updated review of gout...
TRANSCRIPT

ìUpdatedReviewofGoutManagementDrGarethSTarr-28thMay2016
MBBcHFCP(SA)Mmed(IntMed)Cert(Rheum)PhdCandidate(STB)

ReproducEonmadefromacopyheldbytheHarvardMedicalLibraryintheFrancisA.CountwayLibraryofMedicine.

‘TheGout’byJamesGillray(1799)
Epidemiology
ì CommonestinflammatoryarthriEsinmen;ì Increasingfrequencyinfemales.
ì 7%ofmenovertheageof65;
ì 3%ofwomenagedover85years;
ì Stronglyrelatedto:ì Metabolicsyndrome,ì Chronicrenalimpairment,ì Certaindrugtreatments,includingdiureEcs.
MikulsTr,elal.CurOpinRheumatol2006;18:199-203.LawrenceRC,etal.ArthriEsRheum2008;58:26-32.

Epidemiology(cont.)
Severalepidemiologicalstudieshavedemonstratedanincreaseintheseverityandprevalenceofgout.
ì ArromdeeE,etal.JRheumatol2002;29:2403–6.
ì FelsE,etal.CurrOpinRheumatol2008;20:198–202.
ì WallaceKL,etal.JRheumatol2004;31:1582–7.
ì Perez-RuizF.AnnRheumDis2006;65(Suppl2):436.

Conundrum
Why,then,
despitethepossibilityofearlyandaccuratediagnosis,
theavailabilityofeffecEvetreatmentandourinsightintotheseverityandconsequencesofthedisease,
isgoutmanagedsoineffecEvely?

DohertyM,etal.AnnRheumDis2012;71:1765–1770

ProgressionofJointDamage

RheumatoidArthriEs ChronicTophaceousGout

CommonMisconceptions
ì Self-limiteddisease
ì CrystaldeposiEonconEnuesdespitelong‘symptom’freeperiodèDestrucEveArthriEs.
ì Benign,ratherthanserious
ì Humorous.
ì Historically–“Diseaseofkings”.
ì AssociaEonofCardio-renaldiseaseandshortenedlifeexpectancy.
FeigDl,etal.NEnglJMed2008;359:1811–21

Zandman-GoddardG,etal.Rheumatology2013;52:11261131

‘PunchCurestheGout,theColicandthe“tisick”’byJamesGillray
(1799)
ThesedistortedpercepEonsofthenatureofgouthaveamarkednegaEveeffecton
paEents’adtudestotheirgoutand
itstreatment.
WhatabouttheDoctor’sapproach?
ì GoutislargelymanagedbygeneralpracEEoners.
ì MajorityofpaEentsareneverreferredforaspecialistopinion.
ì ApproachtogoutmanagementisbesetwithmisconcepEonsandmyths.

LeslieR,etal.Rheumatology2013;52:16231629

ManagementQuestions
ì WhendoIstartUrateloweringtherapy(ULT)?
ì DoIconEnueULTduringanacuteahack?
ì Whatistheroleofcolchicine?
ì HowlongdoIconEnuecolchicinefor?
ì WhatlevelofserumuricacidamIaimingfor?

ManagementofAcuteGoutyAttack
KhannaD,elAl.ArthriEsCare&Research.2012;64(10):1447–1461.
AssesstheSeverity
Monotherapy
NSAID(e.g.Arcoxia)
SystemicSteroids Colchicine
OpEon:IniEalCombinaEonTherapy
Mild-moderatepain,parEcularlyforanaSackaffecEngonly1orafewsmalljoints,or1-2largejoints.
SeverePain,PolyarEcularaSack,mulEplelargejoints.

Etoricoxibcon
centraEo
n(ng/ml)
Time(hours)0 12 24 36 48
0
500
1500
200060mg120mg(n=12)
t1/2=half-life*SingleoraldosestohealthysubjectsAdaptedfromAgrawalNGBetalJClinPharmacol2003;43:268–276.
1000
EtoricoxibPharmacokineEcs:AbsorpEonandt1/2*

Tmax(hour) t1/2(hour)
Etoricoxib 1 22
Celecoxib 2–3 8–12
Diclofenac 1–5.25 2
Ibuprofen 0.75–1.5 2
Meloxicam 4–5 20
Naproxen 2–4 12–17
Indomethacin 2 4.5
Nimesulide 2–3 2–5
Tmax=EmetomaximumplasmaconcentraEon
Etoricoxib:Tmaxandt1/2

12-W
eekcumulaE
ve
incide
ncerate(%
)a
aCumulaEveincidencerateofgastroduodenalulcers≥3mmatweek12.CumulaEveincidenceratefromlife-tableanalysismaynotequalnumberofevents/n×100;bp<0.001foretoricoxibandplacebovs.naproxen;cp<0.001forplacebovs.ibuprofen;dp=0.007foretoricoxibvs.ibuprofen;e500mgtwicedaily;f800mgthreeEmesdailyHuntRHetalAlimentPharmacolTher2003;17:201–210;HuntRHetalAmJGastroenterol2003;98:1725–1733.
Etoricoxib120mg(n=207)
Naproxen1000mge(n=164)
Etoricoxib120mg(n=186)
Ibuprofen2400mgf(n=181)
Placebo(n=207)
0
RAorOA
510152025
3530
7.42b
25.27
1.35b
OA
0
5
10
15
20
25
8.12d
17.02
1.86c
Placebo(n=203)
Study1 Study2
Althoughthestudieswerenotdesignedtocompareulcerratesofplacebowithetoricoxib,subsequentanalysisrevealedsignificantdifferencesinStudy1(p=0.002)andStudy2(p=0.003).2,3
Etoricoxibvs.NaproxenorIbuprofenEndoscopyStudies:Gastro-duodenalUlcers

NSAIDs=nonsteroidalanE-inflammatorydrugs;PUBs=perforaEons,ulcers,bleeds*Combinedanalysisof10clinicaltrialsinOA,RA,andchroniclowbackpain;**Naproxen1000mg/day,ibuprofen2400mg/day,ordiclofenac150mg/dayAdaptedfromHuntRHetalAmJGastroenterol2003;98:1725–1733;CurEsSetal.PosterpresentedatEULAR,2002.
CumulaE
veincide
nce
Days(acEvetreatmentperiod)
0 90 180 270 360 540
0.02
0.04
0.06
0.00
Etoricoxib≥60mg(n=3142)NonselecEveNSAIDscombined**(n=1828)
p<0.001
~55%Risk
reducEon
450
Etoricoxibvs.NonselecEveNSAIDs:GIPUBsEtoricoxibhadlowerincidenceofconfirmedPUBsintheclinicaldevelopmentprogram*

AcuteGoutyArthritisTrialsDrug No.ofpaEents Year
Indomethacinvs.phenylbutazone 28 1973Proquazonevs.indomethacin 18 1978Sulindacvs.phenylbutazone 47 1979Fenoprofenvs.phenylbutazone 30 1979Feprazonevs.phenylbutazone 24 1980Meclofenamatevs.indomethacin 20 1983Flurbiprofenvs.phenylbutazone 33 1985Flurbiprofenvs.indomethacin 29 1986Indomethacin+allopurinolvs.azapropazone 93 1987Tenoxicam 10 1987Colchicinevs.placebo 43 1987Ketoprofenvs.indomethacin 59 1988Etodolacvs.naproxen 60 1990Etodolacvs.naproxen 61 1991Etoricoxibvs.indomethacin 150 2002Etoricoxibvs.indomethacin 189 2004*Listincludesonlydouble-blindclinicalstudiesoforalagentsbasedonextensiveEnglish-languageMedlineliteraturesearch(drugnamesand*gout assearchterms;nolimitonyearofpublicaEon;accessedJanuary2004).Allpublisheddouble-blindclinicalstudiesmaynotbeincluded.

ìCardiovascularrisk??

Coxib,tradiEonalNTC,etal.Lancet.2013;382(9894):769-79..

Coxib,tradiEonalNTC,etal.Lancet.2013;382(9894):769-79..
• Meta-analysis• 280trials• 124513pateints• 68342paEentyears• ibuprofen=diclofenac=coxibs• Naproxenassociatedlessvascularevents.

Coxib,tradiEonalNTC,etal.Lancet.2013;382(9894):769-79..
BavryAA,etall.Circu
laEonCardiovascular
qualityandoutcomes.2014;7
(4):603-10.


ChronicNSAIDuseininflammatoryconditions.
ì ConEnuousNSAIDsfor30years
ì Overallmortalityrisk14.2%(Cardiovasculardisease=40%).
ì BUT
ì ConEnuousNSAIDsreducedCVSmortality.AnnRheumDis2011;70(11):1921

CelestoneIASvs.IMI
ì Highlyfatsoluble
ì Crossallcellmembranesrapidly.
ì SystemicallyavailablewithinafewminutesauerinjecEon.
ì Youdon’thavetoinjectlocally.
ì Intra-muscular(IM)injecEonsarealsoveryeffecEve.
ì BenefitofalocalinjecEonismainly‘duraEonofsymptomrelief’.
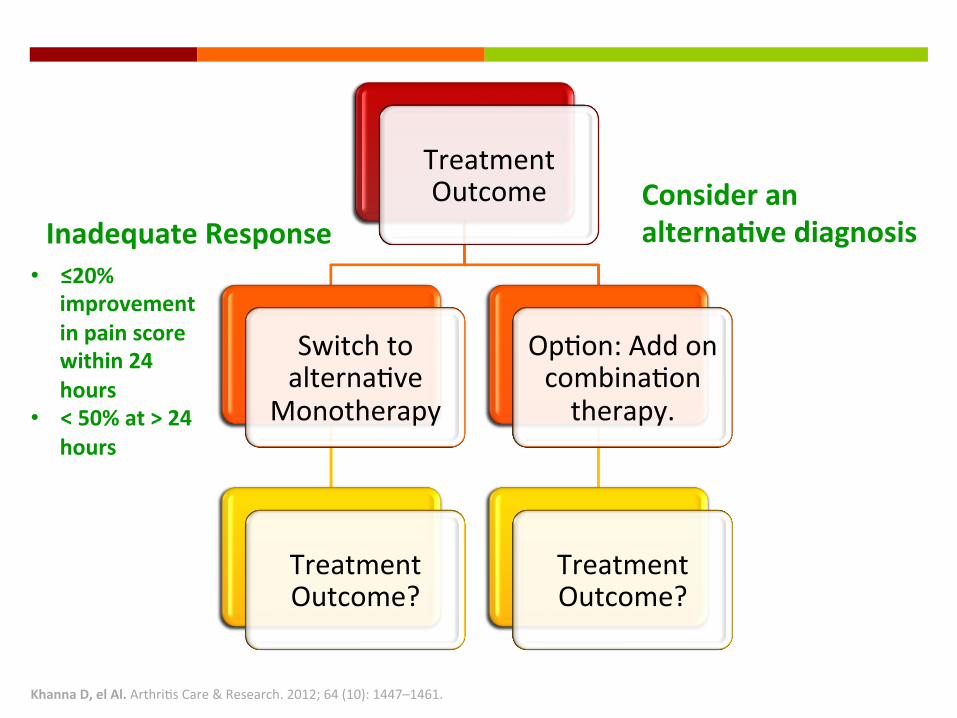
KhannaD,elAl.ArthriEsCare&Research.2012;64(10):1447–1461.
TreatmentOutcome
SwitchtoalternaEve
Monotherapy
TreatmentOutcome?
OpEon:AddoncombinaEontherapy.
TreatmentOutcome?
InadequateResponseConsideranalternaEvediagnosis
• ≤20%improvementinpainscorewithin24hours
• <50%at>24hours
ExperimentalDrugsforanAcuteAttack
ì TherapiestargeEngIL-1bblockagearecurrentlybeinginvesEgated.
ì Theseinclude:ì Anakinra(anIL-1receptorantagonist),ì Rilonacept(asolublereceptor-Fcfusionproteinthat
engagesandinhibitsbothIL-1aandIL-1bì Canakinumab(afullyhumanmonoclonalanE-IL-1b
anEbody).
HarroldL.,CurOpinRheumatol20133;25(3).304-309.


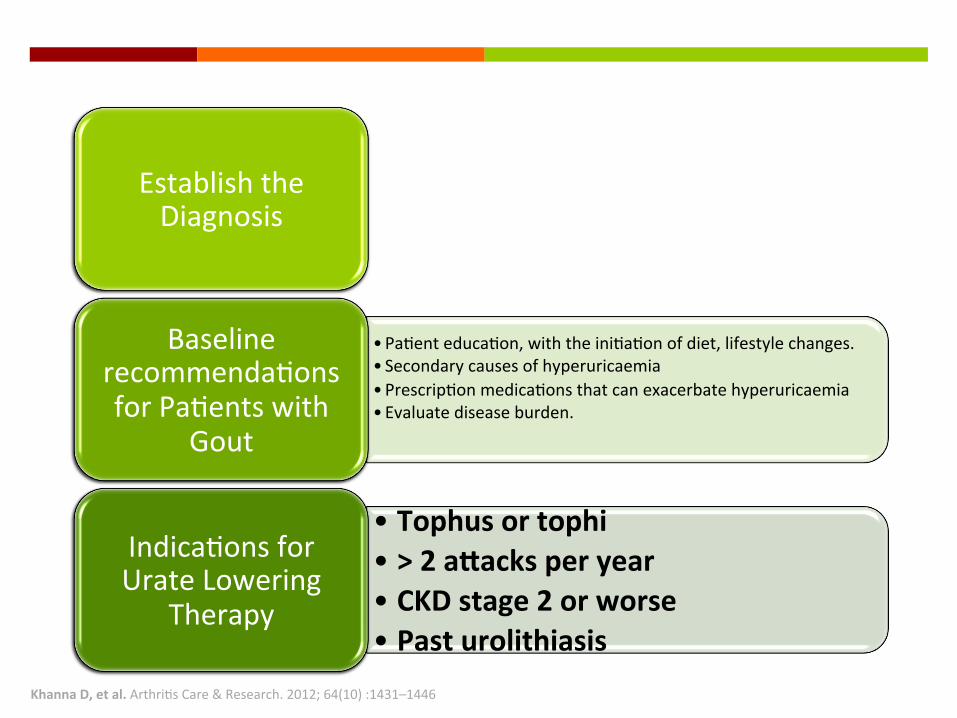
KhannaD,etal.ArthriEsCare&Research.2012;64(10):1431–1446
KhannaD,etal.ArthriEsCare&Research.2012;64(10):1431–1446
EstablishtheDiagnosis
• PaEenteducaEon,withtheiniEaEonofdiet,lifestylechanges.• Secondarycausesofhyperuricaemia• PrescripEonmedicaEonsthatcanexacerbatehyperuricaemia• Evaluatediseaseburden.
BaselinerecommendaEonsforPaEentswith
Gout
• Tophusortophi• >2aSacksperyear• CKDstage2orworse• Pasturolithiasis
IndicaEonsforUrateLowering
Therapy

KhannaD,etal.ArthriEsCare&Research.2012;64(10):1431–1446
TREATTOTARGETURICACIDLEVEL
1stLineXanthineOxidaseInhibitor
Allopurinol
Febuxostat
AlternaEve1stLinetherapy Probenecid
AcuteGoutprophylaxis
Colchicine0.5mgBD
NSAID(egArcoxia)
Uricacid≤0.35mmol/L
Allopurinol
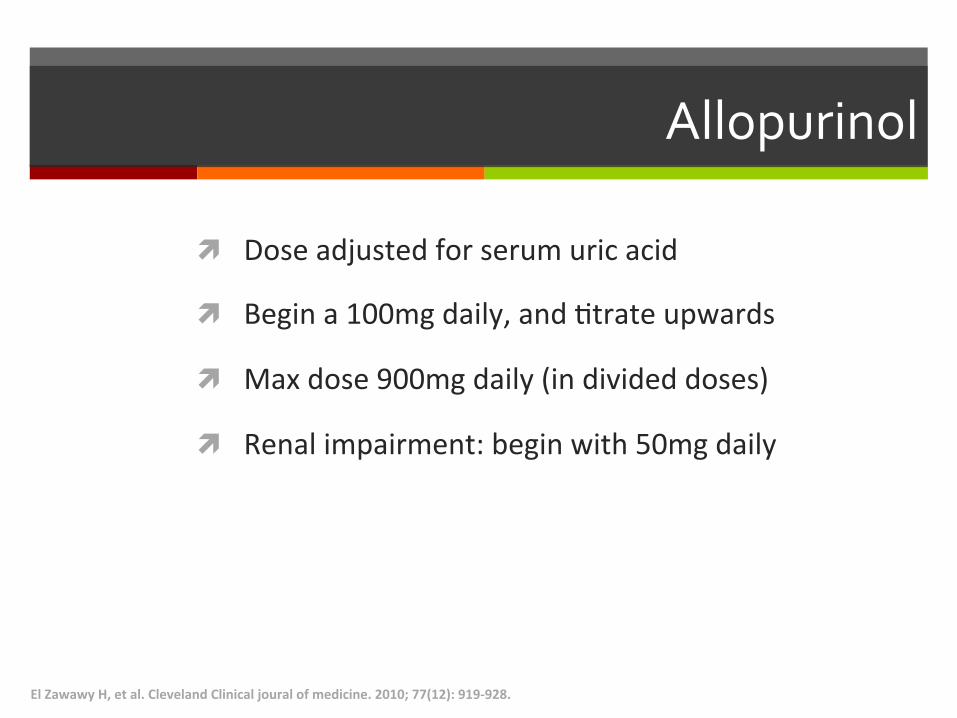
ì Doseadjustedforserumuricacid
ì Begina100mgdaily,andEtrateupwards
ì Maxdose900mgdaily(individeddoses)
ì Renalimpairment:beginwith50mgdaily
ElZawawyH,etal.ClevelandClinicaljouralofmedicine.2010;77(12):919-928.
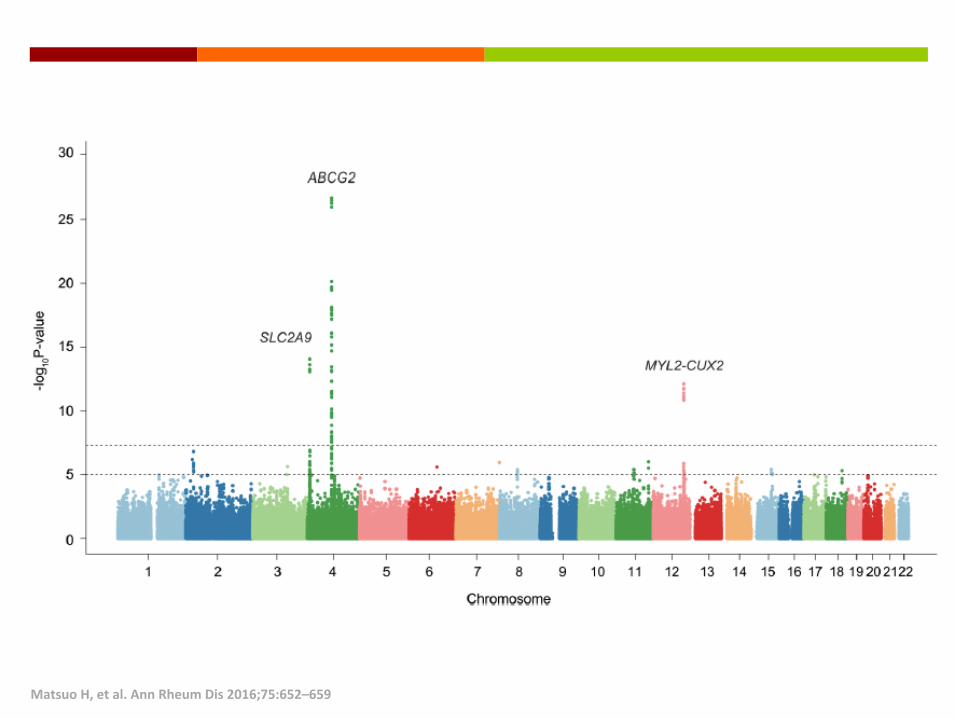
MatsuoH,etal.AnnRheumDis2016;75:652–659

MatsuoH,etal.AnnRheumDis2016;75:652–659

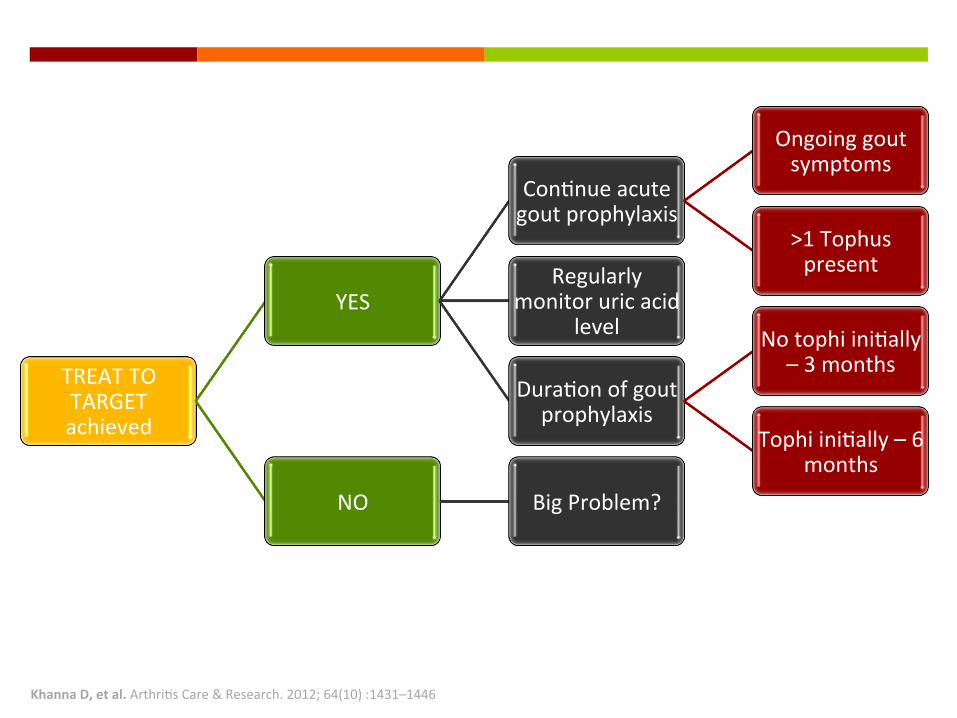
KhannaD,etal.ArthriEsCare&Research.2012;64(10):1431–1446
TREATTOTARGETachieved
YES
ConEnueacutegoutprophylaxis
Ongoinggoutsymptoms
>1TophuspresentRegularly
monitoruricacidlevel
DuraEonofgoutprophylaxis
NotophiiniEally–3months
TophiiniEally–6months
NO BigProblem?
GoutProphylaxis
ì Long-termtreatmentwitheithercolchicineorNSAIDs.
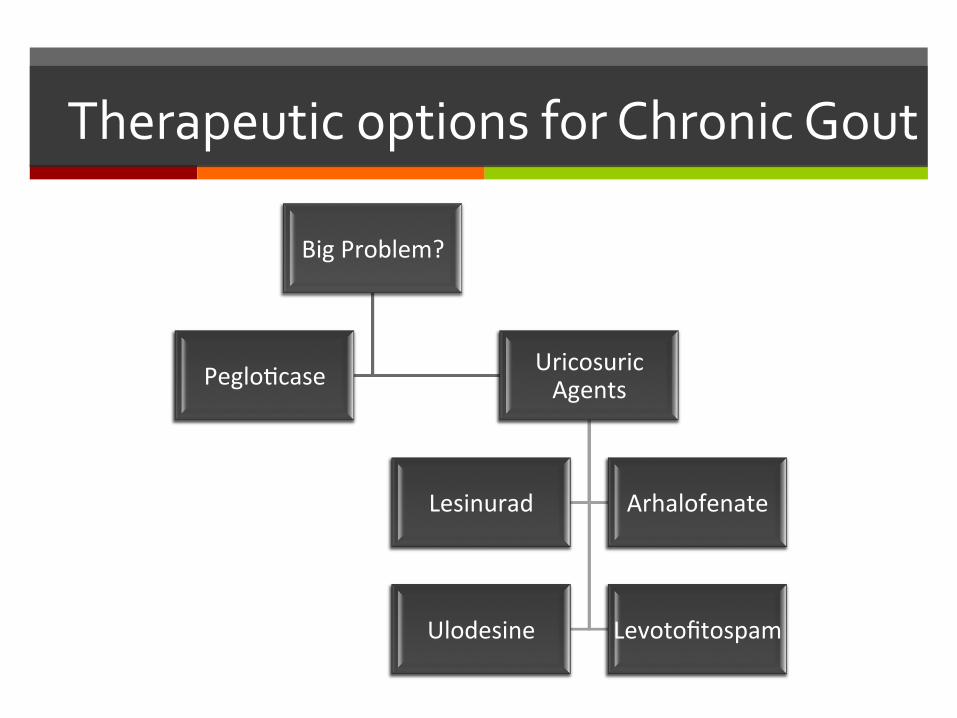
TherapeuticoptionsforChronicGout
BigProblem?
PegloEcase UricosuricAgents
Lesinurad Arhalofenate
Ulodesine Levotofitospam

Reversalofchronicrefractorytophaceousgoutwitherosionswithpegloticase
InternaEonalJournalofRheumaEcDiseases2013;16:369–370

ProgressionofGout
InabaS,etal.Rheumatology2013;52:963-965.
AsymptomaEcHyper-
uricaemiaAcuteAhack
Recurrentahacks
ChronicGout
Uricacidnephro-lithiasis
ChronicNephro-pathy

Study No.ofPaEents RelaEveRiskofHypertension
Hawaii–LosAngeles–Hiroshima,2001
140men 2.0Emesgreaterat15yr(highvs.lowquarEle)
OsakaFactory,2003 433men 1.0mg/dl,increased27mmHgSBPat5yr
OsakaHealthSurvey,2003 2310men 1.13EmesgreaterperSDincrementat6yr
Okinawa,2004 4489men 1.46Emesgreaterformen(uricacid≥7mg/dl)and1.94forwomen(uricacid≥6mg/dl)at13yr
FraminghamHeart,2005 3329adults 1.17EmesgreaterperSDincrementat4yr
NormaEveAging,2006 2062men 125Emesgreaterat21yr(uricacid>6.5mg/dl)
ARIC,2006 9104adults 1.1EmesgreaterperSDincrementat9yr
BeaverDamHealthSurvey,2006
2520adults 1.65Emesgreaterat10yr(highvs.lowquinEle)
MRFIT,2007 3073men 1.1EmesgreaterperSDincrementat6yr

SinghJA.AnnRheumDisApril2015Vol74No4

WeiL,etal.BrJClinPharmacol.2011;71:4600–607.
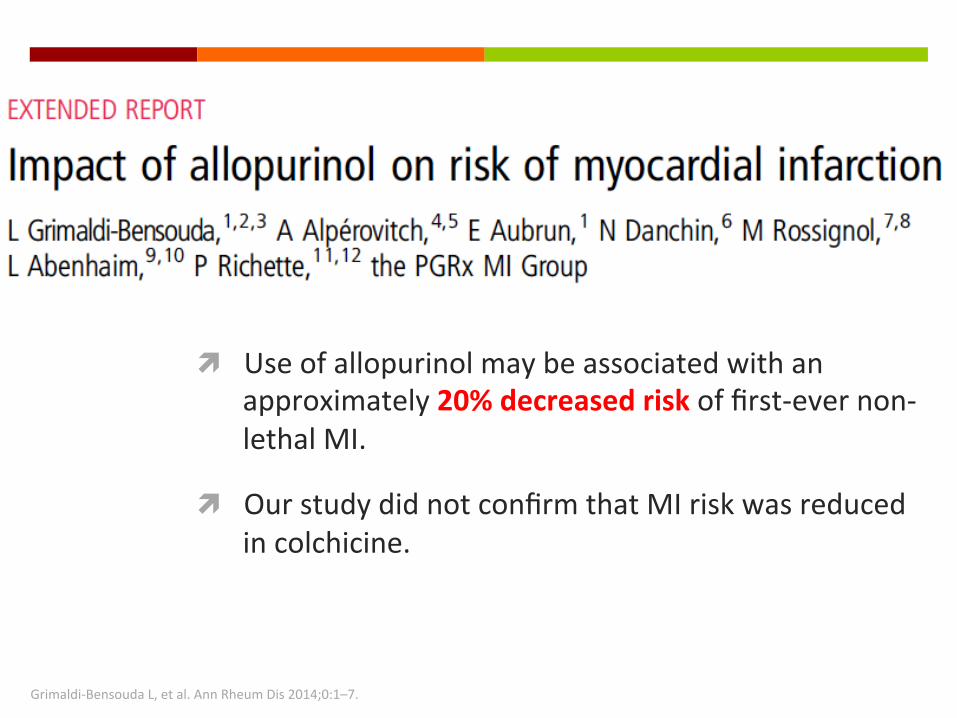
Grimaldi-BensoudaL,etal.AnnRheumDis2014;0:1–7.
ì Useofallopurinolmaybeassociatedwithanapproximately20%decreasedriskoffirst-evernon-lethalMI.
ì OurstudydidnotconfirmthatMIriskwasreducedincolchicine.

ì Gout,althoughcorrelatedwithuricacidandcardiovasculardisease,wasindependentlyassociatedwithtotalandcardiovascularmortality.
ì MortalityimpactofgoutincreasedwithrisinguricacidConcentraEons.
StackA,etal.QJMeddoi:10.1093/qjmed/hct083

OlenaO,etal.Rheumatology2013;52:22512259
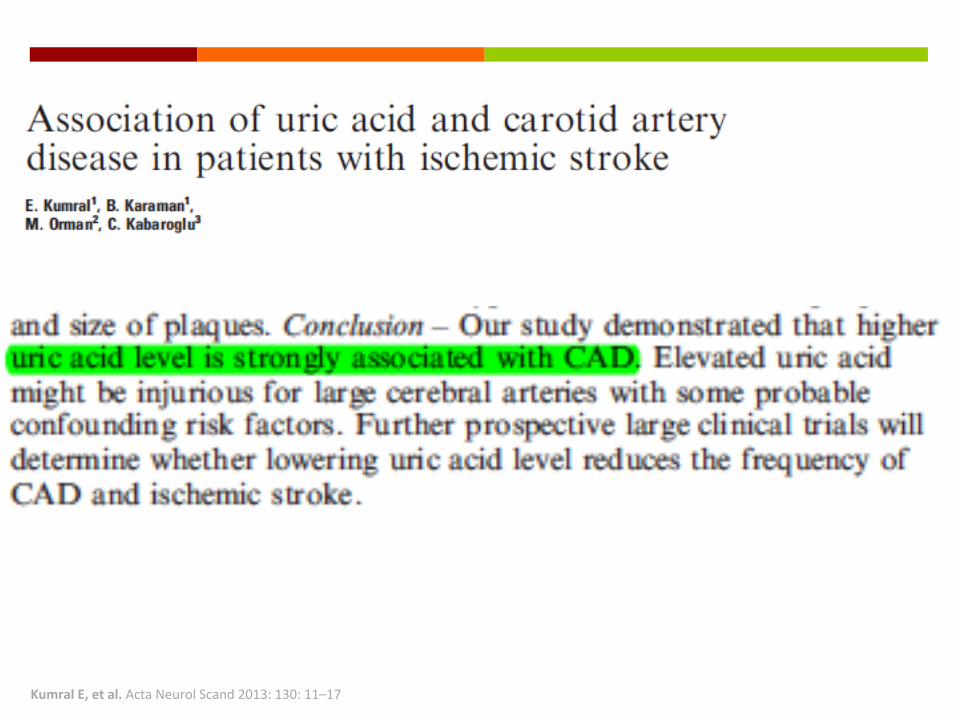
KumralE,etal.ActaNeurolScand2013:130:11–17
AmJCardiol2011;108:1362–1370
• 18%reducedriskofMyocardialInfarcEon• 21%reducedriskfortotalCardio-vasculardisease

Howlowistoolow?
LuN,etal.AnnRheumDis2015;0:1–5.






ìTheEnd–Thankyou