updated interim infection control guidance for 2009 h1n1 influenza cdr arjun srinivasan, md division...
TRANSCRIPT

Updated Interim Infection Control Guidance for 2009 H1N1
InfluenzaCDR Arjun Srinivasan, MD
Division of Healthcare Quality Promotion
David N. Weissman, MDNational Institute for Occupational Safety and Health
The findings and conclusions in this presentation are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention

Note from ONA about this guidance
presented by the CDC The Oregon Dept. of Human Services
infection control guidance for H1N1 is in the process of being updated and may not reflect all of the recommendations made in this presentation by the CDC.
If you have questions about the information presented in this PPT or about Oregon DHS guidance for H1N1 please contact Lynda Enos at [email protected]
L. Enos Nov 5, 2009
Continuing Education Disclaimer
In compliance with continuing education requirements, all presenters must disclose any financial or other relationships with the manufacturers of commercial products, suppliers of commercial services, or commercial supporters as well as any use of unlabeled product(s) or product(s) under investigational use.
CDC, our planners, and our presenters wish to disclose they have no financial interests or other relationships with the manufacturers of commercial products, suppliers of commercial services, or commercial supporters.
Presentations will not include any discussion of the unlabeled use of a product or a product under investigational use with the exception of Dr. Srinivasan’s discussion on the re-use of N-95 respirators that are labeled for single use only. There is no commercial support.

Accrediting Statements
CME: The Centers for Disease Control and Prevention is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. The Centers for Disease Control and Prevention designates this educational activity for a maximum of 1 AMA PRA Category 1 Credit. Physicians should only claim credit commensurate with the extent of their participation in the activity.
CNE: The Centers for Disease Control and Prevention is accredited as a provider of Continuing Nursing Education by the American Nurses Credentialing Center's Commission on Accreditation. This activity provides 1 contact hour.
CEU: The CDC has been approved as an Authorized Provider by the International Association for Continuing Education and Training (IACET), 8405 Greensboro Drive, Suite 800, McLean, VA 22102. The CDC is authorized by IACET to offer 0.1 CEU's for this program.
CECH: The Centers for Disease Control and Prevention is a designated provider of continuing education contact hours (CECH) in health education by the National Commission for Health Education Credentialing, Inc. This program is a designated event for the CHES to receive 1 Category I contact hour in health education, CDC provider number GA0082.
Overview
Guidance released on 10/14/2009 replaces previous infection control guidance.
Applies to all settings where healthcare is delivered.
Applies uniquely to the 2009 H1N1 pandemic- not meant to establish new infection control policies for influenza.
Will be updated as needed as new information becomes available.

Key Difference From Previous Guidance
Increased emphasis on the importance of a multi-faceted approach.
Revised exclusion time period for healthcare personnel (HCP) with H1N1
Changes to isolation precautions Updated and expanded discussion on
respiratory protection

Where and To Whom Does This Guidance Apply?
Guidance applies to any healthcare personnel, defined broadly as “all persons whose occupational activities involve contact with patients or contaminated material”.– Includes non-employees like volunteers, contractors,
students, clergy etc. Applies in any setting where care is delivered:
acute care, long-term care, home care, outpatient care, school clinics etc.

For Which Patients Should this Guidance be Used?
For all patients with confirmed or suspected H1N1 influenza infection.
Because the symptoms are non-specific and because testing for H1N1 infection may be limited, this guidance may be applicable for all patients with respiratory illness.

Modes of 2009 H1N1 Influenza Transmission
Contact- usually of hands with an infectious patient or fomite, followed by self-inoculation onto mucosal surfaces.
Droplet exposure of mucosal surfaces Small particle aerosols in vicinity of an
infectious individual.
Review and Update Pandemic Plans
Facilities should review their pandemic influenza plans in light of the current situation and review implementation considerations.– Resource allocation– Staffing– Surge capacity
Pandemic plan checklists are available at www.pandemicflu.gov.
Implement a Multi-Faceted Infection Control Approach
Facilities should employ a variety of complimentary infection control strategies, referred to as a “hierarchy of controls”.
Groups interventions into categories, based on their effectiveness.

Hierarchy of Controls
1. Eliminate exposures
2. Engineering controls
3. Administrative controls
4. Personal protective equipment

Eliminate Exposures
Minimize outpatient visits for patients with mild respiratory illness.
Postpone elective visits/procedures for patients with respiratory illness.
When possible, exclude ill visitors to facilities.

Engineering Controls
Do not depend on implementation by HCP.
Using partitions in triage and patient care areas to reduce potential exposures.
Using Plexiglas barriers in triage/intake areas.

Administrative Controls
Depend on consistent implementation by management and HCP
Vaccination Respiratory hygiene/cough etiquette Enforcing exclusion of ill HCP

Personal Protective Equipment (PPE)
Dependent on consistent use of PPE whenever exposures occur, technique, and properly functioning equipment.
HCP must be trained on proper use of PPE- both when and how.

Specific Recommendations

Vaccination
Promote and administer both the 2009 seasonal and H1N1 vaccines.
HCP are a high priority group for vaccination.
Where H1N1 vaccine supplies are limited, priority should go to HCP who are most likely to be exposed to infectious patients and those who are at high risk for complications from H1N1 infection.

Vaccination- Live Attenuated Vaccine and HCP
Live attenuated vaccine can be used in HCP who:– Meet labeling eligibility criteria– Do not work with severely immune
compromised patients in protective environments (bone marrow transplant).
LAIV can be used for HCP working with less immune suppressed patients and HCP working in NICUs.

Enforce Respiratory Hygiene/Cough Etiquette
Source control is critical in reducing exposure risks.
Should apply in all triage and waiting areas.
Should also apply even after patients are admitted to facilities.

Establish Access Control and Triage Measures
Establish non-punitive policies to ensure ill HCP do not come to work.
Establish mechanisms to identify patients and visitors with respiratory illness at entry points to the facility.
Design triage/waiting areas to minimize exposure risks (e.g. spacing of patients, partitions).

Manage Visitor Access and Movement
Limit visitors for patients in isolation for influenza.
Instruct visitors to limit movement within the facility.
Ensure visitors are not present during aerosol generating procedures.

Patient Placement and Transport
Instruct ill patients on source control measures- covering mouth and nose, hand hygiene.
Place into a private room with door closed (negative pressure room not needed).– Consult infection control if private rooms are
not available. Transport within facilities should follow
current facility guidance– Limit transport to medically necessary– Ensure communication with receiving areas
Isolation Precautions
Limit the number of HCP entering isolation rooms to those necessary for providing care.
Instruct HCP on the importance of hand hygiene before and after patient interactions.
Use standard precautions for all patient interactions- wear gowns, gloves, eye protection if splashes/contact with infectious material anticipated.

Duration of Isolation Precautions for Patients
Patients with suspected or confirmed H1N1 influenza should remain in isolation for 7 days after the onset of symptoms or until 24 hours after resolution of symptoms, whichever is longer.– Clinical judgment required for cough
If isolation resources are limited, priority should be given to patients earlier in course of illness.

Environmental Cleaning
Routine cleaning and disinfection strategies normally used during influenza season should be used.
Includes management of laundry, utensils and medical waste.

Respiratory Protection
Views of aerosol transmission Does respiratory protection prevent
transmission in healthcare settings? CDC respiratory protection
recommendation Respiratory protection supply
considerations
- Outline of Topics -

Views of Aerosol Transmission Traditional view of viral aerosol transmission: airborne
(small particle) vs. large droplet More contemporary view: viral aerosol transmission
can be characterized along a continuum as obligate, preferential, or opportunistic, depending on an agent’s ability to be transmitted and induce disease through fine particle aerosols and other routes (Roy & Milton. NEJM 2004)
Studies on influenza transmission show that airborne (inhalation) transmission is one of the potential routes of transmission [Institute of Medicine (IOM) 2009] http://www.nap.edu/catalog.php?record_id=12748#description

Does respiratory protection prevent transmission in healthcare settings?
Even if an intervention is efficacious, it may not be effective
Although it recommended respiratory protection as a preventive intervention, IOM noted the need for effectiveness research (IOM 2009)
An important randomized, controlled study comparing incidence of influenza in Canadian nurses using surgical masks or N95 respirators has recently been published [Loeb M et al. JAMA. 2009 Oct 1. (Epub ahead of print)]

Facemasks and disposable N95 respirators
A facemask is a loose-fitting, disposable device. Facemasks may be labeled as surgical, laser, isolation, dental or medical procedure masks and help block large-particle droplets, splashes, sprays or splatter
A disposable N95 respirator is a respiratory protective device designed to achieve a very close facial fit and very efficient filtration of airborne particles. In addition to blocking splashes, sprays and large droplets, the respirator is also designed to prevent the wearer from breathing in very small particles that may be in the air. Text excerpted from: http://www.fda.gov

Results: Surgical Mask vs. N95
SurgicalMask (n = 212)
N 95(n=210)
p value(reported)
Lab Results
Any Lab Diagnosis of Influenza 50 48 0.86
4-fold rise in serum antibody titers 44 44 -
(+) PCR study of resp. secretions 6 4 -
Clinical Illness
Influenza-like illness (cough and temp > 38oC
9 2 0.06
Nurses reporting “fever” 12 2 0.007
Home Exposure
Spouses or Roommates with flu-like illness
55 47 0.39
Children with flu-like illness 48 43 0.59
Loeb M et al. JAMA. 2009 Oct 1. [Epub ahead of print]
Summary 4-fold rise in serum antibody titers was common, rarely
associated with symptoms, and not different between study arms– If asymptomatic influenza is common in nurses, it
might have important implications for infection control Clinical illness was rare and tended to be less frequent in
the N95 group– Lab and clinical findings were not consistent. Small
numbers make clinical outcomes difficult to interpret More studies are needed with better power to address
clinical illness as an outcome As more studies become available, it will be possible to
assess coherence of results across multiple studies and to pool data from multiple studies for meta-analysis
Loeb M et al. JAMA. 2009 Oct 1. [Epub ahead of print]

CDC Respiratory Protection Recommendation
Use of respiratory protection that is at least as protective as a fit-tested disposable N95 respirator for healthcare personnel who are in close contact with patients with suspected or confirmed 2009 H1N1 influenza.
Close contact is defined as working within 6 feet of the patient or entering into a small enclosed airspace shared with the patient (e.g., average patient room).
This recommendation applies uniquely to the special circumstances of the current 2009 H1N1 pandemic during the fall and winter of 2009-2010.

Required Respirator Program ElementsRequired Respirator Program Elements
Written standard operating procedures that include: Permissible practices for respirator use. Respiratory program administration. Respirator selection. Inspection of respirators. Cleaning and maintenance of respirators. Storage of respirators. Training in respiratory protection. Fit testing of respirators. Respirator program evaluation. Medical Surveillance of respirator users.
Excellent Resource: OSHA respiratory protection e-tool: http://www.osha.gov/SLTC/etools/respiratory/

Respiratory Protection Supply Considerations
The updated guidelines recognize supply issues and provide strategies for getting the most benefit from available supplies of respiratory protection.
Highest priority: to ensure that respirators remain available for situations where respiratory protection is most important, such as performance of aerosol-generating procedures on patients with suspected or confirmed 2009 H1N1 flu or provision of care to patients with diseases other than influenza that require respiratory protection, such as TB.

Strategies to Conserve Supplies of Disposable N95 Respirators
Minimize the number of individuals who need to use respiratory protection through the use of engineering and administrative controls;
Use alternatives to disposable N95 respirators where feasible;
Extend the use, and consider reuse of disposable N95 respirators; and
Prioritize the use of N95 respirators for those personnel at highest risk of exposure.
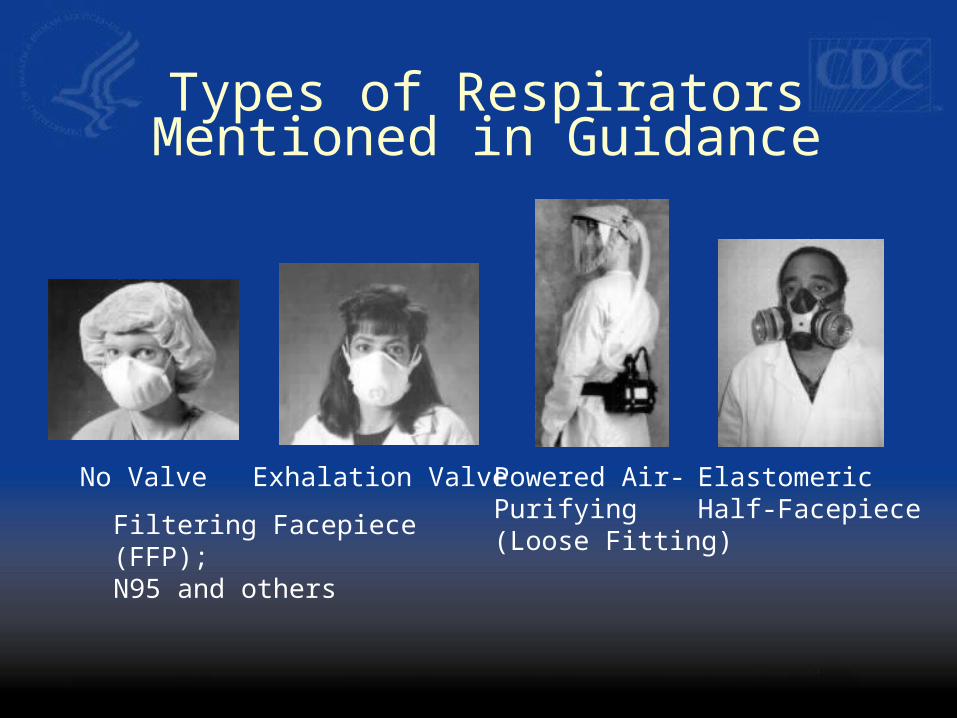
Types of Respirators Mentioned in Guidance
Filtering Facepiece (FFP);N95 and others
No Valve Exhalation Valve Powered Air-Purifying(Loose Fitting)
ElastomericHalf-Facepiece

Filtering Facepiece(FFP) Respirators
Class Description
N95 Filters at least 95% of airborne particles. Not resistant to oil.
N99 Filters at least 99% of airborne particles. Not resistant to oil.
N100 Filters at least 99.97% of airborne particles. Not resistant to oil.
R95 Filters at least 95% of airborne particles. Somewhat resistant to oil.
P95 Filters at least 95% of airborne particles. Strongly resistant to oil.
P99 Filters at least 99% of airborne particles. Strongly resistant to oil.
P100 Filters at least 99.97% of airborne particles. Strongly resistant to oil.

“Extended Use” of Disposable N95 Respirators
Definition: wearing disposable N95 respirators over serial patient encounters, without removal and re-donning between encounters.
Steps to minimize risk of contact transmission– Discard disposable N95 respirators following use during
aerosol generating procedures. – Discard disposable N95 respirators if contaminated with
blood, respiratory secretions, or other bodily fluids from patients.
– Consider use of a face shield over the disposable N95 respirator to prevent surface contamination.
– Perform hand hygiene before and after touching the respirator.

“Reuse” of Disposable N95 Respirators
Definition: removing and re-donning disposable N95 respirators between patient encounters
Involves more touching of the respirator and the face than extended use
Steps to minimize risk of contact transmission– All of those noted for extended use, plus:– Disposable respirators must only be used and re-used
by a single wearer. – Do not re-use a disposable respirator that is obviously
contaminated, damaged or hard to breathe through.– Store the respirator in a clean, breathable container such
as a paper bag between uses. – Avoid touching the inside of the respirator.
Prioritized Use Mode Used when measures to minimize consumption of
available respirators are not enough to overcome supply shortages and the ability to provide respiratory protection for situations where it is most important (e.g., aerosol-generating procedures, other agents such as TB) is threatened.
Goal is to maintain ability to provide respiratory protection for situations where it is most important until supplies are expected to be replenished.
Respiratory protection is extended to other groups in order of priority, as dictated by supply constraints.
Those in close contact with suspected or confirmed influenza cases who do not receive respiratory protection should be provided with surgical masks.

(Numbers 1 through 4 indicate relative priorities for respiratory protection, with 1 the highest priority and 4 the lowest priority)
Exposure Scenario Not Vaccinated Vaccinated
Personnel Without Risk Factors for Influenza-Related Complications
Routine care – frequent close exposure 2 4
Routine care – infrequent close exposure 3 4
Personnel With Risk Factors for Influenza-Related Complications
Routine care – frequent close exposure 1 3
Routine care – infrequent close exposure 2 4
Prioritization of Respiratory Protection During Respirator Shortages for Healthcare
Personnel Not Participating in Aerosol-Generating Procedures

Aerosol-Generating Procedures
Bronchoscopy Sputum induction Endotracheal intubation and
extubation Open suctioning of airways Cardiopulmonary resuscitation Autopsies

Monitoring for Illness in HCP
Facilities should establish mechanisms to proactively identify ill HCP and monitor illness in HCP.– Self monitoring or active symptom surveillance
HCP should be instructed not to report to work when ill.
HCP should be educated on when to seek treatment when ill.
Exclusion of HCP with Respiratory Illness
HCP who develop febrile respiratory illness should be excluded from work for at least 24 hours after they no longer have a fever, without the use of fever reducing medicines.
Exception: HCP who work with severely immune compromised patients.
Exclusion of HCP with Respiratory Illness
HCP who develop acute respiratory symptoms without fever should be allowed to continue or return to work.
Exception: HCP who work with severely immune compromised patients.

Exclusion of HCP with Respiratory Illness
HCP who work with immune compromised patients should be excluded for 7 days or until resolution of symptoms, whichever is longer.– Judgment required for cough as a
symptom– Could return to work sooner if absence of
H1N1 influenza documented by PCR of respiratory secretions.

Antiviral Treatment and Chemoprophylaxis
Recommendations available in a separate guidance document that does address HCP.

Thank You

Continuing Education Credit/Contact Hours for COCA Conference Calls
Continuing Education guidelines require that the attendance of all who participate in COCA Conference Calls be properly documented. ALL Continuing Education credits/contact hours (CME, CNE, CEU and CECH) for COCA Conference Calls are issued online through the CDC Training & Continuing Education Online system http://www2a.cdc.gov/TCEOnline/.
Those who participate in the COCA Conference Calls and who wish to receive CE credit/contact hours and will complete the online evaluation by November 29, 2009 will use the course code EC1265. Those who wish to receive CE credits/contact hours and will complete the online evaluation between November 30, 2009 and October 30, 2010 will use course code WD1265. CE certificates can be printed immediately upon completion of your online evaluation. A cumulative transcript of all CDC/ATSDR CE’s obtained through the CDC Training & Continuing Education Online System will be maintained for each user.