urine under microscope
TRANSCRIPT


Urine Under MicroscopeDr. Abrar Ali KatparDepartment of Nephrology
King Khalid Hospital-Hail
Kingdom of Saudi Arabia.

Introduction
Urinalysis is perhaps the most common investigation performed in clinical
practice it is noninvasive inexpensive and easy to perform test, which
provides wealth of useful information especially on patients with renal
disease. It not only assists in the diagnosis of renal disease but can also
provide information about the severity and outlook of the disease.
In order to obtain maximum information from this elementary investigation,
the physician looking after the patients should preferably do itself. Because
he alone will ultimately be in better position to correlate the findings with
the disease and fully grasp its implications.

Urine Collection
For microscopy, urine should be collected in an open-mouth, clean but not
necessarily a sterile container. Although the first morning specimen is most
concentrated and acidic due to overnight fast, the second urine of the
morning is preferable for microscopy, as it too is concentrated and acidic but
without overnight stay in the bladder which causes lysis of the cells and cast.

For reliable urine microscopy and culture, carefully collected Midstream Urine without contamination from the genitalia is essential. For this, the patient must be instructed about the correct procedure. The patient should be explained in plain simple language that before collecting a specimen of his/her urine, hands and external genitalia should be gently washed with water or saline: disinfectants should not be used. Also that overzealous cleaning is harmful, because it can possibly cause abrasions of the periuretheral area and result in bleeding; thus contaminating the specimen. The patient should also be explained that it would be ideal for him/her to have a moderately full bladder. Furthermore to avoid contamination men should be advised to retract their foreskin (if Present) and women should hold their labia apart. Once they start voiding, the first 200ml of urine should be discarded, and the next 100-200 ml of urine should be collected in container by moving it in and out of free-flowing urine stream.

If a proper mid-stream specimen cannot be collected as in the case of infants,
or young children, or aged persone because of there physical shortcoming or
mental handicap, the requisite urine specimen can be obtained either by an
open-ended catheter or suprapubic aspiration.

STORAGE OF URINE
To avoid any possible alterations in physical or chemical feature, urine should
ideally be analyzed with in an hour of Voiding. With passage of time the cells
in the specimen tend to lyse and cast disintegrate especially in urine with low
specific gravity and or alkaline pH. Moreover, with prolong stay at room
temperature, bacteria have tendency to multiply obscuring the very cells and
casts. Several means of preservations of cells with chemical reagents (0.5%
Glutaryldehyde, Boric Acid, Formalin) and refrigeration at 4 degrees
centigrade have been proposed. But these tends to interfere with chemical
reaction. On the other hand refrigeration of urine causes crystals to
precipitate, obscuring cells and cast.

Starting

URINE MICROSCOPY
To obtain maximum possible information it is important to examine the urine
using a phase-contrast microscope with the added facility of polarized light.
Colorless, or unstained objects, have little effect on the amplitude of light
waves; hance observing such objects under bright field is not very helpful.
With phase-contrast microscopy, light passing through a relatively thick or
dense part of a cell, such as the nucleus, is retarded compared with light
passing through media only, or a thin part of the specimen. The degree of
retardation, and the extent of the phase-shift that result, is proportional to
the thickness of the object.
The the phase-contrast microscope thus exploit the interference effects that
takes place when the two types of light recombine. If the waves complement
each other, the light is brighter, while if they are 180 degrees out of phase,
one cancels other, and the image becomes dark. To sum up phase-contrast
microscopy enhances the ability to see and identify cells and cast, which are
not visible with bright-light microscopy. Polarized light is particularly useful in
identifying free fat, cholesterol and crystals of calcium oxalate, uric acid.

To quantify formed elements in the urine, most authors recomned
centrifugation of a fixed volume of urine, transferring a drop of urine from
the deposit to a glass slide and then counting the cells under high power. With
this semi-quantitative method, cells are described as number or a range of
cells observed per high power field(HPF).

This method has been found open to error at almost every step. The number
of cells/HPF depend largely upon various factors namely:
a- The quantity of urine centrifuged
b- The type and speed of centrifuged
c- The duration of centrifugation
d- The method of discarding the supernatant and
e- The amount of urine in which the sediment is re-suspended.

The volume of urine under the cover slip also varies and depends upon the
size of the drop of urine, weight of the coverslip and viscosity of the urine.
It is not easy to control so many variables; hence this method of semi-
quantitative estimation of cells can be erroneous.
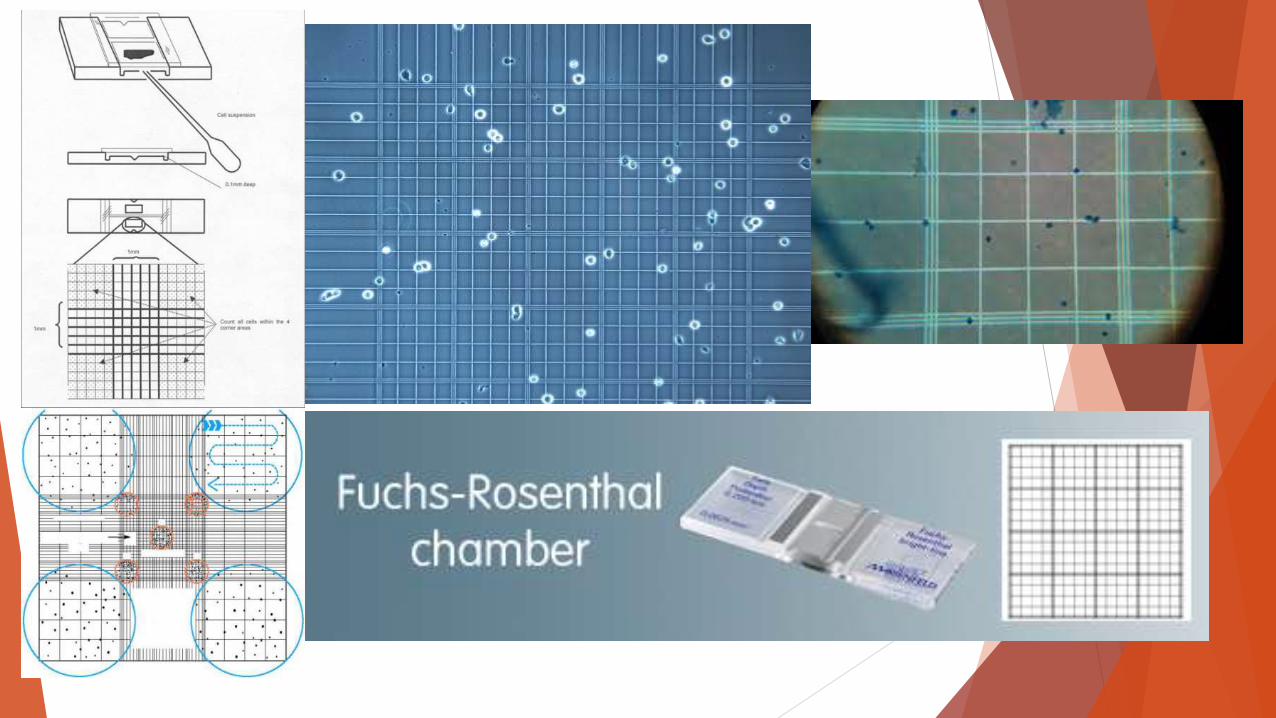
Therefor, with a view to avoid such errors, counting of cells using
uncentrifuged urine and a counting chamber is recommended. A Fuchs-
Rosenthal counting chamber is particularly useful
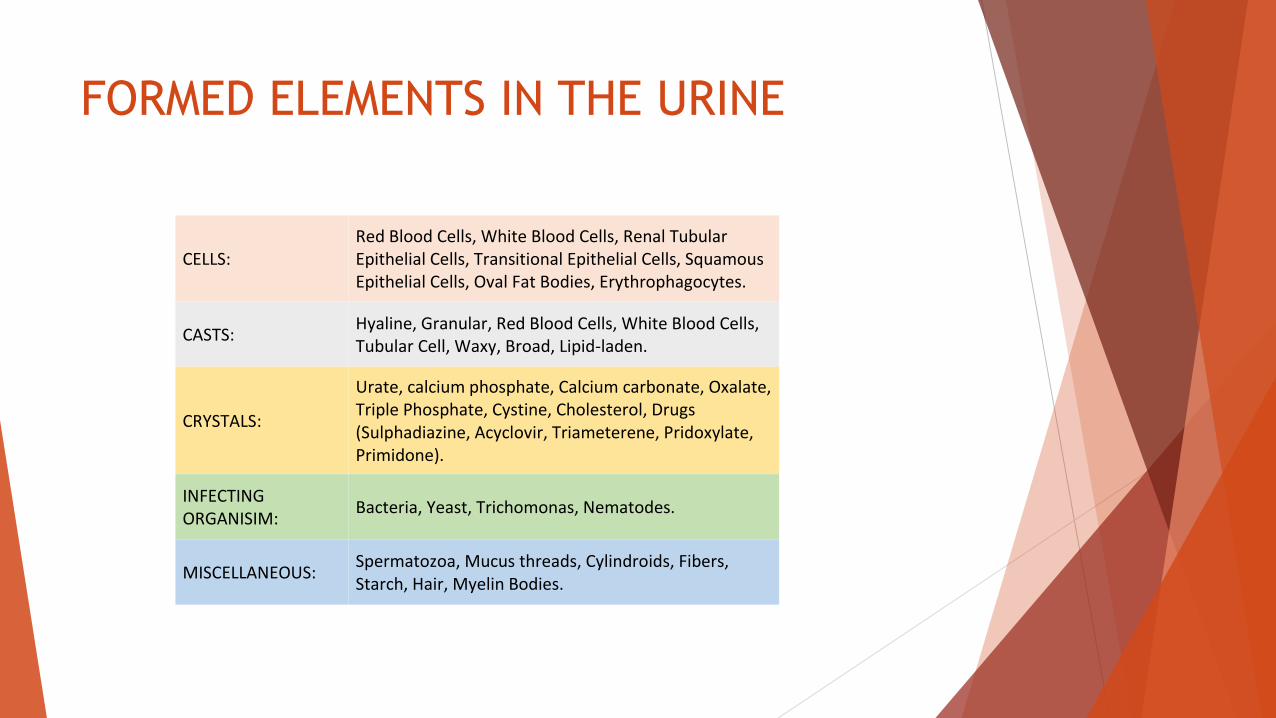
FORMED ELEMENTS IN THE URINE
CELLS: Red Blood Cells, White Blood Cells, Renal Tubular Epithelial Cells, Transitional Epithelial Cells, Squamous Epithelial Cells, Oval Fat Bodies, Erythrophagocytes.
CASTS: Hyaline, Granular, Red Blood Cells, White Blood Cells, Tubular Cell, Waxy, Broad, Lipid-laden.
CRYSTALS:
Urate, calcium phosphate, Calcium carbonate, Oxalate, Triple Phosphate, Cystine, Cholesterol, Drugs (Sulphadiazine, Acyclovir, Triameterene, Pridoxylate, Primidone).
INFECTING ORGANISIM:
Bacteria, Yeast, Trichomonas, Nematodes.
MISCELLANEOUS: Spermatozoa, Mucus threads, Cylindroids, Fibers, Starch, Hair, Myelin Bodies.

Red blood cells
Red Blood Cells may be found in normal urine. With semi-quantitative methods, up to 1-2
RBC/HPF are considered normal. With phase-contrast microscopy, the upper limit of normal in
un-centrifuged urine is 15000 cells/ml and all are of glomerular origin.
About 30% of cells are lost either with centrifugation or resuspension.
Therefore upper limit of normal in a centrifuged urine is 10,000 cells/ml.
The normal limit with bright light is lower, as some of the cells seen with phase contrast are
either not visible or misinterpreted as debris.
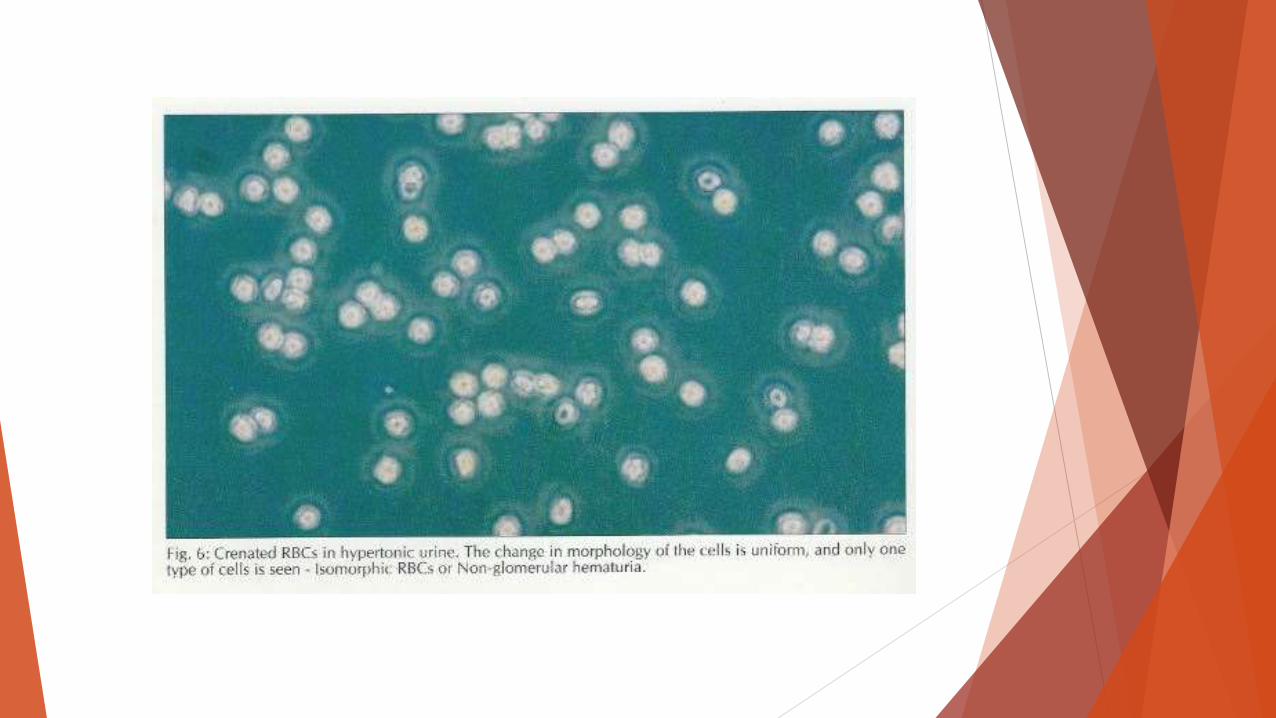
RBC’s are likely to undergo several morphological changes in the urine.
Some of these changes are non specific and due to physiochemical environment. FIG:6

Brich and fairley were
the first to note that
rbc’s cells in the urine of
patients with
glomerulonephritis have
peculiar changes (fig:7-
13).
Other s subsequently
confirmed these
findings.

White blood cells
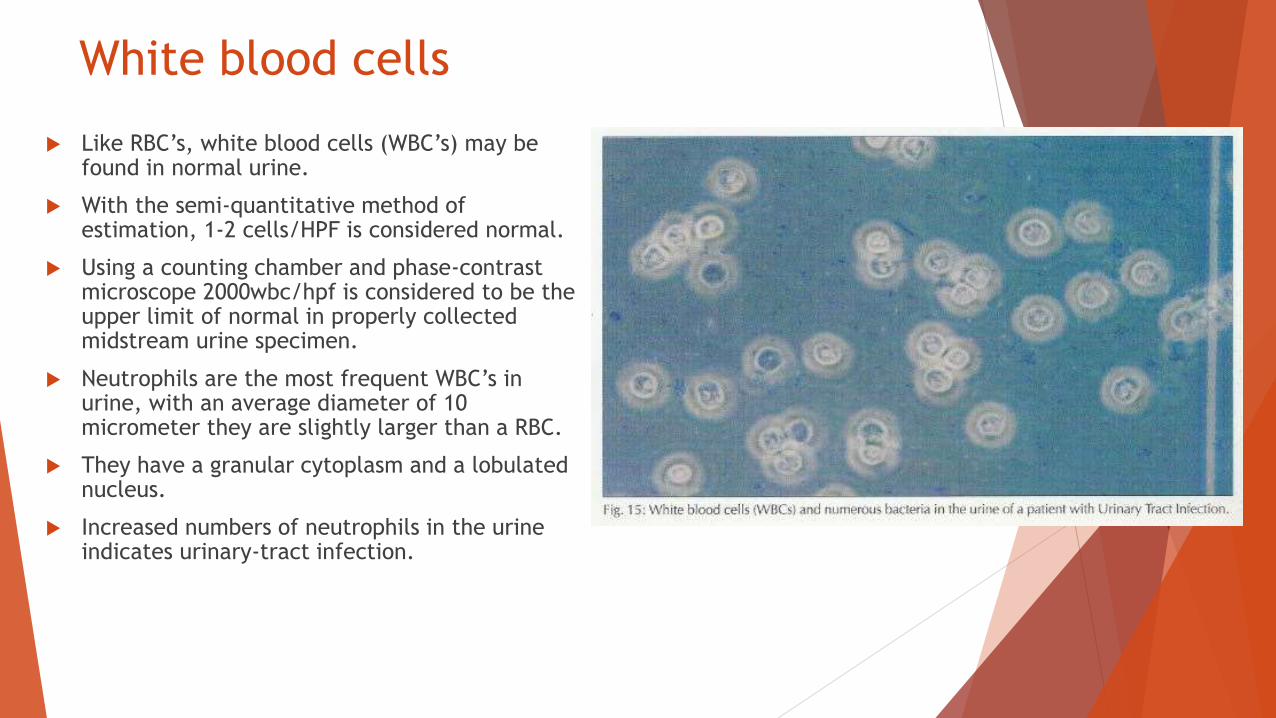
Like RBC’s, white blood cells (WBC’s) may be found in normal urine.
With the semi-quantitative method of estimation, 1-2 cells/HPF is considered normal.
Using a counting chamber and phase-contrast microscope 2000wbc/hpf is considered to be the upper limit of normal in properly collected midstream urine specimen.
Neutrophils are the most frequent WBC’s in urine, with an average diameter of 10 micrometer they are slightly larger than a RBC.
They have a granular cytoplasm and a lobulated nucleus.
Increased numbers of neutrophils in the urine indicates urinary-tract infection.

When their number increases without
bacteriuria or growth on culture, renal
tuberculosis, renal calculi, renal papillary
necrosis, polycystic kidney disease and
infection with fastidious organism should be
considered.
Lymphocytes are smaller than neutrophils.
Although they can be identified with phase-
contrast microscopy, their identification
usually requires special staining.
They are frequently found in the urine of
renal transplant recipient’s during episodes
of acute cellular rejection.
Eosinophils are slightly larger than
neutrophils and are only identified by
special stains.
They are seen in acute interstitial nephritis
and in patients with athero-embolic disease.

Mucus
Mucus in the urine appears as
ribbon-like threads of variable
width and length.
It is a normal constituent of urine
and of no pathological
significance.

Cylindroids
These are similar to cast with
one of their ends resembling a
mucus thread.
In the past there was some
controversy over their origion.
It is now clear that they are
composed of tamm-horsfall
mucoprotein and are therefore
cast.
They may contain particles like
cast. Fig:

Cast
Cast Are elongated cylindrical structure.
They acquire shape from the tubular lumen (distal tubular and collecting
ducts) in which they are formed. They are composed of Tamm-Horsfall
glycoprotein.
Cast formation is favored by factors which promote aggregation of Tamm-
Horsefall proteins, which include increased urinary concentration of
electrolytes, hydrogen ions, and ultra-filtered proteins.
Iteraction between the protein and hemoglobin, myoglobin, Bence-Jones
proteins or radio contrast media also favor formation.
Different formed elements transported along the nephron are traped in them
producing various types of Cast (Table).
Igor Tamm &
Frank Horsfall
Glycoproteins
Uromodulin
Gene= UMOD
Chromosome16

HYALINE CAST These consist of Tamm-Horsfall
Mucoprotein only.
As they have low refractive
index they easily escape
detection if a bright-field
microscope is used.
They are occasionally present
in normal individuals, but are
increased in renal diseases.
They are also observed in
patients with acute cardiac
failure, fever, those receiving
loop diuretics, and in normal
people after strenuous activity.

GRANULAR CAST
These contain granules that
may be either fine or
coarse.
Granules consist of ultra-
filtered proteins or
degenerated cells.
Their presence in the urine
is always pathological.
Large numbers of coarse
granular casts are
particularly seen in acute
tubular necrosis.

WAXY CAST
Waxy casts are highly
retractile, usually large with
clear cut edges.
Their composition is different
from other cast, and are
resistant to dissolution to
alkaline urine.
They are typically found in
patients with advanced renal
failure.

ERYTHROCYTE CAST
Erythrocyte cast show enormous
Variation in morphology, and
contains variable number of RBC’s.
They indicate glomerular bleeding.

LEUKOCYTE CAST These contain variable number of
neutrophils.
They are commonly found in acute
or chronic pyelonephritis.
They are also seen in proliferative
glomerular lesions like acute post
streptococcal glomerulonephritis,
active mesangiocapillary
glomerulonephritis and lupus
nephritis.
It is at time, difficult to
distinguish leukocytes within the
cast from tubular epithelial cells.

FATTY CAST These contain variable amount
of lipids and are usually seen in
the urine of patients of with
Nephrotic syndrome.

Lipid Droplets Lipid droplets can be seen
in the urine either as free
droplets, within the renal
tubular epithelial cells Fig:
or with in the Cast.
Lipids are usually seen in
the urine of patient with
heavy proteinuria.
How ever they are also
described in patients with
Low-Grade proteinuria.

Oval Fat Bodies Oval Fat bodies are renal
tubular epithelial cells full
of cholesterol esters.
The fat is easily identified
with polarized-light
microscopy when a
‘Maltese Cross’
appearance is seen.

Squamous Epithelial Cells
Thease are large (mean
diameter 55 um) flat cells with
abundant granular cytoplasm
and a small central nucleus.
They are exfoliated from the
bladder and urethra.
Un women with vaginal
discharge, they contaminate the
urine.

Renal Tubular Epithelial Cells Renal tubular epithelial cells,
most commonly found in the urine are from the proximal tubules.
They are round to ovioid cells with an average diameter of 13um and have a single nucleus.
Normally they are not present in the urine.
They may be found in increase in number after exercise and after ingestion of certain drugs.
They are frequently present in case of acute tubular necrosis and acute renal allograft rejection.
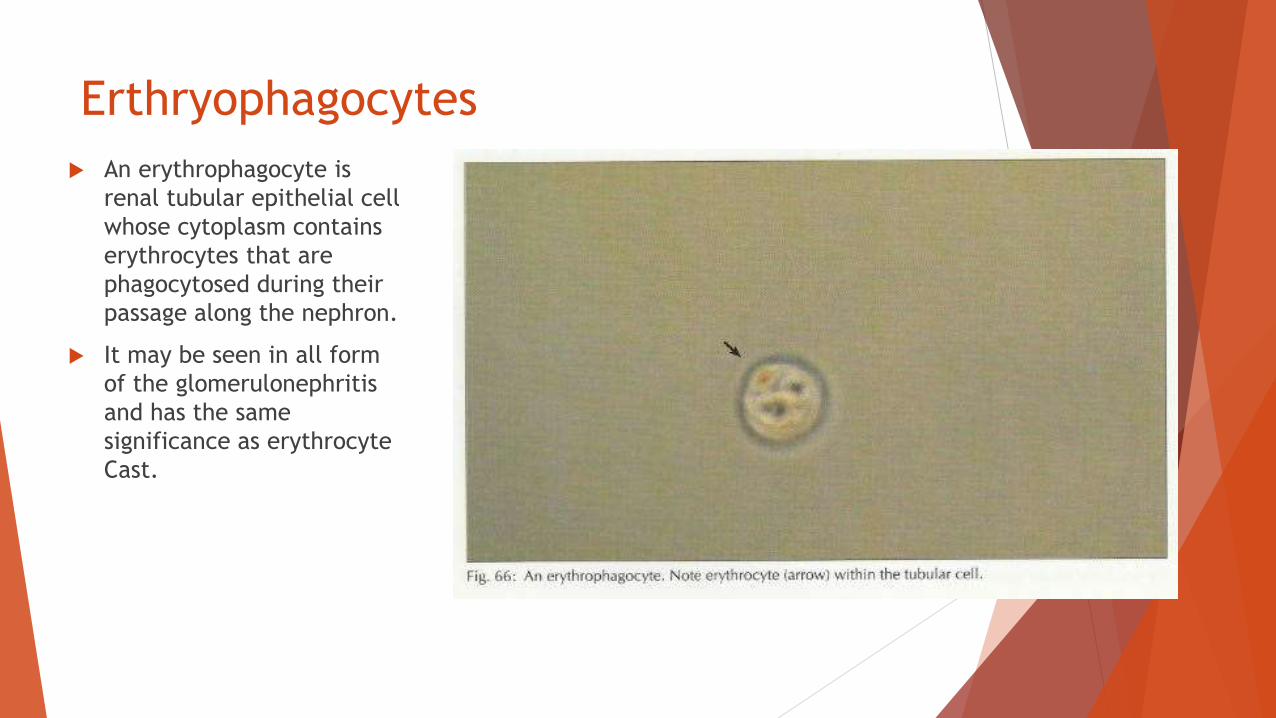
Erthryophagocytes
An erythrophagocyte is
renal tubular epithelial cell
whose cytoplasm contains
erythrocytes that are
phagocytosed during their
passage along the nephron.
It may be seen in all form
of the glomerulonephritis
and has the same
significance as erythrocyte
Cast.
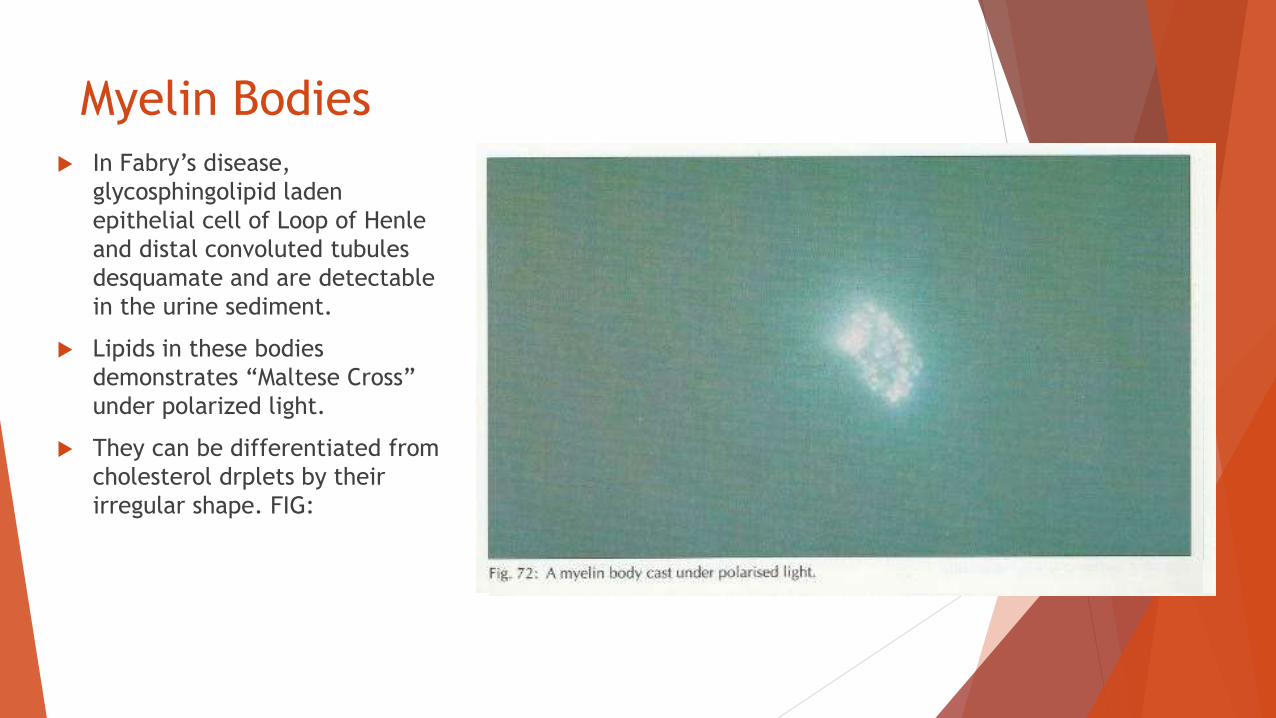
Myelin Bodies In Fabry’s disease,
glycosphingolipid laden
epithelial cell of Loop of Henle
and distal convoluted tubules
desquamate and are detectable
in the urine sediment.
Lipids in these bodies
demonstrates “Maltese Cross”
under polarized light.
They can be differentiated from
cholesterol drplets by their
irregular shape. FIG:

Candida Candida is the most frequent
yeast found in the urine.
They appear as pale-green
cells often nucleated, and
with smooth well-defined
walls.
They are commonly seen in
the urine because of
contamination from genitalia.
They can also grow in urinary
tract of patient with: diabetes
mellitus; having indwelling
catheters; on prolong
antibiotic therapy; or
receiving immunosuppression.

Bacteria
Bacteria are frequently seen in
urine sediment.
They do not necessarily indicate
infection and may be the result
of contamination of urine.
Presence of leukocytes with
bacteria increase the probability
of the infection.

Crystals
The urine can contain several types
of crystals.
Uric Acid, Amorphous Urates,
Calcium oxalates, Cystine, Leucine,
Tyrosine, and Cholesterol crystals
are found in acid urine.
Whereas crystals of Calcium
phosphate, Tripple Phosphate and
Amorphus Phosphate are found in
alkaline urine.

Thank you