value of diabetes as an independent predictor of death in subjects with end-stage renal disease
TRANSCRIPT

Value of Diabetes as an Independent Predictor of Death in Subjects with End-Stage Renal DiseaseMichael Koch1, Markus Hollenbeck2, Rudolf Trapp1, Wolfgang Kulas1, Bernd Grabensee2
1 Center of Nephrology Mettmann, Germany,2 Department of Nephrology, Heinrich Heine University, Düsseldorf, Germany.
Received: March 8, 2006.Revision accepted: November 1, 2006.
ABSTRACT
Background and Purpose: Diabetic subjects on hemodialysis have a poor survival. The authors performed a Kaplan-Meier survival analysis of diabetic versus nondiabetic subjects and investigated the value of diabetes as an inde-pendent predictor of death in these end-stage renal disease (ESRD) subjects.
Patients and Methods: From 1997 to 2003, 135 ESRD subjects (41 diabet-ics) were enrolled in a survival study beginning at the start of dialysis. Inclusion criterion was onset of dialysis at least 6 months before study entry. Exclusion criteria comprised age < 45 years, coronary artery disease (CAD), critical limb ischemia (CLI), or malignancies at ESRD onset up to 6 months after study entry. Subjects with clinical signs of vascular disease were followed up by coronary or peripheral angiographies.
Results: Baseline risk factors were similar between diabetic and nondia-betic subjects. The 5-year survival rate in nondiabetic subjects was 76.9% (95% confidence interval [CI] = 62–86%) versus 76.4% (95% CI = 53–89%) in diabetic patients (p = 0.402). Consistent with this finding, the Cox propor-tional hazards model revealed that diabetes does not significantly change the risk of death in ESRD subjects. De novo CAD developed in 35 and CLI in ten subjects, but both diseases were present more frequently in nonsurvivors (42% vs. 23%; p = 0.052) versus survivors (21% vs. 5%; p = 0.005).
Conclusion: Diabetes is not an independent predictor of death in the ESRD study group presented here. Prevention of CAD and CLI in diabetic subjects is most important to improve survival.
Key Words: End-stage renal disease · Diabetes · Predictor of death Med Klin 2006;101:933–7.
DOI 10.1007/s00063-006-1125-6
ZUSAMMENFASSUNG
Bedeutung des Diabetes als unabhängiger Prädiktor für den Tod bei Patienten mit terminaler Niereninsuffizienz
Hintergrund und Ziel: Die Autoren führten eine Kaplan-Meier-Analyse bei diabetischen und nichtdiabetischen Dialysepatienten durch und untersuch-ten die Bedeutung des Diabetes als unabhängigen Prädiktor für den Tod.
Patienten und Methodik: Von 1997 bis 2003 wurden 135 Patienten mit terminaler Niereninsuffizienz (41 Diabetiker) in die Überlebensstudie aufge-nommen. Studienbeginn war der Start der Dialyse. Einschlusskriterium war Dialysebeginn mindestens 6 Monate vor Studieneintritt. Ausschlusskriterien umfassten Alter < 45 Jahre, koronare Herzkrankheit (KHK), kritische Bein-
Diabetes has become the leading cause of end-stage renal disease
(ESRD), particularly because of the in-creasing number of type 2 diabetic pa-tients worldwide [1]. Diabetic patients on hemodialysis have an excessive mor-tality rate with a 5-year survival rate of only 20% [2], which is comparable to mortality rates of colon cancer [3]. In-terestingly, these patients are twice as likely to co-develop coronary artery disease (CAD), the major pathogenetic factor of cardiovascular disease, than are nondiabetic patients with ESRD [4]. USRDS displayed that the mortality due to cardiovascular disease was higher in long-term hemodialysis patients who were older or had diabetes than in pa-tients without these characteristics [5]. These findings were confirmed in an-other study showing that the death rate was significantly higher in diabetic pa-tients with CAD than in nondiabetic patients with CAD [6]. This poses the question whether it is diabetes itself or associated interacting factors, e.g., age or comorbidities such as CAD, that can independently predict the risk of death in patients with ESRD. In the Framing-ham study [7], it could be demonstrated that diabetes itself represents an inde-pendent risk factor for death, which gender-dependently increases mortality by two- to fourfold in the general pop-ulation. Therefore, it may be assumed that diabetes may also be an independent predictor of death in patients with ESRD. However, the results of different studies evaluating this assumption to date are controversial. Some studies could acknowledge this potential role of dia-betes [8] in ESRD patients while others could not [9–11], whereby this contro-versy may be due to applied different population selection criteria, sample sizes, and tested confounding factors. Our primary goal in this survival study was to perform a Kaplan-Meier sur-vival analysis of diabetic subjects (who, at start of dialysis treatment, did not suf-fer from other potential interacting death
933
ORIGINALARBEIT
2006;101:933–7 (Nr. 12), © Urban & Vogel, München

934
included regular quality controls along with antihypertensive therapy to lower systolic blood pressure to < 140 mmHg. This therapy was the same in diabetic and nondiabetic patients. In addition, statin therapy to lower LDL choles-terol to < 130 mg/dl was given to 33 subjects (eight diabetic, 25 nondiabetic subjects; p = 0.378), and low-dose as-pirin therapy to lower the total risk of myocardial infarction was administered to 60 subjects (24 diabetic, 36 nondia-betic subjects; p = 0.029). Blood sugar of the diabetic subjects was controlled to reach an HbA1c < 7%, and all subjects were given erythropoietin and iron
supplementation. Hemoglobin levels were thus measured once a week, and potassium levels were measured at the beginning of each dialysis session. How-ever, calcium, phosphate and C-reactive protein (CRP) levels to further charac-terize development of atherosclerotic disease were not determined in our study.
Procedures during the Observation Period
During the observation period or until death, subjects were investigated three times per week by the same physicians
ischämie (KBI) oder Malignom zu Dialysebeginn und bis zu 6 Monate nach Studieneintritt. Patienten mit klinischen Anzeichen einer Gefäßkrankheit wurden mittels koronarer oder peripherer Angiographie untersucht.
Ergebnisse: Die Risikofaktoren vor Studienbeginn waren bei Diabetikern und Nichtdiabetikern ähnlich. Die 5-Jahres-Überlebensrate betrug bei Nicht-diabetikern 76,9% (95%-Konfidenzintervall [CI] = 62–86%) versus 76,4% (95%-CI = 53–89%) bei Diabetikern (p = 0,402). Das Cox-Modell zeigte, dass Diabetes das Todesrisiko statistisch nicht signifikant verändert. Eine De-novo-KHK trat bei 35 und eine KBI bei zehn Patienten auf, aber beide Krankheiten waren bei den verstorbenen Patienten (42% vs. 23%; p = 0,052) häufiger zu finden als bei den überlebenden Patienten (21% vs. 5%; p = 0,005).
Schlussfolgerung: Diabetes ist kein unabhängiger Prädiktor für den Tod in der hier vorgestellten Studiengruppe. Die Prävention von KHK und KBI bei Diabetikern hat für eine Verbesserung des Überlebens eine große Bedeu-tung.
Schlüsselwörter: Terminale Niereninsuffizienz · Diabetes · Prädiktor für Tod
Med Klin 2006;101:933–7.DOI 10.1007/s00063-006-1125-6
Koch M, et al.Value of Diabetes as Death PredictorMed Klin 2006;101:933–7 (Nr. 12)
ORIGINALARBEIT
risk factors such as CAD or critical limb ischemia [CLI]) versus nondiabetic sub-jects and to investigate, by means of the Cox proportional hazards model, the value of diabetes as an independent predictor of death in patients with ESRD.
Patients and Methods
Population
From 1997 to 2003, 135 incident subjects (60 men; mean age 68 ± 10 [SD] years, mean weight 72 ± 15 kg, mean systolic RR 140 ± 17 mmHg, mean diastolic RR 79 ± 7 mmHg, LDL cholesterol 127 ± 37 mg/dl) with ESRD were enrolled in this survival study at the Center of Ne-phrology, Mettmann, Germany, after signing informed consent. 41 of the 135 subjects were diabetics, 13 subjects were smokers. Differences of the aforemen-tioned traditional risk factors (i.e., sex, age, weight, blood pressure, cholesterol level, and smoking habits) between dia-betic and nondiabetic subjects were clinically not important and statistically not significant (see Table 1). Inclusion criterion was beginning of hemodialysis at least 6 months before study entry. Ex-clusion criteria comprised age < 45 years, acute renal failure, CAD, CLI, and any malignant disease up to 6 months after study entry.
Subject Treatment
Subjects were dialyzed for a total of 6–18 h/week using bicarbonate-buff-ered dialysate depending on residual renal function. Subjects were treated according to a standard regimen, which
Table 1. Differences of basic characteristics between diabetic and nondiabetic patients.
Diabetic patients Nondiabetic patients Diabetic patients (n)
Nondiabetic patients (n)
p-value
Age (years)a 69.1 (66.0–72.1) 67.5 (65.3–69.6) 41 94 0.40
Weight (kg)a 73.9 (68.8–79.1) 71.8 (68.7–74.9) 41 88 0.46
LDL (mg/dl)a 124.5 (104.2–144.8) 128.6 (115.1–142.0) 16 32 0.73
Blood pressure, systolic (mmHg)a
140.8 (134.6–147.0) 140.2 (136.5–143.8) 38 82 0.86
Sex (male)b 18 42 41 94 0.93
Smokersb 3 10 41 94 0.55
a Values are means (95% confidence intervals). Corresponding p-values computed by two-tailed Student’s t-testb Values are numbers. Corresponding p-values computed by χ2-test

935
who also performed the screening pro-cedure. A coronary angiography was performed in subjects diagnosed with angina pectoris. CAD was defined when observing a stenosis of > 50% in at least one coronary artery. If no an-giography was performed, CAD was diagnosed in subjects with a history of myocardial infarction with concomitant changes in the electrocardiogram. Pe-ripheral angiography was performed in all symptomatic subjects with foot le-sions such as ulceration or gangrene. CLI was diagnosed if angiography showed one or more of the following signs: stenosis, slow-flow phenomenon, and/or a rarefaction of one of the pe-ripheral arteries. Subjects were retro-spectively excluded from the study when CAD or CLI developed up to 6 months after study entry, i.e., begin-ning of dialysis.
Statistical Analysis
Analysis was performed on the 135 re-maining subjects who were not ex-cluded from the study due to any ex-clusion criteria or due to death within 6 months after study entry.
Statistical analysis was performed by using SAS for Windows, version 8.2 (SAS Institute, Cary, NC, USA). Base-line characteristics between nondia-betic and diabetic subjects were com-pared by Student’s t-test (two-tailed). Survival time was calculated from the start of dialysis treatment. Subjects who received a renal graft during the obser-vation period were censored. 5-year survival and mortality were estimated by life tables and survival distribution function according to the Kaplan-Mei-er method. Statistical differences were
calculated by using the log-rank test. The Cox proportional hazards model was used to prove independency of covariates, such as age, diabetes, blood pressure, sex, and smoking.
Results
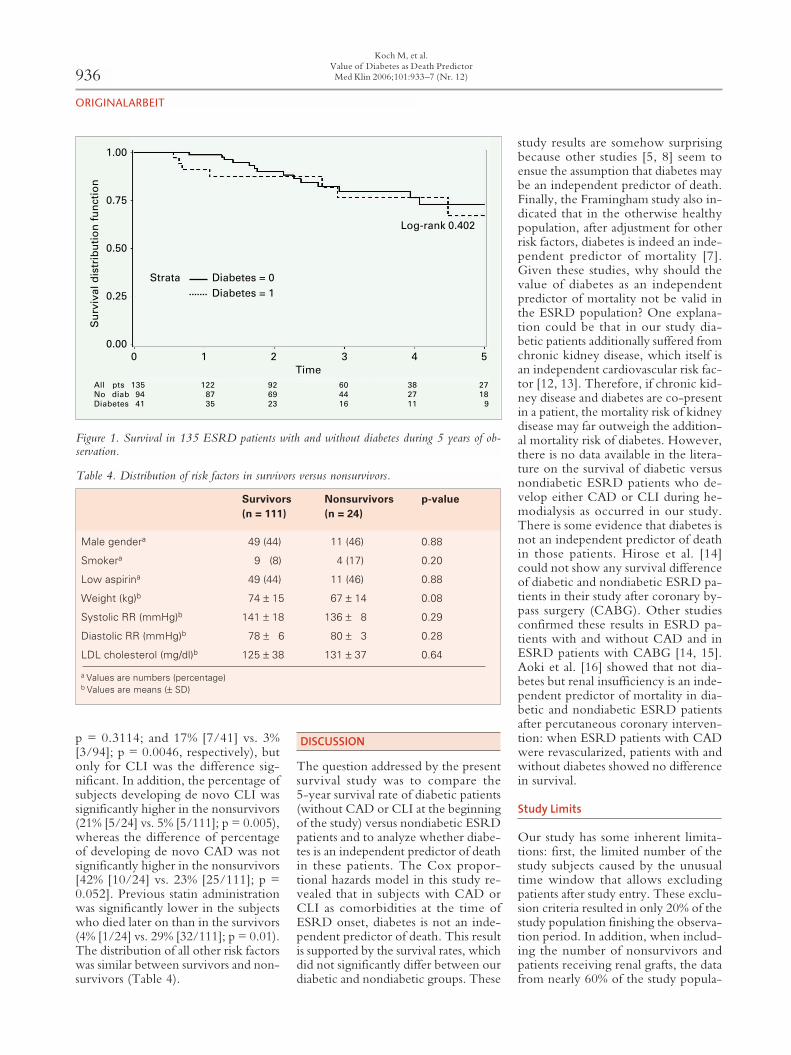
The primary endpoint of this study – the comparison of the survival rate of nondiabetic patients versus diabetic patients in a study population of 135 ESRD patients – showed that the 5-year survival rate in nondiabetic sub-jects was 76.9% (95% confidence in-terval [CI] = 62–86%) versus 76.4% (95% CI = 53–89%) in diabetic patients (see Figure 1). Mean survival time for nondiabetic patients was 4.6 ± 0.19 years and mean survival time for dia-betic patients was 5.2 ± 0.5 years. The log-rank test revealed no statistically significant difference between survival rates (p = 0.402). At the end of the 5-year observation period, 16 of 94 patients from the nondiabetic group had died, and four patients had been
censored because of receiving renal grafts. In the diabetic group, eight of 41 patients had died, and two patients had been censored due to receiving renal grafts (for reasons of death in both groups see Table 2). The prevalence of diabetes in the 24 nonsurvivors was similar to those of the survivors (38% [9/24] vs. 29% [32/111]; p = 0.402).
Further investigation with Cox proportional hazards regression analysis, which controlled for the effect of dia-betes, indicated that none of the tested variables, except age, independently and statistically significantly influenced the risk of death in the ESRD group (Table 3). The influence of age as an independent predictor of death, howe-ver, was statistically significant but clinically irrelevant, as the risk ratio difference is negligible.
55 subjects developed de novo CAD, and ten subjects developed de novo CLI during follow-up. Both diseases were found more frequently in diabetic than in nondiabetic sub-jects (32% [13/41] vs. 23% [22/94];
Koch M, et al.Value of Diabetes as Death PredictorMed Klin 2006;101:933–7 (Nr. 12)
ORIGINALARBEIT
Table 2. Causes of death in diabetic and nondiabetic subjects. CLI: critical limb ischemia.
Total deaths(n = 24)
Diabetics(n = 8)
Nondiabetics(n = 16)
Cardiovascular 4 2 2
• Myocardial infarction 1 0 1• Sudden death 2 2 0• Other cardiac causes 1 0 1
CLI 5 3 2Cerebrovascular 3 1 2Long-standing disease 1 0 1Malignancy 2 0 2Infection/sepsis not related to CLI 2 2 0Other causes 7 0 7
Table 3. Cox proportional hazards model showing the effect of six variables on the risk of death in patients with end-stage renal disease. CAD: coronary arterial disease; CI: confidence interval; PAOD: peripheral arterial occlusion disease.
Variable Coefficient (β) Standard error Wald χ2 p-value Risk ratio 95% CI
Age 0.06 0.03 5.68 0.02 1.06 1.01–1.12
Sex –0.12 0.47 0.07 0.80 0.89 0.35–2.25
Diabetes –0.11 0.47 0.06 0.81 0.90 0.36–2.25
CAD 0.27 0.48 0.35 0.56 1.30 0.54–3.13
PAOD 0.85 0.55 2.36 0.12 2.34 0.79–6.94
Smoking 0.89 0.59 2.31 0.13 2.44 0.77–7.67
ORIGINALARBEIT
936
p = 0.3114; and 17% [7/41] vs. 3% [3/94]; p = 0.0046, respectively), but only for CLI was the difference sig-nificant. In addition, the percentage of subjects developing de novo CLI was significantly higher in the nonsurvivors (21% [5/24] vs. 5% [5/111]; p = 0.005), whereas the difference of percentage of developing de novo CAD was not significantly higher in the nonsurvivors [42% [10/24] vs. 23% [25/111]; p = 0.052]. Previous statin administration was significantly lower in the subjects who died later on than in the survivors (4% [1/24] vs. 29% [32/111]; p = 0.01). The distribution of all other risk factors was similar between survivors and non-survivors (Table 4).
DISCUSSION
The question addressed by the present survival study was to compare the 5-year survival rate of diabetic patients (without CAD or CLI at the beginning of the study) versus nondiabetic ESRD patients and to analyze whether diabe-tes is an independent predictor of death in these patients. The Cox propor-tional hazards model in this study re-vealed that in subjects with CAD or CLI as comorbidities at the time of ESRD onset, diabetes is not an inde-pendent predictor of death. This result is supported by the survival rates, which did not significantly differ between our diabetic and nondiabetic groups. These
study results are somehow surprising because other studies [5, 8] seem to ensue the assumption that diabetes may be an independent predictor of death. Finally, the Framingham study also in-dicated that in the otherwise healthy population, after adjustment for other risk factors, diabetes is indeed an inde-pendent predictor of mortality [7]. Given these studies, why should the value of diabetes as an independent predictor of mortality not be valid in the ESRD population? One explana-tion could be that in our study dia-betic patients additionally suffered from chronic kidney disease, which itself is an independent cardiovascular risk fac-tor [12, 13]. Therefore, if chronic kid-ney disease and diabetes are co-present in a patient, the mortality risk of kidney disease may far outweigh the addition-al mortality risk of diabetes. However, there is no data available in the litera-ture on the survival of diabetic versus nondiabetic ESRD patients who de-velop either CAD or CLI during he-modialysis as occurred in our study. There is some evidence that diabetes is not an independent predictor of death in those patients. Hirose et al. [14] could not show any survival difference of diabetic and nondiabetic ESRD pa-tients in their study after coronary by-pass surgery (CABG). Other studies confirmed these results in ESRD pa-tients with and without CAD and in ESRD patients with CABG [14, 15]. Aoki et al. [16] showed that not dia-betes but renal insufficiency is an inde-pendent predictor of mortality in dia-betic and nondiabetic ESRD patients after percutaneous coronary interven-tion: when ESRD patients with CAD were revascularized, patients with and without diabetes showed no difference in survival.
Study Limits
Our study has some inherent limita-tions: first, the limited number of the study subjects caused by the unusual time window that allows excluding patients after study entry. These exclu-sion criteria resulted in only 20% of the study population finishing the observa-tion period. In addition, when includ-ing the number of nonsurvivors and patients receiving renal grafts, the data from nearly 60% of the study popula-
Koch M, et al.Value of Diabetes as Death PredictorMed Klin 2006;101:933–7 (Nr. 12)
Table 4. Distribution of risk factors in survivors versus nonsurvivors.
Survivors(n = 111)
Nonsurvivors(n = 24)
p-value
Male gendera 49 (44) 11 (46) 0.88
Smokera 9 (8) 4 (17) 0.20
Low aspirina 49 (44) 11 (46) 0.88
Weight (kg)b 74 ± 15 67 ± 14 0.08
Systolic RR (mmHg)b 141 ± 18 136 ± 8 0.29
Diastolic RR (mmHg)b 78 ± 6 80 ± 3 0.28
LDL cholesterol (mg/dl)b 125 ± 38 131 ± 37 0.64
a Values are numbers (percentage)b Values are means (± SD)
Log Rank 0.4022Log-rank 0.402
Su
rviv
al d
istr
ibu
tio
n f
un
ctio
n
1.00
0.75
0.50
0.25
0.00
All pts 135 122 92 60 38 27No diab 94 87 69 44 27 18Diabetes 41 35 23 16 11 9
0 1 2 3 4 5Time
Strata Diabetes = 0Diabetes = 1
Figure 1. Survival in 135 ESRD patients with and without diabetes during 5 years of ob-servation.

ORIGINALARBEIT
937Koch M, et al.
Value of Diabetes as Death PredictorMed Klin 2006;101:933–7 (Nr. 12)
tion could not be assessed adequately. Second, the study is limited by the am-biguous diagnoses of CAD and CLI at baseline. Diagnosis of CLI is highly specific because it is usually performed by detection of gangrene of a digit dur-ing regular foot inspection. In our study, this diagnosis was to be further confirmed by angiographies, and sub-jects were to be excluded from the study if those events occurred up to 6 months after dialysis onset. On the other hand, specificity of CAD diag-nosis is somewhat limited since coro-nary angiographies were not performed in all subjects, because at ESRD onset, patients are often overloaded by diag-nostic measurements and additional angiographies are not much appreci-ated. Thus, diabetic subjects with au-tonomic neuropathy could have been misdiagnosed as not having CAD. This is also true in nondiabetic patients with neuropathy as a widespread disease as-sociated with ESRD. Therefore, if CAD was excluded in diabetic or non-diabetic subjects, who in fact had CAD, the presented results would be more consistent than they actually are. An-other problem in our study was the validation time of coronary or periph-eral arteries, which needed up to 6 months. If CAD or CLI was diagnosed during the first 6 months of dialysis treatment, and then those subjects died during this time, they had to be cen-sored.
A third limitation of the study is that the same survival between diabetic and nondiabetic patients may have been influenced by some different basic char-acteristics: a significantly larger numb-er of diabetic patients versus nondia-betic patients have received low-dose aspirin at the beginning of the study to prevent myocardial infarction. In ad-dition, important atherosclerotic disease characteristics, such as calcium, phos-phate, and CRP levels, have not been measured at all, and LDL levels have been measured only in 48 of the 135 patients (36%).
Another point one should be aware of in this study is that the results only refer to a 5-year observation period. It is, however, possible that the survival of the remaining patients in the dia-betic and nondiabetic groups may be different after this time and that, with further development of the disease, diabetes may become an independent predictor of death in our patient group.
CONCLUSION
In our study group, preliminary results showed that subjects with diabetes – but without the often accompanying comorbidities such as CAD or CLI at the beginning of the observation pe-riod – had a similar survival rate as sub-jects without diabetes. In addition and in agreement with these findings, dia-betes proved not to be an independent predictor of death in our ESRD patient group, as shown by the Cox propor-tional hazards model. It could also be concluded that prevention of CAD and CLI before and during hemodialysis in patients with ESRD is of utmost im-portance to improve survival. To con-firm our above findings in the general ESRD population, the described anal-ysis should be repeated with larger sample sizes. In addition, further stud-ies should be conducted in well-defined ESRD subjects with CAD or periph-eral arterial disease (PAD) who should be compared with ESRD subjects with no vascular diseases to determine the impact of these vascular diseases on the survival rate of subjects with ESRD.
Acknowledgments
We thank Silke Haidekker, PhD, ELS, for her excellent assistance in preparing the manuscript.
References 1. Ritz E, Orth SR. Nephropathy in patients with type
2 diabetes mellitus. N Engl J Med 1999;341:1127–33.
2. Koch M, Thomas B, Tschope W, et al. Survival and predictors of death in dialysed diabetic patients. Diabetologia 1993;36:1113–7.
3. Murphy TK, Calle EE, Rodriguez C, et al. Body mass index and colon cancer mortality in a large prospective study. Am J Epidemiol 2000;152:47–54.
4. Stack AG, Bloembergen WE. Prevalence and clin-ical correlates of coronary artery disease among new dialysis patients in the United States: a cross-section-al study. J Am Soc Nephrol 2001;12:1516–23.
5. USRDS: the United States Renal Data System. Am J Kidney Dis 2003;42:1–230.
6. Raggi P, Shaw LJ, Berman DS, et al. Prognostic value of coronary artery calcium screening in subjects with and without diabetes. J Am Coll Cardiol 2004;43:1663–9.
7. Kannel WB, McGee DL. Diabetes and cardiovas-cular risk factors: the Framingham study. Circulation 1979;59:8–13.
8. Herzog CA, Ma JZ, Collins AJ. Poor long-term survival after acute myocardial infarction among patients on long-term dialysis. N Engl J Med 1998;339:799–805.
9. Shoji T, Shinohara K, Kimoto E, et al. Lower risk for cardiovascular mortality in oral 1alpha-hydroxy vitamin D3 users in a haemodialysis population. Nephrol Dial Transplant 2004;19:179–84.
10. Ono K, Tsuchida A, Kawai H, et al. Ankle-brachi-al blood pressure index predicts all-cause and car-diovascular mortality in hemodialysis patients. J Am Soc Nephrol 2003;14:1591–8.
11. Weiner DE, Tighiouart H, Amin MG, et al. Chron-ic kidney disease as a risk factor for cardiovascular disease and all-cause mortality: a pooled analysis of community-based studies. J Am Soc Nephrol 2004;15:1307–15.
12. Fried LF, Shlipak MG, Crump C, et al. Renal insuf-ficiency as a predictor of cardiovascular outcomes and mortality in elderly individuals. J Am Coll Car-diol 2003;41:1364–72.
13. Szczech LA, Best PJ, Crowley E, et al. Outcomes of patients with chronic renal insufficiency in the bypass angioplasty revascularization investigation. Circulation 2002;105:2253–8.
14. Hirose H, Amano A, Takahashi A, et al. Coronary artery bypass grafting in patients on chronic hemo-dialysis: diabetic nephropathy versus nondiabetic nephropathy. Artif Organs 2002;26:794–801.
15. Dacey LJ, Liu JY, Braxton JH, et al. Long-term survival of dialysis patients after coronary bypass grafting. Ann Thorac Surg 2002;74:458–62.
16. Aoki J, Ikari Y, Nakajima H, et al. Coronary revas-cularization improves long-term prognosis in dia-betic and nondiabetic end-stage renal disease. Circ J 2002;66:595–9.
Address for CorrespondenceMichael Koch, MDGartenstraße 840822 MettmannGermanyPhone (+49/2104) 97996-0Fax -71e-mail: [email protected]