavian vein with longer maintenance of AV graft function.
SESSION IV: SCIENTIFIC ABSTRACT PRESENTATIONS Moderators: Mitchell Henry, MD Dirk Hentschel
1:20 PM - 1:26 PM 4.1 The Exit Site Management Catheter - A
Retrospective Evaluation of the First in Human Use of the NexSite HD Catheter
John Ross, MD, The Regional Medical Center, Orangeburg, SC
OBJECTIVES: Tunnelled dialysis catheters are associated with relatively high rates of catheter related bloodstream infections. Tissue ingrowth at the exit site may decrease catheter related bloodstream infections. The NexSite HD catheter (Marvao Medical, Galway, Ireland) is a tunnelled dialysis catheter with a uniquely designed cuff and subcutaneous DISC (Dermal Ingrowth Support Collar) to support tissue ingrowth at the catheter exit site.METHODS: Patients with end stage renal disease and in need of dialysis through a catheter were eligible for this study. Following vascular access, a subcutaneous pocket was created at the exit site for the catheter and a small incision made on top of the pocket. The NexSite DISC was inserted into the pocket and the NexSite HD catheter inserted through the incision at the top of the pocket and then though the DISC. The NexSite DISC and cuff are aligned so that the Dacron surface of the DISC is positioned under the skin and the Dacron cuff is positioned through the skin. The catheter tunnel formation and catheter tip placement were performed using standard interventional techniques.RESULTS: Eighteen patients have been enrolled in this study to date including two lost to follow up. Of the sixteen patients followed, fourteen NexSite HD catheters were placed in right internal jugular vein and two were placed in the femoral vein. All catheters implanted were 28cm (23cm tip to cuff). Each case resulted in complete
3814th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
healing at the exit site with 100% technical success and no adverse events. One suspected CRBSI was recorded for the first 1000 catheter days.CONCLUSIONS: The NexSite HD catheter is a feasible alternative to standard tunnelled dialysis catheters. NexSite HD is a safe and efficient method to achieve dialysis access. In this study, NexSite HD had one suspected CRBSI for the first 1000 days. Further study is warranted to determine if the use of NexSite HD catheters decreases CRBSI rates in larger patient populations.
1:29 PM - 1:35 PM4.2 Severity of Swing-Segment Stenosis
Following Stage 1 Basilic Vein Transposition is Not Predictive of Outcome in 2-Stage Basilic Vein Transposition
Mostafa A. Gabr, MD; John Yerxa; James C. Otto, PhD; Aamna Ali, MD; Shawn M. Gage; Jeffrey H. Lawson, MD—Duke University, Durham, NC
OBJECTIVES: Basilic vein transposition (BVT) has become an accepted and increasingly prevalent form of autogenous access in the upper arm. Previous studies have suggested stenosis in the swing-segment just proximal to the anastomosis is common in brachiobasilic arteriovenous fistulae (AVF) and is predictive of poor outcome. In a 2-stage BVT, stenoses in the swing-segment are excised from the AVF during transposition. We predict that this will prevent recurrence of swing segment stenosis in the region of the new anastomosis. The aim of our study is to document the incidence of proximal stenosis after stage 1 brachiobasilic arteriovenous fistula (BVT1) creation and determine its effects on second stage (BVT2) outcomes. METHODS: A retrospective observational study was conducted on all patients who had BVT created by the primary investigator from 2006-2012 (n=71). Post-
BVT1 ultrasound records were available for 34 of the 42 patients that progressed to BVT2. Severity of swing-segment stenosis was scored based on maximal peak systolic velocity (PSV) in the anastomosis and proximal third of the BVT1. Successful utilization of the BVT2 for dialysis and time of intervention free use were determined. RESULTS: 40 of 42 BVT2 were successfully used for dialysis, including 32 of the 34 included that retained ultrasound records. 28 of 34 patients (82%) exhibited a maximum swing-segment PSV >400 cm/s, considered to indicate 50% stenosis in AVF. Patients were divided into three equal groups for analysis dependent on maximum PSV: Low (n=11, range 276-464 cm/s), Moderate (n=11, range 482-614 cm/s) and High (n=12, range 646-769 cm/s). Analysis of Kaplan-Meier curves by Mantel-Cox Log Rank test indicated no significant difference in intervention free survival between the three groups at 52 (P=0.6) and 104 (P=0.5) weeks (Figure 1). CONCLUSIONS: This study demonstrates that the severity of BVT1 swing-segment stenosis does not predict BVT2 outcome. This suggests that the every effort should be made to intervene on BVT1 stenosis as early as possible, and proceed to BVT2 even if there is a high grade lesion, as exclusion of the existing stenosis and re-anastomosis with an arterialized vein segment equalizes the rate of AVF failure.
1:38 PM - 1:44 PM4.3 Suction Lipectomy of AVF and AVG
Dramatically Reduces Central Venous Catheter Exposure
Gregg Miller*, MD; Walead Latif†, MD; Yevgeny Savransky††, MD; Elsie Koh, MD**; Dean Preddie*, MD; Aleksandr Khariton*, MD
*Fresenius Vascular Care of Brooklyn, Brooklyn, NY †Fresenius Vascular Care of Union, Union, NJ ** Fresenius Vascular Care of Woodland Park, Woodland
Park, NJ †† Fresenius Vascular Care of Bellmore, Bellmore, NYOBJECTIVES: Suction Lipectomy (SL) to facilitate needle cannulation of a deep access is an infrequently utilized technique. SL efficacy has not yet been demonstrated as part of a Central Venous Catheter (CVC) avoidance strategy.

3914th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
METHODS: Retrospective analysis of thirty consecutive patients presenting with a deep uncannulatable access. The primary outcome was central venous catheter avoidance. SL catheters were purchased from Tulip Medical. A Mercedes 3mm diameter, 15cm length catheter with a SuperLuerLok hub was utilized. A 10cc syringe was used to apply suction. Reciprocating motion with concurrent rotation of the catheter was utilized. Continuous pressure was applied over the suction site to mitigate bleeding from traumatized tissue. Fatty tissue was removed from areas superficial and laterally juxtaposed in order to develop palpable margins alongside the underlying access. SL technique included: a) Ultrasound marking of the overlying skin b) infiltration of the subcutaneous tissue with 10cc of undiluted 1% lidocaine with epi c) 0.5cm incision(s) 2cm lateral and 5cm distal to the targeted area d) 20-30 catheter passes e) folded gauze for focal pressure and arm wrap for 24-48 hours with a Co-Flex bandage g) access to be cannulated in 1 week, when applicable. RESULTS: The mean age was 61 years with a mean BMI of 35.96kg/m2. Access types consisted of 22 upper arm cephalic AVF, 4 forearm AVF, 3 upper arm AVG and 1 thigh AVG. The mean pre-aspiration depth was 12.9mm (range, 9.1-22mm) and mean post-aspiration depth was 4.9mm (range, 2-8mm). Time from initial SL to successful cannulation averaged 12 days (range, 1 - 45 days). Six patients presented with no concurrent catheter. Of this subset only one required a catheter insertion, the remainder utilized the access within 24 hours following SL. Of the 24 patients who presented with a concurrent catheter, all but three catheters were removed at one month. There were no reports of access infections or skin necrosis. CONCLUSION: Using the tools and techniques described above, SL is highly efficacious. In many cases catheters were avoided and in most cases catheter removal was dramatically expedited. Suction lipectomy should be part of a CVC avoidance strategy. These are the first reported cases of AVG salvage using suction lipectomy.
1:47 PM - 1:53 PM4.4 Surgical Treatment of Thrombosed
Arteriovenous Fistulas and Grafts by Nephrologist
Andrey Yankovoy; Alexsandr Sinutin; Alexsandr Smoliacov; Victor Grankin; Vadim Stepanov—
Moscow Regional Clinical Institut, Moscow, Russian Federation
INTRODUCTION: Our clinical experience with surgical treatment of thrombosed arteriovenous (AV) fistula and grafts, performed by a nephrologist is presented. The aim of our study was to determine whether skilled nephrologist performed successful surgical treatment failure of vascular access. OBJECTIVES: Data of all patients who underwent creation of an AVF and polytetrafluoroethylen (PTEF) graft fistulas at the Moscow Regional Clinical institute from January 2002 to December 2012 were reviewed. A total of 286 surgical interventions were performed in 246 chronic hemodialysis patients aged 12-87 years (55 +/- 16 years), 268/286 (93.7%) in AV fistulas, 18/286 (6.3%) in PTEF grafts, and analyzed retrospectively. METHODS: A subgroup of 61 procedures was analyzed prospectively. The type of procedure, immediate success and patency after surgery were evaluated. RESULTS: Thrombectomy with reanastomosis was performed in 197/286 (68.9%) and simple thrombectomy in 89/286 (31.1%) of the procedures. The time from thrombosis to surgery was 1-60 days (3.7 +/- 1.8). Immediate success was achieved in 258/286 (90.2%) of surgical procedures, 95.5% (189/198) in thrombectomies with reanastomosis, and 77.5% (69/89) in simple thrombectomies. Primary and secondary patency rates for AV fistulas after surgical salvage at 3, 6, 9, and 12 months were 93.1, 84.0, 78.3, 75.0% and 96.6, 88.0, 78.3, 77.3%, respectively. In order to maintain secondary patency, 1.15 surgical procedures per AV fistula were needed. The time to thrombosis in PTEF grafts was on average 10.2 months, primary and secondary functioning time from thrombectomy (until the end of observation period) was from 1 to 19 months (average 6.9 +/- 6.3 months) and from 5.5 to 19 months (average 9.1 +/- 5.6 months), respectively. In 7/16 (43.8%) surgical procedures, transluminal angioplasty and in 3/16 endovascular stent was placed after angioplasty. To maintain secondary patency, 2.3 surgical procedures per graft were needed. CONCLUSIONS: Our results suggest that the surgical salvage of thrombosed AV fistulas and grafts, performed by a skilled nephrologist, is successful in the short and long-term.

4014th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
1:56 PM - 2:02 PM4.5 Impact of Ambulatory Dialysis Access
Center Approach to Conversion of Catheter Dependent Hemodialysis Patients to Arteriovenous Access
George Blessios, MD, Surgery, Catholic Health System, Buffalo, NY
OBJECTIVES: Hemodialysis (HD) clinical practice guidelines recommend catheter rate of less than 10% and arteriovenous fistula rate greater than 65% in all prevalent patients. Recent reports estimate 53% catheter use rate by day 91 from initiation of HD, and median time to arteriovenous (AV) access conversion longer than 91 days. The purpose of this study is to evaluate the effect of a three-step protocol based on fistula first clinical practice guidelines, implemented by a ambulatory dialysis access center (DAC), to the conversion rate from catheter to functioning AV access.METHODS: Prospective data were collected on consecutive catheter dependent HD patients referred to the DAC for conversion to AV access. DAC is an ambulatory unit able to accommodate clinic visits, surgical, interventional and hybrid procedures. Step one: initial evaluation, vein mapping and creation of AV access if possible within the same day. Step two: clinical evaluation in 2 weeks and if failure, secondary procedure to restore function. Step three: evaluation in 4 weeks after creation, and if necessary, additional procedure to promote maturation. The success rate, time to conversion and time to catheter removal were recorded.RESULTS: From the 42 referred patients, 41 underwent same day completion of step one (98%). 4 patients were excluded (2 expired and 2 refused the use of the AV access after conversion). From the 38 remaining patients, 1 arteriovenous shunt was ligated for steal syndrome (3%) and 37 patients were successfully converted to AV access (97%). 27 patients were converted to arteriovenous fistulae (73%), and 10 patients to prosthetic arteriovenous shunts (27%). The median time from creation to successful cannulation was 37 days for all converted patients. The median time for conversion to arteriovenous fistulae was 44 days and to arteriovenous shunts 28 days. The median time from AV access creation to catheter removal was 61 days. 18 patients (49%) required additional procedures for successful conversion.CONCLUSIONS: High rates of timely conversion from HD catheter to AV access can be accomplished within the context of the three-step protocol followed by a one-step ambulatory DAC. Fistula rates reached the clinical practice guidelines target.
2:05 PM - 2:11 PM4.6 Cutting Angioplasty Balloon in Native Av
Fistulas - A Seven Year Experience Aurangzaib Khawaja; Robert Jones; Nicholas
Inston; Andrew Willis; Ian Maccafferty; Peter Riley—New Queen Elisabeth Hospital, Birmingham, United Kingdom
OBJECTIVES: Native arteriovenous fistulas are prone to recurrent stenoses which owing to their elastic nature can pose an interventional challenge. Cutting balloons(CB) have been shown to be efficaciuos in managing recalcitrant lesions unresponsive to standard and high pressure balloons but have scarcely been mentioned in literature in recent years. We present a tertiary referral center‘s 7-year experience in using these devices in AV fistulas.METHODS: A retrospective review of all patients in whom a CB was used between 2007-2013. Patient and procedural demographics were recorded. Lesion characteristics and patency rates were calculated following review of surveillance venography. Complications and reason for using a CB was also recorded.RESULTS: We identified 37 patients, female to male ratio-1:1.8, mean age 67 years (SD=13), representing 14 radiocephalic, 14 brachiocephalic & 9 brachiobasilic native fistulas. Twenty patients had a CB for re-stenosis following previous intervention with a non-cutting balloon & 17 had a CB as first treatment. Mean follow-up was 19 months(range1-48months). Primary & assisted patency in the group with previous intervention at 3,6,9 & 18 months was 75%, 50%,35% &10% & 100%, 60% & 40%. Primary patency for the group with no previous intervention was 100%,65%, 59% & 29% at respective intervals & assisted patency of 70%, 70%, 50% & 50%. A sub-group of primary CB treated were identified as having remained intervention free during the follow up period(mean=20 months,SD=14, 95%CI after log transformation +/-0.61). On comparing patency with the re-stenosis CB group(mean=9, SD=11,95% CI+/-0.48), there was a statistically significant difference favouring CB as primary treatment(p<0.05). There were 2 cases of venous rupture and 10 deaths unrelated to interventions.DISCUSSION: Our experience demonstrates acceptable outcomes in the use of CB in AV access intervention & suggests that they maybe more beneficial in cases of primary intervention.

4114th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
2:14 PM - 2:20 PM4.7 Retrograde Jugular Vein Access from the
Inside-out: A Safer New Paradigm for Obtaining First Attempt Central Venous Access Even in High Risk Patients
Lakshmikumar Pillai*, MD; Thomas Lawson*, PhD; Patrick Burt*; Anatole Besarab†, MD; Mark H. Wholey**, MD
*Vascular Access Technologies, Inc., Palo Alto, CA †Henry Ford Hospital, Detroit, MI **Pittsburgh Vascular Institute, Pittsburgh, PAOBJECTIVE: Despite increasing use of ultrasound guidance during outside in internal jugular vein cannulation, serious complications continue to occur particularly in high risk patients (e.g.morbid obesity, CV occlusion, coagulopathy, ventilated critically ill, etc.).Complication rates are higher when less experienced practitioners perform the procedure and more than two access attempts are required. For the over 5 million CV access procedures performed annually, a cumulative 4% rate of serious complications (pneumo-hemothorax,arterial laceration, stroke,etc.)has been reported. A new retrograde inside out method of CV access(SAFE CVAD)has been developed that allows for safer, fluoroscopically controlled, first attempt CV access. METHODS: The device is a 100 cm long 7F catheter with a deflect-able tip through which a fine puncture wire is deployed from the inside of the vessel to the skin surface. Initially, percutaneous femoral venous access is obtained and using fluoroscopy a J wire is passed to the SVC and into the desired central vein. The device is passed over the wire and the tip is deflected under fluoroscopy and brought into contact with the anterior vein surface. The puncture wire is then deployed and recovered at the skin surface. A micro introducer is used to exchange the puncture wire for a standard wire followed by access placement. RESULTS: The SAFE CVAD has been successfully tested in sheep for both jugular and subclavian vein access from the inside out. Advancement of the device to the desired exit was achieved in 6 of 6 insertions, with the puncture wire exiting the skin sufficiently to permit CV access. Position of the puncture wire and rotation of the device tip to target the intended exit site was clear under imaging as there was one to one torque control from handle to tip. In addition, successful multiple CV exit punctures from a single femoral venous entry was possible. Bleeding at the entry and exit sites was minimal and managed with compression. CONCLUSION: The SAFE CVAD allows for safer CV access on the first attempt avoiding the serious complications that may result from repetitive attempts in high risk patients. Use of the device by less experienced practitioners may reduce complications encountered during the learning curve when compared to using the landmark technique or ultrasound guidance.
2: 23 PM - 2:29 PM4.8 Projecting Medical System Assets to Improve
Access in Rural Areas David B. Leeser*, MD; Patricia M. Rosenberry†, RN;
Silke Niederhaus*, MD; Eugene Schweitzer, MD *University of Maryland Medical School, Baltimore, MD †Shore Regional Health System, Baltimore, MDOBJECTIVES: The demand for excellent access care has become increasingly important as CMS evaluations of dialysis centers includes evaluating catheter rates. As part of a University based health system, a Dialysis Access Clinic was created in order to decrease catheter rates in a rural area surrounding one of the system hospitals. The program included hiring a full time nurse access coordinator with experience in hemodialysis and engaging University based access surgeons to provide care at the community hospital on a weekly basis. METHODS: Catheter rates and case volumes were reviewed retrospectively from the time of founding of the access center to the present. Catheter rates were collected from individual dialysis centers for the appropriate time periods. RESULTS: Case volumes at the Dialysis Access Clinic have increased from 105 cases beginning 2009 to 243 in 2013 as shown in the graph below. Catheter rates decreased from as high as 51% prior to patients being referred to the Access Clinic to rates as low as 8%. These results are detailed in the table and include two dialysis centers that began referring to the center less than one year prior to the analysis. CONCLUSIONS: We conclude that bringing University based assets to rural systems hospitals results in better access care of dialysis patients. In addition, the program has lead to local dialysis centers meeting CMS goals. This program can serve as a model of how to better serve rural patients by bringing medical center subspecialty expertise to rural systems facilities.

4214th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
2: 32 PM - 2:38 PM 4.9 Hemodialysis Associated Left Innominate Vein Compression Syndrome Yaxue Shi, Jiejun Cheng; Wei Liang; Meng Ye;
Yiping Zhao; Hao Zhang; Jiwei Zhang— Department of Vascular Surgery, Shanghai RenJi
Hospital, Shanghai, ChinaOBJECTIVES: The aim of this study was to evaluate dialysis history, clinical symptoms, imaging findings, and outcome of the management of left innominate vein (LIV) compression syndrome in hemodialysis patients.METHODS: From July 2006 to July 2013, 19 hemodialysis patients with either LIV stenosis or occlusion were treated and underwent a CT scan. The clinical data were evaluated retrospectively.RESULTS: 16 of the patients were confirmed as LIV compression syndrome by a CT scan, including 9 males and 7 females (mean age: 61.63±13.12 years old). Each of the patients had permanent vascular access without catherization history. The mean access time was 41.94±42.59 months (3-156 months); and all of the patients experienced symptoms such as arm swelling (n=16), ipsilateral face and chest swelling (n=11), visible collateral veins (n=14), arm pigmentation (n=1), and ulcerations (n=1). The mean time course for these symptoms was 4.28±5.40 months, and venography showed the following three types of LIV compression accompanied with jugular vein reflux and collaterals: Type I, flattened LIV compression section, widened superior-inferior diameter, and faded partial pacification (n=3)(Fig 1); Type II, stenotic or obstructed short segment of the LIV (Type IIa, stenosis (n=7)(Fig 2), Type IIb, obstruction (n=2)); and Type III, obstructed long segment of the LIV (n=4)(Fig 3). The CT scan showed the LIV was compressed by the aortic arch (n=10) and the left brachiocephalic artery (n=6), and aortic calcification (n=5). Patients were treated with conservative therapy (n=3), ligation (n=5), or endovascular therapy (n=8); however, the technique failed in 1 patient. With the first two patients, PTA was conducted and primary patency was found at 4 and 5 months, respectively. In the next five patients, stent placement was provided. Upon follow-up examination (mean: 17.4 months, 1-39 months), one patient died of stroke 13 months after treatment, and three patients had undergone re-intervention to resolve symptoms.CONCLUSIONS: LIV compression syndrome was the main cause of LIV stenosis, which presented clinical significance in hemodialysis patients. According to
the venography results, it could be divided into three types. MDCT was the first choice for diagnosis, and stent placement was the first choice for management.
2:41 PM - 2:47 PM4.10 “TV-Contrast Dump” For Central Vein
Visualization During Peripheral Venograms Da-Hee Park; Prakrati Kumar, MD; Dirk M.
Hentschel, MD—Brigham and Women’s Hospital, Boston, MA
OBJECTIVES: Venograms are commonly performed prior to vascular access planning. A technique to rapidly dump pooled contrast from the upper arm into the central venous circulation has been developed but its efficacy to visualize central venous patency has not been determined. This current study describes how well peripheral upper extremity venograms can perform in documenting central venous patency. METHODS: Upper extremity venograms are performed from a vein insertion site on the dorsum of the hand, and pooled contrast is dumped into the central venous circulation during digital subtraction imaging. Patency of axillary, subclavian (SCV) and brachiocephalic (BCV) veins as well as the superior vena cava (SVC) were evaluated separately for left and right arm venograms. Patency, occlusion, and image quality rated on a scale from 1 to 3 for BCV and SVC were determined, as well as the frequency of central venous stenoses. RESULTS: In 112 patients a total of 89 left and 89 right venograms were performed, 14 of the patient had not yet reached ESRD. The average contrast volume per venogram used was 30.6ml in ESRD patient, and 13.5 ml in pre-ESRD patients. In ESRD patients definitive evaluation (=patent or occluded) of axillary, subclavian and brachiocephalic

4314th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas
veins as well as superior vena cava was achieved for left sided venograms in 100% (n=81), 97.4% (n=77), 98.4% (n=65) and 58.6% (n=58), and for right sided venograms in 93.8% (n=81), 100% (n=71), 92.2% (n=64) and 75% (n=56) respectively. In pre-ESRD patient evaluation was achieved in 100% (n=8), 100% (n=8), 50% (n=6), and 66.6% (n=3) for left, and 100% (n=8), 75% (n=8), 100% (n=6), and 50% (n=6) for the right. Central vein stenoses or occlusions were identified in 20 cases, of which an access was created successfully on the ipsilateral side in 12 patients (60%) and in 8 patients on the contralateral side (40%). CONCLUSION: Our study with the use of the contrast-dumping technique peripherial venograms demonstrated direct evaluation of the subclavian and brachiocephalic veins with greater 90% certainty. The superior vena cava is more reliably evaluated on right-sided venograms. Right-sided venograms in pre-ESRD patient have similar success rates, while lefts sided venograms in pre-ESRD patients perform less well.

4414th VASA Biennial Symposium on Dialysis Access May 2-3, 2014 | Dallas, Texas