uva-dare (digital academic repository) on vascular factors ... file50b_bw_dalen_stand.job 100...
TRANSCRIPT

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
On vascular factors, apathy and dementia
van Dalen, J.-W.
Link to publication
Citation for published version (APA):van Dalen, J-W. (2018). On vascular factors, apathy and dementia.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 16 Aug 2019

50A_BW_Dalen_Stand.job
99
Chapter 6
Post-stroke apathy
-
a systematic review and meta-analysis
Jan Willem van Dalen
Eric P. Moll van Charante
Paul J. Nederkoorn
Willem A. van Gool
Edo Richard

50B_BW_Dalen_Stand.job
100
Introduction
In addition to acute motor, sensory, and language impairments, sub-acute and chronic neuropsychiatric
disturbances after stroke can have major impact on activities of daily living (ADL).1 Cognitive
impairment and depression are the most commonly reported neuropsychiatric symptoms, both occurring
in approximately in one third of patients after stroke.2;3 Apathy, most commonly defined as a syndrome
of diminished goal-directed behaviour, emotion, and cognition,4 is far less studied but has also been
reported as a frequent consequence of stroke. Apathy can have negative impact on functional recovery,
activities of daily living, general health and quality of life.5-7 It can also lead to significant burden for
caregivers.8;9
Apathy can occur as an independent syndrome, although it may also occur as a symptom of depression
or dementia.10;11 Patients present with loss of motivation, concern, interest and emotional response,
resulting in a loss of initiative, decreased interaction with their environment and a reduced interest in
social life.11-14 Despite its potentially pervasive and negative consequences, the importance of post-stroke
apathy is difficult to interpret. Differences in study design, results and interpretation have lead to a wide
variety in reported characteristics, prevalence and clinical impact.15;16
In this systematic review and meta-analysis we aim to establish the impact of post-stroke apathy by
assessing the prevalence and the association with disability, depression and cognitive impairment. In
addition, the influence of lesion location on the occurrence of apathy and the possibilities for
pharmacological treatment are systematically reviewed.
Methods
Search strategy
We conducted a comprehensive literature search of the Medline, PsycINFO and Embase (from 1980
onwards) databases. Methods were predetermined in a research protocol. Key search terms for stroke
were cross-referenced to apathy, closely related or descriptive terms for apathy and psychometric
instruments to assess apathy. The full search strategy, including all search terms, is specified in appendix
S1. The search was last updated on the 21st of February 2012. Titles, abstracts and papers were reviewed
by two independent observers (JWD and ER) to assess inclusion criteria. If necessary, full text copies of
articles were obtained. Discrepancies of the two separate selections were compared and were resolved by
discussion. A third investigator (PJN) was available for appeal if disagreements persisted. In addition,
references of all included articles and reviews, and key publications were searched for studies that met
inclusion criteria.
Inclusion criteria were based on recommendations by the Centre for Reviews and Dissemination
(CRD).17 Studies were included if they 1) were on patients with symptomatic stroke, 2) included at least
25 patients, 3) clearly specified a definition of apathy, 4) reported on patient characteristics, selection
process and method of inclusion, 5) were not restricted to specific stroke localisations, 6) were written in

51A_BW_Dalen_Stand.job
101
a European national language, Chinese or Japanese. If there was more than one publication on the same
patient cohort, data were taken from the publication on the most comprehensive stroke-patient group.
Because of a lack of large studies on treatment of post-stroke apathy, our inclusion criteria for this
research question were less strict. Articles on the effect of pharmacological treatment of apathy were
included if they were 1) on patients with symptomatic stroke, and 2) were written in English.
Data extraction
Full text articles of selected studies were obtained for further evaluation. Data from each study were
extracted by two observers (JWD and ER), using a predefined data extraction form (appendix S2).
Authors were contacted if published results lacked information necessary for the meta-analyses. Risk of
bias was assessed using an assessment form based upon the Newcastle–Ottawa quality assessment scale
for cohort studies, and rated selection, confounding and information bias sub-items (appendix S3).18
Statistical analysis
Analysis of statistical heterogeneity of apathy rate between studies was done with I2 tests in every meta-
analysis. Risk of publication bias was assessed by visual interpretation of the funnel plot. The pooled
estimate of the prevalence of apathy in a stroke-population was obtained using the DerSimonian and
Laird random effects binary model. For each proportional characteristic, 95% confidence intervals
(95%CI) were estimated using binomial distribution. When a study provided more than one apathy rate
in a single cohort (e.g. at a different time since stroke or with a different method of assessment used), we
calculated one average apathy rate per study to include in the meta-analysis. To identify variables
associated with post-stroke apathy, separate meta-analyses were performed for age, sex, mini mental state
examination (MMSE) score, depression and disability at assessment. These factors were derived from the
literature. We used a binary random effects model for analysis of the relative risk of apathy for depressed
patients and female patients. A continuous random effects model with unequal within-study variance was
used to estimate associations with age, MMSE score, and disability. Because of the different scales used
to assess disability, we standardized the disability scores using the Hedges’ G method.19 When multiple
values for these factors at different time points were provided in one single cohort, we calculated one
average value and standard deviation for meta-analysis. The relationship of apathy with functional
recovery and with lesion location was assessed qualitatively.
A pre-specified sensitivity analysis was designed to assess the influence of the definition of apathy used
and that of suspected confounding variables. This analysis only included studies reporting on all proposed
explanatory variables and used methods of apathy assessment recommended in an extensive review of
the psychometric evidence on the validity of available apathy measures.15 Two additional analyses were
performed to explore heterogeneity of studies in our main analysis. In the first, to determine the
individual effect of each study on the overall estimate, a range of overall apathy rates was estimated by

51B_BW_Dalen_Stand.job
102
leaving out one study at the time, for all studies (jackknife analysis). The second analysis only included
studies which we estimated to have a relatively low risk of confounding and selection bias (for criteria
and selected studies see appendix S3). To this analysis, we added a sensitivity analysis in which we
excluded studies with an average age below 60 years old, since these may not be representative for the
general stroke population.
Several further exploratory subgroup analyses were performed on the type of assessment instrument
used, source of information (patient-based, informant-based or clinician-based apathy rating scale),
setting, time passed since stroke, exclusion criteria, prior history of stroke and type of stroke included.
These subgroup analyses were not pre-specified but were defined during analysis to explore potential
reasons for large differences between study results. Univariate inverse-varience weighted meta-regression
was used to estimate the effect of age, depression rates and MMSE scores on reported apathy-rate.
Microsoft Office Excel 2003, PASW Statistics 18, and Meta-analyst beta 3.13 were used for the statistical
analysis.20
Results
Our search yielded 5463 articles, of which 4328 remained after duplicate removal (figure 1). In total, 49
research articles were selected for full text analysis. Eight full articles and two abstracts of case-reports
on treatment could be obtained. For reference search 27 reviews were selected of which 19 could be
obtained. Searching the references yielded one additional article on treatment and none on prevalence
(figure 1). After further evaluation, 24 articles on prevalence and 11 on treatment were included in our
review. Reasons for exclusion of studies are listed in appendix S1. After quality assessment, we included
24 articles on the prevalence of apathy.5;6;21-42 Table 1 shows the study design and demographic details of
all 24 selected studies. To supplement data, 22 authors were contacted, of whom nine were able to
complement the data of ten studies.33-42 Assessment of the risk of bias per study is provided in appendix
S3.

52A_BW_Dalen_Stand.job
103
Figure 1: article selection
55463 references from electronic search
1942 from Medline 2011 from Embase
4328 abstracts
1135 duplicates removed
74 selected articles41 on prevalence
19 reviews 10 on treatment
36 articles excluded after full review 19 reviews 7 not concerning apathy 6 same cohort 4 cohort restricted to subcategory
1 article from references1 on treatment
35 articles included in review:24 articles on prevalence 11 articles on treatment
88 selected articles 49 on prevalence
27 reviews 11 on treatment 17 articles unavailable
8 reviews 8 conference/dissertation abstracts Treatment: 1 case report

52B_BW_Dalen_Stand.job
104
AAuth
or
CCoh
MMaj
or e
xclu
sion
crite
ria
EEx
RRecr
uitm
ent
SStro
ke
AApat
hy
DDepr
CCo
gn
SStro
ke se
verit
y DDi
sabi
lity
((yea
r)
AAge
DDis
CCI
MMD
CCD
%%
ssett
ing
pperio
d tty
pe
ccrite
rion
mmea
s mm
eas
mmea
s mm
ean
mmea
s mm
ean
Star
kste
in
(199
3) 3
0 PC
-
- ye
s -
- 17
%
sub
acut
e <
1993
1st
IH
AS
>1
3 (s
) H
DSa
MM
SEb
- -
JHFI
c 6/
27
(i)
Mar
in
(199
4) 2
8 RC
45
- 85
ye
s -
- -
n.r.
outp
<
1991
I
AES
>3
8 (c
) H
RSD
MM
SE
- -
-
-
Ande
rsso
n
(199
9) 2
2 CC
-
- ye
s hi
st
yes
n.a.
in
p re
hab
- IH
AE
S
>33
(c)
MAD
RSa
- -
- -
-
Ange
lelli
(200
4) 2
1 CS
-
yes
yes
- ye
s n.
r. in
- and
ou
tp
1999
- 20
02
1st
I N
PI >
95p
cont
rol (
c)
NPI
Ra
ven
test
-
- FI
M
85.7
/ 10
0 (d
)
Piam
arta
(200
4) 2
7 PC
<6
0 ye
s -
hist
ye
s n.
r. su
b ac
ute
-
1st
IH
Exp.
PSD
RS
PSDR
S SP
SMQ
N
IHSS
2,
9/
42 (i
) BI
c 79
.7/
100
(d)
Brod
aty
(200
5) 2
3 PC
>8
5 -
yes
- ye
s 34
%
in- a
nd
outp
19
97-
2000
I
AES
>3
7 (i)
SC
ID-1
a M
MSE
b ES
S 93
,5/
100
(d)
IADL
c , AD
Lc 7/
8,
5/6
(i)
Caro
ta
(200
5) 3
5 PC
-
yes
- -
- 16
%
inp
1995
- 19
99
I EB
IFn
>0 (c
) Su
bj.
yes/
no
-
- BI
80
/ 10
0 (d
)
Hoc
hste
nbac
h
(200
5) 24
PC
>6
9 ye
s -
< 10
ye
ars
- n.
r. ou
tp
1992
- 19
96
IH
Que
st.
(s, i
) Q
uest
. (s
) -
-
- IA
DL
-
Caei
ro
(200
6) 3
3 PC
-
- -
- ye
s 18
%
sub
ac
ute
- IH
PS
DRS
(c
) M
ADRS
a M
MSE
N
IHSS
-
mRS
-
Kaji
(200
6) 2
5 PC
-
- ye
s -
yes
0%
sub
ac
inp
2004
- 20
05
IH
AS
>15
(s)
HAM
D17a
+MIN
I -
- -
-
-
Ham
a
(200
7) 5
PC
-
- -
hist
ye
s 40
%
inp
reha
b 20
02-
2006
IH
AS
>15
(s)
NPI
>0
(i)
SDS
MM
SE
- -
FIM
d 77
/ 12
6 (d
)
Jarz
ebsk
a
(200
7) 2
6 PC
-
- -
- ye
s 18
%
sub
acut
e 20
04-
2005
I
AS
>13
(s)
HAM
-D
MM
SEb
- -
-
-
Sant
a
(200
8) 3
2 PC
45
- 90
-
yes
- ye
s n.
r. in
p re
hab
1999
- 20
01
1st
IH
AS
>15
(s)
SDS
MM
SE
NIH
SS
9,2/
42
(i)
NIH
SSd
9/
42 (i
)
Tabl
e 1.
Stu
dy c
hara
cter
istic
s

53A_BW_Dalen_Stand.job
105
AAuth
or
CCoh
MMaj
or e
xclu
sion
crite
ria
EEx
RRecr
uitm
ent
SStro
ke
AApat
hy
DDepr
CCo
gn
SStro
ke se
verit
y DDi
sabi
lity
((yea
r)
AAge
DDiss
CCI
MMD
CCD
%%
ssett
ing
pperio
d tty
pe
ccrite
rion
mmea
s mm
eas
mmea
s mm
ean
mmea
s mm
ean
Gre
enop
(2
009)
37
PC
- ye
s -
- ye
s 90
%
in- a
nd
outp
20
03-
2005
IH
N
PI
>0 (i
) N
PI-i
CAM
COG
b -
- M
FAQ
-IA
DL
2.8/
8
(i)
May
o (2
009)
6 PC
-
yes
- -
- 40
%
in- a
nd
outp
20
03-
2004
IH
W
BIBS
(i)
SF
-36
MM
SE
(tel
epho
ne)b
CNS
8.3/
11
.5(d
) SI
S-ph
ysc,
d
65.6
/ 10
0 (d
)
Hof
fman
n (2
010)
38
PC
18-
90
yes
yes
curr
ent
yes
96%
in
p 20
03-
2006
IH
FR
SBE
>65
excl
uded
FR
SBE,
CCN
, W
CST
NIH
SS
3.3/
42
(i)
NIH
SS
33.3/
42
(i)
Ono
da
(201
0) 4
0 PC
-
- -
hist
ye
s n.
r. in
- and
ou
tp
2005
- 20
09
I AS
>1
5 (s
) SD
Sa M
MSE
b -
- m
RSc
3/6
(i)
Rush
(2
010)
29
CC
- -
yes
- -
n.a.
re
plyi
ng
outp
20
05-
2007
I
NPI
>0
(i)
BDI-I
I >1
3 M
MSE
N
IHSS
3.
0/
42 (i
) BI
97
/ 10
0 (d
)
Sage
n (2
010)
42
PC
- -
yes
- ye
s 43
%
in- a
nd
outp
20
03-
2005
IH
AE
S
>33
(s)
HAD
S-D
M
MSE
(s
us)
- -
BI
87/
100
(d)
Caei
ro
(201
1) 34
PC
-
yes
yes
- ye
s 20
%
sub
ac
ute
2000
- 20
02
IH
AES-
10
(c)
MAD
RS
MM
SE
NIH
SS
- m
RSd
-
Cast
ella
nos
(201
1) 36
PC
-
- ye
s -
- n.
r. in
- and
ou
tp
2007
- 20
08
I N
PI
>0 (i
) H
AM-D
M
MSE
CN
S 7.
4/
11.5
(d)
mRS
c , BI
2.
0/6
(i),
79/1
00(d
)
Mar
asco
(2
011)
39
PC
- -
yes
hist
ye
s 22
%
sub
acut
e 20
09
1st I
PSDR
S >0
(c)
PSDR
S M
MSE
N
IHSS
2.
9/
42 (i
) m
RS
2.8/
6
(i)
With
all
(201
1) 3
1 PC
>8
5 -
yes
- ye
s 48
%
in- a
nd
outp
19
97-
2000
I
AESi
>3
7 (i)
SC
ID-1
M
MSE
b ES
S 88
.7/
100
(d)
IADL
c , AD
Lc 7/
8.
5/6
(d)
Plan
ton
(201
2) 41
PC
18
- 80
-
yes
hist
ye
s 80
%
outp
go
od
reco
very
2007
- 20
09
1st I
AS
>13
(s)
BDI-I
I >1
3 Br
oad
test
ing
NIH
SS
2.6/
42
(i)
mRS
0.
7/
6 (i)
~
Tabl
e 1.
Stu
dy c
hara
cter
istic
s con
tinue
d

53B_BW_Dalen_Stand.job
106
Table 1 Study characteristics legend: Coh: cohort type, PC: prospective cohort, RC: retrospective cohort, CC: case-control, CS: Cross Section, Type of stroke: 1st: no prior history of stroke, I: infarction, H: hemorrhage, Exclusion criteria: Dis: major disability and severe disease,, CI: cognitive impairment, MD: major depression, CD: communication disorder, hist: history, Ex %: excluded percentage, n.a.: not applicable, n.r.: not reported, Apathy measures: (s): self assessment, (c) clinician assessment, (i) informant assessment, AS: apathy scale, AES Apathy Evaluation Scale, NPI: Neuropsychiatric Inverntory, EBIF: Emotion Behavior Index Form, PSDRS: Post-Stroke Depression Rating Scale, WBIBS: modified apathy items from the Williams Brain Impairment Behavior Scale, AES-10: Apathy Evaluation Scale modified to 10 items, Depression measures: articles may have used multiple measures, the measure reported is the one used to assess the prevalence of depression used in this review, HDS, HRSD, HAM-D17, HAM-D: Hamilton Rating Scale for Depression, MADRS: Montgomery and Asberg Depression Rating Scale, SCID: Structural Clinical Interview for DSM-IV, SDS: Zung's Self Rating Scale for Depression, SF-36: short form health survey, BDI-II: Beck Depression Inventory II Cognition measures: MMSE: Mini Mental State Examination, SPSMQ: CAMCOG: cognitive section of the Cambrdige Examination for Mental Disorders of the Elderly-Revised, CCN: Coconuts neurological test, WCST: Wisconsin Card Scoring Test, MMSE (sus): MMSE taken only when patients were suspected to have cognitive impairment, stroke severity: NIHSS: national institute of health stroke scale, ESS: European stroke scale mean: mean/maximum score, (d): score decreases with increased disability, (i): score increases with increased disability,,disability, Disability measures: (d): score decreases with disability, (i): score increases with disability, JHFI: John Hopkins Functional Inventory, FIM: Functional Independence Measure, IADL: Lawton Instrumental Activities of Daily Living scale, ADL: Katz Activities of Daily Living scale, BI: Barthel Index, mRS: modified Rankin Scale, NIHSS: National Institute of Health Stroke Score, MFAQ-IADL: Instrumental Activities of Daily Living scale from the Multi Dimensional Functional Assessment Questionnaire, SIS-phys: physical component of the Stroke Impact Scale, Disability score: underlined: study provided enough information for separate meta-analysis on the association between apathy and disability, Superscript: a: significant association between apathy and depression, b: significant association between apathy and a decrease in performance on cognitive test, c: significant association between apathy and increased disability, d: significant association between apathy and worse functional recovery
Patient characteristics and reported apathy rates can be found in figure 2. The total number of patients
included was 2706 with a median number of 88 per study (range 30-408 patients). The median time since
stroke was 120 days (range 2-850). The median reported average age was 65.1 years (range 49.6-76.6). All
but four studies concerned prospectively collected cohorts of stroke patients. Nine studies assessed
patients in a sub acute setting within 30 days after stroke. Six studies were done in a mixed population of
in- and outpatients, four studies were done exclusively among rehabilitating inpatients and another four
exclusively among outpatients. Four articles provided longitudinal data with the length of follow-up
ranging from 6 to 16 months.6;316;21;31;36

54A_BW_Dalen_Stand.job
107
Figu
re 2
. For
est p
lot
and
clin
ical
cha
ract
eris
tics
TSS:
tim
e sin
ce s
trok
e in
day
s, D
ep: d
epre
ssio
n, F
em: f
emal
e ge
nder
, MM
SE: m
ini m
enta
l sta
te e
xam
inat
ion,
*: v
alue
s av
erag
ed
betw
een
asse
ssm
ents
with
in a
rtic
le, *
*: va
lues
ave
rage
d be
twee
n ar
ticle
on
base
line
and
artic
le o
n fo
llow
-up,
***
: ass
essm
ent w
ith th
e m
ost a
dditi
onal
info
rmat
ion
used
, und
erlin
ed:
stud
ies
prov
ided
info
rmat
ion
for s
epar
ate
met
a-an
alys
is on
the
clin
ical
fact
or, I
talic
: add
ition
al in
form
atio
n su
pplie
d by
aut
hor ~
: est
imat
ed v
alue
^: m
ultip
le a
path
y ra
tes
allo
wed
pe
r st
udy
whe
n m
easu
red
with
diff
eren
t m
easu
res,
^^:
mul
tiple
rat
es a
llow
ed p
er s
tudy
whe
n m
easu
red
with
diff
eren
t so
urce
s, ^
^^: m
ultip
le r
ates
allo
wed
whe
n m
easu
red
at
diffe
rent
tim
e sin
ce st
roke
Stu
dyN
% A
path
y95
% C
IW
eigh
tS
cale
Age
(SD
)TS
S (S
D)
Dep
%Fe
m %
MM
SE
Gre
enop
(200
9)51
11.8
%5.
4-23
.80.
08N
PI i
65.7
(11.
0)90
~45
.133
.326
.6 (3
.5)
Pia
mar
ta (2
004)
3315
.2%
6.5-
31.6
0.06
Apa
thy
Q s
76.6
(7.7
)13
.3 (6
.8)
57.6
39.4
- M
aras
co (2
011)
5418
.5%
10.3
-31.
10.
12P
SD
RS
c65
.3 (1
0.5)
7~41
.027
.822
.7 (6
.8)
Rus
h (2
010)
5320
.8%
11.9
-33.
70.
13N
PI i
70 (1
2.0)
854
(488
)13
.238
.027
.4 (2
.4)
San
ta (2
008)
6720
.9%
12.8
-32.
30.
16A
S s
65.4
(1.7
)49
.4 (3
.0)
37.3
43.3
21.9
(0.9
)H
ochs
tenb
ach
(200
5)*
157.
521
.9%
16.1
-29.
00.
39Q
i, Q
s55
.3 (1
0.9)
300
(60)
47.0
39.5
- S
tark
stei
n (1
993)
8022
.5%
14.7
-32.
90.
20A
S s
59.5
(13.
5)6.
2 (4
.0)
33.8
46.3
22.3
(6.3
)A
ngel
elli
(200
4)12
426
.6%
19.6
-35.
10.
35N
PI i
60.1
(12.
9)20
0~61
.340
.4 -
Mar
in (1
994)
4027
.5%
15.9
-43.
20.
12A
ES
c68
.360
8~32
.545
,026
(3.5
)B
roda
ty/W
ithal
l (20
05)*
*12
0.5
28.2
%20
.9-3
6.9
0.35
AE
S i
72.2
(8.8
)28
0.5~
13.7
39.3
27.3
(2.4
)C
aste
llano
s (2
011)
*75
.25
28.6
%19
.5-3
9.7
0.22
NP
I i70
.0 (1
1.9)
61.1
45.8
48.3
22.9
(8.8
)P
lant
on (
2012
)60
35,0
%24
.1-4
7.8
0.20
AS
s, N
PI i
59.7
(14)
109
(20)
3.3
35.0
- O
noda
(201
0)10
236
.3%
27.5
-46.
00.
34A
S s
73.0
(11.
6)11
.75
12.7
44,0
23.7
(4.4
)C
aeiro
(201
1)94
38.3
%29
.1-4
8.5
0.32
AE
S-1
0 c
55.7
(12.
9)2.
4 (1
.1)
19.1
35.1
25.3
(4.0
)K
aji (
2006
)92
40.2
%30
.7-5
0.5
0.32
AS
s64
.9 (1
1.9)
25~
25.0
39.0
- H
ama
(200
7)**
*24
340
.3%
34.3
-46.
60.
85A
S s
, NP
I i65
.2 (1
1.3)
40.7
(19.
6)32
.534
.224
.3 (5
.4)
May
o (2
009)
408
45.8
%41
.1-5
0.7
1,47
0W
BIB
S i
67.0
(14.
6)18
0~23
40.9
- C
arot
a (2
005)
273
47.6
%41
.8-5
3.5
0.99
EB
IF c
64.4
(15.
9)3.
5 (0
.7)
43.6
47.0
- H
offm
ann
(201
0)**
75.5
47.7
%36
.7-5
8.9
0.27
FRS
BE
s, i
49.9
(13.
7)30
excl
.42
.3 -
Sag
en (2
009)
8548
.2%
37.8
-58.
80.
31A
ES
s64
.5 (1
3.6)
134.
6 (1
8.4)
21.2
48.2
- C
aeiro
(200
6)17
851
.7%
44.4
-58.
90.
64P
SD
RS
c56
.8 (1
3)2.
4 (1
.1)
46.1
40.4
25 (4
.6)
And
erss
on (1
999)
3056
.7%
38.8
-72.
90.
11A
ES
c -
390~
- -
- Ja
rzeb
ka (2
007)
9071
.1%
60.9
-79.
50.
27A
S s
536~
43.3
46.7
-
NP
ropo
rtio
n95
% C
IN
stu
dies
I^2:
Age
TSS
Dep
%Fe
m %
Poo
led
2586
34.6
%29
.5-4
0.2
2346
.4%
63.5
120
31.9
40.4
010
2030
4050
6070
8090
100

54B_BW_Dalen_Stand.job
108
Figu
re 3
. Sub
gro
up a
naly
ses T
SS: t
ime
sinc
e st
roke
in d
ays,
Dep
: dep
ress
ion,
Fem
: fem
ale
gend
er, M
MSE
: min
i men
tal s
tate
exa
min
atio
n, *
: mul
tiple
apa
thy
rate
s allo
wed
per
stud
y w
hen
mea
sure
d w
ith d
iffer
ent m
easu
res,
**:
mul
tiple
rate
s allo
wed
per
stud
y w
hen
mea
sure
d w
ith d
iffer
ent s
ourc
es, *
**: m
ultip
le ra
tes a
llow
ed w
hen
mea
sure
d at
diff
eren
t tim
e sin
ce st
roke
Sub
grou
p: m
easu
re*
NP
ropo
rtio
n95
% C
IN
stu
dies
I^2
Age
TSS
Dep
%Fe
m %
MM
SE
NP
I57
723
,0%
18.4
-28.
26
30.0
%65
.223
7.9
46.3
40.7
25.3
Oth
er11
7836
.1%
27.3
-46.
07
47.2
%62
.410
6.2
34.8
341.
524
.5A
S73
437
.7%
27.3
-49.
37
46.9
%63
.733
.07
28.3
39.9
23.5
AE
S36
938
.8%
29.3
-49.
45
42.1
%65
.222
0.5
19.3
37.7
26.4
Sub
grou
p: s
ourc
e**
NP
ropo
rtio
n95
% C
IN
stu
dies
I^2
Age
TSS
Dep
%Fe
m %
MM
SE
Info
rman
t13
1428
.6%
21.5
-35.
810
46.9
%65
.918
0.5
33,0
40.6
26.1
Pat
ient
1103
34.8
%26
.2-4
4.6
1147
.2%
61.8
81.4
31.4
40.7
23.5
Clin
icia
n66
940
.3%
31.2
-50.
26
44.5
%61
.356
.839
.839
.824
.8S
ubgr
oup:
TS
S**
*N
Pro
port
ion
95%
CI
N s
tudi
esI^
2A
geTS
SD
ep %
Fem
%M
MS
ETS
S: <
10
858
39.7
%26
.7-5
4.3
648
.2%
60.9
3.7
39.8
43.2
23.8
TSS
: 10<
5069
635
.7%
29.6
-42.
35
40.3
%65
.831
.129
.440
23.4
TSS
: 50<
181
807
33.9
%24
.9-4
4.3
645
.9%
67.1
146.
122
.740
.427
TSS
: 181
=<
566
28.7
%21
.8-3
6.8
639
,0%
61.6
379.
840
40.2
26
NP
ropo
rtio
n95
% C
IN
stu
dies
I^2:
Age
TSS
Dep
%Fe
m %
Poo
led
2586
34.6
%29
.5-4
0.2
2346
.4%
63.5
120
31.9
40.4
010
2030
4050
6070
8090
100

55A_BW_Dalen_Stand.job
109
The estimate for the mean prevalence of apathy across studies was 34.6% (95%CI 29.5-40.2).
Heterogeneity was moderate (I2=46.4%). The funnel plot was roughly symmetrical (appendix S4).19 The
predefined sensitivity analysis of studies using recommended measurement instruments
(n=9),5;21;23;28;29;31;36;37;42 resulted in an estimated prevalence of 26.3% (95%CI 20.5-33.1, I2=42.8%).
Excluding the study identified by the funnel plot as a major source of heterogeneity,42 reduced
heterogeneity (24.2%, 95%CI 20.4-28.4%, I2=25.2%)(appendix S5). Jackknife sensitivity analysis resulted
in estimates ranging from 33.2% (95%CI 28.5-38.3) to 35.7% (95%CI 30.6-41.2). Sensitivity analysis
including studies with low risk of selection and confounding bias (n=10) resulted in a mean prevalence
of 41.4% (95%CI 33.3-50.0) but did not reduce heterogeneity (I2=47.0%). Excluding studies with an
average patient age under 60 years old from this analysis had no significant effect (38,0%, 95%CI 29.9-
47.9, I2=46.0% n=5).
The reported prevalence of apathy seemed to vary with different methods of assessment used. The
pooled prevalence based on studies using informant-based assessment instruments was lower than that
of studies using patient-based instruments, while that of the studies using clinician-based instruments
exceeded both (figure 3). In studies using the NeuroPsychiatric Inventory (NPI), a lower prevalence was
reported compared to studies using other informant based scales (23.0%; 95%CI: 18.4-28.2 I2: 30.0% vs.
39.4; 95%CI: 30.0-49.5%; I2: 45.5%). Additionally, the analysis stratified for most commonly used
assessment instruments showed significantly lower prevalence when apathy was assessed with the NPI
compared to apathy-specific assessment instruments (figure 3). Studies excluding patients with prior
history of stroke had a lower combined estimate compared to those including patients regardless of stroke
history (24.1%; 95%CI: 19.5-29.5 I2: 22.1% vs. 38.9; 95%CI: 38.9-44.9.%; I2: 46.2%) (appendix S6).
Stratification according to study setting revealed a relatively low prevalence and heterogeneity in the sub
group of studies which only included outpatients (25,6%, 95%CI: 19.6-32.6 I2: 26.9%)(Appendix S6).
Additional sub group analyses did not improve heterogeneity (appendix S6). Finally, meta-regression with
age, depression rates and MMSE-scores did not have significant impact on the overall apathy-rate
(P>0.1).
Associations between apathy and its clinical correlates are reported in table 2a-c. Apathetic patients were
on average 3.8 years older (95%CI 2.1-4.7; I2=0%). Women had a slightly higher chance of being
apathetic than men (RR 1.2; 95%CI >1.0-1.5; I2=6.6%). Other associations that are less commonly
reported are listed in table 2c.
The mean MMSE score of apathetic patients (n=10 studies) was 2.7 points lower (95%CI 1.6-3.8;
I2=60.2%) (table 3). Excluding two outliers identified in the funnel plot somewhat reduced these results
(2.1; 95%CI 1.3-2.9), but significantly reduced heterogeneity (I2=0%)(appendix S7).30;33 In seven studies,
a significant association between the presence of apathy and reduced performance on different tests of
cognitive function was found (figure 2).

55B_BW_Dalen_Stand.job
110
FFactor EEffect of apathy NN studies NN PPSA NNo PSA EEstimate 995% CCI II^2 MMSE Mean Difference 10 808 268 540 -2.7 points -3.8, -1.6 60.2% Age Mean Difference 13 1290 470 820 3.8 years 2.1, 4.7 0.0% Disability Hedges G (SMD) 9 627 194 433 -0.3 -0.7, 0.1 81.6% Female gender Relative Risk 8 681 96/203 180/478 1.2 1.0, 1.5 6.6%
22a. Meta-analysis post-stroke apathy versus no post-stroke apathy
Factor Effect of apathy N studies
N PSA No PSA Estimate 95% CI I^2
PSD Relative Risk 14 1240 179/442 185/798 1.8 1.4, 2.4 52.0%
PSD in PSA Proportion 14 442 179 - 40.1% 0.3, 0.5 42.7% PSD in pop Proportion 14 1240 179 185 28.1% 0.2, 0.4 46.1%
2b. Meta-analysis post-stroke apathy in post-stroke depression
Study Other associations with apathy: Association (95% CI) Test Angelelli (2004) TSS > 2 m p < 0.01 ANOVA Castellanos (2011) TSS > 4 weeks p < 0.05 tTest Caeiro (2011) education < 10 years OR 4.2 (1.3-13.6) Log. Reg. Hama (2007) CT-defined lesion volume p < 0.02 MW U Hochstenbach (2005) low agreement between patients and care givers k=0.5 Kappa Mayo (2009) high comorbidity on Charlson Index OR 2.1 (1.0-4.3) Ord. Reg. Sagen (2009) comorbidity OR: 3.0 ( 1.0-8.3) Log. Reg. Withall (2011) apathy at baseline with depression at follow-up OR: 7.2 (2.2-24.1) Log. Reg. 2c. Reported significant associations with apathy
Table 2. Clinical correlates of poststroke apathy MMSE: mini mental state examination, PSA: post-stroke apathy, PSD: post-stroke depression, pop.: population on which information on depression in apathetic patients was available, TSS: time since stroke, OR: odds ratio, k: kappa value, MW U: Mann-Whitney U-test, Log. Reg.: logistical regression, Ord. Reg.: ordinal regression
The estimated relative risk of depression among apathetic patients (n=11 studies) was 1.8 (95%CI 1.3-
2.4) (table 2b). Depression occurred in 40.1% of patients with apathy (95%CI 29.9-51.1%) and in 46.7%
vice versa (95%CI 36.4-56.3%). The prevalence of depression in the non-apathetic patients was estimated
at 23.6% (95%CI 17.1-31.6%). Six studies reported a significant association between the presence of
post-stroke apathy and post stroke depression (figure 2).
Assessment of the relationship between apathy and disability using Hedges’ g analysis was hampered by
high heterogeneity (I2=81.6%). Visual assessment of the funnel plot did not identify any single obvious
cause and dichotomous stratification based on time since stroke did not substantially improve
heterogeneity. In total, a significant association of apathy with increased disability was reported in nine
of eleven studies. In seven of these, apathy was associated with concurrent increased disability (figure 2).
In two, apathy at baseline was associated with decreased functional status at follow up, 6;33 and in another
two, with decreased functional recovery over time.5;32

56A_BW_Dalen_Stand.job
111
AAuthor TType of stroke pp--vvalue TTest Santa (2008) Non-hemorrhagic stroke < 0.05 X2 Caeiro (2011) Hemorrhagic stroke < 0.03 X2 33a. Association between apathy and type of stroke AAuthor LLaterality pp--vvalue TTest Right Brodaty (2005) Right Hemisphere < 0.02* tTest Right Frontal Subcortical Circuit < 0.02* tTest Left Santa (2008) Left Basal Ganglia < 0.05 X2 Onoda (2011) Left Basal Ganglia < 0.01 X2 Bilateral Hama (2007) Bilateral Basal Ganglia > Right Hemisphere > Left Hemisphere > none < 0.01 ANOVA Bilateral Basal Ganglia > Left Basal Ganglia < 0.001 Fisher Onoda (2011) Reduced regional cerebral blood flow in Basal Ganglia < 0.001** ANCOVA 33b. Association betweeen apathy and laterality of stroke lesion *: corrected for age, gender and time since stroke, ** corrected for age, no longer significant when Bonferroni correction was applied AAuthor RRegion pp--vvalue TTest Sub Cortical Starkstein (1993) Posterior Internal Capsule < 0.05 X2 Yates Brodaty (2005) Right Frontal Subcortical Circuit < 0.02** tTest Basal Ganglia Hama (2007) Bilateral Basal Ganglia > Right Hemisphere > Left Hemisphere > none < 0.01 ANOVA Bilateral Basal Ganlia > no Basal Ganglia damage < 0.01 Fisher Santa (2008) Left Basal Ganglia < 0.05 X2 Onoda (2011) Left Basal Ganglia < 0.01 X2 Reduced rCBF Basal Ganlia < 0.001*** ANCOVA 33c. Association between apathy and region of stroke lesion *: corrected for age, gender and time since stroke, ** corrected for age, no longer significant when Bonferroni correction was applied, *** corrected for age, gender, MMSE, HDS-R, FAB, SDS and false discovery ratio, AAuthor AAssessment pp--vvalue TTest Angelelli (2004) Laterality > 0.05 ANOVA Kaji (2006) Laterality 0.23 tTest 33d. Studies that did not identify any relation between apathy and the location of the stroke lesion
Table 3: associations between apathy and stroke characteristics, rCBF: regional cerebral blood flow, MMSE: mini mental state examination, HDS-R: Hamilton depression rating scale, FAB: frontal assessment battery, SDS: Zungs self-rating depression scale

56B_BW_Dalen_Stand.job
112
Information regarding lesion location and treatment was assessed qualitatively (table 3). Of the nine
studies that assessed the relationship between lesion location and presence of post-stroke apathy, six
reported on a significant association between specific lesion locations and an increased risk of apathy,
although in one study all significant associations disappeared after the appropriate Bonferroni correction
(table 3b).23 No significant difference was found between lacunar and cortical infarctions.
Results regarding apathy treatment are listed in table 4. Two clinical trials assessing the effect of
pharmacological treatment on post-stroke apathy were identified, both using apathy as secondary
outcome (table 4a). In one phase II trial, significantly reduced apathy scores were found in the group
treated with 900 mg of the nootropic agent nefiracetam (n=22) compared to groups receiving 600 mg
(n=26) or placebo (n=22).43 In another small (n=22) open study the acetylcholinesterase inhibitor
donepezil had a modest beneficial effect on functional status, which was also associated with a reduction
in apathy score.44 In five case-reports (table 4b), a favourable effect of treatment with bromocriptine was
reported,14;45-48 and in three with methylphenidate.14;49;50 Ropinirole, zolpidem and selegiline were
reportedly beneficial in one case each.14;51;52

57A_BW_Dalen_Stand.job
113
AAuth
or
YYear
DDe
sign
MMai
n oou
tcom
e SSe
ttin
g DDi
agno
sis
NNI
NND
IInte
rven
tion
DDose
FFo
llow
--uup
OOut
com
e Ro
bins
on 43
20
09
RCT
Depr
essio
n O
utpa
tient
PS
D M
odifi
ed A
S 26
69
N
efira
ceta
m
600
mg
12 w
eeks
IT
T AN
OVA
: 900
mg
vs p
lace
bo:
4 po
int d
ecre
ase
in A
S sc
ore
(p
=0·0
1), A
RR 0
·18
(95-
CI: 0
·02-
0·
34),
mor
e fr
eque
nt re
miss
ions
.
22
90
0 m
g
22
- Pl
aceb
o -
W
hyte
44
2008
OT
+ RC
CI
In
patie
nt
PSCI
AE
S 13
41
Do
nepe
zil
5-10
mg
12 w
eeks
PP
AN
OVA
: Don
epez
il an
d de
crea
se o
f apa
thy
both
in
depe
nden
tly a
ssoc
iate
d w
ith a
n in
crea
se in
FIM
-gai
n ov
er ti
me
13
G
alan
tam
ine
4-12
mg
PS
non
CI
-
98
-
Cont
rol:
none
-
20
wee
ks
44a. T
rials
rega
rdin
g tr
eatm
ent o
f pos
t--sst
roke
apa
thy
AAuth
or
YYear
DDe
sign
MMai
n ou
tcom
e SSe
ttin
g DDi
agno
sis
NN
IInte
rven
tion
DDose
FFo
llow
--uup
SSucc
essf
ully
treaa
ted
Kohn
o 51
20
09
CR
Apat
hy
Inpa
tient
Cl
inic
ian
1 Ro
pini
role
0.
75 m
g/d
-
1 M
arin
14
1995
CS
Ap
athy
O
utpa
tient
Cl
inic
ian
2 M
PH/B
RC, S
eleg
iline
50/
90 m
g/d,
5 m
g 1,
>2
year
s 2
Wat
anab
e 49
1995
CR
Ap
athy
In
patie
nt
Clin
icia
n 1
MPH
5
mg/
d 9
mon
ths
1 Sp
iege
l 50
2009
CS
Ap
athy
In
patie
nt
Clin
icia
n 3
MPH
2.
5 - 1
2,5
mg/
d 1
mon
th
3 Fo
ng 4
6 20
01
CR
Apat
hy
n.a.
n.
a.
1 BR
C 10
mg
n.a.
1
Cats
man
45
1988
CR
CI
, apa
thy
n.a.
n.
a.
1 BR
C n.
a.
n.a.
1
Park
s 47
1992
CR
FL
S In
patie
nt
Clin
icia
n 1
BRC
5 - 6
0 m
g/d
5 m
onth
s 1
Bare
tt 4
8 19
91
CR
Abul
ia
Inpa
tient
Cl
inic
ian
1 BR
C 5
- 55
mg/
d -
1
Mat
hieu
52
2011
CR
Ap
athy
O
utpa
tient
AI
1
Zolp
idem
-
-
1 44b
. Cas
e re
port
s and
serie
s reg
ardi
ng tr
eatm
ent o
f pos
t--sst
roke
apa
thy
Tabl
e 4:
trea
tmen
t of p
ost-
stro
ke a
path
y, R
CT: r
ando
mize
d co
ntro
lled
tria
l, O
T: o
pen
tria
l, RC
: ret
rosp
ectiv
e co
hort
, CS:
cas
e se
ries,
CR:
cas
e re
port
, CI:
cogn
itive
impa
irmen
t, FL
S:
fron
tal l
obe
synd
rom
e, P
SD: p
atie
nts
with
pos
t st
roke
dep
ress
ion,
PSC
I: pa
tient
s w
ith p
ost
stro
ke c
ogni
tive
impa
irmen
t, PS
non
CI:
mat
ched
str
oke
patie
nts
with
out
cogn
itive
im
pairm
ent,
n.a.
: ful
l art
icle
not
ava
ilabl
e, A
S: a
path
y sc
ale,
AES
: apa
thy
eval
uatio
n sc
ale,
AI:
apat
hy in
vent
ory,
NI:
num
ber
for
inte
rven
tion,
ND:
num
ber
of d
rop-
outs
, MPH
: m
ethy
lphe
nida
te, B
RC: b
rom
ocrip
tine,
ITT:
inte
ntio
n to
trea
t, AR
R: a
bsol
ute
risk
redu
ctio
n, P
P: p
er p
roto
col

57B_BW_Dalen_Stand.job
114
Discussion
We found that apathy occurs in every third patient after stroke. This estimate was not importantly affected
by selection and confounding bias, time since stroke or inclusion criteria apart from prior history of
stroke. Concomitant depression was present in only 40% of apathetic patients, confirming the occurrence
of apathy as a distinct entity. Post-stroke apathy is associated with worse cognitive function. There is
considerable evidence for an association of post-stroke apathy with disability and worse outcome of
rehabilitation. No clear association between post-stroke apathy and specific stroke lesion locations could
be established. Systematic trials on treatment of post-stroke apathy have not been conducted and there
is currently insufficient evidence to start any medical treatment of apathy after stroke.
Strengths and limitations
To our knowledge, this is the first systematic review and quantitative analysis covering several aspects of
post-stroke apathy including prevalence, associated symptoms, lesion localisation and treatment. Several
of the included studies had a high risk of selection bias and information bias. Confounding bias was
generally low. The three factors that we hypothesized to be the most influential (depression, age, and
cognitive function) were reported in all but one study.
Since apathy is mostly assessed as a secondary outcome, there might be over-reporting of higher
prevalence rates. In addition, significantly associated factors are more likely to be reported, also increasing
the risk of publication bias. To minimize these shortcomings, we included all studies including a formal
instrument to assess apathy, and tried to acquire unpublished data by contacting the authors.
Studies differed widely in design and patient characteristics. Heterogeneity was moderately high.
Subgroup analyses on type of stroke, method of assessment used, source of information and time since
stroke did not substantially consistently reduce heterogeneity. In the sensitivity analysis regarding
recommended measurement instruments, heterogeneity improved after exclusion of the main outlier.
However, of the six remaining studies, four employed the NPI as measurement instrument, making this
result difficult to interpret. Other sensitivity analyses, using stricter criteria, hardly affected our results.
The persistence of heterogeneity implies that several other factors are involved that have not been taken
into consideration.
Therefore, it appears that many aspects of post-stroke apathy remain to be elucidated. Different methods
of assessment may lack convergent validity, measuring slightly different conditions.15 Also, the specific
range of symptoms of post-stroke apathy may differ from what is regarded apathetic behaviour in other
conditions e.g. Parkinson’s or Alzheimer’s disease. In addition, high scores on apathy scales may be
caused by several other factors and conditions that were not measured in the studies included in our
review, such as post-stroke fatigue, pre-stroke personality traits and cultural factors. These aspects of

58A_BW_Dalen_Stand.job
115
post-stroke apathy may all be important sources of the substantial heterogeneity that was found in this
review.
Studies have tried to correct for these factors by asking patients and caregivers to score their behaviour
relative to their behaviour before the stroke occurred. In three studies the association between apathy
and other concurrent neuropsychiatric symptoms was assessed, but none were found.27,36,42 In one study
personality prior to stroke was assessed and no association with apathy was found.37 More research on
the interplay between other factors such as fatigue, and apathy is needed to further elucidate the
nosological position of post-stroke apathy.
The heterogeneity of the results has some implications for the generalisability of our findings. Although
the weighted average age and depression rates (fig. 2) seem representative of the general stroke
population, this is only an indication. Apathy rates in our subgroup analyses may only differ slightly from
each other but the real difference between these subgroups may be confounded by other factors that are
still unknown. Our study provides a clear example of this ecological fallacy. Although analyses of the
difference between apathetic and non apathetic patient groups within studies show clear relations with
age, MMSE scores and depression rates, these results could not be significantly confirmed by meta-
regression or sub group analyses. Therefore results gained at a group level need to be interpreted with
caution.
Prevalence
With a prevalence of 34.6%, post stroke apathy occurs as frequently as post stroke depression (33%)2
and post-stroke dementia (21.0-41.3%)3. Whereas these neuropsychiatric syndromes are frequently
studied and treatments often initiated, post-stroke apathy has so far been largely ignored. Since the
prevalence of apathy in the general population is largely unknown, it is difficult to establish to which
degree post-stroke apathy should be attributed to the stroke. In healthy volunteers of comparable age,
apathy was found in 6.0% and in 15.8% five years later.53 In another study, a community based sample
of elderly, a prevalence of 19.9% was found.54 This suggests that not all cases of post-stroke apathy are
directly attributable to the stroke although its prevalence is higher in patients with a history of multiple
strokes.
The average estimate of studies using informant-based assessment instruments appears to be lower and
that of studies using clinician-based instruments higher than the average estimate of studies using patient-
based assessment instruments. Use of the NPI leads to a lower estimated apathy prevalence compared
to other scales. Results of a study that estimated the prevalence of apathy at 19.2% using the NPI and at
41.4% using the AS in the same cohort confirm this finding.5 The relatively low apathy-rate found in
studies using informant-based instruments may be explained by the NPI being the most used informant-
based instrument. Studies using a different informant-based instrument found a relatively high apathy-
rate (39.4% vs. 23.0%) (figure 2).6;23;24;31 The NPI uses one to three dichotomous (yes/no) screening

58B_BW_Dalen_Stand.job
116
questions to establish the presence of apathy, which may increase the threshold of its diagnosis, i.e.
through reluctance to describe oneself or someone else as being apathetic. Apathy rates are reported to
be rather stable over time in longitudinal studies,6;31 sometimes after a significantly lower prevalence in
the first months after stroke.21;36 There was insufficient data for pooling the results of longitudinal studies
separately. Stratification of studies according to the average time since stroke shows that reported apathy
rates were generally lower in studies with assessment later after stroke. This is probably due to differences
in study design. In studies with assessment early after stroke, clinician-based instruments, which estimate
higher apathy-rates, were used relatively often. In contrast, studies in which patients were assessed longer
after stroke predominantly used informant-based instruments, which estimate relatively low apathy-rates.
This difference may importantly contribute to the decrease in reported apathy prevalence over time.
Associated symptoms
The association between apathy and age has also been reported in the general population.53;55 Possibly,
post-stroke apathy occurs more frequently in patients with reduced cognitive function, which is more
common in older individuals in both the general and the post-stroke population.55;56 The difference we
observed in MMSE scores between apathetic and non-apathetic patients after stroke supports this
hypothesis.
The association between apathy and reduced cognitive function was also reported in studies that used
more extensive neuropsychological examination.6;37 This association could in turn be confounded by
age,3;55 for which the analysis was corrected in only one study.6 The relationship between post-stroke
apathy and cognitive impairment may be explained by several factors. Incapability of goal oriented
thinking and behaviour may lead to loss of interest en lack of effort in cognitive testing.57;58 Also, both
apathy and cognitive impairment could be a consequence of the same underlying brain damage. Lesions
in distant areas related to memory and learning and their projections may influence anterior cingulate
circuit function, which is associated with motivation.59;60
Apathetic patients have an almost twofold risk of concurrent post-stroke depression. Apathy can occur
as a symptom of depression,10;11 and many instruments to assess depression also contain items that assess
apathy. Therefore, when in studies depression is defined by a cut-off score on a depression scale, high
scores on the apathy items could contribute to misclassification of apathy as depression. Misclassification
of apathetic patients as being depressed could contribute to the reported lack of treatment effect in post-
stroke depression,61 since symptoms of apathy do not to respond well to SSRIs.14;62;63 Distinction between
isolated post-stroke apathy and apathy in the context of post-stroke depression can therefore have
important consequences from a clinical point of view.
Quantitative assessment of the relationship between apathy and disability is difficult due to very high
heterogeneity between studies. Nevertheless, an association between apathy and increased disability was
reported in the majority of studies. In two studies, an association between apathy and increased disability

59A_BW_Dalen_Stand.job
117
remained significant after correction for the effect of functional status at baseline.5;6 Another study
reported significantly worse functional outcome in apathetic patients compared to non-apathetic patients
with comparable functional status at baseline.32 These findings suggest a detrimental effect of post-stroke
apathy on functional recovery.
Lesion location
We found no clear association between apathy and a specific lesion location nor hemisphere. We also did
not find an association with stroke severity or lesion volume on MRI. An association with sub cortical
lesions, mainly the basal ganglia, is reported most consistently. Two studies with high prevalence of post-
stroke apathy (50-55%) described patients with subcortical infarctions, often affecting the basal
ganglia.64;65 Apathy also occurs more frequently in other neurological conditions involving the basal
ganglia e.g. progressive supranuclear palsy, Parkinson’s and Huntington’s disease.66, 67 These findings are
in line with the hypothesis that apathy arises from defects in the frontal subcortical circuit, of which the
anterior cingulate circuit is associated with motivation.12;59
Treatment
There is currently insufficient evidence to support a pharmacological approach to treat post stroke
apathy. High doses of the nootropic agent nefiracetam showed a positive effect on apathy as a secondary
outcome in a group of post-stroke depression patients in a small controlled trial with small treatment
groups,43 but results are difficult to translate to other post-stroke populations. Evidence for an
advantageous effect of the acetylcholinesterase inhibitor donepezil in patients with acute post stroke
cognitive impairment compared to a retrospective control group is circumstantial.44 A number of case
reports describing a beneficial effect of dopamine agonists and methylphenidate may warrant further
study.14;45-51
Implications for clinical practice and future research
Our findings on the prevalence and clinical characteristics of post stroke apathy in a post-stroke
population are clinically relevant for adequately informing patients, caregivers, and clinicians. Post-stroke
apathy is a pervasive but insufficiently recognised neuropsychiatric symptom. The wide array of
definitions and instruments to assess apathy may provide an important barrier for its recognition after
stroke.15 Consensus on its construct and development of a gold standard of assessment is of major
importance.3,11,15 Post-stroke apathy is consistently associated with higher rates of cognitive impairment,
depression and disability, regardless of method of assessment. This renders it an important symptom to
be studied. Although no effective pharmacological therapy is currently available, rehabilitation programs
could be adapted to patients’ needs. Inadequate treatment with antidepressant drugs might be prevented
through improved discrimination between depression and apathy. Research into successful treatment and

59B_BW_Dalen_Stand.job
118
coping strategies for post-stroke apathy could increase rehabilitation success-rates. Given its potential
impact, apathy should be included as an outcome measure in future studies on depression, cognitive
impairment and other neuropsychiatric sequelae of stroke. Apathy may also be an important contributor
to post stroke disability and should be taken into account in studies with a long-term follow up of
functional recovery.
Conclusions
Apathy occurs in every third patient after stroke, often without concomitant depression. Post-stroke
apathy is associated with reduced cognitive function, increased disability and may have a negative effect
on rehabilitation outcome. No specific lesion location associated with apathy could be identified. There
is currently insufficient evidence to support any specific pharmacological treatment of post-stroke apathy.
Better recognition could potentially benefit rehabilitation programs and prevent inadequate treatment of
depression. Some promising treatment strategies warrant further research in randomised controlled trials.
Acknowledgements
We thank R.Spijker and J.G. Daams from the AMC medical library for their help with conducting our
search. We also thank all investigators who helped supply original data, in particular the following:
K. Onoda, (Dept. Of Neurology, Shimane University, Japan), L. Caeiro, (Dept of Neurosciences, Servico
de Neurologia Hospital de Santa Maria, Portugal), F. Castellanos-Pinedo, (Dept. Of Neurology, Hospital
Virgen del Puerto, Spain), S. Hama, (Division of Rehabilitation, Hibino Hospital/Dept. Of
Neurosurgery, Hiroshima University, Japan), M. Planton, (CHU Toulouse Purpan, France), A. Iavarone,
(Neurological and Stroke Unit, CTO Hospital, AORN “ Ospedali dei Colli”, Italy), M. Hoffmann, (James
A. Haley Veterans’ Hospital, Tampa, United States of America), K. Greenop, (Division of population
science, TICHR, University of Western Australia, Australia), U. Sagen (Dept. Psychiatry, Telemark
Hospital, Norway), A. Carota (Hildebrand Clinic, Switzerland)

60A_BW_Dalen_Stand.job
119
References: 1. Robinson RG. Neuropsychiatric consequences of stroke. Annual Review of Medicine 1997 48:217-
229 2. Hackett ML, Yapa C, Parag V, Anderson CS. Frequency of depression after stroke - A systematic
review of observational studies. Stroke 2005;36:1330-1340 3. Pendlebury ST, Rothwell PM. Prevalence, incidence, and factors associated with pre-stroke and
post-stroke dementia:a systematic review and meta-analysis. Lancet Neurology 2009;8:1006-1018 4. Robert P, Onyike CU, Leentjens AFG et al. Proposed diagnostic criteria for apathy in Alzheimer's
disease and other neuropsychiatric disorders. European Psychiatry 2009;24:98-1044. 5. Hama S, Yamashita H, Shigenobu M et al. Depression or apathy and functional recovery after
stroke. International Journal of Geriatric Psychiatry 2007;22:1046-1051 6. Mayo NE, Fellows LK, Scott SC, Cameron J, Wood-Dauphinee S. A longitudinal view of apathy
and its impact after stroke. Stroke 2009;40:3299-3307 7. Samus QM, Rosenblatt A, Steele C et al. The association of neuropsychiatric symptoms and
environment with quality of life in assisted living residents with dementia. Gerontologist 2005;45:19–26
8. Aarsland D, Bronnick K, Ehrt U et al. Neuropsychiatric symptoms in patients with Parkinson's disease and dementia:Frequency, profile and associated care giver stress. Journal of Neurology, Neurosurgery and Psychiatry 2007;78:36-42
9. de Vugt ME, Riedijk SR, Aalten P, Tibben A, van Swieten JC, Verhey FRJ. Impact of Behavioural Problems on Spousal Caregivers:A Comparison between Alzheimer's Disease and Frontotemporal Dementia. Dementia and Geriatric Cognitive Disorders 2006 22:35-41
10. Marin RS. Apathy:A neuropsychiatric syndrome. Journal of Neuropsychiatry and Clinical Neurosciences 1991;3:243-254
11. Starkstein SE, Leentjens AFG. The nosological position of apathy in clinical practice. Journal of Neurology, Neurosurgery & Psychiatry 2008;79:1088-1092
12. Levy R, Dubois B. Apathy and the functional anatomy of the prefrontal cortex-basal ganglia circuits. Cerebral Cortex 2006;16:916-928
13. Marin RS, Wilkosz PA. Disorders of diminished motivation. Journal of Head Trauma Rehabilitation 2005;20:377-388
14. Marin RS, Fogel BS, Hawkins J, Duffy J, Krupp B. Apathy:A treatable syndrome. Journal of Neuropsychiatry and Clinical Neurosciences 1995;7:23-30
15. Clarke DE, Ko JY, Kuhl EA, Van RR, Salvador R, Marin RS. Are the available apathy measures reliable and valid? A review of the psychometric evidence. Journal of Psychosomatic Research 2011;70:73-97
16. Jorge RE, Starkstein SE, Robinson RG. Apathy following stroke. Canadian Journal of Psychiatry 2010;55:350-354
17. Centre for reviews and dissemination, university of York. CRD’s guidance for undertaking reviews in health care [online]. Available at: www.york.ac.uk/inst/crd Accessed July 11, 2011.
18. Wells G, Shae B, O’Connel D. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analysis.
19. Higgins JPT, Green S. Cochrane handbook for systematic reviews of interventions Version 5.1.0 [updated March 2011] The Cochrane Collaboration 2011.
20. Wallace BC, Schmid CH, Lau J, Trikalinos TA. Meta-analyst:software for meta-analysis of binary, continuous and diagnositic data. BMC Medical Research Methodology 2009;9
21. Angelelli P, Paolucci S, Bivona U; et al. Development of neuropsychiatric symptoms in poststroke patients: a cross-sectional study. Acta psychiatrica scandinavica 2004;110:55-63
22. Andersson S, Krogstad JM, Finset A. Apathy and depressed mood in acquired brain damage: Relationship to lesion localization and psychophysiological reactivity. Psychological Medicine 1999;29:447-456
23. Brodaty H, Withall A, Altendorf A, Sachdev PS. Rates of depression at 3 and 15 months poststroke and their relationship with cognitive decline: The Sydney Stroke Study. The American Journal of Geriatric Psychiatry 2007;15:477-486

60B_BW_Dalen_Stand.job
120
24. Hochstenbach J, Prigatano G, Mulder T. Patients' and relatives' reports of disturbances 9 months after stroke: Subjective changes in physical functioning, cognition, emotion, and behavior. Archives of Physical Medicine and Rehabilitation 2005;86:1587-1593
25. Kaji Y, Hirata K, Ebata A. Characteristics of post-stroke depression in Japanese patients. Neuropsychobiology 2006;53:148-152
26. Jarzebska E. Stroke patients' apathy. [Polish]. Polski Merkuriusz Lekarski 2007;22:280-282 27. Piamarta F, Iurlaro S, Isella V et al. Unconventional affective symptoms and executive functions
after stroke in the elderly. Archives of gerontology and geriatrics Supplement 2004;9:315-323 28. Marin RS, Firinciogullari S, Biedrzycki RC. Group differences in the relationship between apathy
and depression. Journal of Nervous and Mental Disease 1994;182:235-239 29. Rush BK, McNeil RB, Gamble DM et al. Behavioral Symptoms in Long-Term Survivors of
Ischemic Stroke. Journal of Stroke and Cerebrovascular Diseases 2010;19:326-332 30. Starkstein SE, Fedoroff JP, Price TR, Leiguarda R, Robinson RG. Apathy following
cerebrovascular lesions. Stroke 1993;24:1625-1630 31. Withall A, Brodaty H, Altendorf A, Sachdev PS. A longitudinal study examining the
independence of apathy and depression after stroke:the Sydney Stroke Study. International Psychogeriatrics 2011;23:264-273
32. Santa N, Sugimori H, Kusuda K, Yamashita Y, Lbayashi S, Lida M. Apathy and functional recovery following first-ever stroke. International Journal of Rehabilitation Research 2008;31:321-326
33. Caeiro L, Ferro JM, Santos CO, Figueira ML. Depression in acute stroke. Journal of Psychiatry and Neuroscience 2006:31:377-383
34. Caeiro L, Ferro JM, Figueira ML. Apathy in acute stroke patients. European Journal of Neurology 2012;19:291-297
35. Carota A, Berney A, Aybek S et al. A prospective study of predictors of poststroke depression. Neurology 2012;64:428-433
36. Castellanos-Pinedo F, Hernandez-Perez JM, Zurdo M et al. Influence of premorbid psychopathology and lesion location on affective and behavioral disorders after ischemic stroke. J Neuropsychiatry Clin Neurosci 2011;23:340-347
37. Greenop KR, Almeida OP, Hankey GJ, Van BF, Lautenschlager NT. Premorbid personality traits are associated with post-stroke behavioral and psychological symptoms: A three-month follow-up study in Perth, Western Australia. International Psychogeriatrics 2009;21:1063-1071
38. Hoffmann M, Cases LB, Hoffmann B, Chen R. The impact of stroke on emotional intelligence. BMC Neurology 2010;10:103 Available at: DOI:10.1186/1471-2377-10-103
39. Marasco G, Iavarone A, Ronga B, Martini V, Crispino M, Postiglione A. Depressive symptoms in patients admitted to a semi-intensive Stroke Unit. Acta Neurologica Belgica 2011;111:276-281
40. Onoda K, Kuroda Y, Yamamoto Y et al. Post-stroke apathy and hypoperfusion in Basal ganglia:SPECT study. Cerebrovascular Diseases 2011;31:6-11
41. Planton M, Peiffer S, Albucher JF et al. Neuropsychological outcome after a first symptomatic ischaemic stroke with 'good recovery'. European Journal of Neurology 2012;19:212-219
42. Sagen U, Finset A, Moum T et al. Early detection of patients at risk for anxiety, depression and apathy after stroke. General Hospital Psychiatry 2010;32:80-85
43. Robinson RG, Jorge RE, Clarence-Smith K, Starkstein S. Double-blind treatment of apathy in patients with poststroke depression using nefiracetam. Journal of Neuropsychiatry and Clinical Neurosciences 2009;21:144-151
44. Whyte EM, Lenze EJ, Butters M et al. An open-label pilot study of acetylcholinesterase inhibitors to promote functional recovery in elderly cognitively impaired stroke patients. Cerebrovascular Diseases 2008;26:317-321
45. Catsman-Berrevoets CE, Harskamp F. Compulsive pre-sleep behavior and apathy due to bilateral thalamic stroke: Response to bromocriptine. Neurology 1988;38:647-649
46. Fong SYY, Ungvari GS, Chow L-Y. The differential diagnosis of depression:Case of basul ganglia infarction. Revista de Psiquiatria Clinica 2001;28:211-214
47. Parks RW, Crockett DJ, Manji HK, Ammann W. Assessment of bromocriptine intervention for the treatment of frontal lobe syndrome:A case study. Journal of Neuropsychiatry and Clinical

61A_BW_Dalen_Stand.job
121
Neurosciences 1992;4:109-111 48. Barett K. Treating organic abulia with bromocriptine and lisuride:four case studies. Journal of
Neurology, Neurosurgery, and Psychiatry 1991;54:718-721 49. Watanabe MD, Martin EM, DeLeon OA, Gaviria M, Pavel DG, Trepashko DW. Successful
methylphenidate treatment of apathy after subcortical infarcts. Journal of Neuropsychiatry and Clinical Neurosciences 1995;7:502-504
50. Spiegel DR, Kim J, Greene K, Conner C, Zamfir D. Apathy due to cerebrovascular accidents successfully treated with methylphenidate:A case series. Journal of Neuropsychiatry and Clinical Neurosciences 2009;21:216-219
51. Kohno N, Abe S, Toyoda G, Oguro H, Bokura H, Yamaguchi S. Successful treatment of post-stroke apathy by the dopamine receptor agonist ropinirole. Journal of Clinical Neuroscience 2010;17:804-806
52. Mathieu S, Autret K, Arnould A et al. Treatment of apathy with Zolpidem (Stilnox): Two double-blind, placebo-controlled single case studies. Annals of Physical and Rehabilitation Medicine 2011;54:e214 Available at: Doi :10.1016/j.rehab.2011.07.389
53. Brodaty H, Altendorf A, Withall A, Sachdev P. Do people become more apathetic as they grow older? A longitudinal study in healthy individuals. International Psychogeriatrics 2010;22:426-436
54. Ligthart SA, Richard E, Fransen NL, et al. Apathy without depression is associated with cardiovascular risk factors and history of stroke. Archives of General Psychiatry 2012;69:1-7
55. Clarke DE, Ko JY, Lyketsos C, Rebok GW, Eaton WW. Apathy and cognitive and functional decline in community-dwelling older adults: Results from the Baltimore ECA longitudinal study. International Psychogeriatrics 2010;22:819-829
56. Pendleburry ST, Rothwell PM. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia:a systematic review and medta-analysis. Lancet Neurology 2009;8:1006-1018
57. Dean AC, Victor TL, Boone KB, Philpott LM, Hess RA. Dementia and effort test performance. Clin Neuropsychol 2009;23:133-152
58. Whitney KA, Maoz O, Hook JN, Steiner AR, Bieliauskas LA. IQ and scores on the Mini-Mental State Examination (MMSE):controlling for effort and education among geriatric inpatients. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn 2007;14:545-552
59. Tekin S, Cummings JL. Frontal-subcortical neuronal circuits and clinical neuropsychiatry:An update. Journal of Psychosomatic Research 2002;53:647-654
60. Bonelli RM, Cummings JL. Frontal-subcortical circuitry and behavior. Dialogues in clinical neuroscience 2007;9:141-151
61. Hackett ML, Anderson CS, House A, Xia J. Interventions for treating depression after stroke. Cochrane Database of Systematic Reviews 2008 CD003437 Available at: DOI:10.1002/14651858.CD003437.pub
62. Barnhart WJ, Makela EH, Latocha MJ. SSRI-induced apathy syndrome:A clinical review. Journal of Psychiatric Practice 2004;10:196-199
63. Sansone RA, Sansone LA. SSRI-induced indifference. Psychiatry (Edgemont) 2010 7:14-18 64. Yamagata S, Yamaguchi S, Kobayashi S. Impaired novelty processing in apathy after subcortical
stroke. Stroke 2004;35:1935-1940 65. Okada K, Kobayashi S, Yamagata S, Takahashi K, Yamaguchi S. Poststroke apathy and regional
cerebral blood flow. Stroke 1997;28:2437-2441 66. Bogart KR, Is apathy a valid and meaningful syptom or syndrome in Parkinson’s disease? A
critical review. Health Psychology 2011;30:386-400 67. Chase TN, Apathy in neuropsychiatric disease: diagnosis, pathophysiology, and treatment.
Neurotoxicity Research 2011;19:266

61B_BW_Dalen_Stand.job
122
Supplementary material Appendix S1: full search report and excluded studies 1. Clinical Question: Prevalence of apathy among stroke patients 2. PICO
P Patients after stroke I C O Prevalence of apathy
3. Search results: Combined total after duplicate removal: 4328
DDatabase ddate ## Records MEDLINE(R) In-Process & Other Non-Indexed Citations (OvidSP)
21-07-2011 1842
Embase 1980—current (OvidSP) 21-07-2011 1816 PsychINFO 17-08-2011 1426 Total after duplicate removal 4060
DDatabase ddate ## Records MEDLINE(R) In-Process & Other Non-Indexed Citations (OvidSP)
06-2011 – 21-02-2012 100
Embase 1980—current (OvidSP) 30-05 – 21-02-2012 195 PsychINFO 06-2011 – 21-02-2012 84 Total after duplicate removal 329
4. Search Strategy Medline: Platform: OvidSP, Database: MEDLINE® In-Process & Other Non-Indexed Citations, No limits were used, no methodological filters were used
## SSearch Term 1. cerebrovascular disorders/ 2. exp basal ganglia cerebrovascular disease/ 3. exp brain ischemia/ 4. stroke/ 5. exp brain infarction/ 6. hypoxia-ischemia, brain/ 7. exp intracranial arterial diseases/ 8. exp "Intracranial Embolism and Thrombosis"/ 9. exp intracranial hemorrhages/ 10. (stroke or poststroke or post-stroke or cerebrovasc$ or brain vasc$ or cerebral vasc$ or cva$ or
apoplex$ or isch?emi$ attack$ or tia$1 or neurologic$ deficit$).tw. 11. ((brain$ or cerebr$ or cerebell$ or cortical or vertebrobasilar or hemispher$ or intracran$ or
intracerebral or infratentorial or supratentorial or MCA or anterior circulation or posterior circulation or basal ganglia) adj5 (isch?emi$ or infarct$ or emboli$ or occlus$ or hypox$ or obstruction or vasculopathy)).tw.
12. ((lacunar or cortical) adj5 infarct$).tw. 13. ((brain$ or cerebr$ or cerebell$ or intracerebral or intracran$ or parenchymal or
intraventricular or infratentorial or supratentorial or basal gangli$ or subarachnoid or putaminal or putamen or posterior fossa) adj5 (haemorrhage$ or hemorrhage$ or haematoma$ or hematoma$ or bleed$)).tw.

62A_BW_Dalen_Stand.job
123
14. ((brain or intracranial or basal ganglia or lenticulostriate) adj5 (vascular adj5 (disease$ or disorder or event))).tw.
15. ((isch?emic or apoplectic) adj5 (event or events or insult or attack$)).tw. 16. ((intracranial or cerebral art$ or basilar art$ or vertebral art$ or vertebrobasilar or vertebral
basilar) adj5 (stenosis or isch?emia or insufficiency or arteriosclero$ or atherosclero$ or occlus$)).tw.
17. exp aphasia/ or anomia/ or hemiplegia/ or hemianopsia/ or exp paresis/ or deglutition disorders/ or dysarthria/ or pseudobulbar palsy/ or muscle spasticity/
18. (aphasi$ or apraxi$ or dysphasi$ or dysphagi$ or deglutition disorder$ or swallow$ disorder$ or dysarthri$ or hemipleg$ or hemipar$ or paresis or paretic or hemianop$ or hemineglect or spasticity or anomi$ or dysnomi$ or acquired brain injur$ or hemiball$).tw.
19. ((unilateral or visual or hemispatial or attentional or spatial) adj5 neglect).tw. 20. or/1-19 21. Apathy/ 22. exp Motivation/ 23. apathy.ti,ab. 24. abulia.mp. 25. amotivation.mp. 26. avolition.mp. 27. (neuropsychiatric adj inventory).ti,ab. 28. "frontal lobe personality scale".ti,ab. 29. NPI.ti,ab. 30. FLOPS.ti,ab. 31. lars.ti,ab. 32. DAIR.ti,ab. 33. "frontal system behaviour scale".ti,ab. 34. FrSBe.ti,ab. 35. "frontal system behavior scale".ti,ab. 36. KBCI.ti,ab. 37. "Key Behaviors Change Inventory".ti,ab. 38. (flat adj2 affect).ti,ab. 39. bluntness.mp. 40. (emotional adj2 indifferen*).ti,ab. 41. (reduced adj2 volition).ti,ab. 42. ((reduced or loss) adj3 (concern or effort or emotional or "action initiation" or interest or
motivation or behavior or behaviour or cognition or drive)).ti,ab. 43. alexithymia.mp. or exp Affective Symptoms/ 44. emotions/ 45. or/21-44 46. animals/ not humans/ 47. 45 and 20 48. 47 not 46
Embase: Platform: OvidSP, Database: Embase 1980-present, No limits were used, No methodological filters were used
## SSearch Term 1. (exp cerebrovascular disease/ or (stroke or poststroke or post-stroke or cerebrovasc$ or brain
vasc$ or cerebral vasc$ or cva$ or apoplex$ or isch?emi$ attack$ or tia$1 or neurologic$ deficit$).tw. or ((brain$ or cerebr$ or cerebell$ or cortical or vertebrobasilar or hemispher$ or intracran$ or intracerebral or infratentorial or supratentorial or MCA or anterior circulation or posterior circulation or basal ganglia) adj5 (isch?emi$ or infarct$ or emboli$ or occlus$ or hypox$ or obstruction or vasculopathy)).tw. or ((lacunar or cortical) adj5 infarct$).tw. or

62B_BW_Dalen_Stand.job
124
((brain$ or cerebr$ or cerebell$ or intracerebral or intracran$ or parenchymal or intraventricular or infratentorial or supratentorial or basal gangli$ or subarachnoid or putaminal or putamen or posterior fossa) adj5 (haemorrhage$ or hemorrhage$ or haematoma$ or hematoma$ or bleed$)).tw. or ((brain or intracranial or basal ganglia or lenticulostriate) adj5 (vascular adj5 (disease$ or disorder or event))).tw. or ((isch?emic or apoplectic) adj5 (event or events or insult or attack$)).tw. or ((intracranial or cerebral art$ or basilar art$ or vertebral art$ or vertebrobasilar or vertebral basilar) adj5 (stenosis or isch?emia or insufficiency or arteriosclero$ or atherosclero$ or occlus$)).tw. or ((unilateral or visual or hemispatial or attentional or spatial) adj5 neglect).tw.) not (stroke adj volume).tw.
2. exp apathy/ 3. exp motivation/ 4. apathy.ti,ab. 5. abulia.mp. 6. amotivation.mp. 7. avolition.mp. 8. exp alexithymia/ 9. alexithymia.ti,ab. 10. emotion/ 11. (neuropsychiatric adj inventory).ti,ab. 12. "frontal lobe personality scale".ti,ab. 13. NPI.ti,ab. 14. FLOPS.ti,ab. 15. LARS.ti,ab. 16. DAIR.ti,ab. 17. ("frontal system behavior scale" or "frontal system behaviour scale").ti,ab. 18. FrSBe.ti,ab. 19. KBCI.ti,ab. 20. ("key behavior change inventory" or "key behaviour change inventory").ti,ab. 21. (flat adj2 affect).ti,ab. 22. bluntness.ti,ab. 23. (emotional adj2 indifferen*).ti,ab. 24. (reduced adj2 volition).ti,ab. 25. ((reduced or loss) adj3 (concern or effort or emotional or "action initiation" or interest or
behavior or behaviour or cognition or drive)).ti,ab. 26. or/2-25 27. 1 and 26 28. animal/ not human/ 29. 27 not 28
PsycINFO, Platform: OvidSP, Database: PsycINFO 1806-present, no limits used, no methodological filters used
# SSearch term 1 (brain adj 2 infarction?).ab,id,ti. 2 brain infarction.ab,id,ti. 3 (brain adj2 infarction).ab,ti,id. 4 (brain adj2 infactions).ab,id,ti. 5 basal ganglia cerebrovascular disease.ab,id,ti. 6 brain ischemia.ab,id,ti. 7 Ischemic Encephalopathy.ab,id,ti. 8 6 or 7 9 brain isch?emia?.ab,id,ti.

63A_BW_Dalen_Stand.job
125
10 cerebrovascular disorders/ or cerebral hemorrhage/ or exp cerebral ischemia/ or cerebrovascular accidents/ or subarachnoid hemorrhage/
11 intracranial arterial disease?.ab,id,ti. 12 (stroke or poststroke or post-stroke or cerebrovasc$ or brain vasc$ or cerebral vasc$ or cva$ or apoplex$ or
isch?emi$ attack$ or tia$1 or neurologic$ deficit$).ab,id,ti. 13 intracranial hemorrhage?.ab,id,ti. 14 intracranial h?emorrhage?.ab,id,ti. 15 ((brain$ or cerebr$ or cerebell$ or cortical or vertebrobasilar or hemispher$ or intracran$ or intracerebral or
infratentorial or supratentorial or MCA or anterior circulation or posterior circulation or basal ganglia) adj5 (isch?emi$ or infarct$ or emboli$ or occlus$ or hypox$ or obstruction or vasculopathy)).ab,id,ti.
16 ((lacunar or cortical) adj5 infarct$).ab,id,ti. 17 ((brain$ or cerebr$ or cerebell$ or intracerebral or intracran$ or parenchymal or intraventricular or infratentorial
or supratentorial or basal gangli$ or subarachnoid or putaminal or putamen or posterior fossa) adj5 (haemorrhage$ or hemorrhage$ or haematoma$ or hematoma$ or bleed$)).ab,id,ti.
18 ((brain or intracranial or basal ganglia or lenticulostriate) adj5 (vascular adj5 (disease$ or disorder or event))).ab,id,ti.
19 ((isch?emic or apoplectic) adj5 (event or events or insult or attack$)).ab,id,ti. 20 ((intracranial or cerebral art$ or basilar art$ or vertebral art$ or vertebrobasilar or vertebral basilar) adj5 (stenosis
or isch?emia or insufficiency or arteriosclero$ or atherosclero$ or occlus$)).ab,id,ti. 21 ((unilateral or visual or hemispatial or attentional or spatial) adj5 neglect).ab,id,ti. 22 aphasia/ or hemiplegia/ or hemianopsia/ or general paresis/ or paralysis/ or dysarthria/ or muscle spasms/ 23 aphasia/ or hemiplegia/ or hemianopsia/ or general paresis/ or paralysis/ or dysarthria/ or muscle spasms/ or
swallowing/ 24 (aphasi$ or apraxi$ or dysphasi$ or dysphagi$ or deglutition disorder$ or swallow$ disorder$ or dysarthri$ or
hemipleg$ or hemipar$ or paresis or paretic or paralysis or hemianop$ or hemineglect or spasticity or anomi$ or dysnomi$ or acquired brain injur$ or hemiball$ or pseudobulbar palsy).ab,id,ti.
25 Isch?emic Encephalopath$.ab,id,ti. 26 hypoxia.ab,id,ti. 27 or/9-26 28 Frontal Systems Behavioral Inventory.tm. 29 (neuropsychiatric adj5 inventory).ti,ab,tm. 30 (ias or ia or aes or as or dair or lars or flops or frsbe or kbci or npi).ab,id,ti. 31 irritability apathy scale.ab,id,ti,tm. 32 apathy inventory.ab,id,ti,tm. 33 apathy evaluation scale.ab,id,ti,tm. 34 apathy scale.ab,id,ti,tm. 35 dementia apathy interview and rating.ab,id,ti,tm. 36 lille apathy rating scale.ab,id,ti,tm. 37 frontal lobe personality scale.ab,id,ti,tm. 38 frontal system behavior scale.ab,id,ti,tm. 39 frontal system behaviour scale.ab,id,ti,tm. 40 key behavio?r change inventory.ab,id,ti,tm. 41 apathy.ab,id,sh,ti. 42 motivation.mp 43 alexithymia.ab,id,sh,ti or emotional responses/ 44 emotions/ 45 exp motivation/ 46 abulia.ab,id,ti. 47 amotivation.ab,id,ti. 48 avolition.ab,id,ti. 49 (flat adj2 affect).ab,id,ti. 50 bluntness.ab,id,ti. 51 indifference.ab,id,ti.

63B_BW_Dalen_Stand.job
126
52 volition.ab,id,ti. 53 ((reduced or loss) adj3 (concern or effort or emotional or "action initiation" or interest or motivation or behavior
or behaviour or cognition or drive)).ab,id,ti. 54 or/28-53 55 27 and 54
No results: basal ganglia cerebrovascular disease.ab,id,ti, intracranial arterial disease?.ab,id,ti, (brain adj 2 infarction).ab,id,ti 5. Excluded studies: Eight studies were conference or dissertation abstracts only. Reasons for exclusion of studies were: not concerning apathy,1-7 duplicate publication on a cohort already described earlier,8-13 restriction to patients with subcortical infarctions only,14-16 or to patients diagnosed with post-stroke depression.17 References: 1. Paradise M, Walker Z, Cooper C et al. Prediction of survival in Alzheimer's disease--The LASER-AD longitudinal study. International Journal of Geriatric Psychiatry 2009;24:739-747 2. Van Heugten CM, Smit RA, Schols JMGA. Cognitive problems in the rehabilitation of stroke patients in the nursing home. [Dutch]. Tijdschrift voor Gerontologie en Geriatrie 2007;38:173-184 3. House A, Dennis M, Mogridge L, Warlow C, Hawton K, Jones L. Mood disorders in the year after first stroke. British Journal of Psychiatry 1991;158:83-92 4. Bour A, Rasquin S, Aben I et al. The symptomatology of post-stroke depression: Comparison of stroke and myocardial infarction patients. International Journal of Geriatric Psychiatry 2009;24:1134-1142 5. de Coster L, Leentjens AFG, Lodder J, Verhey FRJ. The sensitivity of somatic symptoms in post-stroke depression: A discriminant analytic approach. International Journal of Geriatric Psychiatry 2005;20:358-362 6. Kotila M, Waltimo O, Niemi ML, Laaksonen R, Lempinen M. The profile of recovery from stroke and factors influencing outcome. Stroke 1984;15:1039-1044 7. Naarding P, de K, I, van KF, Janzing JGE, Beekman ATF, Koudstaal PJ. Post-stroke dementia and depression: Frontosubcortical dysfunction as missing link? International Journal of Geriatric Psychiatry 2007;22: 1-8 8. Hama S, Yamashita H, Kato T et al. 'Insistence on recovery' as a positive prognostic factor in Japanese stroke patients. Psychiatry and Clinical Neurosciences 2008;62: 386-395 9. Hama S, Yamashita H, Shigenobu M et al. Sitting balance as an early predictor of functional improvement in association with depressive symptoms in stroke patients. Psychiatry and Clinical Neurosciences 2007;61:543-551 10. Angelelli P, Bivona U, Serio M et al. Prevalence and evolution of neuropscyhiatric disturbances after stroke. Preliminiary data. Rivista di Neurobiologia 2001;47:251-257 11. Hama S, Yamashita H, Shingenobu M et al. Post-stroke affective or apathetic depression and lesion location: left frontal lobe and bilateral basal ganglia. European Archives of Pychiatry and Clinical Neuroscience 2007;257:149-152 12. Aybek S, Carota A, Ghika-Schmid F et al.motional behaviour in acute stroke: the Lausanne emotion in stroke study. Cognitive and behavioural neurology 2005;18:37-44 13. Brodaty H, Withall A, Altendorf A, Sachdev PS. Rates of depression at 3 and 15 months poststroke and their relationship with cognitive decline: The Sidney Stroke Study. The American Journal of Geriatric Psychiatry 2007;15:477-486 14. Yamagata S, Yamaguchi S, Kobayashi S. Impaired novelty processing in apathy after subcortical stroke. Stroke 2004;35:2437-2441 15. Okada K, Kobayashi S, Yamagata S, Takahashi K, Yamaguchi S. Poststroke apathy and regional cerebral blood flow. Stroke 1997;28:2437-2441 16. Mok VCT, Wong A, Wong K et al. Executive dysfunction and left frontal white matter hyperintensities are correlated with neuropsychiatric symptoms in stroke patients with confluent white matter hyperintensities. Dementia and Geriatric Cognitive Disorders 2010;30: 254-260

64A_BW_Dalen_Stand.job
127
17. Gainotti G, Azzoni A, Marra C. Frequency, phenomenology and anatomical-clinical correlates of major post-stroke depression. British Journal of Psychiatry 1999;175:163-167 Appendix S2: data extraction form:
DData extraction fields SSub fields Date of extraction Author, Year, Title Hospital and country of origin
Source of funding Study characteristics Aims/objectives Method of inclusion Inclusion/exclusion criteria Inclusion period Number of patients excluded Number of patients included Drop-outs Follow-up Time since stroke Conclusions Apathy Number of patients assessed for apathy Number of apathetic patients Number of non-apathetic patients Measurement, source and cut-off used Significant associations with apathy Remarks Age Age of apathetic patients Age of non-apathetic patients Gender % female of apathetic patients % female of non-apathetic patients Depression Number of patients assessed for depression Number of depressed patients with apathy Number of depressed patients without apathy Measurement and cut-off used Significant associations with depression Remarks Cognitive impairment Non-apathetic score and SD Apathetic score and SD Measurement Significant associations Remarks Motor impairment Apathetic score and SD Non-apathetic score and SD Measurement Significant associations Remarks Outcome: location Significant association Measurement tool Length of follow-up

64B_BW_Dalen_Stand.job
128
Outcome: treatment Setting of intervention Description of protocol and co-interventions Length of follow-up Number of participants enrolled Number of patients for intervention Number of controls Number of participants included in analysis Number of withdrawals, exclusions, lost to follow-up Summary outcome data Type of analysis Results of analysis Additional outcomes Limitations Declared interests Costs and resource use Adverse events Conclusion

65A_BW_Dalen_Stand.job
129
Ap
pen
dix
S3:
bia
s as
sess
men
t fo
rm
Type
of c
ohor
tR
epor
ted
excl
usio
ns%
of p
atie
nts
incl
uded
Patie
nt s
ourc
e (s
ettin
g)A
scer
tain
men
t of
stro
ke
Rep
orte
d ra
te o
f de
pres
sion
Rep
orte
d on
co
gniti
ve
func
tion
Rep
orte
d on
age
Ass
essm
ent
Out
com
e no
t pr
esen
t bef
ore
even
tC
ontro
ls
Follo
w-u
p
Star
kste
in 4
819
93A
A83
%A
AA
AA
AB
CB
Mar
in 46
1994
DC
n.a.
CA
AA
AB
BB
: p.v
.B
And
erss
on 40
1999
BC
n.a.
CB
BB
BB
BC
B
An g
elel
li 39
2004
CC
n.r.
DA
AB
AC
BA
B
Piam
arta
4520
04A
Cn.
r.A
BA
AA
BB
CB
Bro
daty
4120
05A
B66
%A
AA
AA
BB
B: a
.v.
A
Car
ota
5320
05A
A84
%A
AA
BB
DB
CB
Hoc
hste
nbac
h 42
2005
AC
n.r.
AA
BC
AD
BC
B
Cae
iro
5120
06A
A82
%A
BA
BB
CB
B. a
.c.s.
B
Kaj
i 4320
06A
A10
0%C
BA
BA
BB
CB
Ham
a 420
07A
A60
%B
AA
AA
BB
CB
Jarz
ebsk
a 44
2007
AB
82%
AB
AB
BB
BC
B
Sant
a 50
2008
AC
n.r.
BA
AA
AB
BC
B
Gre
eno p
5520
09A
A10
%A
AA
AA
CB
CB
May
o 5
2009
AB
60%
AB
AA
BC
BC
A
Hof
fman
n 56
2010
AB
4%A
Bex
cl.
BA
CB
CB
Sage
n 60
2009
AB
57%
AB
AB
AB
BC
B
Ono
da 5
820
10B
Cn.
r.A
AA
AA
BB
CB
Rus
h 47
2010
AC
n.a.
CA
AA
AC
BA
B
Mar
asco
5720
11A
B78
%A
BA
AA
CB
CB
Cae
iro
5220
11A
A80
%A
BA
AA
BB
B. a
.c.s.
B
Cas
tella
nos
5420
11A
Cn.
r.A
AA
AB
CB
CA
With
all 4
920
11A
B52
%A
AA
AB
BB
B: a
.v.
B
Plan
ton 5
920
12A
A20
%A
AA
AA
BB
B: n
.r.f.
B
Scor
es:
APr
ospe
ctiv
e C
ohor
tW
ith re
ason
s fo
r ex
clus
ion
Rep
rese
ntat
ive
of
com
mun
ityD
iagn
ostic
crit
eria
de
scrib
edFu
llyFu
llyFu
llySc
ale
com
pare
d to
cl
inic
alas
sess
men
tY
esSa
me
com
mun
ityFo
llow
-up
BC
ase-
Con
trol
Parti
ally
Unc
erta
inD
iagn
ostic
crit
eria
no
t des
crib
edIn
par
tIn
par
tIn
par
tSc
ale
desi
gned
for
apat
hyN
ot d
escr
ibed
Diff
eren
t /
unkn
own
No
follo
w-
up
CC
ross
-sec
tion
Not
repo
rted
Not
repr
esen
tativ
e of
co
mm
unit y
Not
re
porte
dN
ot re
porte
dN
ot
repo
rted
Oth
er s
cale
Not
pre
sent
DR
etro
spec
tive
coho
rtN
ot re
porte
dY
es o
r no
ques
tion
Bol
d an
d un
derl
ined
stud
ies:
use
d fo
r sen
sitiv
ity a
naly
sis
with
rela
tivel
y lo
w s
elec
tion
(rep
orte
d ex
clus
ion
< 50
%, i
nclu
sion
from
a s
ourc
e lik
ely
to p
rovi
de a
repr
esen
tive
sam
ple
of a
stro
ke p
opul
atio
n) a
nd c
onfo
undi
ng b
ias
(A o
r B
only
), C
ontr
ols:
a.v
.: ac
tivel
y re
spon
ding
vol
unte
ers,
n.a
.: no
t app
licab
le to
stu
dy d
esig
n, n
.r.:
not r
epor
ted,
a.c
.s.: a
cute
cor
onar
y sy
ndro
me
patie
nts,
p.v
.: vo
lunt
eers
recr
uite
d fr
om a
uni
vers
ity p
ool,
n.r.
f.: n
o ris
k fa
ctor
s fo
r vas
cula
r di
seas
e
Con
foun
ding
bia
sIn
form
atio
n bi
asSe
lect
ion
bias
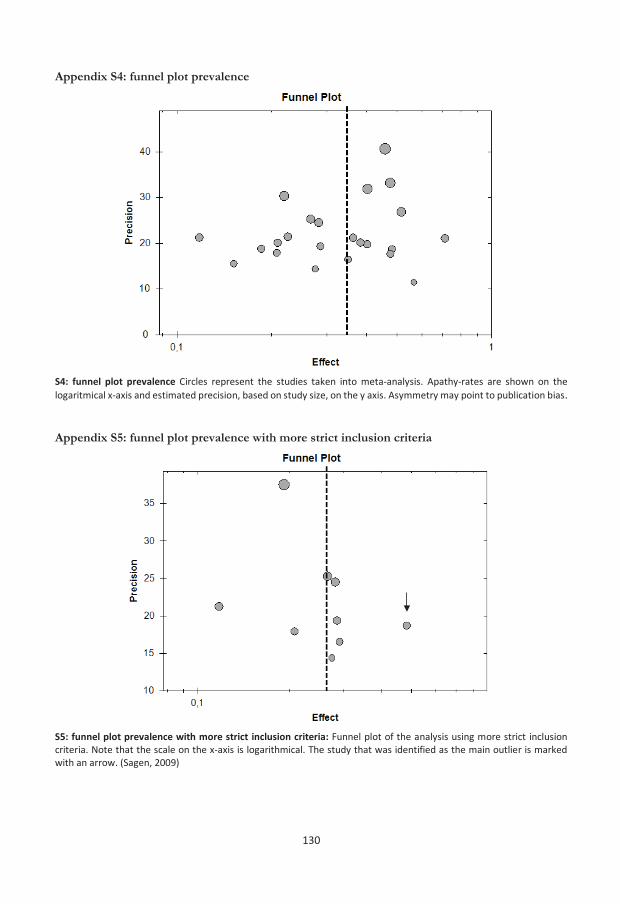
65B_BW_Dalen_Stand.job
130
Appendix S4: funnel plot prevalence
S4: funnel plot prevalence Circles represent the studies taken into meta-analysis. Apathy-rates are shown on the logaritmical x-axis and estimated precision, based on study size, on the y axis. Asymmetry may point to publication bias. Appendix S5: funnel plot prevalence with more strict inclusion criteria
S5: funnel plot prevalence with more strict inclusion criteria: Funnel plot of the analysis using more strict inclusion criteria. Note that the scale on the x-axis is logarithmical. The study that was identified as the main outlier is marked with an arrow. (Sagen, 2009)

66A_BW_Dalen_Stand.job
131
Appendix S6: exploratory sub group analyses Study N Proportion 95% CI N studies Scale
Subgroup: setting N Proportion 95% CI N studies I 2sub acute 996 38,2% 29,1-48,2 9 47,0%inpatients 409 40,5% 22,8-53,4 4 44,3%in- and outpatients 863 31,5% 22,4-42,2 6 46,7%outpatients 310 25,6% 19,6-32,6 4 26,9%Subgroup: depression N Proportion 95% CI N studies I 2Excluded 748 33,4% 25,3-42,7 8 45,0%Not excluded 1830 34,7% 28,7-42,3 15 46,9%Subgroup: CI N Proportion 95% CI N studies I 2Excluded 1009 32,6% 26,9-38,8 13 47,2%Not excluded 1569 37,5% 29,4-46,3 10 39,2%Subgroup: disability N Proportion 95% CI N studies I 2Excluded 1215 32,0% 23,9-41,4 8 47,2%Not excluded 1363 36,0% 29,2-43,5 15 46,1%Subgroup: type of stroke N Proportion 95% CI N studies I 2Infarction only 992 33,7% 25,1-43,5 10 46,9%Infarction and hemorrhage 1594 35,3% 28,9-42,4 12 46,1%Subgroup: medical history N Proportion 95% CI N studies I 21st stroke 418 24,1% 19,5-29,5 6 22,1%Any history of stroke 2160 38,9% 33,1-45,0 17 46,2%
N Proportion 95% CI N studies I 2:Pooled 2580 34,7% 29,5-40,2 23 46,4%
0 10 20 30 40 50 60 70 80 90 100 S6: exploratory sub group analyses. N: number of patients, N studies: number of studies, CI: cognitive impairment Appendix S7: funnel plot of the analysis of differences in MMSE scores between apathetic and non-apathetic groups
S7: funnel plot of the analysis of differences in MMSE scores between apathetic and non-apathetic groups. The difference in MMSE scores of apathetic patients compared to non apathetic patients is represented in points on the X-axis. The two main outliers are marked with arrows. (from left to right: Starkstein, 1993 and Greenop, 2009)