v. karapanou d. kempuraj - biolifesas.org eji vol 7, no. 1.pdf · 2 eur. j. inflamm. 3 to membrane...
TRANSCRIPT

EUROPEAN JOURNAL OF INFLAMMATION
1721-727X (2009)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties1
ORAL NEUROIMMUNE NETWORK AND MAST CELLS
V. KARAPANOU1, D. KEMPURAJ2 and T.C. THEOHARIDES2,3,4
1Department of Endodontics, Tufts University School of Dental Medicine and Departments of 2Pharmacology and Experimental Therapeutics, 3Biochemistry and 4Internal Medicine, Tufts
University School of Medicine and Tufts Medical Center, Boston, MA, U.S.A.
Received December 23, 2008 – Accepted March 10, 2009
EDITORIAL
Mailing address: Virginia Karapanou, D.M.D.Department of Endodontics,Tufts University, School of Dental Medicine,One Kneeland Street,Boston, MA 02111, U.S.ATel: ++1 617 636-6796 Fax: ++1 617 636-6885e-mail: [email protected]
Key words: dental pulp, cytokines, inflammation, MCs, neuropeptides
Inflammation is a critical process in the oral cavity, especially in gingival inflammation and pulpitis, as seen in periodontitis and decayed tooth structure. Nevertheless, the cellular process involved in oral inflammation is not well delineated. Recent evidence from other organs as well as the mouth suggests that neurogenic inflammation involving mast cells (MCs) may be a critical factor. MCs, best known for their role in allergic reactions, are also involved in immunity and inflammation. They are located at strategic points close to small blood vessels and nerve fibers often containing substance P (SP). The pain models of reversible or irreversible pulpitis simply suggest the complexity of neural-inflammatory interactions within the dental pulp. In the pulp and periapical area, neuropeptides and cytokines modulate vascular responses, increase permeability and leukocyte migration. SP-immunoreactive nerve fibers and TNF-positive MCs were found localized around blood vessels in all samples of periapical granulomas. By generating a profound number of potent mediators, MCs may serve as a link between the immune, endocrine and nervous systems in pulp inflammation. This role has been strengthened by recent evidence of MCs involvement in inflammatory conditions.
MCs and the neuroimmune networkMast cells (MCs) and nerves interaction has
been proven in an axon reflex responsible for flare reaction to noxious stimuli, as seen in the skin. Both share neuroeffector junctions in the skin and elsewhere. Local injury and/ or antidromic stimulation of neurons sensitizes local C fibers which release chemical mediators during the axon-reflex such as SP and other neuropeptides. SP has been localized in vagus nerve, trigeminal nerve (1) and the nerve supplying the pars flaccida of the tympanic membrane (2). Moreover, SP has a role in generating neurogenic inflammation on parotid glands of rats, in which the symptoms elicited by SP-infusion, could be diminished by using SP-
antagonist pretreatment. Direct stimulation of the vidian nerve in patients with chronic hypertrophic non-allergic rhinitis causes morphological changes of MCs, significant decrease in tissue-based histamine and concomitant degranulation resulting in vasodilation and enhanced nasal secretion (3). It is interesting that fibers containing SP form neuroeffector junctions with MCs around blood vessels, but rarely form such relationships with MCs elsewhere in the tissues. Further, trachea MCs are situated between epithelial cells at sites neighboring SP and CGRP-containing nerves, close association of SP-containing nerves and apposed MCs was found in the diaphragm, mesentery and liver. Type 2 cerebral MC demonstrated intimate membrane
Vol. 7, no. 1, 1-8 (2009)

2 3Eur. J. Inflamm.
to membrane association with nerves, as well. Antidromic stimulation of sensory neurones resulted in release of SP, induction of mast cell degranulation and histamine release in lung, gut and in the dura by trigeminal nerve stimulation.
In conclusion, inflammatory responses to injury can be of neurogenic origin, including local alterations in blood flow, vascular permeability, smooth muscle tone, fluid and mucus secretion, as well as margination and PMN leukocytes adherence in blood vessels via mast cell degranulation .and histamine release.
MCs and Dental pulpitis
Obtaining dental tissue (tooth splitting, demineralization of the inorganic substance of the teeth and removal of the tissue through conventional access under clinical conditions with barbed broaches), fixation (Astra blue, Toluidine blue, Luna’s staining, and fluorescent microscopy) and preservation (formalin, ethanol, acetic acid) can all alter mast cell integrity, making it difficult to compare relevant studies. For instance, acid-demineralizing agents destroy mast cell fluorescence, thus identification of MCs in the dental pulp has been challenging.
A supposition presented by that the pulp tissue could be lacking MCs as a form of pivotal defense to avoid the vasoactive substances release, as well as the unbearable pain that could result in such a low compliance environment. Occasionally, MCs and lymphocytes found near blood vessels in pulps of extracted teeth.
On the other hand, it should be noted that pulp tissue could contain MCs progenitors that are not “mature” enough to be identified by stains that depend exclusively on the content of the secretory granules. In scleroderma, MCs were so difficult to identify without electron microscopy that they were named “phantom MCs”. Also, it was recently shown that human MCs could release either IL-6 or vascular endothelial growth factor (VEGF), both of which were newly synthesized and did not involve secretory granules.
Irreversibly symptomatic pulpal tissue contained the highest concentration of TNF-α which decreased, as pulp inflammation progressed to necrosis; while the lowest concentration was found in healthy pulp
tissue (4). Similar findings were found in rat teeth after inducing pulp inflammation (5). The source of TNF-α may be oral MCs containing TNF-α in granules, to be released upon degranulation.
Porcine pulp histamine levels increased four-fold within 30 minutes after thermal injury; however, after application of electric current through the teeth with an electric pulp tester, the levels of histamine were reduced (6). Histamine, as potent vasodilator and mediator of vascular permeability, may play a role in initiating pulp inflammation. Prolonged heat application, for more than 5 seconds, may cause a bi-phasic stimulation of A-delta fibers, and then, stimulation of C fibers resulting in SP production; repeated exposure to small doses of SP, caused degranulation in more than 50% of MCs (7). SP may mediate mast cell degranulation leading in detrimental host defense activated systems in the pulp. Clinically, the patient may complain of lingering pain and eventually constant ache. The electric pulp tester produces an ionic shift of the dentinal fluid within the tubules which causes local depolarization and subsequently stimulation of the A-delta fibers and possibly somatostatine (SOM) release. SOM may then inhibit the release of SP and subsequently hinder MCs degranulation and histamine release.
Bacterial invasion of the pulp system during the carious process may also cause MC activation. Differential histamine expression through H1 and H2 receptors from MCs responds to antibody formation and regulation of T-cells. MCs express both MHC class I and class II molecules as well as CD80, and CD54 molecules that serve as the second signal for T-lymphocyte activation during antigen presentation. Furthermore, MCs belong among the potential cells to set off pulpitis, because upon activation, they are the leading producers of matrix metalloproteinases (MMP) -1 and IL -8, expressing MM-2 and the tissue inhibitor of metalloproteinases (TIMP)-1 (8). MMP-8 levels measured in the gingival crevicular fluid were found significantly elevated in the painful tooth (9). In the periradicular area, histamine or other MCs mediators may also activate further host defense systems; clinically inflamed pulps may produce teeth with mechanical allodynia, a painful response upon tapping (10). Mechanical allodynia may be explained by MCs
V. KARAPANOU ET AL.

2 3Eur. J. Inflamm.
activation and degranulation of potent mediators infusing the periradicular area of the involved tooth at all portals of main and lateral canals. It is interesting that increased numbers of osteoclasts and bone destruction has been noted before total pulp necrosis at periapical inflammatory infiltrates. Besides, MCs were abundantly found in granulomas of apical abscesses with proliferating epithelium containing inflammatory infiltrate, and as the lesions became chronic MCs were diminished (11).
These findings support the frequent clinical symptom that teeth with painful responses to cold and hot stimuli, signs of irreversibly inflamed, but vital pulp tissue, may still present radiographic evidence of periapical pathosis or widening of the
periodontal ligament space.
Dental Pulpitis and Neurogenic InflammationIn healthy pulp tissue, neuropeptides play a role
in maintaining the vascular tone for smooth blood flow and in regulating the interstitial pulpal pressure within a non-compliant tissue. The involvement of neurogenic inflammation in the initial or in consequent responses to infectious agents is poorly known, although some intriguing observations have been made. CGRP, SP and VIP are expressed in both primary and even greater in permanent dentitions and have critical interactions with other inflammatory factors in teeth with gross carious lesions (12).
Neurogenic inflammation is regarded as a
19
Table I. Dental pulp and inflammatory mediators.
DENTAL PULP Conditions
Mediators Cells References Main pathophysiologic effect
Thermal injury
Pulp exposure
Histamine �
CGRP �
(6) Vasodilation, mitogenesis, immunosuppression
Oral pulp
exposure
SP �
CGRP �
(14)
Irreversible
pulpitis
TNF-� � (4) Inflammation, leukocyte proliferation/activation
Human dental pulp culture
�SP
� IL-6�
� IL-1beta�
(20) Inflammation, leukocyte migration
Neutrophil chemoattractant
Caries = Pain �SP ----------=
�CGRP -----=
�NKA
� IL-8 mRNA
�IL-18 mRNA
IL-1a,IL-1b ~
�MMP-8
�T-cells
�T-cells
(13)
(17)
(29)
(9) Chemoattraction for MCs Leukocyte chemoattraction
Neovascularization
Periapical granuloma TNF-� MCs (33) leukocyte proliferation/activation
Trigeminal axotomy CGRP � + destruction
+Dentritic cells
+I-A antigen-expressing cells
+CD43 cells
(26)
Sympathectomy �IL-1�
� TNF-�
� MCs bilaterally
(27)
Table I. Dental pulp and inflammatory mediators.

4 5Eur. J. Inflamm.
protective mechanism that forms the first line of defense and protects tissue integrity. Nevertheless, it may also result in persistent dental pulp inflammation and injury upon prolonged noxious biologic or iatrogenic stimulation.
In the para-odontoblastic region of the coronal rat dental pulp, nerves and immunocompetent cells demonstrate close spatial relationship; 70% of the antigen presenting class II cells showed close proximity to nerve fibers immunoreactive for CGRP and 50% of cells were in close association with nerve fibers immunoreactive for SP (13). Furthermore, SP increased the proliferation of purified T-lymphocytes significantly in the presence of pulp-derived accessory cells in rat incisor pulp tissue; while CGRP suppressed this action.
Rat pulp SP and CGRP underwent dynamic, but injury specific and peptide specific, responses following pulp exposure or dentin acid etching; both procedures produced a substantial and prolonged reduction, especially of CGRP, after pulp exposure. SP was reduced only by 10-20% of baseline values for both procedures, indicating a lack of corresponding difference in SP levels for the two forms of injury
(14). On rat pulp exposure-induced irreversible pulpitis, degeneration and regeneration appeared simultaneously, but not equally, in the injured tissue. Important interactions between peptidergic nerve fibers and inflammatory cells are suggested as CGRP axonal branches sprouting started as early as 24 hours and continued to occur even around inflamed abscesses (15) decreased in response to progressive healing and reparative dentin formation (15).
SP and NKA, frequently co-localized in the trigeminal ganglion-derived nerves of the pulp tissue and periodontal ligament, act as critical neurotransmitters for eliciting moderate to intense pain (16). SP also increases vasodilation and pulpal blood flow.
SP cross-talks nerves to the immune system, stimulating the production of cytokines in order to initiate inflammatory cell infiltration (17). In carious painful teeth SP was significantly increased within all nerve trunks (18-19) and in pulp tissue was up-regulated in relation to caries and pain experience. It has been also shown that human dental pulp cells, incubated in the presence of various concentrations of CGRP and SP, significantly increased the
20
Fig. 1. Schematic representation of mast cell-neuronal interactions in dental pulpitis. Our hypothesis is that MCs activation could occur by neuropeptides released locally in pulp or through the apical and other foramen. Then, vasoactive, proinflammatory and nerve sensitizing molecules released could participate in pulp inflammation and serve as diagnostic markers of irreversibly inflamed teeth.
V. KARAPANOU ET AL.

4 5Eur. J. Inflamm.
amounts of IL-6, IL-1ß, and TNF-α in a dose and time-dependent manner (20). In similar manner, LPS causes at least a four-fold increase of the above cytokines (20).
Neurogenic inflammation of the pulp may accentuate inflammatory effects before actual bacterial invasion of the pulp chamber (21). Mild dental injury caused local phenomena of nerve sprouting and pulp reactions that healed in about two weeks, in rat teeth; on the other hand, when severe injuries allowed bacterial invasion into rat pulps, the superficial pulp layer was destroyed resulting in a gradual consumption of vital pulp tissue over several weeks, and rat periapical lesions were obvious within five days (22).
In germ free rats, pulp exposure resulted in minimal pulp inflammation associated with repair, such as new matrix formation and obliteration of the pulp chamber. In this experiment, Kakehashi et al. (1965) commented that the periradicular tissues behaved differently when iatrogenic root perforations resulted in root resorption. In absence of bacteria, neurogenic inflammation and MCs may have cooperated to produce eventual repair of the affected pulp tissue, by utilizing defensive mechanisms available to pulp tissue. The germs free periradicular tissues behaved differently and resulted in the phenomenon of root resorption due to perforations resulting in loss of anatomical boundaries.
Antidromic stimulation of the inferior alveolar nerve produced a significant increase in SP content of pulps and lips in rats, as well as, in vascular permeability; when the lips and the pulp tissue were pretreated with the mast cell secretagogue compound 48/80, histamine content in lips decreased significantly, but it remained unchanged in pulps after nerve stimulation (23). We may conclude that there might be more than one sophisticated mechanisms involving neuropeptides in the pulp tissue. The possibility of at least two existing mechanisms for inflammation initiation and pain onset has been expressed in general terms recognizing the relationship among the neuropeptides and the immune system (24).
Dental pulp and dura matter may share common features on nerves/MCs communication. Both tissues present low compliance with dense sensory innervation. Antidromic stimulation of the trigeminal
nerve promoted dura MCs degranulation and vascular permeability in blood vessels of the rat dura matter and tongue. Interestingly, migraine drugs inhibited dura MCs activation (25) and dura plasma extravasation upon trigeminal nerve stimulation, showing a direct association between MCs activation and plasma extravasation (25).
Also, sympathetic nerve degeneration and increased levels of serum histamine, resulting from MCs activation in dura matter, have been associated as a possible reason for the cluster headache phenomenon, a clinical situation of non-odontogenic facial pain, initially confused with pain of dental pulp inflammation.
Trigeminal nerve fibers axotomy increased destruction of pulp tissue in rat molar pulp (26), possibly due to MCs activation in the terminal branches of pulp or periapical tissues.
In rat dental pulp, after unilateral sympathectomy, a significant increase of MCs was found for the first time in inflamed and non inflamed pulps bilaterally, while a significant increase in cells immunoreactive to CGRP and SP was found in the ipsilateral trigeminal ganglion (27). An interesting observation is that no significant change was noted in morphology or staining characteristics of the sensory immunoreactive fibers; thus a direct mechanism may exist between sympathetic fibers and MCs (27).
Under stress conditions for the dental pulp, as in caries invasion or excessive occlusion forces, the sympathetic nervous system may be activated and stimulate MCs degranulation for TNF-α; cytokines such as IL-1α and TNF- α were found locally in the pulp tissue while others such as IL-6, were produced systemically.
Another remarkable reciprocity between nerves and MCs has been known in regulation of the pulp interstitial fluid. Transient increase of the interstitial fluid is protective because the dentinal fluid outward movement takes diffused antibodies against carious antigens. However, interstitial fluid pressure has to go down for the tissue to survive. An overseeing mechanism may control not only local mechanisms inside the pulp space but also, at the reciprocal periradicular tissues. In mouse skin, the interstitial fluid pressure depends on MCs, but the sensory nerves can also reduce it independently(28); neurogenic vasodilatation of arterioles acts protectively by

6 7Eur. J. Inflamm.
CGRP to counteract increased transient need for inflammatory cells influx but it enhances the SP and NKA response of postcapillary venular permeability, as well. SP and NKA are capable of producing an exudative leakage, or, instead, resolve the escalating pressure (28).
MCs are involved in many different types of protective and or destructive reactions in several tissues including the dental pulp. The ability of MCs to work effectively in an innate immunity profile, to be present in early inflammatory response through proinflammatory cytokines, or establish an acute inflammatory process to chronic, their collaborative communication with the sensory and/or sympathetic nerve fibers, in order to initiate positive or negative mechanisms in hyperalgesia and allodynia situations modulating pain activity make the MCs the top effector cells who coordinate and lead the tissue reactions.
Is Irreversible Pulpitis detected in Gingival Crevicular Fluid(GCF)?
Irreversible pulpitis is a major diagnostic clinical term used when a patient complaints about acute and lingering pain from teeth usually with deep carious lesions, fractures and/or heavy dental restorations. Then, prolonged, noxious, biologic or iatrogenic, stimulation, or both, involves a lower firing threshold and a broader receptive field of C fibers, resulting in release of neurogenic mediators. Among them, substance P is a critical neurotransmitter for eliciting moderate to intense pain (16). Thus, it is speculated that the interaction of SP and its neurokinin -1 receptor (NK-1R) play an important role in the pathophysiology of painful pulpal inflammation. It is known that a direct inflammatory cell infiltrate increases in the carious traumatized dentin-pulp organ (24). Unquestionably, SP, found within a subpopulation of nociceptive afferent nerve fibers, is up-regulated in relation to caries and pain experience (18).
SP expression undergoes dynamic changes following caries and it was significantly increased four times with the progression of caries (19). Additionally, SP acts as an important mediator of cross talk between nerves and the immune system (20).
Increased SP levels in painful human dental pulp
and in GCF of painful teeth (29-30), as well as in adjacent teeth; these increased levels of SP in adjacent teeth are probably due to activation of periodontium fibers, leading to higher concentration of the SP in adjacent GCF. SP concentration varies depending on the cascade of neurogenic inflammation that take place within an individual pulp tissue; NKA and CGRP levels, collected in GCF from painful teeth, were variable but not associated with parameters like gender, location of tooth, assessment of pain on a “10cm visual analogue” scale (29). However, SP was significantly greater in GCF collected from painful teeth when compared with non painful teeth in the same mouth and GCF SP levels one week after endodontic treatment were significantly in all samples and undetectable in 33% of samples (30). Interestingly, painful irreversibly inflamed teeth, found associated with significantly increased peripheral release of SP (30) and also in the adjacent teeth.
Hahn et al. (31), found that, in the presence of bacteria, the immunocompetent cells produce increased IL-6, IL-8, and TNF-α cytokine expression in the pulp. Furthermore, SP and other neuropeptides modulate vascular permeability and communicate with effector cells, such as MCs, in order to promote leukocyte migration in the pulp and periapical tissue (10).
IL- 8 and TNF-α attract neutrophils and T-lymphocytes; activate them, further eliciting host defense system responses. Both are produced by immune cells, especially by MCs. IL-8 was detected significantly greater in GCF of irreversibly inflamed teeth compared with the adjacent or contra lateral teeth (32). Moreover, a trend for increased IL-8 levels was shown by the adjacent teeth as well, in the high pain group of irreversibly inflamed teeth (32). Similar patterns were found by Awawdeh et al (2005) for GCF SP levels of irreversibly inflamed teeth and their adjacent ones (30).
The neurogenic component of pulp tissue is active and definitely prominent in symptomatic painful pulpitis, and possibly excites the local and adjacent effector cells to produce the proinflammatory cytokine IL-8. MCs are one of the richest sources of IL-8. Communication between SP and MCs has been suggested in promoting leukocyte migration in the pulp and periapical tissue (33). In table I we
V. KARAPANOU ET AL.

6 7Eur. J. Inflamm.
Forster C, Kemppainen P. Painful tooth stimulation elevates matrix metalloproteinase-8 levels locally in human gingival crevicular fluid. J Dent Res 2005; 84:335-9.
10. Owatz C, Khan A, Schindler WG, Schwartz S, Keiser K, Hargreaves K. The Incidence of Mechanical Allodynia in Patients With Irreversible Pulpitis. J Endod 2007; 33:552-8.
11. Ledesma-Montes C, Garces-Ortiz M, Rosales-Garcia G, Hernandez-Guerrero JC. Importance of mast cells in human periapical inflammatory lesions. J Endod 2004; 30:855-9.
12. Rodd HD, Boissonade FM. Comparative immunohistochemical analysis of the peptidergic innervation of human primary and permanent tooth pulp. Arch Oral Biol 2002; 47:375-85.
13. Okiji T, Jontell M, Belichenko P, Dahlgren U, Bergenholtz G, Dahlstrom A. Structural and functional association between substance P- and calcitonin gene-related peptide-immunoreactive nerves and accessory cells in the rat dental pulp. J Dent Res 1997; 76:1818-24.
14. Grutzner E, Garry M, Hargreaves K. Effect of injury on pulpal levels of immunoreactive substance P and immunoreactive calcifonin-gene-related peptide. J Endod 1992; 18:553-7.
15. Byers MR, Taylor PE. Effect of sensory denervation on the response of rat molar pulp to exposure injury. J Dent Res 1993; 72:613-8.
16. Cao YQ, Manth PW, Carlson EJ, Gillespie A, Epstein CJ, Basbaum AI. Primary afferent tachykinins are required to experience moderate to intense pain. Nature 1998; 392:390-4.
17. Zehnder M, Delaleu N, Du Y, Bickel M. Cytokine gene expression--part of host defence in pulpitis. Cytokine 2003; 22:84-8.
18. Rodd HD, Boissonade FM. Substance P expression in human tooth pulp in relation to caries and pain experience. Eur J Oral Sci 2005; 108:467-74.
19. Bowles WR, Withrow JC, Lepinski AM, Hargreaves KM. Tissue levels of immunoreactive substance P are increased in patients with irreversible pulpitis. J Endod 2003; 29:265-7.
20. Yamaguchi M, Kojima T, Kanekawa M, Aihara N, Nogimura A, Kasai K. Neuropeptides stimulate production of interleukin-1 beta, interleukin-6, and
summarize the many mediators and inflammatory cytokines identified in the dental pulp under different conditions.
These findings strengthen our understanding of the pathophysiology of pulpitis. Further studies are needed to extend a group of cytokines/chemokines involved with irreversibly inflamed dental pulps in association with pain.
REFERENCES
1. Cuello AC, Del FM, Paxinos G. The central and peripheral ends of the substance P-containing sensory neurones in the rat trigeminal system. Brain Res 1978; 152:499-500.
2. Widemar L, Bloom GD, Hellstrom S, Stenfors LE. Mast cells in the pars flaccida of the tympanic membrane. Acta Otolaryngol 1984; 414:115-7.
3. Masini E, Rucci L, Cirri-Borghi MB, Gianella E, Mannaioni PF. Stimulation and resection of vidian nerve in patients with chronic hypertrophic nonallergic rhinitis: effect of histamine content in nasal mucosa. Agents Actions 1986; 18:251-3.
4. Pezelj-Ribaric S, Anic I, Brekalo I, Miletic I, Hasan M, Simunovic-Soskic M. Detection of tumor necrosis factor alpha in normal and inflamed human dental pulps. Arch Med Res 2002; 33:482-4.
5. Tani-Ishii N, Wang CY, Stashenko P. Immunolocalization of bone-resorptive cytokines in rat pulp and periapical lesions following surgical pulp exposure. Oral Microbiol Immunol 1995; 10:213-9.
6. DelBalso AM, Nishimoura RS, Setterstrom JA. The effects of thermal and electrical injury on pulpal histamine levels. Oral Surg Oral Med Oral Pathol 1976; 41:110-113.
7. Janiszewski J, Bienenstock J, Blennerhassett MG. Picomolar doses of substance P trigger electrical responses in mast cells without degranulation. Am J Physiol 1994; 267:138-45.
8. Naesse EP, Schreurs O, Helgeland K, Schenck K, Steinsvoll S. Matrix metalloproteinases and their inhibitors in gingival mast cells in persons with and without human immunodeficiency virus infection. J Periodontal Res 2003; 38:575-82.
9. Avellan NL, Sorsa T, Tervahartiala T, Mantyla P,

8 EUROPEAN JOURNAL OF INFLAMMATION
1721-727X (2009)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties9
tumor necrosis factor-alpha in human dental pulp cells. Inflamm Res 2004; 53:199-204.
21. Buck S, Reese K, Hargreaves KM. Pulpal exposure alters neuropeptide levels in inflamed dental pulp and trigeminal ganglia: evaluation of axonal transport. J Endod 1999; 25:718-21.
22. Byers MR, Taylor PE, Khayat BG, Kimberly CL. Effects of injury and inflammation on pulpal and periapical nerves. J Endod 1990; 16:78-84.
23. Yamada Y. Role of substance P on neurogenic inflammation in the rat dental pulp and inferior lip. Fukuoka Shika Daigaku Gakkai Zasshi 1990; 17:198-214.
24. Hahn CL, Liewehr FR. Relationships between caries bacteria, host responses, and clinical signs and symptoms of pulpitis. J Endod 2007; 33:213-9.
25. Buzzi MG, Dimitriadou V, Theoharides TC, Moskowitz MA. 5-Hydroxytryptamine receptor agonists for the abortive treatment of vascular headaches block mast cell, endothelial and platelet activation within the rat dura mater after trigeminal stimulation. Brain Res 1992; 583:137-49.
26. Fristad I. Dental innervation: functions and plasticity after peripheral injury. Acta Odontol Scand 1997; 55:236-54.
27. Bletsa A, Heyeraas KJ, Haug SR, Berggreen E. IL-1 alpha and TNF-alpha expression in rat periapical lesions and dental pulp after unilateral sympathectomy. Neuroimmunomodulation 2004;
11:376-84.28. Karlsen TV, Bletsa A, Gjerde EA, Reed RK.
Lowering of interstitial fluid pressure after neurogenic inflammation in mouse skin is partly dependent on mast cells. Am J Physiol Heart Circ Physiol 2007; 292:1821-7.
29. Awawdeh L, Lundy FT, Shaw C, Lamey PJ, Linden GJ, Kennedy JG. Quantitative analysis of substance P, neurokinin A and calcitonin gene-related peptide in pulp tissue from painful and healthy human teeth. Int Endod J 2002; 35:30-6.
30. Awawdeh LA, Lundy FT, Linden GJ, Shaw C, Kennedy JG, Lamey PJ. Quantitative analysis of substance P, neurokinin A and calcitonin gene-related peptide in gingival crevicular fluid associated with painful human teeth. Eur J Oral Sci 2005; 110:185-91.
31. Hahn CL, Best AM, Tew JG. Cytokine induction by Streptococcus mutans and pulpal pathogenesis. Infect Immun 2000; 68:6785-9.
32. Karapanou V, Kempuraj D, Theoharides TC. Interleukin-8 is increased in gingival crevicular fluid from patientss with acute pulpitis. J Endod 2008; 34:148-51.
33. Kabashima H, Nagata K, Maeda K, Iijima T. Involvement of substance P, mast cells, TNF-alpha and ICAM-1 in the infiltration of inflammatory cells in human periapical granulomas. J Oral Pathol Med 2002; 31:175-80.
V. KARAPANOU ET AL.

8 EUROPEAN JOURNAL OF INFLAMMATION
1721-727X (2009)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties9
LIPOXIN A4 AND SERUM AMYLOID A DIFFERENTIALLY MODULATE PHOSPHOLIPASE D IN HUMAN FIBROBLAST-LIKE SYNOVIOCYTES
S. SODIN-SEMRL, G. ANTICO1, R. MIKUS2, K. LAKOTA, J. VARGA3 and S. FIORE4
University Medical Centre, Department of Rheumatology, Ljubljana, Slovenia; 1Northwestern University Feinberg School of Medicine, Department of Pathology, Chicago, IL, USA; 2University of Illinois at Chicago, Department of Medicine, Section of Rheumatology, IL, USA; 3Northwestern
University Feinberg School of Medicine, Division of Rheumatology, Chicago, IL, USA; Present address: 4Genentech Inc., Clinical Science Development ITGR, 1 DNA Way, M/S 211, S. San
Francisco, CA, USA
Received May 14, 2008 – Accepted March 20, 2009
Lipoxin A4 (LXA4) and serum amyloid A (SAA) are endogenous negative and positive modulators of inflammation, respectively. Both molecules bind the shared lipoxin A4 receptor (ALX) and elicit opposing effects on the production of inflammatory cytokines and matrix metalloproteinases. The aim of these studies is to examine the divergence of the intracellular signaling pathways triggered by lipid LXA4 (1 nM) and protein SAA (200 nM) ligands of ALX. Phospholipase D (PLD) is a phosphohydrolase enzyme that catalyzes the generation of phosphatidic acid (PA) from membrane phospholipids. Our results showed that in fibroblast-like synoviocytes, activation of PLD occurred only in response to LXA4, and not SAA. PA (30 µM) mimicked LXA4 and demonstrated inhibition of IL-8 production induced by SAA or interleukin-1β. In sharp contrast to LXA4, SAA confirmed the stimulation of IL-8 release as determined previously. Taken together, these findings suggest that two physiologic ligands sharing the common ALX receptor, LXA4 and SAA, differentially regulate the level of PLD activation and differentially modulate IL-8. These results may have important implications for understanding the regulation of inflammatory responses under physiologic and pathological conditions.
Mailing address: Dr S. Sodin-Semrl,Department of Rheumatology, University Medical Centre,Vodnikova 62, 1000 Ljubljana, SloveniaTel: ++386 1 522 5596 Fax: ++386 1 522 5598e-mail: [email protected]
Key words: inflammation, lipid mediators, lipoxin, signal transduction, phosphatidic acid
Joint inflammation results in the development of synovitis and subsequent joint destruction. Chronic inflammation is a consequence of a loss of the balance between pro- and anti-inflammatory mediators. Cytokines are fundamental regulators of the inflammatory response. Cytokines such as interleukin (IL)-1ß and chemokines, such as IL-8, recruit inflammatory cells into the joint, resulting in the local generation of cartilage and bone-degrading enzymes, and formation of the rheumatoid pannus.
Anti-inflammatory cytokines such as IL-4, IL-10 and IL-13 are present in rheumatoid joints, however in progressive rheumatoid arthritis their levels may be too low to neutralize the deleterious effects of pro-inflammatory cytokines (1).
Lipoxins are endogenous lipid mediators that block the activation of human fibroblast-like synoviocytes (FLS) and dampen the effects of inflammatory agonists, leading to the resolution of the inflammatory response (2) and promotion of
Vol. 7, no. 1, 9-17 (2009)

10 11Eur. J. Inflamm.
wound healing (3-5). Lipoxins exert their biological activities through the lipoxin A receptor (ALX). Signaling via the ALX receptor, LXA4 induces anti-inflammatory responses such as inhibition of neutrophil infiltration, IL-6 and IL-8 production, and secretion of matrix metalloproteinase (6-9).
The acute phase protein serum amyloid A (SAA) is an endogenous mediator of inflammatory responses. Like LXA4, SAA is also a ligand for ALX (10). Human SAA belongs to a multigene family of inducible SAA1 and SAA2 (SAA1/2), SAA3 is a pseudogene, whereas SAA4 is generally considered as constitutively expressed. The levels of SAA are up-regulated in inflammatory synovitis (11) and its plasma concentration can increase 1000-fold, reaching as high as 80 μM or 1 mg/mL during the acute-phase response. In cultured mesenchymal cells SAA induces chemotactic activity (12) and the production of IL-8 and matrix metalloproteinase enzymes, which is mediated via activation of the NF-κB signal transduction pathways (9, 13). Messenger RNA (mRNA) for SAA1/2 and ALX are detectable in macrophages and endothelial cells isolated from rheumatoid synovial tissue (14) and the expression of SAA1/2 and of its receptors is up-regulated by proinflammatory cytokines, indicating a potential functional role in mediating inflammatory responses. Many studies have shown that SAA plasma levels are also significantly elevated in patients with a broad spectrum of chronic inflammatory diseases, such as atherosclerosis, rheumatoid arthritis, Crohn’s disease, diabetes and ankylosing spondylitis (15).
Phospholipase D (PLD) is a phosphohydrolase enzyme that catalyzes the generation of phosphatidic acid (PA) from membrane phospholipids. The activity of PLD is induced by LXA4 and other agonists (16) in HL-60 cells, and has been shown to be mediated by small G proteins such as RhoA, Rac, Arf and Ras (17-19). In order to determine whether PLD activity in FLS is also mediated via Rho, a dominant negative mutant was included in our study.
Phosphatidic acid activates protein phophatase-2A (PP-2A), a target and conveyor of biological signals (20-21). By inactivating IκB kinase (IκK), PP-2A blocks NF-κB activity (22). Taken together, these observations led us to speculate that activation of PLD in fibroblasts could act as a molecular switch regulating the generation of anti-inflammatory
versus pro-inflammatory responses. The ALX receptor ligands LXA4 and SAA could determine the outcome of inflammatory events by regulating PLD activation. To explore this notion and in order to elucidate inflammatory events in the synovium, we investigated the mechanism underlying the divergent cellular responses elicited by LXA4 and SAA in FLS by focusing on early inflammatory events such as PLD activation and phosphatidic acid production with PP-2A activation, and late events, such as production of IL-8. The results indicated that LXA4 and SAA signaling through the shared receptor ALX elicited opposing effects on PLD activity in human FLS. This divergence in inflammatory responses elicited by the ALX receptor ligands LXA4 and SAA could have profound implications in controlling homeostasis and chronic inflammatory responses in arthritis.
MATERIALS AND METHODS
MaterialsSynthetic LXA4 was obtained from Biomol
Inc., Plymouth Meeting, PA, USA, whereas PA and phosphatidylethanol (PEt) were obtained from Avanti Polar Lipids, Alabaster, AL, USA. LXA4 was added to the cultures at a final concentration of 10–9 M unless otherwise stated. Eagle’s minimal essential medium (EMEM) and other cell culture reagents were from BioWhittaker (Walkersville, MD, USA). Human recombinant IL-1β (final concentration 0.5 ng/ml) was from Boehringer Mannheim (Indianapolis, IN, USA) and human recombinant Apo-SAA (final concentration 200 nM) was from Peprotech (Rocky Hill, NJ, USA). Apo-SAA corresponds to SAA-1α, one of the major SAA isoforms in the serum, except for the addition of a methionine at the NH2 terminus as well as the substitution of aspartic acid for asparagine at position 60, which appears in the SAA2 isoform. For the appropriate nomenclature of SAA and its isoforms please refer to Sipe J. (23). Both LXA4 and human recombinant SAA were used at physiological concentrations of 1 nM and 200 nM, respectively.
Cell culturePrimary cultures of human FLS were generated from
explants of arthroscopic synovial biopsies of injured patients (24). All studies were performed in accordance with the Institutional Research Board (University of Illinois at Chicago, USA) approved protocols. Cells were grown under standard 5% CO2 humidified atmosphere at 37ºC in EMEM containing 10% Fetal Bovine Serum
S. SODIN-SEMRL ET AL.

10 11Eur. J. Inflamm.
(FBS), penicillin (100 U/ml), streptomycin (100 µg/ml) and vitamin supplement, and used for experiments at low passages (between 7-11). Twenty-four hours prior to each experiment, fresh media with 5% FBS were added to the cultures. Chinese hamster ovary (CHO) cells (donation from Dr. Varga’s laboratory) were grown in alpha-MEM containing 10% FBS, penicillin (100 U/ml) and streptomycin (100 µg/ml).
ELISAConfluent cultures of FLS were incubated with PA or
PEt (both at 30 µM) for 30 min at 37°C prior to addition of IL-1β, SAA or LXA4. Supernatants were collected 24 h later, centrifuged at 1,500 x rpm for 5 min, aliquoted and stored at -20ºC. Samples were thawed at room temperature and IL-8 was quantified using an ELISA kit following the manufacturer’s instructions (Biosource, Camarillo, CA, USA). Cultures were equilibrated with the vehicle (0.01% ethanol) at the time of experiment treatments.
Phospholipase D (PLD) Activation Assay Confluent FLS were transiently transfected with
pcDNA3 or pcDNA3 expressing a Rho dominant negative mutant, (pcDNA3-Rho T(19)N) as described previously (25-26). Cultures were labeled with 3H-palmitic acid (5 µCi/mL) at 37°C for 120 min. Samples were centrifuged twice at 1200 rpm for 10 min, cells were resuspended in Dulbecco’s phosphate buffer (1x DPBS), and aliquots (2x106cells/sample) were added to DPBS-containing agonists with or without 0.5% EtOH (or indicated final % volume). In selected experiments FLS were first transfected with Rho dominant negative (RhoDN) construct or control before addition of agonists. Following indicated periods of incubation, methanol/chloroform solution was added to cultures, phospholipids were extracted by a modified Bligh and Dyer procedure, and spotted on TLC plates as previously reported (16). PEt bands identified by co-migration with a synthetic standard were scraped from the TLC plates, and their radioactive content was measured by scintillation counting. PEt for each sample was normalized by the percent recovery of 14C-chloramphenicol as internal standard before phospholipid extraction.
PP-2A assaysThe in vitro phosphorylation reactions were performed
as previously described (20). Briefly, 1 mg of histone, type IIIss from calf thymus (Sigma, St. Louis, MO, USA) was used as substrate and 250 units of PKA (Protein kinase A, catalytic subunit from bovine heart, Sigma, St. Louis, MO, USA) was added to reaction mixtures which were incubated for 2 h at 37°C. Precipitated protein pellets were air dried and dissolved in 50 mM Tris-HCl, pH 7.4. In order to monitor the efficiency of the phosphorylation
reactions, 1 µl was taken from the reaction tubes and cpms were counted. The phosphatase assay was performed with 10 mU of PP-2A and an equal concentration of (32P)-labeled substrate. PA (10 µM), PEt (10 µM) and LXA4 (1 nM) were delivered to the reaction tubes in a 10 µl volume. Control reactions received an equal volume of 50 mM Tris-HCl, pH 7.4.
IL-8 promoter-reporter gene construct and transient transfection experiments
Transient transfections were performed with the pXP2 basic luciferase reporter vector (pIL8-Luc) (generous gift of Dr. N. Mukaida, Kanazawa University, Japan). This construct contains a 1.48 kb fragment of the human IL-8 gene promoter harboring an NF-κB binding site (GGAATTTCCTC) located between -80 to -69 bp (27). The pXP2 vector containing a SV40 promoter served as a control to adjust for variation in transfection efficiency and well to well number. CHO cells were grown to ~80% confluence in 12-well plates, and transfected following the manufacturer’s specifications, using FuGENE 6 (Roche Diagnostics Corp., Indianapolis, IN, USA). Dual-luciferase reporter assay system (Promega, Madison, WI, USA) was used for quantitative analysis of the IL-8 promoter activity.
RESULTS
Phosphatidic acid inhibits IL-1β -induced stimulation of IL-8 secretion
First, we examined the effect of PA, the product of PLD activity leading to downstream targets, on inflammatory responses elicited by IL-1β or SAA. Confluent cultures of normal human FLS were incubated with IL-1β and SAA in the presence or absence of PA or PEt (the trapping product of the PLD catalysis, leading to a dead-end of the pathway). The regulation of IL-8 secretion by PEt and PA was compared. The results shown in Table I indicate that incubation of FLS with IL-1β or SAA resulted in marked stimulation of IL-8 secretion, as expected. We have shown previously that LXA4 abrogated the IL-1β-induced stimulation (8). Remarkably, PA also caused inhibition of IL-1β or SAA-induced stimulation of IL-8, thus mimicking the effect of LXA4 (Table I). In contrast to PA, PEt failed to abrogate IL-1β or SAA-induced responses. Since both LXA4 and SAA signal through the shared ALX receptor, these two ALX ligands could participate in the pathogenesis of inflammatory synovitis by

12 13Eur. J. Inflamm.
differentially regulating the production of IL-8.
Differential activation of PLD by LXA4 and SAAPhospholipase D transient activation by LXA4
has been previously demonstrated in cells of myeloid lineage (16). The activity of LXA4 and SAA toward PLD activation was here examined in regard to FLS ability to similarly generate PLD products. Cultures of FLS were incubated for 48 h, and then labeled with 3H-palmitate before adding LXA4 and SAA to determine whether differences exist between lipid (LXA 4) and protein (SAA) ligands of ALX-mediated signaling pathways in inducing a PLD response. Cells were harvested at the indicated time points and PLD activation was determined. The results indicated that LXA4 induced activation of PLD, as shown by marked accumulation of the phosphatidylethanol trapping product PEt (Fig. 1). A similar response was induced by incubation of FLS
with the calcium ionophore A23187, which was used as a positive control.
In striking contrast, however, SAA failed to induce PLD activation. Next, we investigated whether PLD activation induced by LXA4 was mediated via the small GTPase protein RhoA. For this purpose, FLS were transiently transfected with a dominant negative form of RhoA, and the modulation of PLD activity by A23187, LXA4 or SAA was determined. Hence, we observed that the over-expression of dominant negative RhoA was able to knock out the LXA4-induced PLD activity (Fig. 1) as well as the ionophore A23187 PLD activity, suggesting that both are dependent on RhoA.
The results showed that LXA4 induced a stimulation of PLD activity, whereas SAA had no effect (Fig. 1). The LXA4 response was biphasic; a rapid early peak was noted at 2 min, followed by a delayed peak at 90 min. This response pattern is comparable to LXA4-dependent activation of PLD in HL-60 cells stably expressing ALX (16). These results might be due to desensitization or signal transduction coupling in heptahelical receptors (25-26).
Taken together, these results indicate that whereas SAA fails to induce PLD activity in FLS, LXA4 enhanced PLD activity, and the response was abrogated by transfection with dominant negative RhoA, indicating the functional requirement for the small GTPase in mediating the LXA4 response.
PA, but not LXA4 or PEt induces PP-2A activityNext, the molecular pathways induced by PLD
activation were investigated in FLS. Previous studies have shown that PA exerts potent effects on the activity of protein phosphatases (20). To determine whether LXA4 could directly regulate protein phosphatase activity without interaction with ALX receptor, cell-free dephosphorylation assays were performed. We compared the ability of LXA4 and PA and PEt to directly modulate PP-2A catalytic subunit activity by in vitro phosphorylation reaction assays as previously described (20). The results of the dephosphorylation assays indicated that incubation with PA resulted in a dramatic induction of PP-2A catalysis (Fig. 2). In contrast, LXA4 had no effect. These results, indicating that PA can serve as a potent endogenous activator of PP-
IL-8 (pg/ml) Control 25 ± 7.2
PA 11.5 � 0.1 PEt 26 � 1.3
IL-1� 5717.1 � 474.9 IL-1� + PA 3786.5 � 77.0 IL-1� + PEt 6085.9 � 113.2
Control 45 ± 26.5 PA 45.2 ± 20.4 PEt 69.8 ± 35.1
SAA 2586.1 ± 1316.3 SAA + PA 1666.4 ± 975 SAA + PEt 2153.7 ± 1153.7
Table I. PA, but not PEt, mimics the effect elicited by LXA4 on IL-1� and SAA-induced IL-8 production. Fibroblast-like synovial cells were incubated in presence or absence of PA and PEt (both at 30 �M at 37°C) for 30 min prior to addition of IL-1�(0.5 ng/ml) and SAA (200 nM). After 24 h, incubations were stopped and culture supernatants were harvested and subjected to IL-8 ELISA. Results indicate that exogenous PA, but not PEt, mimicked the inhibitory effects of LXA4 on IL-1� and SAA-induced release of IL-8 levels. The results are the mean � SD from four separate experiments with duplicate determinations.
Table I. PA, but not PEt, mimics the effect elicited by LXA4 on IL-1β and SAA-induced IL-8 production.
S. SODIN-SEMRL ET AL.
Fibroblast-like synovial cells were incubated in presence or absence of PA and PEt (both at 30 µM at 37°C) for 30 min prior to addition of IL-1β (0.5 ng/ml) and SAA (200 nM). After 24 h, incubations were stopped and culture supernatants were harvested and subjected to IL-8 ELISA. Results indicate that exogenous PA, but not PEt, mimicked the inhibitory effects of LXA4 on IL-1β and SAA-induced release of IL-8 levels. The results are the mean ± SD from four separate experiments with duplicate determinations.

12 13Eur. J. Inflamm.
2A activity, are consistent with recent studies (20). These observations support a functional correlation between LXA4 inhibitory activities, PA levels, PP-2A activity and IL-8 secretion demonstrated in Table I.
Divergent regulation of IL-8 gene promoter activityTo further investigate the divergent regulation of
FLS inflammatory responses by SAA and LXA4 via the shared ALX receptor, we next investigated the regulation of IL-8 gene promoter activity by these two ligands. For this purpose, CHO cells were first stably transfected with ALX. Next, ALX-expressing cells were transiently transfected with pIL8-Luc, a construct harboring the human IL-8 gene promoter that contains consensus NF-κB and AP-1 binding sequences (27). Transfected CHO cells were then incubated with SAA or IL-1β in the presence and
absence of LXA4 or PA respectively following a 24 h incubation, cultures were harvested and whole cell lysates were assayed for luciferase activities. The results showed that IL-8 promoter activity was markedly induced by SAA, as well as by IL-1β, in transfected CHO cells (Fig. 3). In the presence of LXA4 or PA, IL-8 promoter stimulation by IL-1β/SAA was markedly reduced. Absence of a functional NF-κB consensus sequence in the pIL8-LucNF-kBmut construct (containing a mutated NF-κB binding sequence) was associated with a loss of both positive and negative regulation of promoter activity by IL-1β, SAA or LXA4 (Fig. 3). Together, these results indicate that ALX-mediated regulation of IL-8 gene expression by SAA or by LXA4/PA involved modulation of the transcriptional activities of the gene.
DISCUSSION
Previous studies have addressed ALX receptor binding using aspirin-triggered lipoxins and select peptides to evoke ligand-specific responses in polymorphonuclear cells (28). This same group utilized chimera of LTB4R/ALX receptors to show that a portion of the transmembrane domain of ALX proximal to the cytoplasmic membrane surface was required for LXA4 binding. LXA4 (MW 452D) could intercalate in a pseudopore formed by the seven-transmembrane domains of the receptor, similarly as retinol binds rhodopsin (29). In contrast, the much larger SAA molecule (MW>12KD) is thought to interact with multiple extracellular domains of ALX receptor (10).
The Kd values for LXA4 (0.1-1.0 nM) (16) and SAA (~40 nM) (10) are markedly different, as well as their estimated Kon/off (LXA4 >>> SAA) (30), potentially resulting in radically different times for receptor conformational changes to occur. However, further studies will be necessary to unambiguously resolve the model of ligand-receptor interactions underlying the profoundly different activities elicited by SAA and LXA4 via ALX. Isotopically-labeled SAA and LXA4 will be necessary to determine if these two distinct ALX ligands follow a kinetic mechanism of competitive or non-competitive receptor level antagonism.
The different pathways of LXA4 and SAA
-2000
-1000
0
1000
2000
3000
4000
5000
Pet
(cpm
)
Time (min)
0.5 2 5 30 90
Fig. 1.
Fig. 1. Lipoxin A4, but not SAA, activates PLD via ALX. Cultures of human FLS were stably transfected with pcDNA3 plasmid (full symbols,=, <,5) or a dominant negative form of RhoA (RhoDN) (pcDNA3-Rho-T(19)N, (empty symbols, m, ¨, ê). After 48 h incubation, cultures were labeled with 3H-palmitate, followed by addition of 2.5 µM A23187 (ê), 1 nM LXA4 (¨) or 200 nM SAA (m). At the indicated periods of incubation, cultures were harvested and phospholipids extracted and analyzed (see Materials and Methods). Radioactive content of TLC eluted material co-migrating with authentic PEt was next determined by β-scintillation counting. Results are the means ± SD of three separate experiments with duplicate determinations.

14 15Eur. J. Inflamm.
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
Substrate
Substrate+PP-2A
PP-2A+LXA 4
PP-2A+PEt
PP-2A+PA
PP-2AAc tivity(32 PRelease)
Fig. 2.
Fig. 2. PA, not PEt or LXA4, regulates the activity of PP-2A in vitro. An in vitro phosphorylation reaction was performed with 1 mg of Histone type IIIss as substrate incubated with 250 units of Protein kinase A (bovine heart) in presence of γ-32P-ATP. The Histone substrate was TCA precipitated and washed in acetone. The pellets were air dried and dissolved in 1 ml of 50 mM Tris-HCl, pH 7.4. Next, histone substrate (88 µg/sample) was incubated for 15 min at 30°C in Tris buffer containing 10 mU of protein phosphatase 2A (PP-2A) in presence or absence of LXA4 (1 nM), PEt or PA (10 µM each). The reactions were terminated with 0.1 ml of 1 mM KH2PO4 in 1N H2SO4 and 0.3 ml of 2% ammonium molybdate and free Pi determined. Results are the mean ± SD of values obtained from a representative experiment with triplicate determinations.
0
100
200
300
400
500
600
LUC
IFE
RA
SE
(Arb
itrar
y U
nits
)
SAA+PA
IL-1�+PA
SAAIL-1�PALXA4EtOH IL-1�+LXA4
Fig. 3.
Fig. 3. Modulation of pIL8-LUC promoter activity by LXA4, SAA and IL-1β. CHO cells were grown to 70-80% confluency in 24 well plates, and then transiently transfected with wildtype or mutated IL-8 promoter luciferase gene constructs (NF-κB wildtype, white bars, NF-κB mutated, gray bars). 48 h later, cultures were incubated with PA (30 µM), SAA (200 nM), IL-1β (0.5 ng/ml) or LXA4 (10-9M) for an additional 24 h, followed by assaying cell lysates for their luciferase activities. Results are the means ± SD of three separate experiments with triplicate determinations.
S. SODIN-SEMRL ET AL.

14 15Eur. J. Inflamm.
downstream of ALX have been previously addressed in neutrophils (31) and in FLS (9, 13). Mobilization of intracellular Ca2+ and activation of mitogen-activated protein kinases ERK1/2 was examined in neutrophils, where SAA-induced calcium mobilization and LXA4 failed to induce phosphorylation of ERK 1/2 (31). In FLS, ALX receptor activation by LXA4 or SAA resulted in opposite regulation of IL-8 production and NF-κB activity (9, 13). He et al. (15) reported that there are currently 3 known receptors involved in SAA’s proinflammatory effects: FPRL1/ALX, which was shown to be responsible for SAA-induced chemotaxis, IL-8 secretion, matrix metalloproteinase production and NF-κB and AP-1 activation; receptor for advanced glycation end products (RAGE), which was reported to mediate SAA-induced tissue factor expression; and CLA-1 (CD36 and LIMPII analogous–1, a human ortholog of rodent scavenger receptor BI), which was found to facilitate SAA-triggered proinflammatory downstream signaling pathways, such as extracellular signal-regulated kinase (ERK) and p38 activation. The same group reports that acute-phase proteins, such as SAA, could be danger-signaling molecules which play an active role in the regulation of inflammation and innate immunity. SAA, when recognized by the host, may initiate tissue-controlled immune responses, and toll-like receptor 2 was found to be critically required for these SAA-stimulated activities (15).
PLD is involved in inflammation and arachidonate release (32-36). The sensitivity to RhoDN in our study (Fig. 1) indicates that the inducible PLD isoform (requiring Rho), is involved in the LXA4-dependent PLD activation in FLS. Furthermore, LXA4 has previously been shown to stimulate RhoA and cause actin stress fiber formation in monocytes and macrophages (37).
PA, the secondary messenger of PLD and its immediate metabolites diacylglycerol and lyso-PA, affect numerous cellular responses (36, 38). The potential role of PP-2A in inhibiting IκK complex and leading to reduced NF-κB nuclear localization via stabilization of IκB has been reported (22). The importance of PP-2A as inhibitor of NF-κB activation was established previously by showing that okadaic acid, an inhibitor of serine/threonine phosphatases, could activate NF-κB and induce a dramatic increase in IL-8 secretion in HL-60 cells (39).
In summary, the results presented here indicate for the first time that, in striking contrast to lipid-derived LXA4, SAA does not activate PLD to generate PA in human FLS, despite the fact that these two inflammatory signals share a common cellular receptor. We postulate that the differential PA generation leads to opposing effects on NF-κB DNA binding activity in FLS (13) and ultimately IL-8 release. These opposing events could have a significant impact on regulation of the balance between pro- and anti-inflammatory mediators in arthritic joints.
ACKNOWLEDGEMENTS
We are grateful to Dr. Mark Hutchinson and the staff of University of Illinois Hospital, Orthopedic Surgery Department, Chicago, IL for their help in the acquisition of biopsy material, and to Prof. Naofumi Mukaida (Kanazawa University Cancer Research Institute, Kanazawa, Japan) for supplying IL-8 luciferase reporter constructs.
Support for this study was obtained by the NIH-NIAMS (SF AR45931) and Arthritis Foundation (SSS National Postdoctoral Fellowship).
DISCLOSURE. Dr. S. Fiore is currently employed with Genentech, Inc. (USA) and contributed to this work prior to engagement with Genentech, Inc. Dr. G. Antico is currently employed with Bristol-Myers Squibb (USA) and contributed to this work prior to engagement with Bristol-Myers Squibb. R. Mikus is presently employed at Largo Medical Centre/Sun Coast Hospital, Largo, FL, USA.
REFERENCES
1. Isomaki P, Punnonen J. Pro- and anti-inflammatory cytokines in rheumatoid arthritis. Ann Med 1997; 29:499-507.
2. Serhan CN. Resolution phases of inflammation: novel endogenous anti-inflammatory and proresolving lipid mediators and pathways. Annu Rev Immunol 2007; 25:101-37.
3. Gewirtz AT, Neish AS, Madara JL. Mechanisms of active intestinal inflammation and potential down-regulation via lipoxins. Adv Exp Med Biol 2002; 507:229-36.
4. Bonnans C, Vachier I, Chavis C, Godard P, Bousquet J, Chanez P. Lipoxins are potential endogenous anti-
16 17Eur. J. Inflamm.
inflammatory mediators in asthma. Am J Respir Crit Care Med 2002; 165:1531-5.
5. Serhan CN, Levy BD, Clish CB, Gronert K, Chiang N. Lipoxins, aspirin-triggered 15-epi-lipoxin stable analogs and their receptors in anti-inflammation: a window for therapeutic opportunity. Ernst Schering Res Found Workshop 2000; 31:143-85.
6. Sodin-Semrl S, Spagnolo A, Barbaro B, Varga J, Fiore S. Lipoxin A4 counteracts synergistic activation of human fibroblast-like synoviocytes. Int J Immunopathol Pharmacol 2004; 17:15-25.
7. Takano T, Fiore S, Maddox JF, Brady HR, Petasis NA, Serhan CN. Aspirin-triggered 15-epi-lipoxin A4 (LXA4) and LXA4 stable analogues are potent inhibitors of acute inflammation: Evidence for anti-inflammatory receptors. J Exp Med 1997; 185:1693-1704.
8. Sodin-Semrl S, Taddeo B, Tseng D, Varga J, Fiore S. Lipoxin A4 inhibits IL-1 beta-induced IL-6, IL-8, and matrix metalloproteinase-3 production in human synovial fibroblasts and enhances synthesis of tissue inhibitors of metalloproteinases. J Immunol 2000; 164:2660-6.
9. Fiore S, Sodin-Semrl S, Kang Y, Varga J. Activation of LXA4R by LXA4 or serum amyloid A results in opposite regulation of NF-κB DNA binding in human synovial fibroblasts. Arthritis Rheum 2000; 43:S158.
10. Su SB, Gong W, Gao JL, Shen W, Murphy PM, Oppenheim JJ, Wang JM. A seven-transmembrane, G protein-coupled receptor, FPRL1, mediates the chemotactic activity of serum amyloid A for human phagocytic cells. J Exp Med 1999; 189:395-402.
11. Vallon R, Freuler F, Desta-Tsedu N, et al. Serum amyloid A (apoSAA) expression is up-regulated in rheumatoid arthritis and induces transcription of matrix metalloproteinases. J Immunol 2001; 166:2801-7.
12. Patel H, Fellowes R, Coade S, Woo P. Human serum amyloid A has cytokine-like properties. Scan J Immunol 1998; 48:410-8.
13. Sodin-Semrl S, Spagnolo A, Mikus R, Barbaro B, Varga J, Fiore S. Opposing regulation of interleukin-8 and NF-kappaB responses by lipoxin A4 and serum amyloid A via the common lipoxin A receptor. Int J Immunopathol Pharmacol 2004; 17:145-56.
14. O’Hara R, Murphy EP, Whitehead AS, FitzGerald O, Breshihan B. Local expression of the serum amyloid A and formyl peptide receptor-like 1 genes in synovial tissue is associated with matrix metalloproteinase production in patients with inflammatory arthritis. Arthritis Rheum 2004; 50:1788-99.
15. He RL, Zhou J, Hanson CZ, Chen J, Cheng N, Ye RD. Serum amyloid A induces G-CSF expression and neutrophilia via Toll-like receptor 2. Blood 2009; 113:429-37.
16. Fiore S, Romano M, Reardon EM, Serhan CN. Induction of functional lipoxin A4 receptors in HL-60 cells. Blood 1993; 81:3395-3403.
17. Exton JH. Regulation of phospholipase D. FEBS Lett 2002; 531:58-61.
18. Powner DJ, Wakelam MJ. The regulation of phospholipase D by inositol phospholipids and small GTPases. FEBS Lett 2002; 531:62-4.
19. Cummings R, Parinandi N, Wang L, Usatyuk P, Natarajan V. Phospholipase D/phosphatidic acid signal transduction: role and physiological significance in lung. Mol Cell Biochem 2002; 234:99-109.
20. Kishikawa K, Chalfant CE, Perry DK, Bielawska A, Hannun YA. Phosphatidic acid is a potent and selective inhibitor of protein phosphatase 1 and an inhibitor of ceramide-mediated responses. J Biol Chem 1999; 274:21335-41.
21. Goldberg Y. Protein phosphatase 2A: who shall regulate the regulator? Biochem Pharmacol 1999; 57:321-8.
22. DiDonato JA, Hayakawa M, Rothwarf DM, Zandi E, Karin M. A cytokine-responsive IkappaB kinase that activates the transcription factor NF-kappaB. Nature 1997; 388:548-54.
23. Sipe J. Revised nomenclature for serum amyloid A (SAA). Nomenclature Committee of the International Society of Amyloidosis. Part 2. Amyloid 1999; 6:67-70.
24. Croft D, McIntyre P, Wibulswas A, Kramer I. Sustained elevated levels of VCAM-1 in cultured fibroblast-like synoviocytes can be achieved by TNF-α in combination with either IL-4 or IL-13 through increased mRNA stability. Am J Pathol 1999; 154:1149-58.
25. Kang Y, Sodin-Semrl S, Varai G, Varga J, Taddeo
S. SODIN-SEMRL ET AL.
16 17Eur. J. Inflamm.
B, Fiore S. Impact of selected serine, threonine and tyrosine mutations in the intracellular domains of the human lipoxin A4 receptor on desensitization and signaling. Arthritis Rheum 2000; 42:S191.
26. Kang Y, Taddeo B, Varai G, Varga J, Fiore S. Mutations of serine 236-237 and tyrosine 302 residues in the human lipoxin A4 receptor intracellular domains result in sustained signaling. Biochem 2000; 39:13551-7.
27. Jung YD, Fan F, McConkey DJ, et al. Role of P38 MAPK, AP-1, and NF-kappaB in interleukin-1beta-induced IL-8 expression in human vascular smooth muscle cells. Cytokine 2002; 18:206-13.
28. Chiang N, Fierro IM, Gronert K, Serhan CN. Activation of lipoxin A(4) receptors by aspirin-triggered lipoxins and select peptides evokes ligand-specific responses in inflammation. J Exp Med 2000; 191:1197-1208.
29. Stenkamp RE, Teller DC, Palczewski K. Crystal structure of rhodopsin: a G-protein-coupled receptor. Chem Biochem 2002; 3:963-7.
30. Fiore S, Ryeom SW, Weller PF, Serhan CN. Lipoxin recognition sites. Specific binding of labeled lipoxin A4 with human neutrophils. J Biol Chem 1992; 267:16168-76.
31. He R, Sang H, Ye RD. Serum amyloid A induces IL-8 secretion through a G protein-coupled receptor, FPRL1/LXA4R. Blood 2003; 101:1572-81.
32. Ueno N, Murakami M, Kudo I. Functional crosstalk between phospholipase D(2) and signaling phospholipase A(2)/cyclooxygenase-2-mediated
prostaglandin biosynthetic pathways. FEBS Lett 2000; 475:242-6.
33. Kiel D, Feinmark SJ. Phospholipase D activity regulates the binding of leukotriene B4 to human polymorphonuclear leukocytes. J Pharmacol Exp Ther 1996; 278:645-53.
34. Steed PM, Chow AH. Intracellular signaling by phospholipase D as a therapeutic target. Curr Pharm Biotechnol 2001; 2:241-56.
35. Jenkins GM, Frohman MA. Phospholipase D: a lipid centric review. Cell Mol Life Sci 2005; 62:2305-16.
36. Natarajan V, Jayaram HN, Scribner WM, Garcia JG. Activation of endothelial cell phospholipase D by sphingosine and sphingosine-1-phosphate. Am J Respir Cell Mol Biol 1994; 11:221-9.
37. Maderna P, Cottell DC, Berlasconi G, Petasis NA, Brady HR, Godson C. Lipoxins induce actin reorganization in monocytes and macrophages but not in neutrophils: differential involvement of rho GTPases. Am J Pathol 2002; 160:2275-83.
38. Exton JH. Phospholipase D-structure, regulation and function. Rev Physiol Biochem Pharmacol 2002; 144:1-94.
39. Sonoda Y, Kasahara T, Yamaguchi Y, Kuno K, Matsushima K, Mukaida N. Stimulation of interleukin-8 production by okadaic acid and vanadate in a human promyelocyte cell line, an HL-60 subline. Possible role of mitogen-activated protein kinase on the okadaic acid-induced NF-kappaB activation. J Biol Chem 1997; 272:15366-72.

EUROPEAN JOURNAL OF INFLAMMATION
1721-727X (2009)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties19

EUROPEAN JOURNAL OF INFLAMMATION
1721-727X (2009)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties19
CAROTID INTIMA-MEDIA THICKNESS AND ANTI-PHOSPHOLIPID ANTIBODIES IN PATIENTS WITH SYSTEMIC LUPUS ERYTHEMATOSUS
C. ROLLINO, C. MASSARA, L. BESSO1, C. MARCUCCIO1, M. MANGANARO2, T. BERTERO3, B. MONTARULI4, G. BELTRAME, M. FERRO, G. QUATTROCCHIO,
F. ELIA and F. QUARELLO
Division of Nephrology, Ospedale S.G. Bosco, Turin; 1Nephrology, Ospedale S.G. Battista, Turin; 2Nephrology, 3Immunology, Ospedale Mauriziano, Turin; 4Analysis Laboratory, Ospedale Valdese,
Turin, Italy
Received 15 August, 2008 – Accepted 15 December, 2008
An increase in mortality due to accelerated atherosclerosis has been reported in patients affected with Systemic Lupus Erythematosus (SLE). Anti-phospholipid antibodies (aPA) may play a pathogenetic role in the development of atherosclerosis. We measured carotid intima-media thickness (IMT), as a surrogate parameter of atherosclerosis, by B-mode ultrasound examination in 42 patients affected with SLE (11 men and 31 women) and in 42 healthy age- and sex-matched subjects. Lupus Anticoagulant (LA) (APTT sensitive, silica clotting time, DRVVT), Anti-cardiolipin antibodies (ACA) IgG and IgM, anti-β2glycoprotein 1 (anti-β2GP1) IgG and IgM and anti-prothrombin (anti-PT) IgG and IgM in ELISA (Orgentec Bouty) were also detected. IMT was 0.538±0.128 mm (0.310-0.866 mm) in SLE vs 0.473±0.084 mm in healthy subjects (-p 0.003-). IMT correlated with patients’ age (p<0.005) and with C Reactive Protein (CRP) (p<0.005), but not with years of disease, hypertension, number of anti-hypertensive drugs, total cholesterol, serum creatinine and proteinuria. Sixteen patients (38%) had aPL: 12 LA, 6 ACA IgG, 4 ACA IgM, 4 anti-β2GP1 IgG, 3 anti-β2GP1 IgM, 2 anti-PT IgG and 1 anti-PT IgM. IMT was not statistically correlated with aPA. Positive and negative aPA patients only differed as regards glomerular filtration rate (76 ml/min vs 113 ml/min - p<0.01-). Frequency of aPA positivity was 50% in patients with IMT >0.600 mm and 33.3% in those with IMT <0.600 mm. If LA positivity was considered separately, it was 41.6% in patients with IMT >0.600 mm and 23.3% in patients with IMT <0.600 mm. Among the 5 patients with IMT >0.7 mm, 2 had LA positivity (40%) vs 10/37 (27%) of those with minor carotid thickness. In conclusion, IMT, a surrogate parameter of atherosclerosis, was correlated with patients’ age and CRP and not with presence of aPA, even though, in the group of patients with greater IMT, there was a non-significant higher proportion of positivity for anti-phospholipid antibodies, in particular for Lupus Anticoagulant.
Mailing address: Dr Cristiana Rollino,Divisione di Nefrologia e Dialisi, P.zza Donatore di Sangue 3,10154 Torino, ItalyTel: ++390112402287Fax: ++390112402458e-mail: [email protected]
An increase in mortality due to accelerated atherosclerosis has been reported in patients affected with Systemic Lupus Erythematosus (SLE).
Incidence of myocardial infarction is fifty times as high as in age-matched controls among young patients (1) and thirty percent of deaths in SLE are
Key words: anti-phospholipid antibodies, atherosclerosis, intima-media thickness, lupus
Vol. 7, no. 1, 19-23 (2009)

20 21Eur. J. Inflamm.
- Lupus anticoagulant (LA)- Anticardiolipin antibodies (aCL)- Anti-prothrombin antibodies (aPT)- Anti-ß2glycoprotein 1 antibodies (aß2GP1) These tests were compared with those of sera of 110
healthy subjects (mean age 40.3 years) used as controls.
The criteria proposed by the SSC Subcommittees for Standardization of Lupus Anticoagulant were used for the diagnosis of the phospholipids-dependent inhibitors of coagulation (9).
The following panel of coagulation tests was performed for each patient and control plasma: aPTT (aPTT-SP, IL), Silica Clotting Time (SCT, homemade), Dilute Russel’s Viper Venom Time (DRVVT, American Diagnostica). The prolongation of the screening tests (aPTT, SCT, DRVVT) was expressed as a ratio of patient coagulation time to the mean clotting time of 50 normal plasmas. For inhibitor identification, these clotting tests were carried out on 1:1 and 4:1 mixtures of patients and normal plasmas. As confirmatory tests, platelet neutralisation procedure of APTT, SCT and DRVVT systems were performed. LA was diagnosed when at least one of the screenings and one of the confirmatory procedures were positive.
IgG and IgM aCL, aβ2Gp1 and aPT titre were measured by commercial enzyme-linked immunosorbent assays (Orgentec, France). aCL IgG and IgM antibodies were expressed as G phospholipid (GPL) and M phospholipid (MPL) units. Values exceeding 15 GPL or 11 MPL units were considered abnormal. aβ2Gp1 and aPT IgG and IgM antibodies were expressed as units per ml (U/ml). Values exceeding 10 units were considered abnormal for IgG and IgM aβ2Gp1 and aPT antibodies (IgG and IgM).
Statistical analysisData are presented as mean and standard deviation.Data were analysed with χ2 test, t-student test, Mann-
Whitney U-test and linear regression when appropriate.
RESULTS
Forty-two patients affected with SLE (11 men and 31 women, mean age 39.5±11.3 years) were studied.
Characteristics of the patients are reported in Table I. No patients were diabetic.
The diagnosis of SLE had been made 7.3±6.6 years previously.
Thirty-six patients were affected with lupus nephropathy ascertained by renal biopsy: 5 had class II lupus nephropathy according to the 1982 WHO
due to coronary artery disease (2).A pathogenetic role for anti-phospholipid
antibodies (aPA) in atherosclerosis has been suggested and aPA may represent a risk factor for cardiovascular disease in patients with SLE (3). Laboratory studies and murine models support the pro-atherogenic role of these autoantibodies, as they are involved in uptake of oxidized LDL into macrophages, and immunization of mice with them results in enhanced atherosclerosis (4). However, other authors did not find any association between IMT and aPL (5).
Thickness of carotid intima-media (IMT) has been claimed to be a marker of atherosclerosis in other vascular beds (6). High resolution B-mode ultrasound allows the accurate measurement of the distance between blood-intima and media-adventitia interfaces of the carotid wall, which is defined as carotid intima-media thickness.
We evaluated IMT as a surrogate parameter of atherosclerosis (6) in 42 patients affected with SLE and correlated this parameter with aPA.
MATERIALS AND METHODS
We measured IMT in 42 patients affected with SLE and in 42 healthy age- and sex-matched subjects as controls. We did not evaluate plaque presence.
Healthy subjects were selected among the sanitary staff and were sex- and age-matched for the population of lupus patients. They were chosen for absence of known disease, normal blood pressure and absence of urinary abnormalities.
IMT was measured by a single investigator who was unaware of the clinical information.
Clinical data collected included years of disease, hypertension, number of anti-hypertensive drugs, C Reactive Protein (CRP), total cholesterol, serum Creatinine (SCr), proteinuria, dose of corticosteroid during lifetime calculated as milligrams of prednisone equivalent.
The thickness of carotid intima-media was evaluated by B-mode ultrasound examination, utilizing Esaote Eidos scanner and a 10-MHz linear array probe. The thickness was evaluated at the far wall of distal right and left common carotid. The mean of three left and three right values was considered (7-8). Detection of lupus anticoagulant and of aCL, aβ2Gp1 and aPT antibodies
Serum samples of the 42 SLE patients were tested for:
C. ROLLINO ET AL.

20 21Eur. J. Inflamm.
classification (10), 10 class III, 15 class IV and 7 class V; in 1 patient two classes of lupus nephropathy were contemporarily identified (III+V).
Thickness of IMT wall was 0.538±0.128 mm (0.310-0.866 mm), which was greater than thickness measured in healthy subjects (0.473±0.084 mm -p 0.003-).
In five patients (11.9%) thickness was >0.7 mm,
in twelve it was >0.6 mm (28.5%).IMT correlated with patients’ age (p<0.005) and
with CRP (p<0.005). It did not correlate with years of duration of disease, presence of hypertension, number of anti-hypertensive drugs, total cholesterol, serum Creatinine and proteinuria and corticosteroid dose.
aPA were positive in 16 patients (38%): twelve patients (28.5%) were positive for LA, 6 for aCA IgG, 4 for aCA IgM, 4 for anti-β2GP1 IgG, 3 for anti-β2GP1 IgM, 2 for aPT IgG and 1 for aPT IgM.
IMT was not statistically correlated with the presence of aPA.
Positive and negative aPA patients did not differ as regards IMT (0.606 vs 0.537 mm, p 0.39), age, duration of disease, CRP, total cholesterol and proteinuria. The only difference was relative to estimated glomerular filtration rate (GFR) according to Levey simplified formula (11) (mean GFR 76 ±30.2ml/min/1.73m2 in aPA positive vs 113±37 ml/min/1.73m2 in aPA negative patients p<0.01).
Dividing the patients into two groups (by an arbitrary cut-off of 0.600 mm which was chosen because in the Bogalusa study (12) the 50th percentile of IMT in the white female population between 35 and 40 years was 0.676 mm), frequency of aPA positivity was 50% in patients with IMT >0.600 mm and 33.3% in those with IMT <0.600 mm (p n.s.) (Fig. 1a). If LA positivity was considered separately, it was 41.6% in patients with IMT >0.600 mm and 23.3% in patients with IMT <0.600 mm (Fig. 1b).
Of the 5 patients with IMT >0.7 mm, 2 had LA positivity (40%) vs 10/37 (27%) of those with minor carotid thickness.
DISCUSSION
The incidence of cardiovascular disease is significantly increased in SLE. Cardiovascular mortality is a major cause of death in these patients (1-2) and has been linked to an accelerated atherosclerotic process (13).
Thickness of intima-media carotid is considered a surrogate parameter of atherosclerosis (6). It has been claimed that aPA are implicated in the pathogenesis of atherosclerosis (3, 14-15), but their role has not yet been clearly identified. A correlation between aPA and IMT has been found in rheumatoid
Table I. Clinical and biochemical characteristics of the patients.
Lupus patients
Men/women 11/31
Mean age (years) 39.5 ± 11.3 (range 19-69)
Duration of disease (yrs) 7.3 ± 6.6 (range 0.5-26)
Hypertension 26 (62.2%)
> 3 anti-hypertensive drugs 8 (19%)
Serum Creatinine (mg/dl) 0.97 ± 0.37 (range 0.5-2.4)
Renal failure (GFR <60 ml/min)
5 (11.9%)
Proteinuria (g/day) 0.85 ± 1.54 (range 0.4-7)
Nephrotic syndrome 3 (7.1%)
Total cholesterol (mg/dl) 213.4 ± 66.1 (range 126-413)
C Reactive Protein (mg/dl) 0.48 ± 1.09
Clinical and biochemical characteristics of the forty-two patients affected with lupus. Data were collected at the moment of the evaluation of aPA and IMT. Duration of disease refers to the first diagnosis of lupus, even when nephropathy was evidenced later on. Hypertension is expressed as number and percentage of hypertensive patients at the moment of the evaluation. GFR: Glomerular Filtration Rate according to MDRD simplified formula (11). Nephrotic syndrome is expressed as number and percentage of patients presenting nephrotic syndrome as defined by proteinuria >3.5 g/day and serum albumin < 3 g/dl.
Table I. Clinical and biochemical characteristics of the patients.
Clinical and biochemical characteristics of the forty-two patients affected with lupus.Data were collected at the moment of the evaluation of aPA and IMT. Duration of disease refers to the first diagnosis of lupus, even when nephropathy was evidenced later on. Hypertension is expressed as number and percentage of hypertensive patients at the moment of the evaluation. GFR: Glomerular Filtration Rate according to MDRD simplified formula (11). Nephrotic syndrome is expressed as number and percentage of patients presenting nephrotic syndrome as defined by proteinuria >3.5 g/day and serum albumin < 3 g/dl.

22 23Eur. J. Inflamm.
arthritis (16).We measured IMT in SLE and correlated these
values with aPL.IMT was greater in SLE patients than in healthy
age- and sex-matched subjects studied as controls. IMT correlated with age and CRP, another surrogate parameter of atherosclerosis (17), but did not correlate with years of duration of disease, presence of hypertension, number of anti-hypertensive drugs, total cholesterol, serum Creatinine, proteinuria and corticosteroid dose. The same results were reported by other authors: for example Selzer (18) reports that determinants of the highest quartile of IMT were older age, higher pulse pressure, lower levels of albumin, elevated C-Reactive protein levels, high cholesterol and high levels of glucose. Risk factors for plaque were slightly different (18-19). We did not evaluate plaque because of their very low prevalence in the subjects studied.
aPA were found in 38% of patients and were not statistically correlated with IMT. By choosing a cut-off of 0.600 mm (in the Bogalusa study (12) the 50th percentile of IMT in white female population between 35 and 40 years was 0.676 mm), frequency of aPA positivity was 50% in patients with IMT >0.600 mm and 33.3% in those with IMT <0.600
mm. However, frequency of positivity for aPA was higher, even if not significant, in the group of patients with IMT greater than 0.600 mm than in the group of patients with minor thickness (50% vs 33.3%, p n.s.) (Fig. 1a), in particular as regards LA (41.6 vs 23.3% p n.s.) (Fig. 1b). The same proportion was observed in patients with even greater carotid intima-media thickness (>0.700 mm: 40% vs 27%). This observation is in favour of the hypothesis of a pathogenetic role played by aPA in the development of accelerated atherosclerosis in SLE patients. However, due to the small number of patients, no other considerations can be made on these data. Further studies should analyse this association and its possible pathogenetic implications.
In conclusion, IMT, a surrogate parameter of atherosclerosis, was correlated with patients’ age and CRP and not with presence of aPA, even though, by selecting the group of patients with greater IMT, there was a non-significant higher proportion of positivity for anti-phospholipid antibodies, in particular for LA.
Disclosure. The authors (C. Rollino, C. Massara, L. Besso, C. Marcuccio, M. Manganaro, T. Bertero, B.a Montaruli, G. Beltrame, M. Ferro, G. Quattrocchio, F. Elia and F. Quarello) declare that
a b
0
10
20
30
40
50
60
70
IMT >0.600 mm IMT <0.600 mm IMT all
APA+APA-
0
10
2 0
3 0
4 0
5 0
6 0
7 0
8 0
IMT >0.600 mm IMT <0.600 mm IMT all
LA+LA-
Fig. 1. a) IMT and anti-Phospholipid Antibodies. The figure shows the frequency of aPA positivity in patients with IMT >0.600 mm (50%) and in those with IMT <0.600 mm (33.3%) (p n.s.). b) IMT and Lupus Anticoagulant. This figure shows the frequency of LA positivity, when considered separately, in patients with IMT >0.600 mm (41.6%) and in patients with IMT <0.600 mm (23.3%) (p n.s.).
C. ROLLINO ET AL.
a b

22 23Eur. J. Inflamm.
they have no conflicts of interest.
REFERENCES
1. Manzi S, Meilahn EN, Rairie JE, Conte CG, Medsger TA Jr, Jansen-McWilliams L, D‘Agostino RB, Kuller LH. Age-specific incidence rates of myocardial infarction and angina in women with systemic lupus erythematosus: comparison with the Framingham Study. Am J Epidemiol 1997; 145(5):408-15.
2. Aranow C, Ginzler EM. Epidemiology of cardiovascular disease in systemic lupus erythematosus. Lupus 2000; 9:166-9.
3. Frostegård J. Autoimmunity, oxidized LDL and cardiovascular disease. Autoimmun Rev 2202; 1:233-7.
4. Sherer Y, Shoenfeld Y. Antiphospholipid antibodies: are they pro-atherogenic or an epiphenomenon of atherosclerosis? Immunobiology 2003; 207(1):13-16.
5. Petri M. The lupus anticoagulant is a risk factor for myocardial infarction (but not atherosclerosis): Hopkins Lupus Cohort. Thromb Res 2004; 114:593-5.
6. Lorenz MW, Markus HS, Bots ML, Rosvall M, Sitzer M. Prediction of clinical cardiovascular events with carotid intima-media thickness: a systematic review and meta-analysis. Circulation 2007; 115:459-67.
7. Simon A, Gariepy J, Chironi G, Megnien JL, Levenson J. Intima-media thickness: a new tool for diagnosis and treatment of cardiovascular risk. J Hypertens 2002; 20(2):159-69.
8. Roman MJ, Naqvi TZ, Gardin JM, Gerhard-Herman M, Jaff M, Mohler E; American Society of Echocardiography; Society for Vascular Medicine and Biology American society of echocardiography report. Clinical application of noninvasive vascular ultrasound in cardiovascular risk stratification: a report from the American Society of Echocardiography and the Society for Vascular Medicine and Biology. Vasc Med 2006; 11:201-11.
9. Churg J, Sobin LH. In Renal Disease: Classification and Atlas of Glomerular Disease. Igaku-Shoin:
Tokyo, 1982, p 115.10. Exner T, Triplett DA, Taberner D, Machin SJ.
Guidelines for testing and revised criteria for lupus anticoagulants. SSC Subcommittee for Standardization of Lupus Anticoagulants. Thromb Haemost 1991; 5:320-35.
11. Levey AS, Greene T, Kusek JW, Beck GL, MDRD Study Group. A simplified equation to predict glomerular filtration rate from serum creatinine. J Am Soc Nephrol 2000; 11:155A.
12. Stein JH, Douglas PS, Srinivasan SR, Bond MG, Tang R, Li S, Chen W, Berenson GS. Distribution and Cross-Sectional Age-Related Increases of Carotid Artery Intima-Media Thickness in Young Adults. The Bogalusa Heart Study. Stroke 2004; 35(12):2782-90.
13. van Leuven SI, Kastelein JJ, D’Cruz DP, Hughes GR, Stroes ES. Atherogenesis in rheumatology. Lupus 2006; 15(3):117-21.
14. Frostegård J. SLE, atherosclerosis and cardiovascular disease. J Intern Med 2005; 257:485-95.
15. Bruce IN. ‘Not only...but also’: factors that contribute to accelerated atherosclerosis and premature coronary heart disease in systemic lupus erythematosus. Rheumatology 2005; 44(12):1492-502.
16. Sherer Y, Gerli R, Gilburd B, Bartoloni Bocci E, Vaudo G, Mannarino E, Shoenfeld Y. Thickened carotid artery intima-media in rheumatoid arthritis is associated with elevated anticardiolipin antibodies. Lupus 2007; 16(4):259-64.
17. Davidson J, Rotondo D. C-reactive protein: a surrogate marker for atherosclerosis. Curr Opin Lipidol 2004; 15:365-7.
18. Selzer F, Sutton-Tyrrell K, Fitzgerald SG, Pratt JE, Tracy RP, Kuller LH, Manzi S. Comparison of risk factors for vascular disease in the carotid artery and aorta in women with systemic lupus erythematosus. Arthr Rheum 2004; 50:151-9.
19. Roman MJ, Shanker BA, Davis A, et al. Prevalence and correlates of accelerated atherosclerosis in systemic lupus erythematosus. N Engl J Med 2003; 349:2399-406.

EUROPEAN JOURNAL OF INFLAMMATION
1721-727X (2009)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties25

EUROPEAN JOURNAL OF INFLAMMATION
1721-727X (2009)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties25
PHYSICOCHEMICAL CHARACTERIZATION OF EXHAUST PARTICULATES FROM GASOLINE AND DIESEL ENGINES BY SOLID-PHASE MICRO EXTRACTION
SAMPLING AND COMBINED RAMAN MICROSPECTROSCOPIC/FASTGAS-CHROMOTOGRAPHY MASS SPECTROMETRY ANALYSIS
M. PACENTI, C. LOFRUMENTO1, S. DUGHERI, A. ZOPPI1, I. BORSI2, A. SPERANZA3, P. BOCCALON, G. ARCANGELI, A. ANTONIUCCI4,
E.M. CASTELLUCCI1 and V. CUPELLI
Occupational Medicine Division, Department of Public Health, University of Florence; 1Chemistry Department, University of Florence; 2Department of Mathematics U. Dini, University of Florence;
3Innovazione Industriale Tramite Trasferimento Tecnologico, Florence; 4Occupational Medicine Division, Department of Biomedical Science, University of Chieti-Pescara, Chieti, Italy
Received December 18, 2008 – Accepted March 3, 2009
Ambient Particulate Matter (PM) has been shown to be associated with cardiopulmonary diseases and lung cancer. Several groups of investigators have shown that the size of the airborne particles and their surface area determine the potential to elicit inflammatory injury and other mechanisms of adverse cellular effects. Because traffic is an important source of PM, it seems obvious that physicochemical characterization of vehicles exhaust emission has an important impact on both quantitative and qualitative aspects of ambient PM. In the present study the exhaust emissions of 8 vehicles of different categories were analyzed to attempt to differentiate them. For such purpose the particulate was collected on SPME fibers exposed to the exhaust emission for 150 s. The particulate was first characterized by micro-Raman spectroscopy and then subjected to Fast Gas Chromatography-Mass Spectrometry analyses for the chemical identification of the Polycyclic Aromatic Hydrocarbons (PAHs) compounds, the organic fraction of particulate matter in air pollution with a major role in the toxicity, notably via its effects on inflammation. Both the particle count and the PAHs compositional data were assembled to be interpreted by Principal Components Analysis. This multivariate analysis grouped the data according mainly to the naphthalene amount, as well as the volume concentration of the particles smaller than 0.5 µm, suggesting that the different exhaust emissions could be easily differentiated. With this new methodology, future research should aim at establishing a mechanism of formation during internal engine combustion processes in order to obtain a clearer picture of the inflammatory and carcinogenic mechanisms of PM in the lungs.
Mailing address:Dr. Marco Pacenti, Division of Occupational Medicine, Largo Palagi 1, 50134 Florence, ItalyTel/ Fax: ++390557948296 e-mail: [email protected]
Key words: SPME, Raman microspectroscopy, Fast GC-MS, particulate matter, PAHs
The relationship between the level of particulate matter with an aerodynamic diameter less than 10 µm (PM 10) and the mortality and morbidity rates
from respiratory and cardiovascular diseases is well established, but the biological mechanisms responsible for these associations are still unclear.
Vol. 7, no. 1, 25-37 (2009)

26 27Eur. J. Inflamm.
Soberanes et al (1) reported that airborne PM activates the intrinsic apoptotic pathway in alveolar epithelial cells through a pathway that requires the mitochondrial generation of reactive oxygen species and the activation of p53. PM 2.5 µm induces p53-dependent apoptosis in primary human alveolar epithelial cells and activation of the intrinsic apoptotic pathway by p53 often requires the transcription of the proapoptotic Bcl-2 protein Noxa-dependent cell death that might contribute to PM-induced alveolar epithelial dysfunction and the resulting inflammatory response (2). van Eeden et al (3) conclude that exposure to ambient particulate matter air pollution induces a systemic inflammatory response that includes the release of inflammatory mediators into the circulation that stimulate the bone marrow to release leukocytes and platelets. They postulate that this systemic response to particulate air pollution augments lung inflammation and changes the phenotype of atherosclerotic plaques to make them more vulnerable to rupture. Becker et al (4) revealed that the main proinflammatory response (TNF, IL-6, COX-2) in alveolar macrophages was driven by material present in the coarse PM, containing 90-95% of the stimulatory material in PM10.
It has been suggested that Polycyclic Aromatic Hydrocarbons (PAHs), the major organic fraction of particulate matter in air pollution has a major role in the toxicity of this pollutant, notably via its effects on inflammation. Goulaouic et al showed that when PAHs were absorbed onto the fine particles, any observed increases in cytokine secretion consistently appeared to be due to the particles themselves (5).
Until today few researchers have characterized the exhaust particles according to their morphological features, size distributions and chemical properties of their organic components. Diluted exhaust emissions were sampled by high volume air sampling, and analysed both through physical characteristics, by employing several microscopy techniques including transmission electron microscopy (TEM), field emission scanning electron microscopy (FESEM), and image analysis (IA), and through the chemical characteristics by liquid- or gas-chromatography mass spectrometry (GC-MS). In the previous works the use of solvents and/or clean-up steps were often necessary to extract and eliminate interfering
compounds from the air. This implies an increase of the required manual operations, higher costs, uncertainty in the analysis determination, and the possible loss of the analyte. For that reason a more sensitive analytical method than those available is necessary for the standardization of the analytical factor affecting vehicle emission.
Previous works (6-7) have shown that Solid-Phase Micro Extraction (SPME) technology combined with Raman microspectroscopy can be used for airborne particulate. The Authors present a new methodological procedure based on a sequential mixed application of Raman microspectroscopy and automated SPME Multi Fiber System (MFS)-Fast GC/MS. In this respect new sampling devices are developed with the aim to analyze airborne fine particulate matter and PAHs from exhaust emissions, from gasoline- and diesel-powered vehicles, and compile quali/quantitative source profiles for the conversion to particle number density per unit volume.
MATERIALS AND METHODS
SamplesThe particulate mass was loaded on 7 µm
polydimethylsiloxane (PDMS) SPME fibers purchased from Supelco (Sigma-Aldrich, Milan, Italy). Before sampling, the fibers were conditioned according to manufacturer’s recommendations and the blank was examined by optical light microscope and Raman analysis.
Eight different vehicles were considered for the exhaust emission sampling: four diesel automobiles (A: EURO 1, B: EURO 3, C: EURO 4 without Diesel Particulate Filter-DPF and D: EURO 4 with DPF), a gasoline automobile EURO 3 catalyst-equipped (E), one heavy-duty EURO 3 diesel truck (F), and two motorcycles (G: two-stroke engine EURO 0 non catalyst and H: four-stroke EURO 2 catalyst-equipped).
During the sample collection phase, the engines of the vehicles were rotated at ca. 2000 rpm with no load. Automobiles A-E, heavy-duty diesel truck F, and motorcycles G-H were equipped with diesel or gasoline engines having piston displacements of 1900, 1800, 1400, 2000, 1200, 5000, 1500, 100, and 150 cc, respectively.
The exhaust emissions were sampled keeping the SPME fibers longitudinally near the tailpipe for 150 s, as carried out for the first time by Odziemkowsky et al (7). During the heaping time the SPME fibers were turned around to get a homogenous apportionment of the
M. PACENTI ET AL.

26 27Eur. J. Inflamm.
particulate matter. After the sampling, the SPME fibers were withdrawn ~ 4 mm inside the needle, then protected by a Teflon spigot and sent to Raman and GC analyses. As a final operation, the SPME fibers were rinsed with methanol and dried in air before further analyses. The Authors of this paper indicate that the SPME fibers were non-reusable.
Micro-Raman SpectroscopyThe apparatus used to carry out the micro-Raman
experiments is a Renishaw RM2000 spectrometer coupled to a Leica optical microscope. The near-IR 785 nm line of a diode laser was used as excitation source providing about 26 mW laser power at the source. This power was reduced by filters and optical components to yield power on samples ranging from about 0.1 to 6.9 mW, that can be varied by software through gray internal filters. Such a low laser power was maintained during Raman measurements to prevent the probable sample degradation. The grating used to disperse revealed Raman photons is a 1200 lines/mm, while the detector is a CCD camera (400 x 578 pixels) cooled by Peltier effect. The instrumental spectral broadening, evaluated as line width (full width at half maximum FWHM) of an emission line of a He-Ne lamp, was 3 cm-1. The magnification objective used for the analyses is a 50x type, permitting a quite appreciable spatial resolution of about 1.5 μm in spectra acquiring. This Raman device works in backscattering geometry. The spectral calibration of the grating was performed using the 520 cm-1 Raman signal from a Silicon crystal.
For Raman analysis the SPME fibers were positioned between the XYZ Raman stage and the objective lens of the microscope. The SPME fibers were pulled into a glass cylindrical home-made support to maintain the SPME fiber parallel both to the XYZ stage and the microscope objective. Then the SPME fiber was extracted from the needle to focus the surface area to be subjected to Raman measurements.
Odziemkowski et al (7) stated that high fluorescence from industrial air samples was expected, so they decided to perform Raman analyses in the confocal apparatus configuration, with the aim of diminishing this undesirable effect they supposed to be originated not only from the particulate matter, but also from the surroundings. Such a configuration was not necessary during the study we have performed, since the laser source used for Raman measurements emits light at 785 nm, so that the range interested by the Raman effect is fairly far away from the one proper of organic matter’s fluorescence. For this reason the slit width was maintained at 40 µm, whereas the area of the CCD detector was 40 × 576 pixels.
Finally, Raman results were evaluated based on
equivalence with attainable literature data and data related to the SPME samples spectra.Particle counts
The SPME fibers were also investigated under the optical light microscope of the micro-Raman setup in order to make a numerical evaluation of the particles adsorbed in each tested case. For such purpose the fibers were observed under the 50x magnification objective. The entire area visualized measures about 95 µm x 70 µm wide, but the in-focus image is reduced to about 95 µm x 40 µm, due to the bend surface of the cylindrical fiber. For each sampled fiber five different areas were then randomly selected and used for particles count. The particle size was measured in a micrometer scale using the monitor pointer and taking its maximum linear dimension; due to the camera resolution it was possible to recognize and measure particles as small as 0.2 µm.
Once the total number of particles adhering to the polymer surface was evaluated, the data were grouped according to their linear dimension and averaged over the five areas considered. Then a mathematical algorithm was applied to convert this number and obtain an estimate of the total number of particles emitted by the vehicle per unit volume of exhaust gas emission.
This evaluation is based upon two main simplifications:
1. the exhaust gas flowing through the emission tailpipe is turbulent. This assumption allows us to assume that the distribution of particles within the gas flow is uniform across the tailpipe cross section;
2. All the particles colliding with the fiber surface adhere on it and stick to it. Thus, since the fiber was rotated during the process, one can assume that the particles adhering to the fiber are the ones flowing across a planar section of the exhaust emission tailpipe, that is numerically equivalent to the lateral surface of the fiber itself.
With the two above-mentioned hypotheses, one concludes that, if S is the lateral surface of fiber and A is the cross section of the emission tailpipe, the fraction α of particles colliding with the fiber (and thus adhering to it) is equal to the ratio between the two areas, i.e.,
α = S/A Equation 1
Thus, if G is the total emission rate of the tailpipe, i.e., the total volume of gas emission through the tailpipe per unit time, the volume of gas F crossing our target per unit time will be
F = α·G Equation 2
If we call W the total volume of gas emitted by the

28 29Eur. J. Inflamm.
emission tailpipe in time ∆t, at emission rate G, this will be
W = G·∆t Equation 3
thus the volume of gas crossing our target in the same time is α·W. If C is the volume concentration of particles in the exhaust emission gas (quantity that we actually want to estimate), the number of particles crossing our target in time ∆t is therefore
N = α·W·C Equation 4
Since N is the total number of particles actually observed on the fiber, we have that the volume concentration may be evaluated as:
C = N/(α·W) Equation 5
Fast GC-MSFast GC-MS analyses were performed on a Shimadzu
GC 2010 with the system acquisition GC Solution software using an SLB5-MS column (5 m x 0.10 mm x 0.4 µm film thickness, Supelco, Sigma-Aldrich) with a Shimadzu QP 2010 series mass selective detector operating in the electron ionization (EI), methane negative chemical ionization (NCI), and methane positive chemical ionization (PCI) mode (Shimadzu Italia Srl). Oven settings were 45°C hold for 1 min, with a ramp of 150°C/min up to 100°C and 50°C/min up to 300°C and maintained for 2 min. Full automation of the procedure was achieved using a AO 5000 autosampler from Shimadzu equipped with by automated MFS/SPME-Fast GC/MS. With MFS-SPME, developed by Chromline Srl the multi-fiber analysis sequence works in a simple way: the fibers assembled by Fast kit are transported between the 25-position tray and injector by the new holder equipped with a plunger/magnetic system. At the end of the analysis the desorbed fiber is moved back to the tray and the cycle is repeated.
A group of 26 PAHs were selected for analysis Fast GC-MS. Detection of analytes was accomplished by the use of MS in the Selected Ion Monitoring (SIM) mode and the molecular ions were monitored, as indicated in parentheses. The PAHs include a group of suspected carcinogens including benzo(a)pyrene (m/z=228), benzo(b)fluoranthene (m/z=252), and indeno(1,2,3,cd)pyrene (m/z=276). In addition the concentrations of phenanthrene (m/z=178), anthracene (m/z=178), fluoranthene (m/z=202), pyrene (m/z=202), acenaphthene (m/z=154), and benzo(ghi)perylene (m/z=276) were measured. These compounds have been found in the ambient air, and some of them were identified as potential traces of PAHs emissions. Naphthalene (m/z=128), acenaphthylene (m/z=152), benzo(k)fluoranthene (m/z=252), chrysene (m/z=228), dibenzo(ah)anthracene (m/z=278), benzo(a)anthracene (m/z=228) and fluorene (m/z=166) are the remaining compounds on the EPA PAHs priority pollutants list. 1-Methylnaphthalene (m/z=142), 2-methylnaphthalene (m/z=142), 2,3 dimethylnaphthalene (m/z=156), 1-nitronaphthalene (m/z=173), 2-nitronaphthalene (m/z=173), 1-methylphenanthrene (m/z=192), 2-methylphenanthrene (m/z=192), biphenyl (m/z=154), 1-nitropyrene (m/z=247), and 3-nitrobiphenyl (m/z=199), were also included for fingerprints diesel and gasoline engines exhaust emissions.
RESULTS
Micro-Raman Spectroscopy and particles countThe SPME fibers subjected to micro-Raman
spectroscopy and particle counts are those relative to the vehicles from A to F. The results obtained on the other exhausts (G, H) were not significantly representative, for which a further deepening is needed. Prior to the investigation of the sampled SPME fibers, some Raman spectra had been attained in correspondence of the surface of the PDMS-
Vehicle 0.2 < � < 0.5 0.5 < � < 1 1.2 < � < 2.5 3 < � < 5 5.4 < � < 21 � > 21 A 147 6 9 4 0 0 B 140 1 3 4 2 0 C 42 1 2 1 1 0 D 11 2 6 3 0 0 E 24 5 6 2 2 0 F 17 7 10 6 5 0
Table I � Average number n of particles counted over five different areas selected on the sampled fibers after 150 s of exposure; the diameter ranges are expressed in micron. Vehicle types: A (Diesel automobile EURO 1), B (Diesel automobile EURO 3), C (Diesel automobile EURO 4 without DPF), D (Diesel automobiles EURO 4 with DPF), E (gasoline automobiles EURO 3 catalyst-equipped), F (heavy-duty diesel truck EURO 3).
Table I. Average number n of particles counted over five different areas selected on the sampled fibers after 150 s of exposure; the diameter ranges are expressed in micron.
M. PACENTI ET AL.
Vehicle types: A (Diesel automobile EURO 1), B (Diesel automobile EURO 3), C (Diesel automobile EURO 4 without DPF), D (Diesel automobiles EURO 4 with DPF), E (gasoline automobiles EURO 3 catalyst-equipped), F (heavy-duty diesel truck EURO 3).
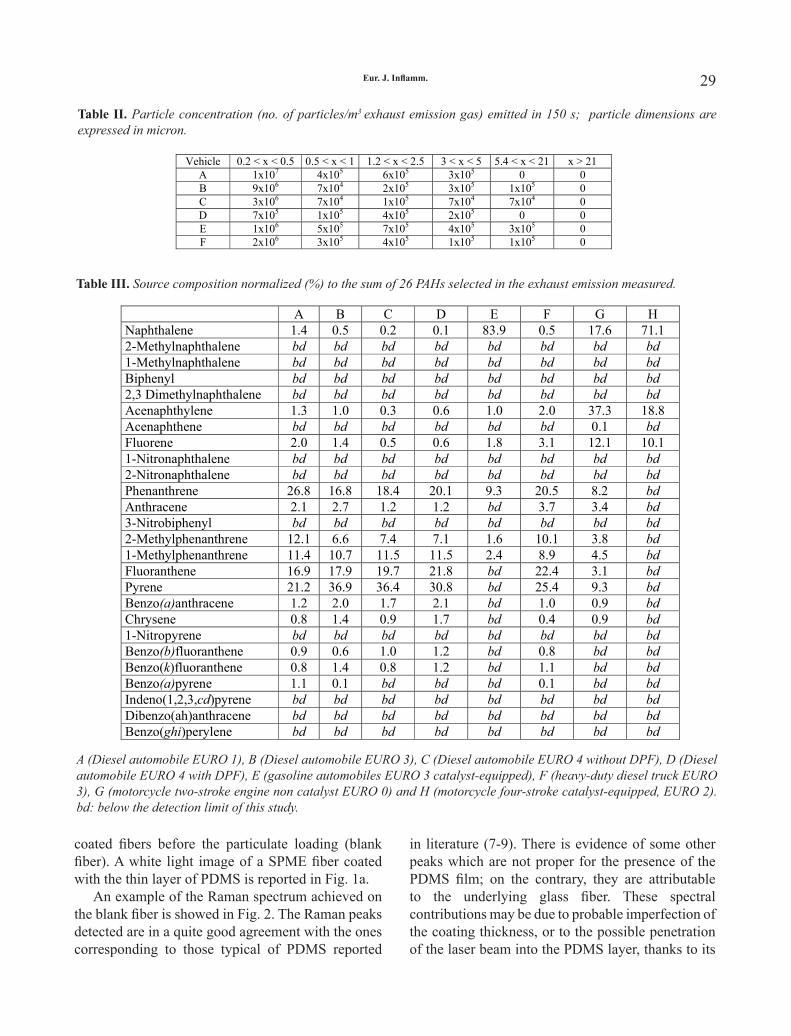
28 29Eur. J. Inflamm.
coated fibers before the particulate loading (blank fiber). A white light image of a SPME fiber coated with the thin layer of PDMS is reported in Fig. 1a.
An example of the Raman spectrum achieved on the blank fiber is showed in Fig. 2. The Raman peaks detected are in a quite good agreement with the ones corresponding to those typical of PDMS reported
in literature (7-9). There is evidence of some other peaks which are not proper for the presence of the PDMS film; on the contrary, they are attributable to the underlying glass fiber. These spectral contributions may be due to probable imperfection of the coating thickness, or to the possible penetration of the laser beam into the PDMS layer, thanks to its
Vehicle 0.2 < x < 0.5 0.5 < x < 1 1.2 < x < 2.5 3 < x < 5 5.4 < x < 21 x > 21 A 1x107 4x105 6x105 3x105 0 0 B 9x106 7x104 2x105 3x105 1x105 0 C 3x106 7x104 1x105 7x104 7x104 0 D 7x105 1x105 4x105 2x105 0 0 E 1x106 5x105 7x105 4x105 3x105 0 F 2x106 3x105 4x105 1x105 1x105 0
Table II. Particle concentration (no. of particles/m3 exhaust emission gas) emitted in 150 s; particle dimensions are expressed in micron.
ADRIANA, CLICCA SU FINALE PER QUESTO
Formattato: Tipo dicarattere:Grassetto
Formattato: Tipo dicarattere:Corsivo
Formattato: Tipo dicarattere:Grassetto, Colorecarattere: Rosso, Italiano(Italia)
Formattato: Tipo dicarattere:Grassetto, Corsivo,Colore carattere: Rosso,Italiano (Italia)
Eliminato: �
Table II. Particle concentration (no. of particles/m3 exhaust emission gas) emitted in 150 s; particle dimensions are expressed in micron.
A B C D E F G H Naphthalene 1.4 0.5 0.2 0.1 83.9 0.5 17.6 71.1 2-Methylnaphthalene bd bd bd bd bd bd bd bd1-Methylnaphthalene bd bd bd bd bd bd bd bdBiphenyl bd bd bd bd bd bd bd bd2,3 Dimethylnaphthalene bd bd bd bd bd bd bd bdAcenaphthylene 1.3 1.0 0.3 0.6 1.0 2.0 37.3 18.8 Acenaphthene bd bd bd bd bd bd 0.1 bdFluorene 2.0 1.4 0.5 0.6 1.8 3.1 12.1 10.1 1-Nitronaphthalene bd bd bd bd bd bd bd bd2-Nitronaphthalene bd bd bd bd bd bd bd bdPhenanthrene 26.8 16.8 18.4 20.1 9.3 20.5 8.2 bdAnthracene 2.1 2.7 1.2 1.2 bd 3.7 3.4 bd3-Nitrobiphenyl bd bd bd bd bd bd bd bd2-Methylphenanthrene 12.1 6.6 7.4 7.1 1.6 10.1 3.8 bd1-Methylphenanthrene 11.4 10.7 11.5 11.5 2.4 8.9 4.5 bdFluoranthene 16.9 17.9 19.7 21.8 bd 22.4 3.1 bdPyrene 21.2 36.9 36.4 30.8 bd 25.4 9.3 bdBenzo(a)anthracene 1.2 2.0 1.7 2.1 bd 1.0 0.9 bdChrysene 0.8 1.4 0.9 1.7 bd 0.4 0.9 bd1-Nitropyrene bd bd bd bd bd bd bd bdBenzo(b)fluoranthene 0.9 0.6 1.0 1.2 bd 0.8 bd bdBenzo(k)fluoranthene 0.8 1.4 0.8 1.2 bd 1.1 bd bdBenzo(a)pyrene 1.1 0.1 bd bd bd 0.1 bd bdIndeno(1,2,3,cd)pyrene bd bd bd bd bd bd bd bdDibenzo(ah)anthracene bd bd bd bd bd bd bd bdBenzo(ghi)perylene bd bd bd bd bd bd bd bd
Table III. Source composition normalized (%) to the sum of 26 PAHs selected in the exhaust emission measured. A (Diesel automobile EURO 1), B (Diesel automobile EURO 3), C (Diesel automobile EURO 4 without DPF), D (Diesel automobile EURO 4 with DPF), E (gasoline automobiles EURO 3 catalyst-equipped), F (heavy-duty diesel truck EURO 3), G (motorcycle two-stroke engine non catalyst EURO 0) and H (motorcycle four-stroke catalyst-equipped, EURO 2). bd: below the detection limit of this study.
Formattato: Tipo dicarattere:Grassetto
Formattato: Giustificato
Formattato: Tipo dicarattere:Corsivo
Formattato: Tipo dicarattere:Corsivo
Table III. Source composition normalized (%) to the sum of 26 PAHs selected in the exhaust emission measured.
A (Diesel automobile EURO 1), B (Diesel automobile EURO 3), C (Diesel automobile EURO 4 without DPF), D (Diesel automobile EURO 4 with DPF), E (gasoline automobiles EURO 3 catalyst-equipped), F (heavy-duty diesel truck EURO 3), G (motorcycle two-stroke engine non catalyst EURO 0) and H (motorcycle four-stroke catalyst-equipped, EURO 2). bd: below the detection limit of this study.

30 31Eur. J. Inflamm.
low refracting index (7).After exposure to the exhaust emissions, the fiber
surface appearance changed and resulted daubed by fluky disseminated black particles of different (regular or irregular) morphology and size (Fig. 1b); the entity of the particulate contamination depends on the engine characteristics, as will be discussed below.
On each of the five SPME fibers analyzed, every black particle/grain visible on the selected areas (five per fiber) was examined through Raman analysis. Almost all the Raman spectra registered in correspondence of the black spots presented the vibrational bands of the PDMS coating and of the glass fiber underneath, together with two bands located near 1300 cm-1 and 1600 cm-1 (Fig. 3); these latter signals are characteristic of carbonaceous material which results from incomplete diesel combustion. Actually Raman scattering is a
highly sensitive optical analysis technique useful to study atomic microstructures in carbonaceous materials and is sensible to the structural change or rearrangement of carbon crystallites (10). The band attribution of the carbonaceous materials is reported elsewhere (11-16).
Some spectra collected in sporadic locations revealed the presence of calcite, hematite or quartz, which are typical species in dust. On the other hand, a very interesting result was obtained once on a black particle. The related spectrum, reported in Fig. 4, shows some peaks which may be attributed to PAHs (17).
After Raman speciation, every black particle/grain was sized as described above. In such a way it has been possible to count the particles that were discernible on the in-focus image of the fiber surface and to group them on the basis of their dimension. The average values of the number of particles n obtained for every sampling are reported in Table I.
These data were then used to evaluate the particle volume concentration C. Assuming that:
1) the tailpipe has an average radius R of 2.5 cm, which let us calculate a cross sectional area A of about 2×10-3 m2;
2) considering an average cubic capacity of 1500 cm3 and an engine load of 2000 rpm in road use, the emission rate G is ~1500×10-6×2000 m3/min = 0.05 m3/s;
3) the fiber has a volume V = 121 × 10-12 m3, a length l = 1 cm and a radius r = 6.2 × 10-6 m, from which the lateral surface results S = 2 π r·l = 3.9 × 10-6 m2;
4) the fiber area analyzed measures a = 95×40 µm2 = 3.8 ×10-9 m2, so that the average number of particles counted per unit area is n/a and the total number of particles adhering to each fiber is N = nS/a;
and using Equations 1-5, the concentration of particles emitted during the exposure time was calculated (Table II).
Fast GC-MSThe PAHs fingerprints for exhaust emissions of
eight vehicles are presented in Table III. The source composition was normalized (%) to the sum of the 26 PAHs selected. The intensity of automobile Diesel EURO 1 profile was two orders of magnitude
M. PACENTI ET AL.
Principal Component Analysis
Calculated from Covariance Matrix by NIPALS
Eigenvalue 1430.1 780.5 Proportion 0.625 0.341 Cumulative 0.625 0.967
Eigenvectors
Variable PC1 PC2 2 �m <�<5.4�m -0.012 -0.089 3 �m <�<5 �m 0.033 -0.199 1.2 �m <�<2 �m -0.029 -0.387 0.5 �m <�<1 �m -0.055 -0.191 0.2 �m <�<0.5 �m 0.064 0.865 Naphthalene -0.897 0.079 Acenaphthylene -0.001 -0.010 Fluorene -0.005 -0.015 Phenantrene 0.116 -0.013 Anthracene 0.022 -0.014 2-Methylphenanthrene 0.092 0.014 1-Methylphenanthrene 0.211 -0.085 Fluoranthene 0.336 0.056 Pyrene 0.285 -0.110 Benzo(a)anthracene 0.018 0.003 Chrysene 0.012 0.002 Benzo(b)fluoranthene 0.010 -0.003 Benzo(k)fluoranthene 0.011 -0.003 Benzo(a)pyrene 0.002 0.005
Table IV. Eigenvectors obtained by the NIPALS algorithm showing the loadings of the considered variables.
Table IV. Eigenvectors obtained by the NIPALS algorithm showing the loadings of the considered variables.

30 31Eur. J. Inflamm.
higher than automobiles of Diesel EURO 4 and of one order of magnitude higher than motorcycle two-stroke engine non-catalyst, EURO 0, while automobile gasoline EURO 3 profile was two orders of magnitude higher than motorcycles than four-stroke catalyst-equipped EURO 2 (Fig. 5).
The results of the analyses performed on field blanks indicate a contamination level lower than the GC detection limit. The instrument detection limit increased with the molecular weight and ranged from 20 to 80 pg, for naphthalene and benzo(ghi)perylene, respectively.
DISCUSSION
For more than five decades, exhaust emissions from gasoline- and diesel-powered vehicles have
received attention because of their potential for producing adverse health effects, contribution to visibility deterioration, and dominant influence on atmospheric smog formation (18-20). Due to the complexity of primary particulate vehicular emissions, characterization of the physical and the chemical composition of vehicle exhaust aerosol is still under study.
PAHs from automobile exhaust are present on urban street surfaces as street dust (21) and they are washed off from roads during heavy rain storms and transported to rivers. Street dust is a mixture of automobile exhaust, asphalt, lubricating oils, gasoline, diesel fuel, atmospheric fallout tire particles, and soils. Some Authors (21) indicated that PAHs contents in the asphalt samples are lower than those in the street dusts, thus suggesting that
Fig. 1. White light images of (a) the blank SPME fiber and (b) after 150s exposure to diesel EURO 3 engine (sample B); magnification 50x. The corresponding Raman spectra are reported in Figs. 2 and 3 respectively.

32 33Eur. J. Inflamm.
asphalt is not the primary source of street dust PAHs. This paper indicates that the gas chromatogram of PAHs in EURO 1 automobile exhaust is similar to that analyzed by Takada et al. in heavily trafficked street dust. This proposes that exhaust emission is the major source of PAHs, which is similar to that in heavily trafficked street dust, particularly
in the abundance of alkyl-substituted PAHs. Some Authors, (22-24) indicated methylphenanthrenes/phenanthrene ratio to estimate gasoline (0.7) or diesel automobile exhaust (5.5). 1-Methylphenanthrenes/phenanthrene ratio higher than 1 was identified with highly trafficked road, but this value is not able to discriminate gasoline or diesel emission. Instead,
Fig. 2. Raman spectrum of the bare glass fiber coated with PDMS.
Fig. 3. Raman spectrum of a carbonaceous particle on the SPME fiber after 150 s exposure to diesel EURO 3 engine (see Fig. 1a).
M. PACENTI ET AL.

32 33Eur. J. Inflamm.
fluoranthene/phenanthrene ratios of 0.61-0.72 was indicated as index diesel automobile exhaust (22, 24-25); in this paper, for EURO 1 the PAHs profiles and the fluoranthene/phenanthrene ratio was similar to those observed in literature, on the contrary for EURO 4 resulted a fluoranthene/phenanthrene ratio
of 1.1.Various conditions (e.g., fuel composition,
fuel to air ratio, engine combustion temperature, fuel injection timing, lubricating oil type, and maintenance schedule for engine adjustment and lubricating oil replacement) affect the PAHs and
Fig. 4. Raman spectrum of a black particle; the signals in the high frequency region may be indicative of some PAHs.
Fig. 5. Group of 26 PAHs selected for Fast GC-MS analysis. 1. Naphthalene, 2. 2-Methylnaphthalene, 3. 1-Methylnaphthalene, 4. Biphenyl, 5. 2,3 Dimethylnaphthalene, 6. Acenaphthylene, 7. Acenaphthene, 8. Fluorene, 9. 1-Nitronaphthalene, 10. 2-Nitronaphthalene, 11. Phenanthrene, 12. Anthracene, 13. 3-Nitrobiphenyl, 14 2-Methylphenanthrene, 15. 1-Methylphenanthrene, 16. Fluoranthene, 17. Pyrene, 18. Benzo(a)anthracene, 19. Chrysene, 20. 1-Nitropyrene, 21. Benzo(b)fluoranthene, 22. Benzo(k)fluoranthene, 23. Benzo(a)pyrene, 24. Indeno(1,2,3,cd)pyrene, 25. Dibenzo(ah)anthracene, 26. Benzo(ghi)perylene. A (motorcycles four-stroke catalyst-equipped, EURO 2), B motorcycles two-stroke engine non catalyst EURO 0) C (Diesel automobiles EURO 1), D (Diesel automobiles EURO 4 without DPF), E (gasoline automobiles EURO 3 catalyst-equipped).

34 35Eur. J. Inflamm.
the related particulates composition in the exhaust. Especially, combustion temperature largely affects the relative abundance of alkyl-substituted PAHs. It was reported that the content of alkyl-substituted PAHs in automobile exhaust decreases as engine load increases and cylinder exhaust temperature increases (21). Thus, the relative abundance of alkyl-PAHs discharged from automobiles under high engine load in road use is probably lower than those in the exhausts collected in the present study (no load). Since the present work is preliminary to obtain mainly the PAHs profile in the diesel and gasoline vehicular exhaust, the factors influencing such a profile were not studied. Further extensive collection of vehicles exhausts should be conducted. Other PAHs in the diesel emissions were fluorene, acenaphthylene, phenanthrene and pyrene. On average the predominant PAHs in gasoline engine samples were naphthalene, fluorene and acenaphthylene. The heavy molecular weight of five and six ring PAHs were below the detection limits of this study for most of the samples. Nevertheless, the sampling performed on scooter with two-stroke engine and in EURO-1 diesel vehicle, indicates that significant high molecular PAHs emission can occur from these classes of vehicles. In Italy motorcycles
represent about 20% of the whole circulating fleet used for individual transport and their prevailing use is in an urban environment (19). Two-stroke non-catalyzed motorcycles still represent a large proportion of circulating two-wheelers in Italy, and the results of this study shows that their emissions can be comparable or even higher than emissions evaluated from EURO-3 and EURO-4 gasoline and diesel vehicles. Low molecular weight PAHs (two and three rings) have relevance for the majority of the mass in gasoline engine samples. The results of this study were verified by comparing the ratio of measured total PAHs to lower molecular weight with those ratio reported for other studies. However lower molecular weight PAHs had higher values for their ratios in this study because both gas and particulate phase were measured. Two and three ring PAHs were responsible for the majority of the total PAHs mass, to vary from 73-96 % of diesel and gasoline engines, respectively. Naphthalene accounted for the majority of the mass in gasoline engine samples, while diesel engines samples did not have a significant concentration of naphthalene in their emission.
Most of the lower molecular weight PAH compounds are not cancer-producing, but their
Fig. 6. Score Plot obtained by the NIPALS algorithm and the covariance matrix.
M. PACENTI ET AL.

34 35Eur. J. Inflamm.
measurement is justified by the fact that some of them are important precursors of highly mutagenic nitro-PAHs (26-29). The specific nitro-PAH isomers formed from the gas-phase OH, NO3 and O3 radical-initiated reactions of naphthalene, acenaphthylene, acenaphthene, fluorene, phenanthrene, anthracene, flouranthene, pyrene, 1-methylnaphthalene, 2-methylnaphthalene, 2,3 dimethylnaphthalene, and biphenyl, are object of studies and the technologies employed in this study can to be of assistance.
The aim of this system is to widen its use to all the working structures which need quick determinations. MFS SPME with robotic system, designed to analyze up to 100 fiber, could be more readily accepted in industrial and public agency application for rapid determinations. This methodology foresees a sampling time range lower than 5 minutes and it provides a simple, sensitive, as well as fast screening tool. Sampling by SPME requires no pumps, no polluting organic solvents, thus cutting down time and the sampling cost. The Fast GC furnishes a rapid separation and the maintenance of an excellent quality of analysis. Further studies suggest that MFS SPME-Fast GC/MS could also be applied to analyze supplementary volatile organic compounds.
Urban particulate matter is a highly heterogeneous, physicochemical mixture which varies within and among cities, and with season, weather conditions and time of day. Thus, both the physical and chemical characteristics of particulate matter are important when attempting to elucidate particle toxicity. Organic compounds are the main contributors to the ultrafine particle mass concentrations. Moreover particles of biological origin, as fungus, pollen, bacterium and virus could be present in the range 0.1-2.5 µm.
In this respect the results obtained for the particle volume concentrations, achieved from particle counts, and PAHs determination can be combined to be used for a differentiation among different engine vehicles (diesel and gasoline) and different engine categories (EURO 1, EURO 3, E URO 4…). Because of the large number of variables, for such purpose the application of a multivariate approach is mandatory, with the effort to take into account the relevant correlation among the variables. PCA (Principal Component Analysis) was carried out to describe the system under investigation and to better
interpret the results inherent to the presence of PAHs, together with those indicating the carbonaceous particle concentrations. The Score Plot diagram (Fig. 6) was derived from the matrix of data containing the various types of vehicles in the rows, while both carbonaceous particle concentrations and different PAHs in the columns. Due to the fact that PCA is scale dependent, the original matrix had to be scaled in a meaningful way to attain relative percentage values; the normalization procedure was separately performed on the two set of data (carbonaceous particle concentrations and the PAHs composition). Due to the large number of variables, the NIPALS algorithm was used (30). Moreover, it was not needed to compute all the principal components of the system, since about the 97% of the variability in the data is captured in the first two principle components, so they are sufficient to explain most of the predictable variations in the process. This is an advantage as it helps in reducing the dimensionality of the variable space. The results of PCA applied to the characterization samples are reported in Table IV. The first two PCs account for 96.7% of the total variance contained in the dataset and they are considered in the subsequent analysis.
Fig. 5 shows that three groups of data can be recognized, well separated one from the other: the first one is formed by points A, B, C; the second one by point D and F, while the third one corresponds only to point E.
Along with the PC1, which explains the 62.5% of the total variability, point E is set aside with respect to the others data. This separation is mainly due to the PAHs composition, in particular to the naphthalene and pyrene contents, which present the highest loadings values. On the other hand, the PC2 explains the 34.1% of the total variability and is indicative of the carbonaceous particle volume concentrations, among which the main contribution comes from particles having a diameter in the range 0.2-0.5 µm. According to this the sampled diesel automobile EURO 4 with DPF and the heavy-duty diesel truck EURO 3 exhausts discharge the lowest amount of fine particulate.
European legislation EURO V recommended for future regulation the measurements of particle matter number and particle mass of the exhaust emissions. These preliminary results suggest a

36 37Eur. J. Inflamm.
procedure to differentiate the exhaust emissions from various vehicle categories. A further development would be the rapidity of the methodology aimed to analyse great quantities of samples in a very short time, by reducing the costs of the monitoring campaigns.
REFERENCES
1. Soberanes S, Urich D, Baker CM, et al. Mitochondrial complex III-generated oxidants activate ASK1 and JNK to induce alveolar epithelial cell death following exposure to particulate matter air pollution. J Biol Chem 2009; 284:2176-86.
2. Urich D, Soberanes S, Burgess Z, et al. Proapoptotic Noxa is required for particulate matter-induced cell death and lung inflammation. FASEB J 2009; published online February 2009; 1-10.
3. van Eeden SF, Hogg JC. Systemic inflammatory response induced by particulate matter air pollution: the importance of bone-marrow stimulation. J Toxicol Environ Health A 2002; 65:1597-613.
4. Becker S, Mundandhara S, Devlin RB, Madden M. Regulation of cytokine production in human alveolar macrophages and airway epithelial cells in response to ambient air pollution particles: further mechanistic studies. Toxicol Appl Pharmacol 2005; 207:269-75.
5. Goulaouic S, Foucaud L, Bennasroune A, Laval-Gilly P, Falla J. Effect of polycyclic aromatic hydrocarbons and carbon black particles on pro-inflammatory cytokine secretion: impact of PAH coating onto particles. J Immunotoxicol 2008; 5:337-45.
6. Koziel JA, Odziemkowski M, Pawliszyn J. Sampling and analysis of airborne particulate matter and aerosols using in-needle trap and SPME fiber devices. Anal Chem 2001; 73:47-54.
7. Odziemkowski M, Koziel JA, Irish DE, Pawliszyn J. Sampling and Raman confocal microspectroscopic analysis of airborne particulate matter using poly(dimethylsiloxane) solid-phase microextraction fibers. Anal Chem 2001; 73:3131-9.
8. Mani V. Properties of commercial SPME coatings. In Applications of Solid Phase Microextraction. J. Pawliszyn, ed. Wiley-VCH: New York, 1999; p. 60.
9. Dobos S, Fogarasi G, Castellucci E. Infrared dichroism of oriented crystalline films of hexamethyl
cyclotrisiloxane. Spectrochim Acta, Part A 1972; 28:877-87.
10. Larsen KL, Nielsen OF. Micro-Raman spectroscopic investigations of graphite in the carbonaceous meteorites Allende, Axtell and Murchison. J Raman Spectr 2006; 37:217-222.
11. McCreery RL. Carbon Electrodes: Structure Effects on Electron-Transfer Kinetics. In Electroanalytical Chemistry. A.J. Bard , ed. Dekker New York, 1991; vol.17:p. 221.
12. Endo M, Kim C, Karaki T, Tamaki T, Nishimura Y, Matthews MJ, Brown SDM, Dresselhaus MS. Structural analysis of the B-doped mesophase pitch-based graphite fibers by Raman spectroscopy. Phys Rev B 1988; 58:8991-6.
13. Kraft T, Nickel KG. Carbon formed by hydrothermal treatment of α-SiC crystals. J Mater Chem 2000; 10:671-80.
14. Vidano RP, Fishbach DB, Willis LJ, Loehr TM. Observation of Raman band shifting with excitation wavelength for carbons and graphites. Solid State Commun 1981; 39:341-4.
15. Wang Z, Huang X, Xue R, Chen L. Dispersion effects of Raman lines in carbons. J Appl Phys 1998; 84:227-31.
16. Matthews MJ, Pimenta MA, Dresselhaus G, Dresselhaus MS, Endo M. Origin of dispersive effects of the Raman D band in carbon materials. Phys Rev B 1999; 59:R6586-8.
17. Costa JCS, Sant’Ana AC, Corio P, Temperini MLA. Chemical analysis of polycyclic aromatic hydrocarbons by surface enhanced Raman spectroscopy. Talanta 2006; 70:1011-6.
18. Rogge WF, Hildemann LM, Mazurek MA, Cass GR. Sources of fine organic aerosol. 2. Non-catalyst and catalyst-equipped automobiles and heavy-duty diesel trucks. Environ Sci Technol 1993; 27:636-51.
19. Spezzano P, Picini P, Cataldi D, Messale F, Manni C, Santino D. Particle-phase Polycyclic aromatic Hydrocarbon Emissions from Non-catalysed, In-use Four-stroke Scooters. Environ Monit Assess 2007; 133:105-17.
20. Zielinska B, Sagebiel J, Arnott WP, et al. Phase and size distribution of polycyclic aromatic hydrocarbon in diesel and gasoline vehicle emissions. Environ Sci Technol 2004; 38:2557-67.
M. PACENTI ET AL.

36 37Eur. J. Inflamm.
21. Takada H, Onda T, Ogura N. Determination of polycyclic aromatic hydrocarbons in urban street dusts and their source materials by capillary gas chromatography. Environ Sci Technol 1990; 24:79-1186.
22. Kuusimäki L, Peltonen Y, Kyyrö E, Mutanen P, Peltonen K, Savela K. Exposure of garbage truck drivers and maintenance personnel at a waste handling centre to polycyclic aromatic hydrocarbons derived from diesel exhaust. J Envir Monit 2002; 4:722-7.
23. Westerholm RN, Almen J,Li H. Chemical and biological characterization of particulate-, semivolatile-, and gas-phase-associated compounds in diluted heavy-duty diesel exhausts: a comparison of three different semivolatile-phase samplers. Environ Sci Technol 1991; 25:332-8.
24. Kuusimäki Peltonen K, Mutanen P, Svela K. Analysis of particle and vapour phase PAHs from the personal air samples of bus garage workers exposed to diesel exhaust. Ann Occup Hyg 2003; 47:389.
25. Khillare PS, Balachandran S, Rafiqul Hoque R. Profile of PAHs in the diesel vehicle exaust in Delhi.
Environ Monit Assess 2005; 105:411-7.26. Atkinson R, Arey J. Atmospheric chemistry of gas-
phase polycyclic aromatic hydrocarbons: formation of atmospheric mutagens. Environ Health Perspect 1994; 102:117-26.
27. Scheepers PTJ, Micka V, Muzyka V, Anzion R, Dahmann D, Poole J, Bos RP. Exposure to dust and particle-associated 1-Nitropyrene of drivers of diesel-powered equipment in underground mining. Ann Occup Hyg 2003; 47:379-88.
28. Scheepers PTJ, Martens MHJ, Velders DD, Fijneman P, van Kerkhoven M, Noordhoek J, Bos RP. 1-Nitropyrene as a marker for the mutagenicity of diesel exhaust-derived particulate matter in workplace atmospheres. Environ Mol Mutagen 1995; 25:134-47.
29. Banceu CE, Mihele C, Lane DA, Bunce NJ. Reactions of methylated naphthalenes with hydroxyl radicals under simulated atmospheric conditions. Polycycl Aromat Comp 2001; 18:415-25.
30. Wold S, Esbensen K, Geladi P. Principal Component analysis. Chemom Int Lab System 1987; 2:37.

EUROPEAN JOURNAL OF INFLAMMATION
1721-727X (2009)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties39

EUROPEAN JOURNAL OF INFLAMMATION
1721-727X (2009)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties39
INCREASED IL-8 LEVELS IN THE CEREBROSPINAL FLUID OF PATIENTS WITH AMYOTROPHIC LATERAL SCLEROSIS
T. MENNINI, L. GIORDANO, M. MENGOZZI, P. GHEZZI, R. TONELLI,R. MANTEGAZZA1, V. SILANI2, M. CORBO2,3, C. LUNETTA2,3 and E. BEGHI
Istituto di Ricerche Farmacologiche Mario Negri, Milano; 1Istituto Nazionale Neurologico Carlo Besta, Milano; 2Dept. Neurology and “Dino Ferrari” Center, University of Milan Medical School, IRCCS Istituto Auxologico Italiano, Milano;3NEuroMuscular Omnicenter (NEMO), Fondazione Serena Onlus, Milano, Italy
Received October 17, 2008 - Accepted March 9, 2009
Inflammation has been implicated in the pathogenesis of many neurodegenerative diseases. The chemokine IL-8 is thought to have a pathophysiological role in neurodegenerative diseases. IL-8 has recently been shown to induce death of primary cultured motor neurons in vitro. We determined IL-8 levels in the cerebrospinal fluid (CSF) from 38 patients with sporadic amyotrophic lateral sclerosis (ALS) compared to patients with other non-inflammatory neurological diseases (cerebrovascular disease, degenerative dementia, Parkinson’s disease, compressive radiculo-myelopathy). Multiple sclerosis (MS) patients were used as positive controls. The levels of IL-8 in the CSF of ALS patients were significantly higher than those of patients with other, non-inflammatory neurological conditions and similar to those of MS patients. The only variable influencing IL-8 in ALS patients was sex, with higher levels in men than in women. The presence of the inflammatory cytokine IL-8 in the CSF of patients with ALS at the time of diagnosis strengthens the hypothesis of a role for this chemokine in neurodegenerative disorders.
Mailing address: Dr Tiziana Mennini,Department of Biochemistry andMolecular Pharmacology,Istituto di Ricerche Farmacologiche Mario Negri, Via Eritrea 62, 20156 Milan, ItalyTel: ++390239014402 Fax: ++39023546277e-mail address: [email protected]
Key words: chemokines, IL-8; CXCR2, amyotrophic lateral sclerosis, cerebro spinal fluid
In the last decade, a role has been proposed for glial-induced neuroinflammation in Amyotrophic Lateral Sclerosis (ALS) (1-5). Although contrasting results on cerebro spinal fluid (CSF ) and plasma cytokine levels have been reported in ALS, increased concentrations of interleukin (IL)-6, tumor necrosis factor (TNF) and monocyte chemoattractant protein-1 (MCP-1) do suggest a neuroinflammatory component (6-8) . IL-8 is an important chemotactic factor for the recruitment and activation of polymorphonuclear cells at the site of tissue damage during inflammatory reactions (9). IL-8 is synthesized by glial cells in the central
nervous system and is thought to have an important role in neuroinflammatory events and to be involved in rapid signaling in neurons (10). IL-8 has also been proposed to have a pathological role, since it regulates recruitment of PMN and activates PMN functional activities such as cytokine expression (11) and release of tissue damage mediators from cytoplasmic granules (12). Nevertheless, IL-8 has also been detected in the circulation (9) and in CNS tissue (13) from patients with multiple sclerosis (MS), a disease for which PMN infiltration is not considered a hallmark, although both IL-8 levels and infiltrating PMN have been described in
Vol. 7, no. 1, 39-44 (2009)

40 41Eur. J. Inflamm.
a probability value lower than 0.016 as significant. Univariate and multivariate (multiple regression) analyses were performed in patients with ALS to assess the influence of age, sex, disease duration, and functional disability (measured by the ALS Functional Rating Scale, ALSFRS) on the IL-8 values.
RESULTS
The CSF levels (mean ± SD) of IL-8 are reported in Fig. 1. No statistical differences were found between samples collected in the two participating centres.
ALS patients had IL-8 concentration (23.5 ± 9.2 pg/ml) significantly higher than that found in patients with other, non-inflammatory neurological conditions (15.9 ± 5.5 pg/ml, p= 0.0026). The IL-8 levels in MS patients (25.9 ± 11.0 pg/ml) were significantly higher than those of patients with other, non-inflammatory neurological conditions (p=0.0009), and not different to those of ALS patients (Fig. 1). Multivariate analysis showed that in patients with ALS, sex was the only variable found to affect the IL-8 values, while age, disease duration, and functional disability (measured by the ALS Functional Rating Scale, ALSFRS) had no influence on the IL-8 values. The IL-8 values were 25.7 ± 9.5 pg/ml in men and 18.7 ± 6.9 pg/ml in women (p= 0.0286) (Fig. 2). In control patients with other, non-inflammatory neurological conditions the mean values were 16.2 ± 6.1 and 15.2 ± 4.8 pg/ml in men and women, respectively (p= ns) (Fig. 2). Stratification by gender showed the difference between ALS cases and controls being significant only in men (p= 0.0075 ).
DISCUSSION
Here we report increased IL-8 levels in the CSF of sporadic ALS patients compared to other non-inflammatory neurological diseases. Of interest, the IL-8 levels in ALS patients were similar to those found in MS patients, already reported to be elevated (14). There was no correlation between IL-8 levels and age, disease severity or duration; the only statistical difference was related to gender, with higher levels found in male patients. This is not surprising since gender is known to significantly influence the serum content and production of chemokines like MCP-1, MIP-1 , MIP-1ß and IL-8 (20-22).
opticospinal MS (14) and in myelin oligodendrocyte glycoprotein peptide 35-55-induced experimental autoimmune encephalomyelitis in mice (15). Studies in patients with Alzheimer’s disease, reporting elevated IL-8 levels in cerebrospinal fluid and microvessels, suggest a role for this chemokine also in neurodegenerative disorders (16-17).
Two receptors with high affinity for IL-8 are known, of these CXCR2, differently from CXCR1, is expressed at high levels in some CNS regions, including motor neurons in the anterior horn of human spinal cord (18). We have recently reported that activation of CXCR2 induces dose-dependent death in cultured motor neurons (19). In this study we tested the hypothesis that CSF levels of IL-8 in ALS patients are higher than those of the general population.
MATERIALS AND METHODS
IL-8 determinations CSF was obtained in two hospitals (Istituto Nazionale
Neurologico Carlo Besta and IRCCS Istituto Auxologico Italiano , Milano) from 38 patients with sporadic ALS, 21 MS patients and 18 patients with non-inflammatory neurological diseases after informed consent. Procedures for sampling and storage (at -80°C) did not differ between the two centres. The protocol of the study was approved by our Ethical Committee.
Table I shows the main demographic and clinical features of the sample. The two control groups were selected to provide the cytokine values expected in the general population (non-inflammatory neurological conditions) and in a chronic CNS immune-mediated disorder (MS). None of the cases and the controls were receiving anti-inflammatory drugs at the time of the spinal tap. IL-8 levels in the CSF were determined using a sandwich enzyme-linked immunosorbent assay (ELISA) for human IL-8 (DuoSet ELISA, R&D Systems, Inc., Minneapolis, MN, USA; sensitivity to 8 pg/ml).
Statistical analysisThe distribution of the IL-8 CSF values was tested
with the Shapiro-Wilk test for normality. The values obtained in patients with ALS and in the two control groups were then compared using the non-parametric Wilcoxon test. A probability value of less than 0.05 was regarded as significant. Multiple comparisons were made among the three groups using the non-parametric Kruskal-Wallis test. To identify the comparisons thought to be significant, the Wilcoxon test was used, considering
T. MENNINI ET AL.

40 41Eur. J. Inflamm.
Our data are at variance with the report by Tanaka et al. who did not find differences in the CSF levels of IL-8 between ALS patients and controls with other non inflammatory neurological disease, although the positive correlation between MCP-1 and IL-8 led the authors to suggest a “proinflammatory cytokine cascade after microglial activation” (23). One
possibility to explain this discrepancy is that the difference in our study was evident only in men, and the M/F ratio is 2.2 in our cohort and 1.05 in the study by Tanaka et al.
Another point to be considered is that in their study a large number of controls were subjects with neurodegenerative disorders, and one may 7
Table I. General characteristics of patients with ALS (n=38), non-inflammatory neurological conditions (n=18) and MS (n=21).
ALS
Age (mean ± SD), years
Sex (M/F)
ALS-FRS (mean ± SD)
Disease duration (mean ± SD), months
55 ± 14.8
26/12
33.5 ± 6.3
18.3 ± 14
Controls
Age (mean ± SD), years
Sex (M/F)
Diagnosis:
Cerebrovascular disease (n)
Degenerative dementia (n)
Parkinson�s disease (n)
Compressive radiculo- myelopathy (n)
55 ± 13.9
11/7
10
3
2
3
MS
Age (mean ±SD)
Sex (M/F)
35 ± 7.2
4/17
SD = standard deviation; (n) = number of subjects; M = Male; F = Female ALS = amyotrophic lateral sclerosis; MS = multiple sclerosis ALS-FRS = a validated rating instrument for the monitoring of the progression of disability in patients with ALS, ranging from 0= normal to 40 = maximal deterioration.
Table I. General characteristics of patients with ALS (n=38), non-inflammatory neurological conditions (n=18) and MS (n=21).
SD = standard deviation; (n) = number of subjects; M = Male; F = FemaleALS = amyotrophic lateral sclerosis; MS = multiple sclerosisALS-FRS = a validated rating instrument for the monitoring of the progression of disability in patients with ALS, ranging from 0= normal to 40 = maximal deterioration.

42 43Eur. J. Inflamm.
question that increased cytokine levels could also be found in the controls, as part of the degenerative process. Indeed in our study we have only 6 subjects with neurodegenerative disease. In spite of this low number, if we stratified our controls into two groups, one including non-degenerative conditions (cerebrovascular disorders, compressive radiculo-myelopathy) and the other including dementia and Parkinson’s disease, only in the first case the IL-8 levels are still significantly higher in patients with ALS compared to controls (p=0.0009).
The role of increased IL-8 levels in the CSF of ALS patients is not clear, since samples from affected patients can be obtained only at the time of diagnosis, when symptoms are already fully developed. For this reason, it is unclear whether IL-8 is involved in the pathogenesis of the disease or it better reflects an inflammatory reaction to motor neuron damage. The elective IL-8 increased levels in men seem to favour the former hypothesis.
Interestingly, studies from our group documented that activation of CXCR-2 induces a dose-dependent death on cultured motor neurons (19), thus suggesting that increased IL-8 production by activated glial cells could contribute to motor neuron degeneration
in ALS patients. The efficacy or reparixin, an orally active CXCR1/2 inhibitor, to prevent CXCL2-induced death of motor neurons (25), warrants future investigations about the possible neuroprotective role of CXCR2 inhibitors.
ACKNOWLEDGEMENTS
This work was supported by the Italian Ministry of Instruction, University and Scientific Research
8
Fig. 1. IL-8 levels in CSF. Data are mean values ± SD. The number of subjects analyzed is 38, 21 and 18 for ALS, MS and controls, respectively. Controls were subjects with non-inflammatory neurological conditions. Both ALS and MS groups are different from controls (*p=0.0026, ^ p=0.0009, Wilcoxon test).
ALS MS
Controls
0
10
20
30
40
50
IL8
pg/m
l ^*
Fig. 1. IL-8 levels in CSF. Data are mean values ± SD. The number of subjects analyzed is 38, 21 and 18 for ALS, MS and controls, respectively. Controls were subjects with non-inflammatory neurological conditions. Both ALS and MS groups are different from controls (*p=0.0026, ^ p=0.0009, Wilcoxon test).
T. MENNINI ET AL.
9
ALS FCTR F
0
20
40
60
Female
IL8
pg/m
l
Male
ALS MCTR M
0
20
40
60IL
8 pg
/ml
*^
Fig. 2. IL-8 levels in CSF in male and female ALS patients or and controls. Data are expressed as pg/ml. Each point is the mean value of duplicate samples from each subject. Male ALS patients have significantly higher values than females (^ p=0.0286, Wilcoxon test) and than control patients with other non-inflammatory neurological diseases (*p=0.0075, Wilcoxon test).
9
ALS FCTR F
0
20
40
60
Female
IL8
pg/m
l
Male
ALS MCTR M
0
20
40
60
IL8
pg/m
l*^
Fig. 2. IL-8 levels in CSF in male and female ALS patients or and controls. Data are expressed as pg/ml. Each point is the mean value of duplicate samples from each subject. Male ALS patients have significantly higher values than females (^ p=0.0286, Wilcoxon test) and than control patients with other non-inflammatory neurological diseases (*p=0.0075, Wilcoxon test).
9
ALS FCTR F
0
20
40
60
Female
IL8
pg/m
l
Male
ALS MCTR M
0
20
40
60
IL8
pg/m
l
*^
Fig. 2. IL-8 levels in CSF in male and female ALS patients or and controls. Data are expressed as pg/ml. Each point is the mean value of duplicate samples from each subject. Male ALS patients have significantly higher values than females (^ p=0.0286, Wilcoxon test) and than control patients with other non-inflammatory neurological diseases (*p=0.0075, Wilcoxon test).
Fig. 2. IL-8 levels in CSF in male and female ALS patients or and controls.Data are expressed as pg/ml. Each point is the mean value of duplicate samples from each subject. Male ALS patients have significantly higher values than females (^ p=0.0286, Wilcoxon test) and than control patients with other non-inflammatory neurological diseases (*p=0.0075, Wilcoxon test).

42 43Eur. J. Inflamm.
(grants RBNE01B5WW003 and RBIP06LSS2-006), the Istituto Superiore di Sanità (contract n° 526/A31), and the Italian Ministry of Health (Malattie Neurodegenerative, Ex art 56, 2004, 533F/N/1).
REFERENCES
1. Di Giorgio FP, Carrasco MA, Siao MC, Maniatis T, Eggan K. Non-cell autonomous effect of glia on motor neurons in an embryonic stem cell-based ALS model. Nat Neurosci 2007; 10:608-14.
2. Ghezzi P, Mennini T. Tumor necrosis factor and motoneuronal degeneration: an open problem. Neuroimmunomodulation 2001; 9:178-82.
3. Nagai M, Re DB, Nagata T, Chalazonitis A, Jessell TM, Wichterle H, et al. Astrocytes expressing ALS-linked mutated SOD1 release factors selectively toxic to motor neurons. Nat Neurosci 2007; 10:615-22.
4. Pehar M, Vargas MR, Cassina P, Barbeito AG, Beckman JS, Barbeito L. Complexity of astrocyte-motor neuron interactions in amyotrophic lateral sclerosis. Neurodegener Dis 2005; 2:139-46.
5. Sargsyan SA, Monk PN, Shaw PJ. Microglia as potential contributors to motor neuron injury in amyotrophic lateral sclerosis. Glia 2005; 51:241-53.
6. Moreau C, Devos D, Brunaud-Danel V, Defebvre L, Perez T, Destee A, et al. Elevated IL-6 and TNF-alpha levels in patients with ALS: inflammation or hypoxia? Neurology 2005; 65:1958-60.
7. Baron P, Bussini S, Cardin V, Corbo M, Conti G, Galimberti D, et al. Production of monocyte chemoattractant protein-1 in amyotrophic lateral sclerosis. Muscle Nerve 2005; 32:541-4.
8. Poloni M, Facchetti D, Mai R, Micheli A, Agnoletti L, Francolini G, et al. Circulating levels of tumour necrosis factor-alpha and its soluble receptors are increased in the blood of patients with amyotrophic lateral sclerosis. Neurosci Lett 2000; 287:211-4.
9. Lund BT, Ashikian N, Ta HQ, Chakryan Y, Manoukian K, Groshen S, et al. Increased CXCL8 (IL-8) expression in Multiple Sclerosis. J Neuroimmunol 2004; 155:161-71.
10. Puma C, Danik M, Quirion R, Ramon F, Williams S. The chemokine interleukin-8 acutely reduces Ca(2+) currents in identified cholinergic septal neurons expressing CXCR1 and CXCR2 receptor mRNAs. J
Neurochem 2001; 78:960-71.11. Martinez FO, Sironi M, Vecchi A, Colotta F,
Mantovani A, Locati M. IL-8 induces a specific transcriptional profile in human neutrophils: synergism with LPS for IL-1 production. Eur J Immunol 2004; 34:2286-92.
12. Baggiolini M, Loetscher P. Chemokines in inflammation and immunity. Immunol Today 2000; 21:418-20.
13. Omari KM, John GR, Sealfon SC, Raine CS. CXC chemokine receptors on human oligodendrocytes: implications for multiple sclerosis. Brain 2005; 128:1003-15.
14. Ishizu T, Osoegawa M, Mei FJ, Kikuchi H, Tanaka M, Takakura Y, et al. Intrathecal activation of the IL-17/IL-8 axis in opticospinal multiple sclerosis. Brain 2005; 28:988-1002.
15. Walter S, Doering A, Letiembre M, Liu Y, Hao W, Diem R, et al. The LPS receptor, CD14, in experimental autoimmune encephalomyelitis and multiple sclerosis. Cell Physiol Biochem 2006; 17(3-4):167-72.
16. Galimberti D, Schoonenboom N, Scheltens P, Fenoglio C, Venturelli E, Pijnenburg YA, et al. Intrathecal chemokine levels in Alzheimer disease and frontotemporal lobar degeneration. Neurology 2006; 66:146-7.
17. Grammas P, Samany PG, Thirumangalakudi L. Thrombin and inflammatory proteins are elevated in Alzheimer’s disease microvessels: implications for disease pathogenesis. J Alzheimers Dis 2006; 9:51-8.
18. Horuk R, Martin AW, Wang Z, Schweitzer L, Gerassimides A, Guo H, et al. Expression of chemokine receptors by subsets of neurons in the central nervous system. J Immunol 1997; 158:2882-90.
19. De Paola M, Buanne P, Biordi L, Bertini R, Ghezzi P, Mennini T. Chemokine MIP-2/CXCL2, Acting on CXCR2, induces motor neuron death in primary cultures. Neuroimmunomodulation 2008; 14:310-6.
20. Holven KB, Myhre AM, Aukrust P, Hagve TA, Ose L, Nenseter MS. Patients with familial hypercholesterolaemia show enhanced spontaneous chemokine release from peripheral blood mononuclear cells ex vivo. Dependency of xanthomas/xanthelasms, smoking and gender. Eur

44 EUROPEAN JOURNAL OF INFLAMMATION
1721-727X (2009)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties45
Heart J 2003; 24:1756-62.21. Jilma-Stohlawetz P, Homoncik M, Drucker C, Marsik
C, Rot A, Mayr WR, et al. Fy phenotype and gender determine plasma levels of monocyte chemotactic protein. Transfusion 2001; 41:378-81.
22. Targowski T, Jahnz-Rozyk K, Plusa T, Glodzinska-Wyszogrodzka E. Influence of age and gender on serum eotaxin concentration in healthy and allergic
people. J Investig Allergol Clin Immunol 2005; 15:277-82.
23. Tanaka M, Kikuchi H, Ishizu T, Minohara M, Osoegawa M, Motomura K, et al. Intrathecal upregulation of granulocyte colony stimulating factor and its neuroprotective actions on motor neurons in amyotrophic lateral sclerosis. J Neuropathol Exp Neurol 2006; 65:816-25.
T. MENNINI ET AL.

44 EUROPEAN JOURNAL OF INFLAMMATION
1721-727X (2009)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties45
A LUPUS HEPATITIS CASE AND ITS ASSOCIATION WITH IgM ANTIBODIES AGAINST CYTOMEGALOVIRUS, HERPES SIMPLEX AND HERPES ZOSTER VIRUSES
A. RICCIO1, G. MORELLI2, M.G. SANGIOLO1, R. MORANTE3, C. ESPOSITO2
and G. TARANTINO1
Departments of 1Clinical and Experimental Medicine and 3Public Medicine, Federico II° University Medical School of Naples, Naples; 2”Domenico Cotugno” Hospital, Naples, Italy
Received May 20, 2008 – Accepted February 2, 2009
The hypothesis for a role of viral infections on the pathogenesis of systemic lupus erythematosus has been discussed in many works, particularly that of cytomegalovirus and Epstein Barr virus infections as trigger of autoimmune processes. Here, we describe the case of a young woman affected by systemic lupus erythematosus with marked hepatic involvement presenting IgM antibodies against cytomegalovirus, herpesvirus and herpes zoster virus in the absence of virus. The meaning of these laboratory findings is discussed.
LETTER TO THE EDITOR
Mailing address: Antonio Riccio, MDDepartment of Clinical and Experimental Medicine, Federico II° University, Medical School of Naples, Via S. Pansini 5, 80131 Naples, ItalyTel/Fax: ++39 081 7462051 e-mail: [email protected]
Key words: systemic lupus erythematosus, cytomegalovirus, herpes zoster virus, Epstein Barr virus, antibodies
Anti-cytomegalovirus (CMV), anti-Epstein Barr Virus (EBV) and anti-Herpes Zoster Virus (HZV) antibodies have often been found in the serum of patients with Systemic Lupus Erythematosus (SLE) (1-6). These findings led to the hypothesis for a role of viral infections on the pathogenesis of this disease, through a mechanism of immunologic cross reactivity of viral antigens with self-antigens, that could induce the synthesis of antiviral antibodies reacting with autoantigens. Such mechanism has been recognized with proteinic components of EBV and CMV (7-10).
Although viral infections were seen as possible causes of inducing the autoimmune process, the altered immune system of such patients could also suggest that infection is an effect rather than a cause of immune over-reaction.
In the present case we report the contemporary presence of anti-CMV, anti-Herpesvirus (HSV) and anti-HZV IgM antibodies in the course of SLE, in
the absence of respective viruses.
Case reportA 22 year-old female patient suffering from
diffuse arthralgias, asthenia and irregular fever with peaks of 39°C every 4-5 days and periods of apyrexia was hospitalized in May 2007. About 10 months prior the observations, mild leukopenia (WBC= 3200/mm3), with granulocytopenia, and increased levels of gamma globulins (24%) had been recorded. Historically, no other symptom has been described, except for the occasional appearance of photosensitivity and malar rash in the last months. Clinical examination at hospitalization revealed only a mild malar rash, hepatomegaly, and left latero-cervical lymph node enlargement. As presented in Table I, laboratory data revealed high erythrocyte sedimentation rate (ESR) (Ia h 50mm), increased levels of gamma globulins, anemia, leukopenia, decreased levels of serum complement fractions
Vol. 7, no. 1, 45-48 (2009)

46 47Eur. J. Inflamm.
Chemiluminescence (Kit DiaSorin, Saluggia, Italy) revealed the presence of anti-CMV, anti-HSV and anti-HZV IgM, and absence of anti-EBV IgM, while IgG antibodies for all these viruses were present. A multiplex polymerase chain reaction (PCR) assay (ARROW Diagnostics – Genova, Italy), performed on plasma sample to amplify herpes simplex virus types 1 and 2, cytomegalovirus, and varicella-zoster virus DNA in the serum, revealed absence of CMV, HZV and HSV. Then, the hypothesis of viral infection was dismissed (11), diagnosis of SLE was made and steroid treatment was started (prednisone 50 mg daily). Fever and arthralgias disappeared within 48 hours, and two weeks later a significant decrease of ESR (Ia h= 5), and increased levels of serum C3, C4 and WBC were
(C3 and C4). Hepatic involvement was evidenced by changes in serum enzyme activities such as increased levels of thransaminases (AST, ALT), gamma-glutamyl-transpeptidase (GGT), and lactate-dehydrogenase (LDH), while alkaline phosphatase (ALP) and creatin kinase (CPK) were within the normal ranges. HBsAG and HCV-Ab were absent. Antinuclear antibodies were present, with anti-nDNA antibodies and ENA (ELISA method, QUANTA Lite™ ENA 4-Company, INOVA Diagnostic, Inc., S.Diego, USA) being at high levels. Anticardiolipin antibodies and lupus anticoagulant were negative (ELISA method, QUANTA Lite™ ACA Screen III-Company, INOVA Diagnostic, Inc., S. Diego, USA). Liver biopsy to evidence hepatic damage was not accepted by the patient.
8
Table I. Main laboratory findings of the patient before treatment.
RBC (cells/mm3) 3,870,000 WBC (cells/mm3) 3,600 Platelets (cells/mm3) 254,000 Haemoblobin (g/dl) 11.7 AST(U/l) 182 ALT (U/l) 189 GGT (U/l) 70 LDH (U/l) 580 ALP (U/l) 62 C3 (g/l) 0.247 (RV= 0.90 -1.80) C4 (g/l) 0.049 (RV = 0.10 � 0.40) ANA (IU/ml)* 8.40 (RV < 1) ENA* Positive Anti-nDNA antibodes (IU/ml)* 405 (RV < 25) CIC-C1q (µg/ml) 79 (RV < 40) CIC-3d (µg/ml) 68 (RV < 24) ESR (Ia h mm) 50 Anti-CMV IgM antibodies �Anti-CMV IgG antibodies
PositivePositive 22,00 I.U./ml (n.v. 0,4 � 0,6)
Anti-HSV IgM antibodies �Anti-HSV IgG antibodies
PositivePositive
Anti-HZV IgM antibodies �Anti-HZV IgG antibodies
PositivePositive 400 mI.U./ml (n.v. 135 � 165)
Anti-EBV IgM antibodies ° Anti-EBV IgG antibodies
NegativePositive 129 U.A./ml
PCR for CMV negative PCR for HSV negative PCR for HZV negative C: Complementemia; ESR: Erythrocyte Sedimentation Rate; CIC: circulating immune
complexes; ANA: Antinuclear antibodies; ENA: extractable nuclear antibodies; PCR: polymerase chain reaction; RV: reference values; *ELISA method was used for ANA, ENA and anti-n DNA research; � chemiluminescence was used for detection of antiviral IgM
Table I. Main laboratory findings of the patient before treatment.
C: Complementemia; ESR: Erythrocyte Sedimentation Rate; CIC: circulating immune complexes; ANA: Antinuclear antibodies; ENA: extractable nuclear antibodies; PCR: polymerase chain reaction; RV: reference values; *ELISA method was used for ANA, ENA and anti-n DNA research; ° chemiluminescence was used for detection of antiviral IgM
A. RICCIO ET AL.

46 47Eur. J. Inflamm.
recorded, while thransaminases were nearly normal. This dosage of steroids was administered for a month and then every 20 days reduced by 10 mg/daily, until reaching a maintenance dose of 15 mg/daily.
In the follow-up (the last time was eight months later) clinical conditions improved: fever and arthralgias were absent, hepatomegaly and lymph node enlargement disappeared. During the follow-up hydroxychloroquine was added to the therapy (200 mg orally twice daily) for the treatment of malar rash.
DISCUSSION
Viruses have been speculated as possible causes of the autoimmune process in SLE (12). In our case, clinical and immunological findings indicated a diagnosis of SLE and, in this regard, the positivity for anti-CMV, anti-HSV and anti-HZV IgM suggested a possible trigger role of viral infections in the onset of the disease. However, the eventual presence of viral agents was considered an obstacle to begin steroid treatment, because of the risk of encephalitis, so Multiplex PCR assay was performed to confirm the presence of viral antigen, and the negativity of this test for all these viruses induced a revision of the viral hypothesis: the absence of viral antigen suggested that anti-viral IgM antibodies could be considered not specific. This possibility has been already described in the course of lupus nephritis (13); obviously, this does not exclude the pathogenic role of viral agents in the beginning of autoimmune process, suggested by many studies (1-6, 14). On the basis of our data, the hypothesis of a transient viraemia with maintenance of specific IgM antiviral antibody synthesis cannot be excluded, but this possibility appears unlikely in our case: first of all, the acute hepatic injury, so evident in our patient, is difficult to explain in the absence of viral replication, and then the ready response to the steroid treatment is typical of an autoimmune condition rather than a viral infection. Our patient refused liver biopsy, but it must be remembered that hepatic damage in the course of SLE occurs in about 25% of cases and its histologic features are unfortunately not specific (15). Concerning the aspecificity of IgM antibodies, a pre-existing autoimmune condition, without clinical evidence, is reinforced by previous laboratory
findings indicating granulocytopenia and immune hyperactivity (increased levels of gamma globulins) ten months before the onset of the symptomatology.
The causes of false positivity in the course of SLE are still unknown, they could be linked to the hyperactivity of B cells, typical of this disease, but until now literature data on this specific point are poor. However, the present study indicates the need to detect, by PCR, the viral replication in all the cases presenting these autoantibodies. There is no agreement among the authors about the possibility of excluding virus infection by PCR, but, at the present time, it is the most widely used method to evidence viral replication. To the best of our knowledge this presentation is the first evidence of non-specific IgM antibodies in course of SLE with prevalent hepatic involvement.
REFERENCES
1. Pincus T. Studies regarding a possible function for viruses in the pathogenesis of systemic lupus erythematosus. Arthritis Rheum 1982; 25:847-56.
2. Sekigawa I, Nawata M, Seta N, Yamada M, Iida N, Hashimoto H. Cytomegalovirus infection in patients with systemic lupus erythematosus. Clin Exp Rheumatol 2002; 20:559-64.
3. Barzilai O, Sherer Y, Ram M, Izhaky D, Anaya JM, Shoenfeld Y. Epstein Barr virus and cytomegalovirus in autoimmune diseases: are they truly notorious? A preliminary report. Ann NY Acad Sci 2007; 1108:567-77.
4. Nagasawa K, Yamauchi Y, Tada Y, Kusaba T, Niho Y, Yoshikawa H. High incidence of herpes zoster in patients with systemic lupus erythematosus: an immunological analysis. Ann Rheum Dis 1990; 49:630-3.
5. Yamauchi Y, Nagasawa K, Tada Y, Tsukamoto H, Yoshizawa S, Mayumi T, Niho Y, Kusaba T. Herpes zoster in connective tissue diseases: association with systemic lupus erythematosus and its immunological abnormalities. Kansenshogaku Zasshi 1991; 65:851-6.
6. James JA, Kaufman KM, Farris AD, Taylor-Albert E, Lehman TJ, Harley JB. An increased prevalence of Epstein Barr virus infection in young patients suggests a possibile etiology for systemic lupus

48 EUROPEAN JOURNAL OF INFLAMMATION
1721-727X (2009)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties49
erythematosus. J Clin Invest 1997; 100:3019-26.7. Petri M. Infection in systemic lupus erythematosus.
Rheum Dis Clin North Am 1998; 24:423-56.8. Denman AM. Systemic lupus erythematosus – is a
viral aetiology a credible hypothesis? J Infect 2000; 40:229-33.
9. Incaprera M, Rindi L, Bazzichi A, Garzelli C. Potential role of Epstein Barr virus in systemic lupus erythematosus autoimmunity. Clin Exp Rheumatol 1998; 16:289-94.
10. James JA, Nears BR, Moser KL et al. Systemic lupus erythematosus in adults is associated with previous Epstein Barr virus exposure. Arthritis Rheum 2001 May; 44:1122-6.
11. Druce J, Catton M, Chibo D, et al. Utility of a multiplex PCR assay for detecting erpesvirus DNA in clinical
samples. J Clin Microbiol 2002; 40:1728-32.12. Chang M, Pan MR, Chen DY, Lan JL. Human
cytomegalovirus pp65 lower matrix protein: a human immunogen for systemic lupus erythematosus patients and autoantibody accelerator for NZB/W F1 mice. Clin Exp Immunol 2006; 143:167-79.
13. Stratta P, Colla L, Santi S, et al. IgM antibodies against cytomegalovirus in SLE nephritis: viral infection or aspecific antibody? J Nephrol 2002; 15:88-92.
14. Rider JR, Ollier WE, Lock RJ, Brookes ST, Pamphilon DH. Human cytomegalovirus infection and systemic lupus erythematosus. Clin Exp Rheumatol 1997; 15:405-9.
15. Dienes H.P. Viral and autoimmune hepatitis. Fischer Verlag, Stuttgart, 1989; p. 47.
A. RICCIO ET AL.

48 EUROPEAN JOURNAL OF INFLAMMATION
1721-727X (2009)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties49
SERUM IL-17 AFTER ONE COURSE OF SUBLINGUAL IMMUNOTHERAPY IN ALLERGIC RHINITIS TO BIRCH
G. CIPRANDI, D. FENOGLIO, M. DE AMICI1, G. MARSEGLIA1, G. MURDACA and M. DI GIOACCHINO2
Department of Internal Medicine, Azienda Ospedaliera Universitaria San Martino, University of Genoa, Genoa; 1Department of Pediatric Science, Pediatric Clinic, University of Pavia, Foundation IRCCS San Matteo, Pavia; 2Allergy-Related Disease Unit, “G. d’Annunzio University” Foundation,
Chieti, Italy
Received July 15, 2008 – Accepted February 4, 2009
Recently, it has been reported that IL-17 may be involved in allergic reaction. Sublingual immunotherapy (SLIT) is the unique curative treatment for allergic rhinitis. This study aims at investigating whether one course of birch SLIT could affect serum IL-17 levels. The findings provided show that some IL-17 producer patients had a reduction of serum IL-17 levels after one SLIT course. Therefore, this preliminary study shows that a single pre-seasonal SLIT course may induce a significant decreasing trend in serum IL-17 levels; further study should be carried out to define the role exerted by IL-17 in allergic rhinitis.
LETTER TO THE EDITOR
Mailing addressGiorgio Ciprandi, M.D.Ospedale San MartinoLargo R. Benzi 1016132 Genoa, ItalyTel: ++39 10 35338120 Fax: ++39 10 3537573e-mail [email protected]
Key words: IL-17, allergic rhinitis, sublingual immunotherapy
Allergic rhinitis (AR) is characterised by an inflammatory reaction, sustained by Th2 polarization. Peripheral blood mononuclear cells of AR patients display a predominant IL-4 production by Th2 cells compared to IFN-γ expression by Th1 cells, thus confirming the functional dichotomy between Th1 and Th2 cells. This bivalent concept has since been modified by the discovery of T-regulatory (Treg) and Th17 cells. As recently pointed out, the discovery of Th17 cells has been fundamental to our understanding of how Th1 cells can actually mediate inflammatory events by producing IFN-γ (1).
Th17 cells are characterized by the production of various cytokines, including IL-17, IL-6, TNF-α, and IL-22. IL-17 may be involved in allergic disorders as anti-IL-17 has been demonstrated to reduce neutrophil infiltration in an experimental
asthma model (2), and, on the other hand, increases eosinophil infiltration. Furthermore, IL-17 induces recruitment and is a survival factor for airway macrophages (3). These facts seem to suggest a regulatory role of IL-17. It appears that Th-17-dependent neutrophil infiltration is inversely related with Th2-dependent eosinophil involvement, similar to the dichotomic Th1-Th2 balance. In addition, animal models indicate that IL-17 might play a pro-inflammatory role. Indeed IL-17 induces the expression of pro-inflammatory cytokines, including TNF-α, IL-1β, and IL-6, and some chemokines, such as CXCL1, 2, and 8, all of which are markers of acute inflammatory events (1). These chemokines induce neutrophil recruitment which may be considered the hallmark functional activity of Th17: neutrophilic inflammation. However, the
Vol. 7, no. 1, 49-51 (2009)

50 51Eur. J. Inflamm.
reported as mean (M), deviation standard (DS) and median (MD). The non- parametric Wilcoxon test was performed to evaluate the differences between allergic/non-allergic subjects and in allergic patients before and after 3 months of SLIT. The package “S-Plus” (MathSoft Corp.) was used for all the analyses.
In 12 of the 19 allergic patients, IL-17 levels at baseline were undetectable, these patients were therefore defined as IL-17 non-producers. In the remaining 7 patients, M levels at baseline were 35.87±49.41 SD pg/ml (MD 25.63); these patients were defined as IL-17 producers. A significant difference (p=0.0176) in serum levels was observed between baseline of IL-17 producer allergic patients (M 35.87±49.41 DS pg/ml; 25.63 MD) and healthy subjects with IL-17 detected (M 1.94±1.68 DS pg/ml; MD 1.33). In IL-17 producer allergic patients, serum levels were observed to significantly decrease (p=0.0213) 3 months after the SLIT course to M 11.59±28.59 DS pg/ml (MD 0.84 pg/ml) (Fig.1). On the contrary, serum levels were unmodified in IL-17 non-producer allergic patients after SLIT.
This preliminary study shows that a single pre-seasonal SLIT course may induce a significant decreasing trend in serum IL-17 levels; further study should be performed to define the role exerted by IL-17 in allergic rhinitis.
role of Th17 cells in allergic inflammation is still unclear. Experimental studies seem to suggest that Th17 cells may be involved in the process of neutrophilic infiltration that occurs during the acute phase of allergic reaction. In this regard, neutrophil infiltration is also observed in acute asthma attacks as well as during the early phase following allergen-specific challenge (4).
Sublingual immunotherapy (SLIT) is the unique causal treatment for AR affecting immune response (5). However, no study has investigated the possible effect of SLIT on serum IL-17 levels. Thus, the aim of this preliminary study is to evaluate IL-17 serum levels in a group of AR patients.
Nineteen patients (11 males and 8 females, mean age: 42 years), with birch AR, were evaluated according to ARIA criteria (6). The patients’ blood samples for assessing IL-17 serum levels were collected before initiating SLIT (baseline) and three months after the end of the pre-seasonal SLIT course (Anallergo, Florence, Italy). Serum samples from 8 healthy donors were also tested as controls.
The human interleukin 17 (IL-17) Immunoassay (R&D Systems) employs the quantitative sandwich enzyme immunoassay technique and was performed according to the Manufacturer’s Instructions and expressed as pg/mL. Descriptive statistics were first performed and quantitative parameters were
Fig. 1. Serum IL-17 distribution in IL-17 producer allergic patients (T0= Baseline; T2= 3 months after SLIT course) and healthy subjects. Values are represented as Mean and Standard Deviation.
Fig. 1. Serum IL-17 distribution in IL-17 producer allergic patients (T0= Baseline; T2= 3 months after SLIT course) and healthy subjects. Values are represented as Mean and Standard Deviation.
G. CIPRANDI ET AL.

50 51Eur. J. Inflamm.
ACKNOWLEDGEMENTS
The authors wish to thank Cristina Torre (Clinica Pediatrica, Fondazione IRCCS Policlinico S. Matteo) for outstanding technical support, Vania Giunta (Dipartimento di Informatica e Sistemistica, Università di Pavia) for data analysis, and Laurene Kelly for correction of the English.
REFERENCES
1. Schmidt-Weber CB, Akdis M, Akdis CA. Th17 cells in the big picture of immunology. J Allergy Clin Immunol 2007; 120:247-54.
2. Hellings PW, Kasran A, Liu Z, Vandekerckhove P, Wuyts A, Overbergh L, et al. IL-17 orchestrates the granulocyte influx into airways after allergen inhalation in a mouse model of allergic asthma. Am J Resp Cell Mol Biol 2003; 28:42-50.
3. Sergejeva S, Ivanov S, Lotvall J, Linden A. IL-17 as a recruitment and survival factor for airway macrophages in allergic airway inflammation. Am J Resp Cell Mol Biol 2005; 33:248-53.
4. Ciprandi G, Buscaglia S, Pesce GP, Villaggio B, Bagnasco M, Canonica GW. Allergic subjects express intercellular adhesion molecule-1 (ICAM-1 or CD54) on epithelial cells of conjunctiva after allergen challenge J Allergy Clin Immunol 1993; 91:783-91.
5. Bousquet J, Lockey RF, Malling HJ. WHO position paper. Allergen immunotherapy: therapeutic vaccines for allergic disease. Allergy 1998; 531-42.
6. Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 Update (in collaboration with the World Health Organization, GA2LEN and AllerGen). Allergy 2008; 63:8-160.