use of business intelligence systems to support effective commissioning decisions, pop up uni, 1pm,...
TRANSCRIPT
Use of Business Intelligence
systems to support effective
commissioning decisions
NHS Commissioning Support Units
Four case studies demonstrating use of Business
Intelligence in high profile commissioning decision
making:
- Improving stroke services
- Improving efficiency ‘Right Care’
- Operational management of urgent care
- Supporting New Models of Care
Presented by three Commissioning Support Units:
- Improving stroke services
South, Central and West
- Improving efficiency through ‘Right Care’
Arden & GEM
- Operational management of urgent care
North of England
- Supporting New Models of Care
South, Central and West
Improving Stroke Services in
Somerset
Use of Geographical Information Systems in South,
Central and West Commissioning Support Unit
• In spring 2014, Somerset Clinical Commissioning Group looked into how a
proposed centralised stroke service, based at Musgrove Park Hospital
Taunton, would affect the population of Somerset.
• This followed an Independent Expert Panel report in November 2013
recommending significant changes to stroke services in Somerset.
• Somerset is a large county measuring 1,330 square miles and 70 miles
across. Previously, the service review had assumed that closing the stroke
services at Yeovil Hospital would benefit patients clinically.
• However, it was decided to use GIS analysis to see how the proposed
changes would impact the population…
Stroke Service Review in Somerset
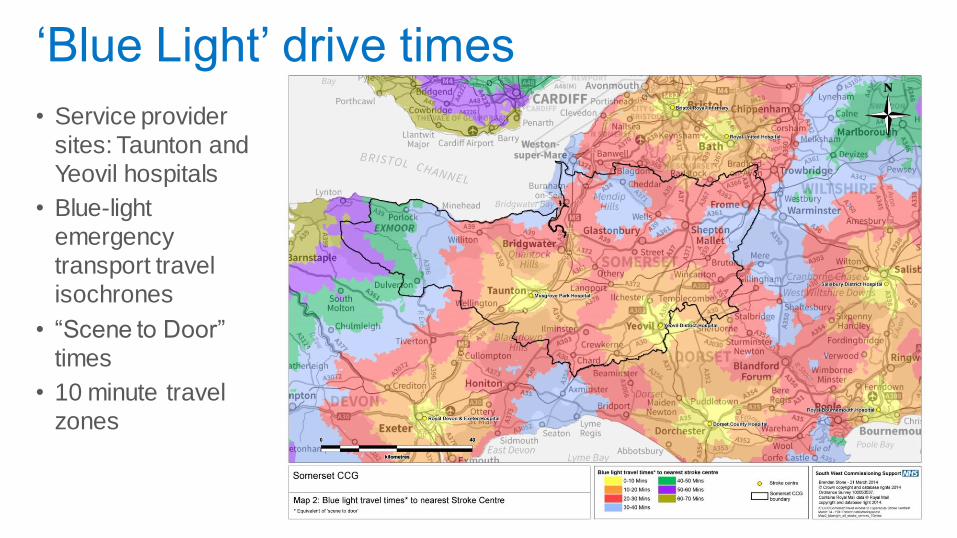
• Service provider
sites: Taunton and
Yeovil hospitals
• Blue-light
emergency
transport travel
isochrones
• “Scene to Door”
times
• 10 minute travel
zones
‘Blue Light’ drive times
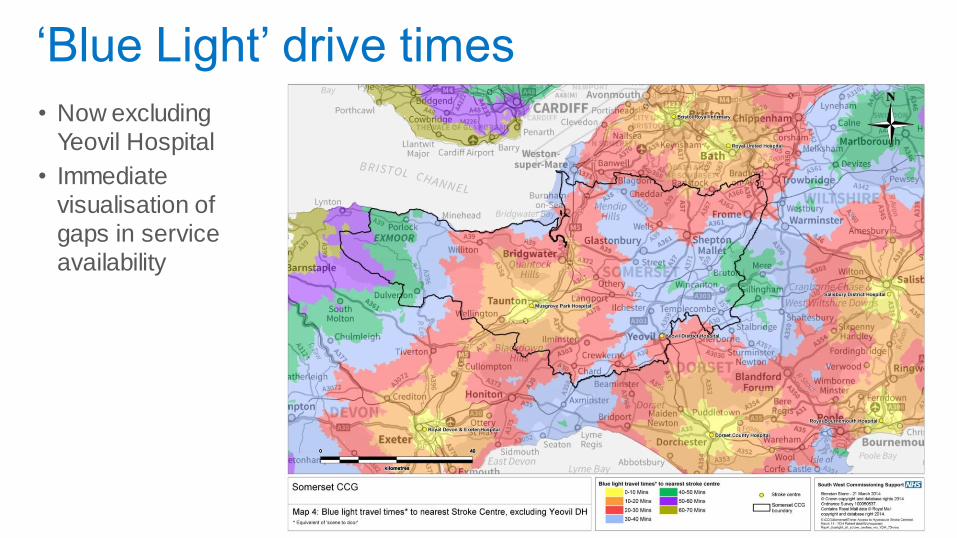
• Now excluding
Yeovil Hospital
• Immediate
visualisation of gaps in service
availability
‘Blue Light’ drive times
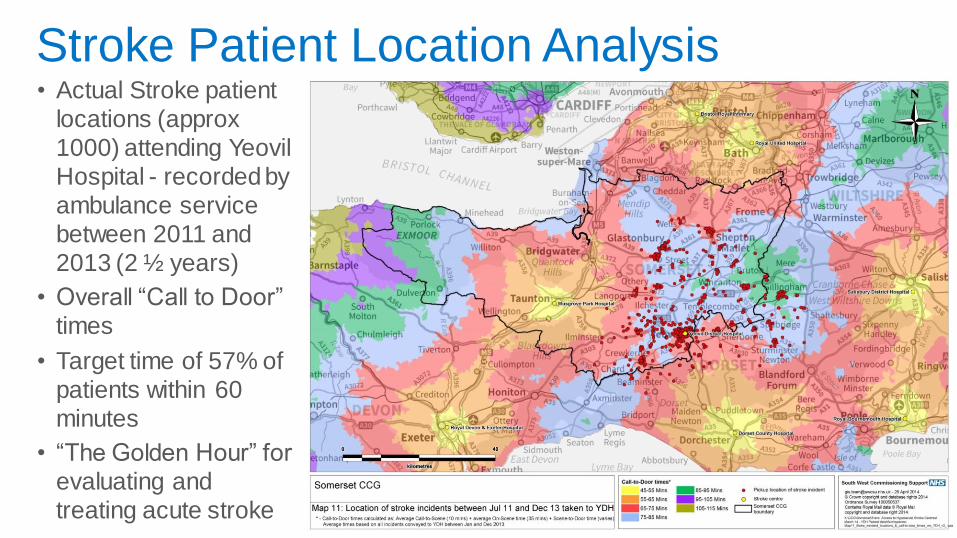
• Actual Stroke patient locations (approx
1000) attending Yeovil
Hospital - recorded by
ambulance service between 2011 and
2013 (2 ½ years)
• Overall “Call to Door”
times
• Target time of 57% of
patients within 60 minutes
• “The Golden Hour” for
evaluating and
treating acute stroke
Stroke Patient Location Analysis
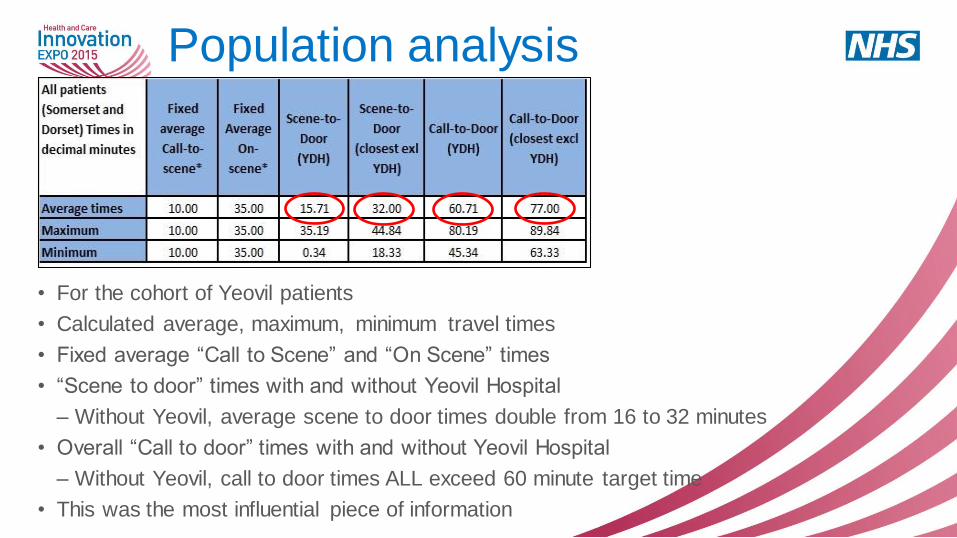
• For the cohort of Yeovil patients
• Calculated average, maximum, minimum travel times
• Fixed average “Call to Scene” and “On Scene” times
• “Scene to door” times with and without Yeovil Hospital
– Without Yeovil, average scene to door times double from 16 to 32 minutes
• Overall “Call to door” times with and without Yeovil Hospital
– Without Yeovil, call to door times ALL exceed 60 minute target time
• This was the most influential piece of information
Population analysis
“The evidence that a centralisation of hyper-acute services would improve outcomes for patients in Somerset is not definitive. The Independent Clinical Expert for the business case has suggested that TSTFT would find it challenging to move in the short term towards being the single hyper-acute centre for stroke services and ensure that such a move resulted in a better service for patients than they currently receive. This is particularly the case because of the rural nature of Somerset and the travel time implications which would mean that Taunton would have to show it can achieve door to needle times that were on average 20 minutes better than Yeovil could achieve in order simply to stand still compared to the status quo (for the small number of patients requiring thrombolysis). Neither the general academic research evidence available on centralisation, nor the Independent Clinical Expert’s work has provided a convincing case that would be credible to local people that the loss of their local access to hyper-acute care and the increased travel times would be mitigated by improved outcomes above what they could have had from services at Yeovil (if those services are properly developed). We do, however, note the intention of NHS England to develop plans this year to centralise stroke services in two areas which may provide further evidence.” Source: Stroke Services Review Consultation Business Case
Version 4. Governing Body 4 June 2014
Business case Conclusions and recommendations
Summary
• Complex information on travel times and access to services presented in an easy to understand way
• Evidence-based information resulted in accurate decision making
• Results showed that the 60 minute call-to-door target time for stroke patients would not be achievable for many patients
• Decision was made not to close the service at Yeovil Hospital
• The methodology and techniques used are repeatable for other service reviews and other geographical areas
Improving Efficiency
Right Care ‘Deep Dives’ by Arden and GEM
Commissioning Support Unit
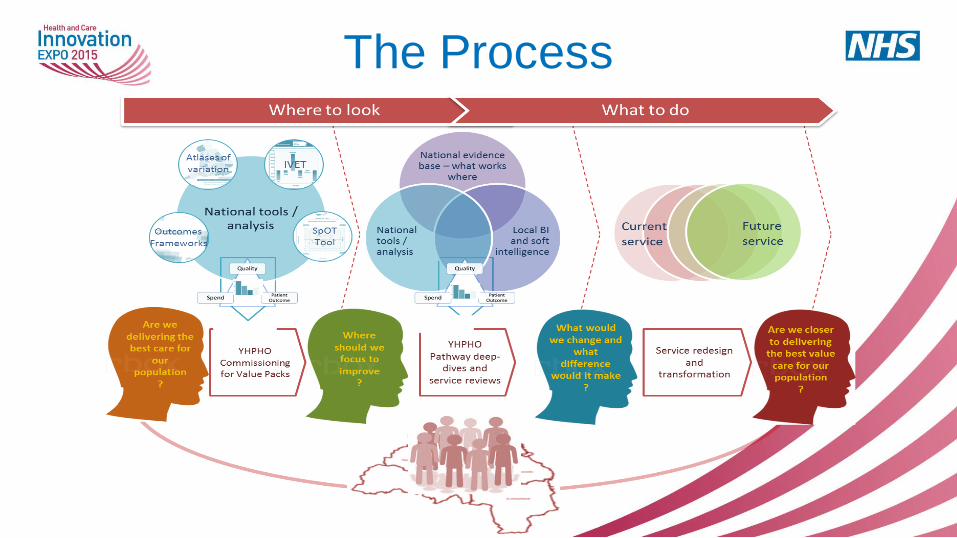
The Process
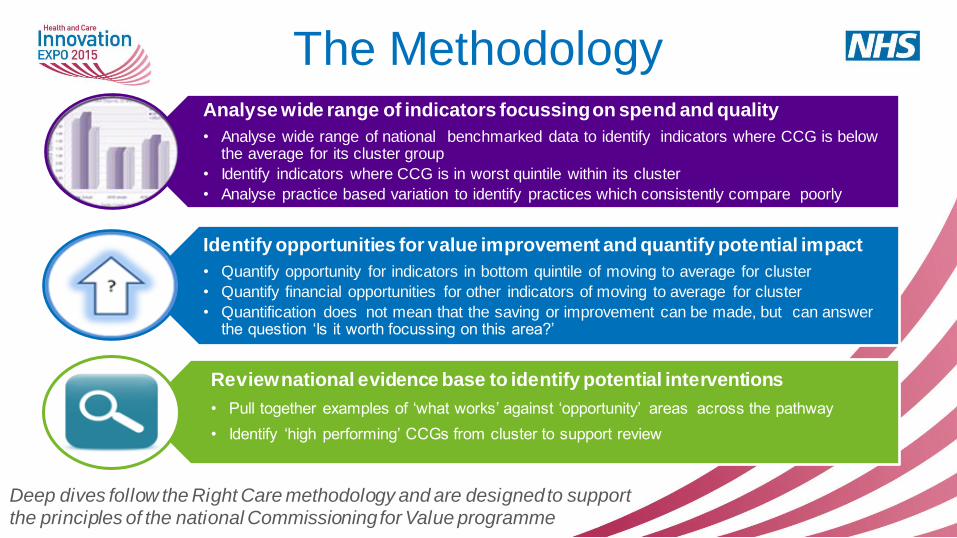
The Methodology Analyse wide range of indicators focussing on spend and quality
• Analyse wide range of national benchmarked data to identify indicators where CCG is below the average for its cluster group
• Identify indicators where CCG is in worst quintile within its cluster
• Analyse practice based variation to identify practices which consistently compare poorly
Identify opportunities for value improvement and quantify potential impact
• Quantify opportunity for indicators in bottom quintile of moving to average for cluster
• Quantify financial opportunities for other indicators of moving to average for cluster
• Quantification does not mean that the saving or improvement can be made, but can answer the question ‘Is it worth focussing on this area?’
Review national evidence base to identify potential interventions
• Pull together examples of ‘what works’ against ‘opportunity’ areas across the pathway
• Identify ‘high performing’ CCGs from cluster to support review
Deep dives follow the Right Care methodology and are designed to support the principles of the national Commissioning for Value programme
We adopt two different perspectives when selecting indicators that are worth
focusing on.
• In the first, we ask ‘Which CCG indicators are definitely outliers compared with the
benchmark group average?’. This ensures we avoid focusing too much on ‘outlier’
indicators that may just reflect a one-off bad year, by using statistical significance
testing.
• In the second, we ask ‘Which CCG indicators point to the greatest potential
financial savings if the CCG were to move to the benchmark group average? This
ensures that we take a thorough look at all indicators where there may be large
potential savings, even if we are less sure whether the ‘outlier’ indicators just
reflect a one-off bad year.
The Deep Dive is able to confirm or challenge the data provided in the Commissioning for Value packs by making area appropriate
adjustments.
Unique Approach

Service Transformation Building on the what Deep Dive tells us, we add in a local ‘situational analysis’ e.g.:
• What are the wider health and social care issues?
• What’s the coverage and performance of primary care?
• What is the quality and spread of nursing and care home sector?
• What is the quality and performance of mental health services?
We work with local area to agree programme of change:
• System wide or pathway
Leadership
Visioning
Strategy development
Facilitation
Stakeholder engagement
Agreeing outcomes
Whole system planning
Care pathway planning
Risk/ gain share
New models of contracting
Measuring outcomes
Changing Culture
Shared Purpose Getting It Done Holding to Account
• Using benchmarking data to identify opportunities for improvement
• Highlighting where a CCG could be delivering better value clinical
services by analysing programme budgeting indicators
• Better value is quantified in terms of improved clinical outcomes and cost
• We explore successful transformational interventions linked to the
opportunities for improvement.
Arden & GEM CSU has now provided almost 30 deep dive packs
for CCGs across England across a range of areas and services
including respiratory disease, diabetes, neurology, mental health
and musculoskeletal care.
The Benefits
Using Timely Business Intelligence to
Proactively Manage Patients
North of England Commissioning Support
Introduction • Traditional data flows are a good view of the past, but how do we get a view
of the present or near future?
• Patients can be vulnerable to readmission immediately following discharge
from hospital
• Targeted patient identification and clinical intervention in primary care can
reduce the risk of readmission
• Initiate targeted patient contacts for other users of urgent care as required
• Requires more than a discharge letter
19
Urgent Care Dashboard • A range of data feeds from clinical and administrative systems
• Produce a range of visual dashboards to provide context for urgent care pressures
– Settings
– Volumes
– Alerts
– Peer benchmarking
– Time of day / day of week analyses
• But, at GP Practice level…
20
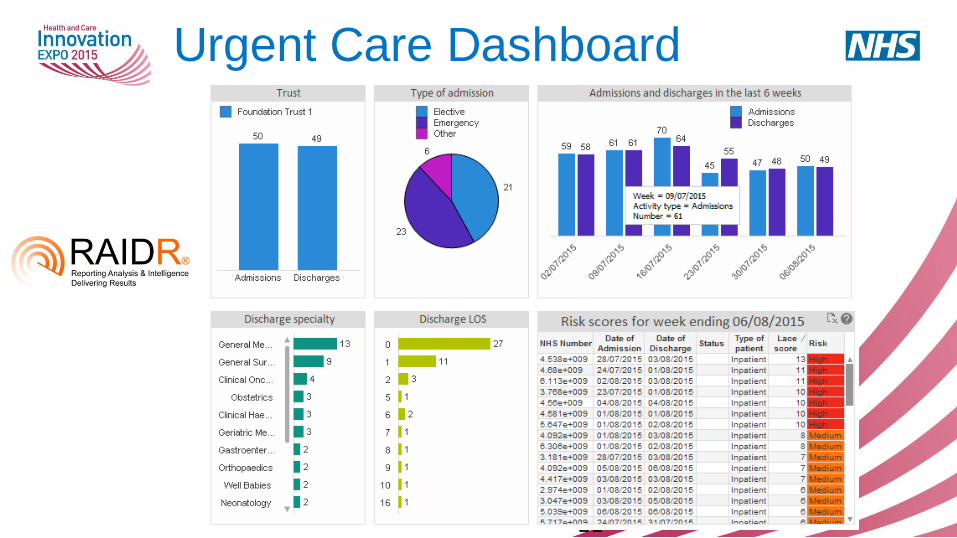
Urgent Care Dashboard
21
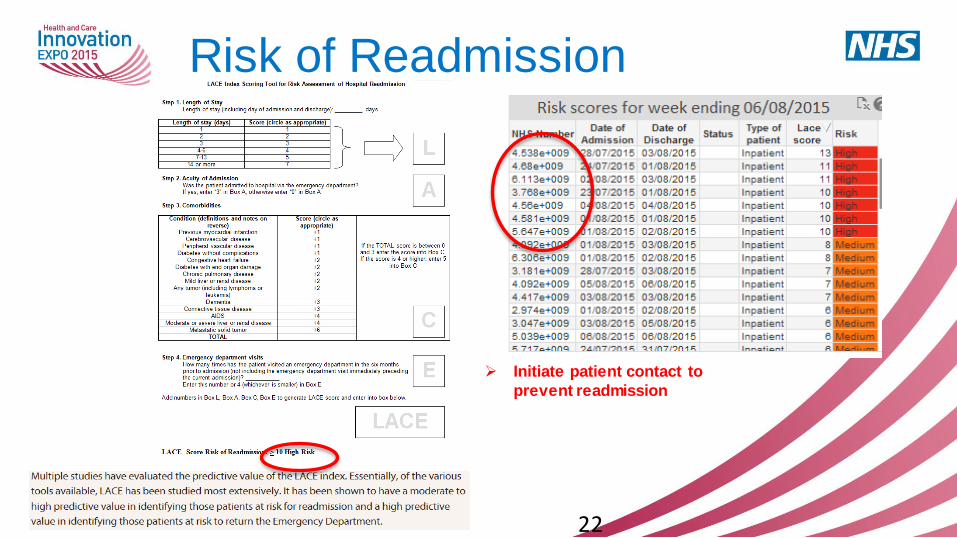
Risk of Readmission
Initiate patient contact to
prevent readmission
22
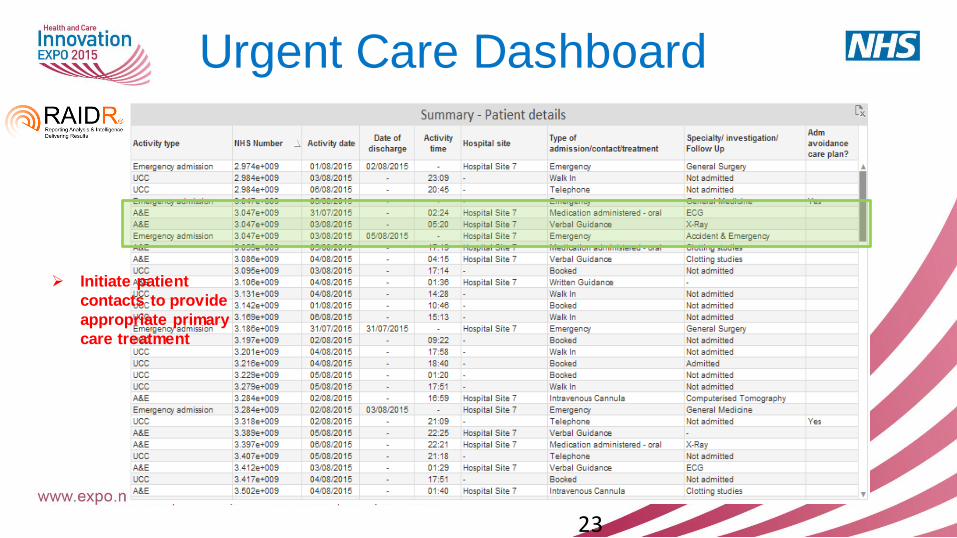
Urgent Care Dashboard
23
Initiate patient
contacts to provide
appropriate primary
care treatment
Supporting New Models of Care
The Symphony Vanguard Project in Somerset
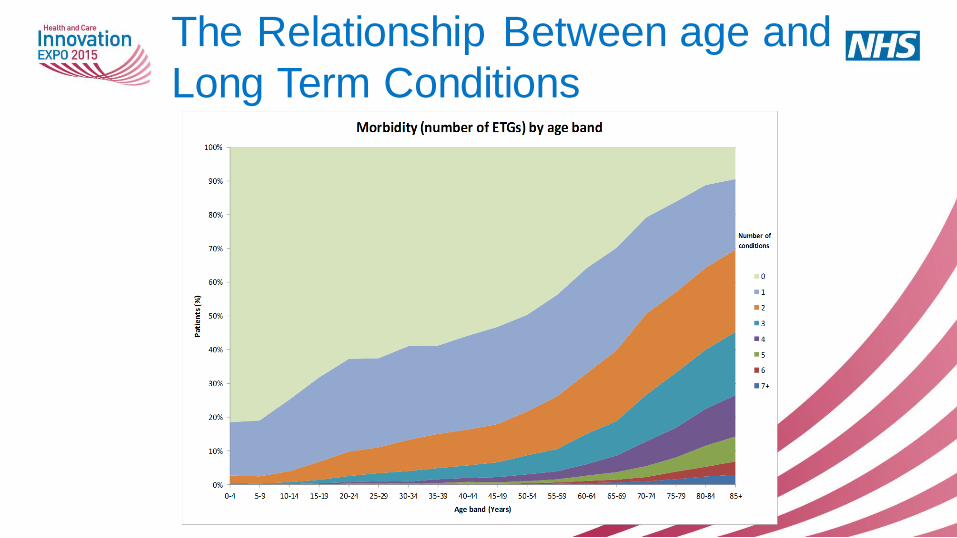
The Relationship Between age and
Long Term Conditions
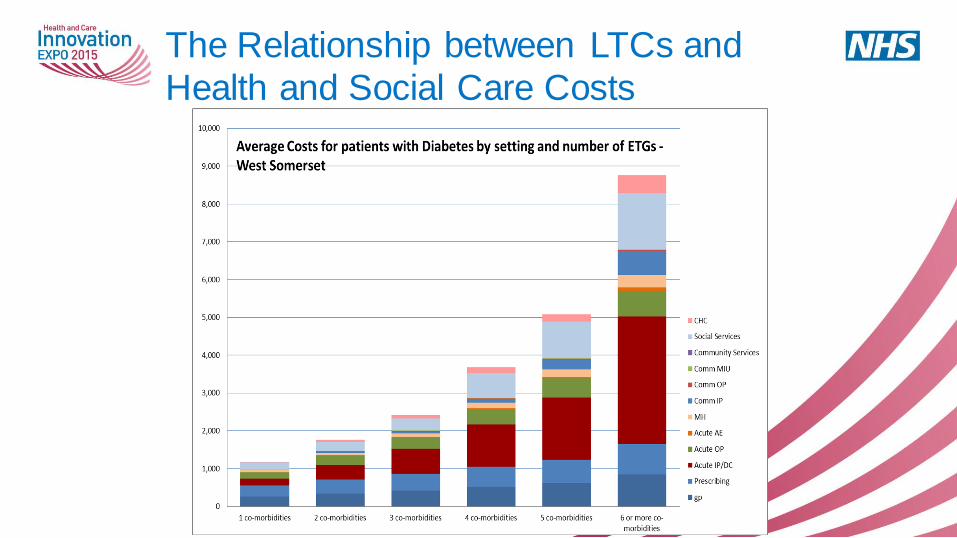
The Relationship between LTCs and
Health and Social Care Costs
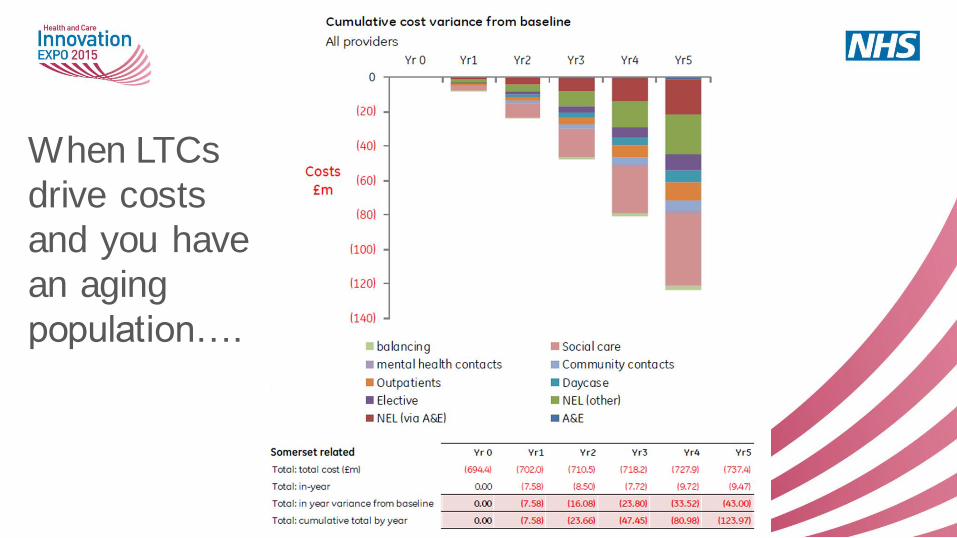
When LTCs
drive costs
and you have
an aging
population….

South Somerset Vanguard
Outcomes Based
Commissioning in
Somerset
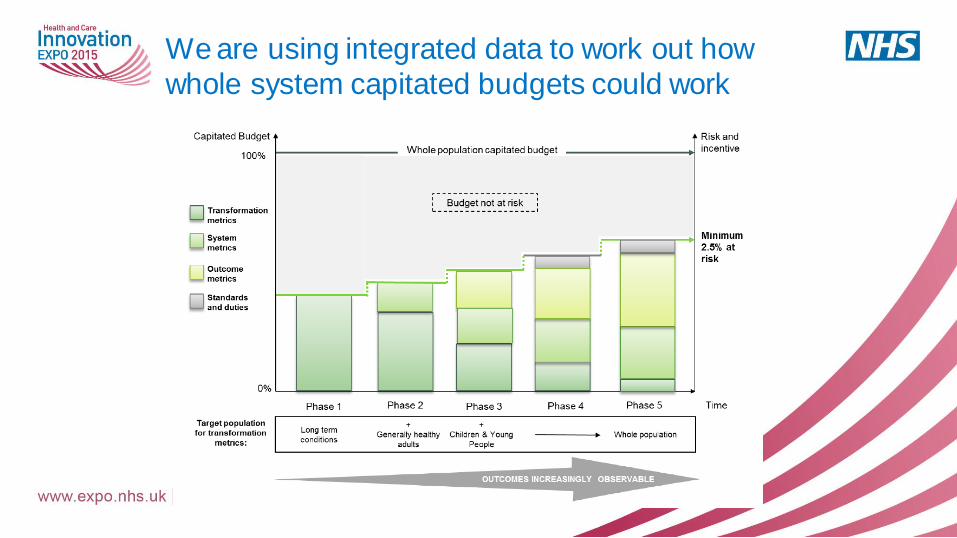
We are using integrated data to work out how
whole system capitated budgets could work
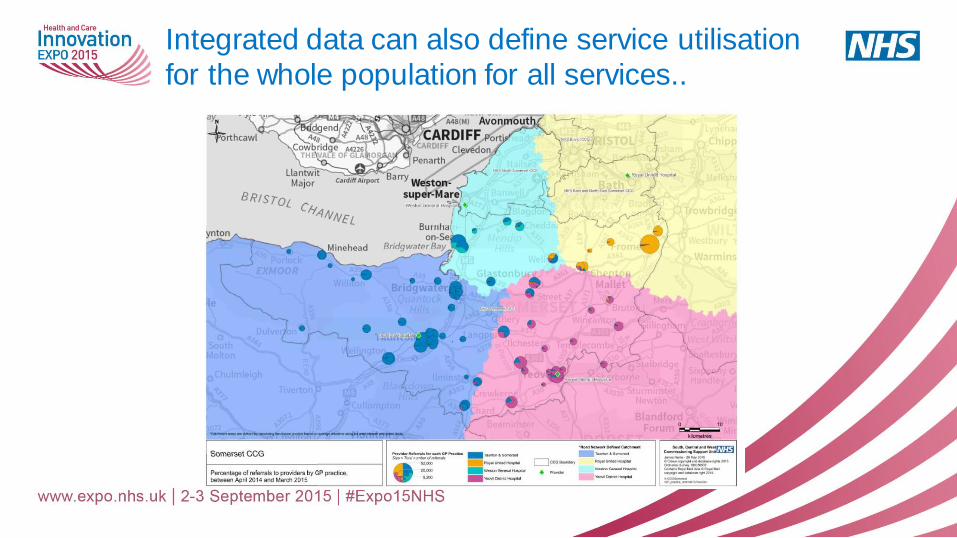
Integrated data can also define service utilisation
for the whole population for all services..
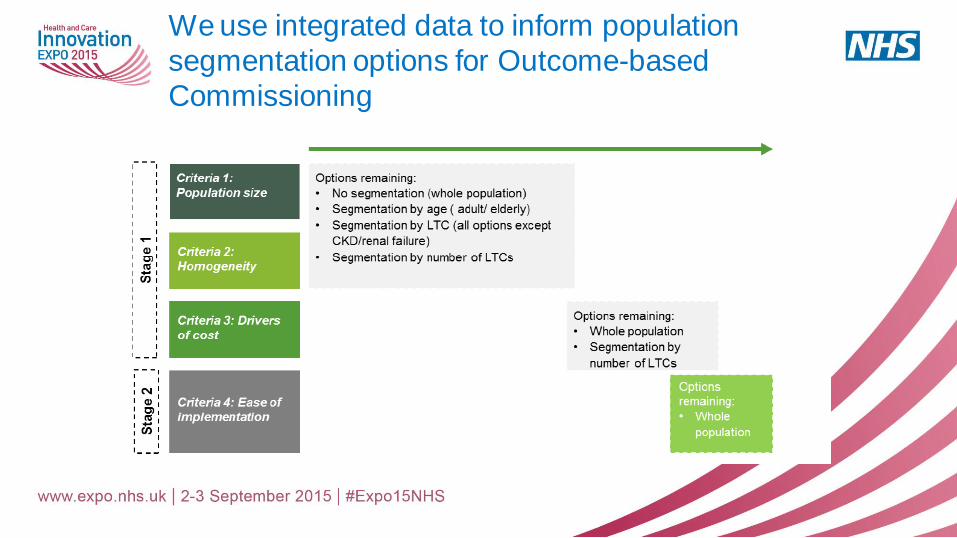
We use integrated data to inform population
segmentation options for Outcome-based
Commissioning
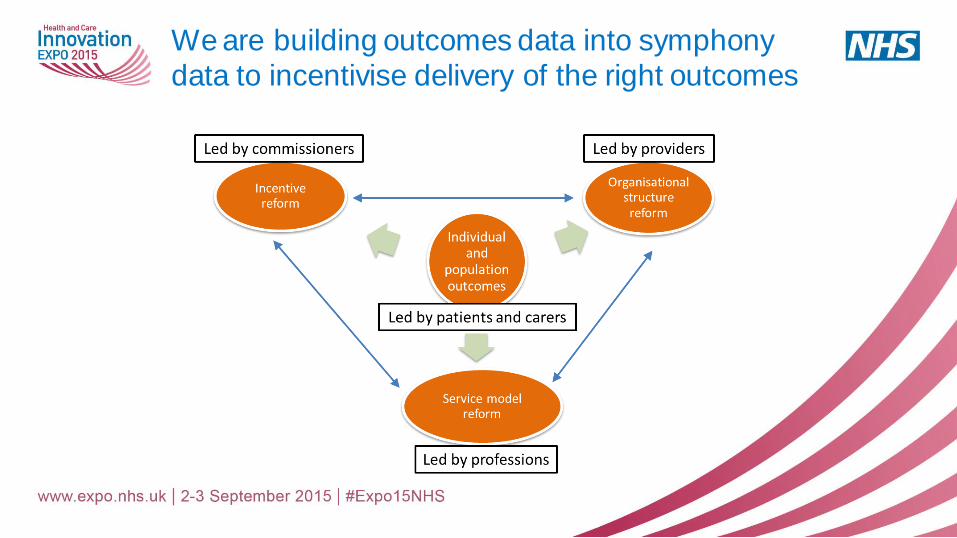
We are building outcomes data into symphony
data to incentivise delivery of the right outcomes
Common themes of these case studies
• Commissioning Support Units are positioned to be able to exploit tools, technologies and skills to support the most important commissioning challenges facing the NHS
• BI solutions can support significant changes in service delivery and patient outcomes when they are delivered at scale across health systems
• Commissioning decisions and those concerning new models of care delivery are becoming more complex. Business intelligence is critical to ensuring that these decisions are based on evidence
• The NHS is using Business Intelligence to ensure decisions are based on what WILL happen not what has happened in the past
• Technology and systems are often the easier bit! The challenge is to build coalitions of clinical sponsors who are committed to work with information specialists to deliver change on the ground.
…Discussion
For further information: • Catherine Dampney Stroke and the Symphony Project
• Simon Freeman Right Care
• Ian Nicolson Urgent Care Dashboard
Many NHS CSUs are also in the NHS Expo Exhibition