using informatics to improve the care of patients ... · pdf filecare of patients susceptible...
TRANSCRIPT
CONTINUING EDUCATION
Using Informatics to Improve theCare of Patients Susceptible toMalignant Hyperthermia 2.3 www.aornjournal.org/content/cme
BONNIE G. DENHOLM, DNP, RN, CNOR
Continuing Education Contact Hoursindicates that continuing education (CE) contact hours are
available for this activity. Earn the CE contact hours byreading this article, reviewing the purpose/goal and objectives,and completing the online Examination and Learner Evalua-tion at http://www.aornjournal.org/content/cme. A score of 70%correct on the examination is required for credit. Participantsreceive feedback on incorrect answers. Each applicant whosuccessfully completes this program can immediately print acertificate of completion.
Event: #16511Session: #0001Fee: For current pricing, please go to http://www.aornjournal.org/content/cme.
The contact hours for this article expire April 30, 2019.Pricing is subject to change.
Purpose/GoalTo provide the learner with knowledge specific to improvingthe care of patients susceptible to malignant hyperthermia(MH) through informatics.
Objectives1. Describe how informatics improves care for patients who
are susceptible to MH.2. Discuss the literature related to MH.3. Discuss the informatics practice implications relevant to
caring for patients who are susceptible to MH.
AccreditationAORN is accredited as a provider of continuing nursingeducation by the American Nurses Credentialing Center’sCommission on Accreditation.
ApprovalsThis program meets criteria for CNOR and CRNFA recerti-fication, as well as other CE requirements.
AORN is provider-approved by theCalifornia Board ofRegisteredNursing, Provider Number CEP 13019. Check with your stateboard of nursing for acceptance of this activity for relicensure.
Conflict-of-Interest DisclosuresBonnie G. Denholm, DNP, RN, CNOR, has no declaredaffiliation that could be perceived as posing a potential conflictof interest in the publication of this article.
The behavioral objectives for this program were created by HelenStarbuck Pashley, MA, BSN, CNOR, clinical editor, withconsultation from Susan Bakewell, MS, RN-BC, director,Perioperative Education. Ms Starbuck Pashley and Ms Bakewellhave no declared affiliations that could be perceived as posingpotential conflicts of interest in the publication of this article.
Sponsorship or Commercial SupportNo sponsorship or commercial supportwas received for this article.
DisclaimerAORN recognizes these activities as CE for RNs. Thisrecognition does not imply that AORN or the AmericanNurses Credentialing Center approves or endorses productsmentioned in the activity.
http://dx.doi.org/10.1016/j.aorn.2016.02.001ª AORN, Inc, 2016
364 j AORN Journal www.aornjournal.org

Using Informatics to Improve theCare of Patients Susceptible toMalignant Hyperthermia 2.3 www.aornjournal.org/content/cme
BONNIE G. DENHOLM, DNP, RN, CNOR
ABSTRACTPerioperative nurses and nurse leaders should understand how to apply a nursing informatics frame-work and informatics concepts to strengthen data interpretation, transitions in care, and engagementwith patients susceptible to malignant hyperthermia (MH) and their family members. Patient outcomescan be improved when informatics solutions facilitate identifying risks, clinical decision making in acrisis situation, retrieving priority information during transitions of care, and involving patients inplanning care. Incorporating informatics solutions into existing quality improvement processes canhelp evaluate knowledge and preparedness related to managing care for a patient in an MH crisis.Informatics solutions can also help enhance interoperability by evaluating workflow related totransitions in care. Perioperative nurses and nurse leaders should advocate for diligence in submittingreports of MH-suspected events to databases. Improved data collection and data sharing enhanceaggregated standardized data sets, which can advance research and increase the quality of evidenceavailable with which to guide practice. AORN J 103 (April 2016) 365-376. ª AORN, Inc, 2016.http://dx.doi.org/10.1016/j.aorn.2016.02.001
Key words: malignant hyperthermia, meaningful use, interoperability, patient health records,data-to-wisdom framework.
Malignant hyperthermia (MH) occurs whengenetically susceptible individuals receive atriggering agent that causes a series of chain
reactions primarily in muscles and results in an increase inintracellular calcium ion concentration and increased energyuse in muscle tissue. The incidence of MH episodes is low;these episodes are considered low-occurrence, high-risk events.Clinicians are better prepared to recognize MH today thanthey were four decades ago, when the condition was firstidentified. Improvements in monitoring techniques (eg, cap-nography, pulse oximetry, quantification of minute ventila-tion) and screening for MH susceptibility combined with anunderstanding of pharmacologic factors have contributed to asignificant drop in mortality related to MH.1-3
Screening for MH has improved through careful preoperativeinterviews with patients and through increased awareness offamily members who have undergone caffeine-halothanecontracture testing. Having an established pharmacologicbasis for MH has allowed clinicians to avoid using triggeringagents when they identify patient susceptibility to MHand to immediately administer IV dantrolene sodium totreat an MH episode when they recognize its symptoms.Despite these improvements, patients who are identified assusceptible to MH and their family members are vulnerableto adverse events when they undergo anesthesia for aninvasive procedure.4,5 Their MH vulnerability may alsoextend to exposure to heat and exertion without pharma-cologic triggers.6,7
http://dx.doi.org/10.1016/j.aorn.2016.02.001ª AORN, Inc, 2016
www.aornjournal.org AORN Journal j 365
HEALTH INFORMATICS AND THE DATA-INFORMATION-KNOWLEDGE-WISDOMFRAMEWORKHealth informatics intersects with the care of patients who aresusceptible to MH and their family members in a numberof ways that can influence the quality of care provided.Perioperative nurses and nurse leaders should know howto apply the nursing informatics data-information-knowledge-wisdom (DIKW) framework,8 as well as informatics concepts tostrengthen data interpretation, transitions in care, and patientengagement for these patients and their family members.Ethical issues, confidentiality, and data security are alsopertinent health care informatics concepts that should beaddressed when planning care for this population; however,these concepts are beyond the scope of this discussion.
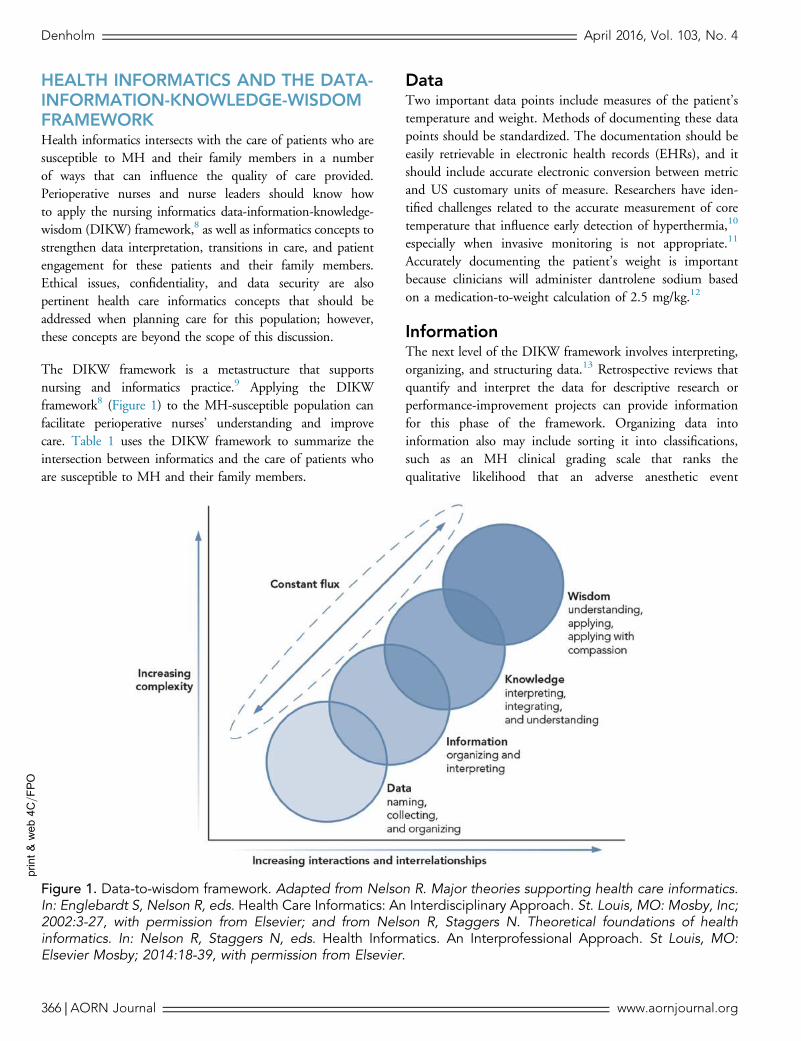
The DIKW framework is a metastructure that supportsnursing and informatics practice.9 Applying the DIKWframework8 (Figure 1) to the MH-susceptible population canfacilitate perioperative nurses’ understanding and improvecare. Table 1 uses the DIKW framework to summarize theintersection between informatics and the care of patients whoare susceptible to MH and their family members.
DataTwo important data points include measures of the patient’stemperature and weight. Methods of documenting these datapoints should be standardized. The documentation should beeasily retrievable in electronic health records (EHRs), and itshould include accurate electronic conversion between metricand US customary units of measure. Researchers have iden-tified challenges related to the accurate measurement of coretemperature that influence early detection of hyperthermia,10
especially when invasive monitoring is not appropriate.11
Accurately documenting the patient’s weight is importantbecause clinicians will administer dantrolene sodium basedon a medication-to-weight calculation of 2.5 mg/kg.12
InformationThe next level of the DIKW framework involves interpreting,organizing, and structuring data.13 Retrospective reviews thatquantify and interpret the data for descriptive research orperformance-improvement projects can provide informationfor this phase of the framework. Organizing data intoinformation also may include sorting it into classifications,such as an MH clinical grading scale that ranks thequalitative likelihood that an adverse anesthetic event
print&web4C=F
PO
Figure 1. Data-to-wisdom framework. Adapted from Nelson R. Major theories supporting health care informatics.In: Englebardt S, Nelson R, eds. Health Care Informatics: An Interdisciplinary Approach. St. Louis, MO: Mosby, Inc;2002:3-27, with permission from Elsevier; and from Nelson R, Staggers N. Theoretical foundations of healthinformatics. In: Nelson R, Staggers N, eds. Health Informatics. An Interprofessional Approach. St Louis, MO:Elsevier Mosby; 2014:18-39, with permission from Elsevier.
Denholm April 2016, Vol. 103, No. 4
366 j AORN Journal www.aornjournal.org

Table 1.Data-to-Wisdom Continuum Application to Malignant Hyperthermia (MH)
The data-information-knowledge-wisdom (DIKW) framework is used to illustrate the intersection between informatics and carefor patients and their family members who are susceptible to MH.1-4
Concept Application to MH
Data-point examples Temperature� Standardize documentation of temperature in either Celsius or Fahrenheit to facilitatethe identification of trends in temperature changes.
� Multiple electronic conversions of temperature may result in calculation errors and causeconfusion about the accuracy of the temperature, potentially delaying the recognition ofhyperthermia.
Weight� The patient’s weight should be captured in an electronic health record (EHR) and beeasily retrievable for clinicians in both metric and US customary units of measure toavoid the need to manually calculate conversions.
� Having the patient’s weight readily available in kilograms is important when caregiverssuspect that the patient is going into an MH crisis, because the dosage of dantrolenesodium to be administered is based on weight (ie, 2.5 mg/kg rapidly injected intothe IV line through a large-bore catheter).
InformationOrganization and quantification ofdata points to create “acontinuum of progressivelyincreased meaning andvalue.”1(p8)
� The nurse who works in informatics manages or presents data in a way that can beunderstood,2 which may be accomplished through performance-improvement projectsrelated to variance reports or compliance with competency validation for MH events.
� Researchers who perform retrospective reviews related to MH transform data intoinformation by grouping it and quantifying it. Organizing data may include sorting it intoclassifications, such as with an MH clinical grading scale that ranks the qualitativelikelihood that the adverse anesthetic event represents MH.3
KnowledgeThe relationship between dataand information. Patterns andrelationships between differenttypes of information arerevealed at this stage of theDIKW continuum allow nursesto determine a nursingdiagnosis and plan appropriateinterventions.1
� Patient information should be documented in the EHR to reflect changes over time andshould be organized in a way that reflects the patient’s results compared with thenorm and compared with previous readings over time to identify trends.
� The clinical presentation and interventions taken should be documented in the EHR toallow continuity of care and analysis in performance-improvement projects.
� The information collected should be reported to the North American MalignantHyperthermia Registry (NAMHR)4 to allow further quantification in a national database.
WisdomWisdom is the ability to reasonand understand and torecognize what is important.1
Ethics also is needed at thisstage of the continuum.1
� Clinical judgments and critical thinking emerge during an MH crisis when clinicians areable to apply treatment protocols based on the symptoms they are identifying.
� Ethics can be related to MH when caregivers use informatics systems to engage patientsand their family members to help them make decisions (eg, participating in the NAMHRdatabase, considering genetic or muscle-biopsy testing to gain understanding about theirspecific risks for MH).
� Web-based support systems can be accessed through the Malignant HyperthermiaAssociation of the United States as another information-management interface (eg, tomanage the posttraumatic stress that is associated with MH events).5
References1.Matney S, Brewster PJ, Sward KA, Cloyes KG, Staggers N. Philosophical approaches to the nursing informatics data-information-knowledge
-wisdom framework. ANS Adv Nurs Sci. 2011;34(1):6-18.2.American Nurses Association. Nursing Informatics: Scope and Standards of Practice. Silver Springs, MD: American Nurses Association; 2008.3. Larach M, Localio A, Allen G. A clinical grading scale to predict malignant hyperthermia susceptibility. Anesthesiology. 1994;80(4):771-779.4.The North American Malignant Hyperthermia Registry of Malignant Hyperthermia Association of the United States. http://www.mhaus.org/registry.
Accessed February 19, 2015.5.Healthcare professionals. Malignant Hyperthermia Association of the United States. http://www.mhaus.org/healthcare-professionals. Accessed
February 25, 2015.
April 2016, Vol. 103, No. 4 Informatics and Malignant Hyperthermia
www.aornjournal.org AORN Journal j 367
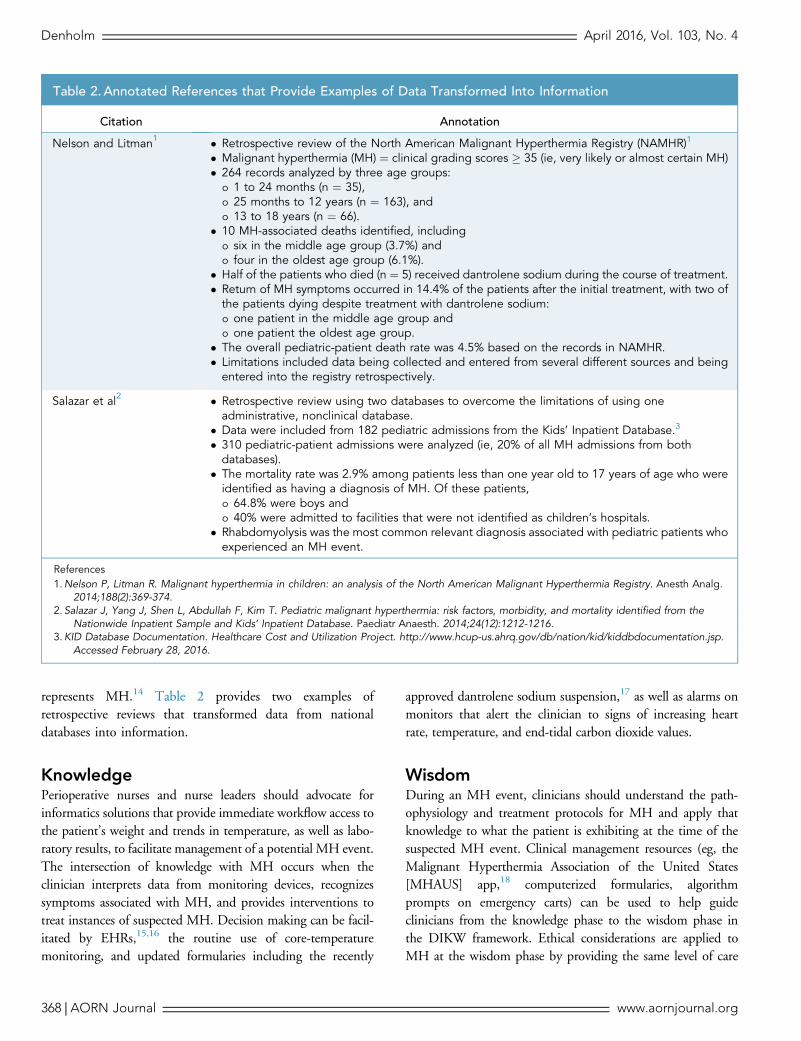
represents MH.14 Table 2 provides two examples ofretrospective reviews that transformed data from nationaldatabases into information.
KnowledgePerioperative nurses and nurse leaders should advocate forinformatics solutions that provide immediate workflow access tothe patient’s weight and trends in temperature, as well as labo-ratory results, to facilitate management of a potential MH event.The intersection of knowledge with MH occurs when theclinician interprets data from monitoring devices, recognizessymptoms associated with MH, and provides interventions totreat instances of suspected MH. Decision making can be facil-itated by EHRs,15,16 the routine use of core-temperaturemonitoring, and updated formularies including the recently
approved dantrolene sodium suspension,17 as well as alarms onmonitors that alert the clinician to signs of increasing heartrate, temperature, and end-tidal carbon dioxide values.
WisdomDuring an MH event, clinicians should understand the path-ophysiology and treatment protocols for MH and apply thatknowledge to what the patient is exhibiting at the time of thesuspected MH event. Clinical management resources (eg, theMalignant Hyperthermia Association of the United States[MHAUS] app,18 computerized formularies, algorithmprompts on emergency carts) can be used to help guideclinicians from the knowledge phase to the wisdom phase inthe DIKW framework. Ethical considerations are applied toMH at the wisdom phase by providing the same level of care
Table 2. Annotated References that Provide Examples of Data Transformed Into Information
Citation Annotation
Nelson and Litman1 � Retrospective review of the North American Malignant Hyperthermia Registry (NAMHR)1
� Malignant hyperthermia (MH) ¼ clinical grading scores � 35 (ie, very likely or almost certain MH)� 264 records analyzed by three age groups:
o 1 to 24 months (n ¼ 35),o 25 months to 12 years (n ¼ 163), ando 13 to 18 years (n ¼ 66).
� 10 MH-associated deaths identified, includingo six in the middle age group (3.7%) ando four in the oldest age group (6.1%).
� Half of the patients who died (n ¼ 5) received dantrolene sodium during the course of treatment.� Return of MH symptoms occurred in 14.4% of the patients after the initial treatment, with two ofthe patients dying despite treatment with dantrolene sodium:o one patient in the middle age group ando one patient the oldest age group.
� The overall pediatric-patient death rate was 4.5% based on the records in NAMHR.� Limitations included data being collected and entered from several different sources and beingentered into the registry retrospectively.
Salazar et al2 � Retrospective review using two databases to overcome the limitations of using oneadministrative, nonclinical database.
� Data were included from 182 pediatric admissions from the Kids’ Inpatient Database.3
� 310 pediatric-patient admissions were analyzed (ie, 20% of all MH admissions from bothdatabases).
� The mortality rate was 2.9% among patients less than one year old to 17 years of age who wereidentified as having a diagnosis of MH. Of these patients,o 64.8% were boys ando 40% were admitted to facilities that were not identified as children’s hospitals.
� Rhabdomyolysis was the most common relevant diagnosis associated with pediatric patients whoexperienced an MH event.
References1.Nelson P, Litman R. Malignant hyperthermia in children: an analysis of the North American Malignant Hyperthermia Registry. Anesth Analg.
2014;188(2):369-374.2.Salazar J, Yang J, Shen L, Abdullah F, Kim T. Pediatric malignant hyperthermia: risk factors, morbidity, and mortality identified from the
Nationwide Inpatient Sample and Kids’ Inpatient Database. Paediatr Anaesth. 2014;24(12):1212-1216.3.KID Database Documentation. Healthcare Cost and Utilization Project. http://www.hcup-us.ahrq.gov/db/nation/kid/kiddbdocumentation.jsp.
Accessed February 28, 2016.
Denholm April 2016, Vol. 103, No. 4
368 j AORN Journal www.aornjournal.org
to all patients, sharing information transparently, and obtaininginformed consent for genetic and muscle-biopsy testing.
LITERATURE REVIEWThe literature related to MH provides insight about how sta-tistics are reported from administrative databases and how theyare related to informatics on meaningful use from theperspective of interoperability and communications duringtransitions in care.Meaningful use is a term that refers to specificobjectives that eligible professionals and health care organiza-tions must achieve to qualify for Centers for Medicare &Medicaid Services Incentive Programs. It involves using EHRtechnology to improve quality, reduce health disparities, engagepatients and their families, and improve coordination whilemaintaining privacy and security for patient healthinformation.19 The author used the key words patient portalsand patient health records in the literature search, to tie in to atheme of continuity of care between patients and providerswith the intent of moving MH susceptibility to the forefrontin this population’s interactions with the health system.
Statistics Related to MHPotential challenges to confirming the statistics related to MHinclude the following realities:
� report submissions to the North American MalignantHyperthermia Registry (NAMHR)20 are voluntary;
� data extracted from the International Classification ofDiseases (ICD)21,22 codes may be flawed because of errors incoding or because the diagnosis was not linked to an anes-thetic trigger;10,23-26
� the diagnosis of MH is difficult to confirm; and� it is difficult to identify patients with MH who havedied with or without exposure to anesthetic triggers(Supplementary Table 1).
Researchers who are using administrative databases to studythe occurrence of MH events can improve specificity in theirsearches by collecting data that include the surgical procedure,anesthesia billing, and dantrolene sodium administration, inaddition to searching for the ICD, ninth revision, (ICD-9)21
and ICD, tenth revision, (ICD-10)22 coding for MHdiagnoses in hospital discharge records.27
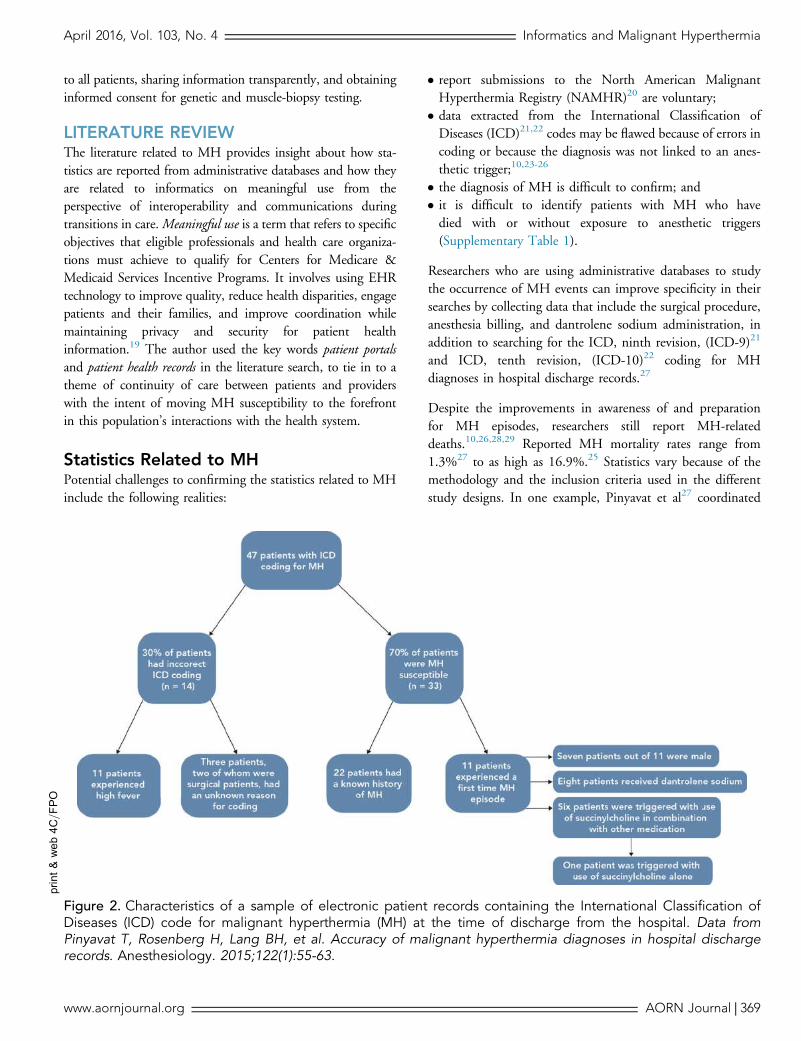
Despite the improvements in awareness of and preparationfor MH episodes, researchers still report MH-relateddeaths.10,26,28,29 Reported MH mortality rates range from1.3%27 to as high as 16.9%.25 Statistics vary because of themethodology and the inclusion criteria used in the differentstudy designs. In one example, Pinyavat et al27 coordinated
print&
web4C=FPO
Figure 2. Characteristics of a sample of electronic patient records containing the International Classification ofDiseases (ICD) code for malignant hyperthermia (MH) at the time of discharge from the hospital. Data fromPinyavat T, Rosenberg H, Lang BH, et al. Accuracy of malignant hyperthermia diagnoses in hospital dischargerecords. Anesthesiology. 2015;122(1):55-63.
April 2016, Vol. 103, No. 4 Informatics and Malignant Hyperthermia
www.aornjournal.org AORN Journal j 369

a critical review of a sample of hospitalization cases containingthe discharge diagnosis of MH (ICD-9 99.5.86 or ICD-10T88.3). Their methodology included an expert panel whosemembers reviewed electronic patient records from sixparticipating hospitals for the three-year period betweenJanuary 1, 2006, and December 31, 2008, to classify thelikelihood of MH as possible, probable, or fulminant.27 Asshown in Figure 2, 47 patients were identified using an MHdiagnosis code, 11 of whom had an incident of possible,probable, or fulminant MH, and all of whom survived todischarge (ie, 0% mortality rate).27 Researchers determinedthat the ICD code for MH is more likely to accuratelycapture the prevalence of MH susceptibility (n ¼ 22) thanMH incidence (n ¼ 11).
Meaningful UseAs a result of the Health Information Technology for Eco-nomic and Clinical Health (HITECH) Act,29 which is part ofthe American Recovery and Reinvestment Act of 2009,30
the mission of the Office of the National Coordinatorfor Health Information Technology includes “coordinatingthe development of a national health IT [informationtechnology] infrastructure and supporting and promotingmeaningful use of EHRs.”31(p20) The goal is to “create anecosystem of safer care while also producing a variety ofbenefits, such as reductions in administrative costs, improvedclinical performance, and better communication betweenpatients and caregivers.”31(p21) Nonprofit organizations havebeen established from state and local funding to improvehealth information exchange. For example, the ColoradoRegional Health Information Organization32 collaborateswith multiple sources (eg, clinicians, large and small healthcare facilities, insurance providers, laboratories, patients) toestablish secured connections for sharing clinicalinformation.33 As more health care providers use the EHRand quality-reporting systems, other forms of meaningfultechnology, such as telemedicine, may be explored further toaddress the perceived increasing burden and lack ofalignment of the current technologies.34
Technical, semantic, and process interoperability are threeconcepts that are components of the meaningful-use interop-erability initiatives associated with the EHR.35 Technicalinteroperability connects one computer to another no matterhow far apart their locations, but it does not involve themeaning of the information that is exchanged.35 Semanticinteroperability is the compatibility of the meaning ofinformation; it helps data to be exchanged betweencomputers with the “same level of understanding . . . andwithout ambiguity and error.”35(p145) The use of defined
terminologies, such as the Systematic Nomenclature ofMedicinedClinical Terms (SNOMED CT),36 is necessaryfor this to happen. Semantic interoperability is especiallyimportant when a patient is being transferred to differentlevels of care. Process interoperability relates to work processesand allows different systems (eg, payroll, staffing, schedulingmodules) to work together to reduce redundancies and errorsthat may occur in the manual documentation process.35
The EHR Incentive Program regulations19 provide therequirements to enable interoperability, data capture, datareuse, and comparative effectiveness studies. When astandardized language is used in the EHR and is mapped toa common nomenclature (eg, SNOWMED CT), researcherscan design comparative reports among multiple systems thatwill facilitate nursing research across multiple settings, aswell as quality improvement studies in one setting.37
Transitions in CareRegardless of the terminology (eg, patient hand over, handoff, transfer of care), there is general agreement that patientsare more vulnerable during transitions in care38,39 and thatpoor communication is often a factor in increasing patientvulnerability.40 The literature review revealed three studiesrelating to transitions in care that may be applied topatients who are MH-susceptible. Johnson et al41 defined acomprehensive generic set of items to be used in anelectronic format as a complement to a verbal hand over inpatient care. In contrast, Hilligoss and Zheng42 conducted atwo-year ethnographic study to evaluate hand overs fromemergency department personnel to internal medicineadmission personnel by focusing on a practice they referredto as chart biopsy, which presents an overview of the patientand preparation for the hand over and subsequent care thatdefend against potential biases. They found that EHRsfacilitated chart biopsies. They report that the chart biopsychanged the recipients of the hand over communicationinto more-active participants in the planning of carebecause the practice shaped their thinking and gave them abetter understanding of the patient. They recommend thatEHRs provide “more intelligent information-retrievalalgorithms”42(p265) so clusters of patient-care data can behighlighted to allow a better comparison of patients fromone health care encounter to the next.
The third study was a systematic review of 36 articles thatevaluated hand over tools between February 1983 and June2012.43 In this review, Abraham et al43 found a significantvariance in the quality and rigor of the articles, making itdifficult to identify a standardized strategy for hand over
Denholm April 2016, Vol. 103, No. 4
370 j AORN Journal www.aornjournal.org

tools. They also found that only five of the 36 articles (14%)reported any form of research-funding support in spite of theperceived importance of developing electronic hand overtools.43 Figure 3 provides an example of their data analysis,showing the percentage of tools that used standardizedmeasures in the various studies that met the criteria for thesystematic review.
Patient EngagementThe Nursing Alliance for Quality Care states that activelyengaging patients and their family members in a partnershipwith their health care providers is an essential component toquality improvement and reductions in medical errors andharm to patients.44 The literature review produced ninestudies with content that is relevant for enhancingcommunication, accessing data, and strengthening researchfor the vulnerable, MH-susceptible population.
Four studies45-48 describe the different types of patient access toinformation. Supplementary Table 2 illustrates examples of thetypes of access, the perceived benefits or challenges, and thelevel of participation or goals related to the patient-engagementtools. Patient health portals, EHRs, and secure e-mails aretools that patients can use to access information that ismeaningful to them; these tools also improve communicationbetween patients and health providers.45-47 Patient-poweredresearch networks, funded by the Patient-Centered OutcomesResearch Institute, are another type of patient-engagementtool. The networks are designed to encourage patients tocontribute to generating new knowledge for others who sharethe same or a similar condition. Shifting the research controlfrom traditional researchers to patients will support a shifttoward more-efficient, cost-effective clinical research that isfocused on more-practical, patient-centered questions andoutcomes.48
print&
web4C=FPO
Figure 3. Articles that included standardized measures. (A) Illustrates the percentage of electronic (standalone)versus electronic medical record (EMR)-integrated and paper-based hand over tools designed for physiciansand/or nurses. (B) Illustrates percentage of electronic (standalone), EMR-integrated, and paper-based hand overtools that used standardization measures. (C) Illustrates percentage of electronic and paper-based hand over toolsthat used outcome measures for efficiency, effectiveness, or satisfaction. Adapted from Abraham J, Kannampallil T,Patel VL. A systematic review of the literature on the evaluation of handoff tools: implications for research andpractice. J Am Med Inform Assoc. 2014;21(1):154-162 with permission from Oxford University Press.
April 2016, Vol. 103, No. 4 Informatics and Malignant Hyperthermia
www.aornjournal.org AORN Journal j 371

Three of the other five studies focus on usability and perceivedusefulness of the patient health records49 and howcommunications can empower patients50 and facilitatecollaborative decision making.51 One systematic reviewthematically grouped patient complaints into a data-drivenpatient-complaint coding taxonomy.52 One white paperpresented recommendations about using data to promotepublic awareness and accessibility rather than ownership ofdata.53 Each of these studies can serve as a resource fordeveloping informatics solutions to strengthen relationshipsbetween MH-susceptible patients, their family members, andhealth providers.
PRACTICE IMPLICATIONSSharing data, improving continuity of care, and advocating forcommunity collaboration to engage patients and their familymembers in their own care are three important concepts theauthor extracted from the literature. These concepts haveimplications for improving care for patients who are suscep-tible to MH and their family members. Perioperative nursesand nurse leaders should address these areas by advocating forchange and applying the quality improvement processesrecognized in their health care organization.
Sharing DataIn 2007, the American Medical Informatics Association Boardof Directors recommended a shift in focus from data ownershipto data sharing to allow for more aggregation and better evi-dence to guide care.53 Clinicians who are conducting researchrelated to MH are particularly interested in learning fromaggregated data collected from people who are susceptible toMH or who have muscle-related conditions and participatein genetic and muscle-biopsy testing. When informationfrom databases that collect data related to MH20,54-57 andothers related to muscular dystrophy and exertional heatstress is aggregated, researchers could gather additional insightfrom the databases. Aggregate data in which patient identitiesare removed from clinical information lose some value whenresearchers try to trace genetic links and duplicate records (B.Brandom, MD, director of the NAMHR of MHAUS,Pittsburgh, PA; telephone communication; November 18,2014). To address this issue, data in the Global Rare DiseasesPatient Registry Data Repository (GRDR) have uniqueidentifiers. When people who join the NAMHR provide theinformation needed to form the unique identifier in GRDR,the issue of duplicate records can be avoided (B. Brandom;e-mail communication; March 1, 2015). Low-quality dataand inadequately powered research methods are among thelimitations related to health information technology that have
been identified by the Institute of Medicine.31 Collaborativeefforts to facilitate aggregate-data collection and data sharingwill strengthen future research studies.
To promote data accessibility and reporting, perioperativenurses and nurse leaders should advocate for diligence insubmitting reports of suspected MH events to existing data-bases. Standardized data sets can then be aggregated to helpadvance research related to MH. Improved data collection anddata sharing will improve the quality of evidence available,which will improve the quality of care for MH-susceptiblepatients and their family members. Administrative reportsare likely to be more comprehensive and accurate when thesoftware systems promote accessibility rather than ownershipof clinical and administrative databases.
Investigating the availability of voice-activated documentationor other technologies that facilitate concurrent documentationduring an MH event also could help improve the accuracy ofdata reporting. Emergency situations are often documentedafter the event has occurred, so perioperative nurses shouldcollaborate with informatics nurse specialists to investigatenanotechnologies that exist or are being developed for con-current documentation and medication administration.13,58
Continuity of CareInteroperability between health care facilities, standardizedpatient hand overs between phases of care, and long-term coor-dination of the patient’s plan of care are all applicable to MH-susceptible patients and their family members. Interoperabilitymust be achieved for laboratory results, monitoring data, medi-cation administration, and patient preferences (eg, living will;spiritual, religious, or cultural practices), which are all importantcomponents that need to be retrievable when a patient is beingtransferred. Larach et al59 identified nine data points (Table 3)that clinicians should include in the transfer-of-care reportwhen they decide to transfer a patient in an MH crisis toanother facility or to transition the patient’s care within thesame health care facility. The data points should be consideredwhen developing or evaluating a chart biopsy approachfor communications and electronic reports. The use ofstandardized nursing languages, in addition to the standardizeddata, allows investigators to compare reports among multiplesystems and facilitates nursing research when MH events occur.
Perioperative nurses and nurse leaders should collaborate witha team of clinicians and nursing informatics specialists todetermine how information technology intersects with thecontinuity of care plan for their facility (eg, highlightingclusters of patient-care data,42 using discharge data interfaces
Denholm April 2016, Vol. 103, No. 4
372 j AORN Journal www.aornjournal.org

that already exist for higher volume or chronic conditions suchas diabetes or organ transplants, using patient portals as theybecome more sophisticated46,47) and enhance informationexchange with patients and their family members in thepreoperative and postdischarge phases of care. Toaccomplish the goals for meaningful use, perioperative nursesand nurse leaders who work in facilities with limited criticalcare resources (eg, rush-order laboratory reports, limitedstaffing) should proactively consider the level ofinteroperability existing between their facility’s EHR andthat of the receiving facility identified in the MH transferplan before an MH crisis occurs. Perioperative nurses alsoshould evaluate the standardization for patient hand overs toeffectively identify MH-susceptible patients and reportunexpected symptoms resembling those of MH. Whenperioperative nurses and nurse leaders apply an informaticsstrategy, patient outcomes are more likely to be improved,because informatics solutions facilitate the retrieval ofpriority information during transitions of care.
Community EngagementCommunity collaboration can be strengthened by setting uphealth information exchange networks. This information ex-change also benefits MH-susceptible patients who have had anevent electronically documented in one facility or database;genetic testing or muscle-biopsy information stored in anotherdatabase; and follow-up data stored at a family-practice pro-vider, specialist clinic, or private practice. Health informationexchange networks are also important in addressing local ornational barriers for information sharing when MH diagnosticcenters close; barriers are removed when the patient is able to
direct the placement of his or her own data. Neither patientsnor clinicians may have adequate awareness of how importantdata will be lost if the patient does not direct the placement ofhis or her own data (B. Brandom; e-mail communication;March 1, 2015).
Patients who are susceptible to MH and their family memberscan benefit from having access to their health information in asecure environment. The benefit is extended when the healthinformation is tailored to their health-related condition andwhen their access allows interaction with their physician,connection to additional resources related to their condition,and more control over their own health information.49 Whenpatients are empowered and the communication betweenclinician and patient is strengthened, patient involvementcan lead to higher-quality decisions that are more tailored tothe patient’s plan of care, whether the health information isdelivered by others or by the patients themselves.50
Furthermore, when physicians report events and clinicalactivities, even when there is a degree of uncertainty, theycan ensure that the best clinical evidence is available, whichis a key aspect of making quality decisions.51
Actions that can be taken to enhance community engagementalso relate to sharing information across platforms and pro-viders. For example, the surgeon is the referring professionalfor surgery, so the preoperative assessment performed by thesurgeon should integrate the high-risk factors that are high-lighted through an interface with the patient’s family-practiceor internal-medicine provider. If the patient has a health portalintegrated with a primary care health record, the surgeon couldaccess the patient’s information (eg, genetic or muscle-biopsy
Table 3. Standardized Data Points for Transfer-of-Care Reports for Patients in a Malignant Hyperthermia (MH)Crisis1,2
Nine data points to include in the transfer-of-care report whena patient in MH crisis is transferred to another facility are
� cardiovascular signs;� temperature measurement and site used;� minute ventilation with end-tidal CO2 value;� electrolytes when available;� IV site location;� medications administered, including the amount of dantrolenesodium administered and the patient’s response;
� presence or absence of muscle rigidity;� presence of urinary catheter; and� the color of the patient’s urine.
These data points can also be included in a patient handover reportwhen the transfer occurs interdepartmentallywithin a health care facility and can be considered whendeveloping or evaluating a chart biopsy approach forcommunications and electronic reports.
References1. Larach MG, Dirksen SH, Belani KG, et al. Special article: creation of a guide for the transfer of care of the malignant hyperthermia patient from
ambulatory surgery centers to receiving hospital facilities. Anesth Analg. 2012;114(1):94-100.2.The North American Malignant Hyperthermia Registry of Malignant Hyperthermia Association of the United States. http://www.mhaus.org/registry.
Accessed February 19, 2015.
April 2016, Vol. 103, No. 4 Informatics and Malignant Hyperthermia
www.aornjournal.org AORN Journal j 373

testing results, anxiety about anesthetics) and incorporaterelevant details into his or her preoperative assessment. Thisassessment information in the surgeon’s records should beavailable to anesthesia professionals and nursing personnelwho are performing preoperative assessments as well. This typeof seamless workflow for intake evaluations can help toimprove the care of patients who are susceptible to MH andreduce the level of anxiety among their family members.
CONCLUSIONMalignant hyperthermia is a low-occurrence, high-risk eventwhose care requires coordination of care providers and accessto pertinent patient information. The use of informatics canhelp collect and interpret data and provide guidance for clin-ical care that offers patients who are susceptible to MH andtheir family members the best care and the most favorableoutcomes when the patients undergo procedures that involvethe use of triggering agents.
Being prepared to make clinical decisions in a crisis situationcan improve the quality of care in health care organizations.Perioperative nurses and nurse leaders should collaboratewith educators, informatics nurse specialists, and clinicians whowork in areas where triggering agents are administeredto evaluate the knowledge and preparedness for managingthe care of a patient who is experiencing a high-risk MH event.Perioperative nurses and nurse leaders also should considerthe availability of clinical management resources, the level ofpreparedness across departments where personnel use triggeringagents, and the level of transparency when sharing informationafter an event occurs. Nurses can play a leading role in advo-cating for data-collection methods, identifying pertinent infor-mation to enhance continuity in care, and facilitatinginformatics solutions to improve direct patient care.�SUPPLEMENTARY DATAThe supplementary tables associated with this article can befound in the online version at http://dx.doi.org/10.1016/j.aorn.2016.02.001.
Acknowledgments: The author acknowledges Barbara W.Brandom, MD, director of North American MalignantHyperthermia Registry of Malignant Hyperthermia Association ofthe United States, Pittsburgh, PA; Sharon Giarrizzo Wilson, MS,RN-BC, CNOR, president, SymQuality Consulting, LLC, Parker,CO, PhD student, Loyola University, Chicago, IL; Rodney Hicks,PhD, APRN, FAANP, FAAN, professor, doctor of nursing pro-gram, Western University of Health Sciences, Pomona, CA; andLisa Spruce, DNP, RN, CNS-CP, ACNP, ACNS, CNOR,FAAN, director of research and evidence-based practice, AORN,
Inc, Denver, CO, for their assistance with document review andKathi Agnes, MSN, RN, CNOR, division clinical analyst, HCAcontinental division office, Denver, CO, for her consultation onnursing informatics.
Editor’s note: The Systematic Nomenclature of MedicinedClinical Terms (SNOMED CT) is a registered trademark ofthe International Health Terminology Standards DevelopmentOrganisation in Copenhagen, Denmark.
References1. Hirshey Dirksen SJ, Larach MG, Rosenberg H. Special article:
future directions in malignant hyperthermia research and patientcare. Anesth Analg. 2011;113(5):1108-1119.
2. Hopkins PM. Malignant hyperthermia: advances in clinical man-agement and diagnosis. Br J Anaesth. 2000;85(1):118-128.
3. Rosenberg H, Davis M, James D, Pollock N, Stowell K. Malignanthyperthermia. Orphanet J Rare Dis. 2007;2:21.
4. Brandom BW, Callahan P, Micalizzi DA. What happens whenthings go wrong? Paediatr Anaesth. 2011;21(7):730-736.
5. Riazi S, Larach MG, Hu C, Wijeysundera D, Massey C, Kraeva N.Malignant hyperthermia in Canada: characteristics of indexanesthetic in 129 malignant hyperthermia susceptible probands.Anesth Analg. 2014;118(2):381-387.
6. Brandom B, Muldoon S. Unexpected MH deaths without exposureto inhalation anesthetics in pediatric patients. Paediatr Anaesth.2013;23(9):851-854.
7. Lavezzi WA, Capacchione JF, Muldoon SM. Case report: death inthe emergency department: an unrecognized awake malignanthyperthermia-like reaction in a six-year-old. Anesth Analg. 2013;116(2):420-423.
8. Nelson R. Major theories supporting health care informatics. In:Englebardt S, Nelson R, eds. Health Care Informatics: AnInterdisciplinary Approach. St. Louis, MO: Mosby, Inc; 2002:3-27.
9. Matney S, Brewster PJ, Sward KA, Cloyes KG, StaggersN. Philosophicalapproaches to the nursing informatics data-information-knowledge-wisdom framework. ANS Adv Nurs Sci. 2011;34(1):6-18.
10. LarachMG, BrandomBW, Allen GC, Groner GA, Lehman EB.Malignanthyperthermia deaths related to inadequate temperature monitoring,2007-2012: a report from theNorth AmericanMalignant HyperthermiaRegistry of the Malignant Hyperthermia Association of the UnitedStates. Anesth Analg. 2014;119(6):1359-1366.
11. Hooper VD, Andrews JO. Accuracy of noninvasive core tempera-ture measurement in acutely ill adults: the state of the science.Biol Res Nurs. 2006;8(1):24-34.
12. FAQs: dantrolene. Malignant Hyperthermia Association of theUnited States. http://www.mhaus.org/faqs/dantrolene. AccessedFebruary 19, 2015.
13. Nursing Informatics: Scope and Standards of Practice. SilverSpring, MD: American Nurses Association; 2008.
14. Larach M, Localio A, Allen G, et al. A clinical grading scale topredict malignant hyperthermia susceptibility. Anesthesiology.1994;80(4):771-779.
15. Cipriano PF. The future of nursing and health IT: the quality elixir.Nurs Econ. 2011;29(5):286-289.
Denholm April 2016, Vol. 103, No. 4
374 j AORN Journal www.aornjournal.org

16. Murphy J. Nursing informatics: the intersection of nursing, com-puter, and information sciences. Nurs Econ. 2010;28(3):204-207.
17. New drug application approval. Ryanodex. Department of Healthand Human Services, US Food and Drug Administration. http://www.ryanodex.com/wp-content/uploads/2014/08/ryanodex-fda-approval-letter.pdf. Accessed January 4, 2016.
18. The MH App. Malignant Hyperthermia Association of the UnitedStates. http://www.mhaus.org/healthcare-professionals/managing-a-crisis/iphone-app. Accessed February 19, 2015.
19. EHR incentives & certification: Meaningful use definition & objectives.HealthIT.gov. https://www.healthit.gov/providers-professionals/meaningful-use-definition-objectives. Accessed February 28, 2016.
20. The North American Malignant Hyperthermia Registry of MalignantHyperthermia Association of the United States. http://www.mhaus.org/registry. Accessed February 19, 2015.
21. World Health Organization. International Classification of Diseases,9th revision (ICD-9). Geneva, Switzerland: World HealthOrganization; 1977.
22. World Health Organization. International Classification of Diseases,10th revision (ICD-10). Geneva, Switzerland: World HealthOrganization; 1992.
23. Larach MG, Brandom BW, Allen GC, Gronert GA, Lehman EB.Administrative databases: are they useful for clinical analyses?[Comment on: Rosero EB, Adesanya AO, Timaran CH, Joshi GP.Trends and outcomes of malignant hyperthermia in the UnitedStates, 2000 to 2005. Anesthesiology. 2009;110(1):89-94.].Anesthesiology. 2009;111(2):450. author reply 450-451.
24. Memtsoudis SG. Limitations associated with the analysis ofdata from administrative databases [Comment on: Rosero EB,Adesanya AO, Timaran CH, Joshi GP. Trends and outcomes ofmalignant hyperthermia in the United States, 2000 to 2005.Anesthesiology. 2009;110(1):89-94.]. Anesthesiology. 2009;111(2):449. author reply 450-451.
25. Rosero EB, Adesanya AO, Timaran CH, Joshi GP. Trends andoutcomes of malignant hyperthermia in the United States, 2000 to2005. Anesthesiology. 2009;110(1):89-94.
26. Rosero EB, Adesanya AO, Timaran CH, Joshi GP. In reply toAdministrative databases: are they useful for clinical analyses?[Author response]. Anesthesiology. 2009;111(2):450-451.
27. Pinyavat T, Rosenberg H, Lang BH, et al. Accuracy of malignanthyperthermia diagnoses in hospital discharge records.Anesthesiology.2015;122(1):55-63.
28. Larach MG, Brandom BW, Allen GC, Gronert GA, Lehman EB.Cardiac arrests and deaths associated with malignant hyperther-mia in North America from 1987 to 2006: a report from the NorthAmerican Malignant Hyperthermia Registry of the MalignantHyperthermia Association of the United States. Anesthesiology.2008;108(4):603-611.
29. Health IT legislation and regulations: health IT legislation. HealthIT.gov.http://healthit.gov/policy-researchers-implementers/health-it-legislation.Accessed February 19, 2015.
30. Get the facts about electronic health records: advancing America’shealth care. The Office of the National Coordinator for HealthInformation Technology. http://www.healthit.gov/sites/default/files/pdf/fact-sheets/ehrs-advancing-americas-health-care.pdf. Acces-sed February 19, 2015.
31. Institute of Medicine. Health IT and Patient Safety: Building SaferSystems for Better Care. Washington, DC: National AcademiesPress; 2012.
32. Colorado Regional Health Information Organization. http://www.corhio.org/. Accessed February 19, 2015.
33. Colorado Regional Health Information Organization. Children’sHospital Colorado expands health information exchange networkby connecting to CORHIO: tens of thousands of children acrossColorado will receive better coordinated care after hospital visitsand medical tests [news release]. New York, NY: PR Newswire;December 13, 2012. http://www.prnewswire.com/news-releases/childrens-hospital-colorado-expands-health-information-exchange-network-by-connecting-to-corhio-183341301.html. AccessedFebruary 19, 2015.
34. Murphy K. Is telemedicine more meaningful than meaningfuluse? AMA maintains that telemedicine could be the answer to a lackof alignment of meaningful use, PQRS, and VBM responsiblefor increasing burdens on providers. EHR Intelligence. http://ehrintelligence.com/2014/11/12/telemedicine-meaningful-meaningful-use/. Published November 12, 2014. Accessed February 19, 2015.
35. Maxwell Downing D. The meaning of electronic health record inter-operability [Clinical Issues]. AORN Journal. 2013;97(1):145-147.
36. Unified Medical Language System (UMLS): SNOMED ClinicalTerms (SNOMED CT). National Institutes of Health, US NationalLibrary of Medicine. http://www.nlm.nih.gov/research/umls/Snomed/snomed_main.html. Accessed February 19, 2015.
37. Baker JD. “Meaningful use”: a call to action [Editorial]. AORN J.2013;97(6):607-609.
38. Meleis A, Sawyer L, Im E, Messias D, Schumacher K. Experiencingtransitions: an emerging middle-range theory. ANS Adv Nurs Sci.2000;23(1):12-28.
39. Uhrenfeldt L, Aagaard H, Hall EOC, Fegran L, LudvigsenMS,Meyer G.A qualitative meta-synthesis of patients’ experiences of intra- andinter-hospital transitions. J Adv Nurs. 2013;69(8):1678-1690.
40. Greenberg CC, Regenbogen SE, Studdert DM, et al. Patterns ofcommunication breakdowns resulting in injury to surgical patients.J Am Coll Surg. 2007;204(4):533-540.
41. Johnson M, Jefferies D, Nicholls D. Developing a minimum data setfor electronic nursing handover. J Clin Nurs. 2011;21(3-4):331-343.
42. Hilligoss B, Zheng K. Chart biopsy: an emerging medical practiceenabled by electronic health records and its impacts on emergencydepartment-inpatient admission handoffs. J Am Med InformAssoc. 2013;20(2):260-267.
43. Abraham J, Kannampallil T, Patel VL. A systematic review of theliterature on the evaluation of handoff tools: implications for researchand practice. J Am Med Inform Assoc. 2014;21(1):154-162.
44. Sofaer S, Schumann MJ. Fostering successful patient andfamily engagement: nursing’s critical role. A white paper from theNursing Alliance for Quality Care. http://www.naqc.org/Main/Resources/Publications/March2013-FosteringSuccessfulPatientFamilyEngagement.pdf. Published March 25, 2013. AccessedFebruary 19, 2015.
45. Woods SS, Schwartz E, Tuepker A, et al. Patient experiences withfull electronic access to health records and clinical notes throughthe My HealtheVet Personal Health Record Pilot: qualitative study.J Med Internet Res. 2013;15(3):182-191.
April 2016, Vol. 103, No. 4 Informatics and Malignant Hyperthermia
www.aornjournal.org AORN Journal j 375
46. Aultman JM,Dean E. Beyond privacy: benefits and burdens of e-healthtechnologies in primary care. J Clin Ethics. 2014;25(1):50-64.
47. Crotty BH, Tamrat Y, Mostaghimi A, Safran C, Landon BE. Patient-to-physician messaging: volume nearly tripled as morepatients joined system, but per capita rate plateaued. Health Aff(Millwood). 2014;33(10):1817-1822.
48. Fleurence RL, Beal AC, Sheridan SE, Johnson LB, Selby JV.Patient-powered research networks aim to improve patient care andhealth research. Health Aff (Millwood). 2014;33(7):1212-1219.
49. Ant Ozok A, Wu H, Garrido M, Pronovost PJ, Gurses AP. Usabilityand perceived usefulness of personal health records for pre-ventive health care: a case study focusing on patients’ andprimary care providers’ perspectives. Appl Ergon. 2014;45(3):613-628.
50. Street RJ, Makoul G, Arora N, Epstein R. How does communicationheal? Pathways linking clinician-patient communication to healthoutcomes. Patient Educ Couns. 2009;74(3):295-301.
51. Politi MC, Street RL. The importance of communication in collab-orative decision making: facilitating shared mind and the manage-ment of uncertainty. J Eval Clin Pract. 2011;17(4):579-584.
52. Reader TW, Gillespie A, Roberts J. Patient complaints in health-care systems: a systematic review and coding taxonomy. BMJQual Saf. 2014;23(8):678-689.
53. Safran C, Bloomrosen M, Hammond W, et al. Toward a nationalframework for the secondary use of health data: an AmericanMedical Informatics Association white paper. J Am Med InformAssoc. 2007;14(1):1-9.
54. National Anesthesia Clinical Outcomes Registry. AnesthesiaQuality Institute. https://www.aqihq.org/introduction-to-nacor.aspx.Accessed February 19, 2015.
55. RYR-1 Foundation. http://www.ryr1.org/. Accessed February 19,2015.
56. Global Rare Diseases Patient Registry Data Repository/GRDR.National Institutes of Health, National Center for AdvancingTranslational Sciences. http://rarediseases.info.nih.gov/research/pages/43/global-rare-disease-patient-registry-and-data-repository.Accessed February 19, 2015.
57. Rubinstein YR, Groft SC, Bartek R, et al. Creating a global raredisease patient registry linked to a rare diseases biorepositorydatabase: Rare Disease-HUB (RD-HUB). Contemp Clin Trials.2010;31(5):394-404.
58. McGonigle D, Mastrian KG. Nursing Informatics and theFoundation of Knowledge. 3rd ed. Burlington, MA: Jones & BartlettLearning; 2015.
59. Larach MG, Dirksen SH, Belani KG, et al; Society for AmbulatoryAnesthesiology; Malignant Hyperthermia Association of the UnitedStates; Ambulatory Surgery Foundation; Society for AcademicEmergency Medicine; National Association of Emergency MedicalTechnicians. Special article: creation of a guide for the transfer of careof the malignant hyperthermia patient from ambulatory surgerycenters to receiving hospital facilities. Anesth Analg. 2012;114(1):94-100.
Bonnie G. Denholm, DNP, RN, CNOR, is a programmanager at Pfiedler Enterprises, Aurora, CO. Dr Denholmhas no declared affiliation that could be perceived asposing a potential conflict of interest in the publication ofthis article.
Denholm April 2016, Vol. 103, No. 4
376 j AORN Journal www.aornjournal.org

EXAMINATION
Continuing Education:Using Informatics to Improve theCare of Patients Susceptible toMalignant Hyperthermia 2.3 www.aornjournal.org/content/cme
PURPOSE/GOALTo provide the learner with knowledge specific to improving the care of patients susceptible tomalignant hyperthermia (MH) through informatics.
OBJECTIVES1. Describe how informatics improves care for patients who are susceptible to MH.2. Discuss the literature related to MH.3. Discuss the informatics practice implications relevant to caring for patients who are susceptible to MH.
The Examination and Learner Evaluation are printed here for your convenience. To receivecontinuing education credit, you must complete the online Examination and Learner Evaluationat http://www.aornjournal.org/content/cme.
QUESTIONS1. The data-information-knowledge-wisdom (DIKW)
framework is a metastructure that supportsa. information technologists’ work.b. nursing educators.c. nursing and informatics practice.d. researchers.
2. Two important data points in informatics informationinclude measuring the patient’s temperature and weight.a. true b. false
3. Informatics solutions that facilitate management of a potentialMH event include immediate workflow access to the patient’s1. weight.2. trends in temperature.3. laboratory test results.
a. 1 and 2 b. 1 and 3c. 2 and 3 d. 1, 2, and 3
4. According to researchers, challenges in confirming sta-tistics related to MH include
1. that report submissions to the North AmericanMalignant Hyperthermia Registry (NAMHR) arevoluntary.
2. errors in coding from the International Classificationof Diseases, ninth revision (ICD-9).
3. difficulty confirming the diagnosis of MH.
4. difficulty identifying patients with MH who havedied with and without exposure to anesthetic triggers.a. 1 and 3 b. 2 and 4c. 1, 2, and 4 d. 1, 2, 3, and 4
5. Research studies report MH mortality rates that rangefrom ____ to as high as ____.a. 1.3%, 16.9% b. 1.4%, 15.1%c. 2.5%, 17.9% d. 3.1%, 9.6%
www.aornjournal.org AORN Journal j 377

6. Researchers using chart biopsy to investigate transfer-of-care communication techniques found that chart biopsy1. presents an overview of the patient.2. presents preparation for hand over and subsequent
care.3. defends against potential biases.4. changes the recipients of the hand over communica-
tion into more-active participants.5. shapes care providers’ thinking and gives them a
better understanding of the patient.6. could be improved by providing more-intelligent
algorithms.a. 1, 3, and 5 b. 2, 4, and 6c. 2, 3, 5, and 6 d. 1, 2, 3, 4, 5, and 6
7. Tools that patients can use to access information that ismeaningful to them and to improve communicationsbetween patients and health providers include1. patient health portals.2. electronic health records (EHRs).3. secure e-mails.4. telephone calls with providers.5. telemedicine.
a. 4 and 5 b. 1, 2, and 3c. 1, 2, 3, and 4 d. 1, 2, 3, 4, and 5
8. The American Medical Informatics Association Board ofDirectors recommended a shift in focus from ______to _____ to allow for more aggregation and betterevidence to guide care.a. data ownership, data sharing.b. data collection, data evaluation.c. data research, data benchmarks.d. data ownership, data copyrighting.
9. When a patient is being transferred to another facility, itis important to ensure the interoperability of certaincomponents that need to be retrieved, including1. laboratory results.2. monitoring data.3. medication administration.4. patient preferences.5. care-provider data.
a. 4 and 5 b. 1, 2, and 3c. 1, 2, 3, and 4 d. 1, 2, 3, 4, and 5
10. Electronic documentation of MH events, test or biopsyinformation, and follow-up data can benefit patientswhen this information is collected in community healthinformation exchange networks.a. true b. false
Denholm April 2016, Vol. 103, No. 4
378 j AORN Journal www.aornjournal.org

LEARNER EVALUATION
Continuing Education:Using Informatics to Improve theCare of Patients Susceptible toMalignant Hyperthermia 2.3 www.aornjournal.org/content/cme
This evaluation is used to determine the extent towhich this continuing education programmet yourlearning needs. The evaluation is printed here for
your convenience. To receive continuing education credit, youmust complete the online Examination and Learner Evaluationat http://www.aornjournal.org/content/cme. Rate the items asdescribed below.
OBJECTIVESTo what extent were the following objectives of this continuingeducation program achieved?1. Describe how informatics improves care for patients who
are susceptible to MH.Low 1. 2. 3. 4. 5. High
2. Discuss the literature related to MH.Low 1. 2. 3. 4. 5. High
3. Discuss the informatics practice implications relevant tocaring for patients who are susceptible to MH.Low 1. 2. 3. 4. 5. High
CONTENT4. To what extent did this article increase your knowledge
of the subject matter?Low 1. 2. 3. 4. 5. High
5. To what extent were your individual objectives met?Low 1. 2. 3. 4. 5. High
6. Will you be able to use the information from this articlein your work setting?1. Yes 2. No
7. Will you change your practice as a result of reading thisarticle? (If yes, answer question #7A. If no, answerquestion #7B.)
7A. How will you change your practice? (Select all thatapply)1. I will provide education to my team regarding why
change is needed.2. I will work with management to change/implement
a policy and procedure.3. I will plan an informational meeting with physicians
to seek their input and acceptance of the need forchange.
4. I will implement change and evaluate the effect ofthe change at regular intervals until the change isincorporated as best practice.
5. Other: __________________________________
7B. If you will not change your practice as a result ofreading this article, why? (Select all that apply)1. The content of the article is not relevant to my
practice.2. I do not have enough time to teach others about the
purpose of the needed change.3. I do not have management support to make a
change.4. Other: __________________________________
8. Our accrediting body requires that we verify the timeyou needed to complete the 2.3 continuing educationcontact hour (138-minute) program: ______________
www.aornjournal.org AORN Journal j 379

Supplementary Table 1. Examples of Limitations When Determining Statistics Related to Malignant Hyperthermia
Citation Annotation
Larach et al1 � Retrospective review of adverse metabolic/muscular reaction to anesthesia (AMRA) reports that hadbeen voluntarily submitted to the North American Malignant Hyperthermia Registry (NAMHR)2 fromJanuary 1, 2007, through December 31, 2012.
� Researchers identified 84 patients with malignant hyperthermia (MH), includingo seven patients who died after cardiac arrests (8.3%) during the initial MH event ando eight patients who died (9.5%) before discharge from the health care facility. In four of these eightpatients (50%), the triggering anesthetics were administered in free-standing surgical facilities.
� A primary finding was the significance of monitoring temperature: 30% of the patients who died froman MH event did not have their temperature monitored. In addition,o four of 19 patients died when care providers monitored only their skin temperature, compared witho one patient of 46 who died when care providers monitored core temperature.
� Limitations of the study includedo incomplete patient data;o “potentially biased reports inherent of a fragmented medical system”;1(p1365) ando the dependence of NAMHR on voluntary reporting of an infrequent event that may result inunderreporting and often results in a small number of incidences, which reduces the power of the study.
Rosero et al3 � Retrospective reviewofdata from theNationwide Inpatient Sample (NIS)4 to evaluate the incidenceofMHfrom 2000 to 2005 and identify predictors associated with in-hospital mortality in the United States.
� Researchers identified patients who were discharged with a diagnosis of MH based on theInternational Classification of Diseases, ninth revision (ICD-9),5 and they found thato the number of patients with MH increased from 372 to 521 per year ando the in-hospital mortality from MH increased to 11.7%.3
� As these rates were higher than those found in previous reports, other research experts expressedconcern that an administrative, nonclinical database can be a serious limitation that can skew theanalysis of clinical data.6,7
� Limitations discussed in the study3 includeo the inability to confirm the diagnosis of MH with a documented in vitro muscle test or MH clinicalgrading scale score;
o the inability to identify the number of patients who were exposed to MH-triggering agents becauseof the nature of the NIS data set;
o a minimal chance that MH cases that were identified in the study were counted multiple times, asnoted from the concerns expressed by commentary;8 and
o the potential that erroneous coding could be a major source of bias in studies that extract data fromadministrative databases.
� When citing the Rosero et al3 study for future studies or reviews, researchers should be aware of thetwo commentaries associated with the study6,7 and be sure to acknowledge the limitations of usingadministrative databases when comparing the incidence and mortality rates of MH.
References1. Larach M, Brandom B, Allen G, Gronert G, Lehman E. Malignant hyperthermia deaths related to inadequate temperature monitoring, 2007-
2012: North American Malignant Hyperthermia Registry of the Malignant Hyperthermia Association of the United States. Anesth Analg.2014;119(6):1359-1366.
2.The North AmericanMalignant Hyperthermia Registry of Malignant Hyperthermia Association of the United States. http://www.mhaus.org/registry.Accessed February 19, 2015.
3.Rosero EB, Adesanya AO, Timaran CH, Joshi GP. Trends and outcomes of malignant hyperthermia in the United States, 2000 to 2005.Anesthesiology. 2009;110(1):89-94.
4.Overview of the National (Nationwide) Inpatient Sample (NIS). Healthcare Cost and Utilization Project. https://www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed February 28, 2016.
5.World Health Organization. International Classification of Diseases, 9th revision (ICD-9). Geneva, Switzerland: World Health Organization, 1977.6. Larach MG, Brandom BW, Allen GC, Gronert GA, Lehman EB. Administrative databases: are they useful for clinical analyses? [Comment on:
Rosero EB, Adesanya AO, Timaran CH, Joshi GP. Trends and outcomes of malignant hyperthermia in the United States, 2000 to 2005.Anesthesiology. 2009;110(1):89-94.] Anesthesiology. 2009;111(2):450; author reply 450-451.
7.MemtsoudisSG. Limitationsassociatedwith theanalysisof data fromadministrativedatabases. [Commenton:RoseroEB,AdesanyaAO,TimaranCH,JoshiGP.Trendsandoutcomesofmalignant hyperthermia in theUnitedStates, 2000 to2005.Anesthesiology. 2009;110(1):89-94.]Anesthesiology.2009;111(2):449; author reply 450-451.
8.Rosero EB, Adesanya AO, Timaran CH, Joshi GP. In reply to Administrative databases: are they useful for clinical analyses? [Author response].Anesthesiology. 2009;111(2):450-451.
Denholm April 2016, Vol. 103, No. 4
379.e1 j AORN Journal www.aornjournal.org

Supplementary Table 2. Examples of Studies That Describe Types of Patient Access, Benefits or Level ofParticipation, and Challenges Related to Patient Engagement
Study or ProjectDescription of Project
or Study Summary of Discussions
Woods et al1 � Qualitative study withpurposeful sampling
� Recruitment letterswere sent to 126eligible patients. 45patients and two familydelegates responded,40 of whom expressedinterest in participatingin the study.
� Focus groups involvedpatients (n ¼ 30) andfamily members (n ¼ 6)who accessed theirhealth informationthrough the MyHealtheVet Pilotprogram.
Type of patient access� Patient health portal allowed patients access to complete healthrecords, including provider notes, discharge summaries, and laboratoryand imaging results. Secure e-mail communication with providers wasnot available in the initial prototype.
Perceived benefits for patients� Enhanced communications with providers
� Improved knowledge and self-care
� Increased participation in decision making
Perceived challenges for patients� Increased stress and worry from health-record transparency and opensharing of notes and test results
� Frustration with technical problems
Recommendations for improvement� Sharing all clinical notes with patients and their family delegates couldserve as a fundamental component of the meaningful use of electronicrecords and health information exchange.
� New skills are needed to achieve shared care planning and decisionmaking.
Aultman et al2 � Mixed-methods studyusing quantitative andqualitative data toidentify benefits of e-health technologiesand to describeunderlying ethical andpragmatic burdens
� Distributed survey tocollect quantitativedata on demographicsand level of satisfactionusing e-healthtechnologies based ona 5-point Likert scale
� Conducted seven focusgroups of primary careprofessionals (n ¼ 41)from five hospitals inOhio
Type of patient access� Defined e-health technologies as a range of services and systems inhealth care technology, medical and health care records, telemedicine,videoconferencing, patient management, and scheduling systems
Perceived benefits for primary health care professionals (HCPs)� Improved patient safety as a result of medication alert
� Improved accessibility and legibility over those of paper records
� Improved delivery of care
� More-comprehensive care
Perceived challenges for primary HCPs� Obstacles in training and support and burdensome systems in whichHCPs felt forced to use templates or defer to default settings rather thanuse critical thinking or that required them to sift through too muchinformation to get to what they needed
� Information security and the threat of hackers was expressed as a social-justice issue (eg, lower-income families may not have access to high-priced security features).
(continued)
April 2016, Vol. 103, No. 4 Informatics and Malignant Hyperthermia
www.aornjournal.org AORN Journal j 379.e2
Supplementary Table 2. (continued)
Study or ProjectDescription of Project
or Study Summary of Discussions
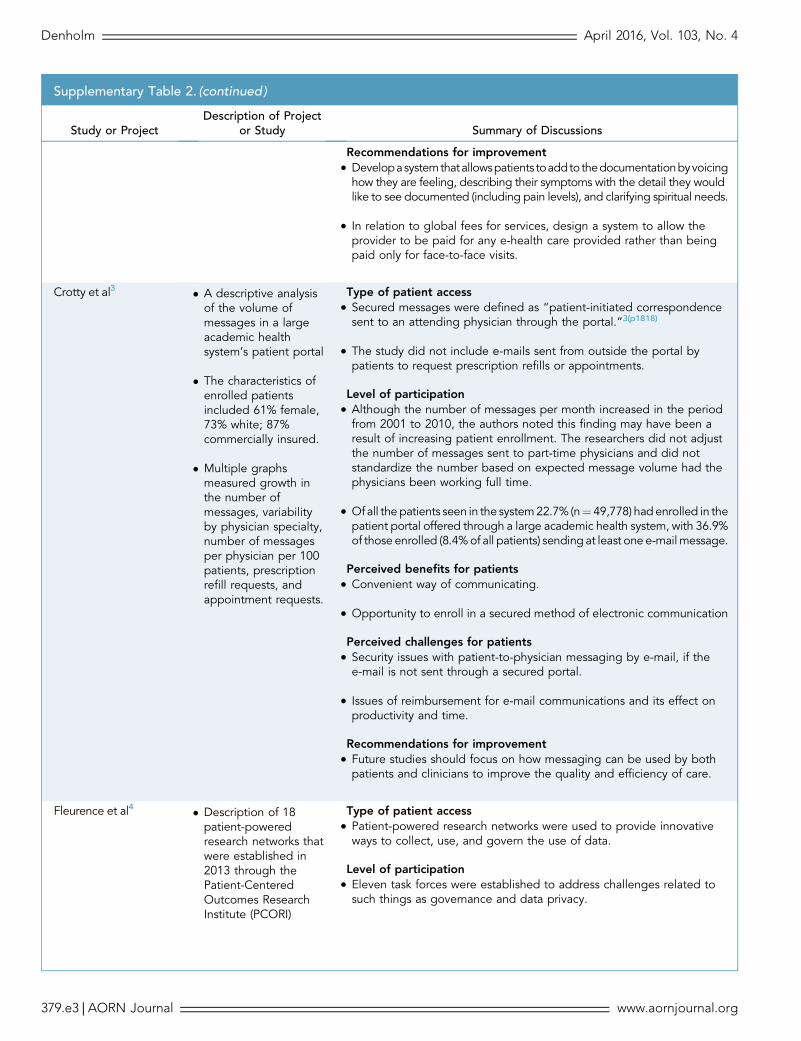
Recommendations for improvement� Developasystemthatallowspatients toaddto thedocumentationbyvoicinghow they are feeling, describing their symptoms with the detail they wouldlike to see documented (including pain levels), and clarifying spiritual needs.
� In relation to global fees for services, design a system to allow theprovider to be paid for any e-health care provided rather than beingpaid only for face-to-face visits.
Crotty et al3 � A descriptive analysisof the volume ofmessages in a largeacademic healthsystem’s patient portal
� The characteristics ofenrolled patientsincluded 61% female,73% white; 87%commercially insured.
� Multiple graphsmeasured growth inthe number ofmessages, variabilityby physician specialty,number of messagesper physician per 100patients, prescriptionrefill requests, andappointment requests.
Type of patient access� Secured messages were defined as “patient-initiated correspondencesent to an attending physician through the portal.”3(p1818)
� The study did not include e-mails sent from outside the portal bypatients to request prescription refills or appointments.
Level of participation� Although the number of messages per month increased in the periodfrom 2001 to 2010, the authors noted this finding may have been aresult of increasing patient enrollment. The researchers did not adjustthe number of messages sent to part-time physicians and did notstandardize the number based on expected message volume had thephysicians been working full time.
� Ofall the patients seen in the system22.7% (n¼ 49,778) had enrolled in thepatient portal offered through a large academic health system, with 36.9%of those enrolled (8.4%of all patients) sending at least one e-mailmessage.
Perceived benefits for patients� Convenient way of communicating.
� Opportunity to enroll in a secured method of electronic communication
Perceived challenges for patients� Security issues with patient-to-physician messaging by e-mail, if thee-mail is not sent through a secured portal.
� Issues of reimbursement for e-mail communications and its effect onproductivity and time.
Recommendations for improvement� Future studies should focus on how messaging can be used by bothpatients and clinicians to improve the quality and efficiency of care.
Fleurence et al4 � Description of 18patient-poweredresearch networks thatwere established in2013 through thePatient-CenteredOutcomes ResearchInstitute (PCORI)
Type of patient access� Patient-powered research networks were used to provide innovativeways to collect, use, and govern the use of data.
Level of participation� Eleven task forces were established to address challenges related tosuch things as governance and data privacy.
Denholm April 2016, Vol. 103, No. 4
379.e3 j AORN Journal www.aornjournal.org

Supplementary Table 2. (continued)
Study or ProjectDescription of Project
or Study Summary of Discussions
� Discussion includedpotential challengesand evaluationtimelines.
� Patients participated in 18 patient-powered research networks bysharing information about a medical condition/disorder or participatingin the network’s leadership and governance.
Perceived benefits for patients� Patient-powered research networks are designed to address thefollowing four key concepts for engaging patients, family members, andcaregivers:
o building trust with secured data entry and protected privacy;o developing strategies to expand diversity to correctunderrepresentation of patient groups in research;
o focusing clinical research activity on more-practical, patient-centeredquestions and outcomes; and
o increasing patient control by including patients in leadership roles andpolicy-setting for patient-powered research networks.
Participants in patient-centered outcomes perceived challenges forresearch� Successful support of the diversity, approaches, expertise, and culture ofeach individual network must be balanced with ensuring that a nationaland functional network is built.
� PCORI will not continue to fund the infrastructure in later phases of theproject.
� Sustainability of the program depends on the willingness and variety ofexternal funders, who will invest in research studies that use the network.
Recommendations for improvement� Build a network that will support the rapid, efficient, and cost-effectiveconduct of research across the United States.
� Collect relevant data by allowing motivated patients to contributeinformation about a specific medical condition in a network with others whoshare the condition, therebyguiding research activities through the network.
� Empower others to get involved in their own plan of care by generatingdata from patients that includes their experiences and preferences formanaging their condition.
References1.Woods S, Schwartz E, Tuepker A, et al. Patient experiences with full electronic access to health records and clinical notes through the My
HealtheVet Personal Health Record Pilot: qualitative study. J Med Internet Res. 2013;15(3):182-191.2.Aultman JM, Dean E. Beyond privacy: benefits and burdens of e-health technologies in primary care. J Clin Ethics. 2014;25(1):50-64.3.Crotty BH, Tamrat Y, Mostaghimi A, Safran C, Landon BE. Patient-to-physician messaging: volume nearly tripled as more patients joined
system, but per capita rate plateaued. Health Aff (Millwood). 2014;33(10):1817-1822.4. Fleurence RL, Beal AC, Sheridan SE, Johnson LB, Selby JV. Patient-powered research networks aim to improve patient care and health
research. Health Aff (Millwood). 2014;33(7):1212-1219.
April 2016, Vol. 103, No. 4 Informatics and Malignant Hyperthermia
www.aornjournal.org AORN Journal j 379.e4