us food and drug administration approval of drugs for the treatment of prostate cancer: a new era...
TRANSCRIPT

for patients with HPV16-positive OPC is currently intensive and re-sults in substantial morbidity, albeit with a high survival rate, ongoingtrials are evaluating radiation deintensification among patients withHPV-positive OPC. Thus, there may be less intensive treatment op-tions in the future, especially for HPV-driven cancers diagnosed at anearlier stage.
On the basis of available data, we estimate that, in regions like theUnited States where rates of HPV-driven OPC are rare but increasing,the number of individuals in the population needed to be screened todetect one case of OPC is approximately 5,000 (assuming 70% oftumors are HPV16 positive and 90% assay sensitivity), and the num-ber of individuals who screened positive that would yield one case isapproximately 50 (assuming 99.0% specificity); this value decreases toapproximately 11 if specificity increases to 99.8% (Table 1). To put thisinto context, in comparison with cervical cancer screening,7,8 thenumber of individuals needed to screen to detect one cancer would behigher for OPC because of differences in incidence, whereas the num-ber of individuals who screen positive needed to detect one case wouldbe lower for OPC because of the high specificity of the HPV16 E6assay, especially if test characteristics can be further improved.
It is too early to judge the suitability of HPV16 E6 antibody as ascreening tool for OPC, and we will continue to evaluate this poten-tially important cancer prevention opportunity. However, becauseOPC is only a subset of head and neck cancers, even if this marker isproven successful as a screening test, efforts to evaluate markers fornon-HPV–related head and neck cancer are also important if we are tohave a global and meaningful impact.
Aimee R. KreimerNational Cancer Institute, National Institutes of Health, Bethesda, MD
Mattias JohanssonInternational Agency for Research on Cancer, Lyon, France
Allan HildesheimNational Cancer Institute, National Institutes of Health, Bethesda, MD
Michael PawlitaGerman Cancer Research Center, Heidelberg, Germany
Paul BrennanInternational Agency for Research on Cancer, Lyon, France
ACKNOWLEDGMENTWe thank Dr Anna Coghill for her input in the calculations related toHPV16 E6 positivity as a screening tool for oropharyngeal cancer.
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTERESTThe authors indicated no potential conflicts of interest.
REFERENCES1. Castle PE: Teaching moment: Why promising biomarkers do not always
translate into clinically useful tests. J Clin Oncol 32:359-360, 20142. Kreimer AR, Johansson M, Waterboer T, et al: Evaluation of human
papillomavirus antibodies and risk of subsequent head and neck cancer. J ClinOncol 31:2708-2715, 2013
3. McShane LM, Altman DG, Sauerbrei W: Identification of clinically usefulcancer prognostic factors: What are we missing? J Natl Cancer Inst 97:1023-1025, 2005
4. de Martel C, Ferlay J, Franceschi S, et al: Global burden of cancersattributable to infections in 2008: A review and synthetic analysis. Lancet Oncol13:607-615, 2012
5. Anantharaman D, Gheit T, Waterboer T, et al: Human papillomavirusinfections and upper aero-digestive tract cancers: The ARCAGE study. J NatlCancer Inst 105:536-545, 2013
6. Ribeiro KB, Levi JE, Pawlita M, et al: Low human papillomavirus prevalencein head and neck cancer: Results from two large case-control studies inhigh-incidence regions. Int J Epidemiol 40:489-502, 2011
7. Nanda K, McCrory DC, Myers ER, et al: Accuracy of the Papanicolaou testin screening for and follow-up of cervical cytologic abnormalities: A systematicreview. Ann Intern Med 132:810-819, 2000
8. Meijer CJ Berkhof J, Castle PE, et al: Guidelines for human papillomavirusDNA test requirements for primary cervical cancer screening in women 30 yearsand older. Int J Cancer 124:516-520, 2009
DOI: 10.1200/JCO.2013.53.2697; published online ahead of print atwww.jco.org on December 23, 2013
■ ■ ■
US Food and Drug AdministrationApproval of Drugs for the Treatmentof Prostate Cancer: A New EraHas Begun
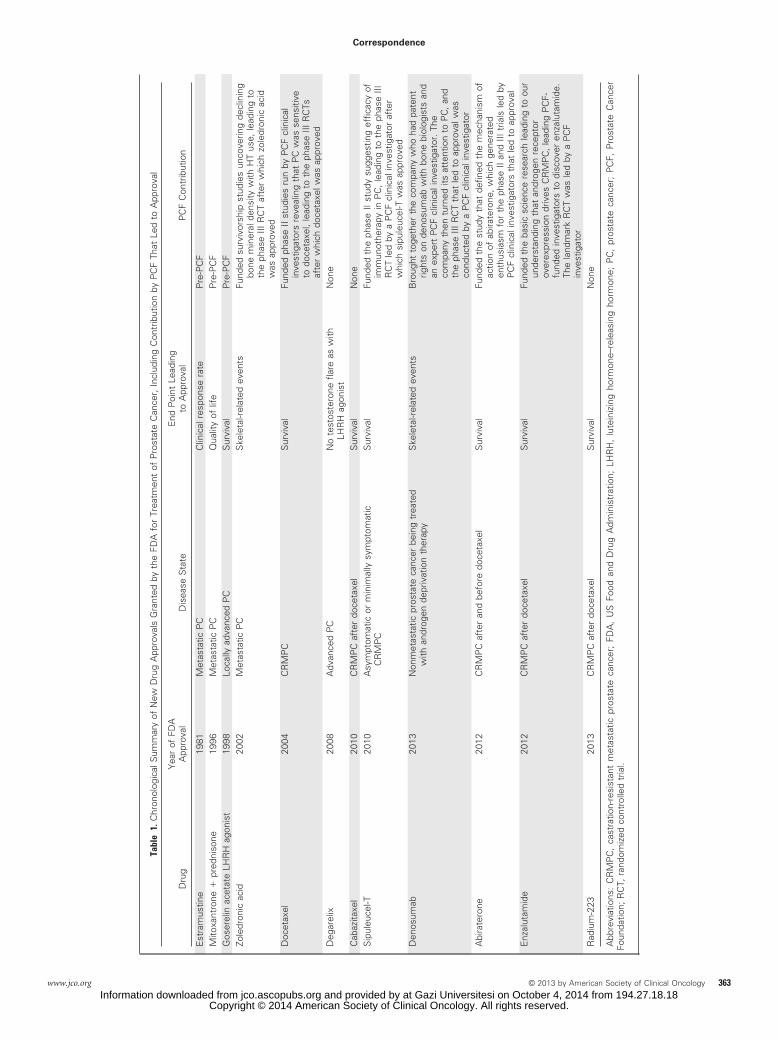
TO THE EDITOR: Before 2002, only three drugs were approved bythe US Food and Drug Administration (FDA) for the treatment ofprostate cancer (PC),1-3 as shown in Table 1, and only one of theseapprovals3 was based on a prolongation of survival from a randomizedclinical trial (RCT). Since then, that number has risen to 12,4 withnearly all new drug approvals (NDAs) a result of a survival benefit thatwas documented in an RCT. What changed?
In 1993, under the umbrella of the newly formed organizationcalled the Prostate Cancer Foundation (PCF),5 formerly the Associa-tion for the Cure of Cancer of the Prostate (CaP CURE), leadingscientific and clinical experts in the treatment of PC were assembledon a board whose mission was to use the resources of PCF to find a wayto expedite new treatments and improve outcomes for men facing a
diagnosis of advanced PC. Significant resources were initially pro-vided by the founder and chairman of this group, Michael Milken,who had been diagnosed with PC in 1993. This was followed by a largefundraising effort by PCF to perpetuate the revenue stream that wasneeded to support ongoing research initiatives. To date, $510 millionhave been raised for PC research, making this organization the largestprivate sponsor of PC research in the world, funding more than 1,600proposals at nearly 200 research centers in 16 countries.
The NDA for zoledronic acid4 was issued by the FDA in 2002.This was the first agent shown to decrease skeletal-related events (eg,compression fractures) in an RCT of men with PC whose primary siteof metastasis is the skeleton. The impetus for this RCT was a PCF-funded survivorship study that elucidated the relationship betweendeclining bone mineral density and hormonal therapy use in PC.Next, work by clinical leaders in the PCF Clinical Consortium contrib-uted to our understanding that PC was sensitive to taxane-basedchemotherapy regimens (ie, docetaxel; sanofi-aventis, Bridgewater,NJ)4; docetaxel was FDA approved in 2004 after the publication of twoRCTs, one of which was led by a PCF clinical investigator and showedan improvement in survival in men with castration-resistant andmetastatic PC. Moving forward, during this new era of NDAs for PC,
Correspondence
362 © 2013 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Information downloaded from jco.ascopubs.org and provided by at Gazi Universitesi on October 4, 2014 from 194.27.18.18Copyright © 2014 American Society of Clinical Oncology. All rights reserved.
Tabl
e1.
Chr
onol
ogic
alS
umm
ary
ofN
ewD
rug
App
rova
lsG
rant
edby
the
FDA
for
Trea
tmen
tof
Pro
stat
eC
ance
r,In
clud
ing
Con
trib
utio
nby
PC
FTh
atLe
dto
App
rova
l
Dru
gY
ear
ofFD
AA
ppro
val
Dis
ease
Sta
teE
ndP
oint
Lead
ing
toA
ppro
val
PC
FC
ontr
ibut
ion
Est
ram
ustin
e19
81M
etas
tatic
PC
Clin
ical
resp
onse
rate
Pre
-PC
FM
itoxa
ntro
ne�
pred
niso
ne19
96M
etas
tatic
PC
Qua
lity
oflif
eP
re-P
CF
Gos
erel
inac
etat
eLH
RH
agon
ist
1998
Loca
llyad
vanc
edP
CS
urvi
val
Pre
-PC
FZo
ledr
onic
acid
2002
Met
asta
ticP
CS
kele
tal-r
elat
edev
ents
Fund
edsu
rviv
orsh
ipst
udie
sun
cove
ring
decl
inin
gbo
nem
iner
alde
nsity
with
HT
use,
lead
ing
toth
eph
ase
IIIR
CT
afte
rw
hich
zole
dron
icac
idw
asap
prov
edD
ocet
axel
2004
CR
MP
CS
urvi
val
Fund
edph
ase
IIst
udie
sru
nby
PC
Fcl
inic
alin
vest
igat
ors
reve
alin
gth
atP
Cw
asse
nsiti
veto
doce
taxe
l,le
adin
gto
the
phas
eIII
RC
Tsaf
ter
whi
chdo
ceta
xelw
asap
prov
edD
egar
elix
2008
Adv
ance
dP
CN
ote
stos
tero
nefla
reas
with
LHR
Hag
onis
tN
one
Cab
azita
xel
2010
CR
MP
Caf
ter
doce
taxe
lS
urvi
val
Non
eS
ipul
euce
l-T20
10A
sym
ptom
atic
orm
inim
ally
sym
ptom
atic
CR
MP
CS
urvi
val
Fund
edth
eph
ase
IIst
udy
sugg
estin
gef
ficac
yof
imm
unot
hera
pyin
PC
,le
adin
gto
the
phas
eIII
RC
Tle
dby
aP
CF
clin
ical
inve
stig
ator
afte
rw
hich
sipu
leuc
el-T
was
appr
oved
Den
osum
ab20
13N
onm
etas
tatic
pros
tate
canc
erbe
ing
trea
ted
with
andr
ogen
depr
ivat
ion
ther
apy
Ske
leta
l-rel
ated
even
tsB
roug
htto
geth
erth
eco
mpa
nyw
hoha
dpa
tent
right
son
deno
sum
abw
ithbo
nebi
olog
ists
and
anex
pert
PC
Fcl
inic
alin
vest
igat
or.
The
com
pany
then
turn
edits
atte
ntio
nto
PC
,an
dth
eph
ase
IIIR
CT
that
led
toap
prov
alw
asco
nduc
ted
bya
PC
Fcl
inic
alin
vest
igat
orA
bira
tero
ne20
12C
RM
PC
afte
ran
dbe
fore
doce
taxe
lS
urvi
val
Fund
edth
est
udy
that
defin
edth
em
echa
nism
ofac
tion
ofab
irate
rone
,w
hich
gene
rate
den
thus
iasm
for
the
phas
eII
and
IIItr
ials
led
byP
CF
clin
ical
inve
stig
ator
sth
atle
dto
appr
oval
Enz
alut
amid
e20
12C
RM
PC
afte
rdo
ceta
xel
Sur
viva
lFu
nded
the
basi
csc
ienc
ere
sear
chle
adin
gto
our
unde
rsta
ndin
gth
atan
drog
enre
cept
orov
erex
pres
sion
driv
esC
RM
PC
,le
adin
gP
CF-
fund
edin
vest
igat
ors
todi
scov
eren
zalu
tam
ide.
The
land
mar
kR
CT
was
led
bya
PC
Fin
vest
igat
orR
adiu
m-2
2320
13C
RM
PC
afte
rdo
ceta
xel
Sur
viva
lN
one
Abb
revi
atio
ns:
CR
MP
C,
cast
ratio
n-re
sist
ant
met
asta
ticpr
osta
teca
ncer
;FD
A,
US
Food
and
Dru
gA
dmin
istr
atio
n;LH
RH
,lu
tein
izin
gho
rmon
e–re
leas
ing
horm
one;
PC
,pr
osta
teca
ncer
;P
CF,
Pro
stat
eC
ance
rFo
unda
tion;
RC
T,ra
ndom
ized
cont
rolle
dtr
ial.
Correspondence
www.jco.org © 2013 by American Society of Clinical Oncology 363Information downloaded from jco.ascopubs.org and provided by at Gazi Universitesi on October 4, 2014 from 194.27.18.18
Copyright © 2014 American Society of Clinical Oncology. All rights reserved.

avoiding a testosterone flare became possible with a single agent in2008 with the approval of degarelix,4 a pure luteinizing hormone–releasing hormone antagonist. Then, in 2010 and 2011, three newagents were approved by the FDA for patients with PC: sipuleucel-T(Provenge; Dendreon, Seattle, WA),4 the first immunotherapy tostimulate the body’s immune system and prolong survival, remark-ably, in the absence of a prostate-specific antigen response; Jevtana(cabazitaxel; sanofi-aventis),4 another taxane-based chemotherapythat prolonged survival after disease progression during treatmentwith docetaxel; and finally, on September 16, 2011, the FDA grantedapproval for Xgeva (denosumab; Amgen, Thousand Oaks, CA)4 as atreatment to increase bone mass in patients who are at high risk offracture from receiving androgen deprivation therapy for nonmeta-static PC. PCF’s sentinel contributions leading to FDA approval fortwo of these three agents are described in Table 1. During the last 2years, abiraterone acetate4 and enzalutamide,4 two novel forms ofhormonal therapy that have been shown in the context of multi-institutional RCTs to prolong survival and improve patient-reportedhealth-related quality of life for men with castration-resistant andmetastatic PC, have been approved by the FDA and are now beingtested in earlier stages of the disease by cooperative groups around theworld. The expectation is that these agents will increase the probabilityof cure for men with newly diagnosed high-risk and nonmetastaticPC. PCF played the major role in defining the mechanism of actionof these drugs, and in one case, supported the research that led tothe discovery of the drug. In both cases, PCF clinical investigatorsled the RCTs that resulted in FDA approval, as detailed in Table 1.Finally, on May 15, 2013, the first radiopharmaceutical, radium-223,4 was found to prolong survival in men with PC and bonemetastasis refractory to conventional hormonal therapy.3 By selec-
tive uptake in bone and the short distance (� 1 mm) over whichthe charged particle (ie, alpha particle) acts, damage to surround-ing hematopoietic tissues was minimal.
Therefore, of the nine NDAs that occurred after 2002, six weredriven by research and collaborations that existed because of PCF, asshown in Table 1. Today, with federal funding initiatives for cancerresearch continuing to decline, the need for novel approaches, such asthat used by PCF to fund the research that lead to NDAs, are neededacross all cancers.
Anthony V. D’AmicoBrigham and Women’s Hospital and Dana-Farber Cancer Institute, Boston, MA
AUTHOR’S DISCLOSURES OF POTENTIAL CONFLICTS OF INTERESTThe author(s) indicated no potential conflicts of interest.
REFERENCES1. Perry CM, McTavish D: Estramustine phosphate sodium: A review of its
pharmacodynamic and pharmacokinetic properties, and therapeutic efficacy inprostate cancer. Drugs Aging 7:49-74, 1995
2. Kantoff PW, Halabi S, Conaway M, et al: Hydrocortisone with or withoutmitoxantrone in men with hormone-refractory prostate cancer: Results of thecancer and leukemia group B 9182 study. J Clin Oncol 17:2506-2513, 1999
3. Bolla M, Gonzalez D, Warde P, et al: Improved survival in patients withlocally advanced prostate cancer treated with radiotherapy and goserelin. N EnglJ Med 337:295-300, 1997
4. Leibowitz-Amit R, Joshua AM: The changing landscape in metastaticcastration-resistant prostate cancer. Curr Opin Support Palliat Care [epub aheadof print on June 28, 2013]
5. Prostate Cancer Foundation. http://www.pcf.org/site/c.leJRIROrEpH/b.5699537/k.BEF4/Home.htm
DOI: 10.1200/JCO.2013.53.9528; published online ahead of print atwww.jco.org on December 16, 2013
■ ■ ■
Correspondence
364 © 2013 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Information downloaded from jco.ascopubs.org and provided by at Gazi Universitesi on October 4, 2014 from 194.27.18.18Copyright © 2014 American Society of Clinical Oncology. All rights reserved.