using the bowen technique to treat symptoms … · causes of adhesive arachnoiditis: known causes...
TRANSCRIPT

Diploma of Specialised Bowen Therapy 22006IVC __________________________ Katherin Phillips
Assessment for Professional Skills
Assessment Task 1: Research task on traditional, alternative and scientific practices in medicine.
USING THE BOWEN TECHNIQUE TO TREAT SYMPTOMS OF
ADHESIVE ARACHNOIDITIS.
2. General Description, beliefs, evolution of this treatment and relevant condition.
History, beliefs and evolution of the Bowen Technique: It states in the Bowtech brochure ‘State of the Art
Healing Technique” that the Bowen Technique was developed in the 1950’s by the late Tom Bowen from
Geelong Australia.
Bowen became a celebrated therapist, regularly treating over 13,000 patients each year. In 1974, he invited
Oswald Rentsch and his wife Elaine to study with him and document his work. Honouring their promise to
Bowen, they began to teach the technique in 1986.
Since then, over 25,000 therapists worldwide have taken Bowen Training. This is where it all started, all Bowen
training is based on Bowtech, who introduced and continue to bring the Bowen Technique to the world.
Dedicated to preserving the technique and ensuring that it is taught in its original form, they founded the
Bowen Therapy Academy of Australia in 1987. (‘State of the Art Healing Technique’ Information Brochure
presented by the Bowen Therapy Academy of Australia).
The Bowen Technique is a gentle form of body work in which subtle moves performed over the muscles and
connective tissue send messages deep into the body, retrieving cellular memory of a preferred, relaxed,
balanced way of wellbeing.
There are frequent but very essential pauses throughout the session that allows the body time to respond and
begin the healing process. The practitioner can target a specific problem or address the body as a whole.
The technique addresses not only the musculoskeletal framework, but also the fascia, nerves and internal
organs. The body's integrated response improves circulation and lymphatic drainage and aids assimilation of
nutrients and elimination of toxins.
Relevant condition - Adhesive Arachnoiditis: Adhesive Arachnoiditis is a condition which begins with the
inflammation of the Arachnoid Membrane covering the spinal canal and brain, this can cause a gradual
buildup of fibrotic scar tissue which disrupts the flow of cerebral spinal fluid (CSF) around the nerves and
deprives them of nutrition. (Burton, C. 2013)
For a greater understanding I have included information and diagrams on the anatomy of Adhesive
Arachnoiditis which was obtained from The Burton Report – see attachment 1.
http://www.burtonreport.com/InfSpine/AdhesArachAnatomy.htm
Symptoms of Adhesive Arachnoiditis: The early symptoms of this condition can be all or some of the following:
Severe low back and leg pain
numbness and chronic pain in leg(s) and feet
burning sensation, especially in the legs and feet
bladder and bowel dysfunction
severe headaches.
Many patients with this condition complain of the feeling of walking on broken glass. Often there are no
outward signs of the condition and the sufferers look deceptively normal; as the condition progress’s the
symptoms may increase and become more permanent. Some patients use wheel chairs and walking aids, and
most patients with Arachnoiditis have to give up work completely which leads to a feeling of uselessness and
loneliness at also losing the strength to keep up a social life.

Causes of Adhesive Arachnoiditis: Known causes of the condition are
Tuberculosis
Meningitis
Spinal Tumor’s
Abscesses
Spinal Surgery or Trauma
Radiculargrams
Epidurals (Steroids) and Lumbar Punctures
Cortisone Injections into the spinal canal.
BUT BY FAR THE LARGEST SINGLE CAUSE: is medical intervention such as Myelograms using Myodil Dye,
(supplied and marketed by Glaxo Smith Kline between 1945 and 1988), which is now known not to be
safe.
(GROVES,P. http://www.aasansw.org.au/ accessed 3/8/2013.)
Over many decades, some of the sufferers of Adhesive Arachnoiditis have been fighting an uphill battle
against Governments and multi-million dollar pharmaceutical companies, to have their concerns and
condition recognised and to raise awareness. While in the sidelines, many more victims have suffered in silence
and have spent the majority of their progressively incapacitated lives trying to get answers and diagnosis from
renowned health specialist, with no avail and with countless misdiagnosis.
Adhesive Arachnoiditis may be diagnoses as:
Failed back surgery syndrome
Epidural (peridural, post-surgical) fibrosis (scarring)
Multiple Sclerosis
Fibromyalgia
Reflex Sympathetic Dystrophy (Complex Regional Pain Syndrome CRPS)
Chronic Pain Syndrome
Lupus-like disorder
Depression
Psychosomatic disorder
Compensation neurosis / Malingering (Burton,C. 2013)
Treatment for Adhesive Arachnoiditis: Adhesive Arachnoiditis is difficult to treat. Treatment is limited to
alleviation of pain and other symptoms. Surgical intervention generally has a poor outcome, and only provides
temporary relief. Steroid injections, administered either intrathecally or epidurally have been linked as a cause
of the disease, therefore they are generally discouraged as a treatment and may even worsen the condition.
(Burton,C. 2013)
As stated in an article written by( Mullen, 2013)which was presented on the Medical Observer website;
(Radiologist and emeritus professor Michael Sage, from Flinders University ), said “Diagnosis was difficult
because there was a wide variation in neurological symptoms”.
Many doctors are unfamiliar with Arachnoiditis and, mistaking it for a common disc or nerve impingement
problem, order treatments that worsen the condition. Patients may be wise to see a physician with specific
experience in this area, though many doctors consider themselves a specialist while aware of the disastrous
outcomes even routine procedures can cause. Patient education is important. (Burton,C. 2013)
How Bowen Therapy addresses the symptoms of Adhesive Arachnoiditis:
Given that the symptoms of Adhesive Arachnoiditis are many and varied, I believe overall, and from the results
of my client, that the Bowen Technique addresses
neurological pain
muscular tension
distortion and wasting of soft tissue
increases circulation and resolved lower limb oedema
initiates lymphatic release
encourages an overall sense of wellbeing
alleviates mental stress
This is achieved by which Bowen moves are transmitted throughout the body by facia. This enables treatments
to be effective as the damaged nerves are not a barrier.
3. Demographic statistics
It is easy for the general community of the Moreton Bay Region to access Bowen Therapy. There are
approximately 15 qualified and registered Bowtech therapists within a 15klm radius. Over the past 2 years I
have found that when talking to others in the community there would be about 50:50 knowledge of the Bowen
Technique. The people that know of Bowen Therapy and have experienced it, love it and it is their preferred
natural therapy. On the other hand the ones that had never heard about it were intrigued with the
explanation and would consider trying it in the future.
The Moreton Bay Regional Council demographic profile, based on results obtained from the 2011 Census of
population and housing, states a population of over 400,000 people in the region.
http://profile.id.com.au/moreton-bay/service-age-groups accessed 25/8/2013.
My research shows there was and increased in use of spinal surgery and imagery investigation since back in
the early 1940’s. This would indicate that the main age group affected by Adhesive Arachnoiditis is from the
ages of 50 to 85 and over. This marries up with populating statistic in the Moreton Bay region of 117,638 people
which is a total of approximately 29% of the local community.
It is unknown of the exact number of suffers of Adhesive Arachnoiditis, due to misdiagnosis and suffers who
have actively been seeking recognition of the initial cause of their symptoms and have not been formally
diagnosed as having Adhesive Arachnoiditis by medical professionals.
It is estimated that approximately over 100,000 people in Australia have had a myelogram between 1945 and
1988. Not to mention others who have been affected by this disease through other causes.
4. Aims and Objectives of the Project
1. To bring awareness to the Bowen Therapy community: With varying views and the unfamiliarity of this
often misdiagnosed, debilitating and incurable disease by medical practitioners, most patients seek alternative
or complementary therapies to assist in reducing their symptoms. My decision to research this disease and the
positive outcomes that the Bowen Technique has had on the presented symptoms of Adhesive Arachnoiditis
will bring awareness to the greater Bowtech community.
2. To evaluate the effectiveness of the Bowen Technique on symptoms of Adhesive Arachnoiditis.
Overall the effectiveness of using the Bowen Technique in treating symptoms of Adhesive Arachnoiditis has
been a slow but positive result. Since first treating this client in June 2012 to present, there has been significant
improvements in my clients overall wellbeing, improved sleep, increased mobility, reduction in lumbar and
lower limb pain, tension and swelling and a vast improvement in medial leg rotation at the hips and a 9o%
reduction of severe oedema to the ankles and feet.
3. To introduce Bowen Therapy to sufferers of Adhesive Arachnoiditis.
One of the aims of this research project is to introduce to sufferers of Adhesive Arachnoiditis, to the prospect of
a modality which has a holistic benefit that supports traditional treatments, and to promote the effectiveness
of the Bowen Technique in improving their quality of life. This can be done by contacting Associations and
promoting to their members through website information links.
4. To compare the perception of the client pre and post treatment.
My client’s pre-treatment perception of the Bowen Technique, and its ability to relieve pain and improve or
reduce symptoms of his disease, was very sceptical.
However, post initial Bowen treatment, my client was pleasantly surprised at just how relaxed, balanced, and
how a reduction in overall pain and muscular tension was achieved after one consultation. These feelings
triggered an increased interest in how the Bowen Technique worked, and the client proceeded to do a little
research himself. The client’s acceptance and perception of the Bowen Technique had relinquished some of
the doubts of success, which was reinforced with continued improvement highlighted in future Bowen sessions.
This client was diligent in following through with my requests for him to increase hydration, gentle
stretches/exercises and to address his diet. Furthermore, the client’s perspective of the treatments and results
will be determined by regular questioning and addressing his needs as time progresses.

5. Research Method / Strategies
As I only have use this one presenting client with this medically diagnosed condition, I felt that a quantitative
method was best used in this research project. The client was interviewed at length with respect to
signs and symptoms, pain levels, quality of life and effectiveness of traditional treatments. This study utilised
many assessments and observations recorded over a period of 17 months. This research is ongoing.
6. The Study Sample / Stakeholders
My study sample was a 65 year old male with medically diagnosed Adhesive Arachnoiditis. Over the past 20
years he has slowly become physical incapacitated, to a point where he now uses a mobility walker. This client
presented for Bowen therapy treatment for relief of lumber and lower limb pain.
After several Bowen therapy treatments provided to this client, I felt that through many discussions he was
happy for me to provide him with any knowledge I had gathered on his condition. An exceptional
client/therapist rapport was developed and when asked, he was extremely happy for me to use his presenting
condition, clinical notes and discuss his history in this research assignment.
This client reports a very healthy childhood with no significant illness, nor did he require hospitalisation or
specialist medical consultation. He led an active life as a young adult, married early with a young family.
At the age of approximately 30 he was suffering with recurrent lumbar pain, which was caused from several
falls while working as a fireman and heavy labouring type work as a concreter, on his days off. The client
obtained treatments from chiropractors, physiotherapists and acupuncturists over many years, with little or no
resolve. In September 1980, as requested by his consulting physician, he underwent a Myelogram to see if that
could shed some light into the cause of his lower back pain. The Myelogram results showed congenital
narrowing of the cervical spinal cord at C1 to C3, with no other abnormalities or skeletal degeneration or
damage. His doctor’s recommendations were to continue with complementary therapies like massage,
physiotherapy etc. (Please note: this client has had no symptoms relating to the congenital narrowing of the
cervical spine).
My client continued to experience significant lumbar and sciatic pain, and as the years went on he became
increasing unable to lead an active life. He had “given up” on all physical therapy treatments and resorted to
taking pain relief medications when symptoms were intolerable. He has now learnt to live with his pain and
copes with his restricted mobility and muscular degeneration and flare up of pain at time to time.
7. Ethical Considerations
Bowen Therapy, its methodology and its effects on the body were explained in detail and written consent for
treatments and subsequent publishing of the collected results was received from the client participating.
8. Data Collection – Results
Bowen Therapy Treatment Plan.
In June 2012 this client presented with constant, central to left sided lumbar and sciatic pain on a scale of
7/10. Also there were a variety of related symptoms due to inactivity. Due to the extended period that this
client hadn’t had any physical activity or treatments, I introduced him slowly to Bowen Therapy to ensure he
didn’t experience an overload. I continued to add appropriate procedures in following treatments if no
adverse effects or minimal results were achieved after previous sessions.
Initial Observations.
On the initial consultation the client was unable to walk or stand unassisted.
Severe medial rotation of the hips, knees, ankles and feet - (spastic type gait).
Drags feet when walking.
His upper body was noticeably tilted forward from the hips.
Significant wasting of the gastrocnemius muscles.
Moderate to high levels of oedema to both ankles/feet.
Noticeably grey complexion.
Extremely dry skin.
Relevant Client Information
During general discussion of symptoms the client comments that he has regular trips and falls, bowel
dysfunction, leads a very sedentary lifestyle and his diet and water consumption is of a very poor standard. He
has learnt to deal with his continual pain and only when his lower back flares up and pain increases he will rest
more and take panadol or nurofen for relief until symptoms subside.
He mentions that he has a slightly painful cyst posteriorly on the left hip, which he has had scanned and shows
as benign.
He experiences unresolved left knee pain, which scans show no ligament or skeletal damage.
A MRI scan report of the lumbar region indicates there is normal vertebral degeneration and slight disc
narrowing.
He also has difficulty getting out of his lounge chair, finding it necessary to slide down onto the ground getting
on his knees, then turning around and using the chair and his upper body strength to get onto his feet.
He sometimes loses balances easily even when using his walker.
Client feels condition has been exacerbated by:
Untreated/unresolved PTSD from continued exposure to trauma whilst working as a fireman in the QFS
(Queensland Fire Service).
Exposure to high stress job as a senior ranked officer in the QFS.
Exposure to chemicals whilst working in QFS for 30 years.
Stress of taking years to have his condition medically diagnosed / recognised by many leading medical
professionals.
Decline in lifestyle due to his lack of ability to get around unassisted.
Assessments / Observations
Neck, thoracic and upper limb assessment shows:
reduced cervical ROM with mild muscular tension at S1
Trapezius and SCM stiffness on palpation
full active ROM in shoulders - no pain or restrictions
reduced thoracic rotation whilst sitting, slightly increasing left lumbar/sciatic pain
no pain or restrictions in upper limbs
Lumbar assessment shows:
lumbar muscle and skin tension
raised thoracic erector spinae muscle on the right
the client unable to perform lumbar extension
limited balance while standing unassisted and unable to step backwards
flattening of lumbar region
no sacroiliac joint dysfunction.
Pelvic and lower limb assessment shows:
medial rotation of legs
extreme hamstring muscle tension
extreme adductor muscle group tension
unable to abduct legs more than 20° passively, while client supine
left knee joint swelling and reduced ROM to both – no ligament weakness
gastrocnemius wasting
legs and feet cold to touch
severely dry flaky skin
wearing away of toenails from dragging feet while walking with no shoes on.
soft tissue bruising and scaring on knees, shins and ankles… from many trip and falls
no leg length, tibial or femoral length discrepancy
severely reduced ankle and foot ROM due to oedema of ankles and feet. This restriction improved
significantly at the completion of the first 3 treatments as swelling reduced remarkably.
Significant improvement noted with
each passive assessment done.
Client almost has full ROM at end of
17 months.
Special tests
1st Assessment
Slump – a positive result with increased pain and restriction to left leg
Thomas – an extremely positive result with the clients L & R legs off the table by almost 40cms
Straight leg raise – positive with L 30° R 40°
Ober test – positive with left and right illotibial tension
Stork test – negative
Follow up results at end of 17 months of Bowen treatments, and daily stretching and strengthening exercise.
Slump – continued to show significant improvement with reduced pain and restriction to left leg. At last
assessment client reported general neural sensation.
Thomas – This test has been the biggest indicator with improvement progressing slowly over each
assessment performed. Client now only has a 2 inch space between back of knee and table.
Straight leg raise – L 75° R 85°
Ober test - negative
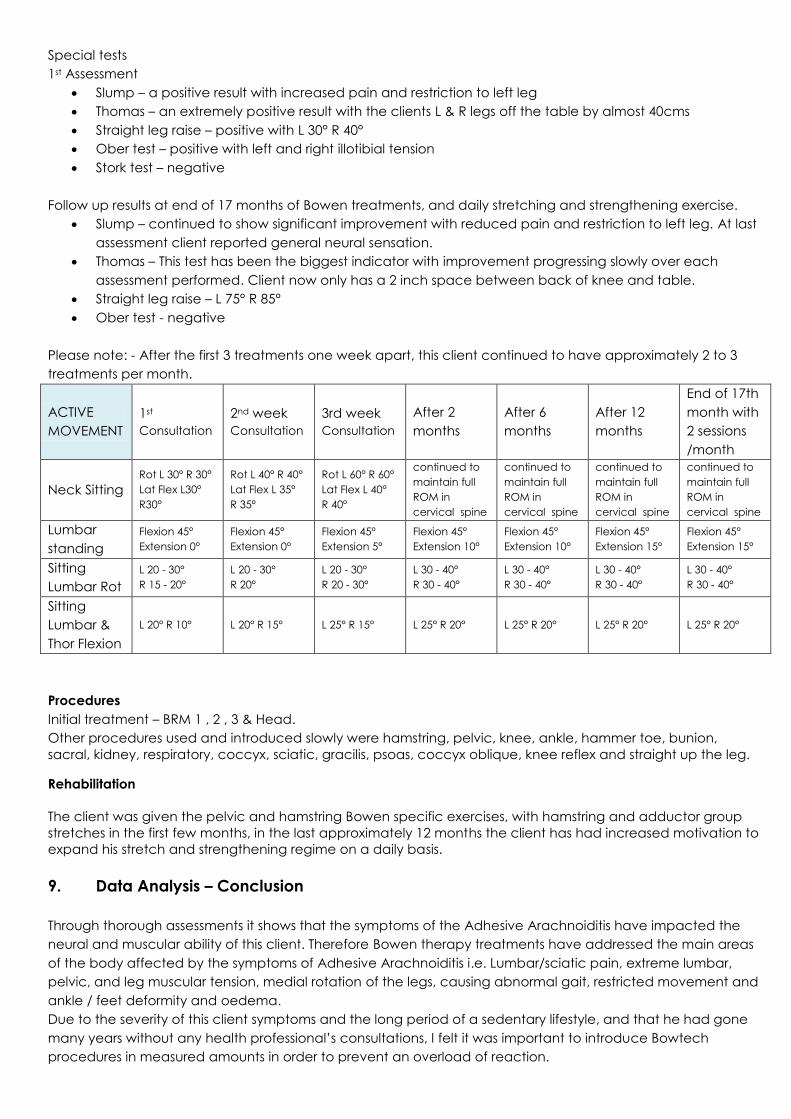
Please note: - After the first 3 treatments one week apart, this client continued to have approximately 2 to 3
treatments per month.
ACTIVE
MOVEMENT
1st
Consultation
2nd week
Consultation
3rd week
Consultation
After 2
months
After 6
months
After 12
months
End of 17th
month with
2 sessions
/month
Neck Sitting
Rot L 30° R 30°
Lat Flex L30°
R30°
Rot L 40° R 40°
Lat Flex L 35°
R 35°
Rot L 60° R 60°
Lat Flex L 40°
R 40°
continued to
maintain full
ROM in
cervical spine
continued to
maintain full
ROM in
cervical spine
continued to
maintain full
ROM in
cervical spine
continued to
maintain full
ROM in
cervical spine
Lumbar
standing
Flexion 45°
Extension 0°
Flexion 45°
Extension 0°
Flexion 45°
Extension 5°
Flexion 45°
Extension 10°
Flexion 45°
Extension 10°
Flexion 45°
Extension 15°
Flexion 45°
Extension 15°
Sitting
Lumbar Rot
L 20 - 30°
R 15 - 20°
L 20 - 30°
R 20°
L 20 - 30°
R 20 - 30°
L 30 - 40°
R 30 - 40°
L 30 - 40°
R 30 - 40°
L 30 - 40°
R 30 - 40°
L 30 - 40°
R 30 - 40°
Sitting
Lumbar &
Thor Flexion
L 20° R 10° L 20° R 15° L 25° R 15° L 25° R 20° L 25° R 20° L 25° R 20° L 25° R 20°
Procedures
Initial treatment – BRM 1 , 2 , 3 & Head.
Other procedures used and introduced slowly were hamstring, pelvic, knee, ankle, hammer toe, bunion,
sacral, kidney, respiratory, coccyx, sciatic, gracilis, psoas, coccyx oblique, knee reflex and straight up the leg.
Rehabilitation
The client was given the pelvic and hamstring Bowen specific exercises, with hamstring and adductor group
stretches in the first few months, in the last approximately 12 months the client has had increased motivation to
expand his stretch and strengthening regime on a daily basis.
9. Data Analysis – Conclusion
Through thorough assessments it shows that the symptoms of the Adhesive Arachnoiditis have impacted the
neural and muscular ability of this client. Therefore Bowen therapy treatments have addressed the main areas
of the body affected by the symptoms of Adhesive Arachnoiditis i.e. Lumbar/sciatic pain, extreme lumbar,
pelvic, and leg muscular tension, medial rotation of the legs, causing abnormal gait, restricted movement and
ankle / feet deformity and oedema.
Due to the severity of this client symptoms and the long period of a sedentary lifestyle, and that he had gone
many years without any health professional’s consultations, I felt it was important to introduce Bowtech
procedures in measured amounts in order to prevent an overload of reaction.

The client feels that his symptoms have significantly improved with each session and will continue with regular
Bowen therapy treatments to maintain his quality of life. With a daily stretching routine and improved diet his
metal attitude has improved. He has also taken it upon himself to purchase a rowing machine and a stationary
bike to increase his fitness and strength.
10. Sharing Knowledge
The Sufferers of Adhesive Arachnoiditis Associations here in Australia, have put in many hard years of work, as
they endeavour to have this condition acknowledged with the government and medical professions. Also with
discussions amongst fellow Bowtech practitioners, mainstream professionals and, indeed, those suffering from
the condition, will help to increase knowledge and hopefully encourage others to look into the causes and
effects of lumbar and lower limb pain more thoroughly. I firmly believe that Bowtech practitioners have a
place in the successful treatment of the symptoms of Adhesive Arachnoiditis and at the very least in the
improvement of the sufferers’ quality of life. This shows the unique means by which Bowen Therapy assists the
body to utilize its own innate healing ability.
Acknowledgements and Bibliography
‘State of the Art Healing Technique’ Information Brochure presented by the Bowen Therapy Academy of
Australia.
The Bowen Technique, Training and Instruction Manual, Modules 1 and 2, Introduction pages vii to ix, 2007.
MAY, Gil 2006 “Arachnoiditis – A toxic Chemical Tragedy” Nexus Magazine, pages 33-37 August/September
edition 2006.
Websites
http://www.bowen.org.au/
(GROVES, P. President of the Australian Arachnoiditis Sufferers Association NSW) ‘The purpose of this site is to
inform the public, sufferers and their families about Adhesive Arachnoiditis’ the author states that most of this
definition was posted on Gateway to Neurology of Massachusetts General Hospital.
http://www.aasansw.org.au/
Burton, C. August 2013 Edition Volume XIII http://www.burtonreport.com/ accessed 1 September 2013.
http://en.wikipedia.org/wiki/Arachnoiditis
http://www.burtonreport.com/InfSpine/AdhesArachAnatomy.htm
http://www.webmd.com/pain-management/guide/pain-management-arachnoiditis
Mullen 12 February 2013, ‘Report on the Public Roundtable into Adhesive Arachnoiditis’ presented on the
Medical Observer website. Accessed - 20 March 2013. http://www.medicalobserver.com.au/news/govt-seeks-to-raise-profile-of-adhesive-arachnoiditis
Books
Manocchia, P. 2009, Anatomy of Exercise. Hinkler Books Pty Ltd, Victoria Australia.
Kendall, FP. 2005, Muscles Testing and Function with Posture and Pain, Fifth Edition. Lipincott Williams & Wilkins.
Baltimore, USA.
Myers, T W. 2009, Anatomy Trains. Second Edition. Churchill Livingstone Elsevier. United Kingdom.
Marieb, EN. 2012, Essentials fo Human Anatomy and Physiology. Tenth Edition. Pearson Education.
San Francisco CA.
Wilks, J. 2007. The Bowen Technique – The Inside Story. CYMA Ltd. Dorset UK.

Attachment 1
The Anatomy of
Adhesive Arachnoiditis
This illustration (from Noback CR: The Human Nervous System, McGraw-Hill, Inc., 1967) illustrates the human
subarachnoid space surrounding the brain and spinal cord. 60% of spinal fluid is produced within the brain
and 40% from the spinal subarachnoid space. It flows, as shown, and is absorbed by the venous arachnoid
granulations. This spinal fluid is produced at the rate of 0.35cc/min, or 500-750cc/day. Turnover rate is 3-
5 times/day. A normal adult has a ventricular volume of about 30cc and about 100+cc in the surrounding
subarachnoid space. The subarachnoid space serves to be a hydraulic cushion for the floating brain, a
source of nutrition as well neurotransmitters. This space is the most fragile and sensitive area of the
human body.
When the subarachnoid space is subject to insult or inflammatory change damage and scarring occur. One
of the primary difficulties in addressing the subject of neuropathologic change, particularly that of

adhesive arachnoiditis is the great amount of confusion regarding nomenclature. Adhesive arachnoiditis is
an advanced form of arachnoiditis and is most often confused with the latter. Some of the other terms by
adhesive arachnoiditis has been referred to have been:
Serosa Circumscripta Spinalis
Intraspinal Granulomatosis
Obliterative Arachnoiditis
Chronic Arachnoiditis
Spinal Meningitis
Chronic Spinal Meningitis
Chemical Meningitis
Sterile Meningitis
Granulomatous Meningitis
There has been a "Tower of Babel" in regard to the terminology used
to define the normal anatomy of the lumbar spinal column, the dural
membranes, and the subarachnoid space. In the image, to the left,
the nerve rootlets of the cauda equina, which are in motor and
sensory pairs (shown as single nerves for simplification). If a lumbar
puncture were to be performed the needle would simply push the
nerve roots, floating in cerebrospinal fluid, out of the way. If a similar
procedure were attempted in a patient with Class III Adhesive
Arachnoiditis, where the nerve roots were fixed to each other and to
the dura mater, the needle could easily injure or sever the nerves.
Adhesive Arachnoiditis comes about as a progression of inflammatory change secondary to insult or
injury occurring over a period of time. This progression involves:
Acute Inflammatory Phase (Class I)
Beginning of Chronic Phase (Class II)
Chronic Scar Phase (Class III)
Arachnoiditis Ossificans

Adhesive Arachnoiditis: Acute Inflammatory Phase (Class I)
In the illustrations of the first, or acute inflammatory phase, shown above, the nerve roots are swollen and
hyperemic (vascular dilatation). Pathologic specimens show acute inflammatory cells predominating.
Adhesive Arachnoiditis: Beginning of Chronic Phase (Class II)
In the illustrations of the second phase, shown above, the nerve root swelling has progressively
decreased (the nerves are beginning to be encased in collagenous scar tissue). Pathologic specimens
show a mix of acute and chronic inflammatory cells.

Adhesive Arachnoiditis: Chronic Scar Phase (Class III)
By the time the process has reached the chronic phase there is prominent collagenous scar deposition. The
nerve roots are adherent to each other and to the meninges. Surgically opening the dura often shows
what appears to be an empty sac because the nerves are now actually part of the dural membrane. By the
Class III stage the inflammatory cells seen document a chronic process. The nerves themselves have been
progressively deprived of nourishment as the nutrient blood vessels have atrophied and the "percolating"
nourishment derived from the cerebrospinal fluid has markedly decreased. It is, in fact, a tribute to the
human nervous system that in the face of such adversity, in can, in the great majority of cases, continue to
maintain "normal" function. The only way this can happen is if the adverse process occurs slowly enough
to allow the system to adapt and acclimate. The acclimization is, however, fragile. Because function is
maintained precariously any additional insult (i.e. trauma, surgery, myelography, etc.) can tip the balance
and cause onset of clinical disability and incapacitation.
By far the greatest number of cases of adhesive arachnoiditis which have occurred throughout the world
during the 20th century resulted from oil myelography with either Pantopaque® or Myodil®. Because

these substances are hyperbaric once they were placed in the subarachnoid space they would migrate to
the distal portion, where they remained, producing progressive scarring.
The patterns of adhesive arachnoiditis scar are typically quite variable in their patterns. Shown above are
drawings of variable scar patterns in three actual cases. These are patterns reflecting diffuse, multi-level
involvement, characteristic of the introduction of a toxic foreign body substance into the sub-arachnoid
space. The last illustrations to the right shows how residual droplets of foreign body substance (in this
case Pantopaque®) are surrounded by encapsulating scar reflecting the body's defense against foreign
body substances.
The illustrations to the left
demonstrate an example of focal
adhesive arachnoiditis. In this case
it is due to the local inflammatory
effect of a hypertrophic facet joint
intruding into the central spinal
canal. Focal inflammation is also
typical following segmental spinal
trauma or focal spinal surgery.
Adhesive Arachnoiditis: Arachnoiditis Ossificans
The image to the left is a year 2000 CT scan performed on a 71 year old
woman who developed clinically significant adhesive arachnoiditis
following a 1971 Pantopaque® myelogram. Control of her constant pain
required implantation of a spinal cord neurostimulator which provided
good pain control allowing the patient return to normal function. In 1990
she began to experience progressive bowel and bladder dysfunction. The
CT scan shows classic arachnoiditis ossificans where the scar tissue has
calcified.
The red dots represent the spaces occupied by the nerve roots. These nerves are being progressively
strangled by the progression of scar calcification.