utilizing navigators to enhance medical/dental integration
TRANSCRIPT
UTILIZING NAVIGATORS TO ENHANCE MEDICAL/DENTAL INTEGRATION
WILLIAM DONIGAN DDS, MPH

OR GETTING MORE CHILDREN INTO YOUR DENTAL PROGRAM.


ZIG ZIGLAR
"THE 3 C'S OF LIFE:

WILLIAM DONIGAN DDS, MPH
• A clinic child
• Marquette University, BS Biology
• University of Illinois Chicago DDS
• University of Kansas MPH
• Private Practice 1983-2007
• Dental Director 1996 – Present
• No financial ties

• 1997 – Martin de Porres
• 2001 – Flint Hills Community Health Center
• 2007 – Gaston Family Health Services
• 2011 – NNOHA Clinician of the Year
• 2011 Safety Net Solutions Expert Advisor
• 2012 – Gaston County Public Health Hero
• 2016 North Carolina Provider of the Year
• MOM – Gastonia 2010,2012,2015,2017,2020 3500 patients, $1.5 M donated care



How many times have you thrown you call list away as
your contact information is no longer relevant?
Community Health Workers, can be the “eyes and ears”
of our colleagues out in the field, they are ready to
address the health care needs of individuals across the
lifespan, from babies to pregnant women to our
esteemed elders.
They can bring the relevance of good overall health to
the community and those living within it. Prevention and
education are their tools of the trade

BRINGING ORAL HEALTH INTO THE OVERALL HEALTH CARE CONVERSATION WILL ENHANCE EFFICIENCY, EFFECTIVENESS, PRODUCTIVITY AND PROFITABILITY (NO MARGIN, NO MISSION).
This integration will truly make a demonstrable
impact within the overall health of the
community, not just in the lives of individuals
who have been lucky enough to “break into the
system.”

BALANCE?
11
Uninsured
Patients
Medicaid Patients,
Commercial
Insurance Patients
Equals Sustainability

• The number of dental encounters
should produce 75% of revenue
for a Health Center dental
program
• How many uninsured patients is
enough for your center?
• How many uninsured patients do
we treat until the need is met?
• We need Medicaid and
Commercial insurance to help
pay for care for the uninsured.
BALANCE?

Where we
are and
who we
serve!

Primary
Care
Pharmacy
Medication
AssistanceBehavioral
Health
Dental
HIV
Case
Management
Disease
Management
SERVICES
Vision

(PHS330 = $7M)
IMPACT
Service Area Gaston County
Patients 45,000 31,000
Patient
Visits172,000 101,000
Staff 600 360
Budget $42M $27M
1 in 7Gaston County Residents
ECONOMIC
ENGINE
45%of Gaston County’s
Uninsured

GASTON FAMILY HEALTHSERVICES

DENTAL SERVICES
• Hudson Boulevard - 1996
• Summit Crossing Pediatric Dental Services – 2004 (Originally Aberdeen)
• Statesville Dental – 2009
• Catawba Dental – 2015
• Lexington Dental– 2015
• Mobile Dental Services (North) – 2016
• Lincolnton Dental – 2019
• Mobile Dental Services (South) – 2019
• Mocksville Dental - 2019

• Recommends that all
children receive an
oral health assessment
(screening) and
appropriate referral
by a trained health
care professional or
trained layperson
within 6 months after
the eruption of the
first primary tooth, but
no later than one year
of age;
AAPHD (AMERICAN ASSOCIATION OF PUBLIC HEALTH DENTISTRY)
18

• ….recommends that
children be seen by a
dentist following the
eruption of the first
tooth, but not later
than 12 months of
age.
AAPD (AMERICAN ASSOCIATION OF PEDIATRIC DENTISTRY)
19

SO WHAT SHOULD THE GOAL OF NAVIGATION BE?
• To increase the number of patients (children) in your dental program by
bringing oral health into the medical visit!
• To employ successful navigation from the medical program to the dental
program
• To create successful data collection (accurate, meaningful and timely)
• To be able to evaluate the integration and modify to meet our practice needs

WHAT’S WRONG IN AMERICA?• Oral diseases and disorders in and of themselves affect health and well-being
through life.
• There are safe and effective measures to prevent the most common dental diseases
dental caries and periodontal diseases.
• Lifestyle behaviors that affect general health such as tobacco use, excessive alcohol
use, and poor dietary choices (soda, juice, sports drinks) affect oral and craniofacial
health as well.
• There are profound and consequential oral health disparities within the American
population.
• The mouth reflects general health and well-being.
• Oral diseases and conditions are associated with other health problems.
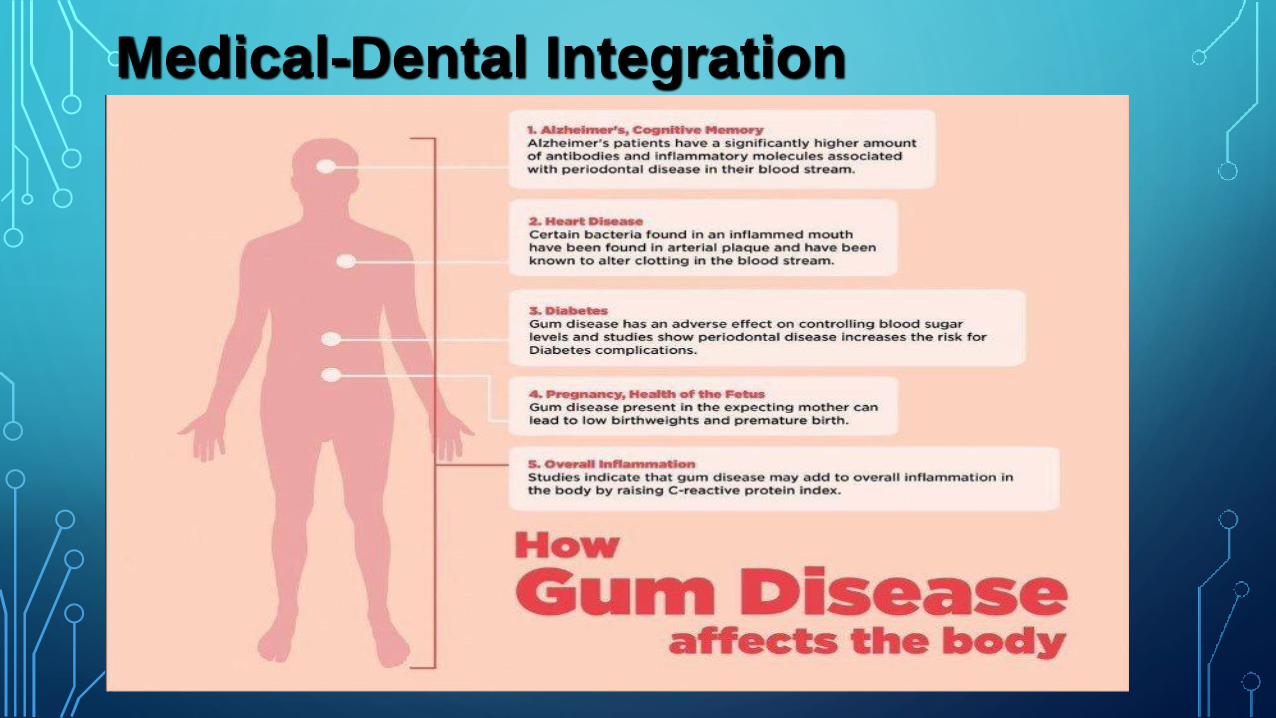
Medical-Dental Integration

WHAT’S WRONG IN AMERICA?
• Overall. Non-Hispanic blacks, Hispanics, and American Indians and Alaska
Natives generally have the poorest oral health of any racial and ethnic groups in the United States.
• Children and Tooth Decay. The greatest racial and ethnic disparity among children aged 2–4
years and aged 6–8 years is seen in Mexican American and black, non-Hispanic children.
• Adults and Untreated Tooth Decay. Blacks, non-Hispanics, and Mexican Americans aged 35–
44 years experience untreated tooth decay nearly twice as much as white, non-Hispanics.
• Tooth Decay and Education. Adults aged 35–44 years with less than a high school education
experience untreated tooth decay nearly three times that of adults with at least some college education.
• Adults and Oral Cancer. The 5–year survival rate is lower for oral pharyngeal (throat) cancers
among black men than whites (36% versus 61%).
• Adults and Periodontitis. 47.2% of U.S. adults have some form of periodontal disease. In adults
aged 65 and older, 70.1% have periodontal disease.
• Periodontal Disease is higher in men than women, and greatest among Mexican Americans and Non-Hispanic blacks, and those
with less than a high school education.


WHAT’S RIGHT (IN MISSISSIPPI) ?
• Percentage with a PCP Visit in the Past Year: Ages 25 Months-6 Years 88%
• Percentage with a PCP Visit in the Past Two Years: Ages 7-11 Years 91%
• Percentage with a PCP Visit in the Past Two Years: Ages 12-19 Years 88%
• Percentage with a PCP Visit in the Past Year: Ages 12-24 Months
99.4%

OPPORTUNITIES
• 2011 statistics
• 1/3 of adults age 35-64 who visit the physician have not seen a dentist in the last
12 months
• 10% of adults age 21-49 who visited the dentist had not seen a physician in the last
12 months
• Mutual benefit
• Both physician and dentist
• Use the registration form
Opportunities
6/17/2014NC Oral Health Collaborative 1

HRSA HAS ADOPTED THE FOLLOWING DEFINITION OF COMPREHENSIVE PRIMARY ORAL HEALTH CARE THAT HAS APPEARED IN POLICY AND PROGRAM GUIDANCE SINCE 1997:
• Comprehensive primary oral health services is defined as personal oral
health care, delivered in the context of family, culture, and community,
that includes all but the most specialized oral health needs of the
individuals being served.


Patients need to take some
responsibility for their own care!
Education!
Education!
Education!!!!!!!!!!!!!!!!!!

Break?

How about an increased
number of children
without caries. Which
should mean:
WHAT SHOULD THE BENEFITS OF NAVIGATION BE?
An increased
number of adult
patients without
caries andAn increased number
of patients having
treatment completed
Education, Education, Education Children - Diet, Soda, Sugars
• Transportation
• Car, Bus or use their feet?
• Childcare
• Isn’t it hard to treat patients
with other little ones in the
room
• Finances
• Can’t even afford the nominal
fee
• Medicaid reimbursement
• 3% loss (shared savings plan),
It has been about 9 years
since our last increase
• Telephone
• Usage, pay as you go, no
minutes, no messages
WHAT ARE THE BARRIERS FACED BY YOURPOPULATION?
32

• Oral Health Literacy
• Cooperation with
provider instructions
• Lack of care
• Many are first timers
or only came when in
pain
• Raised that way
• Lack of discretionary
funds
• Basics, medications
WHAT BARRIERS ARE BROUGHT BY YOUR POPULATION?
33

REMEMBER WE SHOULD ALL WANT TO:
1. Improve Access - Every infant and child is worthy of the
opportunity to benefit from contemporary knowledge and
measures that will improve his or her oral health, overall
health, and health trajectory.
2. Improve oral health outcomes - Oral health is the
window to the entire body.

FACTS ABOUT MEDICAL-DENTAL INTEGRATION
•All CHC Medical patients should be dental patients
•Probable not possible!
•High priority populations:
•Children
•Pregnant women
•HIV/RW
•Diabetics
•Cardiovascular disease

ALL OF OUR CLINICS SEE CHILDREN!
•Why?
•How do we attract more children?
• In this age of corporate dental clinics?
•What are your thoughts?

DAP (DENTAL ACCESS PROGRAM)
• 2007-2008 9 SCHOOLS 353 STUDENTS
• 2008-2009 20 SCHOOLS 900 STUDENTS
• 2012-2013 34 SCHOOLS 2,136 STUDENTS
• 2016 36 SCHOOLS 2,800 STUDENTS
• 2018 56 SCHOOLS 4,100 STUDENTS
• IREDELL COUNTY WAS ADDED IN SCHOOL YEAR 2010-2011
• MDU 2017
• Melissa Boughman RDH, Dental Access Coordinator

WHAT DOES A DAP NAVIGATOR DO?
• Makes appointment
• Verify eligibility
• Verifies parent and child make it to the appointment
• Assist with transportation if Medicaid and requested
• Contact parent within 24 hours
• If no contact
• Three times in next two weeks, different times of day
• No contact postcard

2012 CHOP (CHILD HEALTH OUTREACH PROGRAM)
• Priorities:
• 1. Educate caregiver and children about oral health, caries
transmission, pediatric dental specialty care and especially the one
year dental visit.
• 2. Relieve burden of accessing care by directly scheduling dental
appointments at the location of their choice for children and
caregiver while at their pediatric medical visit.
• 3. Integrate oral health into the medical visit.

CHOP (CHILD HEALTH OUTREACH PROGRAM)
• Components:
• 1. Full time bilingual staff member
• 2. Office space in the pediatric medical clinic
• 3. Laptop computer
• 4. Wireless internet (VPN), EDR capable
• 5. Salary, benefits, and equipment funded by dental
clinic

CHOP (CHILD HEALTH
OUTREACH PROGRAM)• Non-tangible components:
• 1. Hardworking and dedicated individual
• 2. Flexibility of liaison, clinicians and
staff
• 3. “Buy-in” of clinicians with whom the
liaison is working
CHOP (CHILD HEALTH
OUTREACH PROGRAM)• Training with pediatric & general
dentists in oral health
• Training with front office staff in Dentrix
• Training in data collection with PM
• Training in Fluoride Varnish placement

HOW DO YOU SCHEDULE IN YOUR CENTER?
• An hour per patient?
• Two columns per provider?
• How about hygiene patients?
• An hour?
• Hygiene assistant?
• Kids?

HYGIENE APPOINTMENT LENGTHS
• Child/New Patient over 12 treated as adult 60 minutes
• Child/New Patient over 8 50 minutes
• Child/New Patient under 8 40 minutes
• Child Recall no x-rays 30 minutes
• Child Lap to Lap <3 yoa 30 minutes
• Sealants 30-40 Minutes
depending on age/degree of difficulty
• Education! Education!! Education!!!!!!!!!!!!! Of staff

CHOP (CHILD HEALTH
OUTREACH PROGRAM)•Benefits to the patient:
• 1. Education about oral hygiene and diet
at medical visit
• 2. Education about the one year dental
visit
• 3. Convenience of scheduling for both
caregiver and child

CHOP (CHILD HEALTH
OUTREACH PROGRAM)
•Benefits to the dental clinic:
• 1. Constant influx of new patients
especially 1 year olds and special
needs patients.
• 2. Liaison has quick communication
with dentists if needed via e-mail or
Dentrix messenger.
• Benefits to medical clinic
• Time
• Money

DO OUR PRIORITIES MEET WITH OUR OBJECTIVES?
• Increase Patient Dental IQ
• Get children into clinic early (age 1)
• Create a broader patient base of
children
• Increase number of Patients with a
payer source
• Improve sustainability

PROJECT PLANNING PROCESS
• Timeline- CEO, GCHD director and
medical director, providers (medical and
dental)
• Unique and great relationship with HD,
CEO wants the dental clinic run as if my
own? So I took ownership!!!!!

• 75% treatment completion within 6 months,
sealants placed on all molars, premolars, and
primary molars that need placement
WHAT SUCCESS MIGHT LOOK LIKE?
No pain!

“I see in our patients a remarkable improvement in their oral health. The CHOP program is showing families that dental caries can be prevented as well as many other illnesses.”
Cindy TorresDental LiaisonGaston Family Health Services Pediatric DentistryGaston Family Pediatrics

CHOP (CHILD HEALTH OUTREACH PROGRAM)
• Success!!!!!!!!!!!!!!!!!!!!
• The income brought into our dental clinics due to the program far
exceeds the salary and benefits of the liaison (125-175 new
patient appointments monthly)
• Most are new patients or those who have not seen a dentist in
more than six months
• No parent has declined having the liaison provide oral health
education during the child’s medical visit
• The show rate of liaison scheduled patients is around 80-85%
which closely approximates our dental clinic show rate

Child Health Oral
Program 2016
Jan-
16
Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-
16
# Declines 0 0 0 0 0 0 0 0 0 0 0 0 0
# Uninsured appt
made
4 0 6 2 2 3 4 2 5 4 5 3 40
# Appointments
Kept
74 111 81 49 55 70 77 76 77 76 78 69 893
# Insured
appointment made
95 128 90 67 62 74 73 79 81 72 83 70 974
# Appointments
Made
98 129 96 69 64 77 84 81 86 87 88 82 1041

CFD WIC CHOP, 2017
Jan-
17
Feb-
17
Mar-
17
Apr-
17
May-
17
Jun-
17
Jul-
17
Aug-
17
Sep-
17
Oct-
17
Nov-
17
Dec-
17
Tot
al
Number of
Declines
0 0 0 153 151 148 181 221 304
Number of
uninsured appts
made
1 1 2 2 0 0 0 1 1 3 6
Number of
appointments Kept
17 24 50 51 42 28 44 55 48 29 212
Number of Insured
appointments
made
24 40 88 86 77 51 75 94 65 45 366
Total number of
appointments
Made
25 41 90 88 77 51 75 95 66 48 372
Percentage of
appt kept
68% 59% 56% 58% 55% 55% 59% 58% 73% 60% 59%

BUILD IT AND THEY WILL COME!
MAYBE??????????????????????

47 NEW PATIENTS FOR ALL OF
2016 AT STATESVILLE FAMILY
DENTISTRY REFERRED FROM
STATESVILLE CHILDREN’S CLINIC
HOW IMPORTANT IS OUR NAVIGATOR?
4584 new patients 2012 - 2016!

EDUCATION!!!

What Causes Cavities? SUGAR – From foods and drinks left on the teeth
PLAQUE – A bacteria which is on the teeth
ACID – Caused by sugar and plaque left on the teeth
SUGAR + PLAQUE + ACID = CAVITIES
(American Dental Association, 2011b)
EDUCATION!!

BABY ORAL HEALTH PROGRAM (BOHP)
•Cindy Cruz
•http://www.babyoralhealthprogram.org/
•http://www.prenataloralhealth.org/video/moth
ers1-english.mp4

EDUCATION!!!!!!!!!!!!!!!!!!!
But most general dentists, as a rule, only treat as emergency cases.
All dentists see pregnant patients!
Why don’t many general dentists treat pregnant patients?
Fear (recent ADA Journal article)https://www.ada.org/en/press-room/news-releases/2015-archive/august/new-study-shows-dental-treatment-during-pregnancy-is-safe
Lack of medical consultation
Phase I Dentistry (extractions, fillings, etc.)
Many have Medicaid- Regular Medicaid vs. Pregnancy Medicaid

DATA?HOW VITAL IS IT?ACCURATE, MEANINGFUL, TIMELY….
- 1/5 HEALTH CENTER PATIENTS SHOULD BE DENTAL PATIENTS……
- HOW MANY CHILDREN ARE THERE IN YOUR PROGRAM?

HOW ABOUT CLOSING THE LOOP?
• Referral from Medical
• Dental remediation of situation
• Acknowledgment of treatment back to
Medical

WHAT ARE THE CHALLENGES?
Keeping it Vibrant
Coordination of Services (billing)
Staff Turnover (pay scales &
Benefits)
Staff buy in
Parental buy in

WHAT LESSONS CAN WE LEARN?
• Collaboration is powerful
• Implementation phase
• Sustainability

THE AFFORDABLE CARE ACT AND BEYOND
•Where will we be?
•2002 45% utilization ages 25-45 versus
•2012 35% utilization same age group
Why?
Where will you be in 2020 and beyond?
How do we get there?

WHAT DOES IT ALL MEAN?
• 2002 – 287 million, ages 25-45 99.8 million, 173 thousand dentists 45%, 44 million
• 2012 – 314 million, ages 25-45 81.1 million, 190 thousand dentists 35% 28 million
• 2025 – trends, 201 thousand dentists
• 20% DSO
• 12% loss annually nationwide all practices
• New patients to make up for it? How
• Marketing (external)
• CHOP, DAP
• Internal

Ideas – what fits and can you
do it?
THINK
69
Relationships – County with
FQHC, with DSS, WIC, etc.
PDSA’s – small incremental
changes for the better
Program evolution
You will always have
change
When the pain of staying the same becomes
greater than the pain of change you’ll change!

PATIENTS

William Donigan DDS, MPH
Dental Director
Gaston Family Health Services
(704) 862-5376
CONNECTIONS