using patient feedback for creating and improving innovative programs
TRANSCRIPT

Using Patient Feedback for Creating and Improving Innovative Programs
by Doris Quinn, PkD Director, Quality Education and Management Vandevbilt University Clinic Nashville, TN
There are two goals that should be of paramount concern to clinicians today. With the current emphasis on cost control in healthcare, i t has become necessary to search for ways to (a) decrease the total burden of ill- ness for costly conditions and (b) compile outcomes data to measure effec- tiveness and efficiency. This article describes an experimental work therapy program that seeks to address the needs of early-stage Alzheimer's disease and other dementia patients. Feedback from patients and caregivers was used to validate the benefits of the program activities in reducing the total burden of illness. These data also were used as a basis for improving pro- gram components. Once the program was well defined, patient and caregiv- er feedback measures were used to ensure that the program continued to meet their needs.
Introduction There is a general perception that lit-
tle can be done to relieve symptoms and improve quality of life when patients have a debilitating disease, such as Alzheimer's disease (AD). Once diag- nosed, such patients often feel alone in dealing with the depression, the anger, and the many losses associated with AD. Increasing these patients' quality of life by maximizing their re- maining abilities is a new concept. The goal of any program for AD patients should be to defer the need for total nursing care, thus reducing financial and emotional costs.
Financial impact: The financial cost of this disease in 1988 was estimated at $24-40 billion (Cook-Desan, 1988). By the year 2000, Blass (1990) forecasts to- tal costs (including indirect costs) to be more than $88 billion annually, which will make it the third most ex- pensive health condition in the Unit- ed States. Therefore, delaying institu- tionalization could have a significant impact on the families of AD patients and on society.
Adapted Work Services Program The Adapted Work Services (AWS)
program was begun in 1993 and was based on the concept of the sheltered workshop. The parent company, Rochelle Center of Nashville, TN, had a similar program for mentally retard- ed clients, and its program director thought that the concept could be used to help early-stage AD patients. He knew that these patients experienced significant, debilitating emotional prob- lems, which lead to difficult behaviors
that added significantly to the burden of their devastating illness.
Maximizing remaining skills: The director hypothesized that if AD pa- tients' many remaining skdls were max- imized, they would be able to remain productive and increase their feeling of self-worth, which would in turn de-
The goal of any program for AD patients should be to defer the need for total nursing care.
crease the stress on their families. The concept of the clients coming to "work" seemed a positive alternative to day care, especially in the disease's early stages. The director sought the input of experts on AD (including a member of the Nashville Council on Aging, a geropsychiatric nurse, a professor of psychology and human development specializing in the support of caregivers, an assistant professor of psychiatry spe- cializing in geriatrics, and a social work- er specializing in memory disorders), which resulted in the formation of an advisory group. This group was con- vinced that early-stage AD patients would benefit substantially from being in a work atmosphere in which they would be paid for performing repeti- tive but meaningful jobs. Staff would be available to support and train or re- train patients in a safe environment. The patient work group also would provide
26 JHQ . July/August 1996. VO~. 18, No. 4

a \‘enue for socialization and would Serve as a support to its members.
Determining a need for the program: Going from idea to reality requires plan- ning, but even more importantly, it re- quires data. The first task was to veri- fy that the need and desire to work existed for this patient population. Fo- cus groups were conducted to evaluate whether the needs of the key stake- holders matched the perceived needs articulated by the program developers. (The key stakeholders in this endeav- or were the patients and their caregivers, as the burden falls most heavily on care- givers as the disease progresses.) The need seemed sufficient. A proposal to the Robert Wood Johnson Foundation (RWJF) was successful; funding was granted in November 1993 for 3 years, and a new concept became a program.
Determining the program’s goals: The program began with 8 patients, who were very positive about the program. But after nearly 2 years, referrals were very sparse, and the program director was having difficulty recruiting more participants. At this juncture, I was asked to conduct a formative evaluation study of the program. The study’s in- tent was to ensure that the program was indeed meeting the needs of the target population and to provide data for the referral sources, who still seemed skep- tical of the value of AWS. I began the study by formulating the following questions: What are the goals of the pro- gram? Are they meeting the needs of the patient and caregiver? What are the program activities? Do they relate to the goals, and do they need to be improved? Is there a program theory to guide the
choice of activities? Is the theory capa- ble of linking activities to the program goals? What performance measures could be used to monitor the ongoing functioning of the program and the ef- fect of the program on the participants? How could performance measures pre- dict the likely success of a program that had never been tried before?
Using feedback data: Innovative pro- grams can have difficulty in securing additional funding if there are no data to prove their effectiveness. The diffi- culty AWS faced was that there were too few patients to conduct an impact analysis, which would have been the best way to provide this evidence. The alternative was to conduct a formative evaluation of the program; that is, to an- alyze data from program activities and assess their validity with respect to the
Figure 1. Adapted Work Services, as Originally Conceived
Outcomes Structure Process
Workload: Marketing to: Participants: Self-esteem Need for help at Rochelle Center Plan for aging clients and parents
Referral sources (physicians) Families, churches, etc. Early-stage memory loss individuals
Decreased isolation, depression, anger, and anxiety
Community need: Work contracts Use of present abilities Increasing elderly population means increasing Increased quality of life (acceptance
incidence of dementia No services for early-stage dementia
Marketing plan: Referral sources Participants Caregivers
Existing model of sheltered workshop: Rochelle and VA Personnel with experience in sheltered workshops
Other community resources to support AWS
Facility: Building/space
Transportation
4 Work therapy tasks: Simple, repetitive Meaningful Paid
Socialization/support: Identification with peers Interaction with staff
Case Manaeement/Counselinr: Support groups for participank and caregivers Counseling for legal and financial planning Link to other agencies Information about and referrals to community
resources
and dignity) . Usefulness of doing meaningful work Maintained or increased self%are
Caregivers: Long-term caregiving plan Completion of legal and financial
Respite; reduction of stress More normal lifestyle Ability to keep employment
plan
Referral sources: Option to present to families Referrals from AWS
Society: Decreased total cost, because patients
Development of a program that can live at home longer
be replicated
Business customers: Quality of work at an affordable price
JHQ 1 July/August 1996 1 VO~. 18, NO. 4.27

Patient Feedback
patients (Scheirer, 1994). Formative eval- uation relies heavily on feedback from the patient, caregivers, and staff to cre- ate an operational model of the program (a hgh-level flowchart), as well as a con- ceptual or theoretical model. These models then become blueprints for se- lecting measures that will provide data on the functioning of the program, as well as on the program’s effect on the patients and their caregivers.
Reviewing the program as original- ly conceived: We began to address the questions by first mapping out the pro- gram as it was intended to operate, us- ing a framework of structure, process, and outcome. Agency documents such as the RWJF proposal, various talks giv- en by the director, and initial meeting notes were reviewed to put together a diagram of the program as originally conceived by the advisory group (Fig- ure 1). Interviews with the staff, the di- rector, and the advisory board also were helpful in fleshing out this diagram.
Conducting interviews: The next step was to be certain that the identified out- comes or goals of the program were im- portant to the patients and the care- gvers. To obtain these data, I conducted interviews with patients. Although they sometimes had difficulty expressing themselves, the patients were articulate enough to be good sources of informa- tion. This was a significant lesson for the interviewers. Early-stage AD pa- tients are stdl capable of expressing their needs and wants, yet often we treat them as if they are totally demented. The interviews were videotaped (with the patients’ consent) so that content analysis could be done. Focus groups with caregivers also were conducted. We believed that using focus groups would allow caregivers to support one another as they discussed the difficul- ties of dealing with a loved one afflict- ed with AD. A semistructured format was used in which specific questions were asked, although the caregivers were also allowed to speak freely about certain issues important to them. A pro- fessional facilitator was used for two reasons: (a) because the facilitator was not part of the program, he could help elicit complaints as well as praises for the program, and (b) the reliability and
validity of the information were en- hanced by using a trained professional. These sessions also were videotaped.
Analyzing the data: The analysis of the focus group and interview data was accomplished using qualitative data analysis techniques (Miles & Huber- man, 1994). The focus group data and the interview data were compiled in a format that allowed codes to be assigned to various words or ideas (see Figure 2). Themes began to emerge from the data. Qualitative data analysis provided a mechanism for distilling what was im-
~~
The concept of the clients coming t o ”work” seemed a positive alternative to day care.
portant from many pages of narration. Patients’ needs that emerged were as follows: to feel productive, to contin- ue to be part of society by going to work rather than to an agency that felt like baby-sitting, and to be in a safe envi- ronment where there was no need to cover up their forgetfulness. Important themes for caregivers included issues of support and respite from constant care, and the need to have their loved one feel useful and to be prepared for transitions.
Determining response to the pro- gram: The patients’ and caregivers’ overall response to the existing program was very positive, as evidenced from their willingness to be quoted in news releases or promotional information, as well as their comments during focus groups. As a result, the program’s de- signers felt the program was indeed meeting important needs of the AD pa- tients and their caregivers. They need- ed to be sure, however, that the activi- ties the patients engaged in were appropriate. The value of some tasks appeared unclear to the staff. The ad- visory group members also had differ- ing opinions as to what tasks the work group members should perform.
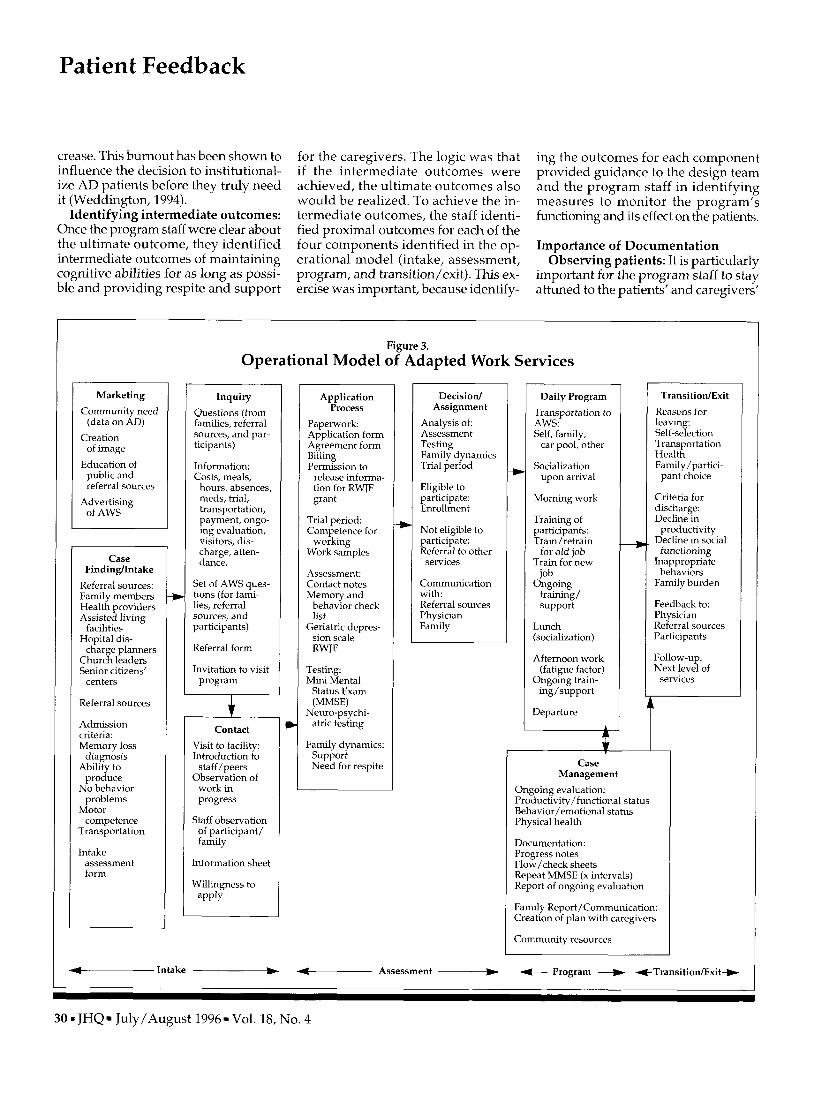
Clarifying the program: To clanfy the program, I facilitated, with staff mem-
bers’ help, the creation of a high-level flowchart, called the operational mod- el (see Figure 3 ) . Staff members were asked to identify all the activities in the program. These activities were then clustered into program components, which were identified as intake, as- sessment, program, and transition/exit. This categorization was useful in that it helped identify ”holes” in the program. Four problem areas we discovered were (a) the lack of clear definition of the pro- gram’s target population-AD patients only, or anyone with memory deficit? (b) the lack of attention to marketing and cultivating new referral sources; (c) the absence of a mechanism to system- atically collect patient and caregiver feedback; (4) the lack of a mechanism for reporting to families and private physicians about participants’ behav- ior and productivity in the program.
Identifying program theory: The next question to be addressed was the iden- tification of program theory. If we are to learn which activities cause which outcomes, it is important that a theory be made explicit. (Theory sometimes is implicit for each staff member/design- er of a program, but unless it is made explicit, it is not shared by all.) Deming often said in his seminars that “With- out theory there is no knowledge.”
The need to identify the program’s theory also was driven by the need eventually to show evidence of its ef- fectiveness. To answer the question “What in the program contributes to its success?” the program staff and I cre- ated a conceptual model (Figure 4). The patients and caregivers already had pro- vided data concerning their needs and their reaction to the program. It now was necessary to put the program into the broader context of societal need. Staff members knew that decreasing the total burden of illness was the ultimate desired outcome. This burden includes cost to families, lost wages of caregvers, the need for support or sitters, the fre- quent caregiver illnesses resulting from stress, and the eventual institutional- ization of patients. It was hypothesized that if patients can be kept productive, many of their problematic behaviors will be lessened, and the emotional burnout of caregivers will therefore de-
28 1 JHQ 1 July/August 1996 1 Vol. 18, NO. 4

Figure 2. Qualitative Data Analysis of Caregiver Focus Group Comments
Comments by Caregivers
We are bombarded with so much negativity about AD. AWS is positive. They helped me take steps to change housing.
Fee of $20-25 is low for this kind of service; it’s cheaper than other programs
My mother‘s paycheck pays costs for one week of the month
They would want to keep this program even if the cost went up.
My sister would not come if she knew I was paying a fee. My father would also resist if he knew I paid for him to come.
Mother does not understand why she has to pay to work, but since she gets confused about it, it’s ok.
Day care is equated with babysitting. They are vegetables there. The patients are too far gone
The only alternative is day care.
This is very stressful, to put it mildly
I turn to old friends in Missouri for help
I talk to other staff members when I need help.
The church has a list of people who can help, but you really feel alone.
I don’t talk to anyone. This is my cross to bear and I do it. I learned fast what I needed to do.
The social worker at the doctor’s office has also been helpful
I cannot cry to my children, because they have lives of their own.
They need to reach out to me; I cannot burden them.
We don’t talk to each other much, because we don’t get together.
Location is not a problem. The real problem is distance from home. Those close by find it great.
He was very nervous about going, because he was afraid he couldn’t do the work. He didn’t remember, but it was OK. Lately he’s been more tired and doesn’t want to go.
When Ruth was moved, she really deteriorated quickly. Major events seem to trigger fast decline.
Mother is so different now than before the program. Sometimes she did not dress at all, but now she dresses herself and makes me hurry to get her here.
There is no other program like this in the country
Code 1
AD
COST
COST
COST
COST
COST
DC
DC
FAM
FAM
FAM
FAM
FAM
FAM
FAM
FAM
FAM
LOC
PART
PART
PART
PRG
Code 2
PRG
WORK
SUP
SUP
SUP
SUP
SUP
SUP
SUP
SUP
SUP
SUP
TRP
WORK
AD
BEH
PUB
Code Summary AD Alzheimer’s disease PRG Program SUP Support COST Cost WORK Work DC Day care FAM Family LOC Location TRP Transportation PART ParticipanUpatient BEH Behavior PUB Publicity/marketing
Note: Data were sorted by Code 1.
Code 3
SUP
PRG
JHQ 1 July/August 1996. Vol. 18, NO. 4.29
Patient Feedback
crease. This burnout has been shown to influence the decision to institutional- ize AD patients before they truly need it (Weddington, 1994).
Identifying intermediate outcomes: Once the program staff were clear about the ultimate outcome, they identified intermediate outcomes of maintaining cognitive abilities for as long as possi- ble and providing respite and support
for the caregivers. The logic was that if the intermediate outcomes were achieved, the ultimate outcomes also would be realized. To achieve the in- termediate outcomes, the staff identi- fied proximal outcomes for each of the four components identified in the op- erational model (intake, assessment, program, and transition/exit). This ex- ercise was important, because identify-
ing the outcomes for each component provided guidance to the design team and the program staff in identifying measures to monitor the program’s functioning and its effect on the patients.
Importance of Documentation Observing patients: It is particularly
important for the program staff to stay attuned to the patients’ and caregivers’
Marketing Community need
(data on AD) Creation
of image Education of public and referral sources
Advertising of AWS
Case FindingIntake
Referral sources: Family members Health providers Assisted living
facilities Hopital dis-
charge planners Church leaders Senior citizens’
centers
Referral sources
Admission criteria: Memory loss
diagnosis Ability to
produce No behavior
problems Motor
competence Transportation
Intake assessment form
*
Figure 3. Operational Model of Adapted Work Services
Inquiry Questions (from families, referral sources, and par- ticipants)
Information: Costs, meals,
hours, absences, meds, trial, transportation, payment, ongo- ing evaluation, visitors, dis- charge, atten- dance.
Set of AWS ques- tions (for fami- lies, referral sources, and participants)
Referral form
Invitation to visit program
1 Contact
Visit to facility: Introduction to
staff/peers Observation of
work in progress
Staff observation of participant/ family
Information sheet
Willingness to apply
Application Process
Paperwork Application form Agreement form Billing Permission to
release informa- tion for RWJF grant
Trial period: Competence for
working Work samples
Assessment: Contact notes Memory and
behavior check list
Geriatric deores- sion scale RWJF
Testing: Mini Mental
Status Exam (MMSE)
Neuro-psychi- atric testing
Family dynamics: Support Need for respite
L
Decision/ Assignment
Analysis of Assessment Testing Family dynamics Trial period
Eligible to participate: Enrollment
Not eligible to participate: Referral to other services
Communication with: Referral sources Physician Family
Daily Program Transportation to AWS: Self, family,
car pool, other
Socialization upon arrival
Morning work
Training of participants: Traidretrain
for old job Train for new
job Ongoing
training/ support
Lunch (socialization)
Afternoon work (fatigue factor)
Ongoing train- ing/support
Departure -
TransitiodExit Reasons for leaving: Self-selection Transportation Health Family/partici- pant choice
Criteria for discharge : Decline in
productivity Decline in social functioning
Inappropriate behaviors
Family burden
Feedback to: Physician Referral sources Participants
Follow-up: Next level of
services . Case
Management Ongoing evaluation: Productivity/functional status Behavior/emotional status Physical health
Documentation: Progress notes Flow/check sheets Repeat MMSE (x intervals) Report of ongoing evaluation
Family Report/Communication: Creation of plan with caregivers
Community resources
-Intake - Assessment -+ + Program + +Transition/Exit+
30 JHQ July/August 1996 Vol. 18, No. 4

Inta
ke
Cha
ract
erist
ics
Prox
imal
out
com
es
prep
arat
ion
of ca
regi
vers
fo
r nex
t st
age
Faci
litat
ion
of c
ontin
u-
um of
car
e se
rvic
es
thro
ugh
tran
sitio
ns
Cle
arly
de
fine
d 1
prog
ram
Cle
arly
de
fine
d po
p-
Prom
pt a
nd
supp
ortiv
e at
tent
ion
ongo
ing
cont
act
1
mat
ch n
eed
to s
ervi
ces
Eas
y ac
cess
F-
Enh
ance
d cu
stom
er
satis
fact
ion
Figu
re 4
. C
once
ptua
l Mod
el o
f Ada
pted
Wor
k Se
rvic
es
Ass
essm
ent
Cha
ract
erist
ics
Prox
imal
out
com
es
Stan
dard
- A
ccur
ate
ized
pr
oced
ures
pria
te to
go
als o
f pr
ogra
m
Prog
ram
Cha
ract
erist
ics
Prox
imal
out
com
es
Wor
k co
mpo
nent
: Si
mpl
e R
epet
itive
M
eani
ngfu
l In
divi
dual
- iz
ed e
xpec
- ta
tions
Use
of
rem
aini
ng
skill
s Pr
oduc
tivity
Feel
ing
of se
lf-w
orth
Soci
aliz
atio
n co
mpo
nent
: Id
entif
icat
ion
with
pee
rs
acce
ptan
ce
by st
aff
Unc
ondi
tion-
al
acc
ep-
tanc
e O
wne
rshi
p of
prog
ram
by
par
tici-
supp
ort/
pant
s
Cas
e m
anag
emen
t:
eval
uatio
n Pr
epar
atio
n of
ca
regv
ers
for t
rans
i-
tiOnS
C
omm
unic
a-
tion
with
fa
mily
and
ca
re pr
o-
vide
rs
ongo
ing
I
Dec
reas
ed
isol
atio
n
Mai
ntai
ned
or in
crea
sed
self-
care
D
ecre
ased
ne
gativ
e em
otio
ns/
beha
vior
s
Out
com
es
Cha
ract
erist
ics
Prox
imal
out
com
es
Mai
nten
ance
of
func
tioni
ng
as lo
ng a
s po
ssib
le
Prov
isio
n of
resp
ite an
d su
ppor
t for
ca
regi
vers
Dec
reas
ed
tota
l bur
den
of i
llnes
s

Patient Feedback
perspectives. The progressive nature of AD makes assessing and using patient feedback more difficult. In the very ear- ly stages of ths disease, patients can ver- balize how they feel, what they think and what they like or do not like about the program. But as the disease pro- gresses, staff members have to get data by observing the patients. What be- haviors do patients exhibit when they arrive in the morning? How do they in- teract with other patients and with the staff? How do they function during the day? These observations are clues to things that patients may not be able to verbalize.
Training aides: Such observations, however, are not useful unless the con- text of what is happening to the patient also is documented. A social worker was available to help with documentation, but she had many duties and could not perform all the documentation. Train- ing the staff aides to take notes was im- portant for collecting good patient data. The aides are the staff members clos- est to the patients; they get to know the individual patients well.
Using documentation: Once the ob- servations are recorded and notes writ- ten about the context of the behavior, they can become feedback to the fami- lies and the referral sources. Patient feedback, whether verbal or indirect through observation, helps the staff an- ticipate and prepare caregivers for the inevitable transitions. Staff members try to meet with families when they first bring the patients to AWS. There are pe- riodic potluck suppers, which bring the staff, patients, and families together. At the present time there is no way to get regular feedback from the caregivers; this need will be addressed soon.
Summary The three models that were developed
as part of the formative evaluation helped answer the question ”Can we predict the likely success of a program that has never been tried before?” The diagram of the program as it was orig- inally conceived provided information on the desired outcomes, the process to achieve these outcomes, and the struc-
ture required. Creating a conceptual model of the program helped ensure that there was a theory behind the ac- tivities; the logic of the program was made explicit by the conceptual model. No research was available on the rela- tionship between work and AD pa- tients, but we did find concepts that could be generalized to this program. For example, work therapy has been used in programs for occupational ther- apy, mental illness, mental retardation, rehabilitation, and geriatric patients in a nursing home. The theory behind these programs seemed also to apply to this program. We also researched the effectiveness of socialization for patients with AD. Little on the subject of social- ization was found in the literature, but our own patients were very clear about its importance to them.
Conceptual model: In deciding whether the AWS program was likely to succeed, we looked at the literature and the questions posed for the forma- tive evaluation study. Both patients and caregivers provided feedback that the program was meeting most of their needs. However, the staff found that there was room for improvement. By creating a conceptual model of the log- ical progression from proximal out- comes to intermediate and to ultimate outcomes, staff members were able to ensure that activities were clearly fo- cused on the needs of the patients, care- givers, and society. The conceptual model also provided the template for identifying measures of program per- formance and more importantly, effects of the program on participants and care- givers. With measures to monitor the functioning of the program and the ef- fect on the target population, the staff are now able to show referral sources and potential funders important data about the program. The likelihood of se- curing additional funding and gaining the confidence of the professional com- munity is greatly enhanced with these data. With the models in hand, the pro- gram’s staff members have been able to show what they did, why they did it, how they knew the program was doing well (operationally and from the pa-
tients‘ perspective), and what evidence from the literature helped ensure that the program was on solid ground. The program will continue to be solid if staff members continue to keep their fingers on the ”customer pulse” and learn to adapt as needed. Flexibility is the key to succeeding, and knowing exactly what the program is meant to be will help to keep it flexible.
References Blass, J.P. (1990). The report of the advi-
sory panel on Alzheimer‘s disease, 1988- 1989. Generations, 14(2), 68-69.
Cook-Desan, R.M. (1988). Losing a million minds: Confronting the tragedy of Alzheimer’s disease and other dernentias. Philadelphia: Office of Technology As- sessment Task Force, Science Informa- tion Resource Center.
Miles, M.B., & Huberman, A.M. (1994). Qualitative data analysis. Thousand Oaks, CA: Sage Publications.
Scheirer, M.A. (1994). Designing and us- ing process evaluation. In J. Wholey, H. Hatry, & K. Newcomer (Eds.), Handbook of practical program evaluation. San Fran- cisco: Jossey-Bass Publications.
Weddington, D. (1994). Early-stage Alzheimer’s care. New York: Springer Publishing Co.
Suggested Reading Deming, W.E. (1982). Out qfthe crisis. Cam-
bridge, MA: MIT Press.
Doris Quinn is the director of quality education and management at Vanderbilt University Clinic in Nashville, TN. She is responsible for facilitating the integration of process improvement and outcomes research in the clinicS clinical practiceand op- erations. Quinn, who assisted W. Ed- wards Deming with consulting and teaching tours in the late 1980s and early 1990s, has 20 yeurs of experi- ence in thefields of management and education.
32 1 JHQ 1 July/August 1996 1 Vol. 18, NO. 4