usefulness of self-report instruments in assessing men accused of
TRANSCRIPT

The Psychological Record, 2006, 56, 171-180
USEFULNESS OF SELF-REPORT INSTRUMENTS IN ASSESSING MEN ACCUSED OF DOMESTIC VIOLENCE
LAURA E. HELFRITZ, MATTHEW S. STANFORD, and SARAH M. CONKLIN
Baylor University
KEVIN W. GREVE University of New Orleans
NICOLE R. VILLEMARETTE-PITTMAN LSU Health Sciences Center
REBECCAJ.HOUSTON State University of New York at Buffalo
Clinical assessment of domestic violence has traditionally relied on self-report methods of data collection , using structured interviews and lengthy questionnaires such as the MMPI-2. However, in certain situations such as court-ordered domestic violence evaluations, information obtained through self-report methods may be tainted because of willful impression management on the part of the client. The purpose of the current study was to compare selfreport response styles of individuals with varying levels of domestic violence potential in order to determine whether the measures used could accurately differentiate between the groups.
Individuals who were currently involved in child custody cases were court ordered to an anger assessment clinic to determine their potential for domestic violence because they had been accused of domestic abuse. Participants were classified into three groups: (a) documented domestic violence (n = 12), (b) high risk for domestic violence (n = 16), and (c) minimal risk for domestic violence (n = 24), and completed several measures of personality including the MMPI-2.
Results indicated that the majority of individuals from all three groups used impression management techniques in an attempt to enhance their appearance. However, documented perpetrators of domestic violence still tended to score higher on specific measures of aggression despite their attempts to minimize. These results imply that individuals accused of domestic violence may employ impression management regardless of their guilt or innocence; therefore, the evaluation process should not disproportionately rely on self-reports.
Correspondence concerning this article should be addressed to Matthew S. Stanford, Department of Psychology and Neuroscience, Baylor University, One Bear Place #97334, Waco, TX 76798-7334. (E-mail: Matthew_Stanford @Baylor.edu) .

172 HELFRITZ ET AL.
Clinical assessment of domestic violence has traditionally relied on self-report methods of data collection, using structured interviews and lengthy questionnaires such as the MMPI-2 (Else, Wonderlich, Beatty, Christie, & Staton, 1993; Langhinrichsen-Rohling, Huss, & Ramsey, 2000; McBurnett et aI., 2001). In many populations, this method of assessment is accurate and helpful. However, in certain populations, impression management may seriously compromise the validity of self-report data. For example, individuals involved in child custody cases who have been accused of domestic violence and court-ordered for evaluation clearly have ample motive to answer dishonestly. Therefore, the validity of selfreport measures in the clinical assessment of violence and aggression is highly questionable.
The current domestic violence literature contains few, if any, studies outlining procedures for the assessment of an individual's potential for violence, and most of the literature seems to focus on using self-report measures such as the MMPI-2 or MCMI to profile batterers after the fact (Craig, 2003; Else et aI., 1993; Tweed & Dutton, 1998). Presumably, these profiles can in turn be used to identify potential batterers in order to prevent violence (Craig, 2003). Although this succession of events sounds plausible on the surface, the underlying threat of impression management presents a major problem that may compromise the usefulness of these profiles in individuals suspected of domestic abuse. Parents involved in child custody litigation have previously been found to produce significantly elevated validity scores on the MMPI-2 (Siegel, 1996) and adding an accusation of domestic violence into the equation only exacerbates the risk of impression management.
The present study compared three groups of fathers who were involved in child custody litigation and had been accused of domestic violence. Individuals were grouped by level of risk for domestic violence (documented domestic violence, high risk for domestic violence, and minimal risk for domestic violence) and completed both general selfreport measures of personality such as the MMPI-2 and specific selfreport measures of aggression and impulsivity such as the Buss-Perry Aggression Questionnaire (Buss & Perry, 1992). The purpose of the study was to compare the self-report response styles of individuals with varying levels of domestic violence potential in order to determine whether the measures used could accurately differentiate between the groups.
Method
Participants Eighty individuals who were currently involved in child custody cases
were court ordered to our Anger Assessment Clinic to determine their potential for violence due to a question of domestic abuse. Twenty-seven of the participants were female and were excluded from the present analysis. One male participant was excluded due to an IQ below 80. All of the remaining male participants (n = 52) were included in the present study.
SELF-REPORTS AND DOMESTIC VIOLENCE 173
All participants in the study were accused of domestic violence by their partners. Participants were placed into one of three violence risk groups: (1) Documented domestic violence (DDV)-all individuals in this group (n = 12) had a documented history of arrest and conviction for partner/spousal abuse. (2) High risk for domestic violence-individuals in this group (n = 16) had a documented history of violent behavior other than domestic violence (n = 10) (such as assault) and/or showed clinically significant problems related to impulse control and/or executive function on neuropsychological measures (n = 6). The neuropsychological measures used to assess executive function and impulsivity included: the Wisconsin Card Sorting Task (WCST; Heaton, Chelune, Talley, Kay, & Curtis, 1993), Trail Making Test (Trails A and B; Reitan , 1958), Controlled Oral Word Association Test (COWAT; Lezak, 1995), Ruff Figural Fluency Test (Ruff, Light, & Evans, 1987), and Conners' CPT (Conners, 1995). These measures are sensitive to impulsivity and/or have been shown to differentiate between impulsive aggressive individuals and nonaggressive controls (O'Dougherty, Nuechterlein, & Drew, 1984; Stanford, Grave, & Gerstle, 1997). Scores from these tests were used in the process of grouping the participants and will not be presented. (3) Minimal risk for domestic violence-individuals in this group (n =: 24) had no documented history of violent behavior and did not show impulse control or executive function problems during neuropsychological assessment.
Materials/Procedure Several self-report measures were administered in order to assess
both specific traits of aggression and impulsivity and more general personality traits.
Lifetime History of Aggression Questionnaire (LHAQ; Coccaro, Berman, & Kavoussi, 1997). Aggression was assessed through a semistructured interview. Aggressive and/or antisocial behaviors occurring since the age of 13 were rated for frequency on a scale of zero to five. In addition to a total score, the LHAQ yielded three subscales: Aggression , Antisocial Behavior, and Self-Destructive Behavior.
Barratt Impulsiveness Scale (BIS-11; Patton, Stanford, & Barratt, 1995). This self-report measure consisted of 30 items and served as a measure of general impulsiveness.
Buss-Perry Aggression Questionnaire (BPAQ; Buss & Perry, 1992). This 29-item self-report questionnaire yielded four measures of aggression: physical aggression, verbal aggression, anger, and hostility.
State-Trait Anger Expression Inventory (STAXI; Spielberger, 1996). This 44-item self-report measure was designed to separate and compare the experience of anger with the expression of anger using the following six scales: state anger, trait anger, anger-in, anger-out, anger control, and anger expression.
Eysenck Personality Questionaire (EPQ; Eysenck & Eysenck, 1975). This 90-item self-report instrument provided a general assessment of personality, including extraversion, neuroticism, and psychoticism.

174 HELFRITZ ET AL.
Minnesota Multiphasic Personality Inventory (MMPI-2; Butcher, Dahlstrom, Graham, Tellegen, & Kaemmer, 1989). This widely used general measure of personality consisted of 567 items and yielded 3 validity scales, 10 clinical scales, and a number of subscales including but not limited to validity and consistency subscales designed to detect underreporting, overreporting, responding unrelated to item content, and inconsistent responding.
Statistical Analysis Univariate analyses of variance (ANOVAs) were used to examine
differences between the documented domestic violence, high risk for domestic violence, and minimal risk for domestic violence groups. The Bonferroni inequality was utilized for follow-up comparisons.
Results
Demographic Information Univariate ANOVAs revealed no significant group differences for age
(DDV: M = 33.50, SO = 6.17; High Risk: M = 35.38, SO = 6.23; Minimal Risk: M = 36.71, SO = 9.92), education (DDV: M = 12.58, SO = 1.62; High
Table 1
Specific Measures of Aggression and Impulsivity
DDV High Risk Minimal Risk (n = 12) (n = 16) (n = 24)
Measure M SO M SO M SO
BPAQ Physical 17.67 6.44 15.44 3.61 15.13 4.89 Verbal 12.33 4.68 10.50 2.39 9.58 2.80 Anger 15.42 6.76 11.75 2.96 10.75** 3.07 Hostility 16.92 8.15 13.38 4.35 11 .17** 2 .82 Total Score 62.33 22.24 51.06 9.51 46.63* 11 .22
STAXI State Anger 10.08 0.29 11.94 4.30 10.54 1.64 Trait Anger 15.17 4.28 13.63 3.86 13.00 2.81 Anger-In 12.50 3.40 12.69 3.74 13.75 3.61 Anger-Out 14.00 4.24 12.25 2.62 12.54 2.98 Anger Control 24.92 4.94 26.75 4.58 27.17 3 .95 Anger Expression 18.08 9.81 14.13 9.65 15.13 7.00
LHAQ Aggressive Behavior 8.42 5.95 4.63 2.75 5.38 3 .69 Antisocial Behavior 4.17 3.19 2.38 1.59 2.08* 2 .34 Self-Destructive 0.00 0.00 0.00 0.00 0.13 0.45 Total Score 12.58 8.20 7.00* 3.14 7.83 5.55
BIS-11 Total Score 56.33 9.72 53.63 10.63 50.83 7 .82
Note. * denotes significant difference from documented domestic violence (DDV) group (Ps.05); ** denotes significant difference from documented domestic violence (DDV) group (Ps .01). BPAQ = Buss-Perry Aggression Questionnaire, STAXI = State-Trait Anger Expression Inventory, LHAQ = Lifetime History of Aggression Questionnaire, BIS-11 = Barratt Impulsiveness Scale .

SELF-REPORTS AND DOMESTIC VIOLENCE 175
Risk: M = 13.44, SO = 2.94; Minimal Risk: M = 13.17, SO = 2.24), number of biological children (DDV: M = 2.42, SO = 1.51 ; High Risk: M = 2.19, SO = 0.83; Minimal Risk: M = 2.50, SO = 1.62), or number of marriages (DDV: M = 1.33, SO = 0.78; High Risk: M = 1.50, SO = 1.15; Minimal Risk: M = 1.50, SO = 1.06).
Personality Results Specific measures of aggression and impulsivity. Table 1 presents
descriptive data for all specific measures of aggression and impulsivity. Univariate ANOVAs and follow-up comparisons revealed a significant group difference on the Lifetime History of Aggression Questionnaire (LHAQ) Antisocial Behavior Subscale, F(2, 49) = 3.251 , P = .047, partial ETA squared = .117, power = .593, with the DDV group scoring significantly higher than the minimal risk group. Results of ANOVA showed an omnibus effect for the LHAQ Aggression Subscale, F(2, 49) = 3.256, P = .047, partial ETA squared = .117, power = .593, but followup comparisons revealed no significant differences between groups. Univariate ANOVA and follow-up comparisons indicated that individuals whose domestic violence had been documented scored significantly
Table 2
General Measures of Personality
DDV High Risk Minimal Risk (n = 12) (/7 = 16) (/7 = 24)
Measure M SO M SO M SO EPQ
Psychoticism 2.83 1.90 1.7~; 1.44 2.17 1.69 Extraversion 12.67 5.19 15.69 3.28 15.08 2.65 Neuroticism 5.25 4.43 5.44 4.46 5.33 5.35 Lie 11 .92 4.89 11.75 3.36 11 .33 4.78
MMPI-2 Consistency Scales VRIN 49.67 10.49 45.31 8.87 41.92 7.83 TRIN 59.00 11 .18 54.94 5.18 55.00 6.51
MMPI-2 Validity Scales Lie (L) 64.83 13.00 69.44 12.96 66.13 10.98 Infrequency (F) 47.45 5.77 47.6~~ 6.41 44.54 5.17 Correction (K) 53.08 12.29 60.56 8.52 60.83 8.88
MMPI-2 Clinical Scales Hypochondriasis 45.25 9.19 43.63 9.47 45.67 7.57 Depression 48.17 5.37 47.94 5.62 51.58 6.18 Conversion Hyst. 48.41 7.65 51.94 6.31 53.46 7.78 Psychopathic Dev. 49.25 9.52 52.7Ei 8.15 47.71 6.31 Masc.-Fem. 42.33 4.81 45.38 9.32 44.00 6.35 Paranoia 47.42 10.55 53.63 10.37 50.58 8.76 Psychastenia 43.92 11.85 41 .31 7.34 41 .04 6.22 Schizophrenia 44.50 9.53 42.44 6.74 41.04 6.20 Hypomania 50.92 14.88 49.25 7.58 46.71 5.86 Social Introversion 47.42 9.01 46.00 8.69 44.29 5.86
Note . EPQ = Eysenck Personality Questionnaire ; Conversion Hyst. = Conversion Hysteria; Psychopathic Dev. = Psychopathic Deviate; Masc.-Fem. = Masculinity-Femininity. No significant group differences were found on any of the above measures.
176 HELFRITZ ET AL.
higher than those in the high risk group on the LHAQ Total Score, F(2 , 49) = 3.763, P = .030, partial ETA squared = .133, power = .661.
Significant differences were also found on the Buss-Perry Aggression Questionnaire Total Score, F(2, 49) = 5.006, p = .011, partial ETA squared = .170, power = .790, and two of its subscales: anger, F(2, 49) = 5.118, p = .010, partial ETA squared = .173, power = .799, and hostility, F(2, 49) = 5.428, P = .007, partial ETA squared = .181, power = .824, with the DDV group scoring significantly higher than the minimal risk group.
No significant differences were found between any of the groups on the Barratt Impulsiveness Scale, the State-Trait Anger Expression Inventory, or the Self-Destructive Behavior Subscale of the Lifetime History of Aggression Questionnaire.
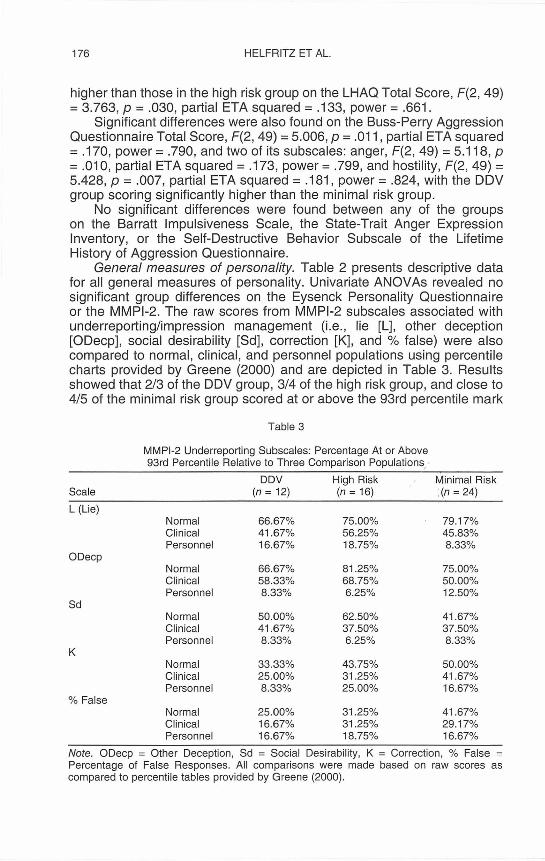
General measures of personality. Table 2 presents descriptive data for all general measures of personality. Univariate ANOVAs revealed no significant group differences on the Eysenck Personality Questionnaire or the MMPI-2. The raw scores from MMPI-2 subscales associated with underreporting/impression management (i.e., lie [L], other deception [ODecp], social desirability [Sd], correction [K], and % false) were also compared to normal, clinical, and personnel populations using percentile charts provided by Greene (2000) and are depicted in Table 3. Results showed that 2/3 of the DDV group, 3/4 of the high risk group, and close to 4/5 of the minimal risk group scored at or above the 93rd percentile mark
Table 3
MMPI-2 Underreporting Subscales: Percentage At or Above 93rd Percentile Relative to Three Comparison Populations.,
DDV High Risk Minimal Risk Scale (n = 12) (n = 16) :(n = 24)
L (Lie) Normal 66,67% 75.00% 79,17% Clinical 41.67% 56,25% 45.83% Personnel 16.67% 18.75% 8.33%
ODecp Normal 66.67% 81 .25% 75,00% Clinical 58.33% 68.75% 50,00% Personnel 8.33% 6,25% 12.50%
Sd Normal 50 ,00% 62.50% 41 ,67% Clinical 41 .67% 37.50% 37.50% Personnel 8,33% 6,25% 8.33%
K Normal 33.33% 43.75% 50.00% Clinical 25,00% 31.25% 41.67% Personnel 8.33% 25.00% 16.67%
% False Normal 25.00% 31 ,25% 41 .67% Clinical 16.67% 31 .25% 29.17% Personnel 16,67% 18,75% 16.67%
Note. ODecp = Other Deception, Sd = Social Desirability, K = Correction , % False = Percentage of False Responses. All comparisons were made based on raw scores as compared to percentile tables provided by Greene (2000),
SELF-REPORTS AND DOMESTIC VIOLENCE 177
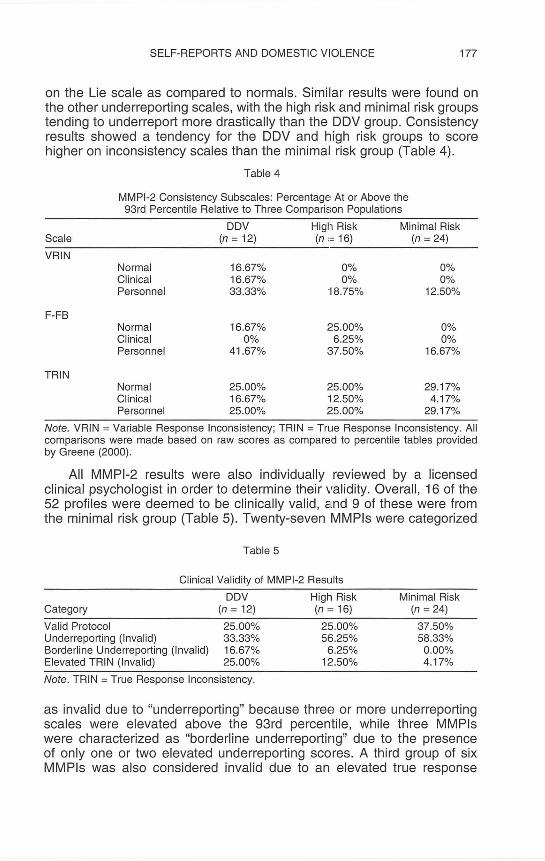
on the Lie scale as compared to normals. Similar results were found on the other underreporting scales, with the high risk and minimal risk groups tending to underreport more drastically than the DDV group. Consistency results showed a tendency for the DDV and high risk groups to score higher on inconsistency scales than the minimal risk group (Table 4).
Table 4
MMPI-2 Consistency Subscales: Percentage At or Above the 93rd Percentile Relative to Three Comparison Populations
DDV Higtl Risk Minimal Risk Scale (n = 12) (n ,= 16) (n = 24)
VRIN Normal 16.67% 0% 0% Clinical 16.67% 0% 0% Personnel 33.33% 18.75% 12.50%
F-FB Normal 16.67% ;~5 .00% 0% Clinical 0% 6.25% 0% Personnel 41 .67% 37.50% 16.67%
TRIN Normal 25.00% 25.00% 29.17% Clinical 16.67% ~12 . 50% 4.17% Personnel 25.00% ;~5.00% 29.17%
Note. VRIN = Variable Response Inconsistency; TRIN = True Response Inconsistency. All comparisons were made based on raw scores as compared to percentile tables provided by Greene (2000) .
All MMPI-2 results were also individually reviewed by a licensed clinical psychologist in order to determine their validity. Overall, 16 of the 52 profiles were deemed to be clinically valid, and 9 of these were from the minimal risk group (Table 5). Twenty-seven MMPls were categorized
Table 5
Clinical Validity of MMPI-2 Results
Category
Valid Protocol Underreporting (Invalid) Borderline Underreporting (Inval id) Elevated TRIN (Invalid)
DDV High Risk (n = 12) (n = 16)
25.00% 33.33% 16.67% 25.00%
25.00% 5E>'25%
6.25% 12.50%
Note. TRIN = True Response Inconsistency.
Minimal Risk (n = 24)
37.50% 58.33% 0.00% 4.17%
as invalid due to "underreporting" because three or more underreporting scales were elevated above the 93rd percentile, while three MMPls were characterized as "borderline underreporting" due to the presence of only one or two elevated underreporting scores. A third group of six MMPls was also considered invalid due to an elevated true response

178 HELFRITZ ET AL.
linconsistency (TRIN) score, which indicated that the responses given were unrelated to item content (Greene, 2000). No protocols were invalid because of inconsistent responding (VRIN) or overreporting.
Discussion
Results clearly indicate that substantial portions of all three groups employed impression management to portray themselves in the most favorable light possible. In some cases, the individuals deemed to have the least potential for domestic violence actually distorted their responses the most. This is surprising because it can easily be assumed that only a guilty party would answer dishonestly; however, due to the high stakes inherent in child custody cases, both violent and nonviolent fathers alike used impression management techniques in an attempt to enhance their appearance. Even so, documented perpetrators of domestic violence still tended to score higher on specific measures of aggression despite their attempts to minimize. It is possible that this occurred because these individuals had a lack of insight into their own problematic behavior, in that when they were confronted with specific sets of items measuring anger, aggression, and hostility, their attempts at impression management, while lowering their scores somewhat, did not lower them enough to make them appear "normal." In other words, these individuals may be unable to estimate normal levels of aggression for the purposes of impression management. This finding provides a basis for encouraging the use of specific measures of aggression and impulsivity such as the Buss-Perry Aggression Questionnaire, as they may provide better insight than more general measures like the MMPI-2. However, all information reported by any population with motive to answer dishonestly should still be interpreted with caution. It should also be kept in mind that given the fact that members of all three groups, whether violent or not, showed elevations on underreporting scales, an invalid MMPI-2 is not necessarily an indication of guilt; indeed, in some cases it is merely a reflection of the high stakes involved.
In short, these results demonstrate that self-report measures have limited use in populations who routinely can be expected to employ high levels of impression management. In critical assessments such as court-ordered domestic violence investigations, both guilty and innocent individuals adopt dishonest strategies in order to present themselves more favorably. This nonspecific finding means the clinician cannot infer guilt based on willful impression management on self-report measures, although specific measures of aggression may lend some support.
The clinician can, however, take advantage of an increased motivation to present oneself favorably. It is recommended that neuropsychological testing, which can capitalize on a highly motivated performance, be used in addition to self-report measures to obtain a more accurate picture of the client. Poor performance on the Wisconsin Card Sorting Task, the Trail Making Test, and the Controlled Oral Word Association Test (COWAT) has

SELF-REPORTS AND DOMESTIC VIOLENCE 179
been associated with impulsive aggressive behavior (Stanford et aI., 1997). Continuous performance tasks such as Conners' CPT have also been well established as measures of impulsivity (O'Dougherty et aI., 1984).
It is important to note that not all individuals who participate in courtordered evaluations use impression management techniques. Indeed, in some individuals the MMPI-2 may be helpful, and its routine use in these critical evaluations is not discouraged. However, the use of sources of independent documentation such as police reports and court records of filing for restraining orders, as well as behavioral measures of impulsivity are encouraged so that the evaluation process is not disproportionately dependent on self-report measures.
References
BUSS, A. H., & PERRY, M. (1992). The aggression questionnaire. Journal of Personality and Social Psychology, 63, 452-459.
BUTCHER, J., DAHLSTROM, W. , GRAHAM, J., TELLEGEN, A., & KAEMMER, B. (1989) . Minnesota Multiphasic Personality Inventory-2 (MMPI-2): Manual for administration and scoring . Minneapolis: University of Minnesota Press.
COCCARO, E. F., BERMAN, M. E., & KAVOUSSI , R. J. (1997) . Assessment of life history aggression: Development and psychometric characteristics. Psychiatry Research , 73,147-157.
CONNERS, C. K. (1995). CPT: Conners ' Continuous Performance Test. Toronto: Multi-Health Systems, Inc.
CRAIG, R. J. (2003). Use of the Millon Clinical Multiaxial Inventory in the psychological assessment of domestic violence. Aggression and Violent Behavior, 8, 235-243.
ELSE, L. T. , WONDERLlCH, S. A., BEATTY, W. W., CHRISTIE, D. W. , & STATON, R. D. (1993). Personality characteristics of men who physically abuse women. Hospital and Community Psychiatry, 44, 54-58.
EYSENCK, H. J ., & EYSENCK, S. B. G. (1975) . Eysenck Personality Questionnaire (Junior and Adult), Manual. San Diego: Educational and Industrial Testing Services.
GREENE, R. L. (2000) . The MMPI-2: An Interpretive Manual (2nd ed.) Boston: Allyn & Bacon.
HEATON, R. K. , CHELUNE, G. J., TALLEY, J. L., KAY, G. G. , & CURTIS, G. (1993). Wisconsin Card Sorting Test Manual: Revised and expanded. Odessa, FL: Psychological Assessment Resources, Inc.
LANGHINRICHSEN-ROHLlNG, J., HUSS, M. T., & RAMSEY, S. (2000) . The clinical utility of batterer typologies. Journal of Family Violence, 15, 37-54.
LEZAK, M. D. (1995) . Neuropsychological assessment (3rd ed.). New York: Oxford University Press.
MCBURNETT, K., KERCKHOFF, C., CAPASSO, L., PFIFFNER, L. J ., RATHOUZ, P. J. , MCCORD, M., & HARRIS, S. M. (2001). Antisocial personality, substance abuse, and exposure to parental violence in males referred for domestic violence. Violence and Victims, 16, 491-506.
O'DOUGHERTY, M. , NUECHTERLEIN, K. H. , & DREW, B. (1984). Hyperactive and hypoxic children : Signal detection , sustained attention, and behavior. Journal of Abnormal Psychology, 93, 178-191.

180 HELFRITZ ET AL.
PATTON, J . H., STANFORD, M. S. , & BARRATT, E. S. (1995). Factor structure of the Barratt Impulsiveness Scale. Journal of Clinical and Consulting Psychology, 51, 768-774.
REITAN, R. M. (1958). Validity of the Trail Making Test as an indication of organiC brain damage. Perceptual and Motor Skills, 8, 271-276.
RUFF, R. M., LIGHT, R. H., & EVANS, R. W. (1987). The Ruff Figural Fluency Test: A normative study with adults. Developmental Neuropsychology, 3, 37-52.
SIEGEL, J. C. (1996). Traditional MMPI-2 validity indicators and initial presentation in custody evaluations. American Journal of Forensic Psychology, 14, 55-63.
SPIELBERGER, C. D. (1996). State-Trait Anger Expression Inventory, Manual. Odessa, FL: Psychological Assessment Resources.
STANFORD, M. S. , GREVE, K. W., & GERSTLE, J. E. (1997). Neuropsychological correlates of self-reported impulsive aggression in a college sample. Personality and Individual Differences , 23, 961-965.
TWEED, R. G. , & DUTTON, D. G. (1998). A comparison of impulsive and instrumental subgroups of batterers. Violence and Victims, 13, 217-230.