urine juli jav - fizioms.ro€¢ an array of tests performed on urine • one of the most common...
TRANSCRIPT
Urinalysis

Urinalysis
• an array of tests performed on urine • one of the most common methods of medical
diagnosis• easy to perform, non-invasive • fresh urine (midstream urine collection, 30-60 ml)
or 24 h urine

Reasons to perform• Routine medical evaluation:
– general yearly screening, – assessment before surgery (pre-operative assessment), admission to hospital, – screening for kidney disease, – chronic diseases: diabetes mellitus, hypertension (high blood pressure), liver disease
• Assessing particular symptoms: – abdominal pain, – jaundice,– thirst, – weight loss– painful urination, – flank pain, – fever, – blood in the urine
• Diagnosing medical conditions:– urinary tract infection, – kidney infection, – kidney stones, – kidney impairment, – kidney inflammation (glomerulonephritis)
• Monitoring disease progression and response to therapy: – diabetes related kidney disease, – blood pressure related kidney disease

Urinalysis
• macroscopic analysis– quantity– color– odour– clarity
• biochemical examination– specific gravity / density– pH– blood, protein– glucose, ketones, bilirubin, urobilinogen
• microscopic assessment

Macroscopic analysis
• Quantity– 1500-2000 ml daily – normal water intake– under 500 ml daily: oliguria– under 100 ml daily: anuria– above 2500 ml daily: polyuria

• Color– transparent solution – can range from colorless to amber, a pale yellow– physiological: the color comes primarily from the
presence of urobilin (← heme ← hemoglobin ←aging red blood cells)
Macroscopic analysis

• Abnormal color:– dark yellow ← dehydration– light orange ← B vitamins– orange ← drugs (rifampicin, phenazopyridine)– dark orange to brown ← jaundice,liver diseases– black or dark-colored (melanuria) ← melanoma– reddish or brown ← porphyria, hematuria– pink or reddish ← consumption of beets– greenish ← consumption of asparagus– fluorescent yellow / greenish ← dietary supplemental
vitamins (B vitamins)
Macroscopic analysis

• Odor– described as urinoid– can be strong in concentrated specimens, does not
imply infection– fruity or sweet odor ← diabetic ketoacidosis– ammoniacal odor ← alkaline fermentation – pungent odor ← UTIs– other abnormal odors : medications and diet,
gastrointestinal diseases
Macroscopic analysis

• Turbidity / Clarity ← bacterial infection← proteinuria← crystallization of salts:
• phosphates – clears if 10% acetic acid is added• urates – clears by heating• oxalates – clears if HCl is added
Macroscopic analysis

Biochemical properties• aqueous solution:
– > 95% water– urea 9.3 g/l– chloride 1.87 g/l– sodium 1.17 g/l– potassium 0.750 g/l– creatinine 0.670 g/l– other dissolved ions, inorganic and organic compounds
• some diseases alter the quantity and consistency of the urine– e.g. glucose ← diabetes

• Density / specific gravity• normal urine specific gravity: 1.015-1.025 • high values:
← the kidney is actively reabsorbing water ← fluid depletion or renal failure due to reduced renal perfusion
← abnormal urinary compounds – e.g. glucose in diabetes
• low values: ← failure of the renal tubules to concentrate urine
usually associated with high urine volumes
Biochemical properties

Biochemical properties
• Acidity (pH)– normally acid (pH = 5-6)– pH can vary between 4.4-8.4– pH can be modified by drugs, diseases (diabetes,
renal tubular acidosis), urinary infections– pH ↑: drugs (acetazolamide, potassium citrate, and
sodium bicarbonate), diet high in citrus, vegetables– pH ↓: drugs (ammonium chloride, chlorothiazide
diuretics, methenamine mandelate), diet high in meat or cranberries
– modified pH can lead to stone formation
Biochemical properties
• Demonstration of proteins• macromolecules → they are not normally present in
measurable amounts in the glomerular filtrate or in the urine
• proteinuria← the permeability of the glomerulus is abnormally
increased ← the function of the proximal convolute tube is altered
• pathological if > 30mg/24 h

• Esbach's test– put 5 ml of urine in a test tube– add 1 ml of Esbach's reagent (10g picric acid and 20
g citric acid dissolved in 1 l of water)– appearance of a white-yellow precipitate indicates the
presence of proteins
Biochemical properties

• reaction with trichloroacetic acid– put 5 ml of urine in a test tube– add 1 ml of trichloroacetic acid (10% or 20%)– appearance of a flocculent precipitate indicates the
presence of proteins
Biochemical properties

• Qualitative determination of urobilinogen• Ehrlich's test
– put 5 ml of fresh urine in a test tube– add 3-4 drops of Ehrlich reagent (p-
dimethylaminobenzaldehyde in HCl)– after 1-2 min pink or faint red color that intensifies on
heating indicates increased urobilinogen levels
Biochemical properties

• Qualitative determination of reducing sugars• Nylander's test
– a test for glucose in the urine using a solution containing bismuth subnitrate which forms a black precipitate in a positive reaction
– put 5 ml of urine in a test tube– add 1 ml of Nylander's reagent (potassium sodium
tartrate, sodium hydroxide, and bismuth subnitrate in water) and heat for 4 min
– in the presense of a reducing sugar the bismuth is reduced and forms a black precipitate
Biochemical properties

Microscopic assessment• the urine sediment is centrifuged and examined using
low power microscope (at least 10 microscope fields)– cells:
• epithelial cells• red blood cells• white bloods cells
– crystals– casts– bacteria or yeast
• in counting chambers using urine produced over a determined time (ex. 180 minutes)

• red blood cells– 1-5 RBC/HPF (400x) or 1000 RBC/min– renal origin: deformed, faded color– from the urinary tract: normal shape and color– inflammation, injury, or disease in the kidneys or
elsewhere in the urinary tract
Microscopic assessment

• white blood cells:– 3-5 WBC/HPF or 2000 WBC/min – usually in groups of 10-15 cells– if they form casts: renal origin– increase ← infection or inflammation in the urinary
tract
Microscopic assessment
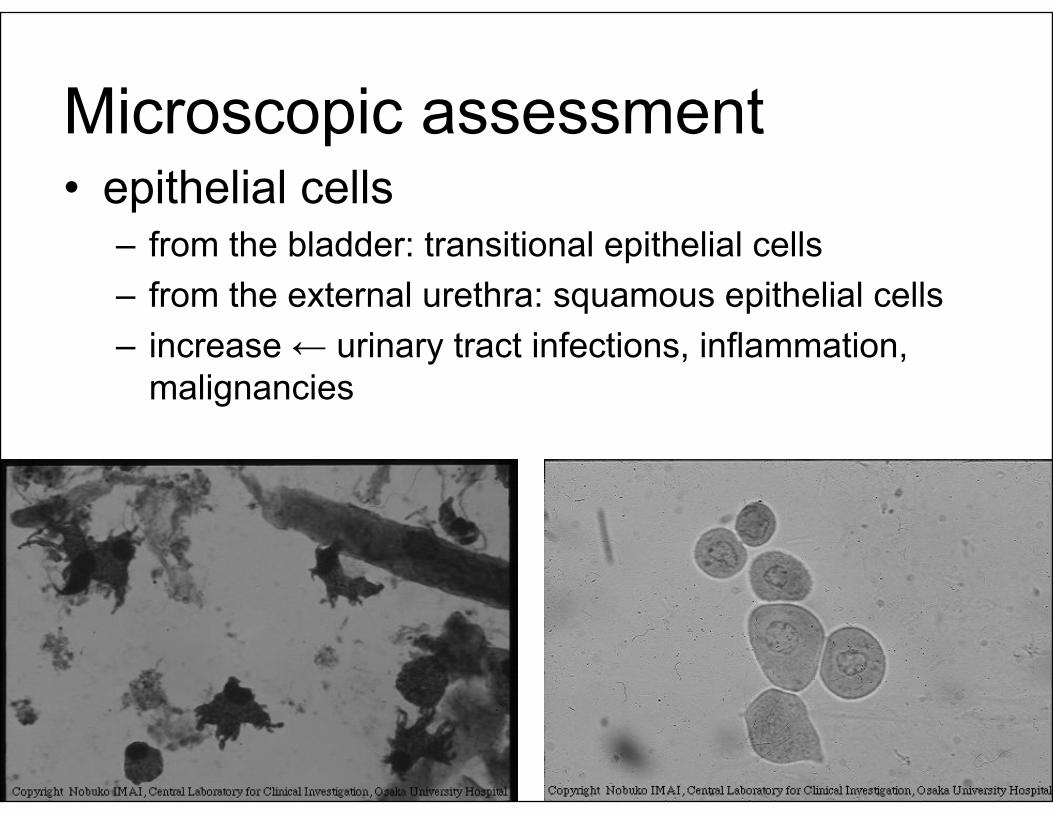
• epithelial cells– from the bladder: transitional epithelial cells – from the external urethra: squamous epithelial cells– increase ← urinary tract infections, inflammation,
malignancies
Microscopic assessment

• Urinary casts:– cylindrical structures produced by the kidney – formed in the distal convoluted tubule and collecting
ducts of nephrons– types:
• hyalin• red cell• granular• epithelial• waxy• fatty
Microscopic assessment

• hyaline casts: – the most frequently occurring – colorless, homogeneous, transparent, usually
rounded ends
Microscopic assessment

• red cell casts:– ← renal hematuria– brown to almost colorless – usually diagnostic of glomerular disease
Microscopic assessment

• white cell casts: – indicative of inflammation or infection of the kidneys
Microscopic assessment

• granular casts: – indicate significant renal disease– color: black to pale yellow
Microscopic assessment

• epithelial casts:– rare; in renal diseases that primarily affects the
tubules
Microscopic assessment

• waxy casts: – result from the degeneration of granular casts– ← severe chronic renal failure, malignant
hypertension, and diabetic disease of the kidney– short, broad casts, with blunt or broken ends
Microscopic assessment

• Crystals– solutes can form crystals if:
• the urine pH is increasingly acidic or basic;• the concentration of dissolved substances is
increased; and• the urine temperature promotes their formation
– they may group together to form kidney "stones" or calculi
Microscopic assessment