update in the treatment of locally advanced breast cancer: a
TRANSCRIPT
These cancers vary widely in biological char-acteristics and clinical behavior, ranging from lo-cally aggressive, but systemically “indolent”, tode novo generalized disease.
The prognosis depends on tumor size, extentof lymph node involvement, and the presence orabsence of an inflammatory component. Accord-ing to the SEER data (1973-1998), the 3- and 5-year relative survival rates for women with stageIII breast cancer are 70% and 55%, respectively.Median survival for women with stage III diseaseis 4.9 years.
The clinical management of LABC is complexand should be tailored to the individual patient. Amultidisciplinary approach is recommendedcombining surgery, radiotherapy and systemictherapy (chemotherapy and/or hormone therapy).
Clinical Features
Locally Advanced Breast CancerLocally advanced breast cancer is a hetero-
geneous disease, including disease which is ei-ther extensive within the breast and/or ipsilater-al nodal areas (Figures 1, 2, 3). Staging isbased on the TNM (tumour, nodes, metastasis)system (Table I). The staging system for breastcancer has varied over time, so categorisationof LABC varies subtly between studies. Somestudies of LABC include patients with large tu-mours, e.g. > 5 cm in size. However, the size ofthe primary tumour on its own does not qualifya tumour for LABC status. These differing def-initions may make comparison of results be-tween studies difficult.
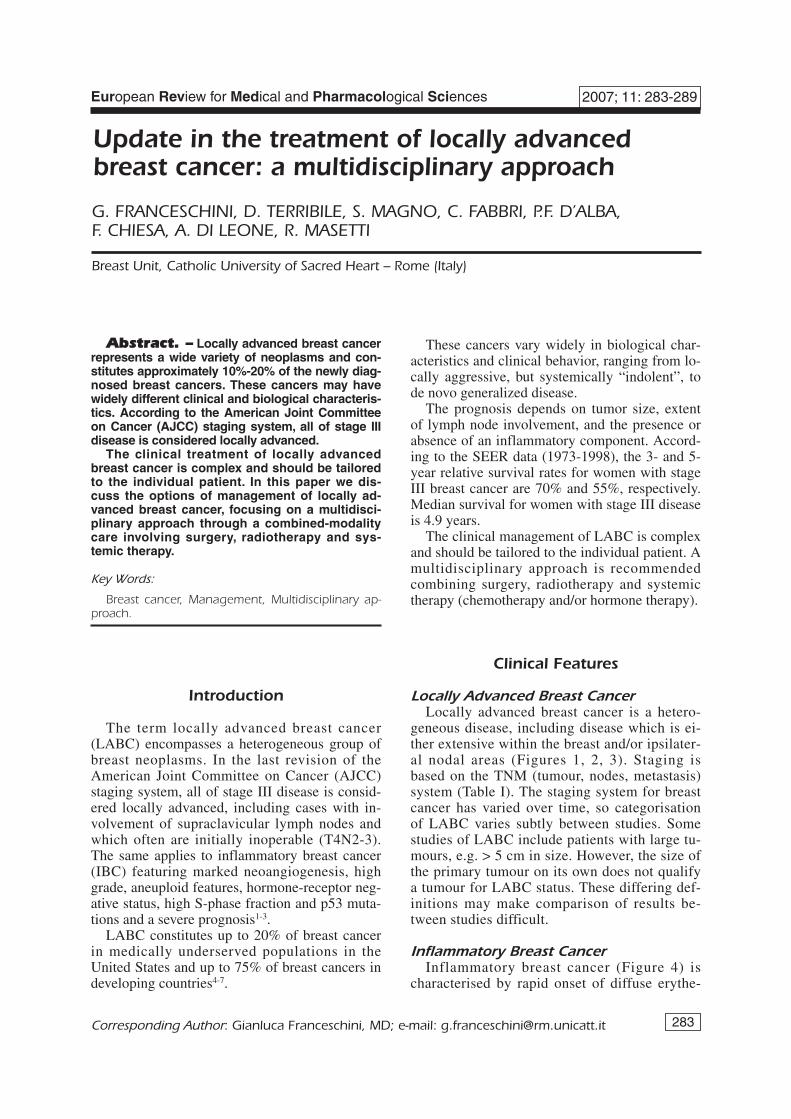
Inflammatory Breast CancerInflammatory breast cancer (Figure 4) is
characterised by rapid onset of diffuse erythe-
283
Abstract. – Locally advanced breast cancerrepresents a wide variety of neoplasms and con-stitutes approximately 10%-20% of the newly diag-nosed breast cancers. These cancers may havewidely different clinical and biological characteris-tics. According to the American Joint Committeeon Cancer (AJCC) staging system, all of stage IIIdisease is considered locally advanced.The clinical treatment of locally advanced
breast cancer is complex and should be tailoredto the individual patient. In this paper we dis-cuss the options of management of locally ad-vanced breast cancer, focusing on a multidisci-plinary approach through a combined-modalitycare involving surgery, radiotherapy and sys-temic therapy.
Key Words:
Breast cancer, Management, Multidisciplinary ap-proach.
Introduction
The term locally advanced breast cancer(LABC) encompasses a heterogeneous group ofbreast neoplasms. In the last revision of theAmerican Joint Committee on Cancer (AJCC)staging system, all of stage III disease is consid-ered locally advanced, including cases with in-volvement of supraclavicular lymph nodes andwhich often are initially inoperable (T4N2-3).The same applies to inflammatory breast cancer(IBC) featuring marked neoangiogenesis, highgrade, aneuploid features, hormone-receptor neg-ative status, high S-phase fraction and p53 muta-tions and a severe prognosis1-3.
LABC constitutes up to 20% of breast cancerin medically underserved populations in theUnited States and up to 75% of breast cancers indeveloping countries4-7.
European Review for Medical and Pharmacological Sciences 2007; 11: 283-289
Corresponding Author: Gianluca Franceschini, MD; e-mail: [email protected]
Update in the treatment of locally advancedbreast cancer: a multidisciplinary approach
G. FRANCESCHINI, D. TERRIBILE, S. MAGNO, C. FABBRI, P.F. D’ALBA,F. CHIESA, A. DI LEONE, R. MASETTI
Breast Unit, Catholic University of Sacred Heart – Rome (Italy)

284
ma and warmth, oedema of most of the breastoften with breast enlargement, diffuse firmnesson palpation, one breast is often ‘heavier’ thanthe other peau d’orange and ridging. Peaud’orange is not uncommon after treatment forbreast cancer (surgery and radiotherapy), but inthis case it usually improves with time. Thesefeatures may also be seen with mastitis or abreast abscess. Consequently, patients with in-flammatory breast cancer are often initiallythought to have infection and are often referredwhen the signs have not responded to treatmentwith antibiotics. A discrete mass may not bepresent.
G. Franceschini, D. Terribile, S. Magno, C. Fabbri, P.F. D’Alba, F. Chiesa, A. Di Leone, R. Masetti
Locally advanced breast cancer is defined as:
• T3 N2-3 M0• T4 N any M0• T any N any M 1(scf)
T = Tumour
T1 Tumour < 2 cmT2 Tumour > 2 cm < 5 cm in greatest diameterT3 Tumour > 5 cm in greatest diameterT4a Extension to chest wall (ribes, intercostal mus-
cles, serratus anterior but not pectoral muscles)T4b Oedema (peau d’orange), ulceration of skin of
breast, satellite nodulesT4c Both T4a and T4bTM Inflammatory carcinoma
N = Nodes
N0 No regional lymph node metastasisN1 Metastasis to movable ipsilateral axillary
lymph nodesN2a Involved axillary nodes fixed to one another or
other structures,N2b Metastasis in clinically apparent ipsilateral
internal mammary nodes (in absence ofclinically evident axillary nodes)
N3a Metastasis to infraclavicular node(s)N3b Metastasis in internal mammary and axillary
node(s)N3c Metastases in supraclavicular node(s)
M = Metastasis
M0 No distant metastasisM1(scf) Metastasis only to ipsilateral supraclavicular
lymph nodesM1 Distant metastasis
Table I. TNM classification.
Figure 1. Patient with a LABC in her right breast. Pictureshows a large primary exophytic ductal invasive carcinomawith massive skin infiltration.
Figure 2. Patient with a LABC in her left breast demon-strating a large primary ductal invasive carcinoma with ul-cerated skin.
Figure 3. Patient with a giant papillary carcinoma andwide skin infiltration in her right breast.
Diagnosis
Breast imaging is essential for all women pre-senting with significant breast symptoms. Mam-mography and ultrasound however, may notdemonstrate the classic features of primary breastcancer in IBC. For instance, imaging may shownonspecific signs such as generalised increase inbreast tissue density and thickening of the skinrather than a discrete lesion. It would not be un-usual to find significant clinical signs with mini-mal radiological abnormality, but at other timesthe imaging findings may be quite obvious.Mammography may be inappropriate for patientswith gross presentations of LABC (bleeding orfungating tumour), although ultrasound is a valu-able method of documenting tumour size and ex-tent before initiation of treatment.
A computed tomography and dynamic magnet-ic resonance imaging must be used to study thebreast and lymph-nodal areas. The diagnosis ofLABC or IBC can be confirmed with core needlebiopsy or fine needle biopsy. A core biopsy hasthe advantage of obtaining sufficient material tocharacterise the tumour in terms of grade, hor-mone receptor status and HER-2 status.
Treatment of Operable Tumours(Stage IIIA)
Patients with stage IIIA breast cancer have tra-ditionally been treated with modified radicalmastectomy (MRM) followed by adjuvant sys-temic therapy and radiotherapy. In the lastdecade neoadjuvant chemotherapy (NAC) fol-lowed by surgery and radiotherapy has progres-sively become the standard approach.
Even though NAC does not improve disease oroverall survival, it does produce in many cases ashrinkage of the tumour allowing the perfor-mance of breast-conserving surgery (BCS), incases that would have required a mastectomy.
The reported response rate following NAC foroperable breast cancer in randomized clinical tri-als varies between 49 and 94%, with a pathologiccomplete response (pCR) rate of 4-34%8-13.
Anthracycline based regimens were beenwidely used, but recent studies indicate a re-sponse rate at least equivalent better using tax-anes as single agent or in combination. Thelargest study using neoadjuvant docetaxel (NS-ABP B-27) showed pCR in 26% of patients whoreceived four cycles of docetaxel following fourcycles of adriamycin–cyclophosphamide com-pared with 14% in those receiving four cycles ofadriamycin–cyclophosphamide only. In manyrandomized studies reported, breast-conservingsurgery could be carried out following NAC in22-82% of patients with III A LABC. The lowestrate of breast conservation was the EORTC10902 trial in which only 22% of patients hadbreast-conserving surgery. Scholl et al demon-strated an 82% breast conservation rate initiallyfollowing NAC and radiotherapy. However, therate decreased to 61% at 5 years because of thedevelopment of local recurrence treated by sub-sequent mastectomy13.
More recently, new drugs have been intro-duced in the routine treatment of locally ad-vanced breast cancers, even in neoadjuvant set-ting; among them, Trastuzumab, a humanizedmonoclonal antibody directed to the extracellulardomain of the HER-2 receptor, has showed en-couraging results.
Mohsin et al carried out a prospective trial in-volving 35 patients with LABC overexpressingHer-2/neu, in the attempt to identify predictiveclinical markers of response to the antibody. Pa-tients received weekly trastuzumab as a singleagent for the first 3 weeks, and then combinedwith docetaxel for 12 weeks before surgery. Theauthors reported an early response to trastuzum-ab as monotherapy, with a median tumour de-
285
Update in the treatment of locally advanced breast cancer: a multidisciplinary approach
Figure 4. Patient with a massive inflammatory carcinomaof the left breast.
Management of operable tumors (IIIA)
• MRM followed by chemotherapy and locoregionalradiotherapy
• Chemotherapy first followed by surgery and locore-gional radiotherapy

286
crease of 20%. Eight patients showed a partial re-sponse. The study suggests that one of the mech-anisms of action is apoptosis. The apoptoticmechanism may result in a synergistic or additiveactivity when it is combined with chemotherapy.In fact, resistance to chemotherapy-induced celldeath may be overcome by a drug that works ona common antiapoptotic pathway. Chemotherapymay exert an additive effect by killing the morerapidly proliferating cells14-16.
A recent trial of neoadjuvant chemotherapy inHER-2 positive tumours compared paclitaxel fol-lowed by FEC (fluorouracil, epirubicin, and cy-clophosphamide) chemotherapy to paclitaxel,FEC, and trastuzumab (Herceptin). Forty-two pa-tients with T1-3 N0-1 tumours were evaluatedwith a median follow-up of 20 months. The re-sults showed the regimen including trastuzumabto be so superior that the trial was stopped10.
Bianchi et al17 showed that trastuzumab ap-pears to be highly effective when given concomi-tantly with doxorubicin and paclitaxel (AT) orwith paclitaxel alone after completion of AT inthe treatment of locally advanced breast cancer.The findings of this study justified the recent ini-tiation of a multicenter, randomized, controlledPhase III trial comparing AT followed by pacli-taxel then by CMF with the same chemotherapyplus trastuzumab in women with HER2-positivelocally advanced breast cancer.
NOAH (NeOAdjuvant Herceptin) is a PhaseIII trial of neoadjuvant trastuzumab in combina-tion with chemotherapy in patients with HER2-positive locally advanced breast cancer. In thisstudy, Gianni et al showed that Neoadjuvant Her-ceptin plus AT/CMF-containing chemotherapysignificantly improved the pCR rate of LABC vschemotherapy alone. Treatment was well tolerat-ed with acceptable cardiac safety. Follow-up isongoing and EFS is maturing18.
Geyer et al19 studied the Lapatinib, a tyrosinekinase inhibitor of human epidermal growth fac-tor receptor type 2 and epidermal growth factorreceptor. They compared lapatinib pluscapecitabine with capecitabine alone in such pa-tients. Women with HER2-positive, locally ad-vanced or metastatic breast cancer that had pro-gressed after treatment with regimens that in-cluded an anthracycline, a taxane, and trastuzum-ab were randomly assigned to receive eithercombination therapy (lapatinib at a dose of 1250mg per day continuously plus capecitabine at adose of 2000 mg per square meter of body-sur-face area on days 1 through 14 of a 21-day cycle)
or monotherapy (capecitabine alone at a dose of2500 mg per square meter on days 1 through 14of a 21-day cycle). They showed that lapatinibplus capecitabine is superior to capecitabinealone in women with HER2-positive advancedbreast cancer that has progressed after treatmentwith regimens that included an anthracycline, ataxane, and trastuzumab16,19.
Accurate monitoring of the response to thera-py should be adopted in all patients undergoingNAC. Magnetic resonance imaging (MRI) hasbeen shown to be most accurate of the currentlyavailable methods for assessment of residual dis-ease after NAC, as mammography and ultra-sonography may not be able clearly to distin-guish chemotherapy-induced fibrosis from resid-ual tumour. At surgery, it may be difficult toidentify the exact tumour location following acomplete clinical response to NAC. A good op-tion is to consider insertion of tissue marker clipsinto the tumour at the time of biopsy to enablepreoperative localization of the tumour bed in theevent of a complete clinical response20,21.
Tumour response following NAC has beenshown to be either concentric or honeycombed.In the latter instance, the tumour shrinkage is un-even and viable tumour foci may remain somedistance away from the central residual tumoursite. This may account for the reported higher lo-cal recurrence rates observed in some of the ran-domized trials. Detailed histopathological assess-ment of margins is essential in such patients. Ifthere is any evidence of multifocal disease, re-ex-cision or mastectomy should be considered.
The results from two trials (NSABP B 18 andEORTC trial) suggested that patients whose tu-mours were down-staged so that BCS could beperformed when it was not initially planned wereat higher risk of local recurrence and had worsesurvival. So, patient with operable stage III dis-ease who desire to preserve their breast should bemade aware that BCS may expose to this risk22-28.
MRM remains the standard surgical treatmentfor operable locally advanced disease that havesuboptional clinical response to NAC. Breast re-construction should be delayed after completionof chemotherapy and radiotherapy.
The role of radiotherapy to locoregional man-agement was investigated in many studies. In thestudy of Olson et al, eligible patients with opera-ble LABC had a mastectomy, 6 cycles of anthra-cycline-based chemotherapy and, if disease-free,were randomly assigned to receive radiotherapyor observation with radiotherapy at isolated sites
G. Franceschini, D. Terribile, S. Magno, C. Fabbri, P.F. D’Alba, F. Chiesa, A. Di Leone, R. Masetti

of locoregional failure29. Locoregional recur-rences were reduced from 24% to 15% with im-mediate radiotherapy29.
When locoregional radiotherapy is deliveredfollowing MRM for locally advanced disease, ra-diation should be delivered to the chest wall andthe supraclavicular and axillary nodes. Whethertreatment to the internal mammary nodes is re-quired is unclear. In many studies the internalmammary nodes were irradiated. However, thereare no studies that examined the impact of suchradiotherapy. It is not unreasonable to include ra-diotherapy to the internal mammary nodal region,provided that this can be done without treating anexcessive amount of heart or lung tissue.
Treatment of Inoperable Tumours(Stage IIIB-IIIC)
Patients with stage IIIB or IIIC disease, in-cluding those with inflammatory breast cancerand those with isolated ipsilateral internal mam-mary or supraclavicular lymph-node involvementare often inoperable.
Patients with stage IIIB or IIIC disease whorespond to primary chemotherapy should betreated until the response plateaux or to a maxi-mum of 6 cycles (minimum 4 cycles) after whichseveral case series have demonstrated that lo-coregional control is improved30-35.
The locoregional management of patientswith stage IIIC disease who respond tochemotherapy is unclear and should be individu-alized. In the absence of evidence on this sub-group of patients, it is reasonable that they re-ceive locoregional radiotherapy (including nodalirradiation). The role of completion mastectomyshould be individualized and based on technicaland disease factors28-33.
The treatment of patients with LABC whosetumours do not respond to anthracycline-contain-ing chemotherapy is unclear.
It is reasonable to try taxane chemotherapy orto proceed directly to locoregional therapy in-cluding irradiation and MRM, if possible28-33.
Following completion of chemotherapy, pre-or postmenopausal patients with locally ad-vanced (operable and inoperable) hormone-re-sponsive tumours should receive adjuvant ta-moxifen therapy, 20 mg/d, for 5 years. Tamox-ifen should be started after completion ofchemotherapy. Patients who are not candidatesfor any chemotherapy can be managed with hor-monal treatment and then receive locoregionalmanagement36-39.
Conclusion
The clinical management of LABC is complexand should be tailored to the individual patient.Locally advanced breast cancer and IBC presentdiagnostic and management challenges. Inflam-matory breast cancer in particular, may be diffi-cult to diagnose and is often mistaken for masti-tis. Persistent inflammatory symptoms musttherefore be investigated and referred to a breastsurgeon if not responding as expected to antibiot-ic therapy. Treatment of LABC and IBC requiresa coordinated multidisciplinary approach thatshould be individualised depending on tumourcharacteristics and response to treatment. Thetreatment may include a combination ofchemotherapy, radiotherapy and surgery. Whilethe prognosis in these cases is poor compared tothat for other presentations of breast cancer, areasonable survival and quality of life can be ob-tained with a team approach to treatment. Newtechnologies such as complementary DNA mi-croarrays,genomics and proteomics should helpclinicians to better characterize the biology ofbreast cancer and to tailor treatment based ondistinct molecular profiles with prognostic andpredictive value.
References
1) THE WESTERN AREAS BREAST GROUP. Breast cancerpatterns of care in the greater western region ofSydney in 1992. Westmead, NSW: the WesternAreas Breast Group and the NSW Breast CancerInstitute, 1997.
2) WINGO PA, JAMISON PM, YOUNG JL, GARGIULLO P.Population based statistics for women diagnosedwith inflammatory breast cancer. Cancer CausesControl 2004; 15: 321-328.
3. BONNIER P, CHARPIN C, LEJEUNE C, ROMAIN S, TUBIANAN, BEEDASSY B, MARTIN PM, SERMENT H, PIANA L. In-flammatory carcinomas of the breast: clinical,pathological, or a clinical and pathological defini-tion? Int J Cancer 1995; 62: 382-385.
4) PARTON M, DOWSETT M, ASHLEY S, HILLS M, LOWE F,SMITH IE. High incidence of HER-2 positivity in in-flammatory breast cancer. Breast 2004; 13: 97-103.
5) PANADES M, OLIVOTTO IA, SPEERS CH, SHENKIER T,OLIVOTTO TA, WEIR L, ALLAN SJ, TRUONG PT. Evolvingtreatment strategies for inflammatory breast can-cer: a population based survival analysis. J ClinOncol 2005; 23: 1941-1950.
287
Update in the treatment of locally advanced breast cancer: a multidisciplinary approach

288
6) SHENKIER T, WEIR L, LEVINE M, OLIVOTTO I, WHELAN T,REYNO L; STEERING COMMITTEE ON CLINICAL PRACTICEGUIDELINES FOR THE CARE AND TREATMENT OF BREASTCANCER. Clinical practice guidelines for the careand treatment of breast cancer: treatment forwomen with stage III or locally advanced breastcancer. CMAJ 2004; 170: 983-994.
7) THERASSE P, MAURIAC L, WELNICKA-JASKIEWICZ M, BRUN-ING P, CUFER T, BONNEFOI H, TOMIAK E, PRITCHARD KI,HAMILTON A, PICCART MJ; EORTC. Final results of arandomized phase III trial comparing cyclophos-phamide, epirubicin, and fluorouracil with a dose-intensified epirubicin and cyclophosphamide + fil-grastim as neoadjuvant treatment in locally ad-vanced breast cancer: an EORTC-NCIC-SAKKmulticenter study. J Clin Oncol 2003; 21: 843-850.
8) CASPER ES, GUIDERA CA, BOSL GJ, HAKES TB, KAUFMANRJ, SHURGOT B, KINNE DW. Combined modalitytreatment of locally advanced breast cancer: ad-juvant combination chemotherapy with and with-out doxorubicin. Breast Cancer Res Treat 1987; 9:39-44.
9) MARANA HRC, ANDRADE JM, TIEZZI DG, et al. Prima-ry chemotherapy in breast cancer shows excel-lent clinical and pathological response with doc-etaxel and epirubicin. Breast 2003; 12(Suppl 1):41.
10) BUZDAR AU, IBRAHIM NK, FRANCIS D, BOOSER DJ,THOMAS ES, THERIAULT RL, PUSZTAI L, GREEN MC, ARUNBK, GIORDANO SH, CRISTOFANILLI M, FRYE DK, SMITHTL, HUNT KK, SINGLETARY SE, SAHIN AA, EWER MS,BUCHHOLZ TA, BERRY D, HORTOBAGYI GN. Significant-ly higher pathologic complete remission rate afterneoadjuvant therapy with trastuzumab, paclitaxel,and epirubicin chemotherapy: results of a ran-domised trial in human epidermal growth factorreceptor 2-positive operable breast cancer. J ClinOncol 2005; 23: 3676-3685.
11) MONTEMURRO F, AGLIETTA M. Incorporatingtrastuzumab into the neoadjuvant treatment ofHER2 overexpressing breast cancer. Clin BreastCancer 2005; 6: 77-80.
12) VALAGUSSA P, ZAMBETTI M, BONADONNA G, ZUCALI R,MEZZANOTTE G, VERONESI U. Prognostic factors inlocally advanced noninflammatory breast cancer.Long term results following primary chemothera-py. Breast Cancer Res Treat 1990; 15: 137-147.
13) SCHOLL SM, BEUZEBOC P, HARRIS AL, PIERGA JY, ASSE-LAIN B, PALANGIÉ T, DORVAL T, JOUVE M, DIÉRAS V,POUILLART P. Is primary chemotherapy useful for allpatients with primary invasive breast cancer? Re-cent Results Cancer Res 1998; 152: 217-226.
14) GIACCHETTI S, CUVIER C, HOCINI H, BOURSTYN E, DEROQUANCOURT A, ESPIÉ M. Neoadjuvant treatment ofearly breast cancer: new drugs contribution. BullCancer 2004; 91(Suppl 4): S232-238.
15) MOHSIN SK, WEISS HL, GUTIERREZ MC, CHAMNESS GC,SCHIFF R, DIGIOVANNA MP, WANG CX, HILSENBECK SG,OSBORNE CK, ALLRED DC, ELLEDGE R, CHANG JC.Neoadjuvant trastuzumab induces apoptosis in
primary. breast cancers. J Clin Oncol 2005; 23:2460-2468.
16) XIA W, GERARD CM, LIU L, BAUDSON NM, ORY TL,SPECTOR NL. Combining lapatinib (GW572016), asmall molecule inhibitor of ErbB1 and ErbB2 tyro-sine kinases, with therapeutic anti-ErbB2 antibod-ies enhances apoptosis of ErbB2-overexpressingbreast cancer cells. Oncogene 2005; 24: 6213-6221.
17) BIANCHI G, ALBANELL J, EIERMANN W, VITALI G,BORQUEZ D, VIGANO L, MOLINA R, RAAB G, LOCATELLIA, VANHAUWERE B, GIANNI L, BASELGA J. Pilot trial oftrastuzumab starting with or after the doxorubicincomponent of a doxorubicin plus paclitaxel regi-men for women with HER2-positive advancedbreast cancer. Clin Cancer Res 2003; 9(16 Pt 1):5944-5951.
18) GIANNI L, SEMIGLAZOV V, MANIKHAS GM, et al.Neoadjuvant trastuzumab in locally advancedbreast cancer (NOAH): Antitumour and safetyanalysis. J Clin Oncol 2007 ASCO Annual Meet-ing Proceedings Part I. 2007; 25(18S) (June 20Suppl): 532.
19) GEYER CE, FORSTER J, LINDQUIST D, CHAN S, ROMIEUCG, PIENKOWSKI T, JAGIELLO-GRUSZFELD A, CROWN J,CHAN A, KAUFMAN B, SKARLOS D, CAMPONE M, DAVID-SON N, BERGER M, OLIVA C, RUBIN SD, STEIN S,CAMERON D. Lapatinib plus capecitabine for HER2-positive advanced breast cancer. N Engl J Med2006; 355: 2733-2743. Erratum in: N Engl J Med2007; 356: 1487.
20) GURNEY H, HARNETT P, KEFFORD R, BOYAGES J. Inflam-matory breast cancer: enhanced local control withhyperfractionated radiotherapy and infusional vin-cristine, ifosphamide and epirubicin. Aust N Z JMed 1998; 28: 400-402.
21) PEREZ CA, GRAHAM ML, TAYLOR ME, LEVY JF, MORTIMERJE, PHILPOTT GW, KUCIK NA. Management of locallyadvanced carcinoma of the breast. I. Noninflam-matory. Cancer 1994; 74: 453-465.
22) RUBENS RD, BARTELINK H, ENGELSMAN E, HAYWARD JL,ROTMENSZ N, SYLVESTER R, VAN DER SCHUEREN E, PAPA-DIAMANTIS J, VASSILAROS SD, WILDIERS J, et al. Locallyadvanced breast cancer: the contribution of cyto-toxic and endocrine treatment to radiotherapy. EurJ Cancer Clin Oncol 1989; 25: 667-678.
23) FREEDMAN OC, VERMA S, CLEMONS MJ. Using aro-matase inhibitors in the neoadjuvant setting: evo-lution or revolution? Cancer Treat Rev 2004; 31:1-17.
24) MICHELETTI E, PLEBANI F, TESTOLIN A, BIGNARDI M. Pri-mary radiotherapy versus surgery and radiothera-py in the management of postmenopausal locallyadvanced breast cancer. Tumori 1991; 77: 141-144.
25) CRISTOFANILLI M, BUZDAR AU, HORTOBAGYI GN. Up-date on the management of inflammatory breastcancer. Oncologist 2003; 8: 141-148.
G. Franceschini, D. Terribile, S. Magno, C. Fabbri, P.F. D’Alba, F. Chiesa, A. Di Leone, R. Masetti

26) RANGAN AM, AHERN V, YIP D, BOYAGES J. Local recur-rence after mastectomy and adjuvant CMF: impli-cations for adjuvant radiation therapy. Aust N Z JSurg 2000; 70: 649-655.
27) WHELAN TJ, JULIAN J, WRIGHT J, JADAD AR, LEVINE ML.Does locoregional radiation therapy improve sur-vival in breast cancer? A meta-analysis. J ClinOncol 2000; 18: 1220-1229.
28) AHERN V, BARRACLOUGH B, BOSCH C, LANGLANDS A,BOYAGES J. Locally advanced breast cancer: defin-ing an optimum treatment regimen. Int J RadiatOncol Biol Phys 1994; 28: 867-875.
29) OLSON JE, NEUBERG D, PANDYA KJ, RICHTER MP, SOLINLJ, GILCHRIST KW, TORMEY DC,VEEDER M, FALKSON G.The role of radiotherapy in the management ofoperable locally advanced breast carcinoma: re-sults of a randomized trial by the Eastern Cooper-ative Oncology Group. Cancer 1997; 79: 1138-1149.
30) SOMLO G, FRANKEL P, CHOW W, et al. Prognostic in-dicators and survival in patients with stage III in-flammatory breast carcinoma after dose intensechemotherapy. J Clin Oncol 2004; 22: 1839-1848.
31) ARDAVANIS A, SCORILAS A, TRYFONOPOULOS D, OR-PHANOS G, MISSITZIS I, KARAMOUZIS M, CHRYSOCHOOUM, SOTIROPOULOU A, ARNOGIANNAKI N, IOANNIDIS G,PISSAKAS G, RIGATOS G. Multidisciplinary therapy oflocally far-advanced or inflammatory breast can-cer with fixed perioperative sequence of Epiru-bicin, Vinorelbine, and Fluorouracil chemothera-py, surgery, and radiotherapy: long-term results.Oncologist 2006; 11: 563-573.
32) BARNI S, MANDALA M. Locally advanced breast can-cer. Curr Opin Obstet Gynecol 2006; 18: 47-52.
33) CINIERI S, ORLANDO L, COLLEONI M. Primary sys-temic therapy on local advanced breast cancer,where are we going? Ann Oncol 2006; 17 (suppl):18-21.
34) CARLSON RW, FAVRET AM. Multidisciplinary manage-ment of locally advanced breast cancer. Breast J1999; 5: 303-307.
35) LOW JA, BERMAN AW, STEINBERG SM, DANFORTH DN,LIPPMAN ME, SWAIN SM. Long-term follow-up forlocally advanced and inflammatory breast cancerpatients treated with multimodality therapy. J ClinOncol 2004; 22: 4067-4074.
36) Hutcheon AW, HEYS SD, SARKAR TK; AND ABERDEENBREAST GROUP. Neoadjuvant docetaxel in locally ad-vanced breast cancer. Breast Canc Res Treat2003; 79(Suppl. 1): S19-S24.
37) VALERO V, BUZDAR A, HORTOBAGYI G. Locally ad-vanced breast cancer. The Oncologist 1996; 1: 8-17.
38) CARLSON R, FAVRET A. Multidisciplinary manage-ment of locally advanced breast cancer. Breast J1999; 5: 303.
39) MANO MS, AWADA A. Primary chemoterapy forbreast cancer: the evidence and future. Ann On-col 2004; 15: 1161-1171.
289
Update in the treatment of locally advanced breast cancer: a multidisciplinary approach