update in the management of sepsis - …thececonsultants.com/images/2little_sepsis.pdf · update in...
TRANSCRIPT
UpdateintheManagementofSepsisNATHANIELLITTLE,MD
UNIVERSITYOFCOLORADO
DIVISIONOFPULMONARYSCIENCES&CRITICALCAREMEDICINE
DisclosureIhavenoactualorpotentialconflictofinterestinrelationtothispresentation.
Objectives
Explore Explorecurrentcontroversiesinthemanagementofsepsisandsepticshock
Review Reviewemergingliteraturesurroundingsepsismanagement
Identify Identifythescientificrationalebehindcoresepsisbundlecomponentsandassesthecontributionofeachcomponenttooverallclinicaleffect
Understand Understandrecentrefinementsinthedefinitionofsepsis-relatedclinicalentitiesandprognosticationtools

ClinicalCase66year-oldLebanesewomanwithhistoryofmigraines,HTN,GERD,DM2,diastolicHF,OSApresentstotheEDwithcomplaintsofalteredmentalstatusandnausea/vomiting
-usualstateofhealthwithexceptionofsevereheadacheandsomeshakingchillslastevening
-retiredtobedfollowinguseofhertriptanandthetrustyCPAPmask
-husbandnotedabnormalsoundscomingfromherroomat10:00amthenextmorning
-findspatientobtunded,vomitingintoherCPAPmaskandshakingvigorously
-intubatedintheEDforrespiratoryextremis,uponfoley catheterplacement,notedtohaveastenchfromurinethatwould“knockyoursocksoff”
ClinicalCaseVitalsintheED:temperature38.3F,respiratoryrate22,pulse112,Osat 83%,GCS6
Intubatedforairwayprotection/hypoxemia,initialABG7.3/28/101on50%FiO2
CBC:WBC12.7Hgb11.1Plt 130
BMP:139/4.7/105/16/17/1.2
LFT’s:AST14,ALT13,TB0.9,AP71,Alb3.7
Followingintubation:developmentofnotablehypotension,MAP67requiring15ug/kg/mindopamineinED
TrendsInSepsisIncidence&Mortality
Rheeetal.IncidenceandtrendsofsepsisinUShospitalsusingclinicalvsclaimsdata,2009-2014.JAMA.2017;318(13):1241.
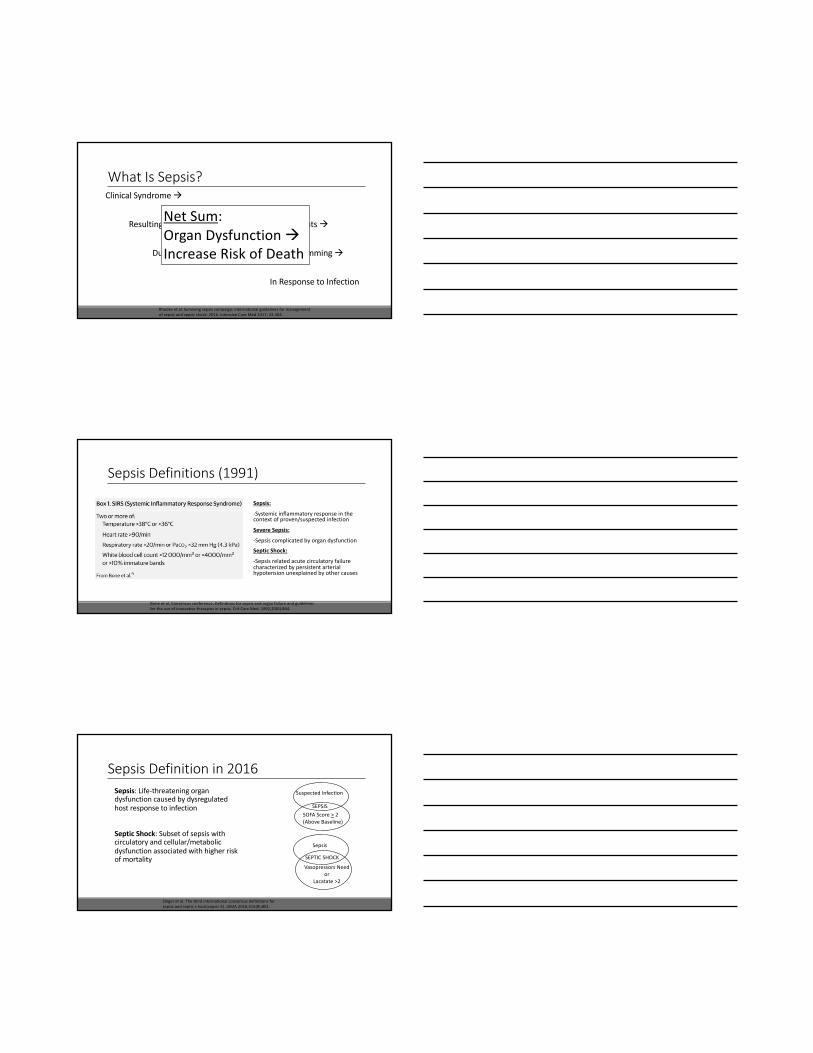
WhatIsSepsis?ClinicalSyndromeà
ResultinginPathologic/BiochemicalDerangementsà
DuetoDysregulatedInflammatoryProgrammingà
InResponsetoInfection
NetSum:OrganDysfunctionàIncreaseRiskofDeath
Rhodesetal.Survivingsepsiscampaign:internationalguidelinesformanagementofsepsisandsepticshock:2016.IntensiveCareMed2017;43:304.
SepsisDefinitions(1991)
Sepsis:
-Systemicinflammatoryresponseinthecontextofproven/suspectedinfection
SevereSepsis:
-Sepsiscomplicatedbyorgandysfunction
SepticShock:
-Sepsisrelatedacutecirculatoryfailurecharacterizedbypersistentarterialhypotensionunexplainedbyothercauses
Boneetal.Consensusconference:Definitionsforsepsisandorganfailureandguidelinesfortheuseofinnovativetherapiesinsepsis.Crit CareMed.1992;20(6):864.
SepsisDefinitionin2016Sepsis:Life-threateningorgandysfunctioncausedbydysregulatedhostresponsetoinfection
SepticShock:Subsetofsepsiswithcirculatoryandcellular/metabolicdysfunctionassociatedwithhigherriskofmortality
Singeretal.Thethirdinternationalconsensusdefinitionsforsepsisandsepticshock(sepsis-3).JAMA.2016;315(8):801.
SuspectedInfection
SOFAScore> 2(AboveBaseline)
SEPSIS
Sepsis
VasopressorsNeedor
Lacatate >2
SEPTICSHOCK

WhatIsSOFA?
Singeretal.Thethirdinternationalconsensusdefinitionsforsepsisandsepticshock(sepsis-3).JAMA.2016;315(8):801.
HowDoWeUseSOFA?-Attemptstodoabetterjobofconnectingevidenceoforgandysfunctionwithsepsis
-OrgandysfunctionisidentifiedasacutechangeintotalSOFAScore> 2(fromknownbaseline)or> 2(ifunknownbaseline)
-SOFAscore>2predictsanoverallmoralityriskof~10%ingeneralinpatientpopulationwithsuspectedinfection
Singeretal.Thethirdinternationalconsensusdefinitionsforsepsisandsepticshock(sepsis-3).JAMA.2016;315(8):801.
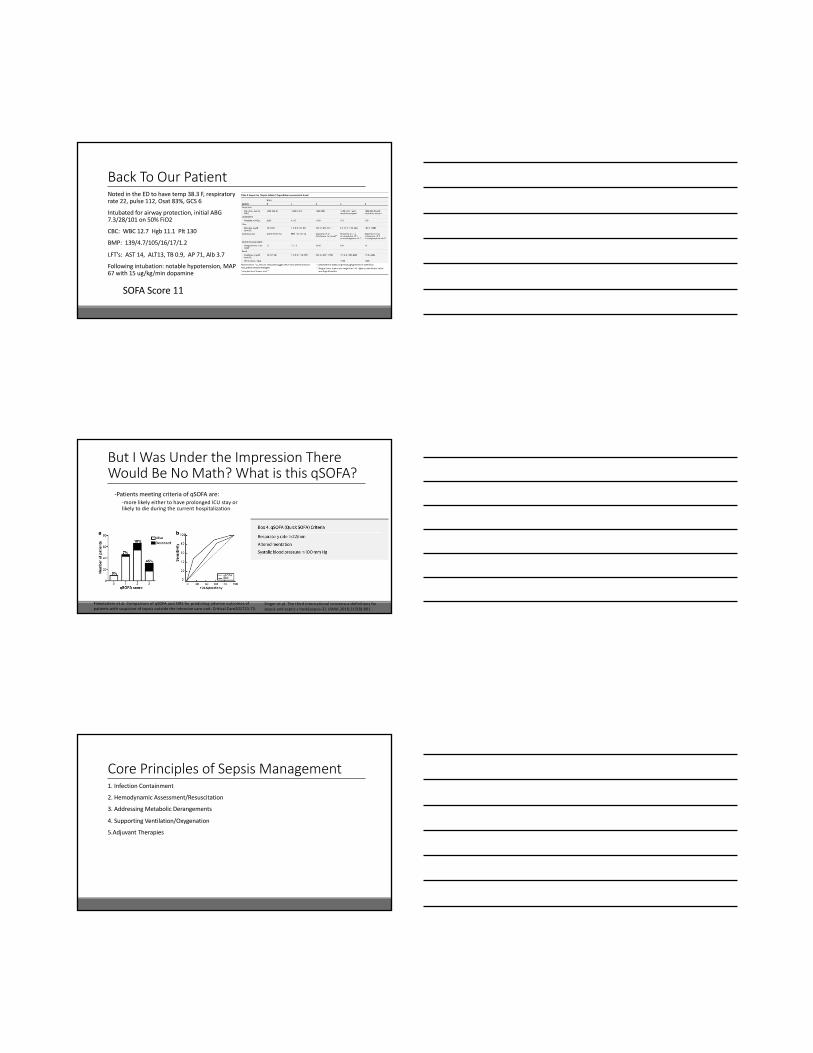
BackToOurPatientNotedintheEDtohavetemp38.3F,respiratoryrate22,pulse112,Osat 83%,GCS6
Intubatedforairwayprotection,initialABG7.3/28/101on50%FiO2
CBC:WBC12.7Hgb11.1Plt 130
BMP:139/4.7/105/16/17/1.2
LFT’s:AST14,ALT13,TB0.9,AP71,Alb3.7
Followingintubation:notablehypotension,MAP67with15ug/kg/mindopamine
BackToOurPatientNotedintheEDtohavetemp38.3F,respiratoryrate22,pulse112,Osat 83%,GCS6
Intubatedforairwayprotection,initialABG7.3/28/101on50%FiO2
CBC:WBC12.7Hgb11.1Plt 130
BMP:139/4.7/105/16/17/1.2
LFT’s:AST14,ALT13,TB0.9,AP71,Alb3.7
Followingintubation:notablehypotension,MAP67with15ug/kg/mindopamine
SOFAScore11
ButIWasUndertheImpressionThereWouldBeNoMath?WhatisthisqSOFA?
-PatientsmeetingcriteriaofqSOFA are:-morelikelyeithertohaveprolongedICUstayorlikelytodieduringthecurrenthospitalization
Singeretal.Thethirdinternationalconsensusdefinitionsforsepsisandsepticshock(sepsis-3).JAMA.2016;315(8):801.
Finkelsztein etal.ComparisonofqSOFA andSIRSforpredictingadverseoutcomesofpatientswithsuspicionofsepsisoutsidetheintensivecareunit.CriticalCare201721:73.
CorePrinciplesofSepsisManagement1.InfectionContainment
2.HemodynamicAssessment/Resuscitation
3.AddressingMetabolicDerangements
4.SupportingVentilation/Oxygenation
5.AdjuvantTherapies
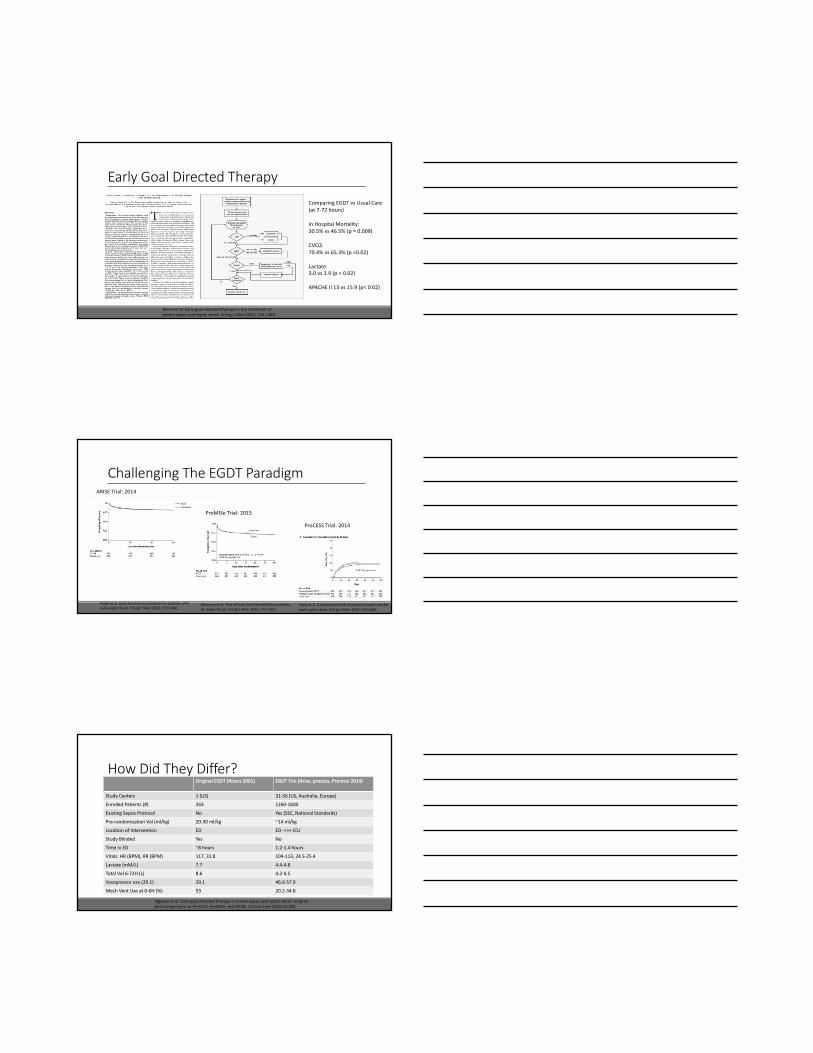
EarlyGoalDirectedTherapyComparingEGDTvsUsualCare(at7-72hours)
InHospitalMortality:30.5%vs46.5%(p=0.009)
CVO2:70.4%vs65.3%(p<0.02)
Lactate:3.0vs3.9(p<0.02)
APACHEII13vs15.9(p<0.02)
Riversetal.Earlygoal-directedtherapyinthetreatmentofseveresepsisandsepticshock.NEngl JMed2001;345:1368.
ChallengingTheEGDTParadigmARISETrial:2014
ProMISe Trial:2015
ProCESS Trial:2014
Mouncey etal.TrialofEarly,Goal-DirectedResuscitationforSepticShock.NEngl JMed.2015;372:1301.
Peakeetal.Goaldirectedresuscitationforpatientswithearlysepticshock.NEngl JMed.2014;371:1496.
Yealy etal.Arandomizedtrialofprotocol-basedcareforearlysepticshock.NEngl JMed.2014;370:1683.
HowDidTheyDiffer?OriginalEGDT(Rivers2001) EGDTTrio(Arise,process,Promise2014)
StudyCenters 1(US) 31-56(US,Australia,Europe)
EnrolledPatients(#) 263 1260-1600
ExistingSepsisProtocol No Yes(SSC,NationalStandards)
Pre-randomizationVol(ml/kg) 20-30ml/kg ~14ml/kg
LocationofIntervention ED ED->>>ICU
StudyBlinded Yes No
TimeinED ~8hours 1.2-1.4hours
Vitals:HR(BPM),RR(BPM) 117,31.8 104-113,24.5-25.4
Lactate(mM/L) 7.7 4.4-4.8
TotalVol6-72H(L) 8.6 4.2-4.5
Vasopressoruse(29.1) 29.1 46.6-57.9
MechVentUseat0-6H(%) 53 20.2-34.8
Nguyenetal.Earlygoaldirectedtherapyinseveresepsisandsepticshock:insightsandcomparisonstoProCESS,ProMISe,andARISE.CriticalCare2016;20:160.

Levyetal.Thesurvivingsepsiscampaign:resultsofaninternationalguidelinebasedperformanceimprovementprogramtargetingseveresepsis.Crit CareMed2010;38:367.
Unbundlingthe[Sepsis]Bundles
http://www.workhouses.org.uk/tour/oakum.shtml
“PickingOakum”
CorePrinciplesofSepsisManagement1.InfectionContainment
2.HemodynamicAssessment/Resuscitation
3.AddressingMetabolicDerangements
4.SupportingVentilation/Oxygenation
5.AdjuvantTherapies

IsThereAnyNewInsightIntoInfectionContainment?
Seymouretal.Timetotreatmentandmortalityduringmandatedemergencycareforsepsis.NEngl JMed2017;376:23.
TimingtoAntibiotics-ED?
Liuetal.Thetimingofearlyantibioticsandhospitalmortalityinsepsis.AJRCC2017;196(7):856.
TimingtoAntibiotics-ED/ICU?
Ferreretal.Empiricantibiotictreatmentreducesmortalityinseveresepsisandsepticshockfromthefirsthour:resultsfromaguideline-basedperformanceimprovementprogram.Crit CareMed2014;42(8):1749.

ReasonsForDelayInEffectiveAntibioticsinSepsis1.Failuretorecognizeinfectioninatimelymanner
2.Failuretorecognizethathypotensionassepticshock
3.Effectofinappropriateantimicrobialinitiation
4.Failuretoappreciateriskofresistantorganismsincertainscenarios(eg,immunocompromisedversusimmunosuppressed;antecedentantimicrobialuse)leadingtoinappropriateinitialantimicrobials
5.Waitingforbloodculturesbeforegivingantibiotic
6.TransferfromERbeforeorderedantibioticsgiven
7.Failuretousestatorders
8.Failuretorecognizethatadministrationofinappropriateantimicrobialsisequivalenttoabsentantimicrobialtherapywhenrespondingtoclinicalfailure
9.Nospecifiedorderwithmultipledrugregimenssothatkeydrug(usuallymostexpensiveandhardesttoaccess)maybegivenlast
10.Administrative/logisticdelays
Funketal.Anti-microbialtherapyforlife-threateninginfections:speedislife.Crit CareClin 2011;27:53.
HowMuchDoesAntibioticChoiceMatter?
Kumaretal.Initiationofinappropriateantimicrobialtherapyresultsinafivefoldreductionofsurvivalinhumansepticshock.Chest2009;136(5):1237.
TimingofCultures
0
20
40
60
80
100
120
140
160
0-4h 4-8h 8-12h 12-24h 24-48h
NumberPositiveCulturesvsTimofAbxAdministration
BacTec BacT/AlertOnly
Zadroga etal.Comparisonof2bloodculturemediashowssignificantdifferencesinbacterialrecoveryforpatientsonantimicrobialtherapy.ClinicalInfectiousDiseases2013;56(6):790.
InterimSummary:InfectionContainment-Empiricantibiotics/antimicrobialsshouldbeinitiatedwithin1hourofpresentationforsepsis
-Outsideofdefinitivesourcecontrol,antibioticslikelyremainthemostessentialpillarofsepsismanagement
-Relevantmicrobialculturesshouldbeobtainedassoonaspossible(preferablypriortoantibiotics),butshouldnotdelayadministrationofantimicrobials
-Appropriatechoiceofempiricantibioticsisnecessaryforoptimaloutcomes(bettertoinitiateappropriatelybroadspectrumandnarrowasrapidlyaspossible)
-Sequenceofantibioticsmatters:(gramnegativecoverage>>>grampositivecoverage>>>doublegramnegativecoverage/anti-fungalcoverage)
CorePrinciplesofSepsisManagement1.InfectionContainment
2.HemodynamicAssessment/Resuscitation
3.AddressingMetabolicDerangements
4.SupportingVentilation/Oxygenation
5.AdjuvantTherapies
InitialResuscitation-Sepsisandsepticshockaremedicalemergencies,itisrecommendthatresuscitationbeginimmediately-Intravascularhypovolemiaandsepsis-relatedhypoperfusion andcommonlyencountered,requiringpromptrecognition/action
DefinitionsofShock:“Theclinicalresultofcirculatoryfailurethatresultsininadequatecellularoxygenutilization.”
Rhodesetal.Survivingsepsiscampaign:internationalguidelinesformanagementofsepsisandsepticshock:2016.IntensiveCareMed2017;43:304.
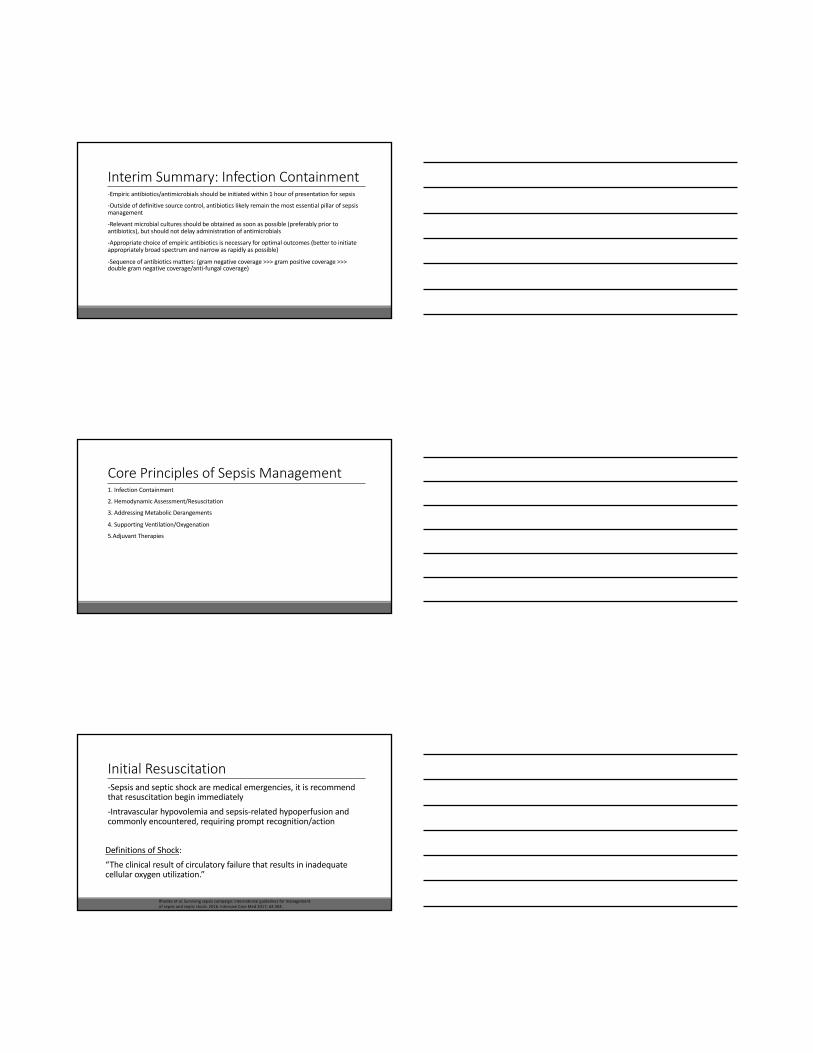
Inadequateoxygendeliverywithincreasedmetabolic
need
⬆ Sympatheticdrive
⬆ Cortisolrelease
⬆ Renin-angiotensinWater/Na+conservationVasoconstriction⬆ Bloodvolume
DEFENSEMECHANISMS:
Multiorgan Dysfunction• Alteredconsciousness• Respiratoryfailure(ARDS)• Renalfailure• Liverfailure• DIC
LessonsinActingQuickly
Seymouretal.Timetotreatmentandmortalityduringmandatedemergencycareforsepsis.NEngl JMed2017;376:23.
InitialResuscitation-TheTemplateHemodynamicGoals:CVP=8-12mmHgMAP=>65mmHgUrineOutput> 0.5ml/kg/hrScvO2>70%Hct >30%
Riversetal.Earlygoal-directedtherapyinthetreatmentofseveresepsisandsepticshock.NEngl JMed2001;345:1368.
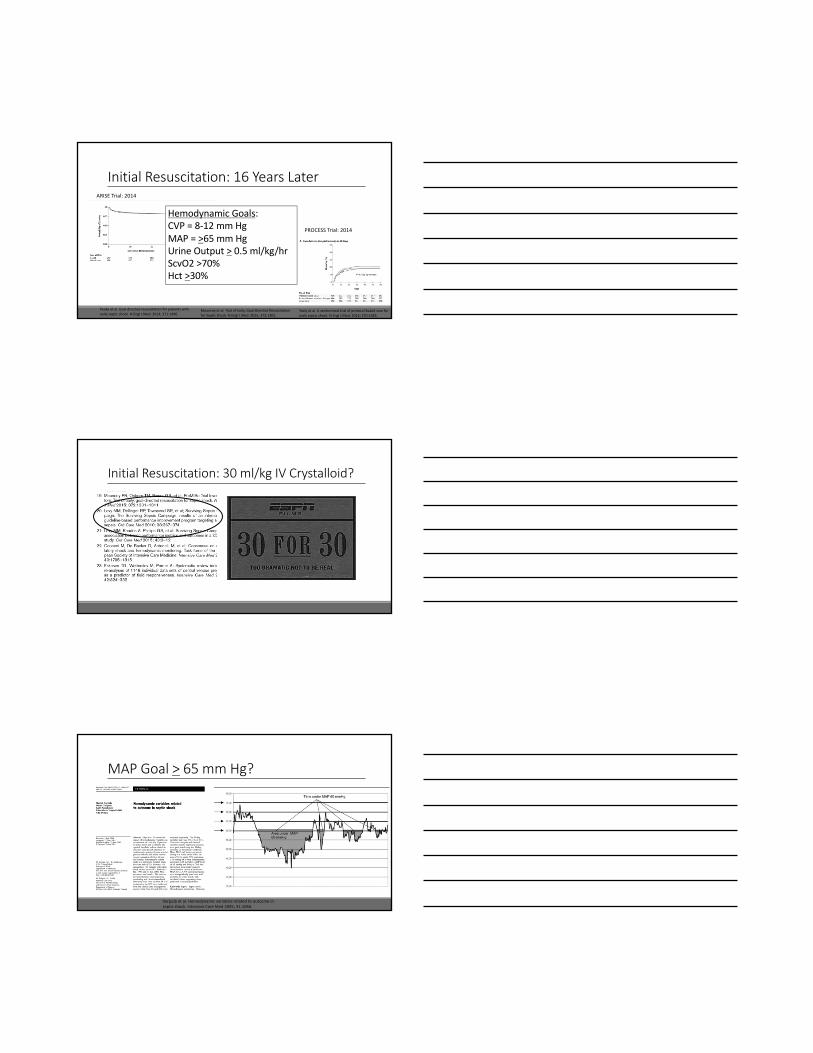
InitialResuscitation:16YearsLaterARISETrial:2014
PROMISETrial:2014
PROCESSTrial:2014
HemodynamicGoals:CVP=8-12mmHgMAP=>65mmHgUrineOutput> 0.5ml/kg/hrScvO2>70%Hct >30%
Mouncey etal.TrialofEarly,Goal-DirectedResuscitationforSepticShock.NEngl JMed.2015;372:1301.
Peakeetal.Goaldirectedresuscitationforpatientswithearlysepticshock.NEngl JMed.2014;371:1496.
Yealy etal.Arandomizedtrialofprotocol-basedcareforearlysepticshock.NEngl JMed.2014;370:1683.
InitialResuscitation:30ml/kgIVCrystalloid?
MAPGoal> 65mmHg?
Varpula etal.Hemodynamicvariablesrelatedtooutcomeinsepticshock.IntensiveCareMed2005;31:1066.
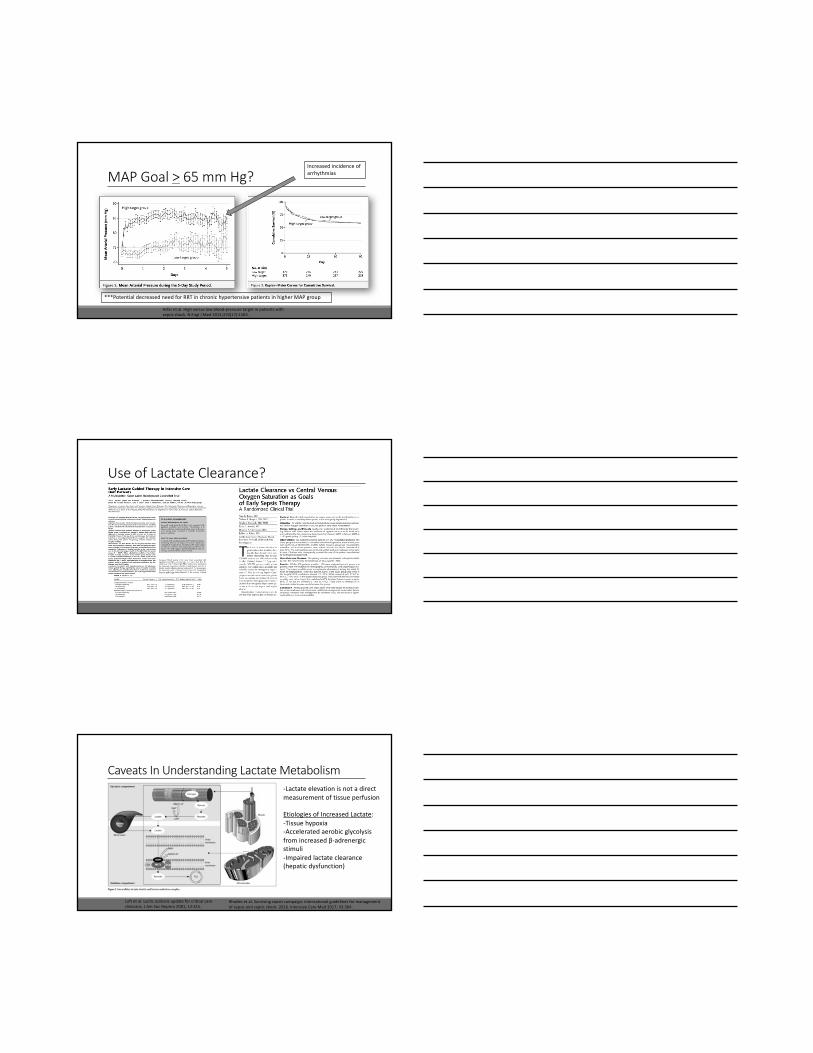
MAPGoal> 65mmHg?
Asfar etal.Highversuslowblood-pressuretargetinpatientswithsepticshock.NEngl JMed2014;370(17):1583.
Increasedincidenceofarrhythmias
***PotentialdecreasedneedforRRTinchronichypertensivepatientsinhigherMAPgroup
UseofLactateClearance?
CaveatsInUnderstandingLactateMetabolism-Lactateelevationisnotadirectmeasurementoftissueperfusion
EtiologiesofIncreasedLactate:-Tissuehypoxia-Acceleratedaerobicglycolysisfromincreasedβ-adrenergicstimuli-Impairedlactateclearance(hepaticdysfunction)
Luft etal.Lacticacidosisupdateforcriticalcareclinicians.JAmSoc Nephro 2001;12:S15.
Rhodesetal.Survivingsepsiscampaign:internationalguidelinesformanagementofsepsisandsepticshock:2016.IntensiveCareMed2017;43:304.
InitialResuscitation:InterimSummary-Actquickly oncesepsissyndromerecognized/entertained-30ml/kgIVcrystalloidadministrationinthe1st 3hours-Additionalfluidshouldbeadministeredbaseduponfrequentdynamicassessment-Initialtargetmeanarterialpressure(MAP)of65mmHg-Guideresuscitationtonormalizelactate
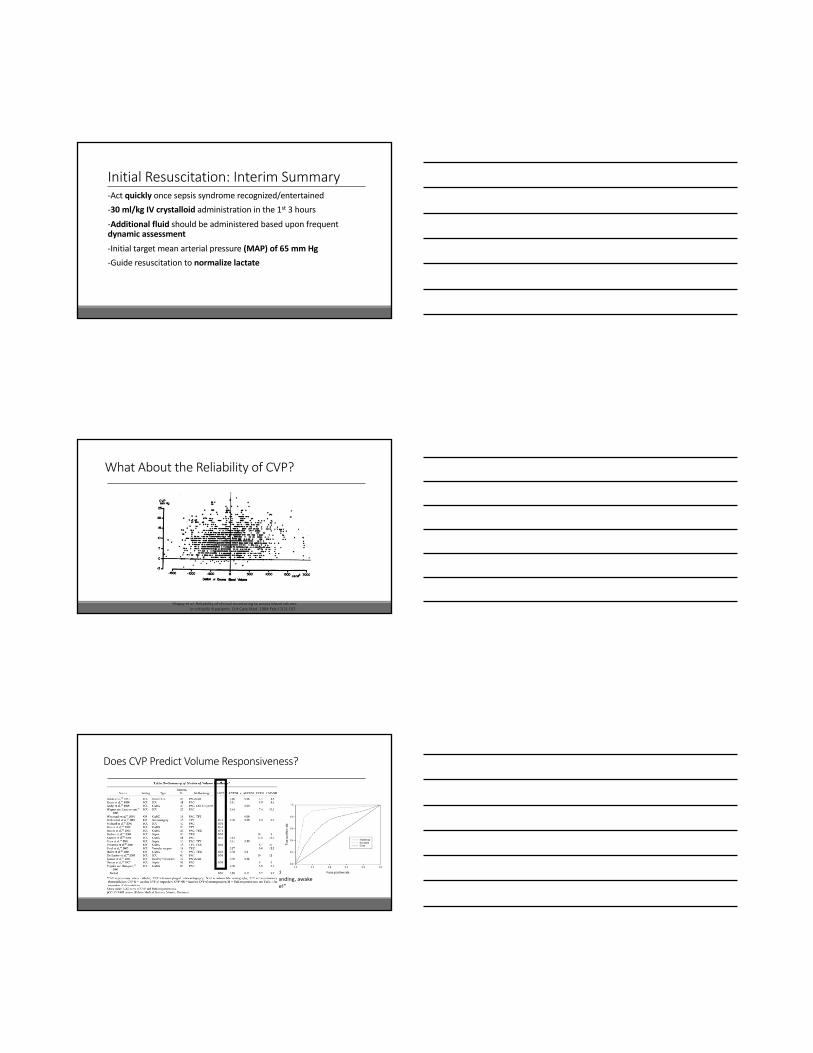
WhatAbouttheReliabilityofCVP?
Shippy etal.Reliabilityofclinicalmonitoringtoassessbloodvolumeincriticallyillpatients.Crit CareMed.1984Feb;12(2):107.
DoesCVPPredictVolumeResponsiveness?
“TheonlystudywecouldfinddemonstratingtheutilityofCVPinpredictingvolumestatuswasperformedinsevenstanding,awake
maresundergoingcontrolledhemorrhage!”

DynamicVolumeAssessment:HowMuchIsEnough?
EchocardiographicAssessment
PulsePressureVariation(PPV)
Bioreactance
WhatFluidShouldWeGive?
WhatFluidShouldWeGive?
BottomLine:-Noheadtoheadcomparisonbetweencrystalloids-LimitedevidencemaypointtowardsCl- restrictiveoverCl-liberalcrystalloidtodecreaserenalinjury-Somestudieshavesuggestedimprovedmortalitywithuseofalbumin(colloid)particularlyinlowalbuminstates,butnotasprimaryresuscitationfluid-Evidencesuggestsincreasedmortality/increasedRRTneed
Haase etal.Hydroxyethylstarchversuscrystalloidoralbumininpatientswithsepsis:systematicreviewwithmeta-analysisandtrialsequentialanalysis.BMJ2013;346:839.
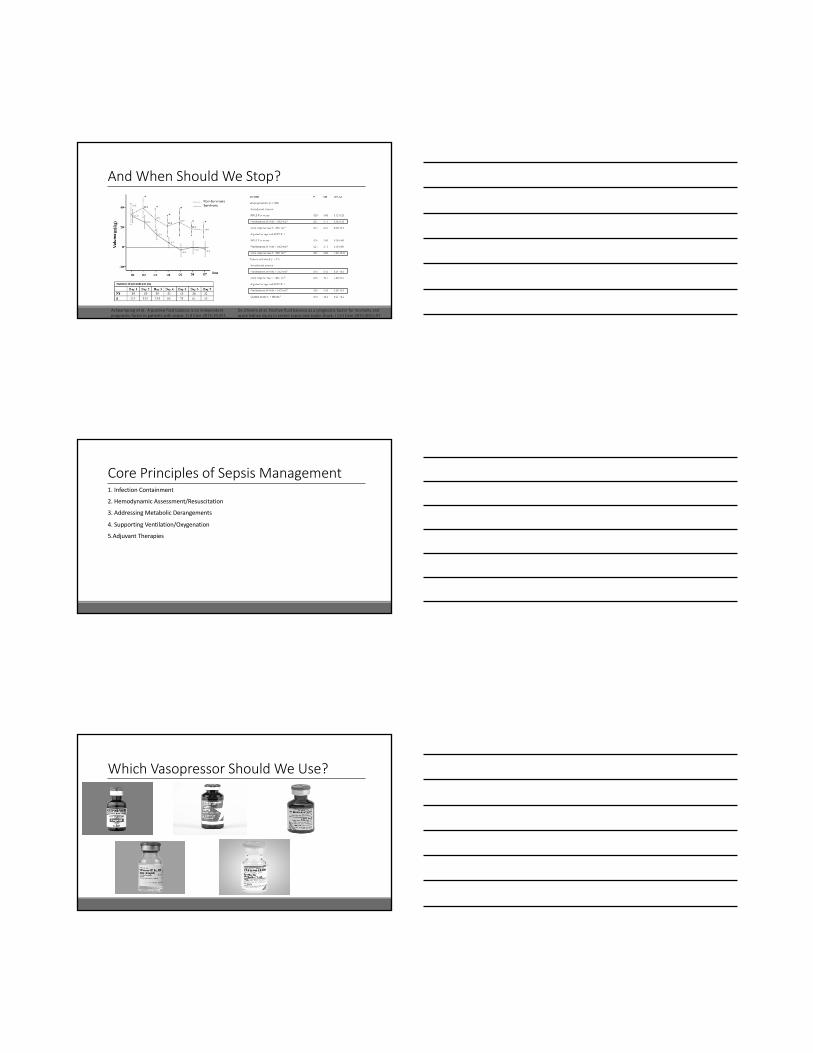
AndWhenShouldWeStop?
Acheampong etal.Apositivefluidbalanceisanindependentprognosticfactorinpatientswithsepsis.Crit Care2015;19:251.
DeOliveiraetal.Positivefluidbalanceasaprognosticfactorformortalityandacutekidneyinjuryinseveresepsisandsepticshock.JCrit Care2015;30(1):97.
CorePrinciplesofSepsisManagement1.InfectionContainment
2.HemodynamicAssessment/Resuscitation
3.AddressingMetabolicDerangements
4.SupportingVentilation/Oxygenation
5.AdjuvantTherapies
WhichVasopressorShouldWeUse?

CurrentControversiesinSepsisManagement
RoleofVitaminS?
Marik etal.Hydrocortisone,vitaminc,andthiamineforthetreatmentofseveresepsisandsepticshock.Chest2017;151(6):1229.
RoleofVitaminS?
Marik etal.Hydrocortisone,vitaminC,andthiamineforthetreatmentofseveresepsisandsepticshock.Chest2017;151(6):1229.

RoleofBeta-BlockadeandSepsis?
Morellietal.EffectofHeartRateControlWithEsmolol onHemodynamicandClinicalOutcomesinPatientsWithSepticShock.JAMA2013;310(16):1683.
RoleofBeta-BlockadeandSepsis?
Morellietal.EffectofHeartRateControlWithEsmolol onHemodynamicandClinicalOutcomesinPatientsWithSepticShock.JAMA2013;310(16):1683.
Questions?
ReviewQuestionsQ1.Promptvolumeresuscitation/volumestatusassessmentiscriticaltotheearlystagesofsepsismanagement.However,increasedevidencesuggeststhatfluidbalanceinthelatestagesofsepsistreatmentisalsolikelytobeimportant.WhichofthefollowinghasNOT beenassociatedwithpositivefluidbalanceinthepost-resuscitativesepticpatient.A)Ongoingpersistenceofapositivedailyfluidbalanceoverhospitalizationdemonstratesanassociationwithahighermortalityrateinsepticpatients.B)Volumeoverloadisindependentlyassociatedwithimpairedmobilityanddischargetoahealthcarefacility.
C)Positivefluidbalanceinpost-resuscitationsepticpatientsisassociatedwithprotectionagainstthedevelopmentofacutekidneyinjury.D)Positivefluidbalanceinpost-resuscitationsepticpatientsconstitutesariskfactorforneworgansystemdysfunctionathospitaldischarge.
ReviewQuestionsQ1.Promptvolumeresuscitation/volumestatusassessmentiscriticaltotheearlystagesofsepsismanagement.However,increasedevidencesuggeststhatfluidbalanceinthelatestagesofsepsistreatmentisalsolikelytobeimportant.WhichofthefollowinghasNOT beenassociatedwithpositivefluidbalanceinthepost-resuscitativesepticpatient.A)Ongoingpersistenceofapositivedailyfluidbalanceoverhospitalizationdemonstratesanassociationwithahighermortalityrateinsepticpatients.B)Volumeoverloadisindependentlyassociatedwithimpairedmobilityanddischargetoahealthcarefacility.
C)Positivefluidbalanceinpost-resuscitationsepticpatientsisassociatedwithprotectionagainstthedevelopmentofacutekidneyinjury.D)Positivefluidbalanceinpost-resuscitationsepticpatientsconstitutesariskfactorforneworgansystemdysfunctionathospitaldischarge.
ReviewQuestionsAnswerQ1.Emergingdataappearstosuggestthatpersistentpositivefluidbalanceinthepost-resuscitativesepticpatientisanindependentriskfactorassociatedwithhighermortality,increasedlikelihoodofimpairedimmobility/readinessforpost-hospitaldischarge,increasedlikelihoodofdevelopingacutekidneydisease,aswellasincreasedriskfordevelopinganeworgandysfunctionbythetimeofhospitaldischarge.Whiledatacontinuestogrow,suchfindingsunderscoretheimportanceofprompt,aggressivevolumeresuscitationintheearlystagesofsepsis/septicshock.However,thepost-resuscitationperiodrequirescarefulattentiontoongoingvolumestatusassessment,avoidanceofexcessiveIVF,andpotentialneedforinterventionstonormalizevolumestatus(i.e.diuretics,mobilization).
References:Acheampong etal.Apositivefluidbalanceisanindependentprognosticfactorinpatientswithsepsis.Crit Care2015;19:251.Brotfain etal.Positivefluidbalanceasamajorpredictorofclinicaloutcomeofpatientswithsepsis/septicshockafterICUdischarge.AmJEmerg Med2016;34(11):2122.Mitchelletal.Volumeoverload:prevalence,riskfactors,andfunctionaloutcomeinsurvivorsofsepticshock.AnnAmThorac Soc.2015;12(12):1837.DeOliveiraetal.Positivefluidbalanceasaprognosticfactorformortalityandacutekidneyinjuryinseveresepsisandsepticshock.JCrit Care2015;30(1):97.Malbrain MLetal.Fluidoverload,de-resuscitation,andoutcomesincriticallyillorinjuredpatients:asystematicreviewwithsuggestionsforclinicalpractice.AnaesthesiolIntensiveTher.2015;46(5):361.

ReviewQuestionsQ2.Whilelactateisnotadirectmeasureoftissueperfusion,increasedlactatelevelsareassociatedwithunfavorableclinicaloutcomes.Thuslactateitisoftenutilizedasanindirectmarkertoassistintheguidanceofresuscitationinsepsis/septicshock.Whichofthefollowingisnotapredominantlycontributingsourceofincreasedserumlactate?
A)Acceleratedaerobicglycolysisfromincreasedβ-adrenergicstimuli
B)Impairedlactateclearanceviahepaticdysfunction
C)Tissuehypoxia
D)Impairedlactateclearanceviarenaldysfunction
ReviewQuestionsQ2.Whilelactateisnotadirectmeasureoftissueperfusion,increasedlactatelevelsareassociatedwithunfavorableclinicaloutcomes.Thuslactateitisoftenutilizedasanindirectmarkertoassistintheguidanceofresuscitationinsepsis/septicshock.Whichofthefollowingisnotapredominantlycontributingsourceofincreasedserumlactate?
A)Acceleratedaerobicglycolysisfromincreasedβ-adrenergicstimuli
B)Impairedlactateclearanceviahepaticdysfunction
C)Tissuehypoxia
D)Impairedlactateclearanceviarenaldysfunction
ReviewQuestionsAnswerQ2.
Aslactateisincreasinglyusedasasurrogatefortissueperfusion/tissuehypoxia,itisimportanttounderstandthevariousphysiologicandpathophysiologicstatesthatcanresultinitsaccumulation.Lactateelevationhasbeenlinkedtoincreasedtissuehypoxia,increasedproductioninthecontextofincreasedaerobicglycolysisfromexcessiveβ-adrenergicstimuli,andimpairedclearanceinthecontexthepaticdysfunction.Whilethekidneysdoindeedparticipateinlactatemetabolism(viaexcretion,gluconeogenesis,andoxidation),itisonlyestimatedtoberesponsiblefor~10-20%oftotallactatemetabolism.Theliver,however,isestimatedtoberesponsiblefor~70-75%oftotallactatemetabolism.
References:Rhodesetal.Survivingsepsiscampaign:internationalguidelinesformanagementofsepsisandsepticshock:2016.IntensiveCareMed2017;43:304.Luft etal.Lacticacidosisupdateforcriticalcareclinicians.JAmSoc Nephro 2001;12:S15.