usaid global health supply chain programme annual report
TRANSCRIPT
1
USAID Global Health Supply Chain Programme
Annual Report
01 October 2017 to 30 September 2018
Contract No.: AID-OAA-I-15-00032
Task Order No.: AID-674-TO-16-00002
15 November 2018

2
USAID Global Health Supply Chain
programme
Annual Report
01 October 2017 - 30 September 2018
Contract No.: AID-OAA-I-15-00032
Task Order No.: AID-674-TO-16-00002
Submitted to:
USAID/South Africa
Prepared by:
Global Health Supply Chain –Technical Assistance
Disclaimer:
This document is made possible by the generous support of the American people through the United States Agency for International
Development (USAID). The contents are the responsibility of Global Health Supply Chain Consortium and do not necessarily reflect the views
of USAID or the United States Government.
3
TABLE OF CONTENTS
1. PROGRAMME OVERVIEW 6
2. ACRONYMS 7
3. EXECUTIVE SUMMARY 10
4. INTRODUCTION 12
4.1 BACKGROUND 12
4.2 SUMMARY OF ACCOMPLISHMENTS 13
5. PROGRAMME OBJECTIVES 16
5.1 RESULTS FRAMEWORK 16
5.2 PROGRAMME GOVERNANCE AND MANAGEMENT 17
6. FINANCIAL STATUS OF THE TASK ORDER 18
7. ACHIEVEMENTS AND MAJOR ACTIVITIES BY OBJECTIVE 20
7.1 OBJECTIVE 1: IMPROVE SELECTION AND USE OF MEDICINES 20
7.1.1 Sub-Objective 1.1: Assist with the Implementation of HTA 20
7.1.2 Sub-Objective 1.2: Improve Rational Medicine Use 20
7.2 OBJECTIVE 2: SUPPORT OPTIMISATION OF THE SUPPLY CHAIN 22
7.2.1 Sub-Objective 2.1: Improve contracting 22
7.2.2 Sub-Objective 2.2: Improve contract management 23
Workforce Management 23
Demand Forecasting 23
7.2.3 Sub-Objective 2.3: Design Supply Chain Operating Model 24
Demand Planning 24
Supply Planning (Informed Push) 24
Distribution Planning 25
7.2.4 Sub-Objective 2.4: Maintain and improve supply chain operations 25
Support to North West Province 26
Central Chronic Medicine Dispensing and Distribution (CCMDD) 27
7.3 OBJECTIVE 3 - STRENGTHEN GOVERNANCE 27
7.3.1 Sub-Objective 3.1: Contribute to Development of Policy and Legislation 27
7.3.2 Sub-Objective 3.2: Support the Implementation of Governance 28
7.3.3 Sub-Objective 3.3: Coordination and Oversight of Stakeholder Engagement and Communication Activities 30
7.4 OBJECTIVE 4 – WORKFORCE MANAGEMENT 31
4
7.4.1 Sub-Objective 4.1: Support the Development of Standardised Structures, Roles, Competencies and Performance Management 31
7.4.2 Sub-Objective 4.2: Change Management Institutionalised 32
7.4.3 Sub-Objective 4.3: Upskilling and Mentoring and Staff 32
7.5 OBJECTIVE 5 – STRENGTHEN INFORMATION SYSTEMS AND INFORMATION MANAGEMENT 32
7.5.1 Sub-Objective 5.1: Design IT System Landscape 33
7.5.2 Sub-Objective 5.2: Provide Support to Strengthen Analytics and Oversight 34
7.5.3 Sub-Objective 5.3: Support the Implementation of Data Governance 35
7.5.4 Sub-Objective 5.4: Assist with Development and Implementation of IT Systems 36
RxSolution Maintenance and Consolidation 36
RxSolution: Application Development 36
SVS Phase I: Maintenance and Consolidation 37
SVS Phase II: Development and Enhancement 38
WMS (gCommerce) Implementation 38
PuLSe application development 39
7.6 OBJECTIVE 6 - IMPROVE FINANCIAL MANAGEMENT 40
7.6.1 Sub-Objective 6.1: Improve Forecasting and Budget Information 40
7.6.2 Sub-Objective 6.2: Assist to Strengthen Accounting Processes 41
7.6.3 Sub-Objective 6.3: Assist to Improve Financial Monitoring and Reporting 42
8. CRITICAL RISKS 43
9. LESSONS LEARNED 45
10. PERFORMANCE MONITORING 46
10.1 OBJECTIVE 1: IMPROVE THE SELECTION AND USE OF MEDICINE. 46
10.1.1 Sub-Objective 1.1: Assist with the Implementation of Health Technology Assessments. 46
10.1.2 Sub-Objective 1.2: Improve Rational Medicine Use. 47
10.2 OBJECTIVE 2: SUPPORT OPTIMISATION OF THE SUPPLY CHAIN. 49
10.2.1 Sub-Objective 2.1: Improve Contracting and 2.2 Improve Contract Management. 49
10.2.2 Sub-Objective 2.3 Design Supply Chain Operating Model and 2.4 Maintain and Improve Supply Chain Operations. 52
10.3 OBJECTIVE 3: STRENGTHEN GOVERNANCE. 52
10.3.1 Sub-Objective 3.1: Contribute to development of policy and legislation, Sub-Objective 3.2: Support the implementation of governance, and Sub-Objective 3.3: Coordination and oversight of stakeholder engagement and communication activities. 52
10.4 OBJECTIVE 4: IMPROVE WORKFORCE 53
10.4.1 Sub-Objective 4.1 – Support the development of standardized structures, roles and competencies & performance management, Sub-Objective 4.2 – Assist to institutionalize change management, and Sub-Objective 4.3 – Contribute to up-skilling and mentoring of AMD staff. 53
10.5 OBJECTIVE 5: STRENGTHEN INFORMATION SYSTEMS AND INFORMATION MANAGEMENT. 54

5
10.5.1 Sub-Objective 5.1 Design an IT System Landscape and 5.2 Provide Support to Strengthen Analytics and Oversight. 54
10.5.2 Sub-Objective 5.3 Support the Implementation of Data Governance. 56
10.6 OBJECTIVE 6: IMPROVE FINANCIAL MANAGEMENT. 56
10.6.1 Sub-Objective 6.1 – Improve forecasting & budget information, Sub-Objective 6.2 - Assist to strengthen accounting processes, & Sub-Objective 6.3- Assist to improve financial monitoring & reporting 56
11. ANNEX 57
6
1. PROGRAMME OVERVIEW
Name USAID Global Health Supply Chain Programme
Contract Number AID-OAA-I-15-00032; AID-674-TO-16-00002
Start Date September 27, 2016
End Date September 30, 2021
The USAID Global Health Supply Chain Programme (GHSC) in South Africa commenced in September
2016. The programme provides technical assistance to the South African government to strengthen public
health systems and supply chains in order to advance an AIDS-free generation and contribute toward the
achievement of universal health coverage.
The GHSC implementing team is led by Guidehouse (formerly PricewaterhouseCoopers Public Sector
LLP) and includes PwC South Africa, Imperial Health Sciences, and Priority Cost Effective Lessons for
Systems Strengthening South Africa (PRICELESS SA), Management Sciences for Health, and Banyan Global.
During this reporting period, PRICELESS SA elected to exit the consortium and ceased technical assistance
activities at the end of March 2018.

7
2. ACRONYMS
AFT Administrative Function Testing
AMD Affordable Medicines Directorate
API Application Programming Interface
APP Annual Performance Plan
ARC Africa Resource Centre
ARV Antiretroviral
CCMDD Central Chronic Medicine Dispensing and Distribution
CDCS Country Development Cooperation Strategy
CMU Contract Management Unit
CPA Contract Price Adjustment
CSIR Council for Scientific and Industrial Research
DDV Direct Delivery
DO Development Objective
EC Eastern Cape
EDP Essential Drugs Programme
EMelA Essential Medicines Electronic Access tool
EML Essential Medicines List
ERC Expert Review Committee
FPD Foundation For Professional Development
FS Free State
GHSC Global Health Supply Chain
GTIN Global Trade Identification Number
HR Human Resources
HRD Human Resource Development
HRM Human Resource Management
HST Health Systems Trust
HTA Health Technology Assessment
ICT Information and Communications Technology
ISP Information Systems and Projects
IT Information Technology
ITSC IT Steering Committee
KPI Key Performance Indicator
LOE Level of Effort
LP Limpopo
M&E Monitoring and Evaluation
MEC Member of the Executive Council
MHPL Master Health Product List
MMDS Medicine Master Data System
MOU Memorandum of Understanding
8
MPC Master Procurement Catalogue
NC Northern Cape
NDoH National Department of Health
NEMLC National Essential Medicine List Committee
NHC National Health Council
NHC-SC-
PS National Health Council – Sub-Committee – Pharmaceutical Services
NHI National Health Insurance
NSC National Surveillance Centre
NT National Treasury
NW North West
OD Organisational Design
ODC Other Direct Costs
OTIF On Time and In Full
PDU Pharmacy Dispensing Unit
PHC Primary Health Care
PIT Programme Implementation Team
PLDP Pharmacy Linked Distribution Points
PMDS Performance Monitoring and Development System
PMLO Provincial Medicine Liaison officer
PMPU Provincial Medicine Procurement Unit
POC Proof of Concept
PTC Pharmaceutical and Therapeutics Committee
PuP Pick Up Point
PwC PricewaterhouseCoopers
RACI Responsible, Accountable, Consulted, and Informed
RMU Rational Medicine Use
RSA Republic of South Africa
SAHPRA South African Health Products Regulatory Authority
SAPC South African Pharmacy Council
SAPICS South African Production and Inventory Control Society
SAVC South African Veterinary Council
SIAPS Systems for Improved Access to Pharmaceuticals and Services
SIMA Strategy to Improve Medicine Availability
SITA State Information Technology Agency
SLA Service Level Agreement
SOP Standard Operating Procedure
SQL Structured Query Language
STG Standard Treatment Guideline
SVS Stock Visibility System
SWP Sector Wide Procurement
TA Technical Assistance
9
TB Tuberculosis
TL Truck Load
TLART Third Line Antiretroviral Treatment
TOR Terms of Reference
UAT User Acceptance Testing
URS User Requirements Specifications
USAID United States Agency for International Development
VAN Visibility and Analytics Network
WG Wave Governance
WMS Warehouse Management System
10
3. EXECUTIVE SUMMARY The focus for Year 2 of the programme has been on implementing design work completed in Year 1, with
a focus on teams providing continued concentrated support to the Affordable Medicines Directorate
(AMD) within the National Department of Health (NDoH) and expanded technical assistance to provincial
departments of health in North West (NW), Eastern Cape (EC), Northern Cape (NC), and Limpopo (LP)
provinces. Key activities and accomplishments are summarised below:
Health Technology Assessments (HTA) and Rational Medicine Use (RMU)
Though focus on HTAs was reduced during Year 2, the team provided AMD with a cost effectiveness and
budget impact analysis for several medicines that supported National Essential Medicines List Committee
(NEMLC) decisions. GHSC TA also developed the National Formulary Guideline, a strategically important
document that guides the development, management, and use of formularies at all levels of the health care
system and supports the Medicine Master Data System (MMDS). In addition to these activities, the team
also drafted five memoranda of understanding (MOUs) that govern sharing antimicrobial resistance
surveillance data between public and private sector institutions.
Supply Chain
Year 2 saw the development and implementation of a new Demand Planning process supported by a
commercial forecasting tool and a guideline drafted by SCTA, both of which will significantly improve the
ability to model future medicine demand at national and provincial levels. This new approach to demand
planning will transform budgeting by providing a more analytically sound demand forecast. In addition,
outputs from the demand planning process are directly informing the contracting process. Importantly,
the process and tool were designed to be rolled out to provincial personnel with EC and NW demand
planners currently developing and submitting forecasts to AMD. Other notable supply chain activities
include developing a Proof of Concept (POC) for Supply Planning, which has the potential to ease the
burden of medicine ordering by clinic personnel, freeing them to focus on patient care.
Technology
Several technology activities continued in Year 2. GHSC personnel are developing the specifications for
the MMDS, a system that forms the basis for all medicine master data used across the entire public health
sector, a critical piece of work that improves system interoperability, promotes visibility and analytics, and
enables generation of formularies.
The team provided technical input to new receiving and ordering functions of the Stock Visibility System
(SVS) and supported the implementation of the gCommerce Warehouse Management System (WMS) in
LP. In addition, GHSC personnel supported completion of, and developed tools for, the implementation
of PuLSe, an online system that enables providers to apply for and manage dispensing licenses and permits
more quickly than the legacy paper process.
North West Province Intervention
During May 2018, NW experienced a period of labour unrest, which led to the closure of the Provincial
Medical Depot in Mahikeng. Facing a crisis, AMD asked GHSC TA personnel to establish and staff a
temporary PMPU at the NDoH, which during this period processed and managed more than 2,000
medicine and medical consumable orders from hospitals and Community Health Centres (CHCs) totalling
more than R 25 million. The team achieved AMD’s goal of rapidly shifting 100% of orders from depot to
supplier direct delivery—an achievement that fundamentally preserved medicine availability throughout
the province. Following our success operating the temporary PMPU, NDoH prioritised NW as the next
province to receive supply chain strengthening support once the labour unrest abated. GHSC TA also

11
conducted rapid analyses of the workforce, supply chain planning, financial management, systems and
processes, and network and distribution operations. The AMD Intervention Lead and the Provincial
Administrator reviewed our findings and personally tasked GHSC to support the province in implementing
recommended improvements.
Performance Reporting, Supply Chain Analytics and Visibility
GHSC TA developed improved KPIs for AMD, which were approved and incorporated into the National
Surveillance Centre (NSC) dashboards. These KPIs span the entire medicine value chain, including
selection and use of medicines, contracting, contract management, and supply chain. They are
communicated to national and provincial stakeholders via eight dashboards with 135 views and 65 reports.
The team also improved performance monitoring and visibility by significantly increasing the number of
sites that report medicine availability to the NSC to 3,137 clinics, 443 hospitals, 8 provincial warehouses,
8 CCMDD stock storage sites and 8 GP Care Cells. To facilitate reporting on medicine availability, GHSC
developed an application that automates reporting processing from sites using RxSolution, which was
successfully tested and deployed in the Free State.
Workforce
AMD requested GHSC TA personnel to provide workforce strengthening services to the Contract
Management Unit (CMU) which is responsible for overseeing demander and supplier performance—
critical enablers of medicine availability. The team delivered a new organizational design, job descriptions,
and performance measures for CMU. In addition, the team reengineered existing processes, drafted SOPs
and provided training and coaching. The team replicated this approach during similar interventions for the
Information Systems and Projects (ISP) Unit within AMD and in the NW.
Way Forward
The aforementioned activities and accomplishments form a foundation for expansion of GHSC TA support
to provinces and the continued improvement in pharmaceutical supply chain performance across the
country. Our experience in NW, working daily and side-by-side with provincial, depot, district, hospital
and clinic personnel, has afforded us significant insight into the complexities and challenges associated with
driving improved pharmaceutical supply chain performance. We look to apply lessons learned as we
support additional provinces and foresee encountering and addressing many of the same challenges and
utilising opportunities encountered to date. In addition to provincial engagement, we look forward to
continuing our collaboration with AMD personnel responsible for selection and rational medicine use,
contracting and contract management, supply chain, information technology, and finance.

12
4. INTRODUCTION
4.1 BACKGROUND
The USAID GHSC Programme in South Africa commenced in September 2016. The GHSC Programme
leverages industry approaches and leading practices to accelerate strengthening of the South African public
health supply chain to respond to current challenges and emerging trends that have the potential to shape
or stress the health system. The programme provides technical assistance (TA) to build capacity of the
South African government, including the AMD within the NDoH and provincial pharmaceutical services
to improve medicine availability.
This work directly supports the USAID/South Africa Country Development Cooperation Strategy
(CDCS) results framework by supporting Development Objective (DO) 1- Health outcomes for South
Africans improved, as well as the NDoH Strategy to Improve Medicine Availability (SIMA) (2016-2021)
and the NDoH Annual Performance Plan (APP).
13
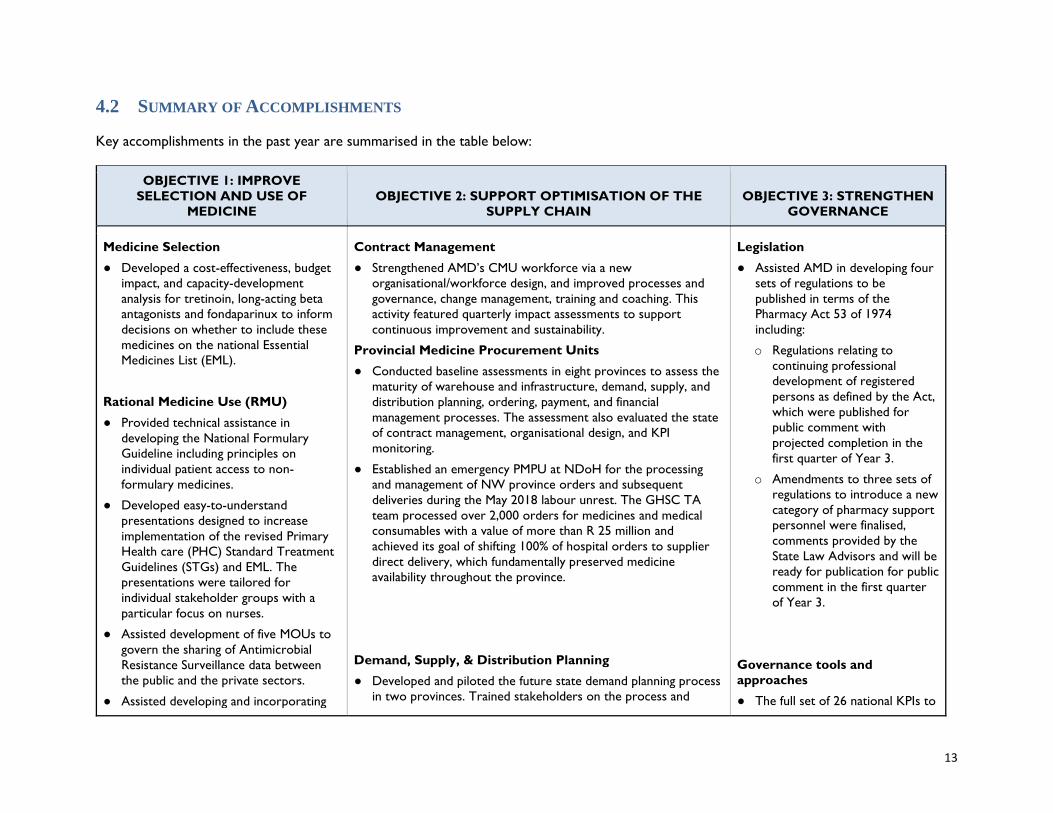
4.2 SUMMARY OF ACCOMPLISHMENTS
Key accomplishments in the past year are summarised in the table below:
OBJECTIVE 1: IMPROVE
SELECTION AND USE OF
MEDICINE
OBJECTIVE 2: SUPPORT OPTIMISATION OF THE
SUPPLY CHAIN
OBJECTIVE 3: STRENGTHEN
GOVERNANCE
Medicine Selection
● Developed a cost-effectiveness, budget
impact, and capacity-development
analysis for tretinoin, long-acting beta
antagonists and fondaparinux to inform
decisions on whether to include these
medicines on the national Essential
Medicines List (EML).
Rational Medicine Use (RMU)
● Provided technical assistance in
developing the National Formulary
Guideline including principles on
individual patient access to non-
formulary medicines.
● Developed easy-to-understand
presentations designed to increase
implementation of the revised Primary
Health care (PHC) Standard Treatment
Guidelines (STGs) and EML. The
presentations were tailored for
individual stakeholder groups with a
particular focus on nurses.
● Assisted development of five MOUs to
govern the sharing of Antimicrobial
Resistance Surveillance data between
the public and the private sectors.
● Assisted developing and incorporating
Contract Management
● Strengthened AMD’s CMU workforce via a new
organisational/workforce design, and improved processes and
governance, change management, training and coaching. This
activity featured quarterly impact assessments to support
continuous improvement and sustainability.
Provincial Medicine Procurement Units
● Conducted baseline assessments in eight provinces to assess the
maturity of warehouse and infrastructure, demand, supply, and
distribution planning, ordering, payment, and financial
management processes. The assessment also evaluated the state
of contract management, organisational design, and KPI
monitoring.
● Established an emergency PMPU at NDoH for the processing
and management of NW province orders and subsequent
deliveries during the May 2018 labour unrest. The GHSC TA
team processed over 2,000 orders for medicines and medical
consumables with a value of more than R 25 million and
achieved its goal of shifting 100% of hospital orders to supplier
direct delivery, which fundamentally preserved medicine
availability throughout the province.
Demand, Supply, & Distribution Planning
● Developed and piloted the future state demand planning process
in two provinces. Trained stakeholders on the process and
Legislation
● Assisted AMD in developing four
sets of regulations to be
published in terms of the
Pharmacy Act 53 of 1974
including:
o Regulations relating to
continuing professional
development of registered
persons as defined by the Act,
which were published for
public comment with
projected completion in the
first quarter of Year 3.
o Amendments to three sets of
regulations to introduce a new
category of pharmacy support
personnel were finalised,
comments provided by the
State Law Advisors and will be
ready for publication for public
comment in the first quarter
of Year 3.
Governance tools and
approaches
● The full set of 26 national KPIs to
14
medicine related principles in the
National Referral Policy
forecasting tool (Forecast Pro), which more accurately models
future medicine demand at provincial and national levels. The
demand planning process informs the contracting process and
shapes Supply and Distribution planning decisions.
● Developed and currently piloting the future state Supply Planning
process in the NW. The new approach shifts ordering from
over-burdened healthcare providers to a centralised team able
to apply analytics to minimum/maximum levels and
replenishment decisions. This is a first step towards an Informed
Push model.
● Applied distribution planning principles to rapidly assess and
identify several potential improvements to NW medicine
distribution including improved routing and scheduling,
increasing Truck Load (TL) utilisation, and increasing supplier
direct delivery (DDV).
Supply Chain Segmentation
● Developed an initial segmentation approach for shaping demand,
supply, and distribution planning. The segmentation includes
considerations for and the ability to weight volume, cost, and
criticality—e.g. using the Vital, Essential, or Necessary
classification —and will be used to better align resources to
predicting the demand, supplying and distributing those
medicines with the highest volumes, cost, and patient impact.
monitor performance of the
supply chain in accordance with
the SIMA, were finalised following
incorporation of provincial input.
The document was submitted to
the National Health Council
Technical Committee of NDOH
and dashboards were revised to
reflect the revised KPIs.
● To improve the ability of AMD to
manage, coordinate, and
recognise efficiencies in work
performed by implementing
partners, GHSC developed the
terms of reference for the Wave
Governance project management
approach, as well as a set of KPIs
to monitor implementation and
usefulness of this planning and co-
ordination mechanism.
OBJECTIVE 4: IMPROVE
WORKFORCE MANAGEMENT
OBJECTIVE 5: STRENGTHEN INFORMATION SYSTEMS
AND INFORMATION MANAGEMENT
OBJECTIVE 6: IMPROVE
FINANCIAL MANAGEMENT
● Reviewed and designed new structures
for the CMU, ISP, and NW
Pharmaceutical Services.
● Reviewed and developed seventeen job
descriptions and performance
● Helped develop specifications for further development of the
SVS including enabling the application to support ordering and
receiving transactions at PHC facilities.
● Implemented the gCommerce Warehouse Management System
(WMS) in Limpopo.
● Designed Standard Operating
Procedures (SOPs) related to
budget management for Sector
Wide Procurement (SWP) and
conducted training with the
relevant Directorates.
15
agreements for both CMU and ISP.
● Developed new dashboards to provide visibility across the
supply chain, including warehouses, Central Chronic Medicine
Dispensing and Distribution (CCMDD) service providers and
contracted general practitioners. The eight dashboards now
offer users multiple customisable views.
● Developed the IT Strategy and Roadmap, including IT operating
model and IT project methodology.
● Developed, tested and deployed the RxSolution middleware
Application Programming Interface (API) in Free State (FS),
enabling automated reporting of medicine availability data.
● Assisted developing master data requirements and design
specifications fa full-fledged online Master Health Product List
(MHPL) that will serve as the authoritative list of approved
medicines that all other databases reference.
● Increased the number of sites reporting medicine availability to
the National Surveillance Centre (NSC) to 3,604. This includes
3,137 clinics, 443 hospital facilities which are supported by the
GHSC programme, 8 provincial warehouses, 8 CCMDD stock
storage sites and 8 GP Care Cells.
● Assisted and provided guidance
with budget forecasting for the
2018/19 financial year for each
Directorate with SWP.
● Designed and implemented
Budget vs. Actual expenditure
monitoring dashboards for SWP.
16
5. PROGRAMME OBJECTIVES
5.1 RESULTS FRAMEWORK
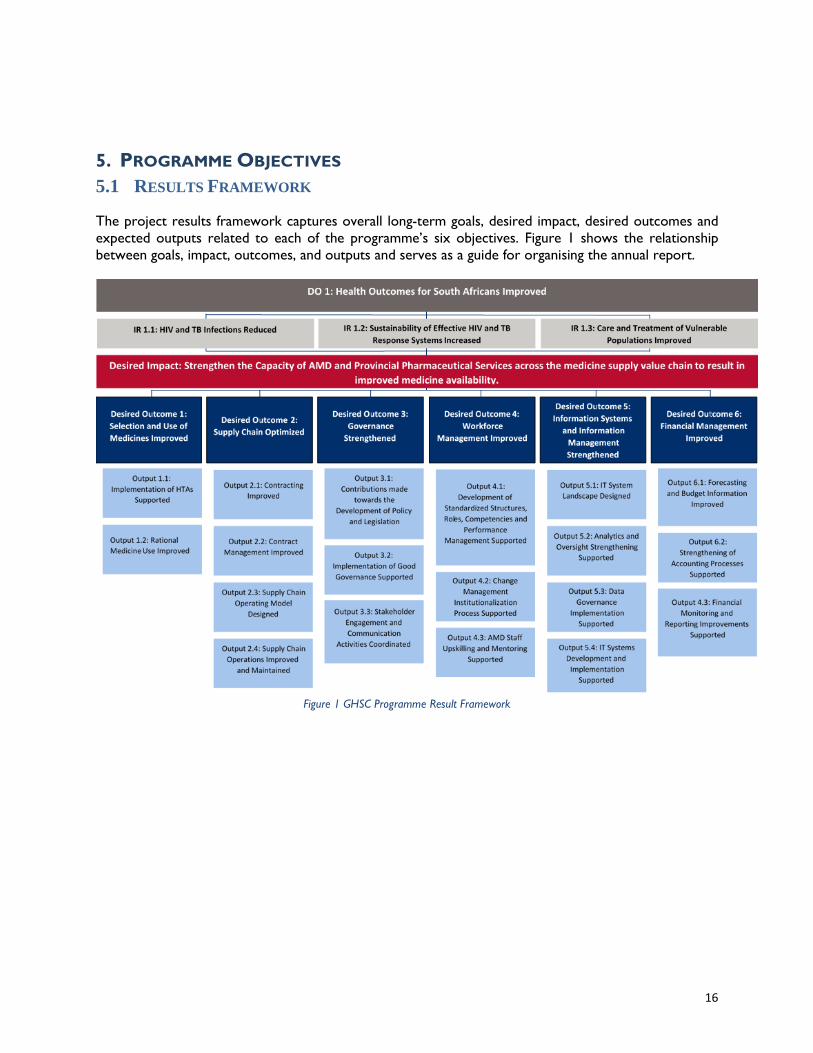
The project results framework captures overall long-term goals, desired impact, desired outcomes and
expected outputs related to each of the programme’s six objectives. Figure 1 shows the relationship
between goals, impact, outcomes, and outputs and serves as a guide for organising the annual report.
Figure 1 GHSC Programme Result Framework
17
5.2 PROGRAMME GOVERNANCE AND MANAGEMENT
Since its inception, GHSC has successfully mobilised a diverse but complementary team to deliver on a
complex scope of work. During the early months of Year 1, the team spent a significant amount of time
and effort developing and refining its work plan and shaping associated interventions to more closely align
with the Department’s strategic priorities, as outlined in the SIMA. To achieve this, the team categorised
activities into eight different “projects,” each of which features an AMD liaison person. This collaborative
structure proved highly successful throughout Year 2 and will continue to be a featured component of
GHSC TA support in South Africa.
During Year 2, the project structure and organisation was further refined, with the eight projects grouped
according to work streams which are further aligned to the objectives and sub-objectives defined in the
Results Framework.
All activities reflected in the Year 2 work plan formed the basis for quarterly detailed Wave Governance
(WG) plans, which were presented to the AMD, USAID, other implementing partners and donors. GHSC
TA personnel regularly reviewed progress against the WG plans with AMD and USAID.
In response to the aforementioned AMD deprioritisation of Health Technology Assessment (HTA) related
activities, PRICELESS withdrew from the consortium and concluded their activities at the end of March
2018, with all HTA deliverables completed and handed over to AMD. As mentioned, AMD has recently
expressed an interest in reinitiating HTA related activities during Year 3 for which discussions are
currently ongoing.
At the end of Year 1, the team consisted of 39 professionals providing technical assistance. During Year
2, the team grew to 42 with the addition of the following personnel:
● An IT Strategist & Programme Manager responsible for managing the projects related to the IT
landscape and master data;
● A supply chain planning subject matter expert, responsible for developing the demand, supply, and
distribution planning along with developing a supply chain segmentation strategy;
● A monitoring, evaluation and continuous improvement team member to assist with developing new
national and provincial KPIs and developing a continuous improvement methodology.
Other changes during Year 2 include realigning provincial support personnel to report to a single provincial
support team lead. This restructuring has provided a higher degree of coordination and alignment across
personnel supporting prioritised interventions in the provinces.
18
6. FINANCIAL STATUS OF THE TASK ORDER

19
20
7. ACHIEVEMENTS AND MAJOR ACTIVITIES BY OBJECTIVE
7.1 OBJECTIVE 1: IMPROVE SELECTION AND USE OF MEDICINES
Objective 1 encompasses technical assistance provided to AMD in the areas of HTA and RMU.
Establishment of a coherent medicine value chain from evidence based medicine selection to the rational
and effective use of medicines is imperative for improved clinical practice and patient outcomes.
7.1.1 SUB-OBJECTIVE 1.1: ASSIST WITH THE IMPLEMENTATION OF HTA
Activities and Impact
Activities under Objective 1 included finalisation of support on the Essential Medicine Electronic Access
(EMelA) system, as well as developing policies, guidelines, processes, and interventions to establish
governance frameworks for evidence-based medicine selection and the rational use of medicines. During
Year 2, many planned HTA activities were suspended at the request of AMD. Towards the end of the
period, however, the Director of AMD requested GHSC to again provide technical assistance with HTA.
Major activities and accomplishments associated with sub-objective 1.1 in Year 2 are outlined below:
● Developed a revised Draft Conflict of Interest Policy for the NEMLC and associated change
management plan. The revised policy adopts a more generic approach to managing potential conflicts
of interest involving committee members.
● Developed a revised version of the Reviewer’s Manual based on observations from the NEMLC and
Expert Review Committees (ERC) processes.
● Delivered cost-effectiveness, budget impact, and capacity-development analyses for tretinoin, long-
acting beta antagonists and fondaparinux. Provided reports to assist the NEMLC in considering the
cost-effectiveness and budget impact of inclusion of the medicines in the National Essential Medicines
List (EML).
● Supported recruiting of potential members of the Paediatric ERC, including developing interview
questions and evaluating applicants. Resulted in appointment of committee members, convening of the
committee and the assumption of its duties.
● GHSC personnel served as core team members assisting AMD in developing a new HTA strategy.
Looking Forward
● Finalizing the Conflict of Interest Policy
● Revising the existing Reviewer’s Manual
● Continuing support of AMD’s efforts to develop a new HTA Strategy.
7.1.2 SUB-OBJECTIVE 1.2: IMPROVE RATIONAL MEDICINE USE
Activities and Impact
Year 2 activities focused on evaluation and handover of EMelA, a web-based application that digitises the
STGs and the EML. The focus then shifted to developing policies, guidelines and interventions to promote
rational medicine use. Specific activities that took place in Year 2 included:
● Delivered the EMelA Phase I Evaluation Report following completion of an analysis of system
functionality. Due to identified functional limitations, AMD decided to cease further development and
implementation. Team personnel then assisted with the handover of documentation and the source
code from developers to AMD.
21
● Applied business rules and lessons learned from supporting the EMelA implementation to the
development of the AMD MMDS including the MHPL. Drafted a policy relating the management of
medicine master data that informs both system development and implementation, which is under
review.
● Provided input in the development of the content, graphics, and communication materials for
Pharmacy Month 2018’s theme, “Use Medicines Wisely.” The messaging launched in September with
the aim of enhancing communication between patients and pharmacists to improve rational and
appropriate medicine use.
● Working with the Essential Drugs Programme (EDP) to develop the National Formulary Guideline, a
strategically important document that guides the development, management, and use of formularies
at all levels of the health care system to promote improved RMU. Collected numerous stakeholder
inputs including principles on individual and special access to medicines by patients, which were aligned
with the national policy on patient referral and medicine master data.
● Provided support in quality control of data on EML Clinical Guide App, which serves as the primary
implementation mechanism of the STGs and EML, to improve the accuracy of information available to
healthcare professionals.
● Assisted the implementation and use of STGs by developing an explanation of major changes to the
STGs and their ramifications. This included summaries of significant decisions made by NEMLC related
to PHC during committee meetings from 2016 to 2018. The team tailored the messaging designed to
accelerate implementation of the revised PHC STGs and EML for target audiences, including simplifying the content for specific stakeholder groups with a particular focus on nurses.
● Developed multiple presentations designed to improve communication on EDP and STG/EML
processes for use by AMD at pharmaceutical conferences and other meetings.
● Drafted five MOUs that have been reviewed by NDoH’s Legal Unit and are awaiting sign off:
‒ NDoH and private laboratories,
‒ NDoH and the National Institute for Communicable Diseases,
‒ NDoH and the South African Society for Clinical Microbiology,
‒ NDoH and the Department of Agriculture, Forestry & Fisheries, and
‒ NDoH and National Health Laboratory Services.
Also developed an Antimicrobial Use Data Surveillance Framework in support of the MOUs.
● Developed a draft NEMLC Appeals Policy, which explains the procedure for lodging an appeal against
an NEMLC medicine related decision. The document is currently under review by the committee.
● Drafted an outline to shape the content of the future National Pharmaceutical and Therapeutics
Committee (PTC) Guideline, which was approved following incorporation of stakeholder comments.
Although delayed (at the request of AMD) due to other higher priority activities, the team has begun
developing new governance tools that will be included in the guideline. A major focus of Year 3 will
be refining and completing the guideline, which will serve as a critical tool in supporting PTC efficiency
and governance with the goal of improving RMU.
● Assisted drafting the National Referral Policy related to the medicine management principles. Created
scenarios to test alignment of the policy with the National Formulary Guideline principles. In addition,
the project provided inputs to the National Palliative Care Implementation Plan related to medicine
use.
22
Looking Forward
GHSC will assist EDP with developing relevant policies, procedures, and interventions for the rational
selection and use of medicines. During Year 3, the GHSC team will perform the following activities in
support of Objective 1.2:
● Developing the PTC Guideline, soliciting input and prioritise PTCs for implementation of the guideline
● Developing an implementation plan for the Formulary Tool of the AMD MMDS
● Finalizing the National Formulary Guideline and Medicine Master Data Policy
● Finalizing the NEMLC Appeals Policy
● Reviewing NEMLC governance documents including the Terms of Reference (TOR)
● Developing and implementing of an EDP Communications and Awareness Plan
7.2 OBJECTIVE 2: SUPPORT OPTIMISATION OF THE SUPPLY CHAIN
Optimising the supply chain is critical to improving availability of medicines and other health commodities
at the right place, at the right time, and in the right quantity. Activities undertaken by GHSC related to
Objective 2 include supporting the design and institutionalisation of elements of the Visibility Analytic
Network (VAN) operating model as well as implementing select components of the Provincial Medicine
Procurement Unit (PMPU) concept. Activities included within this objective also include improving
contracting and contract management.
7.2.1 SUB-OBJECTIVE 2.1: IMPROVE CONTRACTING
Activities and Impact
In Year 2, the GHSC team worked with the tender forecasting team to transition long-term forecasting
responsibilities to NDoH. Long-term forecasting will provide NDoH with improved demand projections
that inform the tendering process for national contracts. Specific activities performed include the
following:
● Conducted training on the demand planning process and the statistical forecasting tool, Forecast Pro
with focus on data cleansing, generating a baseline forecast using the statistical demand planning tool,
forecast enrichment, communicating the initial forecast to provinces and consolidating feedback
received.
● Supported AMD by assisting National Treasury (NT) with the loading and updating of National
Transversal Contracts for medicines and medical related items. This was necessary to populate the
master table used for procurement in gCommerce that will assist in expediting future contracting
processes and activities related to Contractual Price Adjustments (CPA).
Looking Forward
● Assisting NDoH personnel in becoming self-sufficient in generating, communicating and finalising
tender forecasts.
● Completing the tender forecasting guideline that will describe the process and activities associated
with incorporating demand planning information into upcoming tender forecasts.
23
7.2.2 SUB-OBJECTIVE 2.2: IMPROVE CONTRACT MANAGEMENT
Activities and Impact
Workforce Management
AMD requested GHSC TA personnel to provide workforce strengthening services for the CMU within
AMD. The subsequent intervention featured four areas of focus:
● People: Optimised the organisation design, job descriptions, performance measures, communications
and change management, and provided training, development and coaching.
● Governance and Processes: Established new, more efficient processes, frameworks and SOPs.
● Technology: Developed and optimised tools and reports to assist in monitoring and evaluating KPIs
for CMU staff and the whole unit.
● Monitoring and Evaluation: Performed quarterly assessments of the impact of the intervention to
measure improvement, tailor support, and promote continuous improvement and sustainability.
Developed and implemented recommendations to improve CMU operations including designing and
delivering the following:
● A strategy enabling capability map.
● A CMU organisational structure interaction model and performance management framework, with
revised job descriptions and individual performance management plans.
● Governance frameworks (decision making bodies and supporting terms of reference).
● Job impact assessments highlighting the change from the current to future jobs.
● Improved processes and procedures with accompanying SOPs.
Demand Forecasting
In-contract demand forecasting enables the NDoH to review the actual usage and future projected
demand of medicine against the original contracted volumes with suppliers, thus improving the NDoH’s
supplier management capabilities by providing greater insight into the projected requirements for a specific
medicine. GHSC TA support for demand forecasting included the following:
● Trained the national demand planning team on the new demand planning process.
● Provided detailed instruction on use of Forecast Pro, the demand planning forecasting tool, and enabling
activities like data analysis and cleansing and how those activities are used to support CMU’s contract
management responsibilities.
● Trained CMU personnel on developing in-contract forecasts and national level ad hoc forecasts in
response to emergent requests. Data from these forecasts provided CMU resources with greater
information and insight during their discussions with suppliers, allowing for more robust and
meaningful discussions/negotiations. Suppliers also benefitted from receiving a more highly refined
demand signal, which enabled them to better optimise their own operations.
Looking Forward
● Continuing to engage and strengthen contract management capabilities and further integrate demand
plans into contract oversight activities.
● Improving In-Contract demand planning by formally establishing a CMU team that reviews the forecast
against the original tender volumes and coordinates with suppliers to manage variances and adjust
rough-cut capacity plans.
24
7.2.3 SUB-OBJECTIVE 2.3: DESIGN SUPPLY CHAIN OPERATING MODEL
Activities and Impact
Demand, supply, and distribution planning (together known as Planning Services) are critical to improving
medicine availability and reducing stock outs at the provincial, district, and healthcare facility levels.
Demand Planning
In Year 2, GHSC led the implementation of demand planning at National and Provincial level. The objective
of the demand planning implementation is to provide improved projections of medicine demand for short,
medium and long-term requirements. This activity will inform the following:
● Supply planning regarding what medicine should be supplied, at what point of time, to which location.
● Contracting processes (see above).
● Financial management including budget reviews, establishing budget projections, tracking consumption
versus plan, and understanding the financial consequences of demand fluctuations.
During this period, GHSC performed the following activities:
● Investigated and documented options relating to different demand planning statistical forecasting tools
and supported AMD in selecting a “fit for purpose” tool—Forecast Pro.
● Conducted a demand planning Proof of Concept (POC) in the EC which offered team members the
opportunity to:
‒ assess the current process,
‒ adapt the design of the new demand planning process,
‒ implement Forecast Pro,
‒ evaluate the effectiveness of training courses and change management activities on the ability
of provincial teams to conduct demand planning, and
‒ test new demand planning KPIs
● Following the POC, the team delivered a post POC report including lessons learned which were
incorporated in updates to the process that are being rolled out to other provinces.
● Developed guidelines detailing the standard demand planning process, approach and implementation
methodology.
● Together with AMD counterparts, conducted forecast reviews and forecast enrichments, and
received approval of these forecasts as part of finalising the demand plan.
● Subsequently generated initial forecasts for several medicine contracts.
● Rolled out demand planning to the NW, which benefited from insights gained during the EC POC
resulting in production of initial demand forecasts.
Supply Planning (Informed Push)
To improve product availability, realise efficiencies, and reduce the risk of stock-outs, the GHSC team
developed a framework for implementing an Informed Push Model and refined the approach to enable
automated replenishment of stock at the lowest facility level. This activity should positively impact health
outcomes at rural clinics where sole practitioners, often nurses, will no longer have to generate orders
and can then focus additional time on patients.
25
● Proposed and began planning for a Supply Planning POC in NW to test automated replenishment
planning for two sites using RxSolution and two sites using the SVS during Year 3.
● Developed an inventory calculation tool to calculate minimum and maximum stock levels by facility,
which will also be tested as part of the POC.
● Developed an initial segmentation approach for assessing product volume, cost, and criticality—Vital,
Essential, or Non-Essential (VEN)—that will be used to focus planning activities on those medicines
with the greatest impact to health outcomes and the health supply chain.
Distribution Planning
Distribution planning did not formally commence in Year 2 though several GHSC TA personnel were
directly involved in optimising distribution operations in NW at AMD request. Contributions included the
following:
● Documenting the current state of primary (depot to hospital) and secondary (hospital to clinic)
transportation operations in the province including understanding volume and cost of transportation
● Identifying several opportunities to improve distribution operations including:
‒ Optimising routing and scheduling of outbound primary transportation from depot to
hospitals.
‒ Reducing the cost of outbound transportation by shifting from eight to four-ton trucks due
to a non-linear pricing model.
‒ Increasing the rate of depot deliveries from bi-weekly to weekly, which will reduce overall
inventory costs, largely covering commensurate increases in transportation spend while
improving velocity and medicine availability.
‒ Increasing the number of facilities receiving supplier Direct Deliveries (DDVs) which will
reduce the burden on depot staff, reduce transportation spend as many sites are closer to
supplier warehouses than the depot, improve responsiveness, and reduce losses due to
additional handling.
Looking Forward.
● Continuing to roll out demand planning in the provinces, providing training to provincial personnel on
the process and use of Forecast Pro.
● Institutionalising the roll of forecasting and demand planning in financial reporting and the budgeting
process.
● Reviewing a proposed centralisation of demand planning functions with AMD and if approved, agreeing
on an implementation approach.
● Completing the supply planning POC for NW, documenting lessons learned and updating the process
and min/max tool as required.
● Agreeing on an implementation plan for the roll out of supply planning to the rest of the provinces.
● Drafting a Supply Planning Guideline document similar to that produced for demand planning.
● Continuing to support NW’s efforts to improve distribution operations by implementing new routing
and scheduling, increasing supplier direct delivery, optimizing truck type, and increasing depot delivery
frequency.
7.2.4 SUB-OBJECTIVE 2.4: MAINTAIN AND IMPROVE SUPPLY CHAIN OPERATIONS
26
In Year 1 GHSC developed the Provincial Medicine Procurement Unit (PMPU) Blueprint, which aimed to
describe how the supply chain could be improved by strengthening transactional processes at provincial
level. During Year 2, GHSC conducted baseline assessments in eight provinces.
● The assessments highlighted the maturity level of nine critical elements - warehouse and infrastructure,
demand, supply and distribution planning, ordering, payment and financial management, contract
management, organisational design, as well as monitoring against KPIs.
● Key opportunities to strengthen the supply chain identified by the assessment included the following:
‒ Strengthening governance and leadership structures to streamline decision making, escalation,
delegation and monitoring and evaluation processes;
‒ Aligning roles within Pharmaceutical Services to the required capabilities to eliminate
duplication of roles and improve decision making;
‒ Improving planning capability, reviewing planning processes and systems at an operational level
to support efficient stock management;
‒ Strengthening financial practices and processes to promote effective governance including
consistency in accounting reports and supplier performance management; and
‒ Refining logistics networks to reduce lead times improve routing and scheduling of deliveries,
optimise management of transport cost and optimise safety stock levels.
The findings of these assessments will inform planning of future interventions at provincial level.
Support to North West Province
Activities and Impact
During May 2018, NW experienced a period of labour unrest, which led to the closure of the Provincial
Medical Depot in Mahikeng. Facing a crisis, AMD asked GHSC TA to establish and staff a temporary PMPU
at the NDoH, which processed and managed orders from Hospitals and Community Health Centres
(CHCs) across the province. Team personnel processed over 2,000 orders representing more than R 25
million in contracted pharmaceutical items and achieved AMD’s goal of rapidly shifting 100% of orders
from depot to supplier direct delivery—an achievement that fundamentally preserved medicine availability
throughout the province.
Following our success operating the temporary PMPU, NDoH prioritised NW as the next province to
receive supply chain strengthening initiatives once the labour unrest abated. GHSC TA personnel
subsequently focuses on strengthening five specific areas:
● workforce and organisational design
● planning services (demand, supply and distribution)
● financial management (ordering and payment processes)
● depot systems and processes
● network optimisation
A cross-functional project team from GHSC TA was deployed to conduct deep-dive assessments in each
of the five areas culminating in an ‘As-Is’ report highlighting the findings and recommendations for each of
the focus areas. The report was presented to the AMD Intervention Lead and the Provincial Administrator
who then asked the team to support provincial leadership in implementing recommended improvements
to each of the five areas.
27
Looking Forward
The supply chain strengthening team will continue to support implementation activities in the NW.
Lessons learned transforming supply chain operations and supporting activities will be applied to future
provincial interventions with anticipated continuing support of the following focus areas in NW subject to
provincial and AMD coordination:
● Optimising payment and financial management processes
● Implementing new Demand, Supply and Distribution planning services
● Continuing to refine and optimise distribution operations, reducing costs while preserving or
improving operational performance
Central Chronic Medicine Dispensing and Distribution (CCMDD)
Activities and Impact
The Central Chronic Medicine Dispensing and Distribution (CCMDD) programme, where repeat
prescriptions for chronic stable patients are dispensed centrally by contracted service providers and
delivered to a pick up point close to the patient’s home or work, is considered to be one of the flagship
programs of NDoH. Because of the nature of the programme, it is critical that CCMDD service providers
carry sufficient stock to enable prescriptions to be filled. Specific Year 2 CCMDD activities included:
● Worked with the CCMDD National Coordinator and AMD to develop and implement standardised
supply chain processes to support the programme. These processes aim at improving efficiency of the
CCMDD programme, provide guidance during review meetings, and facilitate escalation of process
inefficiencies.
● During the reporting period, NDoH contracted new service providers for the programme with GHSC
TA personnel playing a vital role in preparing for and supporting the transition of CCMDD services
to the new service providers.
Looking Forward
● Monitoring and supporting CCMDD supply chain performance across the provinces and identifying
opportunities to improve processes.
7.3 OBJECTIVE 3 - STRENGTHEN GOVERNANCE
One of the primary functions of AMD is to provide oversight and set policy for the provision of
pharmaceutical services in South Africa. GHSC TA activities in support of this objective include assisting
AMD in establishing relevant legislation and policies, developing appropriate governance structures to
improve accountability and oversight, and making data available for decision-making.
7.3.1 SUB-OBJECTIVE 3.1: CONTRIBUTE TO DEVELOPMENT OF POLICY AND LEGISLATION
Activities and Impact
Activities undertaken in this reporting period included the following:
● Worked with AMD on amendments proposed by the South African Pharmacy Council (SAPC) to
three sets of regulations published in terms of the Pharmacy Act 53 of 1974 (the Pharmacy Act) to
enable the education, registration, and practice of a new category of pharmacy support personnel -
pharmacy technicians. Following consultation and engagement with SAPC representatives and the
Legal Unit of NDoH, the regulations were submitted to the Office of the State Law Advisor for review.
28
● Supported AMD with the revision of draft regulations to be published in terms of the Pharmacy Act
dealing with continuing professional development of persons registered in terms of that Act. After
consultation with the SAPC and the Legal Unit of NDOH, and the incorporation of amendments
proposed by the State Law Advisers, the regulations were signed by the Minister and published for
public comment on 13 July.
● Supported AMD in the revision of the draft guidance for the issuing of pharmacy licences. After
consultation with the Legal Unit and a stakeholder engagement session, the document was finalised
and published in the Government Gazette on 22 December 2017 for public comment. Work is
underway with the task team to review public comment received.
● Assisted AMD in consulting with the South African Veterinary Council (SAVC) on amendments to the
Medicines and Related Substances Act 101 of 1965 (the Medicines Act) regarding the new requirement
that veterinarians must have a licence to dispense and compound medicines if they perform these
functions. After stakeholder engagement and consultation, the team prepared and submitted a
submission for exemption from this requirement to the Minister and the Director General. GHSC
TA personnel provided further assistance by preparing correspondence to the SAVC and suppliers of
medicine to veterinarians relating to a decision that the legislative requirement for vets to hold a
dispensing licence not be implemented at this time.
● Completed and submitted comment on two Board notices published by SAPC in terms of the
Pharmacy Act relating to Pharmacy Linked Distribution Points (PLDPs) and Competency Standards
for Pharmacists. GHSC provided technical assistance to AMD and participated in stakeholder
engagement on the PLDP Board Notice organised by SAPC. Input on the PLDP proposal was of
particular importance as implementation thereof could have a very serious impact on the CCMDD
programme.
● Supported AMD in the processing and consolidation of public comment received for implementation
of Global Trade Identification Number - GTIN-14 and data matrix barcodes published in the
Government Gazette on 15 September 2017. GHSC TA also supported AMD with the presentation
of progress made regarding implementation of GTIN-14 and data matrix barcodes at the GS1 Africa
Healthcare Conference held in Ethiopia. Based on learnings from the conference, a meeting with the
South African Health Products Regulatory Authority (SAHPRA) took place to discuss implementation
of the requirement for barcoding as per amendments to the General Regulations published in terms
of the Medicines Act of 25 August 2017. It was agreed that a Technical Working Group (AMD and
SAHPRA) be set up to develop guidelines for implementation. A barcoding concept note was
developed and submitted to AMD.
● Prepared and submitted a prioritised list of supply chain policies required to AMD.
Looking Forward
● Reviewing and incorporating comment from the State Law Advisors on the regulations published in
terms of the Pharmacy Act to enable the education, registration and practice of pharmacy technicians.
● Reviewing comment received on regulations to be published in terms of the Pharmacy Act dealing
with continuing professional development of persons registered in terms of that Act.
● Continuing working with the task team to review the criteria for pharmacy licences.
● Developing guidelines for labelling and identification of medicines as per amendments to the General
Regulations published in terms of the Medicines Act to incorporate barcoding.
● Providing additional policy related support as directed.
7.3.2 SUB-OBJECTIVE 3.2: SUPPORT THE IMPLEMENTATION OF GOVERNANCE
29
Activities and Impact
● Provided support to AMD in the revision of the norms and standards for the Pharmaceutical Services
Dashboard, which was presented at the National Health Council – Sub-Committee – Pharmaceutical
Services (NHC-SC-PS). The revised norms and standards were finalised and approved by AMD.
● Revised and submitted the TORs for the NHC-SC-PS and the Pharmaceutical Bid Specification
Committee to AMD.
● Assisted AMD in presentations to the Primary Health Care ERC and NEMLC on the principles of the
nurse prescriber policy. Both engagements highlighted the need for speedy implementation of all facets
of the policy (viz. legislative changes, finalisation of the competencies of nurses, appropriate training
of nurses, and developing an IT system to assist in managing the process).
● Provided support to the Foundation for Professional Development (FPD) for review of the draft
service level agreement between that body and the Gauteng Provincial Department of Health relating
to the project where private medical practitioners and pharmacies provide services to patients using
medicines and medical consumables provided by the province – GP Care Cell.
● Worked with AMD and Health Systems Trust (HST) to develop a full set of the documents required
for awarding new contracts for CCMDD service providers.
● Developed a pilot framework and a transition framework for use by AMD and support partners.
● Completed the TOR for the Programme Implementation Team (PIT) and Wave Governance (WG)
meetings, and finalised a set of KPIs to monitor the functioning of the WG mechanism, both of which
were accepted.
● Reviewed the Special Conditions of Contract document and proposed amendments required to align
the document with amendments to the Medicines Act, and the establishment of SAHPRA.
● Prepared input on draft Good Pharmacy Practice rules prepared by the SAPC on the services that can
be provided from a pharmacy (e.g., unit dose dispensing), pharmacy linked distribution points, and
other innovative models of service delivery.
● Finalised the SOP for Ideal Clinics regarding the disposal of obsolete and expired stock and submitted
to the Ideal Clinic team. Supported updating the Ideal Clinic tracer lists with the revised lists being
finalised during this period.
● In collaboration with HST, supported AMD with finalising a document describing criteria and standards
for external pick up points for patients receiving medicine for chronic diseases. AMD subsequently
submitted the document to the SAPC.
● Following a direct request from AMD for support, GHSC assisted EDP with improving governance
and management of requests for initiation of Third Line Antiretroviral Treatment (TLART) and
provincial procurement activities for associated commodities. Activities included the following:
‒ Commenced TLART work after achieving agreement with EDP on a high-level work plan,
detailing governance and system development activities.
‒ Conducted a situation analysis to provide a clear, detailed understanding of the current state
of processes and risks. Identified numerous opportunities to improve efficiency.
‒ Developed and/or revised multiple governance documents including the committee TOR, the
SOP outlining TLART procurement procedure, and an application guide for clinicians.
‒ Supported AMD at a meeting of the TLART Peer Review Committee held in May 2018.
Following the meeting, updated and submitted a revised committee TOR to EDP.
30
● Prepared a National KPI Dictionary describing the KPIs used by AMD to monitor progress toward
achieving the desired outcomes of the SIMA. AMD adopted the dictionary following consultation with
the provinces. The team then conducted assessments to gauge readiness to operationalise the KPIs
and developed continuous improvement plans to establish processes and procedures that align
operational plans to KPIs and APP targets. In cases where existing processes allow for required KPI
data to be retrieved and processed, the team developed new or updated existing dashboards.
● Developed new provincial KPIs in consultation with AMD, which were submitted to provinces for
comment. The provincial KPI Dictionary provides stakeholders with a standard set of common KPIs
used to measure the provincial progress in achieving SIMA outcomes.
● Developed a new governance framework that helps AMD apply a structured approach to developing
and shaping governance interventions and controls, as well as National Surveillance Centre (NSC)
roles and processes that drive use of dashboards and a culture of continuous improvement.
Looking Forward
● Finalising and implementing provincial KPIs.
● Supporting AMD in implementing and institutionalising the NSC roles and functions and the
implementation of continuous improvement plans.
7.3.3 SUB-OBJECTIVE 3.3: COORDINATION AND OVERSIGHT OF STAKEHOLDER ENGAGEMENT AND
COMMUNICATION ACTIVITIES
Activities and Impact
In Year 2, GHSC continued to support coordination and oversight of stakeholder engagement,
communication and change management activities related to programme interventions.
● Identified multiple stakeholder engagement and change management activities required to support
successful implementation of numerous interventions designed to improve supply chain performance
and patient outcomes. The team developed stakeholder maps, Responsible, Accountable, Consulted,
and Informed (RACI) analyses and communications plans for several initiatives including PuLSe,
Dashboards, IT System Landscape, Demand Planning, gCommerce, CMU and ISP units to inform
change management considerations and approaches.
● Held bi-weekly huddle sessions, quarterly pulse checks and regular engagement sessions with unit
personnel during the CMU intervention. The CMU team is currently in transition mode and have
assumed responsibility for the huddle sessions. GHSC personnel successfully applied a similar
engagement approach during the ISP intervention.
● Performed numerous change management and communications activities in support of the Provincial
RxSolution Transition Workshops including delivering presentations to Provincial IT practitioners,
super users, and Pharmaceutical Services representatives. Pre-transition and post-transition surveys
were distributed, collected, and reported on to improve future transition workshops.
● Established Provincial Steering Committees featuring key stakeholders to provide direction in supply
of pharmaceuticals and related products. These committees play a key role in governance and decision
making related to improving medicines availability.
Looking Forward
● Continuing numerous communications and change management activities in support of new policies,
processes, procedures, and system implementations.
● Applying lessons learned from past change management and stakeholder engagement activities to
future stakeholder interactions.

31
7.4 OBJECTIVE 4 – WORKFORCE MANAGEMENT
Activities included within this objective address the management of human resources within the medicine
supply chain, including addressing challenges relating to the lack of staff with the required capabilities, high
vacancy rates, uneven distribution of human resources, and the need to improve staff management and
retention. Year 2 focused on strengthening interventions and activities to improve workforce alignment,
performance management, operational management components and organisational structure for specific
units within AMD
7.4.1 SUB-OBJECTIVE 4.1: SUPPORT THE DEVELOPMENT OF STANDARDISED STRUCTURES, ROLES,
COMPETENCIES AND PERFORMANCE MANAGEMENT
Activities and Impact
During Year 2, GHSC TA personnel assisted both AMD functional units as well as multiple stakeholders
and organisations in NW
● Conducted two organisational interventions including efforts for CMU (described above) and a similar
intervention for AMD’s ISP. Each intervention featured a three-phased strengthening approach based
on assessment, design and implementation.
● Completed the “As-Is” Workforce and Organisational Design (OD) Assessment for ISP including
review of structures, job descriptions, processes and PMDS documents.
● Assisted in aligning AMD strategy with operational plans for CMU, ISP and AMD Governance Units.
● Completed the “To-Be” design of the ISP unit including:
‒ Capability maps focusing on business analysis, project management and systems;
‒ Organisational structure options with supporting job descriptions and PMDS documents;
‒ Interaction models;
‒ A project management lifecycle methodology with a supporting toolkit; and
‒ A governance framework highlighting decision making bodies and terms of reference
● Activities addressed functional, behavioural and performance aspects of the units. The team conducted
ongoing monitoring and evaluation of these interventions to measure sustained impact. Personnel
introduced continuous improvement supported by ‘huddle sessions’ that promote improved change
management. The team conducts brief weekly stand-up sessions to check in with unit members to
monitor and drive performance against departmental KPIs.
● Led a broad workforce management intervention in NW and provided technical assistance to other
work streams including gCommerce, SVS, RxSolution, Demand Planning, and PULSE.
Successful execution of these interventions and strengthening activities played a key role in improving
workforce organisation and are expected to materially improve performance.
● Assessed and provided new organisational designs, structures and supporting artefacts for three
organisational structures (CMU, ISP and NW).
● Drafted or updated 17 job profiles and performance assessment documents that to strengthen AMD,
CMU, ISP and NW workforce organisation. All AMD documents were signed by incumbents and
submitted to Human Resource Management (HRM).

32
Looking Forward
● Continue to monitor past workforce transformation activities and assess the degree to which change
is sustained. Personnel will maintain their high level of continued interaction with AMD, CMU, ISP,
and NW.
● Continue to provide work force transformation and organisational design services where required to
support rollout of new supply chain process and systems.
7.4.2 SUB-OBJECTIVE 4.2: CHANGE MANAGEMENT INSTITUTIONALISED
Activities and Impact
Year 2 featured greater emphasis on stakeholder engagement, communications, initial change
management, and training all of which form the cornerstones of effective and lasting change management.
Detail around this sub-objective is covered in other sections in the report where we explain our approach
to monitoring change and our periodic engagement with stakeholders and organisations to assess the
effectiveness and sustainability of previously implemented changes to people, processes, and systems.
7.4.3 SUB-OBJECTIVE 4.3: UPSKILLING AND MENTORING AND STAFF
Activities and Impact
In Year 2, the GHSC team focused on training, coaching upskilling and mentoring staff in order to affect
performance, impact and sustainability. Activities included:
● Designing and implementing the ‘To–Be’ training framework, curriculum, and pre-and post-knowledge
assessments for ISP.
● Aligning knowledge and skills requirements to operational plans, individual job descriptions, PMDS,
and departmental objectives of each unit.
● Training Provincial Medicine Liaison Officers (PMLOs) on workplace skills, enabling effective initiation
of roles and responsibilities as PMLOs form an important part of the contract management function
within the provinces.
● Engaging with and supporting Africa Resource Centre (ARC), South African Production and Inventory
Control Society (SAPICS), and the University of the Witwatersrand in the research and design of a
performance-based framework for a Heineken sponsored national training programme for national
and provincial supply chain managers and stakeholders.
● Conducted pre-and post-assessments of all training interventions.
Looking Forward
In Year 3, GHSC will continue to engage and strengthen AMD, focusing on the implementation of the To-
Be plan at ISP and the Master Data Project. Provincial strengthening and support will continue in NW, LP
and other provinces, as required by AMD. GHSC will continue to use the three-phased, continuous
improvement and sustainability approach, adapting to the needs of each strengthening intervention and
project.
7.5 OBJECTIVE 5 – STRENGTHEN INFORMATION SYSTEMS AND INFORMATION
MANAGEMENT
Technology and information systems are critical enablers of health supply chain performance and form a
cornerstone of the successful delivery of the SIMA. Key activities performed in support of this objective
33
include drafting an information technology architecture roadmap, and developing and deploying
information systems.
7.5.1 SUB-OBJECTIVE 5.1: DESIGN IT SYSTEM LANDSCAPE
Activities and Impact
Given criticality of IT systems in achieving improved health supply chain performance, AMD sought to
better understand the complexities of managing IT systems in their environment along with potential
approaches to information system management. To this end, the team drafted an IT Strategy and Roadmap
with a focus on improving interoperability and reporting visibility. In addition, during this period, personnel
supporting strengthening of information systems and information management including:
● Documented the existing IT landscape by mapping information systems to SIMA-defined functional
areas and provided a gap analysis between the IT Landscape and critical functions.
● Delivered a new IT strategy comprised of:
‒ a proposed IT operating model,
‒ an approach for managing the IT environment,
‒ an IT project methodology including all required templates needed to successfully deliver IT
projects, and
‒ an IT architecture approach to be followed when building IT components.
● Led workshops for the AMD team and partner organisations focusing on implementing the IT project
methodology. The team then piloted the IT project methodology during the master data project to
test and collect lessons learnt.
● Continued developing and refining the IT roadmap, which illustrates IT initiatives required to address
identified functional gaps and dependencies along with alignment to the SIMA roadmap. The IT
roadmap consists of two sections: one dealing with master data (e.g. the Master Health Product List
(MHPL)); and the other focused on transactional systems that support stock management, planning,
and reporting.
● Led two “IT think tank” meetings that helped shape the IT Steering Committee (ITSC), an advisory
body that will make recommendations on IT strategy and roadmap.
● Drafted the Terms of Reference (TOR) for the ITSC, which will govern the committee’s involvement
in finalising the IT Strategy and Roadmap during Year 3.
Looking Forward
● Working with AMD to finalise the IT Strategy and Roadmap and transition its maintenance to the ISP
unit.
● Supporting cyclical reviews and revisions of the IT Strategy and Roadmap.
● Providing technical assistance to AMD on:
‒ Procuring and sourcing of IT services (as required/directed)
‒ Creating concept notes for key initiatives arising from the roadmap prior to them becoming
official projects
‒ Socializing the strategy and roadmap with relevant stakeholders
● Assisting AMD with helping implementing partners and contractors to adhere to the new IT project
methodology
34
7.5.2 SUB-OBJECTIVE 5.2: PROVIDE SUPPORT TO STRENGTHEN ANALYTICS AND OVERSIGHT
Activities and Impact
Activities and impact on this sub-objective focus on improving surveillance and visibility across the end-
to-end supply chain in accordance with new national KPIs developed under Objective 3:
● Refined the PHC, Hospital and CCMDD dashboards to align with relevant supply chain management
KPIs.
● Developed a new Supplier Management Dashboard (consolidating the previous Supplier Performance
Dashboard, Age Analysis Dashboard & Pipeline Analysis Dashboard) to better convey information
related to contract management performance and associated KPIs.
● Conducted in-depth training sessions for CMU personnel on use of the PHC, Hospital and Supplier
Management Dashboards.
● Led training sessions for the Provincial Medicine Liaison Officers (PMLOs) on the PHC and Hospital
Dashboards.
● Developed several new dashboards specifically designed to support of the goal of hosting all
performance data in a single location and improve stakeholder access to information including:
‒ the Depot Dashboard,
‒ mobile versions of the PHC and Hospital Dashboards (which significantly improve access to
performance data in remote locations), and
‒ dashboards designed for remote Pharmacy Dispensing Units and the GP Care Cell project.
● The utility and popularity of the aforementioned and other dashboards created by GHSC TA
personnel have helped increase the number of facilities reporting performance data to the NSC to
3,604.
● Provided ongoing maintenance of existing dashboards and continued to pursue further automation
and harmonisation of data sources, processes, and visualisations.
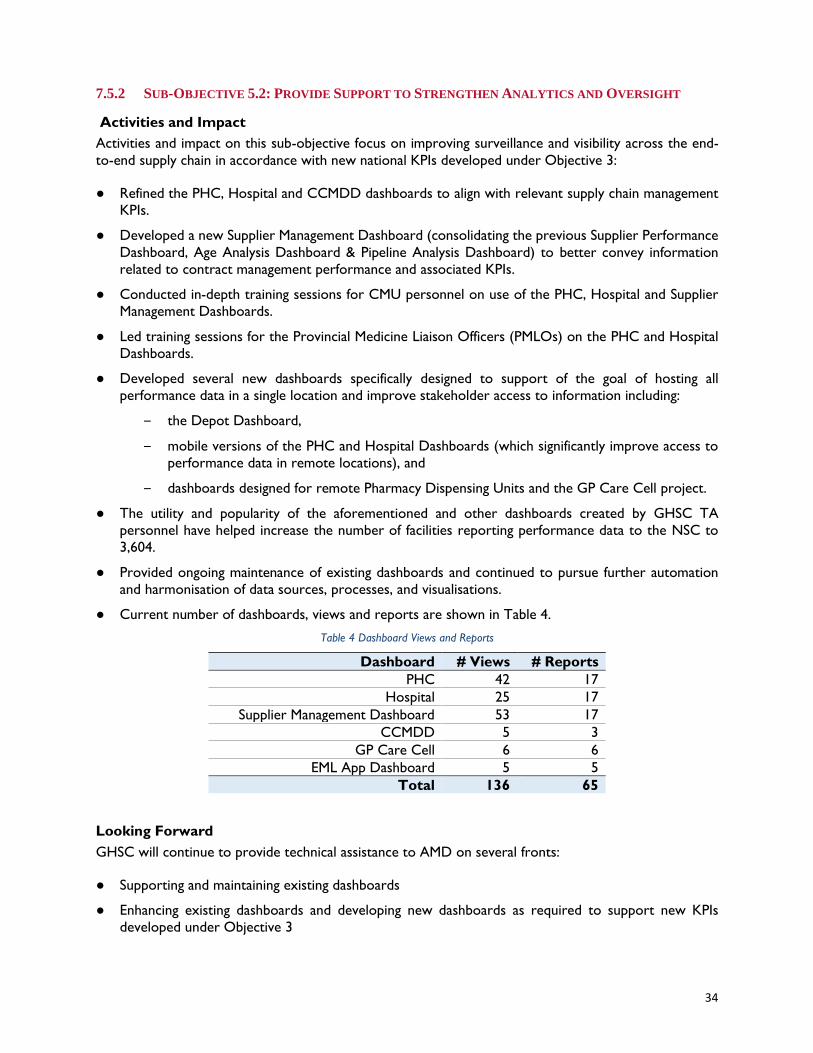
● Current number of dashboards, views and reports are shown in Table 4.
Table 4 Dashboard Views and Reports
Dashboard # Views # Reports
PHC 42 17
Hospital 25 17
Supplier Management Dashboard 53 17
CCMDD 5 3
GP Care Cell 6 6
EML App Dashboard 5 5
Total 136 65
Looking Forward
GHSC will continue to provide technical assistance to AMD on several fronts:
● Supporting and maintaining existing dashboards
● Enhancing existing dashboards and developing new dashboards as required to support new KPIs
developed under Objective 3
35
● Optimizing data sources and feeds for both new and existing dashboards
● Deploying dashboards to provinces and districts along with relevant training and coaching to help
institutionalise data centric management to improve medicine availability1
7.5.3 SUB-OBJECTIVE 5.3: SUPPORT THE IMPLEMENTATION OF DATA GOVERNANCE
Considered the most critical and foundational of IT initiatives within AMD, the Master Data project (SVS
phase III) will have a broad impact on other systems as well as AMD process capability. Aligning master
data across systems will form the basis for communication and passing of work across systems
(interoperability), and improve data aggregation and disaggregation for reporting (visibility). The master
data system will also support achieving the objectives described in the National Formulary Guideline and
AMD Medicine Master Data Policy.
Activities and Impact
GHSC team members have, and are currently supporting, the Master Data project as subject matter
specialists and have performed numerous activities in support of the effort:
● Conceptualised and developed a core data structure for AMD that draws on lessons learned from the
EMelA system development.
● Developed a prototype system to support the core data structure concept, which was then used to
demonstrate reporting across data entities.
● Used the prototype system to verify the suitability of the proposed data structure.
● Participated in review and testing of the first iteration of the online MHPL application and provision
of input to Mezzanine and AMD.
● Completed a detailed first draft of the medicines and repositories specifications (as an extension of
the overarching design specification) to achieve a full replacement of the current Medicine
Procurement Catalogue (MPC) which specifies the components from which medicines and other
system objects are built.
● Completed a first draft of the specifications for the “clinical setup” area of the MMDS, which, once
consultation with stakeholders is completed, will form the underlying system to support ePrescribing
and the revised Clinical Guideline application.
GHSC TA personnel also supported AMD’s efforts to build project management capacity within the ISP
unit through the following activities:
● Assisted the contracted service provider responsible for the master data project to adopt and apply
the new IT project methodology.
● Worked with stakeholders to develop and circulate the new Project Concept Note and Project
Initiation Document.
● Helped AMD expand the focus of the existing planning process from being more narrowly focused on
IT development to having a broader perspective that includes the impact of a project on master data.
Looking Forward
The GHSC team anticipates focusing Year 3 activities on several key areas:
1 This activity is dependent upon AMD’s pending procurement of Tableau user licenses.
36
● Drafting high-level master data requirements and design specifications for the overarching master data
design during sprint planning.
● Supporting the contracted service provider’s capturing requirements and design activities during each
master data sprint.
● Providing technical assistance on the approach for locating master data, developing a concept note for
the location master, and socialising the proposed approach with stakeholders.
● Providing technical inputs to concept notes and project initiation documents related to master data
integration for the RxSolution, RSA Pharma, and SVS systems.
● Supporting the contracted service provider’s master data design activities.
7.5.4 SUB-OBJECTIVE 5.4: ASSIST WITH DEVELOPMENT AND IMPLEMENTATION OF IT SYSTEMS
RxSolution Maintenance and Consolidation
Activities and Impact
RxSolution is a legacy application used in pharmacies in health care facilities for stock management and/or
dispensing. Support to the RxSolution implementation included:
● Assisted the transition of RxSolution support and maintenance to all provinces and, where applicable,
the relevant district support partners. Support calls are now routed directly to provincial call centres
where provincial support personnel are able to resolve calls/issues before escalating to NDoH.
● Helped develop a recommended provincial support structure featuring representatives from
Information and Communications Technology (ICT) and Pharmaceutical Services, to help provinces
better manage the RxSolution. Two provinces, North West and Gauteng, have subsequently
established RxSolution task teams, developed terms of reference, and have begun meeting quarterly
to address RxSolution-related topics.
● Collected and analysed data from the Rx databases for 176 Facilities in five provinces namely, EC, FS,
KwaZulu-Natal (KZN), NC and NW.
● Added 19 facilities to the hospital dashboard in two provinces namely, Eastern Cape and KZN as a
result of facility visits.
● Supported the successful pilot implementation of RxSolution in the Eden district in the Western Cape.
Looking Forward
● Developing an integrated helpdesk support plan for RxSolution that improves visibility into and
understanding of user challenges for both NDoH and the provinces.
RxSolution: Application Development
Activities and Impact
RxSolution is a legacy application running on a modern database (Microsoft Structured Query Language
(SQL) Server) with a Delphi frontend application. New technologies have been used by GHSC to create
a secondary application (middleware API) that bypasses the Delphi frontends and connects directly to the
SQL database. This application employs modern communication technologies to transmit reporting data
where communication networks exist. It is designed to automate reporting by facilities using RxSolution
to the hospital dashboard, thereby improving reporting compliance to the NSC and eliminating reliance
on provinces submitting manual reports. Activities and impact this period include:
37
● Completed the initial version of the “middleware API” and worked to optimise transmission of data
from remote sites to provincial servers and then to the NSC server (push model).
● Deployed the next iteration of the API to the FS provincial server with connects to remote sites. We
are now able to pull data to the provincial server without the need for software at the remote site
(pull model).
● Developed an improved push model installed remotely to manage sites that are not reachable through
the “pull model” by autonomously generating data files. The files are then automatically emailed to
the central server email address, where the central server monitors its email inbox and automatically
harvests the data from the incoming email attachment (push model that autonomously utilises email).
● Tested each of the applications described above to assess their ability to function while dealing with
“real world” issues typically experienced in field. Lessons learned are being applied to ongoing
improvements.
● Rolled out reporting middleware API (pull model) to collect data from 15 sites in the FS.
● Supported the Council for Scientific and Industrial Research (CSIR) in the redevelopment of the
RxSolution prescribing module, on to a modern technology stack. GHSC TA personnel provided
technical assistance in developing the concepts related to the prescribing module.
Looking Forward
● Developing a plan for refreshing the RxSolution store modules, including an architectural vision and
strategy for stock management with open architectural standards for integration and implementation.
● Providing technical assistance for efforts to refresh the RxSolution store modules.
● Automating hospital dashboard reporting for all sites.
SVS Phase I: Maintenance and Consolidation
Activities and Impact
The Stock Visibility System (SVS) is a mobile, internet-based application used to capture and view medicine
availability at PHC clinics on application enabled mobile devices. It is one of the flagship programmes of
NDoH, providing visibility of stock levels at 3,137 PHC clinics across the country. Initially only data relating
to ARV, anti-TB and vaccine commodities was captured. The item list has since been expanded to include
other commodities including contraceptives, psychiatric agents, anti-hypertensive and anti-diabetic agents
and is aligned with the tracer medicine list which forms part of the Ideal Clinic framework.
● Leveraged the implementation repository developed by GHSC personnel to guide provincial
engagement sessions with the various Heads of Health or their representatives. The repository
provided the framework and structure to be used to drive institutionalisation of SVS and improve
associated governance structures and processes.
● Developed a training pack used as the official guide during countrywide SVS refresher training provided
to national, provincial and district users. The revised training approach featured greater focus on
ensuring SVS users use the data and reports available to them to follow an evidence-based approach,
when carrying out routine activities linked to medicine availability monitoring. The training also
promoted sustainability and continuity by training-the-trainer, ensuring that provincial and district
champions are sufficiently trained and equipped to continue providing training across their provinces.
● Technical input was also provided to determine the necessary updates and implementation sequence
for planned changes to the existing SVS mobile application, which has not been altered since
implementation in 2014. These planned changes take into account end-user suggestions on how to
38
improve the application functionality and are designed to address common challenges mobile users
experience when using the system. These changes are due to be implemented in early 2019.
● Developed a time bound transition plan to guide the process of handing over management of all SVS
maintenance related activities to AMD. The plan was approved and will be implemented in Year 3
supported by extensive mentorship and coaching of personnel.
SVS Phase II: Development and Enhancement
Activities and Impact
The SIMA includes implementation of the Visibility and Analytics Network (VAN) as the operating model
to facilitate improved management of the medicine supply chain. One of the key features of the VAN is
the use of technology to support visibility and analytics functions. To this end, the Department’s vision is
to develop SVS to enable other medicine supply management processes, namely placing orders and
receiving stock electronically on mobile devices at PHC clinics. During this period GHSC:
● Developed user requirement specifications (URS) and incorporated them in a living document, which
was routinely updated and used to inform the detailed technical specification (Scope of Work) and
process flows.
● Developed and tested the non-interfaced receiving functionality in the test environment. AMD and
NC provincial procurement team and facility staff the conducted testing in accordance with the SVS
User Acceptance Testing (UAT) plan. Input collected during these sessions helped shape adjustments
to the app in preparation for pilot testing.
● Held project scoping workshops with multiple stakeholder representatives for the third-party systems
with which SVS is required to interface to support planned VAN supply chain system reforms. Input
from these sessions was used to inform all functional and technical specification documents.
Looking Forward
● Continuing to transition SVS maintenance activities to AMD to support sustainability and continuity.
● Supporting implementation of system enhancements to SVS to enable the devices to be used for
ordering and confirming receipt of medicines at PHC clinics. Efforts will focus on creating both non-
interfaced and interfaced versions.
● Expanding UAT to include other provinces and obtain a broad representation of end-user input to
inform newly developed functionality
WMS (gCommerce) Implementation
Activities and Impact
The gCommerce platform (previously known as Intenda Solution Suite) is a scalable, web-based, centrally
hosted suite of applications that includes a variety of modules, such as bid management, contract
management and warehouse management. The warehouse management module will provide depots with
the necessary tools to perform procurement and replenishment activities, as well as real time data to
undertake the demand forecasting and planning and supply planning services anticipated under the VAN
operating model. While the State Information Technology Agency (SITA) is responsible for
implementation, training and change management, GHSC has provided technical assistance in the
customisation of the application and implementation. GHSC personnel further provided critical support
to updating NT contracts used by the system to verify all contract-related data upon receipt of goods into
the system. Specific activities performed under this work stream included the following:
● Supported gCommerce rollout to a second province—the system is now used to manage provincial
depots in the NC and LP provinces.
39
● During this period, the SITA Cloud was developed, tested, and implemented to allow for Cloud
hosting and computing. This is a critical evolution allowing gCommerce to be hosted in a centrally
managed environment.
● Identified a number of system challenges during implementation, which GHSC personnel logged as
bugs and later monitored resolution thereof. System problems and bugs were documented and fixes
were prioritised in consultation with relevant stakeholders.
● Developed User Requirement Specifications (URS) for new system functionality to improve security,
productivity, and throughput.
● Supported the bi-annual stock take in the NC to assess functionalities of the upgraded version of
gCommerce implemented in the province during the course of the reporting period.
● Provided change management and communications support to SITA, with regard to implementation
of gCommerce in LP and Mpumalanga.
Looking Forward
● Supporting improvement of gCommerce functionality related to improving visibility into medicine
availability
● Finalising an approach to post pilot review to give guidance on improving the implementation of the
system in other provinces.
● Providing continued support to existing gCommerce sites
● Supporting the implementation of gCommerce in the other provinces as determined by the AMD
National gCommerce Steering Committee.
● Supporting the development and implementation of service level agreements between AMD, SITA and
NT, which has an impact on the roles and responsibilities between and across parties relating to
contracting and contract management.
PuLSe application development
Activities and Impact
The PuLSe system enables health care providers to apply for and manage dispensing licenses and permits
issued in terms of the Medicines Act, and yellow fever licences issued in terms of the International Health
Regulations online. The system is intended to replace an outdated and heavily paper based system, and
will enable efficiencies and promote good governance. During this period, personnel performed the
following:
● Supported completion of system set up and initial master data load including a legislative change, which
enables the issuing of permits to midwives allowing them to access highly scheduled medicines needed
in the provision of intrapartum care.
● Assisted AMD in negotiations with the South African Veterinary Council (SAVC) regarding
amendments to legislation, which would have required veterinarians to hold a dispensing license. The
inclusion of the management of dispensing licenses for veterinarians in the system was subsequently
halted as a result of a court decision.
● Collaborated with the EDP to revise lists of medicine which permit holders may use and supply, to
align them with the PHC (STGs/EML). Further consultation on these lists with key stakeholders is
ongoing.

40
● Developed, finalised, and obtained sign off from the NDoH Corporate Communications Department
on PuLSe communication materials, including training videos that educate health care professionals on
using the system.
● Finalised the PuLSe System Administrator User Manual and provided training to Licensing Unit staff.
Refined SOPs and processes as needed based on staff feedback. Finalised the monitoring and evaluation
framework and reports to be generated from the system.
● Held discussions with the NDoH division responsible for NHI systems and the CSIR about the
purpose and functionality of the system, and possible linkages between PuLSe and the provider
enrolment application CSIR is developing. This opportunity will be further explored in Year 3.
● Conducted extensive internal UAT of the system and performed bug fixing as needed. After
completing testing, AMD decided that PuLSe should undergo further Administrative Function Testing
(AFT) prior to the outward facing (self-service) functionality going online. This decision resulted in the
need to develop various workarounds and the redesign of forms, SOPs, and guidelines, all of which
were completed.
● Presented the PuLSe system to NDoH’s ICT Steering Committee and obtained to continue
development.
● NDoH and SITA ultimately decided that PuLSe should be hosted by SITA in line with an existing
business agreement between both parties. The process of transitioning from NDoH to SITA proved
challenging, resulted in considerable delays, and is projected to be completed in Year 3.
Looking Forward
● Continuing to resolve hosting challenges followed by commencing additional AFT once PuLSe has
been transitioned to a secure host.
● Consulting with stakeholders on the medicine lists followed by submission of revised lists to NEMLC
for approval. Once approved, they will uploaded to the PuLSe application.
● External testing has been planned and all communication, SOPs, process flows, and other relevant
materials have been created and are ready for distribution. Once the AFT phase is completed, the
team will proceed with external testing.
● Following successful external testing, supporting application go live featuring a phased on-boarding of
healthcare professionals.
7.6 OBJECTIVE 6 - IMPROVE FINANCIAL MANAGEMENT
This objective aims to improve financial management processes including budgeting and forecasting,
financial monitoring, and reporting against the budget for both the Chief Directorate: SWP within NDOH
and in assisted provinces.
7.6.1 SUB-OBJECTIVE 6.1: IMPROVE FORECASTING AND BUDGET INFORMATION
AMD budgeting and reporting is performed at the directorate level. The objectives of this intervention
are to improve budgeting and forecasting, as well as monitoring and reporting.
Activities and Impact
● Conducted an ‘As-Is’ assessment of SWP’s budget processes to obtain a more detailed understanding
of current budget related processes and activities.
● Designed SOPs aimed at improving budget management within the directorates in SWP and provided
training on SOPs for personnel from multiple directorates.
41
● Assisted with and provided guidance on the budget forecasting for the 2018/19 financial year for each
of the directorates within SWP.
● As part of the demand forecasting and planning activities in the EC POC, GHSC personnel
demonstrated how the demand forecast can be used to improve budgeting for medicines and other
health commodities. The team explained how to “cash-up” the demand forecast to arrive at a
recommended budget and how the “cash-up” value of future medicine demand can be incorporated
in both national and provincial budgeting activities.
Looking Forward
● Implementing newly developed budget related SOPs.
● Providing improved, demand informed inputs to budgeting and forecasting during the compilation of
the 2019/20 budget.
7.6.2 SUB-OBJECTIVE 6.2: ASSIST TO STRENGTHEN ACCOUNTING PROCESSES
Activities and Impact
As part of the NW intervention, GHSC TA personnel conducted an intensive analysis of current Accounts
Payable processes and activities related to or directly impacting health supply chain performance. Specific
activities included:
● Evaluated the state of finance/accounting structures, capturing, processing, monitoring and reporting,
as well as Supplier Relationship Management activities to determine their suitability in achieving
compliance with the Public Finance Management Act (PFMA).
● Traced invoice processing activities through the end-to-end payment process documenting touch
points with key stakeholders and organisations.
● Delivered comprehensive process maps detailing specific actions executed by members of Provincial
Treasury, Accounting and Purchasing Departments.
● Measured cycle times including delivery-to-documents-received, documents-receipt-to-payment-
pack-submission, payment-pack-processing at the provincial office, and billing-pack-data-submission to
Treasury for disbursement.
● Identified numerous inefficiencies in existing processes including parallel processes performed using
manual ledgers that hindered the use of the existing ORACLE system functionalities. Other
opportunities for improvement include:
‒ Redefining financial delegations for various sized procurements – both positions and
thresholds.
‒ Increasing the pool of signatories to expedite payment processes along with designating
alternates.
‒ Creating a shared payment service centre for medicines and surgical supplies at the Depot.
‒ Automatic routing of invoices for payment to the appropriate person required for processing
to reduce processing time and create an audit trail that enables visibility & control over the
entire process.
Looking Forward
● Continuing to support the NW province’s efforts to improve Accounts Payable performance and
drive down the Supplier Direct Delivery invoice backlog.

42
● Conducting targeted interventions based on provincial ‘As-Is’ assessments to strengthen accounting
processes.
7.6.3 SUB-OBJECTIVE 6.3: ASSIST TO IMPROVE FINANCIAL MONITORING AND REPORTING
Activities and Impact
● Analysed SWP’s actual expenditures for the 2017/18 fiscal year to better allocate actual expenditure
per directorate.
● Compiled a Finance Dashboard based on the expenditure analysis to assist the directorates with
monthly monitoring and reporting their budget execution.
Looking Forward
● Reviewing the expenditure analysis for 2018/19 and updating the Finance Dashboard accordingly.
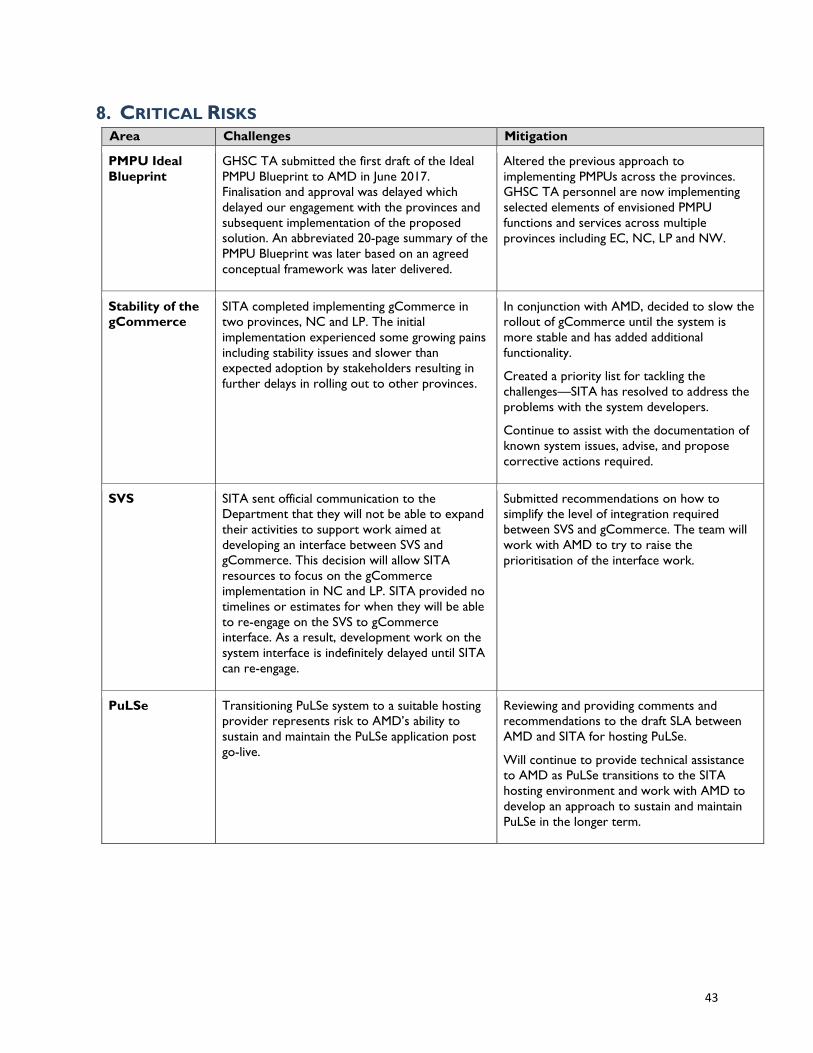
43
8. CRITICAL RISKS Area Challenges Mitigation
PMPU Ideal
Blueprint
GHSC TA submitted the first draft of the Ideal
PMPU Blueprint to AMD in June 2017.
Finalisation and approval was delayed which
delayed our engagement with the provinces and
subsequent implementation of the proposed
solution. An abbreviated 20-page summary of the
PMPU Blueprint was later based on an agreed
conceptual framework was later delivered.
Altered the previous approach to
implementing PMPUs across the provinces.
GHSC TA personnel are now implementing
selected elements of envisioned PMPU
functions and services across multiple
provinces including EC, NC, LP and NW.
Stability of the
gCommerce
SITA completed implementing gCommerce in
two provinces, NC and LP. The initial
implementation experienced some growing pains
including stability issues and slower than
expected adoption by stakeholders resulting in
further delays in rolling out to other provinces.
In conjunction with AMD, decided to slow the
rollout of gCommerce until the system is
more stable and has added additional
functionality.
Created a priority list for tackling the
challenges—SITA has resolved to address the
problems with the system developers.
Continue to assist with the documentation of
known system issues, advise, and propose
corrective actions required.
SVS SITA sent official communication to the
Department that they will not be able to expand
their activities to support work aimed at
developing an interface between SVS and
gCommerce. This decision will allow SITA
resources to focus on the gCommerce
implementation in NC and LP. SITA provided no
timelines or estimates for when they will be able
to re-engage on the SVS to gCommerce
interface. As a result, development work on the
system interface is indefinitely delayed until SITA
can re-engage.
Submitted recommendations on how to
simplify the level of integration required
between SVS and gCommerce. The team will
work with AMD to try to raise the
prioritisation of the interface work.
PuLSe Transitioning PuLSe system to a suitable hosting
provider represents risk to AMD’s ability to
sustain and maintain the PuLSe application post
go-live.
Reviewing and providing comments and
recommendations to the draft SLA between
AMD and SITA for hosting PuLSe.
Will continue to provide technical assistance
to AMD as PuLSe transitions to the SITA
hosting environment and work with AMD to
develop an approach to sustain and maintain
PuLSe in the longer term.
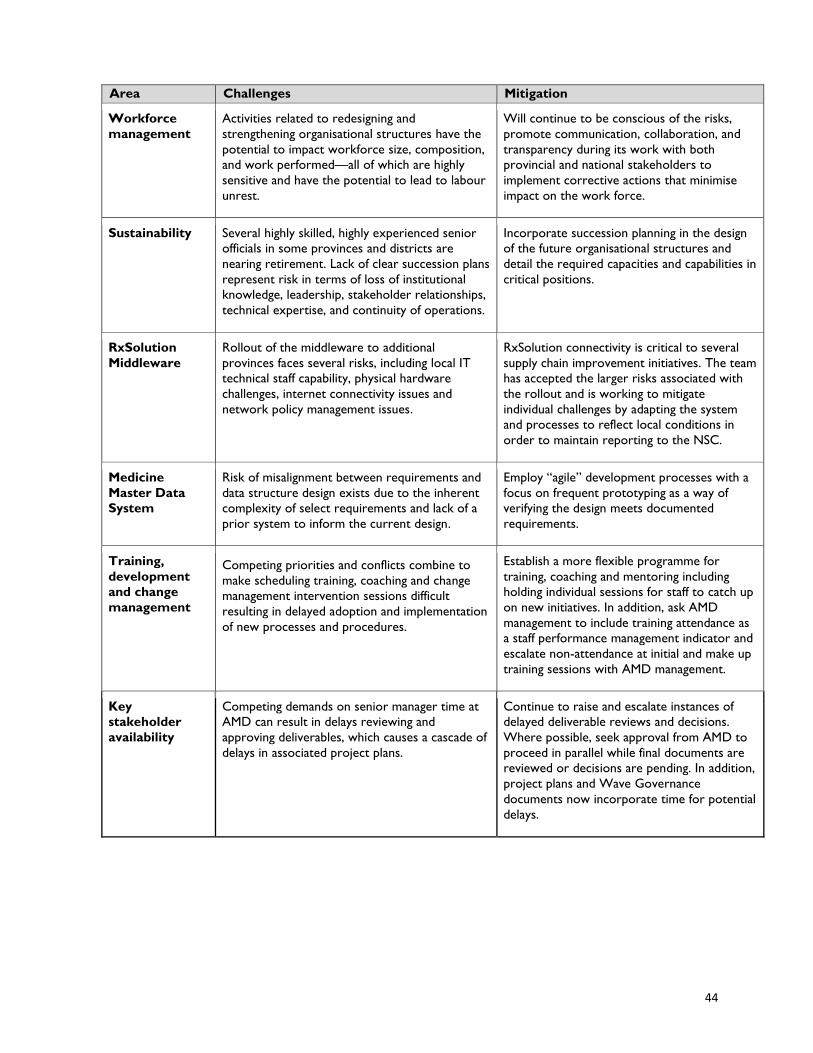
44
Area Challenges Mitigation
Workforce
management
Activities related to redesigning and
strengthening organisational structures have the
potential to impact workforce size, composition,
and work performed—all of which are highly
sensitive and have the potential to lead to labour
unrest.
Will continue to be conscious of the risks,
promote communication, collaboration, and
transparency during its work with both
provincial and national stakeholders to
implement corrective actions that minimise
impact on the work force.
Sustainability Several highly skilled, highly experienced senior
officials in some provinces and districts are
nearing retirement. Lack of clear succession plans
represent risk in terms of loss of institutional
knowledge, leadership, stakeholder relationships,
technical expertise, and continuity of operations.
Incorporate succession planning in the design
of the future organisational structures and
detail the required capacities and capabilities in
critical positions.
RxSolution
Middleware
Rollout of the middleware to additional
provinces faces several risks, including local IT
technical staff capability, physical hardware
challenges, internet connectivity issues and
network policy management issues.
RxSolution connectivity is critical to several
supply chain improvement initiatives. The team
has accepted the larger risks associated with
the rollout and is working to mitigate
individual challenges by adapting the system
and processes to reflect local conditions in
order to maintain reporting to the NSC.
Medicine
Master Data
System
Risk of misalignment between requirements and
data structure design exists due to the inherent
complexity of select requirements and lack of a
prior system to inform the current design.
Employ “agile” development processes with a
focus on frequent prototyping as a way of
verifying the design meets documented
requirements.
Training,
development
and change
management
Competing priorities and conflicts combine to
make scheduling training, coaching and change
management intervention sessions difficult
resulting in delayed adoption and implementation
of new processes and procedures.
Establish a more flexible programme for
training, coaching and mentoring including
holding individual sessions for staff to catch up
on new initiatives. In addition, ask AMD
management to include training attendance as
a staff performance management indicator and
escalate non-attendance at initial and make up
training sessions with AMD management.
Key
stakeholder
availability
Competing demands on senior manager time at
AMD can result in delays reviewing and
approving deliverables, which causes a cascade of
delays in associated project plans.
Continue to raise and escalate instances of
delayed deliverable reviews and decisions.
Where possible, seek approval from AMD to
proceed in parallel while final documents are
reviewed or decisions are pending. In addition,
project plans and Wave Governance
documents now incorporate time for potential
delays.
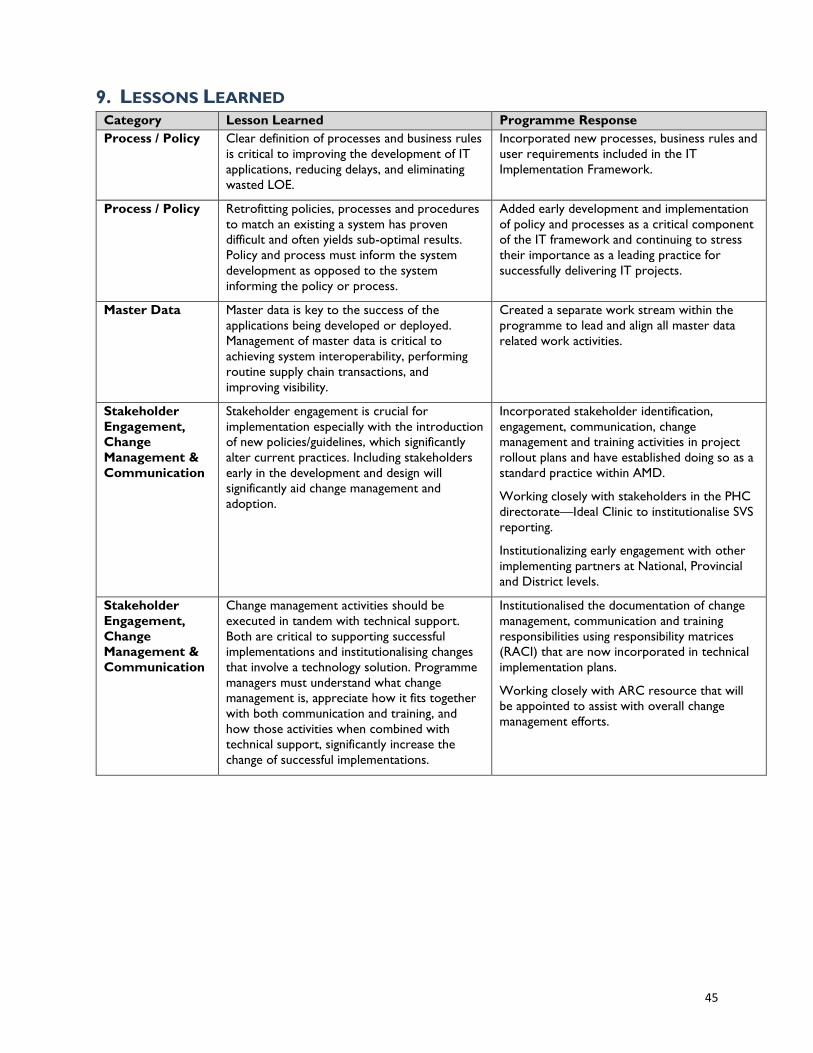
45
9. LESSONS LEARNED Category Lesson Learned Programme Response
Process / Policy Clear definition of processes and business rules
is critical to improving the development of IT
applications, reducing delays, and eliminating
wasted LOE.
Incorporated new processes, business rules and
user requirements included in the IT
Implementation Framework.
Process / Policy Retrofitting policies, processes and procedures
to match an existing a system has proven
difficult and often yields sub-optimal results.
Policy and process must inform the system
development as opposed to the system
informing the policy or process.
Added early development and implementation
of policy and processes as a critical component
of the IT framework and continuing to stress
their importance as a leading practice for
successfully delivering IT projects.
Master Data Master data is key to the success of the
applications being developed or deployed.
Management of master data is critical to
achieving system interoperability, performing
routine supply chain transactions, and
improving visibility.
Created a separate work stream within the
programme to lead and align all master data
related work activities.
Stakeholder
Engagement,
Change
Management &
Communication
Stakeholder engagement is crucial for
implementation especially with the introduction
of new policies/guidelines, which significantly
alter current practices. Including stakeholders
early in the development and design will
significantly aid change management and
adoption.
Incorporated stakeholder identification,
engagement, communication, change
management and training activities in project
rollout plans and have established doing so as a
standard practice within AMD.
Working closely with stakeholders in the PHC
directorate—Ideal Clinic to institutionalise SVS
reporting.
Institutionalizing early engagement with other
implementing partners at National, Provincial
and District levels.
Stakeholder
Engagement,
Change
Management &
Communication
Change management activities should be
executed in tandem with technical support.
Both are critical to supporting successful
implementations and institutionalising changes
that involve a technology solution. Programme
managers must understand what change
management is, appreciate how it fits together
with both communication and training, and
how those activities when combined with
technical support, significantly increase the
change of successful implementations.
Institutionalised the documentation of change
management, communication and training
responsibilities using responsibility matrices
(RACI) that are now incorporated in technical
implementation plans.
Working closely with ARC resource that will
be appointed to assist with overall change
management efforts.
46
10. PERFORMANCE MONITORING During Year 2, the programme was able to collect and report on 15 of the programme’s 20 key
performance indicators (KPIs). These include 12 annual indicators and three of the endline indicators, on
which the programme was able to collect preliminary data. The following section highlights progress made
against these 15 indicators, with 86% of targets having been achieved, exceeded or on track. Of note is
the performance monitored by KPI 17 where the programme exceeded the target of 100% of APP facilities
reporting to the NSC with 3,604 facilities reporting by the end of the reporting period.
Due to unavailable data, the programme was not able to report on KPIs 1, 3 and 20 as well as
baseline/endline KPIs 2 and 6. Activities related to indicators 1, 2, 3, and 6 were suspended during Year 2
due to deprioritisation of HTA activities by AMD. The GHSC programme has, however, been asked to
again support these activities. In addition, the data source originally planned to inform KPI 20 does not
provide the level of detail necessary to track the submission of payment packs. The programme is working
to address this challenge through the design and launch of gCommerce. Each KPI is discussed in detail
below.
10.1 OBJECTIVE 1: IMPROVE THE SELECTION AND USE OF MEDICINE.
The GHSC programme’s theory of change posits that the establishment of a coherent medicine value
chain from evidence-based medicine selection to the rational and effective use of medicines is imperative
for improved clinical practice and patient outcomes. With this in mind, objective 1 focuses on the delivery
of technical assistance to AMD in the areas of HTA (sub-objective 1.1) and RMU (sub-objective 1.2) in
efforts to improve the selection and use of medicines.
10.1.1 SUB-OBJECTIVE 1.1: ASSIST WITH THE IMPLEMENTATION OF HEALTH TECHNOLOGY
ASSESSMENTS.
Under sub-objective 1.1, the programme seeks to measure the effects of the GHSC intervention of
assisting the implementation of HTAs at the outcome levels by examining the number of medicine reviews
conducted by the ERCs, the capacity of medicine selection staff and committee members to perform and
interpret medicine reviews, and the utilization of HTA outputs. Performance to date against the
programme’s outcome level KPIs under sub-objective 1.1 are described below.
Key Performance Indicator 1: Number of medicine reviews conducted by the Expert
Review Committees.
Key performance indicator (KPI) 1 examines the maturity of the medicine selection process utilised by
measuring the number of medicine reviews conducted by the ERCs, which provide recommendations to
the NEMLC. The ERCs support the selection of medicines by determining whether to add, remove, or
change a medicine on the national EML, by assessing and appraising evidence presented during medicine
reviews. Due to confidentiality concerns raised by AMD, it has not been possible to access the only
available data source for this KPI, namely the minutes of meetings of the ERCs to determine the number
of medicine reviews conducted.
Key Performance Indicator 2: Percentage of medicine selection staff and committee
members trained that demonstrate an increased level of self-assessed skills and knowledge
to perform and interpret medicine reviews.
The GHSC programme seeks to build the capacity of ERCs to perform and interpret medicine reviews to
improve medicine selection. Informed by the programme’s customized Skills, Attitudes, and Knowledge
Questionnaire, KPI 2 seeks to measure improvements in the knowledge and skills of trained ERC members
to perform and interpret medicine reviews. Using this questionnaire to determine a baseline, the
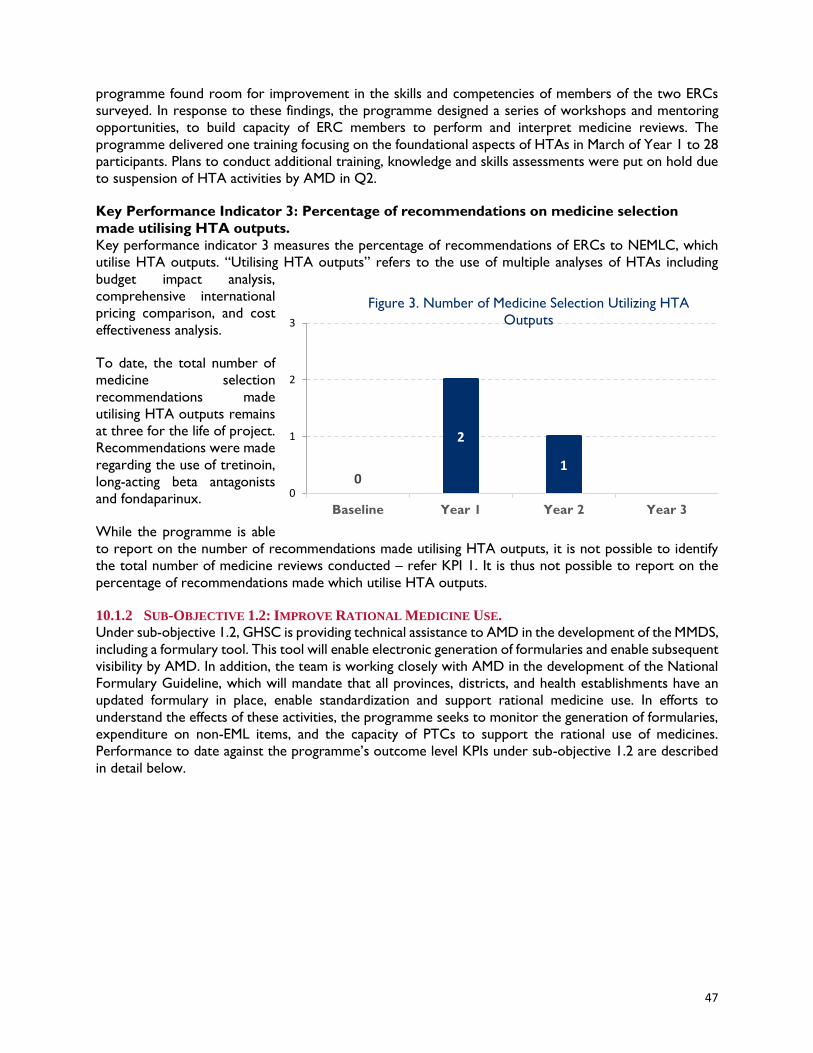
47
programme found room for improvement in the skills and competencies of members of the two ERCs
surveyed. In response to these findings, the programme designed a series of workshops and mentoring
opportunities, to build capacity of ERC members to perform and interpret medicine reviews. The
programme delivered one training focusing on the foundational aspects of HTAs in March of Year 1 to 28
participants. Plans to conduct additional training, knowledge and skills assessments were put on hold due
to suspension of HTA activities by AMD in Q2.
Key Performance Indicator 3: Percentage of recommendations on medicine selection
made utilising HTA outputs.
Key performance indicator 3 measures the percentage of recommendations of ERCs to NEMLC, which
utilise HTA outputs. “Utilising HTA outputs” refers to the use of multiple analyses of HTAs including
budget impact analysis,
comprehensive international
pricing comparison, and cost
effectiveness analysis.
To date, the total number of
medicine selection
recommendations made
utilising HTA outputs remains
at three for the life of project.
Recommendations were made
regarding the use of tretinoin,
long-acting beta antagonists
and fondaparinux.
While the programme is able
to report on the number of recommendations made utilising HTA outputs, it is not possible to identify
the total number of medicine reviews conducted – refer KPI 1. It is thus not possible to report on the
percentage of recommendations made which utilise HTA outputs.
10.1.2 SUB-OBJECTIVE 1.2: IMPROVE RATIONAL MEDICINE USE.
Under sub-objective 1.2, GHSC is providing technical assistance to AMD in the development of the MMDS,
including a formulary tool. This tool will enable electronic generation of formularies and enable subsequent
visibility by AMD. In addition, the team is working closely with AMD in the development of the National
Formulary Guideline, which will mandate that all provinces, districts, and health establishments have an
updated formulary in place, enable standardization and support rational medicine use. In efforts to
understand the effects of these activities, the programme seeks to monitor the generation of formularies,
expenditure on non-EML items, and the capacity of PTCs to support the rational use of medicines.
Performance to date against the programme’s outcome level KPIs under sub-objective 1.2 are described
in detail below.
0
2
1
0
1
2
3
Baseline Year 1 Year 2 Year 3
Figure 3. Number of Medicine Selection Utilizing HTA
Outputs

48
Key Performance Indicator 4: Number of formularies generated.
Key performance indicator 4 measures the number of formularies generated and will monitor
implementation of the formulary tool once finalised and implemented. In the interim, the number of
provinces with a provincial
formulary, as reported to the
Pharmaceutical Services
Dashboard, the system on which
provinces report performance
against a defined set of standards,
is monitored.
During the last two quarters of
Year 2, the dashboard was not
accessible due to a change in the
hosting platform. During the
transition period, provinces were
unable to access the dashboard to
upload data. The Year 2 data is
informed by the most recent dashboard, as reported at the end of the second quarter of the year. As
demonstrated in Figure 4, five of nine provinces reported that a provincial formulary had been generated
and uploaded on the system.
Key Performance Indicator 5: Percentage of expenditures on non-Essential Medicine List
items.
Key performance indicator 5
highlights implementation of the
STGs and EML, by measuring the
percentage of expenditure on
non-EML items by provinces. This
data is reported for provinces by
the Pharmaceutical Services
Dashboard.
As previously noted in relation to
KPI 4 above, the dashboard was
not available during the last two
quarters of the year and the data
is as reported at the end of the
second quarter. During the
period for which data is available, provinces reported 1.6% expenditure on non-EML items against a target
of less than 10%, demonstrating an improvement of 0.7 percentage as compared to Year 1 shown in Figure
5.
Key Performance Indicator 6: Percentage of assisted Pharmaceutical and Therapeutics
Committees with advanced or optimal capacity.
Key performance indicator 6 measures the operational capacity of PTCs by assessing governance, member
management, and performance of core PTC functions. Improvements to PTC operational capacity will
result in strengthened rational medicine use.
To date, the programme has not provided direct assistance to PTCs and does not anticipate doing so until
after Year 3, following the completion of the PTC Guideline, which will include a set of assessment criteria
4 5 5
9 9 9 9
0
2
4
6
8
10
Baseline Year 1 Year 2 Year 3
Figure 4. Number of Provincial Formularies Generated
Performance
Target
1,9% 2,3%1,6%
10% 10% 10% 10%
0%
2%
4%
6%
8%
10%
12%
Baseline Year 1 Year 2 Year 3
Figure 5. Percentage of Expenditures on Non-Essential
Medicine List Items
Performance
Target
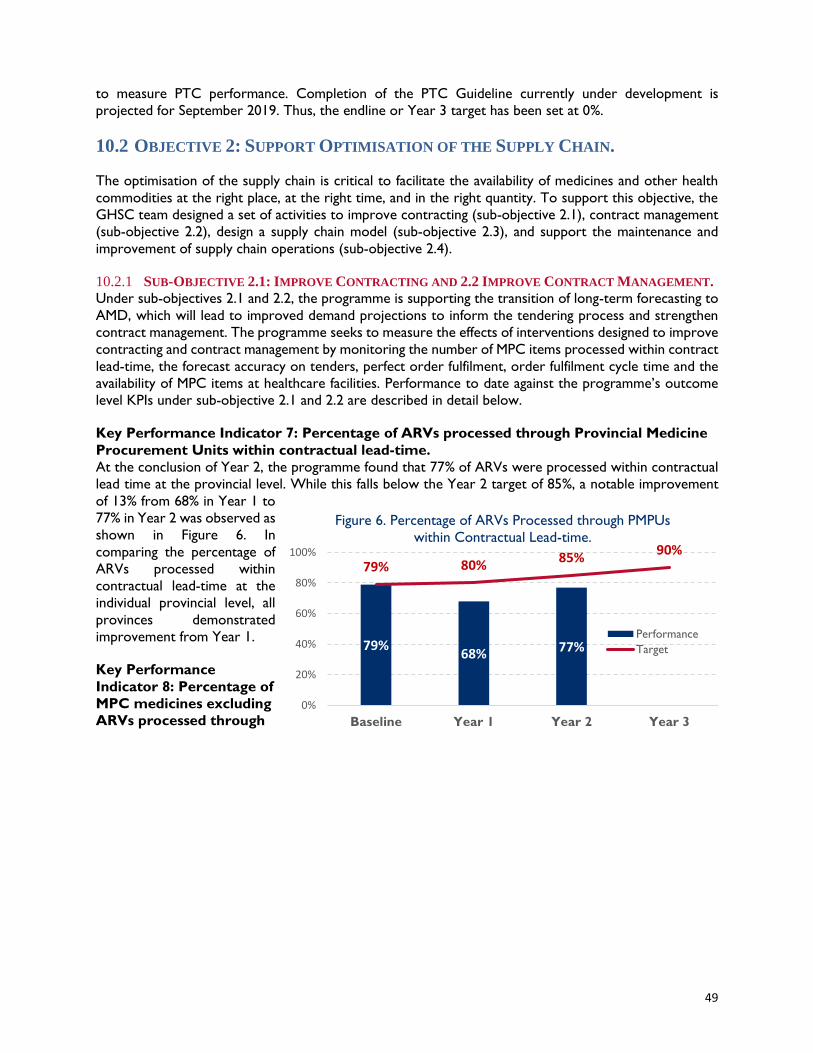
49
to measure PTC performance. Completion of the PTC Guideline currently under development is
projected for September 2019. Thus, the endline or Year 3 target has been set at 0%.
10.2 OBJECTIVE 2: SUPPORT OPTIMISATION OF THE SUPPLY CHAIN.
The optimisation of the supply chain is critical to facilitate the availability of medicines and other health
commodities at the right place, at the right time, and in the right quantity. To support this objective, the
GHSC team designed a set of activities to improve contracting (sub-objective 2.1), contract management
(sub-objective 2.2), design a supply chain model (sub-objective 2.3), and support the maintenance and
improvement of supply chain operations (sub-objective 2.4).
10.2.1 SUB-OBJECTIVE 2.1: IMPROVE CONTRACTING AND 2.2 IMPROVE CONTRACT MANAGEMENT.
Under sub-objectives 2.1 and 2.2, the programme is supporting the transition of long-term forecasting to
AMD, which will lead to improved demand projections to inform the tendering process and strengthen
contract management. The programme seeks to measure the effects of interventions designed to improve
contracting and contract management by monitoring the number of MPC items processed within contract
lead-time, the forecast accuracy on tenders, perfect order fulfilment, order fulfilment cycle time and the
availability of MPC items at healthcare facilities. Performance to date against the programme’s outcome
level KPIs under sub-objective 2.1 and 2.2 are described in detail below.
Key Performance Indicator 7: Percentage of ARVs processed through Provincial Medicine
Procurement Units within contractual lead-time.
At the conclusion of Year 2, the programme found that 77% of ARVs were processed within contractual
lead time at the provincial level. While this falls below the Year 2 target of 85%, a notable improvement
of 13% from 68% in Year 1 to
77% in Year 2 was observed as
shown in Figure 6. In
comparing the percentage of
ARVs processed within
contractual lead-time at the
individual provincial level, all
provinces demonstrated
improvement from Year 1.
Key Performance
Indicator 8: Percentage of
MPC medicines excluding
ARVs processed through
79%68% 77%
0%
79% 80%85%
90%
0%
20%
40%
60%
80%
100%
Baseline Year 1 Year 2 Year 3
Figure 6. Percentage of ARVs Processed through PMPUs
within Contractual Lead-time.
Performance
Target
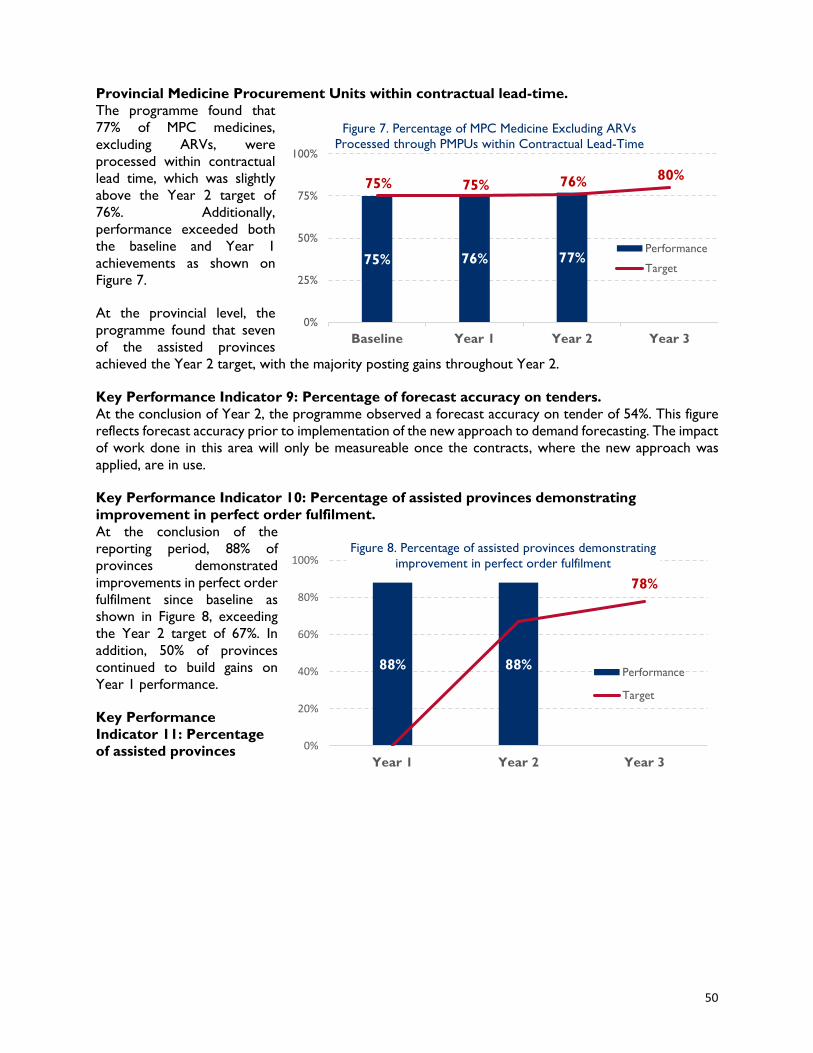
50
Provincial Medicine Procurement Units within contractual lead-time.
The programme found that
77% of MPC medicines,
excluding ARVs, were
processed within contractual
lead time, which was slightly
above the Year 2 target of
76%. Additionally,
performance exceeded both
the baseline and Year 1
achievements as shown on
Figure 7.
At the provincial level, the
programme found that seven
of the assisted provinces
achieved the Year 2 target, with the majority posting gains throughout Year 2.
Key Performance Indicator 9: Percentage of forecast accuracy on tenders.
At the conclusion of Year 2, the programme observed a forecast accuracy on tender of 54%. This figure
reflects forecast accuracy prior to implementation of the new approach to demand forecasting. The impact
of work done in this area will only be measureable once the contracts, where the new approach was
applied, are in use.
Key Performance Indicator 10: Percentage of assisted provinces demonstrating
improvement in perfect order fulfilment.
At the conclusion of the
reporting period, 88% of
provinces demonstrated
improvements in perfect order
fulfilment since baseline as
shown in Figure 8, exceeding
the Year 2 target of 67%. In
addition, 50% of provinces
continued to build gains on
Year 1 performance.
Key Performance
Indicator 11: Percentage
of assisted provinces
75% 76% 77%
0%
75% 75% 76% 80%
0%
25%
50%
75%
100%
Baseline Year 1 Year 2 Year 3
Figure 7. Percentage of MPC Medicine Excluding ARVs
Processed through PMPUs within Contractual Lead-Time
Performance
Target
88% 88%
78%
0%
20%
40%
60%
80%
100%
Year 1 Year 2 Year 3
Figure 8. Percentage of assisted provinces demonstrating
improvement in perfect order fulfilment
Performance
Target
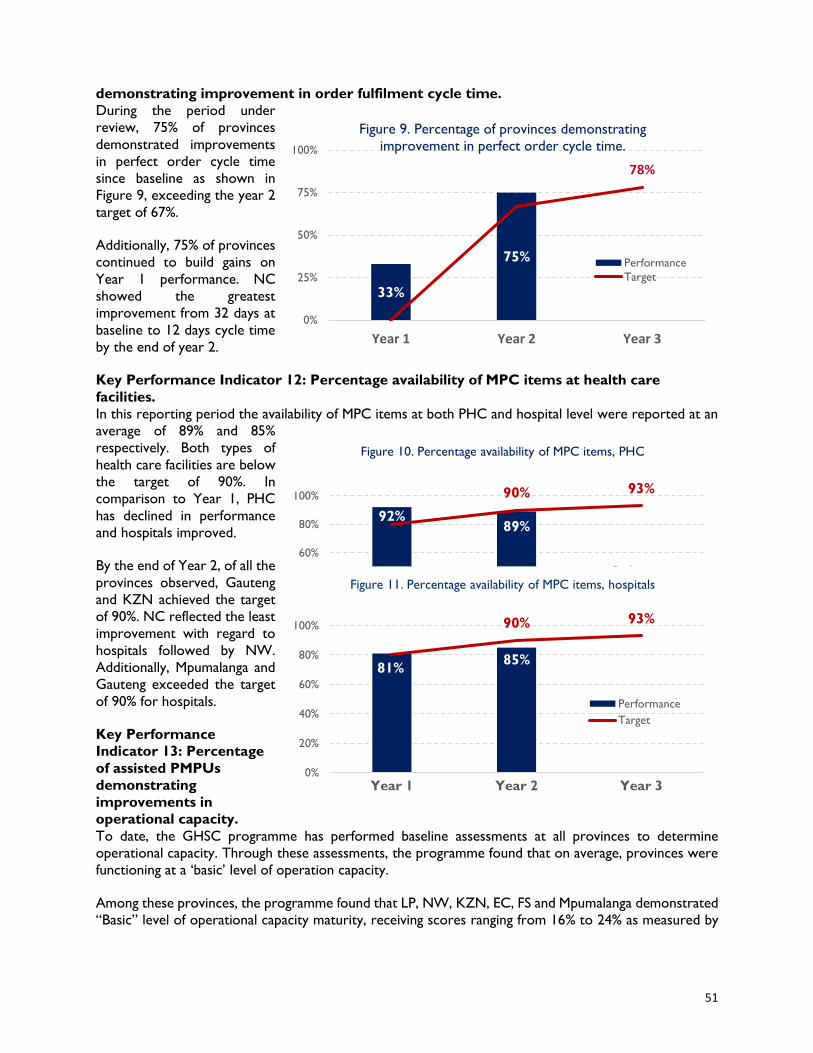
51
demonstrating improvement in order fulfilment cycle time.
During the period under
review, 75% of provinces
demonstrated improvements
in perfect order cycle time
since baseline as shown in
Figure 9, exceeding the year 2
target of 67%.
Additionally, 75% of provinces
continued to build gains on
Year 1 performance. NC
showed the greatest
improvement from 32 days at
baseline to 12 days cycle time
by the end of year 2.
Key Performance Indicator 12: Percentage availability of MPC items at health care
facilities.
In this reporting period the availability of MPC items at both PHC and hospital level were reported at an
average of 89% and 85%
respectively. Both types of
health care facilities are below
the target of 90%. In
comparison to Year 1, PHC
has declined in performance
and hospitals improved.
By the end of Year 2, of all the
provinces observed, Gauteng
and KZN achieved the target
of 90%. NC reflected the least
improvement with regard to
hospitals followed by NW.
Additionally, Mpumalanga and
Gauteng exceeded the target
of 90% for hospitals.
Key Performance
Indicator 13: Percentage
of assisted PMPUs
demonstrating
improvements in
operational capacity.
To date, the GHSC programme has performed baseline assessments at all provinces to determine
operational capacity. Through these assessments, the programme found that on average, provinces were
functioning at a ‘basic’ level of operation capacity.
Among these provinces, the programme found that LP, NW, KZN, EC, FS and Mpumalanga demonstrated
“Basic” level of operational capacity maturity, receiving scores ranging from 16% to 24% as measured by
33%
75%
78%
0%
25%
50%
75%
100%
Year 1 Year 2 Year 3
Figure 9. Percentage of provinces demonstrating
improvement in perfect order cycle time.
Performance
Target
92%89%
90% 93%
0%
20%
40%
60%
80%
100%
Year 1 Year 2 Year 3
Figure 10. Percentage availability of MPC items, PHC
Performance
Target
81%85%
90% 93%
0%
20%
40%
60%
80%
100%
Year 1 Year 2 Year 3
Figure 11. Percentage availability of MPC items, hospitals
Performance
Target
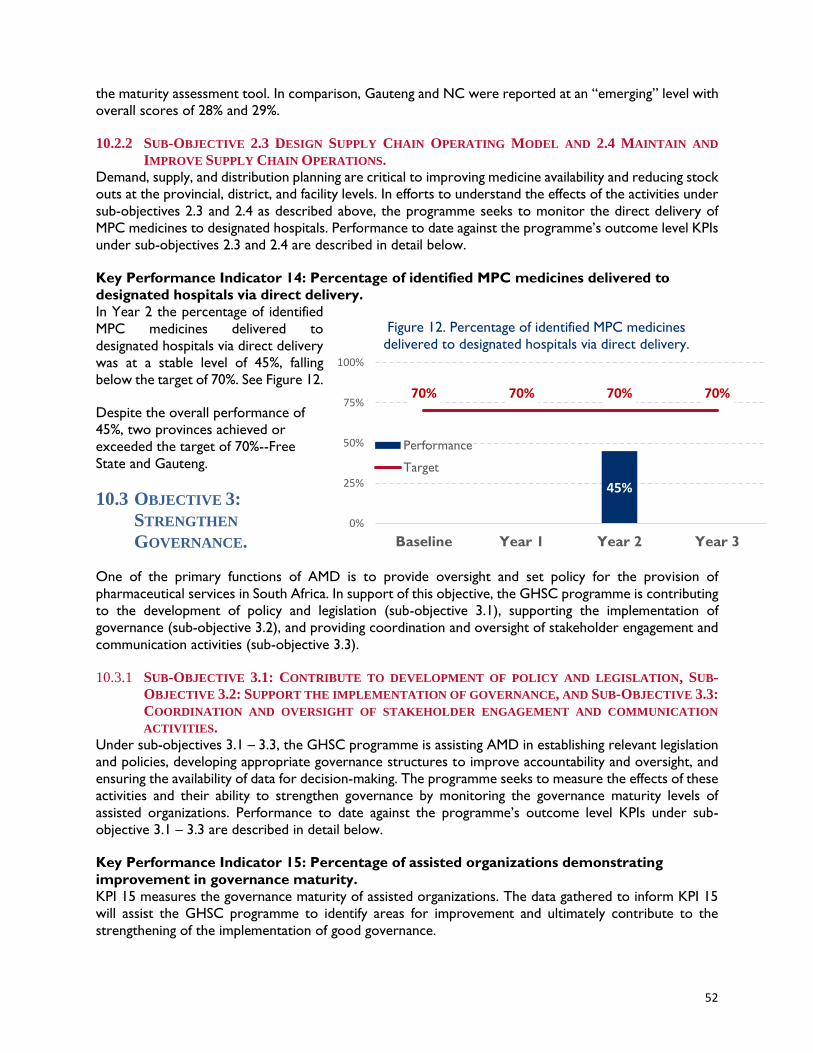
52
the maturity assessment tool. In comparison, Gauteng and NC were reported at an “emerging” level with
overall scores of 28% and 29%.
10.2.2 SUB-OBJECTIVE 2.3 DESIGN SUPPLY CHAIN OPERATING MODEL AND 2.4 MAINTAIN AND
IMPROVE SUPPLY CHAIN OPERATIONS.
Demand, supply, and distribution planning are critical to improving medicine availability and reducing stock
outs at the provincial, district, and facility levels. In efforts to understand the effects of the activities under
sub-objectives 2.3 and 2.4 as described above, the programme seeks to monitor the direct delivery of
MPC medicines to designated hospitals. Performance to date against the programme’s outcome level KPIs
under sub-objectives 2.3 and 2.4 are described in detail below.
Key Performance Indicator 14: Percentage of identified MPC medicines delivered to
designated hospitals via direct delivery.
In Year 2 the percentage of identified
MPC medicines delivered to
designated hospitals via direct delivery
was at a stable level of 45%, falling
below the target of 70%. See Figure 12.
Despite the overall performance of
45%, two provinces achieved or
exceeded the target of 70%--Free
State and Gauteng.
10.3 OBJECTIVE 3:
STRENGTHEN
GOVERNANCE.
One of the primary functions of AMD is to provide oversight and set policy for the provision of
pharmaceutical services in South Africa. In support of this objective, the GHSC programme is contributing
to the development of policy and legislation (sub-objective 3.1), supporting the implementation of
governance (sub-objective 3.2), and providing coordination and oversight of stakeholder engagement and
communication activities (sub-objective 3.3).
10.3.1 SUB-OBJECTIVE 3.1: CONTRIBUTE TO DEVELOPMENT OF POLICY AND LEGISLATION, SUB-
OBJECTIVE 3.2: SUPPORT THE IMPLEMENTATION OF GOVERNANCE, AND SUB-OBJECTIVE 3.3:
COORDINATION AND OVERSIGHT OF STAKEHOLDER ENGAGEMENT AND COMMUNICATION
ACTIVITIES.
Under sub-objectives 3.1 – 3.3, the GHSC programme is assisting AMD in establishing relevant legislation
and policies, developing appropriate governance structures to improve accountability and oversight, and
ensuring the availability of data for decision-making. The programme seeks to measure the effects of these
activities and their ability to strengthen governance by monitoring the governance maturity levels of
assisted organizations. Performance to date against the programme’s outcome level KPIs under sub-
objective 3.1 – 3.3 are described in detail below.
Key Performance Indicator 15: Percentage of assisted organizations demonstrating
improvement in governance maturity.
KPI 15 measures the governance maturity of assisted organizations. The data gathered to inform KPI 15
will assist the GHSC programme to identify areas for improvement and ultimately contribute to the
strengthening of the implementation of good governance.
45%
70% 70% 70% 70%
0%
25%
50%
75%
100%
Baseline Year 1 Year 2 Year 3
Figure 12. Percentage of identified MPC medicines
delivered to designated hospitals via direct delivery.
Performance
Target
53
During Year 2, the GHSC programme supported and monitored the governance maturity level of the
national Contract CMU, following initial strengthening engagements, which commenced in Year 1. The
GHSC programme expanded these efforts by assisting two additional organizations, the Information
Systems and Projects Unit (ISP) within AMD and the North West (NW) province. The programme started
working with CMU in Year 2 and progressed to ISP in May 2018. Work in NW started in July 2018. The
following highlights the progress at the organizational level that has been demonstrated to date:
CMU
Based on the ongoing monitoring of the CMU governance maturity levels, the programme observed an
improvement from a ‘basic’ maturity level at baseline of 25% to an ‘optimal’ maturity level of 83.3% at the
end of Year 2. The CMU demonstrated significant improvement across all elements of governance from
baseline, with optimal maturity levels in policies and operational plan. In Q2, improvement was observed
in four key areas including: operational plan, decision-making authority processes, governance structures,
and standard operating procedures. In Q3, policies, operational plan, oversight, and accountability,
progressed to emerging and advanced levels. In Q4 the majority of elements improved to advanced levels
with the operational plan and policies at the optimal level.
ISP
With regards to ISP, the average baseline score measured in May 2018 was reported at a basic level, with
all elements of the governance maturity model being at a ‘basic’ level of 25%. Over the course of Q3 and
Q4 of Year 2, ISP demonstrated an average increase of 12.5%, from a ‘basic’ level of maturity at baseline
to an ‘emerging’ maturity level. By the end of Q4, oversight and accountability had improved to an
‘emerging’ maturity level, raising the overall ISP governance score to an ‘emerging’ maturity level.
NW
The NW baseline assessment was administered in July 2018 and found that in the area of governance NW
was performing at a ‘basic’ maturity level with an overall score of 25%. Notably most elements on the
assessment were on the lower end of the ‘basic’ scale except for oversight and accountability. The GHSC
programme conducted a follow up assessment in September 2018. While the NW remains at an overall
‘basic’ level of governance maturity, the showed slight improvement during the period under review.
Specifically, the programme found improvements in standard operating procedures, with scores in the
later stage of ‘basic’ maturity level.
10.4 OBJECTIVE 4: IMPROVE WORKFORCE
To address the management of human resources within the medicine supply chain, including challenges
relating to the lack of staff with the required capabilities, high vacancy rates, uneven distribution of human
resources, and the need to improve staff management and retention, the GHSC programme seeks to
improve workforce. Specifically, the GHSC programme seeks to support the standardization of structures,
roles and competencies (sub-objective 4.1), institutionalize change management (sub-objective 4.2) and
the up-skilling and mentoring of staff (sub-objective 4.3).
10.4.1 SUB-OBJECTIVE 4.1 – SUPPORT THE DEVELOPMENT OF STANDARDIZED STRUCTURES, ROLES
AND COMPETENCIES & PERFORMANCE MANAGEMENT, SUB-OBJECTIVE 4.2 – ASSIST TO
INSTITUTIONALIZE CHANGE MANAGEMENT, AND SUB-OBJECTIVE 4.3 – CONTRIBUTE TO UP-
SKILLING AND MENTORING OF AMD STAFF.
Under sub-objectives 4.1 – 4.3, the programme strengthened the interventions and activities to improve
workforce alignment, performance management, operational management components and organizational
structure for specific units. The programme seeks to measure the effects of these activities and their ability
to strengthen workforce by monitoring the workforce maturity levels of assisted organizations.
54
Performance to date against the programme’s outcome level KPIs under sub-objective 4.1 – 4.3 are
described in detail below.
Key Performance Indicator 16: Percentage of assisted organizations demonstrating
improvement in workforce maturity.
KPI 16 measures levels of workforce management maturity among assisted organizations. The GHSC
programme classifies an organization’s level of workforce as mature when the staff of an organization have
a clear delegation of authority and decision-making roles; they agree with the designation of roles and
responsibilities; and maintain clear, documented, and continually assessed workforce development
elements with clearly defined roles and job descriptions standardized across departments and aligned with
the job profiles of an optimised organizational structure.
As of Year 2, the GHSC programme has supported and monitored the workforce maturity of the CMU.
The GHSC programme also assisted two additional organizations the ISP unit and the NW
Depot/Pharmaceutical Services. The following highlights the progress demonstrated to date:
CMU
The programme observed CMU’s improvement in workforce maturity from a ‘basic’ maturity level of 25%
at baseline to an ‘advanced’ maturity level of 75% by the end of Year 2. Improvements were observed in
almost all of the elements with organizational structure, roles and job profiles operating at optimal levels.
On the quarterly analysis, the majority of the elements elevated performance in Q2 and then plateaued in
Q3 and Q4. Notably Succession planning and Retention were the least improved by the end of Year 2.
ISP
The GHSC programme conducted a baseline assessment for ISP workforce maturity in May 2018. As a
result, the programme found that the ISP was operating at a ‘basic’ maturity level of 25% across all five
components of workforce maturity. Ongoing monitoring shows initial improvement in the areas of roles,
job profiles and performance management. The ISP has demonstrated improvement in these areas from
‘basic’ to emerging’. This resulted in the maturity level of ISP increasing to an ‘emerging’ maturity level of
35%, showing a 10% growth from baseline. The quarterly analysis showed that ISP was at the emerging
level at the end of Q4.
NW
For NW, the baseline was conducted in July 2018 and the average baseline score reported at a ‘basic’
level. Ongoing assessments reflected that the maturity level remains at a basic level with a slight
improvement due to the design of the Organizational Structure. Further work is underway.
10.5 OBJECTIVE 5: STRENGTHEN INFORMATION SYSTEMS AND INFORMATION
MANAGEMENT.
Technology and information systems are critical enablers of health supply chain performance and form a
cornerstone of the successful delivery of the SIMA. The GHSC programme seeks to support the
strengthening of information systems and information management by designing an IT system landscape
(sub-objective 5.1) and providing support to strengthen analytics and oversight (sub-objectives 5.2 and
5.3).
10.5.1 SUB-OBJECTIVE 5.1 DESIGN AN IT SYSTEM LANDSCAPE AND 5.2 PROVIDE SUPPORT TO
STRENGTHEN ANALYTICS AND OVERSIGHT.
Under sub-objectives 5.1 and 5.2, the GHSC programme drafted an information technology architecture
roadmap and is deploying information systems. The programme seeks to measure the effects of GHSC
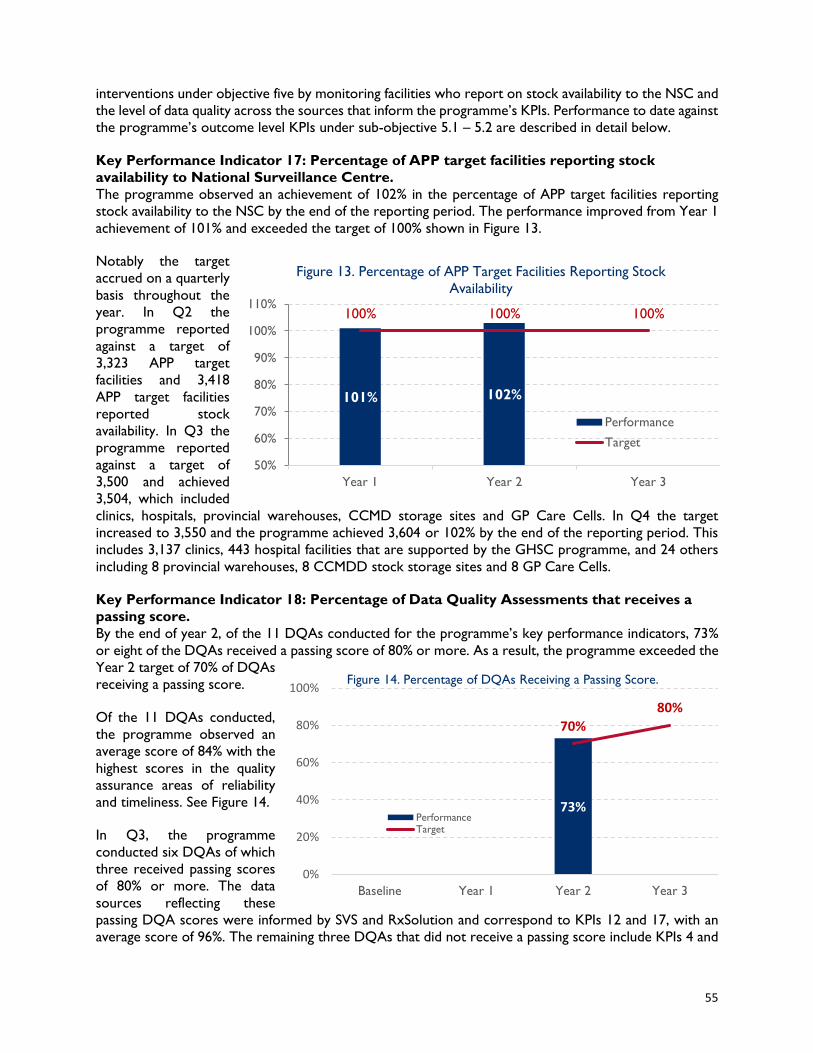
55
interventions under objective five by monitoring facilities who report on stock availability to the NSC and
the level of data quality across the sources that inform the programme’s KPIs. Performance to date against
the programme’s outcome level KPIs under sub-objective 5.1 – 5.2 are described in detail below.
Key Performance Indicator 17: Percentage of APP target facilities reporting stock
availability to National Surveillance Centre.
The programme observed an achievement of 102% in the percentage of APP target facilities reporting
stock availability to the NSC by the end of the reporting period. The performance improved from Year 1
achievement of 101% and exceeded the target of 100% shown in Figure 13.
Notably the target
accrued on a quarterly
basis throughout the
year. In Q2 the
programme reported
against a target of
3,323 APP target
facilities and 3,418
APP target facilities
reported stock
availability. In Q3 the
programme reported
against a target of
3,500 and achieved
3,504, which included
clinics, hospitals, provincial warehouses, CCMD storage sites and GP Care Cells. In Q4 the target
increased to 3,550 and the programme achieved 3,604 or 102% by the end of the reporting period. This
includes 3,137 clinics, 443 hospital facilities that are supported by the GHSC programme, and 24 others
including 8 provincial warehouses, 8 CCMDD stock storage sites and 8 GP Care Cells.
Key Performance Indicator 18: Percentage of Data Quality Assessments that receives a
passing score.
By the end of year 2, of the 11 DQAs conducted for the programme’s key performance indicators, 73%
or eight of the DQAs received a passing score of 80% or more. As a result, the programme exceeded the
Year 2 target of 70% of DQAs
receiving a passing score.
Of the 11 DQAs conducted,
the programme observed an
average score of 84% with the
highest scores in the quality
assurance areas of reliability
and timeliness. See Figure 14.
In Q3, the programme
conducted six DQAs of which
three received passing scores
of 80% or more. The data
sources reflecting these
passing DQA scores were informed by SVS and RxSolution and correspond to KPIs 12 and 17, with an
average score of 96%. The remaining three DQAs that did not receive a passing score include KPIs 4 and
101% 102%
100% 100% 100%
50%
60%
70%
80%
90%
100%
110%
Year 1 Year 2 Year 3
Figure 13. Percentage of APP Target Facilities Reporting Stock
Availability
Performance
Target
73%
0%
70%
80%
0%
20%
40%
60%
80%
100%
Baseline Year 1 Year 2 Year 3
Figure 14. Percentage of DQAs Receiving a Passing Score.
PerformanceTarget
56
5, informed by Pharmaceutical Services Dashboard, with an average score of 70% and KPI 12, informed
by RxSolution, with a score of 71%. In Q4 the DQA scores for the remaining 5 KPIs were completed and
consolidated making a total of eleven. The five additional KPIs were informed by the RSA Pharma database
and received a passing score of 85%.
10.5.2 SUB-OBJECTIVE 5.3 SUPPORT THE IMPLEMENTATION OF DATA GOVERNANCE.
Under sub-objective 5.3, the GHSC programme drafted an information technology architecture roadmap
and is deploying information systems. The programme seeks to monitor the utilization of information
systems and information management systems among assisted facilities to measure the effects of the
programme’s intervention. Performance to date against the programme’s outcome level KPIs under sub-
objective 5.3 are described in detail below.
Key Performance Indicator 19: Percentage of assisted facilities where information systems
and information management systems are utilized.
KPI 19 contributes to the strengthening of data governance, which is key to facilitating the consistent
application of data and fulfilling the prerequisite, improved interoperability of systems within the AMD IT
ecosystem. KPI 19 also accounts for the impact of the GHSC programme’s contributions supporting the
deployment of gCommerce.
By the end of the period under review, the GHSC programme was supporting the deployment of
gCommerce in two of the ten targeted provincial warehouses (Northern Cape and Limpopo).
10.6 OBJECTIVE 6: IMPROVE FINANCIAL MANAGEMENT.
This objective aims to improve financial management processes including budgeting and forecasting,
financial monitoring, and reporting against the budget for both the Chief Directorate: Sector Wide
Procurement (SWP) within NDOH and in assisted provinces. Under objective 6, the GHSC programme
seeks to improve forecasting and budget information (sub-objective 6.1), strengthen accounting processes
(sub-objective 6.2) and improve financial monitoring and reporting (sub-objective 6.3).
10.6.1 SUB-OBJECTIVE 6.1 – IMPROVE FORECASTING & BUDGET INFORMATION, SUB-OBJECTIVE 6.2
- ASSIST TO STRENGTHEN ACCOUNTING PROCESSES, & SUB-OBJECTIVE 6.3- ASSIST TO
IMPROVE FINANCIAL MONITORING & REPORTING
Under sub-objectives 6.1 – 6.3, the programme seeks to measure the effects of the activities designed to
improve budgeting and forecasting, as well as monitoring and reporting by measuring the on-time
submission of PMPU payment packs. Performance to date against the programme’s outcome level KPIs
under sub-objective 6.1 – 6.3 are described in detail below.
Key Performance Indicator 20: Percentage of PMPU payment packs submitted on time.
KPI 20 measures the percentage of PMPU payment packs submitted on time as compared to the total
number of payment packs submitted within a defined period of review.
There is no performance data to report at this time, as GHSC does not have access to data sources that
inform KPI 20. Originally, the programme sought to use the current systems MEDSAS/PDSX to inform
this indicator. These systems, however, do not provide the necessary data to track the submission of
payment packs. gCommerce will provide future data to inform this indicator.

57
11. ANNEX
Indicator Reporting
Year
Baseline
Value
Year 2 Proposed
Target
Year 2 Achievement
to Date
% of Proposed Year 2
Achievement to Date
Objective 1 – Improve selection and use of medicine.
Desired Outcome – Selection and Use of Medicines Improved.
Sub-Objective 1.1- Assist with implementation of Health Technology Assessments (HTAs)
Key Performance Indicator 1:
Number of medicine reviews
conducted by the Expert Review
Committees.2
FY18 N/A 25 N/A N/A
Key Performance Indicator 3:
Percentage of recommendations on
medicines selection utilizing HTA
outputs.3
FY18 0% 10% N/A N/A
Sub-Objective 1.2 – Improve Rational Medicine Use (RMU)
Key Performance Indicator 4:
Number of formularies generated
using Essential Medicines Electronic
Access.
FY18 0 9 5 56%
2 To address the lack of available data, GHSC staff developed a Medicine Review Survey, a tool to capture and document the number of medicine reviews completed
but was neither approved nor implemented by AMD. In Q2 Activities under Sub-Objective 1.1: Assist with the implementation of HTAs were suspended due a
decision by AMD to deprioritize HTA support. Towards the end Year 2, however, the Director of AMD requested GHSC to again support HTA activities. A
concept note is being developed to will inform HTA strategy and required support. A meeting will take place in November 2018 to discuss AMD’s desired HTA
activities, with GHSC personnel forming a key portion of the core team providing support.
3 Since the suspension of HTA activities in Q2, GHSC continued to engage with AMD on future plans for HTA. However, following discussion with the Director of
AMD towards the end of Year 2, it is planned that these activities will commence in Year 3. A concept note is currently under development that will inform an HTA
strategy and the exact support that will be required from GHSC. It is envisioned that HTA support will be commenced including HTA capacity building that will
contribute towards improvement in this indicator. A meeting is due to be held in November 2018 to discuss HTA activities going forward by AMD and GHSC will
form part of the core team assisting AMD with HTA.
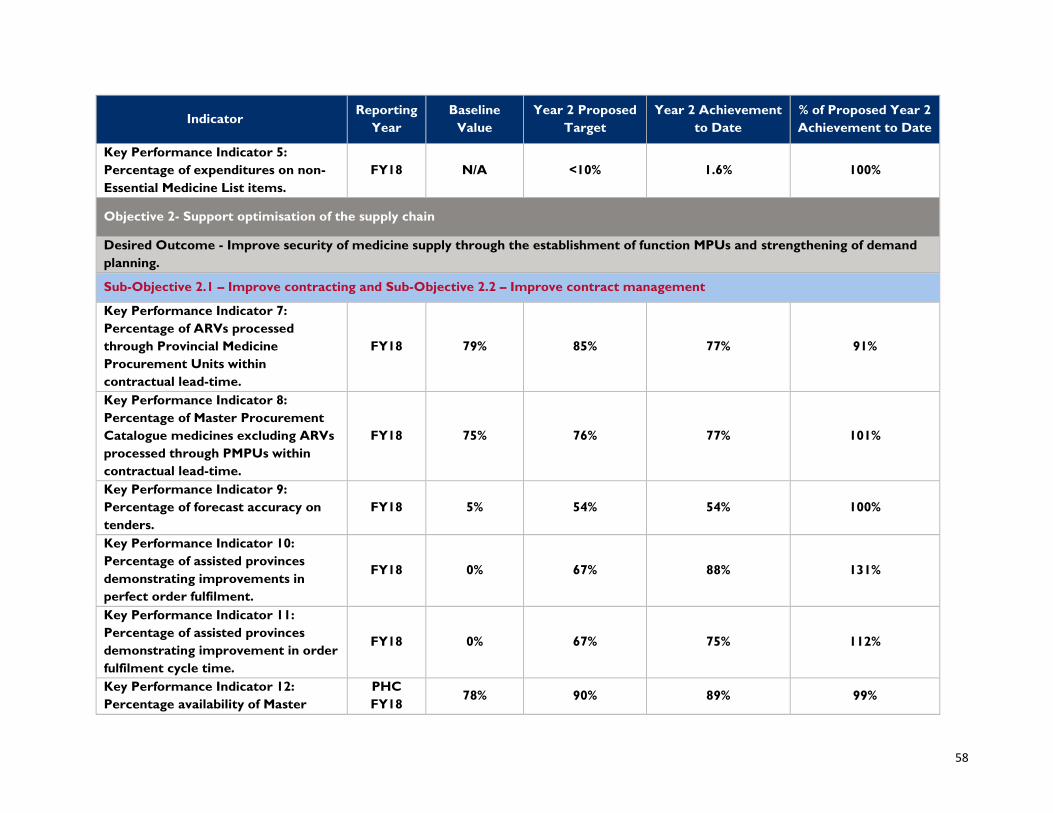
58
Indicator Reporting
Year
Baseline
Value
Year 2 Proposed
Target
Year 2 Achievement
to Date
% of Proposed Year 2
Achievement to Date
Key Performance Indicator 5:
Percentage of expenditures on non-
Essential Medicine List items.
FY18 N/A <10% 1.6% 100%
Objective 2- Support optimisation of the supply chain
Desired Outcome - Improve security of medicine supply through the establishment of function MPUs and strengthening of demand
planning.
Sub-Objective 2.1 – Improve contracting and Sub-Objective 2.2 – Improve contract management
Key Performance Indicator 7:
Percentage of ARVs processed
through Provincial Medicine
Procurement Units within
contractual lead-time.
FY18 79% 85% 77% 91%
Key Performance Indicator 8:
Percentage of Master Procurement
Catalogue medicines excluding ARVs
processed through PMPUs within
contractual lead-time.
FY18 75% 76% 77% 101%
Key Performance Indicator 9:
Percentage of forecast accuracy on
tenders.
FY18 5% 54% 54% 100%
Key Performance Indicator 10:
Percentage of assisted provinces
demonstrating improvements in
perfect order fulfilment.
FY18 0% 67% 88% 131%
Key Performance Indicator 11:
Percentage of assisted provinces
demonstrating improvement in order
fulfilment cycle time.
FY18 0% 67% 75% 112%
Key Performance Indicator 12:
Percentage availability of Master
PHC
FY18 78% 90% 89% 99%
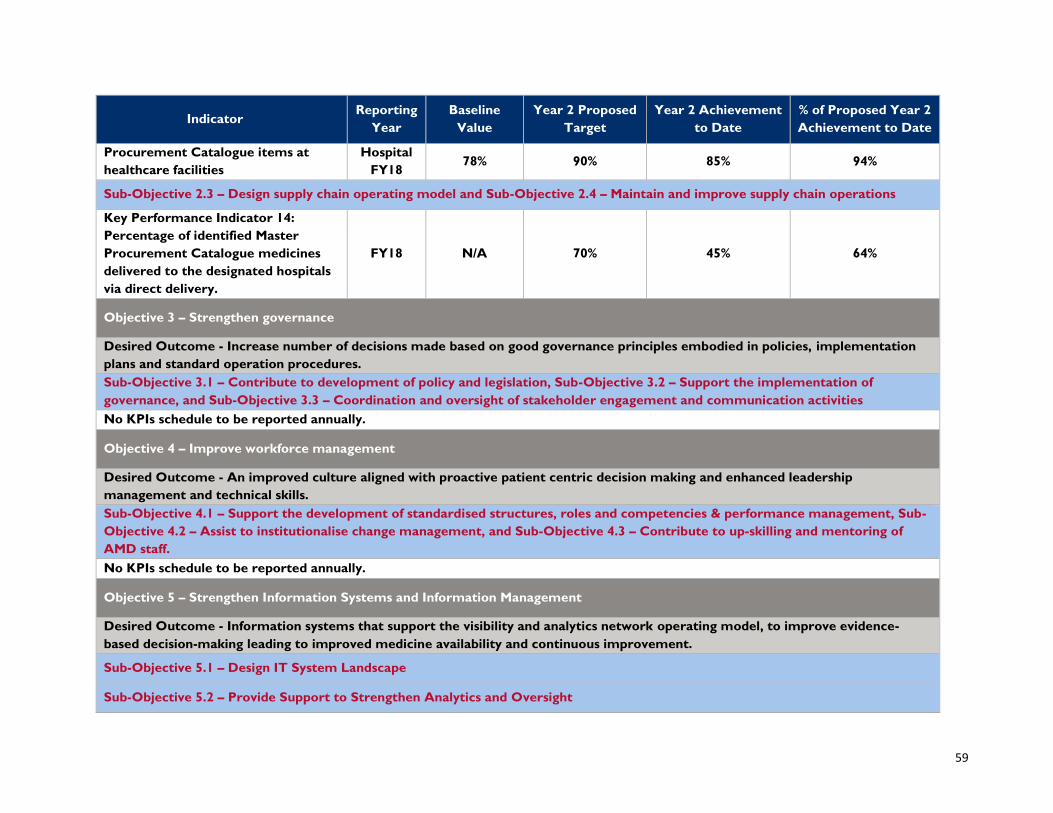
59
Indicator Reporting
Year
Baseline
Value
Year 2 Proposed
Target
Year 2 Achievement
to Date
% of Proposed Year 2
Achievement to Date
Procurement Catalogue items at
healthcare facilities
Hospital
FY18 78% 90% 85% 94%
Sub-Objective 2.3 – Design supply chain operating model and Sub-Objective 2.4 – Maintain and improve supply chain operations
Key Performance Indicator 14:
Percentage of identified Master
Procurement Catalogue medicines
delivered to the designated hospitals
via direct delivery.
FY18 N/A 70% 45% 64%
Objective 3 – Strengthen governance
Desired Outcome - Increase number of decisions made based on good governance principles embodied in policies, implementation
plans and standard operation procedures.
Sub-Objective 3.1 – Contribute to development of policy and legislation, Sub-Objective 3.2 – Support the implementation of
governance, and Sub-Objective 3.3 – Coordination and oversight of stakeholder engagement and communication activities
No KPIs schedule to be reported annually.
Objective 4 – Improve workforce management
Desired Outcome - An improved culture aligned with proactive patient centric decision making and enhanced leadership
management and technical skills.
Sub-Objective 4.1 – Support the development of standardised structures, roles and competencies & performance management, Sub-
Objective 4.2 – Assist to institutionalise change management, and Sub-Objective 4.3 – Contribute to up-skilling and mentoring of
AMD staff.
No KPIs schedule to be reported annually.
Objective 5 – Strengthen Information Systems and Information Management
Desired Outcome - Information systems that support the visibility and analytics network operating model, to improve evidence-
based decision-making leading to improved medicine availability and continuous improvement.
Sub-Objective 5.1 – Design IT System Landscape
Sub-Objective 5.2 – Provide Support to Strengthen Analytics and Oversight

60
Indicator Reporting
Year
Baseline
Value
Year 2 Proposed
Target
Year 2 Achievement
to Date
% of Proposed Year 2
Achievement to Date
Key Performance Indicator 17:
Percentage of APP target facilities
reporting stock availability to
National Surveillance Centre.
FY18 100% 100% 102% 102%
Key Performance Indicator 18:
Percentage of Data Quality
Assessments that receives a passing
score.
FY17 N/A 70% 73% 104%
Sub-Objective 5.3 – Support the implementation of data governance and Sub-Objective 5.4- Assist with development and
implementation of IT systems
Key Performance Indicator 19:
Percentage of assisted facilities where
information systems and information
management systems are utilised.
FY18 0% 50% 20% 40%
Objective 6 – Improve Financial Management
Desired Outcome - Prudent financial management processes that underpin and support improved medicine availability.
Sub-Objective 6.1 – Improve forecasting and budget information, Sub-Objective 6.2 - Assist to strengthen accounting processes, and
Sub-Objective 6.3- Assist to improve financial monitoring and reporting
Key Performance Indicator 20:
Percentage of PMPU payment packs
submitted on time.4
FY18 N/A N/A N/A N/A
4 There is no performance data to report at this time as GHSC does not have access to data sources to inform KPI 20. Originally, the programme sought to use
the current systems MEDSAS/PDSX to inform this indicator, however, these systems do not provide the necessary data to track the submission of payment packs.
The programme has designed gCommerce to track the submission time of payment packs and this will be used to inform this indicator as gCommerce goes live
within each province.