use of clomiphene citrate in in vitro fertilization (ivf) and ivf/intracytoplasmic sperm injection...
TRANSCRIPT

Use of clomiphene citrate in in vitro fertilization(IVF) and IVF/intracytoplasmic sperminjection cycles
Clomiphene citrate (CC) has been used for decades in ovulation induction and assisted reproduction. It hasbeen proven to be especially effective in the treatment of anovulatory patients and polycystic ovariansyndrome (PCOS), but has also been used—especially in the early years—for IVF cycles.
The main advantages of CC are its low price and the nearly negligible risk of ovarian hyperstimulationsyndrome (OHSS). The risk increases, however, when it is combined with gonadotropins. With the introduc-tion of GnRH agonists in the early 1980s (1), and later on with the use of GnRH antagonists, other protocolshave been proven to be much more effective in terms of oocytes retrieved and clinical pregnancy rates.
Edwards et al. (2), however, have called for a softer regimen of ovarian stimulation procedures, and wehave also supported this idea for many years because we think it is better to have more individualized insteadof standardized protocols. This idea has become more important since single ET has been shown to be veryeffective. Even before the establishment of general guidelines in Germany, our own data have shown that alower number of embryos transferred will not affect clinical pregnancy rates in selected groups of patients butwill lower the problems associated with high-order multiple births (3, 4).
The problems associated with CC also have to be taken into consideration: a possible risk of ovariancancer, its antiestrogenic effects on the endometrium, and the problem of premature LH surge. Even thoughit was not proven by other investigators (5), Rossing et al. (6) have shown that there might be a risk of ovariancancer after extensive use of CC for more than 12 treatment cycles. Therefore, 6 cycles is a reasonable limiton the use of this drug.
The antiestrogenic effect on the endometrium might be overcome by the adjunctive use of gonadotropins.This, however, will again raise the risk of a premature LH surge. On the other hand, we have shown that aspontaneous LH surge does not decrease the pregnancy rate in IVF patients (7), although other problems arisebecause of an untimed oocyte pickup (OPU).
The introduction of GnRH antagonists in the field of ovarian stimulation in the mid-1990s may againchange the problems associated with the use of CC. Now it should be possible to reliably prevent an earlyuntimed LH surge after the combined use of CC and gonadotropins (8, 9). GnRH antagonists may beadministered after a 5-day course of CC near the start of gonadotropins.
We have used such a protocol for a couple of years and have shown that there is no difference when usingthe CC/gonadotropin protocol with and without an antagonist in a prospective randomized study (10).
In normal cycling women (25–35 days), 100 mg CC were administered from day 5 to day 9, and from day9 an additional 150 IU of either hMG or FSH were given until the day of hCG administration (largest follicle�18 mm). From day 10 until the day of hCG administration, 0.25 mg of the antagonist was given s.c. daily(Munich protocol [MP]). Monitoring was performed after a learning curve in most cases only at day 12, andhCG was administered to more than 90% of patients on day 13 according to ultrasound results and E2 and P(and LH) levels.
In a 4-year period, from January 1998 to December 2001, we performed 6,530 cycles in our IVF program.From these cycles, 4,704 were treated by a conventional long luteal GnRH agonist protocol, 472 were treatedwith various protocols, and 1,354 were treated using our CC-gonadotropin-GnRH antagonist protocol (MP).
The choice of the protocol did not depend on a randomized schedule, but according to the German IVFregister (Deutsches IVF Register), all our IVF cycles have to be recorded prospectively 8 days before the dayof hCG administration, which means that all cycles canceled for whatever reason will also be registered as astarted cycle without OPU; therefore our study will give good comparable results.
The study was done on an individual basis outside any other study and without the influence ofpharmaceutical companies. We have used clomid stimulation in IVF stimulation protocols in about 20% of ouryearly cycles ever since the introduction of the agonists in the late 1980s because of our good experience, evenwith early LH surges (7).
Received January 7, 2003;revised and accepted April18, 2003.Reprint requests: KlausFiedler, M.D.,Kinderwunsch CentrumMunchen, Frauenklinik Dr.Wilhelm Krusmann,Bodenseestr. 7, D 81241,Munchen, Germany (FAX:49-89 820 99 142; E-mail:[email protected]).
FERTILITY AND STERILITY�VOL. 80, NO. 6, DECEMBER 2003Copyright ©2003 American Society for Reproductive MedicinePublished by Elsevier Inc.Printed on acid-free paper in U.S.A.
0015-0282/03/$30.00doi:10.1016/S0015-0282(03)02208-8
1521
CC/gonadotropin was used not only in young patients with noadditional factors besides tubal infertility, but also in patients athigh risk for severe OHSS because of previous history in othercenters, PCOS, or low budget and in patients with objections to“ too strong protocols.” Finally, we like the more physiologicalapproach compared with the down-regulation.
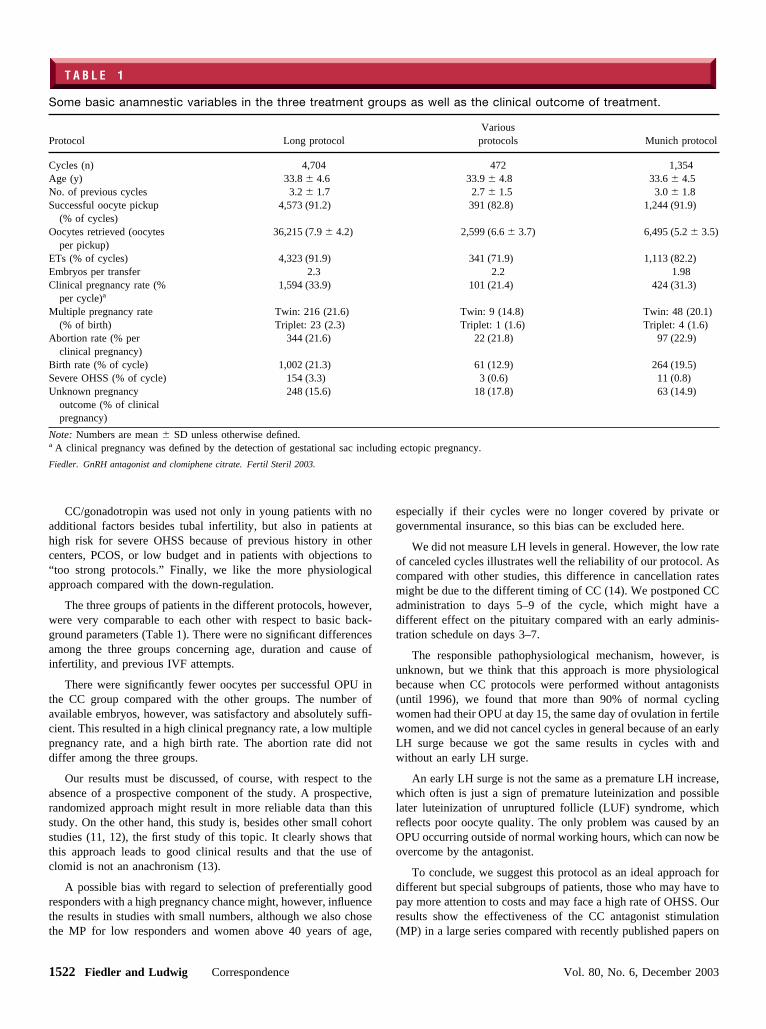
The three groups of patients in the different protocols, however,were very comparable to each other with respect to basic back-ground parameters (Table 1). There were no significant differencesamong the three groups concerning age, duration and cause ofinfertility, and previous IVF attempts.
There were significantly fewer oocytes per successful OPU inthe CC group compared with the other groups. The number ofavailable embryos, however, was satisfactory and absolutely suffi-cient. This resulted in a high clinical pregnancy rate, a low multiplepregnancy rate, and a high birth rate. The abortion rate did notdiffer among the three groups.
Our results must be discussed, of course, with respect to theabsence of a prospective component of the study. A prospective,randomized approach might result in more reliable data than thisstudy. On the other hand, this study is, besides other small cohortstudies (11, 12), the first study of this topic. It clearly shows thatthis approach leads to good clinical results and that the use ofclomid is not an anachronism (13).
A possible bias with regard to selection of preferentially goodresponders with a high pregnancy chance might, however, influencethe results in studies with small numbers, although we also chosethe MP for low responders and women above 40 years of age,
especially if their cycles were no longer covered by private orgovernmental insurance, so this bias can be excluded here.
We did not measure LH levels in general. However, the low rateof canceled cycles illustrates well the reliability of our protocol. Ascompared with other studies, this difference in cancellation ratesmight be due to the different timing of CC (14). We postponed CCadministration to days 5–9 of the cycle, which might have adifferent effect on the pituitary compared with an early adminis-tration schedule on days 3–7.
The responsible pathophysiological mechanism, however, isunknown, but we think that this approach is more physiologicalbecause when CC protocols were performed without antagonists(until 1996), we found that more than 90% of normal cyclingwomen had their OPU at day 15, the same day of ovulation in fertilewomen, and we did not cancel cycles in general because of an earlyLH surge because we got the same results in cycles with andwithout an early LH surge.
An early LH surge is not the same as a premature LH increase,which often is just a sign of premature luteinization and possiblelater luteinization of unruptured follicle (LUF) syndrome, whichreflects poor oocyte quality. The only problem was caused by anOPU occurring outside of normal working hours, which can now beovercome by the antagonist.
To conclude, we suggest this protocol as an ideal approach fordifferent but special subgroups of patients, those who may have topay more attention to costs and may face a high rate of OHSS. Ourresults show the effectiveness of the CC antagonist stimulation(MP) in a large series compared with recently published papers on
T A B L E 1
Some basic anamnestic variables in the three treatment groups as well as the clinical outcome of treatment.
Protocol Long protocolVarious
protocols Munich protocol
Cycles (n) 4,704 472 1,354Age (y) 33.8 � 4.6 33.9 � 4.8 33.6 � 4.5No. of previous cycles 3.2 � 1.7 2.7 � 1.5 3.0 � 1.8Successful oocyte pickup
(% of cycles)4,573 (91.2) 391 (82.8) 1,244 (91.9)
Oocytes retrieved (oocytesper pickup)
36,215 (7.9 � 4.2) 2,599 (6.6 � 3.7) 6,495 (5.2 � 3.5)
ETs (% of cycles) 4,323 (91.9) 341 (71.9) 1,113 (82.2)Embryos per transfer 2.3 2.2 1.98Clinical pregnancy rate (%
per cycle)a1,594 (33.9) 101 (21.4) 424 (31.3)
Multiple pregnancy rate(% of birth)
Twin: 216 (21.6)Triplet: 23 (2.3)
Twin: 9 (14.8)Triplet: 1 (1.6)
Twin: 48 (20.1)Triplet: 4 (1.6)
Abortion rate (% perclinical pregnancy)
344 (21.6) 22 (21.8) 97 (22.9)
Birth rate (% of cycle) 1,002 (21.3) 61 (12.9) 264 (19.5)Severe OHSS (% of cycle) 154 (3.3) 3 (0.6) 11 (0.8)Unknown pregnancy
outcome (% of clinicalpregnancy)
248 (15.6) 18 (17.8) 63 (14.9)
Note: Numbers are mean � SD unless otherwise defined.a A clinical pregnancy was defined by the detection of gestational sac including ectopic pregnancy.
Fiedler. GnRH antagonist and clomiphene citrate. Fertil Steril 2003.
1522 Fiedler and Ludwig Correspondence Vol. 80, No. 6, December 2003

the same issue but with much smaller numbers (11, 12). Whetherother selection criteria should be taken into account cannot beanswered with the present study design, but must be reserved forfurther analysis and studies.
Klaus Fiedler, M.D.a
Michael Ludwig, M.D.b
Kinderwunsch Centrum Munchen an der Frauenklinik Dr.Wilhelm Krusmann,a Munchen, and Centre forReproductive Medicine and Gynecologic Endocrinology,b
Endokrinologikum Hamburg, Hamburg, Germany
References1. Porter RN, Smith W, Craft IL, Ardulwahid NA, Jacobs HS. Induction
of ovulation for in-vitro fertilisation using buserelin and gonadotropins.Lancet 1984;2:1284–5.
2. Edwards RG, Lobo R, Bouchard P. Time to revolutionize ovarianstimulation [editorial]. Hum Reprod 1996;11:917–9.
3. Fiedler K, Krusmann G, von Hertwig I, Wurfel W. Peri- and postnataloutcome of 246 multiple pregnancies after IVF(ICSI) ET. J AssistReprod Genet (abstract) 1997;6:S92.
4. Ludwig M, Schopper B, Katalinic A, Sturm R, l-Hasani S, Diedrich K.Experience with the elective transfer of two embryos under the condi-tions of the German Embryo Protection Law: results of a retrospectivedata analysis of 2573 transfer cycles. Hum Reprod 2000;15:319–24.
5. Modan B, Ron E, Lerner-Geva L, Blumstein T, Menczer J, RabinoviciJ, et al. Cancer incidence in a cohort of infertile women. Am JEpidemiol 1998;147:1038–42.
6. Rossing MA, Daling JR, Weiss NS, Moore DE, Self SG. Ovariantumors in a cohort of infertile women. N Engl J Med 1994;331:771–6.
7. Fiedler K, Mueseler M, Schmidt H, Halbeisen S. Comparison of IVFresults in clomiphen citrate/hMG-treated women with and without aspontaneous luteinizing hormone surge. Hum Reprod (abstract) 1988;3:197.
8. Al-Inany H, Aboulghar M. GnRH antagonists in assisted conception: aCochrane review. Hum Reprod 2002;17:874–85.
9. Ludwig M, Katalinic A, Diedrich K. Use of GnRH antagonists inovarian stimulation for ART compared to the long protocol: a meta-analysis. Arch Gynecol Obstet 2001;265:175–82.
10. Fiedler K, Krusmann G, von Hertwig I, Schleyer M, Wurfel W. Com-parison of Clomid/FSH/HMG stimulation for IVF with and withoutGnRH antagonist. Hum Reprod (abstract) 2001;16:72.
11. Weigert M, Krischker U, Pohl M, Poschalko G, Kindermann C, Feich-tinger W. Comparison of stimulation with clomiphene in combinationwith recombinant follicle-stimulating hormone and recombinant lutein-izing hormone to stimulation with a gonadotropin-releasing hormoneagonist protocol: a prospective randomized study. Fertil Steril 2002;78:34–9.
12. Williams SC, Gibbons WE, Muasher SJ, Oehninger S. Minimal ovarianhyperstimulation for in vitro fertilization using sequential clomiphenecitrate and gonadotropin with or without the addition of a gonadotropin-releasing hormone antagonist. Fertil Steril 2002;78:1068–72.
13. Out HJ, Coelingh-Bennink HJ. Clomiphene citrate in the twenty-firstcentury: an anachronism? Assist Reprod Rev 1997;2:94–101.
14. Engel J, Ludwig M, Felberbaum RE, Albano C, Devroey P, Diedrich K.Use of cetrorelix in combination with clomiphene citrate and gonado-trophins: a suitable approach to “ friendly IVF”? Hum Reprod 2002;17:2022–6.
FERTILITY & STERILITY� 1523