update on health informatics in the uk - soqibs · health informatics update on health informatics...
TRANSCRIPT

Yorkshire Centre for
Health Informatics
Update on Health Informatics in the UK
Dr Rick Jones
12th June 2013

Outline
• Historic Context
– What went wrong with the National Programme for IT
– What went right
• What is happening regarding:
– Scalability
– Standardisation
– Interoperability
• The Research Opportunities
– CPRD
– ResearchOne

National Audit Report – June 2013
• In a note for the Commons’ Public Accounts Committee, the NAO says that 98% of estimated benefits of the London
Programme for IT, the South Programme for IT and the
Electronic Prescription Service and Summary Care Record programme, were still to be realised at March 2012.
• The note, which reports on a much-delayed review of the benefits of the programme demanded by the PAC when it
investigated NPfIT in August 2011, says that in March 2012, the DH put the total cost of the programme at £7.3 billion
with total benefits at that point at £3.7 billion.
• It estimated that by the end of the programme (between
2016 and 2024), the total costs would be £9.8 billion and
the benefits £10.7 billion.

Historic Context
October 2002
April 2005
September 1998January 2001
June 2002
April 2013June 2012

Pro
vid
e P
rescriptions
Serv
ice
Build
Life-long H
ealth
Record
Serv
ice
Pro
vid
e B
ookin
gs
Serv
ice
Pervasive national electronic infrastructure (N3)
2002
1994
1998
IM&T Strategy for the NHS
What went wrong?
Programme Scope - 2002

100%
50%
Daily
usage
Pro
vid
e P
rescrip
tio
ns S
erv
ice
Pro
vid
e B
oo
kin
gs S
erv
ice
Bu
ild L
ife
-lon
g H
ealth
Re
co
rd S
erv
ice
Pa
tien
t C
ho
ice
Dig
ita
l Im
agin
g
NH
S N
um
be
rs f
or
Ba
bie
s
Se
cond
ary
Use
s S
erv
ice
NH
S E
ma
il S
yste
m
Tra
nsfe
r of
reco
rds b
etw
een
G
Ps
Qu
alit
y M
ana
gem
en
t
Ana
lysis
Syste
m
Bo
we
l C
an
ce
r S
cre
enin
g
Pervasive national electronic infrastructure (N3)
0% 0%
100%
50%
Pro
gre
ss
Pro
gre
ss
1.4m
prescriptions
43,000 bookings
4.2m
enquiries
43,000 bookings
2m new images
2m new records
5m
messages
5,000
transfers
£750,000 paid
1,850 babies registered
8,000 screenings
Daily
usage
Original Scope Additional ScopeKey:
Commissioning Payment by Results Plurality of provision
What went wrong?
Programme Scope in 2010

Implementation disaster
• Working with suppliers to implement new systems and services in planned phases
• National Application Service Providers are responsible for purchasing and integrating IT systems common to all users nationally
• Local Service Providers (LSPs) will deliver IT systems and services on a local level for regional clusters of strategic health authorities
• LSPs supply and integrate systems to perform functions in the local setting and to interface with the national system
Accenture bailed
out 2006 - £1bn
loss
CSCA failed to
deliver Lorenzo
2006 - 2012
Accenture bailed
out 2006 - £1bn
loss
CSCA failed to
deliver Lorenzo
2006 - 2012
Fujitsu IDX out 2008
Cerner struggling in
South
Fujitsu IDX out 2008
Cerner struggling in
South
London chaotic
& competitive
London chaotic
& competitive
Big corporates failed to recognise
Healthcare vs Industry differences
Differences
• Management
– Unified in most sectors, but health care has clinical and operational reporting.
• Customer
– Clear customer in most sectors, but health care involves variety, including clinicians, payors, government, service providers, and users.
• Variants
– Few industries exceed tens of thousands of variants. Health care typically caters to many tens of millions of individuals.
• Preference and choice
– Most industrial systems have hard metrics. In health care, people’s feelings and choices matter, too.
Similarities
• Process orientation
– All sectors seek improvement in quality, cost,and delay through integrated processes.
• Center of attention
– Health care is becoming patient-centered, following product-centered and customer centered success in other sectors.
• System integration
– Although health care systems are typically larger, more complex, and employ more people than other systems, they still benefit
Avison & Young, TIME TO RETHINKHEALTH CARE AND ICT? COMMUNICATIONS OF THE ACM June 2007/Vol. 50, No. 6

Why is healthcare difficult?
Multiple non-co-terminosity?
HB
A&C HB GGHB
HB
HB

Multiple non-co-terminosity…for the patient’s record
Primary Care
Secondary Care
Community Care
Tertiary Care
Geography
Patients’ records
(on an EPR?)

Lack of insight:
Development Scale
• Group
intercommunication
formula: n(n − 1) / 2
• Example: 50
developers give 50 ·
(50 – 1) / 2 = 1225
channels of
communication.

Outline
• Historic Context
– What went wrong with the National Programme for IT
– What went right
• What is happening regarding:
– Scalability
– Standardisation
– Interoperability
• The Research Opportunities
– CPRD
– ResearchOne
Despite this many things have been
achieved:
• Universal electronic primary care record
• CPOE now common place
• PACs universally delivered
• National Summary Care Record on 50% of population
(25,512,399 citizens)
• Expanded access to knowledge and information e.g. MapOf
Medicine.
• Nascent patient access to their own records
• etc

New Coalition Government
May 2010
• By July published NHS White Paper
• Fundamental changes to NHS structure and processes
building on previous reforms
• Focus on patient information, choices and outcomes
• Predicated on interoperable information systems
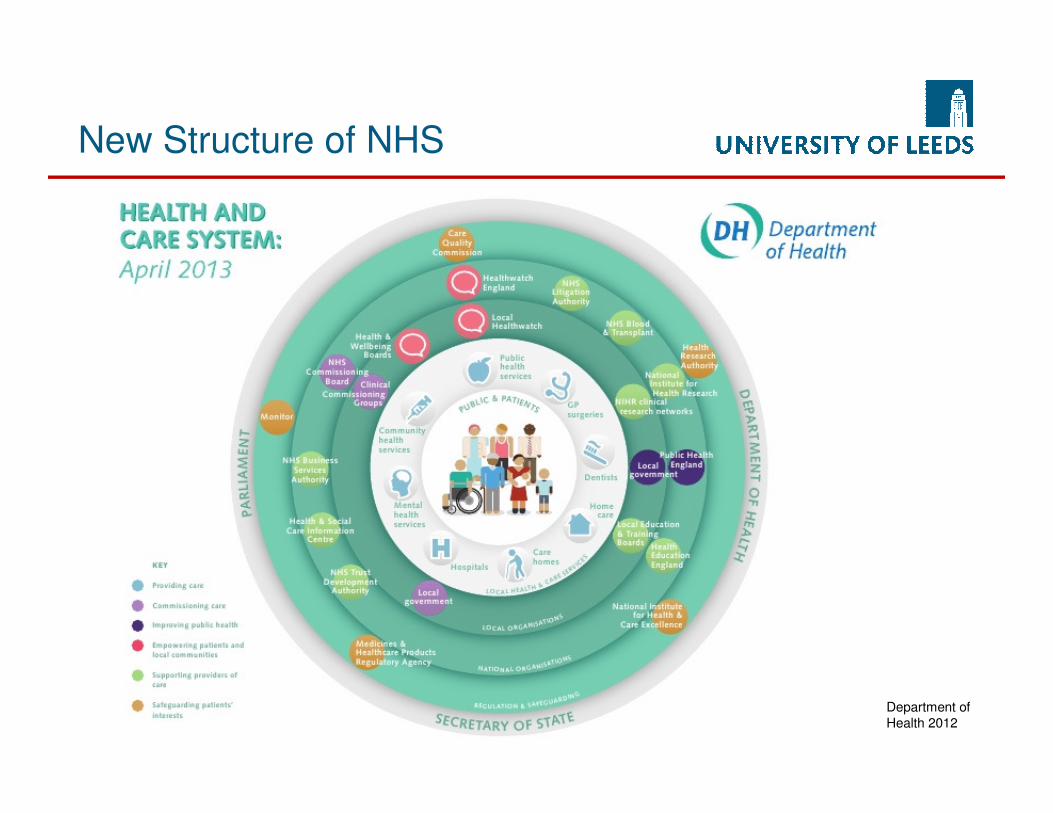
New Structure of NHS
Department of
Health 2012

Consistent with 2009 change of
plan: NHS ‘App Store’
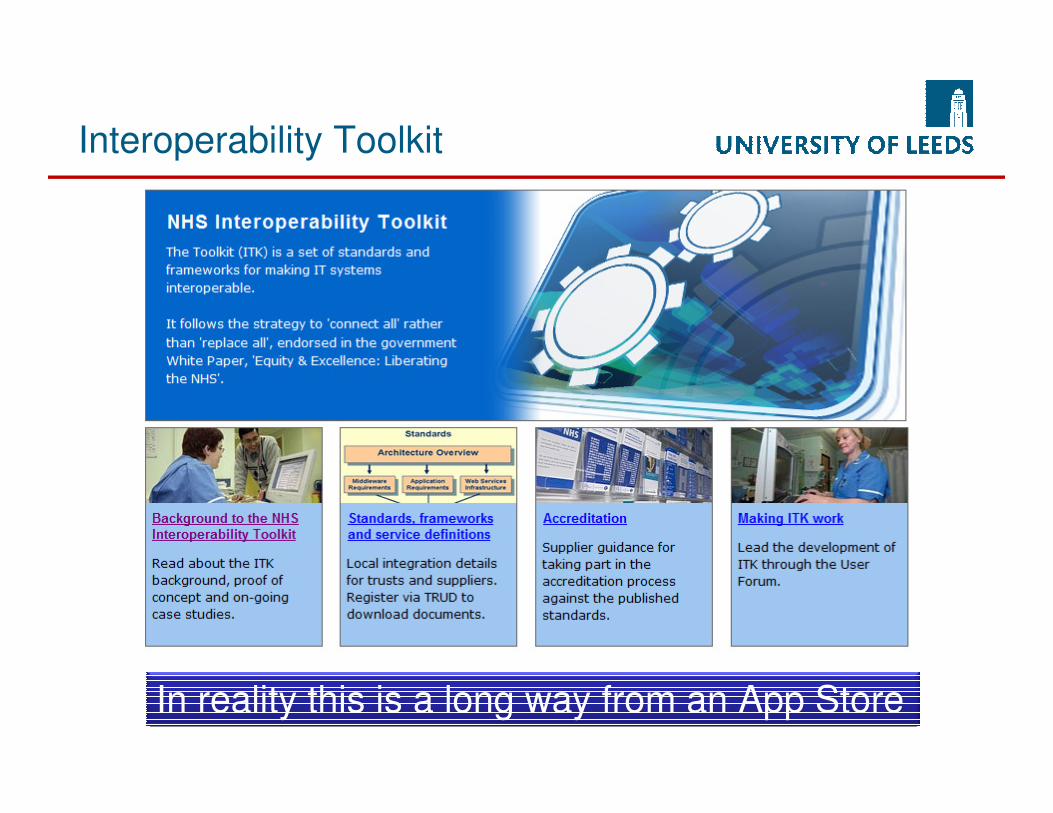
Interoperability Toolkit
In reality this is a long way from an App Store

Example: National Laboratory
Medicine Catalogue
www.laboratorymedicine.nhs.uk
What is in NLMC model
• Fully specified test request name
• Test Display name
• Alternate names
• Valid collected specimen type
• Patient pre-conditions
• Attributes that indicate
topography, laterality
and/or morphology
• Additional information to
ensure appropriate test
• Method of Collection
• Analysed specimen types
• Principle of analysis
• Units of Measurement
• Reference Ranges
• SNOMED CT coding of
content.
• Can consume LOINC
• Links to decision support materials and care
pathways
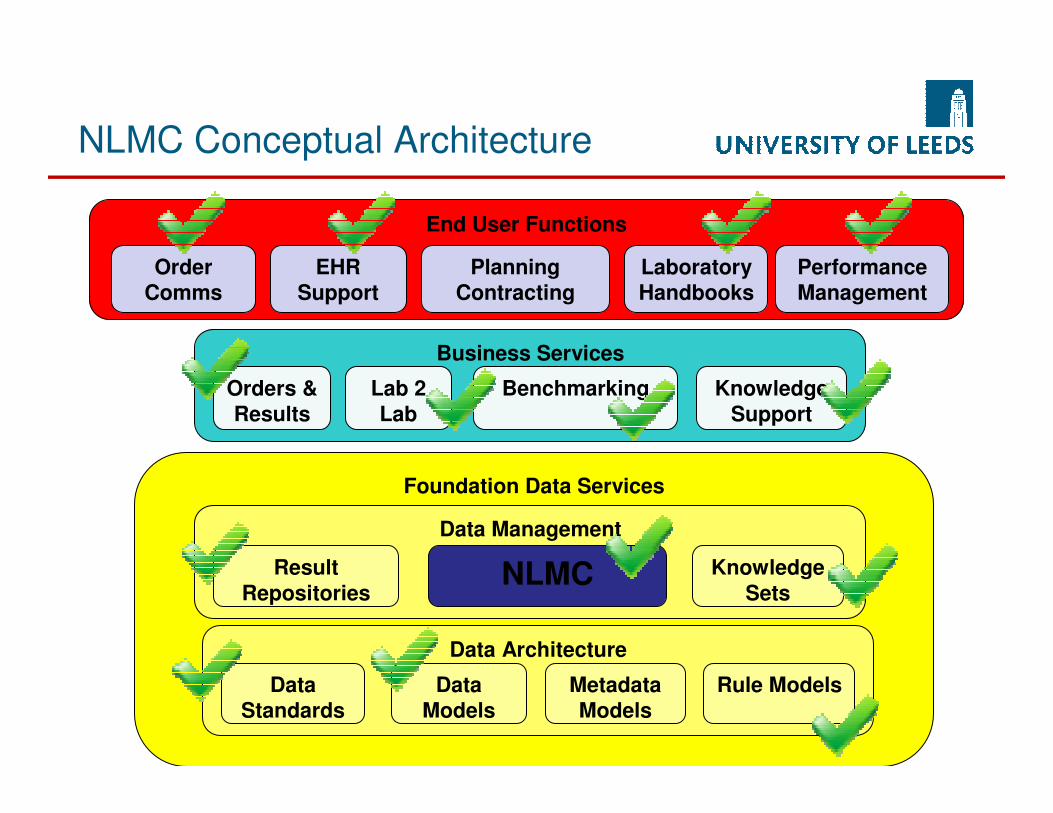
Foundation Data Services
Data Architecture
Data
Standards
Metadata
Models
Data
Models
Rule Models
Data Management
Result
RepositoriesNLMC Knowledge
Sets
Business Services
Orders &
Results
BenchmarkingLab 2
Lab
Knowledge
Support
End User Functions
Order
Comms
Planning
Contracting
EHR
Support
Laboratory
Handbooks
Performance
Management
NLMC Conceptual Architecture

Outline
• Historic Context
– What went wrong with the National Programme for IT
– What went right
• What is happening regarding:
– Scalability
– Standardisation
– Interoperability
• The Research Opportunities
– ResearchOne
– CPRD
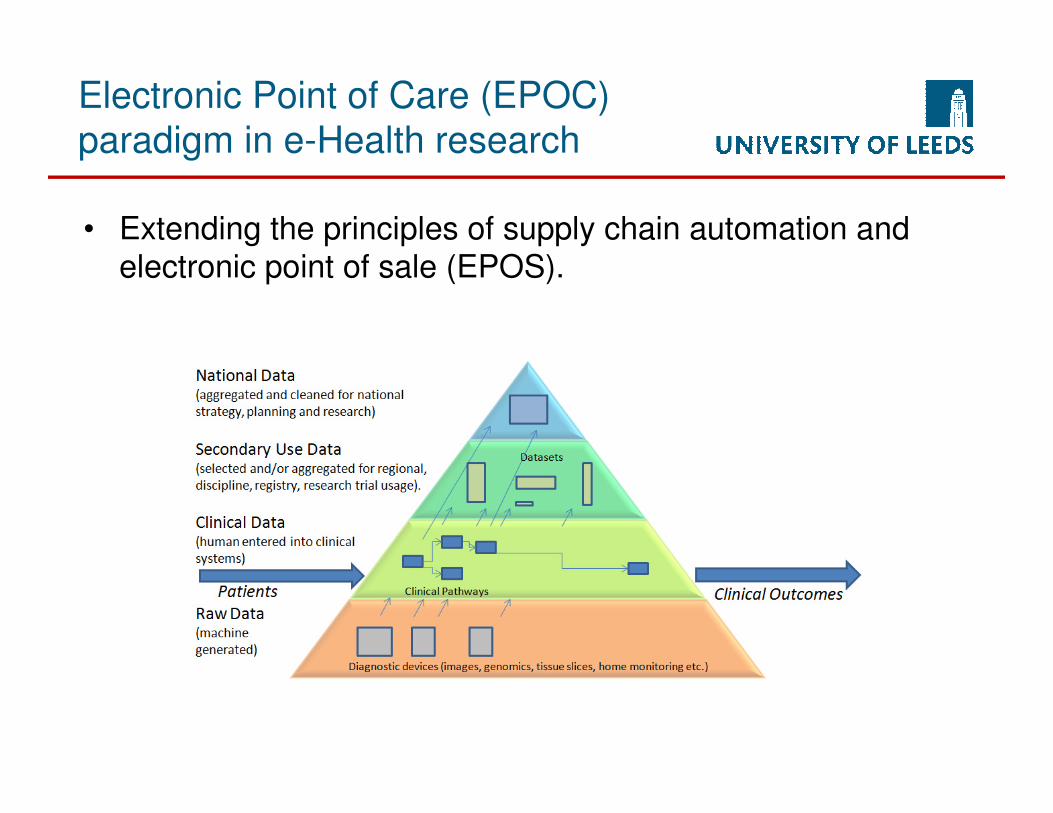
Electronic Point of Care (EPOC)
paradigm in e-Health research
• Extending the principles of supply chain automation and electronic point of sale (EPOS).

The ResearchOne Project
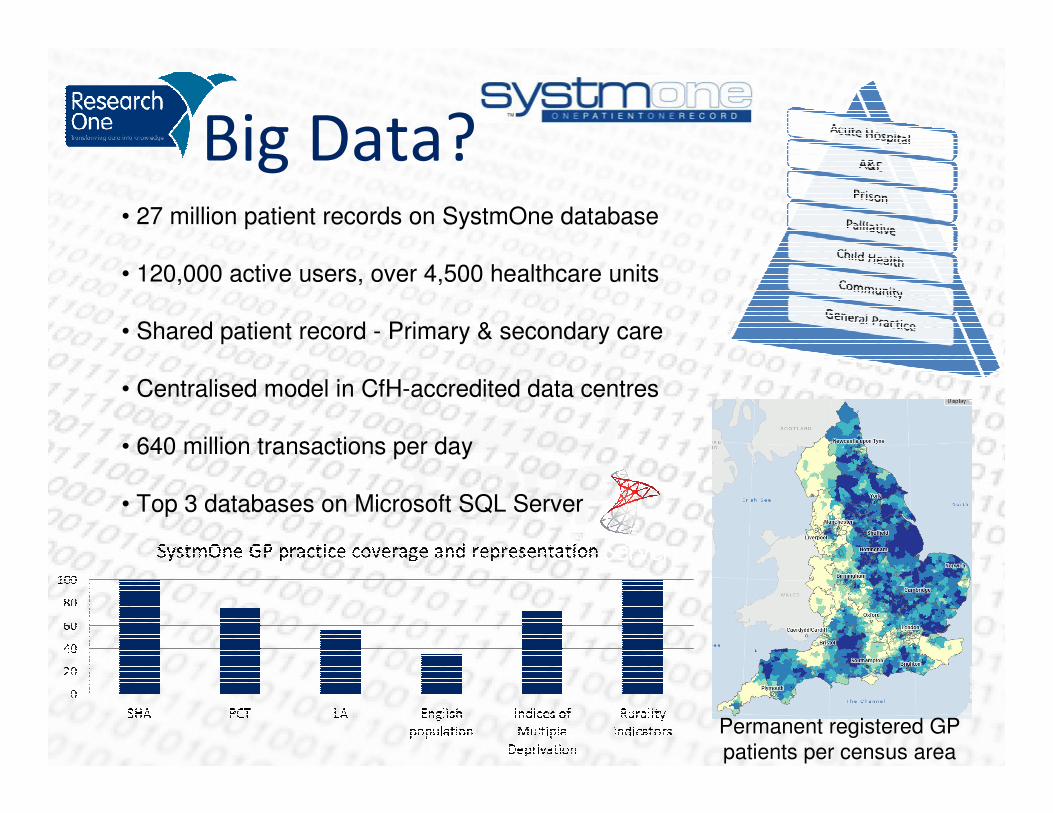
Big Data?• 27 million patient records on SystmOne database
• 120,000 active users, over 4,500 healthcare units
• Shared patient record - Primary & secondary care
• Centralised model in CfH-accredited data centres
• 640 million transactions per day
• Top 3 databases on Microsoft SQL Server
Permanent registered GP
patients per census area

Probably the world’s largest EPR?

SystmOne Live
Backup
Live Environment
Data Centre 2
Data Centre 1
Data Centre 1
Iterative
Feedback
Loop –innovation
into
practice
Weekly
ResearchOne Link
ResearchOne
Anonymised Data Extracts
Analytic
work
Public Health
Surveillance
Monthly
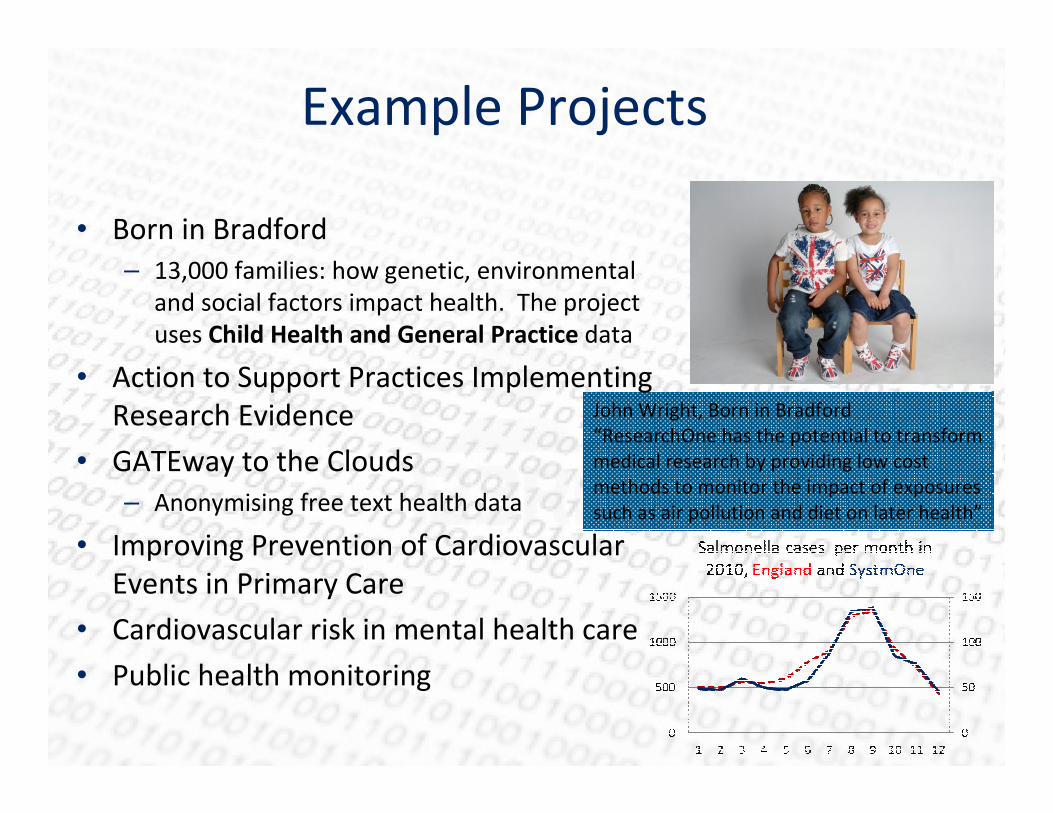
John Wright, Born in Bradford
“ResearchOne has the potential to transform
medical research by providing low cost
methods to monitor the impact of exposures
such as air pollution and diet on later health”
Example Projects
• Born in Bradford
– 13,000 families: how genetic, environmental
and social factors impact health. The project
uses Child Health and General Practice data
• Action to Support Practices Implementing
Research Evidence
• GATEway to the Clouds
– Anonymising free text health data
• Improving Prevention of Cardiovascular
Events in Primary Care
• Cardiovascular risk in mental health care
• Public health monitoring

Anonymisation level required
Smith, Xu, Hina and Johnson (2013). GATEway to the Cloud - Case study: A privacy-aware environment for Electronic Health Records research. 7th IEEE International Symposium on Service Oriented System Engineering, SOSE 2013, San Francisco, CA.
Limited AccessAnonymised e-health records for purposes
other than direct care
Researcher
Virtual Research Environments as
Portals onto a Safe Haven

National linkage of all health data -
CPRD
• Clinical Practice Research Datalink Service
• Follow-on from GPRD
• ~£60m funding
• Feeding data to Pharma & Research
• Extracts GP data
automatically via HSCIC
• Launched 2012

Supported by MRC Funded
Research - 2012

Final words – plus ca change.
• Health Secretary Jeremy Hunt told the audience at a US conference that the UK
was in the third stage of technology’s
transformation of health care.
• The government’s plan to sequence 100,000
human genomes and link these to electronic health records will be “as significant as the
founding of the Internet”.
• Minister for Universities and Science David
Willetts said: “Thanks to the NHS and the UK’s world-leading research base, we are
uniquely positioned to use patient data to
study disease and develop better treatments.”

Summary
• UK National Programme for IT was a mixed blessing
– Many failings but several notable successes
• Health Informatics high on research agenda
– ResearchOne
– CPRD - £60
– Medical Research Council
• eHerc Programme - £20m
• Medical Bioinformatics programme - £60m
• All predicated on increasingly large scale, standardised and
interoperable NHS Information Systems