u.s. small business administration counseling … approval no.:3245-0324 expiration date: 09/30/2006...
TRANSCRIPT

OMB Approval No.:3245-0324 Expiration Date: 09/30/2006
U.S. Small Business Administration Counseling Information Form
Client Number:Location Code: Initials of Data Inputter:
SBA Form 641 (5/04) Previous Editions are Obsolete
1. Name of the Office Providing the Service _______________________________1a. Type of Client: Face to Face Online Telephone 2. City/State of Office Location_________________________
PART I: Client Request for Counseling 3. Client Name (Name of the person completing the form/representative of the business) (Last, First, MI)
4. Email
5. Telephone 6. Fax Primary Secondary 7. Street Address/PO Box (give business address if currently in business) 8. City 9. State 10. Zip +4
11. I request business counseling service from the Small Business Administration (SBA) or an SBA Resource Partner. I agree to cooperate should I be selected to participate in surveys designed to evaluate SBA services. I permit SBA or its agent the use of my name and address for SBA surveys and information mailings regarding SBA products and services (Yes No ). I understand that any information disclosed will be held in strict confidence. (SBA will not provide your personal information to commercial entities.) I authorize SBA to furnish relevant information to the assigned management counselor(s). I further understand that the counselor(s) agrees not to: 1) recommend goods or services from sources in which he/she has an interest, and 2) accept fees or commissions developing from this counseling relationship. In consideration of the counselor(s) furnishing management or technical assistance, I waive all claims against SBA personnel, and that of its Resource Partners and host organizations, arising from this assistance. Please note: The estimated burden for completing this form is 3 minutes. You are not required to respond to any collection information unless it displays a currently valid OMB approval number. Comments on the burden should be sent to: U.S. Small Business Administration, 409 3rd Street, SW, Washington, DC 20416, and to: Desk Officer SBA, Office of Management and Budget, New Executive Office Building, Room 10202, Washington, D.C., 20503. OMB Approval (3245-0324). PLEASE DO NOT SEND FORMS TO OMB. 12. Preferred date & time for appointment Date: Time:
13. Client Signature Date:
PART II: Client Intake (to be completed by all Clients) 14. Race (mark one or more) Asian Black or African American Native American or Alaska Native Native Hawaiian or other Pacific Islander White
15. Ethnicity Hispanic Origin Not of Hispanic Origin
16.Gender Male Female
17. Do you consider yourself a person with a disability?
Yes No
18. Veteran Status Non-Veteran Veteran Service-Disabled Veteran
18a. Military Status Member of Reserve or National Guard On Active Duty
19. What inspired you to contact us? (mark all that apply) SBA Other Client Chamber of Commerce Other (specify) _______________________________ Bank Magazine Educational Institution Business Owner Internet Local Economic Development Official . Television/Radio Newspaper Word of Mouth 20. Is the client currently in business? Yes No (if no, skip to 30)
21. Name of Company
22. Type of Business (choose primary category) Professional, Scientific & Technical Services Mining Manufacturing Real Estate & Rental & Leasing Management of Companies & Enterprises Utilities Finance & Insurance Health Care & Social Assistance Agriculture, Forestry, Fishing & Hunting Information Wholesale Trade Accommodation & Food Services Administrative & Support Construction Public Administration Arts, Entertainment & Recreation Waste Management & Remediation Services Retail Trade Educational Services Transportation & Warehousing Other Services (except Public Administration)
23. Business Ownership – What percentage of your business is male or female ownership? __________% Male__________% Female
24. Month & Year Business Started?
25. Do you conduct business online? Yes No
26. Is this a home based business? Yes No
27. Total No. of Employees (full & part time)
28. For your most recent full business year, what were your: Gross Revenues/Sales $______________ +Profits/-Losses $___________________
29. What is the legal entity of your business? Sole Proprietorship Corporation LLC S-Corporation Partnership Other (specify) ________________________________
30. What is the nature of counseling you are seeking? (Choose primary category) Start-up Assistance (How do I start a
small business?) Business Plan Financing/Capital (such as applying
for a loan, building equity capital) Managing a Business
Human Resources/ Managing Employees
Customer Relations Business Accounting/
Budget Cash Flow Management Tax Planning
Marketing/Sales (promotion, market research, pricing, etc.)
Government Contracting (including certifications)
Franchising Buy/Sell Business
Technology/Computers eCommerce (using the
Internet to do business) Legal Issues (such as,
Should I incorporate?) International Trade
Describe specific assistance requested in the space provided. ___________________________________________________________________________________ ______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Page 1

OMB Approval No.: 3245-0324 Expiration Date: 09/30/2006
U.S. Small Business Administration Counseling Information Form
Client Number: Location Code: Initials of Data Inputer:
Part III: Counselor Record
SBA Form 641 (5/04) Previous Editions are Obsolete
2
31. Client Name (please use the same name from original 641 Part 1) (Last, First, MI)
32. Email
33. Telephone 34. Fax Primary Secondary 35. Street Address /P.O. Box 36. City 37. State 38. Zip +4
39. Is the client currently in business? Yes No (if no, skip to 44)
40. Month & Year Business Started?
41. Total No. of Employees (full & PT)
42. As of the most recent counseling date and for the most recent business year, what are the client’s annual: Gross Revenues/Sales $_____________________ +Profits/-Losses$__________________________
43. SBA or Resource Partner Service Contributed to the Following: ________________ No. of Government Contracts or Subcontracts Received $_______________ Total Amount of SBA Loans $ _______________ Dollar Value of Government Contracts/Subcontracts Received $_______________ Total Amount of Non-SBA Loans ________________ No. of Certifications (i.e. SDB, HUBZone, 8(a), local certifications, etc.) Received $_______________ Amount of Equity Capital Received ________________ Did counseling received result in starting a business? If yes, please check.
44. What was the nature of the counseling you provided the client? (choose primary category) Start-up Assistance (How do I start a
small business?) Business Plan Financing/Capital (such as, applying
for a loan, building equity capital) Managing a Business
Human Resources/Managing Employees
Customer Relations Business Accounting/Budget Cash Flow Management Tax Planning
Marketing/Sales (promotion, market research, pricing, etc.)
Government Contracting (including certifications)
Franchising Buy/Sell Business
Technology/Computers eCommerce (using the Internet
to do business) Legal Issues (such as, Should I
incorporate?) International Trade
Please specify other counseling provided. ___ __________________________________________________________________________________________________ ______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ 45. Type of Counseling Face to Face Online Telephone
46. Language(s) Used
English Spanish Other (Specify)_____________________________
47. History New Case Follow-up Case Close-out One Time 48. Date Counseled
49. Counselor(s) Name
50a. Contact Hours 50b. Prep Hours 50c. Travel Hours
51. (Answer this question during the initial counseling session only) – Did more than one person attend the counseling session? Yes__ No__. If yes, how many people attended the session other than the person completing the form? _______________ 52. Counselor’s Notes:
Page 2

SBA Form 641 Training Guide
FORM 641-To be used for face-to-face, online and telephone counseling. Form Block #
Field Description Explanation
EDMIS2 – Required Field
HEADER. Client Request for Counseling – To be completed by center 1. Name of the
Office Providing the Service
Not required on form. The Name of the Office Providing the Service will be automatically attached to the clients “Request for Counseling” form when batching from each centers independent client management information system to EDMIS. Location information will be assigned by center data maintained in SBA’s PIMS database. Each lead center should insure that SBA has the most current center location information to assure that PIMS codes and information are kept current to reflect accurate information.
YES However, information will be attached during upload to EDMIS by each centers individual client management information system.
1a. Type of client
Designate a Type of Client:
• face-to-face (in-person), • online, or • telephone.
The Type of Client is based on the counseling method used (or expected to be used) to conduct the client’s initial counseling session. (A client only has one initial counseling session regardless of the length of business relationship with the center.) The method used to conduct the initial and all subsequent counseling sessions (i.e. “Type of Counseling”) will be recorded in Part 3, field 45. These fields must equal with the clients initial counseling session, however, may be different in follow-up sessions. These fields are NOT the same and are used differently by SBA. It is expected that the Type of Client assigned will be used by SBA as a basis in reporting the activity for the various types of methods
YES
EDMIS Forms Training Guide Revised 9/1/2005
Page 3

used by resource partners to conduct counseling. That is, if a client is categorized as an “on-line client” because their first counseling session was conducted on-line the client will always be consider by SBA as an on-line client regardless of the method used to counsel the client in follow-up sessions. Once the Type of Client is assigned to a client, and becomes a certified record by EDMIS, i.e. the Request for Counseling, Part 1 is uploaded to EDMIS and certified by the center as being accurate this field can not be edited by the center even with future uploads of Part 1. Centers should take care in making these assignments.
2. City/State of Office Location
Not required on form. The City/State of Office Location will be automatically attached to the clients “Request for Counseling” form when batching from each centers independent client management information system to EDMIS. Location information will be assigned by center data maintained in SBA’s PIMS database. Each lead center should insure that SBA has the most current center location information to assure that PIMS codes and information are kept current to reflect accurate information.
YES However, information will be attached during upload to EDMIS by each centers individual client management information system.
PART I. Client Request for Counseling – To be completed by the client 3. Client Name Enter the full legal name of the client.
SBDCs must maintain a record of each client’s full name on a “Request for Counseling” form and recorded in their client management information systems. No middle initial is necessary. EDMIS NOTE: Client confidentially regulation prohibit SBDC client names from being uploaded to EDMIS2.
NO
(see EDMIS NOTE)
4. Email Enter the email address as provided by the client. EDMIS NOTE: Client confidentially regulation prohibit SBDC client email
NO
(see EDMIS NOTE)
EDMIS Forms Training Guide Revised 9/1/2005
Page 4

addresses from being uploaded to EDMIS2. 5. Telephone Enter the primary and secondary phone
numbers as provided by the client. EDMIS NOTE: Client confidentially regulation prohibit SBDC client telephone numbers from being uploaded to EDMIS2.
NO
(see EDMIS NOTE)
6. Fax Number Enter the fax number as provided by the client. EDMIS NOTE: Client confidentially regulation prohibit SBDC client fax numbers from being uploaded to EDMIS2.
NO
(see EDMIS NOTE)
7. Street Address/PO Box
Enter the home street address if client is a nascent entrepreneur; business street address if an in-business client. EDMIS NOTE: Client confidentially regulation prohibit SBDC client addresses from being uploaded to EDMIS2.
NO
(see EDMIS NOTE)
8. City Enter the home city if client is a nascent entrepreneur; business city if an in-business client. EDMIS NOTE: Client confidentially regulation prohibit SBDC client addresses from being uploaded to EDMIS2.
NO
(see EDMIS NOTE)
9. State Enter the home state if client is a nascent entrepreneur; business state if an in-business client. EDMIS NOTE: EDMIS does not require that centers upload a client’s state. If SBDCs provide this information EDMIS will perform a validation test with the client’s zip code to assure both fields are accurate. It is recommended that SBDCs not provide a client’s state to avoid record rejection.
NO
(see EDMIS NOTE)
10. Zip plus 4 Enter the zip code of home address if client is a nascent entrepreneur; business zip code if an in-business client. If the client is in the military and has an APO, use zip code of client home address. If the client has an out of country address, use zip code of the SBDC providing the service.
YES 5-digit only.
Plus 4 prohibited.
(see EDMIS NOTE)
EDMIS Forms Training Guide Revised 9/1/2005
Page 5

EDMIS NOTE: Client confidentially regulation prohibit the plus-four of a zip code (i.e. last four digits of a nine digit zip code) are prohibited from being uploaded to EDMIS2.
11. Impact Survey
Designate the client’s authorization or denial for SBA to use the client’s name and address for survey and other mailings. If client does not make designation indicate “No”.
YES
12. Preferred Date & Time for Appointment
For SBDC informational purposes only, as provided by the client.
13. Client Signature and Date
SBDCs must have a record that the client has agreed to the disclaimer by having them sign and date the “Request for Counseling” form. SBDCs must record that there is a signature on file and the signature date.
YES
PART II. Client Intake – To be completed by the client 14. Race Designate the client’s race(s) as provided by
the client. More than one choice may be selected. If not provided, leave blank on form and record as “unknown/not stated” in information systems. Default selection “unknown/not stated”. EDMIS NOTE: Though “unknown/not stated” is not an option on the Request for Counseling form, “unknown/not stated” is an EDMIS2 reportable category and should be used when the client does not answer the question.
YES
(see EDMIS NOTE)
15. Ethnicity Designate the client’s Hispanic ethnicity as provided by the client. If not provided, leave blank on form and record as “unknown/not stated” in information systems. Default selection “unknown/not stated”. EDMIS NOTE: Though “unknown/not stated” is not an option on the Request for Counseling form, “unknown/not stated” is an EDMIS2 reportable category and should be used when the client does not answer the question.
YES
(see EDMIS NOTE)
16. Gender Designate the client’s gender as provided by the client. If not provided, leave blank on
YES
EDMIS Forms Training Guide Revised 9/1/2005
Page 6

form and record as “unknown/not stated” in information systems. Default selection “unknown/not stated”. EDMIS NOTE: Though “unknown/not stated” is not an option on the Request for Counseling form, “unknown/not stated” is an EDMIS2 reportable category and should be used when the client does not answer the question.
(see EDMIS NOTE)
17. Disability Designate the client’s disability status as provided by the client. If not provided, leave blank on form and record as “unknown/not stated” in information systems. Default selection “unknown/not stated”. EDMIS NOTE: Though “unknown/not stated” is not an option on the Request for Counseling form, “unknown/not stated” is an EDMIS2 reportable category and should be used when the client does not answer the question.
YES
(see EDMIS NOTE)
18. Veteran Status
Designate the client’s Veteran status as provided by the client. If not provided, leave blank on form and record as “unknown/not stated” in information systems. Default selection “unknown/not stated”. EDMIS NOTE: Though “unknown/not stated” is not an option on the Request for Counseling form, “unknown/not stated” is an EDMIS2 reportable category and should be used when the client does not answer the question.
YES
(see EDMIS NOTE)
18a. Military Status
Designate the client’s military status as provided by the client. If not provided, leave blank on form and record as “unknown/not stated” in information systems. Default selection “unknown/not stated”. EDMIS NOTE: Though “unknown/not stated” is not an option on the Request for Counseling form, “unknown/not stated” is an EDMIS2 reportable category and should be
YES
(see EDMIS NOTE)
EDMIS Forms Training Guide Revised 9/1/2005
Page 7

used when the client does not answer the question.
19. What inspired you to contact us?
Designate the source(s) of the client’s inspiration/referral to seek assistance of the SBDC as provided by the client. More than one choice may be selected. If not provided, leave blank on form and record as “unknown/not stated” in information systems. Default selection “unknown/not stated”. EDMIS NOTE: Though “unknown/not stated” is not an option on the Request for Counseling form, “unknown/not stated” is an EDMIS2 reportable category and should be used when the client does not answer the question.
YES
(see EDMIS NOTE)
20. Is the client currently in business?
Designate if the client is in business as of the client’s initial contact (i.e. Request for Counseling signature date) with the SBDC.
YES
Fields 21 – 29 should be completed by clients currently in business. Nascent entrepreneurs should skip to field 30.
21. Name of Company
Enter the name of the business as provided by the client. EDMIS NOTE: Client confidentially regulation prohibit SBDC client business names from being uploaded to EDMIS2.
NO
(see EDMIS NOTE)
22. Type of Business
Designate the client’s primary type of business as provided by the client. Only one selection should be chosen.
YES
23. Business Ownership
Enter the total percentage of the client’s business owned by men and women. Ownership percentage for each category must be between 0% and 100%. Use whole numbers (e.g. 51%, not .51). Total ownership must equal 100%.
YES
24. Month & Year Business Started
Enter the month and year client established business. If not provided, use January of current year. If business state date is before 1900 use January 1900.
YES
25. Conduct business online?
Designate if client conducts business online. If not provided, use “No”.
YES
26. Is this a home-based business?
Designated if client’s business primarily located at client’s home address as provided by client. If not provided, use “No”.
YES
27. Total Enter the total number of full and part time YES
EDMIS Forms Training Guide Revised 9/1/2005
Page 8
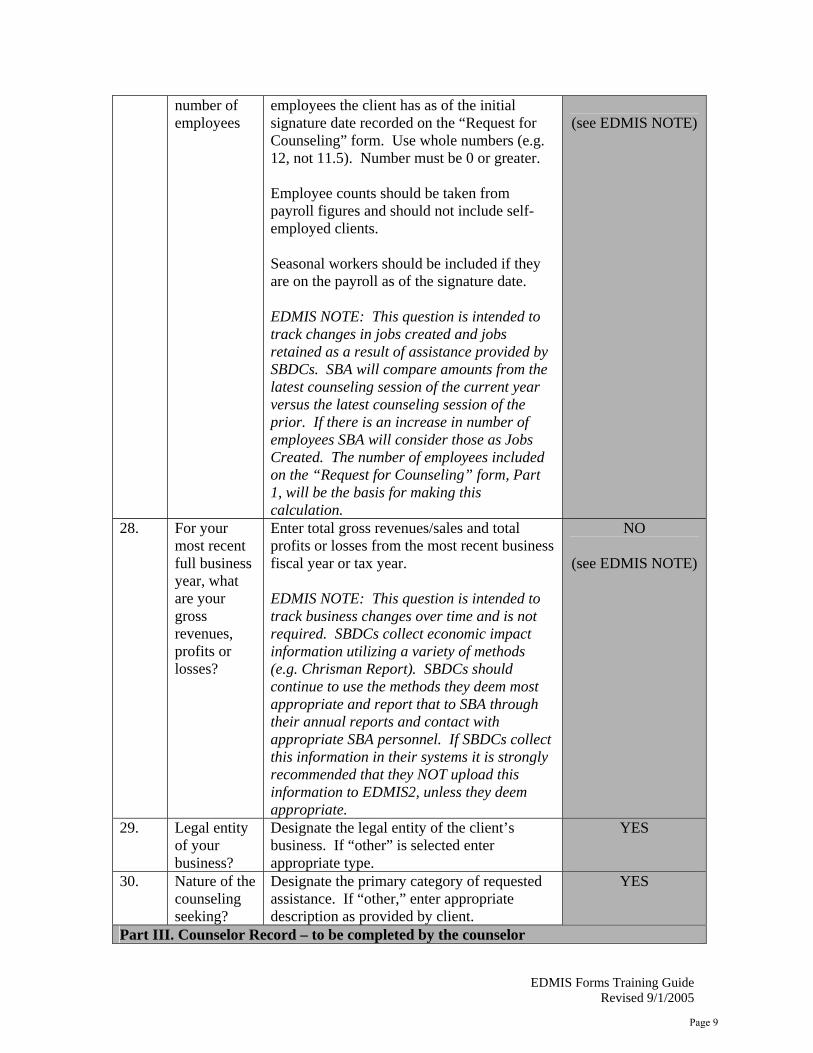
number of employees
employees the client has as of the initial signature date recorded on the “Request for Counseling” form. Use whole numbers (e.g. 12, not 11.5). Number must be 0 or greater. Employee counts should be taken from payroll figures and should not include self-employed clients. Seasonal workers should be included if they are on the payroll as of the signature date. EDMIS NOTE: This question is intended to track changes in jobs created and jobs retained as a result of assistance provided by SBDCs. SBA will compare amounts from the latest counseling session of the current year versus the latest counseling session of the prior. If there is an increase in number of employees SBA will consider those as Jobs Created. The number of employees included on the “Request for Counseling” form, Part 1, will be the basis for making this calculation.
(see EDMIS NOTE)
28. For your most recent full business year, what are your gross revenues, profits or losses?
Enter total gross revenues/sales and total profits or losses from the most recent business fiscal year or tax year. EDMIS NOTE: This question is intended to track business changes over time and is not required. SBDCs collect economic impact information utilizing a variety of methods (e.g. Chrisman Report). SBDCs should continue to use the methods they deem most appropriate and report that to SBA through their annual reports and contact with appropriate SBA personnel. If SBDCs collect this information in their systems it is strongly recommended that they NOT upload this information to EDMIS2, unless they deem appropriate.
NO
(see EDMIS NOTE)
29. Legal entity of your business?
Designate the legal entity of the client’s business. If “other” is selected enter appropriate type.
YES
30. Nature of the counseling seeking?
Designate the primary category of requested assistance. If “other,” enter appropriate description as provided by client.
YES
Part III. Counselor Record – to be completed by the counselor
EDMIS Forms Training Guide Revised 9/1/2005
Page 9

31. Client Name Enter the full legal name of the client. SBDCs must maintain a record of each client’s full name on a “Request for Counseling” form and recorded in their client management information systems. No middle initial is necessary. EDMIS NOTE: Client confidentially regulation prohibit SBDC client names from being uploaded to EDMIS2.
NO
(see EDMIS NOTE)
32. Email Enter the email address as provided by the client. EDMIS NOTE: Client confidentially regulation prohibit SBDC client email addresses from being uploaded to EDMIS2.
NO
(see EDMIS NOTE)
33. Telephone Enter the primary and secondary phone numbers as provided by the client. EDMIS NOTE: Client confidentially regulation prohibit SBDC client telephone numbers from being uploaded to EDMIS2.
NO
(see EDMIS NOTE)
34. Fax Enter the fax number as provided by the client. EDMIS NOTE: Client confidentially regulation prohibit SBDC client fax numbers from being uploaded to EDMIS2.
NO
(see EDMIS NOTE)
35. Street Address/PO Box
Enter the home street address if client is a nascent entrepreneur; business street address if an in-business client. EDMIS NOTE: Client confidentially regulation prohibit SBDC client addresses from being uploaded to EDMIS2.
NO
(see EDMIS NOTE)
36. City Enter the home city if client is a nascent entrepreneur; business city if an in-business client. EDMIS NOTE: Client confidentially regulation prohibit SBDC client addresses from being uploaded to EDMIS2.
NO
(see EDMIS NOTE)
37. State Enter the home state if client is a nascent entrepreneur; business state if an in-business client. EDMIS NOTE: EDMIS does not require that
NO
(see EDMIS NOTE)
EDMIS Forms Training Guide Revised 9/1/2005
Page 10

centers upload a client’s state. If SBDCs provide this information EDMIS will perform a validation test with the client’s zip code to assure both fields are accurate. It is recommended that SBDCs not provide a client’s state to avoid record rejection.
38. Zip plus 4 Enter the zip code of home address if client is a nascent entrepreneur; business zip code if an in-business client. If the client is in the military and has an APO, use zip code of client home address. If the client has an out of country address, use zip code of the SBDC providing the service. EDMIS NOTE: Client confidentially regulation prohibit the plus-four of a zip code (i.e. last four digits of a nine digit zip code) are prohibited from being uploaded to EDMIS2.
YES 5-digit only.
Plus 4 prohibited.
(see EDMIS NOTE)
39. Is the client currently in business?
Not required for pre-FY 2006 clients. Designate if the client is in business as of the counseling session date. EDMIS NOTE: This question is how SBA will determine the number of start-ups assisted over time. 641, Part I, field 20 will be automatically updated in EDMIS if the client switches to an in-business client.
YES
(see EDMIS NOTE)
Fields 40 – 42 should be completed by clients in business at the time of counseling. Nascent entrepreneurs should skip to field 44.
40. Month and year business stated
Enter the month and year client established business. If not provided, use January of current year. If business state date is before 1900 use January 1900. If client is a nascent entrepreneur leave field blank.
YES
41. Total number of employees
Enter the total number of full and part time employees the client has as of the initial signature date recorded on the Request for Counseling form. Use whole numbers (e.g. 12, not 11.5). Number must be 0 or greater. If client is a nascent entrepreneur leave field blank. Employee counts should be taken from payroll figures and should not include self-
YES
(see EDMIS NOTE)
EDMIS Forms Training Guide Revised 9/1/2005
Page 11

employed clients. Seasonal workers should be included if they are on the payroll as of the counseling session date. EDMIS NOTE: This question is intended to track changes in jobs created and jobs retained as a result assistance provided by SBDCs. SBA will compare amounts from the latest counseling session of the current year versus the latest counseling session of the prior. If there is an increase in number of employees SBA will consider those as Jobs Created. The number of employees included on the “Request for Counseling” form, Part 1, will be the basis for making this calculation.
42. As of the most recent counseling date, what are the client’s annual gross revenues, profits or losses?
Enter total gross revenues/sales and total profits or losses from the most recent business fiscal year or tax year. EDMIS NOTE: This question is intended to track business changes over time and is not required. SBDCs collect economic impact information utilizing a variety of methods (e.g. Chrisman Report). SBDCs should continue to use the methods they deem most appropriate and report that to SBA through their annual reports and contact with appropriate SBA personnel.
NO
(see EDMIS NOTE)
43. SBA or resource partner contributed to the following? • SBA
Loans • Non-
SBA Loans
• Equity Capital Received
• Government Contract
SBDCs are only required to ask the client if the counseling resulted in the client starting the business. Designate if the counseling resulted in the start-up of a business. EDMIS NOTE: SBDCs collect the other impact information utilizing a variety of methods (e.g. Chrisman Report). SBDCs should continue to use the methods they deem most appropriate and report that to SBA through their annual reports and contact with appropriate SBA personnel. If SBDCs collect this information in their systems it is strongly recommended that they NOT upload this information to EDMIS2, unless they deem appropriate.
YES (see note)
EDMIS Forms Training Guide Revised 9/1/2005
Page 12

s/Subcontracts
• Certifications
• Result in Starting a Small
44. What is the
nature of the counseling provided to the client?
Designate the primary category of counseling assistance provided. If “other” is selected enter appropriate description.
YES
45. Type of counseling
Designate a type of client:
• face-to-face (in-person), • online, or • telephone
based on the forum used to conduct the counseling session. NOTE: If it is the clients initial counseling session (i.e. New Case, field 47) with the SBDC, the “Type of Counseling” should match the “Type of Client” in field 1a. All subsequent counseling sessions (i.e. follow-up), regardless of the period of the counseling relationship, may be of a different type of counseling session.
YES
46. Language(s) Used
Not required for pre-FY 2006 clients. Designate the language used to provide the counseling. If “other” is selected enter the language used.
YES
47. History Designate the counseling session history type:
• new case, • follow-up, • close-out, or • one time.
NOTE: If the counseling session is a New Case (i.e. first counseling session with the SBDC regardless of the period of the counseling relationship) EDMIS will require that field 1a and field 45 are the same.
YES
EDMIS Forms Training Guide Revised 9/1/2005
Page 13

NOTE: If the counseling session is a Close-out (i.e. anticipated final counseling session with the SBDC) EDMIS will not count it as counseling. If a counseling session and a Close-out occur at the same time, two separate 641, part III’s are needed. All other subsequent sessions can vary.
48. Date Counseled
Enter the date of the counseling session took place. Use the MM/DD/YYYY format.
YES
49. Counselor(s) name
Enter the name of the counselor or counselors who provided the counseling. NOTE: EDMIS limits the number of characters for this field to 80.
YES
50a. Contact Hours
Enter amount of time spent directly interacting with the client specific to the client’s needs.
50b. Prep Hours Enter the amount of time spent preparing and researching information the client. Prep time will be counted toward counseling but will be tracked separately. Enter zero (0) if no preparation/research was involved.
50c. Travel Hours Enter the amount of time spent traveling to a location (i.e. separate from assigned post-of-duty) to meet with the client. Travel time will not count toward counseling time but will be tracked separately. If meeting with more than one client, travel time should only be counted once. Total travel time should be allocated to either a single client or allocated proportionately to each client counseled during the travel. Enter zero (0) if there was no travel involved.
YES EDMIS NOTE: To allow for reporting of time invested in a client, preparatory time will be tracked separately from counseling time but attributed toward counseling time in EDMIS data reporting. That is, EDMIS requires that every counseling session uploaded must have contact time greater than zero (0). An initial counseling session (i.e. New Case, field 47) must be at least 30 minutes in length in Contact Hours to be reported.
51. Did more than one person attend the counseling session?
Designate if more than one person attended the initial (i.e. New Case, field 47) counseling session. To avoid multiple counting, this information will only be counted on the initial session.
YES
52. Counselor’s To be counted as counseling the counseling
EDMIS Forms Training Guide Revised 9/1/2005
Page 14

Notes session must be substantive in nature and require the assistance of the SBDC in the formation, management, financing, and/or operation of a small business enterprise. The following is guidance on what should be documented for every SBDC counseling session:
• An analysis of the client’s problem/situation
• A summary of what the counselor did during the session.
• Recommendation(s) provided by the counselor
• Follow-up required by the counselor and/or the client.
• Any other documentation deemed appropriate by the counselor.
If it is the client’s initial counseling session (i.e. New Case, field 47) with the SBDC, a summary of the clients business or business interest should be included.
EDMIS Forms Training Guide Revised 9/1/2005
Page 15

OMB Approval No.:3245-0324 Expiration Date: 09/30/2006
U.S. Small Business Administration
Management Training Report
Location Code: Initials of Data Inputter:
1. Name of Office Providing the Service: _________________________ City/ State _______________
SBA Form 888 (5/04) Previous Editions are Obsolete
2. Organization SBDC WBC SBA District Office SCORE, Chapter No._______ Other (specify) ________________
3. Date Training Started (mm/dd/yy)
4. No. of Sessions
5. Total Hours of Training
6. Title of Training
7. Location of Training City ___________________________ State__________ Zip _____________
+4 ___________
8. Total Number Trained __________
9. Total Number of Minorities Trained ____________
_______ Currently in Business _______ Not Yet in Business _______ People with Disabilities _______ Women
________ Total Veterans ________ Service-Disabled Veterans _________Members of Reserve or National Guard (please complete to the extent information is available)
Race ________ Asians _________ Blacks or Africans Americans _________ Native Americans or Alaskan Natives _________ Native Hawaiians or other Pacific Islanders _________ White Ethnicity ________Hispanic Origin ________Not of Hispanic Origin
10. Training Topic (check primary topic) Business Start-up/Preplanning Business Plan Business Financing/Capital Sources Managing a Business Human Resources/ Managing Employees Customer Relations
Business Accounting/Budget Cash Flow Management Tax Planning Marketing/Sales Government Contracting Franchising Buy/Sell Business
Technology/Computers eCommerce Legal Issues International Trade Other (Specify) __________________________________
11. Resource Partners Participating (check all that apply)
SCORE SBDC Women's Business Center VBOC Educational Institution Chamber Of Commerce
Trade Or Professional Assoc. For-Profit Organization Online Training Resource SBA District Office Native American Center SBA (specify office) _______________________________
Other Govt. Agency (specify) _______________________________ Other (specify) _______________________________
12. Program Format (check only one) Seminar (short-term training on business-related subjects that is conducted as a single, stand alone program) Course (more formal structured training on business-related subjects that may be conducted over a number of sessions) Online Course (a formal structured training delivered via the Internet) Teleconference (any training delivered via electronic communications, except Online Course)
15. What is the dollar amount of fees that your organization received? 13. Attendee Fee Full Fee _____________ x $__________ = $__________ (no. of attendees) (fee per attendee) Discounted Fee ______________ x $__________ = $__________ No Fee ______________ x $____0_____ = $_____0____ No Show Income_____________x $___________= $__________ Other Income =$__________ 14. Total Gross Fee Income $__________
16. Language(s) Used
English Spanish Other (specify) ________________________
17. Name of Sponsor
18. Name of Co-sponsors (if applicable) _____________________________________________________ ___________________________________________________________________ _____________________________________________________ ___________________________________________________________________
Page 16

SBA Form 888 Training Guide
FORM 888 – To be used for online and in-person training. For a training event to be counted it must have one or more attendees and last a total of one hour or more in length for instructor training and 30 minutes or more for online training. Form Block #
Field Description Explanation
EDMIS2 – Required Field
1. Name of Office Providing the Service
Not required on form. The Name of the Office Providing the Service will be automatically attached to the “Management Training Report” form when batching from each centers independent training management information system to EDMIS. Location information will be assigned by center data maintained in SBA’s PIMS database. Each lead center should insure that SBA has the most current center location information to assure that PIMS codes and information are kept current to reflect accurate information.
YES However, information will be attached during upload to EDMIS by each centers individual training management information system.
2. Organization Not required on form. The Organization will be automatically attached to the “Management Training Report” form when batching from each centers independent client management information system to EDMIS. Location information will be assigned by center data maintained in SBA’s PIMS database. Each lead center should insure that SBA has the most current center location information to assure that PIMS codes and information are kept current to reflect accurate information.
YES However, information will be attached during upload to EDMIS by each centers individual client management information system.
3. Date Training Started
Enter the date of the training event took place. Use the MM/DD/YYYY format.
YES
4. Number of Sessions
Enter the number of times or sessions that the training convened.
YES
5. Total Hours of Training
Enter total length of training event.
YES
EDMIS Forms Training Guide Revised 9/1/2005
Page 17

Total Training Hours equals the total number of curriculum hours of the training event. For example, if a class is scheduled to meet 12 times for 2 hours the “Total Hours of Training” reported would be 24. Total Training Hours is NOT the multiple of training hours multiplied by total attendees. Live training must be a minimum of 1 hour in duration and a minimum of 30 minutes in duration for online training.
6. Title of Training
Training events assigned title. YES
7. Location of the Training
Enter the City, State, and Zip (plus 4) of where the training was held. EDMIS NOTE: EDMIS does not require that centers upload a training events city or state. If SBDCs provide the training events state EDMIS will perform a validation test with the events zip code to assure both fields are accurate. It is recommended that SBDCs not provide a client’s state to avoid record rejection.
YES
Only zip code is required.
Plus 4 not required.
8. Total Number Trained
Enter the actual number of individuals who attended the training and their various characteristics. Each individual attendee may be counted under multiple characteristic categories. Service-Disabled Veterans and Members of Reserve or National Guard should also be counted under Total Veterans. For training events with multiple sessions individual attendees are considered unique and should only be counted once. Do NOT multiply the number of attendees by the number of training sessions attended to get calculate Total Number Trained.
YES
9. Total Number of Minorities Trained
Designate the number of training attendees’ race(s) and Hispanic origin as provided by the training attendee. More than one minority category may be selected for an individual training attendee.
YES
EDMIS Forms Training Guide Revised 9/1/2005
Page 18
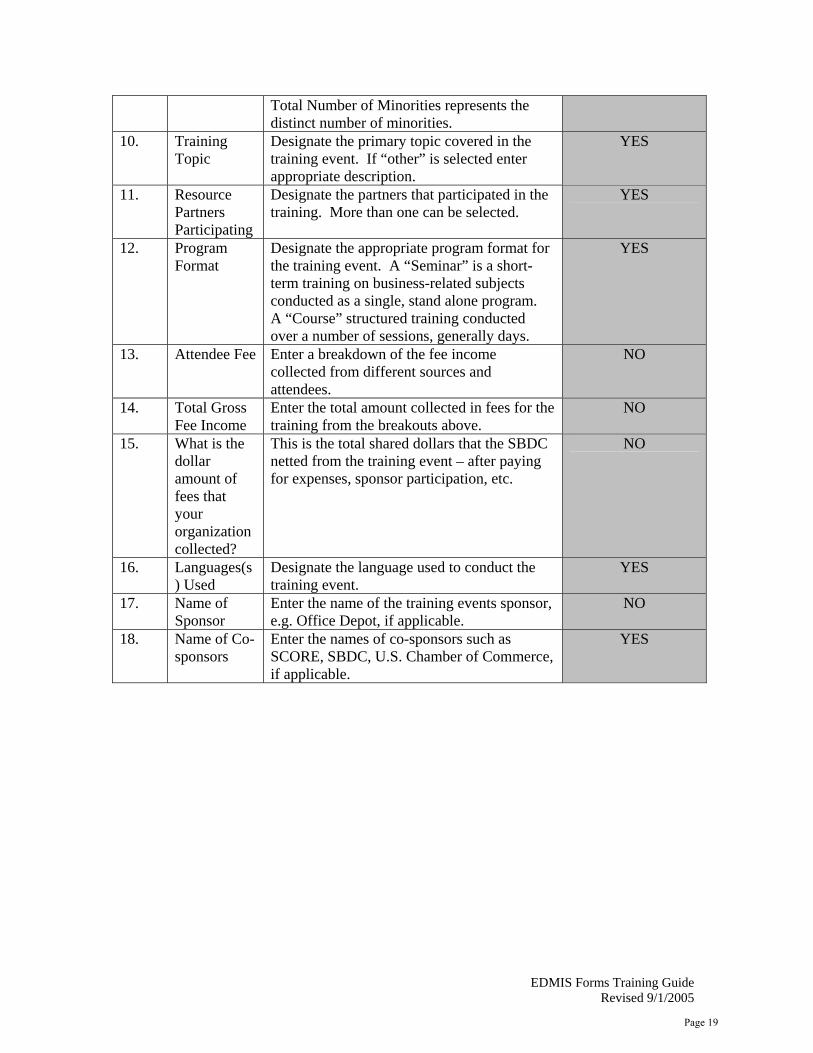
Total Number of Minorities represents the distinct number of minorities.
10. Training Topic
Designate the primary topic covered in the training event. If “other” is selected enter appropriate description.
YES
11. Resource Partners Participating
Designate the partners that participated in the training. More than one can be selected.
YES
12. Program Format
Designate the appropriate program format for the training event. A “Seminar” is a short-term training on business-related subjects conducted as a single, stand alone program. A “Course” structured training conducted over a number of sessions, generally days.
YES
13. Attendee Fee Enter a breakdown of the fee income collected from different sources and attendees.
NO
14. Total Gross Fee Income
Enter the total amount collected in fees for the training from the breakouts above.
NO
15. What is the dollar amount of fees that your organization collected?
This is the total shared dollars that the SBDC netted from the training event – after paying for expenses, sponsor participation, etc.
NO
16. Languages(s) Used
Designate the language used to conduct the training event.
YES
17. Name of Sponsor
Enter the name of the training events sponsor, e.g. Office Depot, if applicable.
NO
18. Name of Co-sponsors
Enter the names of co-sponsors such as SCORE, SBDC, U.S. Chamber of Commerce, if applicable.
YES
EDMIS Forms Training Guide Revised 9/1/2005
Page 19
SBA Form 2226 (5/04) Previous Editions are Obsolete
U.S. Small Business Administration Information Transfers
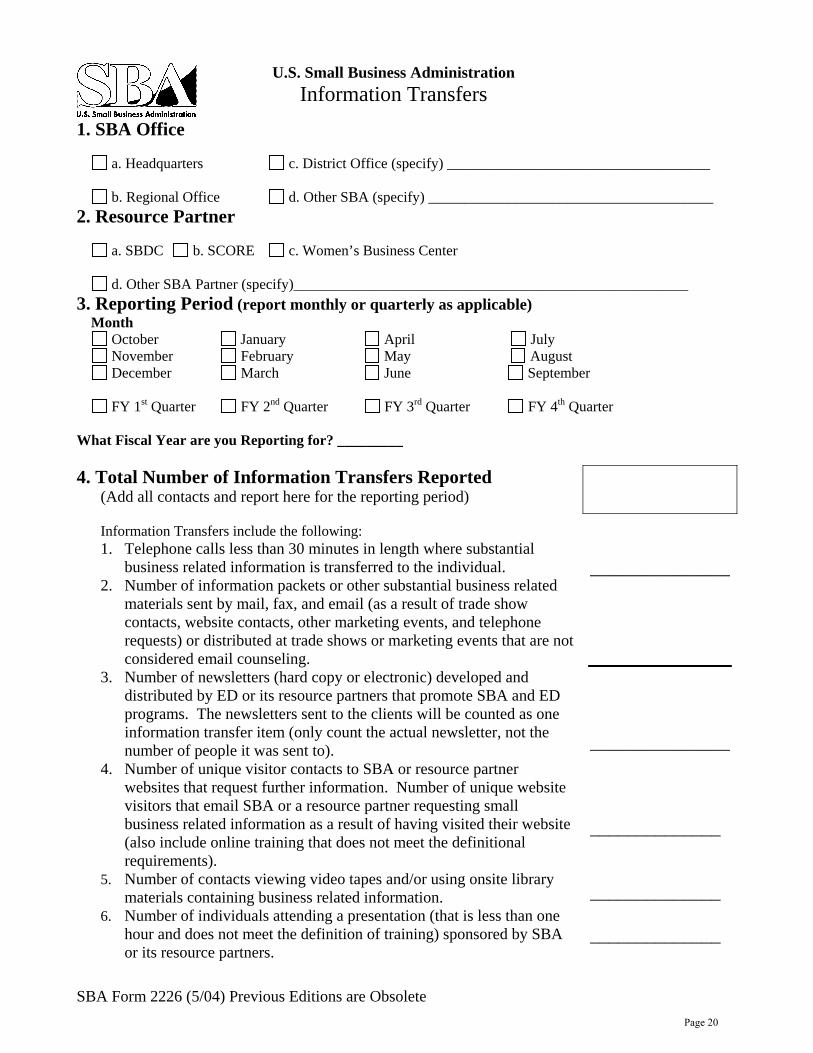
1. SBA Office a. Headquarters c. District Office (specify) ____________________________________ b. Regional Office d. Other SBA (specify) _______________________________________ 2. Resource Partner a. SBDC b. SCORE c. Women’s Business Center d. Other SBA Partner (specify)______________________________________________________ 3. Reporting Period (report monthly or quarterly as applicable)
Month October January April
July November February May August
December March June September FY 1st Quarter FY 2nd Quarter FY 3rd Quarter FY 4th Quarter What Fiscal Year are you Reporting for? _________
4. Total Number of Information Transfers Reported (Add all contacts and report here for the reporting period)
Information Transfers include the following: 1. Telephone calls less than 30 minutes in length where substantial
business related information is transferred to the individual. 2. Number of information packets or other substantial business related
materials sent by mail, fax, and email (as a result of trade show contacts, website contacts, other marketing events, and telephone requests) or distributed at trade shows or marketing events that are not considered email counseling.
3. Number of newsletters (hard copy or electronic) developed and distributed by ED or its resource partners that promote SBA and ED programs. The newsletters sent to the clients will be counted as one information transfer item (only count the actual newsletter, not the number of people it was sent to).
4. Number of unique visitor contacts to SBA or resource partner websites that request further information. Number of unique website visitors that email SBA or a resource partner requesting small business related information as a result of having visited their website (also include online training that does not meet the definitional requirements).
5. Number of contacts viewing video tapes and/or using onsite library materials containing business related information.
6. Number of individuals attending a presentation (that is less than one hour and does not meet the definition of training) sponsored by SBA or its resource partners.
_______________ _______________ ______________ ______________ ______________
Page 20
SBA Form 2226 Training Guide
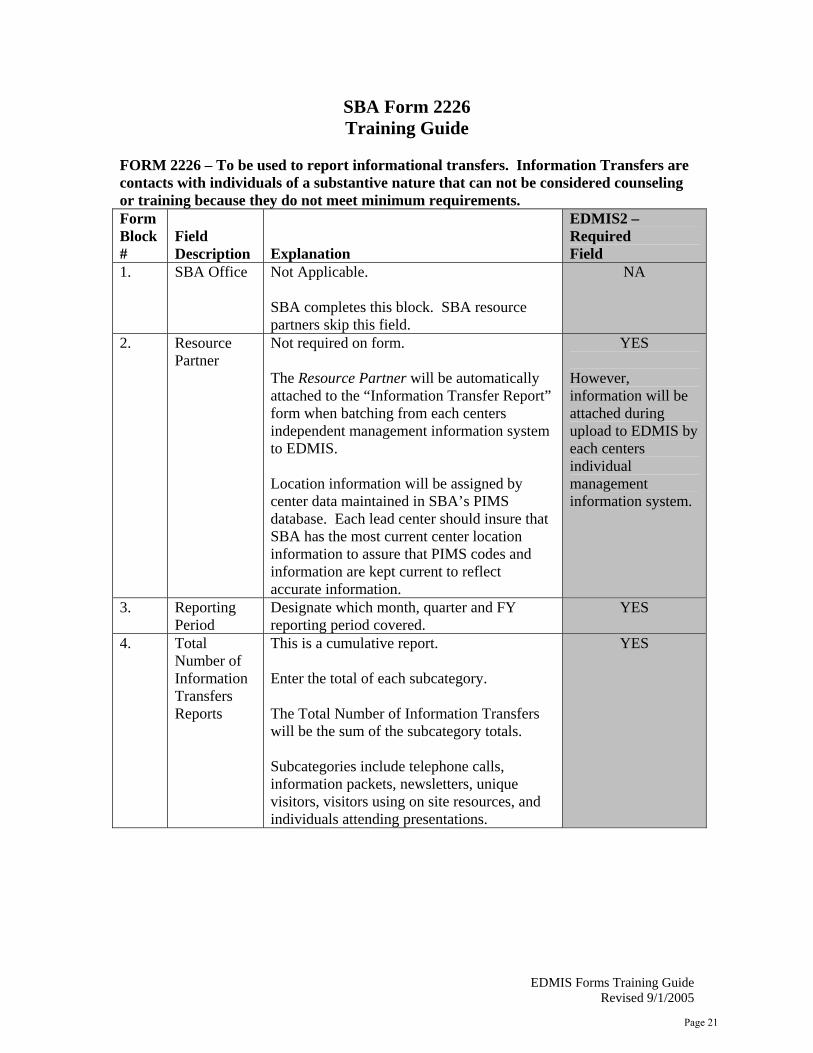
FORM 2226 – To be used to report informational transfers. Information Transfers are contacts with individuals of a substantive nature that can not be considered counseling or training because they do not meet minimum requirements. Form Block #
Field Description Explanation
EDMIS2 – Required Field
1. SBA Office Not Applicable. SBA completes this block. SBA resource partners skip this field.
NA
2. Resource Partner
Not required on form. The Resource Partner will be automatically attached to the “Information Transfer Report” form when batching from each centers independent management information system to EDMIS. Location information will be assigned by center data maintained in SBA’s PIMS database. Each lead center should insure that SBA has the most current center location information to assure that PIMS codes and information are kept current to reflect accurate information.
YES However, information will be attached during upload to EDMIS by each centers individual management information system.
3. Reporting Period
Designate which month, quarter and FY reporting period covered.
YES
4. Total Number of Information Transfers Reports
This is a cumulative report. Enter the total of each subcategory. The Total Number of Information Transfers will be the sum of the subcategory totals. Subcategories include telephone calls, information packets, newsletters, unique visitors, visitors using on site resources, and individuals attending presentations.
YES
EDMIS Forms Training Guide Revised 9/1/2005
Page 21