valutazione della prognosi - aiom.it · sulla variabile dipendente non è lo stesso per tutti i...
TRANSCRIPT

Valutazione della prognosi
Sono utili i test genomici?
Serena Di Cosimo Dipartimento di Ricerca Applicata e
Sviluppo Tecnologico

“Breast cancer is a systemic disease in that, tumor cells were likely to have been disseminated throughout the body by the time of diagnosis and that more expansive locoregional therapy was unlikely to improve survival”
B. Fisher
G. Bonadonna

Chemioterapia adiuvante e miglioramento della sopravvivenza
1970
1980
2000
2006
6.2%
4.1%
2.8%
4%
No CT
CMF
TAXANI
CT+Trastuzumab
ANTRACICLINE
EBCTCG 2011; EBCTCG 2012; EBCTCG 2015
EBCTCG 2011; EBCTCG 2012; EBCTCG 2015

Chemioterapia adiuvante: “overtreatment”
Paik et al, J Clin Oncol 2006
ALL BENEFIT!


Firme genomiche prognostiche disponibili
in commercio

Gluz O et al, J Clin Oncol 2016
Denckert et al, 2016

"one-size-fits-all"

Oncotype DX o “RS assay”
• 16 cancer and 5 reference genes from 3 studies:
Category RS 0-100
Low risk RS <18
Intermediate risk RS 18 to 30
High risk RS ≥ 31

Oncotype DX e prognosi delle pazienti trattate con chemioterapia e tamoxifene (NSABP B-20)
TAMOXIFEN
+ CHEMO
TAMOXIFEN
10-Year Absolute Risk BC Death (%) (95% CI) 0 5 10 15 20 25 30 35 40
Chemotherapy benefit
< 18 18-30 ≥ 31
Recurrence Score value
adapted from Paik et al, J Clin Oncol 2006

NCI Cooperative Groups TAILORx
T1-2, N0, ER positive/HER2 negative Breast Cancer
RS >25 Chemotherapy
+ Hormone Rx
21-Gene Recurrence Score Assay
Register
Specimen banking
Disegno dello studio clinico TAILORx
Recurrence Score <10 Hormone Therapy Registry
RS 11-25 Randomize
Hormone Rx vs
Chemo + Hormone Rx
n= 10273
n= 1629 (16%) n= 6711 (65%) n= 1389 (19%)
Sparano et al, N Engl J Med 2015 Sparano et al, N Engl J Med 2018

• 70% delle pazienti in menopausa
• 67% stage 1
• 93% dei casi G1-G2
Chi sono le donne con RS fino a 10?

*
*
Che prognosi hanno le donne con RS fino a 10 trattate con la terapia endocrina?

ISTITUTO NAZIONALE
PER LO STUDIO
E LA CURA DEI TUMORI


TailoRx Randomized Population
8% PgR negative
20% OA

G-low G-high
C-low 2745 (41%)
592 (8.8%)
C-high 1550
(23.2%) 1806 (27%)
MINDACT: popolazione studiata
84% delle pazienti definite a basso rischio clinico viene classificato allo stesso modo dalla firma genomica (Mammaprint).
Distribuzione delle 6693 pazienti arruolate rispetto alle classi di rischio clinico (C) e genomico (G)
Cardoso F et al, N Engl J Med 2016; 375: 717-729

Slide 32

TAILORx: primary endpoint

TAILORx: primary endpoint cont

TAILORx: exploratory analysis

Interesting Exploratory<br />Analyses<br />Randomized <br />Arms
L’interazione rappresenta l’effetto di una variabile indipendente
sulla variabile dipendente non è lo stesso per tutti i livelli delle altre
variabili indipendenti

How Does This Affect Practice Tomorrow?<br />(for node-negative patients appropriate for chemo)

Considerazioni metodologiche…
PAUL PHAROAH


Slide 27
Fatima Cardoso 2016 ASCO Annual Meeting
N=11288
N=6693

• 66% delle pazienti in menopausa
• 66% T< o = 2 cm
• 79% N0
• 80% ER pos/HER2 neg
• 71% dei casi G1-G2
Chi sono le 6693 donne del MINDACT?

G-low G-high
C-low 2745 (41%)
592 (8.8%)
C-high 1550
(23.2%) 1806 (27%)
MINDACT: popolazione studiata
Il 68% delle pazienti dello studio Mindact viene classificato allo stesso modo dai clinici (Adjuvant! Online) e dalla firma genomica (Mammaprint).
Distribuzione delle 6693 pazienti arruolate rispetto alle classi di rischio clinico (C) e genomico (G)
Cardoso F et al, N Engl J Med 2016; 375: 717-729

G-low G-high
C-low 2745 (41%)
592 (8.8%)
C-high 1550
(23.2%) 1806 (27%)
MINDACT: assegnazione del trattamento
Il 41% delle pazienti del Mindact viene assegnato d'emblée alla terapia endocrina e il 27% alla chemioterapia. 2142 (32%) pazienti vengono randomizzate
Trattamento adiuvante nelle donne classificate allo stesso modo sia dal punto di vista clinico che genomico
Cardoso F et al, N Engl J Med 2016; 375: 717-729

G-low G-high
C-low 2745 (41%)
592 (8.8%)
C-high 1550
(23.2%) 1806 (27%)
MINDACT: assegnazione del trattamento
Trattamento adiuvante nelle donne classificate C-high e G-low
Cardoso F et al, N Engl J Med 2016; 375: 717-729
1550 pazienti vengono randomizzate a essere trattate secondo la classificazione clinica (quindi a chemioterapia, n=542) oppure secondo la classificazione genomica (quindi senza chemioterapia, n=503)

MINDACT: analisi primaria
Dopo cinque anni, le donne ad alto rischio clinico e basso rischio genomico non trattate con chemioterapia adiuvante, presentano una sopravvivenza libera da metastasi del 94,7%, risultato che soddisfa l’obiettivo primario dello studio.
Ipotesi nulla DMFS del 92%
Analisi primaria su 644 pazienti
Cardoso F et al, N Engl J Med 2016; 375: 717-729

L'applicazione della firma genomica risparmierebbe la chemioterapia in 1550/3356 (46%) donne classificate come alto rischio clinico.
MINDACT: analisi terziaria
Cardoso F et al, N Engl J Med 2016; 375: 717-729

MINDACT: validità
• Validità interna= numero di errori basso
• Validità esterna= «so what?»
Lo studio Mindact confronta 2 sistemi di classificazione SENZA integrarli (score multivariati di recidiva?!)
Lo studio Mindact non ha il potere statistico per valutare il beneficio della chemioterapia nei pazienti con rischio clinico e genomico discordante (stime imprecise, CI ampli)

MINDACT: validità
• Validità interna= numero di errori basso
• Validità esterna= «so what?»
Lo studio Mindact confronta 2 sistemi di classificazione SENZA integrarli (score multivariati di recidiva?!)
Lo studio Mindact non ha il potere statistico per valutare il beneficio della chemioterapia nei pazienti con rischio clinico e genomico discordante (stime imprecise, CI ampli)

MINDACT: analisi secondaria
Le donne ad alto rischio clinico e basso rischio genomico randomizzate sulla base del rischio clinico (e quindi sottoposte a chemioterapia) hanno una sopravvivenza senza metastasi a 5 anni del 95,9%, quelle randomizzate sulla base del rischio genomico (e quindi trattate senza chemioterapia) hanno una sopravvivenza del 94,4% (p = 0,27).
Cardoso F et al, N Engl J Med 2016; 375: 717-729
C-high e G-low con chemio senza chemio
svv libera da M1 96.7%
(94.7-98) 94.8%
(92.6-96.3)
DFS 93.3%
(90.7-95.2) 90.3%
(87.6-92.4)
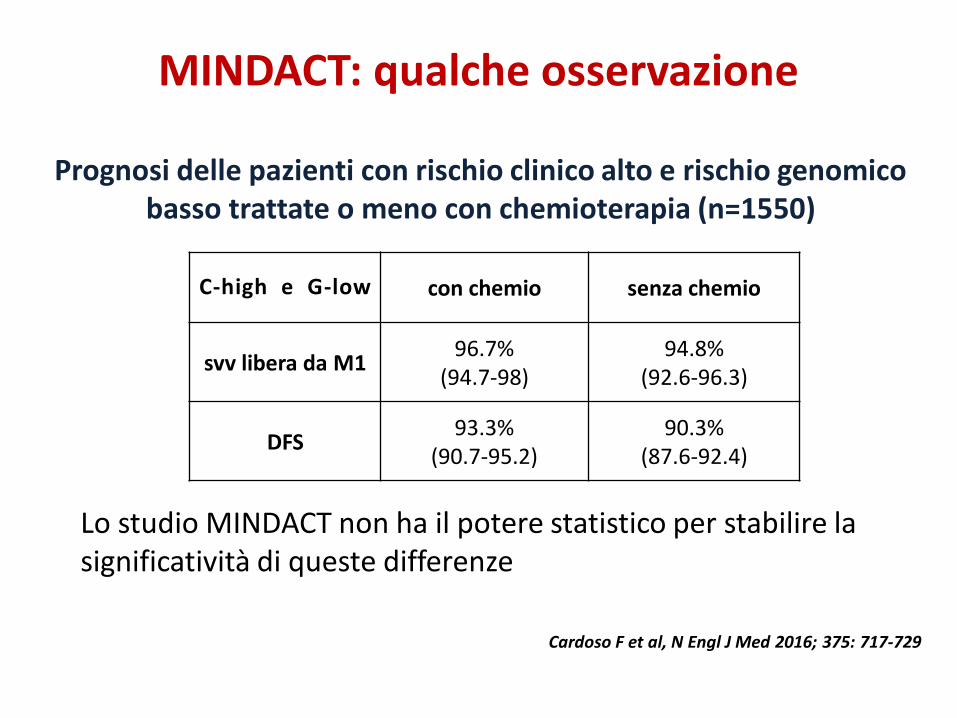
MINDACT: qualche osservazione
Lo studio MINDACT non ha il potere statistico per stabilire la significatività di queste differenze
Prognosi delle pazienti con rischio clinico alto e rischio genomico basso trattate o meno con chemioterapia (n=1550)
Cardoso F et al, N Engl J Med 2016; 375: 717-729

C-high e G-low con chemio senza chemio
svv libera da M1 96.7%
(94.7-98) 94.8%
(92.6-96.3)
DFS 93.3%
(90.7-95.2) 90.3%
(87.6-92.4)
MINDACT: qualche osservazione
p= 0.03
Prognosi delle pazienti con rischio clinico alto e rischio genomico basso trattate o meno con chemioterapia (n=1550)
Cardoso F et al, N Engl J Med 2016; 375: 717-729
Tuttavia nel gruppo trattato con chemioterapia la DFS è superiore!

C-low e G-high con chemio senza chemio
svv libera da M1 96.1%
(92.4-98.1) 93.9%
(89.6-96.5)
DFS 92.7%
(87.9-95.7) 90.5%
(85.7-93.8)
MINDACT: qualche osservazione
Lo studio MINDACT non ha il potere statistico per stabilire la significatività di queste differenze
Prognosi delle pazienti con rischio clinico basso e rischio genomico alto trattate o meno con chemioterapia (n=592)
Cardoso F et al, N Engl J Med 2016; 375: 717-729

MINDACT: validità
• Validità interna= numero di errori basso
• Validità esterna= «so what?»
Lo studio Mindact non ha il potere statistico per valutare il beneficio della chemioterapia nei pazienti con rischio clinico e genomico discordante (stime imprecise, CI ampli)
Lo studio Mindact confronta 2 sistemi di classificazione SENZA integrarli (score multivariati di recidiva?!)

con chemio senza chemio
C-high e G-low 96.7%
(94.7-98) 94.8%
(92.6-96.3)
C-low e G-high 96.1%
(92.4-98.1) 93.9%
(89.6-96.5)
...e una licenza...
Prognosi (svv libera da M1) delle pazienti con rischio genomico discordante trattate o meno con chemioterapia
Cardoso F et al, N Engl J Med 2016; 375: 717-729

con chemio senza chemio
C-high e G-low 96.7%
(94.7-98) 94.8%
(92.6-96.3)
C-low e G-high 96.1%
(92.4-98.1) 93.9%
(89.6-96.5)
In assenza di chemioterapia la prognosi delle donne G-high e G- low non sembrerebbe dissimile!!!
Prognosi (svv libera da M1) delle pazienti con rischio genomico discordante trattate o meno con chemioterapia
Cardoso F et al, N Engl J Med 2016; 375: 717-729
...e una licenza...
conclusioni
Genomic signatures have a demonstrated prognostic value but… their added value is limited to a subpart of the population
Patients with clinical low-risk disease shall not derive a substantial benefit of the use of a gene signature
Patients with low or intermediate risk signature do not derive a substantial benefit of adjuvant chemotherapy although some subgroups may…

…cosa ci aspetta..

DNA extraction
Tumor sample
DNA extraction
Validation by dPCR ctDNA dynamic profil by dPCR
Identification of somatic mutations
Plasma sample
Sequencing
Double step of centrifugation (2,000 x g for 10 min and 16,000 x g for 10 min)
At least 4x10 μm FFPE sections with >50% tumor cells
Somatic muta- tions by Ion AmpliSeq Cancer Hotspot Panel v2 (=50 genes frequently mutated in cancer) or by the Compre- hensive Cancer Panel (=409 genes) when no mutation was etected.
Workflow of the analytical procedures for ctDNA studies
ct-DNA

ctDNA detectable in plasma samples of 4/4 patients with metastasis
Dynamic profile of ctDNA in patients with DISTANT METASTASIS
ct-DNA

ctDNA detectable in plasma samples of 5/6 patients with local relapse
Dynamic profile of ctDNA in patients with LOCAL RELAPSE
ct-DNA

0
50
100
150
0.0
0.5
1.0
1.5
2.0
DF1 Primarytumor
resection
months of follow up
VA
F (
PIK
3C
A)
0
25
50
75
100
0.0
0.5
1.0
1.5
2.0
DF2 Primarytumor
resection
months of follow up
VA
F (
PT
EN
)
0
25
50
75
100
0.0
0.5
1.0
1.5
2.0
DF3 Primarytumor
resection
months of follow up
VA
F (
TP
53)
0
50
100
150
0.0
0.5
1.0
1.5
2.0
DF5 Primarytumor
resection
months of follow up
VA
F (
HN
F1A
)
0 20 40 60 80
0.0
0.5
1.0
1.5
2.0
Primarytumor
resection
DF10
months of follow up
VA
F (
PI3
KC
A)
0 50 100 150
0.0
0.5
1.0
1.5
2.0
Primarytumor
resection
DF11
months of follow up
VA
F (
PI3
KC
A)
0 50 100
0.0
0.5
1.0
1.5
2.0
Primarytumor
resection
DF14
months of follow up
VA
F (
PI3
KC
A)
0 20 40 60
0.0
0.5
1.0
1.5
2.0
Primarytumor
resection
DF16
months of follow up
VA
F (
PI3
KC
A)
0 50 100 150
0.0
0.5
1.0
1.5
2.0
Primarytumor
resection
DF19
months of follow up
VA
F (
TP
53)
0 50 100
0.0
0.5
1.0
1.5
2.0
Primarytumor
resection
DF21
months of follow up
VA
F (
PI3
KC
A)
0 20 40 60 80
0.0
0.5
1.0
1.5
2.0
Primarytumor
resection
DF23
months of follow up
VA
F (
PI3
KC
A)
0 25 50 75 100
0.0
0.5
1.0
1.5
2.0
Primarytumor
resection
DF12
months of follow up
VA
F (
PI3
KC
A)
0 50 100 150 200
0.0
0.5
1.0
1.5
2.0PTEN
PI3KCA
Primarytumor
resection
DF13
months of follow up
VA
F
0 50 100 150
0.0
0.5
1.0
1.5
2.0
Primarytumor
resection
DF22
ERBB2
TP53
months of follow up
VA
F (
ER
BB
2)
Dynamic profile of ctDNA in disease-free patients
0 50 100 150
0.0
0.5
1.0
1.5
2.0
Primarytumor
resection
DF17
PI3KCA -stop
Pi3KCA (N345K)
months of follow up
VA
F
0 50 100
0.0
0.5
1.0
1.5
2.0
Primarytumor
resection
DF24
PI3KCA
TP53
months of follow up
VA
F
ct-DNA

ringraziamenti
MG Daidone Dipartimento di Ricerca Applicata e Sviluppo Tecnologico INT - Milano S Folli S.C. Chir. Gen. Ind. Oncol. 3 (Senologia) INT- Milano G Apolone Direzione Scientifica INT - Milano L Porcu Lab. Metodologia per la Ricerca Clinica Istituto Mario Negri - Milano
GRAZIE

BACK UP

Slide 32

Slide 33

Slide 35
What about chemotherapy reduction?

Conclusions (2)

Considerations for the future
Disseminated tumor cells (DTC) on BMA assessment
Prognostic in EBC Marker of recurrence
Circulating tumor cells (CTC) Poor survival after NACT or primary breast cancer surgery
cf-DNA (cell free-DNA) Plasma miRNA
Markers of relapse in EBC

EBCTCG 2011
Compared with no treatment, the use of anthracycline-containing regimen was associated with the following outcomes at 10 years:
Risk of recurrence Significant improvement
RR 0.73 Absolute gain of 8%
Breast cancer mortality
Significant reduction RR 0.79 Absolute gain of 6.5%
Overall mortality Significant reduction RR 0.84 Absolute gain of 5%
Compared with no treatment, the use of CMF was associated with these outcomes at 10 years:
Risk of recurrence Significant improvement
RR 0.7 Absolute gain of 10.2%
Breast cancer mortality
Significant reduction RR 0.76 Absolute gain of 6.2%
Overall mortality Significant reduction RR 0.84 Absolute gain of 4.7%

Anthracycline-based therapy vs. CMF
The use of “standard” doses of anthracyclines was associated with the following outcomes at 10 years compared with CMF (n=5122 women)
The use of higher cumulative doses of anthracyclines (> 4 cycles, to cumulative dose of >240 mg/m2) compared with CMF was associated with the following outcomes at 10 years (n=9572)
No improvement in the risk of recurrence (RR 0.99)
No improvement in breast cancer mortality (RR 0.98)
No improvement in overall mortality (RR 0.97)
Reduction in risk of recurrence
RR 0.89 Absolute gain of 2.6%
Reduction in breast cancer mortality
RR 0.80 Absolute gain of 4.1%
Reduction of overall mortality
RR 0.84 Absolute gain of 3.9%

EBCTCG 2012 meta-analysis
Trials where the same control regimen was used in both arms (n=11,167 women) (8 year outcome):
Trials where the number of cycles in the control anthracycline regimen was doubled to mirror the addition of cycles of taxanes to anthracyclines (n=33,084) (5 year outcome):
Reduction in risk of recurrence
RR 0.84 Absolute gain of 4.6% in RFS
Reduction in breast cancer mortality
RR 0.86 2.8% improvement in breast cancer-specific OS
Reduction in overall mortality RR 0.86 3.2% improvement in OS
Reduction in risk of recurrence
RR 0.86 Absolute gain of 2.9%
Reduction in breast cancer mortality
RR 0.88 Absolute improvement of 1.4%
Reduction in overall mortality
RR 0.9 Absolute improvement of 1.2%