use of thrombectomy devices for the emergent...
TRANSCRIPT

1
USE OF THROMBECTOMY DEVICES FOR THE EMERGENT TREATMENT
OF ACUTE ISCHEMIC STROKE
A Technology Assessment
INTRODUCTION
The California Technology Assessment Forum (CTAF) is requested to review
the scientific evidence for the use of thrombectomy devices in patients with acute
ischemic stroke. CTAF reviewed the Merci Retriever device in 2007.1 Since that time,
use of these devices has increased exponentially in the United States.2 In addition,
the Food and Drug Administration has approved three additional devices, the
Penumbra System in 2007 and the Solitaire FR and Trevo in 2012. Two randomized
trials were published in 2012 comparing two of the new devices to the Merci
Retriever.3,4 More importantly, three randomized trials5-7 were published online in
February 2013 comparing endovascular therapy to intravenous tissue plasminogen
activator, which is the established alternative.
2
BACKGROUND
Stroke
In the U.S., cerebrovascular disease is currently the third leading cause of
death with more than 215,000 stroke-related fatalities per year.8 Annually, there are
approximately 795,000 strokes and currently there are more than 6.8 million stroke
survivors with varying degrees of disability.8 In patients with acute stroke,
angiography studies done within six hours of symptom onset have demonstrated
that the majority of patients have angiographically visible occlusion of an
extracranial and/or intracranial artery as the primary cause.9 Studies estimate that
87% of strokes are ischemic.8 Long term functional outcomes are worse in patients
who are older, have occlusions of the large intracranial arteries, and have high
disease severity scores at presentation.10-12 Recanalization of the occluded artery is
the only effective therapy for acute stroke. Until recently, patients were mainly
treated supportively to optimize cerebral perfusion and oxygenation with
antithrombotic therapy prescribed on discharge.13 In 1995, a seminal randomized
clinical trial demonstrated that recanalization of the artery with intravenous (IV)
administration of tissue plasminogen activator (tPA) within three hours of the onset
of symptoms from acute stroke improved functional outcomes in patients and was
associated with a trend towards decreased total mortality at three months.14 The
benefits diminish rapidly with the time from symptom onset. A recent pooled
analysis of the trials of IV thrombolysis reported that the benefits outweigh the risks
for patients treated within 4.5 hours of stroke onset, but beyond 4.5 hours the
harms might outweigh the benefits.15 In trials of IV thrombolysis for stroke, there
was an increase in early deaths compared to the placebo arms in the first seven to
ten days following therapy, primarily due to an increase in symptomatic intracranial
hemorrhage (SICH).16 For IV tPA there were an extra 62 cases of SICH for every 1000

3
patients treated (from about two percent in control patients to about eight percent
with tPA).16 Long term functional benefits counterbalanced these risks of early harm.
A recent meta-analysis proposed that recanalization could be used as a
surrogate marker in preliminary trials evaluating interventions for the treatment of
acute stroke.17 Recanalization does not occur universally with treatment. In the
meta-analysis, spontaneous recanalization occurred in 24% of patients and in 46%
of patients treated with IV thrombolytics. It has been hypothesized that large
volume clots in the proximal vessels are less likely to dissolve with intravenous tPA.
Several approaches have been tested including intra-arterial thrombolytic therapy
with or without systematic thrombolysis, mechanical disruption of the clot, sonic
disruption of the clot, a variety of approaches to endovascular thrombectomy, and
combinations of the above therapies.18 Theoretically, each of these approaches
would have a greater likelihood of recanalization of the artery, a lower risk of SICH,
and this should translate into better outcomes. Unfortunately, all of these
approaches require angiography and intra-arterial microcatheter placement prior to
treatment, which may delay the delivery of effective therapy compared to IV
thrombolysis. One randomized clinical trial, the Prolyse in Acute Cerebral
Thromboembolism II (PROACT II) trial, demonstrated that intra-arterial
prourokinase was associated with higher recanalization rates than medical
management with IV heparin (66% versus 18%, p<0.001), although the rates of SICH
were also higher (10% versus 2%).19 Assessment of good long-term functional
outcomes favored the intra-arterial thrombolysis (40% versus 25%, p=0.04) with no
significant difference in mortality (25% vs. 27%, p NS). It is worth noting that the
FDA did not feel that these results were strong enough to support approval of the
drug for this indication, despite the unequivocal increase in recanalization rates.
Most other approaches have case-report level data or are being tested in ongoing

4
clinical trials. Several authorities in the field have argued that the theory that
recanalization is an appropriate intermediate marker for clinical trials is unproven
and that randomized trials are necessary to prove that intra-arterial treatments,
such as thrombectomy, are an improvement on intravenous tPA, the standard
therapy.20-23 Despite those concerns, use of thrombectomy devices has increased
exponentially in the United States.2 Using data from the National Inpatient Sample,
Brinjikji and colleagues found that the use of thrombectomy devices increased from
266 in 2006 to 800 in 2007 up to 2,798 in 2008.
Thrombectomy devices
Merci Retriever
The Merci Retriever is the first of the endovascular mechanical devices to
receive FDA approval for use in the United States. It is designed to physically trap
and then remove the clot occluding an artery. Potential benefits include lower or no
use of thrombolytic agent, thus lower risks of bleeding, and higher recanalization
rates. These are balanced by the need for angiography and intra-arterial access
which delays the time to delivery of initial therapy and can damage the vascular
endothelium.
The initial models (X5, X6) of the device itself were self-expanding tapered
helices made of nitinol, a nickel titanium alloy. The second generation L5 device has
a somewhat different design: the coils of the helix are stronger, they no longer
taper, and there are a series of filaments attached to the coils. These design
changes are intended to reduce the risk of device fracture and to improve the
ability of the device to capture and remove the clot.
The procedure is similar to other angiographic procedures. An introducer is
placed in the femoral artery and a catheter threaded into the extracranial artery
5
leading to the affected artery. A microcatheter is threaded through the guiding
catheter and positioned immediately proximal to the clot. The Merci retriever device
is deployed through the clot and pulled back into the clot. A balloon at the tip of
the guiding catheter is inflated to block blood flow. With the balloon inflated, the
Merci Retriever and the clot are withdrawn into the positioning catheter and out of
the patient’s body.
The Penumbra System
The Penumbra System is a microcatheter system attached to a pump that
can apply continuous suction. The catheter is advanced to the proximal end of the
clot and then retrieved under constant negative pressure. Ideally the clot is drawn
back out with the catheter.
The Solitaire FR
The Solitaire FR device is a member of the class of stent retriever devices.
These are designed as self-expandable, re-sheathable stents. They are threaded
into the clot and opened up so that there is immediate restoration of flow to the
brain. They are usually left in place for several minutes to allow the clot to adhere to
the stent. The stent is then retrieved with the adherent clot.
The Trevo Pro Retriever System
The Trevo Pro Retriever is the second FDA approved stent retriever.
6
TECHNOLOGY ASSESSMENT (TA)
TA Criterion 1: The technology must have final approval from the appropriate
government regulatory bodies.
The Merci Retriever is considered a Class II, Percutaneous Catheter. Models
X5 and X6 were approved through the FDA 510(k) process in August 2004 as
substantially equivalent to legally marketed predicate devices marketed in interstate
commerce prior to May 28, 1976. Modifications to the Merci Retriever were also
approved through the FDA 510(k) process in April 2007 and August 2007.
Per the FDA: “The Merci Retriever is intended to restore blood flow in the
neurovasculature by removing thrombus in patients experiencing ischemic stroke.
Patients who are ineligible for treatment with intravenous tissue plasminogen
activator (IV t-PA) or who fail IV t-PA therapy are candidates for treatment. The
Merci Retriever is also indicated for use in the retrieval of foreign bodies misplaced
during interventional radiological procedures in the neuron, peripheral and
coronary vasculature.”
As mentioned earlier, the other catheters used in thrombectomy for ischemic
stroke - Solitaire FR Revascularization device by Covidien, the TREVO Pro Retriever
by Stryker Neurovascular, and the Penumbra System by Penumbra, Inc. - are also
classified as Class II devices approved via the 510K process.
TA Criterion 1 is met.
7
TA Criterion 2: The scientific evidence must permit conclusions concerning
the effectiveness of the technology regarding health
outcomes.
The Medline database, Cochrane clinical trials database, Cochrane reviews
database and the Database of Abstracts of Reviews of Effects (DARE) were searched
using the key words embolectomy, thrombectomy, mechanical embolus removal,
mechanical thrombus removal, endovascular device, endovascular intervention, or
endovascular recanalization. These were cross-referenced with the keywords
cerebrovascular accident, stroke, CVA, artery occlusion, and human. We included
case series, comparative studies and randomized trials that reported outcomes on
at least five patients with acute stroke treated with a thrombectomy device. The
bibliographies of systematic reviews and key articles were manually searched for
additional references and references were requested from the device
manufacturers. We also reviewed “related articles” in PubMed for each of the key
clinical trials.
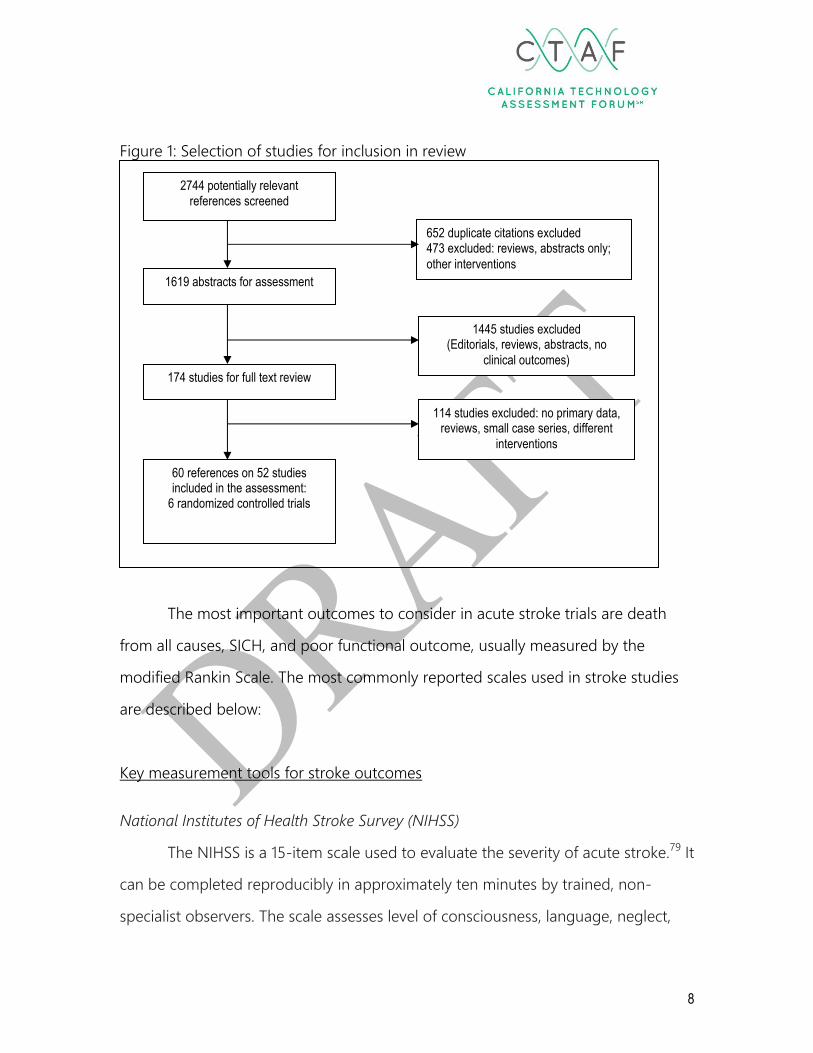
The search identified 2744 potentially relevant studies (Figure 1). After
elimination of duplicate and non-relevant references including reviews, studies of
unrelated devices and procedures, and animal studies the search identified 60
articles describing 39 case series,2,24-66 seven comparative studies67-73 and six
randomized trials.3-7,74-78
8
Figure 1: Selection of studies for inclusion in review
The most important outcomes to consider in acute stroke trials are death
from all causes, SICH, and poor functional outcome, usually measured by the
modified Rankin Scale. The most commonly reported scales used in stroke studies
are described below:
Key measurement tools for stroke outcomes
National Institutes of Health Stroke Survey (NIHSS)
The NIHSS is a 15-item scale used to evaluate the severity of acute stroke.79 It
can be completed reproducibly in approximately ten minutes by trained, non-
specialist observers. The scale assesses level of consciousness, language, neglect,
2744 potentially relevant references screened
1619 abstracts for assessment
60 references on 52 studies included in the assessment:
6 randomized controlled trials
174 studies for full text review
652 duplicate citations excluded 473 excluded: reviews, abstracts only;
other interventions
1445 studies excluded (Editorials, reviews, abstracts, no
clinical outcomes)
114 studies excluded: no primary data, reviews, small case series, different
interventions
9
visual-field loss, extraocular movement, motor strength, ataxia, dysarthria, and
sensation. The scale ranges from 0 for normal to 31 for a stroke patient with
complete hemiparesis, hemianopia, hemineglect, and aphasia. The examination
requires between five and eight minutes to complete. Studies have demonstrated
excellent reliability of the scale in multiple settings.79-81 The NIHSS score correlates
well with the size of the stroke on CT scan at one week79 and with three month
clinical outcomes assessed by standard measures like the modified Rankin Scale or
the Barthel Index.82
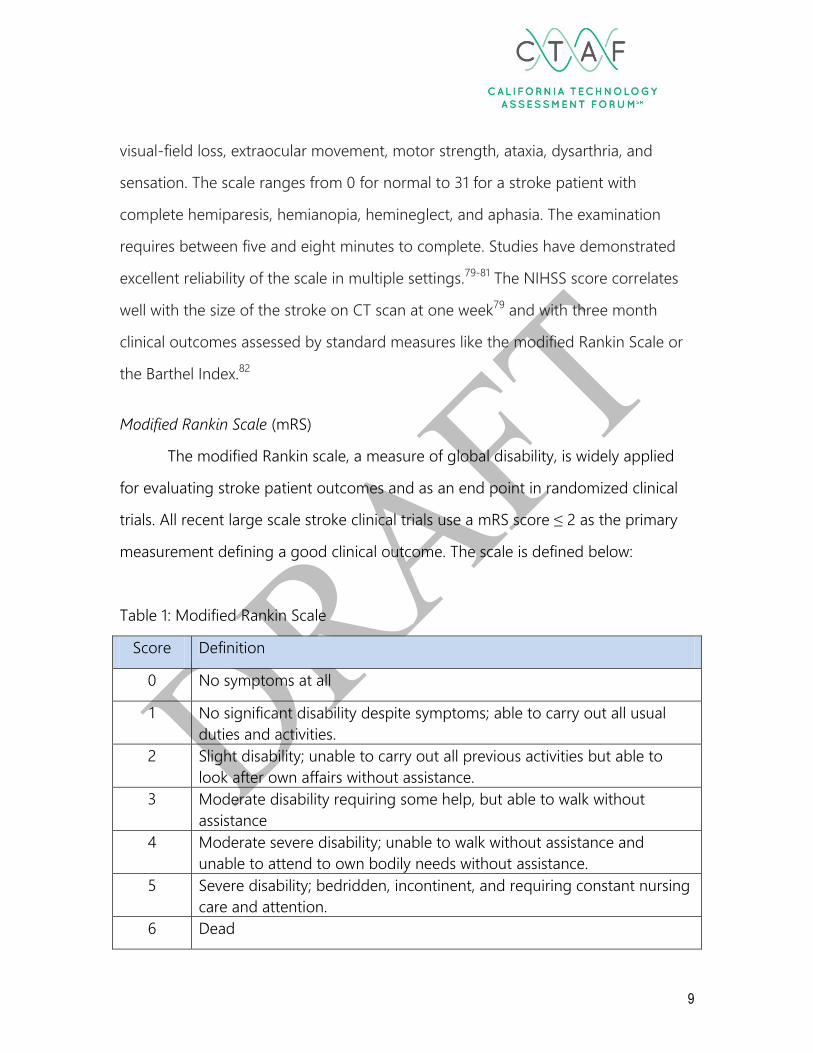
Modified Rankin Scale (mRS)
The modified Rankin scale, a measure of global disability, is widely applied
for evaluating stroke patient outcomes and as an end point in randomized clinical
trials. All recent large scale stroke clinical trials use a mRS score ≤ 2 as the primary
measurement defining a good clinical outcome. The scale is defined below:
Table 1: Modified Rankin Scale
Score Definition
0 No symptoms at all
1 No significant disability despite symptoms; able to carry out all usual
duties and activities.
2 Slight disability; unable to carry out all previous activities but able to
look after own affairs without assistance.
3 Moderate disability requiring some help, but able to walk without
assistance
4 Moderate severe disability; unable to walk without assistance and
unable to attend to own bodily needs without assistance.
5 Severe disability; bedridden, incontinent, and requiring constant nursing
care and attention.
6 Dead
10
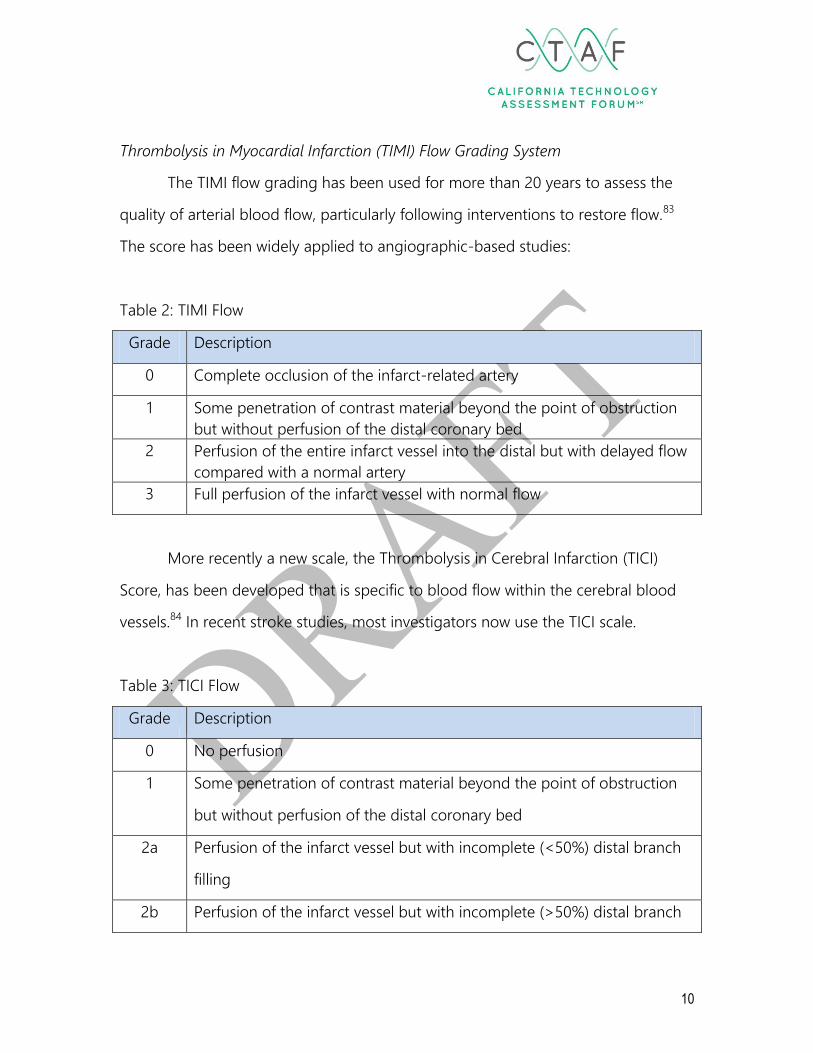
Thrombolysis in Myocardial Infarction (TIMI) Flow Grading System
The TIMI flow grading has been used for more than 20 years to assess the
quality of arterial blood flow, particularly following interventions to restore flow.83
The score has been widely applied to angiographic-based studies:
Table 2: TIMI Flow
Grade Description
0 Complete occlusion of the infarct-related artery
1 Some penetration of contrast material beyond the point of obstruction
but without perfusion of the distal coronary bed
2 Perfusion of the entire infarct vessel into the distal but with delayed flow
compared with a normal artery
3 Full perfusion of the infarct vessel with normal flow
More recently a new scale, the Thrombolysis in Cerebral Infarction (TICI)
Score, has been developed that is specific to blood flow within the cerebral blood
vessels.84 In recent stroke studies, most investigators now use the TICI scale.
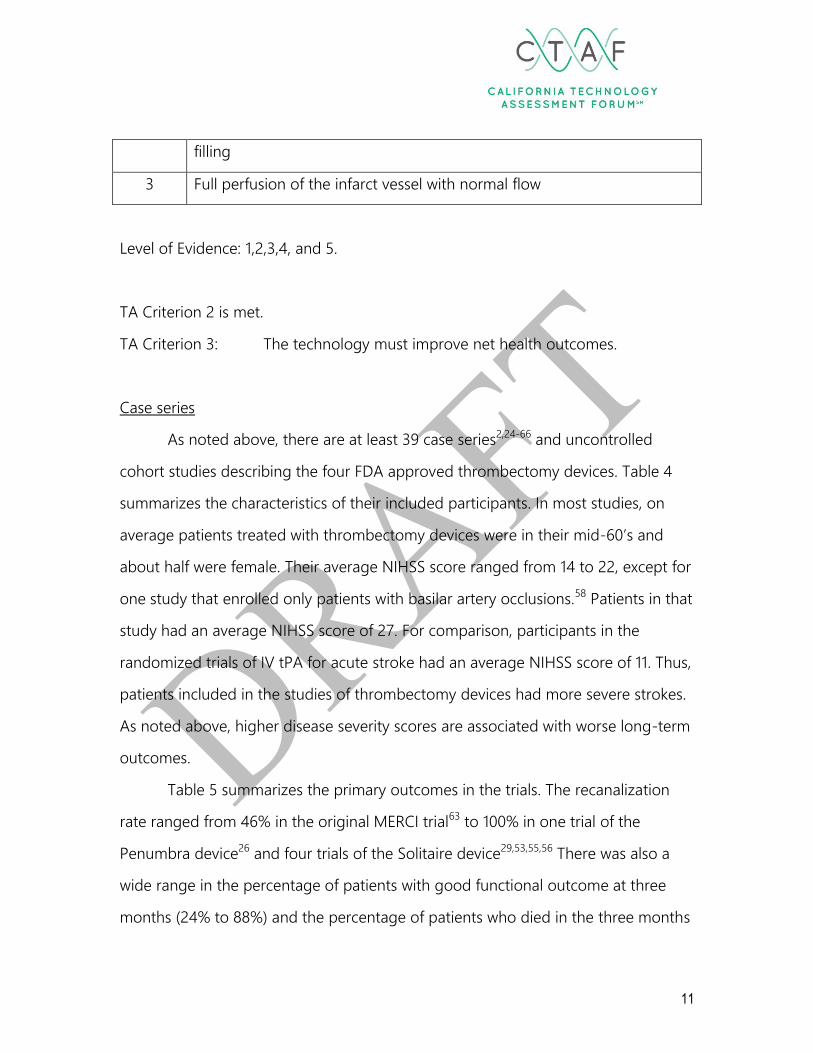
Table 3: TICI Flow
Grade Description
0 No perfusion
1 Some penetration of contrast material beyond the point of obstruction
but without perfusion of the distal coronary bed
2a Perfusion of the infarct vessel but with incomplete (<50%) distal branch
filling
2b Perfusion of the infarct vessel but with incomplete (>50%) distal branch
11
filling
3 Full perfusion of the infarct vessel with normal flow
Level of Evidence: 1,2,3,4, and 5.
TA Criterion 2 is met.
TA Criterion 3: The technology must improve net health outcomes.
Case series
As noted above, there are at least 39 case series2,24-66 and uncontrolled
cohort studies describing the four FDA approved thrombectomy devices. Table 4
summarizes the characteristics of their included participants. In most studies, on
average patients treated with thrombectomy devices were in their mid-60’s and
about half were female. Their average NIHSS score ranged from 14 to 22, except for
one study that enrolled only patients with basilar artery occlusions.58 Patients in that
study had an average NIHSS score of 27. For comparison, participants in the
randomized trials of IV tPA for acute stroke had an average NIHSS score of 11. Thus,
patients included in the studies of thrombectomy devices had more severe strokes.
As noted above, higher disease severity scores are associated with worse long-term
outcomes.
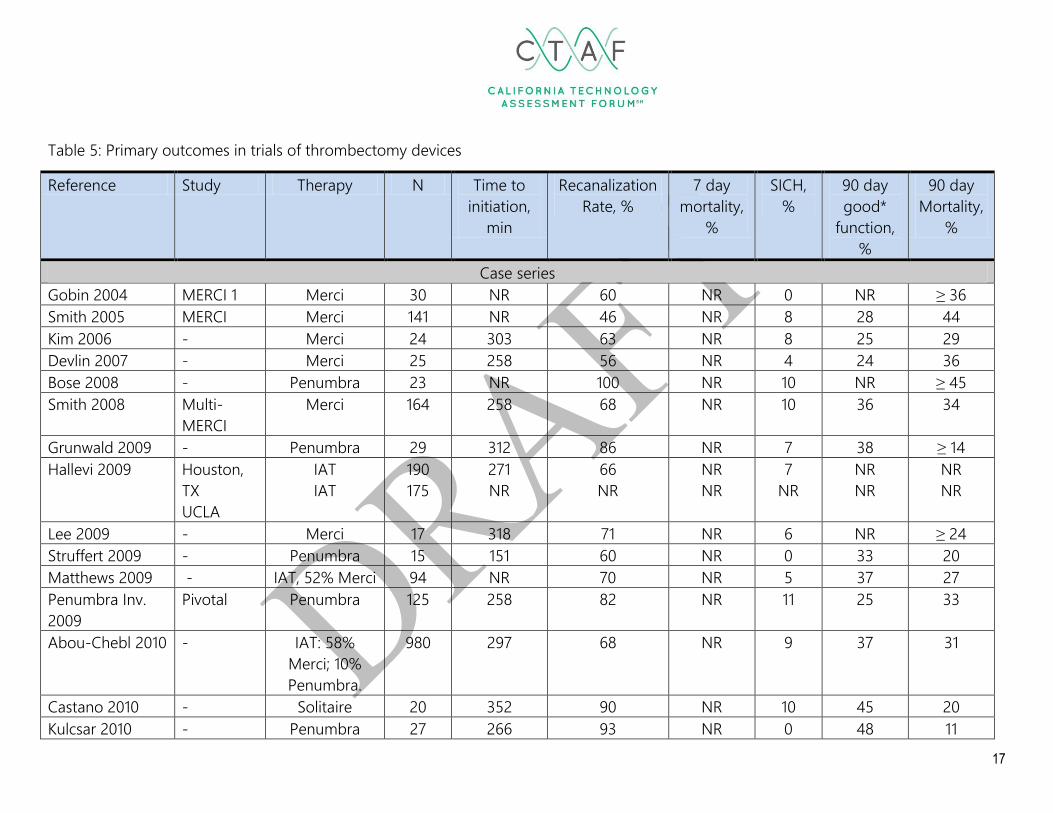
Table 5 summarizes the primary outcomes in the trials. The recanalization
rate ranged from 46% in the original MERCI trial63 to 100% in one trial of the
Penumbra device26 and four trials of the Solitaire device29,53,55,56 There was also a
wide range in the percentage of patients with good functional outcome at three
months (24% to 88%) and the percentage of patients who died in the three months
12
following the stroke (6% to 44%). Good outcomes did not always correlate with
higher rates of recanalization. For example, one of the studies reporting 100%
recanalization with the Solitaire device29 reported that 88% of patients had good
function at three months and a 6% mortality, while a second study with 100%
recanalization with the same device53 reported that only 29% had good function at
three months and a 36% mortality. There are many possible explanations for the
variation in outcomes including differences in the definitions of recanalization, the
age and co-morbidity of the patients, the initial severity of stroke symptoms, the
location of the strokes, the volume of clot, the time to presentation, the time from
presentation to recanalization, the concomitant use of IV and IA thrombolytics, and
the experience of the personnel at the stroke center. Large comparative trials,
ideally randomized, are needed in order to compare different interventions.
The most consistently reported harm was symptomatic intracranial
hemorrhage. Reperfusion itself can convert an ischemic stroke to a hemorrhagic
stroke. Complications from use of the device, such as vessel perforation, can also
cause significant hemorrhage. These case series reported that the rate of SICH
ranged from 0 to 18%. Other potential device-related complications reported in the
case series included arterial vasospasm and dissection, embolism of the clot to
previously unaffected areas of the brain, complications at the site of arterial access,
and an increased need for anesthesia and intubation for the procedure. The rate of
these complications ranged from 0% to about 15%. These will be described in more
detail in the section on the randomized trials below.

13
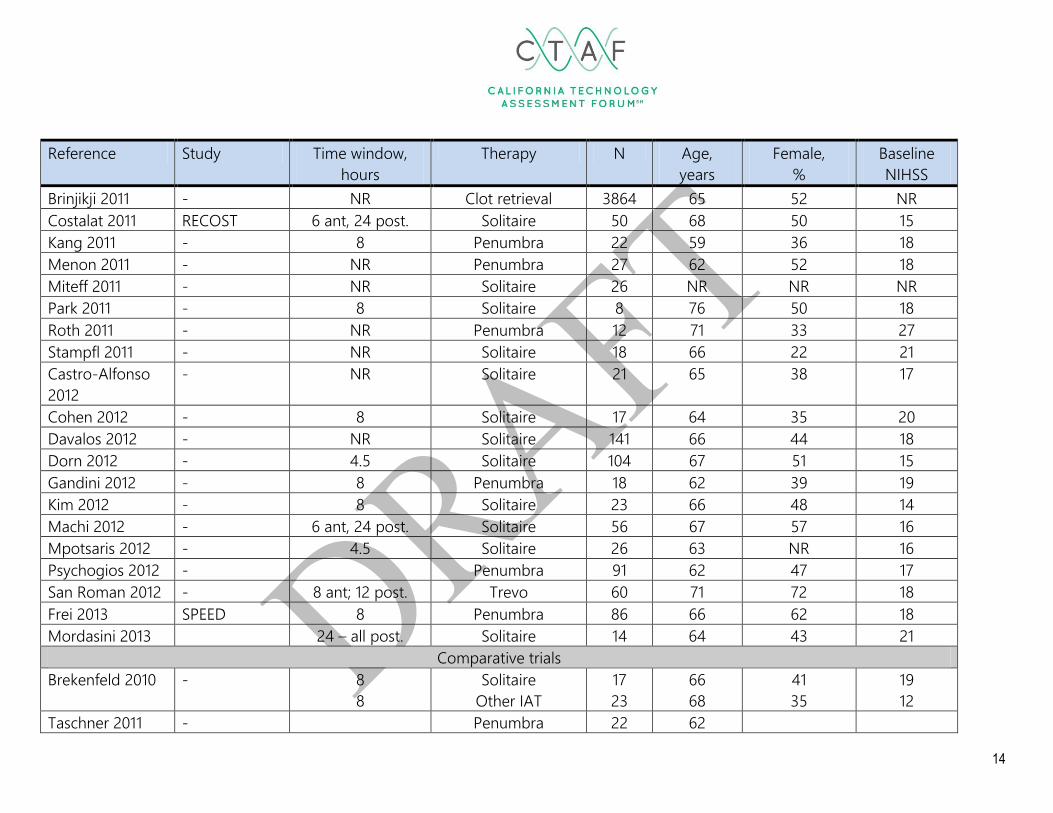
Table 4: Study and patient characteristics in trials of thrombectomy devices
Reference Study Time window,
hours
Therapy N Age,
years
Female,
%
Baseline
NIHSS
Case series
Gobin 2004 MERCI 1 8 Merci 30 68 50 22
Smith 2005 MERCI 8 Merci 141 67 46 20
Kim 2006 - 8 Merci 24 64 42 21
Devlin 2007 - 8 Merci 25 63 36 18
Bose 2008 - 8 Merci 23 60 40 21
Smith 2008 Multi-MERCI 8 Merci 164 68 57 19
Grunwald 2009 - 8 Penumbra 29 59 48 20
Hallevi 2009 Houston, TX
UCLA
6
8
IAT
IAT
190
175
62
70
NR
NR
19
17
Lee 2009 - 8 Merci 17 67 13 18
Struffert 2009 - 6 Penumbra 15 60 40 NR
Matthews 2009 - 3 IAT, 52% Merci 94 68 56 15
Penumbra Inv.
2009
Pivotal 8 Penumbra 125 64 49 18
Abou-Chebl 2010 - NR IAT: 58% Merci; 10%
Penumbra.
980 66 52 17
Castano 2010 P 8 Solitaire 20 66 50 19
Kulcsar 2010 - NR Penumbra 27 66 48 14
Loh 2010 - NR Merci 106 66 55 19
Nayak 2010 - 8 Solitaire 7 70 100 19
Roth 2010 - 6 Solitaire 22 65 27 19
Tarr 2010 POST NR Penumbra 157 65 46 16
14
Reference Study Time window,
hours
Therapy N Age,
years
Female,
%
Baseline
NIHSS
Brinjikji 2011 - NR Clot retrieval 3864 65 52 NR
Costalat 2011 RECOST 6 ant, 24 post. Solitaire 50 68 50 15
Kang 2011 - 8 Penumbra 22 59 36 18
Menon 2011 - NR Penumbra 27 62 52 18
Miteff 2011 - NR Solitaire 26 NR NR NR
Park 2011 - 8 Solitaire 8 76 50 18
Roth 2011 - NR Penumbra 12 71 33 27
Stampfl 2011 - NR Solitaire 18 66 22 21
Castro-Alfonso
2012
- NR Solitaire 21 65 38 17
Cohen 2012 - 8 Solitaire 17 64 35 20
Davalos 2012 - NR Solitaire 141 66 44 18
Dorn 2012 - 4.5 Solitaire 104 67 51 15
Gandini 2012 - 8 Penumbra 18 62 39 19
Kim 2012 - 8 Solitaire 23 66 48 14
Machi 2012 - 6 ant, 24 post. Solitaire 56 67 57 16
Mpotsaris 2012 - 4.5 Solitaire 26 63 NR 16
Psychogios 2012 - Penumbra 91 62 47 17
San Roman 2012 - 8 ant; 12 post. Trevo 60 71 72 18
Frei 2013 SPEED 8 Penumbra 86 66 62 18
Mordasini 2013 24 – all post. Solitaire 14 64 43 21
Comparative trials
Brekenfeld 2010 - 8
8
Solitaire
Other IAT
17
23
66
68
41
35
19
12
Taschner 2011 - Penumbra 22 62
15
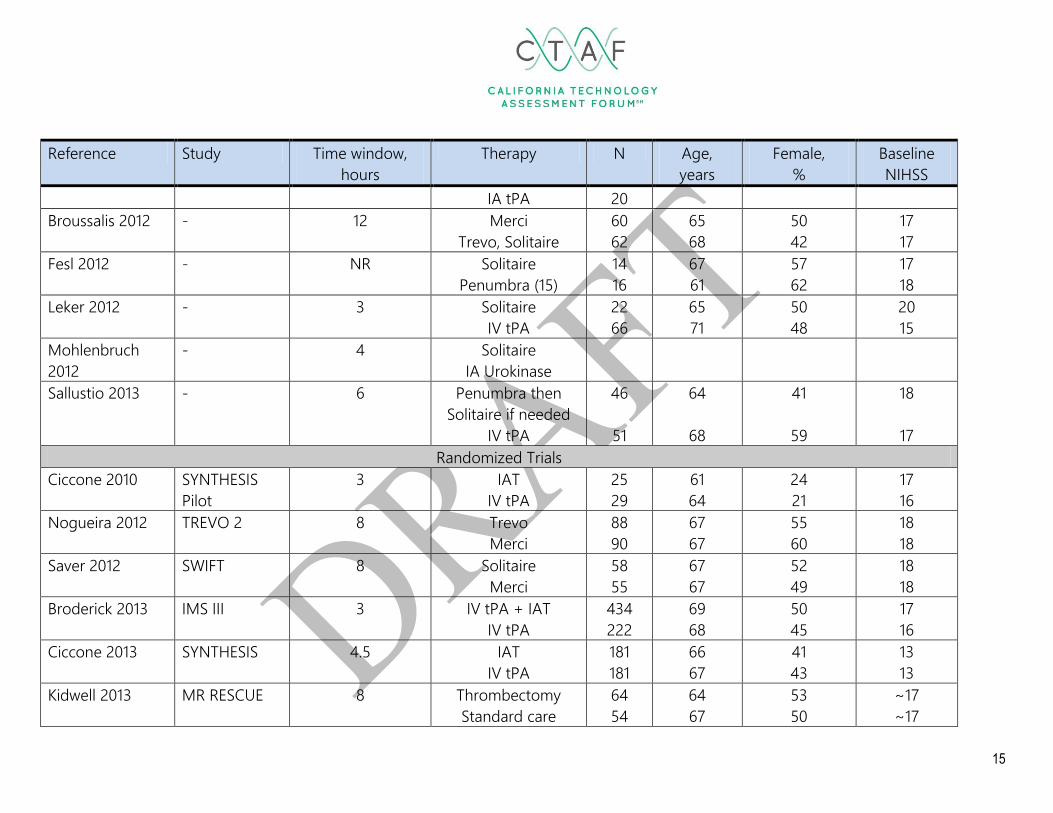
Reference Study Time window,
hours
Therapy N Age,
years
Female,
%
Baseline
NIHSS
IA tPA 20
Broussalis 2012 - 12 Merci
Trevo, Solitaire
60
62
65
68
50
42
17
17
Fesl 2012 - NR Solitaire
Penumbra (15)
14
16
67
61
57
62
17
18
Leker 2012 - 3 Solitaire
IV tPA
22
66
65
71
50
48
20
15
Mohlenbruch
2012
- 4 Solitaire
IA Urokinase
Sallustio 2013 - 6 Penumbra then
Solitaire if needed
IV tPA
46
51
64
68
41
59
18
17
Randomized Trials
Ciccone 2010 SYNTHESIS
Pilot
3 IAT
IV tPA
25
29
61
64
24
21
17
16
Nogueira 2012 TREVO 2 8 Trevo
Merci
88
90
67
67
55
60
18
18
Saver 2012 SWIFT 8 Solitaire
Merci
58
55
67
67
52
49
18
18
Broderick 2013 IMS III 3 IV tPA + IAT
IV tPA
434
222
69
68
50
45
17
16
Ciccone 2013 SYNTHESIS 4.5 IAT
IV tPA
181
181
66
67
41
43
13
13
Kidwell 2013 MR RESCUE 8 Thrombectomy
Standard care
64
54
64
67
53
50
~17
~17

16
Reference Study Time window,
hours
Therapy N Age,
years
Female,
%
Baseline
NIHSS
For comparison
Lees 2010 Pooled RCTs
of IV tPA
6 IV tPA
Placebo
1850
1820
66
66
40
40
11
11
IAT = intra-arterial therapy. In IMS III: Merci retriever, Penumbra System, Solitaire FR, or endovascular tPA; 170 patients were treated with at
least one of the devices. In SYNTHESIS: endovascular tPA with thrombus fragmentation with guidewire in all + 56 with an additional device
(Merci retriever, Penumbra System, Solitaire FR, Trevo).
17
Table 5: Primary outcomes in trials of thrombectomy devices
Reference Study Therapy N Time to
initiation,
min
Recanalization
Rate, %
7 day
mortality,
%
SICH,
%
90 day
good*
function,
%
90 day
Mortality,
%
Case series
Gobin 2004 MERCI 1 Merci 30 NR 60 NR 0 NR ≥ 36
Smith 2005 MERCI Merci 141 NR 46 NR 8 28 44
Kim 2006 - Merci 24 303 63 NR 8 25 29
Devlin 2007 - Merci 25 258 56 NR 4 24 36
Bose 2008 - Penumbra 23 NR 100 NR 10 NR ≥ 45
Smith 2008 Multi-
MERCI
Merci 164 258 68 NR 10 36 34
Grunwald 2009 - Penumbra 29 312 86 NR 7 38 ≥ 14
Hallevi 2009 Houston,
TX
UCLA
IAT
IAT
190
175
271
NR
66
NR
NR
NR
7
NR
NR
NR
NR
NR
Lee 2009 - Merci 17 318 71 NR 6 NR ≥ 24
Struffert 2009 - Penumbra 15 151 60 NR 0 33 20
Matthews 2009 - IAT, 52% Merci 94 NR 70 NR 5 37 27
Penumbra Inv.
2009
Pivotal Penumbra 125 258 82 NR 11 25 33
Abou-Chebl 2010 - IAT: 58%
Merci; 10%
Penumbra.
980 297 68 NR 9 37 31
Castano 2010 - Solitaire 20 352 90 NR 10 45 20
Kulcsar 2010 - Penumbra 27 266 93 NR 0 48 11

18
Reference Study Therapy N Time to
initiation,
min
Recanalization
Rate, %
7 day
mortality,
%
SICH,
%
90 day
good*
function,
%
90 day
Mortality,
%
Loh 2010 - Merci 106 384 NR NR 10 NR NR
Nayak 2010 - Solitaire 7 160 100 NR NR NR NR
Roth 2010 - Solitaire 22 277 91 18 18 50 23
Tarr 2010 POST Penumbra 157 270 87 NR 6 41 20
Brinjikji 2011 - Clot retrieval 3864 NR NR NR NR < 24 > 24
Costalat 2011 RECOST Solitaire 50 323 88 NR 2 54 12
Kang 2011 - Penumbra 22 318 82 NR 9 45 14
Menon 2011 - Penumbra 27 192 85 NR NR 48 19
Miteff 2011 - Solitaire 26 NR 96 NR 8 42 NR
Park 2011 - Solitaire 8 180 100 0 0 50 0
Roth 2011 - Penumbra 12 ~399 75 25 0 33 ≥ 33
Stampfl 2011 - Solitaire 18 241 89 NR NR 33 ≥ 28
Castro-Alfonso
2012
- Solitaire 21 296 90 NR 14 62 10
Cohen 2012 - Solitaire 17 NR 100 NR 6 88 6
Davalos 2012 - Solitaire 141 306 85 NR 4 55 20
Dorn 2012 - Solitaire 104 218 79 NR 2 NR NR
Gandini 2012 - Penumbra 18 288 83 NR NR 39 ≥17
Kim 2012 - Solitaire 23 204 91 NR NR NR NR
Machi 2012 - Solitaire 56 316 89 NR 2 46 ≥7
Mpotsaris 2012 - Solitaire 26 327 88 NR NR NR ≥ 8
Psychogios 2012 - Penumbra 91 235 77 NR 6 29 25
San Roman 2012 - Trevo 60 210 73 NR NR 45 28

19
Reference Study Therapy N Time to
initiation,
min
Recanalization
Rate, %
7 day
mortality,
%
SICH,
%
90 day
good*
function,
%
90 day
Mortality,
%
Frei 2013 SPEED Penumbra 86 306 91 NR 14 35 26
Mordasini 2013 Solitaire 14 414 100 NR 0 29 36
Comparative trials
Brekenfeld 2010 - Solitaire
Other IAT
17
23
NR
NR
94
78
NR
NR
NR
NR
43
52
NR
NR
Taschner 2011 - Penumbra
IA tPA
22
20
78
53
NR
NR
15
35
15
10
Broussalis 2012 - Merci
Trevo, Solitaire
60
62
266
210
62
82
NR
NR
28
10
25
59
30
10
Fesl 2012 - Solitaire
Penumbra (15)
14
16
238
273
93
56
NR
NR
0
0
45
33
NR
NR
Leker 2012 - Solitaire
IV tPA
22
66
234
134
95
NR
NR
NR
5
8
60
38
29
17
Mohlenbruch
2012
- Solitaire
IA Urokinase
25
62
88
53
60
40
Sallustio 2013 - Penumbra
then Solitaire if
needed
IV tPA
46
51
230
176
94
45
NR
NR
11
6
37
35
24
25
Randomized Trials
Ciccone 2010 SYNTHESIS
Pilot
IAT
IV tPA
25
29
195
155
NR
NR
20
14
8
14
48
28
NR
NR
Nogueira 2012 TREVO 2 Trevo 88 276 86 NR 7 40 33
20
Reference Study Therapy N Time to
initiation,
min
Recanalization
Rate, %
7 day
mortality,
%
SICH,
%
90 day
good*
function,
%
90 day
Mortality,
%
Merci 90 270 60 NR 9 22 24
Saver 2012 SWIFT Solitaire
Merci
58
55
294
320
69
30
NR
NR
2
11
58
33
36
49
Broderick 2013 IMS III IV tPA + IAT
IV tPA
434
222
249
NR
~75%
NA
12
11
6
6
41
39
19
22
Ciccone 2013 SYNTHESIS IAT
IV tPA
181
181
225
165
NR
NR
8
6
6
6
42
46
14
10
Kidwell 2013 MR
RESCUE
Thrombectomy
Standard care
64
54
381
NR
71**
87
NR
NR
5
4
19
20
19
24
For comparison
Lees 2010 Pooled
RCTs of IV
tPA
IV tPA
Placebo
1850
1820
233 NR
NR
NR
NR
5
1
42
35
14
12
* Good function is a modified Rankin Score ≤ 2 except the pooled IV tPA analysis (Lees 2010) where ≤ 1 was used.
** Measured by magnetic resonance angiography on day 7
IAT = intra-arterial therapy. In IMS III: Merci retriever, Penumbra System, Solitaire FR, or endovascular tPA; 170 patients were treated with at
least one of the devices. In SYNTHESIS: endovascular tPA with thrombus fragmentation with guidewire in all + 56 with an additional device
(Merci retriever, Penumbra System, Solitaire FR, Trevo).
21
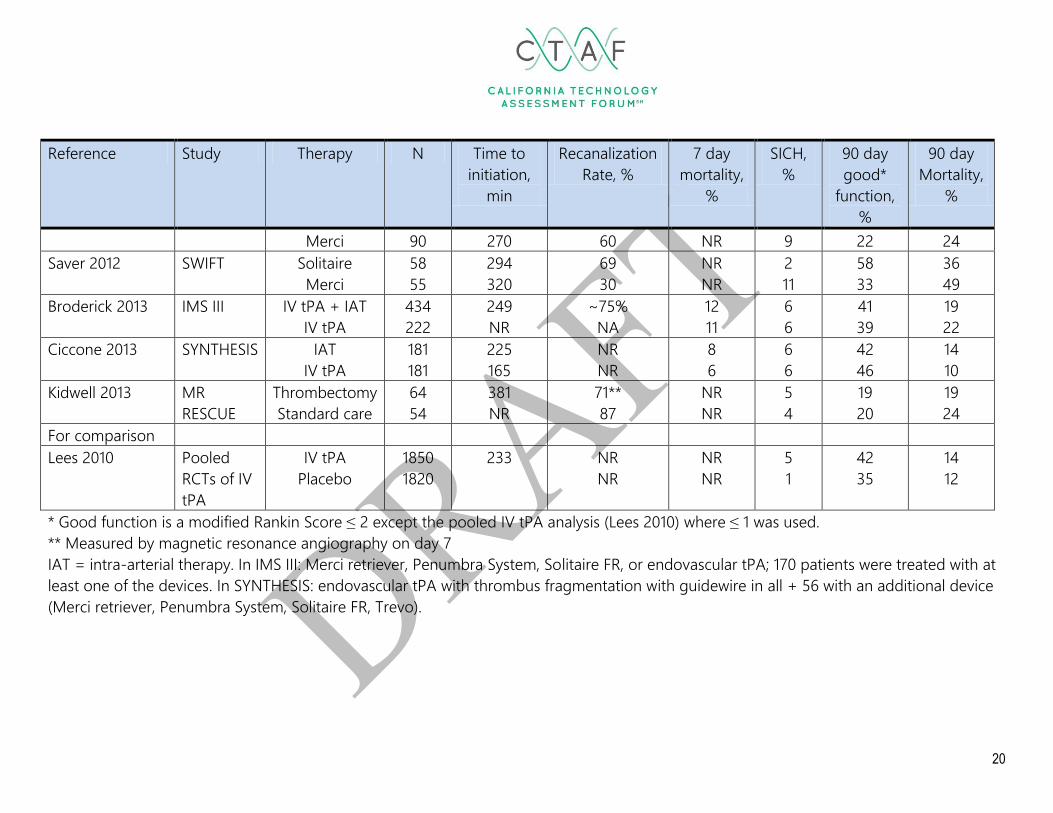
Comparative Trials
The seven comparative trials67-73 are summarized in Tables 4 and 5. Two
studies compared thrombectomy devices to IV tPA, two compared them to IA
thrombolytics, and three compared different thrombectomy devices. The largest
study had only 62 patients in one of the device arms and most only had about 20
patients. These sample sizes are too small to adequately control for selection bias
and confounding. Indeed, there are large differences in the baseline NIHSS score
and the age of the patients in the several of the comparative trials.
In the first two studies, patients treated with the Solitaire and Penumbra
devices had higher rates of recanalization of the target vessels than other intra-
arterial therapy, but patients treated with those devices had worse functional
outcomes at 90 days and higher mortality in the study of the Penumbra device.67,73
In the next study, the two clot retriever devices (Solitaire, Trevo) had higher rates of
recanalization than the Merci device and both better functional outcomes and
lower mortality at 90 days.68 It is noteworthy that the time to initiation of therapy
(arterial puncture) in this study was 46 minutes faster with the clot retrievers than
with the Merci device. This difference, which is not device dependent, could be the
explanation for the improved outcomes rather than anything inherent in the devices
themselves. The most recent study compared a group of patients treated with the
Penumbra device followed by the use of the Solitaire device if needed to a group of
patients treated with the current standard therapy, which is IV tPA. The group
treated with the thrombectomy devices had much higher rates of arterial
recanalization (94% versus 45%), but the differences in good function (37% versus
35%) and mortality (24% versus 25%) at 90 days were minimal.
22
It is difficult to draw firm conclusions from these small comparative trials.
However, a number of randomized trials have been published including several
relatively large trials. The assessment will focus on these randomized trials to better
understand the balance of benefits and harms from the thrombectomy devices
compared to standard IV thrombolytic therapy.
Randomized controlled trials
Two randomized trial comparing the newer stent retrievers to the Merci
device were published in the same issue of Lancet in October 2012.3,4 More
importantly three randomized trial were published online in the New England
Journal of Medicine comparing thrombectomy devices with and without IV tPA to
standard IV tPA therapy.5-7 One of the trials was specifically designed to determine
whether MRI findings differentiating between infarcted and ischemic brain tissue
could be used to identify subgroups of patients benefiting from the use of
thrombectomy devices.7 The trials are summarized in Tables 4 and 5.
The Trevo versus Merci retriever (TREVO 2) Trial
The TREVO 2 trial was a multi-center trial at 26 sites in the United States and
one in Spain.3 The study randomized patients between the ages of 18 and 85 years
who had large vessel strokes presenting within eight hours of symptom onset who
had NIHSS scores between eight and 29. The primary endpoint was recanalization
defined as a TICI score of two or greater using just the randomly assigned device.
The study randomized 88 patients to the Trevo group and 90 patients to the Merci
group. The groups were well matched: the mean age in both groups was 67 years
and their baseline NIHSS score was 18. The time to initiation of therapy was 276
minutes in the Trevo group and 270 minutes in the Merci group. The primary

23
recanalization endpoint was more common in the Trevo group (86% versus 60%,
p<0.0001). This was associated with improved function at 90 days (40% versus 22%,
p=0.013), though a trend towards greater mortality at 90 days (33% versus 24%,
p=0.18). The investigators defined a primary safety endpoint as a composite of
procedure-related adverse events including any vascular perforation or dissection,
symptomatic intracranial hemorrhage, embolization to a previously uninvolved
portion of the brain, access site complication requiring surgical repair or blood
transfusion, device failure, or peri-procedural mortality. There were no significant
differences between the groups in these complications (15% versus 23%, p=0.18),
although the trend favored the Trevo group. The magnitude of the procedure-
related adverse events is noteworthy. The TREVO 2 trial offers strong evidence that
the Trevo device provides superior revascularization than the Merci device and that
this improvement translates into improved functional outcomes without a higher
rate of device related complications or mortality. The sample size is relatively small
and the confidence intervals are relatively wide. As suggested by the FDA with the
original PROACT II trial, a second randomized trial would make these results
convincing.
The Solitaire With the Intention For Thrombectomy (SWIFT) Trial
The SWIFT trial was a multi-center trial at 18 sites in the United States and
one in France.4,78 The study randomized patients between the ages of 22 and 85
years who had large vessel strokes presenting within eight hours of symptom onset
who had NIHSS scores between eight and 30. The primary endpoint was
recanalization defined as a TIMI score of two or greater in all treatable vessels
without SICH. The study randomized 58 patients to the Solitaire group and 55
patients to the Merci group. The groups were well matched: the mean age in both

24
groups was 67 years and their baseline NIHSS score was 18. The time to initiation of
therapy was 294 minutes in the Solitaire group and 320 minutes in the Merci group.
The primary recanalization endpoint was more common in the Solitaire group (69%
versus 30%, p<0.0001). This was associated with improved function at 90 days (58%
versus 33%, p=0.017) and lower mortality at 90 days (17% versus 38%, p=0.02).
There were no significant differences between the groups in study device-related
serious adverse events (9% versus 16%, p=0.26) or procedure-related serious
adverse events (14% versus 16%, p=1.00), although the trends favored the Solitaire
group. Serious adverse events were common with both devices. As with the TREVO
2 trial, the SWIFT offers strong evidence that the Solitaire device provides superior
revascularization than the Merci device and that this improvement translates into
improved functional outcomes without a higher rate of device related complications
or mortality. The sample size is relatively small and the confidence intervals are
relatively wide. Taken together, the TREVO 2 and SWIFT trials provide convincing
evidence that the stent retriever design is an improvement on the Merci retriever
design.
The Interventional Management of Stroke III (IMS III) Trial
The IMS III trial was a multi-center, NIH-funded trial at 58 sites in the United
States, Canada, Australia, and Europe.5,76 It was stopped early because of futility –
the inability to demonstrate a significant difference between the study groups –
after 656 of the planned 900 participants had been randomized. The study
randomized patients between the ages of 18 and 80 years who had ischemic strokes
presenting within three hours of symptom onset who had NIHSS scores greater
than or equal to eight. The primary endpoint was good functional outcome at 90
days defined by mRS ≤ 2. The study randomized 434 patients to a combined IV/IA

25
therapy group and 55 patients to the standard IV tPA group. Participants in both
groups received standard dose IV tPA as soon as possible after randomization. The
combined IV/IA group underwent angiography as soon as possible, followed by IA
therapy at the discretion of the site neurointerventionalist (Merci, Penumbra,
Solitaire, or intra-arterial tPA with or without the MicrosSonic infusion system). In
the IV/IA group 164 participants were treated with intra-arterial tPA, 95 with the
Merci device, 54 with the Penumbra device, five with the Solitaire device, and 16
with multiple or other devices. The groups were reasonably well matched: the mean
age was 69 years in the IV/IA group and 68 years in the IV group. The baseline
NIHSS scores were 17 and 16 respectively. The only significant difference between
the two groups on 19 baseline characteristics was a lower proportion of patients in
the combined IV/IA group with a history of coronary artery disease (23% versus
32%, p=0.01). The time to initiation of intra-arterial therapy was 249 minutes in the
combined IV/IA group (122 minutes to IV tPA) and 121 minutes in the IV group. The
primary outcome, good function at 90 days, did not differ between the two groups
(41% versus 39%, p NR, 95% CI for the difference between the two groups -6.1% to
9.1%). There were no significant interactions identified on ten subgroup analyses.
There were also no significant differences in death within seven days (12% versus
11%, p=0.57) or death within 90 days (19% versus 22%, p=0.52). A total of 16% of
participants in the IV/IA group experienced device or procedure-related
complications including vessel perforation or dissection, embolization to an
uninvolved area of the brain, or groin hematoma.
The IMS III trial suggests that there is no important benefit to adding intra-
arterial therapy to IV tPA for patients presenting with a significant ischemic stroke
within three hours of symptom onset and about one in six of those patients
experienced a complication related to intra-arterial therapy. However, only about
26
half of the participants in the IV/IA group were treated with a thrombectomy device
and the vast majority of those participants were treated with the Merci device. As
noted above, the TREVO 2 and SWIFT trials provide convincing evidence that the
newer stent retriever devices are superior to the Merci device. Thus the IMS III trial
results may not apply to these newer devices.
The SYNTHESIS Pilot Trial
The SYNTHESIS Pilot trial75 was a multi-center trial at four sites in Italy that
formed the basis for the larger SYNTHESIS Extension trial6,74 described below. The
study randomized patients between the ages of 18 and 80 years who had ischemic
strokes presenting within three hours of symptom onset who had NIHSS scores less
than or equal to 25. The primary endpoint was good functional outcome at 90 days
defined by mRS ≤ 1. The study randomized 25 patients to an intra-arterial therapy
alone group (IAT) and 29 patients to the standard IV tPA group. The IAT group
underwent angiography as soon as possible, followed by IAT at the discretion of the
site neurointerventionalist (primarily intra-arterial tPA with mechanical clot
disruption followed by thrombectomy if necessary). The groups were reasonably
well matched: the mean age was 61 years in the IAT group and 64 years in the IV
group. The baseline NIHSS scores were 17 and 16 respectively. The investigators did
not report any significant differences between groups. The time from stroke onset
to randomization was 125 minutes in both groups. The median time from stroke
onset to IAT was 195 minutes and 155 minutes for IV therapy. The primary outcome,
good function at 90 days defined by the more stringent definition of mRS ≤ 1, did
not differ between the two groups (48% versus 28%, p adjusted for stroke severity
and age = 0.067), although the trend favored the IAT group. There were also no
significant differences in death within 90 days (20% versus 14%, p=0.72). This pilot
27
study was underpowered to detect significant differences, but the trend in the
primary outcome suggested potentially important benefits. It appeared that
thrombectomy devices were rarely used, but the details were not reported in the
primary journal article.
The SYNTHESIS Extension Trial
The SYNTHESIS Extension trial6,74 was a multi-center trial at 24 sites in Italy.
The study randomized patients between the ages of 18 and 80 years who had
ischemic strokes presenting within 4.5 hours of symptom onset who had NIHSS
scores less than or equal to 25. The primary endpoint was good functional outcome
at 90 days defined by mRS ≤ 1. The study randomized 181 patients to the IAT group
and 181 patients to the standard IV tPA group. The IAT group underwent
angiography as soon as possible, followed by IAT, which was primarily intra-arterial
tPA with mechanical clot disruption (109 participants) followed by thrombectomy if
necessary (56 participants). The thrombectomy devices used included Soliataire
(n=18), Penumbra (n=9), Trevo (n=5), and Merci (n=5). The groups were reasonably
well matched: the mean age was 66 years in the IA group and 67 years in the IV
group. The baseline NIHSS scores were 13 in both groups. Participants in the IAT
group were less likely to have atrial fibrillation (8% versus 16%, p=0.02) and more
likely to have dissection as the cause of their stroke (8% versus 2%, p=0.03). The
time from stroke onset to randomization was 148 minutes in the IAT group and 145
minutes in the IV group. The median time from stroke onset to IAT was 225 minutes
and 165 minutes for IV therapy. The primary outcome, good function at 90 days
defined by the more stringent definition of mRS ≤ 1, did not differ between the two
groups (35% versus 30%, p=0.37; p adjusted for age, sex, stroke severity and atrial

28
fibrillation at baseline = 0.16). There were also no significant differences in death
within seven days (8% versus 6%, p=0.53) or at 90 days (14% versus 10%, p=0.22).
The Synthesis Extension Trial suggests that there are no important
differences in stroke outcomes between primary IAT and IV tPA for patients
presenting within 4.5 hours of symptoms. As in the IMS III trial, only a minority of
patients in the IAT group were treated with a thrombectomy device, though in this
trial the newer devices were used more commonly than the older Merci device.
The Mechanical Retrieval and Recanalization of Stroke Clots Use Embolectomy (MR
RESCUE) trial
The final clinical trial (MR RESCUE) was a multi-center, NIH-funded trial at 22
sites in North America.7,77 The study was specifically designed to evaluate the utility
of the penumbral pattern in targeting patients for revascularization. The penumbral
pattern is identified using multimodal computed tomography (CT) or magnetic
resonance imaging (MRI) of the brain. If there is a small core of infarcted tissue and
a large surrounding area of potentially salvageable ischemic tissue, the pattern is
considered favorable for revascularization. On the other hand, if the pattern
suggests that there is a large area of infarction and little surrounding ischemic brain
tissue (also known as a non-penumbral pattern), then the hypothesis is that
revascularization will have little value. The study enrolled between the ages of 18
and 85 years who had large-vessel, anterior-circulation ischemic strokes presenting
within eight hours of symptom onset who had NIHSS scores between six and 29.
The primary endpoint was functional outcome at 90 days as measured by the mRS
across all levels (0 to 6). The study randomized patients to either thrombectomy
(Merci or Penumbral device) or standard care. The study randomized 127
participants, but nine participants did not meet the full eligibility requirements and
29
were excluded from the analysis. Randomization was stratified by the penumbral
pattern. Among the 64 patients in the thrombectomy group, 34 had a favorable
penumbral pattern and 30 had a non-penumbral pattern. Among the 53 patients in
the standard care group, 34 had a favorable penumbral pattern and 20 had a non-
penumbral pattern. The groups were reasonably well matched: the mean age was
66 years, 52% were women and 58% had a favorable penumbral pattern. The
baseline NIHSS scores varied by penumbral pattern (p<0.001). Participants with a
favorable penumbral pattern had a median NIHSS score of 16 in both the
thrombectomy and standard care groups. Participants with a non-penumbral
pattern in the thrombectomy group had a median NIHSS score of 19, while those in
the standard care group had a median score of 20.5. The time from symptom onset
to enrollment was 330 minutes with a trend towards short time in the
thrombectomy groups. The recanalization rate (TICI 2a or higher) was 67% in the
thrombectomy group. The primary outcome, good function at 90 days, did not
differ between the two groups overall (mRS 3.9 versus 3.9, p=0.99) or in the
subgroup with a favorable penumbral pattern (3.9 versus 3.4, p=0.233). There were
also no significant differences in death, SICH, or asymptomatic intra-cranial
hemorrhage. A total of 27% of participants in the thrombectomy group experienced
device or procedure-related; 8% experienced serious adverse events related to the
procedure.
The MR RESCUE trial found no benefit to thrombectomy compared to
standard care in patients with large-vessel anterior-circulation strokes presenting
within eight hours of symptom onset, despite a 67% rate of successful
revascularization. In addition, the study did not confirm the hypothesis that
penumbral imaging would identify a subgroup of patients who would benefit from
the use of thrombectomy devices. In contrast to the prior studies, thrombectomy
30
devices were used in all of the participants in the active treatment group. The
authors do not report the numbers, but imply that the majority of their patients
were treated with the Merci retriever. None of the patients were treated with the
newer stent retriever devices, so the results may not apply to that class of
thrombectomy devices.
Summary
Three randomized trials compared the use of intra-arterial therapy including
thrombectomy devices to standard care. Standard care included IV tPA for patients
presenting within 4.5 hours of symptom onset. The IMS III trial compared IAT plus
IV tPA to IV tPA within three hours of symptom onset; the SYNTHESIS trial
compared IAT alone to IV tPA within 4.5 hours of symptom onset, and the MR
RESCUE trial compared thrombectomy with either the Merci or Penumbra device to
standard care within eight hours of symptom onset. There was no benefit to intra-
arterial therapy in any of the studies including the subset of patients with significant
amounts of potentially salvageable ischemic brain tissue seen on brain imaging
prior to the intervention. All of the trials reported significant adverse events related
to the intra-arterial procedure in a clinical important proportion of the treated
patients. With no net benefit and clearly demonstrated harms, TA criterion 3 is not
met.
There are two important caveats to this conclusion. First, in IMS III and
SYNTHESIS, the majority of the participants in the active treatment group were not
treated with thrombectomy devices. Second, the Merci device was most commonly
used and the newer stent retriever devices were less commonly studied. Given the
favorable outcomes in both the TREVO 2 and SWIFT studies, the stent retrievers
may have a role in the treatment of acute ischemic strokes. However, additional

31
randomized trials are needed comparing them to the current standard therapy in
order to define what role they have to play in improving patient outcomes.
TA Criterion 3 is not met.
TA Criterion 4: The technology must be as beneficial as any established
alternatives.
The established therapy for patients presenting with an acute stroke within
three to four and a half hours of symptom onset is IV tPA. There is no established
alternative outside the 4.5 hour window. As noted above under TA 3, the
randomized trials comparing thrombectomy devices to IV tPA demonstrated harms
associated with the use of thrombectomy devices and no net benefits. Thus TA
criterion 4 is not met.
TA Criterion 4 is not met.
TA Criterion 5: The improvement must be attainable outside of the
investigational setting.
In order to successfully use the thrombectomy devices, physicians must have
training and experience in both intra-arterial catheter manipulation and
neuroradiology. Each of the manufacturers has specific recommendations for
training and proctoring with their system. There is intense interest in the use of
these devices and most established stroke centers have trained physicians who are

32
skilled in the use of these devices. The large number of centers involved in the
randomized trials suggests that appropriate training and credentialing is feasible.
However, the utility of thrombectomy devices has not yet been
demonstrated in the investigational setting, so no conclusions can be reached
about the effectiveness of the device in the community setting. Given the
specialized imaging involved and the potential for serious adverse events, it is likely
that the use of such devices should be limited to centers of excellence.13
TA Criterion 5 is not met.
33
CONCLUSION
Strokes are common in the United States: there are approximately 795,000
new strokes annually and there are more than 6.8 million stroke survivors with
varying degrees of disability.8 Recanalization of the occluded artery is the only
effective therapy for acute stroke, but it must happen quickly in order to have good
long-term outcomes. A recent pooled analysis of the trials of IV thrombolysis
reported that the benefits outweigh the risks for patients treated within 4.5 hours of
stroke onset, but beyond 4.5 hours the harms might outweigh the benefits.15 The
best outcomes are for patients treated within three hours of stroke onset. The FDA
indication restricts the use of IV tPA to patients presenting within three hours, but
the 2013 guidelines from the American Hearth Association and American Stroke
Association recommend its use for patients presenting within 4.5 hours.13 The
PROACT II trial demonstrated that intra-arterial therapy with prourokinase improved
recanalization rates and long-term functional outcomes without increasing
mortality, although it did increase the rate of symptomatic intracranial
hemorrhage.19 Subsequently, it was theorized that mechanical thrombectomy could
more effectively recanalize the blocked artery with a lower risk of SICH than
thrombolytic drugs, and this should translate into better outcomes. The downside
of endovascular therapy is the need for angiography and intra-arterial
microcatheter placement prior to treatment, which may delay the delivery of
effective therapy compared to IV thrombolysis. Since the approval of the first
mechanical thrombectomy device, the Merci Retriever, the use of thrombectomy
devices has increased exponentially in the United States.2
The prospect of opening up occluded intra-cerebral arteries with
thrombectomy devices is promising and has precedent in the coronary artery
vasculature where primary PTCA has become first line therapy over thrombolysis at

34
centers where endovascular treatments can be deployed rapidly. There is now a
large literature on the four thrombectomy devices that have received FDA approval.
Our literature search identified 39 case series, seven non-randomized comparative
studies, and six randomized trials. Three key randomized trials comparing
endovascular therapy to standard care were published online in February 2013. The
IMS III trial randomized 656 patients presenting within three hours of symptom
onset to the combination of IV tPA plus intra-arterial therapy including mechanical
thrombectomy or IV tPA alone.5 The combination therapy recanalized
approximately 75% of the occluded arteries, but there was no improvement in long
term functional outcomes. The SYNTHESIS extension trial randomized 362 patients
presenting within 4.5 hours of symptom onset to either intra-arterial therapy or IV
tPA.6 Again, there was no advantage to intra-arterial therapy. Finally, the MR
RESCUE study compared thrombectomy to standard care and found no benefit to
the more aggressive therapy, even in the subgroup with brain imaging suggestive
of a large area of ischemic tissue that could benefit from revacularization.7 The
randomized trials together demonstrate no benefit from intra-arterial therapy,
including thrombectomy devices, and significant procedure-related adverse events.
Thus, thrombectomy devices should not be used routinely at this time.
Two other randomized trials, TREVO 2 and SWIFT, found that the newer
stent retrieval devices had higher recanalization rates and that this translated into
better functional outcomes. These devices were underrepresented in the earlier
randomized trials and may have a role in the treatment of acute stroke. However
randomized trials are needed to define the population of patients who may benefit
from these new devices.

35
DRAFT RECOMMENDATION
It is recommended that the use of the thrombectomy devices does
not meet Technology Assessment Criteria 3 through 5 for safety,
effectiveness and improvement in health outcomes when used to treat acute
ischemic stroke.
March 6, 2013

36
RECOMMENDATIONS OF OTHERS
Blue Cross Blue Shield Association (BCBSA)
The BCBSA Technology Evaluation Center has not conducted a review of this
device.
Centers For Medicare And Medicaid Services (CMS)
In 2006, CMS approved a new ICD-9 Procedure Code for ischemic stroke
patients treated with the Merci Retriever. Neither a National Coverage Decision nor
a Local Coverage Decision was found.
Canadian Agency for Drugs and Technologies in Health (CADTH)
CADTH performed a high level review of the Merci Retrieval device in 2005 on
its emerging technology list. There were no updated reviews of thrombectomy
associated devices found on the website.
Institute for Clinical and Economic Review (ICER)
No reviews or appraisals were found on the ICER website.
National Institute for Health and Clinical Excellence (NICE)
Though guidelines on stroke were found, they did not mention
thrombectomy devices.
CONSENSUS Guidelines
1. Multisociety Consensus Quality Improvement Guidelines for Intraarterial
Catheter-directed Treatment of Acute Ischemic Stroke, from the American
37
Society of Neuroradiology, Canadian Interventional Radiology Association,
Cardiovascular and Interventional Radiological Society of Europe, Society for
Cardiovascular Angiography and Interventions, Society of Interventional
Radiology, Society of NeuroInterventional Surgery, European Society of
Minimally Invasive Neurological Therapy, and Society of Vascular and
Interventional Neurology
This guideline was published in February 2013 and defines processes
and benchmarks to maximize outcomes in acute stroke revascularization.
2. Guidelines for the Early Management of Patients With Acute Ischemic
Stroke: A Guideline for Healthcare Professionals From the American Heart
Association/American Stroke Association
This guideline was published online on January 31, 2013 and provides
an overview of the evidence and management recommendations of patients
with acute ischemic stroke. The guideline provides information on clinical
study outcomes of the four FDA approved devices used in thrombectomy in
ischemic stroke and makes the following recommendations relative to these
devices under the section titled, “Endovascular Interventions”.:
#5 When mechanical thrombectomy is pursued, stent retrievers such as
Solitaire FR and Trevo are generally preferred to coil retrievers such as Merci
(Class I; Level of Evidence A). The relative effectiveness of the Penumbra
System versus stent retrievers is not yet characterized. (New
recommendation)
#6 The Merci, Penumbra System, Solitaire FR, and Trevo thrombectomy
devices can be useful in achieving recanalization alone or in combination
with pharmacological fibrinolysis in carefully selected patients (Class IIa; Level
38
of Evidence B). Their ability to improve patient outcomes has not yet been
established. These devices should continue to be studied in randomized
controlled trials to determine the efficacy of such treatments in improving
patient outcomes.
#8 Rescue intra-arterial fibrinolysis or mechanical thrombectomy may be
reasonable approaches to recanalization in patients with large-artery
occlusion who have not responded to intravenous fibrinolysis. Additional
randomized trial data are needed (Class IIb; Level of Evidence B). (New
recommendation)
#9 The usefulness of mechanical thrombectomy devices other than the
Merci retriever, the Penumbra System, Solitaire FR, and Trevo is not well
established (Class IIb; Level of Evidence C). These devices should be used in
the setting of clinical trials.
Agency for Healthcare Research and Quality (AHRQ)
No reviews or assessments were found on this topic on the website
Washington State Heath Care Authority
No technology assessments were found on this topic on the website.
American College of Cardiology, CA Chapter (ACC-CA)
ACC-CA was invited to provide an opinion on this technology and to send a
representative to the meeting.
American Academy of Neurology (AAN)

39
AAN was invited to provide an opinion on this technology and to send a
representative to the meeting.
American Society of Neuroradiology(ASN)
ASN was invited to provide an opinion on this technology and to send a
representative to the meeting.
National Stroke Association (NSA)
NSA was invited to provide an opinion on this technology and to send a
representative to the meeting.
The Society for Cardiac Angiography and Interventions (SCAI)
SCAI was invited to provide an opinion on this technology and to send a
representative to the meeting.
Society for Interventional Radiology (SIR)
SIR was invited to provide an opinion on this technology and to send a
representative to the meeting.
Society of NeuroInterventional Surgery (SNS)
SNS was invited to provide an opinion on this technology and to send a
representative to the meeting.
Society of Critical Care Medicine (SCCM)
SCCM was invited to provide an opinion on this technology and to send a
representative to participate at the CTAF public meeting.
40
ABBREVIATIONS USED IN THIS REVIEW
CT Computed tomography
DARE Database of Abstracts of Reviews of Effects
IA Intra-arterial
IAT Intra-arterial therapy
ICA Intracranial carotid artery
IMS III International Management of Stroke Trial 3
IV Intravenous
tPA Tissue plasminogen activator
NIHSS National Institutes of Health Stroke Survey
MCA Middle cerebral artery
MERCI Mechanical Embolus Removal in Cerebral Ischemia
M1 First division
M2 Second division
MRI Magnetic Resonance Imaging
MR Rescue MR and Recanalization of Stroke Clots Using Embolectomy trial
mRS Modified Rankin Scale
NIH National Institutes of Health
NIHSS National Institutes of Health Stroke Survey (NIHSS)
NS Not significant
PROACT II Prolyse in Acute Cerebral Thromboembolism II trial
PTCA Percutaneous Transluminal Coronary Angioplasty
SICH Symptomatic intracranial hemorrhage
TIMI Thrombolysis in Myocardial Infarction (TIMI) Flow Grading System
TICI Thrombolysis in Cerebral Infarction Score

41
REFERENCES
1. Tice JA. Use of the Merci Retriever for the emergent treatment of acute
ischemic stroke a technology assessment. San Francisco, Calif.: California
Technology Assessment Forum,; 2007:
http://www.ctaf.org/sites/default/files/assessments/770_file_MERCI1_W.pdf.
2. Brinjikji W, Rabinstein AA, Kallmes DF, Cloft HJ. Patient outcomes with
endovascular embolectomy therapy for acute ischemic stroke: a study of the
national inpatient sample: 2006 to 2008. Stroke. Jun 2011;42(6):1648-1652.
3. Nogueira RG, Lutsep HL, Gupta R, et al. Trevo versus Merci retrievers for
thrombectomy revascularisation of large vessel occlusions in acute ischaemic
stroke (TREVO 2): a randomised trial. Lancet. Oct 6 2012;380(9849):1231-1240.
4. Saver JL, Jahan R, Levy EI, et al. Solitaire flow restoration device versus the
Merci Retriever in patients with acute ischaemic stroke (SWIFT): a
randomised, parallel-group, non-inferiority trial. Lancet. Oct 6
2012;380(9849):1241-1249.
5. Broderick JP, Palesch YY, Demchuk AM, et al. Endovascular Therapy after
Intravenous t-PA versus t-PA Alone for Stroke. The New England journal of
medicine. Feb 7 2013.
6. Ciccone A, Valvassori L, Nichelatti M, et al. Endovascular Treatment for Acute
Ischemic Stroke. The New England journal of medicine. Feb 6 2013.
7. Kidwell CS, Jahan R, Gornbein J, et al. A Trial of Imaging Selection and
Endovascular Treatment for Ischemic Stroke. The New England journal of
medicine. Feb 8 2013.
8. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics--
2013 update: a report from the American Heart Association. Circulation. Jan 1
2013;127(1):e6-e245.
9. Broderick JP. Recanalization therapies for acute ischemic stroke. Seminars in
neurology. 1998;18(4):471-484.

42
10. Costalat V, Lobotesis K, Machi P, et al. Prognostic factors related to clinical
outcome following thrombectomy in ischemic stroke (RECOST study). 50
patients prospective study. Eur J Radiol. Dec 2012;81(12):4075-4082.
11. Nogueira RG, Liebeskind DS, Sung G, Duckwiler G, Smith WS. Predictors of
good clinical outcomes, mortality, and successful revascularization in
patients with acute ischemic stroke undergoing thrombectomy: pooled
analysis of the Mechanical Embolus Removal in Cerebral Ischemia (MERCI)
and Multi MERCI Trials. Stroke. Dec 2009;40(12):3777-3783.
12. Wechsler LR, Roberts R, Furlan AJ, et al. Factors influencing outcome and
treatment effect in PROACT II. Stroke. May 2003;34(5):1224-1229.
13. Jauch EC, Saver JL, Adams HP, Jr., et al. Guidelines for the Early Management
of Patients With Acute Ischemic Stroke: A Guideline for Healthcare
Professionals From the American Heart Association/American Stroke
Association. Stroke; a journal of cerebral circulation. Jan 31 2013.
14. Tissue plasminogen activator for acute ischemic stroke. The National Institute
of Neurological Disorders and Stroke rt-PA Stroke Study Group. The New
England journal of medicine. Dec 14 1995;333(24):1581-1587.
15. Lees KR, Bluhmki E, von Kummer R, et al. Time to treatment with intravenous
alteplase and outcome in stroke: an updated pooled analysis of ECASS,
ATLANTIS, NINDS, and EPITHET trials. Lancet. May 15 2010;375(9727):1695-
1703.
16. Wardlaw JM, Zoppo G, Yamaguchi T, Berge E. Thrombolysis for acute
ischaemic stroke. Cochrane Database Syst Rev. 2003(3):CD000213.
17. Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a
meta-analysis. Stroke. Mar 2007;38(3):967-973.
18. Thomassen L, Bakke SJ. Endovascular reperfusion therapy in acute ischaemic
stroke. Acta Neurol Scand Suppl. 2007;187:22-29.
19. Furlan A, Higashida R, Wechsler L, et al. Intra-arterial prourokinase for acute
ischemic stroke. The PROACT II study: a randomized controlled trial. Prolyse
in Acute Cerebral Thromboembolism. Jama. Dec 1 1999;282(21):2003-2011.

43
20. Ciccone A, Sterzi R. Randomised trials of endovascular treatment of stroke
are needed. Lancet Neurol. Jan 2010;9(1):30; author reply 31-32.
21. Ciccone A, Valvassori L, Gasparotti R, Scomazzoni F, Ballabio E, Sterzi R.
Debunking 7 myths that hamper the realization of randomized controlled
trials on intra-arterial thrombolysis for acute ischemic stroke. Stroke. Jul
2007;38(7):2191-2195.
22. Mullen MT, Pisapia JM, Tilwa S, Messe SR, Stein SC. Systematic review of
outcome after ischemic stroke due to anterior circulation occlusion treated
with intravenous, intra-arterial, or combined intravenous+intra-arterial
thrombolysis. Stroke. Sep 2012;43(9):2350-2355.
23. Tomsick TA, Khatri P, Jovin T, et al. Equipoise among recanalization
strategies. Neurology. Mar 30 2010;74(13):1069-1076.
24. The penumbra pivotal stroke trial: safety and effectiveness of a new
generation of mechanical devices for clot removal in intracranial large vessel
occlusive disease. Stroke. Aug 2009;40(8):2761-2768.
25. Abou-Chebl A, Lin R, Hussain MS, et al. Conscious sedation versus general
anesthesia during endovascular therapy for acute anterior circulation stroke:
preliminary results from a retrospective, multicenter study. Stroke. Jun
2010;41(6):1175-1179.
26. Bose A, Henkes H, Alfke K, et al. The Penumbra System: a mechanical device
for the treatment of acute stroke due to thromboembolism. AJNR Am J
Neuroradiol. Aug 2008;29(7):1409-1413.
27. Castano C, Dorado L, Guerrero C, et al. Mechanical thrombectomy with the
Solitaire AB device in large artery occlusions of the anterior circulation: a
pilot study. Stroke. Aug 2010;41(8):1836-1840.
28. Castro-Afonso LH, Abud TG, Pontes-Neto OM, et al. Mechanical
thrombectomy with solitaire stent retrieval for acute ischemic stroke in a
Brazilian population. Clinics (Sao Paulo). Dec 2012;67(12):1379-1386.
29. Cohen JE, Gomori JM, Leker RR, Moscovici S, Ramirez-Denoriega F, Itshayek
E. Recanalization with stent-based mechanical thrombectomy in anterior
circulation major ischemic stroke. J Clin Neurosci. Jan 2012;19(1):39-43.

44
30. Costalat V, Machi P, Lobotesis K, et al. Rescue, combined, and stand-alone
thrombectomy in the management of large vessel occlusion stroke using the
solitaire device: a prospective 50-patient single-center study: timing, safety,
and efficacy. Stroke. Jul 2011;42(7):1929-1935.
31. Davalos A, Pereira VM, Chapot R, Bonafe A, Andersson T, Gralla J.
Retrospective multicenter study of Solitaire FR for revascularization in the
treatment of acute ischemic stroke. Stroke. Oct 2012;43(10):2699-2705.
32. Devlin TG, Baxter BW, Feintuch TA, Desbiens NA. The Merci Retrieval System
for acute stroke: the Southeast Regional Stroke Center experience. Neurocrit
Care. 2007;6(1):11-21.
33. Dorn F, Stehle S, Lockau H, Zimmer C, Liebig T. Endovascular treatment of
acute intracerebral artery occlusions with the solitaire stent: single-centre
experience with 108 recanalization procedures. Cerebrovasc Dis.
2012;34(1):70-77.
34. Frei D, Gerber J, Turk A, et al. The SPEED study: initial clinical evaluation of
the Penumbra novel 054 Reperfusion Catheter. J Neurointerv Surg. Jan 7
2013.
35. Gandini R, Pampana E, Del Giudice C, et al. Acute stroke treatment using the
Penumbra endovascular mechanical thrombolysis device: a single-centre
experience. Radiol Med. Oct 2012;117(7):1199-1214.
36. Gobin YP, Starkman S, Duckwiler GR, et al. MERCI 1: a phase 1 study of
Mechanical Embolus Removal in Cerebral Ischemia. Stroke. Dec
2004;35(12):2848-2854.
37. Grunwald IQ, Walter S, Papanagiotou P, et al. Revascularization in acute
ischaemic stroke using the penumbra system: the first single center
experience. Eur J Neurol. Nov 2009;16(11):1210-1216.
38. Hallevi H, Barreto AD, Liebeskind DS, et al. Identifying patients at high risk
for poor outcome after intra-arterial therapy for acute ischemic stroke.
Stroke. May 2009;40(5):1780-1785.
39. Kang DH, Hwang YH, Kim YS, Park J, Kwon O, Jung C. Direct thrombus
retrieval using the reperfusion catheter of the penumbra system: forced-

45
suction thrombectomy in acute ischemic stroke. AJNR Am J Neuroradiol. Feb
2011;32(2):283-287.
40. Kim D, Jahan R, Starkman S, et al. Endovascular mechanical clot retrieval in a
broad ischemic stroke cohort. AJNR Am J Neuroradiol. Nov-Dec
2006;27(10):2048-2052.
41. Kim JE, Kim AR, Paek YM, Cho YJ, Lee BH, Hong KS. Safety and efficacy of
mechanical thrombectomy with the Solitaire device in large artery occlusion.
Neurol India. Jul-Aug 2012;60(4):400-405.
42. Kim TK, Rhim JK, Lee CJ, Oh SH, Chung BS. The Limitations of Thrombectomy
with Solitaire AB as First-line Treatment in Acute Ischemic Stroke: A Single
Center Experience. J Cerebrovasc Endovasc Neurosurg. Sep 2012;14(3):203-
209.
43. Kulcsar Z, Bonvin C, Pereira VM, et al. Penumbra system: a novel mechanical
thrombectomy device for large-vessel occlusions in acute stroke. AJNR Am J
Neuroradiol. Apr 2010;31(4):628-633.
44. Lee W, Sitoh YY, Lim CC, Lim WE, Hui FK. The MERCI Retrieval System for the
management of acute ischaemic stroke--the NNI Singapore experience. Ann
Acad Med Singapore. Sep 2009;38(9):749-755.
45. Lin R, Vora N, Zaidi S, et al. Mechanical approaches combined with intra-
arterial pharmacological therapy are associated with higher recanalization
rates than either intervention alone in revascularization of acute carotid
terminus occlusion. Stroke; a journal of cerebral circulation. Jun
2009;40(6):2092-2097.
46. Loh Y, Jahan R, McArthur DL, et al. Recanalization rates decrease with
increasing thrombectomy attempts. AJNR Am J Neuroradiol. May
2010;31(5):935-939.
47. Loh Y, Kim D, Shi ZS, et al. Higher rates of mortality but not morbidity follow
intracranial mechanical thrombectomy in the elderly. AJNR Am J Neuroradiol.
Aug 2010;31(7):1181-1185.
48. Loh Y, Liebeskind DS, Towfighi A, et al. Preprocedural basal ganglionic
infarction increases the risk of hemorrhagic transformation but not worse

46
outcome following successful recanalization of acute middle cerebral artery
occlusions. World Neurosurg. Dec 2010;74(6):636-640.
49. Machi P, Costalat V, Lobotesis K, et al. Solitaire FR thrombectomy system:
immediate results in 56 consecutive acute ischemic stroke patients. J
Neurointerv Surg. Jan 1 2012;4(1):62-66.
50. Mathews MS, Sharma J, Snyder KV, et al. Safety, effectiveness, and
practicality of endovascular therapy within the first 3 hours of acute ischemic
stroke onset. Neurosurgery. Nov 2009;65(5):860-865; discussion 865.
51. Menon BK, Hill MD, Eesa M, et al. Initial experience with the Penumbra
Stroke System for recanalization of large vessel occlusions in acute ischemic
stroke. Neuroradiology. Apr 2011;53(4):261-266.
52. Miteff F, Faulder KC, Goh AC, Steinfort BS, Sue C, Harrington TJ. Mechanical
thrombectomy with a self-expanding retrievable intracranial stent (Solitaire
AB): experience in 26 patients with acute cerebral artery occlusion. AJNR Am
J Neuroradiol. Jun-Jul 2011;32(6):1078-1081.
53. Mordasini P, Brekenfeld C, Byrne JV, et al. Technical Feasibility and
Application of Mechanical Thrombectomy with the Solitaire FR
Revascularization Device in Acute Basilar Artery Occlusion. AJNR Am J
Neuroradiol. Jan 2013;34(1):159-163.
54. Mpotsaris A, Bussmeyer M, Loehr C, Oelerich M, Buchner H, Weber W.
Mechanical thrombectomy in severe acute stroke: preliminary results of the
Solitaire stent. J Neurol Neurosurg Psychiatry. Jan 2012;83(1):117-118.
55. Nayak S, Ladurner G, Killer M. Treatment of acute middle cerebral artery
occlusion with a Solitaire AB stent: preliminary experience. Br J Radiol. Dec
2010;83(996):1017-1022.
56. Park H, Hwang GJ, Jin SC, et al. A retrieval thrombectomy technique with the
Solitaire stent in a large cerebral artery occlusion. Acta Neurochir (Wien). Aug
2011;153(8):1625-1631.
57. Psychogios MN, Kreusch A, Wasser K, Mohr A, Groschel K, Knauth M.
Recanalization of large intracranial vessels using the penumbra system: a
single-center experience. AJNR Am J Neuroradiol. Sep 2012;33(8):1488-1493.

47
58. Roth C, Mielke A, Siekmann R, Ferbert A. First experiences with a new device
for mechanical thrombectomy in acute basilar artery occlusion. Cerebrovasc
Dis. 2011;32(1):28-34.
59. Roth C, Papanagiotou P, Behnke S, et al. Stent-assisted mechanical
recanalization for treatment of acute intracerebral artery occlusions. Stroke.
Nov 2010;41(11):2559-2567.
60. San Roman L, Obach V, Blasco J, et al. Single-center experience of cerebral
artery thrombectomy using the TREVO device in 60 patients with acute
ischemic stroke. Stroke. Jun 2012;43(6):1657-1659.
61. Shrivastava M, Lahoti S, Sanghvi D, Aggarwal A, Hastak S. Stand alone
mechanical thrombectomy (with penumbra system) for acute ischemic stroke
based on MR imaging: Single center experience. Neurol India. Jul-Aug
2012;60(4):406-414.
62. Smith WS, Sung G, Saver J, et al. Mechanical thrombectomy for acute
ischemic stroke: final results of the Multi MERCI trial. Stroke. Apr
2008;39(4):1205-1212.
63. Smith WS, Sung G, Starkman S, et al. Safety and efficacy of mechanical
embolectomy in acute ischemic stroke: results of the MERCI trial. Stroke. Jul
2005;36(7):1432-1438.
64. Stampfl S, Hartmann M, Ringleb PA, Haehnel S, Bendszus M, Rohde S. Stent
placement for flow restoration in acute ischemic stroke: a single-center
experience with the Solitaire stent system. AJNR Am J Neuroradiol. Aug
2011;32(7):1245-1248.
65. Struffert T, Kohrmann M, Engelhorn T, et al. Penumbra Stroke System as an
"add-on" for the treatment of large vessel occlusive disease following
thrombolysis: first results. Eur Radiol. Sep 2009;19(9):2286-2293.
66. Tarr R, Hsu D, Kulcsar Z, et al. The POST trial: initial post-market experience
of the Penumbra system: revascularization of large vessel occlusion in acute
ischemic stroke in the United States and Europe. J Neurointerv Surg. Dec
2010;2(4):341-344.
48
67. Brekenfeld C, Schroth G, Mordasini P, et al. Impact of retrievable stents on
acute ischemic stroke treatment. AJNR Am J Neuroradiol. Aug
2011;32(7):1269-1273.
68. Broussalis E, Trinka E, Hitzl W, Wallner A, Chroust V, Killer-Oberpfalzer M.
Comparison of Stent-Retriever Devices versus the Merci Retriever for
Endovascular Treatment of Acute Stroke. AJNR Am J Neuroradiol. Jul 12 2012.
69. Fesl G, Patzig M, Holtmannspoetter M, et al. Endovascular mechanical
recanalisation after intravenous thrombolysis in acute anterior circulation
stroke: the impact of a new temporary stent. Cardiovasc Intervent Radiol. Dec
2012;35(6):1326-1331.
70. Leker RR, Eichel R, Gomori JM, Ramirez de Noriega F, Ben-Hur T, Cohen JE.
Stent-based thrombectomy versus intravenous tissue plasminogen activator
in patients with acute middle cerebral artery occlusion. Stroke. Dec
2012;43(12):3389-3391.
71. Mohlenbruch M, Seifert M, Okulla T, et al. Mechanical thrombectomy
compared to local-intraarterial thrombolysis in carotid T and middle cerebral
artery occlusions: a single center experience. Clin Neuroradiol. Jun
2012;22(2):141-147.
72. Sallustio F, Koch G, Di Legge S, et al. Intra-arterial Thrombectomy versus
Standard Intravenous Thrombolysis in Patients with Anterior Circulation
Stroke Caused by Intracranial Arterial Occlusions: A Single-center Experience.
J Stroke Cerebrovasc Dis. Feb 1 2013.
73. Taschner CA, Treier M, Schumacher M, Berlis A, Weber J, Niesen W.
Mechanical thrombectomy with the Penumbra recanalization device in acute
ischemic stroke. J Neuroradiol. Mar 2011;38(1):47-52.
74. Ciccone A, Valvassori L, Nichelatti M. SYNTHESIS expansion: design of a
nonprofit, pragmatic, randomized, controlled trial on the best fast-track
endovascular treatment vs. standard intravenous alteplase for acute ischemic
stroke. Int J Stroke. Jun 2011;6(3):259-265.
75. Ciccone A, Valvassori L, Ponzio M, et al. Intra-arterial or intravenous
thrombolysis for acute ischemic stroke? The SYNTHESIS pilot trial. J
Neurointerv Surg. Mar 2010;2(1):74-79.

49
76. Khatri P, Hill MD, Palesch YY, et al. Methodology of the Interventional
Management of Stroke III Trial. Int J Stroke. May 2008;3(2):130-137.
77. Kidwell CS, Jahan R, Alger JR, et al. Design and rationale of the Mechanical
Retrieval and Recanalization of Stroke Clots Using Embolectomy (MR
RESCUE) Trial. Int J Stroke. Sep 13 2012.
78. Saver JL, Jahan R, Levy EI, et al. SOLITAIRE with the intention for
thrombectomy (SWIFT) trial: design of a randomized, controlled, multicenter
study comparing the SOLITAIRE Flow Restoration device and the MERCI
Retriever in acute ischaemic stroke. Int J Stroke. Nov 6 2012.
79. Brott T, Adams HP, Jr., Olinger CP, et al. Measurements of acute cerebral
infarction: a clinical examination scale. Stroke. Jul 1989;20(7):864-870.
80. Goldstein LB, Bertels C, Davis JN. Interrater reliability of the NIH stroke scale.
Archives of neurology. Jun 1989;46(6):660-662.
81. Lyden P, Brott T, Tilley B, et al. Improved reliability of the NIH Stroke Scale
using video training. NINDS TPA Stroke Study Group. Stroke. Nov
1994;25(11):2220-2226.
82. Lyden P, Lu M, Jackson C, et al. Underlying structure of the National
Institutes of Health Stroke Scale: results of a factor analysis. NINDS tPA
Stroke Trial Investigators. Stroke. Nov 1999;30(11):2347-2354.
83. The Thrombolysis in Myocardial Infarction (TIMI) trial. Phase I findings. TIMI
Study Group. The New England journal of medicine. Apr 4 1985;312(14):932-
936.
84. Higashida RT, Furlan AJ, Roberts H, et al. Trial design and reporting
standards for intra-arterial cerebral thrombolysis for acute ischemic stroke.
Stroke. Aug 2003;34(8):e109-137.